
Submitted:
12 June 2024
Posted:
13 June 2024
You are already at the latest version
Abstract
In Pakistan, the incidence of HIV/AIDS is rising, particularly among transgender individuals, who face significant marginalization in various aspects of life, leading to compromised health-related quality of life (HRQoL). This study aimed to assess the HRQoL of transgender individuals living with HIV/AIDS and explore its correlation with social disparities. Using the validated WHO EQ-5D-5L scale, HRQoL was evaluated among 106 transgender patients with HIV/AIDS from Mayo Hospital and Fountain House Hospital, Lahore, Pakistan, following ethical considerations with PACP. Data analysis employed the Mann-Whitney and Kruskal Wallis tests. The research revealed that HIV/AIDS moderately impacts the HRQoL of transgender individuals due to physical, psychological, and social factors. Comorbidities further exacerbated the HRQoL among this population. In conclusion, managing multiple health issues, including comorbidities, can substantially diminish the quality of life for transgender individuals with HIV/AIDS. Hence, comprehensive healthcare services should address both HIV/AIDS and associated comorbidities to ensure holistic care.
Keywords:
HIV/AIDS
; HRQoL
; Transgender
; EQ-5D
; VAS
; Khuwaja Sara
1. Introduction
Transgender individuals, who identify with a gender different from their as-signed sex at birth, encounter numerous challenges globally (7). In Pakistan, the Transgender Persons (Protection of Rights) Act of 2018 defines transgender persons as those whose gender identity deviates from societal norms and their assigned sex at birth (8). Despite legal recognition, transgender individuals in Pakistan grapple with marginalization across various domains, including education, employment, healthcare access, and compounded by factors such as mental health issues, physical violence, social isolation, economic disparities, and inadequate healthcare services tailored to their needs (10).
The global HIV pandemic first emerged prominently in 1981, initially recognized through opportunistic diseases affecting young homosexual males, eventually leading to the identification of HIV as the causative agent (11). As of 2021, an estimated 38.4 million people worldwide were living with HIV, with transgender individuals being particularly susceptible, being 13 times more likely to be infected (12,13).
In Pakistan, the HIV situation is further exacerbated among transgender com-munities. They are 49 times more likely to be infected compared to the general popu-lation, reflecting the magnitude of the issue (15). The existing epidemiological data also suggests a concerning increase in HIV cases among transgender individuals across different provinces, highlighting the urgent need for targeted interventions and policy reforms (14,15).
Sexually transmitted infections (STIs) further compound the health challenges faced by transgender individuals, with viral STDs such as HIV, HSV, HBV, HPV, and HTLV-1 presenting significant treatment challenges due to limited therapeutic op-tions (16-18). Given the high prevalence and transmission rates of STDs among this population, understanding their health-related quality of life becomes imperative for designing effective prevention and treatment strategies (21). Moreover, HIV not only compromises the immune system, leading to severe health complications but also sig-nificantly impacts an individual’s quality of life by affecting their physical, emotional, and social well-being (22,23).
Health-related quality of life (HRQoL) serves as a crucial indicator of an indi-vidual’s overall well-being, encompassing physical, psychological, social, and role-related aspects of their life (1,3). As delineated by the World Health Organization (WHO), Quality of Life represents an individual’s perception of their position in life, taking into account cultural and societal norms, aspirations, and concerns (2). This multidimensional concept, HRQoL, delves deeper into the subjective evaluation of these dimensions, offering a dynamic perspective on an individual’s health and its impact on their overall quality of life (4,5).
The rationale for conducting this study lies in the critical need to understand the intersectionality of HIV and transgender identity in the Pakistani context, particularly in Lahore. The study aims to provide valuable insights into the specific challenges faced by transgender individuals living with HIV, elucidating the complex interplay between health status, societal factors, and quality of life.
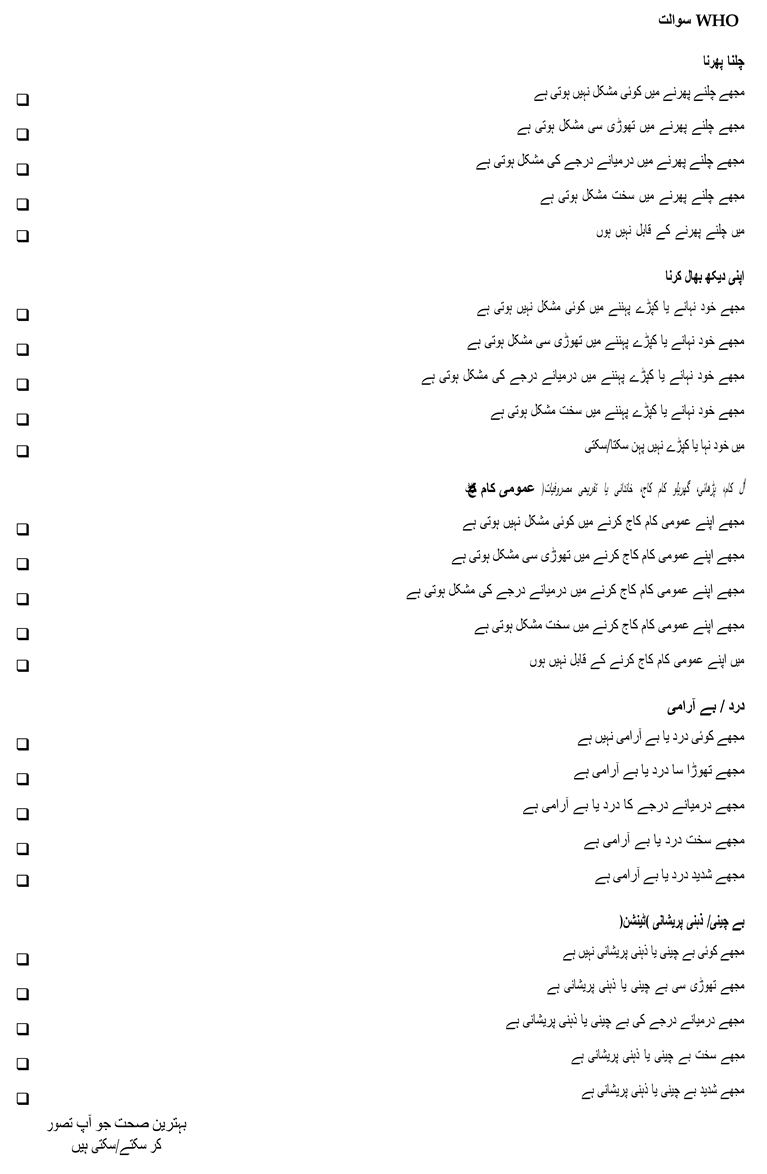
By focusing on Lahore, this research seeks to generate localized data that can in-form targeted interventions, healthcare policies, and community-based initiatives aimed at improving the well-being and quality of life of transgender individuals liv-ing with HIV across Pakistan. The primary objective of this research is to examine the health-related quality of life of transgender individuals living with HIV in Lahore, Pakistan. In addition, we hypothesize that there is a significant correlation between the Visual Analogue Scale (VAS) scores and the EQ-5D questionnaire (Urdu version, modified and approved by research supervisior) results in assessing the HRQoL among transgender individuals living with HIV/AIDS in Lahore.
