
Submitted:
10 June 2024
Posted:
11 June 2024
You are already at the latest version
Abstract
Although vitamin D deficiency has been correlated with an increased risk of cardiovascular disease (CVD), there are few data on the association between 25-hydroxyvitamin D (25(OH) D) and atherogenic indices predictive of CVD. This study aimed to investigate the relationship of vitamin D status with lipid profile and atherogenic indices in adult women in Morocco. Three hundred healthy women, aged 18 to 50 years, from Meknes were included. Fasting 25(OH) D and lipid concentrations were determined using a one-step electrochemiluminescence-based immunoassay and an enzymatic method, respectively. Atherogenic indices (Atherogenic index of plasma (AIP), non-HDL cholesterol (Non-HDL-C), Atherogenic coefficient (AC), Castelli risk indices I and II (CRI-I and II), and CHOLIndex (CI)) were calculated using conventional lipid parameters. Logistic regression models and operating characteristic curve (ROC) analysis were used to assess the relationship of the variables and estimate the threshold of 25(OH) D levels associated with high atherogenic indices. 25(OH) D below 20 ng/ml was significantly associated with an enhanced risk of hypertriglyceridemia and elevated values of AIP, AC, Non-HDL-C, and CRI-I with an OR (95% CI) of 4.904 (1.856-12.959); 3.637(2.149-6.158); 3.589(1.673-7.700); 2.074(1.215-3.540), and 2.481(1.481-4.123), respectively. According to ROC analysis, the likelihood of hypertriglyceridemia and high values of AIP, AC, Non-HDL-C, and CRI-I were associated with 25(OH)D thresholds ≤15.15 ng/ml, ≤ 17.5 ng/ml, ≤ 19.8 ng/ml, ≤ 20.1 ng/ml and ≤ 19.5 ng/ml, respectively, all p < 0.01. Based on atherogenic indices, this study indicates that vitamin D below 20 ng/ml may increase the risk of cardiovascular disease in adult women. Additional health efforts are needed to raise awareness among women and healthcare providers in preventing and controlling cardiovascular risk factors.
Keywords:
Vitamin D
; 25-OH vitamin D
; Dyslipidemia
; Atherogenic indices.
1. Introduction
Vitamin D deficiency is a widespread pandemic worldwide, regardless of age, gender, and country of origin [1]. Low 25(OH)D levels have been shown to be associated with many potential adverse health consequences, such as cancers, autoimmune disorders, infectious diseases, type 1 and 2 diabetes, neurological disorders, and cardiovascular illnesses [1,2,3,4,5,6,7,8]. Several studies have suggested an inverse association between 25(OH)D and biomarkers of cardiovascular risk, including an atherogenic lipid profile [9,10,11,12,13,14,15]. The cardiovascular system is a target for vitamin D. VDR and 1-α-hydroxylase are expressed by cardiomyocytes, smooth muscle cells, and vascular endothelial cells, mainly fibroblasts[16]. Local vitamin D activation by the VDR has various potential cardiovascular benefits, including reduced renin production [17,18], relaxation of vascular smooth muscle cells, and reduced output of atherosclerosis-forming foam cells [19,20]. Vitamin D can also reduce inflammation, which is integral to the development of cardiovascular disease (CVD)[19,21,22].
Cardiovascular disease is the leading cause of mortality and morbidity worldwide, representing 32% of all deaths in 2019 [23,24]. In Morocco, 2 out of 5 deaths are attributable to CVD (38%), making it the leading cause of death nationwide [25]. CVD is also the leading cause of death in women worldwide and was responsible for 35% of all deaths in 2019 [26]. Contrary to popular belief, cardiovascular disease does not just affect older men and women. This type of problem also increasingly affects young women, with other alarming trends, such as the stagnation in the incidence and mortality of coronary heart disease and the increase in acute myocardial infarction, particularly in younger women (<55 years) [27,28,29]. The national survey (Stepwise) on the risk factors (RF) of non-communicable diseases (NCDs) conducted by the Ministry of Health in 2018 showed that 94.3% of Moroccans aged 18 and over present at least an RF for NCDs, and the prevalence of cardiovascular risk is 4.9%[30].
Dyslipidemia, which refers to elevated levels of total cholesterol (TC), triglycerides (TG), and low-density lipoprotein cholesterol (LDL-C), and decreased levels of high-density lipoprotein cholesterol (HDL-C) has been identified as significant risk factors for atherosclerosis and cardiovascular disease [31,32]. Several Cross-sectional studies have reported an association of vitamin D with lipid levels and CVD risk [33,34,35,36]. Nevertheless, the association between 25-hydroxyvitamin D concentrations and serum lipids is inconsistent in various studies [37,38]. It has been argued that different combines of these lipid profile parameters, such as the Castelli Risk Index-I (CRI-I), the CRI-II, the Atherogenic Coefficient (AC), the CHOLIndex and the Atherogenic Index of Plasma (AIP), are diagnostic alternatives for predicting the risk of developing cardiovascular events and identifying high-risk individuals[39,40,41,42,43,44,45,46,47]. A few studies have assessed the relationship between vitamin D and atherogenic biomarkers. Moreover, most of these studies have been conducted on elderly patients, people with diabetes, or patients with metabolic syndrome[48,49].
Despite the increase in cardiovascular disease risk factors among young people in Morocco and the elevated vitamin D deficiency, particularly among adult women under 50 years of age, estimated at 78.8% in 2019 [50], no study has addressed the association between vitamin D and the biomarkers of cardiovascular disease in this population. Thus, this study aimed to assess the relationship between vitamin D insufficiency, lipid profile and atherogenic indices in apparently healthy women aged 18-50 years, and to estimate the optimal 25 (OH) D threshold for maintaining lipid parameters and atherogenic indices at least at limit normal values.
2. Materials and Methods
2.1. Study Design and Population
This cross-sectional study was conducted in an accredited private medical analysis laboratory in Meknes (Morocco). Three hundred apparently healthy women aged between 18 and 50 years meeting inclusion criteria were recruited between June and November 2022. The sample size was calculated based on national data on hypovitaminosis D in women aged 18–49 years, using the Cochrane formula [51]: n0= z2pq/ e2 (Z = 1.96 for 95%; p=78.8% corresponding to the prevalence of hypovitaminosis D reported in the National Nutrition Survey (ENN 2019) [50]; q is 1-p, and e is the desired level of precision set at 5%). Thus, 256 participants were required to obtain statistically representative data.
Exclusion criteria included participants suffering from malabsorption diseases, cancer, liver and kidney disorders, pregnant or lactating women, women who had taken vitamin D supplements in the last six months, and women on drugs known to alter vitamin D metabolism. Women with cardiovascular diseases (e.g., myocardial infarction, stroke…) and diabetes mellitus were also excluded (Figure 1).
Ethical approval (protocol codes CERB-UMI 201901 (January 2019) was received from the Ethics Committee for Biomedical Research of the Moulay Ismail University of Meknes. All women were included after obtaining written informed consent.
2.2. Physical Activity and Sun Exposure Scores Assessment
The scores questionnaire was conducted in a face-to-face interview and supplemented with a demographic questionnaire. Additionally, screening for any diseases that would preclude participation in the study and collecting participants' medical history and anthropometric data was performed.
2.2.1. Physical Activity Assessment
The International Physical Activity Questionnaire-Short Form (IPAQ-S) measured physical activity data. The amount of time per week spent walking, sitting, and engaging in moderate- to vigorous-intensity activities was calculated. Total physical activity in MET/min/week was calculated as follows: (daily minutes of walking x days per week with walking x 3.3) + (daily minutes of moderate-intensity activity x days per week with moderate-intensity activity x 4.0) + (daily minutes of vigorous activity x days per week with vigorous activity x 8.0) [52].
Based on frequency, duration, and intensity of physical activity, participants were categorized into three levels of physical activity based on their overall physical activity: low (<600 METs/min/week), moderate (≥600–2999 METs/min/week) and high (≥3000 METs/min/week) [53].
2.2.2. Sun Exposure Assessment
Sun exposure was assessed using a validated weekly score [54]. The questionnaire comprises two variables: the first covers behaviors influencing sun exposure, such as duration, time slot, frequency of exposure, exposed body part, and sun protection practices, divided into three domains (indoor exposure, outdoor exposure, and sun protection practices). The second is a two-factor adjustment variable: skin phototype based on Fitzpatrick's skin type [55] and weather conditions. The total sun exposure score was calculated as the sum of the scores for the three domains x phototype score x outdoor weather conditions score.
2.3. Anthropometric and Laboratory Assessment
Height in centimeters (cm) and weight in kilograms (kg) were determined following a standard procedure to the nearest 0.1 cm and 0.5 kg, respectively. Body mass index (BMI) was calculated based on the formula: BMI = weight (kg)/height (m)2. Obesity was defined as a BMI ≥ 30.0 kg/m2, and overweight as a BMI between 25.0 and 29.9 kg/ m2 [56].
Fasting venous blood of 10 ml was collected. The serum was centrifuged at 2000 rpm for 10 min and analyzed on the day. Serum 25(OH) D concentration and serum lipids (TC, TG, and HDL-C) were determined using a one-step electrochemiluminescence-based immunoassay and an enzymatic method, respectively. All the laboratory analyses above were carried out using the Abbott Architect ci 4100 Chemistry Analyzer. The concentration of LDL-C was determined using the Friedewald equation for participants with a TG < 400mg/dl (LDL-C = TC – (HDL-C + TG/5))[57]
2.3.1. Vitamin D, Lipids Profiles, and Atherogenic Indices Evaluation
According to Institute of Medicine (IOM) criteria, vitamin D deficiency was defined as 25(OH)D < 12ng/ml, insufficiency as 25(OH)D between 12ng/ml and 20ng , and adequacy as 25(OH) D >20ng [58,59].
Participants' lipid profiles were determined based on NCEP ATP III (2001) classification and V Brazilian Guidelines on Dyslipidemia and Prevention of Atherosclerosis [60,61]. The threshold for each dyslipidemia was as follows: TC concentration ≥200 mg/dL; LDL-C ≥130 mg/dL; TG >150 mg/dL; and HDL-C <50 mg/dL.
AIP = Log (TG/HDL-C)
Non-HDL-C = TC – HDL-C
AC = (TC−HDL-C)/HDL-C
CRI-I = TC/HDL-C
CRI-II = LDL-C/HDL-C
CI = LDL-C – HDL-C (TG < 400 mg/dL) =
= LDL-C – HDL-C + 1/5 TG (TG > 400 mg/dL)
2.4. Statistical Analysis
Statistical analysis was performed using R statistical software (version 4.2.1 R Foundation for Statistical Computing). Descriptive characteristics of participants were presented as medians ± IQR for non-normally distributed continuous variables and expressed as means ± SD for normally distributed continuous variables, determined by a Kolmogorov-Smirnov test. The data at baseline were divided into 25(OH) D levels, and the differences in these variables were tested using Mood's median test for non-normally distributed variables, the ANOVA test for normally distributed variables, and Pearson's chi-squared test for categorical variables. The association of lipid profile and atherogenic indices with age, BMI, physical activity, sun exposure, and 25(OH) D was analyzed using Spearman's rank correlation coefficient. The distribution of 25(OH) D concentrations according to lipid parameters and atherogenic indices was represented using a box plot. A logistic regression analysis model was applied to assess the associations between abnormal atherogenic indices and 25(OH) D level, expressed as odds ratios (OR) with 95% confidence intervals (CI). For multiple regression analysis, vitamin D status was reported as sufficient (>20 ng/mL) and insufficient (<20 ng/mL). The receiver operating characteristic (ROC) curve and area under the curve (AUC) were used to calculate the accuracy of 25(OH) D in predicting high atherogenic indices. The best cutoff points were the concentration of serum 25(OH)D at the associated criterion of the highest Youden Index from the ROC analysis using the MedCalc software (MedCalc® Statistical Software version 22.009 (MedCalc Software Ltd., Ostend, Belgium) [63]. All p-values were at the two extremes, and the value < 0.05 was considered statistically significant.
