
Submitted:
12 September 2024
Posted:
13 September 2024
You are already at the latest version
Abstract
Respiratory infections with RSV account for an important part of hospital admissions for acute respiratory infections. Nirsevimab has been developed to reduce the hospital burden RSV (respiratory syncytial virus) infections: Compared with the product previously used, it has a stronger binding capacity to RSV F protein and a high affinity for FcRn (neonatal receptor for the Fc fragment of IgG), which extends its lifespan. Nirsevimab has been shown to be highly effective in reducing hospitalization rates for RSV infections but a large or unknown number of treated subjects have been excluded in clinical and post-marketing studies. However, analysis of these studies cannot exclude that in rare cases, nirsevimab facilitates and worsens RSV infection (or other respiratory infections). This could be attributable to ADE (antibody-dependent-enhancement) which has been observed with RSV F-protein antibodies in inactivated vaccine trials. This risk has been incompletely assessed in preclinical and clinical trials (incomplete exploration of nirsevimab effector functions and pharmacokinetics). ADE by disruption of the immune system (not studied and due to FcRn binding) could explain there is no reduction in all-cause hospital admissions in treated age groups. Given the high price of nirsevimab, the cost-effectiveness of mass immunization campaigns may therefore be debated from an economic as well as a scientific point of view.
Keywords:
nirsevimab
; beyfortus
; ADE
; RSV
; bronchiolitis
; mAbs
; therapeutic monoclonal antibody
1. Introduction
Respiratory syncytial virus (RSV) is currently a primary cause of hospitalization in infants and young children globally. Worldwide, it is estimated that 33 million cases of RSV-associated ARI (acute respiratory infection) occur each year in children under 5 [1]. Bronchiolitis can severely affect some children under the age of two, and can lead to increased susceptibility to asthma. Hospitalization is required in 3% of cases, and admission to intensive care in 2 to 6% of cases [2]. The RSV virus reinfects children annually, and infection occurs despite the presence of maternal antibodies [3]. In infants under 2 months of age, the presence of maternal antibodies and the immaturity of the immune system prevent an effective immune response to an effective RSV vaccine [4]. Infants have a reduced capacity to produce neutralizing antibodies against RSV, compared with adults, making the former more susceptible to recurrent infections [5]. In infants, the immune response to RSV is polarized towards a Th2 profile, leading to considerable inflammation of the lungs [6]. The development of RSV vaccines has been hampered by the results of the inactivated vaccine, which has caused deaths from vaccine-antibody-enhanced RSV disease (VAERD - Vaccine-associated enhanced respiratory disease, a form of ADE, antibody-dependent enhancement): the mechanism of VAERD is classically associated with an exaggerated Th2 response, high levels of non-neutralizing antibodies, low levels of neutralizing antibodies and the presence of eosinophils in the pulmonary epithelium [7]. However, trials of RSV vaccines for children are underway but they do not concern newborn babies : vector-based vaccines studies in children over 12 months of age, with no proven efficacy against RSV infections [8] and with URTI more frequent in vaccinated children [9] and live attenuated viruses studies in children over 12 months of age, with no proven efficacy against RSV infections [10] in children over 6 months of age, with an unexpected frequency of respiratory events in the treated groups [11] [8]. Given the low capacity of infants to develop immunity to RSV and past failures in vaccine development, another approach to protecting infants from RSV is the development of monoclonal antibodies: this is passive immunization. Vaccination of mothers has also been shown to be effective: placental transfer of maternal antibodies protects the newborn during the first months of life [12].
Nirsevimab was developed to reduce the burden of RSV infections on hospitals, as its predecessor, palivizumab, which was reserved for at-risk children, required several injections and could not be recommended for all children for economic and logistical reasons. The modification of the Fc fragment of nirsevimab compared with palivizumab enables it to bind more strongly to FcRn (Fc neonatal receptor), thus prolonging its lifespan and reducing the number of injections to just one. Both monoclonal antibodies are directed against the RSV F protein. Nirsevimab has strong RSV-neutralizing activity. As the search for vaccines has been hampered by the discovery of an ADE effect due to anti-F protein antibodies, the European Medicines Agency (EMA) has taken into account the theoretical possibility of an ADE through increased FcγR-binding efficacy, and has eliminated this risk based on the results of clinical trials and in vitro and animal studies [13] (no ADE has been observed in humans for palivizumab, which has been in use for 20 years [2]).
Nirsevimab was approved by the EMA under a fast-track procedure [13](p.7) in accordance with European regulations [14]. This application was prompted by the high estimated burden of RSV LRTI (Low Respiratory Tract Infection) worldwide (3.2 million hospital admissions, including 1.4 million for patients under 6 months of age) [1]. Acute bronchiolite due to RSV accounts for about 9% of total infant hospitalisations in the USA [15]. This estimate should be compared with the global burden of ARI in the under-5s, estimated at 12 million hospital admissions [16]. Hospitalizations due to RSV in the under-5s would therefore represent around a quarter of ARI admissions. This proportion is consistent with Del Riccio’s 2023 estimate in Europe : admissions for RSV infections account for between 7% and 51% of hospital admissions for ARI (36.1% for France, 33.6% for Luxembourg and 30.6% for Spain). However, admissions for RSV infection account for only 1.8% to 9.9% (3.7% in France) of hospital admissions in the under-5s, which raises the question of the economic benefits of immunizing all infants. It should be noted, however, that Del Riccio’s estimates are based on incomplete data between 1997 and 2018: various acute respiratory pathologies were grouped together, whether or not they were due to RSV [17]. In France, for example, virological diagnosis is not routinely carried out for all cases of bronchiolitis [18]. Prevention of other respiratory infections must therefore also be taken into account if we wish to relieve the burden on pediatric hospitals. The relative risk of hospital admission for RSV infection has increased in the post-pandemic COVID-19 seasons (2021 and especially 2022); this may be due to an increase in RSV testing. Severe cases increased relatively more in older children (> 1 year) during the post-pandemic seasons [19]. If this pattern continues in the future, prevention should target children over one year of age.
The aim of this study is to independently assess the benefit of administering nirsevimab to all newborns to prevent hospital overcrowding, particularly in intensive care units. To be of benefit, nirsevimab must reduce the burden of hospitalization and admission to intensive care for all causes. Analysis of the results of phases 1 and 2/3 clinical trials and immunization campaigns in 2023-2024 will have to look for traces of a possible ADE effect (facilitation of RSV infections), which is part of the EMA’s Risk Management Plan [13]. The non-specific effect of mAbs on a possible disruption of the immune system leading to non-RSV infections must also be examined. We propose a review of the state of knowledge on the mechanisms of ADE in RSV infections. In particular, we show how the pharmacokinetics (role of low initial concentrations) and mode of action of nirsevimab (binding to FcRn and FcγR) are involved in these mechanisms. The shortcomings of preclinical and clinical studies in exploring these points are highlighted.
2. Clinical Trial Results and 2023-2024 Campaign
2.1. Clinical trial Results
2.1.1. Phase 1 and 2a
In the Phase 1b/2a trial on healthy preterm infants, 5 infants in the treatment group (69 children) developed LRTI (low tract respiratory infection) corresponding to the clinical criteria used for evaluation, and 3 developed febrile convulsions (but none in the placebo group of 16 children); one child in the treatment group was hospitalized for LRTI. With regard to LRTI not corresponding to the protocol definition, 10 children treated versus 1 in the placebo group developed LTRI within 151 days of observation, and RSV A was found 8 days after injection in 2 infants treated with the lowest dose. No RSV viruses were found in hospitalized children, but no virus tests were carried out in children with LRTI who did not meet the protocol criteria (only severe LRTI requiring assisted ventilation were included) or in those with URTI: no virus tests were carried out, despite the fact that 69% of reported adverse events concerned URTI and that 14.1% of treated children developed LRTI compared with 5.6% of placebo-treated children [20]. In the phase 1 trial in adults, the most frequent adverse event was URTI, with an imbalance in the treated group. Unfortunately, no search for RSV was carried out [21].
2.1.2. Results of Phase 2b and 3 Trials
The trials were sometimes carried out during periods of low RSV circulation: the number of cases observed was low, and that may reduce the statistical power of the trials and the ability to assess ADE [22,23]. Phase 2b and 3 clinical trials on nirsevimab [20,21,22,23,24,25,26] were analyzed by the EMA [27] and HAS (Haute Autorité de Santé/French High Authority of Health) [28].
In the MELODY trial, only LTRIs were evaluated. The 150-day efficacy on hospitalization for LRTI due to RSV is calculated on a very small number of participants (14 hospitalized in all, 0.6% in the treated group and 1.6% in the placebo group, so the ARR (absolute reduction risk) is 1%). Treated participants hospitalized for LRTI due to RSV were hospitalized longer than those in the placebo group, but no significance can be drawn from this, as too few individuals were involved. 8.1% (80/987) of treated children were removed from the analysis of results [12].
In the MEDLEY study [24], which combines 2 studies (one phase 2b [26] and one phase 3 [22] ), the ARR of LRTI hospitalization for all causes is 2% (total number 108/2350) and 2% for LRTI due to RSV (28/2350); but 2% of participants in the treated group were excluded before 151 days, compared with 1% in the placebo group, which could distort the estimate of efficacy and safety from the ADE point of view.
In preterm infants study, nirsevimab was effective against hospitalization for RSV infection and reduced the severity of RSV infections (of participants hospitalized for RSV infection, all those who were admitted to the intensive care unit (5 participants) or received assisted ventilation (4 participants) were in the placebo group). The occurrence of LRTI not due to RSV is not affected by treatment. Kaplan-Meier curves show that in the days following the injection, all-cause LRTIs are equally frequent in both groups; the protective effect does not appear until 20 or more days after injection. This does not rule out an early ADE of nirsevimab. All-cause hospitalizations are not reported in this study. 5.79% (56/968) of treated children were withdrawn from the study [26].
The open-label HARMONY study [25] involved 8058 infants under 1 year of age in Europe in 2022-2023. The investigator was sometimes the treating physician and decided whether or not hospitalization was due to RSV. RSV PCR tests were not routinely performed, but only after hospitalization, and 16 hospitalized children did not undergo RSV PCR tests. Final results have not been published, as 12 months’ follow-up is required for all children. The study showed a 1.2% reduction in the ARR of hospitalization for LRTI due to RSV, and a 0.4% reduction for very severe LRTI. For LRTI of all causes, the ARR of hospitalization was 1.3%. The Kaplan-Meier curves differ from country to country, and no explanation is given: in France, hospitalizations for LRTI due to RSV occur from the first day of the study among placebos, whereas in Germany they begin only 15 days post-injection, and 1 month later in the UK. This may reflect the staggered circulation of the virus in these countries. Among grade 3 serious adverse events, there were as many infections in the treated group as in the placebo group, and more severe infections in the treated group than in the placebo group. Among treated children, only 500 out of 4037 (12%) were less than 7 days old. 0.22% of treated children were withdrawn from the study.
The main results of the clinical studies are summarized in Table 1.
In the phase 1b/2a infant and phase 1 adult trials LRTI due or not to RSV are mostly observed in the treated groups and not in the placebo group.
Phase 3 and 2b trials are sometimes carried out outside periods of RSV circulation and therefore only imperfectly assess the possibility of ADE. The imbalance between placebo and treated groups may lead to a result biased in favor of efficacy [29]. Hospitalizations for LRTI due or not to RSV were rare and very slightly less frequent in the treated groups compared with placebo, but they could be more severe following treatment: in these rare cases, ADE could therefore explain these results. The high rate of children withdrawn from studies before analysis could distort efficacy results and the search for ADE. Nevertheless no ADE was observed by the EMA in clinical trials, despite greater signs of infection severity in treated groups and the frequent exclusion of infected subjects immediately after injection.
2.1.3. Deaths in Trials
The FDA notes an imbalance of deaths in favor of the treated group: 12 deaths in the 3,710 treated participants (0.32%) versus 4 in the 1,797 control participants (0.22%), taking into account one death in the placebo group 6 days after the end of the study and without specifying deaths in the treated groups after the end of the study [30]. In the studies listed by the EMA [27], 8 deaths were recorded (with the same percentage - 0.3% - in the treated and placebo groups). The Domachowske study on fragile and preterm infants [20] (which was published as a correspondence, i.e., not peer-reviewed) concerns premature babies and newborns suffering from heart or lung disease, and compares the effect of the monoclonal antibody previously used (Synagis®, palivizumab) with Beyfortus® (nirsevimab). It provides a full description of the deaths observed: of the 6 deaths listed, 5 were related to pneumonia or bronchiolitis not attributed to treatment (5 babies who died were treated with nirsevimab (5/614 = 0.81%) and 1 (1/304 = 0.32%) with palivizumab). Despite the low number of deaths, there was an imbalance against nirsevimab. In the absence of a placebo group, this result may be interpreted in terms of the lower efficacy of nirsevimab compared with palivizumab. It is also possible that nirsevimab facilitates and aggravates bronchiolitis: these injections take place during periods when the virus is circulating. In particular, nirsevimab appears to be more dangerous than its predecessor, palivizumab. RSV testing was not performed except in one case (negative result), which is regrettable in a study of the efficacy of a product against RSV. No autopsies for histopathological analysis of the lungs were reported although the EMA recommends the investigation of immunopathological phenomena after any immunization failure [27]. It was therefore impossible to look for signs of inflammation and VAERD. 6.86% of treated children (63/918) were withdrawn from the study [20]. In conclusion, it is therefore impossible to exclude ADE as a cause of these 5 deaths.
2.2. Phamacovigilance Data and Results of the 2023-2024 Season Immunization Campaign
The EudraVigilance database records spontaneously reported adverse events for nirsevimab. As of April 15, 2024, there were 140 reports, mainly from healthcare professionals (138/140), 89 of which were for “bronchiolitis”, 129 for “RSV” and 56 for “drug ineffective”. Only 26 reports did not concern respiratory events : the most frequently reported adverse event is bronchiolitis, and could be due to an ADE effect [31]. Moreover, according to the Île de France pharmacovigilance center, there is a theoretical risk of aggravation of RSV infection through non-neutralizing antibodies [32].
Following its approval by the EMA on October 31, 2022 [27] and by the FDA on July 17, 2023 [33], nirsevimab was recommended for infants and children under 2 years of age in 4 countries for the 2023-2024 season: USA, France, Spain and Luxembourg. In the USA, on August 3, 2023, the Advisory Committee on Immunization Practices recommended nirsevimab for infants aged <8 months born during or entering their first RSV season and for infants and children aged 8-19 months who are at increased risk of severe RSV disease entering their second RSV season [34]. In France, the HAS recommends nirsevimab for infants born at a gestational age of 35 weeks or under and under 6 months of age entering their first RSV season, infants under 2 years of age having required treatment for bronchopulmonary dysplasia in the past 6 months and infants under 2 years of age with congenital heart disease with a haemodynamic impact [28]. In Spain, the Spanish Society of Neonatology recommends nirsevimab for all newborns and at-risk children under two years of age [35]. In Luxembourg, the government has recommended immunization for all newborns and children under one year of age [36].2.2.1 USA results of immunization campaign
In the USA, immunization coverage for children under 20 months of age is about 20%, but data do not include children born after October 1, 2023 [37] (making it unnecessary to compare hospitalization rates for RSV and non-RSV LRTI with previous seasons). An exceptional peak in the rate of hospitalizations due to RSV was observed in 2022-2023 in 0-4 year-olds [38]. The results of this campaign are set out in a non-peer-review article by the CDC [39]: a 90% effectiveness rate against RSV-associated hospitalizations is announced, but the method of calculation is not set out (this is a case-control study). But it is impossible to match a case with a control given the disproportion of the groups (59 children treated with nirsevimab out of 699) : the most optimum case-to-control ratio is 1:1 and statistical power can be improved by increasing the ratio up to 4 controls/1 case [40]. Participants were infants under 8 months of age hospitalized for ARI, with known nirsevimab status and having been tested for the presence of RSV by PCR. Hospitalizations less than 7 days after nirsevimab injection are excluded. The published figure shows that ARIs are more frequent in the days following injection, and it is unfortunate that the first 7 days have been excluded from the calculation (20 nirsevimab-treated children are excluded for this reason, reducing the number of treated children studied to 59). Of the children hospitalized for ARI due to RSV 6 had received nirsevimab, if we were to add these 20 excluded children, the number would rise to 26, and the product’s effectiveness would be less than the advertised 90%. It is therefore impossible to evaluate the possible ADE, but we can suspect that it exists, since of the total number of hospitalizations due to RSV, 77% (20/26) are observed within 7 days of injection [39].
2.2.2. Luxembourg Results of Immunization Campaign
In Luxembourg, nirsevimab immunization began in maternity hospitals on October 1, 2023, with 84% calculated coverage. Children hospitalized with respiratory symptoms are systematically tested for RSV. RSV-positive newborns under 6 weeks of age are routinely hospitalized, so hospitalization is not a criterion of severity for this age group. As compared with the 2022 season, the reduction in hospitalizations for RSV in children under 5 years of age is lower than in those under 6 months of age, and the reduction in the burden on hospitals may be lower than hoped [41], since severe cases are more frequent among children over 1 year of age [19]. No data have been published on all-cause hospitalizations, and hence on the potential reduction in hospital burden. In 2023, there was a 38% decrease in the number of children under 5 hospitalized for RSV infection (88,4% were not immunised), and a 69% decrease in those under 6 months (65.3% not immunized) as compared with the 2022 season. As in other countries, the number of hospitalizations among young children was high in 2022. So the reduction in the number of children under 5 hospitalized for RSV infection cannot be attributed to immunization with nirsevimab [41].