2. Materials and Methods
Participants
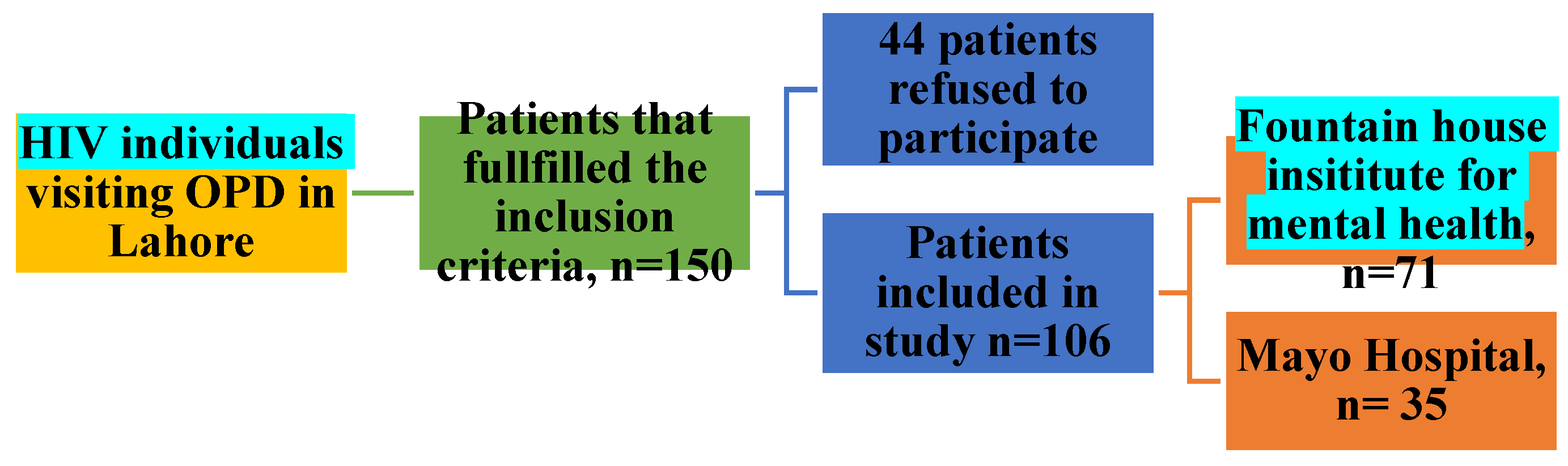
The sample size for the study was determined using the Raosoft Sample Size Calculator. Considering more than 700 registered transgender people living with HIV across the two hospitals in Lahore, a sample size of 150 participants was determined on 16-04-2023. Out of 150 participants, 106 were agreed and 44 were refused to participate in this research. The sample size for the study was determined using the Raosoft Sample Size Calculator. We took a 5% margin of error and a 50% Confidence level in a calculator. Considering more than 700 registered transgender people living with HIV across the two hospitals in Lahore, a sample size of 150 subjects was determined.
The inclusion criteria for the study were transgender individuals living with HIV over 18 years of age who agreed to participate and could understand Urdu, the national language of Pakistan. Participants were excluded if they were male or female, minors, or did not provide informed consent to participate in the study. Unlike other countries where criteria like DSM-5 is used for gender dysphoria, there have not been such studies for classification of transsexuality in Pakistan. Instead PACP provided with the data of transgenders, characterized as per the the Transgender Persons (Protection of Rights) Act of 2018. These transgenders came for the check-up of co-morbidites (common dieases include anxiety, depression, diabetes, high blood pressure, etc.). However, no transgender was enrolled in gender reassignment therapy
Table 1 summarizes the demographic characteristics of the participants, including age, gender identity, education level, monthly income, and household composition.
Procedure
A cross-sectional study design was employed using a validated EQ-5D-5L questionnaire from the World Health Organization (WHO) to assess the health-related quality of life (HRQoL) of HIV-infected transgender individuals. The study was conducted at Mayo Hospital and Fountain house insititute for mental health in Lahore, Pakistan.
Fountain House Institute for Mental Health is a specialized healthcare facility with 100 beds, catering to individuals with psychiatric disorders from underserved communities. Established by Prof. Dr. Rasheed Chaudhry and his team, the institute provides rehabilitation services for individuals with schizophrenia, drug abuse problems, educational programs for children with cerebral impairments, and a dedicated support program for Khwajasira individuals. Fountain house insititute for mental health offers a unique five-day-a-month program providing free medical check-ups and prescription refills for transgender individuals living with HIV.
Mayo Hospital, a 3,000-bed tertiary care hospital, provides comprehensive healthcare services, including diagnosis and treatment for transgender individuals with HIV/AIDS through its outpatient department at government expense.
The research proposal received approval from the Institutional Review Board (IRB) of Lahore Leads University. Subsequently, permission was obtained from the Punjab AIDS Control Program (PACP) to conduct the study in the selected hospitals.
The outpatient departments of Fountain house insititute for mental health and Mayo Hospital were used to recruit volunteers. Prior to data collection, participants were briefed about the study objectives, and informed consent was obtained orally from each participant. The survey was conducted face-to-face to ensure participants understood the questions. Confidentiality and anonymity were assured to all participants.
