
Submitted:
11 June 2024
Posted:
12 June 2024
You are already at the latest version
Abstract
The aim of this case-series report article is to provide a new topical view of the styletubation (video intubating stylet technique) in obese patients undergoing bariatric surgeries. In contrast to various conventional direct laryngoscopes (DLs), videolaryngoscopes (VLs) have been applied in such obese population with potentially difficult airway populations. The safety and effectiveness of VLs have been repeatedly studied and the superiority of VLs then has been observed and is advocated as a routine use. In this article, among our vast use experiences of the styletubation (more than 54,998 patients since 2016) for routine tracheal intubation, we present such unique experience to apply such intubating technique in obese patient undergoing bariatric surgery. Consistent with the experiences applied in other patient populations, we found the styletubation technique to be swift (the time to intubate from 5 s to 24 s), smooth (first-attempt success rate: 100%), safe (no airway complications), and easy (high subjective satisfaction). The learning curve can be steep but is easily overcome if technical pitfalls are avoided. We, therefore, propose that the styletubation technique can be feasibly applied for tracheal intubation in obese patients undergoing bariatric surgery.
Keywords:
styletubation
; video intubating stylet
; tracheal intubation
; oro-tracheal intubation
; laryngoscope
; laryngoscopy
; videolaryngoscope
; anesthesia
; difficult airway
; airway management
; paradigm shift
; new paradigm
; obesity
; bariatric surgery
1. Introduction
Worldwide obesity has been nearly three times more since 1975. More than 1.9 billion adults are overweight and of these over 650 million are obese and 39 million children under the age of five are overweight or obese in 2020. It should be stressed that obesity is preventable. Body mass index (BMI, kg/m2) is a simple index of weight-for-height and is commonly used to differentiate overweight and obesity in adults. Overweight (BMI ≥ 25) and obesity (BMI ≥ 30) are described by excessive or abnormal fat accumulation/deposition in the human body that may impair overall health. Although BMI provides useful population-level measure of overweight and obesity (the same for both sexes and for all ages of adults), however, it should simply be regarded as a rough guide because BMI may not be comparative to the same degree of fat distribution in different individuals.
Currently, bariatric surgery is the most effective therapy and is sometimes the last resort in efforts to lose body weight. Modern bariatric procedures, in addition to usual medical and lifestyle treatment have shown effectiveness and safety [1]. Anesthesia and peri-operative management for bariatric surgeries in all categories of the obese patient populations have become focus issues for discussion [2,3,4,5]. Among all the relevant peri-operative management for bariatric and non-bariatric surgeries, airway management in such obese populations has been extensively discussed in the recent literature [6,7]. Airway management, particularly oro-tracheal intubation, remains the most challenging part of anesthesia care in obese patients [8,9].
2. Obesity and Difficult Airway
Obese patients present with excessive body fat deposition externally on the breast, thoracic wall, extremities, and particularly around the upper airway (neck and oro-pharynx). Such excess fat tissue around the neck and internal upper airway tends to make oro-tracheal intubation worse than in lean patients. Proper pre-operative planning and preparation of airway management are crucial, including ramp positioning [10,11,12], adequate preoxygenation and depth of anesthesia and analgesia. Whether awake intubation, rapid sequence induction and intubation (RSII) or routine oro-tracheal intubation be the choice of airway modality depends on many factors clinically, including patient’s factors, airway operator’s experiences and competencies, environmental issues, and facility support (for review, see [8,13,14,15,16,17,18]. The prevalence rate of difficult tracheal intubation in obese patients is 3.3% defined by three or more attempts and 8.3% defined by Cormack-Lehane views 3 and 4 [19]. Such prevalence rate of difficult intubation in obese patients, if defined differently (e.g., based on the intuation difficulty scale (IDS) score), can be different, e.g., 15.5% [20] and 13.8% [21].
It has been reported that difficult intubation is more common among obese than in non-obese patients and none of the classic risk factors for difficult intubation was satisfactory to be predictive in obese patients [20]. Meta-analysis results indicated that obesity was associated with an increased risk of difficult laryngoscopy, difficult intubation, and a Mallampati score ≥ 3 in adults patients undergoing general surgical procedures [22,23]. Similarly, increased difficult tracheal intubation was observed in patients with extreme obesity, but not in patients with lesser degrees of obesity [24]. When compared to the lean patients, the intubation success rates were found to be significantly lower in the cohorts of overweight and obese patient managed in the emergency room [25]. While it was more difficult to intubate in obese patients than in lean ones, difficult tracheal intubation was no more likely in morbidly obese patients than in only slightly obese ones [26].
In contrast to the influence on mask ventilation difficulty, morbidly obese patients do not have a higher incidence of difficult intubation than in non-morbidly obese patients [27]. However, the morbidly obese patients do have a significantly higher incidence of difficult mask ventilation. Similar conflicting results show that neither absolute obesity nor increasing BMI was associated with problematic intubation in morbidly obese patients (BMI > 40 kg/m2) [28]. Problematic intubation was only associated with increasing neck circumference and a Mallampati score of ≥ 3. Neck circumference (> 42 cm), together with BMI (> 50 kg/m2), were independent predictors of difficult intubation in morbidly obese patient population [29]. Various clinical parameters, such as abundance of pretracheal soft tissue at the level of the vocal cords [30], age, thyromental distance and ultrasonography for the distance from skin to epiglottis [31], have been used to predict difficult tracheal intubation in obese patients (more proposed predictors details are shown in Table 1).
3. Obesity and Laryngoscopy
Obese patients are expectedly at risks of peri-operative hypoxemia, including during tracheal intubation phase (i.e., intolerance to apnea). Meanwhile, higher frequency of difficult airway (i.e., difficult mask ventilation, difficult intubation, and difficulty oxygenation) is anticipated in obese population. When clinical studies regarding difficult oro-tracheal intubation in obese patient population is conducted, the common primary evaluation parameter is the intubation time. Secondary outcomes parameters then include first-pass success rate, number of attempts, Cormack-Lehane grade, intubation difficulty scale score (IDS), airway operator’s subjective difficulty of intubation, desaturation, airway bleeding, postoperative sore throat, and hoarseness.
In general, videolaryngoscope (VL) is believed to be useful for intubating the morbidly obese patient and have advantages over conventional direct laryngoscope (DL), e.g., better overall satisfaction score, intubation time, number of intubation attempts, and necessity of extra adjuncts (for comparison, see Table 2). When compared DL in such obese patients population, however, VL shows longer intubation time in addition to better laryngopscopic views, and lower IDS scores [32,34,46,47,48]. Interesting to note that Macintosh laryngoscope blade reduces, but not replaces, routine stylet use for intubation in such morbidly obese patients [49]. This particular finding is consistent with the notion that laryngoscopy technique itself faced the major potential technical hindrance: difficult insertion of the laryngoscopic blade, difficult acquisition of the glottis view, and difficult insertion or advancement of the endotracheal (ET) tube into trachea. When that happened, other extra adjuncts might be needed to apply to overcome the difficulties. In obese patients with difficult airway, several devices have been found effectively, e.g., laryngeal mask airways (LMA) [50,51,52,53], intubating LMA (ILMA) [54,55,56,57,58], LMA CTrach [51]; proSeal [59]; laryngeal tubes, FOB [60], and awake VL [61,62]. Other alternative or adjuvant devices might be helpful in facilitating airway management in obese patients, e.g., Combitube, gum elastic bougie.
4. Obesity and Styletubation
Recently, it has been demonstrated that VL gained its popularity of use for tracheal intubation in obese adults [47,65]. Even so, an argument was also made on whether VL should be the standard of care for routine tracheal intubation in such obese population [66]. The superior performance of VL routinely applied in obese patients has been demonstrated as follows: (1) more effective for the predicted difficult airway as well as a rescue tool after failed intubating attempts; (2) the video component of VL bypasses the upper pharyngeal structures (which usually are of excess fat tissues and causing narrow passage in obese patients) and therefore capable of providing a superior view of the glottis; (3) requiring less work force and external manipulation for acquiring optimal laryngeal visualization. Therefore, the better overall success rates, higher first-pass success rate, and optimal intubation time serve the crucial surrogate outcome parameters for safety and effectiveness for tracheal intubation in such a high-risk obese population (Table 2). It is, however, still lacking of objective evidence from large randomized clinical trials to support the use of VL as a first-line airway management modality in obese patients [66].
Since 2016, we have universally applied styletubation (video intubating stylet technique) for oro-tracheal intubation as a routine in our medical center (Tzu Chi hospital) (Table 3). Styletubation was conducted with a commercial video intubating stylet which was loaded into an endotracheal tube (Figure 1). Such routine uses of styletubation have been applied in the operating rooms and elsewhere hospital settings (emergency rooms, intensive care units, and general wards) [67]. During the period of last 8 years (from 2016 to 2024), we have practiced the styletubation in both normal airway scenarios and various expected difficult airway scenarios, such as ENT lesions [68], limited cervical spine mobility [69], COVID-19 [70,71], rapid sequence intubation, double-lumen endobronchial tube intubation, pediatric tracheal intubation, trans-nasal tracheal intubation, etc. In the following paragraphs, we present the application of styletubation in 20 obese patients undergoing bariatric surgeries (Table 4). In particular, styletubation technique is feasible even when such obese patient population exhibited certain clinical scenarios which might complicate the airway management [72].
Patients shown in the Table 4 were managed by the same anesthesiologist (HN Luk) with an expertise in anesthesia for bariatric surgery. The following standard anesthesia technique was applied. Routine high-flow pre-oxygenation before induction was performed. Either a high-flow nasal cannulation (30 L/min) or a face mask ventilation (15 L/min) was applied for pre-oxygenation. Patients were positioned in a stacking ramp with reverse Trendelenburg positioning of 25 degree. Standard vital signs monitoring was implemented, including non-invasive blood pressure monitoring, arterial line, pulse oximeter (SpO2), bispectral index-BIS or density spectral array-DSA, capnography (ETCO2), neuromuscular monitoring (train-of-four and post-tetanic contractions), pain intensity monitoring (surgical pleth index-SPI or analgesia nociception index-ANI), hemodynamic monitoring (FloTrac) and body temperature. Glycopyrrolate and lidocaine were first administered. Then, anesthesia was induced with midazolam (2.5 mg), ketamine (25 mg), fentanyl (100 μg), and propofol (using the adjusted dose formula: adjusted dose = ideal body weight (IBW) dose x [1+.007(total body weight – IBW)]), and rocuronium. Two-hand mask ventilation technique used by an airway assistant was performed. Before oral tracheal intubation was conducted, oral suction with a modified airway-suction tube unit was used to clear any possible saliva or secretions along the oro-pharyngeal space. Patient’s mouth was then opened by an airway assistant with an effective jaw-thrust maneuver to lift patient’s epiglottis. Then, styletubation was performed with a video intubating stylet (Figure 1). Anesthesia was then maintained with both inhalational anesthetic (sevoflurane or desflurane, around 0.5 MAC), propofol (ICI, effect concentration around 1.5 μg/ml). Neuromuscular blockade was maintained with rocuronium and monitored with ToF and PTC indices. During emergence, rocuronium was chelated by sugammadex. Tracheal extubation was performed when ToF reached > 0.95 and patient could obey oral command. Post-operative CPAP was used if desaturation or CO2 retention occurred. When necessary, patient would be kept in ICU overnight.
Patients undergoing bariatric surgery may have varied degree of obesity (Table 4). Figure 2 shows such an example of patient with BMI of 34.8 kg/m2. Styletubation was easy and smooth in this category of patients (time from lip to trachea: 5 s). In contrast, in patients with much higher BMI (e.g., above 60 kg/m2), pre-operative airway evaluation may predict potential difficulties on tracheal intubation (e.g., high degrees of Mallampati score, bull-necked, increased neck circumference, accumulation of adipose tissue around upper airway, limited neck extension, etc.). Figure 3 shows such an example. During styletubation for tracheal intubation, more collapsed pharyngeal structures, omega-shaped epiglottis, and limited visualization of glottis were expected seen in this patient (BMI >100 kg/m2). Even so, the oro-tracheal intubation by styletubation was smooth, easy, and prompt (intubation time: 12 s).
The obese patients commonly presented themselves with either pear-shaped or apple-shaped body habitus which displayed over-accumulation of fat in the abdomens, waists, hips, thighs, and buttocks. With higher chance, the fat pad also caused narrowing of the pre-tracheal and pharyngeal space. While in the scenario of obese patient under anaesthetized and muscle relaxation condition, the pharyngeal folds might be weighed down by excess fat around upper airway and therefore prevented visualization of the larynx. Figure 4 shows such expected scenario in patients undergoing bariatric surgery. In additional to omega-shaped epiglottis (Figure 3E,F), the epiglottis might be floppy and collapsed (Figure 4A,B). Also, an exaggerated plica vocalis might severely obstruct the true vocal cords in obese subjects (Figure 4C,D).
The superior roles of VL in patients with limited cervical spine mobility have been widely documented [73,74,75,76]. The advantages of VL include causing less upper cervical spine motion, better probability of first-pass success, less risks of intubation failure during cervical immobilization or limited cervical spine mobility. Recently, application of styletubation has also been demonstrated in such potential difficult airway [69]. The advantages of styletubation include swift intubating time, excellent first-pass success rate, less airway stimulation or injuries. Understandably, in obese patient with limited cervical spine mobility undergoing bariatric surgery, difficult oro-tracheal intubation would be expected. Figure 5 shows such patient underwent bariatric surgery.
