
Submitted:
12 June 2024
Posted:
13 June 2024
You are already at the latest version
Abstract
Additionally, the characteristics of inhaled corticosteroids (inhaled particle sizes) may influence the risk of sleep apnea. In children, the severity of asthma plays a crucial role in influencing the prevalence of sleep apnea, while using inhaled corticosteroids seems to be a less relevant risk factor compared to adults. The overall risk of bias was categorized as high or with some concerns in 100% of the studies analyzed. Each study identified at least one form of bias that raised significant concerns. Studies showed a complex relationship between inhaled corticosteroids use, asthma severity, and the onset of sleep apnea. Further studies are needed.
Keywords:
asthma
; fluticasone propionate
; inhaled corticosteroid
; obstructive sleep apnea
; sleep-disordered breathing
1. Introduction
Sleep-disordered breathing (SDB) can lead to significant health issues in both children and adults [1,2,3]. SDB is linked to a variety of detrimental effects, including intermittent hypoxia, oxidative stress, sleep fragmentation, high blood pressure, and heart disease [4,5,6,7].
Children
In children, the incidence of SDB has been on the rise. Parent-reported habitual snoring varies from 1.5% to 6%, while sleep apnea episodes range from 0.2% to 4%. Depending on the combination of symptoms reported by parents on questionnaires, the prevalence of SDB ranges from 4% to 11%. The minimum prevalence rate for pediatric obstructive sleep apnea syndrome (OSAS) is around 1% [8]. Diagnosed OSA, based on various diagnostic study criteria, ranges from 1% to 4% [9].
Adults
The 5-year incidence rate in adults is roughly 7.5% for moderate to severe SDB and 16% (or less) for mild to moderate SDB combined [10]. The prevalence of OSA associated with daytime sleepiness is about 3-7% for adult males and 2-5% for adult females in the general population [9]. SDB affects approximately 17% of men and 9% of women aged 50 to 70 [11].
Treatment
Regarding treatment, medical therapy with intranasal corticosteroids (ICS) is more effective in reducing OSA than a placebo [12]. ICS manage OSA symptoms by reducing inflammation and nasal congestion [13]. In children with mild OSA, ICS such as budesonide and fluticasone have been shown to improve symptoms and reduce adenoid size, but they do not entirely resolve OSA. However, the effectiveness of ICS in managing OSA symptoms is a matter of debate [14].
Recent evidence has been insufficient to support the efficacy of ICS for OSA treatment in children [15]. In a recent randomized, double-blind, placebo-controlled study, it was reported that in children aged 5-12 years with OSAS, ICS treatment did not result in significant changes in polysomnography (PSG) outcomes, neurobehavioral symptoms, or OSA symptoms after 3 and 12 months of treatment [16].
Adenotonsillectomy (A&T), where applicable, remains the first-line treatment for adenotonsillar hypertrophy (ATH), and it is associated with significant improvements in SDB in most children, being effective in 70% to 100% of patients [17].
Asthma
Asthma is a chronic inflammatory condition of the airways in the lungs characterized by recurrent episodes of wheezing, coughing, chest tightness, and shortness of breath [20].
The overlapping symptoms of OSA and asthma can complicate the diagnosis of either condition. The nocturnal respiratory symptoms of OSA and asthma are often interrelated, necessitating in-hospital PSG for accurate diagnosis, particularly in pediatric cases [21].
Prevalence
A study has revealed significant disparities in asthma prevalence. Over a two-decade period, the overall prevalence of asthma has fluctuated. It increased from 2003 (8.5%) to 2009 (9.6%) and then decreased in 2019 (7.0%) [22]. Asthma prevalence peaked at 17.8% among children aged 5-9 years and then declined to 6.9% among those aged 45-49 years, only to gradually increase to 8.1% among those aged 65-69 years [23]
SDB in Asthmatic Patients
Children
Adults
In adults, research has consistently demonstrated that the incidence of OSA is significantly greater in individuals with asthma compared to those without, with rates varying from 38% to 70%. Asthmatic patients with OSA are 3.6 times more likely to experience uncontrolled asthma [26]. A meta-analysis revealed that the prevalence of OSA in adult patients with asthma was 49.5% and that the likelihood of having OSA was 2.6 times higher in patients with asthma compared to healthy controls [27].
