
Submitted:
03 June 2024
Posted:
04 June 2024
You are already at the latest version
Abstract
The complexity of the current social context leads healthcare professionals to deal daily with users who are increasingly varied in terms of culture, language and religion. Transcultural nursing is a practical discipline that aims to respond to the patient's need for assistance, but must not ignore the study and knowledge of the patient, with his history, his culture, but also with his expectations, in order to respond to his care needs with effectiveness, efficiency, adequacy and respect. This work originates from the desire to investigate the "state of health" of the relationship between nurses/health workers and migrant patients, researching the variables that improve or worsen it. It aims to investigate how diversity affects the care provided to migrant people, highlighting the difficulties felt by nurses and define the areas of possible care improvements. It seems possible to affirm that the nurses and health workers interviewed still respond to the problem of migrant patients with a strong spirit of participation and availability, without, however, this motivational charge being accompanied by a widespread "nursing" awareness of the problem.
Keywords:
Migrants
; Transcultural nursing
; Nurse-migrant patient relation
1. Introduction
The complexity of the current social context leads healthcare professionals to deal daily with users who are increasingly varied in terms of culture, language and religion.
Once upon a time, "different" was synonymous with extraneous because it was actually distant. It was rare to meet or know a "foreigner", and he was in any case always easily distinguishable by a strong belonging to each other's cultural identity. One of the reasons that pushed the cultured man of the past to travel was certainly to get to know "peoples staff during production. and customs" different from his own, aware of their intrinsic richness. Now, however, this stranger has come closer, while remaining a stranger; he settled down without, however, most of the time, being completely integrated. And now the "different" that name was encountered in travel, in cuisine or in "ethnic" music, is close at hand, in schools, markets, hospitals, sometimes also with social tensions on a political, economic, religious and moral level.
Foreigners - considered "different" due to the color of their skin, language, lifestyle habits and professed religion - often also arouse in healthcare workers, despite the ethical mandate, unconscious fears and sometimes rejection, as they are influenced by the social context which is not very oriented towards the culture of the different; the result is the behavior of treating all patients in the same way, acting on people, without considering their cultural and emotional matrix.
Nurses are often the first contact that emigrants have with a healthcare facility. In car- rying out the care process, the nurse must be able to deal with patients of different cul- tures, examining in depth the issues related to immigrant subjects, considering different elements of the care process, including ethnic-cultural, relational, linguistic, values, legal, organizational-structural features of each specific culture.
Italy is slowly transforming from an ancient country of emigrants into a landing country for immigrants, especially from the poor south of the planet. According to statistical data, there were 5,171,895 foreigners residing in Italy on 1 January 2021 (representing 8.7% of the resident population), 2.5% more than the previous year. The number of foreigners resident during 2021 grew mainly as a result of immigration from abroad, but, in part, also due to the births of foreign children[1]. The statistical data show us a growing gap between the group of extremely poor countries (including the countries of sub-Saharan Africa and countries with high mortality in Asia, central and south America and in the countries of the eastern Mediterranean) and the rest of the world [2]. From this point of view, certainly the search for better health is an important factor in human mobility, constituting the cause of migratory movements worldwide[3].
The issue of immigration is an unknown reality, whether it is a clash of civilizations or a cultural and resource enrichment, and is therefore feared and viewed with concern and suspicion. This is a phenomenon which, although of notable complexity, can constitute a stimulus and a resource in the dialectic between identity and difference; supporting the culture of interculturality develops awareness of the heritage of civilization and promotes open encounters with other cultures and models of life[4].
In a multicultural society, understanding the health needs of a person or a community necessarily requires a process open to the development of new skills that must be acquired through permanent and continuous learning throughout the entire professional career[5].
We are used to a social context that is not very oriented towards the culture of otherness and to treating all patients in the same way, without considering their different cultural matrices, in the name of a professional ethnocentrism, which must be overcome by inserting the person into his cultural context and setting the assistance taking this into account[6].
1.1. Transcultural Nursing
Transcultural nursing is a practical discipline that aims to respond to the patient's need for assistance, but must not ignore the study and knowledge of the patient, with his history, his culture, but also with his expectations, in order to respond to his care needs with effectiveness, efficiency, adequacy and respect. The transcultural approach allows for the cancellation of extraneousness, addresses the problem of cultural otherness, both in the diagnostic moment, asking which nursing problem the person is suffering from, and in the prescriptive one, asking how he can be helped[7,8].
With transcultural nursing, the healthcare professional discovers all the needs of the patient, including cultural and social ones, understanding that all social structures, such as religion, culture, kinship, are linked to care and health.
1.2. Italian Research Survey on the Problems Experienced by Nurses in the Care of Foreign People
This work originates from the desire to investigate, even in our own small way, the "state of health" of the relationship between nurses/health workers and migrant patients, researching the variables that improve or worsen it. In fact, if it is known that the quality of the relationship between nurses/health workers and patient co-determines the final result of assistance, this is not the same in the presence of belonging to other cultures, when the protagonists of the healthcare situation do not recognize themselves in the same influence socio-cultural.