Qinstruments
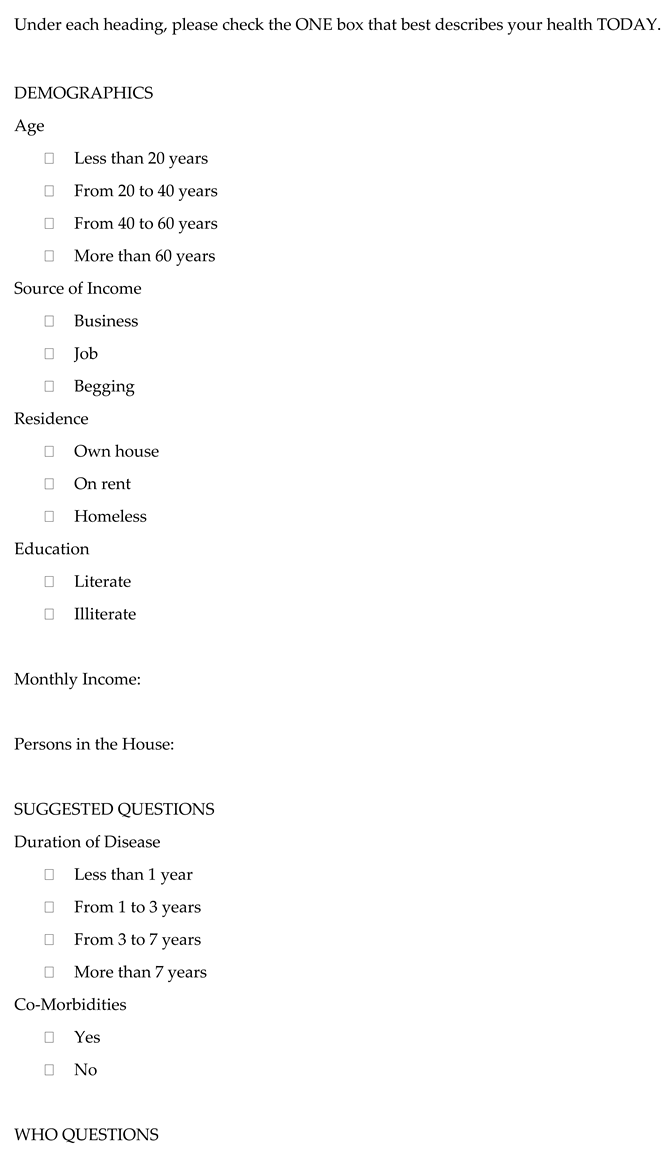
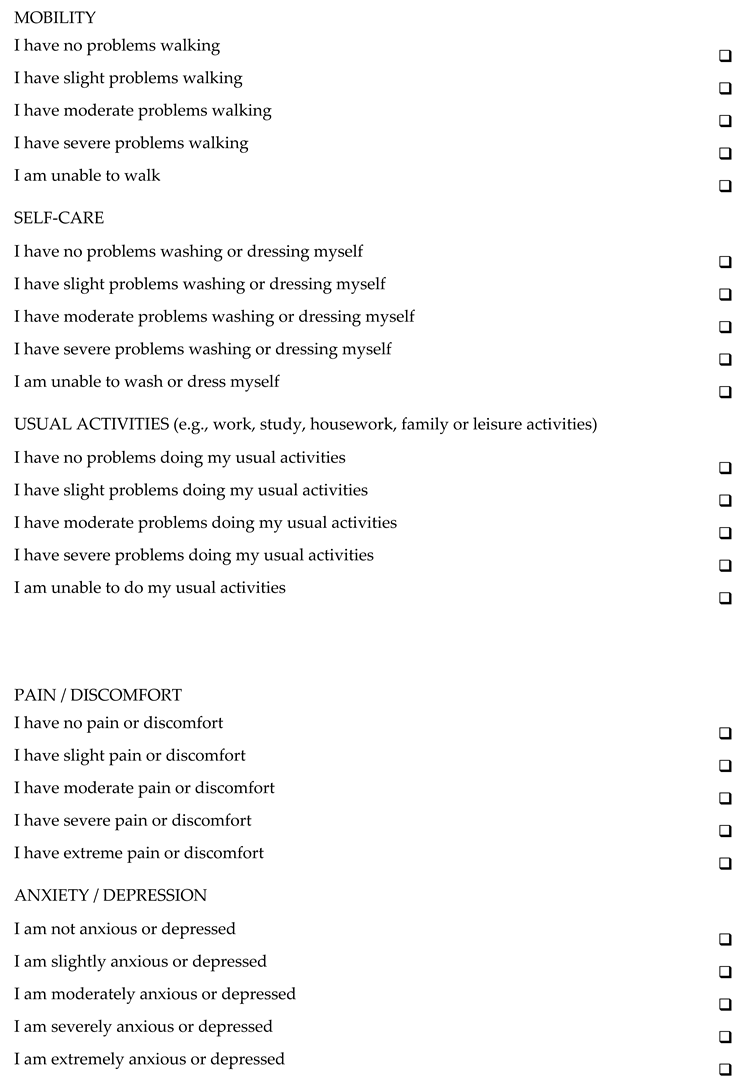
The HRQoL of transgender individuals infected with HIV/AIDS was assessed using the EQ-5D-5L questionnaire, a validated tool that provides a single index value and descriptive profile for health conditions. The questionnaire comprises two parts:
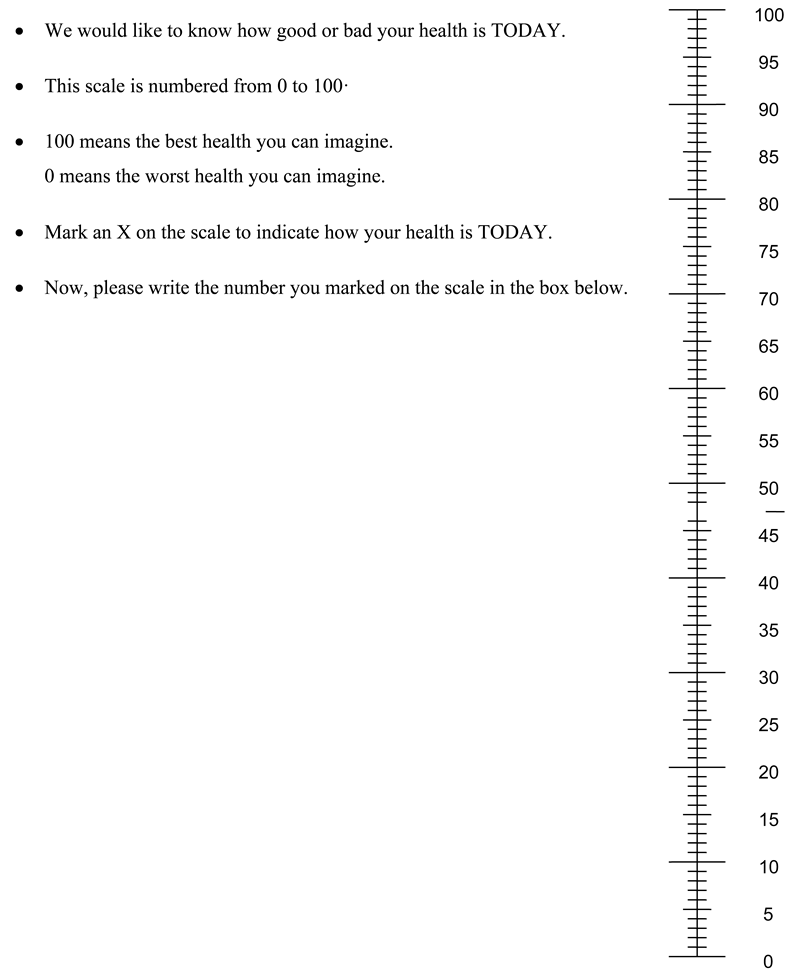
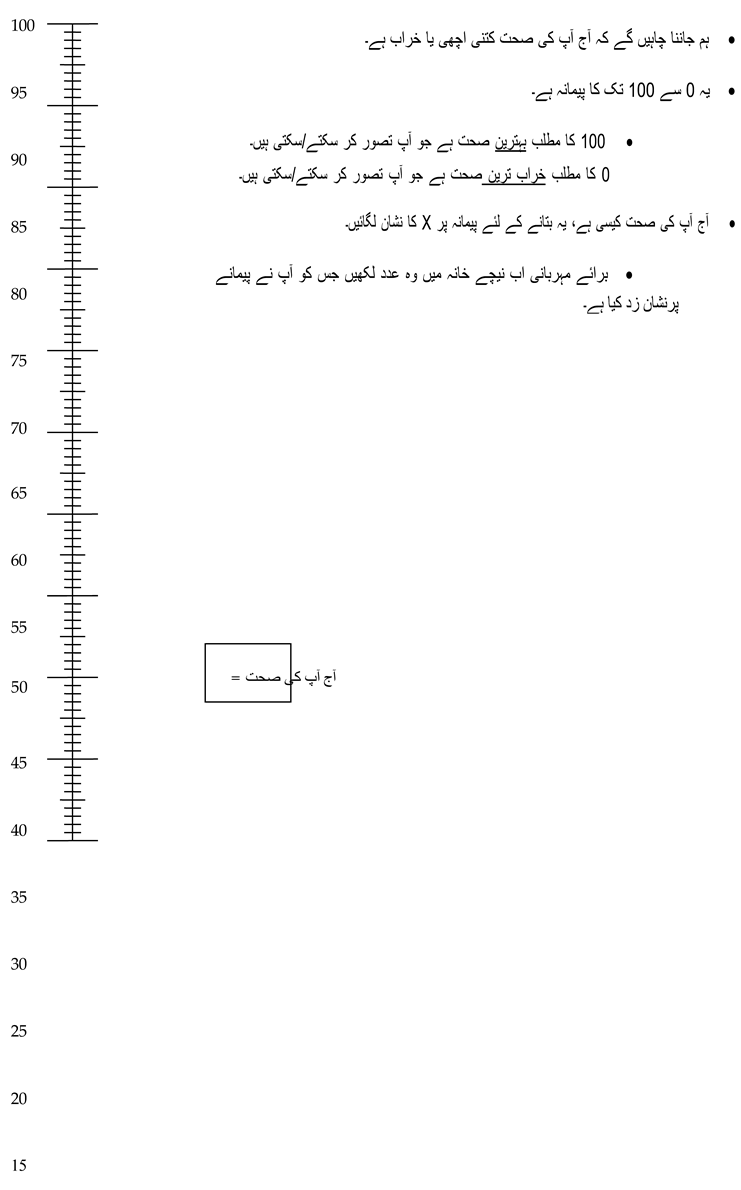
Visual Anatomical Scale (VAS): Participants self-rated their health state on a scale from 0 to 100, with 100 indicating the best health state and 0 representing the worst.
Five Dimensions of Health: The second part of the questionnaire evaluates usual activities, mobility, self-care, pain/discomfort, and depression/anxiety, with each dimension having five different outcomes. These outcomes describe five intensity levels for each question (21).
Additional demographic variables, including age, source of income, residence, education, monthly income, and household composition, were collected to understand potential factors influencing the data.
Data Analysis