Treatment
Aims of the Study
Given the prevalence of OSA in patients with asthma, this review aims to explore the existing literature to determine whether ICSs play a role in SDB/OSA in patients with asthma.
2. Materials and Methods
We systematically searched the Medline PubMed, Scopus, and Web of Science databases for articles published in English from inception until May 12, 2024. We adjusted Medical Subject Heading (MeSH) terms to search each database, including their combinations and truncated synonyms.
PUBMED: (Inhaled Corticosteroids [Title/Abstract] OR Inhaled Glucocorticoids [Title/Abstract] OR Inhaled Steroids [Title/Abstract] OR Inhaled Fluticasone [Title/Abstract] OR inhaled mometasone [Title/Abstract] OR ciclesonide [Title/Abstract] OR inhaled budesonide [Title/Abstract] OR beclomethasone [Title/Abstract]) AND (Obstructive Sleep Apnea[Title/Abstract] OR Obstructive Sleep Apnoea [Title/Abstract] OR OSA [Title/Abstract] OR Sleep Apnea Syndrome[Title/Abstract] OR Sleep Apnoea Syndrome [Title/Abstract] OR Obstructive Sleep Disorder[Title/Abstract] OR sleep apnea [Title/Abstract] OR sleep apnoea [Title/Abstract] OR sleep-disordered breathing [Title/Abstract] OR Obstructive sleep apnea/hypopnea syndrome [Title/Abstract] OR Obstructive sleep apnoea/hypopnea syndrome [Title/Abstract])
SCOPUS: TITLE-ABS-KEY (“Inhaled Corticosteroids" OR "Inhaled Glucocorticoids" OR "Inhaled Steroids" OR “Inhaled Fluticasone” OR “inhaled mometasone” OR “inhaled ciclesonide” OR “inhaled budesonide” OR “inhaled beclomethasone”) AND TITLE-ABS-KEY ( "Obstructive Sleep Apnea" OR osa OR "Sleep Apnoea Syndrome" OR osa OR "Sleep Apnea Syndrome" OR "Sleep Apnoea Syndrome" OR "Obstructive Sleep Disorder" OR "sleep apnea " OR "sleep apnoea " OR "sleep-disordered breathing" OR “Obstructive sleep apnea/hypopnea syndrome” OR “Obstructive sleep apnoea/hypopnea syndrome”)
WEBOFSCIENCE: AB=( "Inhaled Corticosteroids" OR "Inhaled Glucocorticoids" OR "Inhaled Steroids" OR “inhaled fluticasone” OR “inhaled mometasone” OR “inhaled ciclesonide” OR “inhaled budesonide” OR “inhaled beclomethasone” ) AND AB=( "Obstructive Sleep Apnea" OR "Obstructive Sleep Apnoea" OR osa OR "Sleep Apnea Syndrome" OR "Sleep Apnoea Syndrome" OR "Obstructive Sleep Disorder" OR "sleep apnea " OR "sleep apnoea" OR "sleep-disordered breathing" OR “Obstructive sleep apnea/hypopnea syndrome” OR “Obstructive sleep apnoea/hypopnea syndrome”)
PICOS Criteria
The PICOS criteria [30] were followed to define the research scope and select the included studies. The criteria were defined as follows:
Participants:
Inclusion criteria: patients of all ages with a confirmed diagnosis of both asthma and SDB.
Exclusion criteria: patients with significant comorbidities, genetic disorders, or other asthma-related medical conditions. Studies that do not provide information on the use of ICS.
Intervention:
Inclusion criteria: patients with asthma and OSA/SDB/snoring treated with ICS.
Exclusion criteria: patients not explicitly treated with ICS.
Comparison:
Inclusion criteria:
Longitudinal studies: patients with both OSA and asthma observed before and after treatment.
Cross-sectional comparative studies: patients with OSA and asthma compared to a control group.
Exclusion criteria: asthmatic patients without specified OSA/SDB/snoring status and/or ICS treatment.
Outcome:
Primary outcome: changes in OSA/SDB/snoring severity before and after treatment with ICS.
Exclusion criteria: patients with significant comorbidities that could affect OSA outcomes in asthmatic patients treated with ICS.
