
Submitted:
03 June 2024
Posted:
05 June 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Objective: To analyze prevalence of tuberculosis among the people who presented PIMS with complaints of fever, cough, difficulty in breathing during COVID pandemic.Study Design: Retrospective/ Cross-sectional study.Place and Duration: Department of Radiology, Pakistan Institute of Medical Sciences, Islamabad. 2020-2023. Methods: Total 17121 patients who presented PIMS during COVID pandemic with complaints of high grade fever, cough, difficulty in breathing ,were included in this study. Following the acquisition, the HRCT scans were conducted by a skilled and experienced technician and researcher, utilizing GE Healthcare equipment for HRCT Chest procedures. The scans covered the lung apices to the bases and were executed with maximal inspiration, employing a CT scanner from Toshiba Aquilion. Frequency of TB among all cases was recorded. SPSS 21.0 was used to analyze all data.Results: This study incorporated a total of 17,121 patients, comprising 9,961 (58.1%) males and 7,160 (41.8%) females. The mean age of the enrolled cases was 49.11±7.67 years, demonstrating consistency with the findings of a prior study [33]. This study also examined the prevalence of Tuberculosis in different years based on imaging findings of HRCT chest as follows: in 2020, 582 cases out of 2,450, equivalent to 23.7%; in 2021, 2,377 cases out of 9,584, equivalent to 24.8%; in 2022, 1,099 cases out of 3,913, equivalent to 28.1% and in 2023, 295 cases out of 1,174, equivalent to 25.1%. The average prevalence of TB cases from 2020 to 2023 was determined to be 4,353 cases out of 17,121, which is equal to 25.42%.Conclusion: As per the National Tuberculosis Program (NTP) in Pakistan, the prevalence rate of tuberculosis stands at 340 cases per 100,000 population, equivalent to 0.34%. However, our study reveals an exceptionally high frequency of TB cases. Specifically, the prevalence of Tuberculosis in 2020 was 23.7% (582 out of 2,450), in 2021 it was 24.8% (2,377 out of 9,584), in 2022 it surged to 28.1% (1,099 out of 3,913), and in 2023 it was 25.1% (295 out of 1,174). The average prevalence of TB cases over the period from 2020 to 2023 was calculated at 25.4% (4,353 out of 17,121). Consequently, our findings suggest the presence of a substantial tuberculosis burden in Pakistan, equating to a TB Tsunami in Pakistan.
Keywords:
Tuberculosis
; covid
; prevalence
; tsunami
1. Introduction
Pulmonary tuberculosis is widespread among the poor socioeconomic class. Tuberculosis (TB) is one of the major concerns of society and the leading single cause of death due to infection in the world accounting for three million deaths per year. The World Health Organization (WHO) ranks TB as "the world's most neglected crisis [1].
Pakistan is ranked as the fifth-highest nation contracting tuberculosis in the world [1]. Tuberculosis disease is as high as 0.4 million in Pakistan, including more than 15,000 children. Every year 70, 000 of these patients die. Pakistan bears the fifth greatest TB burden in the world, among which 46000 people died of the illness in 2020 alone. Pakistan still accounts for 61% of the TB burden in the WHO Eastern mediterranean Region [2].
Prior to COVID-19, tuberculosis (TB) was the most common infectious illness and continues to be a major global public health concern [1]. 10.4 million new cases were recorded in 2015, and 10.6 million cases are predicted to be reported in 2021[2]. Approximately 10.0 million new cases of tuberculosis infections and 1.5 million tuberculosis deaths occurred worldwide in 2019 alone.[1] Every year, millions of people worldwide pass away from TB. In 2021, 1.6 million individuals died from tuberculosis (TB), including 187,000 people living with HIV, according to the World Health Organization's (WHO) Global TB report. This is a 4.5% increase from the previous year. In the impoverished world, pulmonary TB remains the most prevalent infectious illness that may spread. With around 3 million deaths per year from infectious diseases in underdeveloped nations, it is one of the biggest causes for concern [3]. The World Health Organization states that tuberculosis is the most neglected infectious illness worldwide [4]. All age groups are affected, with the lower socioeconomic class being more affected. Each person's illness presentation is unique, and it influences some sorts of [5]. Individuals who have active infections exhibit fever, weight loss, hemoptysis, productive cough, and night sweats.[6]
It's unclear why there are these gender variances. These might result from variations in the frequency of infection, the speed at which an infection progresses into an illness, the underreporting of cases involving women, or the accessibility of care. It is often known that there is a link between poverty and tuberculosis (TB), with the poorest members of society having the greatest rates of TB [10]. People with low incomes who live in congested locations and those with limited education are more likely to get tuberculosis [11]. Poor nutrition brought on by poverty may be linked to changes in immunological function. However, poverty that leads to cramped living quarters, inadequate ventilation, and unhygienic behaviors increases the likelihood of tuberculosis [12]. Numerous studies have been carried out to understand people's beliefs, behaviors, and knowledge regarding TB [13,14]. According to an Indian poll, most respondents (93%) had heard of tuberculosis (TB), but only 20.5% had enough understanding of the disease [13].
According to National Tuberculosis Program (NTP), Pakistan ranks 5th amongst the high burden countries in the world. The prevalence, incidence, and mortality per 100,000 population per year from TB in Pakistan are 340, 259 and 20 respectively. In 2001, TB was declared a national emergency then, the Ministry of Health initiated the creation of National TB Program (NTP) which by 2025, aims to reduce the incidence of TB by half as compared to the incidence rate in 2012 The goal of NTP is to “Get back on track to end the TB epidemic by 2030” and mission statement is “Effectively end the TB epidemic in Pakistan by 2035” NTP now is implementing Global Fund assisted grant through a mechanism of Single Stream Funding (SSF) as principal recipient [14] . NTP acts as a collaborating body at the central level for the development of uniform policies and strategies in facilitating donor cooperation at national and international levels [14].
WHO applied a TBIC (TB infection control) policy to counteract the spread of TB in 2009 and Pakistan's national TBIC plan approved this policy [15]. Programmatic Management of Drug-Resistant Tuberculosis (PMDT) model of care in 2010 was introduced by NTP [16,17]. The PMDT program of Pakistan contains a macrosystem at the top, which includes WHO and Global Fund, and a microsystem at the bottom, which includes national and provincial TB programs and NGOs working mutually. NTP formed several clinics throughout the country granting free of cost consultation and medicines for drug resistant TB alongside with contact tracing under the mandatory TB case notification project (MCN). The success rate reached 76% as compared to 10%–46% previously and death rate declined from 40% to 13% by 2011 after the initiation of these clinics [17,18]. Accompanied by NTP, provincial TB program (PTP) is also formed in every province and has parallel aims to eradicate TB by the forthcoming decade. To curtail the gap between notified cases and actual cases, NTP established a Public-Private Mix model (PPM) in 2014 which had 4 groups of the public sector namely TB care provided by NGOs, general practitioner (GP), private hospitals, and other public sector hospitals like Railway hospitals, WAPDA etc. PPM model directed to increase case notifications in the age groups of <15 years and > 54 years [19]. Directly Observed Treatment, Short course (DOTS) is also commenced in all the provinces according to WHO guidelines in which the patients are provided short course drugs along with careful watching of treatment by the health care workers [20]. (Table 1)
To diminish the influence on diagnosis and treatment of TB during COVID 19, numerous methods were taken in different cities like Karachi which include co-screening for COVID 19 and TB in pre-existing TB centers, home delivery of medicines, preservation of protocols for the protection of both the patients and healthcare workers, closely monitoring the mental well-being of health care workers and regular check up on the patients who test positive [22].
For tuberculosis to be effectively controlled, several issues must be resolved, especially in poor nations. These include creating an efficient surveillance system, quickly identifying cases, expanding DOTS to difficult-to-reach areas, fortifying DOTS in urban settings, making sure there is enough staff and laboratory space, involving private practitioners, providing MDR case treatment facilities, identifying TB cases in children and extra-pulmonary cases, and efficiently coordinating efforts amongst healthcare providers [5,26,27]. Furthermore, HIV has an impact on the prevalence of TB, thus both illnesses require efficient control strategies. To enhance diagnostics, create new medications and vaccines, create a straightforward and efficient treatment plan for treating HIV and TB concurrently, increase programmed effectiveness, better understand the connection between TB and chronic illnesses like diabetes and smoking, and pinpoint behavioral and social factors that prevent cases from being detected, more research is necessary [8,28].
