
Submitted:
09 June 2024
Posted:
11 June 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
A phase 1-2, prospective, multicenter, randomized, open-label clinical trial (Code RPCEC00000382, https://rpcec.sld.cu/trials/RPCEC00000382-En/), with parallel groups, involving 1161 participants was designed to assess safety and immunogenicity of two Cuban COVID-19 vaccines (Mambisa and Abdala) in boosting COVID-19 immunity of convalescent adults after receiving one dose of either vaccine. The main safety outcome was severe vaccination adverse events occurring in <5% of vaccinees. Main immunogenicity success endpoints were ≥4-fold anti-RBD IgG seroconversion or ≥20% increase in ACE2-RBD inhibitory antibodies in >55% of vaccinees in Phase 1 and >70% in Phase 2. Neutralizing antibody titers against SARS-CoV-2 variants were evaluated. Both vaccines were safe; no deaths or severe adverse events occurred. Mild intensity adverse events were the most frequent (>73%); headache predominated for both vaccines. Phase 1 responders were 83.3% (p = 0.0018) for Abdala. Mambisa showed similar results. Phase 2 responders were 88.6% for Abdala (p <0.0001) and 74.2% for Mambisa (p = 0.0412). In both phases, anti-RBD IgG titers, inhibition percentages and neutralizing antibody titers increased significantly after the booster dose. Both vaccines were safe and their immunogenicity surpassed the study endpoints.
Keywords:
SARS-CoV-2
; COVID-19 vaccines
; convalescents
; booster
; intranasal
; intramuscular
; vaccination
; Cuba
1. Introduction
Since WHO first characterized COVID-19 as a pandemic on March 11, 2020 [1], researchers have developed various medications and vaccines to improve therapies and control.
SARS-CoV-2 infection provides natural immunity due to the virally-induced humoral and cellular memory response. But both disease- and vaccine-induced immunity tend to wane over time [2,3]. As the Omicron variant (B.1.1.529) and its subvariants have emerged globally and spread rapidly, a high risk of breakthrough infection and reinfection has been observed in vaccinees and those previously infected [4]; thus, the necessity for vaccine booster doses. Recent studies suggest that hybrid immunity (natural plus vaccination) is longer lasting and more effective than disease-induced immunity or vaccination alone [5], emphasizing the importance of vaccinating previously infected individuals.
In Cuba, five COVID-19 vaccines have been developed [6]. Abdala vaccine and Mambisa vaccine candidate (from now onwards Abdala and Mambisa) are obtained and manufactured at Havana’s Center for Genetic Engineering and Biotechnology (CIGB). Both are recombinant protein subunit vaccines based on the receptor binding domain (RBD) fragment of the SARS-CoV-2 spike protein S produced in Pichia pastoris yeast (now Komagataella phaffii) [7]. In Abdala, RBD is adjuvanted with aluminum hydroxide gel and injected intramuscularly. Mambisa’s formulation includes RBD plus the hepatitis B virus core antigen (HBcAg) expressed in Escherichia coli; it does not contain adjuvant and its application is intranasal. The rationale of this nasal vaccine is based on the SARS-CoV-2 transmission route, due to its respiratory tropism. Mambisa’s benefits include antigen delivery at the infection site, elicitation of respiratory tract mucosal immunity and needle-free administration.
Previous clinical trials for Abdala and Mambisa assessed safety and immunogenicity in three-dose schedules in seronegative adults [8,9], and also, as a booster dose in healthy adults [10]. Abdala was the first COVID-19 vaccine approved in Cuba for emergency use [11], and was a turning point for epidemic control in the country [12,13]. Studies with Abdala have also been conducted in children, adolescents and pregnant women [14,15].
The aim of this study was to assess safety and immunogenicity of Abdala and Mambisa administered as boosters for COVID-19 convalescents.
2. Materials and Methods
2.1. Vaccines
Abdala contains 50 µg RBD per 0.5 mL [11], and is administered in the deltoid region. Mambisa contains 50 µg RBD plus 40 µg HBcAg per 0.2 mL (0.1 mL per nostril). The RBD antigen sequence is identical to the ancestral SARS-CoV-2 Wuhan-Hu-1 strain (NCBI Acc. No. YP_009724390). Both products were stored at 2‒8 oC, as recommended. Mambisa was approved by the Center for State Control of Medicines, Equipment and Medical Devices (CECMED) for this study [16].
2.2. Nasal Devices for Vaccine Delivery
Three nasal devices were used for Mambisa administration: an intranasal atomization device or atomizer (a prototype employed in Phase 1 [CNEURO, Cuba] similarly designed as the commercial device employed in Phase 2 [Wuxi NEST Biotechnology, China]), identified as AZ; a nasal spray (Gaasch Packaging, UK), identified as S; and a nasal dropper (Sopac Medical, France), identified as D. (See Supplementary materials for details).
2.3. Trial Design
A phase 1-2, prospective, multicenter, randomized, open-label clinical trial, with parallel groups, was designed to assess safety and immunogenicity of Mambisa and Abdala in boosting COVID-19 immunity of convalescent adults, after receiving a single dose of either vaccine.
Phase 1 was an exploratory study to select (in terms of safety and immunogenicity) the appropriate nasal device for Mambisa administration. The selected device was used in Phase 2, to confirm and reinforce Phase 1 results.
Figure 1 shows the study flow diagram. In Phase 1, enrollment of 120 participants was completed at the Hermanos Ameijeiras Clinical-Surgical Hospital in Havana, Cuba (Figure 1A). Phase 2 included 1041 participants (Figure 1B) enrolled at Hermanos Ameijeiras Clinical-Surgical Hospital and three more clinical sites in other cities: Manuel Ascunce Domenech Provincial Clinical-Surgical Teaching Hospital (Camagüey), Pedro Raúl Sánchez Teaching Polyclinic (Pinar del Río) and Saturnino Lora Provincial Clinical-Surgical Hospital (Santiago de Cuba).
The trial was conducted in certified vaccination areas at each clinical site, and participants were vaccinated by nurses certified for this procedure. Monitors verified this process at each site, as well as accuracy of case report forms (CRF) and good clinical practice (GCP) procedures.
This study was registered in the Cuban Public Registry of Clinical Trials (Code RPCEC00000382, https://rpcec.sld.cu/trials/RPCEC00000382-En/).
2.4. Participants
Inclusion criteria: Subjects aged 19‒80 years, COVID-19 convalescents, at least two months after recovery, healthy or with compensated comorbidities. All convalescents had been infected with SARS-CoV-2 before November 2021.
Exclusion criteria: Listed in Figure 1 and detailed in Supplementary materials.
2.5. Variables
Safety. Adverse events (AE) type (local or systemic), duration, severity and causal relationship. Severity was classified as not severe or severe (when hospitalization or its prolongation was required, the reaction was life-threatening or contributed to a patient’s death). AE intensity was established in three levels: (a) mild, vaccination well tolerated, caused minimal discomfort and did not interfere with daily activities; (b) moderate, annoying enough to interfere with daily activities, and (c) severe, when interrupted daily activities.
Immunogenicity. Increase of serum IgG and IgA antibody titer against RBD; percentage inhibition of RBD-ACE2 (angiotensin-converting enzyme 2) binding; and neutralizing antibody (NAb) levels for live SARS-CoV-2 variants.
2.6. Sample Size
For Phase 1, four 30-person experimental groups (120 in total) were established. This exploratory phase did not require controlling the significance level or power. In Phase 2, the number of subjects was a function of the number of individuals who met the main success criterion of Phase 1. Considering 10% dropout, N = 232 subjects were calculated for each of the four strata provided (Mambisa, age ≤60; Mambisa, age >60; Abdala, age ≤60; Abdala, age >60), making it necessary to recruit 928 subjects. The significance level defined (α = 0.0125) guaranteed a global significance level α = 0.05 and a power of 85% to conduct the four hypothesis tests, which constituted the main objectives for analysis.
2.7. Randomization
In both study phases, two control variables were taken into account for participants’ randomization: age and clinical category of COVID-19 infection. Age was stratified into two groups: ≤60 and >60 years. The clinical category of COVID-19 disease was stratified by: symptoms (symptomatic or asymptomatic) and severity of symptoms (mild, moderate or severe).
In Phase 1, subjects were randomly distributed into four groups. Three were assigned to Mambisa, differentiated according to the device used for IN delivery. The fourth group received Abdala (Figure 1A).
In Phase 2, subjects were randomized in two groups, for Abdala and Mambisa vaccination (Figure 1B). Enrollment/allocation was made after the main researcher verified compliance with the subject selection and exclusion criteria.
Randomization lists for both phases were prepared by the trial statistical administrator using the Random Allocation Software for Windows (v 1.2).
2.8. Intervention
The Abdala group received a booster dose of 0.5 mL, intramuscularly (deltoid region). Those in Mambisa groups received a booster dose of 200 µL (100 µL per nostril), using the corresponding nasal application device. For intranasal administration, each participant was seated with the head slightly tilted back with support throughout the procedure. The product was applied into the first nostril after exhaling, keeping the head position for one minute; the same procedure was repeated in the other nostril. Mambisa vaccine application is detailed in Supplementary materials.
2.9. Outcomes
Primary outcomes were safety (severe AE with a causal relationship attributable to the studied products occurring in <5% of subjects) and immunogenicity. The main criterion for immunogenicity success was: ≥4-fold anti-RBD IgG seroconversion or ≥20% increase in RBD-ACE2 inhibitory antibodies with respect to baseline in >55% of vaccinees in Phase 1 and >70% in Phase 2. Secondary endpoints were: anti-RBD IgA titers, percentage of RBD-ACE2 inhibition and NAb against live SARS-CoV-2 variants. For IgA and NAb, seroconversion was defined as 4-fold increase in antibody titers.
2.10. Procedures
Safety. This was evaluated according to report and description of AE occurring within one-hour post-vaccination and during the follow-up of vaccinees. Vital signs were monitored before and after vaccine administration. As vaccination was an outpatient treatment, participants were required to record any AE in an Adverse Event Diary, shared with investigators during follow-up evaluations. In Phase 1, safety monitoring was carried out for 28 days and in Phase 2 for 14 days post-vaccination. AE type, duration, severity, outcome, and causality relationship were carefully registered. Systemic AE (headache, fever, nausea and hypertension, among others), were especially sought. Local adverse reactions associated with IM (pain at the injection site, erythema and induration, among others) or with IN vaccination (as rhinitis), were also explored.
Immunogenicity. Peripheral blood samples were collected on day 0 (baseline), before booster dose application, and 14 days after vaccination, to carry out hematology, clinical chemistry and immunogenicity assessments. Serum samples were aliquoted and stored at ‒20 oC until evaluation.
Immunogenicity assessment was based on seroconversion and geometric mean titers (GMT) of RBD-specific IgG and IgA antibodies, inhibition percentage of RBD-ACE2 binding, as proportions and means, and NAb levels for live SARS-CoV-2, expressed as GMT proportions.
IgG antibodies were quantified by UMELISA anti-SARS-CoV-2 RBD (Immunoassay Center, Cuba). Titers were given in arbitrary units per mL (AU/mL) with a detection limit of 1.95. ACE2-RBD antibody inhibition properties were determined using an in-house surrogate virus neutralization test inhibition (CIGB, Cuba). Results were given in inhibition percentages. The assay positivity threshold was 20%. Both methods have been described by Lemos-Pérez et al. [17].
IgA antibodies were quantified by an in-house ELISA test (CIGB, Cuba). Titers were given in AU/mL with a detection limit of 0.6. (See Supplementary materials)
NAb titers were detected by a viral microneutralization assay (MNA) using the live SARS-CoV-2 variants of concern (VOC) D614G (30654/21 D614G 1PVE6), Beta (34959/21 1PVE6 South Africa) and Delta (57383/21 Delta 1PVE6) in Phase 1, and D614G and Omicron (8649/22 OMICRON BA1 1PVE6) in Phase 2. Vero E6 cells (ATCC No. CRL-1586) were used for isolating passaging and MNA. Serum samples were heat-inactivated at 56 °C for 30 min and diluted in serial twofold dilutions (from 1:10 to 1: 2560) in microtiter plates. NAb titers were calculated using the Reed and Muench method as described by Johnson et al. [18] Viral MNA was performed at the Pedro Kourí Tropical Medicine Institute (IPK, Cuba) under biosafety level 3 (BSL-3) conditions. NAb titers were calculated as the highest serum dilution without cytopathic effect on day 5 post-infection. For NAb titer <10, a final value of 5 was assigned for statistical calculations.
2.11. Data Management
Subject information was recorded chronologically in the medical record (MR) and the CRF. Electronic entries in CRFs using the XAVIA_SIDEC software (UCI, Cuba), were carried out at clinical sites by clinical research coordinators, authorized researchers participating in the study, or by the clinical site coordinator. Database creation and validation were conducted at the National Clinical Trials Coordinating Center (CENCEC, Cuba). New entries or modifications of information collected in the CRF were recorded in auditable system traces.
