
Submitted:
10 June 2024
Posted:
12 June 2024
You are already at the latest version
Abstract
Breast Cancer Associated Susceptibility Proteins Type 1/2 (BRCA1/2) promote cellular functioning by modulating NRF2-mediated antioxidant signaling. Redox failure in women with BRCA1/2 insufficiency increases the risk for breast/ovarian/uterine cancers. Risk‐reducing salpingo‐oophorectomy (RRSO) is a prophylactic surgery of the reproductive organs, which is frequently conducted by the age of 40 to lower the occurrence of cancer in women with BRCA1/2 mutations. However, abrupt estrogen decline following RRSO causes ovarian failure, which implicates various cellular physiological processes, resulting in increased release of free radicals and subsequent severe onset of menopausal symptoms. Comfort measures (e.g., hormonal replacement therapy (HRT) and mindfulness-based stress reduction (MBSR)) may improve chronological menopause-related quality of life, but their specific effects are not clear in women with gene mutations. Aiming to fill the gap, this study used path analysis to examine the effects of HRT and MBSR on menopausal symptoms among RRSO patients (N = 199, mean age = 50.5 ± 6.7 years). HRT alleviated menopausal symptoms in BRCA2 carriers and women who were physically active, premenopausal at the time of RRSO, had a high BMI, and had no history of breast cancer. It increased the severity of urogenital symptoms in those with a history of cancer. MBSR, on the other hand, was associated with increased intensity of most menopausal symptoms. The results suggest that young women undergoing recent RRSO may benefit from HRT at an individual level while their need for extensive measures to optimize their psychological wellbeing is ongoing. Adverse effects of MBSR, which are captured in the present study imply that MBSR may interfere with redox sensitivity associated with estradiol fluctuations in BRCA1/2 carriers. Investigations are needed to test this hypothesis and elaborate on the underlying mechanisms in those women.
Keywords:
hormonal replacement therapy (HRT)
; mindfulness-based stress reduction (MBSR)
; Risk reducing salpingo-oophorectomy (RRSO)
; Breast Cancer Associated Susceptibility Protein Type 1/2 (BRCA1/2) mutations
; Menopause rating scale (MRS)
; menopause/perimenopause/postmenopausal
; psychological symptoms
; physical activity/exercise
; breast cancer
Introduction
Breast cancer is the most prevalent cancer among women [1], with 1 in 8 US women develops invasive breast cancer over the course of lifetime and more than two million cases are annually diagnosed worldwide. It is the second cause of cancer-related female mortality [1,2,3]. Breast Cancer Associated Susceptibility Proteins Type 1/2 (BRCA1/2) are closely related tumor suppressor genes. Mutations in both genes are primarily associated with hereditary breast cancers. They comprise 1863 and 3418 amino acids, in order, which interact with various cellular proteins resulting in the regulation of specific transcriptional pathways involved in cell cycle progression, highly specialized DNA repair processes, DNA damage-responsive cell cycle checkpoints, cytoplasmic division, and apoptosis—denoting their tumor suppressing activity [4,5,6]. Compared with the general population, female carriers of BRCA1 and BRCA2 mutations exhibit an increased lifetime risk of developing breast and ovarian cancer by 59% and 16.5%, respectively [4,7,8]. BRCA1 deficiency is associated with activation of inflammatory signaling (tumor-necrosis factor-α (TNF-α) activation of nuclear factor kappa B (NF-κB) and mRNA expression of NF-κB-dependent target gene superoxide dismutase 2 (SOD2)), as well as increased production of free radicals, resulting in DNA damage, which trigger malignant transformation [9]. Carcinogenesis in BRCA2 deficiency is associated with increased incidence of binucleated cells, alterations in chromosome number (aneuploidy), and structurally abnormal chromosomes [5]. Because of failure of early detection by ovarian cancer screening, current guidelines recommend risk-reducing salpingo-oophorectomy (RRSO), at the age of 35–40 years for BRCA1 mutation carriers and at 40–45 years for BRCA2 mutation carriers, as a standard approach to decrease the incidence of cancer among these women [10]. Evidence denotes that timed RRSO lowers the risk of ovarian cancer by 96% and overall mortality by 76% [8,10].
Estrogen drop following menopause, accelerates ROS production, which parallels alterations in the circadian rhythm—an internal biological clock that regulates physiological processes and organ homeostasis [11,12]. Investigations involving premenopausal and postmenopausal women who do not receive hormone replacement therapy (HRT) or antioxidant supplements spot elevated oxidative stress as a biomarker only in menopausal women. Oxidative stress is associated with the severity of hot flushes and psychological stress in menopausal women [13]. Wide-scale screening of community-dwelling menopausal women in Canada uncovers the highest incidence of depression (odds ratio= 1.45; CI: 1.07-1.97) among women encountering menopause before the age of 40 [14]. Surgical menopause induced by RRSO involves sudden cessation of estrogen release resulting in acute onset of vasomotor, psychological, physical, and sexual symptoms, which are usually more severe than naturally occurring menopausal symptoms. Therefore, HRT is usually prescribed to mitigate the severity of menopausal symptoms [8,15].
HRT is used to treat hot flushes and urogenital symptoms and reduce age-related cardiovascular complications of menopause. Randomized control trials and experimental studies show that the anti-menopausal effects of HRT are linked to a mechanism that implies improved antioxidant production and decreased ROS release [16,17]. Experimental evidence reports that ovariectomy impairs estrogen receptor (ER) expression profile by increasing the ER α/β ratio [18]. Estrogen supplementation shortly after ovariectomy, NOT late supplementation, prevents the shift in the ER α/β ratio, which is associated with restoration of glutathione peroxidase and catalase activity, along with inhibition of mitochondrial hydrogen peroxide release and associated oxidative damage to cellular lipid and protein structures [18]. Nonetheless, the effect of HRT on menopause within the context of cancer-related gene mutations is unclear.
Psychological symptoms of menopause may alter quality of life and social relations, impede women’s work performance, and promote burnout [15,19]. Moreover, these symptoms require special attention because they may signify prodromes of age-related disorders such as Alzheimer’s disease in genetically vulnerable patients [11,15]. Interventions that ameliorate menopausal symptoms, especially related to emotional dysfunction, can improve women’s work ability [19]. Mindfulness-based stress reduction (MBSR) is a well-designed program that combines three meditation activities (body scanning exercises, sitting meditation, and gentle yoga poses). MBSR prompts the individual to pay full attention to the present moment in an accepting, non-judgmental manner [10,20]. Among euthymic women in the menopause transition, MBSR is reported to prevent the occurrence of depressive symptoms, lower perceived stress and trait anxiety as well as increase trait mindfulness and psychological resilience and improve sleep, with more benefits occurring in women with sensitivity to estradiol fluctuation and excessive life stress. However, the development of major depressive episodes may not change in response to MBSR treatment [20] . Among post-menopausal, MBSR alleviated psychological, physical, and sexual symptoms, but it had no effect on vasomotor symptoms [21]. Unlike chronological menopause, MBSR in RRSO women is reported to alleviate vasomotor and physical symptoms [10]. These symptoms are key effectors of psychological distress in the menopause period [15]. However, the effects of MBSR and HRT on menopause-related psychological symptoms are unclear in RRSO patients [10]. Given the interplay among different menopausal symptoms, the effect of vasomotor and urogenital symptoms on psychological symptoms within the context of MBSR and HRT is also unclear. To fill the gap, the current study aims to explore the association among the different climacteric symptoms as well as the effect of MBSR and HRT on menopausal symptoms among BRCA1/2 carriers undergoing RRSO. Based on the available literature, we hypothesized that: 1) the severity of psychological symptoms is associated with more severe physical/vegetative and urogenital symptoms and 2) women receiving MBSR and HRT would experience less psychological and other menopausal complaints than those not attaining either treatment.
Methods
Design, Participants, and Procedure
This cross-sectional study is a secondary analysis based on the data of 199 women with BRCA1/2 mutations from The Netherlands who underwent RRSO and were treated in the University Medical Center Groningen (UMCG) family cancer clinic between November 2015 and December 2016. Participation was limited to those who were aged 18 to 52 years at the time of RRSO, who did not have a severe psychiatric disorder or a currently active cancer. Inadequate fluency of the Dutch language disqualified participation in the study [8].