Study Design:
Inclusion criteria: observational studies with a control group (including observational and comparative designs), studies with temporal perspectives (prospective, observational, cross-sectional, and longitudinal), and studies with unspecified temporal structures (cross-sectional, comparative, observational, retrospective).
Exclusion criteria:
Language: articles not written in English.
Study type: reviews, case reports, letters, studies without specific outcome measures, and duplicate studies identified through various data sources.
Data Extraction:
To minimize potential errors and interpretive bias, two independent reviewers meticulously examined the data extraction process for each study. In discrepancies between reviewers, a third reviewer was consulted to resolve issues, ensuring the accuracy and consistency of data extraction. The PRISMA flow diagram was employed to document and visualize the selection process of included and excluded studies (http://www.prisma-statement.org/PRISMAStatement/FlowDiagram).
Evaluation of the Risk of Publication Quality Distortion
We thoroughly examined potential sources of bias that could influence the results of these studies. The sources of bias considered included:
Measurement of exposure bias: this bias may occur if the exposure is not accurately measured, such as through self-reported questionnaires.
Selection bias: this type of bias can arise if participants are not selected in a representative manner from the target population.
Post-exposure intervention bias may occur if participants receive interventions after exposure to the interest factor.
Missing data bias: this bias can arise if data is missing from the study, such as when participants drop out.
Measurement of outcome bias: this bias may occur if the outcome is not accurately measured, such as when subjective measures are used.
Reporting bias: this type of bias can occur if researchers selectively report results that support their hypothesis.
As a systematic method to assess the risk of bias in observational epidemiological studies, we utilized the ROBINS-E (Risk Of Bias In Non-randomized Studies - of Exposure) tool [31]. The questions in these tools meticulously assessed the methods and results of the studies, providing ratings of "High", "Some concerns" or "Low"..
3. Results
A corpus of 136 articles was discerned upon conducting the literature search, with 36 identified as duplicates. Consequently, 87 studies were excluded: 33 were utterly irrelevant, 38 were immaterial reviews, 3 were guidelines, 6 were non-pertinent case reports or series, and 7 were in languages other than English (Figure 1). A total of 13 articles underwent exhaustive full-text scrutiny, resulting in 6 being considered non-relevant (as encapsulated in the accompanying table). The remaining 7 articles, assessed for eligibility, were incorporated into the final analysis (as summarized in the table).
Study Data
The research enumerated in Table 1, omitted from the review, encompasses four pediatric and two adult studies. Bhattacharjee et al. investigated 5,942 children who underwent A&T alongside 537 control subjects, aiming to evaluate the impact of A&T on SDB and asthma management. They observed a marked decline in asthma symptoms, ICS usage among children post-A&T, and a simultaneous decrease in SDB [32]. Kheirandish-Gozal et al.'s study involved 92 children with poorly controlled asthma (PCA). Using PSG, the authors assessed the prevalence of OSA in asthmatic children and the effect of A&T on the frequency of asthma exacerbations. They demonstrated a significant improvement in asthma exacerbations and a reduction in the use of rescue β-agonists after A&T [33]. Alfurayh et al. conducted a study on a cohort of 363 children, examining asthma exacerbations in those visiting the emergency department (ED) by analyzing demographic data and comorbidities. They found that most children using ICS did not present nocturnal symptoms, with a low prevalence of OSA [34]. Heatley et al. evaluated the association between intermittent ICS usage and adverse outcomes in asthma patients. Based on medical records from various age groups, they discovered an increased risk of pneumonia and OSA related to cumulative exposure to orally administered corticosteroids (OCS), with a higher prescription of ICS in patients with frequent OCS use [35].
Ferguson et al. conducted a comprehensive analysis of 812 individuals with asthma to investigate the relationships between lower airway dimensions, OSA, and asthma-related parameters with systemic hypertension (HTN). By examining medical histories, spirometry results, and medication regimens, they identified a significant link between high-dose ICS usage and increased HTN risk and a strong correlation between a history of OSA and HTN [36]. Magnoni et al. used questionnaires to study 174 patients in a separate investigation, focusing on epidemiology, risk factors, and treatment strategies. They concluded that the combination of ICS with long-acting beta-agonists (LABA) was the preferred therapeutic approach, while OSA and obesity emerged as critical comorbidities and risk factors for PCA [37].
