
Submitted:
06 June 2024
Posted:
07 June 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The aim of this article is to present the course of the COVID-19 pandemic in Poland in 2020-2022, the formation of ad hoc health and anti-crisis policies, an assessment of crisis management and the perceived impact of the pandemic and anti-crisis measures.The paper draws on literature, official reports on the pandemic, data from Eurostat and other information from state institutions and public organisations.Particular attention was paid to the analysis and evaluation of the objectives, instruments and effects of the policies pursued by the state in a coordinated manner, i.e. the anti-pandemic policy and the anti-crisis policy. The anti-pandemic policy in Poland has failed to protect the country from significant personal losses and negative impacts on the health of the population and demographic processes.The anti-crisis policy of the state carried out with the mobilisation of businesses and disciplined society, in the form of anti-crisis shields supplemented and adjusted on an ongoing basis, allowed Poland to avoid a deep crisis and economic recession. Attention was drawn to the need to coordinate the management of health and economic crises nationally and internationally, and to the need to have a medium-term anti-crisis state strategy and a system for the early detection of crisis symptoms.
Keywords:
COVID-19 pandemic
; economic crisis
; health policy
; anti-crisis policy
; consequences of the pandemic in Poland
1. Introduction
A crisis can be defined as a sudden disruption in the functioning of society and the economy threatening, likely to cause immediate losses and halt economic development processes on a national and international scale. There are many definitions of a crisis in the literature, formulated from the perspective of different scientific disciplines and organisations [1,2,3,4]. Most of them emphasise the breakdown of the previously stable development process and the occurrence of economic regression and disruption in the social sphere, as well as the shattering of the previous system of values and social trust. Various other recurring characteristics are attributed to the crisis, such as the suddenness of its onset, violent progress, the unpredictability in terms of its extent, depth and duration, and the consequences caused. In general, there is a loss of control over the course of economic and social processes, a weakening of economic links and social ties, an increased uncertainty which, in aggregate, can lead to panic, the control of which requires extraordinary state interventions.
The sources of the crisis may lie in the natural, biological, economic, social, psychological or political spheres. The causes and sources of the crisis determine the nature of the emergency and affect the social behaviour and conduct of economic actors, i.e. households, businesses, the state, and public institutions. Crises easily cross national borders, spread internationally and become global in nature. The suddenness of the occurrence and the powerlessness in the face of the force of propagation of the crisis-causing agent require the active participation of the state in overcoming the adverse effects of the crisis both during the crisis as well as after it has subsided [4,5]. The state’s anti-crisis measures also require international coordination and the implementation of an appropriate national crisis management system by companies and public institutions, as well as compliance with the anti-crisis policy and crisis management rules by members of the public in the defined territory.
The disruption of the implementation of the development strategy and policy adopted by the country due to the crisis requires the introduction of ad hoc anti-crisis policies and the modification of socio-economic development policies during and after the removal of the sources and the resolution of the crisis [6,7]. Crisis management in Poland in the 2020-2022 period required directing attention to two activity areas in particular: elimination of the cause as well as preventing losses caused by the crisis and supporting development. The first area is referred to as the anti-pandemic policy in this paper, focused mainly at containing the SARS-CoV-2 coronavirus epidemic as the main source of the crisis, the second area is the anti-crisis policy, aimed at preventing the adverse economic and social effects caused by the crisis, sustaining economic activity and initiating and supporting development processes. The two types of policies overlap. In fact, all measures taken by the state at the beginning of the pandemic were aimed at both health and socio-economic considerations.
As soon as the first infections appeared in Poland, restrictive anti-pandemic procedures were introduced, to be replaced by pandemic emergency procedures after the first wave of the pandemic had passed. The basic anti-pandemic measures included: expanding and adjusting the hospital treatment base (hospital wards in stadiums, market halls and sports centres), introducing a sanitary regime in public places and in transport, restricting the freedom of assembly and movement of people, implementing universal multiple vaccination of adults and then adolescents and children. A parallel activity area for the public authorities consisted of various types of anti-crisis economic and financial programmes for enterprises in endangered industries, enabling them to survive the revealed crisis of operation as well as restrictions on the operation of a number of production and service establishments and public institutions, the transition to a distance learning system, facilitation of remote working and other forms of labour market facilitation [8]. By activating the so-called 'crisis shields', the state offered various forms of support to workers and their families who lost their jobs or income and suffered other severe consequences of the pandemic [5]. During the 2020-2022 crisis caused by the COVID-19 pandemic in Poland, these two types of crisis policies are the responsibility of the state, i.e. the government and various public institutions. National policies take into account European Union and World Health Organisation (WHO) regulations. The anti-pandemic and anti-crisis policies provide a framework for crisis management that is up to the businesses, households and NGOs. The pandemic, its course and the implementation of anti-pandemic and anti-crisis policies had a multifaceted impact on socio-economic life and became an amplifying factor for the development of various pre-existing phenomena or new phenomena that emerged during the pandemic. Such new phenomena have appeared in service sector in particular, and their vehicle has been digitisation and the need for various forms of security [9,10,11].
2. COVID-19 Pandemic as a Source of Crisis in Poland between 2020 and 2022
A contagious disease caused by the zoonotic SARS-CoV-2 virus has emerged mid-December 2019 in the Chinese city of Wuhan, among people associated with the animal and seafood market. The new virus that caused pneumonia and respiratory failure was highly contagious, resulting in a rapid spread of the epidemic in China and abroad. In Europe, the disease appeared in 2019/2020 and moved rapidly from country to country. The first infection in Poland was reported on 4 March 2020 in a patient who had returned from Germany and was hospitalized in Zielona Góra, which is close to the German border. Coronavirus has created a huge public health threat everywhere. Soon after, patients returning from Italy and the UK were sent to hospitals in various parts of the country. The first fatal case was reported in Poland on 12 March 2020, i.e. one day after the World Health Organisation raised the COVID-19 pandemic alert [12].
The state of epidemic, entailing heightened health strictures, was in force in Poland from 20 March 2020 to 15 May 2022, and was transformed on 16 May 2022 into an epidemic emergency. The emergence of the coronavirus outbreak created a huge challenge for the national health service, which was unprepared for such a rapid expansion of the disease and such a large-scale threat to people’s health and lives. Despite this, it managed to keep infection status and death rates relatively low for half a year. In March 2020, 2311 people were infected with coronavirus, 33 of whom died [13]. An undulating pattern is evident in the progress of the disease in Poland, with lower rates of infection and death in spring and summer and increased rates in autumn and winter. From March to August 2020, the daily number of infections did not exceed 1,000, with the total number of infections slightly exceeding 67,000. During the first high wave of the pandemic between September 2020 and April 2021, the daily number of infections ranged from 1,500 in September 2020 to almost 33,000 in March 2021. The second high wave of infections began in September 2021 and lasted until April 2022. The daily number of infections sometimes reached 20,000 people during this time. The third wave of the pandemic that occurred between August 2022 and March 2023 was characterised by high variability in the severity of infections and deaths, associated with uneven regional quenching of the disease (Table 1).
The total number of infections since the start of the pandemic reached 1.5 million in late 2020, exceeded 2 million in March 2021, 3 million in October and 4 million in December 2021, 5 million in February 2022 and 6 million in May 2022. According to the Ministry of Health, 6,519,169 people were infected in Poland between the start of the pandemic in March 2020 and May 2023 when the WHO lifted the pandemic alert, of whom 5,335,777 recovered. The total number of deaths reached 119 610 cases, which translates into the rate of 308 deaths per 100 000 inhabitants. The only countries that recorded higher mortality rates than Poland were Bulgaria (535), Hungary (477), and the Czech Republic (377). Coronavirus mortality rates were lower in Western European countries [14]. By region, the highest coronavirus mortality rates were recorded in the provinces of Podkarpackie, Lubelskie, Podlaskie, Warmińsko-Mazurskie and Kujawsko-Pomorskie. High mortality rates were clearly correlated with low levels of antiviral vaccination as well as with other factors such as the equipment and availability of treatment facilities, the employment level of medical staff, efficiency of the health service and the general level of development of the region [5]. The mortality also depended on the demographic structure, with higher death rates observed among men and the elderly population. Among those who died from COVID-19 in 2020. 83% were over 65 years of age. The pandemic exacerbated adverse demographic phenomena such as increasing negative population growth and the so-called excess deaths above the trend line, referred to as health debt [14,15]. Overall, it can be said that the pandemic caused irreparable loss of life and damage due to the deterioration of the health of survivors. It has challenged the entire health care system to a great extent, uncovered its weaknesses and inadequacies in terms of equipment, organisation and management. In addition to the human losses, the pandemic generated high economic and social costs [16]. By piling up challenges for citizens, businesses and the state, it has become the real cause of the economic crisis.