2.2.3. France Results of Immunization Campaign
In France, approximately 230,000 doses of nirsevimab were administered between September 15 and December 15, 2023 for about 186,000 births (the remaining 44,000 doses had to be administered as catch-up doses to older children) [42]. Indeed, 42,290 doses of nirsevimab were administered between September 15, 2023 and January 31, 2024 to children born between February 6 and September 15, 2023 [43]. We can therefore assume that immunization coverage is high in France for this season. According to Santé Publique France [18], in comparison with previous seasons (with the exception of the 2022-2023 season, which was exceptionally intense as in the other countries), bronchiolitis-related activity was comparable in intensity in primary care, while hospital activity was comparable to or slightly higher than the reference seasons. The proportion of intensive care unit admissions for children under 2 years of age was comparable to the reference seasons. In infants aged 3 months and over, emergency room visits and hospitalizations were higher than in previous seasons, and close to levels for the 2022-2023 season. This activity is even higher at the start of the epidemic (weeks 37 to 46: i.e., from September 15, 2023, the start of the immunization campaign). The same type of data (exact number of intensive care unit visits for bronchiolitis) is not available for previous seasons (only the number of hospitalizations is provided [44]). RSV was systematically tested on hospitalized patients only during the 23-24 season. So, it is impossible to derive from these data an estimate of the effectiveness of nirsevimab on the risk of ICU hospitalization for RSV.
A case-control study in preprint surveys children under 5 months of age admitted to intensive care for bronchiolitis between September 15, 2023 and January 31, 2024 in France [45]. Effectiveness of nirsevimab against ICU hospitalization for RSV bronchiolitis was estimated at between 74.4% and 80.6%, depending on the inclusion criteria. Data are from Santé Publique France but 52% of cases are excluded. 238 cases (newborns hospitalized for bronchiolitis with a positive RSV test) were compared with 50 controls (newborns hospitalized with a negative RSV test). It was therefore impossible in this study to match each case with a control, given the disparity in the numbers of cases and controls. The majority of these 52% of excluded cases therefore concerned infants with missing data, which is a pity, since according to SPF’s 23-24 report [18], surveillance of RSV infections in patients admitted to the intensive care unit usually concerns only those over 18 years of age. For the 23-24 season, non-exhaustive surveillance is carried out for all cases of bronchiolitis in patients under 2 years of age, regardless of the virus involved (identified or not). It should be noted that for the 2020-21 and 2021-22 seasons described by Vaux [46], a case of bronchiolitis in a hospitalized child under 2 years of age is defined [47] according to the ICD [48] and corresponds to codes J21, J21.0, J21.8, J21.9, which concern all acute bronchiolitis regardless of the virus involved. Concerning the possible detection of early ADE among nirsevimab-treated newborns, comparison of the main analysis and sensitivity analysis 2 shows that 45% (17/38) of PICU admissions for LRTI not due to RSV and 27% (14/51) of LRTI cases due to RSV occurred less than 8 days (or after an unknown delay) after nirsevimab injection. Among nirsevimab-treated newborns, a comparison between sensitivity analysis 1 and 2 shows that 8% of PICU admissions for LRTI not due to RSV and 8% for LRTI due to RSV definitely occurred less than 8 days after nirsevimab injection. These data cannot rule out ADE from RSV infection or other infections (due to immune system disruption) [45].
A peer-review case-control study indirectly calculates the effectiveness of nirsevimab against RSV bronchiolitis : depending on the different calculation methods, this is around 80%. But 17% (142/832) of children hospitalized for RSV infection were excluded from the study. The calculation of effectiveness against severe RSV infections is incomprehensible (last line and legend of Figure 2 are contradictory). In the intention-to-treat analysis (including all patients regardless of the date of nirsevimab injection), there was no effectiveness during the first 7 days (19% of cases - 15/75- and 20% of controls - 23/120- received nirsevimab), this lack of efficiency compares with the advertised 80%. This does not rule out early ADE. Here again, the number of controls is less (by half) than the number of cases, and does not allow a correct calculation. Recruitment was limited to 6 French hospitals and does not appear to be representative, since only 8.7% of cases and 28.1% of controls were treated with nirsevimab: we should observe much higher coverage for children with a median age of 3 months: in fact, 230,000 doses were administered during the study period for around 186,000 births [42].
2.2.4. Spain Results of Immunization Campaign
According to an October 2023 survey, immunization coverage is above 80% in almost all regions of Spain [49]. This is confirmed by more recent publications (90% in Andalusia [50], 96.5% in Asturias [51], 86% in Madrid [52]. At national level, according to the SIRVA network [53], hospitalization rates for RSV infection in 0-4 year-olds are comparable for the 2022-2023 and 2023-2024 seasons (the peak is 140/100,000). In Galicia, according to the regional Ministry of Health report, epidemic waves of RSV infection are comparable over time between 2022-23 and 2023-24 in terms of positivity to RSV tested in the general population. There has been a drastic reduction in hospitalizations for RSV in both newborns and children born since April 2023, with a high rate of immunization coverage (93% in NN and 86% for catch-up infants born before the campaign). For children entering their 2nd RSV season, hospitalization rates are identical to previous seasons (they have not been immunized) [54].
The first results of the estimation of the effectiveness of nirsevimab on newborns, children under 6 months and at-risk children under 2 years of age, in Galicia, between September 25 and December 31, 2023 have been published [55]. This study is scheduled to run until 2026 [56], so the publication only concerns results from the first 3 months of the immunization campaign. Nirsevimab was offered to all newborns from September 25, 2023 unless medically contraindicated, and to all children born after April 1, 2023. The reasons for non-immunization (parental refusal or medical contraindication - fragile state of health of the newborn) are not precisely known; some of the non-immunized newborns were certainly more fragile than those immunized, and comparison between the 2 groups will be difficult as they do not involve equivalent populations in terms of health status. Given the small number of non-immunized infants, case-control matching is impossible. Hospitalization for RSV with severity criteria occurred only in the treated groups which may be a sign of treatment-induced ADE. Nosocomial infections were excluded. Nirsevimab is administered on the day of birth in Galicia. The study’s lead author confirms that all infections developed in hospital for whatever reason were excluded (personal communication): this means that newborns who acquired the infection during their stay in the maternity hospital were excluded from the study. The estimated effectiveness should have taken into account these excluded cases, the number of which is not provided. Moreover, these “nosocomial” cases can be explained by early post-injection ADE of nirsevimab, which their exclusion does not allow us to evaluate. The effectiveness of nirsevimab against hospitalization for RSV infection was 82% (on 46 cases) in intention-to-treat analysis on children under 6 years of age with no risk factors. Sensitivity analysis excludes breakthrough infections and gives 87.5% effectiveness (on 44 cases). For all-cause hospitalization, effectiveness was 66.2% (on 366 cases). The authors compare the results of the 23-24 season with previous seasons since 2016, excluding the 2020-2022 season because the bronchiolitis epidemic was lower than normal, but does not exclude the 2022-2023 epidemic, which was higher. According to Figure 4 in the appendix, if we exclude the exceptional 22-23 season, the 23-24 hospitalization rate is comparable to previous seasons, albeit slightly lower [55]. So the effectiveness of nirsevimab in reducing all-cause and RSV hospitalization rates is questionable
In Navarre, the effectiveness of nirsevimab was calculated from epidemiological surveillance of newborns between October 2023 and January 2024 (the RSV circulation season) according to their immunization status (92% of newborns were treated, mostly within the first 7 days of life). Despite the low number of non-immunized children, effectiveness could be calculated on emergency room visits for RSV (87.8%), hospitalization for RSV (88.7%) and admission to intensive care (85.9%). No details are given on the clinical results of the 5 children admitted to intensive care (2 non-immunized and 3 immunized) : It is not known whether immunized children developed more or less severe infections than untreated children. It should be noted that newborns injected less than 1 day previously are counted as non-immunized (if they develop RSV infection within 24 hours of injection, early ADE cannot be assessed) and children admitted for respiratory illness not due to RSV were not counted: It is therefore impossible to assess the ADE of RSV and other viral infections and the effectiveness of nirsevimab on all-cause hospitalizations [57]. Data from previous years are not comparable [58]. The main results of post-marketing campaigns are summarized in Table 2.
From these results, we can conclude that nirsevimab is effective against RSV infections. However, in all studies, RSV infections occurring in the first few days following nirsevimab injection were not included. We cannot exclude that nirsevimab could in very rare cases cause facilitation/aggravation of RSV infection in the days following injection. On the other hand, nirsevimab does not reduce the rate of all-cause hospitalization in targeted populations, although hospitalization due to RSV is significantly reduced (however, efficacy and effectiveness may be less than advertised, given the large or unknown number of subjects excluded from clinical trials or observational studies).
2.3. Neonatal Deaths in France
In France, the government recommends injecting nirsevimab into all newborns leaving the maternity hospital [59]. The average length of stay for childbirth is 4.6 days [60]. Based on official French data on deaths [61] and births [62], it is possible to calculate the mortality rate between 2 and 6 days of life during the nirsevimab immunization campaign and to compare it with the periods before and after. (Figure 1) There is a highly significant peak (p=0.006) for babies born in September 2023 and dying between 2 and 6 days with 55 deaths (95% CI 27 - 50). And there is a very highly significant peak (p=0.0007) for babies born in October 2023 with 62 deaths (99.8% CI 22 - 60). In November 2023, after the two highly significant peaks, we observe a significant drop in the number of deaths (p=0.02) with 26 deaths (95% CI 27-50). In December 2023, the number of deaths is high, at the limit of significance at 2.5%, with 50 deaths (95% CI 26-50). And in January 2024 the number of deaths is significant (p=0.022) with 52 deaths (95% CI 27-50). In February, March and April 2024, mortality rates between 2 and 6 days of life returned to normal. Apart from the month of November with a significantly low rate of deaths, the rate of babies dying between 2 and 6 days of age is significantly higher than the rate expected between September 2023 and January 2024, the period of RSV circulation and nirsevimab immunization. Doses of nirsevimab quickly ran out in October [63] (p. 52) and dispensing of doses distributed outside maternity wards was drastically reduced in November, only to resume in early December 2023, with the last doses administered in January 2024 [43]; it is therefore possible that dispensation in maternity units was also reduced in November 2023, this being in line with the low rate of deaths between 2 and 6 days of life compared with other months. According to the data [18], the bronchiolitis epidemic was less intense in November 2023, which could explain the dip in neonatal mortality, although this does not rule out the possible role of an early ADE, since for this to manifest itself, the virus must be circulating strongly. It should be noted that the latest data are not yet fully consolidated. An early ADE of nirsevimab cannot therefore be ruled out to explain why these data significant peaks in neonatal mortality coincide with the immunization campaign.
For each month, newborns born during the month and dying between 2 and 6 days of age are counted. The mortality rate is obtained for each month by dividing the number of deaths by the number of births. The reference rate is calculated by dividing the total number of deaths by the total number of births in 2018 and 2019 (before the Covid-19 pandemic): it is 0.69 deaths between 2 and 6 days of life per 1,000 births. This rate is indicated by the green horizontal line. For each month, the expected death rate is calculated by multiplying the reference rate by the number of births. Poisson’s law (a statistical law used for rare events) was used to calculate the different confidence intervals for mortality rates at 95% (classic threshold) and 99.8% (alarming threshold). The 95% confidence interval is marked by the blue dotted lines, with a probability of less than 2.5% for rates below or above the lines at the bottom and top respectively. The 99.8% confidence interval is denoted by the red dotted lines with a probability of less than 1 ‰ for rates below or above the lines at the bottom and top respectively. The black dotted vertical lines represent the month of September 2023, with the nirsevimab immunization campaign starting on the 15th of that month and the month of January with the last doses administered (the end of the nirsevimab distribution campaign in France has been announced for December 2023 [64]). Monthly numbers of births and deaths are taken from INSEE data (France- Institut National de la Statistique et des Études Économiques-France) [61,62].
Superimposing the neonatal death rates for each month between 2018 and 2024 highlights peaks in deaths that fall outside the average range and recur 2 months in a row (September/October and December/January) for the 2023-2024 season; the sharp drop in November is also found in 2019 (excluding the Covid pandemic and the nirsevimab immunization season) (Figure 2).
It is impossible to perform a time series analysis, as monthly data on the number of doses of nirsevimab administered are not available: we only know the start and end of the immunization campaign, and can only assume that the number of doses administered in hospitals in November 2023 fell drastically. It is therefore impossible to establish a causal link between the administration of nirsevimab and the observed spike in neonatal deaths; however, the biological plausibility of this link is demonstrated by the review of the biological mechanisms of ADE and is suggested by the results of clinical and post-marketing studies. The dip in the November mortality rate is observed not only in 2023, but also in 2019, and cannot therefore be explained only by a possible shortage of nirsevimab doses. This confirms that a causal link between the immunization campaign and the variation in death rates cannot be established with the data currently available. However, the repetition of 2 peaks of excess mortality (each lasting 2 months) could be a signal to watch out for.
Between March 2018 and February 2024 the monthly rate of deaths between 2 and 6 days of life per 1,000 births was calculated according to INSEE data [61,62]. Data have only been collected since 2018, the year for which the early neonatal mortality stabilized (after a drop between 2001 and 2011 and an increase between 2011 and 2018) [65]
3. Design of Nirsevimab
Palivizumab, mAb against RSV F protein (viral-cell membrane fusion protein) reduced hospital admissions in observational studies [2] but a Cochrane review [66] showed no beneficial effect of palivizumab compared with placebo. Pavilizumab should be administered once a month during the RSV circulation season, due to its short serum half-life [67]. Manufacturers of anti-RSV mAbs have made efforts to increase the half-life and affinity for F protein [4] (Figure 3 left). Nirsevimab is derived from this research: it has superior neutralizing power to pavilizumab and an extended half-life thanks to YTE mutations (80-120 days) [2]. YTE mutations increase FcRn binding (the neonatal Fc crystallizable fragment receptor (FcRn) binding to the Fc portion of IgG) [68]. FcRn protects IgG from intracellular degradation by a pH-dependent recycling mechanism, and enables its transport across cell barriers. IgG ingested by the cell via pinocytosis binds to FcRn in the acidic environment of the endosome (Figure 3 right) and is transported intact back to the surface of the plasma membrane [69]. YTE mutations increase mAb affinity for FcRn at acidic pH [4] and nirsevimab binds FcRn with very low affinity at neutral pH [70].
4. Definition, Role and Localization of FcRn : Based on Our Knowledge of the Role of FcRn, what Might be the Consequences of a mAb’s Increased Affinity for This Receptor?
4.1. Transport of Free and Antigen-Bound IgG
The FcRn is a multifunctional atypical Fc-gamma receptor (FcγR). IgG binding to FcRn accounts for its long life (3 weeks) [69]. FcRn enables IgG to be transported across cell barriers, including that of the lungs. FcRn binds IgG only in acidic environments (pH between 5.0 and 6.5). FcRn is expressed on cell surfaces and in cell endosomes in mucous membranes (epithelium of placenta, liver, kidneys, genital tract, lungs) and in endothelial and hematopoietic cells [71,72]. In the lungs, IgG is transcytosed through the respiratory epithelium from the lumen to the serosa by FcRn [68,69]. At these sites, FcRn ensures IgG transport across the mucosal barrier and may play a role in immune surveillance and host defense [73]. FcRn enables bidirectional transcytosis of IgG in the apical to basal and reverse direction [70,74,75,76]. IgG preferentially binds to FcRn on the surface of mucous membranes when these are acidic; this is the case in the intestine [77] which allows newborns to acquire IgG from breast milk. But the neonatal lung mucosa has a variable pH and can be acidic in some individuals [78,79,80,81].
Antigen-bound IgG (IgG-ICs- IgG-immune-complex) also bind to FcRn [82] and cause IgG-IC complexes to enter cells [69,70]. This transport does not require transepithelial pH gradients established at epithelial surfaces [72]. An antigen bound to the Fc fragment allows FcRn-specific transport across the mucosal barrier [83].
4.2. Intracellular Transport of Viruses by FcRn
Echovirus not bound to antiviral IgG can enter in target cells by FcRn binding [73,84,85]. Concerning the viruses linked to specific antibodies, a monoclonal antibody against a reovirus could increase virus growth in a murine macrophage-like cell line; this increase occurred with sub-neutralizing antibody concentrations and was mediated by the macrophage-like cell Fc receptor. No specific reference was made to FcRn, which was not characterized at the time (1983) [86]. FcRn can promote the entry of IgG-virion complexes (CMV cytomegalovirus) by transcytosis across the placenta. It has been suggested that IgG-virion complexes can be transcytosed in other tissues: intestine, kidney, lung and breast. However, this only occurs with low-affinity antibodies (or low levels of neutralizing antibodies) [87]. Highly neutralizing monoclonal antibodies increase HIV transcytosis on a human cell line (and more strongly at acidic pH), this transcytosis depending on the FcRn of the target cells [88]. Strongly neutralizing antibodies do not confer protection in challenge assays and ADE may be an FcRn-mediated mechanism [89].The enhanced binding of nirsevimab to FcRn therefore extends its lifespan, but when bound to the RSV virus, it is not impossible that this binding facilitates entry of the virus into certain cells, particularly in the lower respiratory tract, facilitating or aggravating infection. FcRn is expressed in macrophages [82]. The lungs are an important site of FcRn expression in several species, and FcRn is highly expressed by alveolar macrophages of all species [68].
