
Submitted:
09 June 2024
Posted:
11 June 2024
You are already at the latest version
Abstract
Intracranial metastases from thyroid cancer are rare. Although the prognosis of thyroid cancer patients is generally favorable, the prognosis of patients with intracranial metastases from thyroid cancer has been considered unfavorable having a lower survival rate than those without intracranial involvement. Many questions about their management remain unclear. The aim of this study was to analyze the characteristics, treatments, and outcomes of patients with brain metastases from thyroid cancer. Among 4320 patients with thyroid cancer recorded in our institutional database over a 30-year period, 20 patients with brain metastasis were retrospectively collected and analyzed. The clinical characteristics, histological type of primary cancer and metastatic brain tumor, additional previous distant metastasis, treatment modalities, locations and characteristics on radiologic findings, time interval between the first diagnosis of the primary thyroid cancer and brain metastasis, and survival were analyzed. The mean age at initial diagnosis was 59.3 ± 14.1 years, and at the manifestation of diagnosis of cerebral metastasis 64.8 ± 14.9 years. The histological types of the primary thyroid cancers were papillary in ten patients, follicular in seven, and poorly differentiated carcinoma in three. The average interval between the diagnosis of thyroid cancer and brain metastasis was 63.4 ± 58.4 months (range, 0-180 months). Ten patients had a single intracranial lesion and 10 patients had multiple lesions. Surgical resection was primarily performed in 15 patients and whole-brain radiotherapy, radiotherapy or tyrosine kinase inhibitors were applied in the other 5 patients. Overall median survival time was 15 months after diagnosis of BM from TC (range: 1-252 months). Patients with thyroid cancer can develop brain metastasis even many years after diagnosis of the primary tumor. Our study demonstrates an increased overall survival of patients younger than 60 years of age at the time of diagnosis of brain metastasis. There was no difference in survival between patients with brain metastasis from papillary or follicular thyroid carcinoma.
Keywords:
Thyroid cancer
; brain metastasis
; surgery
; radiotherapy
1. Introduction
Thyroid carcinoma (TC) is the most coparkmmon malignancy of the endocrine system with an average age of 40 years at diagnosis [1,2,3]. Women are more frequently affected than men with a male/female ratio of 1/3 [4,5]. Well differentiated TC including papillary thyroid carcinoma (PTC) and follicular thyroid carcinoma (FTC) are the most common histologic types of TC (85% to 90% of all newly diagnosed TC), both having a favorable prognosis after appropriate treatment [6,7]. Distant metastases from TC may involve the lung and bone [8,9]. Brain metastases (BM) from TC are rare, occurring approximately in only 1% of all patients with TC [10,11]. However, because of the implementation of systematic cerebral imaging before the start of treatment with tyrosine kinase inhibitors (TKIs), a higher frequency of asymptomatic BM has been documented more recently [12,13,14]. Surgical resection has been favored for treatment of BM either combined with stereotactic radiosurgery (SRS) or whole-brain radio therapy (WBRT) resulting in preservation of quality of life and prolonged survival [12,15,16,17,18,19]. Nevertheless, the presence of intracranial metastases from TC has been considered to be associated with poorer outcome and a lower survival rate [20,21,22]. Management of TC with BM is challenging because of limited experience and many questions remain unclear. Furthermore, there is still a lack of studies comparing the clinical characteristics and outcomes of patients with BM from different types of TC.
The aim of the present study was to review the experience with the management of BM from TC over a 30-year period at Hannover Medical School providing a maximum care referral center. For this purpose, we analyzed the clinical characteristics, the therapeutic approaches and corresponding outcomes. Additionally, we evaluated the prognostic factors affecting cancer-specific survival in patients with BM secondary to TC.
2. Materials and Methods
To identify patients with a diagnosis of BM from TC, a systematic review of the databank of the Department of Neurosurgery and the Department of Nuclear Medicine at Hannover Medical School was performed retrospectively over a 30-year period. Among 4320 patients with TC, 20 patients with BM were identified between 1989 and 2019. Histological confirmation of the thyroid origin of BM was present for 15 patients. The charts with demographic and clinical data (age, sex, mode of presentation and radiologic features of BM, treatment modalities including surgery, SRS, WBRT with or without boost, patient outcome, preoperative signs and symptoms and concomitant diseases, and histopathological findings were evaluated. The progress of treatment over the years was taken into account. Neurosurgical procedures were performed according to departmental standard techniques as described elsewhere [23,24]. Patients were followed up until December 2022. Overall survival (OS) after diagnosis of BM was calculated, and survival time was measured from the diagnosis of BM to the date of death or the last follow-up.