3. Health policy in Poland
Health is a fundamental value, a right and a human need. It has a significant impact on people’s quality of life and is an important element of the state’s finances and economic and social policies. In order to ensure the protection of citizens’ health, informed health policy-making is essential, which takes on particular importance during epidemic outbreaks. Conducting an effective and efficient health policy, the aim of which is not only to provide medical treatment but also to create generally favourable conditions for protecting, improving and maintaining the health and fitness of the increasingly longer-living human population, is considered one of the most important tasks and forms of public activity of the state and its institutions [17]. In developing such a policy, it would also be important to anticipate emergencies in which health and life risks escalate. Short- and medium-term health policy programmes rarely contain crisis elements as they arise unexpectedly and have a violent course. Such a situation was created by the occurrence of the COVID-19 pandemic. It disrupted the functioning of the health service as well as social and economic life. The outbreak of the COVID-19 pandemic forced national and local governments, national and international healthcare institutions to take ad hoc measures not provided for in health policy programmes. The need to implement crisis management was necessitated by changes in these programmes, which made it necessary to implement organisational changes, intensify activities and increase health care expenditure and costs.
Individual governments as well as international institutions and organisations were in charge of solving public health problems, sustaining economic activity and implementing anti-pandemic and anti-crisis measures. Member states of the European Union were necessarily involved in the activities undertaken by European agencies. The European Union was involved in coordinating some of the actions taken by the Member States and developing medium-term strategies to conduct fiscal policy and support overall economic and financial stability. To this end, the general pandemic exit clause of the Stability and Growth Pact was triggered, allowing member states to deviate from the budgetary rigours of normal times [18]. A multi-year financial framework and a programme for shaping the conditions for future generations were also formulated. As an ad hoc measure, the Recovery and Resilience Facility was launched, allowing member countries to get on the path to recovery. The European Commission’s action plan adopted in March 2020 provided the following directions [18,19,20]:
- ensuring the necessary supplies for the healthcare sector by preserving the integrity of the single European market as well as the supply chains, i.e. production and distribution;
- support for citizens and workers to prevent excessive losses of income and jobs;
- supporting businesses and ensuring that economic activity and financial balance are sustained by providing liquidity to the financial sector;
- enabling Member States to take strong and coordinated anti-pandemic and anti-crisis action through greater use of state aid instruments and the rules of the Stability and Growth Pact.
The adopted regulations allowed for joint negotiations and joint purchases of ventilators and other medical equipment as well as supplies and vaccines. During the pandemic, it was important to ensure access to equipment, techniques, medicines and materials important to defeating it throughout the community. Central to this was guaranteeing the movement of essential goods across land borders between countries and ensuring that international air transport could continue to operate and would not collapse. The relaxation of various EU regulations gave Member States greater discretion to make remedial decisions on the implementation of specific measures such as wage subsidies, the suspension of tax payments or the payment of social security contributions. States were also given the freedom to introduce direct financial support to both consumers and businesses. The introduction by the European Union of a €1 billion guarantee for the European Investment Fund to provide liquidity to small and medium-sized enterprises, to implement investment initiatives and to protect the labour market and employment was an important instrument [18]. Greater flexibility was introduced in the disbursement of cohesion policy resources from the Structural Funds. The European Union Solidarity Fund was also established, mainly to focus on activities targeting the COVID-19 pandemic [21].
The basis for health policy in Poland consists of the constitution, parliamentary laws and government regulations, as well as international obligations arising from Poland’s membership of the United Nations, the Council of Europe and the European Union [22]. The defining document of the country’s health policy before the COVID-19 pandemic was the National Health Programme 2021-2025. Health plans have been detailed by the Ministry of Health in the document entitled Healthy Future, which created a strategic framework for the development of the health system between 2021 and 2027 with an outlook until 2030. The plan detailed the healthcare measures of the Strategy for Responsible Development in force at the time, which was a document required by the European Union. The aim of these programmes was to extend life and improve the health of citizens. An important objective was to reduce social inequalities in access to health services and various forms of prevention. The programmes pay particular attention to obesity and addiction prevention, health promotion, improving care for the elderly and the mentally ill [23]. The outbreak of the coronavirus pandemic has led to a modification of these programmes by placing the emphasis on combating and preventing the pandemic and combating its effects. The National Recovery Plan approved by the European Commission in June 2022 envisaged an allocation of PLN 18.3 billion for the pillars on efficiency, accessibility and quality of the healthcare system, with an additional loan fund of PLN 1.23 billion [24]. Ongoing anti-pandemic management has been introduced in Poland under the Regulation of the Minister of Health of 27 February 2020 on SARS-CoV-2 coronavirus infection. This meant that such infections were covered by the provisions of the Act of 5 December 2008 on the Prevention and Control of Infections and Infectious Diseases in Humans (Journal of Laws 2008, No. 234, item 1570). On 2 March 2020, the Law on Special Arrangements for the Prevention, Prevention and Control of COVID-19, Other Communicable Diseases and the Emergencies Caused by Them was adopted (OJ 2020, item 374) [25]. This law regulates not only healthcare activities but also other areas of economic and social life that have been affected by the pandemic. Therefore, the law forms the basis for overall crisis management during a pandemic.
With the pandemic declared on 20 March 2020, a package of restrictions was introduced in Poland, limiting the freedom of citizens, businesses and institutions. The operation of large shopping centres, theatres, libraries, museums, casinos; sports, accommodation, tourist and leisure facilities, hostels and agrotourism farms was restricted or banned. Public gatherings and services offered by restaurants, bars, cafés and other catering establishments were banned entirely. Schools and colleges were also closed, and the operation of nurseries, kindergartens, children’s and youth clubs was suspended. On 24 March 2020, restrictions on travel and movement of citizens, the wearing of facemasks, limits on the gatherings in parks, temples and even private homes were introduced [26]. The restrictiveness of the policy introduced was initially high. In December 2020, using the Oxford Coronavirus Tracking Index [27], which includes 13 indicators relating to various restrictions, the level of restrictiveness of the anti-pandemic policy in Poland was rated at 75.48 points (out of a possible 100). However, the restrictiveness of the policy was gradually reduced as both policy makers and citizens gained experience. In February 2022, i.e. during another increase in the number of infections, the restrictiveness of the anti-pandemic policy dropped to 52.28 points, a level lower than in most central and eastern European countries [26].
The significant expansion and strengthening of hospital treatments was an important element of health policy and crisis management. Temporary hospital wards were opened in hotels, market halls and stadiums. Hospitals were provided with additional equipment including ventilators and various sanitary supplies. Efforts were also made to improve the working conditions for hospital staff. From the medical point of view, the primary way to counteract the spread of an epidemic is through antiviral vaccination. In December 2020, Poland’s National Vaccination Programme was adopted, envisaging control of the COVID-19 pandemic by the end of 2021 while maintaining the highest safety standards (Dz.U. 2020, item 2212). The programme provided for the purchase of 62 million vaccines in cooperation with the European Union at the cost of approximately PLN 2.4 million [26=8]. The vaccination of seniors and children over 12 years of age started in June 2021 while the vaccination of children aged 5-11 years and other population groups began at the end of the same year. Booster shots were allowed 6 months after the first dose. From April 2022, a further booster vaccination was made possible, first for seniors over 80 years of age and later for those over 60 years of age and for immunodeficient children over 12. In August 2022, booster vaccinations were given to healthcare workers. More than 56 223 000 people were vaccinated by 3 September 2022. More than 22.5 million people or more than 59% of the total population were fully vaccinated [29].
Most people who contracted coronavirus and were severely affected by it recovered after a few weeks. However, some people, even after a mild course of the disease, still had to deal with its negative effects for a long time, e.g. experiencing shortness of breath, coughing, heart and lung damage, chest and headaches, fatigue, muscle and joint pain, loss of smell and taste, accelerated heart rate, mental disorders and other ailments. Cases of permanent damage to internal organs were not uncommon [14]. Complications and long-term effects have been estimated to affect around 15% of those infected [30]. The negative effects of past illness have a negative impact on the ability to work and its effective performance, which adversely affects the economy and the effectiveness of management [19,31,32,33]. To prevent post-Covid complications that appeared during the pandemic and did not allow patients to return to full health for weeks or months, a post-pandemic rehabilitation programme was announced in April 2021. It was also complemented by the Prevention Plus programme targeting the over-40s, which was announced in July 2021 and ran until the end of 2021. These programmes compensated to some extent for the collapse in citizens’ access to medical facilities and ordinary medical procedures and preventive examinations during the pandemic, which may have contributed the deterioration of the population’s health.
4. Anti-Crisis Policy
With the outbreak of the pandemic, the situation for citizens, businesses and other organisations in Poland became precarious. Faced with the threat of illness and death, people lost their sense of security and there was trauma and anxiety about the future. The introduction of quarantine, restrictions on mobility and interpersonal contacts, interruptions to businesses, public institutions, all education and service establishments, as well as other restrictions and prohibitions created fears, tensions and psychological discomfort in families and social groups. All this reflected negatively on the economy. Restrictions on foreign trade, disrupted supply chains and local disruptions to supply systems have affected both consumption and production. Society faced the threat of unemployment, the economic collapse, loss of income and lack of access to essential services. Insecurity and the inability to meet basic needs gave rise to frustration, radicalisation of views and the possibility of violent social and political behaviour. The prevention of these unfavourable phenomena became the focus of state attention and remedial action in the form of an anti-crisis policy created and modified on an ongoing basis, which complemented the implemented health policy.