Although these studies provide relevant insights into asthma and SDB, they diverged from the primary focus of the main investigation. Specifically, the excluded studies targeted different primary outcomes, such as the effects of A&T, the impact of OCS, or general risk factors like HTN, rather than the direct interplay between ICS and SDB.
The studies in Table 2, included in the analysis, were chosen for their direct relevance to the topic. Five studies were identified in adults and two in children.
Studies in Adulthood
A survey-based investigation examined 284 asthma patients, averaging 46 ± 13 years (range 18-75 years). The authors discovered a linear and dose-dependent relationship between ICS usage (OR 4.05; 95% CI 1.56-10.53) and the risk of OSA, irrespective of asthma severity [39]. Specifically, asthma patients on ICS, especially at higher doses, showed a significantly increased risk of developing OSA. The risk heightened with increased ICS doses (OR 2.29 for low doses, OR 3.67 for medium doses, OR 5.43 for high doses) [39].
A prospective, single-center, single-group study included 18 asthmatic participants with a mean age of 25.9 ± 6.3 years. This research examined the effects of ICS on upper airway collapsibility (UAW) during sleep and wakefulness in asthmatic subjects. Participants were treated with fluticasone propionate (FP) for 16 weeks. Evaluations included passive critical closing pressure (Pcrit) and nuclear magnetic resonance imaging (MRI) to measure the fat fraction and volume around the upper airways [40]. The results indicated variable changes in the AHI, with some patients improving, others worsening, and some showing no significant changes [40].
A retrospective cohort study analyzed factors linked to habitual snoring and the risk of OSA in a large sample of 38,840 asthmatic patients (mean age 52.8 ± 18.1 years) and 155,347 individuals without asthma (mean age 53.3 ± 18.0 years). The follow-up duration was around 7 years for asthmatic patients and approximately 6.5 years for the control group [41]. Findings indicated that asthmatic patients on ICS had a heightened risk of developing OSA compared to those not receiving ICS treatment, with an adjusted hazard ratio (HR) of 1.33 (95% CI = 1.01–1.76). Additionally, the asthmatic cohort overall exhibited a significantly higher risk of OSA compared to non-asthmatic individuals [41].
A prospective, randomized, controlled trial investigated the impact of cPAP on asthma control, airway reactivity, daytime sleepiness, and overall health status in asthmatic patients with nocturnal symptoms and OSA. The study included 122 participants with asthma (mean age 50.5 ± 12.0 years), divided into two groups based on the AHI: ≥ 10 (n = 41) and < 10 (n = 81). Participants were further split into CPAP (n = 17) and control (n = 20) groups [42]. The results showed no significant differences in AHI changes between the groups. However, AHI was associated with BMI and neck circumference, suggesting that OSA in asthmatic patients may be influenced by anthropometric factors and ICS use [42].
A study investigated the influence of ICS on the diagnosis of OSA, with a particular focus on the particle size of ICS. The risk associated with ICS may vary depending on the size of the emitted particles. Inhaler devices produce particles that vary in size, ranging from less than 1 µm to more than 10 µm in diameter. To effectively reach the airways, particles should be smaller than 5 µm. This cohort study included 29,816 asthmatic patients with an average age of 42.8 ± 21.1 years. Evaluations included the asthma control test (ACT) and pulmonary function tests (PFT) [43]. Findings revealed that the use of ICS with standard-size particles was linked to an increased risk of OSA (adjusted odds ratio [aOR] 1.56; 95% confidence interval [CI] 1.45–1.69), whereas ICS with extra-fine particles (<2 µm) did not significantly elevate the risk (aOR 1.11; 95% CI 0.78–1.58). Additionally, asthma control played a crucial role in the risk of OSA, with a higher probability of OSA diagnosis observed in patients with uncontrolled asthma [43].
Studies in Childhood
A prospective observational comparative study examined 108 asthmatic children with an average age of 9.1±3.4 years (range 4 to 18 years). The participants were categorized into groups without SDB (n = 76) and with SDB (n = 32). The study analyzed the associations between SDB, obesity, and asthma severity at follow-up [44]. SDB was more frequently observed in children with severe asthma compared to those with mild or moderate asthma. However, no significant correlation was found between SDB and asthma severity in children using high-dose ICS alone or in combination with other medications [44].