Out of 239 women who took part in the Psychosexual Consequences of Risk-reducing Salpingo-oophorectomy (PURSUE) study, 200 returned the questionnaire, with one respondent excluded from the analysis because of extensive missing data. A subset of the sample comprised women with at least two moderate-to-severe menopausal symptoms (n = 23) who participated in an eight-week standard MRBS training program during the period between January 2015 to October 2015: the entire experimental group comprised 34 women. The intervention is described in detail elsewhere. In brief, the participants attended 2.5-hour weekly MRBS sessions, which did not specifically focus on menopausal symptoms, and a silent retreat evening of 4 hours. They also performed daily mindfulness exercises at home for a duration of 30–45 minutes following instructions on an MP3 player [10]. The rest of the participants received care as usual (n = 176) [8].
All patients signed informed consent before completing the questionnaire. Participation was voluntary, and procedures that protect patients’ privacy and confidentiality were undertaken [8]. The experimental study is registered in the ClinicalTrials.gov with the identifier NCT02372864 [10]. The intervention and data collection protocol of the PURSUE study was approved by the Medical Ethical Committee of the UMCG on 14 November 2014 (registration no. NL46796.042.14). For the current analysis, no ethical approval was obtained because we used a public dataset shared under the terms of Creative Common License (CC BY 4.0) [22].
Measures
Participants completed a self-administered questionnaire, which comprised two sections. Section one inquired about various sociodemographic and clinical variables including age, weight and height to calculate body mass index (BMI), employment, current smoking (yes/no), alcohol drinking habits (yes/no), duration of physical exercise per week, type of BRCA1/2 mutation, date of RRSO, menopausal status at the time of RRSO, history of breast cancer, and past or current use of HRT. The duration of menopausal symptoms was calculated as the time elapsed since RRSO and data on specific breast cancer treatment (chemotherapy, hormone therapy, radiotherapy and immunotherapy) were obtained from the medical record.
Section two comprised the Menopause Rating Scale (MRS), an 11-item measure, which depicts the severity of menopausal symptoms. Items are rated on a five-point response scale (0= no symptoms, 1= mild, 2= moderate, 3= severe, and 4= extremely severe), with total scale scores ranging between zero and 44. Higher scores signify greater symptom severity. Items are categorized into three subscales: 1) psychological symptoms (e.g., irritability, depressive mood, mental exhaustion, and anxiety), 2) somato-vegetative/vasomotor and physical symptoms (e.g., hot flushes and sweating, heart discomfort, joint and muscle discomfort, and sleep difficulties), and 3) urogenital symptoms (e.g., vaginal dryness, sexual problems, and bladder problems).
Statistical Analysis
Descriptive statistics were reported as mean and standard deviation or frequency and percentage based on the type of variables. A path analysis model was conducted to examine the associations among different menopausal symptoms. Psychological symptoms were used as an outcome variable. The model also examined different effects of MBSR and HRT on menopausal symptoms. The model involved many sociodemographic and clinical variables as predictors. Some of these variables were removed from the model through a step-by-step deletion of non-significant predictors. We used multi-group analysis to examine the stability of the final model across different groups (e.g., type of mutation, history of breast cancer, menopausal status at the time of RRSO, BMI, physical activity level, and current smoking). For each model, four levels of group invariance were measured: configural, metric, scalar, and strict. Model fit was based on a non-significant Chi square (χ2) test, along with absolute fit indices: Comparative Fit Index (CFI), Tucker–Lewis Index (TLI), and root mean square error of approximation (RMSEA). Values indicating acceptable fit are >0.90, >0.90, and <0.08, respectively [23]. In multigroup analysis, models with a significant χ2 were considered invariant if ΔCFI and ΔRMSEA were greater than 0.020 and 0.015, respectively [24]. The analysis was performed in SPSS and AMOS version 24, and significance was considered at a probability of 0.05.
Results
Participant Characteristics
The average age of the participants at the time of data collection and at the time of RSSO was 50.5 ± 6.7 and 42.5 ± 4.9 years, respectively. The average time elapsed since RRSO was 7.9 ± 4.8 years. Approximately half of the participants were BRCA1 carriers (n = 102, 51.3%), one-third were BRCA2 carriers (n = 66, 33.2%), and the mutation status was unknown in 31 women (15.6%). One-third of the participants had a history of breast cancer (n = 67, 33.3%). More than one-third of the participants reported a lifetime use of HRT (n = 81, 40.7%). Most women were currently non-smokers (n = 173, 86.9%) and premenopausal at the time of RRSO (n = 134, 67.3%). Less than two-thirds of the participants (n = 122, 61.3%) reported engagement in physical activity for more than 30 minutes/day for five days or more. Most of the women had a BMI of 25 or below (n = 114, 57.3%), with only three women reporting a BMI below 20, while more than one third of the participants had a BMI above 25 (n = 82, 41.2%). More than two-thirds of the participants reported moderate to severe overall menopausal symptoms (n = 137, 68.9%). Severe and moderate urogenital symptoms were reported by a large portion of the sample (n = 103, 51.8%) and (n = 48, 24.1%), respectively. Approximately half of the participants reported moderate to severe somatic-vegetative symptoms (n = 111, 55.8%) and psychological symptoms (n = 95, 47.7%).
The Effect of HRT and MBSR on Menopausal Symptoms (Path Analysis)
After trimming non-significant sociodemographic predictors, the path model had excellent fit (CFI = 1.00, TLI = 1.00, RMSEA = 0.00, χ2 = 14.18, p = 0.585). As shown in Figure 1, urogenital and somato-vegitative symptoms had significant direct effects on psychological symptoms. The direct effects of MBSR on all the symptoms were non-significant (p values range = 0.071 to 0.094). However, it had positive significant indirect effects on the psychological and somato-vegitative symptoms (β = 0.108, p = 0.003 and β = 0.029; p = 0.033, respectively). HRT had a significant negative direct effect only on urogenital symptoms (p = 0.005), which mediated the negative indirect effects of HRT on psychological and somato-vegitative symptoms (β = -0.067, p = 0.004 and β = -0.046; p = 0.004, respectively). Both age at RRSO and time elapsed after RRSO negatively predicted psychological symptoms (both p values = 0.001), but they had no effect on other menopausal symptoms (paths trimmed). The same was true for mutation type (p = 0.018), albeit its effect was positive.
The Effect of HRT and MBSR on Menopausal Symptoms Across Groups (Multigroup Analysis)
Supplementary Table 1 indicates adequate fit of the path model across various groups, at least at the configural and metric levels. In subgroup analysis, MBSR directly increased somatic-vegetative symptoms in BRCA1 mutation carriers. Among BRCA2 carriers, MBSR caused direct and indirect increases in urogenital and psychological symptoms, respectively. HRT caused significant reductions in urogenital and psychological symptoms only in BRCA2 mutation carriers (Table 1). Among women with a history of breast cancer, MBSR predicted a direct increase in somatic somatic-vegetative symptoms along with direct and indirect increases in psychological symptoms. Psychological symptoms were the only menopausal symptom increased as a result (indirect) of MBSR in non-cancer women. HRT resulted in significant declines in all menopausal symptoms only among women with no history of breast cancer, while it significantly increased urogenital symptoms in those with a history of breast cancer (Table 2).
MBSR increased the intensity of all menopausal symptoms in menopausal and premenopausal women, albeit the urogenital symptoms were not significantly affected in the latter. The effects of MBSR on the psychological symptoms in both groups were only indirect. HRT resulted in significant declines in all menopausal symptoms only among women who were pre-menopausal at the time of RSSO (Table 3).
Among normal-weight women, MBSR was associated with a direct increase in symptoms and indirect increases in somatic-vegetative and psychological symptoms, respectively. Meanwhile, it was associated with a direct increase in somatic-vegetative symptoms in overweight women. On the other hand, HRT was associated with a direct decrease in urogenital symptoms as well as with indirect decreases in somatic-vegetative and psychological symptoms in the overweight/obese group (Table 4).
MBSR was associated with an indirect increase in the psychological symptoms in women with both low and high levels of physical activity—the psychological symptoms were directly increased in physically inactive women. HRT was associated with direct and indirect reductions in urogenital and psychological symptoms, in order, among women with low levels of physical activity only (Table 5).