In the first phase of the fight against the pandemic, the government’s efforts focused on objectives that protected people’s health and lives. Nevertheless, decisions have also been taken since the beginning of the pandemic to prevent negative phenomena of an economic nature so as to prevent recession [1]. Such a threat was predicted after the outbreak of the pandemic not only in Poland but also in other EU Member States. Poland joined the programme of measures coordinated by the European Union to support the economic and financial stability of the Member States. Part of this was the activation of the general exit clause of the Stability and Growth Pact, which allowed member states to move away from the budgetary requirements in place at ordinary times [18]. In connection with the restrictions on economic activity applied to protect the population, packages of anti-crisis measures and instruments have also been introduced in various countries, which did not differ in terms of their objectives but rather in terms of their scope and means of implementation [34]. In addition to protecting people’s health and lives in the context of various social constraints and closing economies, the primary objectives focused around sustaining the operation of businesses and ensuring the basic financial and economic security of citizens [35].
A pandemic impacts all aspects of social and economic life, affecting different sectors and different forms of economic activity. The economics of a pandemic indicates that the impact of a pandemic on the economy is mainly via two channels of consumption limitation and production decrease [19]. A pandemic increases morbidity and reduces people’s mobility, resulting in reduced consumption and reduced consumer spending. In addition, supply is reduced as a result of the reduction in economic activity, employment and labour inputs while maintaining fixed costs, and the emergence of corporate indebtedness and the risk of bankruptcy. Disturbances in the labour market, the commodity market and, in particular, in the service market, lead to higher prices and lower budget revenues. In turn, the increased budget expenditure increases the budget deficit, disturbs the economic and budgetary balance and intensifies a trend for higher inflation [5].
From the moment of its outbreak, the COVID-19 pandemic radically changed the realities of social and economic life in Poland, disrupted everyday life and the entire economy. In particular, it impacted the service sectors such as healthcare, education, retail, transport, hospitality, catering, tourism, services to the public, cultural and sporting events, scientific conferences and symposia, religious ceremonies and family gatherings. The government recognised the risks and the need to counter and mitigate the spread of the coronavirus. Individual ministries were tasked with developing remedial programmes coordinated by the Prime Minister's Office. Anti-crisis programmes have been developed by the Ministry of Health, the Ministry of Development, the Ministry of Family, Labour and Social Policy, the Ministry of Finance, the Social Insurance Institution, the National Health Fund, the Polish Development Fund, as well as the Ministries of Internal Affairs and Administration, Education and Science, and other central agencies. These programmes began to be transformed into legal standards as early as March 2020, becoming the basis for crisis management [26]. The Parliamentary Act of 2 March 2020 on Special Solutions Related to the Prevention, Countering and Control of COVID-19, Other Infectious Diseases and Emergencies Caused by Them (OJ 2020, item 374) [25], and the Act of 31 March 2020 (OJ 2020, item 568) [36] amending and supplementing the former became the main basis for the anti-crisis measures. Those two laws were the basis for the formulation of measures included in the Crisis Shield, successively supplemented by legal acts of various ranks [37]. By the end of 2020, six such additions had been introduced with successive crisis shield numbers, and three more were adopted by mid-2021. Such supplements were being introduced almost until the end of the pandemic when the Financial Shield was added as a supplement to the Crisis Shield, which was then transformed into the Anti-Inflation Shield [32,38,39,40]. Selected elements included in the individual Shields during the first 13 months of the pandemic are included in Table 2.
Similar additions and modifications to anti-crisis instruments were applied, albeit less frequently, in the following months until 15 April 2023. Over time, the government began to shift its attention from anti-crisis measures to anti-inflationary measures. This was because public funds pumped into the economy during the pandemic while demand was limited became an inflation factor.
The anti-crisis shields covered a broad spectrum of issues forming ‘pillars of support’. Five basic pillars can be distinguished that made up the anti-crisis policy [32,38,39,40]:
- Protecting residents’ health;
- Protecting jobs and worker safety;
- Financial support for entrepreneurs;
- Strengthening the financial system;
- Public investment.
According to government estimates, PLN 312 billion was earmarked for the purposes identified in the anti-crisis shield and financial shield, which accounted for around 15% of annual GDP. Of this amount, PLN 7.5 billion was allocated to health care, PLN 30 billion to employee safety, PLN 30 billion to the public investment programme, PLN 70.3 billion to strengthen the financial system and PLN 74.2 billion to financially support businesses [20]. In addition to public health institutions, institutions that played an important role in the anti-crisis efforts were the National Bank of Poland, Bank Gospodarstwa Krajowego, Polish Development Fund, Social Insurance Institution, Ministry of Development, Labour and Technology, Industrial Development Agency and other central institutions. From the perspective of its financial structure, the Anti-Crisis Shield contained three main components [32]. The first one, amounting to approximately PLN 67 billion, was a cash package financed from the state budget, the Social Security Fund and special purpose funds. The second component, amounting to PLN 75.5 billion, focused on liquidity and provided for credit holidays and deferred benefits, loans and grants financed by a number of institutions such as the Polish Development Fund, Bank Gospodarstwa Krajowego, the Export Credit Insurance Corporation and the Agency for Enterprise Development. The third component also focused on liquidity; amounting to about PLN 70 billion, it ensured that loans were made available on convenient terms by the National Bank of Poland.
The main lines of the anti-crisis policy have already been formulated in the first Crisis Shield, implemented from 1 April 2020 [28,41]. It established the use of four instruments: wage subsidies, subsidies for business costs in the event of a pandemic-induced drop in turnover, loans to cover the ongoing business costs of micro-enterprises, and standstill benefits. The beneficiaries of these instruments, in addition to micro-enterprises, included natural persons with civil law contracts, persons carrying out non-agricultural business activity, the self-employed, as well as other entrepreneurs affected by the downtime, entrepreneurs with reduced working hours, as well as NGOs and legal entities within the meaning of the Public Finance Act. Wage support came from the Guaranteed Employment Benefit Fund. Standstill benefits available for up to three months were originally available to:
- people on civil law contracts whose income fell by 15% compared to the preceding month as a result of the restrictions caused by the pandemic;
- micro, small and medium-sized enterprises in order to subsidise the costs of employee wages and insurance premiums in the event of a turnover decrease by 30-80% in any two months. The prerequisite was to maintain employment and the aid could be disbursed for up to six months;
- the self-employed, in the event of a 30-80% drop in turnover caused by the pandemic.
The labour market, forms of employment, continuity, working time and conditions were the main socio-economic intervention area of the anti-crisis shield [31,32] these elements are linked to the social security system and the income level of the population. The programmes introduced by the successive anti-crisis shields were aimed at protecting jobs both in the form of employment and self-employment, which provided the basis for adequate labour income, social and economic security for those employed and was a condition for sustaining economic prosperity and economic growth and development. The regulations that the anti-crisis shields provided for the benefit of companies were also aimed at protecting the labour market but mainly used the possibilities contained in the Labour Code to make changes to the organisation and volume of work provided. This goal was attained, e.g. by way of employers reducing the amount of work provided by employees by 20 per cent or even to half-time, making the length of an employee's daily and weekly rest more flexible, and potential other terms and conditions of employment not provided for under the Labour Code [31].
Micro-entrepreneurs were offered micro-loans under the Anti-Crisis Shield 1.0 to cover current business costs and such loans were redeemable on condition that employment level remained unchanged for at least three months. Exemptions from the payment of insurance premiums for a period of three months were also widely applied. Exemptions from social security contributions generated no costs for entrepreneurs. Such exemptions were available to self-employed persons if the income from this activity did not exceed 300% of the projected gross monthly salary in the national economy. The suspension of insurance premiums during the pandemic did not limit the right to benefits and was counted as a contribution period in pension accounts. Other support included tax concessions and write-offs, including potential exemptions from taxes on property and gifts offered for the fight against coronavirus. Under Shield 1.0, subsidies of PLN 60.8 billion were paid out, 347,000 entrepreneurs were supported and 3.2 million employees were protected [42].
The Anti-Crisis Shield 2.0 expands the group of beneficiaries of wage subsidies to include NGOs and state legal entities. It revised the range of entities entitled to benefits, removed the maximum income criterion for downtime benefits and allowed the benefit to be used three times. The range of entrepreneurs to benefit from micro-loans and exemptions from social security contributions was expanded, and deferment of payment deadlines, the possibility of payment in instalments or cancellation have been allowed. The value of aid provided under Shield 2.0 was estimated at PLN 35 billion, benefiting entities in 45 industries [42].
Shield 3.0 has also expanded the group of those eligible for support. Financial assistance and insurance relief were also provided to entrepreneurs currently starting a business. Shield 4.0 retained the catalogue of forms of support and expanded the group of those eligible to use them, and simplified the procedures for processing applications and granting aid. Shield 5.0 was industry-specific and focused on companies in the tourism, events and exhibition industries, which were particularly affected by the lockdown. Successive waves of the pandemic necessitated the granting of additional downtime benefits and extended exemptions from paying insurance premiums. This was provided by Shield 6.0, which enabled micro- and small enterprises to obtain grants of up to PLN 5,000 and employee wage subsidies of up to PLN 2,000 for three months. The shield facilitated the hiring process and suspended the collection of the license fee in 2021 and the related compensation for municipalities. Shield 7.0 extended eligibility for anti-crisis benefits to social cooperatives, extending the provision of assistance to the 84 industries most affected by the pandemic. Shield 8.0 extended the possibility of providing support to further industries, such as rental, beauty and hairdressing services, passenger air transport and others. The new arrangements allowed for the deferral of rent payments for communal premises, property tax, ground rent, waiver of interest on tax arrears and others. Shield 9.0, which was introduced in April 2021, extended the possible period of continued assistance into the following months of that year [37].
