Submitted:
07 June 2024
Posted:
11 June 2024
You are already at the latest version
Abstract
Abstract:
Background: The optimal strategy for the microelimination of HCV within community settings remains ambiguous. We evaluated the percentage of participants who achieved linkage to care (LTC) following the conclusion of the screening campaign, and examined the diverse factors influencing LTC among these individuals. The effectiveness of recall intervention for the non-LTC population and its barriers were analyzed.
Methods:
We initiated an HCV patients recall program to identify the HCV participants who might not be treated after the HCV screening campaign. A program staff recalled HCV participants who lost to follow-up through the telephone from March 2019 to June 2019. They were informed of HCV treatment's importance, efficacy, availability, and safety.
Result:
Among 185 HCV-infected participants, 109 (58.9%) HCV-infected participants had obtained LTC. Compared with those who had LTC, those without LTC were older, lower education levels, were less aware of their HCV infection, less frequently lived in urban areas, and had less health insurance. At the end of the recall program, 125 (67.6 %) persons had liked to care. The proportion of LTC increased by 8.7 %. 119 persons had an HCV RNA test, and 82 (68.9%) had viremia. Of 82 patients with viremia, 78 (95.1%) received antiviral therapy. 76 (97.4 %) of them achieved a sustained virological response.
Conclusion:
After a community screening campaign, 59 % of participants with anti-HCV positive had LTC. The recall program can increase by 9 %. However, there were still 32% of HCV participants who couldn't be linked to care. Outreach care for non-LTC patients is a way worth trying to achieve micro-elimination of HCV in the rural community.
Keywords:
hepatitis C virus
; linkage to care
; hepatitis C microelimination
1. Introduction
The World Health Organization (WHO) has a stated goal of eliminating viral hepatitis C virus (HCV) and B virus (HBV) infection as a public health threat by 2030, defined as a 65% reduction in mortality, a 90% reduction in new infections, diagnosing 90% of all hepatitis infections, and treating 80% of the eligible population [1]. Access to HCV treatment is improving but remains limited. Worldwide, 7% of those diagnosed (1.1 million) were started on treatment in 2015. Although the availability of highly effective direct-acting anti-viral agents (DAA) therapy for HCV has ushered in a new era in HCV treatment and prevention, simply making DAAs widely available will not mean all people living with hepatitis C have access to these medicines [2]. The estimated prevalence of anti-HCV was 3.3% (1.8-5.5%) in the general population in Taiwan, with several regional disparities. Taiwan has accelerated its efforts to eliminate hepatitis C since 2018 by committing to achieve WHO’s 2030 goal of treating 80% of eligible patients by 2025 [3]. Meanwhile, there are about 120,000 chronic hepatitis C (CHC) patients awaiting to be diagnosed in Taiwan. Accelerating the universal screening program of populations aged 45-79 years and resolve the unawareness issue of HCV infection are becoming challenging and critical on the road toward elimination[4].
Community-based screening could provide CHC screening in lower socioeconomic and educational populations and poor access to healthcare systems [5]. Many questions remain about the best funding mechanisms to ensure programme sustainability and the most effective strategies to ensure programme reach, linkage to care (LTC), and access to treatment. Understanding and addressing the specific reasons why patients are lost at each stage is critical if public health and clinical-care practitioners hope to affect the outcomes of chronic HCV infection.
In this community-based study, we assessed the proportion of participants who obtained LTC since the end of the screening campaign and examined various factors affecting LTC in these participants. A recall programme was adopted for the non-LTC population to achieve HCV micro-elimination in the community. The outcomes of persons eligible for treatment were also evaluated.
2. Material and Methods
2.1. HCV-Screening Campaign and LTC
The participant recruitment and sample preservation were carried out from the Northeastern Taiwan Community Medicine Research Cohort (NTCMRC, ClinicalTrials.gov Identifier: NCT04839796). We implemented a community-outreach campaign from August 2013 to Dec 2017 in the northeastern coast region of Taiwan, including four districts (Wan-li, Gong-liao, Rul-fan, and An-le). Three districts were rural townships on the northeastern seaboard, and one was urban. Adult participants (≥30 years old) were recruited from the community by public service announcements, talks to community groups, and notices in clinics. A trained team of interviewers administered a standardized questionnaire to all participants. All participants received a demographic survey, a physical examination, and blood tests. Blood tests included complete blood cell and its differentiation count, liver biochemistry, glucose, lipid profile, HBV surface antigen (HBsAg), and antibody to HCV. All participants were asked if they had ever been infected with HCV. Participants who were HCV-antibody seropositive and had self-reported HCV infection were considered to be aware of hepatitis C (aHC). Participants who were HCV-antibody seropositive and denied a history of HCV infection were considered unaware of hepatitis C (uaHC). The participants who were positive for HCV antibodies were informed of their results by paper mail or in person. Simultaneously, they were recommended to obtain LTC at the Chang Gung Memorial Hospital (CGMH) Keelung branch or other hospitals. The CGMH Keelung branch in Taiwan is a tertiary referral hospital that provides the standard of care for HCV diagnosis and treatment.