Data analysis was performed using appropriate statistical methods. Descriptive statistics were used to summarize demographic characteristics and EQ-5D-5L scores. The relationship between demographic variables and HRQoL scores was explored using inferential statistics. Data analysis was done using statistical tools like SPSS (Statistical Package for Social Sciences). The analysis process was documented to facilitate replication of the study.
3. Results
3.1. Study Population
One hundred and six transgender participants living with HIV were enrolled in the research. All these participants filled out the questionnaire completely. They also marked the visual anatomical scale (VAS) by giving points to their current health status.
Figure 1.
Sample Size of Study.
3.1.1. Demographic Characteristics of Study Respondents
The demographic characteristics of study respondents are listed in Table 1.
3.1.2. Clinical Characteristics of Surveyed Individuals
The clinical characteristics of participants are mentioned in Table 2.
3.1.3. Health-Related Quality of Life of Surveyed Individuals
Health-related quality of life of surveyed individuals is mentioned in Table 3.
3.1.4. EQ-5D Scores by Demographics Characteristics
The mean scores of EQ-5D demographics characteristics are shown in Table 4.
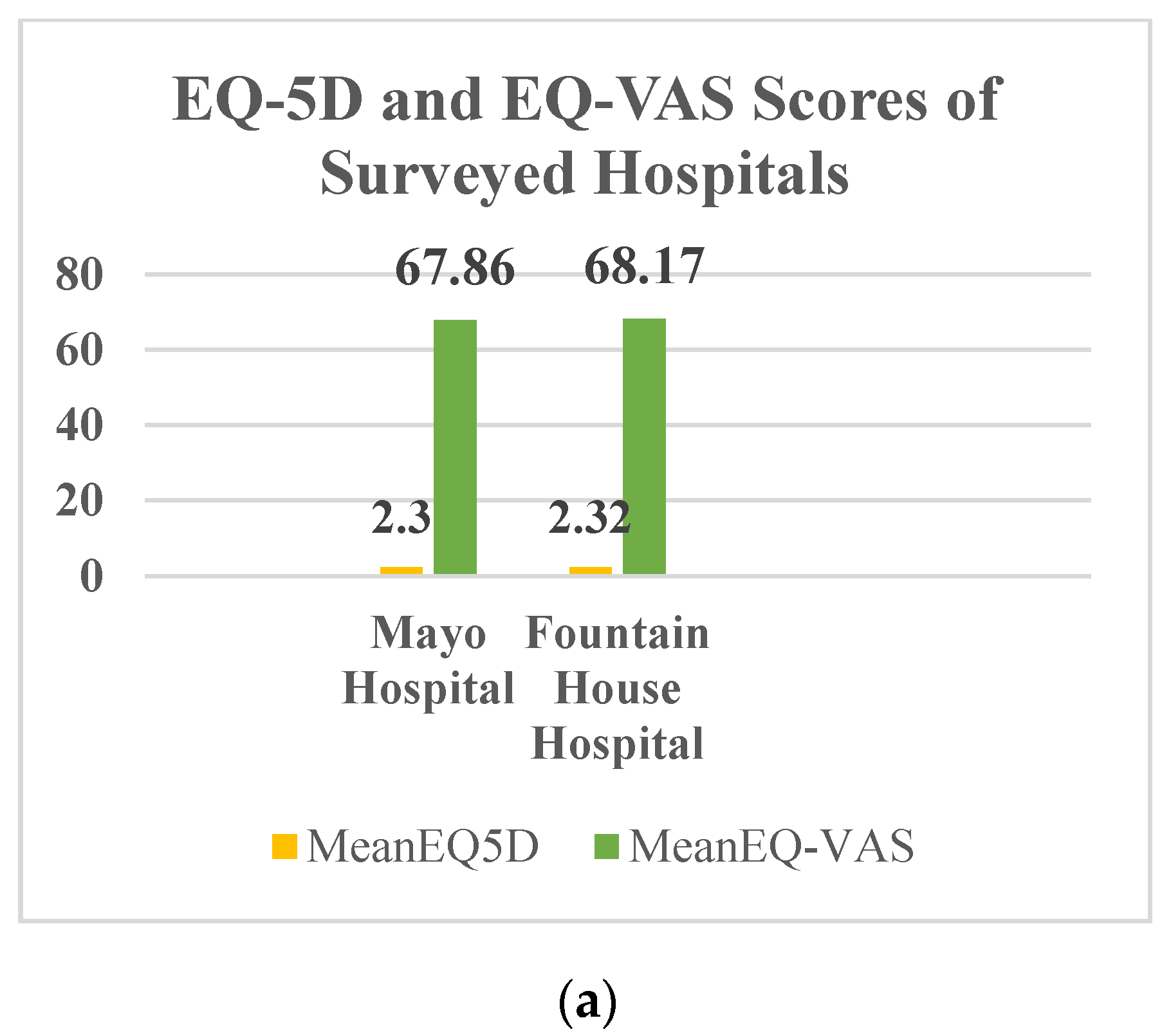
Figure 2.