5. What Are the Mechanisms of ADE in Viral Infections and following Antiviral Vaccinations, and How Might an RSV F-Protein mAb with Increased Affinity to FcRn be Involved? Could mAb Binding to other FcγRs be Involved?
5.1. Mechanisms of ADE of Viral Infections by Specific Anti-Viral Antibodies
ADE has been described in numerous viral infections and anti-viral vaccinations (arthropod-borne viruses, alphaviruses, flaviviruses, respiratory viruses as influenza virus, coronaviruses, RSV, Ebola [90] and measles virus [91]), and has been attributed to sub-neutralizing concentrations of antibodies capable, under certain conditions, of enhancing viral infection by facilitating viral entry into target cells. ADE is produced by interaction between immunoglobulin Fc fragment receptors (FcγR) or complement receptors and the virus-antibody complex. Extrinsic ADE promotes infection of myeloid cells (monocytes, macrophages, dendritic cells and granulocytes). Internalization of virus-antibody complexes can also modulate the expression of the innate cytokine response to the virus: this is intrinsic ADE [90]. The binding of antibodies to cellular FcγRs and to complement can also lead to a more global disruption of the immune system.
5.2. ADE during Infections and Vaccinations with RSV or Other Viruses
ADE is observed during infections with viruses that replicate preferentially in macrophages [92]. Severe RSV infections are observed in the first 6 months of life when maternal antibodies are still circulating. Infants with maternal antibodies to RSV were not only susceptible to RSV infections, but the rate of severe illness was higher in these infants than in infants without maternal antibodies [92,93]. Antibody levels do not correlate with protection against RSV infection in challenged animals [93]. However, the severity of RSV infection requiring oxygen therapy is lower in breast-fed infants than in formula-fed infants [94]. Anti-RSV IgG is found in 95.2% of newborns at birth; maternal antibodies decrease considerably after 2 months of life; the lowest level is reached at 7 months, after which the level rises again with the first infections. The hospitalization rate for newborns peaks at around 6 months of age. Maternal antibodies do not protect against reinfection: this would be due to the short lifespan of the antibodies and also to mutations in the virus, which escapes the antibodies acquired by the previous infection [95]. These aggravated RSV infections could be due to inflammatory cytokines produced during macrophage infection [96]. This was confirmed in a re-examination of the case of two young children who died of RSV disease after being vaccinated with an inactivated vaccine in trial (80% of children vaccinated and subsequently infected with RSV had to be hospitalized). VAERD-associated bronchiolitis is characterized at autopsy by diffuse inflammation of the alveoli and infiltration by neutrophils and eosinophils. Eosinophilia is not found in the blood. In classical bronchiolitis, inflammation is centred on the bronchioles, and eosinophils are virtually absent. In VAERD, unprotective antibodies form immunocomplexes with complement, triggering a Th2 polarization of the cellular response (Th2 cytokines increase bronchoconstriction and lung pathology) [97].
5.3. Role of Complement in ADE (RSV and Other Viruses)
Complement is expressed by many cell types on their surface, and its binding to the virus-antibody complex can facilitate viral entry into cells [98,99]. In influenza virus infection, autopsies of fatal cases have shown large amounts of deposition of a complement component activated by the virus-antibody immune complex [100]. Complement-fixing immune complexes play an important role in enhanced RSV disease: IgG and complement are colocalized in the alveoli and bronchioles of mice suffering from VAERD [101].
5.4. Role of IgG Binding to FcγR in ADE during RSV Infection
In humans, there are 3 types of Fc receptor that bind human IgG. FcγRI is present exclusively on monocytes/macrophages and binds human IgG with high avidity. FcγRII and FcγRIII, are found on monocytes, macrophages, eosinophils, neutrophils, natural killer cells, B lymphocytes and T lymphocytes. Both receptors have relatively low specificity and relatively low avidity for IgG compared with FcγRI [92]. The binding of FcγRs (type I or II) depends on the conformational state of IgG (open or closed) [5]. The role of FcγRIIIa is said to be double-edged. FcγRIIIa in NK cells participates in viral clearance by eliminating infected cells through the ADCC (antibody- dependent cell-mediated cytotoxicity) phenomenon and may play an anti-inflammatory role during RSV disease [102,103]. But FcγRIIIa expression is increased in NK cells from patients with severe RSV-associated pathology, thus suggesting that this receptor may contribute to RSV disease. In mice, FcγRIII has a pro-inflammatory role in RSV infection. FcγRIII is present on nasal epithelial cells and controls the balance between tolerance and inflammation through its interaction with TLR4 [102].
5.5. Involvement of the Monocytic Lineage in ADE (In Case of Viral Infection and after RSV Vaccination)
The involvement of the monocytic lineage, via the FcγRs it expresses, has been shown in ADE during dengue [104] and for other viral infections [105] : macrophages can promote viral replication. Macrophages and bronchial epithelial cells are susceptible to RSV replication [3,106,107,108] and are involved in ADE during RSV infection [3,92,96,109,110,111]. Severe post-vaccination RSV infections may also result from increased viral replication in macrophages [110]. Serum from immunized children is rich in RSV F-protein antibodies and is capable of aggravating infection of a macrophage line [3,111] or pulmonary dendritic cells in vitro [112], this effect being Fc receptor-dependent.
5.6. Immune System Disruption Caused by IgG Binding to FcRn
FcRn located in the lungs could cause non-specific aggravation of infections, under inflammatory conditions. FcRn is expressed in lung parenchyma and lung immune cells, and enables preferential secretion of low-affinity IgG into the lumen. IgG1 with high affinity for FcRn could saturate FcRn receptors locally, counter-intuitively allowing preferential passage of low-affinity IgG into the pulmonary lumen. Under these inflammatory conditions, this process could damage lung tissue [113]. The FcRn binding of IgG-ICs formed in the presence of excess antibody has an immunosuppressive effect, in contrast to those formed in the presence of excess antigen (which are immunogenic) [77]. IgG-antigen ICs can activate TF (tissue factor) via monocyte FcRn; this activation of TF leads to the activation of FXa, which is involved in thrombotic phenomena. In this process, FcRn and FcγRIIa may cooperate [114].
IgG-IC binding to FcRn has an inflammatory role, through FcRn engagement on the cell surface in conjunction with binding to other FcγRs: this process could contribute to autoimmunity phenomena [115].
5.7. Known ADE with Mabs against RSV and Other Viruses
The therapeutic effect of mAbs may result from binding to complement components. Since C1q and FcγR binding sites on the Fc domain are proximal and partially overlapping, amino acid substitutions altering FcγR binding also alter C1q recruitment and vice versa [116]. Binding an mAbs against Ebola virus can worsen the infection. It is necessary to completely (and not partially) eliminate the effector functions of mAbs to obtain a therapeutic effect: these effector functions could induce an ADE effect which would cancel out the therapeutic effect [100]. About RSV, in cultured macrophagic cell lines, neutralizing anti-protein F mAbs induce ADE at low concentrations [111,117]. The extent of ADE correlates with complement fixation and the level of neutralizing antibody and can vary in the presence of antibody mixtures [117]. This has recently been confirmed and attributed to IC deposition [105,109].
5.8. Importance of Antibody levels and Quality: ADE Can Occur in the Presence of Low Levels of Strongly Neutralizing RSV Antibodies
In the case of mAbs capable of neutralizing dengue virus, ADE occurs only with certain epitopes and viral strains. For the same antibody, neutralization occurs at low dilution and ADE at high dilution: neutralization occurs when virions are in the presence of a large excess of antibody [104]. In the same way, ADE induced by anti-dengue vaccine antibodies occurs only at low antibody levels [118]. An in vitro ADE effect has been demonstrated on cells expressing certain FcγRs with sub-neutralizing antibody concentrations in certain viral infections [100]. Nirsevimab has a higher neutralizing capacity than palivizumab, which does not always prevent ADE [12,87,88,89,109,110].
We have seen above the possibility of severe RSV infections in children with low levels of circulating maternal antibodies. The effect of antibody concentration on the ability to induce ADE in vitro has been shown for the anti-RSV F-protein mAbs palivizumab and the precursor to nirsevimab (D25, lacking the YTE mutation that increases affinity for FcRn) : they induce ADE at low concentrations, whereas they are strongly neutralizing; at high concentrations, infection is blocked. This in vitro ADE was shown for palivizumab on a human monocytic cell line. For D25, maximum infection was observed at a dilution corresponding to a concentration as low as 1 ng/ml. D25 induced a stronger ADE effect than palivizumab when binding to the FcγR of cells: the ADE effect outweighed the neutralizing power [93]. Palivizumab recognizes the post-fusion (and pre-fusion) form of F protein, whereas D25, which is more potently neutralizing, is specific for the post-fusion form, as is nirsevimab [7]. It cannot therefore be ruled out that nirsevimab may also induce a low-concentration ADE like D25, since it has the same structure as D25 with the added YTE mutations. Van Mechelen’s experiments at low concentration should be repeated with nirsevimab :does nirsevimab induce a stronger ADE than palivizumab at low concentrations?
6. How Were the Factors Likely to Cause ADE with Nirsevimab Assessed?
No ADE has been observed in humans for palivizumab, which has been in use for 20 years [2]. But all the modifications of nirsevimab compared with palivizumab theoretically open up the possibility of an ADE via binding to FcRn or other FcγRs [71,116,119].
6.1. Pharmacokinetics
Given the possibility that a low level of neutralizing antibodies may be capable of inducing ADE, it is important to be familiar with the pharmacokinetics of nirsevimab.
Animal studies [4,70] are carried out with doses well above those used in clinical trials and for commercial use. One study is IV and with other mAbs close to but different from nirsevimab. The results show a rapid decline (within 24 days) in serum and much lower concentrations in nasal fluid (1/10,000) and broncho-alveolar washings (less than 1/1000), as well as wide inter-individual variations. YTE mutations halve the bronchial bioavailability of mAbs [70]. The EMA report [27] points out that in ADE trials, rats treated with nirsevimab are exposed to RSV at the time of peak antibody concentration. It is therefore possible that, in animals, sub-neutralizing concentrations are present in the lungs in the first few weeks after injection.
Clinical studies in adults [21] and in premature infants with an average age of 6 months [20] show that peak serum concentrations are reached in 3 and 8 days respectively; in adults the peak neutralizing activity is reached 6 days after IM. 5% of children have an antibody level below the effective target concentration (below 4-fold the baseline of neutralizing antibodies) after 8 days, and 10% after 151 days. Anti-drug antibodies (ADAs - targeting YTE mutations) are detected in 28% of treated subjects: these ADAs could impact pharmacokinetics between days 151 and 361 in some subjects [20,24]. Results from other clinical trials also show that in rare children, the theoretical threshold of neutralizing activity is not reached or is only reached after 150 or 200 days [22,24]. Pharmacokinetic studies have not been carried out in healthy neonates a few days old, who represent the target population for the 2023-2024 campaign. In clinical trials, children were at best around 3 months old; in particular, in the open-label study which included a large number of participants (4,037 treated), only 12% were less than 7 days old [25]. The pharmacokinetics at birth may differ from those observed in infants a few months old, but the recommendations concern newborns in the first few days of life (on leaving the maternity ward in France [59], on the first day of life in Galicia [55] and in the first 7 days of life in Navarre, Spain [57] and in the USA from birth [30]. As the maximum concentration is reached in infants within a few days, it is possible that in some infants, the protective concentration is not reached as quickly, and that sub-neutralizing doses of antibodies circulate in the blood (or lungs) for some time, thus favoring ADE in epidemic periods in the event of an encounter with the virus. Similarly, neutralizing serum levels may not be maintained in all infants during the epidemic season, due to the waning immunity conferred by nirsevimab. Pharmacokinetic preclinical studies should be performed in the presence and absence of viral infection to determine the effect of infection on antibody persistence: the half-life in uninfected and infected animals may differ [100]. With regard to the data on neonatal mortality in France during the immunization campaign presented above, it may be objected that mortality peaks are not sustained : if nirsevimab were causing excess deaths, there should be a sustained spike rather than a fluctuating pattern. This can be explained by the hypothesis of early ADE occurring only at sub-neutralizing concentrations in rare individuals, due to inefficient biodistribution in the lungs in the first few days post-injection. Newborns affected by this ADE but who do not die immediately are less severely affected and are saved (to prove this, we would need access to data on ICU stays and the immunization status of patients).
6.2. Study of Nirsevimab Binding to FcγR In Vitro and Ex-Vivo and of Possible ADE in Animals by manufacturers.
As ADE occurs for mAbs through binding of virus-antibody complexes to Fc receptors (FcγR) on target cells, EMA prescribes the methods to be used to assess this risk. In vitro and ex-vivo cytotoxicity (ADCC), phagocytosis (ADCP antibody- dependent cellular phagocytosis) and complement activation must be explored. Preclinical in vitro and in vivo tests did not detect any effector functions of nirsevimab that might give rise to concern about ADE in humans. The analysis below will show why they were incomplete, as they were often carried out on mAbs close to but different from nirsevimab; preclinical trials with nirsevimab were largely published after the product’s approval [120].
6.2.1. In Vitro and Ex Vivo Studies
The conclusions of the EMA-EPAR [27] are contradictory when it comes to studying the effector functions of nirsevimab. For the EMA, nirsevimab should exhibit normal Fc-mediated effector functions (complement activation, mediation of phagocytosis, antibody-mediated destruction of virus-infected cells, etc.). Nirsevimab does not prevent virions from attaching to cells. The EMA considers that effector functions are not part of nirsevimab’s mechanism of action [27] (p.18), yet writes that the contribution of Fc-mediated effector functions to protection against RSV disease cannot be excluded - in the rapporteur’s opinion, preclinical data from the cotton rat model seem ambiguous in this respect [27], (p.15). Mechanisms other than virus neutralization would be necessary for the therapeutic effect, such as viral clearance and killing of infected cells [4]. The EMA reiterates the importance of studying effector functions for their involvement in a possible ADE [27], (p.29) (Fc effector functions are linked to the exacerbation of symptoms due to RSV [120,121]).
Before commercialization, the effector functions of nirsevimab were studied only in vitro or in cotton rats [20,122,123] and cynomolgus monkeys [70], and sometimes with a mAb different from nirsevimab. YTE mutations were shown to reduce FcγRIIIA binding by a factor of 2 (only with allotype F158), as well as ADCC (antibody- dependent cell-mediated cytotoxicity) activity by a factor of 100 [70]. This was confirmed in 2023 for ADCC in an in vitro study (on different human cell types). The EMA does not report any study of ADCC or the role of NK cells (which express only FcγRIIIA), which are nevertheless suspected of playing a primordial role in the balance between protection and pathology following the use of passive immunization [109,121]. Ex vivo (using sera from children participating in the nirsevimab clinical trial), the ADCC of NK cells mediated by FcγRIIIA (whose role is double-edged) is completely suppressed compared with that of palivizumab [120]. But it is known that the level of ADCC activity in vitro does not correlate with clinical symptoms in primary RSV infection, and the role of ADCC in the protection or pathogenesis of RSV infection remains to be determined [109,120]. This reduction in ADCC by nirsevimab could influence the therapeutic effect. Indeed, the role of FcγRIIIa would be double-edged: it may be pro-inflammatory and contribute to RSV disease, or it may be anti-inflammatory [102,103].
Nirsevimab binds to activating and inhibitory FcγRs and the result of these activating and inhibitory functions could vary according to the level of mAb present in the serum [120]. Ex vivo studies show that, at certain dilutions, nirsevimab may possess effector functions linked to the exacerbation of RSV symptoms [120] further underlining the importance of detailed pharmacokinetic studies. Dilution tests are performed on a pool of sera and do not sufficiently explore the influence of individual variations in nirsevimab concentration (the sera are collected 15 days after injection; analyses are performed on serum pools: 30 sera from treated participants are mixed, representing only 1.5% of the treated cohort). The results vary with serum dilutions, and only stand out from controls for certain dilutions. According to the authors, effector functions cannot be predicted beyond 150 days post-injection. Nirsevimab promotes beneficial ADNP (neutrophil phagocytosis), but neutrophilic inflammation with infiltration is also associated with severe RSV disease. At certain dilutions, nirsevimab amplifies phagocytosis by macrophages, which can be double-edged and requires further research. Complement deposition compared to placebo is strongly increased at certain dilutions. However, the authors do not anticipate any deleterious effect on this effector function in vivo, without further clarification. Complement-dependent cytotoxicity (CDC) is not studied, which is unfortunate as complement can have a protective or pathogenic role in viral infections [120] and particularly in RSV infections [121]. Experimental methods proposed in the past, (but overlooked) could be used to assess effector function of nirsevimab : as early as 1989, Gimenez describes an assay for evaluating ADE, which quantifies it by assessing the amount of virus released by a macrophagic line [71]. Gimenez [110] and Bournazos [103] also recall the gap between in vitro ADE assays and experimental in vivo systems.
Other specific studies should have been carried out in the presence of other antibodies, as neutralization and ADE activities are modified when two mAbs are mixed, and a synergistic ADE effect may occur in the presence of different antibodies [117]. The binding of mAbs to antigen can cause structural changes in the region where IgG binds to FcRn, and also in its interaction with complement [71,119]; antigen binding could modify Fc effector functions [100]. No trials have been carried out in the presence of immune complexes of nirsevimab bound to F protein or virus: all trials are performed in the absence of antigen. Binding to FcγRs depends on the conformational state of IgG (open or closed) [5]: a possible conformational change in nirsevimab when bound to F antigen or virus could alter its binding to FcγRIII and consequently its effector functions and hence its therapeutic effect.