A retrospective study investigated the relationships between sleep, obesity, and asthma in urban minority children. This study involved a review of medical records of 443 asthmatic children (average age 10.2 ± 4.1 years), who underwent PSG. The analysis focused on the associations between spirometry measurements, BMI, and PSG parameters, adjusting for asthma and antiallergic medications [45]. Findings indicated that obese children with asthma had a significant AHI (5.9 ± 12.1 events/h) compared to their normal-weight counterparts (3.1 ± 5.7 events/h; p=0.009). ICS usage was prevalent in both groups but did not directly correlate with AHI [45].
Figure 2 illustrates the results regarding three distinct levels of bias, categorized as "Low" risk, "Some concerns," and "High" risk. The assessment of bias resulting from confounding revealed that 5 studies are problematic [39,40,42,44,45]. Bias resulting from exposure measurement was considered problematic or at high risk in 5 studies [39,41,42,44,45]. Bias in participant selection was also identified as problematic in all studies [39,40,41,42,43,44,45]. Bias related to post-exposure intervention was found problematic or with increased risk in 4 studies [42,43,44,45]. Furthermore, bias due to missing data emerged as a significant concern, with a high risk identified in 5 of the studies [39,40,42,43,44]. Moreover, outcome measurement bias was considered problematic or high risk in 5 studies [39,40,43,44,45]. Reporting outcome selection bias was seen as problematic in 100% of the studies [39,40,41,42,43,44,45]. In summary, the overall risk of bias was categorized as high or with some concerns in 100% of the studies analyzed. Each study identified at least one form of bias that raised significant concerns
4. Discussion
Despite the heightened prevalence of OSA among asthmatic patients, the impact of ICS on SDB and OSA remains a controversial issue. The studies herein reviewed offered limited and sometimes conflicting information on the intricate relationship between ICS usage for asthma and the occurrence of SDB, such as OSA.
The potential mechanism underlying the escalation of OSA or SDB in pediatric and adult asthmatic populations may stem from multiple factors. These include nasal obstruction and bronchoconstriction, leading to increased lower airway resistance and the upper airways' collapsibility during sleep [46]. Weight gain and fat accumulation in the upper airway region have also been implicated [47]. The incidence of OSA is generally higher in the asthmatic population compared to non-asthmatics, and this incidence is further elevated in asthmatic patients treated with ICS [41]. Treatment with FP has been observed to induce notable alterations in the structure of tongue muscles, evident by an augmentation in the percentage of laminin-stained areas across various muscle groups [48]. It's noteworthy that ICS usage can elicit localized effects on upper airway dilators, potentially increasing the susceptibility to OSA, akin to the mechanisms underlying the heightened risk of dysphonia in ICS users [49]. In adults, ICS usage has been linked to an increased risk of OSA, with the risk proportionally rising with higher ICS dosages [39]. Moreover, ICS formulations with larger particle sizes may prompt more pronounced pharyngeal adverse effects compared to those with smaller particle sizes [43]. While standard particle size ICS is associated with a greater risk of developing OSA, extra-fine particle ICS does not significantly elevate this risk [43]. The size of particles in ICS emerges as a critical determinant in the context of OSA, with users of extra-fine particle ICS exhibiting no significant increase in OSA risk compared to non-users, unlike those using standard particle sizes [43]. This underscores the potential impact of particle size on adverse outcomes, including OSA development, suggesting the opportunity to consider ICS particle size in asthma treatment to mitigate OSA risk in susceptible individuals [43]. Indeed, extra-fine particle ICS (<2 μm) disperse more uniformly throughout the lower airways in contrast to larger particle sizes (>5 μm), with larger particles tending to deposit more in the upper airways [43].
Prolonged therapy with ICS has been associated with modulations in hormone secretion patterns, particularly affecting growth hormone release, which may lead to metabolic and cardiovascular complications, thereby exacerbating the impact of OSA [50]. Despite some indications, research findings do not unequivocally support the notion that high-dose FP improves lung function without significantly reducing AHI in asthma patients [40]. Furthermore, it is worth pointing out that high-dose FP may not consistently lower AHI below a clinically significant threshold in all adult patients [51]. Notably, using ICS exhibits a dose-dependent relationship with the risk of OSA [39]. The use of FP did not significantly affect the AHI. However, high-dose FP usage appears to be linked to increased fat fraction and total fat volume in the structures surrounding the upper airways [40]. In obese asthmatic children, the use of ICS and montelukast is associated with a reduced AHI, although neither ICS nor montelukast significantly impacts sleep respiratory parameters in children with asthma who have normal weight [45].
