
Submitted:
09 June 2024
Posted:
11 June 2024
You are already at the latest version
Abstract
Introduction:
Gastric cancer (GC) is one of the most frequently diagnosed cancers in the world. Although the incidence is decreasing in developed countries, treatment results are still unsatisfactory. The standard treatment for locally advanced gastric cancer (LAGC) is gastrectomy with perioperative chemotherapy.
Aim:
Assessment of selected microRNAs (miRNAs) in chemoresistance in archival material from LAGC.
Material and method:
The research group consisted of archival material from 10 patients with LAGC. Histological material from each patient was used from a biopsy performed during gastroscopy and after surgery preceded by 4 cycles of neoadjuvant chemotherapy (NAC) according to the FLOT or FLO regimen. The expression of selected miRNAs was assessed in the tissue material, such as miRNA-21-3p, miRNA-21-5p, miRNA-106a-5p, miRNA-122-3p, miRNA-122-5p, miRNA-143-3p, miRNA-143-5p, miRNA-203a-3p, miRNA-203-5p, miRNA-551b-3p, miRNA-551b-5p and miRNA-574-3p. miRNA expression was assessed by quantitative chain reaction polymerase reverse transcriptase (qRT-PCR). The response to NAC was assessed by computed tomography of the abdomen, chest and histopathology after gastrectomy. The statistical analyses were performed using GraphPad Prism 9.The significance limit was set at p
Keywords:
microRNAs
; locally advanced gastric cancer
; pathological staging
; clinical staging
; neoadjuvant chemotherapy
1. Introduction
Gastric cancer (GC) is the fifth most common cancer in terms of incidence and the fourth most common cause of death [1]. The incidence and mortality of GC are decreasing in developed countries, although it is still a significant problem in East Asia and Europe [1,2]. Additionally, an increase in the incidence in people <50 years of age has been recently demonstrated [3]. Despite progress in the treatment of patients with GC, the results are still unsatisfactory [4]. In the early stages of GC according to the TNM and UICC classification, endoscopic or surgical R0 resection is recommended. This is the only treatment option that allows for cure. The 5-year overall survival (OS) rate ranges from 93.6% to 94.2% [5]. Patients with early-stage GC may be asymptomatic. Only patients with advanced GC may experience weight loss, abdominal pain, vomiting, dysphagia, and upper gastrointestinal bleeding. Therefore, patients with advanced GC are more often diagnosed [6,7]. The standard treatment for locally advanced GC is perioperative chemotherapy [8,9,10,11]. The first breakthrough study that confirmed the effectiveness of perioperative chemotherapy was the MAGIC (Medical Research Council Adjuvant Gastric Infusional Chemotherapy) study published in 2006. It was shown that perioperative chemotherapy with epirubicin, cisplatin and fluorouracil or capecitabine (i.e., ECF/ECX regimens) improved overall survival (OS) by 13% compared to surgery alone [8]. This was followed by subsequent studies that clearly demonstrated the superiority of neoadjuvant docetaxel, oxaliplatin, fluorouracil, and leucovorin (FLOT) over ECF/ECX in terms of pathological response and OS. These studies are the basis for current standards using perioperative chemotherapy in locally advanced GC [9,10]. Although perioperative chemotherapy has become the standard for patients with LAGC, only 50–65% of patients who undergo neoadjuvant chemotherapy followed by surgical removal receive postoperative chemotherapy [8,9,12]. Chemotherapy according to the FLOT regimen carries many complications. Which leads to reflection on the use of greater selection of patients with LAGC for perioperative chemotherapy. Van Putten et al. demonstrated improved OS in patients who underwent perioperative treatment compared with those who underwent preoperative treatment [13]. On the other hand, in a more recent analysis, median OS was similar between patients who received adjuvant chemotherapy (AC) and those who did not [14]. Consideration should also be given to patients who did not benefit at all from perioperative chemotherapy, that is, patients who did not respond to neoadjuvant chemotherapy. One of the main causes is the development of drug resistance, which results in the failure of chemotherapy. Drug resistance can be divided into innate and acquired. Resistance mechanisms include inhibition of cell apoptosis, changes in the cell cycle, changes in drug efflux, enhanced DNA damage repair, and dysregulation of epithelial mesenchymal transformation (EMT). However, the detailed mechanisms involved in drug resistance are still unknown [15]. Therefore, our research aims to search for a biomarker that will allow us to identify patients with LAGC who will benefit from perioperative chemotherapy. Aberrantly expressed miRNAs are potential biomarkers for assessing potential chemoresistance in patients with GC. MicroRNAs (miRNAs) are a class of small non-coding nucleic acids. MiRNAs act as master regulators in the control of gene expression. We currently know over 2,600 human-specific miRNAs [16,17,18,19]. Dysregulation is associated with apoptosis, cancer cell proliferation, invasion and metastasis [20,21,22]. Aberrantly expressed miRNAs are potential biomarkers for assessing potential chemoresistance in patients with GC [23,24].
2. Results
2.1. Expression Levels of miRNA in GC Patients Based on The Cancer Genome Atlas
Using data from The Cancer Genome Atlas (TCGA), the expression of selected miRNAs was determined based on the expression levels of miRNA-21-3p, miRNA-21-5p, miRNA-106a-5p, miRNA-122-3p, miRNA-122-5p, miRNA-143-3p, miRNA-143-5p, miRNA-551b-3p, miRNA-551b-5p and miRNA-574-3p in 372 patients with GC and in 32 controls of normal stomach tissue. The data showed that five of our selected miRNAs are expressed in GC. We considered FDR < 0.25 and p-value < 0.05. According to the ENCORI database we observed up-regulation of miRNA-21-3p (p = 1.83E-68), miRNA-21-5p (p = 6.0E-24), miRNA-106a-5p (p = 0.00099), and down-regulation of miRNA-143-5p in cancer than in normal controls. No differences were noted for miRNA-122-3p, miRNA-122-5p, miRNA-143-3p, miRNA-551b-3p, miRNA-551b-5p and miRNA-574-3p.
Moreover, no information was found in the database about miRNA-203a-3p and miRNA-203a-5p. Only the graph included in the graphic was found. All data is presented in Table 1 and Figure 1.
Next, using the UALCAN database we checked the differences in the expression levels of miRNA-21, miRNA-106a, miRNA-122, miRNA-143, miRNA-203a, miRNA-551b and miRNA-574 depending on clinicopathological parameters in GC patients included in the TCGA project. First of all we checked the expression levels of those miRNAs in primary tumor (n= 387) in comparison to normal samples (n = 40). We observed upregulation of miRNA-21 (284’544.649 RPM vs 51’556.679 RPM, p < 10e-12), miRNA-106a (9.102 RPM vs 8.111 RPM, p = 0.000077), and down-regulation of miRNA-143 (148’026.827 RPM vs 452’590.255 RPM, p = 0.00000002) and miRNA-551b (0.691 RPM vs 1.103 RPM, p = 0.000077). No differences were observed for miRNA-122, miRNA-203a and miRNA-574 (p > 0.05). Moreover, no differences (p > 0.05) in the case of miRNA-122, miRNA-203a and miRNA-574 and all analyzed clinicopathological parameters were indicated. Expression levels of miR-21 differ in GC patients for I vs III cancer stages (p = 0.0112) as well as between adenocarcinoma diffuse and intestinal adenocarcinoma tubular (p = 0.0438). Surprisingly, miRNA-106a was the most changes in the expression levels depending on patients’ race (Caucasian vs Asian, p = 0.0160) and age (21-40 vs 41-60, p = 0.0431; 21-40 vs 61-80, p = 0.0081 and 61-80 vs 81-100, p = 0.0172). Similarly, miRNA-143 and miRNA-203a differ in the groups of patients between 41-60 vs 61-80 years of ages (p = 0.0092 and p = 0.0067, respectively). When we look into tumor grade, only for patients with G2 vs G3, differences in the expression levels for miRNA-143 and miRNA-203a were noticed (p = 0.0018 and p = 0.0242, respectively). Expression level of miRNA-203a was also associated with nodal metastasis status and differs depending on N0 vs N3 (p = 0.0047) as well as N1 vs N3 (p = 0.02911). For both of miRNAs, miRNA-143 and miRNA-203a, differences in expression levels between: adenocarcinoma NOS vs intestinal adenocarcinoma tubular (p = 0.000002 and p = 0.04314, respectively), adenocarcinoma diffuse vs intestinal adenocarcinoma tubular (p = 0.00004 and p = 0.0056, respectively), intestinal adenocarcinomas NOS vs tubular (p = 0.02458 and p = 0.02216, respectively) and intestinal adenocarcinomas mucinous vs tubular (p = 0.00846 and p = 0.01260, respectively) were noticed. Moreover, we indicated differences between adenocarcinoma NOS vs intestinal adenocarcinoma mucinous (p = 0.02212) and intestinal adenocarcinomas mucinous vs tubular (p = 0.00634) for miRNA-106a, between adenocarcinoma diffuse vs intestinal adenocarcinoma papillary (p = 0.0082) for miRNA-143; and between adenocarcinomas NOS vs signet ring (p = 0.00184), adenocarcinoma signet ring vs intestinal adenocarcinoma NOS (p = 0.0052) as well as adenocarcinoma signet ring vs intestinal adenocarcinoma tubular (p = 0.0001) for miRNA-203a. The last parameter, TP53 mutation status was associated with differences in the expression levels of only miRNA-143 (p = 0.006). All data is presented in Table 2 and in the UALCAN database website (accessed on 7 June 2024).
