
Submitted:
05 June 2024
Posted:
06 June 2024
You are already at the latest version
Abstract
Background
Oral anticoagulation (OAC) for atrial fibrillation (AF) patients is administered frequently. Vitamin K antagonist (VKA) and direct oral anticoagulants (DOACs) prevent thromboembolic events, but information about the quality of life (QoL) and patient satisfaction, related to both anticoagulants, is limited.
Methods
REGUEIFA is an observational and multicentre study that included patients with AF diagnosis treated by cardiologist. Those on OAC, VKA, and DOACs were selected. The EuroQol-5D (EQ-5D) questionnaire evaluated QoL, and the ACTS (Anti-Clot Treatment Scale) questionnaire investigated patient satisfaction with OAC.
Results
From a total of 1007 patients, 904 patients were on OAC, 532 on VKA and 372 on DOACs. In total, 846 patients completed the EQ-5D questionnaire, with results significantly worse in patients on VKA than on DOACs: (1) mobility limitations (37.6% vs. 24.2%, p
Keywords:
quality of life
; patient satisfaction
; atrial fibrillation
; oral anticoagulation
1. Introduction
Atrial fibrillation (AF) is the most common arrhythmia in clinical practice and is associated with increased mortality and morbidity, mainly due to stroke and heart failure. However, death due to stroke is largely mitigated by anticoagulation, either vitamin K antagonist (VKA) or direct oral anticoagulants (DOACs) 1-4. Both anticoagulants are effective and safe, and widely used for AF 5; it is also associated with a significantly reduced quality of life (QoL), as patients experience a variety of symptoms, including palpitations, dyspnoea, lethargy, chest pain, sleeping difficulties, psychosocial distress and depressed mood 6-8. Some factors are related to poorer QoL: younger age, obesity, symptomatic heart failure, and higher heart rate 9, 10. The impact of oral anticoagulation in terms of QoL is not clearly characterised, as data about the role of different oral anticoagulants in QoL is scarce. VKA was the first anticoagulant used in AF, but is limited by its narrow therapeutic interval, necessitating frequent monitoring and dose adjustment. Multiple drug interactions and food affect the metabolism of VKA, while DOACs, in clinical practice is increasing rapidly; they have a predictable effect without the need for regular monitoring and a lower drug interaction profile. Multiple interactions and efforts to monitor and dose-adjust VKA therapy could have a direct impact on patient QoL and satisfaction. We have evaluated differences in QoL between patients on VKA and DOACs, and patient satisfaction when taking them.
2. Methods
Patients in the REGUEIFA study (Registro Gallego Intercéntrico de Fibrilación Auricular) on anticoagulant treatment were included. This study is an observational and multicentre registry of patients with a primary or secondary diagnosis of AF, as well as being more than 18-years-old, and diagnosed and treated by a cardiologist. Patients were included from January 2018 to February 2020, and all completed the informed consent 11. Demographic characteristics and QoL were evaluated at inclusion time.
The EuroQol-5D (EQ-5D) questionnaire was used to evaluate QoL; it is an instrument that evaluates generic QoL developed in Europe, and widely used 12. The EQ-5D consists of five questions, one for each of five dimensions that include mobility, self-care, usual activities, pain/discomfort, and anxiety/depression with three severity levels for each: level 1 represents no problems, level 2 represents some problems, and level 3 represents extreme problems. The health state 11111 indicates no health problems in any dimension. EQ-5D answers can be converted into an EQ-5D index, ranging from 0 (death) to 1 (perfect health) 13. The associated questionnaire includes the Visual Analog Scale (VAS), in which patients can report their perceived health with a grade from 0 (worst possible health) to 100 (best possible health).
The Anti-Clot Treatment Scale (ACTS) questionnaire measured the burden and benefits of patients on VKA and DOACs (see Appendix): it consists of 17 items and is a Likert-type scale with five possible answers (1= none, to 5= a lot) 14. The first 12 items assess the patient burden on anticoagulant therapy, ranging from 12 to 60, while items 14–16 assess treatment benefits, ranging from 3 to 15. Item 13 assesses the negative impact of anticoagulant treatment on daily life, while item 17 assesses the positive impact of treatment on patients’ lives. Scores for the burden scale (items 1-12) are considered inversely (from 1= a lot to 5= none). Higher scores on the burden and benefits scale indicate greater satisfaction with anticoagulation treatment (burden: the higher the score, the lower the burden; benefit: the higher the score, the greater the benefit).
Statistical Analysis
The quantitative variables are described as mean ± standard deviation (SD), with qualitative variables given as percentages. The Mann-Whitney test was used to evaluate the differences between groups for continuous variables, and the Chi-squared test or the Fisher's exact test were used for categorical variables.