3. Results
3.1. Characteristics of Participants according to 25(OH) D Status
In this cross-sectional study of 300 healthy women with a median age of 38, the results showed that 67.6% of participants had a 25(OH)D level below 20 ng/ml, with 34.6% presenting a severe vitamin D deficiency of less than 12 ng/ml, with a median total level of 13.97 ng/ml. Assessment of the lipid profile revealed dyslipidemia in 33.3% of participants. According to the atherogenic index of plasma (AIP), 60.7% of subjects were at high risk of CVD. Abnormal HDL-C, AC, CRI-I, and CRI-II ratios were identified in 43%, 22.3%, 59%, and 6% of participants, respectively (Table 1).
Table 1 shows that vitamin D-deficient participants were younger (33 vs. 41, p=0.006), more obese (26.2% vs. 6.2%, P=0.001), and had the lowest sun exposure scores (13.21 vs 18.35, P<0.0001) compared with vitamin D sufficient status participants.
Concerning participants' lipid profile and atherogenic indices according to vitamin D status, the results of Mood's median test and ANOVA test showed that TG, AIP, Non-HDL-C, AC, , CRI I, CRII, and CI levels decreased significantly with improving serum vitamin D status (1.16 vs 0.81, P <0.0001; 0.30 vs 0.11, P <0.0001; 1.29 vs 1.10, P =0.004, 2.35 vs 1.82, P <0.0001; 3.35 vs 2.82, P <0.0001; 1.91 vs 1.63, P=0.035, and 0.52 vs 0.38, P=0.011, respectively). However, no differences were noted in TC, HDL, and LDL levels compared to vitamin D status.
3.2. Association of Lipid Profiles, and Atherogenic Indices with 25(OH) D Concentrations
The association of lipid profile and atherogenic indices with age, BMI, physical activity, and sun exposure scores was analyzed using Spearman's rank correlation coefficient. As show in table 2, BMI was positively correlated with AIP, AC, Non-HDL-C, CRI, and CHOLIndex values, as well as TC, LDL-C, and TG serum concentrations. The results of Table 2 revealed that sun exposure and physical activity scores were positively associated with HDL-C; and negatively associated with TG, AIP, AC, CRI-I, and CRI-II. Physical activity was also negatively associated with Non-HDL-C and CHOLIndex. However, no association was found between those parameters with age.
Non-parametric regression analysis was used to evaluate the associations of serum 25(OH) D concentrations with lipid profile and atherogenic indices. Figure 2 illustrates that 25(OH)D could account for 13,4% of the variability seen in the AIP, 9.8% of TG, 6.4% of AC, 6% of Non-HDL-C and CRI-I, p<0.0001. Regarding the association with lipid profile, 25(OH) D serum concentrations was negatively associated with TC, LDL-C, TG, and positively associated with HDL-C.
Table 3 showed that per 1 ng/ml increase in serum 25(OH) D was associated with decreases of 1.53 mg/dl in TG, 0.55 mg/dL in TC, and 0.49 mg/dl in LDL-C and an increase of 0.22 mg/dL in HDL-C. We also found a significantly negative association between 25(OH) D and all atherogenic indices. Each 1 ng/mL increase in 25(OH) D serum was associated with decreases of 0.817 mg/dl in non-HDL-C, 0.009 in AIP, 0.021 in AC and CRI-I, 0.012 in CRI-II and 0.006 in CHOLIndex, respectively.
Figure 3 illustrates that participants with high levels of TG, AIP, AC, Non-HDL-C, and CRI I had markedly reduced levels of 25(OH)D concentration compared with those in the normal-group ( 10.40 vs 15.6, p=0.001; 11.5 vs 20.4, p<0.0001; 11.5 vs 15.15, p=0.027; 11.89 vs 15.5, p=0.020; 12.02 vs 17.7, p=0.002, respectively). However, there was no significant association between 25(OH) D serum and elevated TC, HDL-C, LDL-C, and CRI-II levels.
3.3. The Association between 25(OH) D Level and the Occurrences of Hypertriglyceridemia and High Atherogenic Indices
To assess whether the 25(OH) D level relationship with hypertriglyceridemia and high atherogenic indices values differs by vitamin D status, we categorized the participants into two subgroups: vitamin D insufficiency and vitamin D sufficiency.
Binary logistic regression adjusted for IBM, physical activity, and sun exposure score showed that increasing serum 25(OH)D concentration significantly reduced the probability of having an elevated level of triglycerides, AIP, AC, Non-HDL-C, and CRI-I with an OR (95% CI) of 0.954 (0.916–0.993), p=0.023, 0.940. (0.915–0.965), p<0.0001, 0.958 (0.922–0.995), p=0.026, 0.962 (0935–0.991), p=0.011 and 0.971 (0.948–0.994), p = 0.017, respectively (Table 4).
According to vitamin D status, multinomial logistic regression in Table 4 showed that 25(OH)D below 20 ng/ml was significantly associated with an increased risk of hypertriglyceridemia and elevated indices of AIP, AC, non-HDL-C, and CRI-I with an OR (95% CI) of 4.904 (1.856–12.959), p=0.001, 3.637 (2.149–6.158), p<0.0001, 3.589 (1.673–7.700), p=0.001, 2.074 (1.215–3.540), p=0.007, and 2.481 (1.481–4.123), respectively after adjusting for BMI ( Model 1). The ORs then decreased slightly but remained significant after adjusting for BMI, physical activity, and sun exposure score (Model 2)
ROC curve analysis was used to analyze the prognostic accuracy of 25(OH) D and to specify the optimal Cutoff predictive of hypertriglyceridemia and high levels of atherogenic indices. The results showed that the area under the curve (AUC) of the association of 25(OH)D with hypertriglyceridemia and atherogenic indices was significantly good, indicating that decreased vitamin D concentration predicted increases in TG levels (AUC= 0. 669, p<0.0001, Cutoff ≤ 15.15 ng/ml), AIP levels (AUC= 0. 702, p<0.0001, Cutoff ≤ 17.5 ng/ml), AC levels (AUC= 0.615, p= 0.004, Cutoff ≤ 19.8 ng/ml), Non-HDL-C levels (AUC= 0.609, p= 0.001, Cutoff ≤ 20.1 ng/ml) and CRI-I levels (AUC=0.626, p<0.0001 Cutoff ≤ 19.5 ng/ml). The results of the ROC curve are reported in Table 5 and Figure 4.
4. Discussion
Vitamin D deficiency and insufficiency is an epidemic health problem worldwide. This study showed that 67.6% of women aged 18-50 suffered from vitamin D insufficiency below 20 ng/ml. This prevalence is roughly in line with that reported in other studies. In Morocco, the national nutrition survey [50] revealed vitamin D insufficiency in 78.8% of women aged 18 to 49. In the United Arab Emirates, a study of migrant women from Arab and South Asian countries aged 18 and over revealed an overall prevalence of vitamin D deficiency < 20ng/ml of 67% [64]. In a cross-sectional study in China, Wang et al. [33] reported vitamin D deficiency in 63.7% of adult women. The causes of vitamin D deficiency in adult women could be explained by conservative clothing, lack of sun exposure, relatively high obesity, and low vitamin D dietary intake [54,65,66,67,68,69].
Hypovitaminosis D has recently been implicated in several health conditions, such as cardiovascular disease. Crowe et al. [70], in a large prospective UK study of 180,263 patients aged 18 and over with no history of CVD, suggested that circulating 25(OH)D concentrations below 15 ng/ml are associated with an increased risk of CVD. A meta-analysis of 34 publications involving 180,667 participants found an inverse association between serum 25(OH)D levels and total cardiovascular events, and the pooled RRs per 10-ng/mL increment were 0.90 (95% CI: 0.86, 0.94) for total CVD events [71].
Various explanations for the role of vitamin D in the development of cardiovascular disease have been suggested. Previous studies have supported that vitamin D may reduce the risk of CVD by inhibiting the renin-angiotensin system [17,18], decreasing parathyroid hormone levels, reducing inflammation, lowering coagulation, subsequently reducing atherosclerosis, and increasing insulin production[19,21,22]. Vitamin D may also prevent cardiovascular disease by regulating several genes involved in cell differentiation, proliferation, apoptosis, and angiogenesis [72]. In fact, another proposed mechanism for the protective effect of vitamin D on CVD is the control of lipid parameters [11,12,33,73,74,75,76]
In the present study, lipid profile assessment revealed dyslipidemia in 33.3% of all participants. Non-parametric regression showed that 25(OH)D concentration was inversely associated with TC, TG, and LDL-C levels and positively associated with HDL-C. Per of 1ng/ml in 25(OH)D serum was associated with decreases of 1.53 mg/dl in TG, 0.55 mg/dl in TC, 0.49 mg/dl in LDL-C, and an increase of 0.22 mg/L in HDL-C. These results are consistent with previous research on the association between 25(OH) D and lipid parameters. In Southern Thailand, Jeenduang and Sangkaew [35] showed that serum 25(OH)D was negatively correlated with TC, TG, and LDL-C levels in women. Wang et al. [33] in a study of 646 Chinese adult women, showed that serum 25(OH)D levels were inversely associated with LDL-C and positively associated with TC after adjustment for age and BMI. However, there was no significant association with HDL-C and TG. The authors reported that each 10 nmol/L increase in 25(OH) D concentration was associated with a 0.25 mmol/L decrease in LDL-C and a 0.39 mmol/L increase in TC in women [33]. In the Very Large Database of Lipids (VLDL) included 20,360 adults (≥18 years of age) in the United States, Lupton et al. [77] showed that deficient serum 25(OH)D below 20 ng/ml was associated with significantly lower serum HDL-C (-5.1%) and higher TC (+9.4%), LDL-C (+13.5%), and TG (+26.4%) when compared with the optimal group.
Vitamin D insufficiency was associated with triglyceride dyslipidemia, with an OR (95% CI) adjusted for BMI, physical activity, and sun exposure of 3.876 (1.427-10.525), p=0.008. In contrast, there was no significant association of vitamin D status with TC, LDL, and HDL dyslipidemia. These results are consistent with those of Alquaiz et al.[11], in their study of apparently healthy men and women, showed a significant excess odds ratio for elevated TG levels in association with 25(OH) D deficiency in women (AOR = 3.0; 95% CI = 1.1, 7.9), but not in men. Similarly, Jeenduang and Sangkaew [35] showed that elevated serum 25(OH)D levels were associated with a reduced risk of hypertriglyceridemia and reduced HDL-C levels, particularly in women. Furthermore, our study revealed that a serum vitamin D level ≤ 15.15 ng/ml may predicts the likelihood of hypertriglyceridemia with a sensitivity of 77.19% and a specificity of 52.26%.
The pathophysiology of vitamin D deficiency leading to lipid profile is unclear. Multiple mechanisms could explain the relationship between vitamin D and lipid and lipoprotein concentrations. Previous data suggest that increased intestinal calcium absorption may reduce fatty acids in the gut due to the formation of insoluble calcium fatty acid soaps complexes, increase fat absorption and reduce hepatic triglyceride levels [78]. Serum LDL-C levels are thought to be reduced by decreased fat absorption, particularly of saturated fatty acids [79,80]. Moreover, calcium may favor the translation of cholesterol into bile acids, thus reducing cholesterol levels [81]. Vitamin D has also been shown to play a role in cholesterol transport by regulating apolipoprotein A-1 levels, and may act to reduce LDL-C uptake, decrease foam cell formation and increase HDL-C production [82]. In addition, previous studies have provided strong evidence that vitamin D deficiency could be linked to altered B-cell function and insulin resistance, which may affect lipoprotein metabolism and eventually lead to elevated TG levels and decreased HDL-C levels [83,84]. Similarly, vitamin D can affect lipoprotein metabolism, with Larrick et al.[85], demonstrating that by regulating the expression of genes involving lipid metabolism, vitamin D enhances HDL-C levels, decreases fatty acid synthesis and improves fatty acid β-oxidation, thereby lowering triglyceride levels.
