
Submitted:
06 June 2024
Posted:
07 June 2024
You are already at the latest version
Abstract
Background: Population studies have shown that prehypertension is associated with adverse cardiometabolic risk profile even among apparently healthy populations. Although associations between serum triglyceride (TG) concentrations and the risk of atherosclerotic cardiovascular disease have been reported, there are lack of data on the association of hypertriglyceridemia with cardiovascular risk (CVR) in a low risk prehypertensive population. Aim: Our aim was to analyze the cardiorenometabolic characteristics of prehypertensives (PHT) compared to normotensives (NT) and untreated hypertensives (HT) and its associations with CVR. Materials and methods: In our cross-sectional study we included 323 apparently healthy untreated subjects 18-45 years who underwent basic anthropometric and standardized blood pressure measurement, fasting blood sampling, spot urine collection and transthoracic echocardiogram. Results: Higher BMI, waist circumference, HOMA-IR, LDL-cholesterol, TG, uric acid and LVMI contribute to higher CVR in PHT compared to true NT (p
Keywords:
prehypertension
; hypertriglyceridemia
; uromodulin
; cardiovascular risk
Introduction:
Many studies found correlations between prehypertension and a higher risk of the future development of hypertension, cardiovascular diseases, and mortality, even before prehypertension was introduced as a new blood pressure category in the JNC-7 guidelines [1,2,3,4]. In Framingham Heart Study follow-up participants, compared to optimal blood pressure, high–normal blood pressure was associated with a cardiovascular disease risk-factor-adjusted hazard ratio of 2.5 (95 percent confidence interval, 1.6 to 4.1) in women and 1.6 (95 percent confidence interval, 1.1 to 2.2) in men who were initially free of hypertension and/or cardiovascular disease [2]. A meta-analysis on about one million subjects showed a linear increase in the risk of mortality due to ischemic heart disease and stroke in people between the ages of 40 and 89, starting from a blood pressure (BP) above 115/75 mmHg and doubling with each systolic and diastolic BP (SBP and DBP, respectively) increase of 20 mmHg and 10 mmHg, respectively [3]. However, the BP range defined as prehypertension in the JNC-7 guidelines was classified as normal (120–129/80–84 mmHg) and high–normal (130–139/85–89 mmHg) BP in the European Society of Cardiology and the European Society of Hypertension and (ESC/ESH) 2007 and subsequent ESC/ESH guidelines, while the American College of Cardiology/American Heart Association (ACC/AHA) 2017 guidelines consider an SBP or DBP within 130–139 mmHg or 80–89 mmHg, respectively, as stage 1 hypertension [4,5,6,7,8,9]. As the definition of “normal BP” and the advantages of more intensive BP control remain unclear, there is no consensus on optimal interventions. Studies on Western and Asian populations have shown that prehypertension is associated with adverse cardiometabolic risk profiles even among apparently healthy populations [10,11,12].
Prehypertension was established to focus on a segment of the population who were at higher-than-normal CVD risk and in whom therapeutic approaches to prevent or delay the onset of hypertension and CVD would be of value [13].
We aimed to analyze the clinical characteristics of young and apparently healthy PHT patients compared to NT and untreated HT patients and correlations with BP and cardiovascular risk.