A logistic regression model evaluated clinical factors related to EQ-5D dimensions and whether the OAC type was an independent predictor of EQ-5D dimensions. The model included all characteristics that differed between VKA and DOACs, and the relevant baseline characteristics associated to QoL.
A lineal regression model was used to evaluate clinical factors related to EQ-5D index and VAS score, and to evaluate if the OAC type was an independent predictor of these values. The model included all characteristics that differed between VKA and DOACs, and relevant baseline characteristics associated with QoL.
3. Results
A total of 904 patients on anticoagulant treatment were included, as well as 532 patients on VKA and 372 on DOACs. Patients on VKA were older than those on DOACs (71.69 ± 10.35 vs. 63.61 ± 11.81, p<0.001), with more women on VKA than DOACs (37.03% vs.29.57%, p<0.001). Patients on VKA had higher CHA2DS2-VASc and HASBLED scores (2.87 ± 1.4 vs. 1.93 ± 1.43, p<0.001 and 0.91 ± 0.78 vs. 0.47 ± 0.66, p<0.001, respectively) and comorbidity. Table 1 summarises baseline characteristics.
In addition, 846 patients completed the EQ-5D questionnaire, with 490 on VKA and 356 on DOACs. Patients on VKA had more mobility limitations than patients on DOACs (37.55% vs. 24.16%, p <0.001), more restriction with usual activities (24.69% vs. 18.26%, p=0.026), and more pain/discomfort (31.84% vs. 24.16%, p=0.015). There were fewer patients with health status 11111 in the VKA group (39.39% vs. 55.34%, p<0.001). Table 2 shows results of the EQ-5D questionnaire. The VAS score was also lower in patients on VKA (66.35 vs 70.75, p<0.001) (Table 2 and Figure 1).
Adjusting for baseline characteristics, the type of anticoagulant was not an independent factor for more mobility limitations, more restriction in usual activities, or more pain/discomfort (Table 3). Yet, female gender, coronary artery disease, HASBLED score, and symptomatic AF (EHRA scale ≥2) were associated with greater limitations. The type of anticoagulant was not an independent predictor of the EQ-5D index, as was the VAS score in a multivariate analysis (Table 4). Clinical factors (female gender, chronic obstructive pulmonary disease (COPD), higher CHA2DS2-VASc scores, EHRA scale ≥2 and diuretic use were linked to a lower EQ-5D index and VAS score.
In addition, 713 patients completed the ACTS questionnaire, along with 416 on VKA, and 297 on DOACs. Patients on VKA had lower scores for burden and benefit than those on DOACs (52.1 vs. 55.5, p<0.001 and 11.13 vs. 11.75, p<0.001, respectively), which indicates lower satisfaction with anticoagulation treatment (Table 5). The negative impact of anticoagulant treatment on daily life was higher for VKA, and the positive impact of anticoagulant treatment was also lower for VKA (Table 5).
4. Discussion
This study includes a contemporary cohort of AF patients on OAC treatment, and evaluates differences in QoL and patient satisfaction while taking VKA or DOACs.
Main findings: (1) Patients on VKA had more mobility limitations, more restriction in usual activities, and more pain/discomfort, as well as a lower EQ-5D index and VAS scores than patients on DOACs; (2) Baseline characteristics differed between taking VKA and DOACs; (3) Patient satisfaction with anticoagulant treatment improved on DOACs.
It is well-known that QoL is impaired in AF patients, independent of other cardiovascular conditions 6-9. There is limited data comparing the benefit of different anticoagulant treatments regarding QoL. Moreover, QoL assessment is constrained by the presence of different tools to assess it, and the lack of cross-validation of several AF-specific QoL tools 6, 15-17. We used the EQ-5D questionnaire to evaluate QoL in AF patients receiving OAC, VKA, and DOACs, although we found more mobility limitations, more restriction in usual activities, and more pain/discomfort in patients taking VKA. We also found a lower EQ-5D index and a lower VAS score in those on VKA. However, when analysing baseline characteristics, we found more comorbidity in patients on VKA, as it was not an independent factor for worse QoL; female gender, CHADS-VASc and HASBLED scores, coronary artery disease, COPD, and EHRA classification were associated with more QoL limitations. These findings are assessed according to the literature, which consistently describes poorer QoL in female AF patients, but it is not clear if this reflects gender differences in the population, or is related to AF per se 18. The EHRA scale describes symptom severity in AF patients, and is related to QoL 19, 20. Several patient factors, such as symptomatic heart failure, diabetes, COPD, and coronary artery disease, are associated with worse QoL 9, 21.
