Submitted:
04 June 2024
Posted:
07 June 2024
You are already at the latest version
Abstract
Colorectal cancer (CRC) is a weighty cause of mortality worldwide, with growing incidence in the Middle East. Understanding the level of awareness about CRC screening among the Syrian pop-ulation is crucial public health interventions. A cross-sectional study was conducted from Sep-tember 22, 2023, to October 15, 2023, involving 928 participants from six major governorates in Syria. An online questionnaire containing socio-demographic, knowledge, and attitude sections was used to collect data. Descriptive statistics and chi-square tests were employed for data analysis using (SPSS) v28.0. The survey revealed a lack of awareness regarding CRC screening among the Syrian population, with only 499(53%) of the proportion demonstrating adequate knowledge about the disease and its screening methods. Significant associations were observed between the level of knowledge and socio-demographic factors including gender, work status, and economic status (p < 0.05). The findings emphasize the need for public health initiatives to enhance awareness and knowledge about CRC and its early screening methods in Syria. Education is essential for improving early detection and reducing the burden of colorectal cancer in the region. Efforts to increase public understanding of CRC screening are critical for reducing the incidence and mortality.
Keywords:
colorectal cancer
; colonscopy
; coloncancer
; awareness
; knowledge
; practice
; attitude
; rectal cancer
; helth education
; cancer prevention
1. Introduction
Colorectal cancer (CRC) is defined as a proliferation of abnormal cells in the colon and rectum that can spread and metastasize to other organs [1]. CRC is the second cancer-related cause of death worldwide [2]. The incidence of colorectal cancer (CRC) reached the highest prevalence in Western nations. however, there has been a reported increase in the Middle East particularly in the nations along the Eastern Mediterranean coast [2]. Many factors can contribute to The risk of developing CRC such as age, lifestyle, genetic abnormalities, chronic ulcerating colitis, and Crohn’s disease. Moreover, elevated body mass index (BMI), smoking, consuming of red meat, lack of physical exercise, diminished consumption of vegetables, and low consumption of fruit could also be potential contributing factors [1,3,4].In Syria, according to a retrospective study, males, aged over 50 years old, and occupation without physical activity are the risk factors related to CRC there with an annual rate incidence of 8.2% [6].However, early colorectal cancer has a better prognosis compared to advanced and metastatic colorectal cancer [8].A person’s awareness of CRC screening determines whether or not they choose to participate in it. Awareness affected opinions about CRC screening methods, cancer evaluations, and screening motivation. Public education targets factors that mediate awareness [9].CRC screening is different between countries but most of them recommend colonoscopy, fecal immunochemical test (FIT), computed tomography (CT) colonography, FIT-fecal DNA, and flexible sigmoidoscopy [10,11,12].The objective of CRC screening is to discover cancerous and precancerous lesions in obviously healthful people, to decrease both the occurrence and death rate of CRC [13].
In this cross-sectional study, we aim to examine the level of awareness towards colorectal cancer screening among the Syrian population from six different Syrian governments.
2. Materials and Methods
Data Collection and Ethical Considerations
An ethical approval from The Scientific Research Ethics Committee of Damascus University was obtained ( approval ID number: MD-160124-168)
During the period from September 22, 2023, to October 15, 2023, we conducted a cross-sectional study to investigate the level of awareness regarding early screening for colorectal cancer in Syria. To collect the necessary information, we obtained responses to an online questionnaire from participants residing in six major governorates of Syria: Damascus, Homs, Aleppo, Lattakia, Hama, and Tartous. It was communicated to all participants that their responses would be used exclusively for scientific research purposes and Informed consent was obtained from all participants who enrolled in the study. The questionnaire was distributed via social media and all the participants in-rolling the study by self-selection method.
Inclusion and Exclusion Criteria
Eligibility criteria for our study included Syrian participants aged 30 and above, however, individuals under 30 and those who declined participation were excluded.
Sample Size
The sample size for this study was determined via a well-established statistical method by AI tools [14,15]. Specifically, we estimated the sample size (N) using the formula:
N = Z2x P x (1-P) e2
Where Z represents the z-score and is set equal to 1.96 at a 95% level of significance, P represents the population proportion and was set equal to 0.5 in this study, and e is the margin of error which was set equal to 0.05 or 5%. The calculated sample size was N=384. Nevertheless, we received responses from 928 individuals who completed the questionnaire, including the socio-demographic section as well as the sections on knowledge and information about colorectal cancer.