Among smoking women, MBSR contributed to a direct increase in urogenital symptoms and a direct decrease in somatic-vegetative symptoms. Interestingly, MBSR caused an indirect increase in somatic-vegetative symptoms in the smoking group, which was mediated by urogenital symptoms. On the other hand, MBSR directly increased somatic vegetation and indirectly increased psychological symptoms in the non-smoking group. HRT was associated with considerable reductions in all menopausal symptoms only in non-smoking women (Table 6).
Table 7 reports the standardized effects of age at RRSO and time since RRSO on psychological menopausal symptoms across different groups. Age at RRSO and time after RRSO negatively predicted psychological symptoms in BRCA1 carriers only, women without a history of cancer, those who were pre-menopausal at the time of RRSO, current non-smokers, or those who exercised for more than 4 days. Older normal-weight women at RRSO had significantly lower psychological symptoms than their counterparts with higher BMI regardless of the time elapsed since RSSO.
Discussion
This research successfully examined the impact of MBSR and HRT on menopausal symptoms in women with BRCA1/2 gene mutations who had undergone RRSO. As expected, a considerable proportion of our mutation carriers expressed severe-moderate intensity of menopausal symptoms after RRSO. Psychological climacteric symptoms appeared as direct effects of other menopausal symptoms. Young age and short time elapsed after RRSO were associated with greater symptom severity. The results globally indicate positive effects of HRT, particularly in women who were BRCA2 carriers, physically active, non-smoking, premenopausal at RRSO, overweight, and with no history of breast cancer. However, HRT exacerbated urogenital symptoms in breast cancer survivors. Contrary to our expectations, MBSR negatively affected the intensity of menopausal symptoms among women with both mutations, especially those with a history of breast cancer. Such effects were consistent regardless of women’s level of physical activity, body weight, current smoking status, and menopausal status at the time of RSSO. The findings emphasize the significance of early HRT administration and a healthy lifestyle to maximize its benefits for climacteric symptom alleviation in RRSO patients, particularly young women who are premenopausal at the time of surgery. However, those suffering psychological distress may need specialized counseling.
Although BRCA1/2 mutation carriers display chronic distress/anxiety secondary to intrusive and avoidant thoughts following genetic testing, prophylactic surgeries of the reproductive organs (e.g., RRSO) are associated with reduction in state anxiety [25], possibly due to the elimination of cancerphobia as noted by decreased cancer-risk perception [26]. However, estrogen deprivation associated with premature ovarian failure in BRCA1/2 patients who underwent RRSO in our study resulted in noxious levels of different menopausal symptoms: genitourinary (e.g., vaginal dryness and urinary incontinence), somato-vegitative (e.g., hot flushes, and musculoskeletal discomfort), and psychological (e.g., insomnia, anxiety, memory problems, and depression). Psychological climacteric symptoms fulminated among women with higher levels of vasomotor and urogenital symptoms. These results are congruent with the current literature, which associates RRSO with considerable reductions in the quality of life (QoL) and increases in the severity of depressive symptoms secondary to the propagation of key climacteric symptoms (e.g., vasomotor symptoms) [14,15,25,27]. Thus, women with high levels of RRSO-related psychological discomfort may be in need for early targeted counseling.
MBSR is known as an effective meditation intervention [28]. Despite its reported beneficial effects on psychological and physical symptoms, our results indicate that MBSR may be not beneficial or may be even harmful in women with BRCA1/2 mutations. Consistent with our findings, a lack of response to MBSR is documented in a considerable proportion of Veterans with posttraumatic stress disorder [28]. Genetic evidence denotes that MBSR may be linked to stress-related pathways at the molecular level [28]. In detail, peripheral blood samples were obtained from Veterans responding and not-responding to MBSR who were matched by baseline symptoms, age, sex, current smoking status, and current use of antidepressants. Comparing percent methylation levels at CpG sites in regions of the serotonin transporter (SLC6A4, which is involved in the expression of depression and its outcomes) and the Intron 7 region of the FK506 binding protein 5 (FKBP5) were compared from pre- to post-MBSR treatment in both groups. Methylation in FKBP5 intron 7 bin 2 at CpG_35558513 site (containing known glucocorticoid response elements, GRE) decreased in responding and increased in non-responding Veterans [28]. BRCA1 can enhance glucocorticoid receptor (GR) levels and GR transcriptional activity independent of its effect on GR levels, which is associated with the reduction of pro-inflammatory cytokine mRNA levels [29]. GR also plays a major role in the regulation of circadian rhythm, stress response, and organ homeostasis [30].
BRCA1 deficiency in BRCA1 mutations is associated with GR dysregulation, which activates TNF-α-induced NF-κB activity and mRNA expression of NF-κB-dependent target gene SOD2 during the luteal phase. This activity causes prolonged postovulatory inflammation in nonmalignant fallopian tube epithelium [9,29]. Indeed, GR dysregulation in breast cancer women with BRCA1 mutation embroils decreased phosphorylation of GR at the Ser-211 position compared with women with normal breast [30]. In line, exposure to BRCA1/2 genetic test results in high-risk women affected with cancer is reported to have a significant increase in perceptions of stress (β = 0.38, p = 0.0001). Women with trait anxiety also express a significant rise in perceptions of stress (β = 0.44, p = 0.0001) and reduction in confidence (β = −0.41, p = 0.001) [31]. In another study, distress associated with genetic testing for BRCA1/2 was not moderated by test results, and it remained constantly high in patients with high baseline level of distress and remained low in those with low baseline level of distress [32]. Moreover, problems of memory and concentration may occur following RRSO [25], and higher levels of executive dysfunction in those patients are mediated by mood dysregulations pertinent to early life stress [33]. Chronic psychosocial stress persistently activates GR signaling allowing glucocorticoid dysregulation to trigger negative physiological and pathological effects, including the development of aggressive and drug-resistant cancers [34,35]. Taken together, poor response to MBSR in BRCA1/2 carriers probably implicates an insult of the hypothalamic-pituitary-adrenal (HPA) axis, which is associated with GR dysregulation secondary to the basic effects of BRCA1/2 mutations, which may be further exacerbated by an interplay with MBSR-induced methylation.
Our results highlight significant positive effects of HRT in women undergoing RRSO, especially in BRCA 2 carriers. HRT is prescribed to improved QoL following menopause by reducing perimenopausal symptoms and lowering the risk of osteoporosis and cardiovascular diseases [8,36]. Among healthy UK women aged 46–65 (105 199 HRT users and 224 643 matched non-users controls), combined HRT is associated with a 9% reduction in all-cause mortality [36]. Increased survival in menopausal women receiving HRT is probably due to improved overall physiological functioning. In this respect, experimental evidence shows that ovariectomized rats treated with phytoestrogens, compounds which act as estrogen receptor (ER) agonists such as Coumestrol, as well as 17β-estradiol (E2) replacement demonstrate improvement in voluntary physical activity, uterine growth, and metabolism (protein expression responsible for the browning of white fat and insulin signaling, including hepatic expression of fibroblast growth factor 21) [37]. In line, early HRT treatment in ovariectomized rats inhibits the shift in the ER α/β ratio and mitochondrial-related oxidative destruction of the cellular lipid and protein structures [18]. These findings provide a mechanism for justifying the reported improvement in all menopausal symptoms among HRT recipients with BRCA2 mutations across different groups in our study.
The positive effects of HRT were more profound among women who were premenopausal at the time of RRSO as well as in physically active women whereas smoking was associated with diminished benefits of HRT. Moreover, time elapsed since RRSO and age at RRSO consistently predicted psychological symptoms in women with BRCA1, those with no history of breast cancer, and those who were premenopausal at RRSO. Thus, greater benefits of HRT in RRSO patients may be achieved through early HRT administration along with a healthy lifestyle, especially in those who were premenopausal.