The role of the glycosylation of nirsevimab on Fc binding has not been explored. According to EMA [27], nirsevimab is produced on CHO (Chinese hamsters ovary) cells and has a glycosylation site in the Fc domain (Asn-306) like most mAbs; this glycosylation is of the complex type (EPAR specifies that it has been characterized without further precision). mAbs produced from Chinese hamster CHO cell can produce afucosylated mAbs [124]. Glycosylation may play a role in mAb binding to FcRγ and C1q [125,126]. In particular, non-fucosylated IgGs bind more strongly to human FcγRIIIA and ADCC assays may show enhanced cytotoxicity [72]. Glycosylation of the Fc region affects mAb stability, and plays a role in CDC and ADCC functions by modulating binding to the Fcγ receptor [127]. Sialylation would not affect FcγRIIIa binding, but afucosylated IgG would have no ADCC activity [124,125]. Galactosylation of IgG1 positively influences C1q binding and CDC, and sialylation increases C1q binding of galactosylated IgG [125]. The glycosylation of nirsevimab should have been studied as well as its effect on the effector functions of the molecule [121].
mAbs with high anti-viral activity could contribute to inflammation in the advanced stages of the disease, which is probably why they are not used therapeutically [109]. This possible immune disruption [77,113,114,115] was not assessed in the trials. Yet there is a method for assessing the pro-inflammatory effect of immun-complexes (IgG binding to FcγRI) on a macrophagic line [128].
In vitro and ex vivo studies, albeit incomplete, show that nirsevimab has altered effector functions compared with other anti-RSV mAbs, particularly with regard to NK cytotoxic activity and phagocytosis by neutrophils and macrophages, as well as complement deposition (this is summarized in Figure 4). Increased binding to FcRn may disrupt the immune system: this risk has not been assessed. Many unknowns therefore remain, and it is a pity that some of the preclinical in vitro experiments were carried out only after the clinical trials, and were incomplete.
6.2.2. Animal Challenge Studies
During animal challenge studies, risk assessment should be carried out according to Munoz [129], as prescribed by EMA : all cases of vaccine failure should be investigated for VAERD, viral infection should be confirmed by detection and quantification of the virus in specific sites (blood, upper and lower respiratory tracts, tissues) as well as characterization and sequencing of the virus; the immune response should be assessed and compared (in the present case mAb levels should be measured). Deposits and consumption of complement should be detected. Tissues obtained by autopsy should be evaluated for evidence of immunopathology. Although these post-challenge checks have not been carried out, EMA concludes that ADE has not been observed in cotton rats, even at sub-effective doses [27].
In rat trials, it is necessary to use a mAb without YTE mutations, as these increase the affinity of FcRn in rats at neutral pH and suppress the protective effect of FcRn binding [4,120,122]. It is therefore difficult to extrapolate the results in these models to assess the absence of VAERD in humans. In the two studies with an antibody almost identical to nirsevimab (lacking the YTE mutations), pulmonary viral loads in cotton rats treated with the mAb and then challenged with RSV where greatly reduced compared with controls who had not received antibodies [4,120]. The authors conclude that these trials rule out the risk of ADE. However, we do not know what effect the increased affinity of YTE mutations would have on the viral loads. The reduction in viral loads does not depend on Fc effector functions [120], however, in humans, Fc effector functions are linked to exacerbation of RSV symptoms [5,101,121]. This calls into question the usefulness of ADE trials in rats. The effect of nirsevimab is being studied in cynomolgus monkeys, but they are not challenged with the virus, so the possible VAERD effect is not studied. No studies of ADE by immune system disruption have been carried. No histopathological evaluation was carried out in rats in the trials (in particular to look for alveolitis and neutrophilic infiltration, which are the signs of ADE in this animal model). Moreover, the animals used were not suitable for characterizing ADE. The EMA stresses that as the rats used in the studies were mature, the translability of the finding to highly immature infants is unknown [24]. The choice of animals to test for ADE is also problematic. In rats, effector functions are not necessary for protection against RSV infection, so the cotton rat model is not representative of human disease [120]. The animals usually used to study RSV (non-human primates, cotton rats, mice and lambs) are semi-permissive to virus replication and experimental infection. Only chimpanzees are completely permissive to RSV. Cynomolgus macaques do not usually produce signs of disease unless infected with a high titer inoculum. In the VAERD study in cynomolgus monkeys immunized with inactivated RSV virus, pulmonary pathology was not associated with increased viral replication, suggesting that the pathology was due to non-viral antigens. In cotton rats, too, the severity of alveolitis, used as a primary marker of VAERD with inactivated vaccine, depends on the response to non-viral antigens [130].
6.3. Clinical trials
In clinical trials, tissues obtained by autopsy or biopsy should also be evaluated for immunopathology evidence; chest computed tomography (CT) has a high sensitivity for diagnosis of lower respiratory tract disease involvement [129] and should have been performed on participants with RSV LRTI . This has not been done, EMA concludes however that ADE was not observed in clinical trials [27]. Moreover, respiratory infections not caused by RSV or not corresponding to the protocol have been neglected in clinical trials [20,23,26]. We found in the results of the immunization campaign that all-cause hospitalizations were not reduced compared with previous seasons.
7. Economic Benefits of Nirsevimab: Price and All-Cause Hospitalization Rates
The estimate of the comparative cost of nirsevimab immunization campaigns versus vaccination of mothers, based on product effectiveness, does not take into account all-cause hospitalizations. The price estimated to be profitable for society is lower than the price finally applied: Shoukat [131] proposes a price of $290 to make nirsevimab cost-effective, and the Canadian NACI [132] a price of $215 in a program aimed at all infants. However, the price set was higher in the USA ($495) [133] and was raised to $519.75 in April 2024 [134]. In France, the public price of nirsevimab was revealed in spring 2024 at €401.80 [135]. It was not public when the 2023 campaign was launched [136]. In Germany, the price was €1,350.03 until May 15, 2024, when it was reduced to €453.83 [137].
Neumann asks that the waning immunity and the possibility of emergence of resistant strains be taken into account in the real cost of nirsevimab (although Neumann, like the other authors, relies solely on effectiveness against hospitalizations due to RSV). Immunized children are protected from RSV for only 6 months; nirsevimab-resistant strains are beginning to emerge [133]. All studies conclude that the immunization program is cost-effective only if applied to at-risk infants. A price reduction of 80-88% has been proposed to make the all-infants seasonal nirsevimab program with catch-up cost-effective [138]. Thus, taking into account only the burden of RSV infections, the price of nirsevimab would be too high to make immunization of all newborns cost-effective. The stated aim of nirsevimab immunization campaigns is to reduce the burden on hospitals. As no reduction in all-cause hospitalizations is observed in the age group concerned by nirsevimab immunization, the cost-effectiveness of mass campaigns will be even more questionable.
8. Conclusion
Nirsevimab has been recommended in 2023 for all newborns and as a catch-up treatment for children during their first season of RSV circulation, with the aim of reducing the hospital burden due to infections. Based on clinical trials and published results from the first immunization campaign, it has been shown to be effective in reducing hospitalizations due to RSV (with the caveat that a large or unknown number of treated subjects were excluded in both clinical trials and post-marketing observational studies). But the overall burden on the hospital may not be reduced (all-cause hospitalizations are not reduced for infants and young children during the 2023-2024 season). This lack of net effect on the hospital’s overall burden may be attributed to the low share of RSV admissions in hospital admissions among under-5s. The results of the clinical studies show that the rare cases of hospitalization for LRTI due to RSV could have been more severe in treated participants, and that the exclusion of a non-negligible proportion of treated participants could also have masked part of this effect. The responsibility of nirsevimab cannot be excluded for the deaths observed in fragile children. As regards the results of post-marketing immunization campaigns, the almost systematic exclusion of neonates hospitalized in the days following injection cannot rule out an early ADE effect. Some post-marketing observational studies exclude early cases (between 1 and 7 days) of RSV infection after treatment, and when data on these cases are available, they show a spike in early respiratory infections. Similarly, the small but significant increase in the number of newborn deaths between 2 and 6 days of age during the campaign in France is a warning signal of a possible ADE, even if no causal link can be established.
This ADE is well known as a consequence of inactivated vaccines, and is due to antibodies against F-protein, against which nirsevimab is directed. Nirsevimab has a very high affinity for RSV F protein and FcRn. Binding to FcRn protects nirsevimab from degradation, but may also facilitate entry of the virus-antibody complex into cells expressing this receptor, particularly in the respiratory tract. This binding could be enhanced in certain individuals with acidic pH lung mucosa. The expansion of affinity for FcRn compared with the previously used mAb (palivizumab) could result in altered effector functions through binding to other FcγRs as well as to complement components. All these mechanisms have been proposed to explain ADE during RSV infection and this ADE has been shown in vitro on a monocyte line in the presence of anti-F antibodies. The early ADE effect in the days following injection may be due to sub-neutralizing concentrations of circulating anti-F antibody, which facilitates rather than blocks viral entry. Partial pharmacokinetic studies show this possibility. The lack of effect on all-cause hospitalizations could also be attributed to increased susceptibility to other infections, particularly respiratory. The immuno-disruptive effect of IgG1 binding to FcRn could explain the increased susceptibility to other respiratory infections. Preclinical and clinical studies should therefore have paid particular attention to this risk. In preclinical studies, the FcγR-mediated effector functions were incompletely evaluated, but showed that at certain dilutions nirsevimab may possess effector functions linked to the exacerbation of RSV symptoms. In clinical studies, RSV should have been systematically investigated in all participants, as should any immunopathological phenomena in hospitalized individuals (for RSV or not). In post-marketing studies, the immunization status of the subjects examined is not always known, and RSV testing is not systematically carried out in participants presenting a respiratory infection. The main bias of these studies lies in the exclusion of many subjects, particularly those who developed RSV infection within days of nirsevimab injection. Careful examination of the few data available suggests, however, that RSV infections are facilitated during this time interval (sub-neutralizing antibody concentrations may explain this phenomenon).
The strength of this study lies in the convergence of epidemiological and molecular arguments suggesting the possibility of nirsevimab-induced ADE. If this ADE exists, it is of low frequency: given the shortcomings of published studies, it is therefore impossible to assert or evaluate its occurrence, and this is the main limitation of this work.
For future campaigns, immunization status should be systematically collected and all children presenting with ARI should be tested for RSV. Immunopathological phenomena should be explored in all those presenting with RSV infection after immunization with nirsevimab. mAb levels should be measured in serum and bronchoalveolar lavage (where available). In case of autopsy, diffuse inflammation of the alveoli and infiltration by neutrophils and eosinophils should be sought. In premature or unhealthy infants, it should be verified that sub-neutralizing levels do not persist longer than in healthy, full-term neonates. Long-term follow-up of treated children is needed to verify that sub-neutralizing concentrations circulating in the season following injection are not capable of causing ADE in the longer term, even if nirsevimab is protective in the short term. Nirsevimab should not be recommended for all neonates until these verifications have been carried out. These checks will enable us to confirm that it is scientifically and economically reasonable to continue recommending immunization of all infants and young children for the following seasons. This expensive product could be reserved only for at-risk children.
Funding
This research received no external funding.
Informed Consent Statement
Not applicable
Acknowledgments
Christine Mackoi, data extraction-methodology-software-data curation. Dr Corinne Reverbel for the production of schematics
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
ADE: antibody dependent enhancement (of the infection)
ADCC : antibody- dependent cell-mediated cytotoxicity
ADCD antibody-dependent complement deposition
ADCP : antibody- dependent cellular phagocytosis
ADNKA antibody-dependent NK cell activation ADNP antibody-dependent neutrophil phagocytosis
APC : antigen presenting cell
ARR : absolute reduction risk
ASL : airway surface liquid
ARI : acute respiratory infection
CDC or CDCC : complement-dependent cytotoxicity
CDCP : complement-dependent cell-mediated phagocytosis
CR : complement receptors
EMA : European Medicines Agency
EPAR : European Public Assessment Report
ERD : enhanced respiratory disease
F : RSV membrane fusion protein
Fc : IgG crystallizable fragment
FcγR : IgG Fc receptor
FcRn : Fc neonatal receptor
IC : immune-complex
LRTI : low tract respiratory infection
mAb : monoclonal antibody
PICU : pediatric intensive care unit
RSV : respiratory syncytial virus
URTI : upper respiratory tract infection
VAED : Vaccine-associated enhanced disease, a form of ADE, antibody-dependent enhancement
VAERD : Vaccine-associated enhanced respiratory disease
References
- Li Y, Wang X, Blau DM, Caballero MT, Feikin DR, Gill CJ, Madhi SA, Omer SB, Simões EAF, Campbell H, Pariente AB, Bardach D, Bassat Q, Casalegno JS, Chakhunashvili G, Crawford N, Danilenko D, Do LAH, Echavarria M, Gentile A, Gordon A, Heikkinen T, Huang QS, Jullien S, Krishnan A, Lopez EL, Markić J, Mira-Iglesias A, Moore HC, Moyes J, Mwananyanda L, Nokes DJ, Noordeen F, Obodai E, Palani N, Romero C, Salimi V, Satav A, Seo E, Shchomak Z, Singleton R, Stolyarov K, Stoszek SK, von Gottberg A, Wurzel D, Yoshida LM, Yung CF, Zar HJ; Respiratory Virus Global Epidemiology Network; Nair H; RESCEU investigators. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: a systematic analysis. Lancet. 2022 May 28;399(10340):2047-2064. Available online: https://pubmed.ncbi.nlm.nih.gov/35598608/. [CrossRef] [PubMed]
- Rocca A, Biagi C, Scarpini S, Dondi A, Vandini S, Pierantoni L, Lanari M. Passive Immunoprophylaxis against Respiratory Syncytial Virus in Children: Where Are We Now? Int J Mol Sci. 2021 Apr 2;22(7):3703. [CrossRef] [PubMed]
- Osiowy C, Horne D, Anderson R. Antibody-dependent enhancement of respiratory syncytial virus infection by sera from young infants. Clin Diagn Lab Immunol. 1994 Nov;1(6):670-7. [CrossRef] [PubMed]
- Zhu Q, McLellan JS, Kallewaard NL, Ulbrandt ND, Palaszynski S, Zhang J, Moldt B, Khan A, Svabek C, McAuliffe JM, Wrapp D, Patel NK, Cook KE, Richter BWM, Ryan PC, Yuan AQ, Suzich JA. A highly potent extended half-life antibody as a potential RSV vaccine surrogate for all infants. Sci Transl Med. 2017 May 3;9(388):eaaj1928. [CrossRef] [PubMed]
- Acevedo OA, Díaz FE, Beals TE, Benavente FM, Soto JA, Escobar-Vera J, González PA, Kalergis AM. Contribution of Fcγ Receptor-Mediated Immunity to the Pathogenesis Caused by the Human Respiratory Syncytial Virus. Front Cell Infect Microbiol. 2019 Mar 29;9:75. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6450440/. [CrossRef] [PubMed]
- Diethelm-Varela B, Soto JA, Riedel CA, Bueno SM, Kalergis AM. New Developments and Challenges in Antibody-Based Therapies for the Respiratory Syncytial Virus. Infect Drug Resist. 2023 Apr 8;16:2061-2074. [CrossRef] [PubMed]
- Rigter A, Widjaja I, Versantvoort H, Coenjaerts FE, van Roosmalen M, Leenhouts K, Rottier PJ, Haijema BJ, de Haan CA. A protective and safe intranasal RSV vaccine based on a recombinant prefusion-like form of the F protein bound to bacterium-like particles. PLoS One. 2013 Aug 12;8(8):e71072. [CrossRef] [PubMed]
- Diez-DomingoJ,Sáez-LlorensX,Rodriguez-WeberMA,EpalzaC,ChatterjeeA, Chiu C-H, et al. Safety and immunogenicity of a ChAd155-vectored respiratory syncytial virus (RSV) vaccine in healthy RSV-seropositive children 12-23 months of age. J Infect Dis (2023) 227(11):1293–302. Available online: https://pubmed.ncbi.nlm.nih.gov/36484484/. [CrossRef]
- Stuart ASV, Virta M, Williams K, Seppa I, Hartvickson R, Greenland M, et al. Phase 1/2a safety and immunogenicity of an adenovirus 26 vector respiratory syncytial virus (RSV) vaccine encoding prefusion F in adults 18-50 years and RSV- seropositive children 12-24 months. J Infect Dis (2022) 227(1):71–82. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9796164/. [CrossRef]
- Karron RA, Luongo C, Mateo JS, Wanionek K, Collins PL, Buchholz UJ. Safety and immunogenicity of the respiratory syncytial virus vaccine RSV/DeltaNS2/ Delta1313/I1314L in RSV-seronegative children. J Infect Dis (2020) 222(1):82–91. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7199783/. [CrossRef]
- CunninghamCK,KarronRA,MuresanP,KellyMS,McFarlandEJ,PerlowskiC, et al. Evaluation of recombinant live-attenuated respiratory syncytial virus (RSV) vaccines RSV/deltaNS2/delta1313/I1314L and RSV/276 in RSV-seronegative children. J Infect Dis (2022) 226(12):2069–78. Available online: https://pubmed.ncbi.nlm.nih.gov/35732186/]. [CrossRef]
- Kampmann B, Madhi SA, Munjal I, Simões EAF, Pahud BA, Llapur C, Baker J, Pérez Marc G, Radley D, Shittu E, Glanternik J, Snaggs H, Baber J, Zachariah P, Barnabas SL, Fausett M, Adam T, Perreras N, Van Houten MA, Kantele A, Huang LM, Bont LJ, Otsuki T, Vargas SL, Gullam J, Tapiero B, Stein RT, Polack FP, Zar HJ, Staerke NB, Duron Padilla M, Richmond PC, Koury K, Schneider K, Kalinina EV, Cooper D, Jansen KU, Anderson AS, Swanson KA, Gruber WC, Gurtman A; MATISSE Study Group. Bivalent Prefusion F Vaccine in Pregnancy to Prevent RSV Illness in Infants. N Engl J Med. 2023 Apr 20;388(16):1451-1464. Available online: https://pubmed.ncbi.nlm.nih.gov/37018474/. [CrossRef] [PubMed]
- European Union Risk Management Plan (EU RMP) for Beyfortus® (Nirsevimab) 3 May 2021, Available online:. Available online: https://www.ema.europa.eu/en/documents/rmp-summary/beyfortus-epar-risk-management-plan_en.pdf (accessed on 25 April 2024).