This is a 56–year-old man with past history of cervical spondylosis with radiculopmyelopathy and quadriparesis. Surgical history of anterior cervical discectomy and fusion (ACDF) in C3/C4, C4/C5, and C5/C6, with PEEK cage fusion and Zephir plate fixation was noted. Other medical history included hypertension, type 2 diabetes mellitus, old cardiovascular accident, and obstructive sleep apnea. His BMI was 45.4 kg/m2 and underwent LSG and mesh repair of ventral hernia. Pre-operative airway evaluation showed higher degree of Mallampati grading, short neck and less cervical extension (Figure 5A–D). During styletubation, copious saliva and secretions, collapsed airway soft tissues, and dropped epiglottis were observed (Figure 5E,F). Even in the presence of unfavorable conditions for oro-tracheal intubation in such case scenario, the performance of styletubation was still smooth and swift.
Videolaryngoscopy is prevalently used in routine airway management and has been demonstrated a higher overall rate of successful intubation in certain clinical scenarios, including difficult airways [77,78,79,80]. In comparison to the learning curve of using DL by the novice trainees, VL shows safer and more usable for the unexperienced airway providers and learners, especially for difficult airway scenarios [81,82,83]. The advantageous roles of VL include video camera and a hyperangulated blade geometry to acquire a better glottis visualization, especially in difficult airway situations with limited mouth opening or restricted neck movement. Such advantages of VL prompted the learning curve of novice airway trainees.
It is important to know whether styletubation, when used by novices of airway management, is effective in both normal and difficult airway scenarios [84,85,86]. In mannequin studies, styletubation provided faster, easier, and less traumatic intubation than the DL or VL [87,88,89,90,91]. The learning curve for applying styletubation by novice trainees is steep. Figure 6 shows the performance of styletubation by a third-year anesthesia resident in an obese patient undergoing bariatric surgery. The intubation was swift and smooth with first-pass success.
5. Technical Pitfalls and Pearls
It has been reported that more than half of all airway incidents and complications followed primary difficulties with tracheal intubation. Most important, sup-optimal attempts at laryngoscopy are wasted attempts which might lead to clinical disasters [92]. In that sense, VL shows better chance and possible superiority over DL under difficult airway scenarios and in critically ill patients [32,93,94]. Therefore, VL has been called for use as a first-line tool for routine airway management and be accessible at all times, including application in obese patients [36,95]. In contrast to the potentially dominant and superiority role of VL in the field of airway management, the emerging role of styletubation for tracheal intubation might be in a challenge position in such already leading-position of VL in the near future [67,96].
Several limitations and technical pitfalls of VL have been discussed [97]. Similarly, the pitfalls and pearls of use of styletubation existed which has been described earlier [98]. Those commonly identified disadvantages of a rigid optical airway management device include: (1) losing orientation or a clear/identified visualization of oro-pharyngeal structures; (2) anatomical images becoming blurred and un-identifiable because the close contact of the scope lens abut to the airway anatomical structures or secretions/blood; (3) inadequate lift-up of the epiglottis and therefore sub-optimal glottis visualization. Other human engineering factors include (1) the poor coordination of the airway operator’s eye/wrist/arm movements; (2) without establishing a compulsory habit to identify the signposts/landmarks along the airway pathway (e.g., palate, uvula, tongue base, epiglottis); (3) without proper prevention/minimization of fogging over the lens; (4) without a stopper device on to the proximal end of the stylet to hold the endotracheal tube in a proper position.
As the common “did not work-problems” of endoscopy technique, the suboptimal image quality and invisibility of regions of interest (e.g., vocal cords, anterior commissure) similarly occurred when styletubation was applied. Possible troublesome scenarios include: oro-pharyngeal accumulation of saliva/secretions, retention and pooling of copious secretions nearby glottis, diffusely blurred images due to fogging of the lens, partially blurred image due to secretions on lens itself. The solutions for aforementioned scenarios which can cause prolonged intubation time or intubating failure include use a suction apparatus and effectively suck all secretions away beforehand [99].
Figure 7 demonstrates the impact of secretions on styletubation in two obese patients undergoing bariatric surgery (Figure 7A–F). Foaming occurs when excessive saliva/secretions pooled in the mouth and throat. Such bubbles might obstruct view during intubation. Although pre-anesthesia administration of anticholinergic might be beneficial in some aspects in obese patients (e.g., post-operative nausea and vomiting, reduction in gastric contents and saliva secretions), its role has not been consistently addressed in the current guidelines of anticholinergics [100,101]. Therefore, the problems of copious saliva secretions need to be carefully handled during styletubation. In obese patients undergoing bariatric surgeries, an adequate and effective suctioning method is in particular helpful and crucial. Figure 8 shows such an example with a modified suction tube-airway tube unit [99] to clear the airway before styletubation commenced.
Similar to the application of DL or VL in obese patients, styletubation itself could also be facilitated by and conjoined with laryngoscopy in the obese patient population [102,103,104]. Combined styletubation with VL (video-twin technique) has been applied in order to enhance the effectiveness of tracheal intubation in certain clinical scenarios, including in obese patients [105]. Figure 9 shows such combined styletubation with VL in an obese patient undergoing bariatric surgery. Both the first-pass success and time to intubation are excellent with such combined technique, especially for novice airway operator to learn.
Limitations
There are several limitations of the present series case report and narrative review article. In contrast to the highest level of evidence of the systematic reviews and meta-analyses, this article may still provide a new insight of the of unique airway management modality in obese patients undergoing bariatric surgery and serve as a source of quick up-to-date reference for readers with interest in styletubation and laryngoscopy. It should be emphasized, however, our article does involve inherent shortcomings in terms of non-standardized prospective study design, completeness of the literature searching and potential human bias in the appraisal of retrieved articles, and validity and objectivity of interpretation of findings.
Although we have a vast array of clinical case experiences (more than 50,000 cases since 2016) of applying styletubation technique, we have not conduct a prospective comparative study of styletubation against laryngoscopy in obese patients undergoing bariatric surgery. Some of the difficulties of such a robust study design include different competencies and preferences of the airway operators, un-controlled clinical conditions and scenarios, ethic issues involving human subjects, etc. While we presented 20 clinical cases for using styletubation in this article, the sample size is small, and it is impossible to make any statistical analysis on its significance. Also, this clinical cases report was conducted mainly by a very small group of airway operators in a single medical center. Therefore, the generalizability of the study conclusion may be limited, and use and interpretation of the results should be carefully considered to avoid any unnecessary overstatements.
6. Conclusion
The popular role of VL for tracheal intubation, including in obese patients, has been evolved since two decades ago. However, one of the inherent problems with VL is difficulty in landing the endotracheal tube into trachea correctly and smoothly, although a better laryngeal view obtained than DL. This technical difficulty possibly attributes to thickness and width of the blades, and the more acute angle of the VL’s view, which possibly is poorly negotiable by the curvature of the endotracheal tube. To solve this problem, a rigid metal stylet to enhance the curvature of the endotracheal tube has conventionally been used to optimize the intubation attempt with laryngoscopy. Similar to such design of a rigid stylet, a rigid/semi-rigid fiberscope, e.g., the Bonfils endoscope, has garnered less-than-expected interest in the management of difficult airways (e.g., in obese patients) since then. Bonfils endoscope, however, was also found to be more difficult to intubate an obese patient, mostly due to redundant or collapsed soft tissues impeding the glottic view. Unfortunately, an asleep/awake flexible fiberoptic technique (FOB) is of less clinical interest as it does neither circumvent airway collapsibility after induction of anesthesia, and hence may be more difficult to maneuver by the airway operator [16].
The success of tracheal intubation by a variety of airway intubating tools is dependent on many factors, including the training programs, skills, and competency of the airway operator. Meanwhile, the basic tenets of tracheal intubation remain to be the “first-attempt success” and “intubation time”, both are even more crucial in obese patient undergoing bariatric surgery. We have demonstrated, in this article, that styletubation serves well for such goal of tracheal intubation in this particular clinical scenario (Table 2). With the increasing attention at the styletubation technique in various clinical scenarios [67,96,106,107,108], we believe the potential clinical role of styletubation will eventually supersede that of laryngoscopy in the near future. In conclusion, in obese patients undergoing bariatric surgery, the role of routine application of styletubation is promising and worthy to test.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Videos S1-S19 cited in the Table 4.
Author Contributions
Conceptualization, H.-C. L., H.-N.L., J.Z.Q.; methodology, H.-C.L., B.-G.W., B.-C.C., H.-N.L.; formal analysis, H.-C.L., J.P., H.-N.L., J.Z.Q.; investigation, H.-C.L., H.-N.L.; resources, H.-N.L.; data curation, H.-N.L., J.Z.Q.; writing—original draft preparation, H.-C.L., H.-N.L.; writing—review and editing, H.-N.L., J.Z.Q; visualization, H.-C.L., J. P., H.-N.L.; supervision, H.-N.L.; project administration, H.-N.L.; funding acquisition, H.-N.L. All the authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and was approved by REC, Hualien Tzuchi Hospital (approved letter number: CR113-XX).
Informed Consent Statement
Written informed consent was obtained from all patients or their legally authorized representatives.
Data Availability Statement
Data is contained within the article.
Acknowledgments
This work was supported by Hualien Tzuchi Hospital.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Arterburn, D.E.; Telem, D.A.; Kushner, R.F.; Courcoulas, A.P. Benefits and risks of bariatric surgery in adults: A review. JAMA. 2020, 324, 879–887. [Google Scholar] [CrossRef] [PubMed]
- Ogunnaike, B.O.; Jones, S.B.; Jones, D.B.; Provost, D.; Whitten, C.W. Anesthetic considerations for bariatric surgery. Anesth Analg. 2002, 95, 1793–1805. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, K.H.; Helm, M.; Lak, K.; Higgins, R.M.; Gould, J.C.; Kindel, T.L. The risk of post-operative complications in super-super obesity compared to super obesity in accredited bariatric surgery centers. Obes. Surg. 2019, 29, 2964–2971. [Google Scholar] [CrossRef]
- Mulier, J.P.; Dillemans, B. Anaesthetic factors affecting outcome after bariatric surgery, a retrospective levelled regression analysis. Obes Surg. 2019, 29, 1841–1850. [Google Scholar] [CrossRef] [PubMed]
- Marinari, G.; Foletto, M.; Nagliati, C.; Navarra, G.; Borrelli, V.; Bruni, V.; Fantola, G.; Moroni, R.; Tritapepe, L.; Monzani, R.; Sanna, D.; Carron, M.; Cataldo, R. Enhanced recovery after bariatric surgery: an Italian consensus statement. Surg Endosc. 2022, 36, 7171–7186. [Google Scholar] [CrossRef] [PubMed]
- Seyni-Boureima, R.; Zhang, Z.; Antoine, M.M.L.K.; Antoine-Frank, C.D. A review on the anesthetic management of obese patients undergoing surgery. BMC Anesthesiol. 2022, Apr 5;22(1):98. [CrossRef]