2.12. Statistical Methods
We assessed safety and immunogenicity primary outcomes by intention-to-treat (ITT) (i.e., subjects who underwent randomization) and per-protocol (PP) analyses (i.e., subjects who, in compliance with the protocol, received a booster dose of vaccine according to protocol requirements, and had serum-test results before and after immunization). To evaluate vaccination effect, the main analysis consisted in applying one-sided test of comparison of a proportion with a reference value. The hypotheses tested were: H0 = π ≤ π0 (null hypothesis) and H1 = π > π0 (alternative hypothesis), where π represents the proportion of subjects who met the main success criterion or vaccine responders and π0 is the reference value for comparison. The hypotheses were examined in each of the four vaccination groups or strata conceived in both phases of the study. The level of significance (α = 0.0125), set at a quarter of the nominal value, guaranteed a global significance level α = 0.05. Pearson χ2 test or Fisher’s exact test were used to analyze categorical outcomes. We calculated 95% confidence intervals (95% CI) for all categorical outcomes using the Clopper-Pearson method.
Immunogenicity analyses based on quantitative results of immune response were performed in the PP population. Anti-RBD specific IgG and IgA were determined using seroconversion rates and geometric titers (GMT). The percentage of RBD-ACE2 inhibition was determined by seroconversion rates (percentage increase ≥20%) and means. NAb titers were measured by seroconversion rates and GMT. Estimates of vaccination effect size were determined using the median of differences (MD). The 95% CIs were determined in all cases. Lilliefors or Shapiro-Wilks tests were used to prove the normality of linear model residues comparing two or more groups. Wilcoxon matched-pairs signed rank test (p <0.05) was used to statistically compare pre- and post-vaccination outcomes. SAS for Windows (version 9.3), SPLUS (version 6.2) and SPSS (version 25) and GraphPad Prism (v. 9.4.1) were used for data processing and analysis.
3. Results
In eight months (from 15 July, 2021 to 28 March, 2022), 1161 subjects out of 1235 screened were included. Their distribution is shown in Figure 1. Table 1 shows participants’ demographic and baseline characteristics. No relevant imbalances were observed. Women predominated in both phases, but mainly in Phase 2 (70.5%).
Regarding control variables, subject composition in each vaccine group showed no statistically significant difference (p >0.05) in terms of age and clinical category of COVID-19 disease (see Table 2).
3.1. Safety
Abdala and Mambisa were well tolerated. AE were reported in 333 participants (51 in Phase 1 and 281 in Phase 2). Of the 746 AE reported, 126 occurred in Phase 1 and 620 in Phase 2, with causality related to vaccination of 91.3% (115/126) and 81.1% (503/620) respectively. All AE were classified as not severe and no AE-related withdrawals occurred. Thus, the safety endpoint of <5% of participants with serious AE was met in both study phases.
Phase 1. Vaccination-related AE were reported in 42.5% (51/120) of participants, 8.3% (10/120) who had been vaccinated with Abdala; and 10% (12/120), 12.5% (15/120) and 11.7% (14/120) to groups AZ, S and D vaccinated with Mambisa, respectively. Of the 115 vaccination-related AE, 14.8% (17/115) occurred in subjects who received Abdala, 27.0% (31/115) in those who used the AZ nasal delivery device, 28.7% (33/115) in group S and 30.2% (38/126) in group D. Headache was the most frequent AE observed in all groups, followed by low-incidence AE such as asthenia, more frequent in Abdala and Mambisa D vaccination groups. Nasal congestion and rhinitis were the most frequent local AE in the Mambisa groups (Figure 2). In terms of intensity, AE of mild intensity predominated, 73.9% (85/115), followed by moderate, 19.1% (22/115) and severe intensity, 7.0% (8/115). In this phase, 4.2% (5/120) of participants reported AE of severe intensity. In those vaccinated with Abdala, one subject reported insomnia. In Mambisa group S, one subject reported hypertension and one subject pruritus. Group D reported the majority of severe intensity AE per participant, observed in two: one reported headache, sore throat and otalgia; the other reported otalgia and nasal congestion.
Phase 2. Vaccination-related AE were reported in 27.9% (290/1041) of participants, lower than in Phase 1. AE were reported in 12.8% (133/1041) of Abdala vaccinees and 15.1% (157/1041) of Mambisa’s. A total of 503 vaccine-related AE were reported, 45.5% (229/503) in Abdala vaccinees and 54.5% (274/503) in those receiving Mambisa. Regarding AE intensity, as in Phase 1, mild intensity AE predominated, 77.3% (389/503) of reported AE were mild, followed by 21.3% (107/503) moderate, similar to Phase 1. However, severe intensity AE were lower, only 1.2% (6/503) and reported by 0.4% of participants (4/1041). One Abdala vaccinee reported asthenia, myalgia and epigastric pain and two others reported hypertension. In Mambisa groups, one participant reported headache. As in Phase 1, headache was the predominant AE in all groups, followed by asthenia (Figure 2). Pain at the injection site was a frequent local AE in the Abdala group, while nasal congestion and rhinitis were again the most frequent local AE for Mambisa vaccinees. Most of AE resolved spontaneously in the first 24‒48 hours without medication.
3.2. Immunogenicity
Some convalescents showed high baseline IgG titers or inhibition percentages due to a recent SARS-CoV-2 infection. Although most increased the immune response after the booster dose, when they did not comply with the seroconversion end-point levels established by protocol, they were not considered as responders. Table 3 summarizes the percentages of response to vaccination per ITT and PP populations. All convalescents increased their titers and functionality of RBD antibodies after the booster dose with both vaccines (Figure 3).
Phase 1. In ITT population, the percentage of Abdala vaccine responders was 83.3% (p = 0.0009), comparable results for Mambisa’s application device groups AZ and S. Group D showed 73.3% (p = 0.0218). Similar results were obtained in PP population. All responder percentages were significantly >55%, the defined endpoint (Table 3).
Table 4 summarizes the immunogenicity results in both study phases.
Serum anti-RBD IgG titers increased significantly in all vaccination groups (Figure 3A). In subjects receiving Abdala, the vaccine effect given by the MD in IgG titers was 463.8 AU/mL (95% CI 173.2-1473). Mambisa application device group AZ showed an MD of 22.0 AU/mL (95% CI 11.4-122.3); group S showed the highest MD, 57.5 AU/mL (95% CI 28.6-186.3), followed by group D, 45.5 AU/mL (95% CI 12.7-89.89) (Table 4).
Serum anti-RBD IgA titers increased in all vaccination groups (Figure 3B). However, when comparing Mambisa group devices, group D showed the lowest MD and seroconversion rates, likely due to the delivery method.
ACE2: Angiotensin-converting enzyme 2. AU/mL: Arbitrary units per mL. AZ, S and D: Mambisa nasal application devices (atomizer, spray and dropper). NAb: Neutralizing antibody titers. RBD: Receptor binding domain
Brackets contain the results of the Wilcoxon matched-pairs signed rank test. Numbers and red lines represent the median.
Phase 1: Graphs represent vaccination groups: Abdala (n = 27) and Mambisa AZ (n = 30), S (n = 29) and D (n = 29). Panel A: Anti-RBD IgG titers. Panel B: Anti-RBD IgA titers. Panel C: Inhibition percentages of RBD-ACE2 binding. Panels D, E and F: NAb titers in Abdala (n=15) and Mambisa AZ (n = 15), S (n = 15) and D (n = 14) vaccination groups against D614G, Beta and Delta SARS-CoV-2 variants respectively.
Phase 2: Graphs represent vaccination groups: Abdala (n = 509) and Mambisa (n = 494). Panel G: Anti-RBD IgG titers. Panel H: Anti-RBD IgA titers. Panel I: Inhibition percentages of RBD-ACE2 binding. Panels J and K: NAb titers for Abdala (n = 50) and Mambisa (n = 52) vaccination groups against D614G and Omicron (BA.5) SARS-CoV-2 variants respectively.Antibody functionality given by inhibition percentages also increased after booster doses for both vaccines (Figure 3C). Abdala vaccinees showed the highest increase with an MD of 70.3% (95% CI 59.0-84.9). Mambisa group AZ showed an MD of 53% (95% CI 30.7-65.6), similar to group S, but group D showed the lowest (Table 4).
NAb titers against SARS-CoV-2 VOCs significantly increased in all vaccination groups (Figure 3; D, E and F panels), but mainly against Delta variant in all vaccine groups. For both vaccines, the lowest response was observed against D614G variant, and differences between the responses against VOCs, from highest to lowest, were as follows: Delta >Beta >D614G (Table 4). Although results for the three nasal devices did not differ greatly, AZ was chosen for Phase 2 due to its easy availability.
Phase 2. For ITT population, the percentage of responders was 85.6% (p < 0.0001) for Abdala and 71.2% (p = 0.2753) for Mambisa. These were similar for PP population. All percentages were higher than 70%, the success criteria established (Table 3).
As a whole, there were a similar proportion of responders in both age groups: 81.9% for those aged ≤60 years (p <0.0001) and 80.8% for >60 years (p< 0.0001). All responder percentages were higher than 70% (Table 3).
Anti-RBD IgG titers increased significantly after the booster dose in both vaccination groups (Figure 3G). In both of them, MD values were higher than those observed in Phase 1 (Table 4).
Anti-RBD IgA titers also increased after the booster dose (Figure 3H). Abdala group showed an MD of 3416 AU/mL (95% CI 3080-3803) and the Mambisa group 2143 AU/mL (95% CI 1658-2485).
Inhibition of RBD-ACE2 binding increased significantly after booster application (Figure 3I). The Abdala group showed an MD in inhibitory percentages of 59.0% (95% CI 53.0-63.4); Mambisa group showed 34.5% (95% CI 29.3-38.1).
NAb titers were high after the booster dose (Figure 3; Panels J and K) for both vaccination groups. NAb titers against D614G variant almost doubled those against Omicron (Table 4).
When immune response was compared by age groups, a similar statistically significant increase in anti-RBD IgG titers was observed for both vaccines. However, anti-RBD IgG and IgA titer medians were slightly higher in older vaccinees on day 14 (Figure 4).
Regarding anti-RBD IgA titers, Abdala vaccinees >60 years had an MD of 3680 AU/mL (95% CI 3146-4167), similar to those ≤60 years. However, Mambisa vaccinees >60 years showed an MD of 2460 (95% CI 1811-3133), nearly double that of those ≤60 (Table 4).
Results of the RBD-ACE2 binding inhibition were similar in both age groups with both vaccines. Abdala vaccinees seroconversion rates showed differences, probably due to higher baseline inhibition levels in individuals >60 years. After vaccination, inhibition percentages were similar in both age groups.
Regarding age influence on NAb results, baseline neutralizing titers were low against D614G and Omicron. After the booster dose, a significant NAb increase was observed due to vaccination. This increase was higher in subjects >60 years, both against D614G and Omicron variants and with both vaccines (Figure 4; panels D, E, I, and J).
NAb against D614G increased both in Abdala and Mambisa vaccinees showing no significant differences in individuals ≤60 and >60 years. Individuals >60 years responded as well as those ≤60 years in both immunization groups. In Abdala group the neutralization titers were slightly higher in those >60 years (Table 4).
NAb titers against Omicron in Abdala vaccinees >60 years doubled the result of subject’s ≤60 after vaccination. However, Mambisa age groups showed very similar MD values, the highest, 150.0 (95% CI 20.0-290.0), corresponding to those >60 years.
Summarizing, the expected seroconversion outcome was observed in all immunogenicity variables of both vaccines (Table 4).
4. Discussion
Although most of the world population is recovering from the COVID-19 pandemic, having a vaccine to boost immunity against SARS-CoV-2 VOCs is of utmost importance.
In our study, a booster dose was applied to COVID-19 convalescents to evaluate the capacity of both vaccines to enhance immune response to SARS-CoV-2. As these products have different formulations and administration routes, their mechanisms for inducing response at the immune system’s local and systemic levels differ, too. Thus, the results obtained should not be expected to be exactly the same, but should meet the study’s established success outcomes.
Regarding safety, no serious AE were recorded. AE reports were minimal, mostly of mild intensity and short duration, which resolved spontaneously. Headache is a common systemic vaccine AE that was observed for both vaccines. Pain at the injection site was the most frequent local reaction for Abdala and rhinitis for Mambisa, as expected for IM and IN vaccines, but of very low incidence. These safety results were consistent with previous studies conducted with both vaccines [8,9,12].
In previous Phase 1-2 and Phase 3 clinical trials in seronegative adult populations, Abdala demonstrated to be safe and well tolerated in its three-dose schedule, and vaccine reactogenicity was dose-independent [8,12]. Pain at the injection site is consistent with findings for other COVID-19 IM vaccines [19]. Abdala’s safety has also been evaluated in children and adolescents aged 3–18 years [14], in pregnant women [15], and as a booster dose for seronegative individuals [8], with the same results.