The introduction of new instruments via successive anti-crisis shields had an important impact on supporting the labour market and households. Stronger social security was also achieved through instruments such as the Polish Tourist Voucher, an additional care allowance for parents of children up to the age of eight, and a solidarity allowance for people who lost their jobs following or during a pandemic.
5. Effects of the Anti-Crisis Policy
5.1. General Assessment
An analysis of the course of the pandemic and the successive anti-crisis shields makes it possible to see the adequacy of the implemented instruments to the course of the pandemic and the risks generated by it. As the epidemic progressed, economic restrictions and limitations on citizens’ freedoms were being introduced or lifted. The first lockdown was implemented in March/April 2020. It entailed a number of restrictions such as the ban on movement except in justified situations, the closure of educational establishments, shopping malls, hotels, sports facilities, cultural institutions, churches, some shops and even forests. However, some restrictions were gradually lifted at the end of April. In the autumn, some of them were reinstated. At that time, zones began to be introduced, with mandatory restrictions depending on the number of infections. At the end of the year, limits were introduced for Christmas and New Year’s meetings. The second lockdown was applied in March 2021 when the number of infections began to reach 30,000 cases per day. These restrictions were lifted from the end of May, at which point the possibility of in-person education was reinstated in schools. A mass vaccination campaign against coronavirus was launched at the same time. An overall assessment of the anti-crisis policy in Poland carried out in the form of anti-crisis shields, identifying its strengths and weaknesses, is presented in Table 3.
The effects of the COVID-19 pandemic control and countermeasure policy are spread across all areas of society and sectors of the economy. They manifest themselves in macroeconomic growth rates, budget revenues and expenditures, consumption, the labour market, the functioning of enterprises, households and public institutions, foreign exchange, the value of money and the prices of goods and services. A full assessment of the impact of the anti-crisis policies in place requires in-depth studies in various areas and sectors of the economy. In this work, we will only refer to selected issues related to security, economic and social activity, digitisation of services and macroeconomic impacts.
5.2. Health and Economic Security
The pandemic primarily threatened the health and lives of citizens, so the physical necessity of health security was the overriding objective of the state and its institutions. The COVID-19 pandemic also caused security risks in other areas where physical, social, economic, informational or emotional interactions were taking place. The aim of the anti-crisis policy was therefore to provide security in these areas [9]. Achieving these types of security became a key trust factor during the pandemic in Poland, especially in the process of service provision [10]. The nature of services changed during the COVID-19 pandemic and they took on a special significance. The importance of mutual trust between the provider and recipient of services has increased, ensuring security has become a key trust factor in service provision. The threat to safety and reduced trust in service providers entailed the need for innovative solutions, products, and service delivery mechanisms. The pandemic increased the demand for information delivered using digital technologies, and security requirements were changing the nature of services by reinforcing the separation feature (separation of the service provider from the consumption of the service). The need to improve security in the service sector by eliminating risks arising from interactions in the service delivery process and building trust has made services highly susceptible to innovations related to the use of information and digital technologies. The most spectacular use of such technologies during the pandemic was visible in educational, financial, health and administrative services. In these areas, as well as in other service and public service sectors such as commerce, culture and entertainment, and science, online means of communication, procurement, teaching and participation were widely used. Remote working became more widespread in all areas.
The provision of economic security was strengthened by two main trends: protecting entrepreneurs and businesses from bankruptcy and by protecting households and workers from an excessive decrease of income and consumption levels. With this in mind, the anti-crisis shield focused on the situation on the labour market: on one hand, ensuring the liquidity of companies, maintaining employment, reducing the tax and insurance burden through allowances, grants and subsidies and, on the other hand, ensuring the continuity and forms of employment, the level of wages and working conditions of employees as well as various forms of self-employment. In addition to economic instruments, various forms of social support for families were used to strengthen the socio-economic security.
5.3. Sustaining Economic and Social Activities
After the WHO declared the pandemic, Poland, like other countries, reacted to the dynamic increase in infections by introducing administrative restrictions necessary to maintain the sanitary regime, limiting business activities, direct interactions and mobility of the population, which disrupted the functioning of labour markets, educational institutions, public administration and the entire service sector. The effects of the pandemic on the labour market are multifaceted, manifesting themselves with varying strength in different sectors of the economy. The pandemic reduced the labour force participation rate and an increased the inactivity rate. In Q2 2020, the economically active population in Poland amounted to 16,801,000, i.e. 230,000 less than in Q2 2019. The labour force participation rate was 55.5% in Q2 2020, i.e. 0.7 pp lower than a year earlier. The number of economically inactive people increased by 217 000, i.e. 1.6%, at the same time [31]. The reduced number of economically active people was mainly due to a change in the number of those employed as the number of unemployed people has been relatively low, i.e. less than 4% since 2018. According to Eurostat [43], Poland was one of the countries with the lowest levels of unemployment in 2000, i.e. during the height of the pandemic. Between April and December 2020, the unemployment rate rose in Poland to 5.8–6.3 per cent. The reduction in the number of those employed was more related to an increase in the number of economically inactive people than to an increase in unemployment. Some of the employees in establishments that took advantage of the support offered by the shields were waiting to return to work once the administrative restrictions were lifted and the companies reinstated their operations. According to the estimates, 625,000 people, or 34.4 per cent of the total workforce, were temporarily out of work due to interruptions in the operation of workplaces in 2020 [31]. The inactivity increase was also due to the imposition of general protective restrictions, as well as the introduction of distance learning in schools. A significant proportion of parents with school-age children have had to stay at home to provide childcare. The pandemic also caused a widespread periodic reduction in job offers. In April 2020, the number of job offers in Poland decreased by 25% compared to April 2019. Restrictions and changes in the labour market had repercussions spreading throughout the economy and society. The production and consumption growth rates declined as a result, and there were changes in their forms and structure.
The pandemic contributed to the spread of remote working and working from home [8,39,40]. Before the pandemic, the share of remote working in Poland reached 4.6% in 2018, lower than the EU average of 5.2% [44]. In 2020, the share of remote working in Poland increased to 8.9%, while the EU average increased to 12.3%. Remote working has both advantages and disadvantages from the point of view of both employees and employers. The basic prerequisite for its use is that employees have access to the Internet and appropriate ICT equipment, as well as the skills necessary to use it, and a number of organisational issues have to be resolved on the employer’s side. The pandemic contributed to the legal regulation of remote working in the Labour Code in 2023 [44]. The development of remote working will have a significant impact on future structural changes in the labour market. Hybrid working will become more widespread. Evaluations of governmental anti-covid programmes show that subsidising jobs during stoppages or when working hours were reduced allowed businesses to reduce labour costs by as much as 60-75%, which was more beneficial than laying off workers during stoppages and then hiring them later, which requires re-training and induction into the workforce. The Ministry of Labour estimates that the anti-crisis shields saved around 6 million jobs during the pandemic [32]. According to estimates by the Central Statistical Office [42], employment in the first half of 2021 was higher than in the first half of 2020. Almost PLN 163 billion, more than half of the planned pandemic budget, was used for various forms of labour market support up to mid-2021. Almost 3 million employees benefited from the subsidisation of jobs by the Guaranteed Employment Benefit Fund, and 1.4 million benefited from the partial subsidisation of wage costs related to the payment of social security contributions. Research by the Polish Economic Institute [41] shows that 86% of entrepreneurs took advantage of the support offered under the anti-crisis shields. Almost 73% of the companies surveyed benefited from exemptions in the payment of social security contributions, 66% took advantage from reduced working hours or remote working and 65% used wage and social security contribution subsidies. More than half of the entrepreneurs used more than 10 instruments offered under the shields, some of them even multiple times. Entrepreneurs were most satisfied with exemptions from social security contributions.
5.4. Digitisation of Services
The pandemic has been instrumental in accelerating the widespread use of information (digital) technologies in commerce, finance, services, administration, as well as in other sectors of the economy and public services. Online shopping has become a common practice, especially for the younger generation. Online banking, payment of fees and tax obligations, remote education, customer service in offices and public institutions, booking of tickets and tourist and catering services, medical appointments, deliveries of food and other products are examples of the widespread use of digital technologies. The digitisation of services has reduced the pandemic-induced danger related to in-person interactions, and services have become particularly affected by the introduction of technologies that guarantee the distribution of services [10]. In particular, remote forms of communication and remote working, including distance learning, developed during the pandemic. Before, remote working in Poland was mainly practised by individual professionals, large companies and multinational corporations [8]. During the pandemic, remote employment or work from home became widespread, especially in education, communications and administration, mainly among managerial staff and programmers, accounting, finance, insurance and marketing, customer service and sales sectors [39,40].
After the outbreak of the pandemic, there was a surge in the number of employees working remotely or from home in all countries. In Poland, the rate reached 8.9 per cent in 2020 against the average of 12.3 per cent in the European Union countries. Research carried out by CEBOS in April 2020, i.e. shortly after the pandemic was declared, showed that half of those employed had not changed their form of employment, and one in four respondents worked reduced hours, 21% of those employed switched to remote working, while 9% of those previously employed stopped working due to the need for childcare or other similar reasons. Remote working was more frequent in large companies, and carried out mostly by university-educated people with IT qualifications. Work in this form was performed by approximately 55% of managers, 38% of employees in state and public institutions, 34% of administrative and office workers and 32% of self-employed workers [8]. A study by the Central Statistical Office (CSO) found that the percentage of people working remotely in Poland was 11% in Q1 2020, before falling to 5.8% in Q3 of that year and rising again to 14.2% in Q1 2021 [45]. Therefore, we can see that the scale of the use of remote working was strongly dependent on the current state of infection severity.