2.2. Expression Levels of miR-143, miR-143* and miR-574-3p before and miR-143* and miR-574-3p after Surgery Are Up-Regulated in GC Patients
First of all, we checked the expression levels of the panel miRNAs named, miRNA-21-3p, miRNA-21-5p, miRNA-106a-5p, miRNA-122-3p, miRNA-122-5p, miRNA-143-3p, miRNA-143-5p, miRNA-203a-3p, miRNA-203-5p, miRNA-551b-3p, miRNA-551b-5p and miRNA-574-3p before, biopsy performed during gastroscopy, and after surgery preceded by 4 cycles of neoadjuvant chemotherapy according to the FLOT or FLO regiment and in normal samples taken from healthy individuals. Only in the case of miRNA-143-5p, miRNA-143-3p, and miRNA-574-3p we observed significant down-regulation of those three miRNAs in patients before treatment in comparison to the normal samples taken from healthy individuals (p = 0.0117, p = 0.0434 and p = 0.0062, respectively). When we compared the changes in miRNA expression after treatment to the normal samples, significant changes were observed only in the case of miRNA-143-3p and miRNA-574-3p (p = 0.0325 and p = 0.0253, respectively). For the rest of analyzed miRNAs no differences (p > 0.05) were indicated. All results are presented in Figure 2. The expression level of all determined miRNAs was not related to age, gender or location of GC.
2.3. miR-143, miR-143* and miR-574-3p Have Potential as a Diagnostic Marker in GC Patients
Next, we checked if miRNA-143-5p, miRNA-143-3p, and miRNA-574-3p have potential as diagnostic marker and receiver operating characteristic curve (ROC) analyses of those three miRNAs in patients’ samples taken before and after surgery were compared to the normal samples taken from healthy, non-cancer individuals, and area under the ROC curve (AUC) with with 95% CI (confidence interval) as well as sensitivity and specificity were calculated. We indicated miRNA-143-5p (AUC = 0.8500, 95% CI = 0.6459 to 1.000, p = 0.0129), miRNA-143-3p (AUC = 0.7875, 95% CI = 0.5404 to 1.000, p = 0.0410), and miRNA-574-3p (AUC = 0.9500, 95% CI = 0.8310 to 1.000, p = 0.0084), that displayed high ability as a potential diagnostic marker for distinguishing patients’ before treatment in comparison to healthy, Figure 3A.
2.4. miR-143 Could Be Used for Assessment of Therapy Response in GC Patients
In the analysis of the entire group of patients, comparing the miRNA level before and after adjuvant chemotherapy, we can demonstrate that miR-143 could be a potential biomarker in response to chemotherapy, although it should be noted that not all cases showed histopathological and clinical improvement. A detailed analysis taking into account this data is provided in the point below. miR-143 showed a reduced expression level compared to the material after surgery, i.e., after chemotherapy. However, these data did not show statistical significance. We can notice a similar relationship in miR-574-3p. However, after additional analysis using receiver operating characteristic curve (ROC) of miR-21, miR-143 and miR-574-3p in patients’ samples taken before and after surgery and whiskers with 5-95 percentile, Wilcoxon matched-pairs signed rank the test showed that miR-143 may be a potential biomarker of response to chemotherapy in LAGC. The other miRNA expressions were far from statistical significance in this analysis.
2.5. miR-551b* Could Be Used for Assessment of Therapy Response in GC Patients—Better Than CT Scan?
We also assessed miRNAs expression in each patient and assessed the correlation with response to NAC according to the FLOT or FLO regimen. Responses to NAC were taken into account: histopathological (HP) and imaging, i.e., assessed on the basis of computed tomography (CT). The expression of miR-143-3p, miR-143-5p, miR-203a-3p and miR- 551b-5p were found to be statistically significant in individual patients with response to NAC asseded by CT or/and HP (p>0.05). One patient had miR-14-3p3 expression with a CT and HP response to NAC, three patients had miR-143-5p and miR-203a-3p expression with a CT and HP response to NAC. Additionally, miR-551b-5p expression was demonstrated in four cases, three cases were with CT and HP response to NAC, but in one case, with CT scan was asseded the disease progressed, although the postoperative material showed high-grade regression in this patient. No expression were observed for miR-21-3p, miR-21-5p, miR-106a-5p, miR-122-3p, miR-122-5p, miR-203a-5p, miRNA-551b-3p and miR-574-3p in all cases (p > 0.05).
3. Discussion
To date, more than 2600 miRNAs have been identified, and some of them are significantly associated with tumorigenesis, cancer invasion, metastasis and also apoptosis in GC [30]. A recent study demonstrated that one single miRNA could act as an oncogenic miRNA as well as tumor suppressor miRNAs which seem to have a significant role in drug resistance [31]. The relationship between miRNA expression and sensitivity of GC to chemotherapeutic drugs is studied extensively. We chose seven GC-related miRNAs for our study: miRNA-551b-3p, miRNA122, miRNA-21, miRNA-106a, miRNA-143, miRNA-574-3p and miRNA-203. In addition, selected miRNAs were either already tested for chemoresistance to selected drugs, but different from our chemotherapy regimens, or were associated with the development of metastasis in GC. The miRNAs associated with metastases may also play a major role in chemoresistance, as both develop neoplasms. And miRNAs previously tested for chemoresistance to other drugs may also play a role in the FLOT and FLO regimens.
3.1. miRNA-21
MicroRNA-21 (miR-21) is one of the most frequently studied oncomiRNAs. It has been proved that phosphatase and tensin homologue is the direct target of miR-21 whose expression is elevated in GC tissues and GC derived cell lines [32]. Chan et al. demonstrated that miR-21 was overexpressed in GC tissues of 92% patients compared to normal counterparts [33]. In addition, overexpression of miR-21 is associated with worse tumor differentiation, lymph node metastasis, and TNM stage. The TCGA database showed upregulation levels of miR-21-3p and miR-21-5p in patients with GC. Moreover, the UALCAN database showed the expression of miR-21 differ in GC patients for I vs III cancer stages. Differences in expression in stages may be helpful in the correct staging of the patient with LAGC, if CT scan is ambiguous. Our research not confirmed this information. We have not demonstrated expression of miR-21-3p and miR-21-5p in GC. The discrepancy in the results of our study and that of others may be related to the material examined or the small number of cases. Due to the inconsistency, studies involving this miRNA should be continued to clearly indicate its role in the development of GC.
3.2. miRNA-106a-5p
Overexpression of the tumor suppressor LnCRNA GAS5 inhibits GC development by percolating miR-106a-5p through the Akt/mTOR pathway. Decreased levels of GAS5 and increased levels of miRNA-106a-5p were demonstrated in cell lines and GCs. GAS5 level was significantly inversely correlated with miRNA-106a-5p level in GC. Additionally, it has been shown that GAS5 binds to miRNA-106a-5p and negatively regulates its expression in GC cells. GAS5 overexpression inhibits GC cell proliferation, migration, and invasion and promotes apoptosis. Moreover, overexpression of miRNA-106a-5p reverses the functional effects induced by GAS5 overexpression. In vivo, GAS5 overexpression inhibited tumor growth by negatively regulating miRNA-106a-5p expression. Additionally, in vitro and in vivo, GAS5 overexpression inactivates the Akt/mTOR pathway by suppressing miRNA-106a-5p expression [34]. Other studies have shown that hypermethylation of TFAP2E results in its reduced expression and chemoresistance to 5-FU in GC cells. And strong expression of miRNAs miR-106a-5p and miR-421 regulated chemoresistance induced by TFAP2E methylation [35]. Furthermore, in GC, upregulated miRNA-106a is associated with GC size, stage, lymph nodes and distant metastasis [36,37]. The TCGA database also showed overexpression of miR-106a in GC compared to normal tissue. Moreover, we checked UALCAN database that miRNA-106a was shown the most changes in the expression levels depending on patients’ race and age. We have not demonstrated a statistically significant relationship between the expression of miR-106a and the development of GC in our results. The discrepancy in the data may be related not only to the difference in material use, but also to the action of miR-106a. The cited studies indicate that miR-106a influences the development of GC by taking part in complex cellular pathways. Perhaps we should follow this lead in research to determine the roles of miR-106a in GC. However, it is worth considering whether miRNA-106a will be an appropriate tool for the diagnosis of GC or response to NAC in patients with LAGC. The high variability of expression levels depending on age and race rather excludes this parameter as a potential biomarker.
3.3. miRNA-122
MicroRNA-122 (miR-122) acts as a tumor suppressor in various cancers including GC. Meng et al. showed in their study a low level of miR-122-5p expression in GC tissues and cell lines. Additionally, miR-122-5p overexpression was shown to inhibit GC cell proliferation, migration, and invasion by targeting LYN. The expression of LYN, a Src family tyrosine kinase, was inversely correlated with the expression of miR-122-5p in GC tissues [34]. Further, decreased miR-122 expression is directly involved in the induction of cisplatin (CDDP) resistance by increasing excision repair cross-complementing 1 (ERCC1) expression [35]. The TCGA database not shown miR-122 expression in GC. Our research also confirmed this. The discrepancies may result from the type of material used for testing and the detection tool used.
3.4. miRNA-143
Overexpression of miR-143 has a negative effect on MKN-45 cell proliferation and invasion. Additionally, downstream targets of miRNA-143 were assessed and GC cells showed reduced expression of K-Ras, MMP9 and C-Myc and increased expression of Bax, caspase-3 and caspase-9 [36]. Data from TCGA also showed decreased hsa-miR-143-3p expression in GC compared to normal tissue. miR-143-3p is detected in both tumor tissue and plasma. Which makes it an even more interesting potential biomarker for GC detection [39]. miR-143 is involved in the development of cisplatin resistance via IGF1R and BCL2. miR-143 expression is decreased in human GC cell lines and in the cisplatin-resistant GC cell line SGC7901/cisplatin (DDP). Additionally, it is related to an increase in the levels of IGF1R and BCL2, compared to the parent SGC7901 cell line. Which I suggest is that they are target genes of miR-143. Overexpression of miR-143 sensitizes SGC7901/DDP cells to cisplatin-induced apoptosis and inhibits proliferation [40]. miR-143 as a potent inhibitor of autophagy enhances chemosensitivity of Quercetin through autophagy inhibition via target GABARAPL1 in GC cells [41]. Decreased miR-143-3p expression correlates with late stage and lymph node metastasis. Additionally, miR-143-3p negatively regulates cell growth, apoptosis, migration, and invasion by directly targeting the AKT2 gene [42]. The TCGA database demonstrated decrease expression of miR-143-5p in GC patients. Our studies confirm the involvement of miR-143 in the development of GC. In our study, we showed decreased expression levels of miR-143-3p, miR-143-5p preoperatively, and miR-143-3p postoperatively after NAC in LAGC patients. After additional analyses, it was shown that miR-143-3p and miR-143-5p may be a potential tool for detecting GC. All data indicate an important role of miR-143-3p and miR-143-5p in the development of GC. Further studies are needed to more specific identify the roles of miR-143-3p and miR-143-5p in the development of GC. And in the future, it could be use in clinical practice.