Baseline clinical characteristics are significantly different between anticoagulants, VKA and DOACs, and these variations are associated with patient QoL, as we mentioned before. The marked differences between patients in this study, in which patients were included and treated by a cardiologist, can be explained by the restriction to prescribe DOACs, established by our health system 22. Briefly, our National Health System considers the use of DOACs in patients with allergy or specific contraindication for VKA, in those with previous intracranial haemorrhage, in patients with a stroke and high risk of haemorrhagic transformation, in patients with arterial embolism, despite use of VKA with good range control, and those on VKA with poor controls (time of therapeutic range <60% for 6 months). In all other cases, our National Health System does not finance prescriptions for DOAC. The only way to prescribe them, excluding previous criteria, involves intervention (electrical cardioversion or ablation), in which the need for OAC lasts 2-3 months without chronic anticoagulation; in these cases, the hospital pharmacy provides patient treatment. VKA patients are older, have more women, and more risk factors.
Finally, we used the ACTS questionnaire, a validated metric of patient-reported burden and benefit of oral anticoagulation, to evaluate patient satisfaction with anticoagulant treatment, which was higher for DOACs than for VKA. Higher ACTS scores for patients on DOACs vs. VKA were previously reported in other cohorts 23, 24. These findings are likely due to differences between each treatment. VKA was the mainstay of OAC, but is a difficult drug to dose and monitor. Due to the variability in dose-response with VKA treatment, monitoring the degree of anticoagulation is imperative, usually needing a changed dose 25. Patients on VKA must follow a strict diet, due to multiple food interactions and drug-drug interactions. However, DOACs have major pharmacologic advantages over VKA, including rapid onset and offset of action, few drug interactions, and predictable pharmacokinetics, eliminating the need for regular coagulation monitoring 26. All these advantages may justify the greater satisfaction found in patients on DOACs. This information, provided by ACTS questionnaire, suggests that for patients taking VKA, patient-reported care satisfaction should be routinely assessed, and, in those patients with low satisfaction, switching from VKA to DOACs should be considered.
5. Limitations
This is an observational study; however, it included a high number of patients from different regions, so findings on baseline characteristics, QoL, and patient satisfaction with treatment reflect the data of a wide AF population.
The EQ-5D questionnaire is generic and not designed specifically for AF patients; such that its sensitivity and discriminative capacity is lower than that of other questionnaires. It has been described as a ceiling effect (patients with maximum scores and health status 11111), which may present some difficult comparisons.
The ACTS questionnaire does not provide information about patient satisfaction, so some issues may not be represented as outcomes, self-efficacy, or patient acceptance of treatment. Other factors, such as the duration of OAC therapy before administering the ACTS questionnaire could influence results. In this first study, we did not evaluate whether the burden and benefit scores changed during follow-up.
6. Conclusions
In a contemporary cohort of AF patients taking OAC, those on VKA had more comorbidity, more mobility limitations, more restriction in usual activities and more pain/discomfort, and a lower EQ-5D index and VAS scores than patients on DOACs. As such, patient satisfaction with anticoagulants is higher when taking DOACs.
Funding
The REGUEIFA study was supported by Daiichi-Sankyo, Tokyo, Japan.
Acknowledgments
We want to express thanks for the efforts and contributions of all participants, as well as the support from the Sociedad Gallega de Cardiología, Coruña, Spain.
Conflicts of Interest
None.
Appendix (ACTS questionnaire)
During the past 4 weeks...
- How much does the possibility of bleeding as a result of anti-clot treatment limit you from taking part in vigorous physical activities? (e.g. exercise, sports, dancing, etc.).
- How much does the possibility of bleeding as a result of anti-clot treatment limit you from taking part in your usual activities? (e.g. work, shopping, housework etc.).
- How bothered are you by the possibility of bruising as a result of anti-clot treatment?
- How bothered are you by having to avoid other medicines (e.g. aspirin) as a result of anti-clot treatment?
- How much does anti-clot treatment limit your diet? (e.g. food or drink, including alcohol).
- How much of a hassle (inconvenience) are the daily aspects of anti-clot treatment? (e.g. remembering to take your medicine at a certain time, taking the correct dose of your medicine, following a diet, limiting alcohol, etc.).
- How much of a hassle (inconvenience) are the occasional aspects of anti-clot treatment? (e.g. the need for blood tests, going to or contacting the clinic/doctor, making arrangements for treatment while travelling etc.).
Now I want to ask you about daily and occasional aspects of your ACT during the past 4 weeks!
- 8.
- How difficult is it to follow your anti-clot treatment?
- 9.
- How time-consuming is your anti-clot treatment?
- 10.
- How much do you worry about your anti-clot treatment?
- 11.
- How frustrating is your anti-clot treatment?
- 12.
- How much of a burden is your anti-clot treatment?
- 13.
- Overall, how much of a negative impact has your anti-clot treatment had on your life?
- 14.
- How confident are you that your anti-clot treatment will protect your health? (e.g. prevent blood clots, stroke, heart attack, DVT, embolism)
- 15.
- How reassured do you feel because of your anti-clot treatment?
- 16.