In 2022, the funding allocated for Tuberculosis (TB) amounted to $36 million, with 35% coming from domestic sources and the remaining 65% from international sources. However, in the subsequent year, the National TB budget for 2023 experienced a significant increase, reaching $158 million. Despite this augmentation, the distribution of funding sources underwent a notable shift [29]. In 2023, domestic funding comprised only 5.5% of the total budget, while international funding constituted 32%. Shockingly, a substantial 63% of the budget remained unfunded, highlighting a significant gap in financial resources for addressing the pressing public health issue of Tuberculosis. The disparity between the national budget and available funding underscores the urgency for increased support, both domestically and internationally, to effectively combat and control TB in the coming years [29].
In addition to providing some recommendations for resolving these issues, this article aims to highlight the critical importance of Pakistan's TB health surveillance infrastructure and highlight the serious challenges in TB management that have befallen one of the nations with the highest TB burden, Pakistan.
2. Materials and Methods
Tuberculosis (TB) continues to pose a persistent challenge to public health in Pakistan. This study aims to comprehensively assess the impact of this condition through a retrospective/cross-sectional population study utilizing High-Resolution Computed Tomography (HRCT) scans obtained from the Radiology Department at the Pakistan Institute of Medical Sciences (PIMS) spanning a four-year duration. The HRCT scans were conducted by a skilled and experienced technician and researcher, utilizing GE Healthcare equipment for HRCT Chest procedures. The scans covered the lung apices to the bases and were executed with maximal inspiration, employing a CT scanner from Toshiba Aquilion.
The pattern of HRCT included: Centrilobular nodules, Tree-In-Bud, Upper lung Fibrotic changes, Consolidation. Cavity formation, Bronchiectatic changes, Calcific granuloma, Mediastinal lymph nodes.
3. Results
This study incorporated a total of 17,121 patients, comprising 9,961 (58.1%) males and 7,160 (41.8%) females. The mean age of the enrolled cases was 49.11±7.67 years, demonstrating consistency with the findings of a prior study [33].
This study also examined the prevalence of Tuberculosis in different years: 23.7 % (582/2,450) in 2020, 24.8% (2,377/9,584) in 2021, 28.1% (1,099/3,913) in 2022, and 25.1% (295/1,174) in 2023. The average prevalence of TB cases from 2020 to 2023 was determined to be 25.42% (4,353/17,121).
Out of the total cases of 17121, 15.9% presented with previous instances of tuberculosis i.e. 3.1 % seen in 2020; 2.1 % seen in 2021; 5.4 % seen in 2022 and 5.3 % seen in 2023. while 62.2% were newly diagnosed cases i.e. 13.7 % seen in 2020; 18.8% seen in 2021; 15.5% seen in 2022; 14.2% seen in 2023.
And disease reactivation was observed in 23.7 % of the cases. i.e. 7.0 % seen in 2020; 3.9 % seen in 2021; 7.2 % seen in 2022 and 5.6 % seen in 2023.
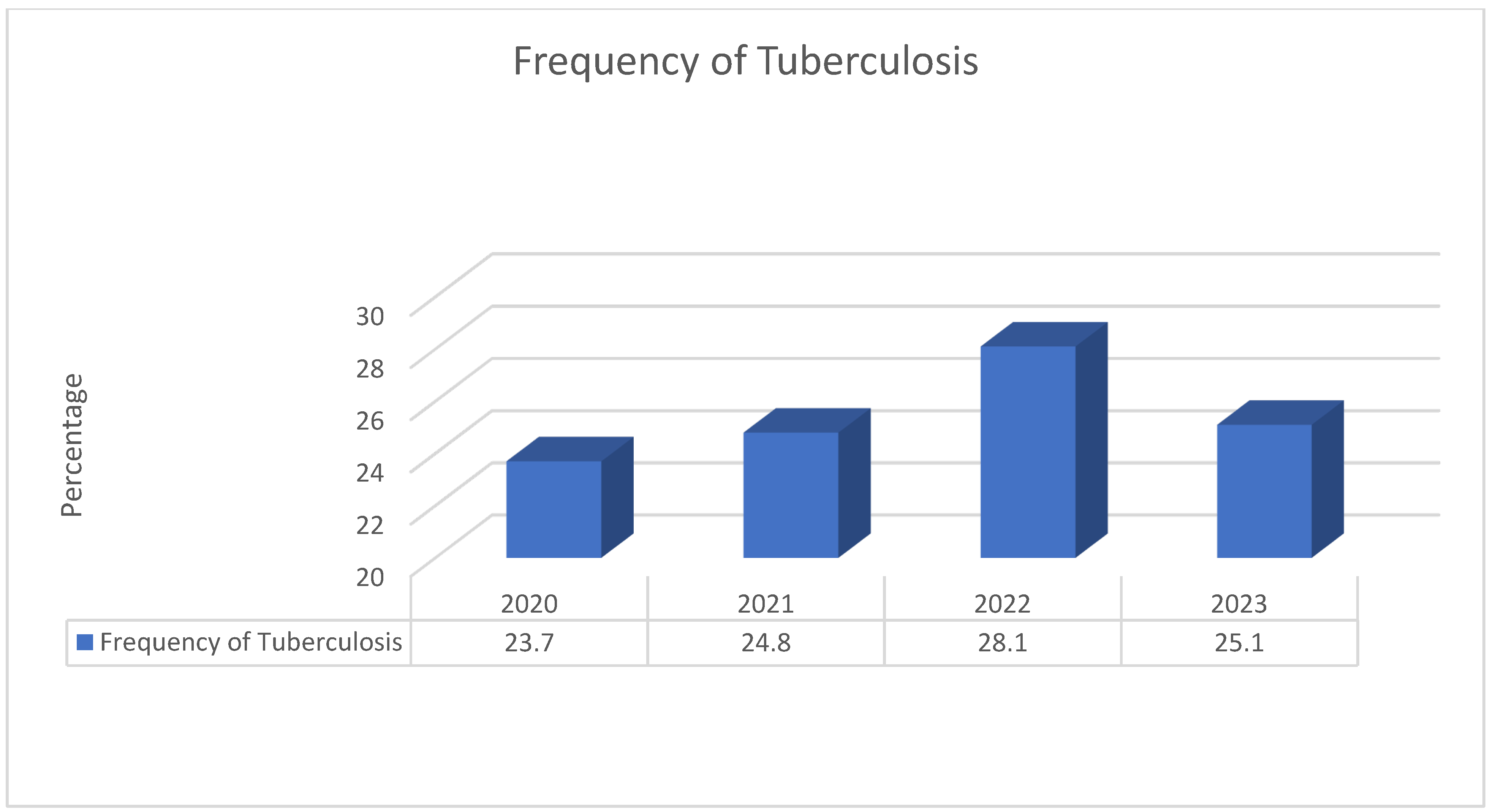
Figure 1.
Frequency of TB cases from 2020 to 2023.
Among 2450 cases of TB in 2020, 36.9% were females and 63.1% were males.