Materials and Methods:
Methods: This cross-sectional study included 326 healthy untreated subjects between the ages of 18 and 45 who were randomly selected from general medicine practice registries. The exclusion criteria were kidney, heart, thyroid, and liver disorders; psychiatric diseases; secondary hypertension; atherosclerotic peripheral disease; stroke; myocardial infarction; or any chronic or acute infections. Data were collected from 04/2016 to 04/2018. All measurements were performed in the morning between 08:00 and 09:30 after an overnight fast. Basic anthropometric measurements were performed on all subjects in a standardized manner. BP was measured when patients were in the sitting position using an Omron M6 device with a cuff appropriate to the length and circumference of their arm after a resting period of 5 minutes. BP values were expressed in mmHg, and the measurement was repeated 3 times to avoid bias [6]. Fasting venous blood (10.5 ml) and spot urine samples were collected from all subjects. The complete blood count was determined via laser scattering technology (analyzer XN 1000, Sysmex); the biochemistry panel was obtained after 10 minutes of blood centrifugation. The serum glucose was assessed via UV photometry with hexokinase (Architect analyzer), triglycerides via photometry with glycerol phosphate oxidase (GPOPAP), HDL-cholesterol via the homogeneous enzyme-immunoinhibitory method, LDL-cholesterol via the homogeneous method (CHE, CHOD-DSBmT), and C-reactive protein via the immunoturbidimetric method with latex particles. The serum urate levels were assessed via the spectrophotometric uricase enzyme-based method, serum insulin levels via electrochemiluminescent immunoassay (ECLIA, Cobas e 411, Roche), serum and urinary creatinine levels via photometry with alkaline picrate (Architect analyzer, Abbott), serum and urine electrolytes via the indirect potentiometric method, and urine alpha-1-microglobulin via continuous photometry with alkaline picrate and latex immunonephelometric (Nephelometer analyzer, BNII, Siemens). Uromodulin (UM) was measured from urinary samples stored at -60°C using an enzyme-linked immunosorbent assay (Bio-Vendor, Cobas Roche) and standardized to urinary creatinine [indexed UM (iUM)]. The glomerular filtration rate was estimated using the CKD-EPI creatinine equation: {eGFR, ml/min/1.73 m2=141 x min (SCr/κ, 1)α x max(SCr/κ, 1)-1.209 x 0.993Age x 1.018 [if female] x 1.159 [if Black]} [14]. Insulin resistance and pancreatic beta cell function were assessed using the HOMA method, i.e., HOMA-IR (Homeostasis Model Assessment for Insulin Resistance): [HOMA-IR = fasting plasma insulin x fasting plasma glucose)/22.5] and HOMA-β (Homeostasis Model Assessment of β-Cell Function) [HOMA ß (%ß) = HOMA-IR – (20xfasting plasma insulin)/(fasting plasma glucose – 3.5)] [15]. Transthoracic echocardiograms were obtained for 143 participants by one observer, and the left ventricular mass was calculated according to a method presented in the literature [16].
According to the estimated cardiovascular risk assessed using the “Framingham 10 Year Risk of General Cardiovascular Disease” risk score, the participants were categorized into either the lower (<5%) or the higher (>5%) group [17].
The study protocol complies with the Declaration of Helsinki and the local institutional guidelines and was approved by the local ethics committees. Written informed consent was obtained from all participants.
Statistical analysis: Data were analyzed using descriptive statistical methods. The continuous variables are expressed as the mean±SD when approximately normally distributed and as the median and interquartile range when not. Categorical variables are expressed as absolute and relative frequencies. The variance in the category variables was tested using the Chi-square and Fisher’s exact tests. The differences between the variables in the two independent groups were tested with the Mann–Whitney U Test. The differences between three and more groups were tested via ANOVA (post hoc Bonferroni, Scheffe) or Kruskal–Wallis test (post hoc Conover). The correlation between numeric variables was evaluated using Spearman’s correlation coefficient ρ (rho). Stepwise multivariate linear models and logistic regression were finally used to explore the associations of interest. All P values were two-sided. The level of significance was set to Alpha = 0.05. The analysis was conducted while using MedCalc Statistical Software version 18.2.1 (MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org; 2018) and IBM SPSS Statistics 23 (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.).
Results:
The basic demographic, anthropometric, and clinical measurements of enrolled subjects are shown in Table 1. Although not significantly different, the NT and PHT groups were younger than the HT group. There were significant differences in gender (p<0.001). The PHT group had intermediate body mass index (BMI) values (p=0.009)) and waist circumferences (p=0.001) compared to the NT and HT groups, but a statistically significant difference was only present between the NT and HT groups and the PHT and HT groups.
Increasing values of serum uric acid (p<0.001), glucose (p<0.001), glycated hemoglobin (HbA1c) (p=0.01), insulin (p=0.002), HOMA-IR (p=0.001), total cholesterol (p=0.04), and TG (p<0.001) were observed between the BP categories. Although there was significant difference in HOMA-IR between the PHT and NT groups, glucose and HbA1c values were not significantly different between the PHT and NT groups, only between the PHT and HT groups. There was a significant difference in uric acid, total cholesterol, and TG between all three groups.
There were no differences in estimated glomerular filtration rate (eGFR), urine albumin-creatinine-ratio (uACR), and serum and urine electrolyte concentrations among the BP groups (Table 1). The sodium/potassium ratio in urine (Na/K) and estimated salt intake was higher than recommended, but without any differences between groups. Although not significant, a trend of higher UM values in higher BP groups was observed.
The echocardiographic data of participants according to the JNC-7 BP categories are shown in Table 2. The PHT group had intermediate values of interventricular septum (IVS) (P=0.02), left ventricular posterior wall (LVPW) (P<0.001), left ventricular mass (LVM) (P=0.001), relative wall thickness (RWT) (<0.001), left ventricular mass index (LVMI) (P=0.01), and the ratio of early diastolic mitral inflow velocity to early diastolic mitral annulus velocity (E/e' ratio) (p=0.03), without significant differences in IVS, LVMI, and E/e’ between the PHT and HT groups.