Serum HCV-RNA level was determined by the Cobas TaqMan HCV Test v. 2.0 (Roche Molecular Diagnostics, Pleasanton, CA), with a lower limit of quantification of 15 IU/mL. The hepatitis C virus genotype was determined by Cobas HCV GT (Roche Molecular Diagnostic). Hepatic fibrosis stages were assessed by using transient elastography (FibroScan®; Echosens). Screening for comorbidities and contraindications to treatment was performed. Patients found to be eligible for treatment were prescribed interferon based therapy (IBT) and/or DAA according to the national treatment guidelines at the time.
2.2. Recall Programme
Since Dec 2018, we initiated an intervention named the “recall programme” to identify participants who might not have obtained LTC after screening and to enhance their access to treatment. Initially, the programme staff reviewed the medical records of all HCV-antibody-positive participants in CGMH. People who did not visit a hepatologist or were lost to follow-up were contacted by telephone from March 2019 to June 2019. Those individuals were asked if they had visited other clinics to manage hepatitis C. The people who had not obtained LTC were informed of the importance, efficacy, availability, and safety of HCV treatment. The programme staff provided education and counseling, scheduled hepatologist appointments, accompanied participants to appointments, and provided information about subsidies for medical expenses. The reasons concerning non-LTC and subsequent follow-up results were recorded. The factors affecting LTC and the effectiveness of the recall programme were evaluated.
2.3. Description of the HCV Treatment in Taiwan
The Bureau of National Health Insurance (NHI) of Taiwan began to reimburse CHC patients for IBT in 2003. A 48 or 24-week regimen of pegylated interferon plus ribavirin combination therapy has been the standard of care. Since January 2017, DAAs have been reimbursed by the Taiwan NHI programme for CHC patients with advanced hepatic fibrosis or compensated cirrhosis . On January 1, 2019, the Taiwan NHI authorized the prescription of DAAs to all Taiwanese citizens with CHC. Sustained virologic response (SVR) was defined as undetectable HCV-RNA for ≥ three months after DAA treatment completion or six months after IBT, as indicated in the patient’s medical chart [3].
2.4. Statistical Analysis
Continuous variables were expressed as the mean ± standard deviation (SD). Statistical comparisons between groups of patients were assessed by performing the t-test for continuous variables and the Pearson chi-square test for categorical variables. The McNemar test was used to check if the proportion of LTC after the recall programme significantly differed from the same proportion before the recall programme. Database manipulation and analyses were performed using SPSS version 19 (IBM SPSS Statistics for Windows; IBM Corp., Armonk, NY). A p-value < 0.05 was considered to be indicative of statistical significance.
3. Results
Among the 6161 participants screened for viral hepatitis infection, 185 (3.0%) were seropositive for the HCV-antibody (59 men, 126 women, mean age: 65 years). The prevalence of HCV-antibody positivity increased with age, and 74% were aged > 60 (Figure 1). Of the 185 positive participants, 23 (12.4%) were also seropositive for HBsAg. Thirty-one (16.7%) participants had received anti-HCV treatment before screening.
3.1. Self-Awareness of HCV Infection and LTC
Among the 185 participants who were seropositive for HCV-antibody, 74 (40.0%) were aware of hepatitis C infection. The age group from 45 to 60 years old had the highest disease awareness (63.3%), and the age group >75 years old had the lowest disease awareness (11.5%) (Figure 2). Compared with uaHC, aHC participants were younger, had higher education levels, more private health insurance, greater alcohol consumption, and more elevated alanine aminotransferase (Table 1). Sex, living in an urban area, and family history of liver disease were not significantly associated with awareness of HCV serostatus.
After the screening campaign, 109 (58.9%) HCV-infected participants had obtained LTC, including 93 who had regular follow-ups at CGMH and 16 who had regular follow-ups at other hospitals. The remaining 76 (41.1%) participants had not visited a hepatologist or were lost to follow-up after one visit. Compared with those who had LTC, those without LTC were older (67.0 ± 11.6 vs. 63.7 ± 8.6 years old, p = 0.035), lower education levels (p = 0.032), less aware of their HCV infection (23.7% vs. 51.4%, p < 0.001), less frequently lived in urban areas (36.8% vs. 52.3%, p = 0.038), and had less health insurance (53.4% vs. 70.2%, p = 0.023) (Table 2).
3.2. Effectiveness of the Recall Programme
Attempts were made to contact the 76 non-LTC participants in the recall programme, but 35 (43.4%) could not be contacted because of incorrect telephone numbers or non-responses, 3 (3.9%) died, 16 (19.7%) subsequently started participating in LTC at CGMH, and 22 (28.9%) still did not start LTC despite our advice. After the recall programme, 125 (67.6%) HCV-infected participants got linkage to care. The proportion of LTC participants significantly increased by 8.7% (p < 0.001). The reasons those 22 non-LTC participants gave were “I need time to consider whether to start treatment” (n = 8), “I will seek treatment by myself” (n = 7), “I am not willing to be treated because of old age,” “I am too busy,” or “I do not think it would be good for my well-being” (n = 5). Two participants did not keep their outpatient appointments.