Lack of improvement secondary to HRT treatment in BRCA1 mutation carriers may be attributed to excessive oxidative stress associated with BRCA1 deficiency. BRCA1 protects against neuronal damage through a mechanism that involves activation of the Antioxidant Response Element signaling pathway as it interacts with the nuclear factor (erythroid-derived 2)-like 2 (NRF2) through BRCA1 C-terminal (BRCT) domain [6]. Estrogen as a neuroendocrine molecule affects neuronal metabolism and functioning [11]. Therefore, estrogen drop following RRSO in BRCA1 carriers may be associated with more severe (psychological) menopausal symptoms secondary to excessive neuronal alterations, especially within the context of intense redox failure associated with absence of the antioxidant effects of BRCA1 [6]. This justification seems feasible since HRT aggravated urogenital symptoms in women with a history of cancer in our study. The severity of menopausal symptoms is an indication for HRT. However, there seems to be an interplay between the mechanisms underlying severe menopausal symptoms and carcinogenesis. On one hand, severe menopausal symptoms may be linked to estrogen metabolism enzyme polymorphisms, which are associated with excessive overproduction of reactive oxygen species (ROS) and inappropriate detoxification due to reduced production of internal antioxidant enzymes [13,38,39]. As an example, improper inactivation of catechol estrogen quinones, specific reactive estrogen metabolites, allow the surge of ROS, which interact with DNA and promote the initiation of cancer by inducing mutations in critical genes [39]. On the other hand, estrogen and progesterone receptor (ER, PR) signaling regulates mammary cell development and interferes with breast carcinogenesis [3,40]. It regulates different mechanisms of the generation of ROS and corrosive free radicals, which promote carcinogenesis [38,39]. Accordingly, ER-targeted endocrine therapies have been employed to significantly improve clinical outcomes in breast cancer [3]. However, the literature reports HRT as a risk factor for cancer in menopausal women [17,41]. Concerning the target population of our investigation, a diagnostic meta-analysis of prospective studies reports an increased incidence of endometrial carcinoma in BRCA carriers receiving certain HRT types (e.g., tamoxifen) [42]. Likewise, a meta-analysis involving four RCTs with 4050 breast cancer survivors associates HRT with cancer recurrence in patients with hormone receptor-positive tumors (HR 1.8, 95% CI 1.15–2.82, p = 0.010) but not in those with hormone receptor-negative disease (HR 1.19, 95% CI 0.80–1.77, p = 0.390) [27]. In line, a pre-clinical trial involving the administration of physiologically relevant levels of E2 and progesterone (P4) to immunocompromised mice, which were formerly injected with ER plus breast cancer cell lines and patient-derived tumor cells in the milk ducts, resulted in increased tumor growth and metastatic spread. The proliferative mechanism was patient-specific, with low MYC family oncogene and androgen receptor signatures promoting transcription and proliferation upon stimulation with P4 [40]. HRT seems to aggravate oxidative stress in BRCA1/2 women with cancer who already express higher baseline levels of inflammation and oxidative stress, resulting in the potentiation of menopausal symptoms. In support of this logic, HRT significantly alleviated menopausal symptoms in participants without a history of breast cancer. Indeed, a large-scale study comprising 616 patients with confirmed breast cancer and 1,082 age and race-matched normal controls revealed that ever use and 5 years use of HRT is associated with increased risk of breast cancer. In the meantime, polymorphisms in the promoter region of the CAT gene (rs1001179) were not associated with breast cancer. However, CAT genotyping revealed a significant increase in the incidence of estrogen receptor-positive tumors in women with CT or TT variants who received HRT compared with women with CC allele who received HRT, suggesting that HRT contribution to breast cancer involves dysfunctional modulation of oxidative stress [43]. Therefore, HRT use among BRACA1/2 carriers may be considered at an individual level.
Strengths, Implications, and Limitations
This study has the merit of employing already available public data to investigate the effects of HRT and MBSR on menopausal symptoms among BRACA1/2 carriers who underwent RRSO. The results revealed that MBSR was ineffective/harmful while HRT exerted positive effects in certain groups. Lifestyle (e.g., physical activity and smoking) was an important factor that interfered with the effects of HRT. In this study, most participants (61.1%) reported engagement in physical activity for 30 minutes or more per day for 5 days or more. Although exercise activates signaling cascades involved in the correction of metabolic dysfunctions, autophagy, and the production of antioxidants—which all promote optimal physiological functioning [44,45,46]—none of the menopausal symptoms correlated with physical activity. Thus, participating in physical activity alone does not seem to be effective for the management of menopausal symptoms in this population. However, it is worth mentioning that categorizing physical activity into two groups (0-4 days; 5 days or more) in the current study might have precluded estimating the differences between those who do not participate in physical activity at all and those who do. In addition, the level of physical activity (mild, moderate, and strenuous) was not evaluated, which may be considered in future studies. Because of the likely negative effects of HRT in women with a history of cancer, the need is ongoing to search for possible alternatives to HRT that worth investigation of their anti-menopausal effects in this population such as natural phytochemicals/phytoestrogens — a large family of molecules that exist in natural products (e.g., royal jelly, bee honey, soybeans, floral pollen, etc.), which mimic the physiological effects of estrogen [11,47]. Natural agents with potent anti-inflammatory activities (e.g., propolis, black cumin seeds, ginger,) may also be particularly helpful [48]. This is because investigations involving BRCA1-mutated luteal phase samples show that BRCA1 mutations activate TNF-α-induced NF-κB activity and mRNA expression of NF-κB-dependent target gene superoxide dismutase 2 resulting in prolonged postovulatory inflammation in nonmalignant fallopian tube epithelium [9]. Traditional alternative modalities such as foot herbal water baths, foot massage/reflexology, and acupuncture, which are reported to exert anti-menopausal effects [47], represent other options that deserve research attention to alleviate the suffering associated with sharp menopausal onset following RRSO among women with BRCA1/2 gene mutations.
This study has some limitations, which may call for caution when interpreting the current findings. Although an experimental design was originally initiated, we could only use post-experimental cross-sectional data, which were available. Lack of pre-treatment measures of menopausal symptoms may confound the reports. The data of 11 participants from the original experimental group were missing—attrition risk may also bias the results. Data collection took place over a long period of time following the intervention. Thus, the results may be influenced by the time-treatment effect. Some variables were vaguely defined, e.g., physical activity was assessed as 30 minutes per day regardless of the level of the activity. Data on compliance with MBSR and women’s satisfaction with this therapy were also missing.
Conclusions
The results uncover the high prevalence of menopausal symptoms following RRSO in BRCA1/2 mutation carriers, with psychological distress frequently mirroring the severity of somatic and urogenital discomforts. Menopausal symptoms following RRSO should not be underestimated given their significant influence on women's quality of life. This realization emphasizes the need for individualized interventions that target the various facets of menopausal symptoms. HRT arises as a ray of hope for alleviating menopausal symptoms in specific subgroups: BRCA2 carriers, premenopausal, physically active, and nonsmoking women. Accordingly, lifestyle factors such as physical activity and smoking have a substantial impact on its efficacy. Moreover, the administration of HRT necessitates a nuanced evaluation of its potential benefits and risks, particularly for those with a breast cancer history—highlighting the significance of individualized care in BRCA1/2 carriers. On the other hand, MBSR presents a more complex picture, implying that its utility may not be ubiquitous, and that caution should be exercised when contemplating it as an intervention for this specific population. Our study emphasizes ongoing efforts to improve the well-being of BRCA1/2 carriers, highlighting the critical need for of further investigations in refining mechanisms underlying therapeutic strategies and providing individualized solutions to alleviate their suffering.
Ethics approval and consent to participate
The protocol of data collection was approved by the Medical Ethical Committee of the UMCG on 14 November 2014 (registration no. NL46796.042.14). For the current analysis, no ethical approval was obtained because we used a public dataset shared under the terms of Creative Common License (CC BY 4.0) [22]. The present study was conducted according to the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest.
Author Contributions
Conceptualization, Amira Ali and Haitham Khatatbeh; Data curation, Musheer A Aljaberi and Haitham Khatatbeh; Formal analysis, Amira Ali, Saeed Al-Dossary, Ebtesam Abdullah Alzeiby Alzeiby and Hammad Fadlalmola; Investigation, Abdulmajeed A. Alkhamees and Musheer A Aljaberi; Methodology, Saeed Al-Dossary and Carlos Laranjeira; Project administration, Amira Ali; Resources, Carlos Laranjeira, Faten Amer, Souheil Hallit, Abdulmajeed A. Alkhamees and Annamária Pakai; Validation, Amira Ali, Saeed Al-Dossary and Hammad Fadlalmola; Visualization, Aljawharah Aljubilah; Writing – original draft, Faten Amer, Aljawharah Aljubilah, Ebtesam Abdullah Alzeiby Alzeiby, Annamária Pakai and Haitham Khatatbeh; Writing – review & editing, Carlos Laranjeira, Souheil Hallit and Hammad Fadlalmola.