According to the “Framingham 10 Year Risk of General Cardiovascular Disease” score (FRS), 258 (78,8%) participants were in the higher FRS category and 61 (18,7%) in the lower FRS category. There was a stepwise increase in the number of participants in the higher FRS category within BP categories (7,9 % vs. 24,6% vs. 48.1%).
Multivariate logistic regression (stepwise method) showed that waist circumference, uromodulin, and triglycerides were independent predictors of cardiovascular risk in the entire cohort. In the PHT group, only triglycerides showed statistical significance (Table 3). The ROC analysis of the sensitivity, specificity, and cut-off value for triglycerides regarding CVR in the PHT group is shown in Table 4 and Figure 1.
Discussion:
We observed that metabolic disorders are present risk factors in the PHT group. Higher HOMA-IR, total cholesterol, triglycerides, and uric acid contribute to higher CVR in the PHT group compared to the NT group. Worsening metabolic disorders were observed in the HT group because they had higher glucose and HbA1c values compared to the PHT group.
Our findings are in line with previous studies. Grotto et al. examined the prevalence of prehypertension and the associated cardiovascular risk factors in a large population-based sample of young Israeli adults. The prehypertensive group had higher levels of blood glucose, total cholesterol, low-density lipoprotein cholesterol, and triglycerides; higher body mass index; and lower levels of high-density lipoprotein cholesterol than the normotensive group. Multivariate logistic regression analysis showed that the body mass index was the strongest predictor of prehypertension among both males and females (odds ratio, 1.100; 95% CI, 1.078 to 1.122 and odds ratio, 1.152; 95% CI, 1.097 to 1.21, respectively, for every 1 kg/m2 increase) [18]. Chiang et al. found that higher levels of blood glucose, HbA1c, and BMI were associated with prehypertension in three ethnic Asian groups in Singapore (12). Contrary to our study, the diversity in age and ethnicity might explain the differences in cardiometabolic risk factors between these studies.
We observed differences in hypertension-mediated organ damage (HMOD) between the PHT and NT groups. Left ventricle changes, particularly higher left ventricle mass, concentric remodeling, and diastolic dysfunction, were present in the PHT group, while they presented no signs of kidney damage (in term of lower eGFR, higher ACR and tubular function markers), which may support the hypothesis that early renal damage is not an important initial trigger for developing prehypertension.
Other authors have also reported on the impact of prehypertension on left ventricular structure, function, and geometry [19,20,21,22]. Early left atrial mechanics and volume abnormalities were observed in subjects with prehypertension [23]. Furthermore, left ventricle hypertrophy was shown to have prognostic value for the progression of prehypertension to hypertension [24].
Contrary to previous results indicating a higher prevalence of glomerular hyperfiltration and microalbuminuria in prehypertensive individuals, there were no differences in glomerular and tubular function markers between the BP groups in our study. Kim et al. found a higher prevalence of microalbuminuria in a high–normal BP group compared to a normal BP group (4.9% vs 2.8%, p=0.009) [25]. Besides older age, a clustering of other risk factors observed in the high–normal BP group could contribute to kidney injury [25].
There was a stepwise increase in the prevalence of participants classified into the higher FRS BP category. Among all included traditional risk factors, triglycerides were shown to be independent cardiovascular risk predictors in the PHT group. Genetic, epidemiologic, and clinical studies have shown that low-density lipoproteins cause atherosclerotic cardiovascular disease [26,27]. Hypertriglyceridemia is a common condition with elevated levels of plasma triglycerides (TG), which are mainly transported in the blood via TG-rich lipoproteins (TRLs). Various task forces and national societies have suggested different cut-off values for elevated TG levels. However, there is consensus on using TG >150 mg/dL (>1.7 mmol/L) as the definition of hypertriglyceridemia [28]. Elevated TG levels are only one marker of altered lipid/lipoprotein metabolism and reflect altered concentrations of one or more classes or subfractions of TG, which, in turn, may have a different association with CV risk. Many epidemiological studies have reported on correlations between serum TG concentrations and the risk of coronary heart disease (CHD). Available data indicate consistent, moderate, and highly significant associations between triglyceride levels and CHD risk but appear to considerably depend on the levels of established risk factors [29]. A real-world administrative claim analysis of statin-treated patients pointed to high residual cardiovascular risk, medical costs, and resource use associated with high triglycerides [30]. Despite having optimal levels of LDL-cholesterol from taking statins, some people may still have a “residual” (or leftover) risk of developing cardiovascular disease. After adjusting for established risk factors and statin use, triglyceride-carrying apolipoproteins (ApoC1, ApoC3, and ApoE) were associated with a two- to three-fold higher risk of coronary heart disease in PROCARDIS and Bruneck studies [31].