An alternative explanation of this association may be related to confounding factors affecting both 25(OH)D and lipid levels. For example, obesity, lower amounts of physical activity and sun exposure. Our results showed that vitamin D deficiency and insufficiency was associated with high BMI, and low physical activity and sun exposure scores. These results are similar to other studies [65,86,87,88,89,90] . In addition, this study showed that BMI has positively significant association with TC, TG and LDL-C, which could increased risk of dyslipidemia and obesity-related cardiovascular events [91,92,93]. In Morocco, there has been an alarming increase in the number of overweight and obese women (29.2% and 28.4%, respectively) [50]. Associated with these changes in BMI, other pathologies may emerge, such as metabolic syndrome and diabetes, which increase the risk of developing CVD. Excess adipose tissue appears to be directly responsible for the dyslipidemia associated with abdominal obesity, by inducing an increase in the flow of free fatty acids to the liver and contributing to insulin resistance[94].
Moreover, sun exposure and physical activity scores were found positively associated with HDL-C and negatively associated with TG levels. Weller [95] demonstrated that exposure to sunlight has health benefits independently of Vitamin D. The skin contains significant stores of nitrogen oxides, which can be converted to NO by UV radiation and exported to the systemic circulation, thus causing arterial vasodilation, decreased blood pressure. Other studies suggest that enhancing the bioavailability of nitric oxide could have beneficial effects on obesity and the lowering of triglyceride levels [96,97]. Additionally, regular physical activity and fitness have shown inverse associations with cardiovascular disease in many observational studies [98,99,100]. It has been shown that physical activity can lead to significant positive changes in lipid profile [101,102].
Other than these risk factors, the identification and validity of new measures of cardiovascular disease risk have attracted considerable recent interest. In fact, atherogenic indices, including AIP, AC, CRI-I, Non HDL-C and others, have been proposed as alternative biomarkers to diagnose individuals at CVD risk beyond the usual risk factors [40,45,103]. The AIP was suggested by the National Cholesterol Education Program [60], as a powerful predictor of atherosclerosis and coronary heart disease could be used as an effective mass screening method to identify patients at high risk of cardiovascular events [103,104]. Non-HDL-C was recommended by the 2019 ESC/EAS guidelines for the management of dyslipidemia as an effective biomarker for the estimation of cardiovascular risk in subjects with elevated TG levels, T2DM, obesity or a very high risk of cardiovascular events. low LDL levels [105]. For CRI-I it has been particularly shown to reflect coronary plaque formation and intima-media thickness in the carotid arteries of young adults [39].
The current study showed elevated cardiovascular risk according to atherogenic indices values, in particular AIP, CRI-I, non-HDL-C, and AC (60.7%, 59%, 43%, and 22.3% respectively). Molani et al. [62], in adults healthy women reported that the prevalence of elevated AIP, AC, CI, CRI-I, CRI-II and non-HDL-C indices were 64.5%, 36.2%, 20.4%, 77%, 7.2% and 44.7%, respectively. According to AIP levels, Fernández-Macías et al.[46], showed that around 55% of healthy Mexican women aged 18 and over were at moderate or high risk of cardiovascular disease. Wang et al. found a lower incidence among Chinese women, at 25% [33].
25(OH)D values were negatively and independently correlated with AIP, AC, Non-HDL-C and CRI-I levels. Logistic regression showed that vitamin D insufficiency compared with the sufficient group increased significantly the risk of elevated AIP, AC, Non-HDL-C and CRI-I values with an OR (95% CI) of 3.637(2.149-6.158), p<0.0001; 3.589(1.673-7.700), p=0.001; 2.074(1.215-3.540), p=0.007, and 2.481(1.481-4.123), respectively, after adjustment for BMI. These findings corroborate those presented in other studies. Lupton et al. [77] showed that serum 25(OH) D deficiency (<20 ng/ml) was associated with higher levels of non-HDL-C (+15.4%, +20.3 mg/dL). Barbalho et al. reported that patients with impaired vitamin D values had significantly higher values of CRI-I, CRI-II and non-HDL-C [8]. Similarly, Pokhrel et al. [107], demonstrated that 25 (OH) D was negatively associated with AIP, AC and non-HDL-C. In addition, in a longitudinal community study of 13,039 participants in the ARIC (Atherosclerosis Risk in Communities) study, Faridi et al. [108], reported that deficient 25(OH)D was prospectively associated with greater CRI-I ratio after considering factors such as diabetes and adiposity.
A gender difference was reported by Wang et al. who showed that vitamin D levels were inversely significantly associated with AIP levels in men, but not in women [33]. Huang et al. confirmed a relatively stronger association of AIP and vitamin D in men [36], while, Izadi et al. showed a significant negative association of vitamin D and AIP in both sexes [106]. Mahmoodi et al. [49], in a case-control study among participants with T2DM found that all atherogenic indices including AIP, CRII, and AC decreased significantly with improving serum vitamin D status in men in the control group only. Although, the trends of the levels of atherogenic indices were irregular in case and control females with improving vitamin D status. Furthermore, studies in children and young adolescents revealed an inverse association between vitamin D levels and atherogenic indices [109,110,111,112]. Thus, maintaining adequate vitamin D status contributes to the early prevention of cardiovascular disease in individuals with or without risk factors.
ROC curve analysis showed that a decrease in vitamin D concentration independently predicted an increase in atherogenic index values. Thresholds predicting elevated AIP, AC, non-HDL-C, and CRI-I values were serum 25(OH) D ≤ 17.5 ng/ml, ≤ 19.8 ng/ml , ≤ 20.1 ng/ml, and ≤ 19.5 ng/ml respectively, all p<0.001. These results attest that serum 25(OH) D concentrations below 20 ng/ml imply an increased risk of short- or long-term cardiovascular disease. In contrast, Barbalho et al. [8] showed that for an individual to maintain triglycerides, CRI-I , CRI-II, and non-HDL-C metabolic parameters, at least at borderline values, the levels of VD should be 37.64; which is above the reference values; implying that further in-depth studies are needed to determine the 25(OH)D threshold value predictive of dyslipidemia and high levels of atherogenic indices.
Our study has several limitations. Firstly, the generalizability of the results of our study to the general population is limited; the study sample was based solely on women from the city of Meknes. Due to the cross-sectional nature of this study, the results should not be considered in terms of cause and effect relationships. Another limitation is the absence of baseline data affecting lipid and vitamin D status, such as dietary intake, which can provide information on participants' daily lipid and vitamin D intake. Finally, although the sample size was sufficient to achieve the required significance, a larger sample could have strengthened the results.
Despite these limitations, the study is well founded. This is the first study to examine healthy adult women and evaluate the association of vitamin D with lipid and atherogenic profiles in Morocco. This could open up new avenues of research and diagnosis in the scientific and medical fields.
5. Conclusions
Vitamin D deficiency and insufficiency is common among adult women in Morocco, and a 25(OH)D serum below 20 ng/ml appears to be correlated with elevated triglyceride and atherogenic indices, particularly those known to be predictors of premature atherosclerosis and coronary events. Randomized controlled trials (RCTs) are warranted to determine the adequate level of vitamin D that reduces the risk of cardiometabolic diseases. Thus, additional health efforts are needed to raise awareness among women and healthcare providers about the prevention and control of metabolic and cardiovascular risk factors.
Author Contributions
Conceptualization, L.I. and Z.N.; methodology, L.I.; data collection and processing, L.I. and Z.N.; statistical processing, L.I. and F.-Z.Y.; writing—original draft preparation, L.I.; scientific supervision, E.M.A., G.L., and F.-Z.Y.; supervision of the study and validation of the manuscript E.M.A., G.L., F.-Z.Y. and E.J.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Institutional University Cooperation Program with Moulay Ismail University, which is funded by the VLIR-UOS (Phase I: 2017–2021; Contract n°MA2017IUC038A104) and by the Research and Development Project “SEBIO” (Morocco, PDR-MA-SEBIO (2017–2022).
Institutional Review Board Statement
This study was conducted in accordance with the guidelines set out in the Declaration of Helsinki and all procedures involving human subjects were approved by the Ethics Committee for Biomedical Research of Moulay Ismail University of Meknes (CERB-UMI protocol codes 201901 (January 2019). The written consent of all subjects has been obtained.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated and analyzed for the current study are available from Prof Filali-Zegzouti Younes, upon request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Holick, M.F. The Vitamin D Deficiency Pandemic: Approaches for Diagnosis, Treatment and Prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Schöttker, B.; Haug, U.; Schomburg, L.; Köhrle, J.; Perna, L.; Müller, H.; Holleczek, B.; Brenner, H. Strong Associations of 25-Hydroxyvitamin D Concentrations with All-Cause, Cardiovascular, Cancer, and Respiratory Disease Mortality in a Large Cohort Study. Am. J. Clin. Nutr. 2013, 97, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Pludowski, P.; Holick, M.F.; Pilz, S.; Wagner, C.L.; Hollis, B.W.; Grant, W.B.; Shoenfeld, Y.; Lerchbaum, E.; Llewellyn, D.J.; Kienreich, K.; et al. Vitamin D Effects on Musculoskeletal Health, Immunity, Autoimmunity, Cardiovascular Disease, Cancer, Fertility, Pregnancy, Dementia and Mortality-A Review of Recent Evidence. Autoimmun. Rev. 2013, 12, 976–989. [Google Scholar] [CrossRef] [PubMed]
- Silva, I.C.J.; Lazaretti-Castro, M. Vitamin D Metabolism and Extraskeletal Outcomes: An Update. Arch. Endocrinol. Metab. 2022, 66, 748–755. [Google Scholar] [CrossRef] [PubMed]
- Karonova, T.; Grineva, E.; Belyaeva, O.; Bystrova, A.; Jude, E.B.; Andreeva, A.; Kostareva, A.; Pludowski, P. Relationship between Vitamin D Status and Vitamin D Receptor Gene Polymorphisms with Markers of Metabolic Syndrome among Adults. Front. Endocrinol. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Chen, T.C. Vitamin D Deficiency: A Worldwide Problem with Health Consequences. Am. J. Clin. Nutr. 2008, 87, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- Hossein-Nezhad, A.; Holick, M.F. Vitamin D for Health: A Global Perspective. Mayo Clin. Proc. 2013, 88, 720–755. [Google Scholar] [CrossRef] [PubMed]
- Barbalho, S.M.; Tofano, R.J.; De Campos, A.L.; Rodrigues, A.S.; Quesada, K.; Bechara, M.D.; De Alvares Goulart, R.; Oshiiwa, M. Association between Vitamin D Status and Metabolic Syndrome Risk Factors. Diabetes Metab. Syndr. Clin. Res. Rev. 2018, 12, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Al-Said, N.H.; Mohamed, N.A.E.G.; Salam, R.F.; Fawzy, M.W. Vitamin D as a Risk Factor for Premature Atherosclerosis in Patients with Type 2 Diabetes. Ther. Adv. Endocrinol. Metab. 2015, 6, 249–257. [Google Scholar] [CrossRef]
- Ali Shah, S.I.; lqbal, S.; Sikandar, M.Z.; Yaqub Qazi, U.; Haq, I. Serum Vitamin D and Cardiometabolic Markers: A Comparative Study in Adult Men Based on Body Mass Index. IIUM Med. J. Malays. 2021, 20, 67–74. [Google Scholar] [CrossRef]
- Alquaiz, A.M.; Kazi, A.; Youssef, R.M.; Alshehri, N.; Alduraywish, S.A. Association between Standardized Vitamin 25(OH)D and Dyslipidemia: A Community-Based Study in Riyadh, Saudi Arabia. Environ. Health Prev. Med. 2020, 25. [Google Scholar] [CrossRef]
- Alyami, A.M.; Lam, V.; Soares, M.J.; Zhao, Y.; Sherriff, J.L.; Mamo, J.C.; James, A.P.; Coombes, F. The Association of Vitamin D Status with Dyslipidaemia and Biomarkers of Endothelial Cell Activation in Older Australians. Nutrients 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Amirkhizi, F.; Pishdadian, A.; Asghari, S.; Hamedi-Shahraki, S. Vitamin D Status Is Favorably Associated with the Cardiovascular Risk Factors in Adults with Obesity. Clin. Nutr. ESPEN 2021, 46, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Arif, M.A.; Niazi, R.; Arif, S.A. Association of Dyslipidaemia in Patients with Varying Degrees of Vitamin D Deficiency in the Asian Population. J. Pak. Med. Assoc. 2017, 67, 1843–1847. [Google Scholar]
- Baker, J.; Mehta, N.; Baker, D.; Toedter, G.; Shults, J.; Von Feldt, J.; Leonard, M. Vitamin D, Metabolic Dyslipidemia, and Metabolic Syndrome in Rheumatoid Arthritis. Am. J. Med. 2012, 125. [Google Scholar] [CrossRef]
- Cosentino, N.; Campodonico, J.; Milazzo, V.; De Metrio, M.; Brambilla, M.; Camera, M.; Marenzi, G. Vitamin D and Cardiovascular Disease: Current Evidence and Future Perspectives. Nutrients 2021, 13, 3603. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.C. Vitamin D and the Renin-Angiotensin System; Fourth Edition.; Elsevier Inc., 2018; Vol. 1; ISBN 978-0-12-809966-7. [CrossRef]
- Han, L.; Xu, X.-J.; Zhang, J.-S.; Liu, H.-M. Association between Vitamin D Deficiency and Levels of Renin and Angiotensin in Essential Hypertension. Int. J. Clin. Pract. 2022, 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-H.; Meza, C.A.; Clarke, H.; Kim, J.-S.; Hickner, R.C. Vitamin D and Endothelial Function. Nutrients 2020, 12, 575. [Google Scholar] [CrossRef] [PubMed]
- Polly, P.; Tan, T.C. The Role of Vitamin D in Skeletal and Cardiac Muscle Function. Front. Physiol. 2014, 5. [Google Scholar] [CrossRef]
- Mellenthin, L.; Wallaschofski, H.; Grotevendt, A.; Völzke, H.; Nauck, M.; Hannemann, A. Association between Serum Vitamin D Concentrations and Inflammatory Markers in the General Adult Population. Metabolism. 2014, 63, 1056–1062. [Google Scholar] [CrossRef]
- Karkeni, E.; Bonnet, L.; Marcotorchino, J.; Tourniaire, F.; Astier, J.; Ye, J.; Landrier, J.-F. Vitamin D Limits Inflammation-Linked microRNA Expression in Adipocytes in Vitro and in Vivo : A New Mechanism for the Regulation of Inflammation by Vitamin D. Epigenetics 2018, 13, 156–162. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO) WHO List of Priority Medical Devices for Management of Cardiovascular Diseases and Diabetes; 2021; ISBN 9789240027978. https://www.who.int/publications-detail-redirect/9789240027978%0Afiles/1046/9789240027978.html. (Accessed on 15 Septembre 2022).