Funding
None.
Data Availability Statement
The dataset supporting the conclusions of this article is available in Mendeley repository [22], [https://data.mendeley.com/datasets/6wtd46ry6s], and also the datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
- Noman, S.; Shahar, H.K.; Abdul Rahman, H.; Ismail, S.; Abdulwahid Al-Jaberi, M.; Azzani, M. The Effectiveness of Educational Interventions on Breast Cancer Screening Uptake, Knowledge, and Beliefs among Women: A Systematic Review. International Journal of Environmental Research and Public Health 2021, 18, 263. [Google Scholar] [CrossRef]
- Ling, J.; Kumar, R. Crosstalk between NFkB and glucocorticoid signaling: A potential target of breast cancer therapy. Cancer Lett 2012, 322, 119–126. [Google Scholar] [CrossRef]
- Fei, F.; Siegal, G.P.; Wei, S. Characterizing Clinicopathologic Features of Estrogen Receptor-Positive/Progesterone Receptor-Negative Breast Cancers. Clin Breast Cancer 2022, 22, e788–e797. [Google Scholar] [CrossRef] [PubMed]
- Rosen, E.M.; Fan, S.; Pestell, R.G.; Goldberg, I.D. BRCA1 gene in breast cancer. Journal of Cellular Physiology 2003, 196, 19–41. [Google Scholar] [CrossRef] [PubMed]
- Xie, C.; Luo, J.; He, Y.; Jiang, L.; Zhong, L.; Shi, Y. BRCA2 gene mutation in cancer. Medicine (Baltimore) 2022, 101, e31705. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.; Liu, Q.; Xie, Y.; Shi, X.; Li, Y.; Peng, M.; Guo, H.; Sun, R.; Li, J.; Hong, Y.; et al. Breast cancer susceptibility protein 1 (BRCA1) rescues neurons from cerebral ischemia/reperfusion injury through NRF2-mediated antioxidant pathway. Redox Biology 2018, 18, 158–172. [Google Scholar] [CrossRef] [PubMed]
- Djedovic, V. BRCA1 modulation of glucocorticoid receptor signaling in high-grade serous ovarian cancer cells. University of Toronto, Canada, 2016.
- Stuursma, A.; van Driel, C.M.G.; Wessels, N.J.; de Bock, G.H.; Mourits, M.J.E. Severity and duration of menopausal symptoms after risk-reducing salpingo-oophorectomy. Maturitas 2018, 111, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Tone, A.A.; Virtanen, C.; Shaw, P.; Brown, T.J. Prolonged postovulatory proinflammatory signaling in the fallopian tube epithelium may be mediated through a BRCA1/DAB2 axis. Clin Cancer Res 2012, 18, 4334–4344. [Google Scholar] [CrossRef] [PubMed]
- van Driel, C.; de Bock, G.H.; Schroevers, M.J.; Mourits, M.J. Mindfulness-based stress reduction for menopausal symptoms after risk-reducing salpingo-oophorectomy (PURSUE study): a randomised controlled trial. Bjog 2019, 126, 402–411. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Kunugi, H. Royal jelly as an intelligent anti-aging—a focus on cognitive aging and Alzheimer's disease: a review. Antioxidants 2020, 9, E937. [Google Scholar] [CrossRef] [PubMed]
- Rangel-Zuñiga, O.A.; Cruz-Teno, C.; Haro, C.; Quintana-Navarro, G.M.; Camara-Martos, F.; Perez-Martinez, P.; Garcia-Rios, A.; Garaulet, M.; Tena-Sempere, M.; Lopez-Miranda, J.; et al. Differential menopause- versus aging-induced changes in oxidative stress and circadian rhythm gene markers. Mech Ageing Dev 2017, 164, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Rodríguez, M.A.; Zacarías-Flores, M.; Arronte-Rosales, A.; Mendoza-Núñez, V.M. Association between hot flashes severity and oxidative stress among Mexican postmenopausal women: A cross-sectional study. PLoS One 2019, 14, e0214264. [Google Scholar] [CrossRef] [PubMed]
- Shea, A.K.; Sohel, N.; Gilsing, A.; Mayhew, A.J.; Griffith, L.E.; Raina, P. Depression, hormone therapy, and the menopausal transition among women aged 45 to 64 years using Canadian Longitudinal Study on aging baseline data. Menopause 2020. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Ahmed, A.H.; Smail, L. Psychological Climacteric Symptoms and Attitudes toward Menopause among Emirati Women. Int. J. Environ. Res. Public Health 2020, 17, 5028. [Google Scholar] [CrossRef] [PubMed]
- Leal, M.; Díaz, J.; Serrano, E.; Abellán, J.; Carbonell, L.F. Hormone replacement therapy for oxidative stress in postmenopausal women with hot flushes. Obstet Gynecol 2000, 95, 804–809. [Google Scholar] [CrossRef] [PubMed]
- Szabó, R.; Hoffmann, A.; Börzsei, D.; Kupai, K.; Veszelka, M.; Berkó, A.M.; Pávó, I.; Gesztelyi, R.; Juhász, B.; Turcsán, Z.; et al. Hormone Replacement Therapy and Aging: A Potential Therapeutic Approach for Age-Related Oxidative Stress and Cardiac Remodeling. Oxid Med Cell Longev 2021, 2021, 8364297. [Google Scholar] [CrossRef]
- López-Grueso, R.; Gambini, J.; Abdelaziz, K.M.; Monleón, D.; Díaz, A.; El Alami, M.; Bonet-Costa, V.; Borrás, C.; Viña, J. Early, but not late onset estrogen replacement therapy prevents oxidative stress and metabolic alterations caused by ovariectomy. Antioxid Redox Signal 2014, 20, 236–246. [Google Scholar] [CrossRef]
- Geukes, M.; Anema, J.R.; van Aalst, M.P.; de Menezes, R.X.; Oosterhof, H. Improvement of menopausal symptoms and the impact on work ability: A retrospective cohort pilot study. Maturitas 2019, 120, 23–28. [Google Scholar] [CrossRef]
- Gordon, J.L.; Halleran, M.; Beshai, S.; Eisenlohr-Moul, T.A.; Frederick, J.; Campbell, T.S. Endocrine and psychosocial moderators of mindfulness-based stress reduction for the prevention of perimenopausal depressive symptoms: A randomized controlled trial. Psychoneuroendocrinology 2021, 130, 105277. [Google Scholar] [CrossRef]
- Yazdani Aliabadi, M.; Javadnoori, M.; Saki Malehi, A.; Aslani, K. A study of mindfulness-based stress-reduction training effects on menopause-specific quality of life in postmenopausal women: A randomized controlled trial. Complement Ther Clin Pract 2021, 44, 101398. [Google Scholar] [CrossRef]
- Stuursma, A.; Wessels, N.; Bock, G.H.d.; Mourits, M.; Driel, C.V. Data for: Severity and duration of menopausal symptoms after risk-reducing salpingo-oophorectomy. Mendeley Data 2018, Version 1, doi:10.17632/6wtd46ry6s.1. 1. [CrossRef]
- Ali, A.M.; Hendawy, A.O.; Al-Amer, R.; Shahrour, G.; Ali, E.M.; Alkhamees, A.A.; Ibrahim, N.; Lamadah, S.M.T.; Ahmed, A.H. Psychometric evaluation of the Depression Anxiety Stress Scale 8 among women with chronic non-cancer pelvic pain. Scientific Reports 2022, 12, 20693. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Al-Amer, R.; Kunugi, H.; Stănculescu, E.; Taha, S.M.; Saleh, M.Y.; Alkhamees, A.A.; Hendawy, A.O. The Arabic version of the Impact of Event Scale – Revised: Psychometric evaluation in psychiatric patients and the general public within the context of COVID-19 outbreak and quarantine as collective traumatic events. Journal of Personalized Medicine 2022, 12, 681. [Google Scholar] [CrossRef] [PubMed]