1.3. Objective and Plan of the Study
This work aims to investigate how diversity affects the care provided to migrant people, highlighting the difficulties felt by nurses and define the areas of possible care improvements.
The subject of the investigation was a group of 29 professionals including 20 nurses and 9 social and healthcare workers from the Pneumology Operating Unit of a hospital in the Italian province (Cittadella, Padua), who during the year 2022 assisted migrant patients in hospitalization.
Pneumology local services were excluded from the study, even though they were very frequented by migrants, preferring to study the migrant topic during hospitalization, which is therefore more long-lasting.
2. Materials and Methods
The survey tool consists of an anonymous questionnaire made up of 11 questions. The questionnaire is divided into three parts: the first part contains general descriptive questions of the group; the second investigates the global perception of the migratory phenomenon by nurses/health workers and the third aims to investigate the relational and emotional sphere in the relationship between nurses and foreign patients.
In the questionnaire, a control question was formulated, placed at a certain distance from the question to which it referred and aimed at evaluating the reliability of the answers provided on an item considered fundamental, as it implies nursing responsibility for the object of study. The two questions read respectively: "In your opinion, in which cases is it necessary to consider the socio-cultural background of patients to provide good nursing care?" (question n. 8) and "In your opinion, are the patient's nursing care needs influenced by his/her socio-cultural origin?" (question n. 6).
The questionnaires were personally delivered to the professionals; everyone had been adequately informed in advance about the investigation criteria and the approach methods. The delivery and collection of the questionnaires took place at a fixed interval of 16 days, so that all nurses and operators had the time and opportunity to complete the questionnaire. Additionally, interviewees were provided with a cover letter, which explained the objectives of the study. This letter was shown 2 days before the administration of the questionnaire.