3.3. Clinical Features and Outcomes of the LTC Participants
Among 125 LTC participants, 119 (95.2%) were tested for HCV-RNA. Of them, 82 (68.9%) were positive for HCV-RNA. Fifty-five participants had undergone Fiboscan® (Echosens). The liver fibrosis stages were F0 = 15 (25.9%), F1 = 13 (22.4%), F2 = 10 (17.2%), F3 = 11 (19.0), and F4 = 9 (15.5%). The genotype distribution was GT1b = 41 (62.1%), GT2 = 24 (36.3%), and indeterminate = 1 (1.5%). Seventy-eight (95.1%) eligible patients received anti-viral therapy, including 36 (46.2%) who received IBT, 3 (3.8%) who had IBT failure and then been retreated with DAA, and 39 (50.0%) who received DAA. All of these patients completed treatment and showed end-of-treatment virological responses. Seventy-six (97.4%) patients achieved SVR. Of the 82 HCV-RNA-positive patients, 76 (92.7%) were cured (Table 3, Figure 3).
4. Discussion
Our study aimed to evaluate the HCV-care continuum among participants after an HCV screening campaign and the effectiveness of a recall programme in Northeastern Taiwan communities. We found that 41% of diagnosed HCV participants did not have LTC. The associated factors affecting LTC included older age, living in a rural area, unaware of their HCV infection, and lack of health insurance. Our recall programme significantly increased the proportion of patients with LTC by 9%. Among those with LTC, most eligible patients (95.1%) received anti-viral therapy, and 97.4% were successfully treated.
Lack of awareness of HCV infection among affected individuals might be attributed to the asymptomatic nature of CHC until the development of end-stage liver disease. A population-based study surveyed from 2013 through 2016 in the United States highlighted the continued inadequate state of viral hepatitis awareness (<50%) among all individuals and especially among high-risk subpopulations [6]. Another nationwide community-outreach screening programme in Taiwan found that 44.6% of people were aware of their infection [7]. In this study, aware subjects were younger, had higher education levels, more health insurance, and greater alcohol consumption. We found that people among 45 to 60 years old were more likely to be aware of their HCV status than younger or older people. This finding was consistent with data from NHANES [8]. This result reflects that middle-aged adults are more motivated and likely to be screened for the virus. As for the more significant amount of alcohol consumed by aware subjects, it may be related to their age. However, this result revealed a notable conclusion. In Taiwan, the major transmission of HCV is through the iatrogenic route in the early years [9]. Patients >60 years old accounted for 74% of all patients in our study, but their awareness of the disease was relatively low. As countries that have successfully treated all diagnosed cases run out of patients without increasing the diagnostic rate through screening, their progress toward elimination will slow substantially [10]. There is still a need to design additional community-based screening strategies to identify and treat more infected individuals.
At the population level, the “cascade of care” is a continuum of recommended services for persons living with hepatitis as they go through various stages, from diagnosis to treatment to chronic care and, for hepatitis C, to cure [1]. A nationwide survey in Taiwan by Yu et al. reported that 36.2% of HCV-antibody seropositive subjects aware of their diagnosis. Among those with disease awareness, 39.6% had accessibility. The recommendation/ acceptance rate of antiviral therapy was 70.6% [5]. Our study found that 41% of HCV-antibody seropositive participants did not start LTC after learning of their HCV infection. Of those participants, 29% still chose not to start LTC despite our recall programme and recommendation. Previous studies have shown that barriers to LTC and treatment include a lack of trust in healthcare providers [11], misconceptions regarding treatment adherence [12], and higher rates of depression and psychiatric illness [13].
We addressed three significant factors from the multivariate analysis associated with LTC. First, our study indicated that being unaware of their infection itself was a predictor of non-LTC. The movement of infected individuals through the viral hepatitis care cascade is first contingent on awareness of their diagnosis, often the step with the largest drop-off in the cascade [14]. According to Zhou’s study, less than half of those aware of HCV infection reported receiving treatment, which identified an additional gap in the care cascade [6]. The studies based on data from the HANES Hepatitis C Follow-Up Survey also indicated that knowledge about having HCV infection was the only independent predictor of receiving treatment [8,15]. As shown in this study, more than half of the older participants were unaware of their HCV infection and tended to be lost to follow-up. A strategy to provide structured and facilitated referrals for treatment needs to be developed.