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Morocco GUIDE D’EVALUATION ET DE PRISE EN CHARGE DU RISQUE CARDIOVASCULAIRE; AZ Edition.; Direction de l’Epidémiologie et de Lutte contre les Maladies, 2019. (Accessed on 15 April 2022). Available online: https://www.sante.gov.ma/Documents/2023/03/Guide risque cardiovasculaire VF AZ 08 juillet 2019.pdf.
- Vogel, B.; Acevedo, M.; Appelman, Y.; Bairey Merz, C.N.; Chieffo, A.; Figtree, G.A.; Guerrero, M.; Kunadian, V.; Lam, C.S.P.; Maas, A.H.E.M.; et al. The Lancet Women and Cardiovascular Disease Commission: Reducing the Global Burden by 2030. The Lancet 2021, 397, 2385–2438. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Stouffer, G.A.; Kucharska-Newton, A.M.; Qamar, A.; Vaduganathan, M.; Pandey, A.; Porterfield, D.; Blankstein, R.; Rosamond, W.D.; Bhatt, D.L.; et al. Twenty Year Trends and Sex Differences in Young Adults Hospitalized With Acute Myocardial Infarction: The ARIC Community Surveillance Study. Circulation 2019, 139, 1047–1056. [Google Scholar] [CrossRef] [PubMed]
- Gabet, A.; Danchin, N.; Juillière, Y.; Olié, V. Acute Coronary Syndrome in Women: Rising Hospitalizations in Middle-Aged French Women, 2004–14. Eur. Heart J. 2017, 38, 1060–1065. [Google Scholar] [CrossRef] [PubMed]
- Wilmot, K.A.; O’Flaherty, M.; Capewell, S.; Ford, E.S.; Vaccarino, V. Coronary Heart Disease Mortality Declines in the United States From 1979 Through 2011: Evidence for Stagnation in Young Adults, Especially Women. Circulation 2015, 132, 997–1002. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Morocco Enquette Nationale Sur Les Facteurs de Risques Communs Des Maladies Non Transmissibles 2017 - 2018.; 2019; pp. 1–120;. Available online https://www.sante.gov.ma/Documents/2019/05/Rapport%20de%20l%20enqu%C3%AAte%20Stepwise.pdf. (Accessed on ). 15 April; 2022.
- Hedayatnia, M.; Asadi, Z.; Zare-Feyzabadi, R.; Yaghooti-Khorasani, M.; Ghazizadeh, H.; Ghaffarian-Zirak, R.; Nosrati-Tirkani, A.; Mohammadi-Bajgiran, M.; Rohban, M.; Sadabadi, F.; et al. Dyslipidemia and Cardiovascular Disease Risk among the MASHAD Study Population. Lipids Health Dis. 2020, 19, 42. [Google Scholar] [CrossRef]
- Du, Z.; Qin, Y. Dyslipidemia and Cardiovascular Disease: Current Knowledge, Existing Challenges, and New Opportunities for Management Strategies. J. Clin. Med. 2023, 12, 363. [Google Scholar] [CrossRef]
- Wang, Y.; Si, S.; Liu, J.; Wang, Z.; Jia, H.; Feng, K.; Sun, L.; Song, S.J. The Associations of Serum Lipids with Vitamin D Status. PLOS ONE 2016, 11, e0165157. [Google Scholar] [CrossRef]
- Rashidbeygi, E.; Rahimi, M.H.; Mollahosseini, M.; Yekaninejad, M.S.; Imani, H.; Maghbooli, Z.; Mirzaei, K. Associations of Vitamin D Status and Metabolic Dyslipidemia and Hypertriglyceridemic Waist Phenotype in Apparently Healthy Adults. Diabetes Metab. Syndr. Clin. Res. Rev. 2018, 12, 985–990. [Google Scholar] [CrossRef]
- Jeenduang, N.; Sangkaew, B. The Association between Serum 25-Hydroxyvitamin D Concentrations and Serum Lipids in the Southern Thai Population. Arch. Med. Sci. 2020. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Liu, Q.; Zhang, Q.; Wan, Z.; Hu, L.; Xu, R.; Cheng, A.; Lv, Y.; Wang, L. Sex-Specific Association between Serum Vitamin D Status and Lipid Profiles: A Cross-Sectional Study of a Middle-Aged and Elderly Chinese Population. J. Nutr. Sci. Vitaminol. (Tokyo) 2020, 66, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Dziedzic, E.A.; Przychodzeń, S.; Dąbrowski, M. The Effects of Vitamin D on Severity of Coronary Artery Atherosclerosis and Lipid Profile of Cardiac Patients. Arch. Med. Sci. 2016, 6, 1199–1206. [Google Scholar] [CrossRef] [PubMed]
- Hafez, M.; Musa, N.; Atty, S.; Ibrahem, M.; Wahab, N. Effect of Vitamin D Supplementation on Lipid Profile in Vitamin D-Deficient Children with Type 1 Diabetes and Dyslipidemia. Horm. Res. Paediatr. 2019, 91, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Abid, H.; Abid, Z.; Abid, S. Atherogenic Indices in Clinical Practice and Biomedical Research: A Short Review. Baghdad J. Biochem. Appl. Biol. Sci. 2021, 2, 60–70. [Google Scholar] [CrossRef]
- Afsin, A.; Kaya, H.; Suner, A.; Uzel, K.E.; Bursa, N.; Hosoglu, Y.; Yavuz, F.; Asoglu, R. Plasma Atherogenic Indices Are Independent Predictors of Slow Coronary Flow. BMC Cardiovasc. Disord. 2021, 21, 608. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, S.; Bhattacharjee, J.; Bhatnagar, M.K.; Tyagi, S. Atherogenic Index of Plasma, Castelli Risk Index And Atherogenic Coefficient- New Parameters In Assessing Cardiovascular Risk. Int. J. Pharm. Biol. Sci. 2013, 3, 359–364, https://api.semanticscholar.org/CorpusID:2598875. [Google Scholar]
- Olamoyegun, M.; Oluyombo, R.; Asaolu, S. Evaluation of Dyslipidemia, Lipid Ratios, and Atherogenic Index as Cardiovascular Risk Factors among Semi-Urban Dwellers in Nigeria. Ann. Afr. Med. 2016, 15, 194. [Google Scholar] [CrossRef] [PubMed]
- Sujatha, R.; Kavitha, S. Atherogenic Indices in Stroke Patients: A Retrospective Study. Iran J Neurol. 2017 Apr 4;16(2):78-82. PMCID: PMC5526781. [PubMed]
- Ulloque-Badaracco, J.R.; Hernandez-Bustamante, E.A.; Alarcon-Braga, E.A.; Mosquera-Rojas, M.D.; Campos-Aspajo, A.; Salazar-Valdivia, F.E.; Valdez-Cornejo, V.A.; Benites-Zapata, V.A.; Herrera-Añazco, P.; Valenzuela-Rodríguez, G.; et al. Atherogenic Index of Plasma and Coronary Artery Disease: A Systematic Review. Open Med. 2022, 17, 1915–1926. [Google Scholar] [CrossRef]
- Cai, G.; Liu, W.; Lv, S.; Wang, X.; Guo, Y.; Yan, Z.; Du, Y.; Zhou, Y. Gender-Specific Associations between Atherogenic Index of Plasma and the Presence and Severity of Acute Coronary Syndrome in Very Young Adults: A Hospital-Based Observational Study. Lipids Health Dis. 2019, 18, 99. [Google Scholar] [CrossRef]
- Fernández-Macías, J.C.; Ochoa-Martínez, A.C.; Varela-Silva, J.A.; Pérez-Maldonado, I.N. Atherogenic Index of Plasma: Novel Predictive Biomarker for Cardiovascular Illnesses. Arch. Med. Res. 2019, 50, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Guo, Q.; Zhou, S.; Feng, X.; Yang, J.; Qiao, J.; Zhao, Y.; Shi, D.; Zhou, Y. The Sensibility of the New Blood Lipid Indicator——Atherogenic Index of Plasma (AIP) in Menopausal Women with Coronary Artery Disease. Lipids Health Dis. 2020, 19, 27. [Google Scholar] [CrossRef] [PubMed]
- Ban, J.; Zhao, X.; Jia, Z.; Li, Z.; Chen, S. Association Between Vitamin D Levels and the Atherogenic Index of Plasma Among Chinese with Type 2 Diabetes Mellitus. Diabetes Metab. Syndr. Obes. 2023, Volume 16, 523–531. [Google Scholar] [CrossRef]
- Mahmoodi, M.R.; Najafipour, H. Associations between Serum Vitamin D3, Atherogenic Indices of Plasma and Cardiometabolic Biomarkers among Patients with Diabetes in the KERCADR Study. BMC Endocr. Disord. 2022, 22, 126. [Google Scholar] [CrossRef] [PubMed]
- Ministère de la Santé. ENQUETE NATIONALE SUR LA NUTRITION (ENN 2019-2020). 2022, 1–144, https://www.sante.gov.ma/Documents/2022/07/rapport%20ENN%202019-2020%20ajout%20preface%20.pdf. ( Accessed on ). 15 September; 2022.
- Glenn, D. Israel. Determining Sample Size 1.University of Florida IFAS Extension. Available At. Http://Edis.Ifas.Ufl.Edu. 2022, 1-5.