- Kaye, A.D.; Lingle, B.D.; Brothers, J.C.; Rodriguez, J.R.; Morris, A.G.; Greeson, E.M.; Cornett, E.M. The patient with obesity and super-super obesity: Perioperative anesthetic considerations. Saudi J Anaesth. 2022, 16, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.; Wong, D.T. Airway management and oxygenation in obese patients. Can J Anaesth. 2013, 60, 929–945. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, E. Airway management of the morbidly obese patient. J Perioperative Practice. 2016, 26, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Collins, J.S.; Lemmens, H.J.; Brodsky, J.B.; Brock-Utne, J.G.; Levitan, R.M. Laryngoscopy and morbid obesity: a comparison of the "sniff" and "ramped" positions. Obes Surg. 2004, 14, 1171–1175. [Google Scholar] [CrossRef]
- Rao, S.L.; Kunselman, A.R.; Schuler, H.G.; DesHarnais, S. Laryngoscopy and tracheal intubation in the head-elevated position in obese patients: a randomized, controlled, equivalence trial. Anesth Analg. 2008, 107, 1912–1918. [Google Scholar] [CrossRef]
- Lee, S.; Jang, E.A.; Hong, M.; Bae, H.B.; Kim, J. Ramped versus sniffing position in the videolaryngoscopy-guided tracheal intubation of morbidly obese patients: a prospective randomized study. Korean J Anesthesiol. 2023, 76, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, M.S. Airway management and morbid obesity. Eur J Anaesthesiol. 2010, 27, 923–927. [Google Scholar] [CrossRef] [PubMed]
- Aceto, P.; Perilli, V.; Modesti, C.; Ciocchetti, P.; Vitale, F.; Sollazzi, L. Airway management in obese patients. Surg Obes Relat Dis. 2013, 9, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Langeron, O.; Birenbaum, A.; Le Saché, F.; Raux, M. Airway management in obese patient. Minerva Anestesiol. 2014, 80, 382–392. [Google Scholar] [PubMed]
- Liew, W.J.; Negar, A.; Singh, P.A. Airway management in patients suffering from morbid obesity. Saudi J Anaesth. 2022, 16, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Thota, B.; Jan, K.M.; Oh, M.W.; Moon, T.S. Airway management in patients with obesity. Saudi J Anaesth. 2022, 16, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Waheed, Z.; Amatul-Hadi, F.; Kooner, A.; Afzal, M.; Ahmed, R.; Pande, H.; Alfaro, M.; Lee, A.; Bhatti, J. General anesthetic care of obese patients undergoing surgery: A review of current anesthetic considerations and recent advances. Cureus. 2023, Jul 8;15(7):e41565. [CrossRef]
- Neligan, P.J.; Porter, S.; Max, B.; Malhotra, G.; Greenblatt, E.P.; Ochroch, E.A. Obstructive sleep apnea is not a risk factor for difficult intubation in morbidly obese patients. Anesth Analg. 2009, 109, 1182–1186. [Google Scholar] [CrossRef] [PubMed]
- Juvin, P.; Lavaut, E.; Dupont, H.; Lefevre, P.; Demetriou, M.; Dumoulin, J.L.; Desmonts, J.M. Difficult tracheal intubation is more common in obese than in lean patients. Anesth Analg. 2003, 97, 595–600. [Google Scholar] [CrossRef]
- Kim, W.H.; Ahn, H.J.; Lee, C.J.; Shin, B.S.; Ko, J.S.; Choi, S.J.; Ryu, S.A. Neck circumference to thyromental distance ratio: a new predictor of difficult intubation in obese patients. Br J Anaesth. 2011, 106, 743–748. [Google Scholar] [CrossRef]
- De Jong, A.; Molinari, N.; Pouzeratte, Y.; Verzilli, D.; Chanques, G.; Jung, B.; Futier, E.; Perrigault, P.F.; Colson, P.; Capdevila, X.; Jaber, S. Difficult intubation in obese patients: incidence, risk factors, and complications in the operating theatre and in intensive care units. Br J Anaesth. 2015, 114, 297–306. [Google Scholar] [CrossRef]
- Wang, T.; Sun, S.; Huang, S. The association of body mass index with difficult tracheal intubation management by direct laryngoscopy: a meta-analysis. BMC Anesthesiol. 2018, Jun 30;18(1):79. [CrossRef]
- Holmberg, T.J.; Bowman, S.M.; Warner, K.J.; Vavilala, M.S.; Bulger, E.M.; Copass, M.K.; Sharar, S.R. The association between obesity and difficult prehospital tracheal intubation. Anesth Analg. 2011, 112, 1132–1138. [Google Scholar] [CrossRef] [PubMed]
- Yakushiji, H.; Goto, T.; Shirasaka, W.; Hagiwara, Y.; Watase, H.; Okamoto, H.; Hasegawa, K.; Japanese Emergency Medicine Network investigators. Associations of obesity with tracheal intubation success on first attempt and adverse events in the emergency department: An analysis of the multicenter prospective observational study in Japan. PLoS One. 2018, Apr 19;13(4):e0195938. [CrossRef]
- Saasouh, W.; Laffey, K.; Turan, A.; Avitsian, R.; Zura, A.; You, J.; Zimmerman, N.M.; Szarpak, L.; Sessler, D.I.; Ruetzler, K. Degree of obesity is not associated with more than one intubation attempt: a large centre experience. Br J Anaesth. 2018, 120, 1110–1116. [Google Scholar] [CrossRef] [PubMed]
- Moon, T.S.; Fox, P.E.; Somasundaram, A.; Minhajuddin, A.; Gonzales, M.X.; Pak, T.J.; Ogunnaike, B. The influence of morbid obesity on difficult intubation and difficult mask ventilation. J Anesth. 2019, 33, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Brodsky, J.B.; Lemmens, H.J.; Brock-Utne, J.G.; Vierra, M.; Saidman, L.J. Morbid obesity and tracheal intubation. Anesth Analg. 2002, 94, 732–736. [Google Scholar] [CrossRef] [PubMed]
- Riad, W.; Vaez, M.N.; Raveendran, R.; Tam, A.D.; Quereshy, F.A.; Chung, F.; Wong, D.T. Neck circumference as a predictor of difficult intubation and difficult mask ventilation in morbidly obese patients: A prospective observational study. Eur J Anaesthesiol. 2016, 33, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Ezri, T.; Gewürtz, G.; Sessler, D.I.; Medalion, B.; Szmuk, P.; Hagberg, C.; Susmallian, S. Prediction of difficult laryngoscopy in obese patients by ultrasound quantification of anterior neck soft tissue. Anaesthesia. 2003, 58, 1111–1114. [Google Scholar] [CrossRef] [PubMed]
- Prathep, S.; Jitpakdee, W.; Woraathasin, W.; Oofuvong, M. Predicting difficult laryngoscopy in morbidly obese Thai patients by ultrasound measurement of distance from skin to epiglottis: a prospective observational study. BMC Anesthesiol. 2022, May 14;22(1):145. [CrossRef]
- Marrel, J.; Blanc, C.; Frascarolo, P.; Magnusson, L. Videolaryngoscopy improves intubation condition in morbidly obese patients. Eur J Anaesthesiol. 2007, 24, 1045–1049. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, R.; Galway, U.; You, J.; Kurz, A.; Sessler, D.I.; Doyle, D.J. A randomized comparison between the Pentax AWS video laryngoscope and the Macintosh laryngoscope in morbidly obese patients. Anesth Analg. 2011, 113, 1082–1087. [Google Scholar] [CrossRef]
- Ranieri, D. Jr.; Filho, S.M.; Batista, S.; do Nascimento, P. Jr. Comparison of Macintosh and Airtraq™ laryngoscopes in obese patients placed in the ramped position. Anaesthesia. 2012, 67, 980–985. [Google Scholar] [CrossRef]
- El Sharkawy, O.; Ibrahim, S. A comparative study on tracheal intubation using Airtraq laryngoscope versus Macintosh laryngoscope in morbidly obese patients. Menoufia Med. J. 2014, 27, 169–173. [Google Scholar] [CrossRef]
- Yumul, R.; Elvir-Lazo, O.L.; White, P.F.; Sloninsky, A.; Kaplan, M.; Kariger, R.; Naruse, R.; Parker, N.; Pham, C.; Zhang, X.; Wender, R.H. Comparison of three video laryngoscopy devices to direct laryngoscopy for intubating obese patients: a randomized controlled trial. J Clin Anesth. 2016, 31, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Ander, F.; Magnuson, A.; Berggren, L.; Ahlstrand, R.; de Leon, A. Time-to-intubation in obese patients. A randomized study comparing direct laryngoscopy and videolaryngoscopy in experienced anesthetists. Minerva Anestesiol. 2017, 83, 906–913. [Google Scholar] [CrossRef] [PubMed]
- Castillo-Monzón, C.G.; Marroquín-Valz, H.A.; Fernández-Villacañas-Marín, M.; Moreno-Cascales, M.; García-Rojo, B.; Candia-Arana, C.A. Comparison of the macintosh and airtraq laryngoscopes in morbidly obese patients: a randomized and prospective study. J Clin Anesth. 2017, 36, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Nandakumar, K.P.; Bhalla, A.P.; Pandey, R.K.; Baidya, D.K.; Subramaniam, R.; Kashyap, L. Comparison of Macintosh, McCoy, and Glidescope video laryngoscope for intubation in morbidly obese patients: Randomized controlled trial. Saudi J Anaesth. 2018, 12, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Ruetzler, K.; Rivas, E.; Cohen, B.; Mosteller, L.; Martin, A.; Keebler, A.; Maheshwari, K.; Steckner, K.; Wang, M.; Praveen, C.; Khanna, S.; Makarova, N.; Sessler, D.I.; Turan, A. McGrath video laryngoscope versus Macintosh direct laryngoscopy for intubation of morbidly obese patients: A randomized trial. Anesth Analg. 2020, 131, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Çakir, M.; Özyurt, E. Comparison of direct laryngoscope and McGrath videolaryngoscope in terms of glottic view and hemodynamics in bariatric surgery. Turk J Med Sci. 2020, 50, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, H.; Minville, V.; Delanoue, K.; Mazerolles, M.; Concina, D.; Fourcade, O. The importance of increased neck circumference to intubation difficulties in obese patients. Anesth Analg. 2008, 106, 1132–1136. [Google Scholar] [CrossRef] [PubMed]
- Uribe, A.A.; Zvara, D.A.; Puente, E.G.; Otey, A.J.; Zhang, J.; Bergese, S.D. BMI as a predictor for potential difficult tracheal intubation in males. Front Med (Lausanne). 2015, Jun 4;2:38. [CrossRef]
- Özdilek, A.; Beyoglu, C.A.; Erbabacan, Ş.E.; Ekici, B.; Altındaş, F.; Vehid, S.; Köksal, G.M. Correlation of neck circumference with difficult mask ventilation and difficult laryngoscopy in morbidly obese patients: an observational study. Obes Surg. 2018, 28, 2860–2867. [Google Scholar] [CrossRef] [PubMed]
- Yadav, N.K.; Rudingwa, P.; Mishra, S.K.; Pannerselvam, S. Ultrasound measurement of anterior neck soft tissue and tongue thickness to predict difficult laryngoscopy - An observational analytical study. Indian J Anaesth. 2019, 63, 629–634. [Google Scholar] [CrossRef]
- Andersen, L.H.; Rovsing, L.; Olsen, K.S. GlideScope videolaryngoscope vs. Macintosh direct laryngoscope for intubation of morbidly obese patients: a randomized trial. Acta Anaesthesiol Scand. 2011, 55, 1090–1097. [Google Scholar] [CrossRef]
- Hoshijima, H.; Denawa, Y.; Tominaga, A.; Nakamura, C.; Shiga, T.; Nagasaka, H. Videolaryngoscope versus Macintosh laryngoscope for tracheal intubation in adults with obesity: A systematic review and meta-analysis. J Clin Anesth. 2018, 44, 69–75. [Google Scholar] [CrossRef]
- Evrin, T.; Szarpak, L.; Katipoglu, B.; Mishyna, N.; Kockan, B.S.; Ruetzler, K.; Schläpfer, M. Video-assisted versus macintosh direct laryngoscopy for intubation of obese patients: a meta-analysis of randomized controlled trials. Disaster Emerg Med J. 2022, 7, 30–40. [Google Scholar] [CrossRef]
- Maassen, R.; Lee, R.; Hermans, B.; Marcus, M.; van Zundert, A. A comparison of three videolaryngoscopes: the Macintosh laryngoscope blade reduces, but does not replace, routine stylet use for intubation in morbidly obese patients. Anesth Analg. 2009, 109, 1560–1565. [Google Scholar] [CrossRef] [PubMed]
- Zoremba, M.; Aust, H.; Eberhart, L.; Braunecker, S.; Wulf, H. Comparison between intubation and the laryngeal mask airway in moderately obese adults. Acta Anaesthesiol Scand. 2009, 53, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Dhonneur, G.; Ndoko, S.K.; Yavchitz, A.; Foucrier, A.; Fessenmeyer, C.; Pollian, C.; Combes, X.; Tual, L. Tracheal intubation of morbidly obese patients: LMA CTrachTMvs direct laryngoscopy. Br J Anaesth. 2006, 97, 742–745. [Google Scholar] [CrossRef] [PubMed]
- Yousef, G.T.; Abdalgalil, D.A.; Ibrahim, T.H. Orotracheal intubation of morbidly obese patients, comparison of GlideScope® video laryngoscope and the LMA CTrach™ with direct laryngoscopy. Anesth Essays Res. 2012, 6, 174–179. [Google Scholar] [CrossRef]
- Gaszynski, T. TotalTrack video intubating laryngeal mask in super-obese patients - series of cases. Ther Clin Risk Manag. 2016, 12, 335–338. [Google Scholar] [CrossRef] [PubMed]
- Frappier, J.; Guenoun, T.; Journois, D.; Philippe, H.; Aka, E.; Cadi, P.; Silleran-Chassany, J.; Safran, D. Airway management using the intubating laryngeal mask airway for the morbidly obese patient. Anesth Analg. 2003, 96, 1510–1515. [Google Scholar] [CrossRef] [PubMed]
- Combes, X.; Sauvat, S.; Leroux, B.; Dumerat, M.; Sherrer, E.; Motamed, C.; Brain, A.; D'Honneur, G. Intubating laryngeal mask airway in morbidly obese and lean patients: a comparative study. Anesthesiology. 2005, 102, 1106–1109. [Google Scholar] [CrossRef]
- Herman, A.G.; Mahla, M.E. Awake intubating laryngeal mask airway placement in a morbidly obese patient with ankylosing spondylitis and unstable thoracic spine. J Clin Anesth. 2016, 32, 62–64. [Google Scholar] [CrossRef]
- Gaszyński, T. The visualization of glottis during intubation's efforts in super obese patients: a comparison of total track video intubating laryngeal mask and McGrath MAC videolaryngoscope. J Clin Monit Comput. 2017, 31, 1329–1332. [Google Scholar] [CrossRef] [PubMed]