Emergence of new SARS-CoV-2 variants, such as Omicron and its sub-variants, has revealed substantial immune evasion in serum samples from infected persons [20], or in seronegative persons who received two-dose vaccine schedules [21]. A booster dose can substantially increase neutralizing antibodies and surrogate markers, such as anti-RBD titers. It also allows an improved immune response to different SARS-CoV-2 VOC, and can reduce reinfection rates, or, if reinfection occurs, at least ensure milder symptoms. The booster dose also helps to stimulate immune response among people who do not respond to standard vaccination schedules, such as immunocompromised individuals [22].
The proposed success criteria for vaccine immunogenicity were met in both phases of this clinical trial. Eighty percent of those vaccinated with Abdala and 75% receiving Mambisa showed an increase in anti-RBD IgG titers and/or at least RBD-ACE2 inhibition percentages.
In previous studies, Abdala has shown to be highly immunogenic [8,10,23]. One of the reasons proposed is the presence of mannose structures in the recombinant RBD protein expressed in the yeast. These carbohydrate structures act as strong adjuvants and are easily detected by the receptors of antigen-presenting cells, promoting antigen presentation and T cell activation [8,24].
The humoral response induced by the IM route will protect the lower respiratory tract, but will not activate tissue-specific resident memory cells, necessary for long lasting protection in the upper respiratory tract and reduction of transmission rates [25,26]. Mucosal immunization can induce extensive adaptive immune responses, characterized by secretory IgA antibodies [27]. It can also effectively stimulate a potent systemic immune response and generate serum antibodies with neutralizing properties, reflecting the interaction between the mucosal and systemic immune systems [27].
We observed that COVID-19 convalescents boosted with Abdala elicited a strong systemic humoral response. In both study phases, anti-RBD IgG median titers increased more than 40-fold after the booster dose, and in the case of the mean of inhibition percentages, increased more than 50%. Anti-RBD IgA titers also increased.
Since the three devices used for nasal delivery in the exploratory study (Phase 1) exhibited similar results, the most readily available device was chosen for Phase 2. This atomizer permits precision dosing of the vaccine into the atrium or anterior region of the nasal respiratory epithelium, allowing immunogen contact in the nasal environment [28].
Although the study’s endpoints were based exclusively on systemic immunogenicity variables, Mambisa vaccinees showed a strong humoral immune response after the booster dose. In Phase 2, anti-RBD IgG titers increased more than 5-fold, and in the case of antibody inhibition capacity, they increased more than 30%. Also, anti-RBD IgA titers increased more than 2000 AU/mL.
Mambisa’s HBcAg immunopotentiating capacity favored local and systemic immune response to the vaccine through multiple toll-like receptor signaling pathways [29]. Similar results of increased systemic humoral response from IN vaccination have been observed elsewhere, including vaccines based on adenovirus vectors, such as the ChAdOx1 nCoV-19 vaccine [30]. For example, in a phase 3 study, the BBV154 nasal vaccine showed higher humoral immune response compared to Covaxin (BBV152), a vaccine comprised of inactivated SARS-CoV-2 and administered IM in two doses. At 42 days post-vaccination, participants showed 2- and 1.5-fold increases in serum IgG and IgA antibody levels, respectively [31].
Regarding viral neutralization, both vaccines showed significantly-increased NAb titers after the booster dose. In Phase 1, different responses were observed to the different variants, with the highest NAb titers against Delta and Beta VOCs, and lower titers against D614G. It was interesting, because generally, COVID-19 vaccines have shown a lower neutralizing response to the Beta variant [32]. In this study, the booster dose was found to significantly enhance responses to various variants, with particularly substantial increases observed against the Beta and Delta variants. An explanation could be that Beta and Delta variants were the ones that had circulated the most in Cuba before the recruitment of volunteers for this study and the results show the ability of the vaccines to recall B cells that produce high-affinity antibodies against the epitopes conserved between the different variants. These findings underscore the critical role of booster doses for convalescent individuals and highlight the robust response generated by hybrid immunity. Additionally, the significant increase in response to Delta can be explained by its local circulation; it was dominant at the time when most of the volunteers were infected with the virus [33].
In Phase 2, post-booster antibodies showed neutralization activity against Omicron in both vaccination groups. Noteworthy is the fact that convalescents enrolled in the study were infected before November 2021, when Omicron variants were not yet circulating in Cuba [32]. This corroborates previous reports referring that Omicron’s immune evasion seems to be less pronounced in individuals with hybrid immunity resulting from prior infection and vaccination [5].
We observed no difference in compliance with the trial success criteria, for subjects ≤60 and >60 years of age, in both vaccine groups. As analyzed in Phase 2, systemic anti-RBD IgG and IgA levels were higher in those aged >60 years. RBD-ACE2 inhibitory activity percentages were similar for both age groups. However, older adults also showed higher NAb titers against D614G and Omicron VOCs, with titers against the ancestral variant being 2-fold higher. In those vaccinated with Abdala, MD values were twice as high in older adults compared to younger individuals.
Effectiveness of COVID-19 vaccines depends largely on the titers of SARS-CoV-2 neutralizing antibodies [34], regardless of vaccine type, but with a booster dose effective in increasing these antibody titers in older adults [35]. In our study, the best neutralizing antibody response was seen in convalescents >60 years of age, in both IN and IM routes. It is well known that older adults are most susceptible to infections, due to more restricted antibody and T cell repertoires, which limits de novo generation of antibodies [36]. However, in previous studies with the BNT162b2 vaccine, enhancement of a strong memory B cell response was observed in individuals >60 years of age after booster doses, showing a greater increase than younger subjects [37]. A study in 2022 postulated that presence of increased population of RBD-specific memory (CD27+ CD21–) B cells in older adults may indicate prolonged persistence of the virus and, therefore, B-cell activation following SARS-CoV-2 infection [38]. This could explain the higher humoral response to vaccination in this age group, results that were unrelated to convalescents’ record of disease severity. The best neutralization results observed in subjects >60 years of age in our study corroborates results obtained when comparing the levels of IgA and IgG antibodies, with anti-RBD activity due to the booster dose, being the most responsible for the neutralizing capacity of the samples.
Our study has two main limitations. First, we were unable to measure secretory IgA and Tissue-resident memory T cells or TRM cells at the mucosal level, a helpful analytical tool to demonstrate upper respiratory tract immune status before and after the booster dose. Second, anti-RBD IgG titers were expressed in AU/mL, since at the time of the evaluations, the reference material employed by the UMELISA anti-SARS-CoV-2 RBD was not yet calibrated against the WHO International Standard for anti-SARS-CoV-2 immunoglobulin.
This is the first clinical-study report featuring a nasal subunit vaccine targeting COVID-19. Additionally, this study also demonstrated the capacity of the particulate antigen from the hepatitis B virus nucleocapsid to stimulate the immune response when administered through the nasal route.
Abdala and Mambisa proved to be highly immunogenic. A booster dose in individuals previously infected with the SARS-CoV-2 strengthened the immune response, resulting in better protection against new viral variants. Additionally, both vaccines are easy to apply and store, since they do not need low storage temperatures required for some other COVID-19 vaccines.
5. Conclusions
Administration of Abdala IM vaccine and Mambisa IN vaccine as booster doses for COVID-19 convalescents was safe and well tolerated. Both products surpassed the clinical trial’s immunogenicity endpoints. The booster dose with both vaccines strengthened participants’ immune response, including among older adults.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Abdala-Mambisa Clinical Trial Research Group list, authors name and surname, email and ORCID, Nasal devices for Mambisa vaccine delivery: Specifications, use instructions and images; Figure S1: Components of the intranasal atomization device (Device AZ); Figure S2: Components of the nasal spray device (Device S); Figure S3: Steps for nasal spray device (Device S) preparation and nasal application; Figure S4. Components of the nasal dropper (Device D); Figure S5. Components of the intranasal atomization device-Device AZ; Figure S6. Steps for intranasal atomization device AZ preparation and nasal application. Exclusion criteria for study participation. Quantification of IgA antibodies using an in-house ELISA test (CIGB, Cuba).
Author Contributions
Conceptualization, Yinet Barrese-Pérez, Rolando Uranga-Piña and Gerardo Guillén-Nieto; Data curation, Yinet Barrese-Pérez, Rolando Uranga-Piña, Yisel Avila-Albuerne, Iglermis Figueroa-García, Osaida Calderín-Marín, Martha Gómez-Vázquez and Marjoris Piñera-Martínez; Formal analysis, Yinet Barrese-Pérez and Rolando Uranga-Piña; Funding acquisition, Miladys Limonta-Fernández, Marta Ayala-Avila, Eduardo Martínez-Díaz and Eulogio Pimentel-Vazquez; Investigation, Gilda Lemos-Pérez, Yahima Chacón-Quintero, Yisel Avila-Albuerne, Iglermis Figueroa-García, Osaida Calderín-Marín, Martha Gómez-Vázquez, Marjoris Piñera-Martínez, Sheila Chávez-Valdés, Ricardo Martínez-Rosales, Lismary Ávila-Díaz, Amalia Vázquez-Arteaga, Hany González-Formental, Giselle Freyre-Corrales and Edelgis Coizeau-Rodríguez; Methodology, Gerardo Guillén-Nieto; Project administration, Iglermis Figueroa-García and Gerardo Guillén-Nieto; Supervision, Yinet Barrese-Pérez, Yisel Avila-Albuerne, Iglermis Figueroa-García, Osaida Calderín-Marín, Martha Gómez-Vázquez and Marjoris Piñera-Martínez; Writing – original draft, Gilda Lemos-Pérez; Writing – review & editing, Gerardo Guillén-Nieto.
Funding
This research was funded by the Center for Genetic Engineering and Biotechnology (CIGB), Havana, Cuba and the National Science, Technology and Innovation Program (Ministry of Science, Technology and Environment, CITMA, Cuba). CIGB had a role in study design, data interpretation and report writing, but not in data collection or analysis.
Institutional Review Board Statement
The trial was conducted according to GCP principles and was approved by the Cuban National Regulatory Authority (CECMED); code IG/CIGB-66I-669N/SARS-CoV-2/2101. The protocol followed Declaration of Helsinki guidelines [39], and was approved by the Ethics and Review Committees at each clinical site.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study
Data Availability Statement
The study protocol is provided in the appendix. The study data is available upon requests directed to the corresponding authors (gilda.lemos@cigb.edu.cu and gerardo.guillen@cigb.edu.cu). Requested data can be shared through a secure online platform after signing a data access agreement.
Acknowledgments
The authors are grateful to the participants for their willingness to participate in the study. The Abdala-Mambisa Clinical Trial Research Group, listed in Supplementary Materials, includes personnel and institutions responsible for monitoring and conducting the study, samples evaluation and investigators from the participant clinical sites. We also like to thank the health care workers from all health facilities included in this study. We appreciate the support of the CIGB National Promotion and Distribution Group for the support provided to the study in the collection and transportation of samples, supplies and vaccines. Medical writing assistance was provided by Eloisa X. Le Riverend-Morales, Esther M. Fajardo-Díaz and Gail A. Reed.
Conflicts of Interest
The authors G.L.P., Y.C.Q., S.C.V., R.M.R., L.A.D., A.V.A., H.G.F., G.F.C., E.C.R., M.L.F., M.A.A. and G.E.G.N. are employees of the Center for Genetic Engineering and Biotechnology, in Havana, where the active ingredients of the Abdala and Mambisa vaccines are produced and where the vaccine formulations were developed. The rest of the authors have no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results. None of the authors have received honoraria, consulting fees, or payments for seminar presentations, speeches, or appearances.
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. (accessed on 11 March 2020). Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020.