- Papathanasiou, G.; Georgoudis, G.; Papandreou, M.; Spyropoulos, P.; Georgakopoulos, D.; Kalfakakou, V.; Evangelou, A. Reliability Measures of the Short International Physical Activity Questionnaire (IPAQ) in Greek Young Adults. Hell. J. Cardiol. HJC Hellēnikē Kardiologikē Epitheōrēsē 2009, 50, 283–294. [Google Scholar]
- Pas-a-Pas research group; Arija, V. ; Villalobos, F.; Pedret, R.; Vinuesa, A.; Timón, M.; Basora, T.; Aguas, D.; Basora, J. Effectiveness of a Physical Activity Program on Cardiovascular Disease Risk in Adult Primary Health-Care Users: The “Pas-a-Pas” Community Intervention Trial. BMC Public Health 2017, 17, 576. [Google Scholar] [CrossRef]
- Lhilali, I.; Zouine, N.; Menouni, A.; Godderis, L.; Kestemont, M.-P.; El Midaoui, A.; El Jaafari, S.; Filali-Zegzouti, Y. Sun Exposure Score and Vitamin D Levels in Moroccan Women of Childbearing Age. Nutrients 2023, 15, 688. [Google Scholar] [CrossRef]
- Fitzpatrick, T.B. The Validity and Practicality of Sun-Reactive Skin Types I Through VI. Arch. Dermatol. 1988, 124, 869–871. [Google Scholar] [CrossRef]
- Lin, X.; Li, H. Obesity: Epidemiology, Pathophysiology, and Therapeutics. Front. Endocrinol. 2021, 12, 706978. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimationof the Concentrationof Low-Density LipoproteinCholesteroiln Plasma,Without Useof the PreparativeUltracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- IOM (Institute of Medicine) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium; A. Catharine Ross, Christine L. Taylor, Ann L. Yaktine, Valle, H.B.D., Eds.; Washington (DC): National Academies Press (US), 2011; ISBN 978-0-309-16394-1. [Google Scholar]
- Munns, C.F.; Shaw, N.; Kiely, M.; Specker, B.L.; Thacher, T.D.; Ozono, K.; Michigami, T.; Tiosano, D.; Mughal, M.Z.; Mäkitie, O.; et al. Global Consensus Recommendations on Prevention and Management of Nutritional Rickets. J. Clin. Endocrinol. Metab. 2016, 101, 394–415. [Google Scholar] [CrossRef] [PubMed]
- Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Final Report. Circulation 2002, 106, 3143–3421. [CrossRef]
- Xavier, H.T.; Izar, M.C.; Faria Neto, J.R.; Assad, M.H.; Rocha, V.Z.; Sposito, A.C.; Fonseca, F.A.; Santos, J.E.D.; Santos, R.D.; Bertolami, M.C.; et al. V Diretriz Brasileira de Dislipidemias e Prevenção da Aterosclerose. Arq. Bras. Cardiol. 2013, 101, 01–22. [Google Scholar] [CrossRef]
- Molani Gol, R.; Rafraf, M.; Asghari Jafarabadi, M. Assessment of Atherogenic Indices and Lipid Ratios in the Apparently Healthy Women Aged 30–55 Years. Arter. Hypertens. 2022, 25, 172–177. [Google Scholar] [CrossRef]
- Hajian-Tilaki, K. Receiver Operating Characteristic (ROC) Curve Analysis for Medical Diagnostic Test Evaluation. Casp. J. Intern. Med. 2013, 4, 627–635. [Google Scholar] [PubMed] [PubMed Central]
- Anouti, F.A.; Ahmed, L.A.; Riaz, A.; Grant, W.B.; Shah, N.; Ali, R.; Alkaabi, J.; Shah, S.M. Vitamin D Deficiency and Its Associated Factors among Female Migrants in the United Arab Emirates. Nutrients 2022, 14, 1074. [Google Scholar] [CrossRef] [PubMed]
- Dadda, S.; Azekour, K.; Sebbari, F.; El Houate, B.; El Bouhali, B. Sun Exposure, Dressing Habits, and Vitamin D Status in Morocco. E3S Web Conf. 2021, 319, 01097. [Google Scholar] [CrossRef]
- Dimakopoulos, I.; Magriplis, E.; Mitsopoulou, A.V.; Karageorgou, D.; Bakogianni, I.; Micha, R.; Michas, G.; Chourdakis, M.; Ntouroupi, T.; Tsaniklidou, S.M.; et al. Association of Serum Vitamin D Status with Dietary Intake and Sun Exposure in Adults. Clin. Nutr. ESPEN 2019, 34, 23–31. [Google Scholar] [CrossRef]
- Santana, K.V. de S. de; Oliver, S.L.; Mendes, M.M.; Lanham-New, S.; Charlton, K.E.; Ribeiro, H. Association between Vitamin D Status and Lifestyle Factors in Brazilian Women: Implications of Sun Exposure Levels, Diet, and Health. eClinicalMedicine 2022, 47, 101400. [Google Scholar] [CrossRef]
- Mehdad, S.; Belghiti, H.; Zahrou, F.E.; Guerinech, H.; Mouzouni, F.Z.; El hajjab, A.; El Berri, H.; El Ammari, L.; Benaich, S.; Benkirane, H.; et al. Vitamin D Status and Its Relationship with Obesity Indicators in Moroccan Adult Women. Nutr. Health 2022, 1–9. [Google Scholar] [CrossRef]
- Zouine, N.; Lhilali, I.; Menouni, A.; Godderis, L.; El Midaoui, A.; El Jaafari, S.; Zegzouti Filali, Y. Development and Validation of Vitamin D- Food Frequency Questionnaire for Moroccan Women of Reproductive Age: Use of the Sun Exposure Score and the Method of Triad’s Model. Nutrients 2023, 15, 796. [Google Scholar] [CrossRef] [PubMed]
- Crowe, F.L.; Thayakaran, R.; Gittoes, N.; Hewison, M.; Thomas, G.N.; Scragg, R.; Nirantharakumar, K. Non-Linear Associations of 25-Hydroxyvitamin D Concentrations with Risk of Cardiovascular Disease and All-Cause Mortality: Results from The Health Improvement Network (THIN) Database. J. Steroid Biochem. Mol. Biol. 2019, 195, 105480. [Google Scholar] [CrossRef]
- Zhang, R.; Li, B.; Gao, X.; Tian, R.; Pan, Y.; Jiang, Y.; Gu, H.; Wang, Y.; Wang, Y.; Liu, G. Serum 25-Hydroxyvitamin D and the Risk of Cardiovascular Disease: Dose-Response Meta-Analysis of Prospective Studies. Am. J. Clin. Nutr. 2017, 105, 810–819. [Google Scholar] [CrossRef] [PubMed]
- Umar, M.; Sastry, K.; Chouchane, A. Role of Vitamin D Beyond the Skeletal Function: A Review of the Molecular and Clinical Studies. Int. J. Mol. Sci. 2018, 19, 1618. [Google Scholar] [CrossRef] [PubMed]
- Biswas, M.; Allabhakshu, S.; Prabhu, K. Does Serum Vitamin D Affect Lipid Profile? Biomed. India 2021, 41, 787–792. [Google Scholar] [CrossRef]
- Yassir, S.; Ramarajan, M.G.; Patil, S.; Shaikh, S.B.; Abdulla, Y.M.; Manjrekar, P.A. Impact of Serum 25 Hydroxyvitamin D Deficiency on Lipid Biomarkers in Established Coronary Artery Disease. Turk. J. Biochem. 2022, 47, 79–84. [Google Scholar] [CrossRef]
- Zittermann, A.; Gummert, J.; Borgermann, J. The Role of Vitamin D in Dyslipidemia and Cardiovascular Disease. Curr. Pharm. Des. 2011, 17, 933–942. [Google Scholar] [CrossRef] [PubMed]
- Conghui Guan; Songbo Fu; Donghu Zhen; Xuehong Li; Jinglei Niu; Jianguo Cheng; Nan Zhao; Jinjin Liu; Hongtao Yin; Xulei Tang Correlation of Serum Vitamin D with Lipid Profiles in Middle-Aged and Elderly Chinese Individuals. Asia Pac. J. Clin. Nutr. 2020, 29. [CrossRef] [PubMed]
- Lupton, J.R.; Faridi, K.F.; Martin, S.S.; Sharma, S.; Kulkarni, K.; Jones, S.R.; Michos, E.D. Deficient Serum 25-Hydroxyvitamin D Is Associated with an Atherogenic Lipid Profile: The Very Large Database of Lipids (VLDL-3) Study. J. Clin. Lipidol. 2016, 10, 72–81.e1. [Google Scholar] [CrossRef]
- Muñoz-Aguirre, P.; Flores, M.; Macias, N.; Quezada, A.D.; Denova-Gutiérrez, E.; Salmerón, J. The Effect of Vitamin D Supplementation on Serum Lipids in Postmenopausal Women with Diabetes: A Randomized Controlled Trial. Clin. Nutr. 2015, 34, 799–804. [Google Scholar] [CrossRef]
- Stellaard, F. From Dietary Cholesterol to Blood Cholesterol, Physiological Lipid Fluxes, and Cholesterol Homeostasis. Nutrients 2022, 14, 1643. [Google Scholar] [CrossRef]
- Han, Y.-Y.; Hsu, S.H.-J.; Su, T.-C. Association between Vitamin D Deficiency and High Serum Levels of Small Dense LDL in Middle-Aged Adults. Biomedicines 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Vaskonen, T. Dietary Minerals and Modification of Cardiovascular Risk Factors. J. Nutr. Biochem. 2003, 14, 492–506. [Google Scholar] [CrossRef]
- Mousa, A.; Naderpoor, N.; De Courten, M.P.J.; Scragg, R.; De Courten, B. 25-Hydroxyvitamin D Is Associated with Adiposity and Cardiometabolic Risk Factors in a Predominantly Vitamin D-Deficient and Overweight/Obese but Otherwise Healthy Cohort. J. Steroid Biochem. Mol. Biol. 2017, 173, 258–264. [Google Scholar] [CrossRef]