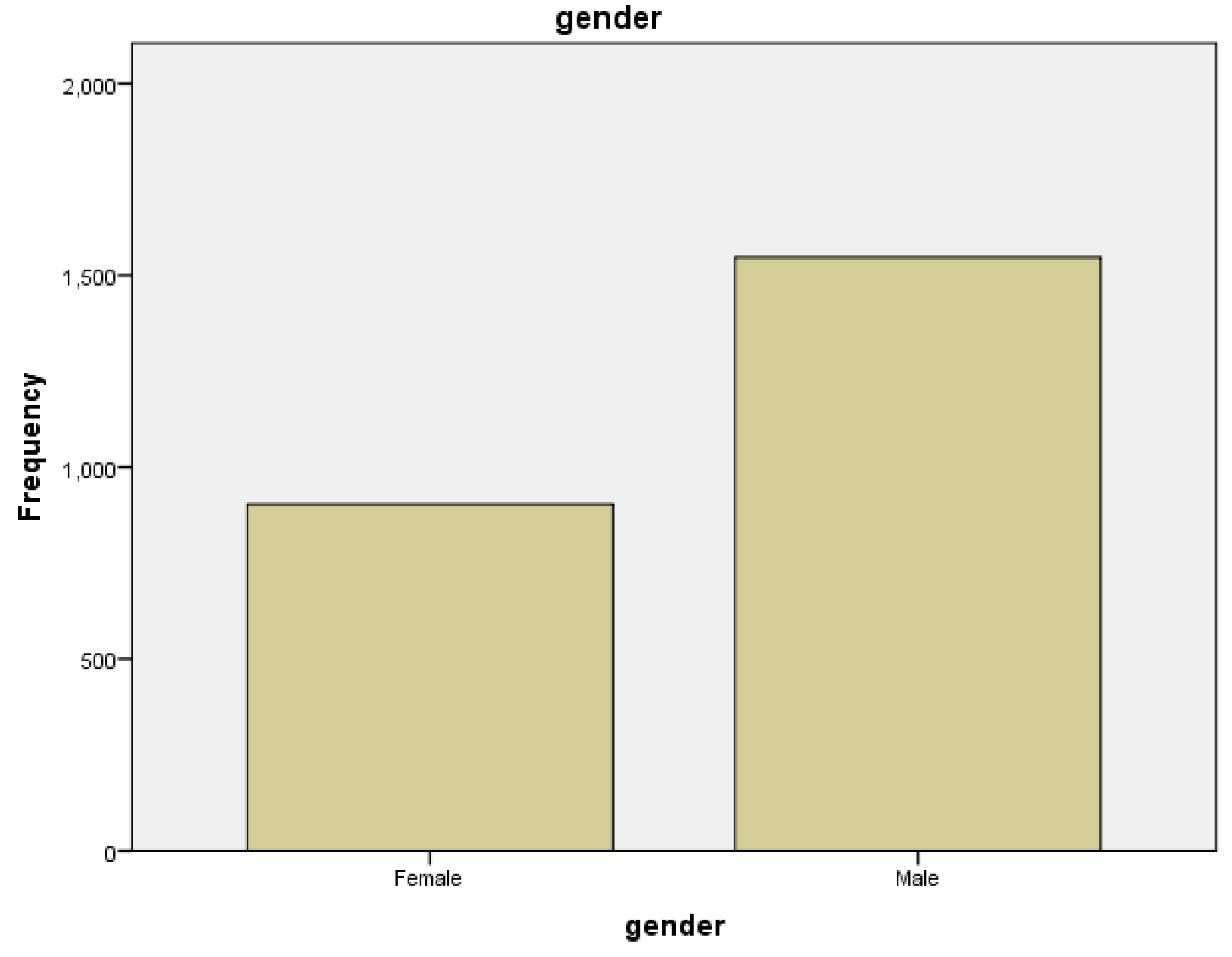

Table 3.
Gender of all the presented cases in 2020.
| Gender | Frequency | Percent | Valid Percent |
|---|---|---|---|
| Female | 903 | 36.9 | 36.9 |
| Male | 1547 | 63.1 | 63.1 |
| Total | 2450 | 100.0 | 100.0 |
Figure 2.
Gender of all the presented cases in 2020.
Among all, 3.1% cases had old Tb and 13.7% cases had newly diagnosed. Reactivation of disease was found in 7.0% of cases. (Table 4)
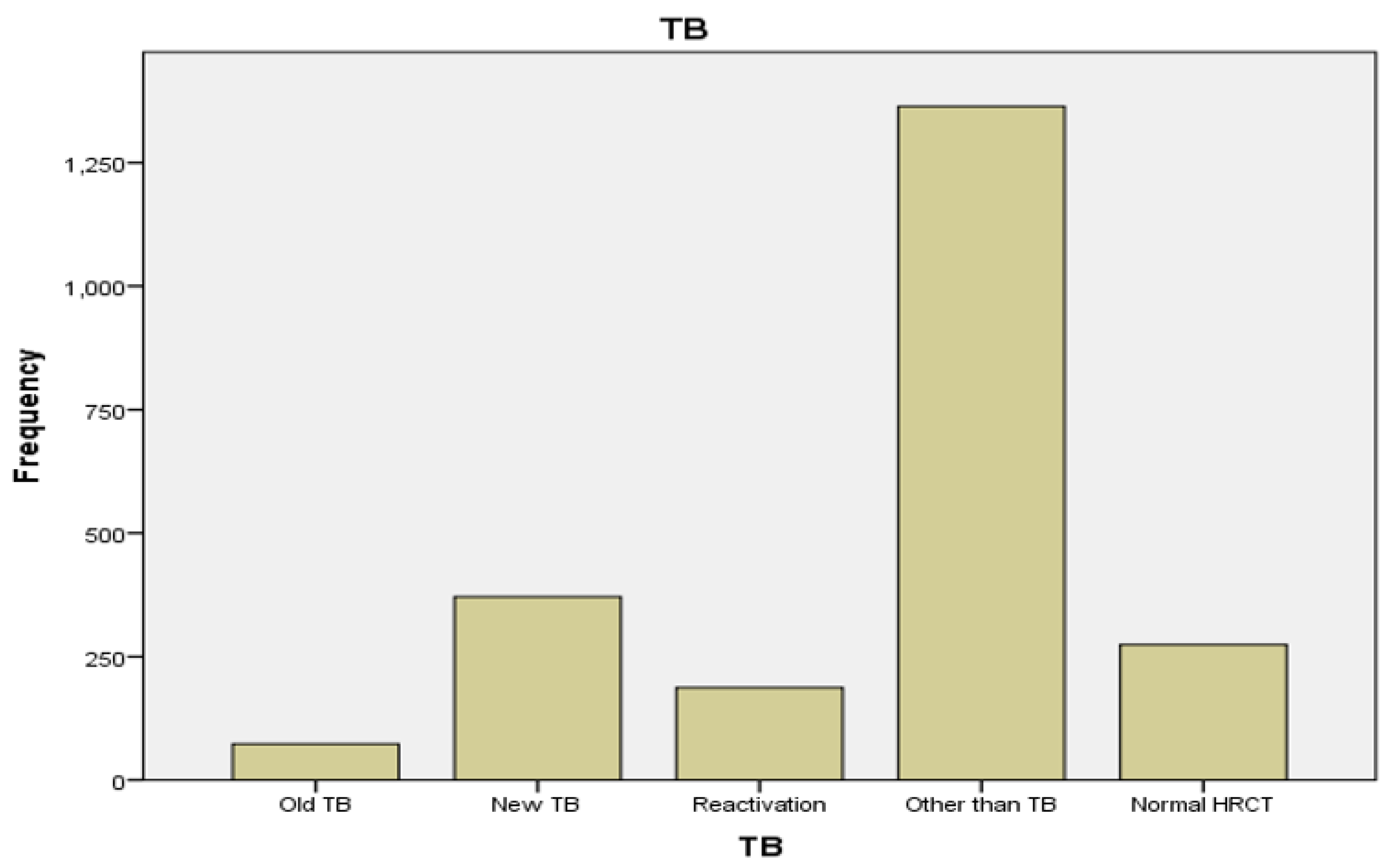
Figure 3.
Frequency of TB among all cases in 2020.
Frequency of the other diseases, than TB in 2020 was Covid-19, followed by cardiac disease, ILD and pneumonia. (Table 5)
In 9584 cases of year 2021, 42.1% were females and 57.9% were males. (Table 6)

Figure 4.
Gender of all the presented cases in 2021.