Data from the Mendelian Randomization Study support a direct causal relationship between increased TG levels (total plasma TG-rich lipoproteins) and the risk of atherosclerotic cardiovascular disease (ASCVD) events [32,33]. Furthermore, genetically reduced concentrations of nonfasting plasma TG are associated with reduced all-cause mortality, likely through reduced amounts of cholesterol in remnant lipoproteins [34]. In the TG-REAL retrospective cohort analysis, hypertriglyceridemia’s correlation with all-cause mortality and atherosclerotic cardiovascular events was observed in a low-risk Italian population [35].
The main strength of our study is that we have a relatively homogenous cohort of young and apparently healthy, untreated subjects with normal renal function. Moreover, measurements were performed under standardized conditions using a validated method. The main drawback may be the relatively small number and unbalanced gender distribution of participants and non-well-matched groups. It is important to point out that we assessed fasting TG, although it has been suggested that nonfasting TG levels are better predictors of increased CVR [36]. Due to the cross-sectional design of our study, we only assessed TG levels at baseline. Therefore, patients with normal fasting TG but high postprandial TG levels may have been misclassified into the lower risk category.
Conclusion:
Although epidemiological and Mendelian randomization studies have reported correlations between serum TG concentrations and the risk of atherosclerotic cardiovascular disease, the literature lacks data on hypertriglyceridemia’s correlation with all-cause mortality and atherosclerotic cardiovascular events in a low-risk PHT population. Our study highlights the importance of hypertriglyceridemia as an early marker of cardiovascular risk in a younger, apparently healthy, PHT population.
References
- Robinson, S.C.; Brucer, M. Range of normal blood pressure: a statistical and clinical study of 11,383 persons. Arch Intern Med 1939; 64:409-44. [CrossRef]
- Vasan, R.S.; Larson, M.G.; Leip, E.P. , et al. Impact of high-normal blood pressure on the risk of cardiovascular disease. N Engl J Med. 2001: 345(18):1291-7. [CrossRef]
- Lewington, S.; Clarke, R.; Qizilbash, N. , et al. Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet.2002;360(9349):1903-13. [CrossRef]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R. , et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003; 289:2560-72. [CrossRef]
- Mancia, G.; De Backer, G.; Dominiczak, A. , et al. ESH-ESC Task Force on the Management of Arterial Hypertension. 2007 ESH-ESC Practice Guidelines for the Management of Arterial Hypertension: ESH-ESC Task Force on the Management of Arterial Hypertension. J Hypertens. 2007;25(9):1751-62. [CrossRef]
- Mancia, G.; Fagard, R.; Narkiewicz, K. , et al. Task Force Members. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013;31(7):1281-357. [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W. , et al. ESC Scientific Document Group. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018; 39(33):3021-3104. [CrossRef]
- Mancia, G.; Kreutz, R.; Brunström, M. , et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). J Hypertens. 2023;41(12):1874-2071. [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S. , et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2018;138(17):e426-e483. [CrossRef]
- Gupta, A.K.; Brashear, M.M.; Johnson, W.D. : Coexisting prehypertension and prediabetes in healthy adults: a pathway for accelerated cardiovascular events. Hypertens Res. 2011; 34 (4): 456-461. [CrossRef]
- Gupta, A.K.; McGlone, M.; Greenway, F.L. , et al. Prehypertension in disease-free adults: a marker for an adverse cardiometabolic risk profile. Hypertens Res. 2010; 33 (9): 905-910. [CrossRef]
- Chiang, P.P.; Lamoureux, E.L.; Shankar, A. et al. Cardio-metabolic risk factors and prehypertension in persons without diabetes, hypertension, and cardiovascular disease. BMC Public Health 2013; 13; 730. [CrossRef]
- Chobanian, A.V. Prehypertension revisited. Hypertension. 2006;48:812–814. [CrossRef]
- Levey, A.S.; Stevens, L.A. Estimating GFR using the CKD Epidemiology Collaboration (CKD-EPI) creatinine equation: more accurate GFR estimates, lower CKD prevalence estimates, and better risk predictions. Am J Kidney Dis 2010; 55:622–7. [CrossRef]
- Wallace, T.M.; Levy, J.C.; Matthews, D.R. Use and abuse of HOMA modeling. Diabetes Care 2004;27(6):1487—95. [CrossRef]