- Öztürk Özkan, G. Does Vitamin D Level Affect Beta Cell Activity? Bagcilar Med. Bull. 2021, 6, 397–406. [Google Scholar] [CrossRef]
- Szymczak-Pajor, I.; Śliwińska, A. Analysis of Association between Vitamin D Deficiency and Insulin Resistance. Nutrients 2019, 11, 794. [Google Scholar] [CrossRef] [PubMed]
- Larrick, B.M.; Kim, K.-H.; Donkin, S.S.; Teegarden, D. 1,25-Dihydroxyvitamin D Regulates Lipid Metabolism and Glucose Utilization in Differentiated 3T3-L1 Adipocytes. Nutr. Res. 2018, 58, 72–83. [Google Scholar] [CrossRef]
- Farrar, M.D.; Webb, A.R.; Kift, R.; Durkin, M.T.; Allan, D.; Herbert, A.; Berry, J.L.; Rhodes, L.E. Efficacy of a Dose Range of Simulated Sunlight Exposures in Raising Vitamin D Status in South Asian Adults : Implications for Targeted Guidance on Sun Exposure 1 – 3. 2013; 25, 1216. [Google Scholar] [CrossRef]
- Vimaleswaran, K.S.; Berry, D.J.; Lu, C.; Tikkanen, E.; Pilz, S.; Hiraki, L.T.; Cooper, J.D.; Dastani, Z.; Li, R.; Houston, D.K.; et al. Causal Relationship between Obesity and Vitamin D Status: Bi-Directional Mendelian Randomization Analysis of Multiple Cohorts. PLoS Med. 2013, 10, e1001383. [Google Scholar] [CrossRef] [PubMed]
- Savastano, S.; Barrea, L.; Savanelli, M.C.; Nappi, F.; Di Somma, C.; Orio, F.; Colao, A. Low Vitamin D Status and Obesity: Role of Nutritionist. Rev. Endocr. Metab. Disord. 2017, 18, 215–225. [Google Scholar] [CrossRef]
- Song, K.; Park, G.; Choi, Y.; Oh, J.; Choi, H.; Suh, J.; Kwon, A.; Kim, H.; Chae, H. Association of Vitamin D Status and Physical Activity with Lipid Profile in Korean Children and Adolescents: A Population-Based Study. Child.-BASEL 2020, 7. [Google Scholar] [CrossRef]
- Fernandes, M.R.; Barreto Junior, W. dos R. Association between Physical Activity and Vitamin D: A Narrative Literature Review. Rev. Assoc. Médica Bras. 2017, 63, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.-P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2021, 143. [Google Scholar] [CrossRef] [PubMed]
- Ugwuja, E.; Ogbonna, N.; Nwibo, A.; Onimawo, I. Overweight and Obesity, Lipid Profile and Atherogenic Indices among Civil Servants in Abakaliki, South Eastern Nigeria. Ann. Med. Health Sci. Res. 2013, 3, 13. [Google Scholar] [CrossRef] [PubMed]
- Vekic, J.; Zeljkovic, A.; Stefanovic, A.; Jelic-Ivanovic, Z.; Spasojevic-Kalimanovska, V. Obesity and Dyslipidemia. Metabolism 2019, 92, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Klop, B.; Elte, J.; Cabezas, M. Dyslipidemia in Obesity: Mechanisms and Potential Targets. Nutrients 2013, 5, 1218–1240. [Google Scholar] [CrossRef] [PubMed]
- Weller, R.B. Sunlight Has Cardiovascular Benefits Independently of Vitamin D. Blood Purif. 2016, 41, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Fleury, N.; Geldenhuys, S.; Gorman, S. Sun Exposure and Its Effects on Human Health: Mechanisms through Which Sun Exposure Could Reduce the Risk of Developing Obesity and Cardiometabolic Dysfunction. Int. J. Environ. Res. Public. Health 2016, 13, 999. [Google Scholar] [CrossRef] [PubMed]
- Zand, J.; Lanza, F.; Garg, H.K.; Bryan, N.S. All-Natural Nitrite and Nitrate Containing Dietary Supplement Promotes Nitric Oxide Production and Reduces Triglycerides in Humans. Nutr. Res. 2011, 31, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Tikkanen, E.; Gustafsson, S.; Ingelsson, E. Associations of Fitness, Physical Activity, Strength, and Genetic Risk With Cardiovascular Disease: Longitudinal Analyses in the UK Biobank Study. Circulation 2018, 137, 2583–2591. [Google Scholar] [CrossRef]
- Chomistek, A.K.; Henschel, B.; Eliassen, A.H.; Mukamal, K.J.; Rimm, E.B. Frequency, Type, and Volume of Leisure-Time Physical Activity and Risk of Coronary Heart Disease in Young Women. Circulation 2016, 134, 290–299. [Google Scholar] [CrossRef]
- Gersh, B.J. Dose Response Between Physical Activity and Risk of Coronary Heart Disease: A Meta-Analysis. Yearb. Cardiol. 2012, 2012, 271–273. [Google Scholar] [CrossRef]
- Silva, R.C.D.; Diniz, M.D.F.H.S.; Alvim, S.; Vidigal, P.G.; Fedeli, L.M.G.; Barreto, S.M. Physical Activity and Lipid Profile in the ELSA-Brasil Study. Arq. Bras. Cardiol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Maciel, E.D.S.; Silva, B.K.R.; Figueiredo, F.W.D.S.; Pontes-Silva, A.; Quaresma, F.R.P.; Adami, F.; Fonseca, F.L.A. Physical Inactivity Level and Lipid Profile in Traditional Communities in the Legal Amazon: A Cross-Sectional Study: Physical Inactivity Level in the Legal Amazon. BMC Public Health 2022, 22, 542. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Cho, Y.K.; Kim, Y.-J.; Jung, C.H.; Lee, W.J.; Park, J.-Y.; Huh, J.H.; Kang, J.G.; Lee, S.J.; Ihm, S.-H. Association of the Atherogenic Index of Plasma with Cardiovascular Risk beyond the Traditional Risk Factors: A Nationwide Population-Based Cohort Study. Cardiovasc. Diabetol. 2022, 21, 81. [Google Scholar] [CrossRef] [PubMed]
- Fu, L.; Zhou, Y.; Sun, J.; Zhu, Z.; Xing, Z.; Zhou, S.; Wang, Y.; Tai, S. Atherogenic Index of Plasma Is Associated with Major Adverse Cardiovascular Events in Patients with Type 2 Diabetes Mellitus. Cardiovasc. Diabetol. 2021, 20, 201. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; Backer, G.G.D.; Delgado, V.; Ference, B.A.; Graham, I.M.; et al. 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias: Lipid Modification to Reduce Cardiovascular Risk. European Heart Journal 2019, 1–78. [Google Scholar] [CrossRef] [PubMed]
- Izadi, A.; Aliasghari, F.; Gargari, B.P.; Ebrahimi, S. Strong Association between Serum Vitamin D and Vaspin Levels, AIP, VAI and Liver Enzymes in NAFLD Patients. Int. J. Vitam. Nutr. Res. 2020, 90, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Pokhrel, S.; Giri, N.; Pokhrel, R.; Pardhe, B.; Lamichhane, A.; Chaudhary, A.; Bhatt, M. Vitamin D Deficiency and Cardiovascular Risk in Type 2 Diabetes Population. OPEN LIFE Sci. 2021, 16, 464–474. [Google Scholar] [CrossRef]
- Faridi, K.F.; Zhao, D.; Martin, S.S.; Lupton, J.R.; Jones, S.R.; Guallar, E.; Ballantyne, C.M.; Lutsey, P.L.; Michos, E.D. Serum Vitamin D and Change in Lipid Levels over 5 y: The Atherosclerosis Risk in Communities Study. Nutrition 2017, 38, 85–93. [Google Scholar] [CrossRef]
- Lee, M.; Ebert, J.R.; Kadakia, M.P.; Zhang, J.; Czerwinski, S.A. Inverse Associations between Cardiometabolic Risk Factors and 25-Hydroxyvitamin D in Obese American Children and Adolescents. Am. J. Hum. Biol. 2016, 28, 736–742. [Google Scholar] [CrossRef]
- Censani, M.; Hammad, H.T.; Christos, P.J.; Schumaker, T. Vitamin D Deficiency Associated With Markers of Cardiovascular Disease in Children With Obesity. Glob. Pediatr. Health 2018, 5. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.R.; Jeong, S.J. Relationship between Vitamin D Level and Lipid Profile in Non-Obese Children. Metabolites 2019, 9. [Google Scholar] [CrossRef] [PubMed]
- Xiao, P.; Zhao, X.Y.; Hong, W.; Hou, D.Q.; Yu, Z.C.; Wang, L.G.; Wang, H.J.; Gao, A.Y.; Cheng, H.; Mi, J. A prospective cohort study on the associations between vitamin D nutritional status and cardiometabolic abnormities in children. Zhonghua Liu Xing Bing Xue Za Zhi Zhonghua Liuxingbingxue Zazhi 2020, 41, 2059–2065. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The flow chart of study subjects.
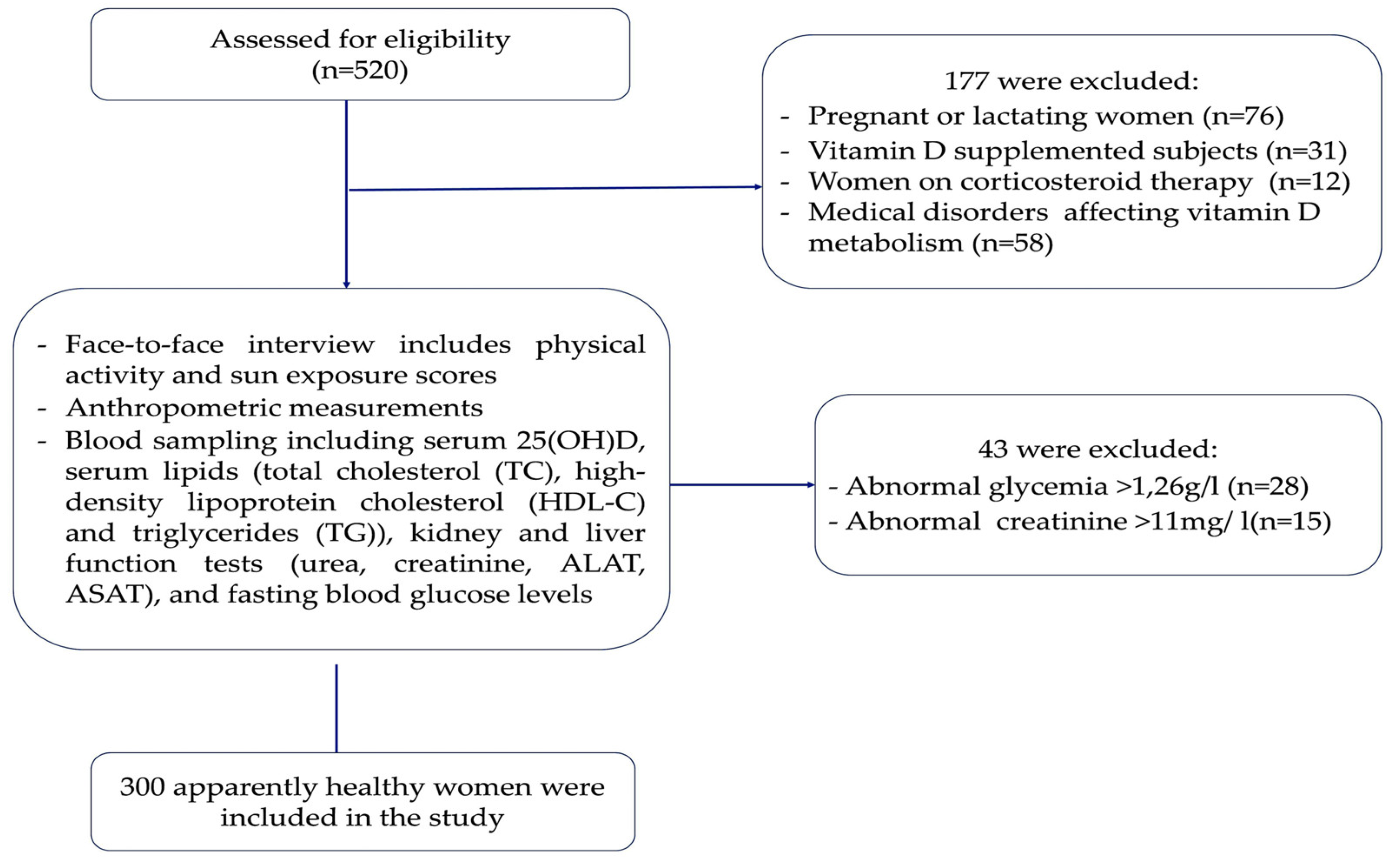
Figure 2.
Scatter plot showing the relations of serum 25(OH) D concentrations with lipid profile and atherogenic indices.
Figure 2.
Scatter plot showing the relations of serum 25(OH) D concentrations with lipid profile and atherogenic indices.