- How satisfied are you with your anti-clot treatment?
- 17.
- Overall, how much of a positive impact has your anti-clot treatment had on your life?
References
- Chugh SS, Havmoeller R, Narayanan K, Singh D, Rienstra M, Benjamin EJ, Gillum RF, Kim YH, McAnulty JH Jr, Zheng ZJ, Forouzanfar MH, Naghavi M, Mensah GA, Ezzati M, Murray CJ. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation 2014;129:837–847.
- Andersson T, Magnuson A, Bryngelsson IL, Frobert O, Henriksson KM, Edvardsson N, Poci D. All-cause mortality in 272,186 patients hospitalized with incident atrial fibrillation 1995-2008: a Swedish nationwide long-term casecontrol study. Eur Heart J 2013;34:1061–1067.
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor.
- for stroke: the Framingham Study. Stroke 1991;22:983–988.
- Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med 2007; 146:857–867.
- Ruff CT, Giugliano RP, Braunwald E, Hoffman EB, Deenadayalu N, Ezekowitz MD,.
- Camm AJ, Weitz JI, Lewis BS, Parkhomenko A, Yamashita T, Antman EM. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet 2014;383:.
- 955–962.
- Dorian P, Jung W, Newman D, Paquette M, Wood K, Ayers GM, Camm J, Akhtar M, Luderitz B. The impairment of health-related quality of life in patients with intermittent atrial fibrillation: implications for the assessment of investigational therapy. J Am Coll Cardiol 2000;36:1303–1309.
- Thrall G, Lane D, Carroll D, Lip GY. Quality of life in patients with atrial fibrillation: a systematic review. Am J Med 2006;119:448.e1–19.
- Steg PG, Alam S, Chiang CE, Gamra H, Goethals M, Inoue H, Krapf L, Lewalter T, Merioua I, Murin J, Naditch-Brule L, Ponikowski P, Rosenqvist M, Silva-Cardoso J, Zharinov O, Brette S, Neill JO, RealiseAF investigators. Symptoms, functional status and quality of life in patients with controlled and uncontrolled atrial fibrillation: data from the RealiseAF cross-sectional international registry. Heart 2012;98: 195–201.
- Tiffany C. Randolph, DaJuanicia N. Simon, Laine Thomas, Larry A. Allen, Gregg C. Fonarow, Bernard J. Gersh, Peter R. Kowey, James A. Reiffel, Gerald V. Naccarelli, Paul S. Chan, John A. Spertus, Eric D. Peterson, Jonathan P. Piccini, and on behalf of the ORBIT AF Investigators and Patients. Patients Factors Associtatted with Quality of Life in Atrial Fibrillation Randolph-Determinants of Quality of Life in Atrial Fibrillation. Am Heart J. 2016;182:135-143.
- Zhuang J, Lu Y, Tang K, PengW, Xu Y. Influence of body mass index on recurrence and quality of life in atrial fibrillation patients after catheter ablation: a meta-analysis and systematic review. Clin Cardiol 2013;36:269–275.
- Javier García Seara, Laila González Melchor, María Vázquez Caamaño, Emilio Fernández-Obanza Windcheid, Miriam Piñeiro Portela, Eva González Babarro, Pilar Cabanas Grandío, Olga Durán Bobín, Óscar Prada Delgado , Juliana Elices Teja, Evaristo Freire, Mario Gutiérrez Feijoo, Óscar Díaz Castro, Javier Muñiz García, Carlos González Juanatey. Rationale, design and basal characteristics of REGUEIFA study (Multicenter Registry of Atrial. REC: CARDIOCLINICS, ahead of print.
- Fibrillation in Galicia).
- Rosalind Rabin and Frank de Charro. EQ-SD: a measure of health status from the EuroQol Group. Annals of Medicine. 2001; 33(5): 337-343.
- Herdman, M, Badía X and Berra S. El EuroQol-5D: una alternativa sencilla para la medición de la calidad de vida relacionada con la salud en atención primaria. Atención primaria. 2001;28(6):425-429.
- Carmen Suárez, Antonio Pose, Manuel Montero-Pérez Barquero, Jaume Roquer, Jaime Gállego, Carles Ráfols, Daniel Cazorla, José Vivanco son behalf of the Grupo de Trabajo Comité Científico Estudio ALADIN. Validation of satisfaction questionnaire ACTS in outpatients with atrial fibrillation treated with oral anticoagulants in Spain. ALADIN Study. Med Clin (Barc). 2016;147(5):192-198.
- Arribas F, Ormaetxe JM, Peinado R, Perulero N, Ramirez P, Badia X. Validation of.
- the AF-QoL, a disease-specific quality of life questionnaire for patients with atrial fibrillation. Europace 2010;12:364–370.