Data obtained from the questionnaires were summarized using double-entry tables, thanks to which it was possible to calculate the frequencies and make graphs. In some tables the average values are calculated, in order to summarize the different characteristics with which a phenomenon manifested itself with a single numerical value, in order to make it more representative.
3. Results
18 responses were collected, so the group's compliance with the survey was 62.06%. Those who did not respond to the questionnaire were nurses and health workers who did not consider it necessary to participate in the study, or were absent during the survey period.
As far as qualifications are concerned, the majority of those interviewed (72%) have a degree in nursing, 6% have a university diploma for nurses and 5% of those interviewed have a regional diploma for nurses. The “other” item (17%) is represented by Health Workers. Furthermore, it turns out that a nurse interviewed also graduated in Psychol-ogy.
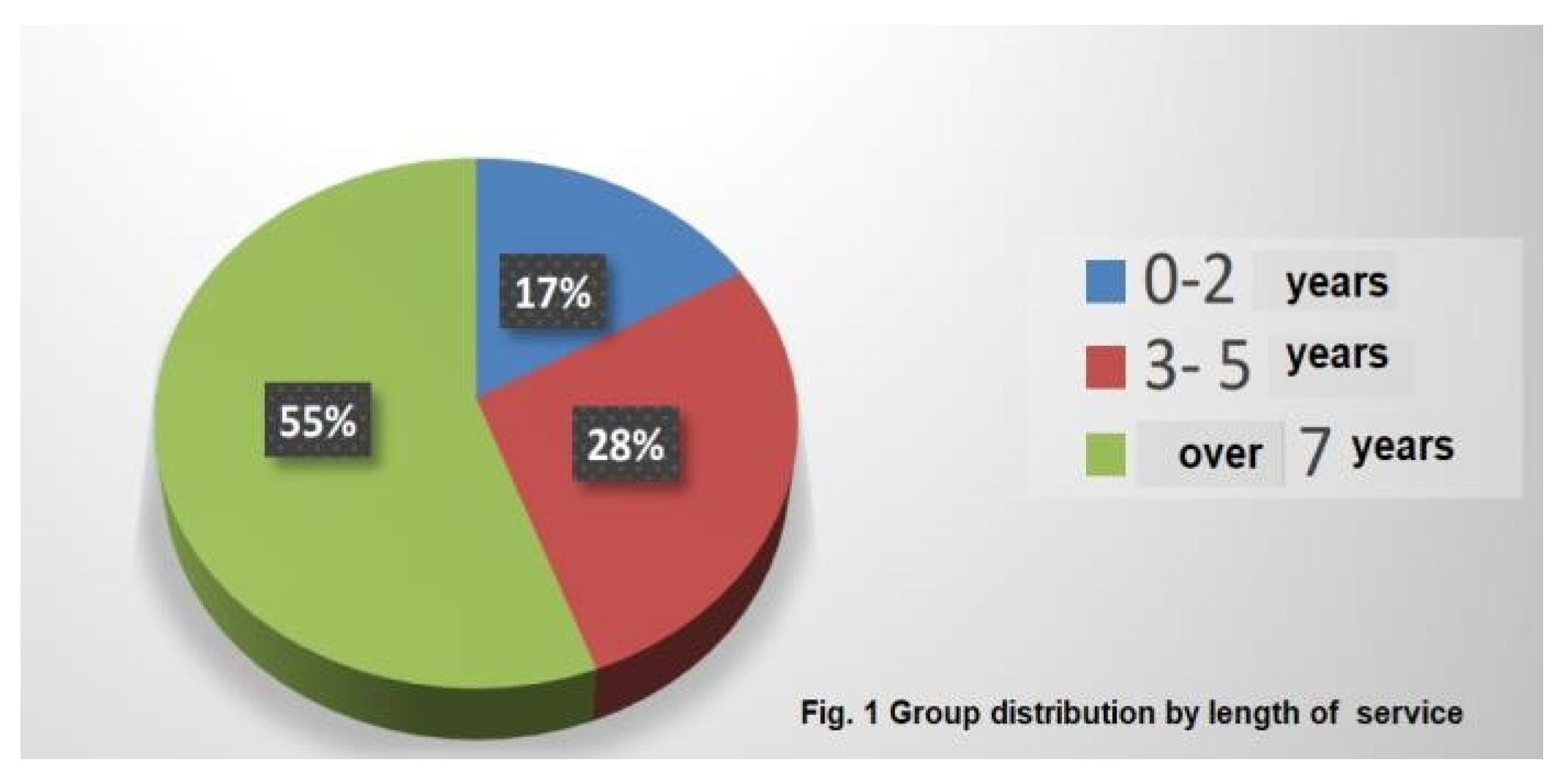
17% of those interviewed de- clared work experience be- tween 0 and 2 years, 28% between 3 and 5 years, while 55% declared more than 7 years. (Figure 1).
91% of nurses/health workers declared professional experi- ence in assisting foreign people. The results of the survey can at this point be presented in two categories:
- (a)
- the description of the global perception of the phenomenon by the nurses/health workers;
- (b)
- the description of the relational and emotional sphere in the relationship between nurse/ health workers and migrant patient.
3.1. The Description of the Global Perception of the Phenomenon by the Nurses/health Workers
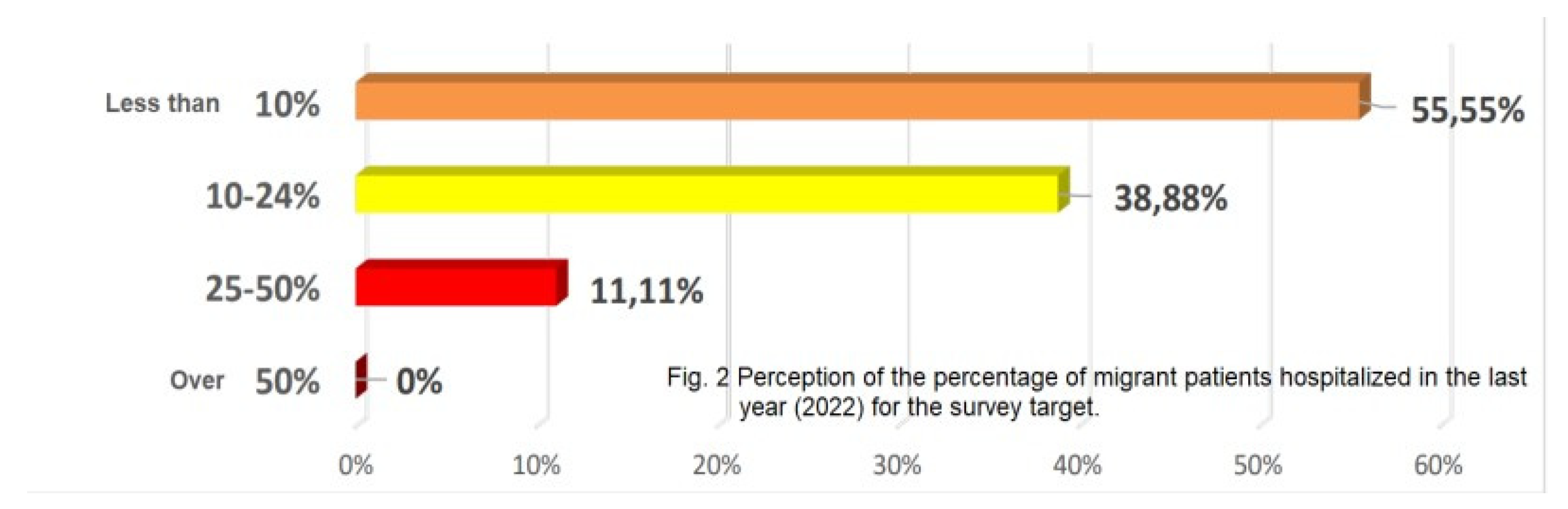
Figure 2 contains the answers to the question asking interviewees what, in their opinion, was the percentage of migrant patients hospitalized at their Operating Unit over the reference year (2022).