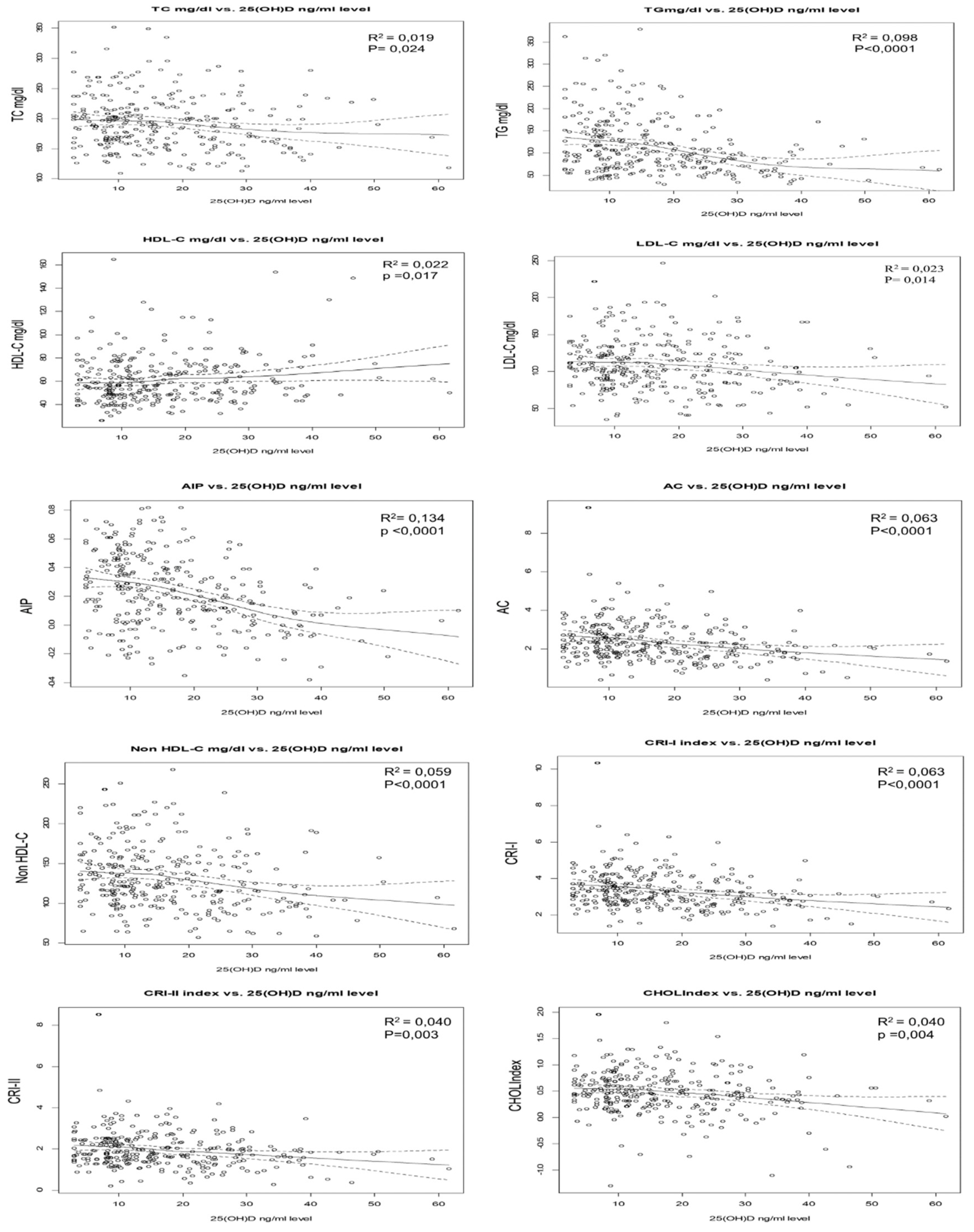
Figure 3.
Box-plot representing the 25(OH) D concentration according to lipid profile and atherogenic indices levels. Cutoff values to define dyslipidemias were as follows: TC ≥ 200 mg/dL, TG > 150 mg/dL, LDL-C ≥ 130 mg/dL, and HDL-C <50 mg/dL. Elevated atherogenic indices were defined as: AIP > 0.15; Non-HDL-C > 130 mg/dL, AC > 3.0, CRI-I >3.0, and CRI-II > 3.3. Data are shown as the median. P-values obtained from Mann– Whitney U test. P-values < 0.05 were considered significant.
Figure 3.
Box-plot representing the 25(OH) D concentration according to lipid profile and atherogenic indices levels. Cutoff values to define dyslipidemias were as follows: TC ≥ 200 mg/dL, TG > 150 mg/dL, LDL-C ≥ 130 mg/dL, and HDL-C <50 mg/dL. Elevated atherogenic indices were defined as: AIP > 0.15; Non-HDL-C > 130 mg/dL, AC > 3.0, CRI-I >3.0, and CRI-II > 3.3. Data are shown as the median. P-values obtained from Mann– Whitney U test. P-values < 0.05 were considered significant.
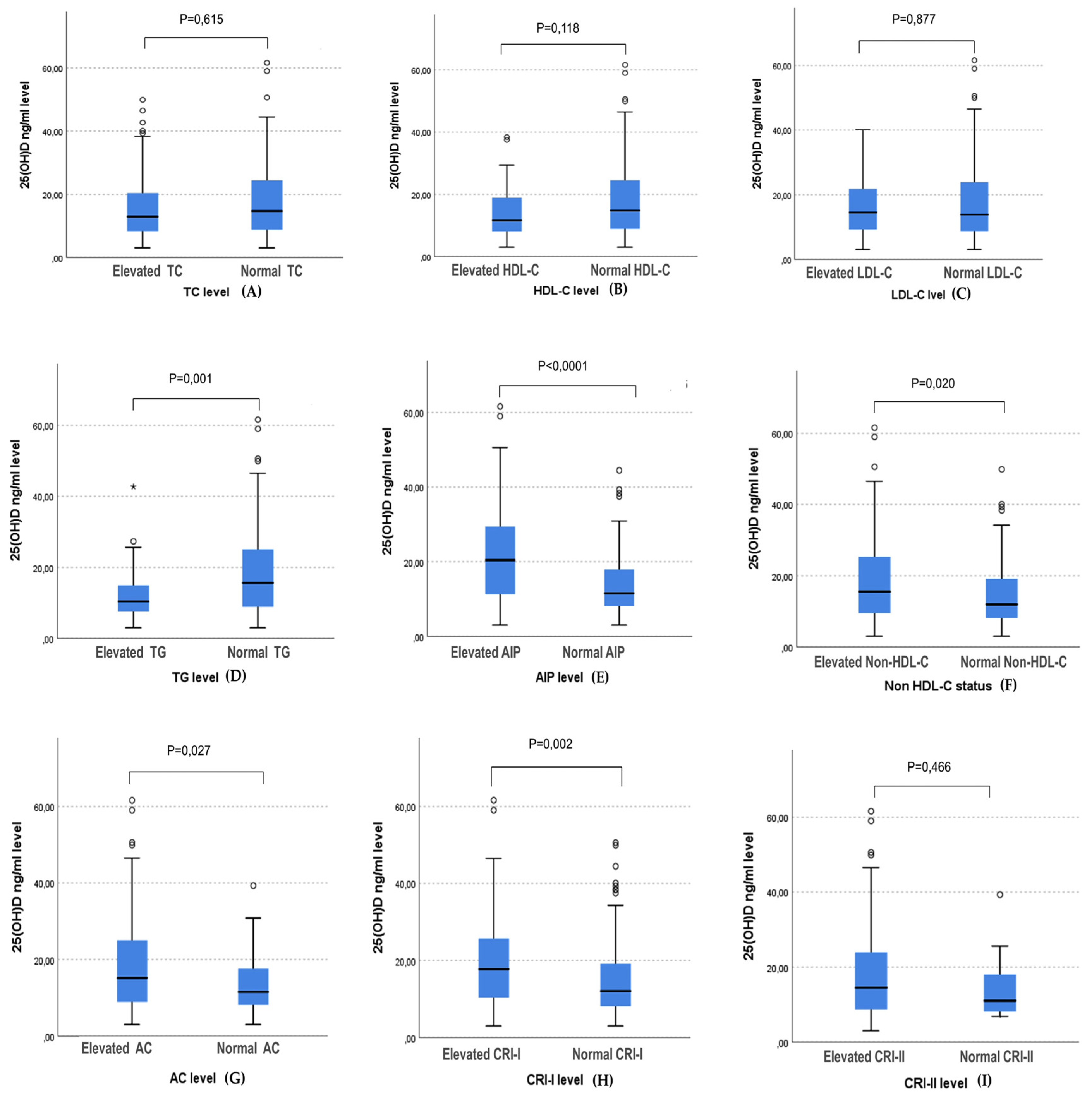
Figure 4.
ROC curve to identify the optimal vitamin D levels threshold to predict hypertriglyceridemia and high atherogenic indices. The value of p was derived from ROC analysis. Statistical significance p < 0.05. Abbreviations: AUC, Area under the curve. A, ROC curve analysis of 25(OH)D and hypertriglyceridemia. B, ROC curve analysis of 25(OH)D and elevated AIP levels. C, ROC curve analysis of 25(OH)D and elevated Non-HDL-C levels; D, ROC curve analysis of 25(OH)D and elevated AC levels. E, ROC curve analysis of 25(OH)D and elevated CRI-I levels.
Figure 4.
ROC curve to identify the optimal vitamin D levels threshold to predict hypertriglyceridemia and high atherogenic indices. The value of p was derived from ROC analysis. Statistical significance p < 0.05. Abbreviations: AUC, Area under the curve. A, ROC curve analysis of 25(OH)D and hypertriglyceridemia. B, ROC curve analysis of 25(OH)D and elevated AIP levels. C, ROC curve analysis of 25(OH)D and elevated Non-HDL-C levels; D, ROC curve analysis of 25(OH)D and elevated AC levels. E, ROC curve analysis of 25(OH)D and elevated CRI-I levels.


Table 1.
Clinical and biological characteristics of participants stratified by 25(OH) D status.
| Participants characteristics | Total = 300 |
25(OH)D <12 ng/ml N= 129 |
25(OH)D (12-20ng/ml) N= 73 |
25(OH)D > 20ng/ml N= 97 |
P-value |
|---|---|---|---|---|---|
| Clinical characteristics N (%) | |||||
|
Age (yrs) * |
38 ± 18 (18 – 50) |
33 ± 20 (20 – 50) |
38 ± 18 (18 – 50) |
41 ± 14 (19 – 50) |
0.006b |
| 18-28 | 96 (32) | 53 (40.8) | 23 (31.5) | 20 (20.6) | 0.020c |
| 29-39 | 89 (29.7) | 37 (28.5) | 22 (30.1) | 30 (30.9) | |
| 40-50 | 115 (38.3) | 40 (30.8) | 28 (38.4) | 47 (48.5) | |
| BMI ( (kg/m2) * | 25.74 ± 4.81 (14.53 – 38.10) |
26.45 ± 5.92 (17.47 – 38.10) |
26.35 ± 4.60 (14.53 – 36.65) |
24.84 ± 4.08 (14.53 – 32.39) |
0.008b |
| Normal weight | 122 (40.7) | 45 (34.6) | 25 (34.2) | 52 (53.6) | 0.001c |
| Overweight | 124 (14.3) | 51 (39.2) | 34 (46.6) | 39 (40.2) | |
| Obese | 54 (18) | 34 (26.2) | 14 (19.2) | 6 (6.2) | |
| Sun exposure score * | 15.25 ± 6.86 |
13.21 ± 5.75 (5.06 -23.06) |
14.75 ± 8.09 (7.5 – 31) |
18.35 ± 8.99 (8.5 – 34.50) |
<0.0001b |
| Physical activity score (MET-min/week)* | 2038.8 ± 1838.7 (519 – 4458) |
1778.4 ± 1721.1 (519.6 – 4458) |
1597.6 ± 1318.8 (519 – 4197.8) |
2896.6 ±1300.3 (799 – 4197) |
<0.0001b |
|
low physical activity score < 600MET-min/week |
19 (6.3) | 9 (6.9) | 10 (13.7) | 0 (0) | <0.0001c |
| Moderate physical activity score ≥600–2999 METs/min/week | 213 (71) | 97 (74.6) | 54 (74) | 62 (63.9) | |
|
High physical activity score ≥ 3000 MET-min/week |
68 (22.7) | 24 (18.5) | 09 (12.3) | 35 (36.1) | |
| Biochemical Characteristics N (%) | |||||
| 25(OH) D (ng/ml) * | 13.97 ± 15.17 (3 – 61.60) |
8.30 ± 3.43 (3 – 11.89) |
15.70 ± 4.04 (1.02 – 19.80) |
27.84 ± 10.52 (20.10 – 61.60) |
<0.0001b |
| TC (mg/dL) * | 188 ± 55 (109 – 352) |
195 ± 49 (109 – 352) |
190 ± 65 (109 – 349) |
177 ± 48 (113 – 287) |
0.153b |
| Elevated TC (mg/dL) | 91 (30.3) | 41 (31.5) | 26 (35.6) | 24 (24.7) | 0.288 c |
| HDL-C (mg/dl) * | 56 ± 23 (0.26 – 165) |
55 ± 24 (26 – 165) |
56 ± 21 32 – 128) |
60 ± 24 (32 – 154) |
0.153 b |
| Low HDL-C (mg/dl) | 56 (18.7) | 29 (22.3) | 15 (20.5) | 12 (12.4) | 0.147 c |
| LDL-C (mg/dl) * | 104 ± 044 (35 – 247) |
107 ± 36 (35 – 222) |
107 ± 48 (58 – 247) |
96 ± 44 (41 – 202) |
0.334 b |
| Elevated LDL-C (mg/dl) | 50 (16.7) | 21 (16.2) | 15 (20.5) | 14 (14.4) | 0.559 c |
| TG (mg/dl) * | 97 ± 75 (29 – 379) |
116 ± 86 (40 – 320) |
109 ± 87 (29 – 379) |
81 ± 42 (30 – 227) |
<0.0001b |
| Elevated TG (mg/dl) | 57 (19%) | 33 (25.4) | 19 (26) | 5 (5.2) | <0.0001c |
| Atherogenic indices characteristics N (%) | |||||
| AIP (N”) | 0.23 ± 0.25 (-0.38 – 0.82) |
0.30 ± 0.25 (-0.23 – 0.81) |
0.28 ± 0.25 (-0.35 – 0.82) |
0.11 ± 0.25 (-0.38 – 0.58) |
<0.0001a |
| Elevated AIP | 182 (60.7) | 96 (73.8) | 50 (68.5) | 36 (37.1) | <0.0001c |
| Non- HDL-C mg/dl * | 123 ± 50 (57–268) |
129 ± 46 (64 – 251) |
130 ± 50 (72 – 268) |
110 ± 50 (57 – 239) |
0.004b |
| Elevated Non-HDL-C | 129 (43) | 65 (50) | 36 (49.3) | 28 (28.9) | 0.003c |
| AC * | 2.19 ±1.17 (0.39 – 9.35) |
2.35 ± 1.29 (0.39 – 9.35) |
2.32 ± 1.32 (0.56 – 5.29) |
1.82 ± 0.91 (0.40 – 4.98) |
<0.0001b |
| Elevated AC | 67 (22.3) | 35 (26.9) | 23 (31.5) | 9 (9.3) | 0.001c |
| CRI-I * | 3.19 ±1.17 (1.39 – 10.35) |
3.35 ± 1.29 (1.39 – 10.35) |
3.30 ± 1.33 (1.56 – 6.29) |
2.82 ± 0.91 (1.40 – 5.98) |
<0.0001b |
| Elevated CRI-I | 177 (59) | 88 (67.7) | 48 (65.8) | 41 (42.3) | <0.0001c |
| CRI-II * | 1.79 ±0.98 (0.21–8.54) |
1.91 ± 0.99 (0.21 – 8.54) |
1.98 ± 1.05 (0.45 – 3.97) |
1.63 ± 0.81 (0.29 – 4.21) |
0.035b |
| Elevated CRI-II | 18 (6) | 10 (7.7) | 5 (6.8) | 3 (3.4) | 0.332 c |
| CHOLIndex (CI) * | 0.45 ± 0.44 (-1.30 – 1.96) |
0.52 ± 0.43 (-1.30 – 1.96) |
0.53 ± 0.47 (-0.70 – 1.80) |
0.38 ±0.41 (-1.10 – 1.54) |
0.011b |
| Elevated CI | 0% | - | - | - | |