- Rossi, M.A.; Cena, T.; Binala, J.; Alessi, D.; Scotti, L.; Faggiano, F. Evaluation of the risk of SARS-CoV-2 infection and hospitalization in vaccinated and previously infected subjects based on real world data. Sci. Rep. 2023, 13, 1–8. [Google Scholar] [CrossRef]
- Pilz, S.; Theiler-Schwetz, V.; Trummer, C.; Krause, R.; Ioannidis, J.P. SARS-CoV-2 reinfections: Overview of efficacy and duration of natural and hybrid immunity. Environ. Res. 2022, 209, 112911. [Google Scholar] [CrossRef]
- Altarawneh, H.N.; Chemaitelly, H.; Hasan, M.R.; Ayoub, H.H.; Qassim, S.; AlMukdad, S.; Coyle, P.; Yassine, H.M.; Al-Khatib, H.A.; Benslimane, F.M.; et al. Protection against the Omicron Variant from Previous SARS-CoV-2 Infection. New Engl. J. Med. 2022, 386, 1288–1290. [Google Scholar] [CrossRef]
- Bobrovitz, N.; Ware, H.; Ma, X.; Li, Z.; Hosseini, R.; Cao, C.; et al. Protective effectiveness of previous SARS-CoV-2 infection and hybrid immunity against the omicron variant and severe disease: a systematic review and meta-regression. Lancet Infect Dis 2023, 23, 556–7. [Google Scholar] [CrossRef]
- Gorry, C. Vaccines and Public Trust: Containing COVID-19 in Cuba Verena Muzio-González PhD DSc Director of Clinical Research, Genetic Engineering and Biotechnology Center. MEDICC Rev. 2022, 24, 9–13. [Google Scholar] [CrossRef]
- Limonta-Fernández, M.; Chinea-Santiago, G.; Martín-Dunn, A.M.; Gonzalez-Roche, D.; Bequet-Romero, M.; Marquez-Perera, G.; González-Moya, I.; Canaan-Haden-Ayala, C.; Cabrales-Rico, A.; Espinosa-Rodríguez, L.A.; et al. An engineered SARS-CoV-2 receptor-binding domain produced in Pichia pastoris as a candidate vaccine antigen. New Biotechnol. 2022, 72, 11–21. [Google Scholar] [CrossRef]
- Hernández-Bernal, F.; Ricardo-Cobas, M.C.; Martín-Bauta, Y.; Navarro-Rodríguez, Z.; Piñera-Martínez, M.; Quintana-Guerra, J.; Urrutia-Pérez, K.; Chávez-Chong, C.O.; Azor-Hernández, J.L.; Rodríguez-Reinoso, J.L.; et al. Safety, tolerability, and immunogenicity of a SARS-CoV-2 recombinant spike RBD protein vaccine: A randomised, double-blind, placebo-controlled, phase 1-2 clinical trial (ABDALA Study). EClinicalMedicine 2022, 46, 101383. [Google Scholar] [CrossRef]
- Registro Público Cubano de Ensayos Clínicos (CU). Ensayo clínico fase I/II adaptativo; aleatorizado; de grupos paralelos; para evaluar la seguridad e inmunogenicidad en adultos de dos candidatos vacunales; basados en subunidades de RBD recombinante para la prevención de COVID-19 en esquemas que emplean la vía de administración nasal. Estudio MAMBISA. https://rpcec.sld.cu/ensayos/RPCEC00000345-Sp (Spanish) [accessed 2 January 2024].
- Registro Público Cubano de Ensayos Clínicos (CU). Evaluación del efecto y la seguridad de una dosis de refuerzo de Mambisa o Abdala contra la COVID-19 (Estudio BACONAO). https://rpcec.sld.cu/ensayos/RPCEC00000398-Sp (Spanish) [accessed 2 January 2024].
- Centro para el Control Estatal de Medicamentos; Equipos y Dispositivos Médicos (CECMED) (CU). ABDALA 50 μg (Vacuna anti COVID-19 de subunidad proteica). Resumen de las Características del Producto. 2021. Havana: CECMED; 2021. https://www.cecmed.cu/registro/rcp/biologicos/abdala-50-mg-vacuna-anti-covid-19-subunidad-proteica. (Spanish) [Accessed 19 July 2023].
- Hernández-Bernal, F.; Ricardo-Cobas, M.C.; Martín-Bauta, Y.; Rodríguez-Martínez, E.; Urrutia-Pérez, K.; Quintana-Guerra, J.; Navarro-Rodríguez, Z.; Piñera-Martínez, M.; Rodríguez-Reinoso, J.L.; Chávez-Chong, C.O.; et al. A phase 3, randomised, double-blind, placebo-controlled clinical trial evaluation of the efficacy and safety of a SARS-CoV-2 recombinant spike RBD protein vaccine in adults (ABDALA-3 study). Lancet Reg. Heal. - Am. 2023, 21, 100497. [Google Scholar] [CrossRef]
- Más-Bermejo, P.I.; Dickinson-Meneses, F.O.; Almenares-Rodríguez, K.; Sánchez-Valdés, L.; Guinovart-Díaz, R.; Vidal-Ledo, M.; Galbán-García, E.; Olivera-Nodarse, Y.; Morgado-Vega, I.; Dueñas-Carrera, S.; et al. Cuban Abdala vaccine: Effectiveness in preventing severe disease and death from COVID-19 in Havana, Cuba; A cohort study. Lancet Reg. Heal. - Am. 2022, 16, 100366. [Google Scholar] [CrossRef]
- Cinza-Estévez, Z.; Resik-Aguirre, S.; Figueroa-Baile, N.L.; Oquendo-Martínez, R.; Campa-Legrá, I.; Tejeda-Fuentes, A.; Rivero-Caballero, M.; González-García, G.; Chávez-Chong, C.O.; Alonso-Valdés, M.; et al. Immunogenicity and safety assessment of a SARS-CoV-2 recombinant spike RBD protein vaccine (Abdala) in paediatric ages 3–18 years old: a double-blinded, multicentre, randomised, phase 1/2 clinical trial (ISMAELILLO study). EClinicalMedicine 2023, 63, 102160. [Google Scholar] [CrossRef]
- Aguilar-Estrada, J.A.; Anaya-Herazo, C.A.; Trujillo-Ricaño, M.; Navarro-Marín, E.; Sosa-Leyva, M. COVID-19 y uso de vacunación de emergencia en el embarazo. Rev Cubana Obstetr Ginecol 2022; 48(2):e1131. https://revginecobstetricia.sld.cu/index.php/gin/article/view/1131 (Spanish) [accessed 2 January 2024].
- Centro para el Control Estatal de Medicamentos; Equipos y Dispositivos Médicos (CECMED) (CU). Mambisa (CIGB 669 y CIGB 66). Aprobación. Ensayo clínico fase I/II adaptativo; aleatorizado; de grupos paralelos; para evaluar la seguridad e inmunogenicidad en adultos de dos candidatos vacunales; basados en subunidades de RBD recombinante para la prevención de COVID-19 en esquemas que emplean la vía de administración nasal. (COVID-19). 2020. https://www.cecmed.cu/covid-19/aprobaciones/mambisa-cigb-669-cigb-66. (Spanish) [Accessed 2 January 2024].
- Lemos-Perez, G.; Chavez-Valdes, S.; Gonzalez-Formental, H.; Freyre-Corrales, G.; Vazquez-Arteaga, A.; Alvarez-Acevedo, B.; Avila-Díaz, L.; Martínez-Rosales, R.U.; Chacon-Quintero, Y.; Coizeau-Rodriguez, E.; et al. Elevated Antibody Titers in Abdala Vaccinees Evaluated by Elecsys® Anti-SARS-Cov-2 S Highly Correlate with UMELISA SARS-Cov-2 ANTI RBD, ACE-2 Binding Inhibition and Viral Neutralization Assays. J. Biotechnol. Biomed. 2022, 05, 151–157. [Google Scholar] [CrossRef]
- Johnson, V.A.; Byington, R.E.; Nara, P.L. Quantitative Assays for Virus Infectivity. In: Aldovini A; Walker BD (eds). Techniques in HIV Research. Chapter 5. London: Palgrave Macmillan; 1990. p. 87‒119. [CrossRef]
- Anand, P.; Stahel, V.P. The safety of Covid-19 mRNA vaccines: a review. Patient Saf. Surg. 2021, 15. [Google Scholar] [CrossRef]
- Mannar, D.; Saville, J.W.; Zhu, X.; Srivastava, S.S.; Berezuk, A.M.; Tuttle, K.S.; Marquez, A.C.; Sekirov, I.; Subramaniam, S. SARS-CoV-2 Omicron variant: Antibody evasion and cryo-EM structure of spike protein–ACE2 complex. Science 2022, 375, 760–764. [Google Scholar] [CrossRef]
- Cele, S.; Jackson, L.; Khoury, D.S.; Khan, K.; Moyo-Gwete, T.; Tegally, H.; San, J.E.; Cromer, D.; Scheepers, C.; Amoako, D.G.; et al. Omicron extensively but incompletely escapes Pfizer BNT162b2 neutralization. Nature 2022, 602, 654–656. [Google Scholar] [CrossRef]
- Bertrand, D.; Hamzaoui, M.; Lemée, V.; Lamulle, J.; Laurent, C.; Etienne, I.; Lemoine, M.; Lebourg, L.; Hanoy, M.; Le Roy, F.; et al. Antibody and T-cell response to a third dose of SARS-CoV-2 mRNA BNT162b2 vaccine in kidney transplant recipients. Kidney Int. 2021, 100, 1337–1340. [Google Scholar] [CrossRef]
- Zambrana, J.V.; Saenz, C.; Maier, H.E.; Brenes, M.; Nuñez, A.; Matamoros, A.; Hernández, M.; Dumas, K.; Toledo, C.; Peralta, L.; et al. Comparative Analysis of SARS-CoV-2 Antibody Responses across Global and Lesser-Studied Vaccines. Vaccines 2024, 12, 326. [Google Scholar] [CrossRef]
- Munson, S.; Parker, J.; King, T.H.; Lu, Y.; Kelley, V.; Guo, Z. et al. Coupling innate and adaptive immunity with yeast-based cancer immunotherapy. In: Orentas R; Hodge JW; Johnson BD (eds). Cancer Vaccines and Tumor Immunity. Hoboken; NJ: John Wiley & Sons; 2008. p. 131–49. [CrossRef]
- Butler, S.E.; Crowley, A.R.; Natarajan, H.; Xu, S.; Weiner, J.A.; Bobak, C.A.; Mattox, D.E.; Lee, J.; Wieland-Alter, W.; Connor, R.I.; et al. Distinct Features and Functions of Systemic and Mucosal Humoral Immunity Among SARS-CoV-2 Convalescent Individuals. Front. Immunol. 2021, 11, 618685. [Google Scholar] [CrossRef]
- Alu, A.; Chen, L.; Lei, H.; Wei, Y.; Tian, X.; Wei, X. Intranasal COVID-19 vaccines: From bench to bed. EBioMedicine 2022, 76, 103841. [Google Scholar] [CrossRef]
- Miquel-Clopés, A.; Bentley, E.G.; Stewart, J.P.; Carding, S.R. Mucosal vaccines and technology. Clin. Exp. Immunol. 2019, 196, 205–214. [Google Scholar] [CrossRef]
- Harris, A. Review: Clinical Opportunities Provided by the Nasal Administration of Peptides. J. Drug Target. 1993, 1, 101–116. [Google Scholar] [CrossRef]
- Aguilar, J.C.; Aguiar, J.A.; Akbar, S.M.F. Action Mechanisms and Scientific Rationale of Using Nasal Vaccine (HeberNasvac) for the Treatment of Chronic Hepatitis B. Vaccines 2022, 10, 2087. [Google Scholar] [CrossRef]
- Madhavan, M.; Ritchie, A.J.; Aboagye, J.; Jenkin, D.; Provstgaad-Morys, S.; Tarbet, I.; Woods, D.; Davies, S.; Baker, M.; Platt, A.; et al. Tolerability and immunogenicity of an intranasally-administered adenovirus-vectored COVID-19 vaccine: An open-label partially-randomised ascending dose phase I trial. EBioMedicine 2022, 85, 104298. [Google Scholar] [CrossRef]
- Singh, C.; Verma, S.; Reddy, P.; Diamond, M.S.; Curiel, D.T.; Patel, C.; Jain, M.K.; Redkar, S.V.; Bhate, A.S.; Gundappa, V.; et al. Phase III Pivotal comparative clinical trial of intranasal (iNCOVACC) and intramuscular COVID 19 vaccine (Covaxin®). npj Vaccines 2023, 8, 125. [Google Scholar] [CrossRef]
- Evans, J.P.; Zeng, C.; Carlin, C.; Lozanski, G.; Saif, L.J.; Oltz, E.M.; Gumina, R.J.; Liu, S.-L. Neutralizing antibody responses elicited by SARS-CoV-2 mRNA vaccination wane over time and are boosted by breakthrough infection. Sci. Transl. Med. 2022, 14, eabn8057. [Google Scholar] [CrossRef]
- Guzmán, M.G.; Pérez, L.; Tejero, Y.; Mederos, D.; Aguado, M.E.; Pintos, Y. et al. Emergence and evolution of SARS-CoV-2 genetic variants during the Cuban epidemic. J Clin Virol Plus 2022; 2:100104. [CrossRef]
- Cromer, D.; Steain, M.; Reynaldi, A.; E Schlub, T.; Wheatley, A.K.; A Juno, J.; Kent, S.J.; A Triccas, J.; Khoury, D.S.; Davenport, M.P. Neutralising antibody titres as predictors of protection against SARS-CoV-2 variants and the impact of boosting: a meta-analysis. Lancet Microbe 2022, 3, e52–e61. [Google Scholar] [CrossRef]
- Mattiuzzi, C.; Lippi, G. Efficacy of COVID-19 vaccine booster doses in older people. Eur. Geriatr. Med. 2022, 13, 275–278. [Google Scholar] [CrossRef]
- Henry, C.; Zheng, N.-Y.; Huang, M.; Cabanov, A.; Rojas, K.T.; Kaur, K.; Andrews, S.F.; Palm, A.-K.E.; Chen, Y.-Q.; Li, Y.; et al. Influenza Virus Vaccination Elicits Poorly Adapted B Cell Responses in Elderly Individuals. Cell Host Microbe 2019, 25, 357–366. [Google Scholar] [CrossRef]
- Renia, L.; Goh, Y.S.; Rouers, A.; Le Bert, N.; Ni Chia, W.; Chavatte, J.-M.; Fong, S.; Chang, Z.W.; Zhuo, N.Z.; Tay, M.Z.; et al. Lower vaccine-acquired immunity in the elderly population following two-dose BNT162b2 vaccination is alleviated by a third vaccine dose. Nat. Commun. 2022, 13, 4615. [Google Scholar] [CrossRef]
- Jeffery-Smith, A.; Burton, A.R.; Lens, S.; Rees-Spear, C.; Davies, J.; Patel, M.; Gopal, R.; Muir, L.; Aiano, F.; Doores, K.J.; et al. SARS-CoV-2–specific memory B cells can persist in the elderly who have lost detectable neutralizing antibodies. J. Clin. Investig. 2022, 132, e152042. [Google Scholar] [CrossRef]
- 39. World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [CrossRef]
Figure 1.