3.5. miRNA-203a
Many studies show that miR-203a inhibits invasion, growth, and metastasis by regulating multiple pathways in GC. Studies indicate that miR-203a-3p is decreased in both GC tissues and cell lines. Moreover, overexpression of miR-203a-3p reduced GC cell proliferation and cell cycle progression in vitro. In GC cells, miR-203a-3p can inhibit tumor development by negatively regulating IGF-1R expression. In GC cells, an insulin-like growth factor 1 receptor (IGF-1R) is a target mediator of miR-203a-3p [43]. Other studies show that miR-203a expression was decreased in GC. Moreover, miR-203 expression was associated with the radiosensitivity of GC cells by promoting cell apoptosis in GCs subjected to radiotherapy by targeting Zinc finger E-box binding homeobox 1 (ZEB1) [44]. In GC downregulated miR-203, are associated with gastric tumor size, stage, lymph nodes and distant metastasis [37,38]. The TCGA database were not shown numerical data on miR-203a-3p and miR-203-5p in GC. Only graphic forms were revealed. In our studies have not demonstrated expression of miR-203a in patients with GC. However, a detailed analysis were shown that miR-203a overexpression was observed in three patients with a response to NAC according to the FLOT or FLO regimen. Data about miR-203a are incomplete and divergent. However, these data provide hope and should encourage further research to clearly assess the role of miR-203a in assessing response to NAC in LAGC.
3.6. miRNA-551b
Guo et al. demonstrated that the LncRNA-GC1-miRNA-551b-3p-dysbindin signaling pathway can serve as a predictor of response to oxaliplatin. lncRNA-GC1 and miRNA-551b-3p were elevated in chemotherapy-resistant GC. miR-551b-3p binds to the noncoding region of dysbindin mRNA, thereby negatively regulating the expression of dysbindin, which is involved in chemoresistance in GC cells. Additionally, it has been shown that IncRNA-GC1 increases chemoresistance in GC through competitive binding with miR-551b-3p [45]. A recent study reported that the miR-551b-3p directly binds to the intronic region of dysbindin mRNA and negatively regulates the expression and is involved in Platinum resistance in GC cells [35]. The analyzed TCGA database showed an increased level of miR-551b-3p in GC patients compared to normal tissue. The analyzed TCGA database showed an increased level of miR-551b-3p in GC patients compared to normal tissue. Interestingly, we have not demonstrated overexpression of miR-551b-3p or miR-551-5p in GC patients. The statistical data have not demonstrated a potential role of miR-551b in response to NAC in GC or as a potential biomarker in the detection of GC. However, after analyzed the individual cases, miR-551b-5p was showed increased levels of expression in four patients. Additionally, two patients showed discordant response to NAC in LAGC on CT and HP. CT scan showed a higher stage GC than HP examination, and even in one case CT showed progression and HP examination showed complete regression of GC in the same case. Unfortunately, it is a very common case described in the literature that the response to NAC in patients with LAGC on CT, although it is the standard of care, is incorrectly assessed compared to HP examination in LAGC. This may even lead to incorrect disqualification of the patient from radical treatment, which is why it is so important to find a new, more precise tool to asses to response to NAC in GC. The UALCAN database have not shown statistically significant differences in expression of miRNA-551b-5p between clinical stages of GC. However, the staging of GC described by UALCAN database were only clinical. Our study was more detailed and drew attention to the problem of inconsistency between clinical stage and pathological stage in GC after NAC. Therefore the results may be diffrent. Our data are innovative, although we need larger case studies to evaluate the role of miR-551b-3p and the role of miR-551b-5p in response to NAC in LAGC.
3.7. miRNA-574
miR-574-5p is involved in GC by promoting angiogenesis [46]. Under hypoxic conditions, the expression level of miR-574-5p increases. Inhibition of miR-574-5p reduces the expression of endothelial growth factor A (VEGFA) [46,47]. Furthermore, Wang et al. showed that overexpression of miR-574-3p reduced the migratory and invasive properties of the GC cells and inhibited the EMT and enhanced cisplatin sensitivity in GC cells by suppressing in vitro and in vivo [48]. Additionally a study has shown that the reduced expression of miR-574–3p occurs mainly in the early stages of GC or in cancers with a high level of differentiation, suggesting that it may be used as a marker for mild cases of GC [49]. Zhiwu et al. showed that miR-574-3p was overexpressed in GC tissues and cells. miR-574-3p targeted CUL2 to increase HIF-1α expression, affecting GC progression [50]. The TCGA database have not shown increased miR-574 values in GC. In our studies, on the contrary, we showed a statistically significantly increased miR-574-3p expression level before and after surgery in patients with GC. Additional analyzes demonstrated the potential role of miR-574-3p as a tool for GC diagnosis.
4. Materials and Methods
4.1. Patients’ Criteria Included in the Study and Samples Preparation
We collected 98 histologically confirmed LAGC patients between Jan. 2018 and Dec. 2022. Patients had to meet the inclusion criteria described below and had to not meet the exclusion criteria also described below. Finally, 10 patients with LAGC were included in the analysis. We required two histological materials from LAGC from each selected patient. The first histological material came from a biopsy taken during gastroscopy. This was the material on which the diagnosis of LAGC was made. Then, these patients were qualified for perioperative chemotherapy. These patients received 4 cycles of neoadjuvant chemotherapy according to the FLOT or FLO regimen. Further histological material from GC was obtained from these patients after radical gastrectomy. The eligibility criteria were as follows: preoperative cT2–4, histologically proven adenocarcinoma, neoadjuvant chemotherapy according to the FLOT or FLO regimen, complete clinical records and no distant metastasis such as liver, lung or bone. The exclusion criteria were: previous history of other cancers and received preoperative radiotherapy. Patients qualified for neoadjuvant chemotherapy received either the FLOT or FLO regimen every 2 weeks depending on their clinical condition. FLOT regimen consisting of docetaxel (60 mg/m2), oxaliplatin (85 mg/m2), leucovorin (200 mg/m2), and 5- fluorouracil (2.600 mg/m2 as a 24 hr infusion), all given on day 1. and FLO regimen without docetaxel. Patients received 4 cycles prior to elective surgery. Patients underwent imaging evaluation CT after neoadjuvant chemotherapy. If the tumor size decreased or was stable, the operation was performed at the earliest available time in the Department of Oncological Surgery. Response to chemotherapy, were evaluated by CT scan after four cycles according to RECIST criterion v 1.1, and compared with the baseline CT scan performed before treatment. Additional responses to chemotherapy were evaluated in histological postoperative material. The control group was composed of 7 tissue materials from gastric without cancer. The material was obtained during gastrectomy. Studies were carried out on a group of 6 men and 4 women with GC. Patients’ ages ranged from 40 to 77 years, and the mean age of patients was 61 years (Table 3).

Table 3.
Basic patients’ characteristics included into study; n - number of cases, G - grade, FLOT - chemotherapy with docetaxel, oxaliplatin, and fluorouracil/leucovorin FLO - chemotherapy with 5-FU, leucovorin, and oxaliplatin.
Table 3.
Basic patients’ characteristics included into study; n - number of cases, G - grade, FLOT - chemotherapy with docetaxel, oxaliplatin, and fluorouracil/leucovorin FLO - chemotherapy with 5-FU, leucovorin, and oxaliplatin.
| Variable | All patients (n = 10) |
|
|---|---|---|
| Age [mean] | 61 years | |
| Sex | Female | 4 (40%) |
| Male | 6 (60%) | |
| Localization | Corpus | 5 (50%) |
| Cardia | 5 (50%) | |
| Grade before chemotherapy | G1 | 1 (10%) |
| G2 | 4 (40%) | |
| G3 | 5 (50%) | |
| Grade after chemotherapy | G1 | 3 (30%) |
| G2 | 1 (10%) | |
| G3 | 3 (30%) | |
| Gx | 5 (50%) | |
| Chemotherapy | FLOT | 6 (60%) |
| FLO | 4 (40%) | |
Table 4.
Basic patients’ characteristics – cTNM, ycTNM and ypTNM, T-Tumor, N- Lymph Node, M- Metastasis, c-clinical, p-pathological, ny-post therapy stages.
Table 4.
Basic patients’ characteristics – cTNM, ycTNM and ypTNM, T-Tumor, N- Lymph Node, M- Metastasis, c-clinical, p-pathological, ny-post therapy stages.
| Variable | cTNM | ycTNM | ypTNM | |
|---|---|---|---|---|
| Stage | T0 T1 |
0 0 |
2 (20%) 0 |
5 (50%) 2 (20%) |
| T2 | 1 (10%) | 0 | 0 | |
| T3 | 4 (40%) | 4 (40%) | 3 (30%) | |
| T4 | 5 (50%) | 4 (40%) | 0 | |
| Lymph nodes | N0 | 3 (30%) | 6 (60%) | 7 (70%) |
| N1 | 3 (30%) | 2 (20%) | 2 (20%) | |
| N2 | 3 (30%) | 1 (10%) | 0 | |
| N3 | 1 (10%) | 1 (10%) | 1 (10%) | |
| Metastasis | M0 | 10 (100%) | 10 (100%) | 10 (100%) |
| M1 | 0 | 0 | 0 | |
4.2. Ethical Issues
The study was carried out with the approval of the local ethics committee and is based on archival material - formalin-fixed paraffin-embedded tissue (FFPET) sections’ blocks from surgical specimens. All analyzes included in this study do not bear any traces of a medical experiment in accordance with the law in the Republic of Poland.