Among all, 2.1% cases had old Tb and 18.8% cases had newly diagnosed. Reactivation of disease was found in 3.9% of cases. (Table 7)
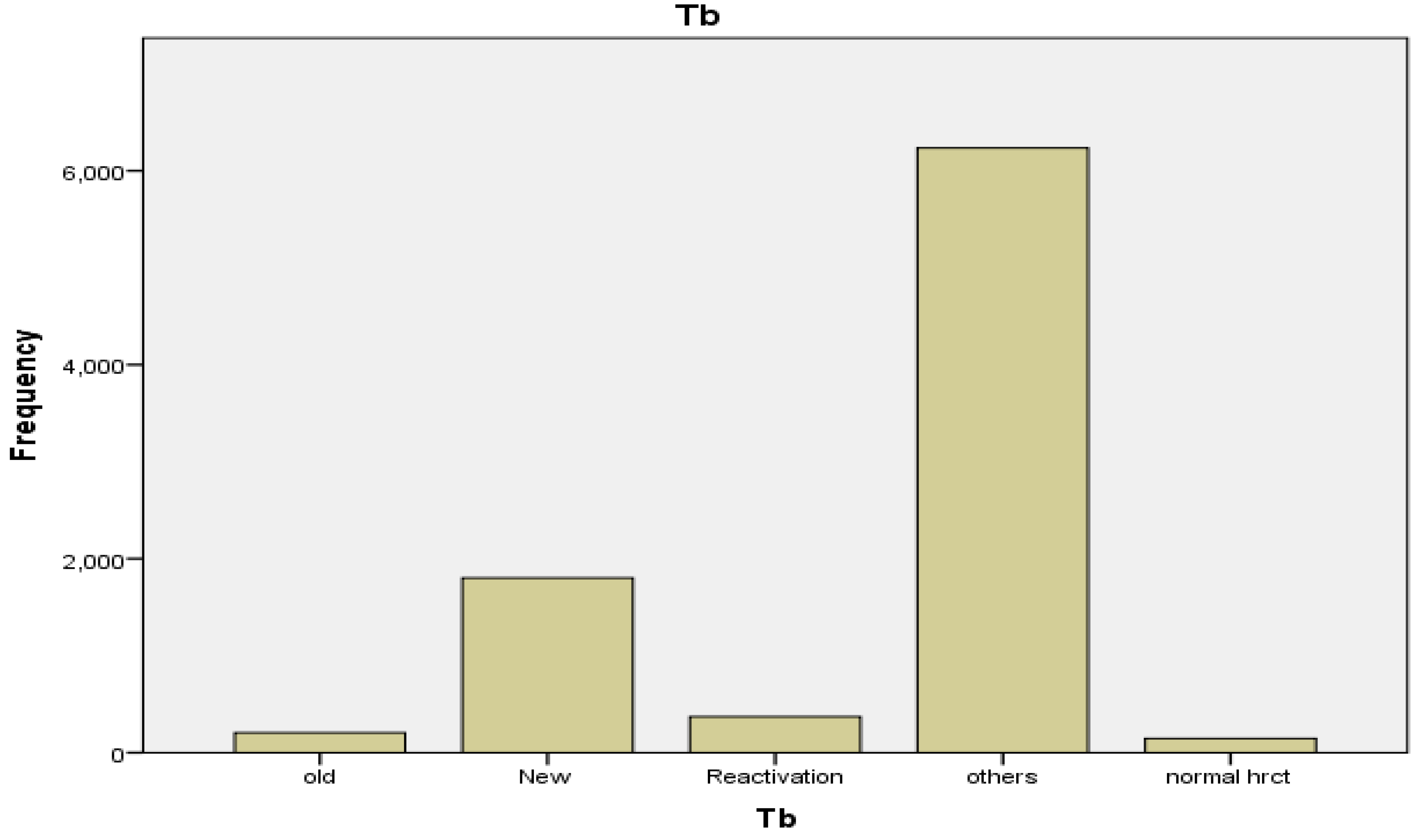
Figure 5.
Frequency of TB among all cases in 2021.
Frequency of diseases other than TB in 2021 was Covid-19, followed by cardiac disease, ILD and pneumonia in in cases of 2021. (Table 8)
In 3913 cases of 2022, 43.8% were females and 56.2% were males. (Table 9)
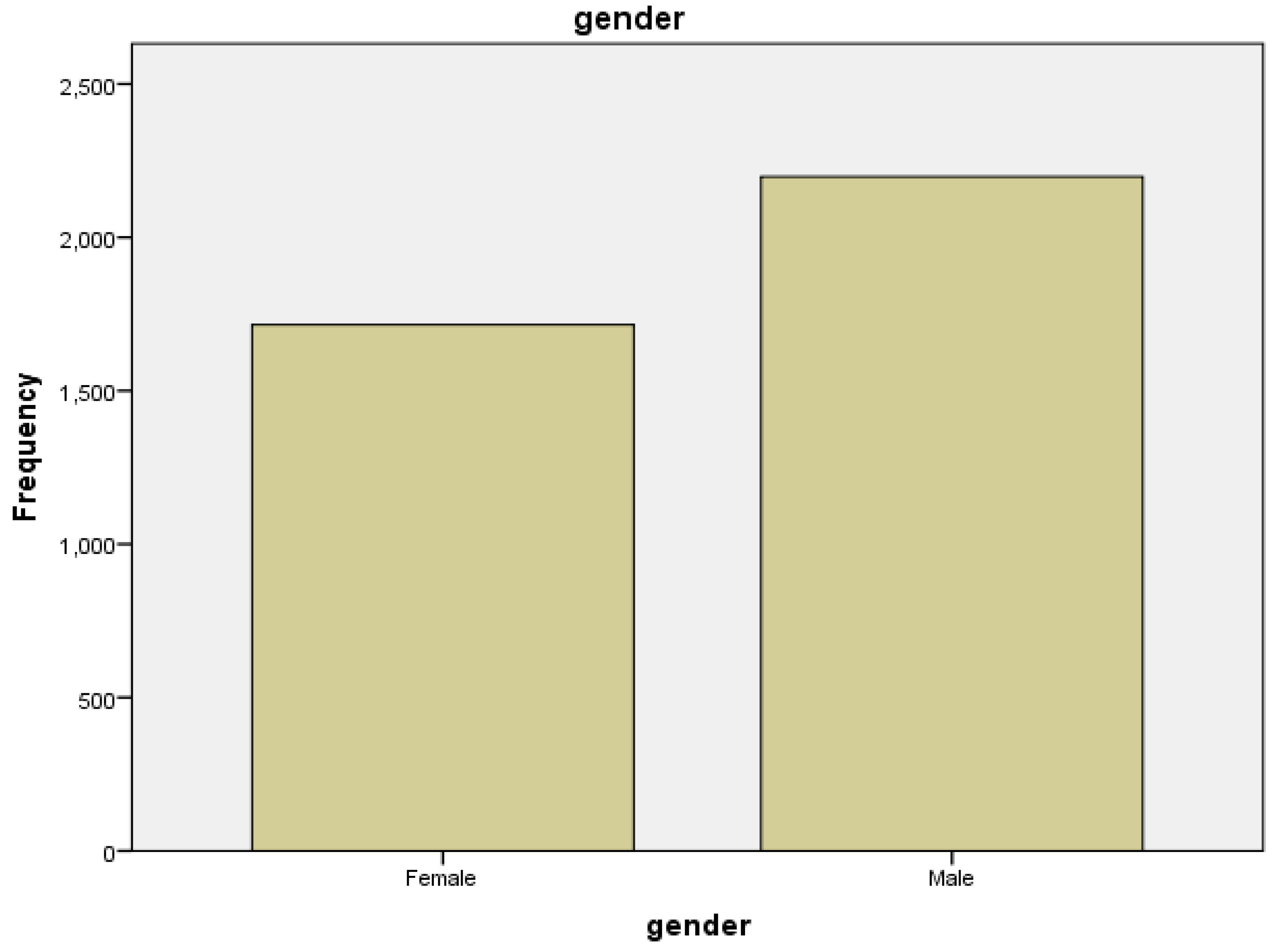
Figure 6.
Gender of presented cases in 2022.