55.55% of those interviewed perceived the presence of migrant patients as less than 10% compared to the total number of hospitalized patients, while none of the nurses/health workers perceived the presence of foreign patients as greater than 50%.
The nurses/health workers were asked to make a sort of self-assessment regarding their level of preparation for the problem. Half of the interviewees claim to have good preparation to assist foreign patients; however, the other half believes that it is not adequately prepared to assist this type of user.
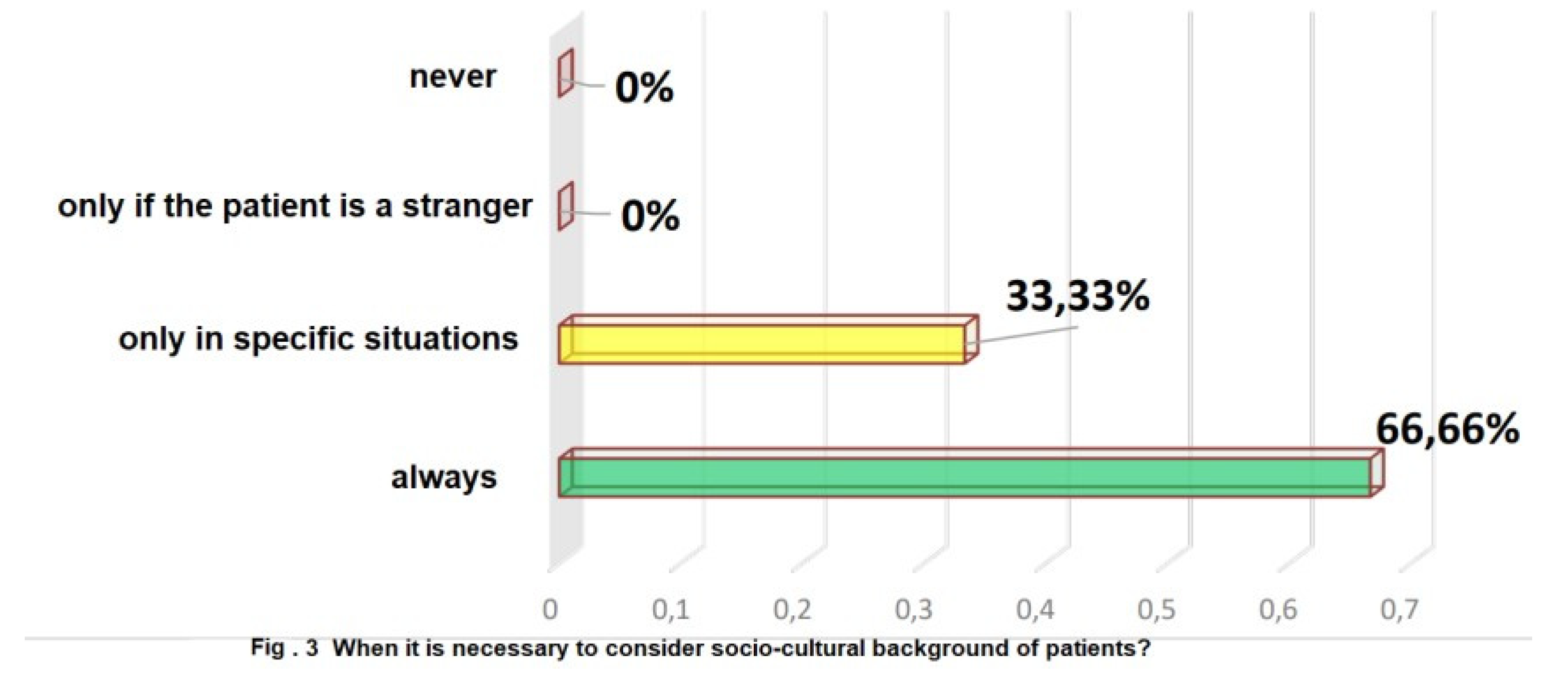
Regarding the answers to the question that investigated in which cases, according to the nurses, it was necessary to consider the socio-cultural origin of the patients in order to provide good and effective care, 66.66% of those interviewed believe it is necessary, in order to provide adequate assistance, to always consider the socio-cultural origin of the patients, 33.33% think that the latter is important only in the presence of particular healthcare situations (Figure 3).
As mentioned before, this particular aspect of the problem, due to its importance, had a control question which aimed to evaluate the reliability of the answers given to the previous one.