Study flow diagram. * Other exclusion criteria were: not attending the inclusion consultation (19 subjects in Phase 1), immunodeficiency, and unconfirmed COVID-19 disease by PCR (1 subject each in Phase 2). All withdrawals were due to voluntary abandonment. In Phase 2, the intervention was discontinued in one participant due to uncontrolled hypertension.
Figure 1.
Study flow diagram. * Other exclusion criteria were: not attending the inclusion consultation (19 subjects in Phase 1), immunodeficiency, and unconfirmed COVID-19 disease by PCR (1 subject each in Phase 2). All withdrawals were due to voluntary abandonment. In Phase 2, the intervention was discontinued in one participant due to uncontrolled hypertension.
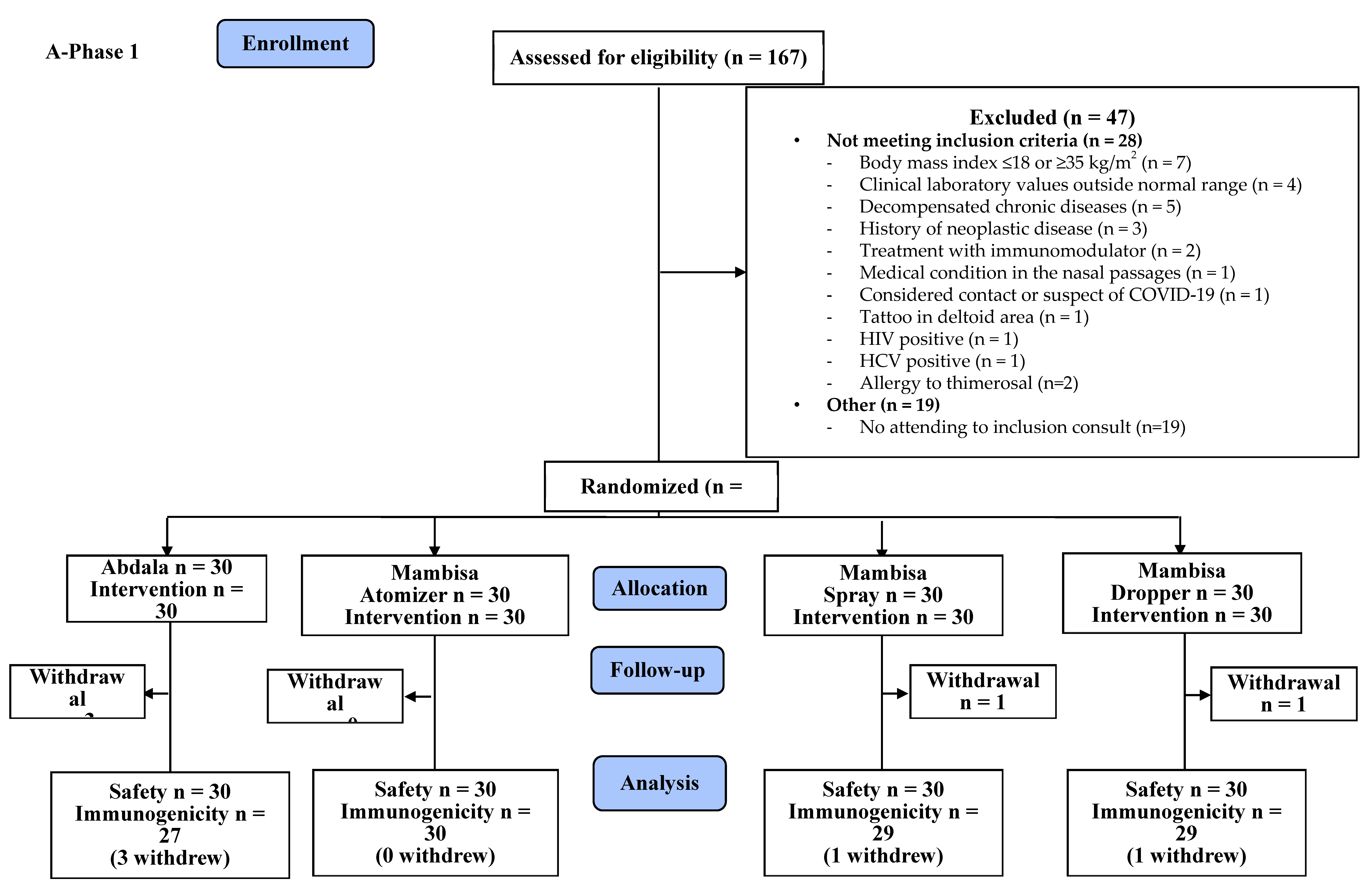
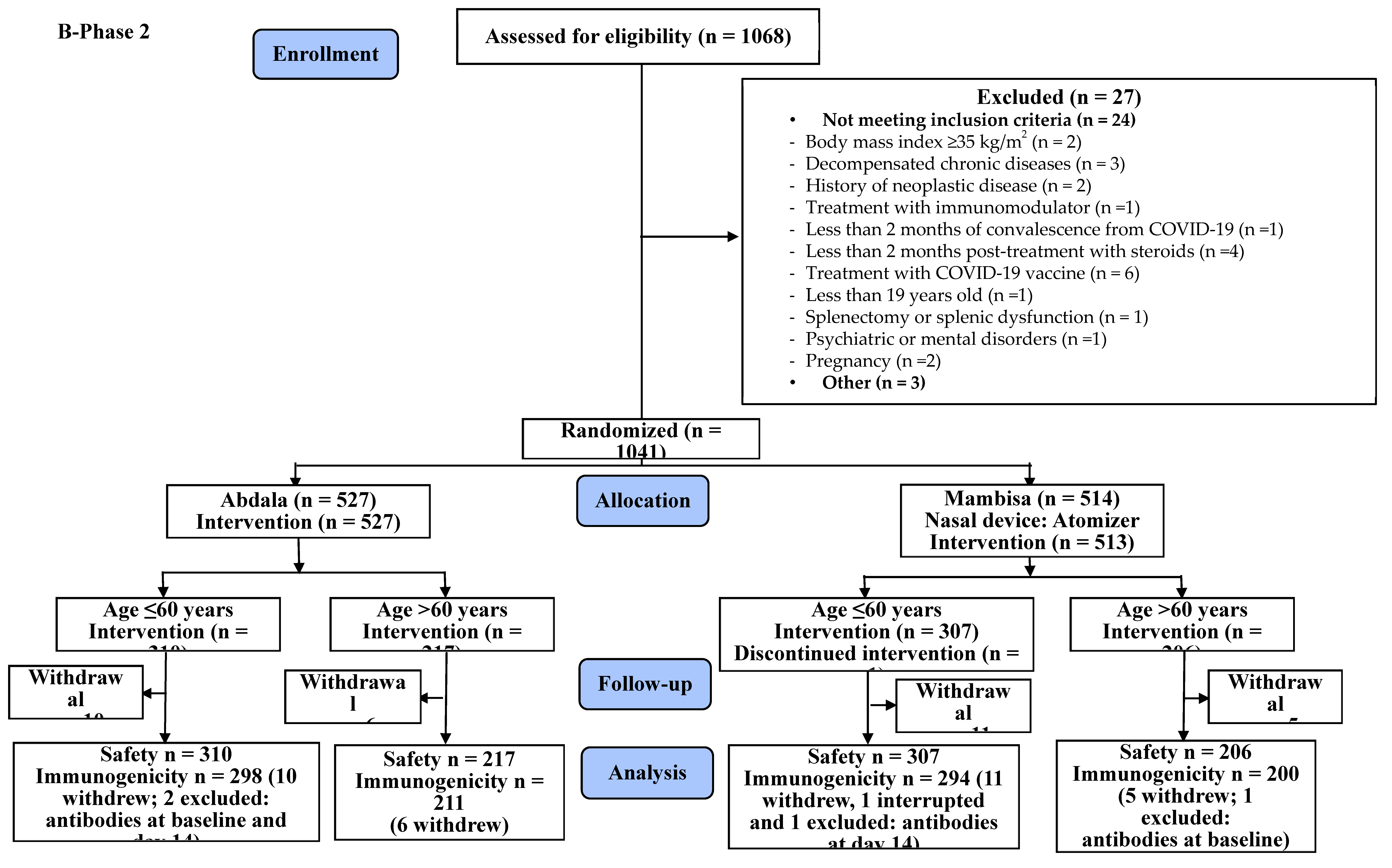
Figure 2.
Percentage of participants in each vaccination group according to the most frequently detected adverse events with certain or probable causality due to vaccination. A: Abdala vaccine. M: Mambisa vaccine candidate. Mambisa nasal vaccine delivery devices: AZ: Intranasal atomization device. D: Dropper. S: Nasal spray. Participants reporting 0 adverse events make up the remainder of the 100% in each vaccination group. Bar colors represent adverse events’ intensity levels. Other adverse events: Phase 1: Odynophagia, fever, diarrhea, pruritus, otalgia and nasal itching, among others. Phase 2: Myalgia, drowsiness, pharyngeal burning, cough with expectoration and rhinorrhea, among others.
Figure 2.
Percentage of participants in each vaccination group according to the most frequently detected adverse events with certain or probable causality due to vaccination. A: Abdala vaccine. M: Mambisa vaccine candidate. Mambisa nasal vaccine delivery devices: AZ: Intranasal atomization device. D: Dropper. S: Nasal spray. Participants reporting 0 adverse events make up the remainder of the 100% in each vaccination group. Bar colors represent adverse events’ intensity levels. Other adverse events: Phase 1: Odynophagia, fever, diarrhea, pruritus, otalgia and nasal itching, among others. Phase 2: Myalgia, drowsiness, pharyngeal burning, cough with expectoration and rhinorrhea, among others.