Survey Design
the questionnaire consisted of 24 questions, divided into three parts. The first section was socio-demographic, requesting limited options to determine the characteristics of the participants. The second section focused on knowledge and practice related to colorectal cancer and its screening and required polar responses (yes/no). Finally, the third section aimed to assess participants’ attitudes toward early screening of colorectal cancer using a Likert scale (strongly agree, agree, neutral, disagree, and strongly disagree). Additionally, a question regarding the source of their information was provided with limited options, The survey was designed in Arabic after considering the Syrian society’s cultural habits and performing a literature review. we used The questionnaire a previously published study [5]. The Cronbach’s alpha coefficient for the knowledge items in the modified instrument was 0.88.
Sampling Methods
Eligibility criteria for our study included Syrian participants aged 30 and above, while individuals under 30 and those who declined participation were excluded.
Data Analysis
we employed the Statistical Package for Social Sciences (SPSS) v28.0. Descriptive statistics were calculated. To assess the level of knowledge among participants, the median frequency of yes answers was calculated and responses were separated into two groups according to whether they were above the median (sufficient level of knowledge or information) or less than the median( insufficient level of knowledge or information). chi-square tests were utilized to determine the association between the level of knowledge and socio-demographic factors. P-values less than 0.05 were considered statistically significant(P<0.05).
3. Results
A total of 928 participants starting from the age of 30 were included in this study. The predominant age group was 30-35 (54.6%). Most participants were females (61.2%), had bachelor’s degrees (50.4%), and workers (58.9%). Married represent most of the included respondents (61.4%). (42.7%) of the participants had a median economic status. More details can be seen in Table 1.
Among the participants, 488(52.6%) mentioned that they had heard of early cancer screening tests. Only 237(25.5%) know that colon cancer can be prevented but more than half of the participants 538(58%) reported that they think colon cancer is fatal. Most of the participants 791(85.2) know that Colon cancer recovery rates are increased when detected in the early stages. Furthermore, regarding methods of early detection of colon cancer, the majority of participants 754 (81.2%) reported Colonoscopy, followed by 491 (53%) who reported blood detection in the stool sample. For risk factors for colon cancer, 658 (70.9%) answered with “yes” to the statement (Men and women are susceptible to colon cancer), moreover, more than half of the participants 516 (55.6%) agreed that High Fat Low Fiber Diet is a risk factor for colon cancer, while only 174 (18.7%) knows that Physical inactivity is a risk factor.
For colon cancer symptoms, firstly was the presence of blood in the stool 668 (71.9%), followed by Sudden weight loss 552 (59.4%), then Sudden change in number of bowel motions and Diarrhea 522 (56.2%), the least chosen symptom was feeling that the rectum was not fully emptied with defecation 295 (31.7%). Only 8% of participants have done early checkups for colon cancer. this is illustrated inTable 2. In our study, Figure 1 illustrates that 53% of respondents demonstrated a sufficient knowledge level based on our criteria. However, 47% fell short and exhibited insufficient knowledge.
According to Table 3, only 44 (4.7%) of participants strongly agreed with the statement “I think I’m susceptible to colon cancer”, while around half of the participants 429 (46.2%) strongly agreed with undergoing early screening for colon if advised by a doctor, and only 15 (1.6%) disagreed.