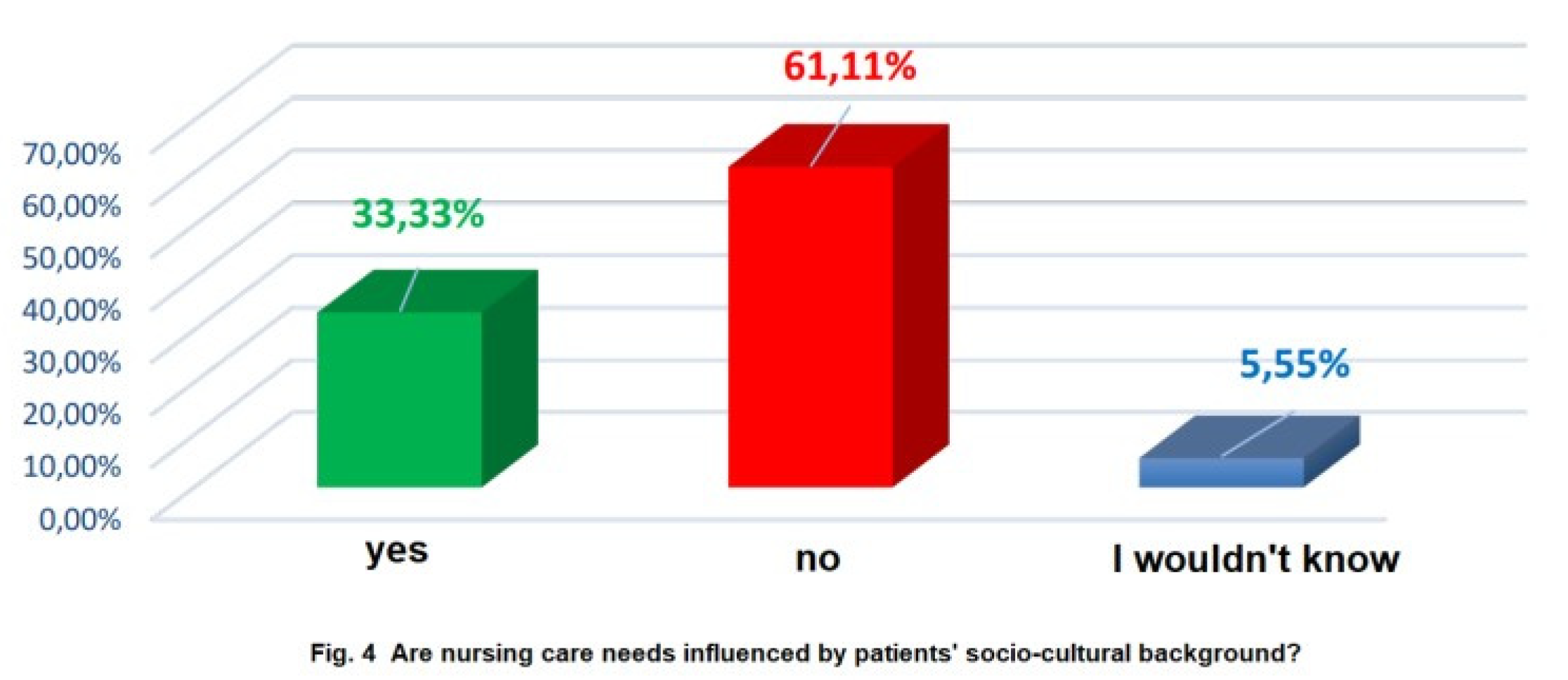
In essence, nurses/health workers were asked whether, in their opinion, patients' nursing care needs are influenced by their socio-cultural belonging. The two questions complement each other because the first probes the interviewees' personal opinion on the issue, while the second probes the professional reasons for this opinion. To this second question, 33.33% of interviewees responded that they believe that patients' nursing care needs are conditioned by their socio-cultural belonging, 61.12% responded "no", while 5.55% stated that they did not know whether the two factors were related to each other (Figure 4).
3.2. Description of the Relational and Emotional Sphere in the Nurse-Migrant Patient Relation
This sub-paragraph presents the data investigating the relational and emotional sphere of nurses/health workers who find themselves in contact with migrant patients.
A general evaluation shows that for the nurses and health workers interviewed, the relationship with a migrant patient appears rewarding. However, the indication of frustration emerges in 67%, although perhaps less frequently than might have been expected.