Second, we found that older persons with lower education levels were significantly less likely to have LTC. This result might be because those individuals lacked knowledge about HCV infection and did not recognize themselves as at risk for liver disease progression. Additionally, poor knowledge of HCV treatment, fear of treatment side effects, and the asymptomatic nature of HCV infection were also the main reasons for not considering HCV treatment. Our recall programme elucidated how more HCV-infected individuals were successfully mobilized from screening into care and treatment. Engaging with people in discussions about HCV, its treatment, and the potential long-term consequences of HCV-related liver disease if left untreated individually would increase the willingness to seek treatment. This engagement led to 20% of people who previously did not have LTC being successfully referred for HCV care.
Third, people who had less health insurance and lived in rural areas were less likely to have LTC. There were differences in the sociodemographic characteristics of patients diagnosed with HCV and in the success rate linking patients to outpatient care. Those patients who had already seen a doctor or other health care professional were more likely to have health insurance and a usual source of medical care than those who had not [8]. Furthermore, inadequate health insurance coverage and limited access to regular health care may limit patients’ health-seeking behaviors [16]. We noted that even if case managers scheduled hepatologist appointments and provided follow-up reminder phone calls, some people still did not start LTC due to economic and transportation considerations. A simplified two-step care cascade enabling a test and treat model will enhance HCV treatment scale-up [17].
Our epidemiological survey showed that approximately 69% of the HCV-antibody seropositive patients were viremic in the community. We speculated that 128 (69%) of the 185 HCV-antibody-positive patients should be treated. Accordingly, we estimated that ≥ 60.9% of the eligible patients were treated, and 59.3% were finally cured. The current results have not reached the desired WHO goal. To achieve micro-elimination of HCV in the community, there are areas for improvement in the care of continuum. Although the recall programme could increase the uptake of LTC, there is still a proportion of patients who were unreachable or refused LTC. We suggested outreach care would be an effective strategy for HCV treatment provision in the rural community. For residents with limited medical resources, the development of point-of-care HCV-RNA diagnostics may facilitate a real “test and treat” model of care. Simplification of the therapeutic pathway continues to evolve, as described in updated clinical guidelines. The mobile outreach care, including motivational education, non-invasive liver disease assessment, and DAA home-delivery service, would provide convenient services to enhance treatment uptake, particularly for socioeconomically disadvantaged older people.
The present study had several limitations. First, a significant proportion (19%) of the HCV-antibody seropositive participants could not be contacted and were lost to follow-up. So, we cannot be sure if they had participated in LTC by being evaluated or treated in other medical clinics. The percentage of patients participating in LTC and receiving treatment could have been underestimated. Still, we believe any discrepancy should be very low because the CGMH conducted this screening campaign and was mainly responsible for referral and anti-viral treatment in these areas. Second, the study sample size was small, so the intervention possibly cannot be generalized to a larger population. The study purpose, outreach testing capacity, and grant funding limited the number of participants who could be enrolled. The other barriers specific to a rural community study include inconvenient testing facilities and a lack of advocacy and promotion [18,19]. To scale up the screening and treatment uptake, further intervention and cascade of care should integrate local medical resources, including public health systems, primary health care, and pharmacies. Self-sampling and self-testing also can potentially increase testing coverage. Third, the cost and effectiveness of the recall programme were not analyzed. The research staff managed the programme, and we did not record and estimate the cost of conducting recall activities. Further research that includes cost-effectiveness analysis will be more informative for public policy-making.
5. Conclusions
Our study demonstrated that as long as the patient has LTC, a high treatment uptake and cure rate can be expected in the DAA era. However, disadvantaged populations still face obstacles to seeking medical treatment even after knowing that they are infected with HCV. The COVID-19 pandemic has resulted in suspension or delay of the HCV-elimination programme. To scale up the treatment coverage, performing large-scale or universal screening of a population and then linking patients to a point-of-care facility is critical. Engaging with people to increase awareness of HCV-related liver disease and scheduling specialist appointments via a recall programme has been shown to be effective. Outreach care for non-LTC patients is a way worth trying to achieve micro-elimination of HCV in the rural community.
Acknowledgments
This research is supported by the Chang Gung Memorial Hospital Research Projects CLRPG2L0052, CRRPG2H0032, CRRPG2H0033.
References
- WHO, Global hepatitis report, 2017.Geneva:World Health Organization. 2017.