Among all 5.4% cases had old Tb and 15.5% cases had newly diagnosed. Reactivation of disease was found in 7.2% cases. (Table 10)
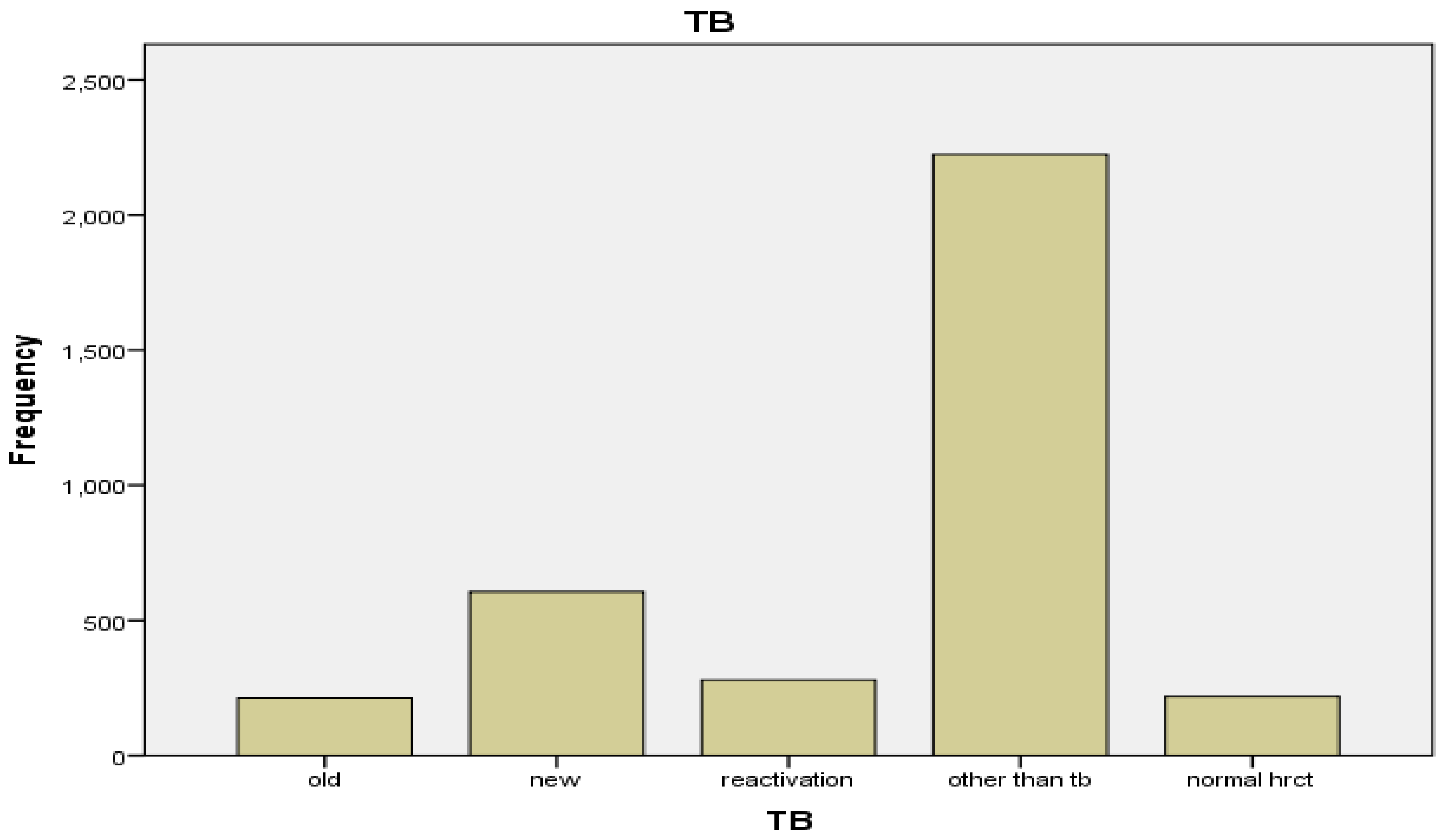
Figure 7.
Frequency of TB among all cases in 2022.
Frequency of Others disease, then TB in 2022 was Covid-19, followed by cardiac disease, ILD and pneumonia in in cases of 2022. (Table 11)
In 2023, 56.6% were males and 43.4% were females among 1174 cases. (Table 12)
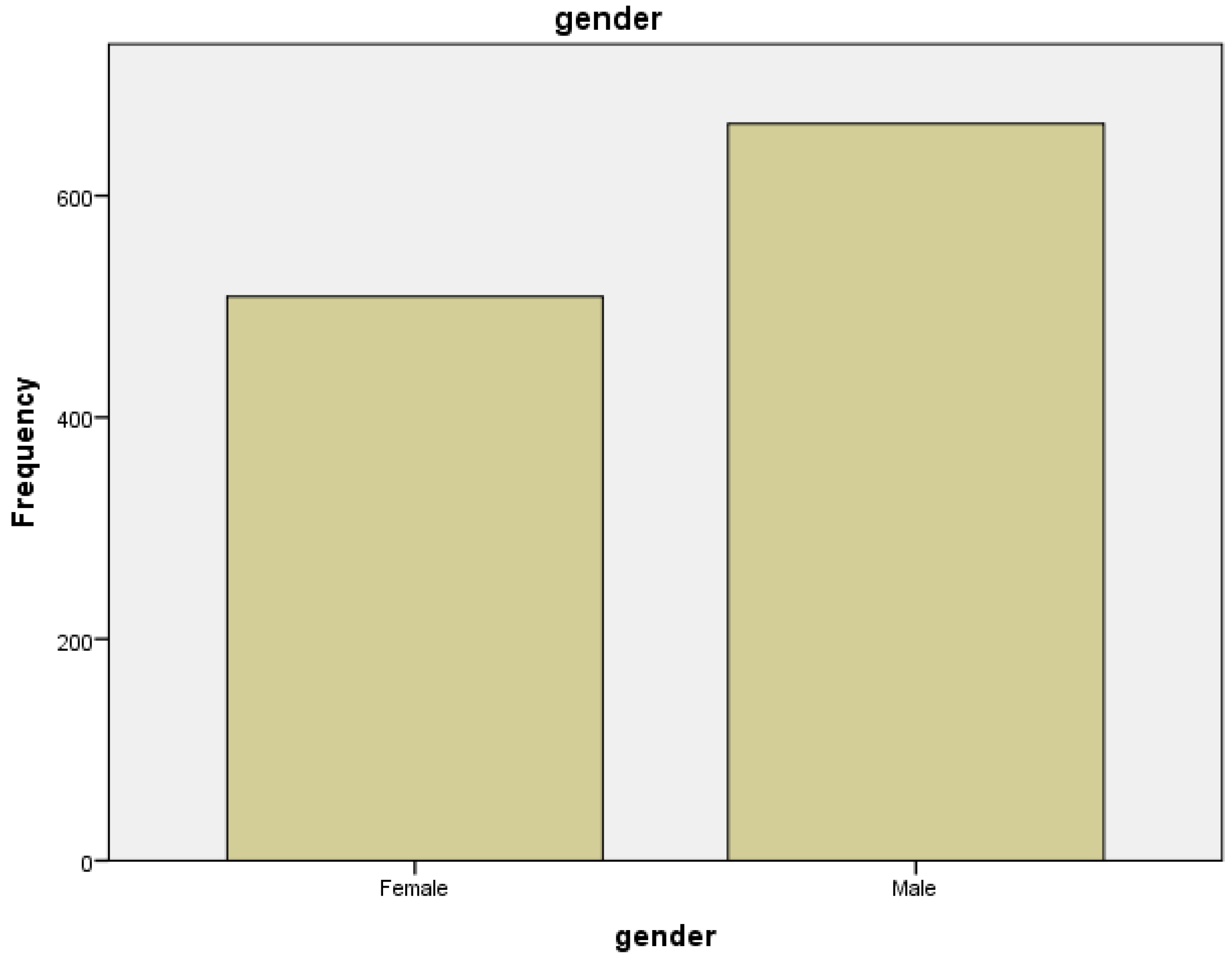
Figure 8.