(a) EQ-5D and EQ-VAS Scores of Surveyed Hospitals.
3.1.5. EQ-5D Scores by Clinical Characteristics
The mean scores of EQ-5D and EQ-VAS by clinical factors are shown in Table 5.
3.1.6. EQ-5D Scores of WHO Questions
The mean EQ-5D scores WHO question is given in Table 6.
3.1.7. Correlation between EQ-5D and EQ-VAS by Demographic Characteristics
The mean score of EQ-5D and EQ-VAS of the surveyed individuals by demographic characteristics is shown in Table 4.7.

Table 7.
Correlation between EQ-5D and EQ-VAS by Demographic Characteristics.
| Demographics | Mean EQ-5D Score | P-value | Mean EQ-VAS Score | P-value | |
|
Hospital |
Fountain house insititute for mental health | 2·32 | 0·895 | 68·17 | 0·930 |
| Mayo Hospital | 2·30 | 67·86 | |||
|
Age |
From 20 to 40 years | 2·13 | 0·932 | 67·81 | 0·714 |
| From 40 to 60 years | 2·36 | 68·19 | |||
| Above 60 years | 2·31 | 67·78 | |||
|
Residence |
Own House | 2·25 | 0·325 | 50 | 0·338 |
| On Rent | 2·24 | 76·76 | |||
| Homeless | 2·49 | 64·15 | |||
| Education | Literate | 2·18 | 0·250 | 71·75 | 0·008 |
| Illiterate | 2·37 | 67·41 | |||
3.1.8. Correlation between EQ-5D and EQ-VAS by Clinical Characteristics
Table 8 shows the link between the research respondents’ EQ-5D and EQ-VAS scores and clinical features.
3.1.8. Correlation between EQ-5D and EQ-VAS by WHO Questionnaire
Table 9 depicts the link between research participants’ EQ-5D and EQ-VAS scores.
4. Discussion
Despite extensive work on HIV/AIDS, transgender people remain one of the most neglected groups in Pakistan. With a population exceeding 300,000, and likely higher, transgender individuals face significant social stigma and discrimination. This marginalized status exacerbates their vulnerability to severe health issues, including HIV/AIDS. Transgender individuals are at a higher risk of contracting HIV/AIDS compared to the general population.
Our study, a community-based cross-sectional research, targeted 106 transgender patients from Fountain Hospital and Mayo Hospital in Lahore. Using the WHO-approved EQ-5D questionnaire (Urdu version), we aimed to assess the impact of HIV/AIDS on the health-related quality of life (HRQoL) of transgender individuals. The EQ-5D and EQ-VAS scores were calculated to determine their correlation. HRQoL is a multifaceted concept encompassing various aspects of well-being and functioning, including physical, social, psychological, and role-related dimensions. This study is pioneering in specifically targeting the HRQoL of transgender people living with HIV/AIDS in Lahore, Punjab.
Pakistan, an underdeveloped country with over 240 million people and a literacy rate of around 62%, lacks basic education on AIDS and transgender issues. This ignorance, coupled with societal disdain, further marginalizes transgender individuals. Our study aims to promote awareness about HRQoL among transgender people, emphasizing the need for improved educational resources.
Comparing our findings with previous studies, such as Aneela Hussain et al.‘s research on transgender QoL in Karachi, we observed similar trends. Their study indicated a decline in well-being and quality of life among transgender individuals, which aligns with our findings that transgender people suffer from moderately worse health. Both studies highlight that education and family support are crucial for improving the lives of transgender individuals with HIV/AIDS.
Detailed analysis of our study revealed that most transgender individuals affected by HIV/AIDS were between the ages of 40 and 60 (67.9%), with a significant majority being uneducated (72.6%). The lack of education is a significant factor in the prevalence of HIV/AIDS. Studies suggest that adequate training for healthcare workers and students can enhance disease awareness, ultimately improving the overall HRQoL of transgender individuals.
The clinical characteristics of the disease showed that most patients had been living with HIV/AIDS for one to three years (38.7%), followed by three to seven years (28.3%). This duration aligns with the typical disease progression window of five to ten years, indicating effective disease management despite limited education, thanks to the efforts of healthcare workers.
The mean EQ-5D score was 2.32 ± 0.85, indicating a moderate decline in HRQoL. Similarly, the mean EQ-VAS score was 68.07 ± 18.42, suggesting moderate improvement in HRQoL. The discrepancy between the EQ-5D and EQ-VAS scores may be attributed to differences in patient perception when rating specific health factors versus overall health.
Demographic analysis showed correlations between EQ-5D and EQ-VAS scores with variables such as hospital (p = 0.895, 0.930), age (p = 0.932, 0.714), residence (p = 0.325, 0.338), and education (p = 0.250, 0.008). Clinical characteristics also showed correlations, with disease duration (p = 0.216, 0.033) and comorbidities (p = 0.045, 0.011) being significant factors.
A notable finding was the lack of significant correlation between EQ-5D and EQ-VAS scores in WHO-based questions. Analysis of individual dimensions such as mobility (p = 0.056, 0.000), self-care (p = 0.560, 0.000), usual activities (p = 0.338, 0.000), pain/discomfort (p = 0.872, 0.000), and anxiety/depression (p = 0.085, 0.000) highlighted these discrepancies.
Interestingly, the moderate HRQoL observed in our study is partly due to the absence of comorbidities in most subjects—61.3% had only HIV/AIDS. Transgender individuals without comorbidities reported a relatively better quality of life. However, overall HRQoL remains poor, as evidenced by the moderate mean EQ-5D index and EQ-VAS score. This is primarily due to moderate impairments in mobility and anxiety/depression, compared to other domains like routine activities and self-care.