- Spertus J, Dorian P, Bubien R, Lewis S, Godejohn D, Reynolds MR, Lakkireddy DR, Wimmer AP, Bhandari A, Burk C. Development and validation of the Atrial Fibrillation Effect on QualiTy-of-Life (AFEQT) Questionnaire in patients with atrial fibrillation. Circ Arrhythm Electrophysiol 2011;4:15–25.
- Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, Bonsel G, Badia X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res 2011;20:1727–1736.
- Linn Arvidsson Strømnes, Helene Ree, Knut Gjesdal, Inger Ariansen. Sex Differences in Quality of Life in Patients With Atrial Fibrillation:A Systematic Review. J Am Heart Assoc. 2019;8:e010992.
- Kirchhof P, Auricchio A, Bax J, Crijns H, Camm J, Diener HC, Goette A, Hindricks G, Hohnloser S, Kappenberger L, Kuck KH, Lip GY, Olsson B, Meinertz T, Priori S, Ravens U, Steinbeck G, Svernhage E, Tijssen J, Vincent A, Breithardt G. Outcome parameters for trials in atrial fibrillation: executive summary. Eur Heart J 2007;28:2803–2817.
- Gareth J. Wynn, Derick M. Todd, MatthewWebber, Laura Bonnett, James McShane, Paulus Kirchhof, and Dhiraj Gupta. The European Heart Rhythm Association.
- symptom classification for atrial fibrillation: validation and improvement through a simple modification. Europace. 2014; 16, 965–972.
- Justin B. Echouffo-Tcheugui, Peter Shrader, Laine Thomas, Bernard J. Gersh, Peter R. Kowey, Kenneth W. Mahaffey, Daniel E. Singer, Elaine M. Hylek, Alan S. Go, Eric D. Peterson, Jonathan P. Piccini, Gregg C. Fonaro. Care Patterns and Outcomes inAtrial Fibrillation Patients With andWithout DiabetesORBIT-AF Registry. JAm Coll Cardiol 2017;70:1325–35.
- Informe de posicionamiento terapéutico UT_ACOD/V5/21112016. Criterios y recomendaciones generales para el uso de los anticoagulantes orales directos (ACOD) en la prevención del ictus y la embolia sistémica en pacientes con fibrilación auricular no valvular. Fecha de publicación 21 de noviembre de 2016. https://www.aemps.gob.es/medicamentosUsoHumano/informesPublicos/docs/criterios-anticoagulantes-orales.pdf.
- Coleman CI, Haas S, Turpie AG, Kuhls S, Hess S, Evers T, Amarenco P, KirchhofP, Camm AJ; XANTUS Investigators. Impact of switching from a vitamin Kantagonist to rivaroxaban on satisfaction with anticoagulation therapy: theXANTUS-ACTS substudy.Clin Cardiol. 2016;39:565–569.
- Contreras Muruaga MD, Vivancos J, Reig G, Gonzalez A, Cardona P, Ramirez-Moreno JM, Marti J, Fernandez CS; ALADIN Study Investigators. Satisfaction,quality of life and perception of patients regarding burdens and benefits ofvitamin K antagonists compared with direct oral anticoagulants in patientswith nonvalvular atrialfibrillation.J Comp Eff Res. 2017;6:303–312.
- Ute I. Schwarz, Marylyn D. Ritchie, Yuki Bradford, Chun Li, ScottM. Dudek, Amy Frye-Anderson, Richard B. Kim, Dan M. Roden, and C. Michael Stein. Genetic determinants of response to warfarin during initial anticoagulation. N Engl J Med 2008;358:999–1008.
- Kenneth A Bauer. Pros and cons of new oral anticoagulants. Hematology Am Soc Hematol Educ Program 2013;2013:464–470.
Figure 1.
Visual Anolog Scale scores.