4.3. Sample Preparation
All samples were clinically and histologically confirmed by pathologists based on tumor testing performed on formalin-fixed paraffin-embedded tissue (FFPET) sections’ blocks from surgical specimens, using hematoxylin and eosin (H&E) histological stains and rated by microscopic observation. Next, cancer cells were marked on the on FFPET sections’ blocks and sliced to the parts about 10 μm thickness for RNA isolation.
4.4. Total RNA Isolation
Total RNA from FFPET slides were isolated using GeneMATRIX FFPE RNA Purification Kit (EURx Sp. z o.o., Gdansk, Poland) according to manufacturers’ protocol. Briefly, one FFPET tissue preparation was approximately 10 μm thick and formaldehyde/paraffin was removed by dissolving and removing the paraffin using xylene/heptane/methanol method. After removing the supernatant, the pellet was allowed to dry and the RNA isolation procedure began. Dry tissue pellets were suspended in Lyse ALL solution, mixed and Proteinase K were added and incubated in 56°C and then in 80°C. Samples were cooled and centrifuged at maximum speed. Obtained supernatants were transferred to the new tube and incubated with RL buffer, and next 96-100% ethyl alcohol were added and mixed. All were transferred into the homogenization mini columns and centrifuged. Next, columns were washed using Wash RNA buffer and centrifugation. To the obtained supernatant, DNRII buffer and DNase I were added, and incubated, after that RL buffer and 96-100% ethyl alcohol were added and mixed. Prepared mixes were transferred to the RNA-binding mini-column, washed twice by Wash buffer and centrifugation. Completely dry spin columns were placed in new Eppendorf tubes and RNase-free water and centrifugation were applied to release RNA molecules.
Next, the quality and quantity of isolated RNA samples were examined using the NanoDrop 2000 spectrophotometer (Thermo Scientific, Waltham, MA, USA). After that RNA was stored in -80°C until used.
4.5. Assessment of miRNA Expression Levels
We used a preselected panel of 12 miRNAs, composed of miRNA-21-3p (MIMAT0004494, assay ID: 002438), miRNA-21-5p (MIMAT0000076, assay ID: 000397), miRNA-106a-5p (MIMAT0000103, assay ID: 002169), miRNA-122-3p (MIMAT0004590, assay ID: 002130), miRNA-122-5p (MIMAT0000421, assay ID: 002245), miRNA-143-3p (), miRNA-143-5p (MIMAT0000435, assay ID: 002249), miRNA-203a-3p (MIMAT0000264, assay ID: 000507), miRNA-203a-5p (MIMAT0031890, assay ID: 477013_mat), miRNA-551b-3p (MIMAT0003233, assay ID: 001535), miRNA-551b-5p (MIMAT0004794, assay ID: 002346) and miRNA-574-3p (MIMAT0003239, assay ID: 002349), and U6 snRNA (NCBI Accession: NR_004394, assay ID: 001973) as reference gene, which are the commercially available primers from TaqMan™ MicroRNA Assay (Catalog number: 4427975, Applied Biosystems, Foster City, CA, USA). miRNA expression levels were defined by a two-step qRT-PCR method, using TaqMan microRNA Assay (Applied Biosystems, Foster City, CA, USA), according to the manufacturer’s protocol and as described previously [25] using LightCycler 96 thermocycler (Roche, USA).
4.6. miRNA Calculation
The miRNA expressions were analyzed by quantitative reverse transcriptase polymerase chain reaction (qRT-PCR). Profiles of miRNA were prepared using preoperative biopsies without prior therapy and the next after neoadjuvant therapy (ie. we used the material after surgery -LAGC). Obtained cycle threshold (CT) values were calculated using the 2−ΔCT method and normalizing against the mean of U6 snRNA expression for each sample as described previously [26]. The chosen TaqMan microRNA Assay enables the determination of the level of mature forms of miRNA and their differentiation with an accuracy of one nucleotide in the sequence of the tested miRNA with high accuracy and sensitivity [27].
4.7. Databases
For assessment of expression levels of miRNA-21-3p (MIMAT0004494), miRNA-21-5p (MIMAT0000076), miRNA-106a-5p (MIMAT0000103), miRNA-122-3p (MIMAT0004590), miRNA-122-5p (MIMAT0000421), miRNA-143-3p (MIMAT0000435), miRNA-143-5p (MIMAT0004599), miRNA-203a-3p (miRNA-203-3p; MIMAT0000264), miRNA-203-5p (), miRNA-551b-3p (MIMAT0003233), miRNA-551b-5p (MIMAT0004794) and miRNA-574-3p (MIMAT0003239) in stomach adenocarcinoma (STAD) patients and in normal samples we used ENCORI database presented as log2 [RPM+0.01] [28] (accessed on 7 June 2024), which is based on included in the TCGA project. Moreover, differences in the miRNAs expression levels (RPM, reads per million) depending on clinicopathological parameters including sample type, race, gender, age, cancer stage, tumor grade, nodal metastasis status, tumor histology, and TP53 mutation status of STAD patients were taken and analyzed from the UALCAN database (accessed on 7 June 2024). Only data of miRNAs named there as miRNA-21, miRNA-106a, miRNA-122, miRNA-143, miRNA-203a, miRNA-551b and miRNA-574 were available [28].
The data used and presented in this study are openly available at the TCGA-based databases and do not violate any copyrights.
4.8. Statistical Analysis
We used GraphPad Prism9 (GraphPad, San Diego, CA, United States) for calculation of all statistical analyses. T-test, Mann-Whitney U test, were used depending on data normality estimated using the Shapiro-Wilk normality test. All t-tests and ANOVA tests were performed as two-tailed and considered significant at p < 0.05, similarly as described previously [29].
5. Conclusions
miR-143-3p, miR-143-5p and miR-574-3p have potential as diagnostic markers in GC patients. miR-143-3p, miR-143-5p and miR-551b-5p may be used to assess the response to NAC according to FLOT or FLO regimen in patients with LAGC. However, the most noteworthy is miR-551b-5p, the expression of which could correctly assess the response to NAC. miR-551b-5p was expressed in a patient in whom CT erroneously suggested progression. CT is the standard for assessing the response to NAC in LAGC, although according to the literature and everyday practice, it is often not clear with the postoperative material assessed. Incorrect assessment of the response to NAC in LAGC may even result in disqualification of the patient from radical treatment. Therefore, finding another tool to asess to response to NAC in LAGC is highly anticipated. Our preliminary research is innovative and the results are promising. It is advisable to repeat the study on a larger number of cases to confirm our results.
Author Contributions
Conceptualization, Marlena Janiczek-Polewska; Methodology, Tomasz Kolenda, Paulina Poter, Joanna Kozłowska-Masłoń and Inga Jagiełło; Software, Tomasz Kolenda; Formal analysis, Marlena Janiczek-Polewska and Tomasz Kolenda; Investigation, Tomasz Kolenda, Paulina Poter and Inga Jagiełło; Resources, Marlena Janiczek-Polewska and Katarzyna Regulska; Data curation, Joanna Kozłowska-Masłoń; Writing – original draft, Marlena Janiczek-Polewska; Supervision, Julian Malicki and Andrzej Marszałek.
Funding
This research was funded in whole by the National Science Centre, Poland [2022/06/X/NZ5/01813]. For the purpose of Open Access, the author has applied a CC-BY public copyright license to any Author Accepted Manuscript (AAM) version arising from this submission.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Conflicts of Interest