: Gender of presented cases in 2023.
Among all 5.9% cases had old Tb and 15.9% cases had newly diagnosed. Reactivation of disease was found in 6.3% cases. (Table 13)
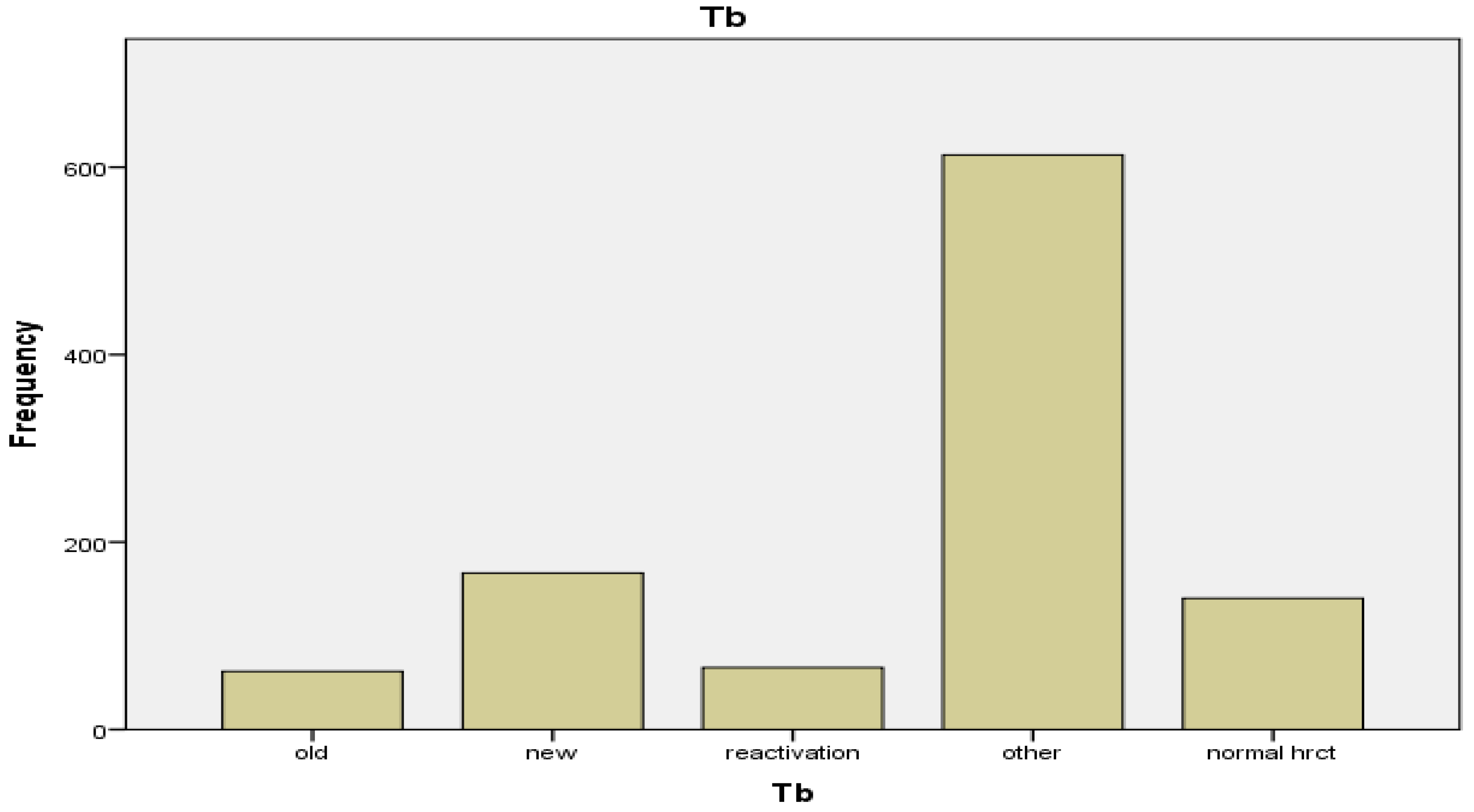
Figure 9.
Frequency of TB among all cases in 2023.
Frequency of other disease than TB in 2023 was Covid-19, followed by cardiac disease, ILD, pneumonia and cancer in in cases of 2023. (Table 14)
4. Discussion
Pakistan has been grabbing with a high load of TB for several decades, with the emergence of multidrug-resistant TB further complicating efforts to control the disease.
Human remains have been uncovered with TB traces dating back to thousands of years. In recent years, a joint international effort to eradicate mycobacterium tuberculosis has been initiated to decrease the survival potential of the human pathogen with no existing reservoir for the ecosystem. This has been mostly successful since 2000, when the World Health Organization (WHO 2017) approximate that global incidence of tuberculosis has declined by 1.5% every year. Furthermore, death from tuberculosis has been significantly and gradually reduced. The WHO has reported that the global TB mortality rate has dropped by 22% from 2000 to 2015 [31].
This study incorporated a total of 17,121 patients, comprising 9,961 (58.1%) males and 7,160 (41.8%) females. The mean age of the enrolled cases was 49.11±7.67 years, demonstrating consistency with the findings of a prior study [33]. This study also examined the prevalence of Tuberculosis in different years: 23.7% (582/2,450) in 2020, 24.8% (2,377/9,584) in 2021, 28.1% (1,099/3,913) in 2022, and 25.1% (295/1,174) in 2023. The average prevalence of TB cases from 2020 to 2023 was determined to be 25.42% (4,353/17,121). Out of the total cases, 15.9% presented with previous instances of tuberculosis, while 61.6% were newly diagnosed cases. Disease reactivation was observed in 23.7 % of the cases. Frequency of other diseases than TB was also observed which included Covid-19 followed by cardiac disease, ILD and pneumonia.
5. Conclusions
As per the National Tuberculosis Program (NTP) in Pakistan, the prevalence rate of tuberculosis stands at 340 cases per 100,000 population, equivalent to 0.34%. However, our study reveals an exceptionally high frequency of TB cases. Specifically, the prevalence of Tuberculosis in 2020 was 23.7% (582 out of 2,450), in 2021 it was 24.8% (2,377 out of 9,584), in 2022 it surged to 28.1% (1,099 out of 3,913), and in 2023 it was 25.1% (295 out of 1,174). The average prevalence of TB cases over the period from 2020 to 2023 was calculated at 25.42% (4,353 out of 17,121). Consequently, our findings suggest the presence of a substantial tuberculosis burden in Pakistan, which has reached epidemic proportion, which has reached epidemic proportion substantiating our claim of a TB Tsunami in Pakistan.
Funding
No funding sources.
Ethical Approval
The study was approved by the Ethical Review Board, SZABMU.
Conflict of Interest
The authors declare no conflict of interest.
References
- Alexandra Jaye Zimmer, Joel Shyam Klinton, Charity Oga-Omenka, Petra Heitkamp, Carol Nawina Nyirenda, Jennifer Furin, Madhikar Pai. Tuberculosis in times of COVID-19. The BMJ. 2021 September; 76: 310-16. [CrossRef]
- Zhenhong Wei, Xiaoping Zhang, Chaojun Wei, Liang Yao, Yonghong Li, Xiaojing Zhang, Hui Yanjuan Jia, Rui Guo, Yu Wu, Kehu Yang and Xiaoling Gao. Diagnostic accuracy of in-house real-time PCR assay for Mycobacterium tuberculosis: a systematic review and meta-analysis. BMC Infect Dis. BMC Infectious Disease. 2019; 19(1): 701. [CrossRef]
- Muhammad Amin, Musserat Javed, Afshan Noreen, Maria Mehboob, Nazahat Pasha, Umaima Majeed. Accuracy of High Resolution Computed Tomography Chest in Diagnosing Pulmonary Tuberculosis by taking AFB culture findings as Gold Standard. Pakistan Journal of Medical and Health Sciences. 2021; 15(Jun): 1429-30. [CrossRef]
- Philippe Glaziou MD Katherine Floyd PhD Mario C. Raviglione MD. Global Epidemiology of Tuberculosis. Seminars in Respiratory and Critical Care Medicine. 2018; 39: 271-85. [CrossRef]
- Sharanya Ponni S, Prabakaran M. Comparative High Resolution Computed Tomography and X-Ray Findings of Non-tuberculosis Lung Diseases and Pulmonary Tuberculosis in Patients with Acid-Fast Bacilli Smear-Positive Sputum. Journal Research in Medical and Dental Sciences JRMDS. 2021 Apr; 9(4): 343-47.