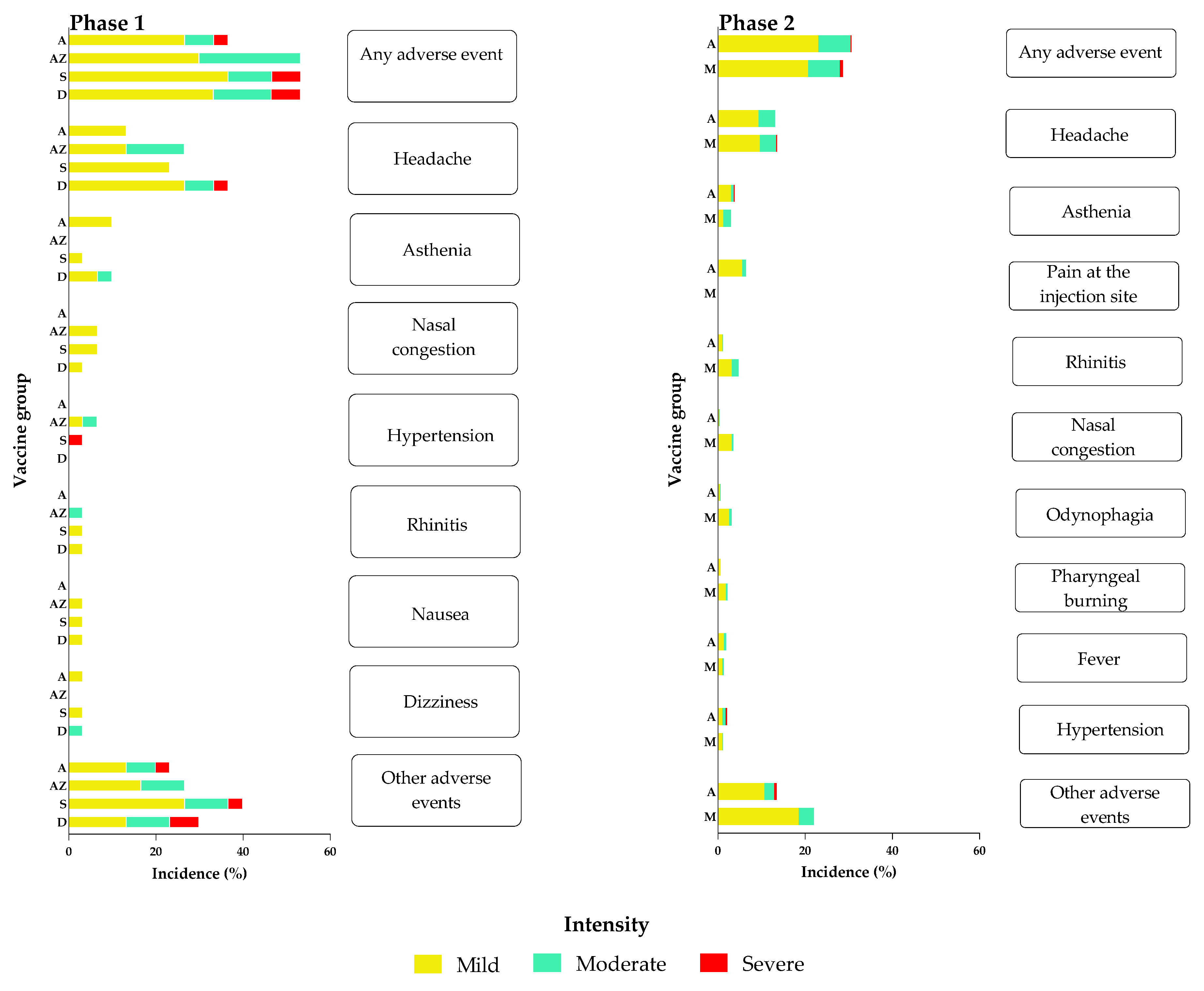
Figure 3.
Quantitative results for immunogenicity variables in both study phases, at the beginning (Day 0) and 14 days after the booster dose (Day 14).
Figure 3.
Quantitative results for immunogenicity variables in both study phases, at the beginning (Day 0) and 14 days after the booster dose (Day 14).
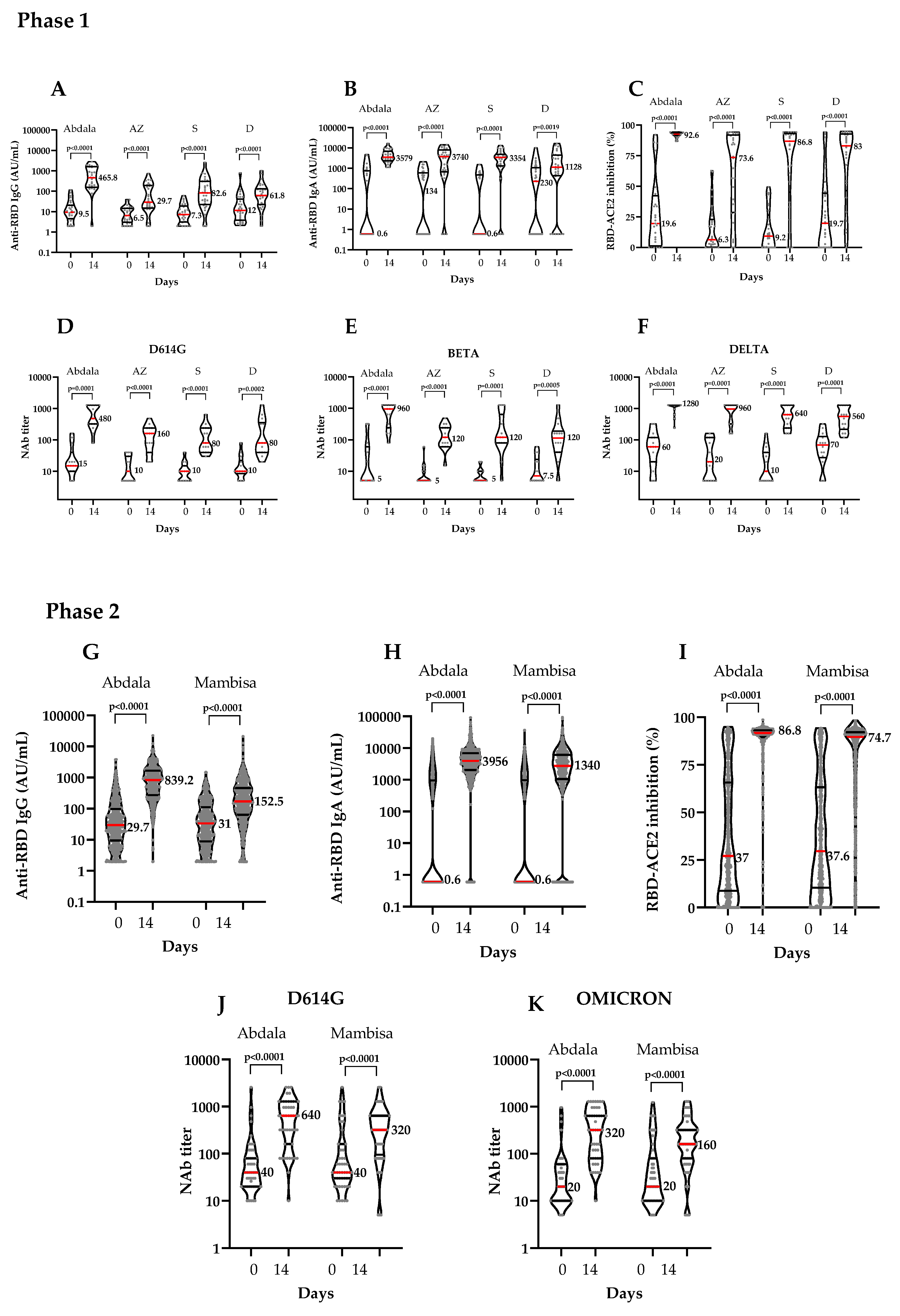
Figure 4.
Phase 2 immunogenicity results by age group (≤60 years and >60 years), at the beginning (Day 0) and 14 days after the booster dose (Day 14). ACE2: Angiotensin-converting enzyme 2. AU/mL: Arbitrary units per mL. NAb: Neutralizing antibody titers. RBD: Receptor binding domain Graphs represent vaccination groups. Abdala (Panels A to E) and Mambisa (Panels F to J). Panels A, I and panels B, G show RBD IgG and IgA antibody titers respectively. Panels C and H show inhibition percentages of RBD-ACE2 binding. Panels D, E, I and J show NAb titers against D614G (panels D and I) and Omicron (Panels E and J) SARS-CoV-2 variants, respectively. Brackets contain the results of the Wilcoxon matched-pairs signed rank test. The number and red line represent the median.
Figure 4.
Phase 2 immunogenicity results by age group (≤60 years and >60 years), at the beginning (Day 0) and 14 days after the booster dose (Day 14). ACE2: Angiotensin-converting enzyme 2. AU/mL: Arbitrary units per mL. NAb: Neutralizing antibody titers. RBD: Receptor binding domain Graphs represent vaccination groups. Abdala (Panels A to E) and Mambisa (Panels F to J). Panels A, I and panels B, G show RBD IgG and IgA antibody titers respectively. Panels C and H show inhibition percentages of RBD-ACE2 binding. Panels D, E, I and J show NAb titers against D614G (panels D and I) and Omicron (Panels E and J) SARS-CoV-2 variants, respectively. Brackets contain the results of the Wilcoxon matched-pairs signed rank test. The number and red line represent the median.
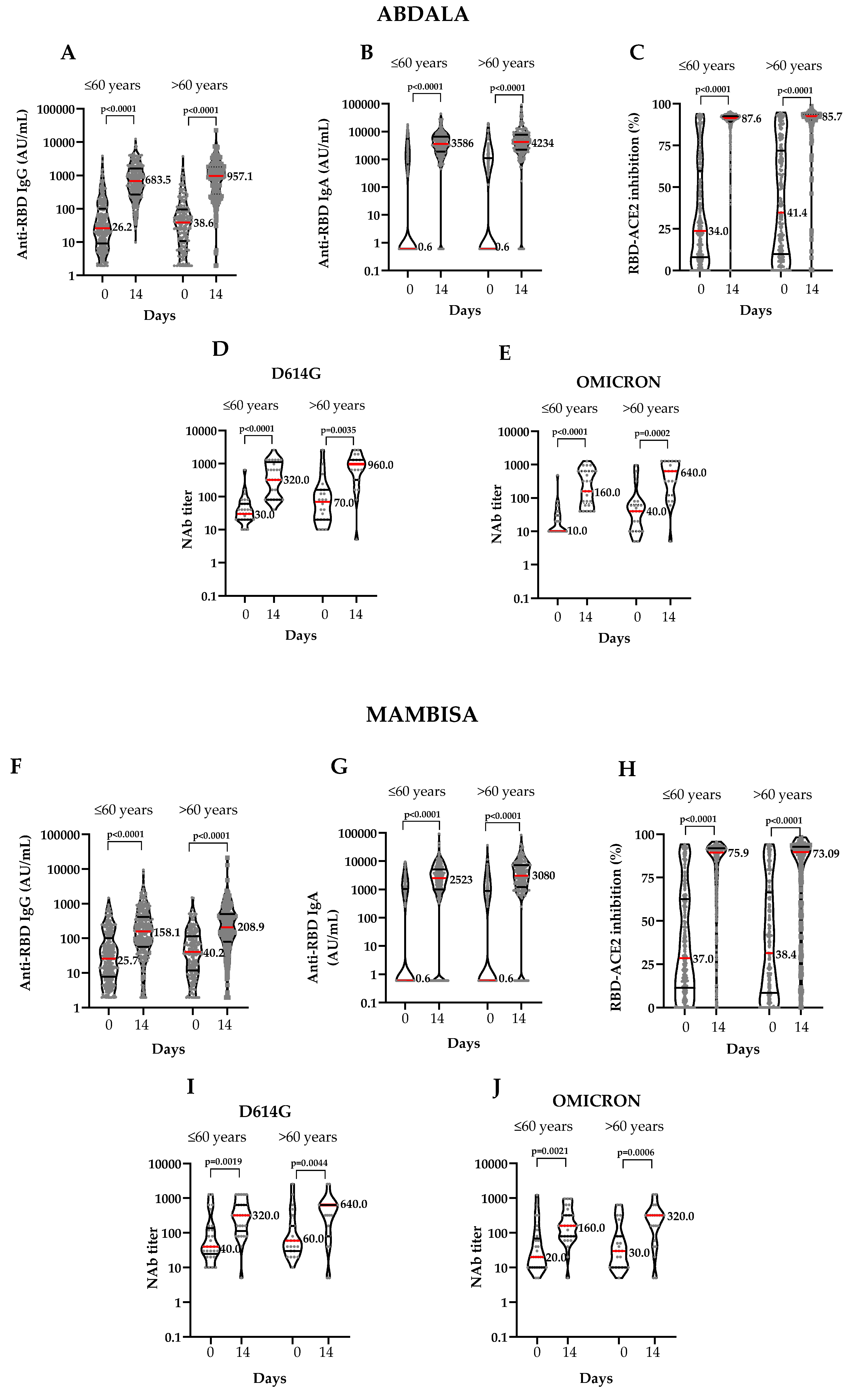

Table 1.