The authors declare no conflict of interests for this article.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F.; Bsc, M.F.B.; Me, J.F.; Soerjomataram, M.I.; et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J.; et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef]
- Arnold, M.; Park, J.Y.; Camargo, M.C.; Lunet, N.; Forman, D.; Soerjomataram, I. Is gastric cancer becoming a rare disease? A global assessment of predicted incidence trends to 2035. Gut 2020, 69, 823–829. [Google Scholar] [CrossRef]
- Arnold, M.; Rutherford, M.J.; Bardot, A.; Ferlay, J.; Andersson, T.M.L.; Myklebust, T.Å.; et al. Progress in cancer survival, mortality, and incidence in seven high-income countries 1995–2014 (ICBP SURVMARK-2): A population-based study. Lancet Oncol. 2019, 20, 1493–1505. [Google Scholar] [CrossRef]
- Johnston, F.M.; Beckman, M. Updates on Management of Gastric Cancer. Curr. Oncol. Rep. 2019, 21, 67. [Google Scholar] [CrossRef]
- Kabel, A.M.; Marghalani, A.M.; Bin Salman, T.; Faqeeh, F.J.; Asiri, M.K. Gastric carcinoma: Insights into risk factors, methods of diagnosis, possible lines of management, and the role of primary care. J. Fam. Med. Prim. Care 2020, 9, 2659–2663. [Google Scholar] [CrossRef]
- Roviello, G.; Catalano, M.; D’angelo, A.; Palmieri, V.E. Second line of treatment for HER2-positive gastric cancer: An evolving issue. Rep. Pr. Oncol. Radiother. 2021, 26, 316–317. [Google Scholar] [CrossRef]
- Cunningham, D.; Allum, W.H.; Stenning, S.P.; Thompson, J.N.; Van de Velde, C.J.; Nicolson, M.; Scarffe, J.H.; Lofts, F.J.; Falk, S.J.; Iveson, T.J.; et al. Perioperative Chemotherapy versus Surgery Alone for Resectable Gastroesophageal Cancer. New Engl. J. Med. 2006, 355, 11–20. [Google Scholar] [CrossRef]
- Al-Batran, S.-E.; Homann, N.; Pauligk, C.; Goetze, T.O.; Meiler, J.; Kasper, S.; Kopp, H.-G.; Mayer, F.; Haag, G.M.; Luley, K.; et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. Lancet 2019, 393, 1948–1957. [Google Scholar] [CrossRef]
- Al-Batran, S.-E.; Homann, N.; Schmalenberg, H.; Kopp, H.-G.; Haag, G.M.; Luley, K.B.; Schmiegel, W.H.; Folprecht, G.; Probst, S.; Prasnikar, N.; et al. Perioperative chemotherapy with docetaxel, oxaliplatin, and fluorouracil/leucovorin (FLOT) versus epirubicin, cisplatin, and fluorouracil or capecitabine (ECF/ECX) for resectable gastric or gastroesophageal junction (GEJ) adenocarcinoma (FLOT4-AIO): A multicenter, randomized phase 3 trial. J. Clin. Oncol. 2017, 35, 4004. [Google Scholar] [CrossRef]
- Mansouri, H.; Zemni, I.; Achouri, L.; Mahjoub, N.; Ayedi, M.A.; Safta, I.B.; Dhiab, T.B.; Chargui, R. Chemoradiotherapy or chemotherapy as adjuvant treatment for resected gastric cancer: Should we use selection criteria? Reports of Practical Oncology and Radiotherapy 2021, 26, 266–280. [Google Scholar] [CrossRef]
- Duque-Santana, V.; Campos, F.L.; Martín, M.; Pelari, L.; Hernandez, A.; Valero, M.; Galindo, J.; Priego, P.; Cuadrado, M.; Longo, F.; et al. Dose-escalated neoadjuvant chemoradiotherapy for locally advanced oesophageal or oesophagogastric junctional adenocarcinoma. Rep. Pr. Oncol. Radiother. 2022, 27, 500–508. [Google Scholar] [CrossRef]
- van Putten, M.; Lemmens, V.E.P.P.; van Laarhoven, H.W.M.; Pruijt, H.F.M.; Nieuwenhuijzen, G.A.P.; Verhoeven, R.H.A. Poor compliance with perioperative chemotherapy for resectable gastric cancer and its impact on survival. European Journal of Surgical Oncology 2019, 45, 1926–1933. [Google Scholar] [CrossRef]
- Drake, J.A.; Stiles, Z.E.; Tsao, M.W.; Deneve, J.L.; Glazer, E.S.; Yakoub, D.; Grothey, A.; Somer, B.G.; Dickson, P.V. Analysis of the Survival Impact of Postoperative Chemotherapy After Preoperative Chemotherapy and Resection for Gastric Cancer. Ann. Surg. Oncol. 2021, 28, 1417–1427. [Google Scholar] [CrossRef]
- Bukowski, K.; Kciuk, M.; Kontek, R. Mechanisms of Multidrug Resistance in Cancer Chemotherapy. Int. J. Mol. Sci. 2020, 21, 3233. [Google Scholar] [CrossRef]
- Plotnikova, O.; Baranova, A.; Skoblov, M. Comprehensive Analysis of Human microRNA–mRNA Interactome. Front. Genet. 2019, 10, 933. [Google Scholar] [CrossRef]
- Kolenda, T.; Paszkowska, A.; Braska, A.; Kozłowska-Masłoń, J.; Guglas, K.; Poter, P.; Wojtczak, P.; Bliźniak, R.; Lamperska, K.; Teresiak, A. Host gene and its guest: Short story about relation of long-noncoding MIR31HG transcript and microRNA miR-31. Rep. Pr. Oncol. Radiother. 2023, 28, 114–134. [Google Scholar] [CrossRef]
- Guglas, K.; Kozłowska-Masłoń, J.; Kolenda, T.; Paszkowska, A.; Teresiak, A.; Bliźniak, R.; et al. Midsize noncoding RNAs in cancers: A new division that clarifies the world of noncoding RNA or an unnecessary chaos? Reports of Practical Oncology and Radiotherapy, 2022; 27, 1077–1093. [Google Scholar] [CrossRef]
- Kolenda, T.; Guglas, K.; Kopczyńska, M.; Sobocińska, J.; Teresiak, A.; Bliźniak, R.; Lamperska, K. Good or not good: Role of miR-18a in cancer biology. Rep. Pr. Oncol. Radiother. 2020, 25, 808–819. [Google Scholar] [CrossRef]
- Kipkeeva, F.; Muzaffarova, T.; Korotaeva, A.; Nikulin, M.; Grishina, K.; Mansorunov, D.; Apanovich, P.; Karpukhin, A. MicroRNA in Gastric Cancer Development: Mechanisms and Biomarkers. Diagnostics 2020, 10, 891. [Google Scholar] [CrossRef]
- He, L.; Hannon, G.J. MicroRNAs: Small RNAs with a big role in gene regulation. Vol. 5, Nature Reviews Genetics. 2004.
- Kozłowska-Masłoń, J.; Guglas, K.; Kolenda, T.; Lamperska, K.; Makałowska, I. miRNA in head and neck squamous cell carcinomas: Promising but still distant future of personalized oncology. Rep. Pr. Oncol. Radiother. 2023, 28, 681–697. [Google Scholar] [CrossRef]
- Kolenda, T.; Guglas, K.; Baranowski, D.; Sobocińska, J.; Kopczyńska, M.; Teresiak, A.; et al. cfRNAs as biomarkers in oncology – still experimental or applied tool for personalized medicine already? Reports of Practical Oncology and Radiotherapy 2020, 25, 783–792. [Google Scholar] [CrossRef]
- Kolenda, T.; Przybyła, W.; Kapałczyńska, M.; Teresiak, A.; Zajączkowska, M.; Bliźniak, R.; Lamperska, K.M. Tumor microenvironment – Unknown niche with powerful therapeutic potential. Rep. Pr. Oncol. Radiother. 2018, 23, 143–153. [Google Scholar] [CrossRef]
- Lamperska, K.M.; Kolenda, T.; Teresiak, A.; Kowalik, A.; Kruszyna-Mochalska, M.; Jackowiak, W.; Bliźniak, R.; Przybyła, W.; Kapałczyńska, M.; Kozlowski, P. Different levels of let-7d expression modulate response of FaDu cells to irradiation and chemotherapeutics. PLoS ONE 2017, 12, e0180265. [Google Scholar] [CrossRef]
- Guglas, K.; Kolenda, T.; Kozłowska-Masłoń, J.; Severino, P.; Teresiak, A.; Bliźniak, R.; Lamperska, K. The Impact of YRNAs on HNSCC and HPV Infection. Biomedicines 2023, 11, 681. [Google Scholar] [CrossRef]
- https://www.thermofisher.com/es/es/home/life-science/pcr/real-time-pcr/real-time-pcr-assays/mirna-ncrna-taqman-assays.html?gclid=Cj0KCQjwsPCyBhD4ARIsAPaaRf2gjNp3MXKK0M3WXnwJtno3nH5JKHS5Dxt7gPsOiNHdVlV9WSGJVtoaAjlnEALw_wcB&ef_id=Cj0KCQjwsPCyBhD4ARIsAPaaRf2gjNp3MXKK0M3WXnwJtno3nH5JKHS5Dxt7gPsOiNHdVlV9WSGJVtoaAjlnEALw_wcB:G:s&s_kwcid=AL!3652!3!606132911486!p!!g!!microrna%20assay!17574808760!139287690658&cid=gsd_pcr_sbu_r03_co_cp1491_pjt9622_gsd00000_0se_gaw_rs_pur_&gad_source=1.