- Mian Waheed Ahmad, Nawaz Rashid, Sadaf Arooj, Sidra Shahzadi. Diagnostic Accuracy of High- Resolution Computed Tomography in Assessing Activity of Pulmonary Tuberculosis. Journal of Sheikh Zayed Medical College. 2020; 11(04): 07-10. [CrossRef]
- Arkapal Bandyopadhyay, Sarika Palepu, Krishna Bandyopadhyay, Shailendra Handu. COVID-19 and tuberculosis co-infection: a neglected paradigm. Monaldi Archives for Chest Disease. 2020 July; 90:1437: 518-22. [CrossRef]
- Surya Kant and Richa Tyag. The impact of COVID-19 on tuberculosis. Therapeutic Advances in Infectious Disease. 2021; 8: 1-7. [CrossRef]
- Diwan VK, Thorson A. Sex, gender, and tuberculosis. Lancet 1999;353:1000-1. [CrossRef]
- Davies PD. Tuberculosis: the global epidemic. J Ind Med Assoc 2000;98:100-02.
- Cantwell MF, Mckenna MT, McCray E, Onorato IM. Tuberculosis and race/ethnicity in United States: impact of socioeconomic status. Am J Respir Crit Care Med 1998;157:1016-20. [CrossRef]
- Spence DP, Hotchkiss J, Williams CSD, Davies PD. Tuberculosis and poverty. BMJ 1993;307:759-61. [CrossRef]
- Devey J. Report on a knowledge, attitude, and practices (KAP) survey regarding tuberculosis conducted in northern Bihar: report on an independent study conducted during a HNGR internship with: Champak and Chetna Community Health and Development Projects, Duncan Hospital Bihar, India, May to November 2000. 23 p. (http://www.ehahealth.org/component/docman/doc_view/11-tbstudy?tmpl=component&format=raw, accessed on 3 March 2010).
- National TB Control Program, Pakistan. Resource Center (2021). https://ntp.gov.pk/resource-center/ (Accessed 11 October 2021).
- Waheed, M.A. Khan, R. Fatima, et al., Infection control in hospitals managing drug-resistant tuberculosis in Pakistan: how are we doing? Public Health Action 7 (1) (2017) 26. [CrossRef]
- National TB Control Program - National Institute of Health Islamabad. Accessed March 11, 2022. https://www.nih.org.pk/national-tb-control-program/.
- S. Abbas, M. Kermode, S. Kane, Strengthening the response to drug-resistant TB in Pakistan: a practice theory-informed approach, Public Health Action 10 (4) (2020) 147. [CrossRef]
- Mandatory TB Case Notification (MCN) - National TB Control Programme - Pakistan : National TB Control Programme - Pakistan. Accessed March 11, 2022. https://ntp.gov.pk/mandatory-tb-case-notification-mcn/.
- W. Ullah, A. Wali, M.U. Haq, A. Yaqoob, R. Fatima, G.M. Khan, Public–private Mix models of tuberculosis care in Pakistan: a high-burden country perspective, Front. Public Health 9 (2021) 1116. [CrossRef]
- J.D. Walley, M.A. Khan, J.N. Newell, M.H. Khan, Effectiveness of the direct observation component of DOTS for tuberculosis: a randomized controlled trial in Pakistan, Lancet 357 (9257) (2001) 664–669. [CrossRef]
- President for collective efforts to eliminate TB. Accessed March 21, 2022. https ://www.thenews.com.pk/print/926344-president-for-collective-efforts-to-elimi nate-tb.
- A.A. Malik, H. Hussain, R. Maniar, et al., Integrated tuberculosis and COVID-19 activities in Karachi and tuberculosis case notifications, Trav. Med. Infect. Dis. 7 (1) (2022). [CrossRef]
- Kabra SK, Lodha R, Seth V. Some current concepts on childhood tuberculosis. Ind J Med Res 2004;120:387-97.
- Bannon MJ. BCG and tuberculosis. Arch Dis Child 1999;80:80-3. [CrossRef]
- Abel B, Tameris M, Mansoor N, Gelderbloem S, Hughes J, Abrahams D et al. The novel TB vaccine, AERAS-402, induces robust and polyfunctional CD4 and CD8 T cells in adults. Am J Respir Crit Care Med 2010 (in press). [CrossRef]
- Luby SP, Brooks WA, Zaman K, Hossain S, Ahmed T. Infectious diseases and vaccine sciences: strategic directions. J Health Popul Nutr 2008;26:295-310. [CrossRef]
- Nair N, Wares F, Sahu S. Tuberculosis in the WHO south-east Asia region. Bull World Health Organ 2010;88:164. [CrossRef]
- Onyebujoh P, Rodriguez W, Mwaba P. Priorities in tuberculosis research. Lancet 2006;367:940-2. [CrossRef]
- Tuberculosis profile: Pakistan. TB profile (shinyapps.io).
- Radiopedia. https://radiopaedia.org/articles/tuberculosis-pulmonary-manifestations-1.
- Dong E, Du H and Gardner L (2020) An interactive web-based dashboard to track COVID-19 in real time. Lancet Infectious Diseases 20, 533–534. [CrossRef]
- Finn McQuaid C et al. (2020) The potential impact of COVID-19-related disruption on tuberculosis burden. European Respiratory Journal 56. [CrossRef]
- Kim, JH., Kim, E.S., Jun, KI. et al. Delayed diagnosis of extrapulmonary tuberculosis presenting as fever of unknown origin in an intermediate-burden country. BMC Infect Dis 18, 426 (2018). [CrossRef]
- Kassa E, Enawgaw B, Gelaw A, Gelaw B. Effect of anti-tuberculosis drugs on hematological profiles of tuberculosis patients attending at University of Gondar Hospital, Northwest Ethiopia. BMC Hematol. 2016;16:1. [CrossRef]
- Gonzalez Saldana N, Macias Parra M, Hernandez Porras M, Gutierrez Castrellon P, Gomez Toscano V, Juarez Olguin H. Pulmonary tuberculous: symptoms, diagnosis and treatment. 19-year experience in a third level pediatric hospital. BMC Infect Dis. 2014;14:401. [CrossRef]
- Onur ST, Iliaz S, Iliaz R, Sokucu S, Ozdemir C. Serum alkaline phosphatase may play a role in the differential diagnosis of sarcoidosis and tuberculosis. Int J Clin Exp Med 2016;9(7):14266–70. [CrossRef]
- Mert A, Arslan F, Kuyucu T, Koc EN, Ylmaz M, Turan D, et al. Miliary tuberculosis: Epidemiologicaland clinical analysis of large-case series from moderate to low tuberculosis endemic country. Medicine (Baltimore). 2017;96(5):e5875. [CrossRef]
- Abubakar I, Story A, Lipman M, Bothamley G, Hest R, van Andrews N, et al. Diagnostic accuracy of digital chest radiography for pulmonary tuberculosis in a UK urban population. European Respiratory Journal. 2010;35(3):689–92. [CrossRef]
- Rozenshtein A, Hao F, Starc MT, Pearson GDN. Radiographic Appearance of Pulmonary Tuberculosis: Dogma Disproved. American Journal of Roentgenology. 2015;204(5):974–8. [CrossRef]
- Geng E, Kreiswirth B, Burzynski J, Schluger NW. Clinical and radiographic correlates of primary and reactivation tuberculosis: A molecular epidemiology study. JAMA. 2005;293(22):2740–5. [CrossRef]
- Toman K, Frieden T, Toman K World Health Organization. Toman’s tuberculosis: case detection, treatment, and monitoring: questions and answers. Geneva: World Health Organization; 2004.