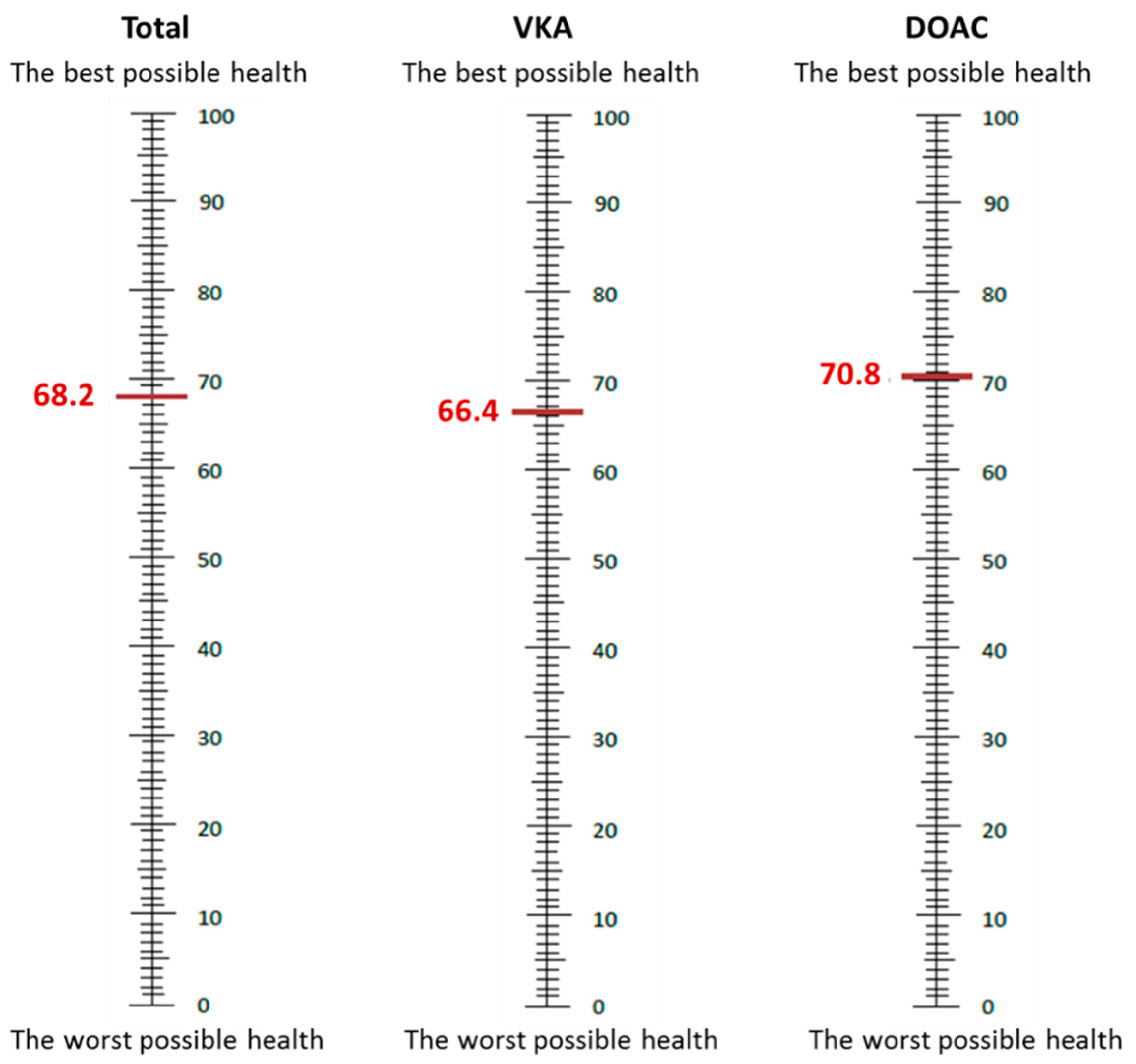

Table 1.
Baseline characteristics.
| Variables | Total (n=904) | VKA (n=532) | DOAC (n=372) | p-value |
|---|---|---|---|---|
| Age, mean ± SD | 68.36 ± 11.67 | 71.69 ± 10,35 | 63.61 ± 11.81 | <0.001 |
| Women, % | 33.96 | 37.03 | 29.57 | 0.020 |
| Renal failure, % | 6.86 | 10.34 | 1.88 | <0.001 |
| PAD, % | 2.99 | 4.14 | 1.34 | 0.016 |
| CAD, % | 12.17 | 14.29 | 9.14 | 0.020 |
| Dementia, % | 0.66 | 1.13 | 0.00 | 0.046 |
| OSAHS, % | 4.87 | 4.89 | 4.84 | 0.973 |
| COPD, % | 11.28 | 13.35 | 8.33 | 0.019 |
| Anaemia, % | 3.98 | 5.45 | 1.88 | 0.009 |
| Diabetes, % | 19.91 | 22.74 | 15.86 | 0.011 |
| Hyperlipidaemia, % | 50.00 | 53.57 | 44.89 | 0.010 |
| Hypertension, % | 66.37 | 72.93 | 56.99 | <0.001 |
| Obesity (BMI≥30), % | 42.29 | 41.24 | 43.78 | 0.448 |
| CHA2DS2-VASc score, mean±SD | 2.48 ± 1.48 | 2.87 ± 1.4 | 1.93 ± 1.43 | <0.001 |
| HAS-BLED score, mean ± SD | 0.73 ± 0.77 | 0.91 ± 0.78 | 0.47 ± 0.66 | <0.001 |
| EHRA ≥ II, % | 66.48 | 65.41 | 68.01 | 0.416 |
| AF classification | <0.001 | |||
| First diagnosed episode, % | 23.12 | 25.56 | 19.62 | |
| Paroxysmal, % | 20.24 | 17.86 | 23.66 | |
| Persistent, % | 27,43 | 21.80 | 35.48 | |
| Long standing persistent, % | 2.54 | 2.26 | 2.96 | |
| Permanent, % | 26.66 | 32.52 | 18.28 | |
| EF <50%, % | 18.30 | 19.55 | 16.57 | 0.268 |
| Valvular heart disease, % | 17.26 | 21.05 | 11.83 | <0.001 |
| Beta blockers, % | 68.47 | 65.98 | 72.04 | 0.053 |
| Calcium channel blockers, % | 5.64 | 6.02 | 5.11 | 0.561 |
| Digoxin, % | 6.64 | 7.89 | 4.84 | 0.069 |
| ACE inhibitors / ARBs, % | 54,20 | 54,89 | 53,23 | 0,622 |
| Diuretics, % | 36,06 | 42,67 | 26,61 | <0,001 |
| Antiarrhythmic drugs, % | 38,83 | 28,01 | 54,30 | <0,001 |
Abbreviations: PAD, peripheral artery disease; CAD, coronary artery disease; OSAHS, obstructive sleep apnoea-hypopnea syndrome; COPD, chronic obstructive pulmonary disease; BMI, body mass index; EF, ejection fraction; ACE, angiotensin converting enzyme; ARBs, angiotensin II receptor blockers.