During the pandemic, remote working became an almost exclusive form of work for the entire education system and in the dissemination of knowledge, including scientific conferences. Hybrid training and conferences were also organised, with small groups of conference participants connecting with remotely dispersed speakers and presenters. The COVID-19 pandemic in Poland and the subsequent epidemiological emergency became the main reason for introducing relatively rapid changes in the way universities, as well as secondary schools, functioned. The purpose of these changes was to ensure the continuity, effectiveness and efficiency of education and the continuation of research by transferring most of it to a remote environment. Surveys on distance learning conducted among students, academics and managerial staff at universities have shown that e-learning is perceived differently by these groups of learners, who also point out the main issues to be addressed in distance learning. For example, students considered an excessive number of hours spent in front of a computer daily and the lack of in-person contact with mates from the same group/year are important areas in need of improvement, while lecturers saw the main problems of distance learning in the lack of direct contact with students while teaching, as well as in many hours spent in in front of a computer during the day [46].
An important factor in the spread of remote working and learning has been the availability of the Internet and remote communication devices. Poland has seen a rapid increase in the number of households with Internet access between 2010 and 2020: from 67% to 90%. In this respect, Poland is not far behind the average of the European Union Member States. Remote working and remote teaching widely used during the pandemic were phased out once the pandemic subsided. Indeed, these forms of activity entail both positive and negative consequences for employees, employers and participants in educational processes. Such consequences often result from challenges related to work organisation and lack of equipment necessary for remote activities, as well as challenges related to a lack of knowledge and experience in performing remote activities. The pandemic has highlighted the need for workplaces and institutions to be better equipped with ICT infrastructure and for regulations to be adapted to apply the new business model, protecting employer resources, employee interests and the rights of customers and participants in the processes of producing goods and services. The pandemic has contributed significantly to improving the provision of telecommunications equipment to households, businesses and institutions and has necessitated the acceleration of public education in the use of electronic devices. This should be considered a positive social effect of the pandemic.
5.5. Macroeconomic Impact of the Pandemic
In addition to the effects that are ad hoc and observable in short periods of time, the COVID-19 Pandemic affects the economy and society in the medium and longer term, and its effects may be observable in various macroeconomic indicators. Forecasts of Poland’s economic growth were optimistic before the pandemic. The forecast made by the National Bank of Poland in November 2019 foresaw GDP growth of 3.6% in 2020 and 3.3% in 2021 [26]. A revision of these forecasts by the Polish Economic Institute after the outbreak of the pandemic predicted not an increase but a decrease in GDP by up to 7.1% [41]. However, despite difficulties and periodic growth slumps, the Polish economy has been relatively resilient to the crisis. When comparing growth on a quarterly basis, we see that GDP in the fourth quarter of 2021 reached PLN 754 billion, which was significantly higher than in the third quarter of 2019 when that figure amounted to PLN 640 billion (Figure 1).
Source: Author’s own compilation based on Statistics Poland www.stat.gov.pl/produkt krajowy brutto.
Poland’s per capita GDP measured in purchasing power parities equalled 73% of the EU average in 2019, rising to 76% in 2020 and to 77% in 2021. At the time, this placed Poland 22nd among the 27 Community member states [43]. Economic growth maintained in Poland during the pandemic resulted mainly from an increase in domestic demand for investments. The pandemic, especially in its initial phase, resulted in a significant drop in retail sales and a significant slowdown in consumption growth (Figure 2).
Gross Domestic Product measured on a quarterly basis between 2018 and 2021 fluctuated periodically with a clear upward trend, and labour income increased too. The outbreak of the pandemic brought a slight decrease in average monthly wages in the business sector during the first three quarters of 2020 but this was followed by a steady increase in wages.
Poland belonged to a small group of countries where the pandemic did not have a lasting negative impact on GDP and income levels of the population. The effect of the anti-crisis shields introduced has also been to keep unemployment low. At the end of 2020, unemployment reached 6.3% and fell to 5.4% during 2021 [48]. The 2020 slowdown was much shallower than in most EU Member States. However, the implementation of the anti-crisis policies, especially the cash transfers to businesses and households, resulted in a significant increase in public debt from around 46% of GDP before the pandemic to 56% during and to 59% at the end of the pandemic [47]. Expenditure made in order to overcome the crisis was becoming a significant factor in the rise in inflation. However, an increase in public debt as a result of anti-crisis policies has to be considered less costly to the economy and society than the likely collapse of companies and the potential increase in unemployment in the absence of such policies.
The anti-crisis policy was linked to the growing problem of inflation. The pre-pandemic consumer price index remained low at 102.1 in 2019 compared to the preceding year. It rose to 103.7 in 2020 and to 105.2 in 2021. In December 2021, the inflation rate rose to 8.6% [49]. Rising inflation rates started to exceed the inflation target set by the Monetary Policy Council. The significant influx of funds into the market caused by the launch of the Crisis Shield and the rapid process of moving away from the anti-pandemic restrictions introduced earlier were the main reasons for inflation. There was a large increase in prices of fuel and other raw materials as well as food. The external cause of this increase was the outbreak of the Russo-Ukrainian war. The increase in public debt and the cost of servicing it inhibited the propensity to invest in fixed assets and strengthened the orientation towards saving.
The pandemic has undoubtedly had an impact, especially in the initial period, on the deterioration of sentiments of producers and consumers, and on the general social climate. By the end of 2021, this sentiment has improved. Nevertheless, entrepreneurs pointed to rising production costs and labour shortages, as well as uncertainty about longer-term prospects [48]. Consumers, in turn, expressed more pessimistic opinions about the future. Consumer sentiment only improved after the pandemic subsided in 2023.
6. Conclusions
As a phenomenon that spread rapidly worldwide at the beginning of 2020, the COVID-19 pandemic caused threats to the health and lives of citizens in Poland and profound disruptions to economic and social, cultural and political life. The state swiftly responded to the rapidly disclosed health risks to the nation, and the response had two main aspects in the form of anti-pandemic and anti-crisis policies. The former was to protect the health and lives of citizens, i.e. to ensure health security for the population, through the introduction of restrictions against the spread of epidemics and the decisive organisational, infrastructural, material and personnel strengthening of the healthcare service, especially in terms of hospital treatment. The challenge was in the rapidity and unpredictability of the infections, and the shortcomings of the healthcare infrastructure. The latter policy was aimed at responding quickly and preventing emerging difficulties in the economic, social and financial sectors. The actions taken in this area were constantly being expanded and revised, with the intention to create a strategy to protect economic security and shield the country from a deep economic crisis. All state institutions, economic sectors, enterprises, non-governmental institutions, as well as households and citizens participated in the implementation of health and anti-crisis policies.
The two policies, i.e. the anti-pandemic policy and the anti-crisis policy were conducted in a coordinated manner during the pandemic in Poland, and the applied administrative, legal and economic instruments supported the objectives of both policies. However, the anti-pandemic policy failed to protect the country from adverse effects in terms of health and demographics, while the anti-crisis policy, despite the hampering of growth rates, disruptions in the labour market, a clearly visible crisis in certain sectors and service industries, as well as the general downturn and tensions in the financial sphere, made it possible to protect society and the economy from a deep economic recession. Despite restrictions on mobility and activity, anti-crisis shields have helped businesses to survive and mitigate the effects of the crisis and helped workers to protect themselves from excessive falls in income and consumption levels. Compared to other EU countries, the macroeconomic indicators at the end of the pandemic were favourable in Poland. It is recognised that this is the result of an effective state response to the pandemic and the channelling of significant forces and resources to overcome it.
The COVID-19 pandemic reached Poland in March 2020. Like many other countries, Poland did not have a previously developed anti-pandemic strategy, hence the measures taken were ongoing responses to emerging threats. They were primarily designed to protect the life and health of the population, and were followed by protective measures to strengthen industries at risk. Fluctuation was a characteristic feature of the course of the pandemic, expressed as successive increases and decreases in infections and deaths. The health regulations introduced were implemented in accordance with WHO recommendations and in cooperation with the European Union. Such cooperation mainly had to do with the placement and execution of equipment, material and vaccine orders. In this respect, the possibility of deviating from the various formal procedures was used, which, after the threats had subsided, became the basis for political disputes. Health policy had a strong impact on the functioning of society and the economy, and has also become the basis for conflicts in the political sphere (e.g. the possibility of organising elections and their execution). Despite the efficient handling of the pandemic, death rates were quite high compared to other countries. Reasons for this included infrastructural, staffing and organisational constraints as well as late vaccination and varying uptake across regions and social groups. The pandemic combined with unfavourable demographic developments has caused significant loss of life and reduced the level of health of the population, as well as upset the economic processes and influenced changes in the behaviour of businesses, as well as revealed new forms of functioning of the economy.