2.1. Statistical Analysis
Cox proportional hazards regression analysis was used for metric predictor variables and categories. In addition, the Cox regression model was applied for survival analysis including the simultaneous effects of multiple risk factors on survival. The model's coefficients formed the computational basis for hazard ratios (HR) to determine the effect size of predictors on survival (ranging in an open-right interval from 0 to infinity).
As predictors, a list of variables with a possible impact on survival time was selected such as patient age, the time interval between initial diagnosis and detection of BM, number of metastases found, presence of neurologic deficits, number of intracranial lesions, and gender. All predictors were categorized (dichotomized) using a two-level nominal scale into set thresholds (Table 1). Survival times were given as months; censoring data excluded four patients with extreme survival time data. Thus, 80% of data were found between 6 and 77 months. Two predictors, metastases and neurological deficits showed one missing value each.
Statistical analyses were performed using JMP®, Version 16.2.0 (SAS Institute Inc., Cary, NC, 1989–2021) and R Core Team (ver. 4.2.3, R Foundation for Statistical Computing, Vienna, Austria, 2023). A p-value of less than 0.05 was considered statistically significant.
3. Results
3.1. Patient Characteristics
Of the 20 patients with BM form TC, 14 were women and 6 were men (female/male ratio = 2.33:1). Age at the time of diagnosis of TC ranged between 26 and 79 years, with a mean age of 59.3 ± 14.1 years. The mean age at BM diagnosis was 64.8 ± 14.9 years.
3.2. Histological Findings of the Primary Tumor
Ten patients had PTC, seven had FTC, and three had a poorly differentiated carcinoma. According to the TMN classification, 2 patients were in stage I-II, 15 in stage III-IV, and in 3 patients the stage could not be determined. Nineteen patients presented with other previous and/or synchronous distant metastases: lung (n=17), bone (n=7), liver (n=1), kidney (n=2), spine (n=2), and 1 unknown. Total surgical thyroidectomy was performed in 17 patients, while 3 patients had subtotal thyroidectomy. Lymph node dissection was added in 15 patients, and five patients did not undergo lymph node dissection.
3.3. Clinical Features of BM from TC
Table 2 summarizes the demographic and clinical data of the patients with BM. The mean interval between the diagnosis of TC and BM was 63.4 ± 58.4 months (range 0-180 months), and from BM diagnosis to death 41.2 ± 60.7 months (range 1-252 months). Ten patients had a single BM, 8 patients had 2 or 3, and 2 patients had 4 or more BM. BM were revealed by neurologic symptoms in 11 patients (headache, nausea, motor or sensory deficits, ataxia, aphasia, confusion, and epileptic seizures). The other 9 patients had no symptoms and the BM were diagnosed incidentally. The diagnosis was made by magnetic resonance imaging in eight patients, by computed tomography in 6 patients, by iodine scans in three, and by PET imaging in three. The most common site of brain metastasis was the parietal lobe (10, 32%), followed by the frontal lobe (7, 22%), cerebellum (5, 17%), occipital lobe (5, 17%), temporal lobe (2, 6%) and brainstem (2, 6%). The Karnofsky Performance Score (KPS) in 17 patients (85%) was > 70, and in 3 patients (15%) it was ≤ 70.
3.4. Treatment
The primary treatment for BM was surgical resection in 15 patients, and surgery was the only treatment for BM in 4 instances. SRS and isotretinoin therapy was only used in one patient, respectively. WBRT alone was accomplished in three patients. The 11 other patients underwent a combined treatment algorithm. Surgical resection plus WBRT was performed in 8 patients. In one patient, radioactive iodine was applied after surgical resection, another patient underwent WBRT and tyrosinkinase inhibitor therapy after surgical resection. In another instance, WBRT was performed following SRS.
3.5. Survival
The overall median survival time was 15 months after diagnosis of BM from TC, and it ranged from 1 to 252 months. At the time of the last follow-up, 16 patients were dead, and 4 patients were still alive. Information regarding the cause of death was available for 14 patients. Death was presumed to be related to progression of multiple BM, recurrence of BM and progression of extracranial metastases in 12 patients, while two patients died from septic shock, and in 2 patients the cause of death was unknown.