In nutshell, our study underscores the urgent need for targeted interventions to improve the education and healthcare support for transgender individuals in Pakistan. Addressing these gaps can significantly enhance the HRQoL of this vulnerable population, particularly those living with HIV/AIDS.
5. Conclusions
This study aims to examine the HRQoL of transgender people living with HIV/AIDS in Lahore, Pakistan. Transgender individuals, particularly those with HIV/AIDS, face unique challenges that can significantly impact their HRQoL.
The outcomes shows that the presence of HIV/AIDS has a mild effect on the HRQoL of transgender people. The mobility scores of transgender individuals in this study indicate a moderate level of disability, reflecting limitations in physical movement. Therefore, interventions targeting physical rehabilitation, assistive devices, and accessible infrastructure are crucial to enhance mobility and promote inclusivity.
Another significant finding is the difficulties faced by transgender individuals in carrying out their usual activities. These challenges may stem from social stigma, discrimination, and limited resource access.
The study also highlights the substantial emotional distress experienced by transgender individuals living with HIV/AIDS. The mean scores for anxiety and depression indicate significant levels of psychological burden within this population.
The results of research shed light on the HRQoL of transgender individuals living with HIV/AIDS in Lahore, Pakistan. It underscore the importance of implementing targeted interventions, educational programs, and community-based services to enhance HRQoL and address the challenges faced by this marginalized population. By adopting a multidisciplinary and inclusive approach to care, healthcare providers and policymakers can contribute to the overall well-being and improved HRQoL of transgender individuals with HIV/AIDS.
6. Limitations
This report had some limitations that should be considered. First, it was a cross-sectional study that did not include healthy individuals as a control group. Also, there is no exposure to transgenders under 18 years old, so they are excluded.
This limited the generalization of the findings. Second, it faced ethical and practical challenges in data collection, such as obtaining informed consent from the participants, respecting their privacy and confidentiality, and dealing with their refusal or reluctance to answer some questions. Third, the study only recruited transgender individuals from two hospitals in one area of Lahore, which may not be representative of the entire population of Pakistan.
Therefore, future studies should try to prevent this error by selecting more transgenders from different places and different kinds of healthcare institutions in Pakistan. Fourth, the acceptance of the EQ-5D-5L WHO questionnaire was delayed by PACP. They recommended adding some questions to it. Then they approved the questionnaire form.
Moreover, this study used a method to convert the scores of the five aspects of HRQoL (self-care, mobility, usual activities, discomfort/pain, depression/anxiety) into a single number that represents the overall health condition of a person. The method relied on a set of values called the UK time-trade-off value-set. These values represent how much people in the UK are willing to give up some of their remaining years of life in exchange for better health.
This value set may not be appropriate for the Pakistani community because transgender from different countries may have different opinions and values about their health and quality of life.
Funding
No fundings.
Conflicts of Interest
There is no conflict of interest in this research.
Appendix A


References
- Nigusso FT, Mavhandu-Mudzusi AH. Health-related quality of life of people living with HIV/AIDS: the role of social inequalities and disease-related factors. Health Qual Life Outcomes. 2021;19(1):63. [CrossRef]
- WHO. WHOQoL: Measuring Quality of Life [Available from: https://www.who.int/tools/whoQoL#:~:text=WHO%20defines%20Quality%20of%20Life%20as%20an%20individual%27s,relation%20to%20their%20goals%2C%20expectations%2C%20standards%20and%20concerns.
- Karimi M, Brazier J. Health, Health-Related Quality of Life, and Quality of Life: What is the Difference? Pharmacoeconomics. 2016;34(7):645-9.
- Karimi M, Brazier J. Health, Health-Related Quality of Life, and Quality of Life: What is the Difference? PharmacoEconomics. 2016;34.
- de Wit M, Hajos T. Health-Related Quality of Life. In: Gellman MD, Turner JR, editors. Encyclopedia of Behavioral Medicine. New York, NY: Springer New York; 2013· p. 929-31.
- Center JHA. What is Health Related Quality of Life [Available from: https://www.hopkinsarthritis.org/arthritis-research/patient-centered-outcomes-research/what-is-health-related-quality-of-life/.
- Transgender: Evidence on the biological nature of gender identity 2015 [Available from: https://www.sciencedaily.com/releases/2015/02/150213112317·htm.
- Ministry of Human Rights P. The Transgender Persons (Protection of Rights) Act 2018 2018 [Available from: https://mohr.gov.pk/SiteImage/Misc/files/1614147088_465·pdf.
- Saddique K, Gang C, Mirbehar S, Batool H, Ahmad I. Transgender Issues in Pakistani Community. European Academic Research. 2017;IV:9048-57.
- Herbst JH, Jacobs ED, Finlayson TJ, McKleroy VS, Neumann MS, Crepaz N. Estimating HIV prevalence and risk behaviors of transgender persons in the United States: a systematic review. AIDS Behav. 2008;12(1):1-17.
- Greene WC. A history of AIDS: Looking back to see ahead. European Journal of Immunology. 2007;37(S1):S94-S102.
- WHO. Summary of the global HIV epidemic, 2021 2021 [Available from: https://www.who.int/data/gho/data/themes/hiv-AIDS.
- Trans women 66 times more likely to have HIV, with trans men nearly 7 times more likely, global analysis finds 2022 [Available from: https://www.AIDSmap.com/news/mar-2022/trans-women-66-times-more-likely-have-hiv-trans-men-nearly-7-times-more-likely-global.
- Ahmadi L, Nocerino A, Puneky D. HIV Infection in Transgender Persons. Transgender Medicine: A Multidisciplinary Approach. 2019:239-81.
- KHAN A. An update on HIV in transgenders of Pakistan. Asian Pacific Journal of Tropical Medicine. 2019:21-.
- A K, Chaudhary S, Rb S, H V, Sisodia S, A G. A REVIEW ON: HIV AIDS. Indian Journal of Pharmaceutical and Biological Research. 2016;4.
- Weichseldorfer M, Reitz M, Latinovic OS. Past HIV-1 medications and the current status of combined antiretroviral therapy options for HIV-1 individuals. Pharmaceutics. 2021;13(11):1798.
- Bhatti AB, Usman M, Kandi V. Current scenario of HIV/AIDS, treatment options, and major challenges with compliance to antiretroviral therapy. Cureus. 2016;8(3). [CrossRef]
- Maartens G, Celum C, Lewin SR. HIV infection: epidemiology, pathogenesis, treatment, and prevention. The Lancet. 2014;384(9939):258-71. [CrossRef]
- AIDS.gov.hk. STAGING, CLASSIFICATION AND MONITORING OF HIV/AIDS [Available from: https://www.AIDS.gov.hk/pdf/g190htm/04·htm.