The work also investigated the main relational problems encountered in the approach with migrant patients. Aggregating these responses, the types of problems encounteredby nurses and health workers were, in order of importance, the following:
- language-communication (94%);
- misunderstanding of the socio-cultural, ethical and religious values of reference (50%);
- social and health legislation (22%);
- definition of health care priorities (17%);
- nurses' prejudices towards patients and respect for hospital rule (1%)
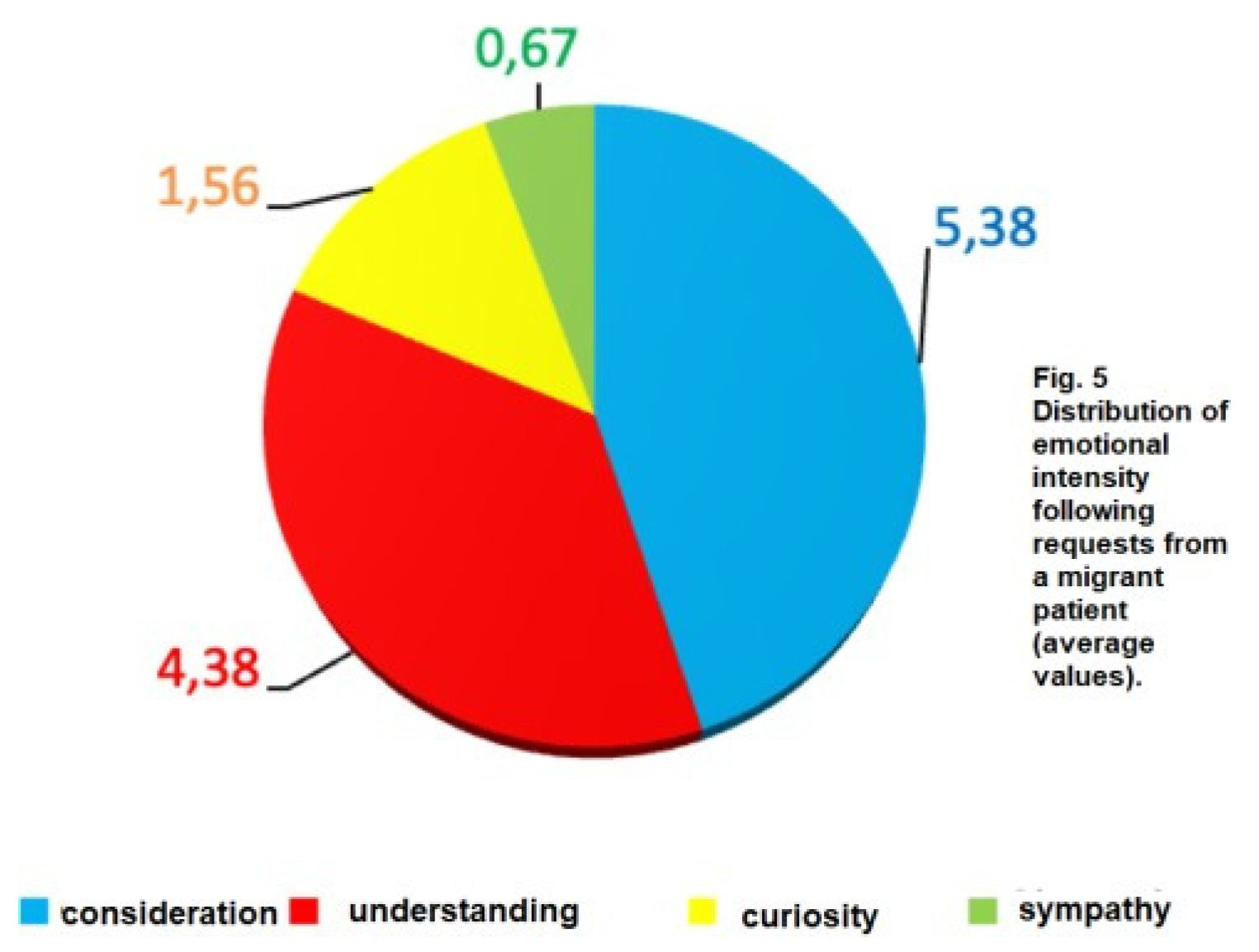
Very interesting are the emotional reactions aroused in nurses and health workers following the needs of a migrant patient. It appears that understanding and respect are the most significant feelings aroused by the relationship with the foreign patient; someone feels fear, conflicting feelings such as suffering, hostility and resentment are not present. It should be noted that feelings such as curiosity have an important relevance, while sympathy is only felt by an interviewee. Finally, it is interesting to note which target expresses the full range of "positive" feelings expected from the question.
By aggregating the average values recorded on the entire group interviewed for this question, the distribution of emotional intensity shown in Figure 5 is recorded. Note that the presence of only "positive" feelings is highlighted.