Table 2.
EQ-5D questionnaire scores.
| Total (n=846) | VKA (n=490) | DOAC (n=356) | p-value | |
|---|---|---|---|---|
| Mobility | ||||
| Patients with some problems (%) | 31.91 | 37.55 | 24.16 | <0.001 |
| Patients with extreme problems (%) | 0.47 | 0.41 | 0.56 | 1.000 |
| Self-care | ||||
| Patients with some problems (%) | 7.92 | 8.78 | 6.74 | 0.279 |
| Patients with extreme problems (%) | 0.71 | 0.61 | 0.84 | 0.700 |
| Usual activities | ||||
| Patients with some problems (%) | 21.99 | 24.69 | 18.26 | 0.026 |
| Patients with extreme problems (%) | 1.89 | 2.04 | 1.69 | 0.802 |
| Pain / Discomfort | ||||
| Patients with some problems (%) | 28.61 | 31.84 | 24.16 | 0.015 |
| Patients with extreme problems (%) | 2.72 | 3.47 | 1.69 | 0.136 |
| Anxiety / depression | ||||
| Patients with some problems (%) | 26.12 | 26.53 | 25.56 | 0.751 |
| Patients with extreme problems (%) | 3.19 | 3.88 | 2.25 | 0.235 |
| Visual Analog Scale (VAS), mean ± SD | 68.2 ± 16.1 | 66.35 ± 16.21 | 70.75 ± 15.62 | <0.001 |
| EQ-5D index, mean ± SD | 0.82 ± 0.21 | 0.79 ± 0.21 | 0.85 ± 0.2 | <0.001 |
| Patients with health status 11111 (%) | 46.10 | 39.39 | 55.34 | <0.001 |
Table 3.
Multivariate logistic regression analysis.
| Mobility | ||||
|---|---|---|---|---|
| Final model | ||||
| OR | CI 95% | P value | ||
| OAC (DOAC) | 0.99 | 0.69 | 1.42 | 0.959 |
| Age | 1.04 | 1.02 | 1.07 | <0.001 |
| Female | 2.46 | 1.71 | 3.55 | <0.001 |
| CAD | 1.84 | 1.13 | 2.98 | 0.014 |
| COPD | 1.91 | 1.15 | 3.20 | 0.013 |
| CHA2DSVASc score | 1.2 | 1 | 1.43 | 0.044 |
| HASBLED score | 1.2 | 1 | 1.43 | 0.006 |
| EHRA scale ≥2 | 1.75 | 1.20 | 2.56 | 0.004 |
| AF type | ||||
| Paroxysmal | 1.41 | 0.82 | 2.42 | 0.212 |
| Persistent | 2.42 | 1.42 | 4.14 | 0.001 |
| Long-standing persistent | 2.43 | 0.84 | 7.06 | 0.102 |
| Permanent | 1.59 | 0.96 | 2.63 | 0.069 |
| Diuretics | 1.57 | 1.09 | 2.27 | 0.015 |
| Usual Activity | ||||
| Final model | ||||
| OR | CI 95% | P value | ||
| OAC (DOAC) | 0.99 | 0.68 | 1.44 | 0.966 |
| Female | 2.01 | 1.41 | 2.88 | <0.001 |
| CAD | 2.05 | 1.27 | 2.31 | 0.003 |
| HASBLED score | 1.70 | 1.32 | 2.19 | <0.001 |
| EHRA scale 3-4 | 4.27 | 2.40 | 7.62 | <0.001 |
| AF type | ||||
| Paroxysmal | 2.70 | 1.48 | 4.93 | 0.001 |
| Persistent | 2.81 | 1.54 | 5.11 | 0.001 |
| Long-standing persistent | 2.04 | 0.63 | 6.55 | 0.233 |
| Permanent | 2.80 | 1.59 | 4.94 | <0.001 |
| Diuretics | 1.77 | 1.22 | 2.58 | 0.003 |
| Pain/Discomfort | ||||
| Final model | ||||
| OR | CI 95% | P value | ||
| OAC (DOAC) | 0.97 | 0.69 | 1.36 | 0.854 |
| Female | 1.95 | 1.39 | 2.74 | <0.001 |
| CAD | 1.57 | 0.99 | 2.48 | 0.055 |
| CHA2DSVASc score | 1.25 | 1.08 | 1.44 | 0.003 |
| HASBLED score | 1.28 | 1 | 1.68 | 0.047 |
| EHRA scale 3-4 | 2.42 | 1.43 | 4.11 | 0.001 |
| Valvular heart disease | 1.51 | 1.01 | 2.27 | 0.046 |
Abbreviations as table 1.