- Tran BX, Ohinmaa A, Nguyen LT. Quality of life profile and psychometric properties of the EQ-5D-5L in HIV/AIDS individuals. Health and quality of life outcomes. 2012;10(1):1-8.
- Galt KA. Media Review: SPSS Text Analysis for Surveys 2·1· Chicago, IL: SPSS Inc. http://www. spss. com/textanalysis_surveys. Journal of Mixed Methods Research. 2008;2(3):284-6.
- Welle D. Pakistan: Coronavirus makes life harder for transgenders 2020 [Available from: https://www.dw.com/en/pakistan-transgender-coronavirus/a-54817362.
- White Hughto JM, Reisner SL, Pachankis JE. Transgender stigma and health: A critical review of stigma determinants, mechanisms, and interventions. Soc Sci Med. 2015;147:222-31. [CrossRef]
- Neumann MS, Finlayson TJ, Pitts NL, Keatley J. Comprehensive HIV Prevention for Transgender Persons. Am J Public Health. 2017;107(2):207-12. [CrossRef]
- Review WP. Pakistan Population 2023 2023 [Available from: https://worldpopulationreview.com/countries/pakistan-population.
- Ministry of Federal Education & Professional Training P. ADULT LITERACY [Available from: http://mofept.gov.pk/ProjectDetail/NjQ4ZTg2NjItOWM2NC00Y2IxLTkzMDgtMjU2OTFhMjA4NzNh.
Table 1.
Demographics of Surveyed Individuals.
| Characteristics | Frequency | Percentage | Mean (SD) | |
|---|---|---|---|---|
|
Hospital |
Fountain House Mayo Hospital |
67% 33% |
71 35 |
1.33 (±0.473) |
| Age | Less than 20 years From 20 to 40 years From 40 to 60 years More than 60 years |
0% 15·1% 67·9% 17% |
0 16 72 18 |
3.08(±0.619) |
| Source of Income | Business Job Begging |
0·9% 32·1% 67% |
1 34 71 |
2.78(±0.437) |
| Residence | Own house On rent Homeless |
18·9% 50·9% 30·2% |
20 54 32 |
2.10 (±0.689) |
| Education | Literate Illiterate |
27·4% 72·6% |
29 77 |
1.83 (±0.377) |
| Persons in House | 1 2 3 4 5 6 7 8 9 10 15 |
17·9% 23·6% 18·9% 14·2% 5·7% 6·6% 4·7% 3·8% 2·8% 0·9% 0·9% |
19 25 20 15 6 7 5 4 3 1 1 |
3.4 (±2.540) |
Table 2.
Clinical Characteristics of Surveyed Individuals.
| Characteristics | Frequency | Percentage | |
|---|---|---|---|
| Duration of disease | Less than 1 year From 1 to 3 years From 3 to 7 years More than 7 years |
20 41 30 15 |
18·9% 38·7% 28·3% 14·2% |
| Co-Morbidities | Yes No |
40 65 |
37·7% 61·3% |
Table 3.
Health-related Quality of Life of Surveyed Individuals.
| Characteristics |
Frequency | Percentage | |
|---|---|---|---|
|
Mobility |
I have no problems walking | 34 | 32·1% |
| I have slight problems walking | 24 | 22·6% | |
| I have moderate problems walking | 22 | 20·8% | |
| I have severe problems walking | 23 | 21·7% | |
| I am unable to walk | 3 | 2·8% | |
|
Self- care |
I have no problems washing or dressing | 46 | 43·4% |
| I have slight problems washing or dressing | 22 | 20·8% | |
| I have moderate problems washing or dressing | 25 | 23·6% | |
| I have severe problems washing or dressing | 9 | 8·5% | |
| I am unable to wash or dress myself | 4 | 3·8% | |
|
Usual- activities |
I have no problems doing my usual activities | 48 | 45·3% |
| I have slight problems doing my usual activities | 20 | 18·9% | |
| I have moderate problems doing my usual activities | 22 | 20·8% | |
| I have severe problems doing my usual activities | 13 | 12·3% | |
| I am unable to do my usual activities | 3 | 2·8% | |
|
Pain/ Discomfort |
I have no pain or discomfort | 39 | 36·8% |
| I have slight pain or discomfort | 19 | 17·9% | |
| I have moderate pain or discomfort | 20 | 18·9% | |
| I have severe pain or discomfort | 23 | 21·7% | |
| I have extreme pain or discomfort | 5 | 4·7% | |
|
Anxiety/Depression |
I am no anxious or depressed | 34 | 32·1% |
| I am slightly anxious or depressed | 15 | 14·2% | |
| I am moderate anxious or depressed | 25 | 23·6% | |
| I am severe anxious or depressed | 19 | 17·9% | |
| I am extremely anxious or depressed | 13 | 12·3% | |
Table 4.
EQ-5D Scores by Demographics Characteristics.
| Characteristics | Frequency | Mean EQ-5D Score | Mean VAS-Score | |
|---|---|---|---|---|
| Hospital | Fountain House Mayo Hospital |
71 35 |
2·32(0·85) | 68·17 (18·67) |
| 2·30 (0·86) | 67·86 (18·32) | |||
| Age | From 20 to 40 years | 16 | 2·13 (0·91) | 67·81 (18·79) |
| From 40 to 60 years | 72 | 2·36 (0·78) | 68·19 (19·34) | |
| More than 60 years | 18 | 2·31 (1·04) | 67·78 (15·26) | |
| Source Of Income | Business | 1 | 2·00 (0·0) | 50 (0·0) |
| Job | 34 | 2·14 (0·86) | 76·76 (14·81) | |
| Begging | 71 | 2·41 (0·84) | 64·15 (18·74) | |
| Residence | Own house | 20 | 2·25 (0·92) | 71·75 (20·21) |
| On rent | 54 | 2·24 (0·89) | 67·41 (18·03) | |
| Homeless | 32 | 2·49 (0·72) | 66·87 (18·39) | |
| Education | Literate | 29 | 2·18 (0·87) | 74·14 (19·91) |
| Illiterate | 77 | 2·37 (0·84) | 65·78 (17·49) | |
| Persons in House | 1 | 19 | 2·53 (1·06) | 59·74 (17·98) |
| 2 | 25 | 2·43 (0·70) | 67·60 (18·49) | |
| 3 | 20 | 2·55 (0·86) | 65·75 (20·27) | |
| 4 | 15 | 2·58 (0·43) | 72·67 (15·33) | |
| 5 | 6 | 1·93 (0·81) | 78·33 (11·69) | |
| 6 | 7 | 1·71 (0·78) | 80·71 (13·04) | |
| 7 | 5 | 1·72 (0·86) | 64·00 (8·944) | |
| 8 | 4 | 1·10 (0·20) | 67·50 (22·17) | |
| 9 | 3 | 1·80 (0·72) | 81·67 (18·93) | |
| 10 | 1 | 3·20 (0·0) | 90·00 (0·0) | |
| 15 | 1 | 2·20 (0·0) | 25·00 (0·0) | |
Table 5.