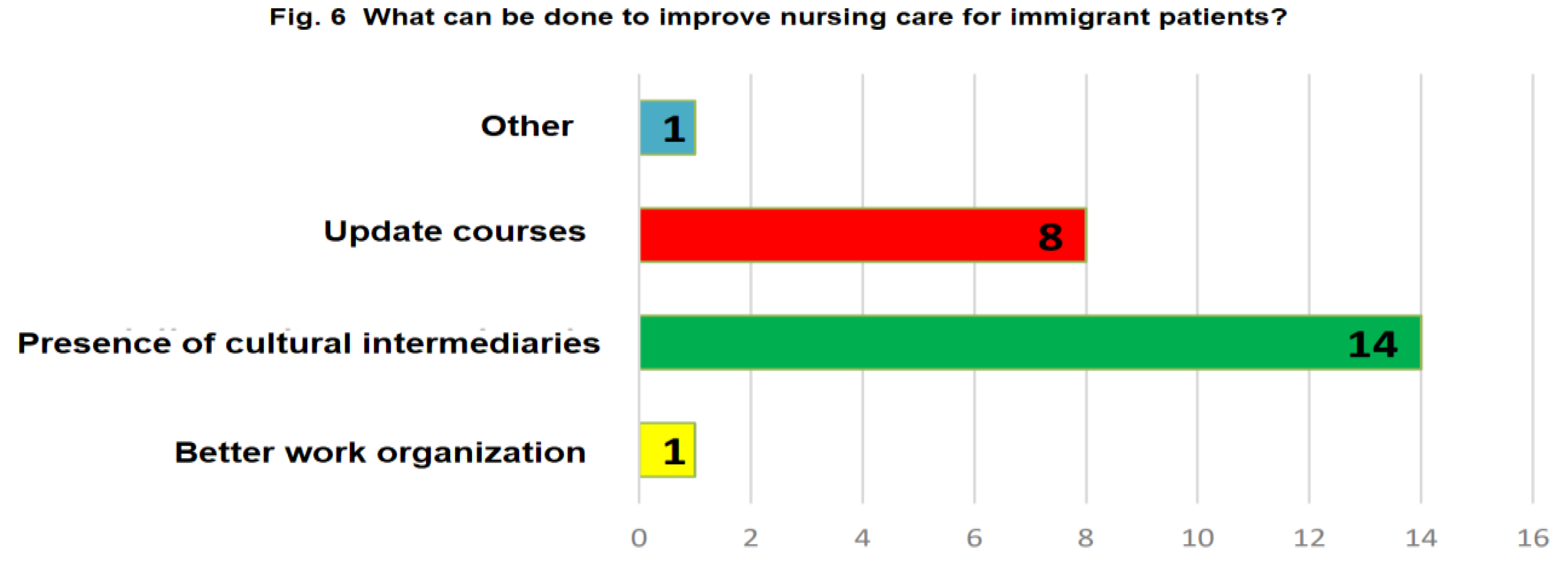
Finally, nurses and health workers were asked what, in their opinion, it would be useful to do to improve the care offered to migrant patients (Figure 6). It is clear that cultural mediation followed by the in-depth study of transcultural nursing were considered the most important elements for improving nursing care.
The interviewees do not feel a great need to improve work organization. Only on one occasion was the answer "other" found and was reported the following wording: "enrich the general culture of the operators (nurses/health workers) to better understand the cultural and religious differences of the patients. Often healthcare personnel have a poor understanding of other cultures simply due to personal ignorance."
4. Discussion
As a first note, it is observed that 55.55% of the interviewees perceive the numerical percentage of migrant patients as less than 10% of total hospitalizations, while the majority of nurses/health workers of the remaining half showed a significant overestimation of the phenomenon, perceiving the percentage of migrant patients between 10 and 24% of hospitalizations. According to the data obtained from the hospital register of the department, the hospitalizations of foreign citizens in the year 2022 at the Operational Unit involved in the study (residents and non-residents in Italy) were found to be equal to 5% .
As regards the main problems that the group reports as most frequent in the approach and relationship with migrant patients, they concern, first of all and as one might expect, communication and language in 94%. What is best understood is the difficulty in explaining the hospital rules that concern these patients. This difficulty may be perceived by the patient as a form of unfair "discrimination" against them and give rise to, or increase, a negative prejudice towards healthcare personnel.
The data concerning the emotional reactions aroused in interviewees by contact with a migrant patient deserve extreme interest. It was seen that nurses and health workers consider contact with migrants as "rewarding" (67%), except for 6 interviewees who consider it "frustrating". It should be noted, however, that the emotional reactions aroused by the requests and the relationship with migrant patients are almost all, if they can be defined as such, "positive" and are, in decreasing order of importance: understanding, respect, curiosity and sympathy. 3 interviewees chose the item "other", writing the following notes: "emotional reaction depends on the requests", "listening" and "impossibility of satisfying it".
A further note of great operational interest emerges from the questions that probed the perception of direct nursing responsibility for the problem. To the first question, the interviewees who answered that to provide good care it is always necessary to consider the socio-cultural origin of the patients were 66.66%, but in the control question the percentage of those who believed that nursing care needs are always influenced by culture it falls to 33.33%. At the same time, the percentage of those who in some way deny a direct influence of culture in the work of nurses and obstetricians rises from 0% of those interviewed in the first question (those who believe that it is never necessary to consider the socio-cultural origin of patients) to 61.11% in the control question (who believe that socio-cultural origin does not influence the need for assistance), to which we must add 5.55% of undecided. Consequently, it seems correct to maintain that more than half of the interviewees are not clear on why it is essential to consider the cultural origin of each patient in the scientific disciplinary. In other words, it is not clear that it is always necessary to investigate the socio-cultural origin of all patients as it always influences the manifestation of nursing care needs. Half of the interviewees stated that they had inadequate training to deal with the problem.