- Stoove, M.; Wallace, J.; Higgs, P.; Pedrana, A.; Goutzamanis, S.; Latham, N.; Scott, N.; Treloar, C.; Crawford, S.; Doyle, J.; Hellard, M. , Treading lightly: Finding the best way to use public health surveillance of hepatitis C diagnoses to increase access to cure. Int J Drug Policy 2020, 75, 102596. [Google Scholar] [CrossRef] [PubMed]
- Chien, R. N.; Lu, S. N.; Pwu, R. F.; Wu, G. H.; Yang, W. W.; Liu, C. L. , Taiwan accelerates its efforts to eliminate hepatitis C. Glob Health Med 2021, 3, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Chien, R. N.; Lu, S. N.; Hui-Min Wu, G.; Yang, W. W.; Pwu, R. F.; Liu, C. L.; Cheng, K. P.; Chen, S. C.; Chen, C. J. , Policy and Strategy for Hepatitis C Virus Elimination at the National Level: Experience in Taiwan. J Infect Dis 2023, (Suppl 3) (Suppl 3), S180–S188. [Google Scholar] [CrossRef]
- Yu, M. L.; Yeh, M. L.; Tsai, P. C.; Huang, C. I.; Huang, J. F.; Huang, C. F.; Hsieh, M. H.; Liang, P. C.; Lin, Y. H.; Hsieh, M. Y.; Lin, W. Y.; Hou, N. J.; Lin, Z. Y.; Chen, S. C.; Dai, C. Y.; Chuang, W. L.; Chang, W. Y. , Huge gap between clinical efficacy and community effectiveness in the treatment of chronic hepatitis C: a nationwide survey in Taiwan. Medicine (Baltimore) 2015, 94, e690. [Google Scholar] [CrossRef] [PubMed]
- Zhou, K.; Terrault, N. A. , Gaps in Viral Hepatitis Awareness in the United States in a Population-based Study. Clin Gastroenterol Hepatol 2020, 18, 188–195 e4. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Clark, R.; Tu, P.; Tu, R.; Hsu, Y. J.; Nien, H. C. , The disconnect in hepatitis screening: participation rates, awareness of infection status, and treatment-seeking behavior. J Glob Health 2019, 9, 010426. [Google Scholar] [CrossRef] [PubMed]
- Denniston, M. M.; Klevens, R. M.; McQuillan, G. M.; Jiles, R. B. , Awareness of infection, knowledge of hepatitis C, and medical follow-up among individuals testing positive for hepatitis C: National Health and Nutrition Examination Survey 2001-2008. Hepatology 2012, 55, 1652–61. [Google Scholar] [CrossRef] [PubMed]
- Sun, C. A.; Chen, H. C.; Lu, S. N.; Chen, C. J.; Lu, C. F.; You, S. L.; Lin, S. H. , Persistent hyperendemicity of hepatitis C virus infection in Taiwan: the important role of iatrogenic risk factors. J Med Virol 2001, 65, 30–4. [Google Scholar] [CrossRef] [PubMed]
- Kondili, L. A.; Robbins, S.; Blach, S.; Gamkrelidze, I.; Zignego, A. L.; Brunetto, M. R.; Raimondo, G.; Taliani, G.; Iannone, A.; Russo, F. P.; Santantonio, T. A.; Zuin, M.; Chessa, L.; Blanc, P.; Puoti, M.; Vinci, M.; Erne, E. M.; Strazzabosco, M.; Massari, M.; Lampertico, P.; Rumi, M. G.; Federico, A.; Orlandini, A.; Ciancio, A.; Borgia, G.; Andreone, P.; Caporaso, N.; Persico, M.; Ieluzzi, D.; Madonia, S.; Gori, A.; Gasbarrini, A.; Coppola, C.; Brancaccio, G.; Andriulli, A.; Quaranta, M. G.; Montilla, S.; Razavi, H.; Melazzini, M.; Vella, S.; Craxi, A.; Group, P. C. , Forecasting Hepatitis C liver disease burden on real-life data. Does the hidden iceberg matter to reach the elimination goals? Liver Int 2018, 38, 2190–2198. [Google Scholar] [CrossRef] [PubMed]
- Treloar, C.; Rance, J.; Backmund, M. , Understanding barriers to hepatitis C virus care and stigmatization from a social perspective. Clin Infect Dis 2013, 57 Suppl 2, S51–5. [Google Scholar] [CrossRef]
- Aspinall, E. J.; Corson, S.; Doyle, J. S.; Grebely, J.; Hutchinson, S. J.; Dore, G. J.; Goldberg, D. J.; Hellard, M. E. , Treatment of hepatitis C virus infection among people who are actively injecting drugs: a systematic review and meta-analysis. Clin Infect Dis 2013, 57 Suppl 2, S80–9. [Google Scholar] [CrossRef]
- Schaefer, M.; Sarkar, R.; Diez-Quevedo, C. , Management of mental health problems prior to and during treatment of hepatitis C virus infection in patients with drug addiction. Clin Infect Dis 2013, 57 Suppl 2, S111–7. [Google Scholar] [CrossRef]
- Yehia, B. R.; Schranz, A. J.; Umscheid, C. A.; Lo Re, V. , 3rd, The treatment cascade for chronic hepatitis C virus infection in the United States: a systematic review and meta-analysis. PLoS One 2014, 9, e101554. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z. M.; Stepanova, M.; Afendy, M.; Lam, B. P.; Mishra, A. , Knowledge about infection is the only predictor of treatment in patients with chronic hepatitis C. J Viral Hepat 2013, 20, 550–5. [Google Scholar] [CrossRef] [PubMed]
- Viner, K.; Kuncio, D.; Newbern, E. C.; Johnson, C. C. , The continuum of hepatitis C testing and care. Hepatology 2015, 61, 783–9. [Google Scholar] [CrossRef] [PubMed]
- Bajis, S.; Dore, G. J.; Hajarizadeh, B.; Cunningham, E. B.; Maher, L.; Grebely, J. , Interventions to enhance testing, linkage to care and treatment uptake for hepatitis C virus infection among people who inject drugs: A systematic review. Int J Drug Policy 2017, 47, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Zuure, F. R.; Heijman, T.; Urbanus, A. T.; Prins, M.; Kok, G.; Davidovich, U. , Reasons for compliance or noncompliance with advice to test for hepatitis C via an internet-mediated blood screening service: a qualitative study. BMC Public Health 2011, 11, 293. [Google Scholar] [CrossRef] [PubMed]
- Seedat, F.; Hargreaves, S.; Friedland, J. S. , Engaging new migrants in infectious disease screening: a qualitative semi-structured interview study of UK migrant community health-care leads. PLoS One 2014, 9, e108261. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Prevalence rate of 6161 participants who were seropositive for HCV antibody by age and sex.