- Lang, R.M.; Bierig, M.; Devereux, R.B. , et al. Recommendations for chamber quantification: A report from the American Society of Echocardiography's guidelines and standards committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. Journal of the American Society of Echocardiography 2005; 18: 1440-63. [CrossRef]
- D’Agostino RB, Vasan SR; Pencina MJ, et al. General Cardiovascular Risk Profile for Use in Primary Care: The Framingham Heart Study. Circulation. 2008;117: 743-53. [CrossRef]
- Grotto, I.; Grossman, E.; Huerta, M. , et al. Prevalence of prehypertension and associated cardiovascular risk profiles among young Israeli adults. Hypertension. 2006;48(2):254-9. [CrossRef]
- Ahn, H.S.; Kim, S.J.; Kim, M.K. , et al. The Difference of Left Ventricular Hypertrophy and the Diastolic Function between Prehypertensives and Normotensives. Korean Circ J 2006; 36:437. [CrossRef]
- Di Bello, V.; Talini, E.; Dell’Omo, G. , et al. Early left ventricular mechanics abnormalities in prehypertension: A two-dimensional strain echocardiography study. Am J Hypertens 2010; 23:405–12. [CrossRef]
- Jang, S.Y.; Kim, S.; Lee, C.K.; Cho, E.J.; Cho, S.J.; Lee, S. Prehypertension and Left Ventricular Diastolic Dysfunction in Middle-Aged Koreans. Korean Circ J. 2016; 46: 536–41. [CrossRef]
- Bajpai, J.K.; Sahay, A.P.; Agarwal, A.K.; De, A.K.; Garg, B.; Goel, A. Impact of prehypertension on left ventricular structure, function and geometry. J Clin Diagnostic Res 2014; 8:7–10. [CrossRef]
- Aktürk, E.; Ermis, N.; Yaǧmur, J. , et al. Early left atrial mechanics and volume abnormalities in subjects with prehypertension: A real time three- dimensional echocardiography study. Echocardiography 2012; 29:1211–7. [CrossRef]
- De Marco, M.; De Simone, G.; Roman, M.J. , et al. Cardiovascular and metabolic predictors of progression of prehypertension into hypertension: The strong heart study. Hypertension 2009; 54:974–80. [CrossRef]
- Kim, B.J.; Lee, H.J.; Sung, K.C. , et al. Comparison of Microalbuminuria in 2 Blood Pressure Categories of Prehypertensive Subjects. Circ J 2007; 71:1283–7. [CrossRef]
- Ference, B.A.; Ginsberg, H.N.; Graham, I. , et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38(32):2459–72. [CrossRef]
- Ginsberg, H.N.; Packard, C.J.; Chapman, M.J. , et al. Triglyceride-rich lipoproteins and their remnants: metabolic insights, role in atherosclerotic cardiovascular disease, and emerging therapeutic strategies – a consensus statement from the European Atherosclerosis Society. Eur Heart J. 2021;42(47):4791–806. [CrossRef]
- Berglund, L.; Brunzell, J.D.; Goldberg, A.C. , et al. Endocrine Society. Evaluation and treatment of hypertriglyceridemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2012;2969–2989. [CrossRef]
- Sarwar, N.; Danesh, J.; Eiriksdottir, G. , et al. Triglycerides and the risk of coronary heart disease: 10,158 incident cases among 262,525 participants in 29 Western prospective studies. Circulation. 2007;115(4):450-8. [CrossRef]
- Toth, P.P.; Granowitz, C.; Hull, M. , et al. High triglycerides are associated with increased cardiovascular events, medical costs, and resource use: a real-world administrative claims analysis of statin-treated patients with high residual cardiovascular risk. J Am Heart Assoc. 2018;7(15): e008740. [CrossRef]
- Farniera, M.; Zellera, M.; Massonc, D. , et al. Triglycerides and risk of atherosclerotic cardiovascular disease: An update. Archives of Cardiovascular Disease. 2021; 114: 132—139. [CrossRef]
- Jørgensen, A.B.; Frikke-Schmidt, R.; West, A.S. , et al. Genetically elevated non-fasting triglycerides and calculated remnant cholesterol as causal risk factors for myocardial infarction. Eur Heart J. 2013;1826–1833. [CrossRef]
- Sarwar, N.; Sandhu, M.S.; Ricketts, S.L. , et al. Triglyceride Coronary Disease Genetics Consortium and Emerging Risk Factors Collaboration, Triglyceride-mediated pathways and coronary disease: collaborative analysis of 101 studies. Lancet. 2010;1634–1639. [CrossRef]
- Thomsen, M.; Varbo, A.; Tybjærg-Hansen, A. , et al. Low nonfasting triglycerides and reduced all-cause mortality: a Mendelian randomization study. Clin Chem. 2014;737–746. [CrossRef]
- Arca, M.; Veronesi, C.; D'Erasmo, L. , et al. Association of hypertriglyceridemia with all-cause mortality and atherosclerotic cardiovascular events in a low-risk Italian population: the TG-REAL retrospective cohort analysis. J Am Heart Assoc. 2020;9(19): e015801. [CrossRef]
- Miller, M.; Stone, N.J.; Ballantyne, C. , et al. Triglycerides and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2011; 123:2292–2333. [CrossRef]
Figure 1.