Participant demographics and COVID-19 disease characteristics.
| Phase 1 | ||||||||
| Group | ||||||||
| Variable | Abdala | Mambisa (three nasal application devices) | ||||||
| Atomizer | Spray | Dropper | Subtotal | Total | ||||
| N | 30 | 30 | 30 | 30 | 90 (100) | 120 (100) | ||
| Sex – n (%) | Female | 18 (60.0) | 14 (46.7) | 15 (50.0) | 23 (76.7) | 52 (57.8) | 70 (58.3) | |
| Male | 12 (40.0) | 16 (53.3) | 15 (50.0) | 7 (23.3) | 38 (42.2) | 50 (41.7) | ||
| Age | Years | 47.9 ± 15.1 | 50.9 ± 13.1 | 49.5 ± 17.1 | 48.6 ± 15.7 | 49.1 ± 14.5 | 49.2 ± 15.2 | |
| Skin color – n (%) | White | 19 (63.3) | 18 (60.0) | 17 (56.7) | 20 (66.7) | 55 (61.1) | 74 (61.7) | |
| Mulatto | 3 (10.0) | 8 (26.7) | 4 (13.3) | 4 (13.3) | 16 (17.8) | 19 (15.8) | ||
| Black | 8 (26.67) | 4 (13.3) | 9 (30.0) | 6 (20.0) | 19 (21.1) | 27 (22.5) | ||
| BMI ± SD | kg/m2 | 26.5 ± 4.0 | 27.4 ± 3.7 | 26.6 ± 3.0 | 27.2 ± 4.0 | 26.7 ± 3.6 | 26.9 ± 3.7 | |
| Age group – n (%) | ≤ 60 years | 24 (80.0) | 25 (83.3) | 23 (76.7) | 23 (76.7) | 71 (78.9) | 95 (79.2) | |
| > 60 years | 6 (20.0) | 5 (16.7) | 7 (23.3) | 7 (23.3) | 19 (21.1) | 25 (20.8) | ||
| p-value | 0.9065 | |||||||
| COVID-19 symptoms – n (%) | Asymptomatic | 9 (30.0) | 8 (26.7) | 10 (33.3) | 7 (23.3) | 25 (27.8) | 34 (28.3) | |
| Symptomatic | 21 (70.0) | 22 (73.3) | 20 (13.3) | 23 (76.7) | 65 (72.2) | 86 (71.7) | ||
| p-value | 0.8445 | |||||||
| COVID-19 disease severity – n (%) | Severe | 2 (9.5) * | 1 (4.5) * | 2 (10.0) * | 5 (21.7) * | 8 (8.9) * | 10 (11.6) * | |
| Mild | 12 (57.4) * | 19 (86.4) * | 11 (55.0) * | 12 (52.2) * | 42 (46.7) * | 54 (62.8) * | ||
| Moderate | 7 (33.3) * | 2 (9.1) * | 7 (35.0) * | 6 (26.1) * | 25 (27.8) * | 22 (25.6) * | ||
| p-value | 0.1582 | |||||||
| Phase 2 | ||||||||
| Group | ||||||||
| Variable | Abdala | Mambisa | Total | |||||
| N | 527 | 514 | 1041 (100) | |||||
| Sex – n (%) | Female | 370 (70.2) | 364 (70.8) | 734 (70.5) | ||||
| Male | 157 (29.8) | 150 (29.2) | 307 (29.5) | |||||
| Age | Years | 55.3 ± 13.7 | 55.0 ± 14.1 | 55.1 ± 13.9 | ||||
| Skin color – n (%) | White | 397 (75.3) | 384 (74.7) | 781 (75.0) | ||||
| Mulatto | 49 (10.0) | 56 (26.7) | 105 (10.1) | |||||
| Black | 81 (26.67) | 74 (13.3) | 155 (14.9) | |||||
| BMI ± SD | kg/m2 | 26.9 ± 4.2 | 26.6 ± 4.1 | 26.7 ± 4.1 | ||||
| Age group – n (%) | ≤ 60 years | 310 (58.8) | 308 (59.9) | 618 (59.4) | ||||
| > 60 years | 217 (41.2) | 206 (40.1) | 423 (40.6) | |||||
| p-value | 0.3830 | |||||||
| COVID-19 symptoms – n (%) | Asymptomatic | 27 (5.1) | 35 (6.8) | 62 (6.0) | ||||
| Symptomatic | 500 (94.9) | 479 (93.2) | 979 (94.0) | |||||
| p-value | 0.1543 | |||||||
| COVID-19 disease severity – n (%) | Severe | 38 (7.6) * | 50 (10.4) * | 88 (9.0) * | ||||
| Mild | 305 (61.0) * | 276 (57.6) * | 581 (59.3) * | |||||
| Moderate | 157 (31.4) * | 153 (31.9) * | 310 (31.7) * | |||||
| p-value | 0.2608 | |||||||
BMI: Body-mass index (weight in kilograms divided by the square of the height in meters; calculation was based on the weight and height measured at the time of screening). N: number of participants in the specified group or the total sample (also the denominator for percentage calculations). n: number of participants with the specified characteristic. SD: standard deviation. * Percentage calculations based on symptomatic individuals. P-values are for comparisons between vaccination groups.
Table 2.
COVID-19 disease category stratification in participants according to age groups in PP population.
Table 2.
COVID-19 disease category stratification in participants according to age groups in PP population.
| Phase 1 | |||||||||
| Group | |||||||||
| Variable | Abdala | Mambisa (three nasal application devices) | |||||||
| Atomizer | Spray | Dropper | |||||||
| Age | ≤ 60 years | > 60 years | ≤ 60 years | > 60 years | ≤ 60 years | > 60 years | ≤ 60 years | > 60 years | |
| N | 22 | 5 | 25 | 5 | 22 | 7 | 22 | 7 | |
| Asymptomatic - n (%) | 8 (36.4) | 0 (0.0) | 8 (32.0) | 0 (0.0) | 7 (31.8) | 3 (42.8) | 7 (31.8) | 0 (0.0) | |
| Symptomatic - n (%) | 14 (63.6) | 5 (100.0) | 17 (68.0) | 5 (100.0) | 15 (57.1) | 4 (57.1) | 15 (68.2) | 7 (100.0) | |
| p-value | 0.2798 | 0.2868 | 0.6647 | 0.1470 | |||||
| COVID-19 disease severity - n (%) | Severe | 1 (7.1) * | 1 (20.0) * | 1 (5.9) * | 0 (0.0) * | 1 (6.7) * | 1 (25.0) * | 2 (13.3) * | 3 (42.8) * |
| Mild | 10 (71.4) * | 1 (20.0) * | 15 (88.2) * | 4 (80.0) * | 10 (66.7) * | 1 (25.0) * | 9 (60.0) * | 2 (28.6) * | |
| Moderate | 3 (21.4) * | 3 (60.0) * | 1 (5.9) * | 1 (20.0) * | 4 (26.7) * | 2 (50.0) * | 4 (26.7) * | 2 (28.6) * | |
| p-value | 0.4213 | >0.9999 | 0.3860 | 0.2743 | |||||
| Phase 2 | |||||||||
| Variable | Group | ||||||||
| Abdala | Mambisa | ||||||||
| Age | ≤ 60 years | > 60 years | ≤ 60 years | > 60 years | |||||
| N | 298 | 211 | 294 | 200 | |||||
| Asymptomatic - n (%) | 19 (6.4) | 7 (3.3) | 21 (7.1) | 12 (6.0) | |||||
| Symptomatic - n (%) | 279 (93.6) | 204 (96.6) | 273 (92.8) | 188 (94.0) | |||||
| p-value | 0.1534 | 0.7149 | |||||||
| COVID-19 disease severity - n (%) | Severe | 22 (7.9) * | 15 (7.3) * | 25 (9.1) * | 21 (11.2) * | ||||
| Mild | 171 (61.3) * | 123 (60.3) * | 170 (62.3) * | 97 (51.6) * | |||||
| Moderate | 86 (30.8) * | 66 (32.3) * | 78 (28.6) * | 70 (37.2) * | |||||
| p-value | 0.9276 | 0.0726 | |||||||
N: number of participants in the specified group or the total sample (this value is the denominator for percentage calculations). n: number of participants with the specified characteristic. * Percentage calculations based on symptomatic individuals. P-values are for comparisons between vaccination groups.
Table 3.
Percentages of responders to vaccination in each group in ITT and PP population. *.
| Phase 1 | |||||||
| Group | |||||||
| Variable | Abdala | Mambisa (three nasal delivery devices) | TOTAL | ||||
| Atomizer (AZ) | Spray (S) | Dropper (D) | |||||
| ITT population | |||||||
| Responders-n/N (%; 95% CI) | 25/30 (83.3; 65.2‒94.3) |
25/30 (83.3; 65.2-94.3) |
25/30 (83.3; 65.2-94.3) |
22/30 (73.3; 54.1-87.7) |
97/120 (80.8; 72.6-87.4) |
||
| p-value | 0.0009 | 0.0009 | 0.0009 | 0.0218 | <0.0001 | ||
| PP population | |||||||
| Responders-n/N (%; 95% CI) | 25/27 (92.6; 75.7-99.1) |
25/30 (83.3; 65.2-94.3) |
25/29 (86.2; 68.3-96.1) |
22/29 (80.0; 61.0-92.4) |
97/115 (84.3; 76.4-90.4) |
||
| p-value | 0.0000 | 0.0009 | 0.0007 | 0.0119 | <0.0001 | ||
| Phase 2 | Group | ||||||
| Variable | Abdala | Mambisa | TOTAL | ||||
| ITT population | |||||||
| Responders-n/N (%; 95% CI) | 451/527 (85.6; 82.3- 88.5) |
366/514 (71.2; 67.1-75.1) |
817/1041 (78.5; 75.7-81.0) |
||||
| p-value | <0.0001 | 0.2753 | <0.0001 | ||||
| PP population | |||||||
| Responders-n/N (%; 95% CI) | 451/509 (88.6; 85.5-91.2) |
366/494 (74.1; 70.0-77.9) |
817/1003 (81.4; 78.9-83.8) |
||||
| p-value | <0.0001 | 0.0237 | <0.0001 | ||||
| Age | ≤60 years | ||||||
| Responders-n/N (%; 95% CI) | 263/298 (88.2; 84.0-91.6) |
222/294 (75.5; 70.2-80.3) |
485/592 (81.9; 78.6-84.9) |
||||
| p-value | <0.0001 | 0.0196 | <0.0001 | ||||
| Age | >60 years | ||||||
| Responders-n/N (%; 95% CI) | 188/211 (89.1; 84.1-93.0) |
144/200 (72.0; 65.2-78.1) |
332/411 (80.8; 76.6-84.5) |
||||
| p-value | <0.0001 | 0.2685 | <0.0001 | ||||
ITT: Intention to treat. N: number of participants in the specified group or the total sample. n: Number of participants with the specified characteristic. PP: Per protocol. * Immunogenicity endpoints for responders were ≥4-fold anti-RBD IgG seroconversion or ≥20% of inhibitory antibodies (inhibition of the RBD-ACE2 binding) from baseline in >55% of vaccinees in Phase 1 and >70% in Phase 2. P-values are for one-sided test of comparison of a proportion (α = 0.0125) with the defined endpoints mentioned above for each study phase.
Table 4.
Overall immunogenicity results by vaccination group in both study phases.