Figure 1.
Prevalence rate of 6161 participants who were seropositive for HCV antibody by age and sex.

Figure 2.
Proportion of 185 participants who were aware of their HCV infection by age and sex.
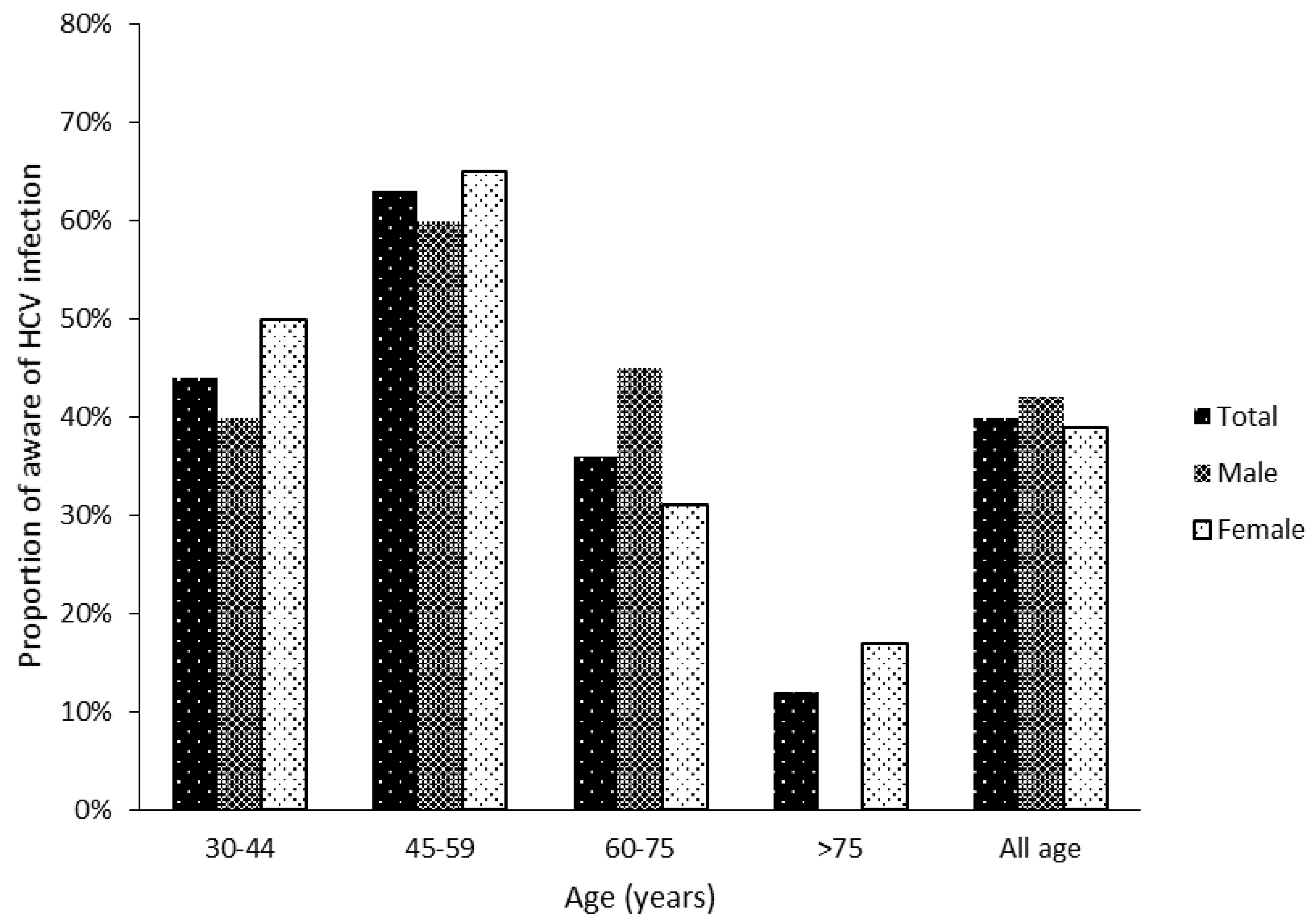
Figure 3.