- Stanisz, M.; Panczyk, M.; Kurzawa, R.; Grochans, E. The Effect of Prophylactic Adnexectomy on the Quality of Life and Psychosocial Functioning of Women with the BRCA1/BRCA2 Mutations. International Journal of Environmental Research and Public Health 2019, 16, 4995. [Google Scholar] [CrossRef] [PubMed]
- Borreani, C.; Manoukian, S.; Bianchi, E.; Brunelli, C.; Peissel, B.; Caruso, A.; Morasso, G.; Pierotti, M.A. The psychological impact of breast and ovarian cancer preventive options in BRCA1 and BRCA2 mutation carriers. Clin Genet 2014, 85, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Poggio, F.; Del Mastro, L.; Bruzzone, M.; Ceppi, M.; Razeti, M.G.; Fregatti, P.; Ruelle, T.; Pronzato, P.; Massarotti, C.; Franzoi, M.A.; et al. Safety of systemic hormone replacement therapy in breast cancer survivors: a systematic review and meta-analysis. Breast Cancer Res Treat 2022, 191, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Bishop, J.R.; Lee, A.M.; Mills, L.J.; Thuras, P.D.; Eum, S.; Clancy, D.; Erbes, C.R.; Polusny, M.A.; Lamberty, G.J.; Lim, K.O. Methylation of FKBP5 and SLC6A4 in Relation to Treatment Response to Mindfulness Based Stress Reduction for Posttraumatic Stress Disorder. Front Psychiatry 2018, 9, 418. [Google Scholar] [CrossRef] [PubMed]
- Giudice, A.; Aliberti, S.M.; Barbieri, A.; Pentangelo, P.; Bisogno, I.; D'Arena, G.; Cianciola, E.; Caraglia, M.; Capunzo, M. Potential Mechanisms by which Glucocorticoids Induce Breast Carcinogenesis through Nrf2 Inhibition. Front Biosci (Landmark Ed) 2022, 27, 223. [Google Scholar] [CrossRef] [PubMed]
- McNamara, K.M.; Kannai, A.; Sasano, H. Possible roles for glucocorticoid signalling in breast cancer. Mol Cell Endocrinol 2018, 466, 38–50. [Google Scholar] [CrossRef] [PubMed]
- Halbert, C.H.; Schwartz, M.D.; Wenzel, L.; Narod, S.; Peshkin, B.N.; Cella, D.; Lerman, C. Predictors of Cognitive Appraisals Following Genetic Testing for BRCA1 and BRCA2 Mutations. J Behav Med 2004, 27, 373–392. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.W.; Dougall, A.L.; Posluszny, D.M.; Somers, T.J.; Rubinstein, W.S.; Baum, A. Psychological distress and quality of life associated with genetic testing for breast cancer risk. Psychooncology 2008, 17, 767–773. [Google Scholar] [CrossRef] [PubMed]
- Shanmugan, S.; Sammel, M.D.; Loughead, J.; Ruparel, K.; Gur, R.C.; Brown, T.E.; Faust, J.; Domchek, S.; Epperson, C.N. Executive function after risk-reducing salpingo-oophorectomy in BRCA1 and BRCA2 mutation carriers: does current mood and early life adversity matter? Menopause 2020, 27, 746–755. [Google Scholar] [CrossRef] [PubMed]
- Woods-Burnham, L.; Stiel, L.; Martinez, S.R.; Sanchez-Hernandez, E.S.; Ruckle, H.C.; Almaguel, F.G.; Stern, M.C.; Roberts, L.R.; Williams, D.R.; Montgomery, S.; et al. Psychosocial Stress, Glucocorticoid Signaling, and Prostate Cancer Health Disparities in African American Men. Cancer Health Disparities 2020, 4, e1–e30. [Google Scholar]
- Halbert, C.H.; Jefferson, M.S.; Danielson, C.; Froeliger, B.; Giordano, A.; Thaxton, J.E. An observational study and randomized trial of stress reactivity in cancer disparities. Health Psychol 2020, 39, 745–757. [Google Scholar] [CrossRef] [PubMed]
- Akter, N.; Kulinskaya, E.; Steel, N.; Bakbergenuly, I. The effect of hormone replacement therapy on the survival of UK women: a retrospective cohort study 1984−2017. BJOG 2022, 129, 994–1003. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Sim, K.-S.; Heo, W.; Kim, J.-H. Protective Effects of Coumestrol on Metabolic Dysfunction and Its Estrogen Receptor-Mediated Action in Ovariectomized Mice. Nutrients 2023, 15, 954. [Google Scholar] [CrossRef] [PubMed]
- Wen, C.; Wu, L.; Fu, L.; Wang, B.; Zhou, H. Unifying mechanism in the initiation of breast cancer by metabolism of estrogen (Review). Mol Med Rep 2017, 16, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Faria, C.C.; Peixoto, M.S.; Carvalho, D.P.; Fortunato, R.S. The Emerging Role of Estrogens in Thyroid Redox Homeostasis and Carcinogenesis. Oxid Med Cell Longev 2019, 2019, 2514312. [Google Scholar] [CrossRef] [PubMed]
- Scabia, V.; Ayyanan, A.; De Martino, F.; Agnoletto, A.; Battista, L.; Laszlo, C.; Treboux, A.; Zaman, K.; Stravodimou, A.; Jallut, D.; et al. Estrogen receptor positive breast cancers have patient specific hormone sensitivities and rely on progesterone receptor. Nature Communications 2022, 13, 3127. [Google Scholar] [CrossRef] [PubMed]
- Kunugi, H.; Ali, A.M. Royal Jelly and Its Components Promote Healthy Aging and Longevity: From Animal Models to Humans. Int. J. Mol. Sci 2019, 20, 4662. [Google Scholar] [CrossRef] [PubMed]
- Lu, G.; Lu, T.; Pan, J.; Guo, L.; Pang, Y.; Liu, P. Association between BRCA mutations and endometrial carcinoma: a systematic review with meta-analysis. Arch Gynecol Obstet 2021, 303, 1569–1579. [Google Scholar] [CrossRef] [PubMed]
- Quick, S.K.; Shields, P.G.; Nie, J.; Platek, M.E.; McCann, S.E.; Hutson, A.D.; Trevisan, M.; Vito, D.; Modali, R.; Lehman, T.A.; et al. Effect modification by catalase genotype suggests a role for oxidative stress in the association of hormone replacement therapy with postmenopausal breast cancer risk. Cancer Epidemiol Biomarkers Prev 2008, 17, 1082–1087. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Ali, E.M.; Mousa, A.A.; Ahmed, M.E.; Hendawy, A.O. Bee honey and exercise for improving physical performance, reducing fatigue, and promoting an active lifestyle during COVID-19. Sports Med Health Sci 2021, 3, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Kunugi, H. Physical frailty/sarcopenia as a key predisposing factor to coronavirus disease 2019 (COVID-19) and its complications in older adults. BioMed 2021, 1, 11–40. [Google Scholar] [CrossRef]
- Ali, A.M.; Kunugi, H. Apitherapy for age-related skeletal muscle dysfunction (sarcopenia): A review on the effects of royal jelly, propolis, and bee pollen. Foods 2020, 9, E1362. [Google Scholar] [CrossRef] [PubMed]
- Pinkerton, J.V.; Stovall, D.W.; Kightlinger, R.S. Advances in the treatment of menopausal symptoms. Womens Health (Lond) 2009, 5, 361–384. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Alkhamees, A.A.; Al-Dwaikat, T.N.; Khatatbeh, H.; A1-Dossary, S.A. The Depression Anxiety Stress Scale 8: Investigating its cutoff scores in relevance to loneliness and burnout among dementia family caregivers. Research Square 2023, V1. [Google Scholar] [CrossRef]
Figure 1.
Path analysis predicting the effects of mindfulness-based stress reduction (MBSR) and hormonal replacement therapy (HRT) on different menopausal symptoms among women with risk-reducing salpingo-oophorectomy (RRSO).
Figure 1.