Table 4.
Multivariate lineal regression analysis.
| EQ-5D index | ||||
|---|---|---|---|---|
| Final model | ||||
| Coefficient | CI 95% | P value | ||
| OAC (DOAC) | 0.009 | -0.019 | 0.036 | 0.534 |
| Female | -0.092 | -0.121 | -0.063 | <0.001 |
| CAD | -0.055 | -0.095 | -0.016 | 0.006 |
| COPD | -0.059 | -0.101 | -0.017 | 0.006 |
| CHA2DSVASc score | -0.014 | -0.026 | -0.001 | 0.029 |
| HASBLED score | -0.040 | -0.061 | -0.019 | <0.001 |
| EHRA scale ≥2 | -0.040 | -0.068 | -0.013 | 0.004 |
| AF type | ||||
| Paroxysmal | -0.026 | -0.065 | 0.013 | 0.185 |
| Persistent | -0.039 | -0.076 | -0.001 | 0.042 |
| Long-standing persistent | -0.041 | -0.123 | -0.042 | 0.336 |
| Permanent | -0.044 | -0.082 | -0.006 | 0.024 |
| Diuretics | -0.039 | -0.068 | -0.009 | 0.011 |
| VAS | ||||
| Final model | ||||
| Coefficient | CI 95% | P value | ||
| OAC (DOAC) | 1.47 | -0.74 | 3.68 | 0.192 |
| Female | -3.39 | -5.73 | -1.05 | 0.005 |
| COPD | -4.31 | -7.68 | -0.93 | 0.012 |
| Anaemia | -5.68 | -11.03 | -0.33 | 0.038 |
| Hyperlipidaemia | -2.91 | -5.03 | -0.79 | 0.007 |
| CHA2DSVASc score | -1.09 | -2 | -0.19 | 0.018 |
| EHRA scale ≥2 | -5.10 | -7.33 | -2.86 | <0.001 |
| Diuretics | -2.80 | -5.18 | -0.41 | 0.021 |
| Antiarrhythmic drug treatment | 2.44 | 0.16 | 4.72 | 0.036 |
Abbreviations as table 1.
Table 5.
ACTS questionnaire scores.
| Total (n= 713= | VKA (n= 416) | DOAC (n= 297) | p-value | |
|---|---|---|---|---|
| Burden score, mean ± SD | 53.51 ± 7.96 | 52.09 ± 8.44 | 55.5 ± 6.75 | <0.001 |
| Benefit score, mean ± SD | 11.39 ± 2.51 | 11.13 ± 2.42 | 11.75 ± 2.6 | <0.001 |
| General negative impact, mean ± SD | 1.68 ± 1.01 | 1.77 ± 1.02 | 1.56 ± 0.99 | <0.001 |
| Distribution of scores, % | <0.001 | |||
| 1 | 58.20 | 51.20 | 68.01 | |
| 2 | 26.51 | 31.73 | 19.19 | |
| 3 | 6.59 | 8.65 | 3.70 | |
| 4 | 6.17 | 5.29 | 7.41 | |
| 5 | 2.52 | 3.13 | 1.68 | |
| General positive impact, mean ± SD | 3.65 ± 0.99 | 3.56 ± 0.96 | 3.78 ± 1.02 | <0.001 |
| Distribution of scores, % | <0.001 | |||
| 1 | 3.65 | 3.61 | 3.70 | |
| 2 | 9.96 | 10.34 | 9.43 | |
| 3 | 20.62 | 25.00 | 14.48 | |
| 4 | 49.51 | 49.04 | 50.17 | |
| 5 | 16.27 | 12.02 | 22.22 |
Burden: the higher the score, the lower burden. Benefit: the higher the score, the greater the benefit.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