| Attitude | Strongly agree n(%) | Agree n(%) | Neutral$$$n(%) | Disagree$$$n(%) | Strongly disagree n(%) |
| I think I’m susceptible to colon cancer | 44(4.7) | 224(24.2) | 417(44,9) | 216(23.3) | 27(2.9) |
| I will undergo early screening for colon cancer if my doctor advises me to do so | 429(46.2) | 387(41.7) | 91(9.8) | 15(1.6) | 6(0.6) |
| I think I have adequate information | 37(4) | 200(21.6) | 312(33.6) | 333(35.9) | 46(5) |
| Variable | ||
| Knowledge | Frequency of yes | Percentage * |
| Have you ever heard of early cancer screening tests? | 488 | 52.6% |
| Colon cancer can be prevented | 237 | 25.5% |
| I think colon cancer is fatal | 538 | 58% |
| Colon cancer recovery rates are increased when detected in early stages | 791 | 85.2% |
| Methods of early detection of colon cancer | Frequency of yes | Percentage |
| Colonoscopy | 754 | 81.2% |
| PR speculum | 473 | 51% |
| Blood detection in the stool sample | 491 | 53% |
| Barium dye for large intestine | 340 | 37% |
| Blood tests | 333 | 36% |
| Abdominal CT scan | 227 | 24% |
| Clinical examination of the rectum | 341 | 37% |
| Other | 44 | 5% |
| Risk factors for colon cancer | Frequency of yes | Percentage |
| Men and women are susceptible to colon cancer | 658 | 70.9% |
| Physical inactivity | 174 | 18.7% |
| Overweight | 338 | 36.4% |
| High Fat Low Fiber Diet | 516 | 55.6% |
| The presence of polyps in the lining of the colon and rectum | 473 | 50.9% |
| Increasing age | 405 | 43.6% |
| Smoking | 316 | 34% |
| Symptoms of colon cancer | Frequency of yes | Percentage |
| The presence of blood in the stool | 668 | 71.9% |
| Sudden weight loss | 552 | 59.4% |
| Increase mucus secretions in the stool | 443 | 47.7% |
| Feeling that the rectum was not fully emptied with defecation | 295 | 31.7% |
| Pain and cramps in the stomach | 502 | 54% |
| Sudden change in the number of bowel motions and Diarrhea | 522 | 56.2% |
| Practice | Frequency of yes | Percentage |
| Have you done early checkups for colon cancer? | 74 | 8% |
| Have you ever thought about undergoing a screening for early detection of colon cancer? | 306 | 33% |
*Percentage is based on the overall sample.
Knowledge and socio-demographic cross tabs are displayed in Table 4. There was a significant relation between Gender and Knowledge ( p = 0.001, p < 0.05), work and knowledge ( p = 0.001, p < 0.05), economic-status and knowledge ( p = 0.001, p < 0.05).
4. Discussion
In this study, we assess the awareness of the early screening of CRC in Syria, a developing country in the Middle East. Only 25.6% of the study participants think they have adequate information about CRC early screening. This low number corresponds with the findings of other studies conducted in the region [16,17,18] 52.6% answered that they had heard of early CRC screening tests. When asked to specify the screening methods, Colonoscopy was the most common choice 81.2%. Blood detection in the stool sample was chosen by a smaller percentage of people 53%, while other methods were less known. This pattern was noticed in a Saudi study [16]. Some people are hesitant to undergo screening by colonoscopy because of expected pain, discomfort, or embarrassment from the procedure. In these cases, other methods of screening such as Fecal occult blood testing (FOBT) might be more acceptable [17]. Therefore, the screening rate is expected to improve by increasing people’s knowledge of its various methods.
When asked to specify the sources of their information on CRC early screening, 56% of the respondents chose their physician, and 40% didn’t specify any source. TV/Radio and social media websites were mentioned by small percentages of responders which indicates their underutilization to inform the public about CRC screening tests. In contrast, the Saudi study found that the top choices were awareness campaigns, booklets, TV/Radio, and newspapers which might indicate a more coordinated effort to educate the public. Syria had public awareness campaigns and advertisements about breast cancer screening and the effects of Tobacco on health. However, knowledge of Colorectal cancer detection and prevention is not promoted on a similar magnitude.
The age group of the participants didn’t correlate with better awareness of screening. This is concerning because the risk of developing CRC increases with age, and screening is recommended at the age of 45 years old by the American Cancer Society [19]. In our study, 19.7% of the study participants are older than 45 which is the age when screening is recommended and 8% of responders have done early checkups for colon cancer and 33% thought about it. This means that less than half of the people eligible for screening tests in our sample took them. This low result is similar to the one found in a Saudi study [16]. However, 87.9% of our participants said they were willing to undergo early screening if their doctor advised them to do so.
There was a statistically significant correlation between gender and awareness with females being less aware. This finding is similar to studies in Saudi Arabia [16] but studies in Lebanon [17], Jordan [18], and Britain [20] found no correlation. The level of education had no significant impact on awareness in our study and others in Lebanon [17]and Saudi Arabia [16], in contrast to other studies in Jordan [18] and Portugal [21]. Teaching the benefits of cancer screening in schools could have a beneficial impact in this regard.