State measures designed to avoid economic recession in Poland were undertaken partly in agreement and cooperation with the European Union. Poland has joined EU programmes designed to preserve economic and financial stability, shaping and expanding the impact by its own means to various forms of activity and sectors of the economy. The pandemic has caused a decline in business activity, a consumption and production drop, threatened to bring down small and medium-sized enterprises, especially in the services sector, affected the way businesses, the labour market and other markets operated, increased production costs and caused loss of income from work. Regulation of the economy has taken the form of an Anti-Crisis Shield, which was updated and supplemented as problems arose. nine anti-crisis shields were designed and implemented between March 2020 and April 2021. Later, the previously implemented instruments were used until the Anti-Crisis Shield started to target inflation in spring 2023. The anti-crisis shields covered a broad spectrum of issues forming the ‘pillars of growth’ that, in addition to health security, covered four areas supporting businesses against collapse, protecting jobs and workers’ incomes, continuing public investment and the stability of the financial system.
Mass adverse events occurring rapidly and difficult to control, triggered by nature or the superimposition of multiple adverse anthropogenic factors, occurring irregularly at medium and longer intervals, cause social and economic crises and are often the cause of economic recessions. To fighting and counter such threats, and to overcome such crises, extraordinary actions and measures are required along with the dedication of all socio-economic actors, the efficient action of the state and its bodies, and the mobilisation and cooperation of society as a whole. Achieving success against the COVID-19 pandemic and preventing economic recession requires the rapid, immediate implementation of measures to create a barrier to the spread of the disease (the root cause of the emergency) as well as various protective and stimulatory measures in the economy in the form of anti-crisis policies. These two areas of activity should be coordinated, framed by a rational organisational plan, resourced with extraordinary resources and managed efficiently. States on which the main part of the anti-crisis action depends are usually not prepared for the occurrence of emergencies and crises in their various forms. Such actions can be more easily carried out by affluent states that are able to gather adequate forces and resources in a short period of time. For less affluent countries, it may be easier to prevent and deal with crises by developing a medium-term strategy for how the country will operate in the event of an emergency and having an efficient system for capturing the symptoms of a potential crisis. This requires the installation of a crisis-oriented early warning system. The crisis strategy should indicate of the size and location of reserves and necessary resources and a framework for dealing with emergencies.
In addition to its negative effects, the pandemic has also had positive effects, having contributed to the introduction of a number of technical, organisational and marketing innovations using digital technologies, especially in the administration and services related to health, education, catering, retail, tourism and other areas. It can also be concluded that the coordinated action of the Polish state in implementing health and anti-crisis policies has had a positive effect, has made it possible to limit the spread of the disease and emerge from the pandemic in a relatively short period of time, and has prevented the occurrence of a deep economic recession. This assessment of the impact of the COVID-19 pandemic in Poland and the anti-crisis policies that have been in place for almost three years is neither complete nor exhaustive. There is a need for further research into its long-term effects. There also needs to be an assessment of the feasibility of pre-emptive anti-crisis strategies and the introduction of an early warning system for emergencies.
Funding
This research was funded by John Paul II University in Biała Podlaska, Poland.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Kacperska, E.; Gomółka, P.; Łukasiewicz, K.; Wróblewski, J. Państwo i jego rola w gospodarce. In Gospodarka w dobie pandemii COVID-19. Wybrane zagadnienia. Oficyna Wydawnicza ASPR: Wraszawa, Poland, 2023.
- Militz, M. (ed.). Wsparcie udzielone przedsiębiorstwom w związku z pandemią COVID-19. Rozliczenia i kontrola. Wolters Kluwer, 2021.
- Otwinowski, W. Kryzys i sytuacja kryzysowa. Przegląd Naukowo-Metodyczny. Edukacja dla Bezpieczeństwa 2010, 2, 83–89. [Google Scholar]
- Adamowicz, M.; Adamowicz, T. The World Financial Crisis and The Polish Economy. Zeszyty Naukowe SGGW W Warszawie – Problemy Rolnictwa Światowego 2019, 19, 5–21. [Google Scholar] [CrossRef]
- Adamowicz, M. Policies aiming at combating COVID-19 pandemic and economic crisis in Poland/Polityka antypandemiczna i polityka antykryzysowa w czasie pandemii COVID-19 w Polsce. Economic and Regional Studies 2023, 16, 538–566. [Google Scholar]
- Dergiades, T.; Milas, C.; Mossialos, E.; Panagiotidis, T. COVID-19 anti-contagion policies and economic support measures in the USA. Oxford Economic Papers 2023, 75, 613–630. [Google Scholar] [CrossRef]
- Giuliani, M. Complying with Anti-COVID Policies Subnational Variations and their Correlates. Rivista Italiana di Politiche Pubbliche. Rivista quadrimestrale 2022, 2, 241–267. [Google Scholar] [CrossRef] [PubMed]
- Radziukiewicz, M. Remote work in Poland and perspectives. Economic and Regional Studies / Studia Ekonomiczne i Regionalne 2021, 14, 409–427. [Google Scholar] [CrossRef]
- Berry, L.L.; Danaher, T.S.; Askoy, L.; Keiningham, T.L. Service Safety in the pandemic age. Journal of Service Research 2020, 23, 391. [Google Scholar] [CrossRef]
- Kamiński, J. Cyfryzacja usług jako efekt pandemii. In Rozwój e-gospodarki wobec wyzwań pandemii COVID-19; Siedlecka, A., Guzal-Dec, D., Żurakowska-Sawa, J., Eds.; Wydawnictwo AB: Biała Podlaska, Poland, 2023. [Google Scholar]
- Zbucki, Ł. Wpływ pandemii koronawirusa SARS-CoV-2 na ruch turystyczny w polskich parkach narodowych. Wydawnictwo AB: Biała Podlaska, Poland, 2023.
- WHO. Coronavirus Disease 2019 (COVID-19). Situation Report 2020, 82. [Google Scholar]
- http://koronawirus.pl.
- Janiszewska, A.; Klima, E. Wybrane aspekty demograficzne pandemii COVID-19 w polskich regionach a reaktywne działania polityki zdrowotnej. Rozwój Regionalny i Polityka Regionalna 2023, 14, 123–147. [Google Scholar] [CrossRef]
- Basiukiewicz, P. Ani jednej łzy. Ochrona zdrowia w pandemii. Warsaw Enterprise Institute: Warsaw, Poland, 2021.
- Wójcicki, W. Crisis Aspects of the COVID-19 Pandemic in the Social Sphere and Secondarily in the Economic One. Economic and Regional Studies/ Studia Ekonomiczne i Regionalne 2023, 15, 74-89. [CrossRef]
- Włodarczyk, C. Wprowadzenie do polityki zdrowotnej. Warszawa: Wolters Kluwer Polska, Poland, 2010.
- Rosiek, J. Antypandemiczna polityka gospodarcza Unii Europejskiej w aspekcie możliwości ograniczenia negatywnych skutków pandemii COVID-19. Horyzonty Polityki 2021, 12, 156–176. [Google Scholar]
- Sieroń, A. Czy pandemia COVID-129 spowoduje zapaść globalnej gospodarki? Available online: https://mises.pl/artykul/sieron-czy-pandemia-covid-19-spowoduje-zapasc-globalnej-gospodarki (accessed on 2 April 2021).
- Sienkiewicz, I. Wpływ pandemii COVID-19 na gospodarki wybranych krajów Unii Europejskiej. The Review of European Affairs, PESCA 2021, 5, 43–59. [Google Scholar] [CrossRef]
- Komisja Europejska. Europejska Unia Zdrowotna. Available online: https://eur-lex.europa.eu/en/legal-content/.
- Jarosz-Żukowska, S. Prawo do ochrony zdrowia i dostępu do świadczeń opieki zdrowotnej. In Realizacja i ochrona konstytucyjnych wolności i praw jednostki w polskim porządku prawnym, Jabłoński, M. (ed.); Uniwersytet Wrocławski, E-wydawnictwo: Wrocław, Poland, 214, 659-707.
- NPZ. Narodowy Program Zdrowia na lata 2022-2025, Ministerstwo Zdrowia: Warszawa, Poland, 2021.
- KPO. Krajowy Plan Odbudowy. Urząd Rady Ministrów: Warszawa, Poland, 2022.
- Ustawa z dnia 2 marca 2020, r. o szczególnych rozwiązaniach związanych z zapobieganiem, przeciwdziałaniem i zwalczaniem COVID-19, innych chorób zakaźnych oraz wywołanych nimi sytuacji kryzysowych (Dz.U. 2020 poz.374).
- Staniszewski, R.M. Gospodarka Polska w czasie pandemii COVID-19: spowolnienie czy regres? Studia Politologiczne 2022, 65, 58–86. [Google Scholar] [CrossRef]
- OxCGRT. The Oxford Covid-19 Government Response Tracker. Available online: https://www.bsg.ox.ac.uk/research/research project/covid-19-government-response-tracker.
- KPMG. Poland – Measures in response to COVID-19 – KPMG Global. Available online: https://kpmg.com/xx/en/home/insights/poland-government.
- www.gov.pl.