- Article 14(9) EC-726/2004 of the European Parliament and of the Council of 31 March 2004 laying down Community procedures for the authorisation and supervision of medicinal products for human and veterinary use and establishing a European Medicines Agency. Available online: http://data.europa.eu/eli/reg/2004/726/oj.
- Suh M, Movva N, Jiang X, Bylsma LC, Reichert H, Fryzek JP, Nelson CB. Respiratory Syncytial Virus Is the Leading Cause of United States Infant Hospitalizations, 2009-2019: A Study of the National (Nationwide) Inpatient Sample. J Infect Dis. 2022 Aug 15;226(Suppl 2):S154-S163. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9377046/. [CrossRef] [PubMed]
- Nair H, Simões EA, Rudan I, Gessner BD, Azziz-Baumgartner E, Zhang JSF, Feikin DR, Mackenzie GA, Moiïsi JC, Roca A, Baggett HC, Zaman SM, Singleton RJ, Lucero MG, Chandran A, Gentile A, Cohen C, Krishnan A, Bhutta ZA, Arguedas A, Clara AW, Andrade AL, Ope M, Ruvinsky RO, Hortal M, McCracken JP, Madhi SA, Bruce N, Qazi SA, Morris SS, El Arifeen S, Weber MW, Scott JAG, Brooks WA, Breiman RF, Campbell H; Severe Acute Lower Respiratory Infections Working Group. Global and regional burden of hospital admissions for severe acute lower respiratory infections in young children in 2010: a systematic analysis. Lancet. 2013 Apr 20;381(9875):1380-1390. Available online: https://pubmed.ncbi.nlm.nih.gov/23369797/. [CrossRef] [PubMed]
- Del Riccio M, Spreeuwenberg P, Osei-Yeboah R, Johannesen CK, Fernandez LV, Teirlinck AC, Wang X, Heikkinen T, Bangert M, Caini S, Campbell H, Paget J; RESCEU Investigators. Burden of Respiratory Syncytial Virus in the European Union: estimation of RSV-associated hospitalizations in children under 5 years. J Infect Dis. 2023 Nov 28;228(11):1528-1538. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10681872/. [CrossRef] [PubMed]
- Bulletin Infections Respiratoires Aiguës, publié le 17 avril 2024. Available online: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-et-infections-respiratoires/grippe/documents/bulletin-national/infections-respiratoires-aigues-grippe-bronchiolite-covid-19-.-bilan-de-la-saison-2023-2024 (accessed on 22 April 2024).
- Suss RJ, Simões EAF. Respiratory Syncytial Virus Hospital-Based Burden of Disease in Children Younger Than 5 Years, 2015-2022. JAMA Netw Open. 2024 Apr 1;7(4):e247125. Available online: https://pubmed.ncbi.nlm.nih.gov/38635270/. [CrossRef] [PubMed]
- Domachowske JB, Khan AA, Esser MT, Jensen K, Takas T, Villafana T, Dubovsky F, Griffin MP. Safety, Tolerability and Pharmacokinetics of MEDI8897, an Extended Half-life Single-dose Respiratory Syncytial Virus Prefusion F-targeting Monoclonal Antibody Administered as a Single Dose to Healthy Preterm Infants. Pediatr Infect Dis J. 2018 Sep;37(9):886-892. [CrossRef] [PubMed]
- Griffin MP, Khan AA, Esser MT, Jensen K, Takas T, Kankam MK, Villafana T, Dubovsky F. Safety, Tolerability, and Pharmacokinetics of MEDI8897, the Respiratory Syncytial Virus Prefusion F-Targeting Monoclonal Antibody with an Extended Half-Life, in Healthy Adults. Antimicrob Agents Chemother. 2017 Feb 23;61(3):e01714-16. [CrossRef] [PubMed]
- Hammitt LL, Dagan R, Yuan Y, Baca Cots M, Bosheva M, Madhi SA, Muller WJ, Zar HJ, Brooks D, Grenham A, Wählby Hamrén U, Mankad VS, Ren P, Takas T, Abram ME, Leach A, Griffin MP, Villafana T; MELODY Study Group. Nirsevimab for Prevention of RSV in Healthy Late-Preterm and Term Infants. N Engl J Med. 2022 Mar 3;386(9):837-846. Available online: https://pubmed.ncbi.nlm.nih.gov/35235726/. [CrossRef] [PubMed]
- Domachowske J, Madhi SA, Simões EAF, Atanasova V, Cabañas F, Furuno K, Garcia-Garcia ML, Grantina I, Nguyen KA, Brooks D, Chang Y, Leach A, Takas T, Yuan Y, Griffin MP, Mankad VS, Villafana T; MEDLEY Study Group. Safety of Nirsevimab for RSV in Infants with Heart or Lung Disease or Prematurity. N Engl J Med. 2022 Mar 3;386(9):892-894. Available online: https://pubmed.ncbi.nlm.nih.gov/35235733/. [CrossRef] [PubMed]
- Simões EAF, Madhi SA, Muller WJ, Atanasova V, Bosheva M, Cabañas F, Baca Cots M, Domachowske JB, Garcia-Garcia ML, Grantina I, Nguyen KA, Zar HJ, Berglind A, Cummings C, Griffin MP, Takas T, Yuan Y, Wählby Hamrén U, Leach A, Villafana T. Efficacy of nirsevimab against respiratory syncytial virus lower respiratory tract infections in preterm and term infants, and pharmacokinetic extrapolation to infants with congenital heart disease and chronic lung disease: a pooled analysis of randomised controlled trials. Lancet Child Adolesc Health. 2023 Mar;7(3):180-189. Available online: https://pubmed.ncbi.nlm.nih.gov/36634694/. [CrossRef] [PubMed]
- Drysdale SB, Cathie K, Flamein F, Knuf M, Collins AM, Hill HC, Kaiser F, Cohen R, Pinquier D, Felter CT, Vassilouthis NC, Jin J, Bangert M, Mari K, Nteene R, Wague S, Roberts M, Tissières P, Royal S, Faust SN; HARMONIE Study Group. Nirsevimab for Prevention of Hospitalizations Due to RSV in Infants. N Engl J Med. 2023 Dec 28;389(26):2425-2435. Available online: https://pubmed.ncbi.nlm.nih.gov/38157500/. [CrossRef] [PubMed]
- Griffin MP, Yuan Y, Takas T, Domachowske JB, Madhi SA, Manzoni P, Simões EAF, Esser MT, Khan AA, Dubovsky F, Villafana T, DeVincenzo JP; Nirsevimab Study Group. Single-Dose Nirsevimab for Prevention of RSV in Preterm Infants. N Engl J Med. 2020 Jul 30;383(5):415-425. Erratum in: N Engl J Med. 2020 Aug 13;383(7):698. Available online: https://pubmed.ncbi.nlm.nih.gov/32726528/. [CrossRef] [PubMed]
- EMA-EPAR Beyfortus-Nirsevimab, Available on line : https://www.ema.europa.eu/en/medicines/human/EPAR/beyfortus#assessment-history https://web.archive.org/web/20240105135355/ https://www.ema.europa.eu/en/medicines/human/EPAR/beyfortus#assessment-history (accessed on April 15, 2024). Available online :.
- HAS nirsevimab Transparency Committee, , accessed April 22, 2024 https://www.has-sante.fr/plugins/ModuleXitiKLEE/types/FileDocument/doXiti.jsp?id=p_3476336 https://web.archive.org/web/20240104100601/https://www.has-sante.fr/upload/docs/application/pdf/2023-11/beyfortus_19072023_summary_ct20356_en.
- Sullivan K, Sullivan B. Does nirsevimab prevent lower respiratory infections caused by respiratory syncytial virus? J Perinatol. 2024 May;44(5):767-769. Available online: https://pubmed.ncbi.nlm.nih.gov/38637681/. [CrossRef] [PubMed]
- Biologics License Application (BLA) 761328 Nirsevimab Antimicrobial Drugs Advisory Committee Meeting , 2023 Division of Antivirals, Office of Infectious Diseases Center for Drug Evaluation and Research, accessed April 13,2024. Available online: https://www.fda.gov/media/169322/download https://web.archive (accessed on 13 April 2024).
- EudraVigilance European database of suspected adverse drug reaction reports. 15 April. Available online: https://www.adrreports.eu/fr/eudravigilance.html (accessed on 15 April 2024).
- Pharmacovigilance d’Île de France, campagne d’immunisation contre le VRS-Beyfortus, 31 janvier 2024, accessed ,2024 https://www.pharmacovigilance-iledefrance.fr/d%C3%A9tails-dune-br%C3%A8ve/campagne-dimmunisation-contre-le-vrs-beyfortus-nirs%C3%A9vimab https://web.archive.org/web/20240223011807/ https://www.pharmacovigilance-iledefrance.
- US-FDA FDA Approves New Drug to Prevent RSV in Babies and Toddlers, Available on line : https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-prevent-rsv-babies-and-toddlers https://web.archive.org/web/20230801224229/https://www.fda.
- Jones JM, Fleming-Dutra KE, Prill MM, et al. Use of Nirsevimab for the Prevention of Respiratory Syncytial Virus Disease Among Infants and Young Children: Recommendations of the Advisory Committee on Immunization Practices — United States, 2023. MMWR Morb Mortal Wkly Rep 2023;72:920–925. [CrossRef]
- Sánchez Luna M, Fernández Colomer B, Couce Pico ML; en representación de la Junta Directiva de la Sociedad española de Neonatología SENEO Comisión de Infecciones SENEO y Comisión de Estándares de SENEO. Recommendations of the Spanish Society of Neonatology for the prevention of severe respiratory syncytial virus infections with nirsevimab, for the 2023-2024 season. An Pediatr (Engl Ed). 2023 Oct;99(4):264-265. Available online: https://pubmed.ncbi.nlm.nih.gov/37739825/. [CrossRef] [PubMed]
- New immunisation to protect newborns and young children against bronchiolitis, The Luxembourg Governement press release, , 2023 accessed May 17, 2024. https://gouvernement.lu/en/actualites/toutes_actualites/communiques/2023/09-septembre/22-immunisation-bronchiolite-nourrissons.html https://web.archive.org/web/20230922222249/https://gouvernement.lu/en/actualites/toutes_actualites/communiques/2023/09-septembre/22-immunisation-bronchiolite-nourrissons.
- CDC, Nirsevimab Coverage, Children 0 to 19 months, United States, Data are current through February 29, 2024. Available online: https://www.cdc.gov/vaccines/imz-managers/coverage/rsvvaxview/nirsevimab-coverage-children-0-19months.
- RSV-NET Interactive Dashboard, CDC, Available on line. Available online: https://www.cdc.gov/rsv/research/rsv-net/dashboard.html (accessed on 15 May 2024).
- Moline HL et al., Early Estimate of Nirsevimab Effectiveness for Prevention of Respiratory Syncytial Virus–Associated Hospitalization Among Infants Entering Their First Respiratory Syncytial Virus Season — New Vaccine Surveillance Network, October 2023–February 2024. Available online: https://www.cdc.gov/mmwr/volumes/73/wr/mm7309a4.htm?s_cid=mm7309a4_w.
- Setia MS. Methodology Series Module 2: Case-control Studies. Indian J Dermatol. 2016 Mar-Apr;61(2):146-51. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4817437/. [CrossRef] [PubMed]
- Ernst C, Bejko D, Gaasch L, Hannelas E, Kahn I, Pierron C, Del Lero N, Schalbar C, Do Carmo E, Kohnen M, Andlauer E, Hublart P, Masi S, de la Fuente Garcia I, Vergison A, Mossong J. Impact of nirsevimab prophylaxis on paediatric respiratory syncytial virus (RSV)-related hospitalisations during the initial 2023/24 season in Luxembourg. Euro Surveill. 2024 Jan;29(4):2400033. [CrossRef] [PubMed]
- Assad Z, Romain AS, Aupiais C, Shum M, Schrimpf C, Lorrot M, Corvol H, Prevost B, Ferrandiz C, Giolito A, Valtuille Z, Bendavid M, Cohen JF, Toubiana J, de Pontual L, Delande CF, Levy M, See P, Cohen R, Levy C, Angoulvant F, Lenglart L, Gits-Muselli M, Biran V, Diallo K, Alemede O, El Hebil MM, Durrmeyer X, Labouret G, Casanovas N, Hallak B, Maréchal O, Jung C, Bréhin C, Ouldali N. Nirsevimab and Hospitalization for RSV Bronchiolitis. N Engl J Med. 2024 Jul 11;391(2):144-154. Available online: https://pubmed.ncbi.nlm.nih.gov/38986058/. [CrossRef] [PubMed]
- EPI-PHARE Utilisation du Nirsévimab (Beyfortus®) en ville en France lors de la première campagne de prévention (saison 2023/2024) April 8, 2024. Available online: https://www.epi-phare.fr/rapports-detudes-et-publications/utilisation-beyfortus/ (accessed on 3 June 2024).
- Bronchiolite : bilan de la surveillance hivernale 2022-2023, Santé Publique France, July 19, 2023. Available online: https://www.santepubliquefrance.fr/les-actualites/2023/bronchiolite-bilan-de-la-surveillance-hivernale-2022-2023 (accessed on 1 May 2024).
- Paireau J., Durand C., Raimbault S., Cazaubon J., Mortamet G., et al.. Nirsevimab effectiveness against cases of respiratory syncytial virus bronchiolitis hospitalised in pediatric intensive care units in France, September 2023 -January 2024. 2024. pasteur-04501286. Available online: https://hal.science/pasteur-04501286 (accessed on 12 March 2024).
- Vaux S, Viriot D, Forgeot C, Pontais I, Savitch Y, Barondeau-Leuret A, Smadja S, Valette M, Enouf V, Parent du Chatelet I. Bronchiolitis epidemics in France during the SARS-CoV-2 pandemic: The 2020-2021 and 2021-2022 seasons. Infect Dis Now. 2022 Sep;52(6):374-378. Available online: https://pubmed.ncbi.nlm.nih.gov/35753628/. [CrossRef] [PubMed]
- Delestrain C, Danis K, Hau I, Behillil S, Billard MN, Krajten L, Cohen R, Bont L, Epaud R. Impact of COVID-19 social distancing on viral infection in France: A delayed outbreak of RSV. Pediatr Pulmonol. 2021 Dec;56(12):3669-3673. Available online: https://pubmed.ncbi.nlm.nih.gov/34473914/. [CrossRef] [PubMed]
- International Classification of Diseases, Tenth Revision, International Statistical Classification of Diseases and Related Health Problems 10th Revision latest version 2019, WHO. Available online: https://icd.who.int/browse10/2019/en (accessed on 12 May 2024).
- La sanidad pública paga 209 euros por cada vacuna infantil contra la bronquiolitis, Civio, October 30, 2023. Available online: https://civio.es/medicamentalia/2023/10/30/nirsevimab-beyfortus-precio-virus-respiratorio-sincitial/.
- Servicio Andaluz de Salud, El Distrito Serranía recibe un reconocimiento por la cobertura de la vacuna combinada frente a difteria, tétanos, tosferina y poliomielitis 30 January 2024, Available online : https://www.sspa.juntadeandalucia.es/servicioandaluzdesalud/todas-noticia/el-distrito-serrania-recibe-un-reconocimiento-por-la-cobertura-de-la-vacuna-combinada-frente https://web.archive.org/web/20240602170353/ https://www.sspa.juntadeandalucia.es/servicioandaluzdesalud/todas-noticia/el-distrito-serrania-recibe-un-reconocimiento-por-la-cobertura-de-la-vacuna-combinada-frente accessed February 10 2024.
- Administradas 452.000 vacunas por virus respiratorios, Ondacero.es ; April 8,2024, Available on line : https://www.ondacero.es/emisoras/asturias/noticias/administradas-452000-vacunas-virus-respiratorios_202404086613a4ec099903000111cfb3.html https://web.archive.org/web/20240602170546/ https://www.ondacero.es/emisoras/asturias/noticias/administradas-452000-vacunas-virus-respiratorios_202404086613a4ec099903000111cfb3.html accessed April 23, 2024.