| Phase 1 | |||||||||||||||||||||||||||
| Group | |||||||||||||||||||||||||||
| Variable | Abdala | Mambisa (three nasal application devices) | |||||||||||||||||||||||||
| Atomizer | Spray | Dropper | |||||||||||||||||||||||||
| Day 0 | Day 14 | Day 0 | Day 14 | Day 0 | Day 14 | Day 0 | Day 14 | ||||||||||||||||||||
| Anti-RBD IgG | |||||||||||||||||||||||||||
| GMT (95% CI) | 11.0 (7.0-17.2) | 399 (219.6-724.9) | 6.79 (4.8-9.5) | 41.4 (22.5-76.2) | 7.9 (5.3-11.7) | 72.6 (37.7-139.9) | 13.6 (7.9-23.5) | 59.84 (34.5-103.8) | |||||||||||||||||||
| Seroconversion rate-n/N (%; 95% CI) | 25/27 (92.6; 75.7-99.1) |
21/30 (70; 50.6-85.3) |
20/29 (68.9; 49.1-84.7) |
15/29 (51.7; 32.5-70.5) |
|||||||||||||||||||||||
| p-value | 0.2646 | ||||||||||||||||||||||||||
| MD(95% CI) | 463.8 (173.2-1473) | 22.0 (11.4-122.3) | 57.5 (28.6-186.3) | 45.5 (12.7-89.89) | |||||||||||||||||||||||
| Anti-RBD IgA | |||||||||||||||||||||||||||
| GMT (95% CI) | 12.3 (2.8-54.3) | 3937 (2997-5172) | 19.8 (5.2-75.5) | 1244 (433.1-3571) | 7.9 (2.2-28.9) | 1262 (439.8- 3620) | 26.2 (6.2-110.9) | 389.2 (101.9-1486) | |||||||||||||||||||
| Seroconversion rate-n/N (%; 95% CI) | 23/27 (85.2; 66.3-95.8) |
22/30 (73.3; 54.1-87.7) |
24/29 (82.7; 64.2-94.1) |
14/29 (48.3;29.5-67.9) |
|||||||||||||||||||||||
| p-value | 0.0142 | ||||||||||||||||||||||||||
| MD (95% CI) | 3333 (2357-6104) | 2635 (813.9-5947) | 2825 (1345-4245) | 650.4 (0.0-2929) | |||||||||||||||||||||||
| Inhibition of the RBD-ACE2 binding | |||||||||||||||||||||||||||
| Mean (95% CI) | 27.5 (16.0-38.9) | 92.16 (91.3-93) | 15.1 (8.2- 22) | 60.36 (47.5-73.2) | 14.5 (8.3-20.7) | 68.5 (55.8-81.2) | 27.7 (16.1-39.2) | 67.94(55.8-80) | |||||||||||||||||||
| Seroconversion rate-N/n (%, 95% CI) | 23/27 (85.2; 66.3-95.8) |
23/30 (84.1; 66.2-94.8) |
24/29 (82.7; 64.2-94.1) |
18/29 (62.1; 42.3-79.3) |
|||||||||||||||||||||||
| p-value | 0.1826 | ||||||||||||||||||||||||||
| MD (95% CI) | 70.3 (59.0-84.9) | 53.0 (30.7-65.6) | 57.7 (40.1-75.5) | 40.8 (4.1-73.9) | |||||||||||||||||||||||
| Neutralizing antibodies to live SARS-CoV-2 variants | |||||||||||||||||||||||||||
| VOC | D614G | ||||||||||||||||||||||||||
| GMT (95% CI) | 20.9 (11.8- 37.1) | 526 (317.2-872.3) | 11.3 (6.9-18.4) | 107.2 (62.0-185.5) | 9367 (6.5-13.4) | 106 (63.1-178.1) | 12.9 (8.1-20.7) | 111.8 (52.8-236.5) | |||||||||||||||||||
| Seroconversion rate-n/N (%; 95% CI) | 14/15 (93.3; 68.1-99.8) |
14/15 (93.3; 68.1-99.8) |
14/15 (93.3; 68.1-99.8) |
12/14 (85.7; 57.2-98.2) |
|||||||||||||||||||||||
| p-value | 0.7152 | ||||||||||||||||||||||||||
| MD (95% CI) | 475 (305-1240) | 155 (30-220) | 75 (35-230) | 57.5 (20-475) | |||||||||||||||||||||||
| VOC | Beta | ||||||||||||||||||||||||||
| GMT (95% CI) | 15.6 (6.5-37.5) | 576.9 (340.7-976.9) | 7.5 (5.0-11.1) | 122.7 (74.1-203.3) | 7.2 (5.4-9.6) | 147 (61.9-349.2) | 10.8 (6.3-18.5) | 100.4 (45.4-222.1) | |||||||||||||||||||
| Seroconversion rate-n/N (%; 95% CI) | 13/15 (86.7; 59.6-98.3) |
14/15 (93.3; 68.1-99.8) |
14/15 (93.3; 68.1-99.8) |
11/14 (78.5;49.1-95.3) |
|||||||||||||||||||||||
| p-value | 0.3561 | ||||||||||||||||||||||||||
| MD (95% CI) | 955 (235-1260) | 115 (55-235) | 115 (70-620) | 87.5 (15-280) | |||||||||||||||||||||||
| VOC | Delta | ||||||||||||||||||||||||||
| GMT (95% CI) | 47.9 (22.9-100.5) | 1004 (763.2-1322) | 21.3 (9.7-46.5) | 713.1 (462.4-1100) | 15.3 (7.7-30.3) | 540.4 (352-829.6) | 52.1 (25.2-107.6) | 469.8 (288.8-764.3) | |||||||||||||||||||
| Seroconversion rate-n/N (%; 95% CI) | 15/15 (100; 78.2-100) |
13/15 (86.7; 59.6-98.3) |
15/15 (100; 78.2-100) |
12/14 (85.7; 57.2-98.2) |
|||||||||||||||||||||||
| p-value | 0.3201 | ||||||||||||||||||||||||||
| MD (95% CI) | 1160 (800-1260) | 955 (315-1260) | 560 (235-1220) | 360 (155-1160) | |||||||||||||||||||||||
| Phase 2 | |||||||||||||||||||||||||||
| Group | |||||||||||||||||||||||||||
| Variable | Abdala | Mambisa | |||||||||||||||||||||||||
| Day 0 | Day 14 | Day 0 | Day 14 | ||||||||||||||||||||||||
| Anti-RBD IgG | |||||||||||||||||||||||||||
| GMT (95% CI) | 31.6 (27.4-36.3) | 647.9 (578.1-726.1) | 31.0 (27.0-35.7) | 152.5 (132.3- 175.7) | |||||||||||||||||||||||
| Seroconversion rate-N/n (%; 95% CI) | 408/509 (80.1; 76.4-83.5) | 261/494 (52.1; 48.3-57.3) | |||||||||||||||||||||||||
| MD (95% CI) | 667.0 (519.4-804.0) | 95.8 (78.0-125.0) | |||||||||||||||||||||||||
| Anti-RBD IgA | |||||||||||||||||||||||||||
| GMT (95% CI) | 11.0 (7.9-15.4) | 3086 (2666-3573) | 10.0 (7.2-14) | 1340 (1053-1706) | |||||||||||||||||||||||
| Seroconversion rate-N/n (%; 95% CI) | 387/509 (76.0; 72.1-79.7) | 326/494 (66.0; 61.8-70.4) | |||||||||||||||||||||||||
| MD (95% CI) | 3416 (3080-3803) | 2143 (1658-2485) | |||||||||||||||||||||||||
| Inhibition of the RBD-ACE2 binding | |||||||||||||||||||||||||||
| Mean (95% CI) | 37.1 (34.3-39.8) | 86.8 (85.4-88.2) | 37.6 (34.9-40.3) | 74.8 (72.4-77.1) | |||||||||||||||||||||||
| Seroconversion rate-N/n (%; 95% CI) | 381/509 (74.8; 70.8-78.5) | 317/494 (64.2; 48.5-57.5) | |||||||||||||||||||||||||
| MD (95% CI) | 59.0 (53.0-63.4) | 34.5 (29.3-38.1) | |||||||||||||||||||||||||
| Neutralizing antibodies to live SARS-CoV-2 variants | |||||||||||||||||||||||||||
| VOC | D614G | ||||||||||||||||||||||||||
| GMT (95% CI) | 50.0 (35.6-70.3) | 428.7 (300.6-611.3) | 68.5 (46.0-101.9) | 262 (176-390) | |||||||||||||||||||||||
| Seroconversion rate-N/n (%; 95% CI) | 43/50 (86.0; 64.0-88.5) | 30/52 (57.7; 41.3-69.5) | |||||||||||||||||||||||||
| MD (95% CI) | 480.0 (280.0-630.0) | 220.0 (50.0-310.0) | |||||||||||||||||||||||||
| VOC | Omicron (BA.5) | ||||||||||||||||||||||||||
| GMT (95% CI) | 25.6 (18.1-36.2) | 261.5 (182.6-374.0) | 34.7 (23.2-51.9) | 156.3 (108-226.4) | |||||||||||||||||||||||
| Seroconversion rate-N/n (%; 95% CI) | 39/50 (78.0; 64.0-88.5) | 34/52 (65.4; 48.9-76.3) | |||||||||||||||||||||||||
| MD (95% CI) | 280.0 (140.0-580.0) | 150.0 (60.0-240.0) | |||||||||||||||||||||||||
| Phase 2 immunogenicity results according to age groups | |||||||||||||||||||||||||||
| Group | |||||||||||||||||||||||||||
| Variable | Abdala | Mambisa | |||||||||||||||||||||||||
| Age | ≤60 years | >60 years | ≤60 years | >60 years | |||||||||||||||||||||||
| Day 0 | Day 14 | Day 0 | Day 14 | Day 0 | Day 14 | Day 0 | Day 14 | ||||||||||||||||||||
| Anti-RBD IgG | |||||||||||||||||||||||||||
| GMT (95% CI) | 30.1 (25.1-36.1) | 616.2 (536-708.4) | 33.7 (27.0-42.0) | 695.4 (573.5-843.3) | 27.6 (22.9-33.2) | 134.6 (112-161.8) | 36.9 (29.9-45.6) | 183.2 (146.7-228.6) | |||||||||||||||||||
| Seroconversion rate-N/n (%; 95% CI) | 223/298 (74.8, 69.5-79.7) |
173/211 (81.9; 73.1-86.9) |
148/294 (50.3; 44.4-56.2) |
101/200 (50.5; 43.4-57.6) |
|||||||||||||||||||||||
| p-value | 0.0656 | >0.9999 | |||||||||||||||||||||||||
| MD (95% CI) | 541.0 (445.9-720.5) | 845.0 (645.4-966.2) | 79.3 (58.6-106.9) | 125.7 (89.8-195.0) | |||||||||||||||||||||||
| Anti-RBD IgA | |||||||||||||||||||||||||||
| GMT (95% CI) | 6.9 (4.5-10.5) | 2891 (2399-3484) | 20.8 (12.2-35.3) | 3385 (2672-4288) | 9.0 (5.8-13.8) | 1052 (754.9-1465) | 11.8 (6.9-20.1) | 1915 (1363-2690) | |||||||||||||||||||
| Seroconversion rate-N/n (%; 95% CI) | 234/298 (78.5; 73.3-83.0) |
153/211 (72.5; 66.0-78.4) |
189/294 (64.3; 58.5-69.7) |
137/200 (68.5; 61.4-74.9) |
|||||||||||||||||||||||
| p-value | 0.1399 | 0.3840 | |||||||||||||||||||||||||
| MD (95% CI) | 3212 (2712-3604) | 3680 (3146-4167) | 1893 (1435-2376) | 2460 (1811-3133) | |||||||||||||||||||||||
| Inhibition of the RBD-ACE2 binding | |||||||||||||||||||||||||||
| Mean (95% CI) | 34.05 (30.6-37.5) | 87.6 (86.2-89.0) | 41.4 (37.0-45.8) | 85.7 (82.8-88.6) | 37.0 (33.6-40.5) | 75.9 (73.0-78.8) | 38.4 (34-42.9) | 73.1 (69.1-77.1) | |||||||||||||||||||
| Seroconversion rate-N/n (%; 95% CI) | 236/298 (79.2; 74.1-83.7) |
145/211 (68.7; 62.0-74.9) |
197/294 (67.0; 60.6-71.7) |
120/200 (60.0; 52.8-66.8) |
|||||||||||||||||||||||
| p-value | 0.0094 | 0.1262 | |||||||||||||||||||||||||
| MD (95% CI) | 63.5 (58.9-66.7) | 44.0 (31.3-58.2) | 35.4 (29.6-45.5) | 31.8 (24.1-38.1) | |||||||||||||||||||||||
| Neutralizing antibodies to live SARS-CoV-2 variants | |||||||||||||||||||||||||||
| VOC | D614G | ||||||||||||||||||||||||||
| GMT (95% CI) | 37.3 (26.6-52.3) | 340.4 (218.4-530.5) | 68.5 (35.5-132.1) | 570.4 (297.8-1092) | 61.9 (36.0-106.5) | 264.3 (164-426) | 77.8 (41.6-145.8) | 259.1 (126.9-529.3) | |||||||||||||||||||
| Seroconversion rate-N/n (%; 95% CI) | 27/29 (93.1; 77.2-99.1) |
16/21 (76.2; 52.8-91.8) |
24/29 (82.7; 64.2-94.1) |
16/23 (69.6; 47.1-86.8) |
|||||||||||||||||||||||
| p-value | 0.1153 | 0.3290 | |||||||||||||||||||||||||
| MD (95% CI) | 294.0 (120.0-620.0) | 610.0 (40.0-1240) | 200.0 (40.0-310.0) | 290.0 (0.0-560.0) | |||||||||||||||||||||||
| VOC | Omicron (BA.5) | ||||||||||||||||||||||||||
| GMT (95% CI) | 18.8 (13.3-26.7) | 208.6 (133-327.1) | 37.8 (20.1-71.3) | 345.7 (181-660.2) | 31.7 (18.2-55.2) | 151.4 (96.0 -238.7) | 38.8 (20.6-73.1) | 162.8 (84.9-312.5) | |||||||||||||||||||
| Seroconversion rate-N/n (%; 95% CI) | 25/29 (86.2; 68.3-96.1) |
14/21 (66.7; 43.1-85.4) |
20/29 (69.0; 49.2-84.7) |
14/23 (60.9; 38.6-80.3) |
|||||||||||||||||||||||
| p-value | 0.1658 | 0.5711 | |||||||||||||||||||||||||
| MD (95% CI) | 150.0 (60.0-600.0) | 320.0 (80.0-950.0) | 120.0 (50.0-260.0) | 150.0 (20.0-290.0) | |||||||||||||||||||||||
ACE2: angiotensin-converting enzyme 2. GMT: geometric mean titer. MD: median of differences. RBD: receptor binding domain. VOC: variant of concern. Seroconversion was considered ≥4-fold increase in anti-RBD IgG, anti-RBD IgA or NAb titer, or ≥20% of inhibitory antibodies (inhibition of the RBD-ACE2 binding). P-value is for seroconversion rate comparison between Mambisa vaccination groups in Phase 1; and age strata in each vaccination group in Phase 2.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