The regression model’s significance level indicated a difference in survival time when at least one of the covariates was included in the model, i.e., the omnibus null hypothesis of multivariate Cox analysis could soundly be rejected (chi2(6) = 17.0149, p = 0.0092).
In detail, the hazard ratio for age, HR = eCoef = 6.19, indicated a highly increased risk of death for patients over 60 years of age. Contrarily, the covariate duration, i.e., an interval longer than 24 months between the initial diagnosis and BM detection, markedly decreased the risk of death (HR = 0.21). Both test results reached statistical significance. The remaining analyses of the covariates metastases (HR = 1.62) and gender (HR = 1.07) showed opposite trends compared to neurological deficits (HR =0.79) and lesions (HR = 0.97) in their statistical relationship to survival times. The four latter effects, however, failed to be statistically significant (Table 3). Figure 1 shows the Kaplan-Meier survival analyses with corresponding 95% confidence intervals of predictors in the Cox regression analyses.
4. Discussion
The prevalence of BM in patients with TC was rare in our study (less than 1%) which was in keeping with published previous studies [2,13]. BM from TC, however, were reported more frequently in the last few years [25,26,27]. This increase is likely due to the more frequent use of cranial imaging and also to a longer survival in patients with advanced disease. BM were detected in several of our patients without neurological symptoms incidentally after a systemic image survey before targeted therapy. There was no difference between OS in patients with PTC or FTC. Patients with a single BM had a better outcome than those with multiple metastases. Our study demonstrated also that OS in patients younger than 60 years of age at the time of diagnosis of BM was significantly better in comparison to patients older than 60 years. Additionally, OS was better in patients with a period longer than 24 months between TC and BM diagnosis.
The interval between the first diagnosis of TC and BM in our study was relatively long, similar to previously published studies [3,16,28,29]. The most common location of BM was in the telencephalon, while 3 patients had cerebellar lesions and 2 patients had both infra- and supratentorial BM. Remarkably, Kwon et al reported that BMs from lung adenocarcinoma might preferentially involve the distal MCA territory and the cerebellum [30]. Further, Kyeong et al showed that different breast cancer subtypes might show different distributions of BMs [31]. Moreover, Kim et al. postulated that a “seed and soil theory” with an affinity of the tumor to a microenvironment would be partially responsible for the involvement of specific brain regions [3].
Our study is in line with previous studies concerning the coexistence of other organ metastases and BM [2,32,33,34]. In our series, 90% of patients had metastases involving two or more organs. The most frequent coexisting metastatic sites were lung (85%) and bone (35%). Further, our study showed that BM develops generally after the onset of other metastases [2,27].
Treatment decisions for BM in TC are influenced by various clinical factors including the extent of systemic tumor spread, the specific histopathology type, the tumor's responsiveness to radioiodine, and its location within the brain [33,34]. As recommended by the National Comprehensive Cancer Network (NCCN) guideline in 2022, surgical removal followed by WBRT or SRS combined with WBRT is recommended for patients with stable systemic disease or those newly diagnosed. Furthermore, either neurosurgical resection or stereotactic SRS is preferred over WBRT for patients who have solitary BM. Also, survival was significantly improved by surgical resection of one or more tumor foci. On the other hand, WBRT or SRS alone is suggested for patients with multiple (>3) metastatic lesions. According to published studies, radioiodine might not prove effective in treating cranial metastases from thyroid cancer due to the inability of most cranial metastatic lesions to concentrate radioiodine [35,36].
Various retrospective studies have shown that resection of BM improves OS in patients with BM from TC [12,37,38]. Previous studies [11,39,40] showed also, that patients with a KPS score of 70 or more have a better prognosis with longer survival. Chiu et al [41] reported that patients with a single BM have a better outcome than patients with multiple BM, while Wu et al [13] reported no difference in patients with single metastases in comparison to multiple metastases.
The results of the present study should be interpreted with caution due to the retrospective design of the study and the inclusion of a sample of patients from a single center. Moreover, the prognostic subgroups defined in the study were not validated in a prospective form, which, however, is not likely to be expected because of the rare incidence of BM from TC.