- La Comunidad de Madrid reduce un 90% los ingresos hospitalarios de menores de un año tras incorporar la vacuna contra la bronquiolitis, Communiqué de presse de la Comunidad de Madrid, April 16,2024, Available on line : https://www.comunidad.madrid/notas-prensa/2024/04/16/comunidad-madrid-reduce-90-ingresos-hospitalarios-menores-ano-incorporar-vacuna-bronquiolitis https://web.archive.org/web/20240602170719/ https://www.comunidad.madrid/notas-prensa/2024/04/16/comunidad-madrid-reduce-90-ingresos-hospitalarios-menores-ano-incorporar-vacuna-bronquiolitis accessed April 23,2024.
- Ministerio de ciencia, innovacion y universidades, Gobierno de Espana, Informes semanales de vigilancia centinela de IRAs y de IRAG: Gripe, Covid-19 y otros virus respiratorios, Available on line : https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Paginas/VIGILANCIA-CENTINELA-DE-INFECCION-RESPIRATORIA-AGUDA.aspx https://web.archive.org/web/20240122052000/ https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/GRIPE/Informes%20semanales/Temporada_2023-24/Informe%20semanal_SiVIRA_022024.pdf https://web.archive.org/web/20230316142333/ https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/GRIPE/Informes%20semanales/Temporada_2022-23/Informe%20semanal_SiVIRA_102023.pdf accessed April 23, 2024.
- FOLLOW-UP REPORT ON IMMUNIZATION WITH NIRSEVIMAB IN GALICIA Dirección Xeral de Saúde Pública Data up to week 13, 2024 (31-03-2024), Available online : https://www.nirsegal.es/en https://web.archive.org/web/20240409062929/ https://assets-global.website-files.com/65774b0d3a50ee58b24dba82/660e95b8142542e4cae669d2_Report_RSV_week13.pdf accessed April 23, 2024.
- Ares-Gómez S, Mallah N, Santiago-Pérez MI, Pardo-Seco J, Pérez-Martínez O, Otero-Barrós MT, Suárez-Gaiche N, Kramer R, Jin J, Platero-Alonso L, Alvárez-Gil RM, Ces-Ozores OM, Nartallo-Penas V, Mirás-Carballal S, Piñeiro-Sotelo M, Malvar-Pintos A, González-Pérez JM, Rodríguez-Tenreiro-Sánchez C, Rivero-Calle I, Salas A, Durán-Parrondo C, Martinón-Torres F; NIRSE-GAL study group. Effectiveness and impact of universal prophylaxis with nirsevimab in infants against hospitalisation for respiratory syncytial virus in Galicia, Spain: initial results of a population-based longitudinal study. Lancet Infect Dis. 2024 Apr 30:S1473-3099(24)00215-9. Available online: https://pubmed.ncbi.nlm.nih.gov/38701823/. [CrossRef] [PubMed]
- Evaluation of the Effectiveness and Impact of Nirsevimab Administered as Routine Immunization (NIRSE-GAL), accessed May 10, 2024. https://classic.clinicaltrials.gov/ct2/show/NCT06180993 https://web.archive.org/web/20240602172604/https://classic.clinicaltrials.gov/ct2/show/NCT06180993.
- Ezpeleta G, Navascués A, Viguria N, Herranz-Aguirre M, Juan Belloc SE, Gimeno Ballester J, Muruzábal JC, García-Cenoz M, Trobajo-Sanmartín C, Echeverria A, Martínez-Baz I, Vera-Punzano N, Casado I, López-Mendoza H, Ezpeleta C, Castilla J. Effectiveness of Nirsevimab Immunoprophylaxis Administered at Birth to Prevent Infant Hospitalisation for Respiratory Syncytial Virus Infection: A Population-Based Cohort Study. Vaccines (Basel). 2024 Apr 4;12(4):383. Available online: https://pubmed.ncbi.nlm.nih.gov/38675765/. [CrossRef] [PubMed]
- Boletin de Salud Publica de Navarra, n°126, September 2023, Available on line http://www.navarra.es/home_es/Gobierno+de+Navarra/Organigrama/Los+departamentos/Salud/Organigrama/Estructura+Organica/Instituto+Navarro+de+Salud+Publica/Publicaciones/Publicaciones+profesionales/Epidemiologia/Boletin+ISP.htm https://web.archive.org/web/20231129071427/ http://www.navarra.es/NR/rdonlyres/AECCD760-AB2A-4841-818A-FA53478FD6DC/488194/BOL126INT1.pdf accessed May 1, 2024.
- DGS-URGENT 9, 08/24/2023, DGS-URGENT N°2023_14, PREVENTION MEDICAMENTEUSE DES BRONCHIOLITES A VRS A PARTIR DE SEPTEMBRE accessed August 30, 2023. https://sante.gouv.fr/IMG/pdf/dgs-urgent_2023-14_-_traitement_preventif_vrs.pdf https://web.archive.org/web/20240202032041/https://sante.gouv.fr/IMG/pdf/dgs-urgent_2023-14_-_traitement_preventif_vrs.
- DREES, La Naissance : caractéristiques des accouchements, Available online: https://drees.solidarites-sante.gouv.fr/sites/default/files/2021-07/Fiche%2024%20-%20La%20naissance%20-%20caract%C3%A9ristiques%20des%20accouchements.pdf https://web.archive.org/web/20231206003500/ https://drees.solidarites-sante.gouv.fr/sites/default/files/2021-07/Fiche%2024%20-%20La%20naissance%20-%20caractéristiques%20des%20accouchements.pdf accessed April 23, 2024.
- INSEE Décès et Mortalité, Available online : https://www.insee.fr/fr/statistiques/7767420?sommaire=7764286 et https://www.insee.fr/fr/statistiques/6959517?sommaire=4487854 , accessed April 30, 2024.
- Nombre mensuel de naissances (de janvier 2015 à octobre 2023), Available on line : https://www.insee.fr/fr/statistiques/7758827?sommaire=5348638 et https://www.insee.fr/fr/statistiques/8064935?sommaire=7944361 , accessed April 30,2024.
- Journal Officiel, France, 12/231/2023. Available online: https://www.senat.fr/questions/jopdf/2023/2023-12-21_seq_20230050_0001_p000.pdf (accessed on 3 June 2024).
- DGS Beyfortus, fin de la campagne de distribution, 12/26/2023, reference MARS n° 2023-23, limited diffusion. Available online: https://sante.gouv.fr/professionnels/article/dgs-urgent (accessed on 12 January 2024).
- COUR DES COMPTES 06.05.2024 La politique de périnatalité, p.37. Available online: https://www.ccomptes.fr/fr/publications/la-politique-de-perinatalite (accessed on 6 August 2024).
- Sanders SL, Agwan S, Hassan M, van Driel ML, Del Mar CB. Immunoglobulin treatment for hospitalised infants and young children with respiratory syncytial virus infection. Cochrane Database Syst Rev. 2019. [CrossRef]
- Resch, B. Product review on the monoclonal antibody palivizumab for prevention of respiratory syncytial virus infection. Hum Vaccin Immunother. 2017 Sep 2;13(9):2138-2149. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5612471/. [CrossRef] [PubMed]
- Roopenian DC, Akilesh S. FcRn: the neonatal Fc receptor comes of age. Nat Rev Immunol. 2007 Sep;7(9):715-25. Available online: https://pubmed.ncbi.nlm.nih.gov/17703228/. [CrossRef] [PubMed]
- Patel DD, Bussel JB. Neonatal Fc receptor in human immunity: Function and role in therapeutic intervention. J Allergy Clin Immunol. 2020 Sep;146(3):467-478. Available online: https://pubmed.ncbi.nlm.nih.gov/32896307/. [CrossRef] [PubMed]
- Dall’Acqua WF, Kiener PA, Wu H. Properties of human IgG1s engineered for enhanced binding to the neonatal Fc receptor (FcRn). J Biol Chem. 2006 Aug 18;281(33):23514-24. Available online: https://pubmed.ncbi.nlm.nih.gov/16793771/. [CrossRef] [PubMed]
- Qi T, Cao Y. In Translation: FcRn across the Therapeutic Spectrum. Int J Mol Sci. 2021 Mar 17;22(6):3048. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8002405/. [CrossRef] [PubMed]
- Spiekermann GM, Finn PW, Ward ES, Dumont J, Dickinson BL, Blumberg RS, Lencer WI. Receptor-mediated immunoglobulin G transport across mucosal barriers in adult life: functional expression of FcRn in the mammalian lung. J Exp Med. 2002 Aug 5;196(3):303-10. Erratum in: J Exp Med. 2003 Jun 2;197(11):1601. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2193935/. [CrossRef] [PubMed]
- Pyzik M, Sand KMK, Hubbard JJ, Andersen JT, Sandlie I, Blumberg RS. The Neonatal Fc Receptor (FcRn): A Misnomer? Front Immunol. 2019 Jul 10;10:1540. [CrossRef] [PubMed]
- Schlachetzki F, Zhu C, Pardridge WM. Expression of the neonatal Fc receptor (FcRn) at the blood-brain barrier. J Neurochem. 2002 Apr;81(1):203-6. [CrossRef] [PubMed]
- Kim KJ, Fandy TE, Lee VH, Ann DK, Borok Z, Crandall ED. Net absorption of IgG via FcRn-mediated transcytosis across rat alveolar epithelial cell monolayers. Am J Physiol Lung Cell Mol Physiol. 2004 Sep;287(3):L616-22. Available online: https://pubmed.ncbi.nlm.nih.gov/15169676/. [CrossRef] [PubMed]
- Pyzik M, Kozicky LK, Gandhi AK, Blumberg RS. The therapeutic age of the neonatal Fc receptor. Nat Rev Immunol. 2023 Jul;23(7):415-432. Available online: https://pubmed.ncbi.nlm.nih.gov/36726033/. [CrossRef] [PubMed]
- Pyzik M, Rath T, Lencer WI, Baker K, Blumberg RS. FcRn: The Architect Behind the Immune and Nonimmune Functions of IgG and Albumin. J Immunol. 2015 May 15;194(10):4595-603. [CrossRef] [PubMed]
- Fischer, H. Function of Proton Channels in Lung Epithelia. Wiley Interdiscip Rev Membr Transp Signal. 2012 May;1(3):247-258. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3362208/. [CrossRef] [PubMed]
- Garland AL, Walton WG, Coakley RD, Tan CD, Gilmore RC, Hobbs CA, Tripathy A, Clunes LA, Bencharit S, Stutts MJ, Betts L, Redinbo MR, Tarran R. Molecular basis for pH-dependent mucosal dehydration in cystic fibrosis airways. Proc Natl Acad Sci U S A. 2013 Oct 1;110(40):15973-8. Available online: https://pubmed.ncbi.nlm.nih.gov/24043776/. [CrossRef] [PubMed]
- Abou Alaiwa MH, Beer AM, Pezzulo AA, Launspach JL, Horan RA, Stoltz DA, Starner TD, Welsh MJ, Zabner J. Neonates with cystic fibrosis have a reduced nasal liquid pH; a small pilot study. J Cyst Fibros. 2014 Jul;13(4):373-7. Available online: https://pubmed.ncbi.nlm.nih.gov/24418186/. [CrossRef] [PubMed]
- Schultz A, Puvvadi R, Borisov SM, Shaw NC, Klimant I, Berry LJ, Montgomery ST, Nguyen T, Kreda SM, Kicic A, Noble PB, Button B, Stick SM. Airway surface liquid pH is not acidic in children with cystic fibrosis. Nat Commun. 2017 Nov 10;8(1):1409. Available online: https://pubmed.ncbi.nlm.nih.gov/29123085/. [CrossRef] [PubMed]
- Challa DK, Wang X, Montoyo HP, Velmurugan R, Ober RJ, Ward ES. Neonatal Fc receptor expression in macrophages is indispensable for IgG homeostasis. MAbs. 2019 Jul;11(5):848-860. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6601554/. [CrossRef] [PubMed]
- Ye L, Zeng R, Bai Y, Roopenian DC, Zhu X. Efficient mucosal vaccination mediated by the neonatal Fc receptor. Nat Biotechnol. 2011 Feb;29(2):158-63. Available online: https://pubmed.ncbi.nlm.nih.gov/21240266/. [CrossRef] [PubMed]
- Zhao X, Zhang G, Liu S, Chen X, Peng R, Dai L, Qu X, Li S, Song H, Gao Z, Yuan P, Liu Z, Li C, Shang Z, Li Y, Zhang M, Qi J, Wang H, Du N, Wu Y, Bi Y, Gao S, Shi Y, Yan J, Zhang Y, Xie Z, Wei W, Gao GF. Human Neonatal Fc Receptor Is the Cellular Uncoating Receptor for Enterovirus B. Cell. 2019 ;177(6):1553-1565.e16. Available online: https://pubmed.ncbi.nlm.nih.gov/31104841/. [CrossRef] [PubMed]
- Morosky S, Wells AI, Lemon K, Evans AS, Schamus S, Bakkenist CJ, Coyne CB. The neonatal Fc receptor is a pan-echovirus receptor. Proc Natl Acad Sci U S A. 2019 Feb 26;116(9):3758-3763. Available online: https://pubmed.ncbi.nlm.nih.gov/30808762/. [CrossRef] [PubMed]
- Burstin SJ, Brandriss MW, Schlesinger JJ. Infection of a macrophage-like cell line, P388D1 with reovirus; effects of immune ascitic fluids and monoclonal antibodies on neutralization and on enhancement of viral growth. J Immunol. 1983 Jun;130(6):2915-9. [PubMed]
- Maidji E, McDonagh S, Genbacev O, Tabata T, Pereira L. Maternal antibodies enhance or prevent cytomegalovirus infection in the placenta by neonatal Fc receptor-mediated transcytosis. Am J Pathol. 2006 Apr;168(4):1210-26. [CrossRef] [PubMed]
- Gupta S, Gach JS, Becerra JC, Phan TB, Pudney J, Moldoveanu Z, Joseph SB, Landucci G, Supnet MJ, Ping LH, Corti D, Moldt B, Hel Z, Lanzavecchia A, Ruprecht RM, Burton DR, Mestecky J, Anderson DJ, Forthal DN. The Neonatal Fc receptor (FcRn) enhances human immunodeficiency virus type 1 (HIV-1) transcytosis across epithelial cells. PLoS Pathog. 2013;9(11):e1003776. Erratum in: PLoS Pathog. 2013 Nov;9(11). [CrossRef] [PubMed]
- Gupta S, Pegu P, Venzon DJ, Gach JS, Ma ZM, Landucci G, Miller CJ, Franchini G, Forthal DN. Enhanced in vitro transcytosis of simian immunodeficiency virus mediated by vaccine-induced antibody predicts transmitted/founder strain number after rectal challenge. J Infect Dis. 2015 Jan 1;211(1):45-52. [CrossRef] [PubMed]
- Taylor A, Foo SS, Bruzzone R, Dinh LV, King NJ, Mahalingam S. Fc receptors in antibody-dependent enhancement of viral infections. Immunol Rev. 2015 Nov;268(1):340-64. [CrossRef] [PubMed]
- Banoun, H. Measles and Antibody-Dependent Enhancement (ADE): History and Mechanisms. Explor Res Hypothesis Med. 2022;7(4):246-252. Available online: https://www.xiahepublishing.com/2472-0712/ERHM-2022-00018. [CrossRef]
- Tirado SM, Yoon KJ. Antibody-dependent enhancement of virus infection and disease. Viral Immunol. 2003;16(1):69-86. Available online: https://pubmed.ncbi.nlm.nih.gov/12725690/. [CrossRef] [PubMed]
- van Mechelen L, Luytjes W, de Haan CA, Wicht O. RSV neutralization by palivizumab, but not by monoclonal antibodies targeting other epitopes, is augmented by Fc gamma receptors. Antiviral Res. 2016 Aug;132:1-5. Available online: https://pubmed.ncbi.nlm.nih.gov/27185625/. [CrossRef] [PubMed]
- Jang MJ, Kim YJ, Hong S, Na J, Hwang JH, Shin SM, Ahn YM. Positive association of breastfeeding on respiratory syncytial virus infection in hospitalized infants: a multicenter retrospective study. Clin Exp Pediatr. 2020 Apr;63(4):135-140. [CrossRef] [PubMed]
- Pasittungkul S, Thongpan I, Vichaiwattana P, Thongmee T, Klinfueng S, Suntronwong N, Wanlapakorn N, Vongpunsawad S, Poovorawan Y. High seroprevalence of antibodies against human respiratory syncytial virus and evidence of respiratory syncytial virus reinfection in young children in Thailand. Int J Infect Dis. 2022 Dec;125:177-183. [CrossRef] [PubMed]