- Fiłon, J.; Łukaszuk, R.C. Epidemie i pandemie w kontekście epidemiologicznym. In Życie w cieniu pandemii. Aspekty medyczne, estetyczne, społeczne, Krajewska-Kułak, E., Łukaszuk, C., Fiłon, J., Guzowski A. (eds.); Wydawnictwo Naukowe SILVA RERUM: Poznań, Poland, 2020; pp. 39–50. [Google Scholar]
- Radlińska, K.M. Pandemia COVID-19, Implikacje dla polskiego rynku pracy. Zeszyty Naukowe Wydziału Nauk Ekonomicznych 2020, 24, 113–126. [Google Scholar]
- Uścińska, G. Rozwiązania ukierunkowane na przeciwdziałanie skutkom pandemii COVID-19 w zakresie bezpieczeństwa socjalnego obywateli w wybranych programach rządowych. Zabezpieczenie Społeczne, Teoria, Prawo, Praktyka 2021, 13, 9–17. [Google Scholar]
- Dymecka, J. Psychospołeczne skutki pandemii COVID-19. Neuropsychiatria i Neuropsychologia/Neuropsychiatry and Neuropsychology 2022, 16, 1–10. [Google Scholar] [CrossRef]
- Drewniowska, K. Ograniczenie prowadzenia działalności w czasie pandemii COVID-19. Zeszyt Prawniczy UAM 2021, 11, 75–87. [Google Scholar] [CrossRef]
- Czech, K.; Karpio, A.; Wielechowski, T.; Żebrowska-Suchodolska D. Polska gospodarka w początkowym okresie pandemii COVID-19. Wydawnictw SGGW: Warszawa, Poland, 2020, 29-32.
- Ustawa z dnia 31 marca 2020 r. o zmianie ustawy z 2 marca 2020 r. (Dz.U. 2020 poz.568).
- Tarcza Antykryzysowa. Available online: https://www.gov.pl/web/rozwój/tarczaantykryzysowa (accessed on 29 September 2023).
- Kubiczek, J.; Derej, W. Tarcze antykryzysowe jako źródło wsparcia działalności MŚP w dobie pandemii COVID-19. Przegląd Prawno-Ekonomiczny 2022, 1, 33–58. [Google Scholar] [CrossRef]
- Adamowicz, M. Czynniki przemian rynku pracy w Polsce w latach 1989-2021. In Rynek pracy wobec wyzwań przyszłości – ewolucja i współczesne uwarunkowania; Siedlecka, A., Guzal-Dec, D. (eds). Wydawnictwo AB: Biała Podlaska, Poland, 2022; pp. 113–147. [Google Scholar]
- Adamowicz, M. COVID-19 pandemic as a change factor in the labour market in Poland. Sustainability 2022, 14, 9107. [Google Scholar] [CrossRef]
- PIE. Polish Economic Institute. Tarcza antykryzysowa. Koło ratunkowe dla firm i gospodarki. Polish Economic Institute, 2021.
- Tarcza Finansowa PFR. Available online: https://pfrsa.tarcza-finansowa-pfr-html (accessed on 25 July 2021).
- Eurostat. European Statistical Recovery Dashboard, Annual inflation rate. Available online: https://ec.europa.eu/eurostat/cache/recovery-dashboard.
- Chamera, K. Wyzwania pracy zdalnej w obliczu COVID-19. In Rozwój e-gospodarki wobec wyzwań pandemii COVID-19; Siedlecka, A., Guzal-Dec, D., Żurakowska-Sawa, J., Eds.; Wydawnictwo AB: Biała Podlaska, Poland, 2023. [Google Scholar]
- GUS. Wpływ epidemii COVID-19 na wybrane elementy rynku pracy w Polsce w I, II, III, i IV kwartale 2020 r. i w I kwartale 2021 r. GUS: Warszawa, Poland, 2021.
- Detyna, B. E-learning i praca zdalna w szkołach wyższych – doświadczenia i wyzwania w kontekście pandemii COVID-19 oraz zagrożenia epidemicznego. In Rozwój e-gospodarki wobec wyzwań pandemii COVID-19; Siedlecka, A., Guzal-Dec, D., Żurakowska-Sawa, J., Eds.; Wydawnictwo AB: Biała Podlaska, Poland, 2023. [Google Scholar]
- GUS. Kwartalne i roczne wskaźniki makroekonomiczne, część I i II. GUS: Warszawa, Poland, 2022.
- GUS. Wpływ pandemii COVID-19 na koniunkturę gospodarczą – oceny i oczekiwania. GUS: Warszawa, Poland, 2021.
- GUS. Wskaźnik cen towarów i usług w grudniu 2021 r. GUS: Warszawa, Poland, 2022.
Figure 1.
Gross domestic product, 2018-2021 (in billion PLN).
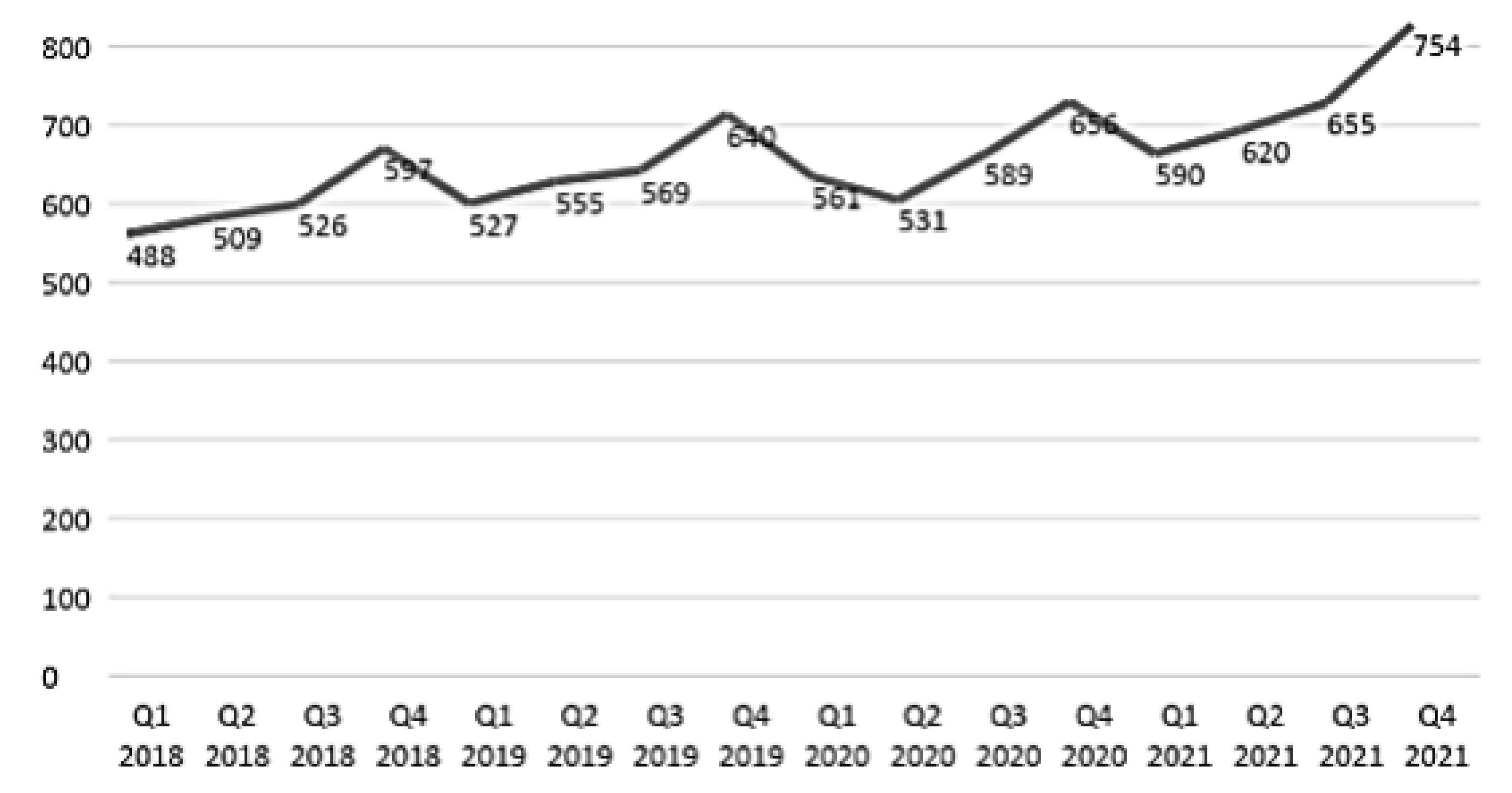
Figure 2.
Average monthly gross nominal salary in the business sector in 2018-2021, in PLN. Source: Author’s own compilation based on Statistics Poland data – quarterly macroeconomic indicators, part II [47].
Figure 2.
Average monthly gross nominal salary in the business sector in 2018-2021, in PLN. Source: Author’s own compilation based on Statistics Poland data – quarterly macroeconomic indicators, part II [47].