In summary, giving their rarity, the exact incidence of BM from TC has been difficult to estimate. Although patients with thyroid cancer generally have a favorable prognosis, those with BM typically experience a poorer prognosis, characterized by a shorter survival period. In our study the number of BM does not play a significant role in determining patient survival. Furthermore, in the case of a longer interval (more than 24 months) between TC diagnosis and BM manifestation, patients have a significantly better OS. Both, surgical resection and multidisciplinary adjuvant treatment are critical for patients with BM from TC.
Author Contributions
M.E.: Conceptualization, Methodology, Writing-Original Draft, Writing-Review & Editing. O.A.: Conceptualization, Methodology, Writing-Original Draft. H.E.H.: Formal analysis, Writing-Original Draft. M.P.: Methodology, Writing-Review & Editing. A.M.: Supervision, Writing-Review & Editing. F.B.: Supervision, Writing-Review & Editing, Validation. J.K.K.: Conceptualization, Supervision, Writing-Review & Editing, Validation. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was performed in accordance with the ethical standards detailed in the Declaration of Helsinki. In view of the retrospective nature of the study, formal approval of the institutional ethics committee is not required at the authors’ institution.
Informed Consent Statement
All patients consented to the scientific use of their medical data.
Data Availability Statement
The data presented in this study are available on request from the corresponding authors.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Pu W, Shi X, Yu P, Zhang M, Liu Z, Tan L, Han P, Wang Y, Ji D, Gan H, Wei W, Lu Z, Qu N, Hu J, Hu X, Luo Z, Li H, Ji Q, Wang J, Zhang X, Wang YL. Single-cell transcriptomic analysis of the tumor ecosystems underlying initiation and progression of papillary thyroid carcinoma. Nat Commun 2021, 12, 6058.
- Hong YW, Lin JD, Yu MC, Hsu CC, Lin YS. Outcomes and prognostic factors in thyroid cancer patients with cranial metastases: A retrospective cohort study of 4,683 patients. Int J Surg. 2018, 55, 182–187. [CrossRef] [PubMed]
- Kim SS, Kim SM, Park M, Suh SH, Ahn SJ. Clinico-radiological features of brain metastases from thyroid cancer. Medicine (Baltimore) 2021, 100, e28069. [CrossRef] [PubMed]
- Toraih EA, Hussein MH, Zerfaoui M, Attia AS, Marzouk Ellythy A, Mostafa A, Ruiz EML, Shama MA, Russell JO, Randolph GW, Kandil E. Site-specific metastasis and survival in papillary thyroid cancer: the importance of brain and multi-organ disease. Cancers (Basel). 2021, 13, 1625. [CrossRef]
- Alonso-Gordoa, T. Multimodal approach to the treatment of patients with radioiodine refractory differentiated thyroid cancer and metastases to the central nervous system. Cancer Med. 2022, 11, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Mitchell AL, Gandhi A, Scott-Coombes D, Perros P. Management of thyroid cancer: United Kingdom National Multidisciplinary Guidelines. J Laryngol Otol 2016, 130, S150–S160. [CrossRef] [PubMed]
- Gubbiotti MA, Livolsi V. Brain metastases of papillary thyroid carcinoma origin are derived from aggressive histologic variants and demonstrate similar adverse morphology in the metastatic lesion. Clin Neurol Neurosurg. 2023, 227, 107639. [Google Scholar] [CrossRef] [PubMed]
- Yoo J, Kim HJ, Kim SM, Park HH. Prognostic factors to predict the efficacy of surgical interventions against brain metastasis secondary to thyroid cancer. Eur Thyroid J. 2022, 11, e220087. [Google Scholar]
- Yoon JH, Jeon MJ, Kim M, Hong AR, Kim HK, Shin DY, Kim BH, Kim WB, Shong YK, Kang HC. Unusual metastases from differentiated thyroid cancers: A multicenter study in Korea. PLoS One 2020, 15, e0238207.
- Saito F, Uruno T, Shibuya H, Kitagawa W, Nagahama M, Sugino K, Ito K. Prognosis after brain metastasis from differentiated thyroid carcinoma. World J Surg. 2016, 40, 574–581. [Google Scholar] [CrossRef]
- Henriques de Figueiredo B, Godbert Y, Soubeyran I, Carrat X, Lagarde P, Cazeau AL, Italiano A, Sargos P, Kantor G, Loiseau H, Bonichon F. Brain metastases from thyroid carcinoma: a retrospective study of 21 patients. Thyroid. 2014, 24, 270–6.