Path analysis predicting the effects of mindfulness-based stress reduction (MBSR) and hormonal replacement therapy (HRT) on different menopausal symptoms among women with risk-reducing salpingo-oophorectomy (RRSO).
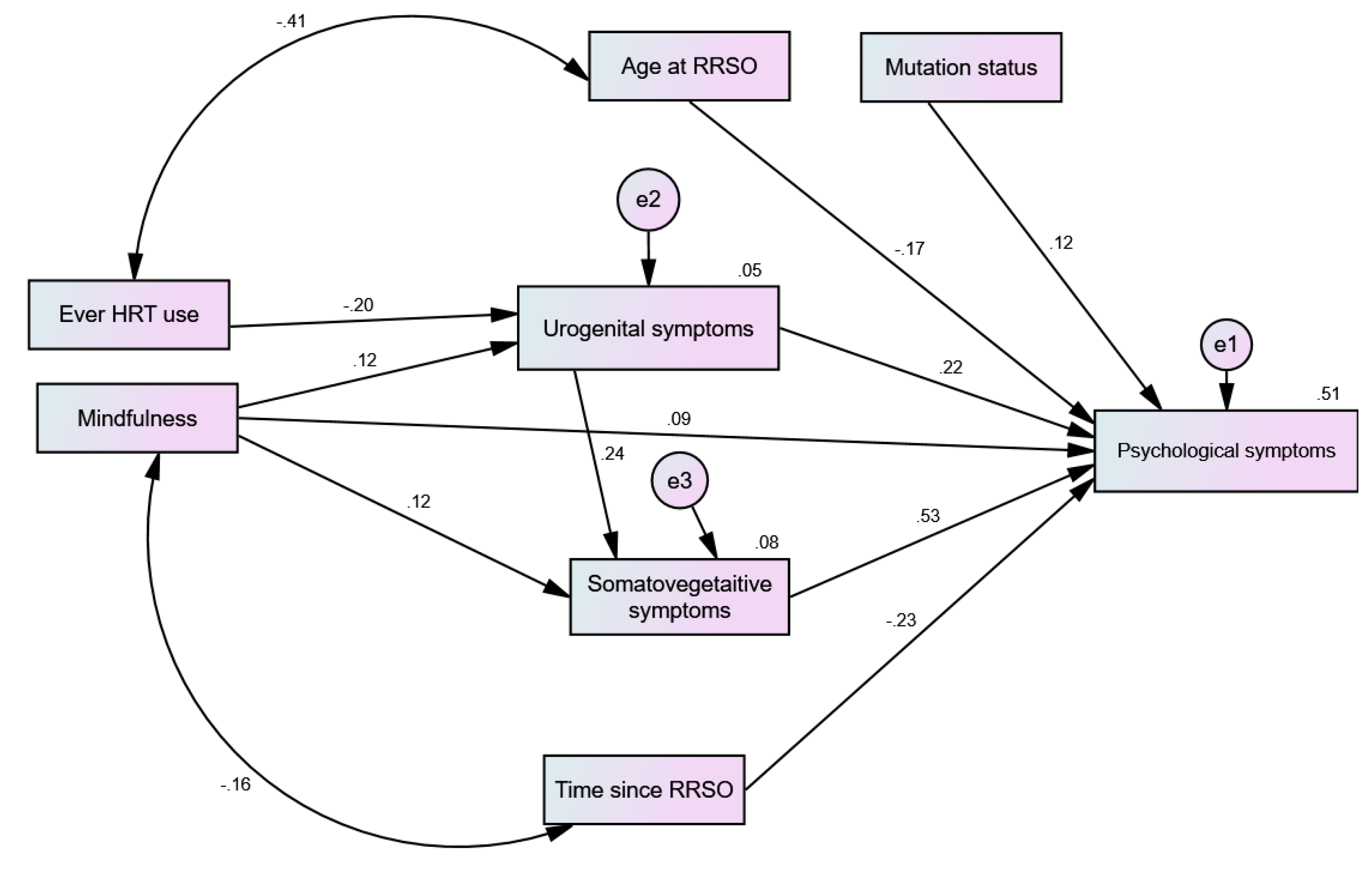

Table 1.
Multigroup analysis examining the effects of mindfulness-based stress reduction (MBSR) and hormone replacement therapy (HRT) across groups of BRCA1/2 mutation carriers.
Table 1.
Multigroup analysis examining the effects of mindfulness-based stress reduction (MBSR) and hormone replacement therapy (HRT) across groups of BRCA1/2 mutation carriers.
| Predictors | Type of Mutation | Type of Effect | Outcome Variables | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Urogenital | Somatic-Vegetative | Psychological | |||||||||
| β | p | 95% CI | β | p | 95% CI | β | p | 95% CI | |||
| MBSR | BRCA1 BRCA2 |
Direct Indirect Direct Indirect |
-0.006 0.304 |
0.905 0.001 |
-0.200 to 0.160 0.157 to 0.439 |
0.164 -0.001 0.112 0.066 |
0.039 0.892 0.259 0.052 |
0.010 to 0.330 -0.058 to 0.045 -0.073 to 0.311 -0.001 to 0.172 |
0.089 0.085 0.116 0.172 |
0.263 0.071 0.158 0.010 |
-0.065 to 0.230 -0.006 to 0.173 -0.039 to 0.285 0.042 to 0.305 |
| HRT | BRCA1 BRCA2 |
Direct Indirect Direct Indirect |
-0.160 -0.291 |
0.119 0.019 |
-0.342 to 0.031 0.498 to -0.049 |
-0.039 -0.063 |
0.078 0.063 |
-0.124 to 0.003 -0.200 to 0.003 |
-0.049 -0.102 |
0.089 0.018 |
-0.133 to 0.005 -0.257 to -0.011 |
MBSR: Mindfulness-based stress reduction; HRT: hormone replacement therapy; bold-face values reflect significant results.
Table 2.
Multigroup analysis examining the effects of mindfulness-based stress reduction (MBSR) and hormone replacement therapy (HRT) across groups of history of breast cancer.
Table 2.
Multigroup analysis examining the effects of mindfulness-based stress reduction (MBSR) and hormone replacement therapy (HRT) across groups of history of breast cancer.
| Predictors | Breast Cancer History | Type of Effect | Outcome Variables | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Urogenital | Somatic-Vegetative | Psychological | |||||||||
| β | p | 95% CI | β | p | 95% CI | β | p | 95% CI | |||
| MBSR | Yes No |
Direct Indirect Direct Indirect |
0.105 0.156 |
0.191 0.082 |
-0.073 to 0.227 -0.018 to 0.283 |
0.211 -0.004 0.086 0.049 |
0.004 0.565 0.175 0.054 |
0.054 to 0.362 -0.049 to 0.020 -0.038 to 0.222 -0.001 to 0.117 |
0.163 0.113 0.054 0.108 |
0.045 0.004 0.351 0.012 |
0.003 to 0.311 0.038 to 0.216 -0.063 to 0.171 0.019 to 0.189 |
| HRT | Yes No |
Direct Indirect Direct Indirect |
0.169 -0.191 |
0.024 0.030 |
0.026 to 0.277 -0.351 to -0.022 |
-0.006 -0.060 |
0.701 0.019 |
-0.052 to 0.034 -0.133 to -0.010 |
0.008 -0.078 |
0.634 0.022 |
-0.039 to 0.060 -0.158 to -0.012 |
MBSR: Mindfulness-based stress reduction; HRT: hormone replacement therapy; bold-face values reflect significant results.
Table 3.
Multigroup analysis examining the effects of mindfulness-based stress reduction (MBSR) and hormone replacement therapy (HRT) across groups of menopausal status at the time of RRSO.
Table 3.