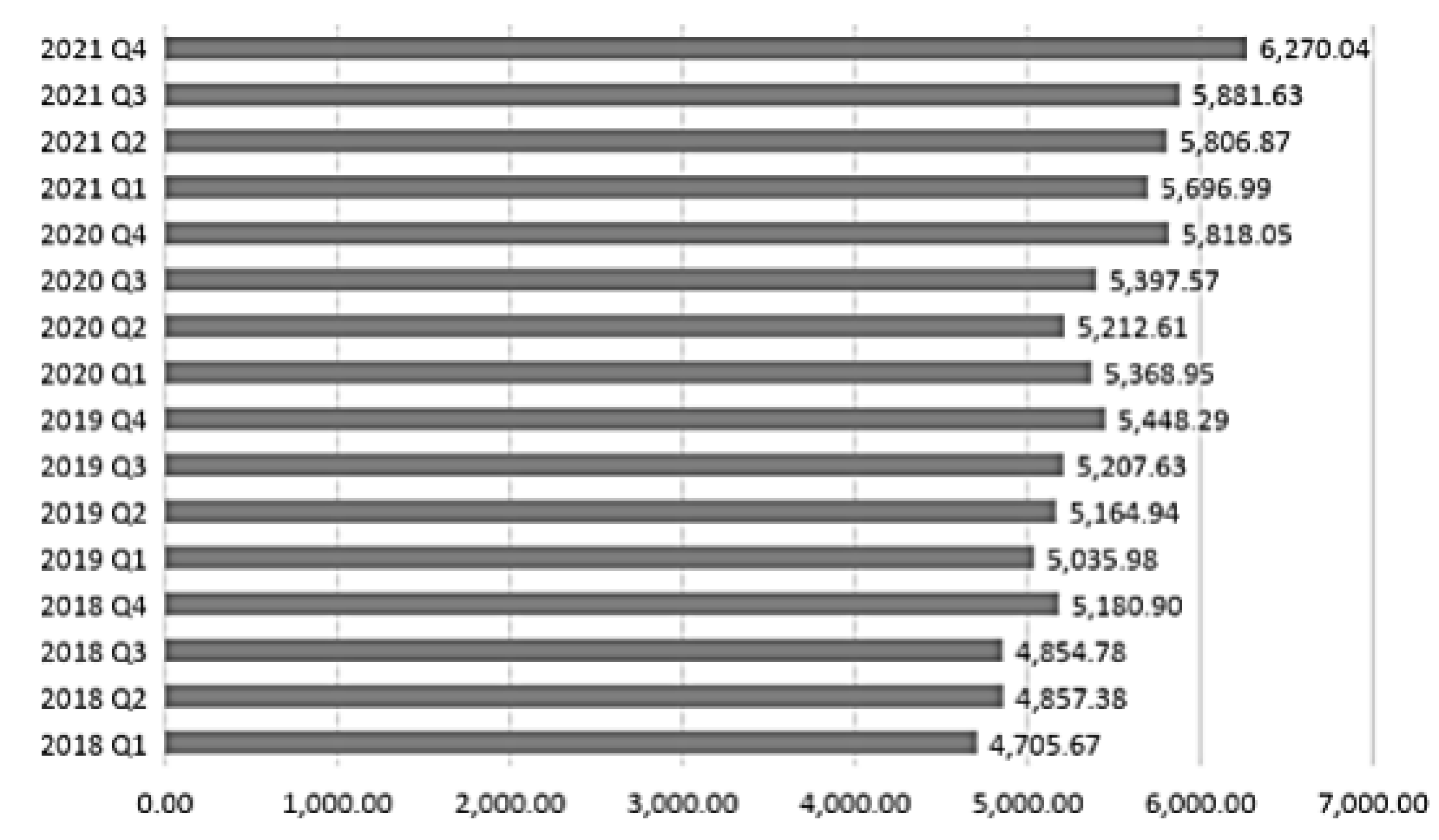

Table 1.
The course of the 2020-2023 COVID-19 pandemic in Poland. Figures as of the last day of a given month.
Table 1.
The course of the 2020-2023 COVID-19 pandemic in Poland. Figures as of the last day of a given month.
| Month - Year Hospitalisation | Infections | Deaths | |
|---|---|---|---|
| New | Total | Total | |
| March – 2020 | 256 | 2311 | 33 |
| April – 2020 | 300 | 12/87 | 64 |
| May – 2020 | 215 | 25,786 | 1,064 |
| June – 2020 | 239 | 34,393 | 1,463 |
| July – 2020 | 657 | 45,688 | 1716 |
| August - 2020 | 502 | 67,372 | 2,039 |
| September - 2020 | 1,552 | 91,514 | 2,513 |
| October - 2020 | 21,897 | 362,731 | 5,631 |
| November - 2020 | 5,733 | 990,811 | 17,150 |
| December - 2020 | 13,397 | 1,294,878 | 28,554 |
| January - 2021 | 4,706 | 1,513,385 | 37,180 |
| February - 2021 | 10,099 | 1,706,986 | 43,769 |
| March - 2021 | 32,874 | 2,321,719 | 53,045 |
| April – 2021 | 6,796 | 2,792,142 | 67,502 |
| May – 2021 | 333 | 2,872,283 | 73,745 |
| June – 2021 | 104 | 2,879,912 | 75,021 |
| July – 2021 | 153 | 2882939 | 75,261 |
| August - 2021 | 285 | 2,888,670 | 75,345 |
| September - 2021 | 1,208 | 2,907,071 | 75,650 |
| October - 2021 | 7,145 | 3,025 247 | 76,989 |
| November - 2021 | 19,074 | 3,540,065 | 83,583 |
| December - 2021 | 13,601 | 4,108,215 | 97,054 |
| January - 2022 | 33,480 | 4,886,154 | 105,194 |
| February - 2022 | 6,564 | 5,667,054 | 111,317 |
| March - 2022 | 4,997 | 5,962,931 | 115,193 |
| April – 2022 | 842 | 5,996,514 | 116,059 |
| May – 2022 | 346 | 6007584 | 116,318 |
| June – 2022 | 589 | 6,014,992 | 116,424 |
| July – 2022 | 651 | 6,069,665 | 116,570 |
| August - 2022 | 3,840 | 6,176,885 | 117,083 |
| September - 2022 | 3,890 | 6,293,558 | 117,569 |
| October - 2022 | 150 | 6,340,435 | 118,124 |
| November - 2022 | 584 | 6,352,755 | 118,319 |
| December - 2022 | 623 | 6,368,479 | 118,533 |
| January - 2023 | 989 | 6,379,391 | 118,727 |
| February - 2023 | 3,772 | 6,419,480 | 118,884 |
| March - 2023 | 1,461 | 6,496,176 | 119,346 |
| April – 2023 | 45 | 6,513,849 | 119,555 |
| May – 2023 | 62 | 6,516,915 | 119,610 |
Source: Ministry of Health and Statistics Poland. Statistics concerning the COVID-19 pandemic in Poland from 2020 to 2023.
Table 2.
Selected programmes and aid instruments introduced in the subsequent Crisis Shields.
| Name of the Programme and Date of Introduction | Beneficiaries | Type and Nature of Aid |
|---|---|---|
| Crisis Shield 1.0 Law of 14.05.2020 |
entrepreneur, NGO, legal person | Subsidies for employee wages who were furloughed or had their working hours reduced |
| Crisis Shield 2.0 Law of 14.05.2020 |
entrepreneur, NGO, legal person | Social security contributions exemptions, wage subsidies, cost subsidies, loans, furlough benefit |
| Crisis Shield 3.0 Law of 14.05.2020 |
As above | Extension of social security contribution exemption, furlough benefits, Labour Office loans |
| Crisis Shield 4.0 Law of 14.05.2020 |
entrepreneurs meeting the relevant conditions | Wage subsidies for employees not impacted by furloughs or shorter working hours |
| Crisis Shield 5.0 Law of 14.05.2020 |
Entrepreneurs with relevant business registration codes | Furlough benefits for agents, tour pilots and guides Additional benefits for non-agricultural busi- nesses operating in selected industries |
| Crisis Shield 6.0 Law of 14.05.2020 |
Entrepreneurs with relevant business registration codes | One-time additional benefit for non-agricultural businesses |
| Crisis Shield 7.0 Law of 14.05.2020 |
Any entrepreneur meeting the relevant conditions | Wage subsidies, cost subsidy, Social Security contribution exemptions |
| Crisis Shield 8.0 Law of 14.05.2020 |
Small and micro-enterprises | Social Security contributions exemptions, fur- lough benefits, Labour Office subsidies, wage subsidies |
| Crisis Shield 9.0 Law of 14.05.2020 |
Any entrepreneur meeting the relevant conditions Small and micro-enterprises Entrepreneurs with relevant business registration codes Entrepreneurs with relevant business registration codes meeting the conditions |
Wage subsidies for specific sectors according to main type of business operations Subsidies covering ongoing operating costs Furlough benefits for businesses in selected industries Social Security contribution exemptions |
1 Author’s own compilation based on https://www.gov.pl/web/rozwój/tarcza antykryzysowa.
Table 3.
This is a table. Tables should be placed in the main text near to the first time they are cited.
Table 3.
This is a table. Tables should be placed in the main text near to the first time they are cited.
| Strengths | Weaknesses |
|---|---|
| Adequate goals, i.e. ensuring liquidity and stabilisation of vulnerable sectors of the economy | Potential for public debt increase |
| An adequate implementation process taking into account the course of the pandemic | Reallocation of funds in the state budget at the expense of other areas |
| Consideration of the industries that were most affected by the restrictions | A complex process of applying for assistance under the various instruments |
| A wide and continuously updated range of aid instruments on offer | Limitations on the proper evaluation of the effectiveness of the instruments used |
1 Source: Own work using: Kubiczek, Derej, 2022 [38].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