The continuum of viral hepatitis services and the retention cascade after recall program. The proportion of LTC increased by 8.7 % (58.9% to 67.6%) after recall program. LTC, Link to care. RP, recall program. SVR, sustained viral response.
Figure 3.
The continuum of viral hepatitis services and the retention cascade after recall program. The proportion of LTC increased by 8.7 % (58.9% to 67.6%) after recall program. LTC, Link to care. RP, recall program. SVR, sustained viral response.
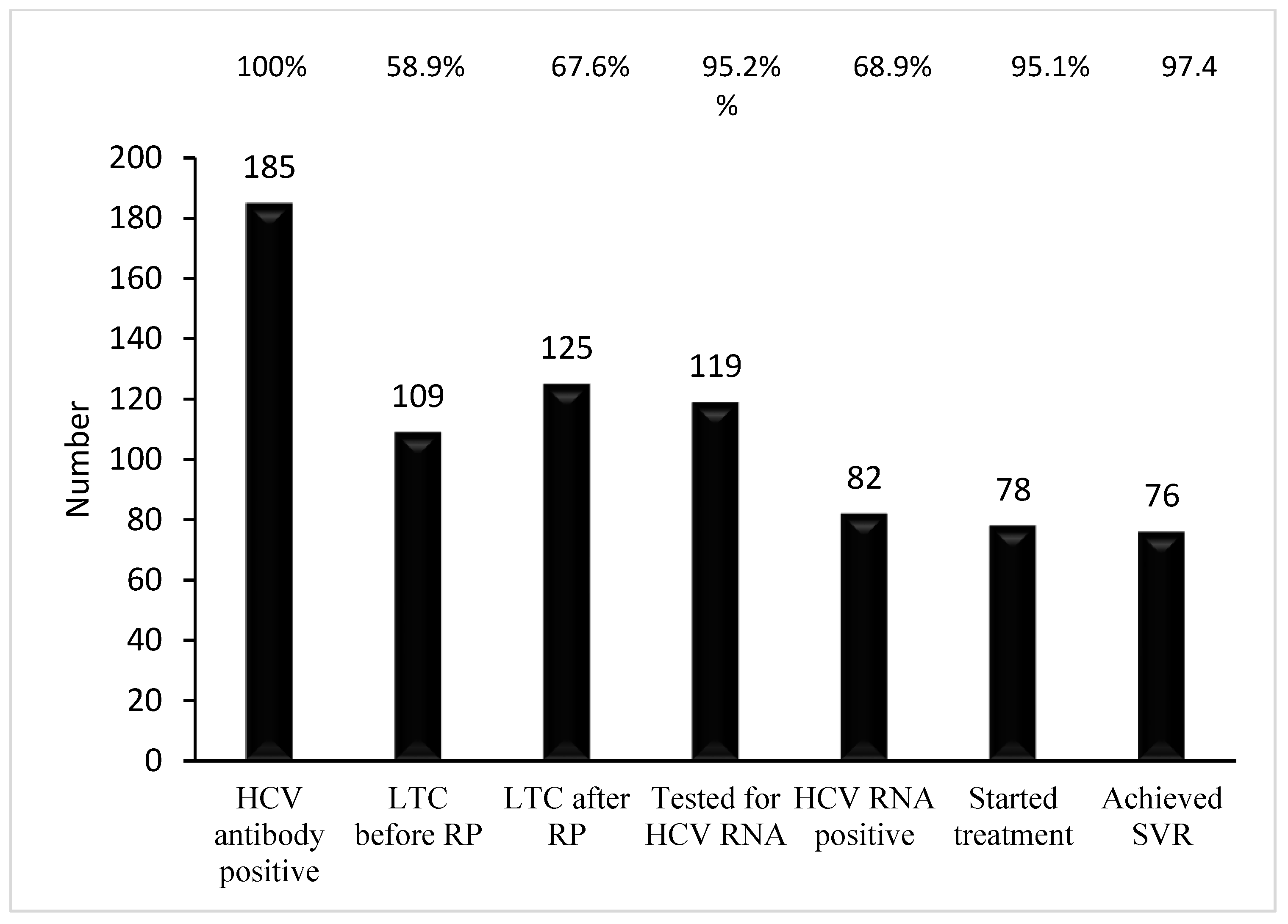

Table 1.
Comparison of baseline characteristics and clinical profiles of participants by awareness of HCV.
Table 1.