EQ-5D Scores by Clinical Characteristics.
| Characteristics | Frequency | Mean EQ-5D Score | Mean VAS-Score | |
| Duration of disease | Less than 1 year |
20 | 1·91 (0·91) | 75·75 (14·07) |
| From 1 to 3 years |
41 | 2·24 (0·84) | 66·83 (20·54) | |
| From 3 to 7 years |
30 | 2·60 (0·78) | 64·00 (18·30) | |
| More than 7 Years |
15 | 2·50 (0·70) | 69·33 (16·24) | |
| Co-Morbidities | Yes | 40 | 2·53 (0·89) | 61·75 (20·39) |
| No | 65 | 2·20 (0·80) | 71·92 (16·31) | |
Table 6.
EQ-5D Scores of WHO Questions.
| Characteristics | Frequency | Mean EQ-5D Score | Mean VAS-Score | |
|
Mobility |
I have no problems walking | 34 | 1·51 (0·57) | 74·85 (15·64) |
| I have slight problems walking | 24 | 2·25 (0·50) | 68·33 (16·12) | |
| I have moderate problems walking | 22 | 2·63 (0·47) | 67·27 (18·24) | |
| I have severe problems walking | 23 | 3·13 (0·65) | 59·78 (22·18) | |
| I am unable to walk | 3 | 3·53 (0·61) | 58·33 (16·07) | |
|
Self- care |
I have no problems washing or dressing | 46 | 1·73 (0·71) | 69·57 (15·84) |
| I have slight problems washing or dressing | 22 | 2·51 (0·45) | 65·91 (18·62) | |
| I have moderate problems washing or dressing | 25 | 2·76 (0·62) | 70·40 (21·51) | |
| I have severe problems washing or dressing | 9 | 3·35 (0·80) | 64·44 (20·22) | |
| I am unable to wash or dress myself | 4 | 2·90 (0·84) | 56·25 (24·28) | |
|
Usual- activities |
I have no problems doing my usual activities | 48 | 1·68 (0·59) | 70·00 (17·32) |
| I have slight problems doing my usual activities | 20 | 2·54 (0·50) | 69·00 (20·43) | |
| I have moderate problems doing my usual activities | 22 | 2·74 (00·43) | 69·55 (16·10) | |
| I have severe problems doing my usual activities | 13 | 3·24 (0·78) | 60·77 (21·39) | |
| I am unable to do my usual activities | 3 | 0·93 (0·11) | 51·67 (23·62) | |
|
Pain/discomfort |
I have no pain or discomfort | 39 | 1·72 (0·73) | 70·13 (18·51) |
| I have slight pain or discomfort | 19 | 2·15 (0·53) | 68·16 (15·11) | |
| I have moderate pain or discomfort | 20 | 2·76 (0·63) | 63·50 (22·13) | |
| I have severe pain or discomfort | 23 | 2·90 (0·62) | 69·13 (17·36) | |
| I have extreme pain or discomfort | 5 | 3·16 (1·07) | 65·00 (22·91) | |
| Anxiety/ depression |
I am no anxious or depressed | 34 | 1·53 (0·61) | 75·00 (15·66) |
| I am slightly anxious or depressed | 15 | 2·14 (0·52) | 62·00 (16·56) | |
| I am moderate anxious or depressed | 25 | 2·64 (0·62) | 66·40 (20·49) | |
| I am severe anxious or depressed | 19 | 3·07 (0·69) | 65·53 (21·20) | |
| I am extremely anxious or depressed | 13 | 2·87 (0·47) | 63·85 (16·09) |
|
| Mean EQ-5D Index score* | 2·32 ± 0·85 | |||
| Mean EQ-5D VAS score** | 68.07 ± 18·42 | |||
*0-1= no decline in health,1-2 = decline in health, 2-3 = moderate decline in health, 3-4= severe decline in health, 4-5 = extreme decline in health. **0-20 = no decline in health, 20-40 = decline in health, 40-60 = moderate decline in health, 60-80 = severe decline in health, 80-100 = extreme decline in health.
Table 8.
Correlation between E-5D and EQ-VAS by Clinical Characteristics.
| Clinical Characteristics | Mean EQ-5D Score | p-value | Mean EQ-VAS Score | p-value | |
| Duration of disease | Less than 1 year | 1·91 | 0·216 | 75·75 | 0·033 |
| From 1 to 3 years | 2·24 | 66·83 | |||
| From 3 to 7 years | 2·60 | 64·00 | |||
| More than 7 years | 2·50 | 69·33 | |||
| Comorbidities | Yes | 2·53 | 0·045 | 61·75 | 0·011 |
| No | 2·20 | 71·92 | |||
Table 9.
Correlation between EQ-5D and EQ-VAS by WHO Questionnaire.
| EQ-5D | Mean EQ-5D | p-value | Mean EQ-VAS Score | p-value | |
| Mobility | I have no problems walking | 1·51 | 0·056 |
74·85 | 0·000 |
| I have slight problems walking | 2·25 | 68·33 | |||
| I have moderate problems walking | 2·63 | 67·27 | |||
| I have severe problems walking | 3·13 | 59·78 | |||
| I am unable to walk | 3·53 | 58·33 | |||
| Self-care | I have no problems washing or dressing myself | 1·73 | 0·560 | 69·57 | 0·000 |
| I have slight problems washing or dressing myself | 2·51 | 65·91 | |||
| I have moderate problems washing or dressing myself | 2·76 | 70·40 | |||
| I have severe problems washing or dressing myself | 3·35 | 64·44 | |||
| I am unable to wash or dress myself | 2·90 | 56·25 | |||
| Usual activities | I have no problems doing my usual activities | 1·68 | 0·338 | 70·00 | 0·000 |
| I have slight problems doing my usual activities | 2·54 | 69·00 | |||
| I have moderate problems doing my usual activities | 2·74 | 69·55 | |||
| I have severe problems doing my usual activities | 3·24 | 60·77 | |||
| I am unable to do my usual activities | 0·93 | 51·67 | |||
| Pain/ Discomfort |
I have no pain or discomfort | 1·72 | 0·872 | 70·13 | 0·000 |
| I have slight pain or discomfort | 2·13 | 68·16 | |||
| I have moderate pain or discomfort | 2·76 | 63·50 | |||
| I have severe pain or discomfort | 2·90 | 69·13 | |||
| I have extreme pain or discomfort | 3·16 | 65·00 | |||
| Anxiety/ depression |
I am no anxious or depressed | 1·53 | 0·085 | 75·00 | 0·000 |
| I am slightly anxious or depressed | 2·14 | 62·00 | |||
| I am moderate anxious or depressed | 2·64 | 66·40 | |||
| I am severe anxious or depressed | 3·07 | 65·53 | |||
| I am extremely anxious or depressed | 2·87 | 63·85 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