Multigroup analysis examining the effects of mindfulness-based stress reduction (MBSR) and hormone replacement therapy (HRT) across groups of menopausal status at the time of RRSO.
| Predictors | Menopausal Status | Type of Effect | Outcome Variables | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Urogenital | Somatic-Vegetative | Psychological | |||||||||
| β | p | 95% CI | β | p | 95% CI | β | p | 95% CI | |||
| MBSR | Menopausal Pre-menopausal |
Direct Indirect Direct Indirect |
0.201 0.134 |
0.038 0.124 |
0.009 to 0.375 -0.032 to 0.263 |
0.234 0.045 0.141 0.032 |
0.017 0.080 0.031 0.082 |
0.033 to 0.470 -0.004 to 0.156 0.011 to 0.276 -0.003 to 0.091 |
0.059 0.202 0.111 0.120 |
0.626 0.006 0.099 0.002 |
-0.179 to 0.306 0.046 to 0.383 -0.018 to 0.229 0.041 to 0.204 |
| HRT | Menopausal Pre-menopausal |
Direct Indirect Direct Indirect |
-0.081 -0.212 |
0.575 0.016 |
-0.461 to 0.199 -0.366 to -0.032 |
-0.018 -0.051 |
0.396 0.016 |
-0.170 to 0.036 -0.123 to -0.007 |
-0.037 -0.069 |
0.472 0.010 |
-0.270 to 0.080 -0.147 to -0.012 |
MBSR: Mindfulness-based stress reduction; HRT: hormone replacement therapy; bold-face values reflect significant results.
Table 4.
Multigroup analysis examining the effects of mindfulness-based stress reduction (MBSR) and hormone replacement therapy (HRT) across groups of body mass index.
Table 4.
Multigroup analysis examining the effects of mindfulness-based stress reduction (MBSR) and hormone replacement therapy (HRT) across groups of body mass index.
| Predictors | Body Mass Index | Type of Effect | Outcome Variables | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Urogenital | Somatic-Vegetative | Psychological | |||||||||
| β | p | 95% CI | β | p | 95% CI | β | p | 95% CI | |||
| MBSR | ≤25 >25 |
Direct Indirect Direct Indirect |
0.203 -0.008 |
0.001 0.919 |
0.104 to 0.303 -0.213 to 0.164 |
0.075 0.042 0.179 -0.002 |
0.217 0.031 0.020 0.920 |
-0.044 to 0.212 0.004 to 0.098 0.023 to 0.339 -0.063 to 0.054 |
0.140 0.098 0.039 0.099 |
0.084 0.006 0.510 0.073 |
-0.021 to 0.285 0.024 to 0.180 -0.084 to 0.152 -0.009 to 0.205 |
| HRT | ≤25 >25 |
Direct Indirect Direct Indirect |
-0.068 -0.351 |
0.489 0.003 |
-0.540 to -0.125 -0.366 to -0.032 |
-0.014 -0.104 |
0.355 0.003 |
-0.083 to 0.013 -0.217 to -0.028 |
-0.020 -0.130 |
0.415 0.001 |
-0.094 to 0.030 -0.258 to -0.041 |
MBSR: Mindfulness-based stress reduction; HRT: hormone replacement therapy; bold-face values reflect significant results.
Table 5.
Multigroup analysis examining the effects of mindfulness-based stress reduction (MBSR) and hormone replacement therapy (HRT) across groups of physical activity level.
Table 5.
Multigroup analysis examining the effects of mindfulness-based stress reduction (MBSR) and hormone replacement therapy (HRT) across groups of physical activity level.
| Predictors | Physical Activity Level | Type of Effect | Outcome Variables | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Urogenital | Somatic-Vegetative | Psychological | |||||||||
| β | p | 95% CI | β | p | 95% CI | β | p | 95% CI | |||
| MBSR | Yes No |
Direct Indirect Direct Indirect |
0.134 0.090 |
0.145 0.301 |
-0.058 to 0.275 -0.077 to 0.233 |
0.132 0.046 0.129 0.016 |
0.076 0.080 0.061 0.198 |
-0.015 to 0.291 -0.007 to 0.125 -0.009 to 0.274 -0.008 to 0.065 |
0.052 0.120 0.112 0.099 |
0.548 0.042 0.043 0.006 |
-0.113 to 0.211 0.004 to 0.230 0.003 to 0.221 0.022 to 0.182 |
| HRT | Yes No |
Direct Indirect Direct Indirect |
-0.162 -0.201 |
0.205 0.019 |
-0.390 to 0.082 -0.363 to -0.022 |
-0.056 -0.035 |
0.129 0.061 |
-0.171 to 0.018 -0.102 to 0.001 |
-0.070 -0.059 |
0.176 0.012 |
-0.199 to 0.029 -0.137 to -0.008 |
MBSR: Mindfulness-based stress reduction; HRT: hormone replacement therapy; bold-face values reflect significant results.
Table 6.
Multigroup analysis examining the effects of mindfulness-based stress reduction (MBSR) and hormone replacement therapy (HRT) across smoking groups.
Table 6.
Multigroup analysis examining the effects of mindfulness-based stress reduction (MBSR) and hormone replacement therapy (HRT) across smoking groups.
| Predictors | Smoking | Type of Effect | Outcome Variables | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Urogenital | Somatic-Vegetative | Psychological | |||||||||
| β | p | 95% CI | β | p | 95% CI | β | p | 95% CI | |||
| MBSR | Yes No |
Direct Indirect Direct Indirect |
0.292 0.086 |
0.002 0.193 |
0.099 to 0.554 -0.050 to 0.189 |
-0.289 0.202 0.161 0.018 |
0.029 0.002 0.001 0.108 |
-0.526 to -0.013 0.057 to 0.479 0.055 to 0.272 -0.004 to 0.055 |
0.097 0.008 0.098 0.114 |
0.462 0.983 0.074 0.001 |
-0.182 to 0.438 -0.282 to 0.264 -0.009 to 0.200 0.049 to 0.182 |
| HRT | Yes No |
Direct Indirect Direct Indirect |
0.035 -0.247 |
0.876 0.004 |
-0.403 to 0.502 -0.381 to -0.067 |
0.024 -0.051 |
0.857 0.006 |
-0.308 to 0.322 -0.111 to -0.011 |
0.019 -0.084 |
0.829 0.002 |
-0.246 to 0.256 -0.152 to -0.030 |
MBSR: Mindfulness-based stress reduction; HRT: hormone replacement therapy; bold-face values reflect significant results.
Table 7.
Standardized total effects of age at RRSO and time elapsed since RRSO on psychological menopausal symptoms across different groups among women undergoing RRSO.
Table 7.
Standardized total effects of age at RRSO and time elapsed since RRSO on psychological menopausal symptoms across different groups among women undergoing RRSO.
| Predictors | Groups | β | p | 95% CI |
|---|---|---|---|---|
|
Age at RRSO Time since RRSO |
Type of mutation BRCA1 BRCA2 BRCA1 BRCA2 |
-0.224 -0.122 -0.210 -0.084 |
0.002 0.234 0.003 0.316 |
-0.393 to -0.077 -0.351 to 0.083 -0.342 to -0.067 -0.258 to 0.081 |
|
Age at RRSO Time since RRSO |
Menopausal status Yes No Yes No |
-0.010 0.064 -0.176 0.053 |
0.937 0.001 0.215 0.001 |
-0.307 to 0.251 -0.357 to -0.151 -0.458 to 0.087 -0.379 to -0.135 |
|
Age at RRSO Time since RRSO |
Body mass index ≤25 >25 ≤25 >25 |
-0.189 -0.142 -0.154 -0.309 |
0.006 0.120 0.031 0.001 |
-0.331 to -0.052 -0.307 to 0.034 -0.278 to -0.014 -0.438 to -0.171 |
|
Age at RRSO Time since RRSO |
Cancer history Yes No Yes No |
-0.065 -0.234 -0.275 -0.239 |
0.475 0.001 0.003 0.001 |
-0.245 to 0.109 -0.368 to -0.104 -0.454 to -0.097 -0.346 to -0.124 |
|
Age at RRSO Time since RRSO |
Current smoking Yes No Yes No |
-0.243 -0.156 -0.133 -0.221 |
0.327 0.011 0.507 0.001 |
-0.518 to 0.307 -0.271 to -0.036 -0.451 to 0.266 -0.320 to -0.117 |
|
Age at RRSO Time since RRSO |
Physical activity 0 to 4 days > 4 days 0 to 4 days > 4 days |
-0.095 -0.185 -0.311 -0.162 |
0.256 0.005 0.001 0.013 |
-0.266 to 0.072 -0.316 to -0.055 -0.452 to -0.166 -0.278 to -0.041 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