- Kolenda, T.; Śmiełowska, M.I.; Lipowicz, J.; Ostapowicz, J.; Pacześna, P.; Rosochowicz, M.; et al. The RNA world: From experimental laboratory to “in silico” approach. Part 1: User friendly RNA expression databases portals. Reports of Practical Oncology and Radiotherapy 2024, 29, 245–257. [Google Scholar] [CrossRef]
- Kolenda, T.; Poter, P.; Guglas, K.; Kozłowska-Masłoń, J.; Braska, A.; Kazimierczak, U.; Teresiak, A. Biological role and diagnostic utility of ribosomal protein L23a pseudogene 53 in cutaneous melanoma. Rep. Pr. Oncol. Radiother. 2023, 28, 255–270. [Google Scholar] [CrossRef]
- Li, W.; Ng, J.M.K.; Wong, C.C.; Ng, E.K.W.; Yu, J. Molecular alterations of cancer cell and tumour microenvironment in metastatic gastric cancer. Oncogene 2018, 37, 4903–4920. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, Q.; Tang, X. Long non-coding RNA XIST contributes into drug resistance of gastric cancer cell. Minerva Medica 2019, 110, 270–272. [Google Scholar] [CrossRef]
- Zeng, Z.; Wang, J.; Zhao, L.; Hu, P.; Zhang, H.; Tang, X.; He, D.; Tang, S.; Zeng, Z. Potential Role of microRNA-21 in the Diagnosis of Gastric Cancer: A Meta-Analysis. PLoS ONE 2013, 8, e73278. [Google Scholar] [CrossRef]
- Chan, S.-H.; Wu, C.-W.; Li, A.F.Y.; Chi, C.-W.; Lin, W.-C. miR-21 microRNA expression in human gastric carcinomas and its clinical association. Anticancer Res. 2008, 28, 907–911. [Google Scholar]
- Meng, L.; Chen, Z.; Jiang, Z.; Huang, T.; Hu, J.; Luo, P.; Zhang, H.; Huang, M.; Huang, L.; Chen, Y.; et al. MiR-122-5p suppresses the proliferation, migration, and invasion of gastric cancer cells by targeting LYN. Acta Biochim. et Biophys. Sin. 2019, 52, 49–57. [Google Scholar] [CrossRef]
- Song, A.; Zhao, L.; Wang, Y.; He, D.; Li, Y. Retracted: Chemoresistance in gastric cancer is attributed to the overexpression of excision repair cross-complementing 1 (ERCC1) caused by microRNA-122 dysregulation. J. Cell. Physiol. 2019, 234, 22485–22492. [Google Scholar] [CrossRef]
- Hosseinahli, N.; Zeinali, T.; Hosseinahli, N.; Karimi, L.; Shanehbandi, D.; Mansoori, B.; Mohammadi, A.; Kazemi, T.; Hajiasgharzadeh, K.; Baradaran, B. Restoration of miRNA-143 Expression Inhibits Growth and Migration of MKN-45 Gastric Cancer Cell Line. Adv. Pharm. Bull. 2022, 12, 183–190. [Google Scholar] [CrossRef]
- Chiang, Y.; Song, Y.; Wang, Z.; Chen, Y.; Yue, Z.; Xu, H.; Xing, C.; Liu, Z. Aberrant Expression of miR-203 and Its Clinical Significance in Gastric and Colorectal Cancers. J. Gastrointest. Surg. 2011, 15, 63–70. [Google Scholar] [CrossRef]
- Xiao, B.; Guo, J.; Miao, Y.; Jiang, Z.; Huan, R.; Zhang, Y.; Li, D.; Zhong, J. Detection of miR-106a in gastric carcinoma and its clinical significance. Clin. Chim. Acta 2008, 400, 97–102. [Google Scholar] [CrossRef]
- Ju, Y.; Choi, G.-E.; Lee, M.W.; Jeong, M.; Kwon, H.; Kim, D.H.; Kim, J.; Jin, H.; Lee, K.E.; Hyun, K.-Y.; et al. Identification of miR-143-3p as a diagnostic biomarker in gastric cancer. BMC Med Genom. 2023, 16, 1–16. [Google Scholar] [CrossRef]
- Zhuang, M.; Shi, Q.; Zhang, X.; Ding, Y.; Shan, L.; Shan, X.; Qian, J.; Zhou, X.; Huang, Z.; Zhu, W.; et al. Involvement of miR-143 in cisplatin resistance of gastric cancer cells via targeting IGF1R and BCL2. Tumor Biol. 2014, 36, 2737–2745. [Google Scholar] [CrossRef]
- Du, F.; Feng, Y.; Fang, J.; Yang, M. MicroRNA-143 enhances chemosensitivity of Quercetin through autophagy inhibition via target GABARAPL1 in gastric cancer cells. Biomed. Pharmacother. 2015, 74, 169–177. [Google Scholar] [CrossRef]
- Wang, F.; Liu, J.; Zou, Y.; Jiao, Y.; Huang, Y.; Fan, L.; Li, X.; Yu, H.; He, C.; Wei, W.; et al. MicroRNA-143-3p, up-regulated in H. pylori-positive gastric cancer, suppresses tumor growth, migration and invasion by directly targeting AKT2. Oncotarget 2017, 8, 28711–28724. [Google Scholar] [CrossRef]
- Wang, Z.; Zhao, Z.; Yang, Y.; Luo, M.; Zhang, M.; Wang, X.; Liu, L.; Hou, N.; Guo, Q.; Song, T.; et al. MiR-99b-5p and miR-203a-3p Function as Tumor Suppressors by Targeting IGF-1R in Gastric Cancer. Sci. Rep. 2018, 8, 1–12. [Google Scholar] [CrossRef]
- Jiang, Y.; Jin, S.; Tan, S.; Shen, Q.; Xue, Y. MiR-203 acts as a radiosensitizer of gastric cancer cells by directly targeting ZEB1. OncoTargets Ther. 2019, 12, 6093–6104. [Google Scholar] [CrossRef]
- Guo, X.; Wang, X.; Li, S.; Lu, Y.; Xie, T.; Qiu, Z.; et al. LncRNA-GC1 contributes to gastric cancer chemo-resistance through inhibition of miR-551b-3p and the overexpression of dysbindin. Annals of Oncology 2019, 30, v8. [Google Scholar] [CrossRef]
- Zhang, S.; Zhang, R.; Xu, R.; Shang, J.; He, H.; Yang, Q. MicroRNA-574-5p in gastric cancer cells promotes angiogenesis by targeting protein tyrosine phosphatase non-receptor type 3 (PTPN3). Gene 2020, 733, 144383. [Google Scholar] [CrossRef]
- Bruick, R.K.; McKnight, S.L. A Conserved Family of Prolyl-4-Hydroxylases That Modify HIF. Science 2001, 294, 1337–1340. [Google Scholar] [CrossRef]
- Wang, M.; Zhang, R.; Zhang, S.; Xu, R.; Yang, Q. MicroRNA-574-3p regulates epithelial mesenchymal transition and cisplatin resistance via targeting ZEB1 in human gastric carcinoma cells. Gene 2019, 700, 110–119. [Google Scholar] [CrossRef]
- Xu, X.; Yang, X.; Xing, C.; Zhang, S.; Cao, J. miRNA: The nemesis of gastric cancer (Review). Oncol. Lett. 2013, 6, 631–641. [Google Scholar] [CrossRef]
- Ji, Z.; Wang, X.; Liu, Y.; Zhong, M.; Sun, J.; Shang, J. MicroRNA-574-3p Regulates HIF-α Isoforms Promoting Gastric Cancer Epithelial-Mesenchymal Transition via Targeting CUL2. Dig. Dis. Sci. 2021, 67, 3714–3724. [Google Scholar] [CrossRef]
- Matuszcak, C.; Haier, J.; Hummel, R.; Lindner, K. MicroRNAs: Promising chemoresistance biomarkers in gastric cancer with diagnostic and therapeutic potential. World Journal of Gastroenterology. 2014, 20, 13658–13666. [Google Scholar] [CrossRef]
Figure 1.
Expression levels of miR-21*, miR-21, miR-106a, miR-122, miR-122*, miR-143, miR-143*, miR-203a-5p, miR-203, miR-551b, miR-551b*, miR-574-3p before, biopsy performed during gastroscopy, and after surgery preceded by 4 cycles of neoadjuvant chemotherapy according to the FLOT or FLO regiment and in normal samples taken from healthy individuals; box and whiskers with 5-95 percentile, Mann Whitney test; p < 0.05 considered as significant.
Figure 1.
Expression levels of miR-21*, miR-21, miR-106a, miR-122, miR-122*, miR-143, miR-143*, miR-203a-5p, miR-203, miR-551b, miR-551b*, miR-574-3p before, biopsy performed during gastroscopy, and after surgery preceded by 4 cycles of neoadjuvant chemotherapy according to the FLOT or FLO regiment and in normal samples taken from healthy individuals; box and whiskers with 5-95 percentile, Mann Whitney test; p < 0.05 considered as significant.
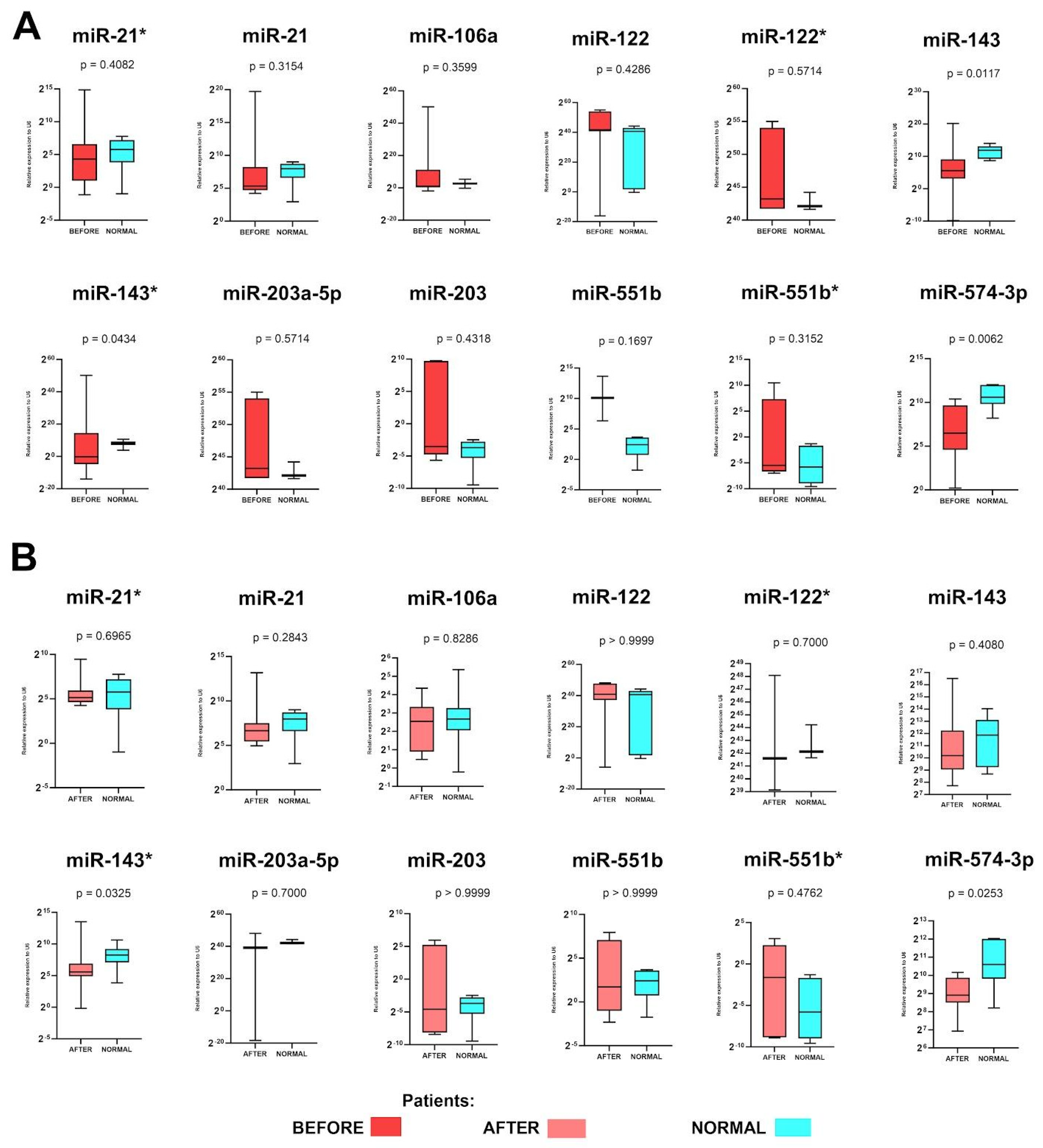
Figure 2.
Receiver operating characteristic curve (ROC) analyses of miR-143, miR-143* and miR-574-3p in patients’ samples taken A) before and B) after surgery in comparison to the normal samples taken from healthy, non-cancer individuals; CI - confidence interval, n - number of cases in analyses, p < 0.05 considered as significant.
Figure 2.