- Sara Ijaz Gilani MK (2012) Perception of tuberculosis in Pakistan: findings of a nation-wide survey. Journal of Pakistan Medical Association. https://pubmed.ncbi.nlm.nih.gov/22755370/ (Accessed 11 October 2021).
- Saima Perwaiz Iqbal MR (2013) Challenges faced by general practitioners in Pakistan in management of tuberculosis: a qualitative study. Rawal Medical Journal 38, 249–252.
- World Health Organization (2021) Tuberculosis deaths rise for the first time in more than a decade due to the COVID-19 pandemic. https://www.who.int/news/item/14-10-2021-tuberculosis-deaths-rise-for-the-first-time-in-more-than-a-decade-due-to-the-covid-19-pandemic (Accessed 4 February 2022).
- The value of Chest X-ray as an Early Case Detection Option for Diagnostic of Pulmonary TB 1st Author Pak.J.of Neurology. Surg-Col.17, No. 1 Jan-June 2013.
Table 1.
Surveillance programs in the Pakistan.
| Surveillance Programs | Purposes |
|---|---|
| National Tuberculosis (Tb) Program (NTP) [15] | It runs according to WHO guidelines and aims to decrease the incidence of TB and the number of deaths by Tb to almost zero. |
| National TBIC (Tuberculosis infection control) plan [15] | To reduce the risk of TB among the health care workers by providing TBIC supplies such as masks, education, and training. |
| Programmatic Management of Drug Resistant Tuberculosis (PMDT) [17] | Formation of clinics through the country to guarantee free provision of cost consultation and drugs for treatment beside with some financial support for patients involving their transportation expenses. |
| Mandatory Case Notification (MCN) project [18] | Its goal is to increase the number of reported cases so that well-timed diagnosis and treatment can be succeeded along with contact tracing. |
| Provincial TB Program (PTP) [19] | Works hand in hand with NTP to eliminate TB from Pakistan and runs a systematic approach on the provincial level in controlling the risk of spread of TB. |
| Public-Private Mix model (PPM) [19] | Started by NTP so that the public and private sector work jointly for the goal of stopping the spread of TB along with better treatment strategies for TB. |
Table 2.
Classification of Tuberculosis based on HRCT Findings.
| Primary Tuberculosis | Reactivation Tuberculosis | Chronic Tuberculosis |
|---|---|---|
| -smaller nodules in upper lung zone, superior segment of lower lobe. -Consolidation -Mediastinal Lymph nodes |
-cavity formation -Focal/patchy heterogeneous consolidation involving the apical and posterior segment of the upper lobes and superior segments of lower lobe -Poorly defined nodules giving tree-in-bud appearances and linear opacities |
-Fibrosis -collapse of lung segment -pleural thickening -pulmonary nodules in hilar area/upper lobes with or without fibrosis and volume loss -Bronchiectasis -Pleural effusion. |
Table 4.
Frequency of TB among all cases in 2020.
| Variables | Frequency | Percent | Valid Percent |
|---|---|---|---|
| Old TB | 75 | 3.1 | 3.1 |
| New TB | 335 | 13.7 | 13.7 |
| Reactivation | 172 | 7.0 | 7.0 |
| Other than TB | 1427 | 58.2 | 58.2 |
| Normal HRCT | 266 | 10.9 | 10.9 |
| Missing system | 175 | 7.1 | 7.1 |
| Total | 2450 | 100.0 | 100.0 |
Table 5.
Frequency of diseases other than TB in 2020.
| Others | Frequency | Percent | Valid Percent |
|---|---|---|---|
| covid | 491 | 34.4 | 34.4 |
| cardiac | 152 | 10.6 | 10.6 |
| ILD | 168 | 11.8 | 11.8 |
| pneumonia | 289 | 20.3 | 20.3 |
| cancer | 35 | 2.4 | 2.4 |
| miscellaneous | 292 | 20.3 | 20.3 |
| Total | 1427 | 100.0 | 100.0 |
Table 6.
Gender of presented cases in 2021.
|
Gender |
Frequency | Percent | Valid Percent | Cumulative Percent | |
| Female | 4033 | 42.1 | 42.1 | 42.1 | |
| Male | 5551 | 57.9 | 57.9 | 100.0 | |
| Total | 9584 | 100.0 | 100.0 | ||
Table 7.
Frequency of TB among all cases in 2021.
| Variables | Frequency | Percent | Valid Percent |
| Old | 205 | 2.1 | 2.1 |
| New | 1801 | 18.8 | 18.8 |
| Reactivation | 371 | 3.9 | 3.9 |
| Others | 6234 | 65.1 | 65.1 |
| Normal HRCT | 146 | 1.5 | 1.5 |
| Missing system Total |
827 9584 |
8.6 100.0 |
8.6 100.0 |
Table 8.
Frequency of diseases other than TB in 2021.
| Other than Tuberculosis | Frequency | Percent | Valid Percent |
|---|---|---|---|
| covid | 1844 | 29.6 | 29.6 |
| cardiac | 575 | 9.2 | 9.2 |
| ILD | 682 | 10.9 | 10.9 |
| pneumonia | 1768 | 28.4 | 28.4 |
| cancer | 434 | 7.0 | 7.0 |
| miscellaneous | 931 | 14.9 | 14.9 |
| Total | 6234 | 100.0 | 100.0 |
Table 9.
Gender of presented cases in 2022.
| Gender | Frequency | Percent | Valid Percent |
|---|---|---|---|
| Female | 1715 | 43.8 | 43.8 |
| Male | 2198 | 56.2 | 56.2 |
| Total | 3913 | 100.0 | 100.0 |
Table 10.
Frequency of TB among all cases in 2022.
| Variables | Frequency | Percent | Valid Percent |
|---|---|---|---|
| Old | 213 | 5.4 | 5.4 |
| New | 606 | 15.5 | 15.5 |
| Reactivation | 280 | 7.2 | 7.2 |
| Other than tb | 2224 | 56.8 | 56.8 |
| Normal HRCT | 221 | 5.6 | 5.6 |
| Missing system Total |
369 3913 |
9.5 100.0 |
9.5 100.0 |
Table 11.
Frequency of other diseases in 2022.
| Other than Tuberculosis | Frequency | Percent | Valid Percent |
|---|---|---|---|
| Covid | 410 | 18.4 | 18.4 |
| Cardiac | 244 | 11.0 | 11.0 |
| ILD | 403 | 18.1 | 18.1 |
| Pneumonia | 525 | 23.6 | 23.6 |
| Cancer | 212 | 9.5 | 9.5 |
| Miscellaneous | 430 | 19.3 | 19.3 |
| Total | 2224 | 100.0 | 100.0 |
Table 12.
Gender of presented cases in 2023.
| Variables | Frequency | Percent | Valid Percent |
|---|---|---|---|
| Female | 509 | 43.4 | 43.4 |
| Male | 665 | 56.6 | 56.6 |
| Total | 1174 | 100.0 | 100.0 |
Table 13.
Frequency of TB among all cases in 2023.
| Variables | Frequency | Percent | Valid Percent |
|---|---|---|---|
| Old | 62 | 5.3 | 5.3 |
| New | 167 | 14.2 | 14.2 |
| Reactivation | 66 | 5.6 | 5.6 |
| Other | 613 | 52.2 | 52.2 |
| Normal HRCT | 140 | 11.9 | 11.9 |
| Missing System | 126 | 10.8 | 10.8 |
|
Total |
1174 |
100.0 |
100.0 |
Table 14.
Frequency of other disease than TB in 2023.
| Other than Tuberculosis | Frequency | Percent | Valid Percent |
|---|---|---|---|
| Covid | 69 | 11.3 | 11.3 |
| Cardiac | 122 | 19.9 | 19.9 |
| ILD | 111 | 18.1 | 18.1 |
| Pneumonia | 139 | 22.7 | 22.7 |
| Cancer | 52 | 8.5 | 8.5 |
| Miscellaneous | 120 | 19.6 | 19.6 |
| Total | 613 | 100.0 | 100.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