ROC analysis of sensitivity, specificity, and cut-off value for triglycerides regarding CVR in the PHT group.
Figure 1.
ROC analysis of sensitivity, specificity, and cut-off value for triglycerides regarding CVR in the PHT group.
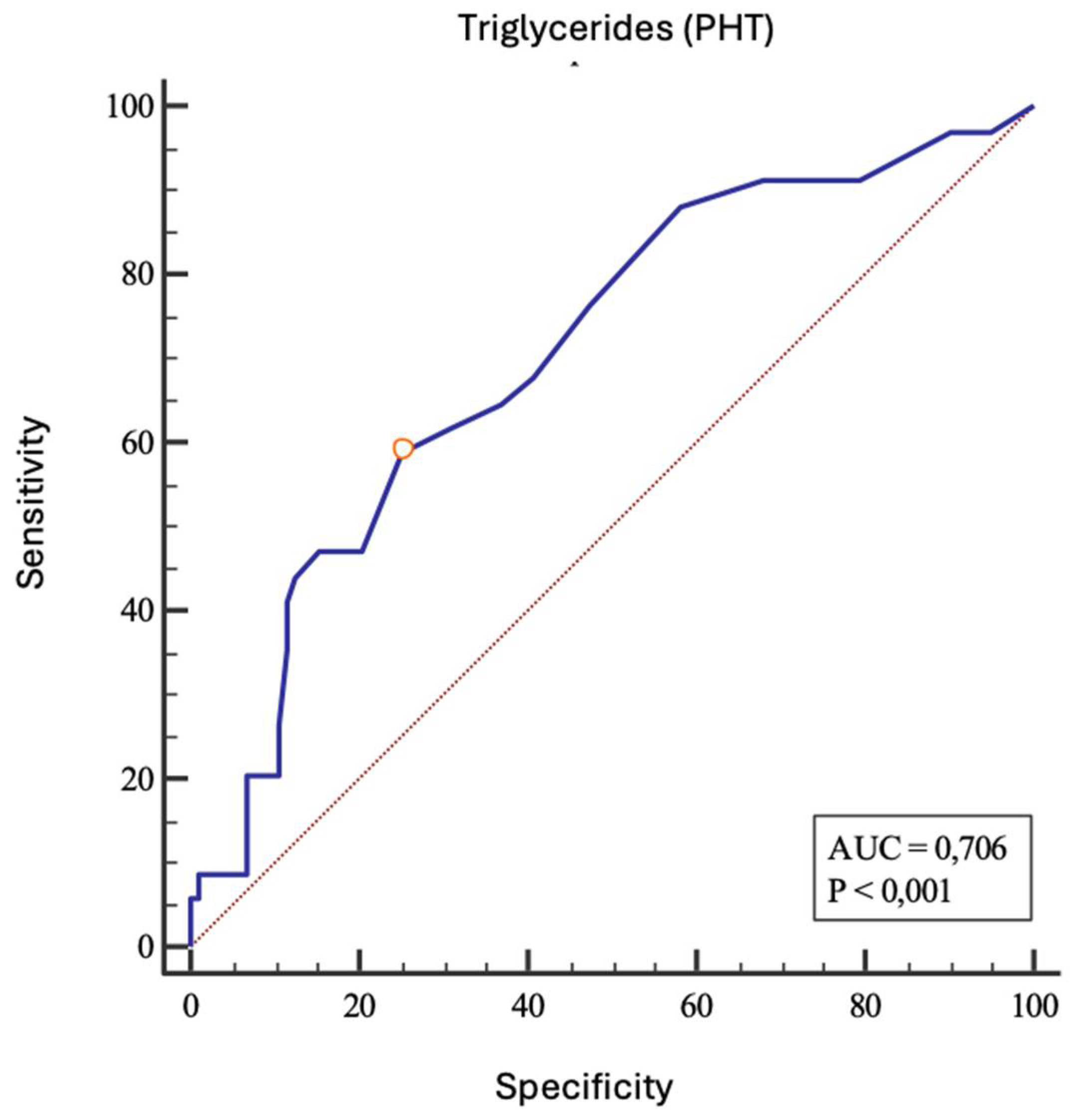

Table 1.