When assessing the awareness of CRC risk factors, only 34% chose tobacco, in other studies in the region, the majority were aware of the connection between tobacco and CRC [16,17,22]. a minority of responders considered physical inactivity and obesity as risk factors in our study and other studies. It is estimated that about half of colorectal cancer cases could be attributed to diet and lifestyle [7]. Awareness campaigns should put more emphasis on prevention since it is the most cost-effective method
One limitation is the relatively young age of the participants. 80.3% of the study participants are younger than 45 years old, the age at which screening should begin. And since the risk of CRC increases with age it is important to examine the knowledge and health practices of this at-risk population.
Another limitation is that our study doesn’t adequately represent all the citizens of Syria. it was limited to specific regions in the country and didn’t cover some regions with a different socioeconomic profile.
5. Conclusions
The findings underscore the imperative for targeted public health interventions aimed at augmenting awareness and knowledge regarding colorectal cancer (CRC) and its early screening modalities in Syria. Education plays a pivotal role in enhancing early detection and alleviating the burden of colorectal cancer within the region. Strategic efforts to enhance public comprehension of CRC screening hold significant promise for mitigating both incidence and mortality rates
Author Contributions
Conceptualization and methodology, Ammer alabed.;software, Raghad Samha.; validation, Raghad Samha.; formal analysis, Ammer alabed; investigation, Raghad Samha; resources, Sami Droubi.; data curation, Shahad Almansour; writing—original draft preparation, Sami Droubi.; writing—review and editing, Shahad Almansour, Majed Alkhalil.; visualization, Majed Alkhalil.; supervision, Youssef Latifeh.; project administration, Ammer alabed.; funding acquisition, Y.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Scientific Research Ethics Committee of Damascus University (protocol code MD-160124-168 and 16-8-2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
I would like to express my gratitude to all the doctors in the data collection group: Noor Khaled, Esraa Hammoria, Ali Alhaj, Aalaa Hammoud, Sara Nouh, Ayman Alahmad, for their invaluable contributions to the data collection process. Their diligent efforts have been instrumental in advancing our research
Conflicts of Interest
The authors declare no conflicts of interest
References
- Assi, R., et al., Metastatic colorectal cancer presenting with bone marrow metastasis: a case series and review of literature. Journal of gastrointestinal oncology, 2016. 7(2): p. 284. [CrossRef]
- Organization, W.H., Cancer https://www.who.int/news-room/fact-sheets/detail/cancer. Son Erişim Tarihi, 2021. 24.
- Van Der Kraak, L., P. Gros, and N. Beauchemin, Colitis-associated colon cancer: is it in your genes? World journal of gastroenterology, 2015. 21(41): p. 11688. [CrossRef]
- Johnson, C.M., et al., Meta-analyses of colorectal cancer risk factors. Cancer causes & control, 2013. 24: p. 1207-1222. [CrossRef]
- Alshammari, S.A., H.A. Alenazi, and H.S. Alshammari, Knowledge, attitude and practice towards early screening of colorectal cancer in Riyadh. J Family Med Prim Care, 2020. 9(5): p. 2273-2280. [CrossRef]
- Harfouch, R., et al., Epidemiology and risk factors of colorectal cancer in Syria: a single-center retrospective study. Eur Rev Med Pharmacol Sci, 2022. 26(13): p. 4654-4658. [CrossRef]
- Kim H, Wang K, Song M, Giovannucci EL. A comparison of methods in estimating population attributable risk for colorectal cancer in the United States. Int J Cancer. 2021 Jun 6;148(12):2947. [CrossRef]
- Siegel, R.L., et al., Colorectal cancer statistics, 2020. CA: a cancer journal for clinicians, 2020. 70(3): p. 145-164. [CrossRef]
- ALmutlaq, B., et al., Assessment of awareness levels toward colorectal cancer early detection and prevention in Saudi Arabia. Gastroenterol Hepatol Open Access, 2017. 6(3): p. 00195. [CrossRef]
- Rex, D.K., et al., Colorectal cancer screening: recommendations for physicians and patients from the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology, 2017. 153(1): p. 307-323. [CrossRef]
- Issa, I.A. and M. Noureddine, Colorectal cancer screening: An updated review of the available options. World journal of gastroenterology, 2017. 23(28): p. 5086. [CrossRef]
- Bibbins-Domingo, K., et al., Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. Jama, 2016. 315(23): p. 2564-2575. [CrossRef]
- Zayegh, O., et al., Awareness and knowledge of colorectal cancer screening among medical students at the University of Aleppo: a cross-sectional study. Avicenna Journal of Medicine, 2022. 12(02): p. 054-060. [CrossRef]
- Hot Questions - Stack Exchange.