- Barr FE, Pedigo H, Johnson TR, Shepherd VL. Surfactant protein-A enhances uptake of respiratory syncytial virus by monocytes and U937 macrophages. Am J Respir Cell Mol Biol. 2000 Nov;23(5):586-92. [CrossRef] [PubMed]
- Polack FP, Alvarez-Paggi D, Libster R, Caballero MT, Blair RV, Hijano DR, de la Iglesia Niveyro PX, Menendez DR, Gladwell W, Avendano LM, Velozo L, Wanek A, Bergel E, Prince GA, Kleeberger SR, Johnson J, Pociask D, Kolls JK. Fatal enhanced respiratory syncytial virus disease in toddlers. Sci Transl Med. 2021 Oct 20;13(616):eabj7843. Available online: https://pubmed.ncbi.nlm.nih.gov/34669442/. [CrossRef] [PubMed]
- Xu L, Ma Z, Li Y, Pang Z, Xiao S. Antibody dependent enhancement: Unavoidable problems in vaccine development. Adv Immunol 2021;151:99–133. [CrossRef] [PubMed]
- von Kietzell K, Pozzuto T, Heilbronn R, Grössl T, Fechner H, Weger S. Antibody-mediated enhancement of parvovirus B19 uptake into endothelial cells mediated by a receptor for complement factor C1q. J Virol 2014;88(14):8102–8115. [CrossRef] [PubMed]
- Crowe JE, Jr. Human Antibodies for Viral Infections. Annu Rev Immunol. 2022 Apr 26;40:349-386. Available online: https://pubmed.ncbi.nlm.nih.gov/35113730/. [CrossRef] [PubMed]
- Polack FP, Teng MN, Collins PL, Prince GA, Exner M, Regele H, et al. A role for immune complexes in enhanced respiratory syncytial virus disease. J Exp Med (2002) 196(6):859–65. [CrossRef]
- Golebski K, Hoepel W, van Egmond D, de Groot EJ, Amatngalim GD, Beekman JM, Fokkens WJ, van Drunen CM, den Dunnen J. FcγRIII stimulation breaks the tolerance of human nasal epithelial cells to bacteria through cross-talk with TLR4. Mucosal Immunol. 2019 Mar;12(2):425-433. Available online: https://pubmed.ncbi.nlm.nih.gov/30664707/. [CrossRef] [PubMed]
- Bournazos S, Gupta A, Ravetch JV. The role of IgG Fc receptors in antibody-dependent enhancement. Nat Rev Immunol. 2020 Oct;20(10):633-643. [CrossRef] [PubMed]
- Halstead SB, Venkateshan CN, Gentry MK, Larsen LK. Heterogeneity of infection enhancement of dengue 2 strains by monoclonal antibodies. J Immunol. 1984 Mar;132(3):1529-32. Available online: https://pubmed.ncbi.nlm.nih.gov/6607288/. [PubMed]
- Thomas S, Smatti MK, Ouhtit A, Cyprian FS, Almaslamani MA, Thani AA, Yassine HM. Antibody-Dependent Enhancement (ADE) and the role of complement system in disease pathogenesis. Mol Immunol. 2022 Dec;152:172-182. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9647202/. [CrossRef] [PubMed]
- Cirino NM, Panuska JR, Villani A, Taraf H, Rebert NA, Merolla R, Tsivitse P, Gilbert IA. Restricted replication of respiratory syncytial virus in human alveolar macrophages. J Gen Virol. 1993 Aug;74 ( Pt 8):1527-37. [CrossRef] [PubMed]
- Makris S, Bajorek M, Culley FJ, Goritzka M, Johansson C. Alveolar Macrophages Can Control Respiratory Syncytial Virus Infection in the Absence of Type I Interferons. J Innate Immun. 2016;8(5):452-63. [CrossRef] [PubMed]
- Wang Y, Zheng J, Wang X, Yang P, Zhao D. Alveolar macrophages and airway hyperresponsiveness associated with respiratory syncytial virus infection. Front Immunol. 2022 Oct 20;13:1012048. [CrossRef] [PubMed]
- Vanderven HA, Kent SJ. Fc-mediated functions and the treatment of severe respiratory viral infections with passive immunotherapy - a balancing act. Front Immunol. 2023 Nov 22;14:1307398. Available online: https://pubmed.ncbi.nlm.nih.gov/38077353/. [CrossRef] [PubMed]
- Gimenez HB, Keir HM, Cash P. In vitro enhancement of respiratory syncytial virus infection of U937 cells by human sera. J Gen Virol. 1989 Jan;70 ( Pt 1):89-96. Available online: https://pubmed.ncbi.nlm.nih.gov/2732688/. [CrossRef] [PubMed]
- Krilov LR, Anderson LJ, Marcoux L, Bonagura VR, Wedgwood JF. Antibody-mediated enhancement of respiratory syncytial virus infection in two monocyte/macrophage cell lines. J Infect Dis. 1989 Nov;160(5):777-82. Available online: https://pubmed.ncbi.nlm.nih.gov/2809253/. [CrossRef] [PubMed]
- Gómez RS, Ramirez BA, Céspedes PF, Cautivo KM, Riquelme SA, Prado CE, González PA, Kalergis AM. Contribution of Fcγ receptors to human respiratory syncytial virus pathogenesis and the impairment of T-cell activation by dendritic cells. Immunology. 2016 Jan;147(1):55-72. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4693880/. [CrossRef] [PubMed]
- Vogelzang A, Lozza L, Reece ST, Perdomo C, Zedler U, Hahnke K, Oberbeck-Mueller D, Dorhoi A, Kaufmann SH. Neonatal Fc Receptor Regulation of Lung Immunoglobulin and CD103+ Dendritic Cells Confers Transient Susceptibility to Tuberculosis. Infect Immun. 2016 Sep 19;84(10):2914-21. Available online: https://pubmed.ncbi.nlm.nih.gov/27481246/. [CrossRef] [PubMed]
- Cines DB, Zaitsev S, Rauova L, Rux AH, Stepanova V, Krishnaswamy S, Sarkar A, Kowalska MA, Zhao G, Mast AE, Blumberg LJ, McCrae KR, Poncz M, Hubbard JJ, Pyzik M, Blumberg RS. FcRn augments induction of tissue factor activity by IgG-containing immune complexes. Blood. 2020 Jun 4;135(23):2085-2093. Available online: https://pubmed.ncbi.nlm.nih.gov/32187355/. [CrossRef] [PubMed]
- Hubbard JJ, Pyzik M, Rath T, Kozicky LK, Sand KMK, Gandhi AK, Grevys A, Foss S, Menzies SC, Glickman JN, Fiebiger E, Roopenian DC, Sandlie I, Andersen JT, Sly LM, Baker K, Blumberg RS. FcRn is a CD32a coreceptor that determines susceptibility to IgG immune complex-driven autoimmunity. J Exp Med. 2020 Oct 5;217(10):e20200359. Available online: https://pubmed.ncbi.nlm.nih.gov/32658257/. [CrossRef] [PubMed]
- Lee CH, Romain G, Yan W, Watanabe M, Charab W, Todorova B, Lee J, Triplett K, Donkor M, Lungu OI, Lux A, Marshall N, Lindorfer MA, Goff OR, Balbino B, Kang TH, Tanno H, Delidakis G, Alford C, Taylor RP, Nimmerjahn F, Varadarajan N, Bruhns P, Zhang YJ, Georgiou G. IgG Fc domains that bind C1q but not effector Fcγ receptors delineate the importance of complement-mediated effector functions. Nat Immunol. 2017 Aug;18(8):889-898. Erratum in: Nat Immunol. 2017 Sep 19;18(10 ):1173. [CrossRef] [PubMed]
- Gimenez HB, Chisholm S, Dornan J, Cash P. Neutralizing and enhancing activities of human respiratory syncytial virus-specific antibodies. Clin Diagn Lab Immunol. 1996 May;3(3):280-6. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC170331/. [CrossRef] [PubMed]
- Katzelnick LC, Gresh L, Halloran ME, Mercado JC, Kuan G, Gordon A, Balmaseda A, Harris E. Antibody-dependent enhancement of severe dengue disease in humans. Science. 2017 Nov 17;358(6365):929-932. Available online: https://pubmed.ncbi.nlm.nih.gov/29097492/. [CrossRef] [PubMed]
- Mokhtary P, Pourhashem Z, Mehrizi AA, Sala C, Rappuoli R. Recent Progress in the Discovery and Development of Monoclonal Antibodies against Viral Infections. Biomedicines. 2022 Aug 2;10(8):1861. Available online: https://pubmed.ncbi.nlm.nih.gov/36009408/. [CrossRef] [PubMed]
- Brady T, Cayatte C, Roe TL, Speer SD, Ji H, Machiesky L, Zhang T, Wilkins D, Tuffy KM, Kelly EJ. Fc-mediated functions of nirsevimab complement direct respiratory syncytial virus neutralization but are not required for optimal prophylactic protection. Front Immunol. 2023 Oct 11;14:1283120. Available online: https://pubmed.ncbi.nlm.nih.gov/37901217/. [CrossRef] [PubMed]
- van Erp EA, Luytjes W, Ferwerda G, van Kasteren PB. Fc-Mediated Antibody Effector Functions During Respiratory Syncytial Virus Infection and Disease. Front Immunol. 2019 Mar 22;10:548. Available online: https://pubmed.ncbi.nlm.nih.gov/30967872/. [CrossRef] [PubMed]
- Dall’Acqua WF, Woods RM, Ward ES, Palaszynski SR, Patel NK, Brewah YA, Wu H, Kiener PA, Langermann S. Increasing the affinity of a human IgG1 for the neonatal Fc receptor: biological consequences. J Immunol. 2002 Nov 1;169(9):5171-80. Available online: https://pubmed.ncbi.nlm.nih.gov/12391234/. [CrossRef] [PubMed]
- Cingoz, O. Motavizumab. MAbs. 2009 Sep-Oct;1(5):439-42. Epub 2009 Sep 10. Erratum in: MAbs. 2010 Sep-Oct;2(5):591. [CrossRef] [PubMed]
- Liu, L. Antibody glycosylation and its impact on the pharmacokinetics and pharmacodynamics of monoclonal antibodies and Fc-fusion proteins. J Pharm Sci. 2015 Jun;104(6):1866-1884. [CrossRef] [PubMed]
- Dekkers G, Treffers L, Plomp R, Bentlage AEH, de Boer M, Koeleman CAM, Lissenberg-Thunnissen SN, Visser R, Brouwer M, Mok JY, Matlung H, van den Berg TK, van Esch WJE, Kuijpers TW, Wouters D, Rispens T, Wuhrer M, Vidarsson G. Decoding the Human Immunoglobulin G-Glycan Repertoire Reveals a Spectrum of Fc-Receptor- and Complement-Mediated-Effector Activities. Front Immunol. 2017 Aug 2;8:877. [CrossRef] [PubMed]
- Hiatt A, Bohorova N, Bohorov O, Goodman C, Kim D, Pauly MH, Velasco J, Whaley KJ, Piedra PA, Gilbert BE, Zeitlin L. Glycan variants of a respiratory syncytial virus antibody with enhanced effector function and in vivo efficacy. Proc Natl Acad Sci U S A. 2014 Apr 22;111(16):5992-7. [CrossRef] [PubMed]
- Zheng K, Bantog C, Bayer R. The impact of glycosylation on monoclonal antibody conformation and stability. MAbs. 2011 Nov-Dec;3(6):568-76. [CrossRef] [PubMed]
- Kecse-Nagy C, Szittner Z, Papp K, Hegyi Z, Rovero P, Migliorini P, Lóránd V, Homolya L, Prechl J. Characterization of NF-κB Reporter U937 Cells and Their Application for the Detection of Inflammatory Immune-Complexes. PLoS One. 2016 May 27;11(5):e0156328. [CrossRef] [PubMed]
- Munoz FM, Cramer JP, Dekker CL, Dudley MZ, Graham BS, Gurwith M, Law B, Perlman S, Polack FP, Spergel JM, Van Braeckel E, Ward BJ, Didierlaurent AM, Lambert PH; Brighton Collaboration Vaccine-associated Enhanced Disease Working Group. Vaccine-associated enhanced disease: Case definition and guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine. 2021 May 21;39(22):3053-3066. Available online: https://pubmed.ncbi.nlm.nih.gov/33637387/. [CrossRef] [PubMed]
- Taylor, G. Animal models of respiratory syncytial virus infection. Vaccine. 2017 Jan 11;35(3):469-480. [CrossRef] [PubMed]
- Shoukat A, Abdollahi E, Galvani AP, Halperin SA, Langley JM, Moghadas SM. Cost-effectiveness analysis of nirsevimab and maternal RSVpreF vaccine strategies for prevention of Respiratory Syncytial Virus disease among infants in Canada: a simulation study. Lancet Reg Health Am. 2023 Nov 9;28:100629. Available online: https://pubmed.ncbi.nlm.nih.gov/38026446/. [CrossRef] [PubMed]
- Shoukat A, Abdollahi E, Galvani AP, Halperin SA, Langley JM, Moghadas SM. Cost-effectiveness analysis of nirsevimab and maternal RSVpreF vaccine strategies for prevention of Respiratory Syncytial Virus disease among infants in Canada: a simulation study. Lancet Reg Health Am. 2023 Nov 9;28:100629. Available online: https://pubmed.ncbi.nlm.nih.gov/38026446/. [CrossRef] [PubMed]
- An Advisory Committee Statement (ACS) National Advisory Committee on Immunization (NACI) Statement on the prevention of respiratory syncytial virus (RSV) disease in infants: Supplementary systematic review of economic evidence, Available on line : https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/vaccines-immunization/national-advisory-committee-immunization-statement-prevention-respiratory-syncytial-virus-disease-infants-supplementary-systematic-review-economic-evidence/naci-appendix-2024-05-17.pdf https://web.archive.org/web/20240521111714/ https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/vaccines-immunization/national-advisory-committee-immunization-statement-prevention-respiratory-syncytial-virus-disease-infants-supplementary-systematic-review-economic-evidence/naci-appendix-2024-05-17.pdf accessed May 26, 2024.
- Neumann S, Alverson B. Nirsevimab: The Hidden Costs. Hosp Pediatr. 2024 May 9;14(6):e2024007739. Available online: https://pubmed.ncbi.nlm.nih.gov/38721666/. [CrossRef] [PubMed]
- AAP news, Sanofi raising price of RSV immunization nirsevimab April 12, 2024, Available on line : https://publications.aap.org/aapnews/news/28657/Sanofi-raising-price-of-RSV-immunization https://web.archive.org/web/20240530142639/ https://publications.aap.org/aapnews/news/28657/Sanofi-raising-price-of-RSV-immunization accessed April 20, 2024.
- BEYFORTUS 50 mg sol inj ser préremplie, Vidal, Available online : https://www.vidal.fr/medicaments/beyfortus-50-mg-sol-inj-ser-preremplie-242583.html https://web.archive.org/web/20240526204604/https://www.vidal.fr/medicaments/beyfortus-50-mg-sol-inj-ser-preremplie-242583.html accessed May 26, 2024.
- Circuit de prescription du Nirsevimab (BEYFORTUS ®) ARS de Bretagne, Available on line: https://www.bretagne.ars.sante.fr/system/files/2023-09/Presentation%20Dr%20Lefevre.pdf https://web.archive.org/web/20240329150151/https://www.bretagne.ars.sante.fr/system/files/2023-09/Presentation%20Dr%20Lefevre.pdf accessed October 10, 2023.
- anofi senkt Preis für Beyfortus, Apotheke-Adhoc, 16 May 2024. Available online: https://www.apotheke-adhoc.de/nachrichten/detail/pharmazie/sanofi-senkt-preis-fuer-beyfortus/ (accessed on 4 June 2024).
- Gebremedhin, B. Gebretekle, Man Wah Yeung, Raphael Ximenes, Alexandra Cernat, Alison E. Simmons, April Killikelly, Winnie Siu, Ellen Rafferty, Nicholas Brousseau, Matthew Tunis, Ashleigh R. Tuite medRxiv 2024.03.21.24304675. [CrossRef]
Figure 1.
Rates of death per month between 2 and 6 days of life per 1,000 births in France (from April 2018 to April 2024) displaying the time window of the nirsevimab immunization campaign (Beyfortus©).
Figure 1.
Rates of death per month between 2 and 6 days of life per 1,000 births in France (from April 2018 to April 2024) displaying the time window of the nirsevimab immunization campaign (Beyfortus©).
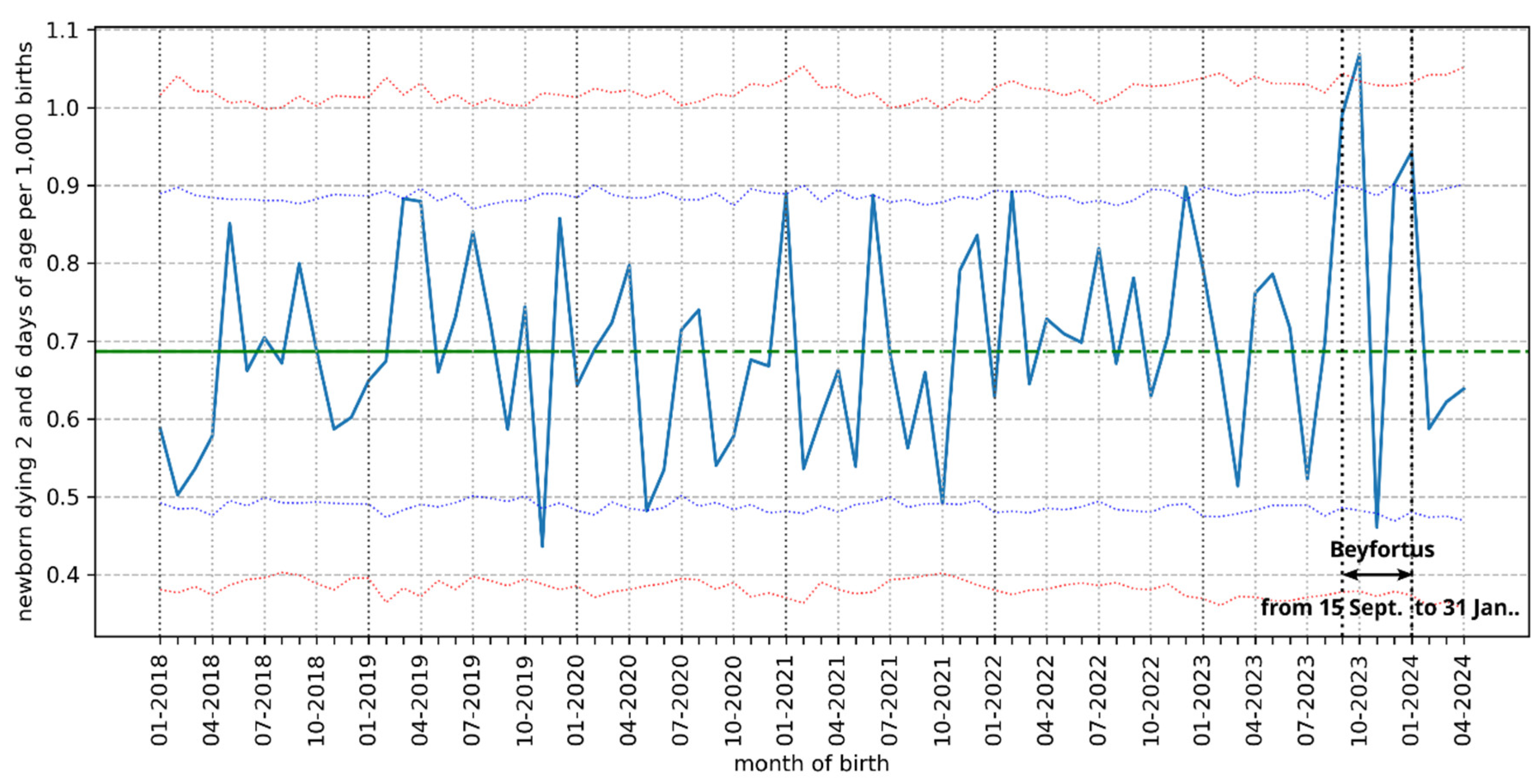
Figure 2.