- Turna, C.K.; Arslan, Z.I.; Alparslan, V.; Okyay, K.; Solak, M. Comparison of channelled videolaryngoscope and intubating laryngeal mask airway for tracheal intubation in obese patients: a randomised clinical trial. Braz J Anesthesiol. 2020, 70, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Cook, T.M. Difficult airway in an obese patient managed with the ProSeal laryngeal mask airway. Eur J Anaesthesiol. 2005, 22, 241–243. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Zhang, Y.; Hu, T.; Li, X.; Fu, Q. Anesthesia management of morbid obesity and ankylosing spondylitis with a difficult airway: a case report. Am J Transl Res. 2022, 14, 4860–4863. [Google Scholar] [PubMed]
- Uakritdathikarn, T.; Asampinawat, T.; Wanasuwannakul, T.; Yoosamran, B. Awake intubation with Airtraq laryngoscope in a morbidly obese patient. J Med Assoc Thai. 2008, 91, 564–567. [Google Scholar] [PubMed]
- Moore, A.R.; Schricker, T.; Court, O. Awake videolaryngoscopy-assisted tracheal intubation of the morbidly obese. Anaesthesia. 2012, 67, 232–235. [Google Scholar] [CrossRef] [PubMed]
- Ndoko, S.K.; Amathieu, R.; Tual, L.; Polliand, C.; Kamoun, W.; El Housseini, L.; Champault, G.; Dhonneur, G. Tracheal intubation of morbidly obese patients: a randomized trial comparing performance of Macintosh and Airtraq laryngoscopes. Br J Anaesth. 2008, 100, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Dhonneur, G.; Abdi, W.; Ndoko, S.K.; Amathieu, R.; Risk, N.; El Housseini, L.; Polliand, C.; Champault, G.; Combes, X.; Tual, L. Video-assisted versus conventional tracheal intubation in morbidly obese patients. Obes Surg. 2009, 19, 1096–1101. [Google Scholar] [CrossRef] [PubMed]
- Carron, M.; Ieppariello, G.; Linassi, F. Videolaryngoscopy versus direct laryngoscopy for tracheal intubation in obese adults: A meta-analysis. J Clin Anesth. 2021, 71, 110216. [Google Scholar] [CrossRef]
- King, M.R.; Jagannathan, N. Should videolaryngoscopy be the standard of care for routine tracheal intubation in obese adults? J Clin Anesth. 2018, 45, 33–34. [Google Scholar] [CrossRef]
- Luk, H.N.; Qu, J.Z. Styletubation versus laryngoscopy: A new paradigm for routine tracheal intubation. Surgeries. 2024, 5, 135–161. [Google Scholar] [CrossRef]
- Tsay, P.J.; Yang, C.P.; Luk, H.N.; Qu, J.Z.; Shikani, A. Video-assisted intubating stylet technique for difficult intubation: A case series report. Healthcare (Basel). 2022, Apr 15;10(4):741. [CrossRef]
- Shih, T.L.; Koay, K.P.; Hu, C.Y.; Luk, H.N.; Qu, J.Z.; Shikani, A. The use of the Shikani video-assisted intubating stylet technique in patients with restricted neck mobility. Healthcare (Basel). 2022, Sep 4;10(9):1688. [CrossRef]
- Yang, C.P.; Luk, H.N.; Qu, J.Z.; Shikani, A. The use of a video-assisted intubating stylet technique in a critically ill and contagious COVID-19 patient. Healthcare (Basel). 2022, Feb 18;10(2):388. [CrossRef]
- Huang, C.H.; Su, I.M.; Jhuang, B.J.; Luk, H.N.; Qu, J.Z.; Shikani, A. Video-assisted stylet intubation with a plastic sheet barrier, a safe and simple technique for tracheal intubation of COVID-19 patients. Healthcare (Basel). 2022, Jun 14;10(6):1105. [CrossRef]
- Wu, B.G.; Luk, H.N.; Qu, J.Z.; Shikani, A. Styletubation in bariatric surgery: A case report. Healthcare (Basel). 2023, Aug 10;11(16):2256. [CrossRef]
- Foulds, L.T.; McGuire, B.E.; Shippey, B.J. A randomised cross-over trial comparing the McGrath(®) Series 5 videolaryngoscope with the Macintosh laryngoscope in patients with cervical spine immobilisation. Anaesthesia. 2016, 71, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Suppan, L.; Tramèr, M.R.; Niquille, M.; Grosgurin, O.; Marti, C. Alternative intubation techniques vs Macintosh laryngoscopy in patients with cervical spine immobilization: systematic review and meta-analysis of randomized controlled trials. Br J Anaesth. 2016, 116, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Singleton, B.N.; Morris, F.K.; Yet, B.; Buggy, D.J.; Perkins, Z.B. Effectiveness of intubation devices in patients with cervical spine immobilisation: a systematic review and network meta-analysis. Br J Anaesth. 2021, 126, 1055–1066. [Google Scholar] [CrossRef] [PubMed]
- Paik, H.; Park, H.P. Randomized crossover trial comparing cervical spine motion during tracheal intubation with a Macintosh laryngoscope versus a C-MAC D-blade videolaryngoscope in a simulated immobilized cervical spine. BMC Anesthesiol. 2020, Aug 15;20(1):201. [CrossRef]
- Maharaj, C.H.; Costello, J.F.; Higgins, B.D.; Harte, B.H.; Laffey, J.G. Learning and performance of tracheal intubation by novice personnel: a comparison of the Airtraq and Macintosh laryngoscope. Anaesthesia. 2006, 61, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Ray, D.C.; Billington, C.; Kearns, P.K.; Kirkbride, R.; Mackintosh, K.; Reeve, C.S.; Robinson, N.; Stewart, C.J.; Trudeau, T. A comparison of McGrath and Macintosh laryngoscopes in novice users: a manikin study. Anaesthesia. 2009, 64, 1207–1210. [Google Scholar] [CrossRef] [PubMed]
- Ambrosio, A.; Pfannenstiel, T.; Bach, K.; Cornelissen, C.; Gaconnet, C.; Brigger, M.T. Difficult airway management for novice physicians: a randomized trial comparing direct and video-assisted laryngoscopy. Otolaryngol Head Neck Surg. 2014, 150, 775–778. [Google Scholar] [CrossRef]
- Choi, J.W.; Kim, J.A.; Jung, H.J.; Kim, W.H. Tracheal Intubation with a McGrath® Series 5 Video Laryngoscope by Novice Personnel in a Cervical-immobilized Manikin. J Emerg Med. 2016, 50, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Eismann, H.; Sieg, L.; Etti, N.; Friedrich, L.; Schröter, C.; Mommsen, P.; Krettek, C.; Zeckey, C. Improved success rates using videolaryngoscopy in unexperienced users: a randomized crossover study in airway manikins. Eur J Med Res. 2017, Aug 10;22(1):27. [CrossRef]
- Yong, S.A.; Chaou, C.H.; Yu, S.R.; Kuan, J.T.; Lin, C.C.; Liu, H.P.; Chiu, T.F. Video assisted laryngoscope facilitates intubation skill learning in the emergency department. J Acute Med. 2020, 10, 60–69. [Google Scholar] [CrossRef]
- Nalubola, S.; Jin, E.; Drugge, E.D.; Weber, G.; Abramowicz, A.E. Video versus direct laryngoscopy in novice intubators: A systematic review and meta-analysis. Cureus. 2022, Sep 25;14(9):e29578. [CrossRef]
- Webb, A.; Kolawole, H.; Leong, S.; Loughnan, T.E.; Crofts, T.; Bowden, C. Comparison of the Bonfils and Levitan optical stylets for tracheal intubation: a clinical study. Anaesth Intensive Care. 2011, 39, 1093–1097. [Google Scholar] [CrossRef]
- Kleine-Brueggeney, M.; Greif, R.; Urwyler, N.; Wirthmüller, B.; Theiler, L. The performance of rigid scopes for tracheal intubation: a randomised, controlled trial in patients with a simulated difficult airway. Anaesthesia. 2016, 71, 1456–1463. [Google Scholar] [CrossRef]
- Theiler, L.; Greif, R.; Bütikofer, L.; Arheart, K.; Kleine-Brueggeney, M. The skill of tracheal intubation with rigid scopes-a randomised controlled trial comparing learning curves in 740 intubations. BMC Anesthesiol. 2020, Oct 16;20(1):263. [CrossRef]
- Tseng, K.Y.; Chau, S.W.; Su, M.P.; Shih, C.K.; Lu, I.C.; Cheng, K.I. A comparison of Trachway intubating stylet and Airway Scope for tracheal intubation by novice operators: a manikin study. Kaohsiung J Med Sci. 2012, 28, 448–451. [Google Scholar] [CrossRef]
- Hung, K.C.; Tan, P.H.; Lin, V.C.; Wang, H.K.; Chen, H.S. A comparison of the Trachway intubating stylet and the Macintosh laryngoscope in tracheal intubation: a manikin study. J Anesth. 2013, 27, 205–210. [Google Scholar] [CrossRef]
- Ong, J.; Lee, C.L.; Huang, S.J.; Shyr, M.H. Comparison between the Trachway video intubating stylet and Macintosh laryngoscope in four simulated difficult tracheal intubations: A manikin study. Ci Ji Yi Xue Za Zhi. 2016, 28, 109–112. [Google Scholar] [CrossRef]
- Park, J.W.; An, S.; Park, S.; Nahm, F.S.; Han, S.H.; Kim, J.H. Comparison of a new video intubation stylet and McGrath® MAC video laryngoscope for intubation in an airway manikin with normal airway and cervical spine immobilization scenarios by novice personnel: A randomized crossover study. Biomed Res Int. 2021, Nov 10;2021:4288367. [CrossRef]
- Chen, Y.Y.; Lin, J.C.; Tsai, M.J.; Cheng, K.Y. Retromolar intubation with video intubating stylet in difficult airway: A randomized crossover manikin study. Am J Emerg Med. 2022, 54, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Kelly, F.E.; Cook, T.M. Seeing is believing: getting the best out of videolaryngoscopy. Br J Anaesth. 2016, 117, Suppl 1:i9–i13. [Google Scholar] [CrossRef]
- Bathory, I.; Granges, J.C.; Frascarolo, P.; Magnusson, L. Evaluation of the Video Intubation Unit in morbid obese patients. Acta Anaesthesiol Scand. 2010, 54, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Prekker, M.E.; Driver, B.E.; Trent, S.A.; Resnick-Ault, D.; Seitz, K.P.; Russell, D.W.; Gaillard, J.P.; Latimer, A.J.; Ghamande, S.A.; Gibbs, K.W.; Vonderhaar, D.J.; Whitson, M.R.; Barnes, C.R.; Walco, J.P.; Douglas, I.S.; Krishnamoorthy, V.; Dagan, A.; Bastman, J.J.; Lloyd, B.D.; Gandotra, S.; Goranson, J.K.; Mitchell, S.H.; White, H.D.; Palakshappa, J.A.; Espinera, A.; Page, D.B.; Joffe, A.; Hansen, S.J.; Hughes, C.G.; George, T.; Herbert, J.T.; Shapiro, N.I.; Schauer, S.G.; Long, B.J.; Imhoff, B.; Wang, L.; Rhoads, J.P.; Womack, K.N.; Janz, D.R.; Self, W.H.; Rice, T.W.; Ginde, A.A.; Casey, J.D.; Semler, M.W. DEVICE investigators and the pragmatic critical care research group. Video versus direct laryngoscopy for tracheal intubation of critically ill adults. N Engl J Med. 2023, 389, 418–429. [Google Scholar] [CrossRef]
- Maassen, R.; Lee, R.; van Zundert, A.; Cooper, R. The videolaryngoscope is less traumatic than the classic laryngoscope for a difficult airway in an obese patient. J Anesth. 2009, 23, 445–448. [Google Scholar] [CrossRef]
- Luk, H.N.; Qu, J.Z.; Shikani, A. Styletubation: The paradigmatic role of video-assisted intubating stylet technique for routine tracheal intubation. Asian J Anesthesiol. 2023, 61, 102–106. [Google Scholar] [CrossRef]
- Treki, A.A.; Straker, T. Limitations of the videolaryngoscope: An anesthetic management reality. Int Anesthesiol Clin. 2017, 55, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Thong, S.Y.; Wong, T.G. Clinical uses of the Bonfils retromolar intubation fiberscope: a review. Anesth Analg. 2012, 115, 855–866. [Google Scholar] [CrossRef] [PubMed]
- Lan, C.H.; Luk, H.N.; Qu, J.Z.; Shikani, A. An approach to improve the effectiveness of the video-assisted intubating stylet technique for tracheal intubation: A case series report. Healthcare (Basel). 2023, Mar 20;11(6):891. [CrossRef]
- Wilson, S.L.; Mantena, N.R.; Halverson, J.D. Effects of atropine, glycopyrrolate, and cimetidine on gastric secretions in morbidly obese patients. Anesth Analg. 1981, 60, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Halliday, T.A.; Sundqvist, J.; Hultin, M.; Walldén, J. Post-operative nausea and vomiting in bariatric surgery patients: an observational study. Acta Anaesthesiol Scand. 2017, 61, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Van Zundert, A.A.; Pieters, B.M. Combined technique using videolaryngoscopy and Bonfils for a difficult airway intubation. Br J Anaesth. 2012, 108, 327–328. [Google Scholar] [CrossRef] [PubMed]
- Gaszynski, T.; Pietrzyk, M.; Szewczyk, T.; Gaszynska, E. A comparison of performance of endotracheal intubation using the Levitan FPS optical stylet or Lary-Flex videolaryngoscope in morbidly obese patients. Scientific World J. 2014, 2014:207591. [CrossRef]
- Chiu, W.C.; Wu, Z.F.; Lai, M.F.; Lai, H.C. Combination use of laryngoscope, jaw thrust, and trachway for improving difficult tracheal intubation in obese. J Med Sci. 2022, 42, 197–198. [Google Scholar] [CrossRef]
- Jhuang, B.J.; Luk, H.N.; Qu, J.Z.; Shikani, A. Video-twin technique for airway management, combining video-intubating stylet with videolaryngoscope: A case series report and review of the literature. Healthcare (Basel). 2022, Oct 30;10(11):2175. [CrossRef]
- Yang, M.; Kim, J.A.; Ahn, H.J.; Choi, J.W.; Kim, D.K.; Cho, E.A. Double-lumen tube tracheal intubation using a rigid Video Stylet: a randomized controlled comparison with the Macintosh laryngoscope. Br J Anaesth. 2013, 111, 990–995. [Google Scholar] [CrossRef]
- Zhang, T.; Zhao, K.Y.; Zhang, P.; Li, R.H. Comparison of video laryngoscope, video stylet, and flexible videoscope for transoral endotracheal intubation in patients with difficult airways: a randomized, parallel-group study. Trials. 2023, Sep 21;24(1):599. [CrossRef] [PubMed] [PubMed Central]
- Gu, Y.; Zhou, Q.; Zhou, H.; Liu, M.; Feng, D.; Wei, J.; Min, K.; Zhu, W.; Chen, Y.; Lv, X. A randomized study of rigid video stylet versus Macintosh laryngoscope for double-lumen endobronchial tube intubation assistance in thoracoscopic pulmonary surgery. J Clin Med. 2023, Jan 9;12(2):540. [CrossRef]
Figure 1.