It seems possible to affirm that the nurses and health workers interviewed still respond to the problem of migrant patients with a strong spirit of participation and availability, without, however, this motivational charge being accompanied by a widespread "nursing" awareness of the problem.
In other words, the hypothesis that seems possible to make is that as the migratory phenomenon grows, there is the risk of a "negative" emotional response, especially if the conceptual, methodological and organizational tools that could help nurses and health workers in situations of friction or conflict with the cultural diversity of their patients. The need, or rather the urgency, of specific training on these issues seems well-established, and it is an urgency that is perhaps strongest where it is least perceived by those directly involved.
5. Conclusions
The confrontations and relational difficulties that often occur between culturally different individuals are widespread and often profound. In the nursing context, the professional community has expressly declared the need to orient the development of the profession in a coherent way with respect to the path undertaken in the social sphere. Precisely for this reason it seems fundamental today to recover "the centrality of the human being" in his physical-psycho-social entirety, also considering cultural differences.
This study highlights the need to intervene in the organizational context with specific technical-operational approaches with a significant impact on the solution of nursing problems, so as to attribute concrete effectiveness to professional interventions; to ade-quately strengthen the conceptual, methodological and organizational tools, which could help nurses and health workers in situations of friction or conflict with the cultural otherness of their patients; to carry out specific training for these problems.
The identity of the culture to which one belongs is a value that must be known and understood [9]. This is why the training of healthcare personnel is important, which includes not only linguistic and medical knowledge of the main pathologies of the countries of origin or of the environmental impact and of the practices that can be implemented in the current legal context of the same conceptions of life and death, of health and of the disease. It is necessary to prepare healthcare personnel for a culture of hospitality and solidarity in the perspective of transcultural medicine, while still respecting ethics and the law.
Today, transcultural nursing and the trend towards globalization of healthcare stimulate healthcare professionals to acquire information relating to different cultures [10]. The growing number of immigrants, refugees and other people from different cultures makes transcultural nursing indispensable for today's and tomorrow's nurses to provide appropriate care to these people.
It is important that the healthcare professional does not reduce the patient to a clinical case or an object of treatment, but considers him or her as a person, with all his or her background, experiences, values, cultural model, with which structuring a helping relationship [11].
Author Contributions
Conceptualization, L.D. and L.M.; methodology, L.D. and L.M.; validation, L.D. and L.M; writing—review and editing L.D. and L.M.; supervision, L.M.; All authors have read and agreed to the published version of the manuscript
Funding
“This research received no external funding”
Public Involvement Statement
“No public involvement in any aspect of this research”.
Conflicts of Interest
“The authors declare no conflicts of interest.”
References
- https://www.tuttitalia.it/statistiche/cittadini-stranieri-2021/.
- Mango, L. Health Systems of Underdeveloped and Developing Countries. IJGH 2020, 1/2, 2–3. [Google Scholar] [CrossRef]
- Ambrosio, S. , Mango L. The Migratory Phenomenon in Italy-Access to Health Services. JPHI 2020, 2/3, 15–18. [Google Scholar] [CrossRef]
- UNESCO Convention on the Protection and Promotion of the Diversity of Cultural Expressions Paris 20 October 2005.
- Global Education Guidelines. North-South Centre of the Council of Europe, 2008 Lisbon.
- Vissio G. , Zanini R.C. Dimensioni interculturali nella professione infermieristica. InnovCom Working Papers. 2021 Torino.
- Leininger M. Transcultural nursing: concepts, theories, research and practice. New York: 2002, McGraw-Hill.
- McFarland M.R, Wehbe-Alamah H. Transcultural Nursing Concepts, Theories, Research, & Practice. 4th edition. 2018, Mc Grow-Hill.
- Lee, E. S. , Wechtler, H. Hidden agenda for cross-cultural training: understanding refugees’ cross-cultural experience through the capability approach. The International Journal of Human Resource Management 2024, 35, 1007–1047. [Google Scholar] [CrossRef]
- Tang, C. , Tian, B., Zhang, X., Zhang, K., Xiao, et al. The influence of cultural competence of nurses on patient satisfaction and the mediating effect of patient trust. Journal of Advanced Nursing 2019, 75, 749–759. [Google Scholar] [CrossRef] [PubMed]
- Charon, R. Narrative Medicine: A Model for Empathy, Reflection, Profession, and Trust. JAMA. 2001, 286, 1897–1902. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