- Wu SS, Lamarre ED, Scharpf J, Prendes B, Ku JA, Silver N, Burkey B, Woody N, Campbell SR, Yilmaz E, Koyfman SA, Geiger J. Survival Outcomes of Advanced Thyroid Cancer Enriched in Brain Metastases Following Treatment With Small Molecule Inhibitors. Endocr Pract. 2023, 29, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Wu T, Jiao Z, Li Y, Peng J, Yao F, Chen W, Yang A. Brain metastases from differentiated thyroid carcinoma: a retrospective study of 22 patients. Front Endocrinol (Lausanne). 2021, 12, 730025.
- Alimonti P, Gonzalez Castro LN. The current landscape of immune checkpoint inhibitor immunotherapy for primary and metastatic brain tumors. Antibodies (Basel). 2023, 12, 27.
- Osborne JR, Kondraciuk JD, Rice SL, Zhou X, Knezevic A, Spratt DE, Sabra M, Larson SM, Grewal RK. Thyroid Cancer Brain metastasis: survival and genomic characteristics of a large tertiary care cohort. Clin Nucl Med 2019, 44, 544–549. [CrossRef] [PubMed]
- Gomes-Lima C., J. , Wu, D., Rao, S. N., Punukollu, S., Hritani, R., Zeymo, A., Burman, K. D. Brain metastases from differentiated thyroid carcinoma: prevalence, current therapies, and outcomes. Journal of the Endocrine Society 2019, 3, 359–371. [Google Scholar] [CrossRef]
- Eatz T, Levy A, Merenzon M, Bystrom L, Berry K, Morell A, Bhatia S, Daggubati L, Higgins D, Schlumbrecht M, Komotar RJ, Shah AH, Ivan ME. Surgically treated brain metastases from uterine origin: a case series and systematic review. World Neurosurg 2023, 173, e91–e108. [CrossRef] [PubMed]
- Vlachos N, Lampros MG, Filis P, Voulgaris S, Alexiou GA. Stereotactic radiosurgery versus whole-brain radiotherapy after resection of solitary brain metastasis: A systematic review and meta-analysis. World Neurosurg X. 2023, 18, 100170. [CrossRef] [PubMed]
- Rostampour N, Badrigilan S, Rezaeian S, Sarbakhsh P, Meola A, Choupani J, Doosti-Irani A, Nemati H, Almasi T, Chang SD. Efficacy of stereotactic radiosurgery as single or combined therapy for brain metastasis: A systematic review and meta-analysis. Crit Rev Oncol Hematol 2023, 186, 104015. [CrossRef]
- Blomain E, Berta S, Hug N, Giao D, Meola A, Binkley M, Hui C, Churilla T, Shahsavari N, Desai K, Chang S, Soltys S, Pollom E. Radiotherapy for brain metastases from thyroid cancer: an institutional and national retrospective cohort study. Thyroid. 2022, 32, 781–788. [CrossRef] [PubMed]
- Luo H, Liao X, Qin Y, Hou Q, Xue Z, Liu Y, Shen F, Wang Y, Jiang Y, Song L, Chen H, Zhang L, Wei T, Dai L, Yang L, Zhang W, Li Z, Xu H, Zhu J, Shu Y. Longitudinal genomic evolution of conventional papillary thyroid cancer with brain metastasis. Front Oncol. 2021, 11, 620924. [Google Scholar] [CrossRef] [PubMed]
- Alsabbagh R, Ahmed M, Alqudah MAY, Hamoudi R, Harati R. Insights into the molecular mechanisms mediating extravasation in brain metastasis of breast cancer, melanoma, and lung cancer. Cancers (Basel). 2023, 15, 2258. [CrossRef] [PubMed]
- Hermann EJ, Petrakakis I, Polemikos M, Raab P, Cinibulak Z, Nakamura M, Krauss JK. Electromagnetic navigationguided surgery in the semi-sitting position for posterior fossa tumours: a safety and feasibility study. Acta Neurochir 2015, 157, 1229–1237. [CrossRef] [PubMed]
- Hong B, Wiese B, Bremer M, Heissler HE, Heidenreich F, Krauss JK, Nakamura M. Multiple microsurgical resections for repeated recurrence of glioblastoma multiforme. Am J Clin Oncol. 2013, 36, 261–268. [Google Scholar]
- Bunevicius A, Fribance S, Pikis S, Lee JYK, Buch LY, Moran M, Yang AI, Bernstein K, Mathieu D, Perron R, Liscak R, Simonova G, Patel S, Trifiletti DM, Martínez Álvarez R, Martínez Moreno N, Lee CC, Yang HC, Strickland BA, Zada G, Chang EL, Kondziolka D, Sheehan J. Stereotactic radiosurgery for differentiated thyroid cancer brain metastases: an international, multicenter study. Thyroid. 2021, 31, 1244–1252.