The styletubation (video intubating stylet technique). (A) The video intubating stylet-endotracheal tube unit (upper panel) and an inside-out clear view acquired from the camera at the tip of the stylet (lower panel). An example of two-person model to operate the styletubation. The airway assistant either stands should-to-shoulder with the operator (B) or face-to-face to the operator (C). The assistant ensures effective mouth-opening and jaw-thrust on the obese patient.
Figure 1.
The styletubation (video intubating stylet technique). (A) The video intubating stylet-endotracheal tube unit (upper panel) and an inside-out clear view acquired from the camera at the tip of the stylet (lower panel). An example of two-person model to operate the styletubation. The airway assistant either stands should-to-shoulder with the operator (B) or face-to-face to the operator (C). The assistant ensures effective mouth-opening and jaw-thrust on the obese patient.
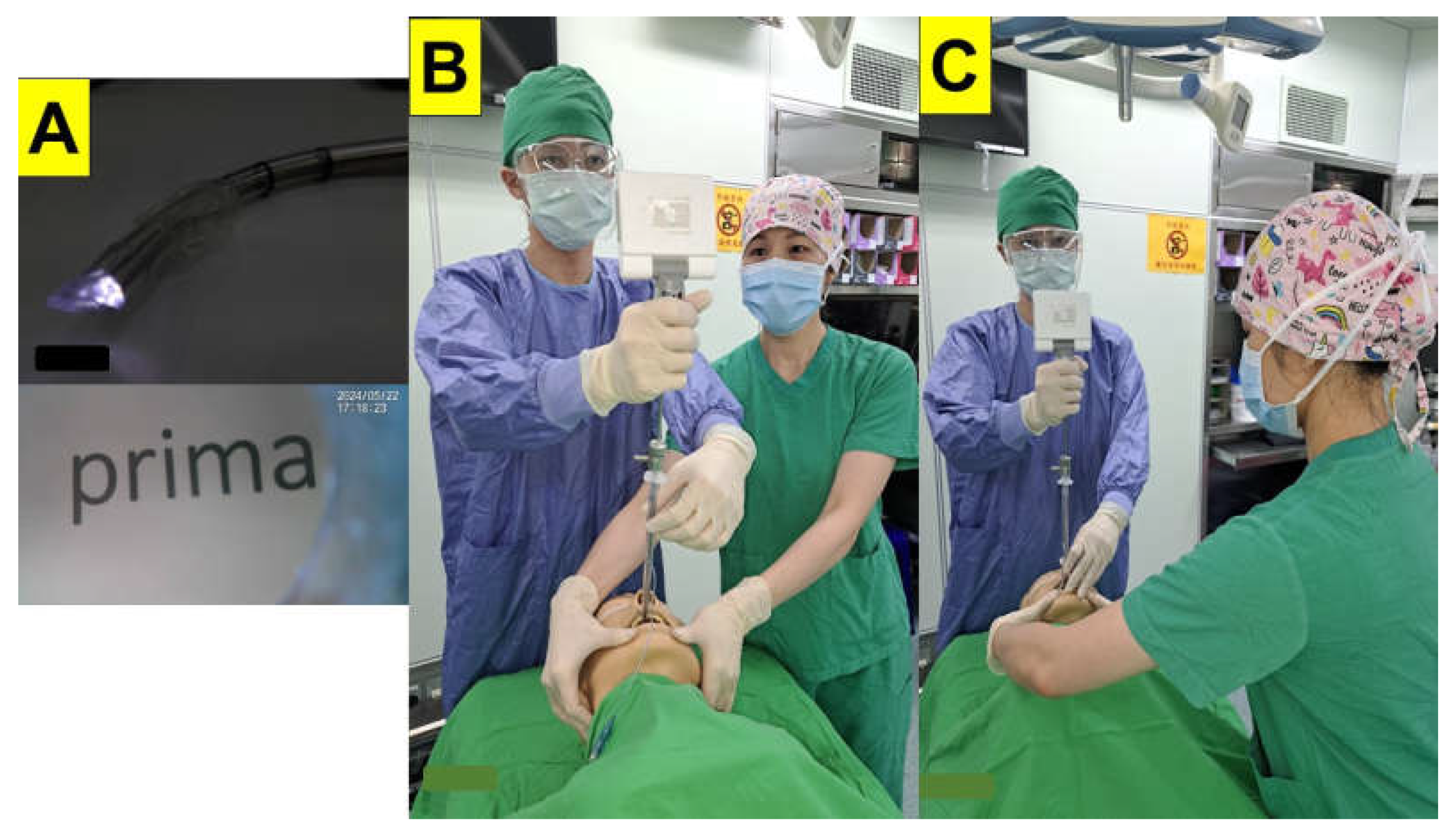
Figure 2.
An example of obese patient with BMI 34.8 kg/m2 (Case-20, Table 4) undergoing bariatric surgery. Pre-operative airway evaluation included mouth-opening (A) and upper-lip bite test (B). (C) Mask ventilation with jaw-thrust. (D). Clear visualization of glottis (E) and trachea (F). Time to intubate: 5 s and succeeded in the first attempt. (See Video S19 in the Supplementary Materials).
Figure 2.
An example of obese patient with BMI 34.8 kg/m2 (Case-20, Table 4) undergoing bariatric surgery. Pre-operative airway evaluation included mouth-opening (A) and upper-lip bite test (B). (C) Mask ventilation with jaw-thrust. (D). Clear visualization of glottis (E) and trachea (F). Time to intubate: 5 s and succeeded in the first attempt. (See Video S19 in the Supplementary Materials).
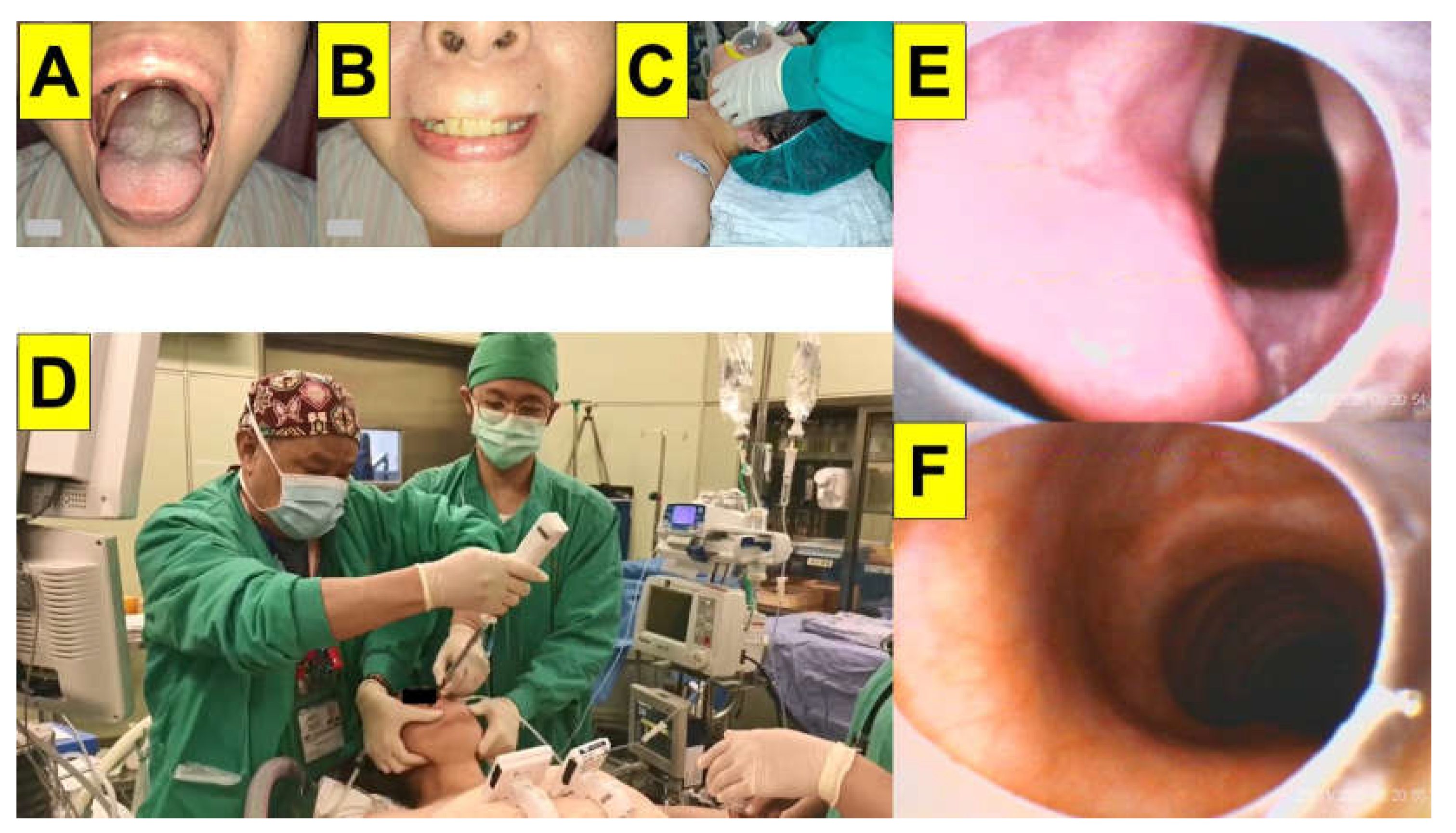
Figure 3.
An example of obese patient with BMI 103.0 kg/m2 (Case-1, Table 4) undergoing bariatric surgery. (A) Pre-operative airway evaluation included mouth-opening. (B) Excessive fat tissue deposition around the neck. (C) Reverse Trendelenburg position. (D) Styletubation with two-person model. (E) Pharyngo-laryngeal view. (F) Close-up view of the omega-shaped epiglottis. Time to intubate: 12 s and succeeded in the first attempt. (See Video S1 in the Supplementary Materials).
Figure 3.
An example of obese patient with BMI 103.0 kg/m2 (Case-1, Table 4) undergoing bariatric surgery. (A) Pre-operative airway evaluation included mouth-opening. (B) Excessive fat tissue deposition around the neck. (C) Reverse Trendelenburg position. (D) Styletubation with two-person model. (E) Pharyngo-laryngeal view. (F) Close-up view of the omega-shaped epiglottis. Time to intubate: 12 s and succeeded in the first attempt. (See Video S1 in the Supplementary Materials).
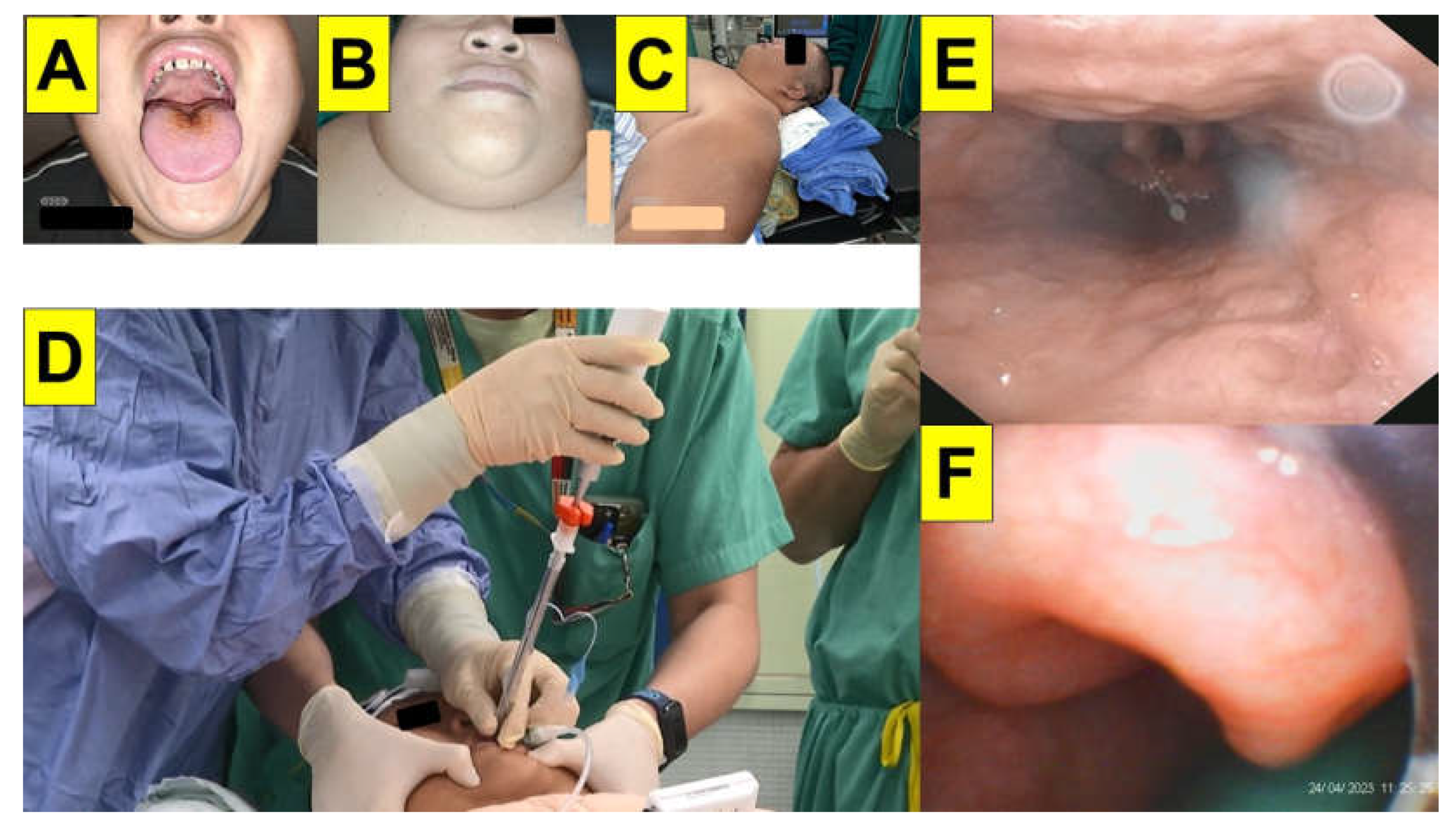
Figure 4.