- Microsoft Copilot in Bing.
- Alshammari SA, Alenazi HA, Alshammari HS. Knowledge, attitude and practice towards early screening of colorectal cancer in Riyadh. J Fam Med Prim Care. 2020 May;9(5):2273–80. [CrossRef]
- Tfaily MA, Naamani D, Kassir A, Sleiman S, Ouattara M, Moacdieh MP, et al. Awareness of Colorectal Cancer and Attitudes Towards Its Screening Guidelines in Lebanon. Ann Glob Health [Internet]. 2019 May 28 [cited 2024 Mar 26];85(1). Available from: https://annalsofglobalhealth.org/articles/10.5334/aogh.2437. [CrossRef]
- Taha H, Jaghbeer MA, Shteiwi M, AlKhaldi S, Berggren V. Knowledge and Perceptions about Colorectal Cancer in Jordan. Asian Pac J Cancer Prev APJCP. 2015;16(18):8479–86. [CrossRef]
- Wolf AMD, Fontham ETH, Church TR, Flowers CR, Guerra CE, LaMonte SJ, et al. Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA Cancer J Clin. 2018;68(4):250–81. [CrossRef]
- Lynes K, Kazmi SA, Robery JD, Wong S, Gilbert D, Thaha MA. Public appreciation of lifestyle risk factors for colorectal cancer and awareness of bowel cancer screening: A cross-sectional study. Int J Surg. 2016 Dec 1;36:312–8. [CrossRef]
- Teixeira C, Martins C, Trabulo D, Ribeiro S, Cardoso C, Mangualde J, et al. Colorectal Cancer Screening: What Is the Population’s Opinion. GE - Port J Gastroenterol. 2018;25(2):62–7. [CrossRef]
- Saeed RS, Bakir YY, Alkhalifah KH, Ali LM. Knowledge and Awareness of Colorectal Cancer among General Public of Kuwait. Asian Pac J Cancer Prev APJCP. 2018 Sep 26;19(9):2455–60. [CrossRef]