Comparison of baseline characteristics and clinical profiles of participants by awareness of HCV.
| Aware of HCV infection | |||
|---|---|---|---|
| No | Yes | P value | |
| Number | 111 | 74 | |
| Male (%) | 34(30.6) | 25(33.8) | 0.625 |
| Age, years | 67.7 ± 10.1 | 61.0 ± 8.5 | <0.001 |
| 30-44 | 5(4.5) | 4(5.4) | <0.001 |
| 45-59 | 18(16.2) | 31(41.9) | |
| 60-75 | 65(58.6) | 36(48.6) | |
| >75 | 23(20.7) | 3(4.1) | |
| BMI, kg/m2 | 25.3 ± 3.6 | 24.3 ± 3.9 | 0.075 |
| Private health Insurance, Yes (%) | 56(52.8) | 56(78.9) | <0.001 |
| Education level (%) | |||
| No education completed | 29(26.9) | 3(4.2) | <0.001 |
| Elementary school | 39(36.1) | 21(29.2) | |
| Middle school | 18(16.7) | 21(29.2) | |
| High school | 12(11.1) | 15(20.8) | |
| College and higher | 10(9.3) | 12(16.7) | |
| Live in urban area (%) | 45(40.5) | 40(54.1) | 0.071 |
| Alcohol consumption, Yes (%) | 16(14.7) | 23(32.9) | 0.04 |
| Smoking, Yes (%) | 22(19.8) | 19(26.0) | 0.322 |
| Diabetes mellitus (%) | 19(17.1) | 14(18.9) | 0.754 |
| Hypertension (%) | 44(39.6) | 25(33.8) | 0.42 |
| Hepatitis B carrier (%) | 11(10.0) | 10(13.7) | 0.442 |
| Family history of liver disease (%) | 12(10.9) | 13(17.8) | 0.183 |
| AST > 34 U/L (%) | 25(22.5) | 25(33.8) | 0.091 |
| ALT > 36 U/L (%) | 25(22.5) | 27(36.5) | 0.038 |
Table 2.
Comparison of baseline characteristics and clinical profiles of participants by linkage to care. LTC, linkage to care.
Table 2.
Comparison of baseline characteristics and clinical profiles of participants by linkage to care. LTC, linkage to care.
| Linkage to care | |||
| No | Yes | P value | |
| Number | 76 | 109 | |
| Male (%) | 26(34.2) | 33(30.3) | 0.572 |
| Age, years | 67.0±11.6 | 63.7±8.6 | 0.035 |
| BMI, kg/m2 | 24.9 ± 3.3 | 24.9 ± 4.0 | 0.982 |
| Live in urban area (%) | 28(36.8) | 57(52.3) | 0.038 |
| Education level (%) | |||
| No education completed | 21(28.8) | 11(10.5) | 0.032 |
| Elementary school | 20(26.7) | 40(38.1) | |
| Middle school | 13(17.3) | 26(24.8) | |
| High school | 11(14.7) | 16(15.2) | |
| College and higher | 10(13.3) | 12(11.4) | |
| Insurance, Yes (%) | 39(53.4) | 73(70.2) | 0.023 |
| Alcohol consumption, Yes (%) | 15(19.7) | 24(23.3) | 0.568 |
| Smoking, Yes (%) | 19(25.0) | 22(20.4) | 0.457 |
| Aware of HCV infection | 18(23.7) | 55(51.4) | <0.001 |
| Diabetes mellitus | 12(15.8) | 20(18.7) | 0.611 |
| Hypertension | 27(35.5) | 40(37.4) | 0.797 |
| Stroke | 1(1.3) | 4(3.7) | 0.322 |
| HBsAg(+) | 11(14.5) | 12(11.0) | 0.482 |
| Family history of liver disease | 13(17.1) | 12(11.2) | 0.253 |
| AST > 34 U/L | 16(21.1) | 34(31.2) | 0.127 |
| ALT > 36 U/L | 17(22.4) | 35(34.4) | 0.147 |
Table 3.
Clinical features and outcomes of participants with linkage to care.
| Percentage of LTC before recall program | 58.9(109/185) |
| Percentage of mortality | 1.6(3/185) |
| Percentage of LTC after recall program | 67.6(125/185) |
| Percentage of viremia in HCV antibody positive | 68.9(82/119) |
| Genotype (N=66), %(n) | |
| Type 1b, | 62.1(41) |
| Type 2 | 36.3(24) |
| Indeterminated | 1.5(1) |
| Fibrosis stage (N=58), %(n) | |
| F0 | 25.9(15) |
| F1 | 22.4(13) |
| F2 | 17.2(10) |
| F3 | 19.0(11) |
| F4 | 15.5(9) |
| Percentage of treatment in eligible patient | 95.1(78/82) |
| Antiviral drug, %(n) | |
| Interferon based | 46.2(36) |
| Interferon based then DAA | 3.8(3) |
| DAA | 53.8(39) |
| End of treatment response, % | 100(78/78) |
| Sustained viral response, % | 97.4(76/78) |
| Cured rate of eligible patient % | 92.7(76/82) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