Baseline data of participants according to the JNC-7 blood pressure categories.
| NT (n=103) | PHT (n=140) | HT (n=80) | P• | |
| *SBP (mmHg) | 108.3 (7.1) | 126.9 (80.8) | 143.9 (94.2) | <0.001‡ |
| *DBP (mmHg) | 70.9 (6.2) | 80.8 (6.5) | 94.2 (8.2) | <0.001‡ |
| Sex, m, [n(%)] | 74 (71.8) | 61 (42.7) | 30 (37.5) | <0.001# |
| Age, (g) [median (25%-75%)] | 36 (30 - 42) | 37 (29 - 44) | 39 (33 - 45) | 0.07 |
| **BMI (kg/m2) | 25.6 (22.5 – 28.7) | 26.6 (23.8 - 30) | 28.56 (24.7-32.6) | 0.009 |
| **WC (cm) | 90 (79– 100) | 92 (84 – 102) | 99.5 (89– 110) | 0.001 |
| *Acid uric (µmol/l) | 252 (211 - 307) | 297 (244.5 - 370) | 328 (274 – 412.8) | <0.001 |
| **Glucose (mmol/L) | 4.9 (4.5 – 5.2) | 5 (4.6 – 5.3) | 5.3 (4,8 – 5.6) | <0.001 |
| ±HbA1c (%) | 5.1 (4.9 – 5.4) | 5.1 (4.9 – 5.1) | 5.2 (5 – 5.4) | 0.01 |
| Insulin (mIU/L) | 9.3 (6.6 – 14.6) | 13.4 (8.6 – 17.7) | 14.9 (10 – 25.9) | 0.002 |
| §HOMA-IR (%) | 1.9 (1.4 – 2.7) | 2.9 (1.7 – 4.1) | 3.5 (2.1 – 5.6) | 0.001 |
| *Total cholesterol (mmol/L) | 4.9 (4.3 – 5.6) | 5.2 (4.55 – 5.7) | 5.2 (4.6 – 5.9) | 0.04 |
| HDL-cholesterol (mmol/L) | 1.3 (1.1 – 1.6) | 1.3 (1.1 – 1.7) | 1.3 (1 – 1.6) | 0.35 |
| LDL-cholesterol (mmol/L) | 3.0 (2.4 – 3.6) | 3.1 (2.6 – 3.7) | 3.1 (2.6 – 3.9) | 0.32 |
| *Triglycerides (mmol/L) | 0.9 (0.7 – 1.4) | 1.0 (0.7 – 1.5) | 1.4 (0.9 - 2) | <0.001 |
| Serum potassium (mmol/l) | 4.3 (4.2 – 4.63) | 4.4 (4.1 – 4.7) | 4.3 (4.1 – 4.5) | 0.09 |
| Serum sodium (mmol/l) | 140 (139 - 141) | 140 (139 - 142) | 140 (139 - 141) | 0.48 |
| §Serum creatinine µmol/l) | 68 (63 - 76) | 75 (65 - 86) | 74 (65 – 86.3) | 0.001 |
| CKD-EPI eGFR (ml/min/1,73m2) | 107 (96.3 - 115) | 105 (91 - 113) | 104.5 (94 - 110) | 0.32 |
| ACR urine (mg/g creatinine) | 4.14 (2.64 – 6.05) | 4.1 (2.3 – 6.6) | 4,7 (2,8 - 8,3) | 0.54 |
| A1mCR urine (mg/g creatinine) | 5.6 (3.3 – 7.7) | 4.3 (3.2 - 6,7) | 5.1 (3.6 – 8.4) | 0.07 |
| Na/K ratio, urine | 3.3 (2.5 – 4.5) | 3.3 (2.4 – 5.2) | 3.1 (2.4 – 4.1) | 0.71 |
| Uromodulin (mg/g creatinine) | 43 (27 - 66) | 42.9 (25.5 – 65.3) | 40.6 (24.1 – 60.4) | 0.73 |
| C-reactive protein | 1.8 (0.9 – 2.8) | 1.2 (0.6 – 2.4) | 2 (0.9 – 4.1) | 0.05 |
| Kruskal–Wallis test [median (25%-75%)] •; χ2 test #; ANOVA‡; post hoc Conover: * significant differences btw. NT vs. PHT, NT vs. HT, and PHT vs. HT; ** significant differences btw. NT vs. HT and PHT vs. HT; § significant differences btw. NT vs. PHT and NT vs.HT; §§ significant difference btw. NT vs.HT; ±significant difference btw. PHT vs. HT; NT, normotensive; PHT, prehypertensive; HT, hypertensive; SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; WC, waist circumference; HbA1c, glycated hemoglobin A1c; HOMA-IR, Homeostasis Model Assessment for Insulin Resistance; HDL, high-density lipoprotein; LDL, low-density lipoprotein; eGFR, estimated glomerular filtration rate; CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration Estimated Glomerular Filtration Rate; ACR, albumin/creatinine ratio in spot urine; A1mCR, alpha-1-microglobulin creatinine ratio in spot urine; spot urine Na/K ratio, sodium/potassium ratio in spot urine. | ||||
Table 2.