- Colombo E, Ottini A, Licitra L. Oligometastatic disease from differentiated thyroid cancer: best treatment schemes. Curr Opin Oncol 2023, 35, 15–21. [CrossRef] [PubMed]
- Choi J, Kim JW, Keum YS, Lee IJ. The Largest known survival analysis of patients with brain metastasis from thyroid cancer based on prognostic groups. PLoS One. 2016, 11, e0154739. [Google Scholar]
- Park H, Park J, Park SY, Kim TH, Kim SW, Chung JH. Clinical course from diagnosis to death in patients with well-differentiated thyroid cancer. Cancers (Basel). 2020, 12, 2323. [CrossRef] [PubMed]
- Kiyota N, Robinson B, Shah M, Hoff AO, Taylor MH, Li D, Dutcus CE, Lee EK, Kim SB, Tahara M. Defining radioiodine-refractory differentiated thyroid cancer: efficacy and safety of lenvatinib by radioiodine-refractory criteria in the SELECT Trial. Thyroid 2017, 27, 1135–1141. [CrossRef] [PubMed]
- Kwon H, Kim JW, Park M, Kim JW, Kim M, Suh SH, Chang YS, Ahn SJ, Lee JM. Brain metastases from lung adenocarcinoma may preferentially involve the distal middle cerebral artery territory and cerebellum. Front Oncol. 2020, 10, 1664. [Google Scholar] [CrossRef] [PubMed]
- Kyeong S, Cha YJ, Ahn SG, Suh SH, Son EJ, Ahn SJ. Subtypes of breast cancer show different spatial distributions of brain metastases. PLoS One. 2017, 12, e0188542. [Google Scholar]
- Lee JS, Lee JS, Yun HJ, Chang H, Kim SM, Lee YS, Chang HS, Park CS. Prognosis of anaplastic thyroid cancer with distant metastasis. Cancers (Basel). 2022, 14, 5784. [Google Scholar] [CrossRef]
- Matsui JK, Perlow HK, Upadhyay R, McCalla A, Raval RR, Thomas EM, Blakaj DM, Beyer SJ, Palmer JD. Advances in radiotherapy for brain metastases. Surg Oncol Clin N Am. 2023, 32, 569–586. [Google Scholar] [CrossRef] [PubMed]
- Ha LN, Khanh LQ, Hanh NTM, Seo HJ, Son MH. Screening and treatment of brain metastasis from papillary thyroid carcinoma: a case series. Thyroid Res. 2023, 16, 1. [CrossRef] [PubMed]
- Meng J, Yan Z, Cheng W, Wang Z, Chen Z, You W, Wang Z. Long-term survival of patients with intracranial metastases from thyroid cancer presenting with seizures: a case report and literature review. Transl Cancer Res 2023, 12, 439–446. [CrossRef] [PubMed]
- Nahed BV, Alvarez-Breckenridge C, Brastianos PK, Shih H, Sloan A, Ammirati M, Kuo JS, Ryken TC, Kalkanis SN, Olson JJ. Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines on the Role of Surgery in the Management of Adults With Metastatic Brain Tumors. Neurosurgery 2019, 84, E152–E155.