Examples of narrowing and collapse of airway in obese patients undergoing bariatric surgery. (A) BMI: 51.1 (Case-6, Table 4). Oro-pharyngeal laterally narrowing with a concave epiglottis is prominent. (B) BMI: 48.0 (Case-10, Table 4) A suction-airway device was placed under the epiglottis in advance. (C) BMI: 54.0 (Case-4, Table 4). (D) BMI: 63.1 (Case-2, Table 4). Plica vocalis was observed both in (C) and (D). (See Video S6, S10, S4, and S2, respectively in the Supplementary Materials).
Figure 4.
Examples of narrowing and collapse of airway in obese patients undergoing bariatric surgery. (A) BMI: 51.1 (Case-6, Table 4). Oro-pharyngeal laterally narrowing with a concave epiglottis is prominent. (B) BMI: 48.0 (Case-10, Table 4) A suction-airway device was placed under the epiglottis in advance. (C) BMI: 54.0 (Case-4, Table 4). (D) BMI: 63.1 (Case-2, Table 4). Plica vocalis was observed both in (C) and (D). (See Video S6, S10, S4, and S2, respectively in the Supplementary Materials).
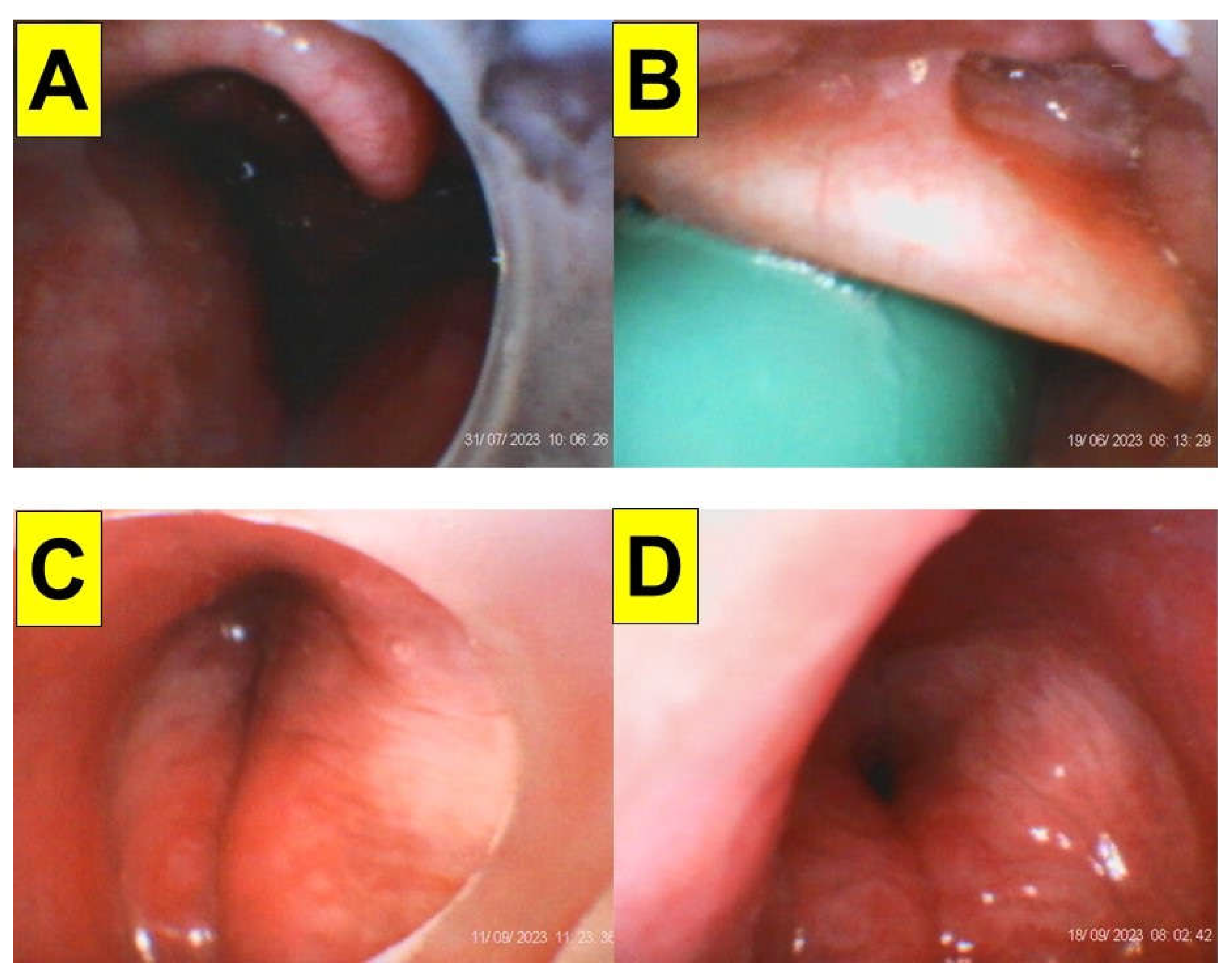
Figure 5.
An obese patient with restricted cervical spine mobility undergoing bariatric surgery. BMI 45.4 (Case-12, Table 4). (A) Mouth-opening. (B) Compromised upper-lip bite test. (C) Stiff neck with limited extension. (D) Prior treatment with cervical spine fixation shown in X-ray. (E) An omega-shaped epiglottis obscured by saliva. (F) Glottis visualization. (See Video S12 in the Supplementary Materials).
Figure 5.
An obese patient with restricted cervical spine mobility undergoing bariatric surgery. BMI 45.4 (Case-12, Table 4). (A) Mouth-opening. (B) Compromised upper-lip bite test. (C) Stiff neck with limited extension. (D) Prior treatment with cervical spine fixation shown in X-ray. (E) An omega-shaped epiglottis obscured by saliva. (F) Glottis visualization. (See Video S12 in the Supplementary Materials).
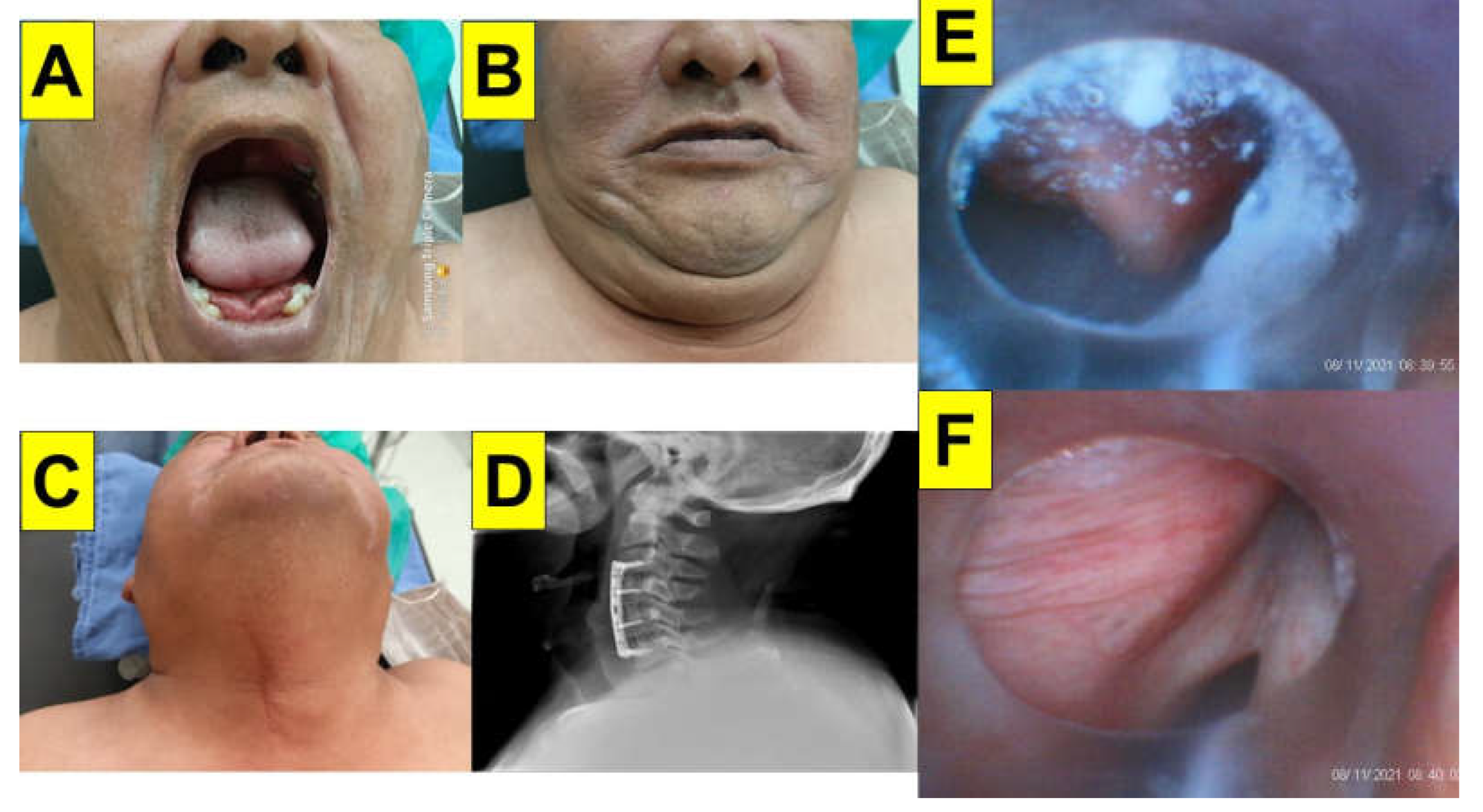
Figure 6.
The performance of styletubation by a resident anesthesiologist. BMI 47.1 (Case-11, Table 4) (A-C) The collapsed and jammed soft tissues obstructed the upper airway. (D) Glottis. (E) Vocal cords. (F) Placement of endotracheal tube into trachea. (See Video S11 in the Supplementary Materials).
Figure 6.
The performance of styletubation by a resident anesthesiologist. BMI 47.1 (Case-11, Table 4) (A-C) The collapsed and jammed soft tissues obstructed the upper airway. (D) Glottis. (E) Vocal cords. (F) Placement of endotracheal tube into trachea. (See Video S11 in the Supplementary Materials).