Receiver operating characteristic curve (ROC) analyses of miR-143, miR-143* and miR-574-3p in patients’ samples taken A) before and B) after surgery in comparison to the normal samples taken from healthy, non-cancer individuals; CI - confidence interval, n - number of cases in analyses, p < 0.05 considered as significant.
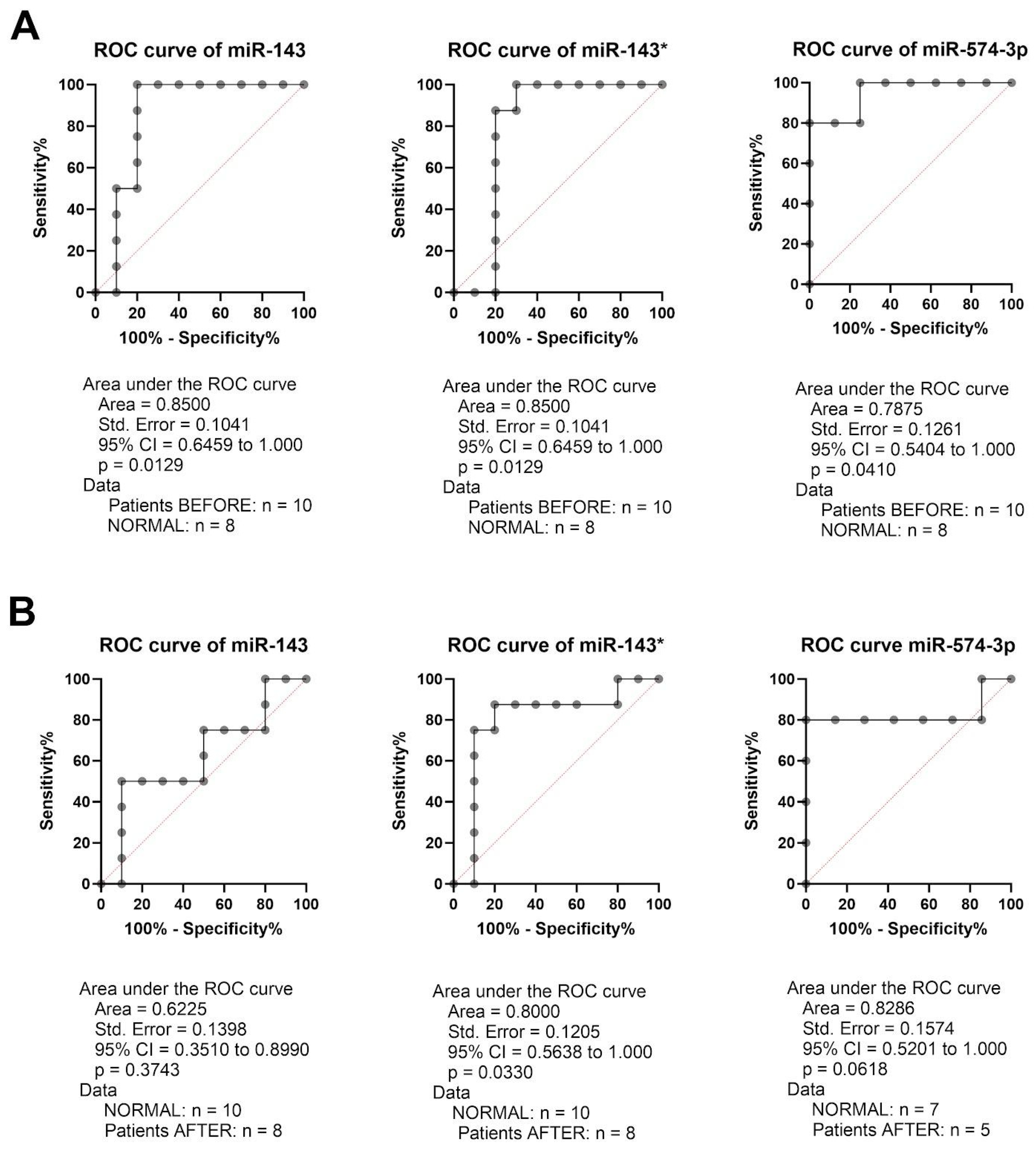
Figure 3.
Expression levels of miR-21*, miR-21, miR-106a, miR-122, miR-122*, miR-143, miR-143*, miR-203a-5p, miR-203, miR-551b, miR-551b*, miR-574-3p in A) before, biopsy performed during gastroscopy, and after surgery preceded by 4 cycles of neoadjuvant chemotherapy according to the FLOT or FLO regiment and B) receiver operating characteristic curve (ROC) analyses of miR-21, miR-143 and miR-574-3p in patients’ samples taken before and after surgery; box and whiskers with 5-95 percentile, Wilcoxon matched-pairs signed rank test; CI - confidence interval, n - number of cases in analyses, NC - no calculated due to the lack of gene expression, p < 0.05 considered as significant.
Figure 3.
Expression levels of miR-21*, miR-21, miR-106a, miR-122, miR-122*, miR-143, miR-143*, miR-203a-5p, miR-203, miR-551b, miR-551b*, miR-574-3p in A) before, biopsy performed during gastroscopy, and after surgery preceded by 4 cycles of neoadjuvant chemotherapy according to the FLOT or FLO regiment and B) receiver operating characteristic curve (ROC) analyses of miR-21, miR-143 and miR-574-3p in patients’ samples taken before and after surgery; box and whiskers with 5-95 percentile, Wilcoxon matched-pairs signed rank test; CI - confidence interval, n - number of cases in analyses, NC - no calculated due to the lack of gene expression, p < 0.05 considered as significant.
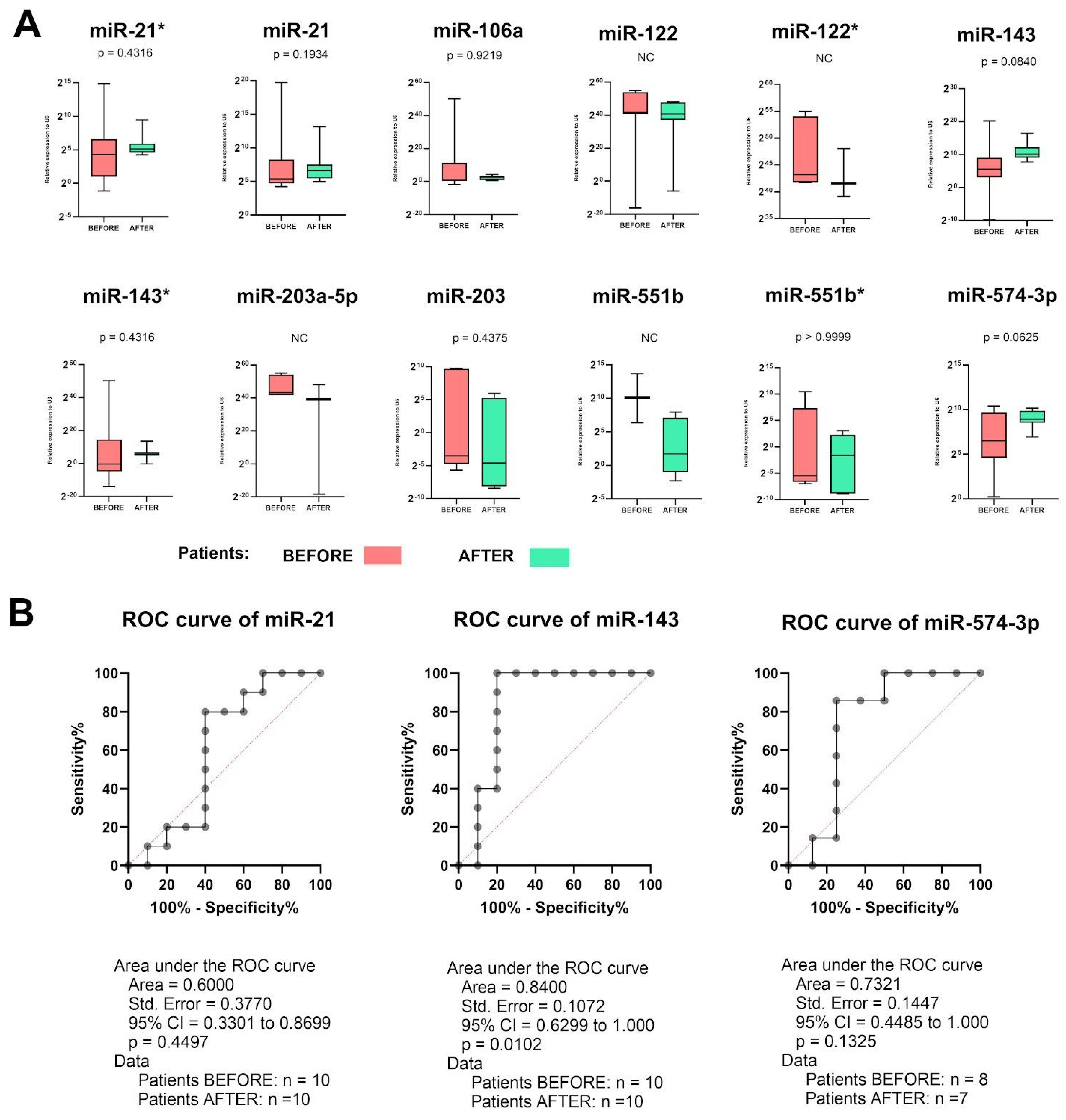
Table 1.
Expression levels of selected miRNAs in cancer and normal samples from gastric patients analyzed during the TCGA project; data taken from ENCORI database; n - number of samples, FDR - false discovery rate.
Table 1.