Echocardiographic data of participants according to the JNC-7 BP categories.
| NT (n=41) | PHT (n=52) | HT (n=50) | P* | |
| LA (mm) §§§ | 32.5 (30.3 - 36) | 33 (30 - 36) | 36.5 (32.8 - 39) | 0.007 |
| LAVI (ml/m2) | 20.8 (16.8 – 23.6) | 19.1 (16.5 – 22.7) | 21.2 (17.4 - 26) | 0.25 |
| LV (mm) | 47 (44 – 50.5) | 49 (45 - 51) | 46.5 (43 - 52) | 0.43 |
| IVS (mm) §§ | 10 (8 - 10) | 10 (9 - 11) | 10 (9 - 12) | 0.02 |
| LVPW (mm) § | 9 (8 – 10.5) | 10 (9 - 11) | 11 (10 - 12) | <0.001 |
| LVM (g) § | 142.1 (122.3 – 180.9) | 163.72 (146.4 -193.8) | 190.4 (145.9 – 228.3) | 0.001 |
| LVMI (g/m2) §§ | 77.5 (67.6-88.3) | 84.3 (73.3-95.9) | 87.7 (74.3-107.4) | 0.01 |
| RWT (cm) § | 0.4 (0.4 – 0.4) | 0.4 (0.4-0.5) | 0.5 (0.4 – 0.6) | <0.001 |
| E/A | 1.3 (1 – 1.5) | 1.3 (1 – 1.5) | 1.3 (1 – 1.5) | 0.89 |
| E/e' §§ | 7 (5.6 – 8.7) | 7.4 (6.3 - 9) | 8.2 (6.8 – 9.4) | 0.03 |
| SV (ml) | 67.5 (58.5 – 82.8) | 74 (63.5 - 86) | 74 (61 – 95.5) | 0.24 |
| EFLV (%) | 66 (62 - 70) | 64 (60 - 69) | 67 (62 – 68.3) | 0.34 |
| * Kruskal–Wallis test (median and interquartile range); NT, normotensive; PHT, prehypertensive; HT, hypertensive; LA, left atrium; LAVI, indexed left atrium volume; LV, left ventricle; IVS, interventricular septum; LVPW, left ventricular posterior wall; LVM, left ventricular mass; LVMI, left ventricular mass indexed; RWT, relative wall thickness; E/A, the ratio of peak velocity blood flow from left ventricular relaxation in early diastole (the E wave) to peak velocity flow in late diastole caused by atrial contraction (the A wave); E/e', the ratio of early filling velocity on transmittal Doppler (E) with the early relaxation velocity on tissue Doppler (E′); SV, stroke volume; EFLV, left ventricular ejection fraction; post hoc Conover : § NT vs. PHT, NT vs.HT, and PHT vs.HT; §§ NT vs. HT; §§§ NT vs.HT and PHT vs.HT. | ||||
Table 3.
Final model of significant predictors of CVR in the PHT group.
| Parameter | ß | Standard error | Wald | p | Odds ratio (Exp ß) | 95% CI za Exp ß |
| Triglycerides (mmol/L) | 0.63 | 0.28 | 4.96 | 0.03 | 1.88 | 1.08 do 3.28 |
| Constant | -2.8 | 0.73 | 15.0 | <0.001 |
ß, regression coefficient; CI, confidence interval
Table 4.
ROC curve parameters for CVR in the PHT group.
| Parameters | AUC | 95% CI | Sensitivity | Specificity | Cut-off | Youden index |
P |
| Triglycerides (mmol/L) | 0.706 | 0.622-0.781 | 58.8 | 74.8 | > 1.3 | 0.34 | <0.001 |
AUC, area under the curve
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