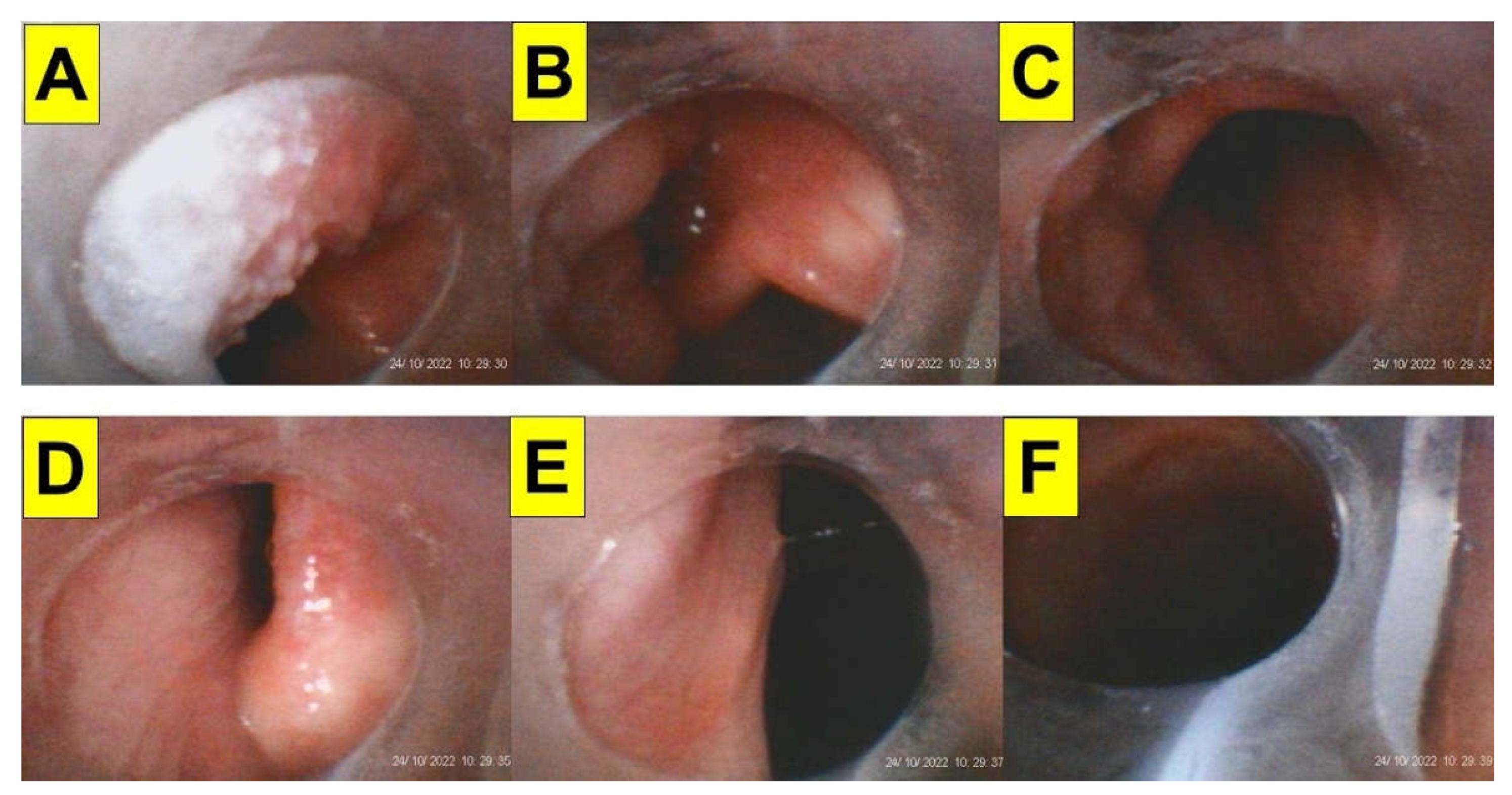
Figure 7.
Disturbance of visualization by saliva/secretions during styletubation in obese patients. (A-C) BMI 36.6 kg/m2 (Case-18, Table 4). (D-F) BMI 63.6 kg/m2, (Case-3, Table 4). (See Video S17 and Video S3 in the Supplementary Materials).
Figure 7.
Disturbance of visualization by saliva/secretions during styletubation in obese patients. (A-C) BMI 36.6 kg/m2 (Case-18, Table 4). (D-F) BMI 63.6 kg/m2, (Case-3, Table 4). (See Video S17 and Video S3 in the Supplementary Materials).
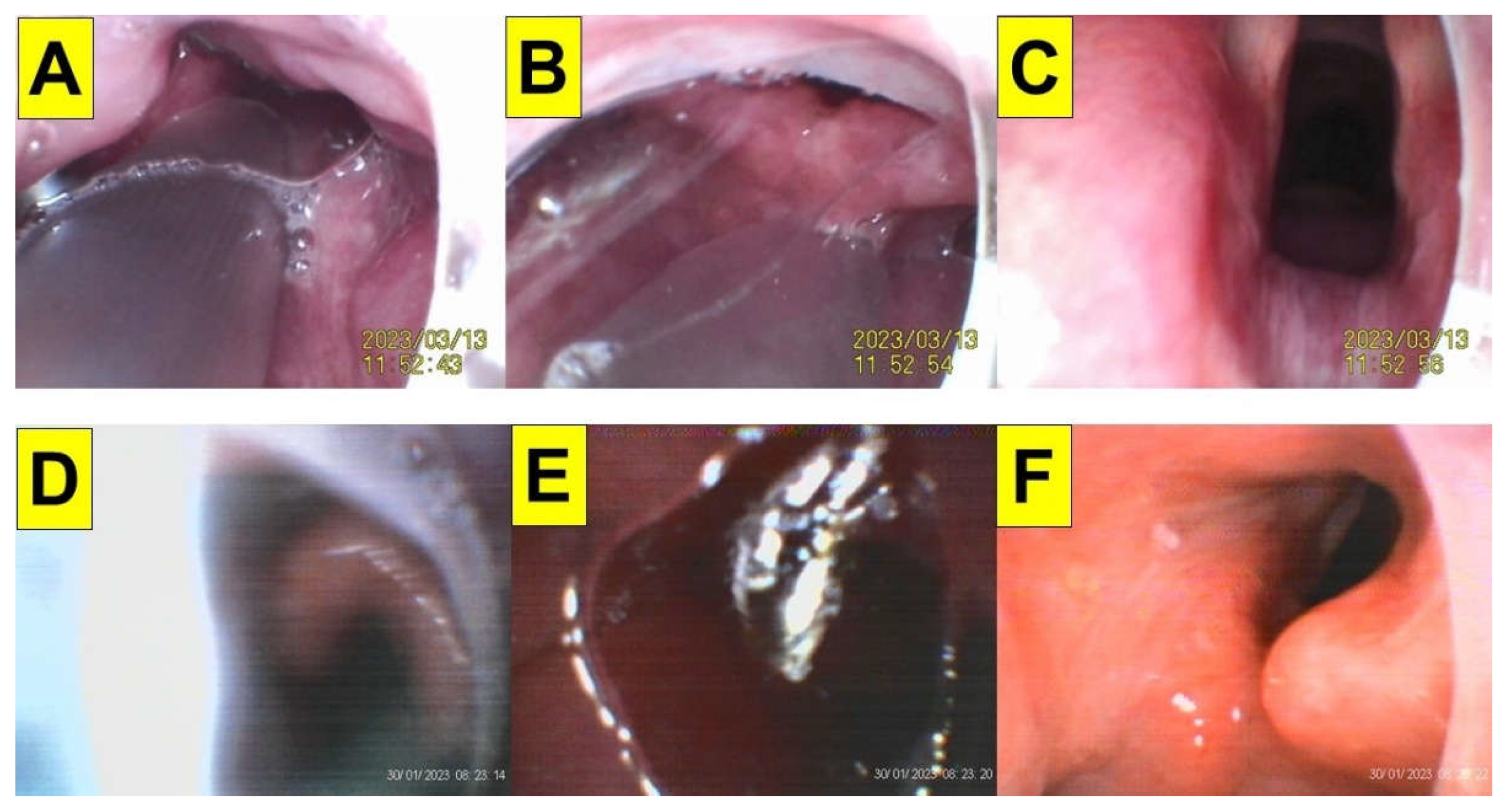
Figure 8.
An easy solution to acquire clear airway visibility during styletubation in obese patient. BMI 37.8 kg/m2 (Case-17, Table 4) (A-C) A modified airway-suction tube unit (in green color) was used in advance to clear the saliva/secretions. (D-F) Clear visualization of glottis, vocal cords and trachea. (See Video S and Video S16 in the Supplementary Materials).
Figure 8.
An easy solution to acquire clear airway visibility during styletubation in obese patient. BMI 37.8 kg/m2 (Case-17, Table 4) (A-C) A modified airway-suction tube unit (in green color) was used in advance to clear the saliva/secretions. (D-F) Clear visualization of glottis, vocal cords and trachea. (See Video S and Video S16 in the Supplementary Materials).
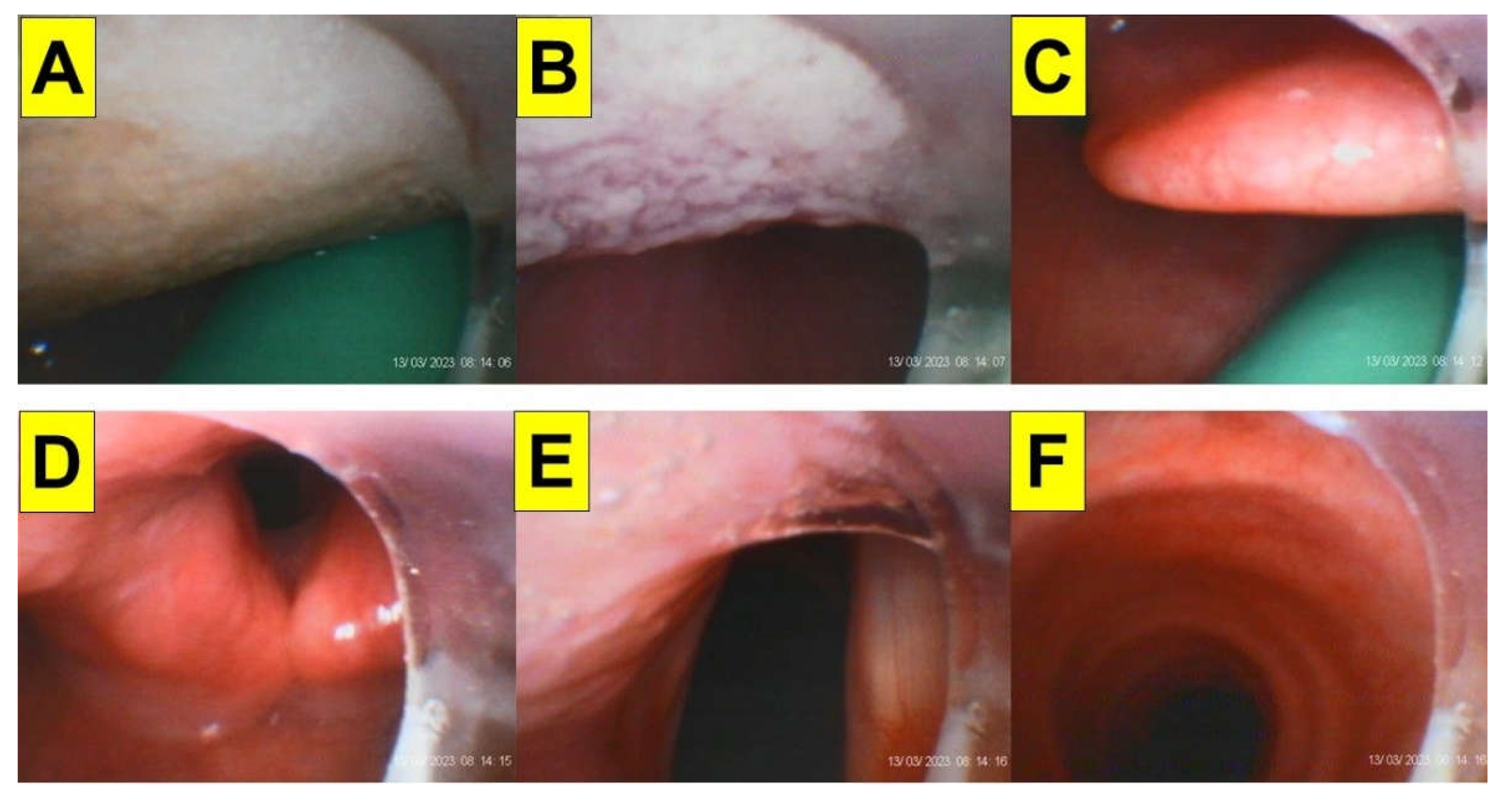
Figure 9.
Styletubation assisted by laryngoscopy in obese patient. BMI 43.9 kg/m2 (Case-14, Table 4) (A) White star denotes the VL blade in blue color. (B) An exposed glottis by laryngoscopy before styletubation set out. (C and D) Views of vocal cords and trachea from styletubation. (See Video S13 in the Supplementary Materials).
Figure 9.
Styletubation assisted by laryngoscopy in obese patient. BMI 43.9 kg/m2 (Case-14, Table 4) (A) White star denotes the VL blade in blue color. (B) An exposed glottis by laryngoscopy before styletubation set out. (C and D) Views of vocal cords and trachea from styletubation. (See Video S13 in the Supplementary Materials).