Abbreviations: 25(OH)D, 25-hydroxyvitamin D; BMI, Body mass index; TC, Total cholesterol; TG, Triglycerides; LDL-C, Low-density lipoprotein; HDL-C, High-density lipoprotein; AIP, Atherogenic index of plasma, Non-HDL-C, Non-HDL- Cholesterol ; CRI, Castelli’s risk index I, CRI II, Castelli risk index-II ; AC, Atherogenic coefficient, CI, CHOLIndex. Note: Data presented as N (%) for categorical variables, mean ± SD (Min-Max) for continuous normal variables (N”), and medians ± IQR (Min-Max) for continuous non-normal variables (*). The difference between variables and 25(OH) D level was calculated by Univariate ANOVA test for normally distributed variables (a), Mood's median test for non-normally distributed continuous variables (b), and Pearson’s chi-squared test for the categorical variables (c). P < 0.05 was considered significant.
Table 2.
Correlation of participant characteristics with lipid profiles and atherogenic indices.
| Age (yr) | BMI(kg/m2) | Sun exposure score | Physical activity score (MET-min/week) | ||
|---|---|---|---|---|---|
| TC (mg/dL) | Rho | 0.085 | 0.288 | -0.027 | -0.072 |
| P-value | 0.141 | <0.0001 | 0.639 | 0.215 | |
| HDL-C (mg/dL) | Rho | 0.054 | 0.071 | 0.204 | 0.226 |
| P-value | 0.350 | 0.220 | <0.0001 | <0.0001 | |
| LDL-C (mg/dL) | Rho | 0.106 | 0.196 | -0.034 | -0.060 |
| P-value | 0.068 | 0.001 | 0.559 | 0.299 | |
| TG (mg/dL) | Rho | -0.50 | 0.266 | -0.232 | -0.371 |
| P-value | 0.385 | <0.0001 | <0.0001 | <0.0001 | |
| AIP | Rho | -0.052 | 0.226 | -0.306 | -0.432 |
| P-value | 0.369 | <0.0001 | <0.0001 | <0.0001 | |
| AC | Rho | 0.032 | 0.141 | -0.206 | -0.264 |
| P-value | 0.579 | 0.015 | <0.0001 | <0.0001 | |
| Non-HDL-C (mg/dL) | Rho | 0.060 | 0253 | -0.091 | -0.147 |
| P-value | 0.303 | <0.0001 | 0.116 | 0.011 | |
| CRI-I | Rho | 0.032 | 0.141 | -0.206 | -0.264 |
| P-value | 0.579 | 0.015 | <0.0001 | <0.0001 | |
| CRI-II | Rho | 0.078 | 0.096 | -0.157 | -0.194 |
| P-value | 0.180 | 0.097 | 0.006 | 0.001 | |
| CHOLIndex | Rho | 0.091 | 0.136 | -0.106 | -0.133 |
| P-value | 0.117 | 0.019 | 0.067 | 0.021 | |
Spearman test showing relationships of lipid profile and atherogenic indices, with serum 25(OH) D level, age, BMI, sun exposure score, and physical activity score.
Table 3.
Non- parametric linear regression of lipid profile and atherogenic indices with 25(OH) D concentrations.
Table 3.
Non- parametric linear regression of lipid profile and atherogenic indices with 25(OH) D concentrations.
| Dependent variables | 25(OH)D ng/ml | |||
|---|---|---|---|---|
| B | B (95% CI) | Beta | P-value | |
| TC | -0.555 | -0.701 to -0.414 | -0.130 | 0.024 |
| HDL-C | 0.216 | 0.159 to 0.272 | 0.137 | 0.017 |
| LDL-C | -0.484 | -0.569 to -0.349 | -0.144 | 0.014 |
| TG | -1.528 | -1.688 to -1.362 | -0.314 | P < 0.0001 |
| AIP | -0.009 | -0.011 to -0.006 | -0.366 | P < 0.0001 |
| AC | -0.021 | -0.024 to -0.018 | -0.261 | P < 0.0001 |
| Non-HDL-C | -0.817 | -0.930 to-0.707 | -0.231 | P < 0.0001 |
| CRI-I | -0.021 | -0.024 to -0.018 | -0.261 | P < 0.0001 |
| CRI-II | -0.012 | -0.014 to-0.01 | -0.176 | 0.003 |
| CHOLIndex | -0.006 | -0.007 to -0.005 | -0.169 | 0.004 |
Β coefficient is a standardized coefficient in non-parametric regression analysis. Beta corresponds to the Rho Spearman coefficient.
Table 4.
Logistic regression for the association between atherogenic indices.
| Dependent variables a | 25(OH)D ng/ml | 25(OH) D status b | |||||||
|---|---|---|---|---|---|---|---|---|---|
| B | Wald | OR (95% CI) | P-value | B | Wald | OR (95% CI) | P-value | ||
| TG | Unadjusted | -0.071 | 13.490 | 0.931(0.897–0.967) | <0.0001 | 1.846 | 14.40 | 6.336(2.442–16.443) | <0.0001 |
| Model 1 | -0.056 | 8.086 | 0.946(0.910–0.983) | 0.004 | 1.590 | 10.28 | 4.904(1.856–12.959) | 0.001 | |
| Model 2 | -0.047 | 5.164 | 0.954(0.916–0.993) | 0.023 | 1.355 | 7.065 | 3.876(1.427–10.525) | 0.008 | |
| AIP | Unadjusted | -0.078 | 34.926 | 0.924(0.901–0.949) | <0.0001 | 1.468 | 31.427 | 4.340(2.598–7.251) | <0.0001 |
| Model 1 | -0.072 | 28.495 | 0.931(0.906–0.956) | <0.0001 | 1.291 | 23.111 | 3.637(2.149–6.158) | <0.0001 | |
| Model 2 | -0.062 | 20.811 | 0.940(0.915–0.965) | <0.0001 | 1.069 | 14.642 | 2.912(1.684–5.035) | <0.0001 | |
| AC | Unadjusted | -0.050 | 9.753 | 0.951(0.921-0.981) | 0.001 | 1.364 | 12.687 | 3.911(1.847–8.284) | <0.0001 |
| Model 1 | -0.047 | 7.885 | 0.954(0.924–0.986) | 0.005 | 1.278 | 10.765 | 3.589(1.673–7.700) | 0.001 | |
| Model 2 | -0.042 | 4.924 | 0.958(0.922–0.995) | 0.026 | 1.103 | 7.511 | 3.190(1.463–6.957) | 0.006 | |
| Non-HDL-C | Unadjusted | -0.041 | 11.325 | 0.959(0.937–0.983) | 0.001 | 0.892 | 11.382 | 2.440(1.453–4.097) | 0.001 |
| Model 1 | -0.32 | 6.381 | 0.969(0.945–0.993) | 0.012 | 0.729 | 7.154 | 2.074(1.215–3.540) | 0.007 | |
| Model 2 | -0.038 | 6.497 | 0.962(0935–0.991) | 0.011 | 0.716 | 6.318 | 2.047(1.171–3.578) | 0.012 | |
| CRI-I | Unadjusted | -0.039 | 12.10 | 0.961(0.939–0.982) | <0.0001 | 1.020 | 16.116 | 2.772(1.685–4.561) | <0.0001 |
| Model 1 | -0.034 | 8.264 | 0.967(0.944–0.989) | 0.004 | 0.905 | 11.998 | 2.481(1.481–4.123) | 0.001 | |
| Model 2 | -0.029 | 5.727 | 0.971(0.948–0.994) | 0.017 | 0.823 | 9.098 | 2.278(1.334–3.888) | 0.003 | |
a: Dependent variables are the elevated level of each constant; b: Vitamin D status was categorized into 25(OH)D > 20 ng/ml as sufficient, and 25(OH)D < 20ng/ml as insufficient, vitamin D sufficiency was the reference levels. Model 1: Odds ratio adjusted for IBM. Model 2: Odds ration adjusted for IBM, Physical activity, and sun exposure score. Statistical significance: P ≤ 0.05.
Table 5.
ROC curve analysis of 25(OH) D accuracy in predicting high triglycerides and atherogenic indices.
Table 5.
ROC curve analysis of 25(OH) D accuracy in predicting high triglycerides and atherogenic indices.
| Variable | AUC (95% CI) | P-value | Youden Index | Cutoff (ng/ml) | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|---|---|
| TG> 150 mg/dL | 0.657 (0.586 – 0.727) | <0.0001 | 0.294 | ≤ 15.15 | 77.19 | 52.26 |
| AIP > 0.15 | 0.702 (0.641– 0.764) | <0.0001 | 0.346 | ≤ 17.5 | 73.63 | 61.02 |
| AC > 3.0 | 0.615 (0.545 – 0.685) | 0.004 | 0.243 | ≤ 19.8 | 86.57 | 37.77 |
| Non-HDL-C > 130 mg/dL | 0.609 (0.545 – 0.672) | 0.001 | 0.188 | ≤ 20.1 | 79.07 | 39.77 |
| CRI-I >3.0 | 0.626 (0.562 – 0.690) | <0.0001 | 0.228 | ≤ 19.5 | 75.71 | 47.15 |
AUC, Area under a curve. The value of cutoff, AUC, sensitivity, specificity, and Youden index were calculated by ROC analysis. P < 0.05 indicates statistical significance.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