Figure 1.
illustrate that 499(53%) of respondents had a sufficient knowledge level based on our study criteria.
Figure 1.
illustrate that 499(53%) of respondents had a sufficient knowledge level based on our study criteria.

Figure 2.
Sources of information of the participants about early screening of colorectal cancer.
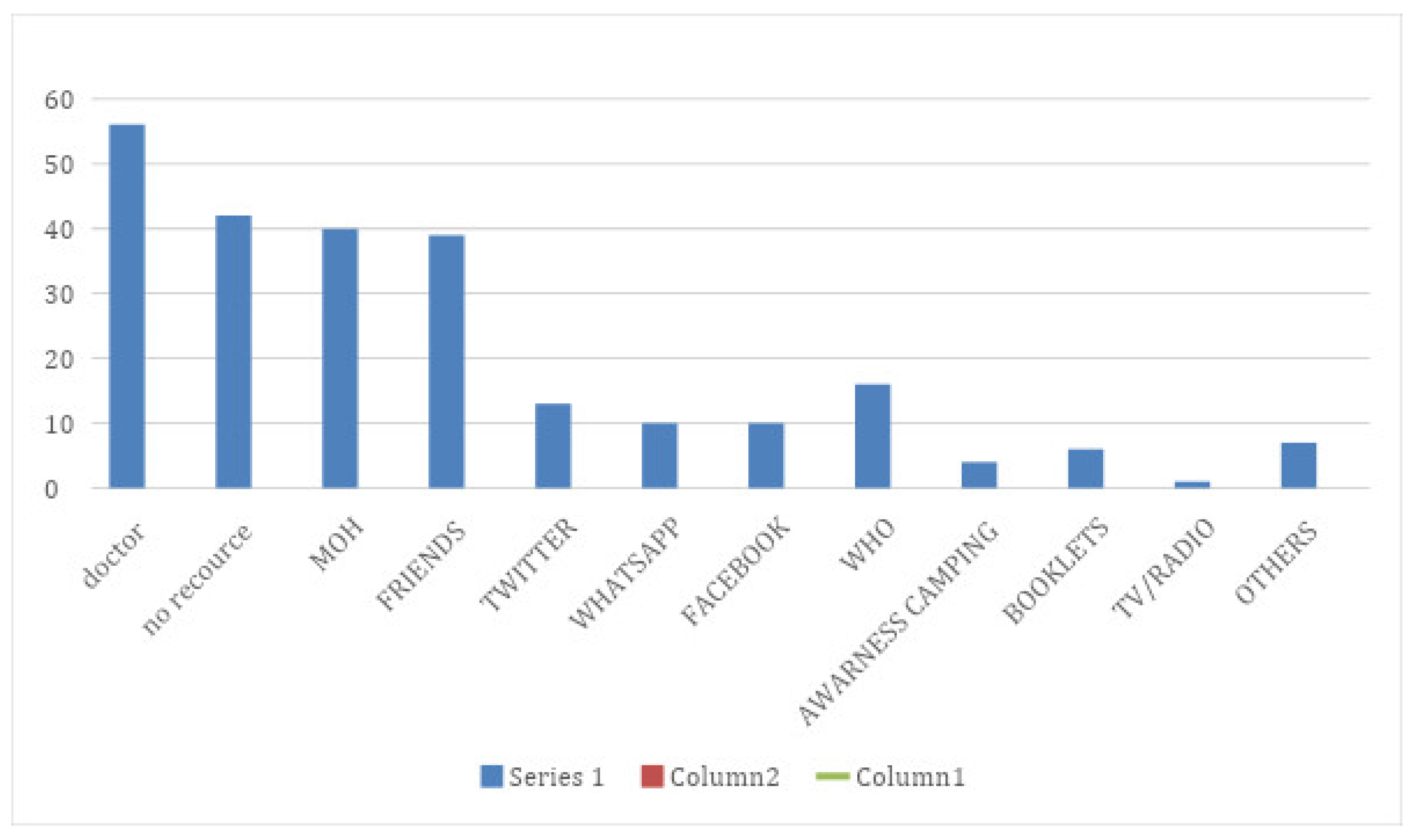

Table 1.
Socio-demographic characteristics of participants.
| Variable | N | % | |
| Knowledge | Sufficient | 499 | 53.8% |
| Insufficient | 429 | 46.2% | |
| Gender | Male | 359 | 38.7% |
| Female | 569 | 61.2% | |
| Familial history | Positive | 95 | 10.2% |
| Negative | 833 | 89.8% | |
| Educational level | Elementary | 223 | 24% |
| Middle school | 76 | 8.2% | |
| High school | 161 | 17.3% | |
| University | 468 | 50.4% | |
| Age categories | 30-35 | 507 | 54.6% |
| 36-40 | 118 | 12.7% | |
| 41-45 | 121 | 13% | |
| 46-50 | 103 | 11.1% | |
| 51-55 | 79 | 8.5% | |
| Work status | Worker | 547 | 58..9% |
| Non- worker | 381 | 41.1% | |
| Martial status | Single | 250 | 26.9% |
| Engaged | 53 | 5.7% | |
| In relationship | 19 | 2% | |
| Married | 570 | 61.4% | |
| Widower | 36 | 3.9% | |
| Economic status | Bad | 76 | 8.2% |
| Median | 396 | 42.7% | |
| Good | 386 | 41.6% | |
| Excellent | 70 | 7.5% |
Table 2.
knowledge and practice towards colorectal cancer and its screening (N=928).