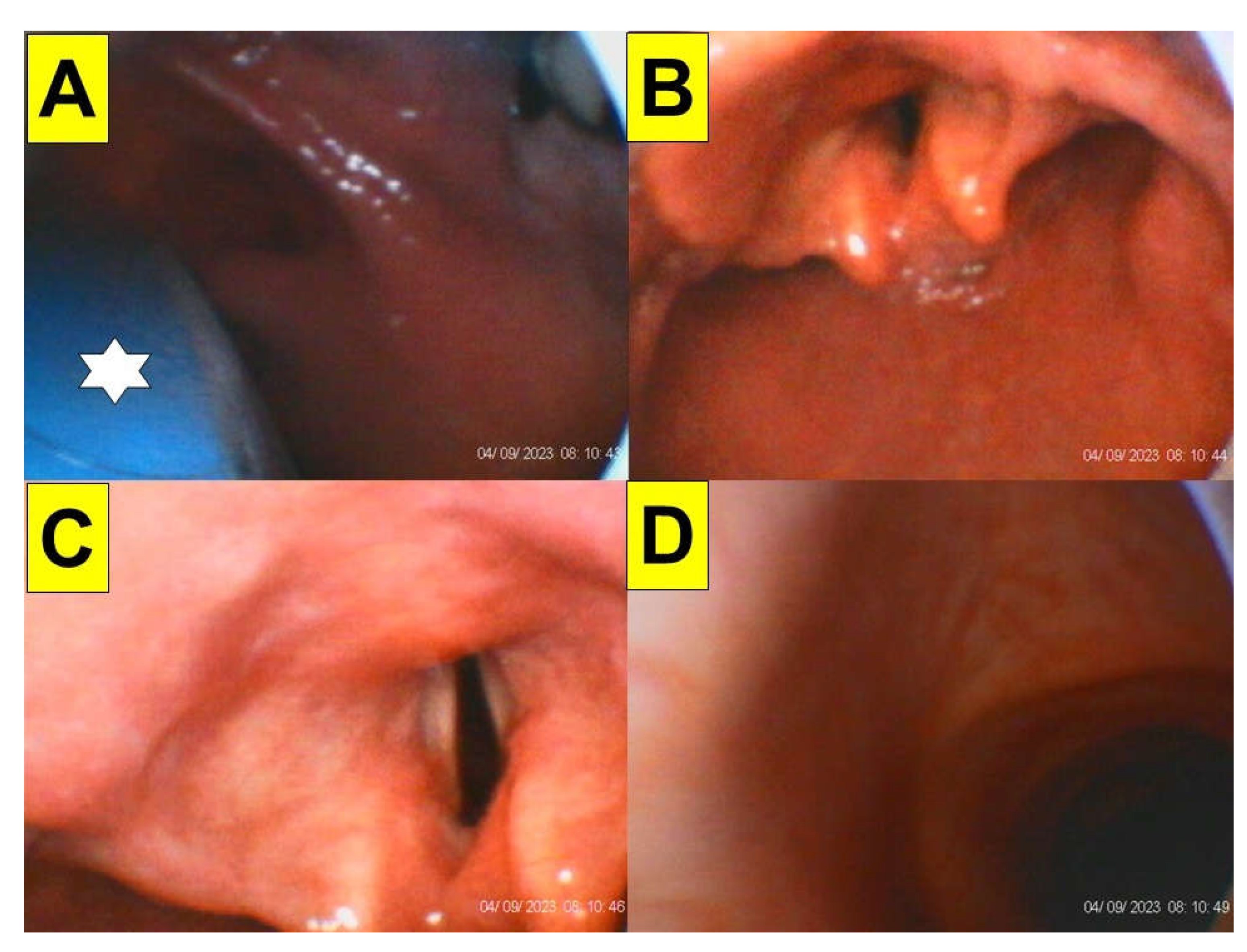

Table 1.
Predictive factors for difficult airway in obese patient population.
| Predictive Factors | References |
|---|---|
| Gender | [19,27,29,32,33,34,35,36,37,38,39,40,41] |
| Age | [27,32,33,34,35,36,37,38,39,40,41] |
| BMI | [29,31,32,33,34,35,36,37,38,39,40,41,42,43] |
| Mallampati score | [19,21,27,29,32,33,34,35,36,37,38,40,41,42,43,44,45] |
| Mouth opening (inter-incisor distance) | [32,34,35,36,38,40] |
| Poor dentition | [27,36,40] |
| Tongue thickness | [45] |
| Neck circumference | [29,30,32,34,35,36,37,38,40,42,44,45] |
| Thyro-mental distance | [27,31,32,35,36,38,40,42] |
| Sternomental distance | [31,34,40,44] |
| Neck circumference/thyro-mental distance ratio | [21] |
| Range of motion of neck | [40,44] |
| Upper lip bite test | [40,44] |
| Sleep apnea syndrome | [29,32,40] |
| Anterior neck soft tissue thickness (distance from skin to epiglottis) | [30,31,45] |
Table 2.
Comparison of oro-tracheal intubation using DL, VL, and styletubation in obese patients.
| Parameters | DL | VL | Styletubation (Table 4, n = 20) |
|---|---|---|---|
| BMI (kg/m2) | 44 [32] 43 [63] 40 [64] 41 [46] 43 [33] 43 [34] 44 [52] 41 [35] 42 [36] 47 [40] 46 [41] 47 [38] 45 [39] |
43 [32] 44 [63] 43 [64] 42 [46] 41 [33] 44 [34] 43 [52] 40 [35] 41 [36] 46 [40] 46 [41] 46 [38] 47 [39] |
38 (mean; 103 ― 34.8); 48 (median) |
| Intubation time | 93 s [32] 56 s [63] 69 s [64] 32 s [46] 26 s [33] 37 s [34] 100 s [52] 18 s [35] 43 s [36] 26 s [37] 27 s [40] 46 s [41] 22 s [38] 32 s [39] |
59 s [32] 24 s [63] 29 s [64] 48 s [46] 38 s [33] 14 s [34] 86 s [52] 12 s [35] 40 s [36] 25 s [37] 28 s [40] 57 s [41] 17 s [38] 54 s [39] |
12 s (mean; 5 s ― 22 s); 11 s (median) |
| First-attempt success rate | 80% [32] 93 [63] 92% [46] 92% [33] 84% [34] 70% [52] 90% [35] 74% [36] 87% [37] 89% [40] 91% [38] |
95% [32] 100% [63] 98% [46] 86% [33] 100% [34] 90% [52] 100% [35] 70% [36] 100% [37] 92% [40] 91% [38] |
100% |
| Failed intubation | 0% [32] 0.9% [64] 4% [46] 0% [33] 1.6% [34] 20% [52] 20% [35] 0% [36] 13% [37] 8% [40] 0% [38] |
0% [32] 0% [64] 0% [46] 10% [33] 0% [34] 0% [52] 5% [35] 0% [36] 0% [37] 3% [40] 0% [38] |
0% |
| Cormack–Lehane grade 3/4 | 15%/0% [32] 19%/2% [63] 15%/0% [64] 20%/8% [46] 22% [33] 6%/5% [34] 20%/3% [52] 40%(3) [35] 16%/19% [36] 10%/6% [40] 58% [41] |
0%/0% [32] 0%/0% [63] 0%/0% [64] 4%/0% [46] 14% [33] 0%/0% [34] 0%/0% [52] 5%(3) [35] 0%/0% [36] 5%/0% [40] 58% [41] |
NA |
| POGO | 75% [64] 57% [36] 29%/35% [POGO75%/100%] [40] |
97% [64] 91% [36] 17%/67% [POGO75%/100%] [40] |
100% |
| Increased lifting force required (%) | 40% [46] 33% [52] |
22% [46] 0% [52] |
NA |
| Subjective difficulty of intubation | More difficult [63] Similar to VL [46] 40 (0-100 scale) [33] 15% [35] 11% [40] 13% [38] 0% [39] |
Easy [63] Similar to DL [46] 52 (0-100 scale) [33] 40% [35] 6% [40] 4% [38] 7% [39] Easier than DL [52] |
Easy |
Table 3.
Use rate of styletubation technique for oro-tracheal intubation in the Department of Anesthesia, Hualien Tzuchi Medical Center, Hualien, Taiwan.
Table 3.
Use rate of styletubation technique for oro-tracheal intubation in the Department of Anesthesia, Hualien Tzuchi Medical Center, Hualien, Taiwan.
| 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | 2023 | |
|---|---|---|---|---|---|---|---|---|
| Total anesthesia number | 16077 | 17831 | 17998 | 19307 | 19721 | 19244 | 19765 | 22438 |
| GA number | 15339 | 16893 | 17497 | 18481 | 19009 | 18574 | 19061 | 22099 |
| LMA-GA number | 5544 | 5134 | 5816 | 5902 | 5863 | 5714 | 4932 | 5763 |
| ET-GA number | 5953 | 6504 | 6920 | 6966 | 7418 | 6982 | 7602 | 8329 |
| VL | 0 | 0 | 20 | 100 | 635 | 336 | 305 | 280 |
| Styletubation | 5953 | 6504 | 6900 | 6866 | 6783 | 6646 | 7297 | 8049 |
GA: general anesthesia. LMA: laryngeal mask airway. ET: endotracheal intubation. VL: videolaryngoscope.
Table 4.
Styletubation applied in 20 obese patients undergoing bariatric surgery.
| Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | Case 6 | Case 7 | Case 8 | Case 9 | Case 10 | Case 11 | Case 12 | Case 13 | Case 14 | Case 15 | Case 16 | Case 17 | Case 18 | Case 19 | Case 20 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age/Gender (years old) | 33/M | 42/M | 42/F | 49/M | 57/F | 51/F | 26/F | 45/M | 32/F | 37/F | 23/M | 56/M | 41/F | 26/M | 48/M | 56/M | 38/M | 42/M | 40/M | 58/F |
| Height (cm) | 158 | 165 | 161 | 180 | 153 | 160 | 160 | 171 | 157 | 162 | 176 | 159 | 158 | 166 | 175 | 170 | 178 | 166 | 174 | 166 |
| Weight (kg) | 258 | 172 | 165 | 175 | 120 | 131 | 130 | 147 | 119 | 126 | 146 | 115 | 111 | 121 | 124 | 112 | 120 | 101 | 109 | 96 |
| BMI (kg/m2) | 103 | 63.1 | 63.6 | 54 | 51.2 | 51.1 | 50.7 | 50.2 | 48.2 | 48 | 47.1 | 45.4 | 44.4 | 43.9 | 40.4 | 38.7 | 37.8 | 36.6 | 36 | 34.8 |
| Surgery | LSG | OAGB | OAGB | LSG | LSG | OAGB | LSG | LSG | OAGB | OAGB | LSG | LSG | LSG | LSG | LSG | OAGB | LSG | LSG | LSG | LSG |
| Comorbidity | HTN/DM/OSAS | HTN/DM/OSAS | HTN/OSAS | HTN/OSAS | HTN/CAD/cirrhosis of liver | HTN/OSAS | Obesity/OSAS | CAD/CVA/OSAS | OSAS | HTN/DM | OSAS | HTN/DM/CVA | DM/asthma | OSAS | OSAS | HTN/DM/CAD | OSAS | OSAS/COPD | HTN/DM/OSAS | HTN/DM |
| ASA class | III | III | II | II | III | II | II | III | II | III | II | III | II | II | II | III | II | II | III | III |
| MMT | 4 | 4 | 3 | 3 | 3 | 3 | 2 | 2 | 2 | 2 | 2 | 3 | 2 | 2 | 2 | 2 | 3 | 3 | ||
| Interincisor distance | 4.5 | 5.5 | 5 | 5.5 | 5 | 4.5 | 6 | 5 | 4 | 4 | 4.5 | 4.5 | 4 | 5 | 5.5 | 4.5 | 5 | 4.5 | 4 | 4.5 |
| ULBT | 2 | 2 | 1 | 2 | 2 | 1 | 1 | 1 | 2 | 1 | 1 | 2 | 1 | 1 | 2 | 1 | 1 | 1 | 2 | 1 |
| Thyromental distance (cm) | 8 | 6 | 7 | 9 | 8 | 7 | 9 | 9 | 9 | 9 | 8 | 6 | 7 | 7 | 9 | 9 | 7 | 7 | 6 | 8 |
| Sternomental distance (cm) | 17 | 15 | 16 | 15 | 14 | 16 | 20 | 18 | 16 | 17 | 16 | 15 | 16 | 18 | 13 | 16 | 17 | 16 | 16 | 18 |
| Neck circumference (cm) | 54 | 54 | 42 | 50 | 37 | 47 | 39 | 48 | 45 | 39 | 50 | 49 | 45 | 47 | 44 | 46 | 44 | 41 | 44 | 38 |
| Neck fat deposition/soft tissue loading on the upper airway | moderate | moderate | mild | moderate | moderate | moderate | Mild | mild | mild | Mild | mild | moderate | mild | mild | mild | mild | mild | mild | mild | mild |
| Waist circumference (cm) | 200 | 166 | 155 | 150 | 142 | 155 | 132 | 143 | 142 | 133 | 143 | 133 | 114 | 124 | 140 | 115 | 124 | 112 | 119 | 110 |
| Hip circumference (cm) | 202 | 154 | 158 | 148 | 144 | 150 | 146 | 126 | 156 | 134 | 148 | 126 | 140 | 128 | 124 | 115 | 118 | 120 | 120 | 126 |
| LQS grading | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 1 |
| POGO (%) | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| Time to intubation | 12 s | 14 s | 18 s | 22 s | 6 s | 10 s | 8 s | 11 s | 5 s | 5 s | 11 s | 13 s | 9 s | 6 s | 18 s | 8 s | 12 s | 22s | 20 s | 5 s |
| Expected cause of prolonged time of tracheal intubation | Performed by a third- year resident | Prior cervical spine surgery, copious secretions | For demonstration purpose | For demonstration purpose | ||||||||||||||||
| First-pass success | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes |
| Subjective easiness | easy | easy | easy | easy | easy | easy | easy | easy | easy | easy | easy | easy | easy | easy | easy | easy | easy | easy | easy | easy |
| Airway-related complications | none | none | none | none | none | none | none | none | none | none | none | none | none | none | none | none | none | none | none | none |
| Supplemental video-clips | Video S1 | Video S2 | Video S3 | Video S4 | Video S5 | Video S6 | Video S7 | Video S8 | Video S9 | Video S10 | Video S11 | Video S12 | NA | Video S13 | Video S14 | Video S15 | Video S16 | Video S17 | Video S18 | Video S19 |
BMI: body mass index; LSG: laparoscopic sleeve gastrectomy; OAGB: one-anastomosis gastric bypass; HTN: hypertension; DM: diabetes mellitus; OSAS: obstructive sleep apnea syndrome; CAD: coronary artery disease; CVA: cerebrovascular accident; ASA: American Society of Anesthesiologists; MMT: Modified Mallampati test; ULBT: upper lip bite test; LQS grading: Luk-Qu-Shikani grading; POGO: percentage of glottic opening scale.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