Expression levels of selected miRNAs in cancer and normal samples from gastric patients analyzed during the TCGA project; data taken from ENCORI database; n - number of samples, FDR - false discovery rate.
| miRNA | Cancer samples [n] | Normal samples [n] | Median expression level in cancer samples | Median expression level in normal samples | Fold change | P-value | FDR |
|---|---|---|---|---|---|---|---|
| miRNA-21-3p | 372 | 32 | 3285.16 | 1165.75 | 2.82 | 6.8e-24 | 2.5e-21 |
| miRNA-21-5p | 372 | 32 | 282109.88 | 64062.21 | 4.4 | 1.83e-68 | 4.7e-65 |
| miRNA-106a-5p | 372 | 32 | 18.72 | 7.85 | 2.38 | 0.00099 | 0.0068 |
| miRNA-122-3p | 372 | 32 | 0.21 | 0.01 | 20.55 | 0.25 | 0.6 |
| miRNA-122-5p | 372 | 32 | 17.3 | 0.57 | 29.92 | 0.54 | 0.83 |
| miRNA-143-3p | 372 | 32 | 193518.49 | 443164.16 | 0.44 | 3.6e-10 | 9.3e-9 |
| miRNA-143-5p | 372 | 32 | 121.59 | 229.49 | 0.53 | 0.011 | 0.054 |
| miRNA-203a-3p | 372 | 32 | - | - | - | - | - |
| miRNA-203a-5p | 372 | 32 | - | - | - | - | - |
| miRNA-551b-3p | 372 | 32 | 1.53 | 07.02 | 0.22 | 0.037 | 0.15 |
| miRNA-551b-5p | 372 | 32 | 0.02 | 0.03 | 0.56 | 0.13 | 0.39 |
| miRNA-574-3p | 372 | 32 | 81.06 | 85.97 | 0.94 | 0.2 | 0.54 |
Table 2.
Differences in the expression levels of miRNA-21, miRNA-106a, miRNA-122, miRNA-143, miRNA-203a, miRNA-551b and miRNA-574 depending on clinicopathological parameters in GC patients based on the TCGA project. Data taken from UALCAN database; AC - adenocarcinoma, IAC - intestinal adenocarcinoma; p < 0.05 considered as significant.
Table 2.
Differences in the expression levels of miRNA-21, miRNA-106a, miRNA-122, miRNA-143, miRNA-203a, miRNA-551b and miRNA-574 depending on clinicopathological parameters in GC patients based on the TCGA project. Data taken from UALCAN database; AC - adenocarcinoma, IAC - intestinal adenocarcinoma; p < 0.05 considered as significant.
| Parameter | Groups | miRNA-21 | miRNA-106a | miRNA-122 | miRNA-143 | miRNA-203a | miRNA-551b | miRNA-574 |
|---|---|---|---|---|---|---|---|---|
| Sample type | Normal vs Primary | <1E-12 | 0,00008 | 0,14658 | 0,00000 | 0,16578 | 0,00242 | 0,69254 |
| Race | Caucasian vs African American | 0,59606 | 0,65550 | 0,19030 | 0,05878 | 0,66776 | 0,05402 | 0,05402 |
| Caucasian vs Asian | 0,30630 | 0,01604 | 0,17484 | 0,02172 | 0,31662 | 0,63522 | 0,63522 | |
| African American vs Asian | 0,29902 | 0,56788 | 0,62328 | 0,29880 | 0,99920 | 0,13424 | 0,13424 | |
| Gender | Male vs Female | 0,74084 | 0,53014 | 0,24308 | 0,32242 | 0,28556 | 0,56872 | 0,56872 |
| Age | 21-40 vs 41-60 | 0,14104 | 0,04318 | 0,18056 | 0,43436 | 0,22830 | 0,41534 | 0,41534 |
| 21-40 vs 61-80 | 0,25226 | 0,00808 | 0,12376 | 0,76562 | 0,77240 | 0,05157 | 0,05157 | |
| 21-40 vs 81-100 | 0,05878 | 0,34576 | 0,90334 | 0,55958 | 0,13628 | 0,08584 | 0,08584 | |
| 41-60 vs 61-80 | 0,08270 | 0,23986 | 0,20184 | 0,00918 | 0,00672 | 0,93720 | 0,93720 | |
| 41-60 vs 81-100 | 0,49906 | 0,15064 | 0,17968 | 0,56066 | 0,61330 | 0,55180 | 0,55180 | |
| 61-80 vs 81-100 | 0,11083 | 0,01720 | 0,10224 | 0,43432 | 0,06366 | 0,63018 | 0,63018 | |
| Cancer stage | I vs II | 0,15316 | 0,16144 | 0,29706 | 0,47704 | 0,43726 | 0,54456 | 0,54456 |
| I vs III | 0,01124 | 0,60368 | 0,32454 | 0,54468 | 0,05878 | 0,56204 | 0,56204 | |
| I vs IV | 0,23102 | 0,53414 | 0,36276 | 0,40824 | 0,07544 | 0,75392 | 0,75392 | |
| II vs III | 0,15882 | 0,23550 | 0,47678 | 0,87786 | 0,12802 | 0,90778 | 0,90778 | |
| II vs IV | 0,88272 | 0,49128 | 0,25600 | 0,68498 | 0,15774 | 0,28022 | 0,28022 | |
| III vs IV | 0,48102 | 0,81706 | 0,58708 | 0,62610 | 0,89714 | 0,35976 | 0,35976 | |
| Tumor grade | G1 vs G2 | 0,67776 | 0,74114 | 0,30394 | 0,79310 | 0,60826 | 0,22676 | 0,22676 |
| G1 vs G3 | 0,65476 | 0,90388 | 0,09204 | 0,57692 | 0,17936 | 0,13166 | 0,13166 | |
| G2 vs G3 | 0,86524 | 0,34396 | 0,46276 | 0,00182 | 0,02424 | 0,83656 | 0,83656 | |
| Nodal metastasis status | N0 vs N1 | 0,30396 | 0,88494 | 0,27724 | 0,78988 | 0,75946 | 0,83018 | 0,83018 |
| N0 vs N2 | 0,29180 | 0,71396 | 0,29278 | 0,71558 | 0,80560 | 0,72304 | 0,72304 | |
| N0 vs N3 | 0,71348 | 0,49888 | 0,42276 | 0,28858 | 0,00474 | 0,17108 | 0,17108 | |
| N1 vs N2 | 0,96318 | 0,88320 | 0,55314 | 0,56090 | 0,98958 | 0,89646 | 0,89646 | |
| N1 vs N3 | 0,78694 | 0,48110 | 0,35356 | 0,24474 | 0,02912 | 0,15342 | 0,15342 | |
| N2 vs N3 | 0,75010 | 0,39538 | 0,42578 | 0,41616 | 0,09393 | 0,14404 | 0,14404 | |
| Tumor histology | AC NOS vs AC Diffuse | 0,52732 | 0,75522 | 0,22130 | 0,21224 | 0,20154 | 0,13558 | 0,13558 |
| AC NOS vs AC Signet Ring | 0,12324 | 0,13950 | 0,65222 | 0,62216 | 0,00184 | 0,10358 | 0,10358 | |
| AC NOS vs IAC NOS | 0,45426 | 0,55860 | 0,36642 | 0,11122 | 0,66980 | 0,92958 | 0,92958 | |
| AC NOS vs IAC Mucinous | 0,39568 | 0,02212 | 0,28880 | 0,43058 | 0,33528 | 0,12252 | 0,12252 | |
| AC NOS vs IAC Papillary | 0,55152 | 0,84612 | 0,94758 | 0,09892 | 0,27432 | 0,47208 | 0,47208 | |
| AC NOS vs IAC Tubular | 0,09716 | 0,55192 | 0,32894 | 0,00000 | 0,04314 | 0,09158 | 0,09158 | |
| AC Diffuse vs AC Signet Ring | 0,07644 | 0,29140 | 0,33310 | 0,36696 | 0,06108 | 0,53796 | 0,53796 | |
| AC Diffuse vs IAC NOS | 0,21652 | 0,46906 | 0,27970 | 0,02094 | 0,37026 | 0,14580 | 0,14580 | |
| AC Diffuse vs IAC Mucinous | 0,66654 | 0,06158 | 0,30358 | 0,89524 | 0,93058 | 0,78986 | 0,78986 | |
| AC Diffuse vs IAC Papillary | 0,40010 | 0,96520 | 0,16990 | 0,00822 | 0,19376 | 0,90458 | 0,90458 | |
| AC Diffuse vs IAC Tubular | 0,04388 | 0,86194 | 0,31354 | 0,00004 | 0,00562 | 0,78714 | 0,78714 | |
| AC Signet Ring vs IAC NOS | 0,22388 | 0,22494 | 0,52088 | 0,81776 | 0,00520 | 0,11222 | 0,11222 | |
| AC Signet Ring vs IAC Mucinous | 0,10170 | 0,11510 | 0,35920 | 0,42808 | 0,09626 | 0,67820 | 0,67820 | |
| AC Signet Ring vs IAC Papillary | 0,61504 | 0,45914 | 0,56958 | 0,37434 | 0,11228 | 0,62612 | 0,62612 | |
| AC Signet Ring vs IAC Tubular | 0,42724 | 0,38018 | 0,37260 | 0,33454 | 0,00010 | 0,58822 | 0,58822 | |
| IAC NOS vs IAC Mucinous | 0,19918 | 0,17518 | 0,28926 | 0,09030 | 0,56498 | 0,13216 | 0,13216 | |
| IAC NOS vs IAC Papillary | 0,75650 | 0,64798 | 0,35850 | 0,29404 | 0,24576 | 0,63370 | 0,63370 | |
| IAC NOS vs IAC Tubular | 0,41558 | 0,26374 | 0,29396 | 0,02458 | 0,02216 | 0,09702 | 0,09702 | |
| IAC Mucinous vs IAC Papillary | 0,35352 | 0,22480 | 0,23418 | 0,07300 | 0,20372 | 0,78462 | 0,78462 | |
| IAC Mucinous vs IAC Tubular | 0,07514 | 0,00634 | 0,78488 | 0,00846 | 0,01260 | 0,92004 | 0,92004 | |
| IAC Papillary vs IAC Tubular | 0,95976 | 0,97014 | 0,20794 | 0,84260 | 0,55078 | 0,79666 | 0,79666 | |
| TP53 mutation status | Mutant vs Non-mutant | 0,64328 | 0,28594 | 0,21586 | 0,00600 | 0,26196 | 0,35738 | 0,35738 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