- McWilliams RR, Giannini C, Hay ID, Atkinson JL, Stafford SL, Buckner JC. Management of brain metastases from thyroid carcinoma: a study of 16 pathologically confirmed cases over 25 years. Cancer 2003, 98, 356–62. [CrossRef] [PubMed]
- Sheu NW, Jiang HJ, Wu CW, Chiang FY, Chiou HC, Hsiao PJ. Lenvatinib complementary with radioiodine therapy for patients with advanced differentiated thyroid carcinoma: case reports and literature review. World J Surg Oncol. 2019, 17, 84. [CrossRef]
- Slutzky-Shraga I, Gorshtein A, Popovitzer A, Robenshtok E, Tsvetov G, Akirov A, Hirsch D, Benbassat C. Clinical characteristics and disease outcome of patients with non-medullary thyroid cancer and brain metastases. Oncol Lett. 2018, 15, 672–676.
- Akiba T, Kunieda E, Kogawa A, Komatsu T, Tamai Y, Ohizumi Y. Re-irradiation for metastatic brain tumors with whole-brain radiotherapy. Jpn J Clin Oncol. 2012, 42, 264–269. [CrossRef] [PubMed]
- Chiu AC, Delpassand ES, Sherman SI. Prognosis and treatment of brain metastases in thyroid carcinoma. J Clin Endocrinol Metab. 1997, 82, 3637.
Figure 1.
Template of Kaplan-Meier survival analyses and corresponding 95% confidence intervals of predictors in Cox regression analyses. 1 Number of metastases; 2 Duration from initial diagnosis to brain metastases; 3 Neurological deficits; 4 Number of intracranial lesions.
Figure 1.
Template of Kaplan-Meier survival analyses and corresponding 95% confidence intervals of predictors in Cox regression analyses. 1 Number of metastases; 2 Duration from initial diagnosis to brain metastases; 3 Neurological deficits; 4 Number of intracranial lesions.
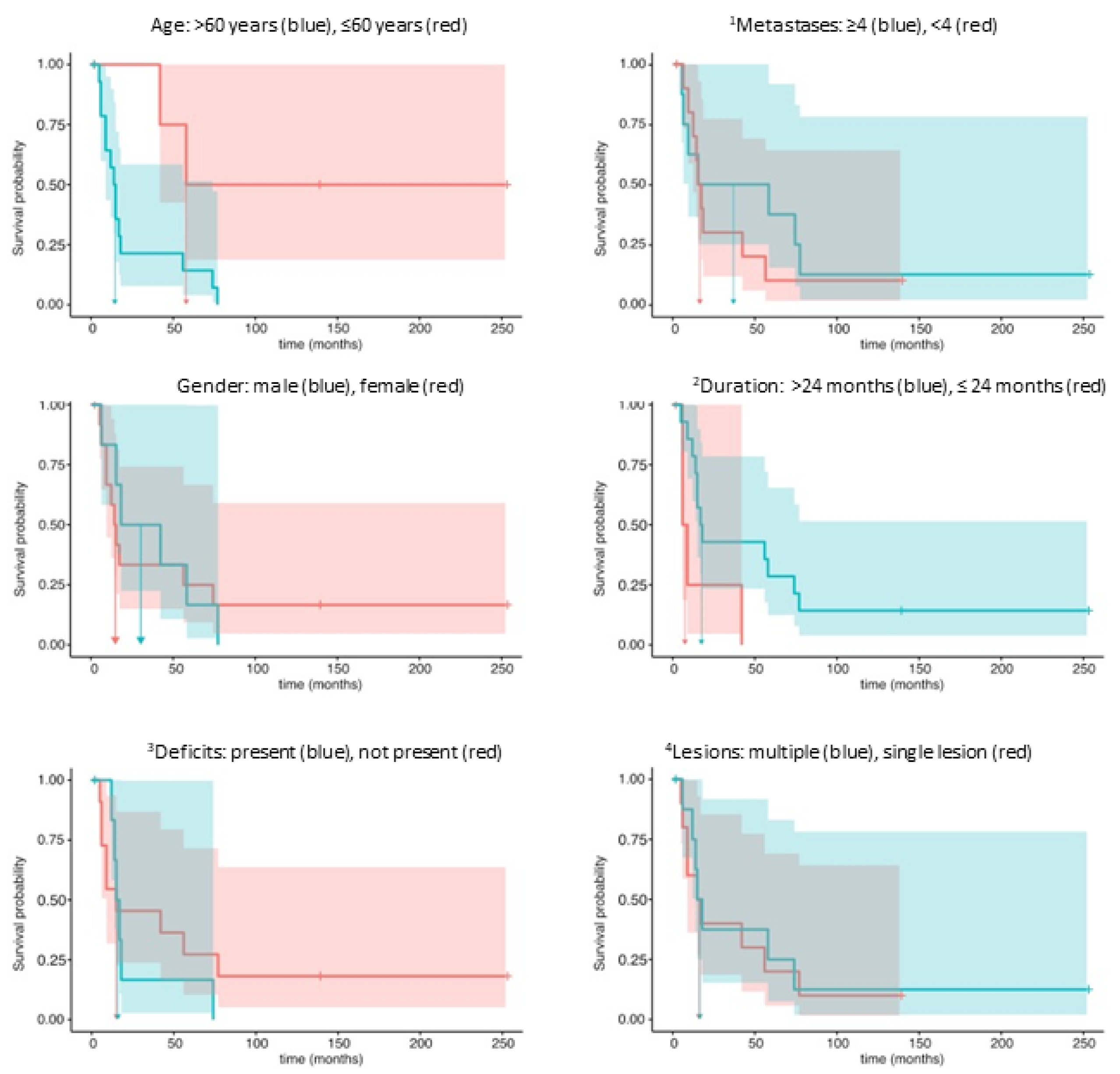

Table 1.