| Variable | ||
| Knowledge | Frequency of yes | Percentage * |
| Have you ever heard of early cancer screening tests? | 488 | 52.6% |
| Colon cancer can be prevented | 237 | 25.5% |
| I think colon cancer is fatal | 538 | 58% |
| Colon cancer recovery rates are increased when detected in early stages | 791 | 85.2% |
| Methods of early detection of colon cancer | Frequency of yes | Percentage |
| Colonoscopy | 754 | 81.2% |
| PR speculum | 473 | 51% |
| Blood detection in the stool sample | 491 | 53% |
| Barium dye for large intestine | 340 | 37% |
| Blood tests | 333 | 36% |
| Abdominal CT scan | 227 | 24% |
| Clinical examination of the rectum | 341 | 37% |
| Other | 44 | 5% |
| Risk factors for colon cancer | Frequency of yes | Percentage |
| Men and women are susceptible to colon cancer | 658 | 70.9% |
| Physical inactivity | 174 | 18.7% |
| Overweight | 338 | 36.4% |
| High Fat Low Fiber Diet | 516 | 55.6% |
| The presence of polyps in the lining of the colon and rectum | 473 | 50.9% |
| Increasing age | 405 | 43.6% |
| Smoking | 316 | 34% |
| Symptoms of colon cancer | Frequency of yes | Percentage |
| The presence of blood in the stool | 668 | 71.9% |
| Sudden weight loss | 552 | 59.4% |
| Increase mucus secretions in the stool | 443 | 47.7% |
| Feeling that the rectum was not fully emptied with defecation | 295 | 31.7% |
| Pain and cramps in the stomach | 502 | 54% |
| Sudden change in the number of bowel motions and Diarrhea | 522 | 56.2% |
| Practice | Frequency of yes | Percentage |
| Have you done early checkups for colon cancer? | 74 | 8% |
| Have you ever thought about undergoing a screening for early detection of colon cancer? | 306 | 33% |
*Percentage is based on the overall sample.
Table 3.
Attitude toward early screening of colorectal cancer.
| Attitude | Strongly agree n(%) | Agree n(%) | Neutral$$$n(%) | Disagree$$$n(%) | Strongly disagree n(%) |
| I think I’m susceptible to colon cancer | 44(4.7) | 224(24.2) | 417(44,9) | 216(23.3) | 27(2.9) |
| I will undergo early screening for colon cancer if my doctor advises me to do so | 429(46.2) | 387(41.7) | 91(9.8) | 15(1.6) | 6(0.6) |
| I think I have adequate information | 37(4) | 200(21.6) | 312(33.6) | 333(35.9) | 46(5) |
Table 6.
Sources of information of the participants about early screening of colorectal cancer.
| Source | % |
| doctor | 56 |
| no resource | 42 |
| MOH | 40 |
| FRIENDS | 39 |
| 13 | |
| 96 | |
| 10 | |
| WHO | 16 |
| AWARENESS CAMPING | 4 |
| BOOKLETS | 6 |
| TV/RADIO | 1 |
Table 4.
knowledge and socio-demographic cross tabs.
| Gender*knowledge | Knowledge | Chi-square test | |||
| Sufficient | Insufficient | p-value | |||
| Gender | Male | 220 | 139 | 359 | 0.001 |
| Female | 279 | 290 | 569 | ||
| Familial history*knowledge | Knowledge | Chi-square test | |||
| Sufficient | Insufficient | p-value | |||
| Familial history | Positive | 50 | 45 | 0.81 | |
| Negative | 449 | 384 | |||
| Education*knowledge | Knowledge | Chi-square test | |||
| Sufficient | Insufficient | p-value | |||
| Education | Elementary | 125 | 98 | 223 | 0.84 |
| Middle school | 42 | 34 | 76 | ||
| High school | 84 | 77 | 161 | ||
| University | 248 | 220 | 468 | ||
| Work*knowledge | Knowledge | Chi-square test | |||
| Sufficient | Insufficient | p-value | |||
| Work-status | Worker | 324 | 223 | 547 | .001 |
| Non-worker | 175 | 206 | 381 | ||
| Age*knowledge | Knowledge | Chi-square test | |||
| Age | Sufficient | Insufficient | p-value | ||
| 30-35 | 277 | 230 | 507 | 0.4 | |
| 36-40 | 57 | 61 | 118 | ||
| 41-45 | 60 | 61 | 121 | ||
| 46-50 | 69 | 43 | 103 | ||
| 51-55 | 45 | 34 | 79 | ||
| E-status*knowledge | Knowledge | Chi-square test | |||
| E-status | Sufficient | Insufficient | p-value | ||
| Bad | 32 | 44 | 76 | 0.001 | |
| Median | 183 | 213 | 396 | ||
| Good | 237 | 149 | 386 | ||
| Excellent | 47 | 23 | 70 | ||
| Relationship*knowledge | Knowledge | Chi-square test | |||
| Relationship | Sufficient | Insufficient | p-value | ||
| Single | 131 | 119 | 250 | 0.08 | |
| Engaged | 37 | 16 | 53 | ||
| In relationship | 13 | 6 | 19 | ||
| Married | 301 | 269 | 570 | ||
| Widower | 19 | 17 | 36 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