Rate of deaths per month between 2 and 6 days of life per 1,000 births in France between March 2018 and February 2024: superposition of the curves obtained for each year.
Figure 2.
Rate of deaths per month between 2 and 6 days of life per 1,000 births in France between March 2018 and February 2024: superposition of the curves obtained for each year.
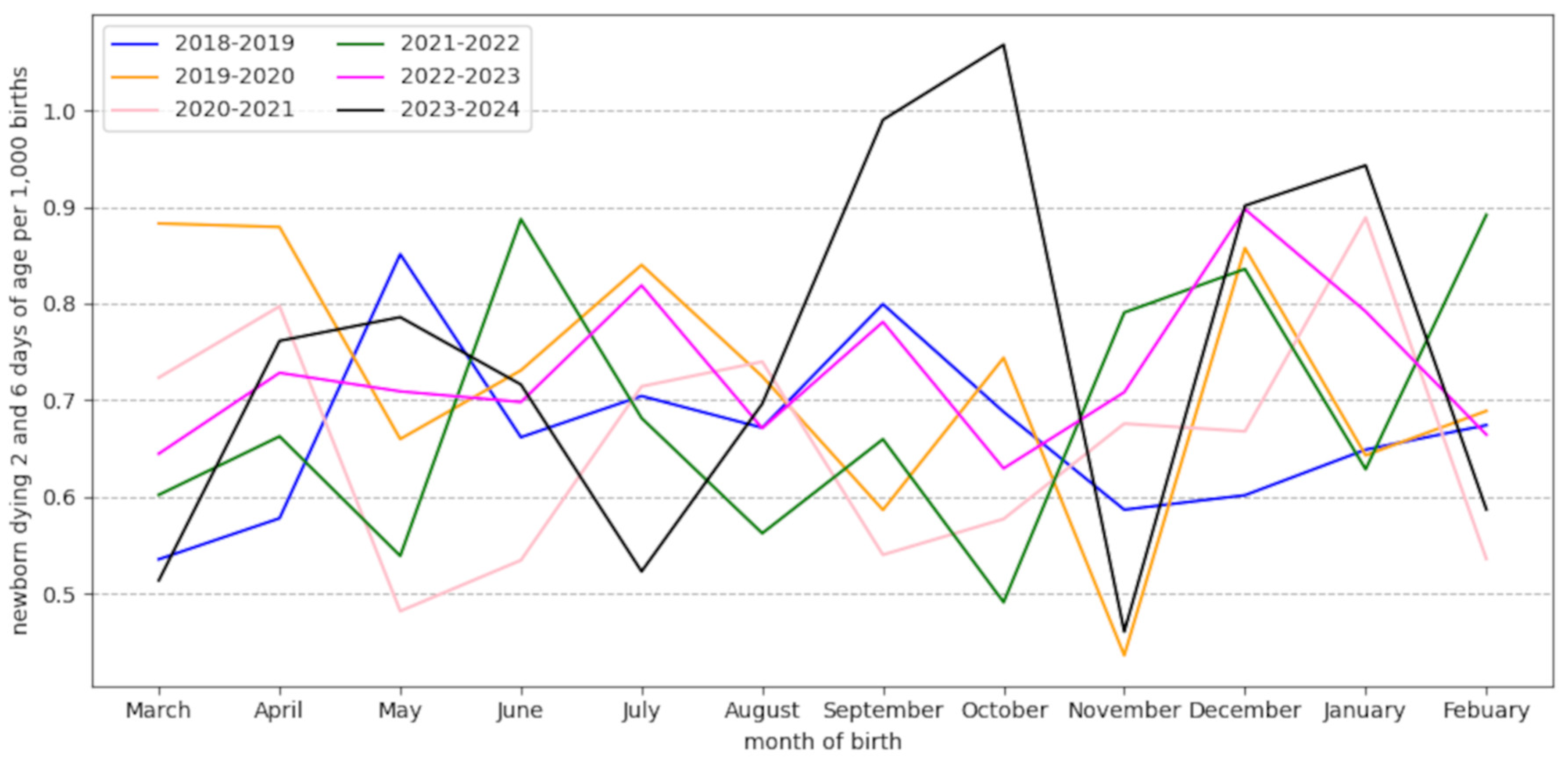
Figure 3.
Function of nirsevimab. Left: nirsevimab binds strongly to epitope Ø of the RSV fusion protein in prefusion conformation [4]. Right: after endocytosis, YTE mutations on the Fc fragment of nirsevimab give it a high affinity for FcRn, protecting it from degradation in the acidic environment of the endosome.
Figure 3.
Function of nirsevimab. Left: nirsevimab binds strongly to epitope Ø of the RSV fusion protein in prefusion conformation [4]. Right: after endocytosis, YTE mutations on the Fc fragment of nirsevimab give it a high affinity for FcRn, protecting it from degradation in the acidic environment of the endosome.
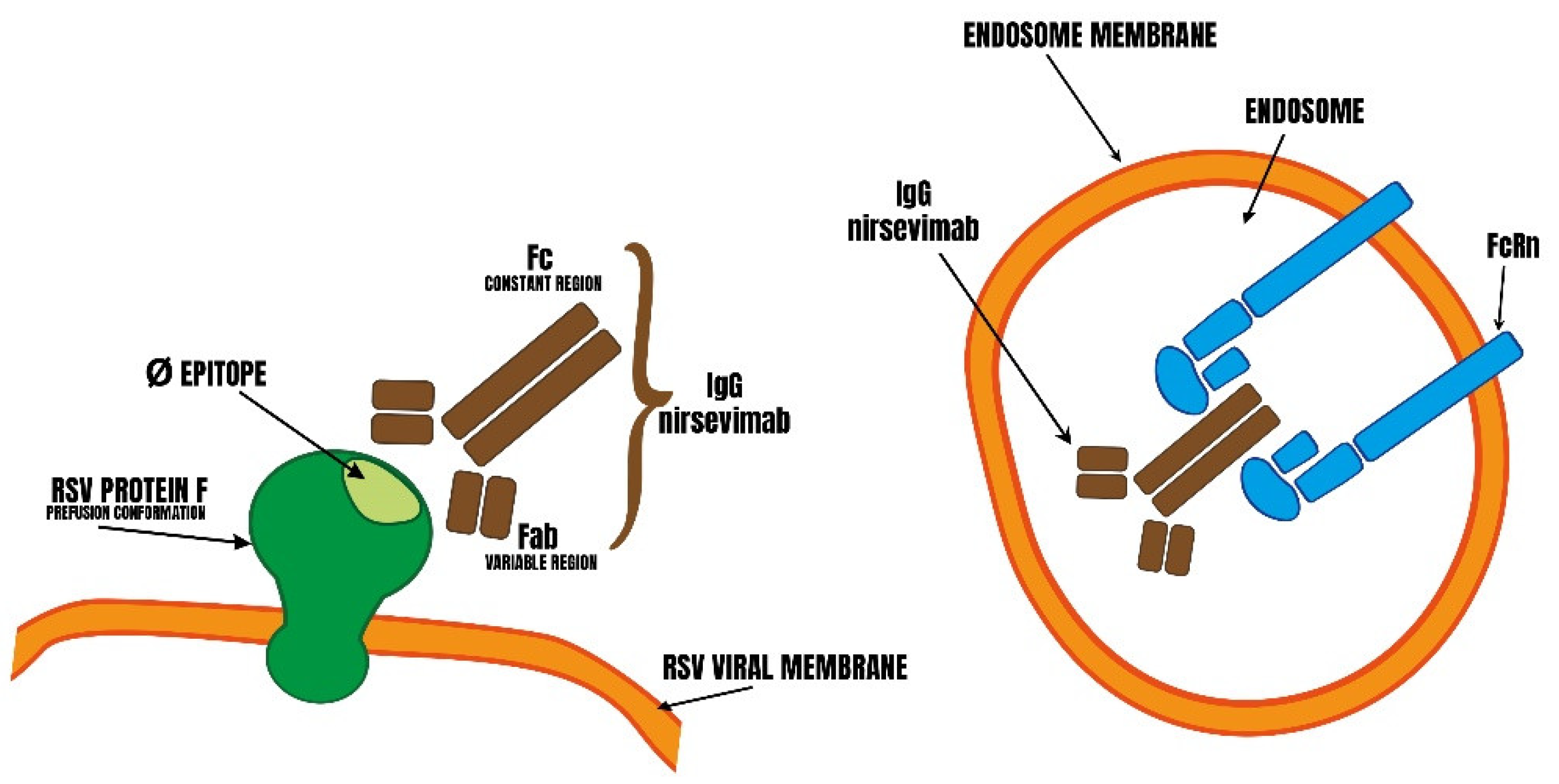
Figure 4.
Relationship between nirsevimab function and ADE Left: Strong binding to FcRn is able to modify other effector functions of nirsevimab that may be involved in its therapeutic effect (binding to FcγR of NK cells and complement components), particularly at low concentration. Right: FcRn is able to facilitate the entry of certain virus-antibody complexes into target cells (macrophages, pulmonary epithelial cells) at sub-neutralizing concentrations.
Figure 4.
Relationship between nirsevimab function and ADE Left: Strong binding to FcRn is able to modify other effector functions of nirsevimab that may be involved in its therapeutic effect (binding to FcγR of NK cells and complement components), particularly at low concentration. Right: FcRn is able to facilitate the entry of certain virus-antibody complexes into target cells (macrophages, pulmonary epithelial cells) at sub-neutralizing concentrations.
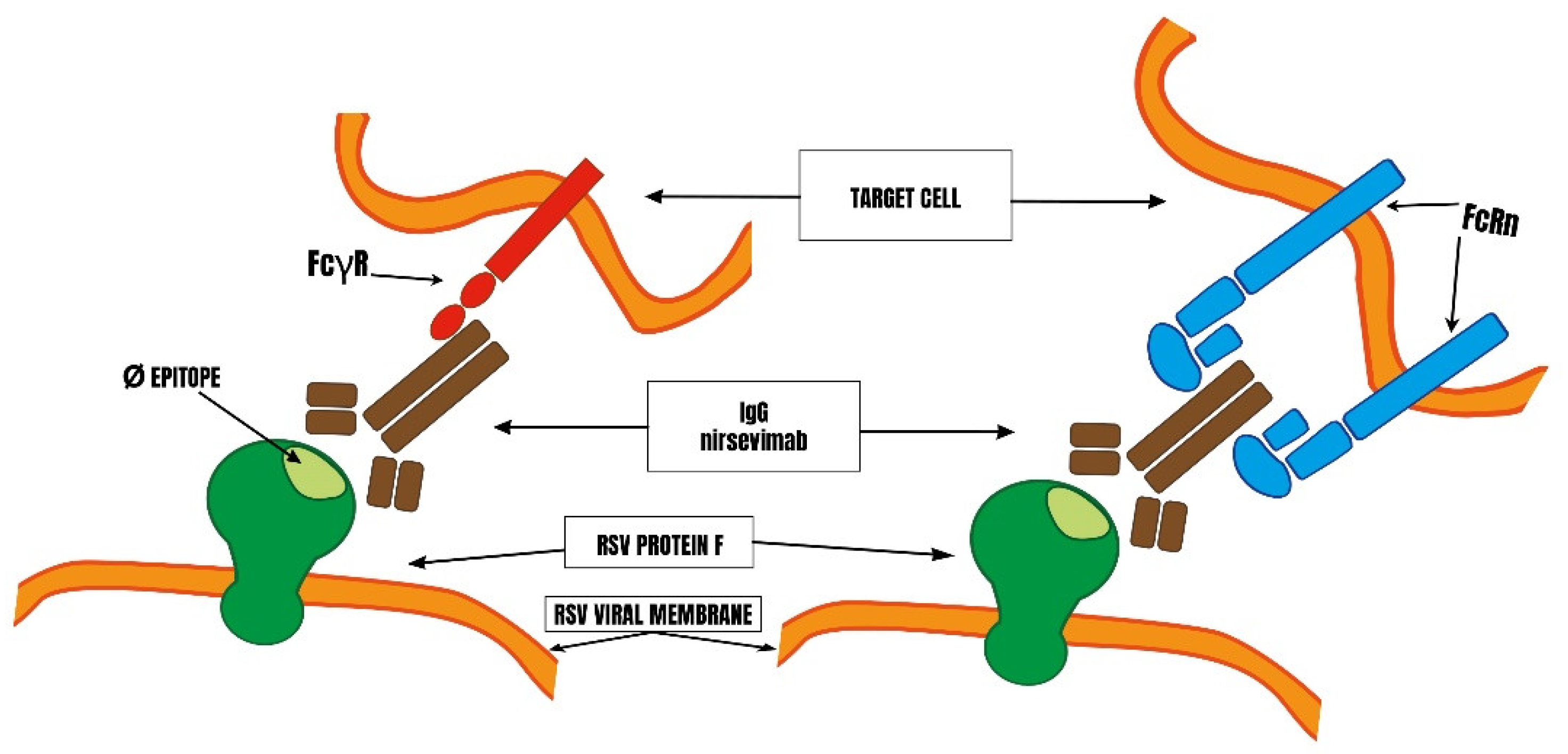

Table 1.
Summary results of clinical studies: efficacy of nirsevimab, argument in favor of ADE, biases.
Table 1.
Summary results of clinical studies: efficacy of nirsevimab, argument in favor of ADE, biases.
| Absolute reduction risk RSV hospitalization | Argument in favor of ADE | Bias | |
|---|---|---|---|
| Domachowske 2018 -phase 1- healthy preterm [20] | not evaluated | LRTI in treated group : 5 (5/69) LRTI in placebo group : 0 (0/16) | 6.86% of treated participants are excluded |
| Griffin 2017 adults [21] | not evaluated | URTI in 19% of treated participants URTI in 9% of placebo group | No search of RSV carried out |
| Hammitt phase 2 [22] | 1 % | Treated participants hospitalized longer than placebo | 8,1% of treated are excluded |
| Simöes [24] | 2 % | See [12,16] | 2% of treated are excluded |
| Griffin 2020 preterms [26] | 3,3 % | Within 20-30 days after treatment LRTI all causes are equally frequent in both groups (early ADE not excluded) | 5,8% of treated are excluded |
| Drysdale open label [25] | 1,2 % | More severe infections (any cause) in the treated group than in the placebo group | 0,22% of treated are excluded Investigator is sometimes the treating physician |
Table 2.
Nirsevimab mmunization coverage, effectiveness in post-marketing studies, argument in favor of ADE and biases.
Table 2.
Nirsevimab mmunization coverage, effectiveness in post-marketing studies, argument in favor of ADE and biases.
| Nationwide immunization coverage | Effectiveness RRR : relative risk reduction ARR : absolute risk reduction | Argument in favor of ADE | Biases | |
|---|---|---|---|---|
| USA-CDC Moline [39] | 20,0 % | RRR 90% against RSV hospitalization | 77% of RSV hospitalization observed within 7 days of injection | symptoms < 7 days of injection are excluded |
| Luxembourg Ernst [41] | 84 % | not evaluated | Impossible to assess | immune status of participants not studied |
| France Paireau [45] | unknown | RRR 74,4-80,6% against ICU admission due to RSV | occurence of PICU admission <8 days of injection (or unknown) : 45% | 52% of cases excluded Case/control study 5/1 |
| France Assad [42] | unknown | RRR against RSV bronchiolitis 80 % | No effectiveness during 7 first days | Case/control study 1/0,5 non-representative population? |
| Spain Ares-Gomez [55] | > 90% | * RRR 82% against RSV hospitalization * ARR of RSV LRTI admission : 1,6% * RRR 66,2% against all causes hospitalizations (comparison between seasons) | Nosocomial cases excluded (unknown number) | *Non-comparable populations? *No case-control possible *Exclusion of seasons of low epidemic intensity and retention of the exceptional 2022-2023 season |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