Set of predictors for the Cox regression model.
| Predictor | Meaning | Threshold | Unit |
|---|---|---|---|
| Age | patients’ age | ≤60, >60 | years |
| Duration | time interval between the initial and brain metastasis diagnostics | ≤24, >24 | months |
| Metastases | number of metastases found | ≤4, >4 | |
| Neurological deficits | existence of neurological deficits | yes, no | |
| Gender | patient gender | male, female | |
| Lesions | number of intracranial lesions | single, multiple |
Table 2.
Demographic and clinical characteristics at the time of BM diagnosis.
| N | |
|
Mean age at BM diagnosis (yr) |
64.8 (26-89) |
|
Mean interval between initial diagnosis to BM diagnosis (months) |
63.4 ± 58.4 |
|
Mean interval between BM diagnosis to death (months) |
41.2 ± 60.7 |
|
Symptoms associated with BM |
|
| Yes | 11 |
| No | 9 |
|
Modalitiy of diagnosis |
|
| MRI | 8 |
| CT | 6 |
| FDG-PET-CT | 3 |
| 131J-Scinti | 3 |
|
KPSS |
|
| > 70% | 17 |
| ≤ 70% | 3 |
|
Number of intracranial lesions |
|
| Single | 10 |
| Multiple | 10 |
|
Number of distant metastases |
|
| ≤ 3 | 11 |
| > 3 | 8 |
| Unknown | 1 |
|
Treatment |
|
| Surgery | 15 |
| Radiosurgery | 1 |
| WBRT | 3 |
| Isotretinoin | 1 |
|
Postoperative adjuvant therapy |
|
| WBRT | 10 |
| RCT | 1 |
| Radioactive iodine | 1 |
| WBRT + TKI | 1 |
| WBRT + Isotretinoin | 1 |
| None | 6 |
WBRT: Whole brain radiation therapy, RCT: Radiochemotherapy, TKI: Tyrosinkinase inhibitor, KPS: Karnofsky performance score.
Table 3.
Multivariate analysis of covariates.
| Covariate | Coef | HR | 95% - CIcoef | LR Test | p | unit |
|---|---|---|---|---|---|---|
| Age (>60) | 1,8228 | 6.1892 | 0,6865, 3,5655 | chi2(1) = 12,0981 | 0.0005 | years |
| Duration (>24) | -1,5682 | 0.2084 | -2,8077, -0,5466 | chi2(1) = 9,2470 | 0.0024 | months |
| Metastases (<4) | 0,4846 | 1.6235 | -0,1578, 1,2459 | chi2(1) = 2,1383 | 0.1437 | |
| Neurological deficits (no) | -0,2417 | 0.7853 | -1,1459, 0,7033 | chi2(1) = 0,2721 | 0.6020 | |
| Gender (female) | 0,0712 | 1.0738 | -0,5441, 0,7342 | chi2(1) = 0,0501 | 0.8229 | |
| Lesions (multiple) | -0,0267 | 0.9737 | -0,7675, 0,7816 | chi2(1) =0,0048 | 0.9450 |
HR::Hazard ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