Asthmatic patients undergoing ICS treatment face an elevated likelihood of OSA development [41]. This risk is particularly pronounced in cases of PCA. OSA exerts an influence on airway inflammation within asthmatic airways and correlates with inadequate asthma control. Although the precise interplay between these conditions remains elusive, inflammation should be recognized as a significant contributing factor [21]. The inflammatory infiltration of the upper airways in asthma and increased fat accumulation in pharyngeal walls due to ICS usage results in diminished cross-sectional diameter of the upper airways, likely impacting pharyngeal muscle function [21]. Consequently, asthma and its pharmacological treatments can augment the collapsibility of the upper airways, thereby contributing to OSA development and exacerbation [52].
In children, obesity and SDB heighten the risk of severe asthma. Obese asthmatic subjects tend to utilize all classes of asthma medications more frequently and particularly higher doses of ICS compared to their normal-weight counterparts [53]. Moreover, obesity and SDB escalation amplify the risk of severe asthma in children, particularly in conjunction with elevated ICS doses [44]. The correlation between ICS and nocturnal respiratory parameters varies depending on BMI [45].
Clinical studies have evidenced the positive impact of CPAP on asthma outcomes in patients concurrently experiencing OSA [54]. CPAP, advocated as the primary treatment for OSA, can potentially ameliorate asthma symptoms in adults [55]. As the frontline intervention for OSAS, CPAP therapy might modulate airway smooth muscle function and enhance asthma management in individuals with both conditions, particularly demonstrating efficacy in severe OSA cases or in those with PCA [56]. Consequently, in patients with comorbid asthma and OSA, the effectiveness of ICS therapy in alleviating asthma symptoms might be limited [42]. Notably, asthma control did not show marked improvement with CPAP, even with administering moderate doses of ICS, suggesting that CPAP might not be effective in alleviating asthma symptoms in patients with asthma and OSA [42].
This review's limitations encompass the scarcity of available studies and the heterogeneity of research findings from both pediatric and adult populations, potentially affecting the uniformity and comparability of results. Disparities in OSA definitions, aetiology, and treatments between adults (primarily addressing obesity and CPAP therapy) and paediatrics (concerning adenotonsillar hypertrophy and adenotonsillectomy) further complicate the analysis [42]. Moreover, the overall quality of existing studies is deemed suboptimal.
Since no studies have specifically investigated the interplay between ICS usage and OSA in asthmatic patients, further research to elucidate the factors contributing to the heightened prevalence of OSA among asthma patients, especially those with severe asthma, is needed. Exploring the potential variances in the interaction between ICS and OSA among pediatric and adult patients, likely influenced by distinct OSA etiologies, may shed light on such intricate relationships and guide more effective management strategies for patients affected by asthma and OSA.
5. Conclusions
In adult patients, using ICS, especially at high doses, appears to increase the risk of OSA in a dose-dependent manner. Additionally, the characteristics of ICS (inhaled particle sizes) may influence the risk of OSA. In children, the severity of asthma plays a crucial role in influencing the prevalence of SDB, while using ICS seems to be a less relevant risk factor compared to adults. These studies suggest a complex relationship between ICS use, asthma severity, and the onset of SDB. Further studies are needed.
Author Contributions
all authors contributed equally.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bitners, A.C.; Arens, R. Evaluation and Management of Children with Obstructive Sleep Apnea Syndrome. Lung 2020, 198, 257–270. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, R.; Kheirandish-Gozal, L.; Pillar, G.; Gozal, D. Cardiovascular Complications of Obstructive Sleep Apnea Syndrome: Evidence from Children. Progress in Cardiovascular Diseases 2009, 51, 416–433. [Google Scholar] [CrossRef] [PubMed]
- Nosetti, L.; Zaffanello, M.; Katz, E.S.; Vitali, M.; Agosti, M.; Ferrante, G.; Cilluffo, G.; Piacentini, G.; La Grutta, S. Twenty-year follow-up of children with obstructive sleep apnea. J Clin Sleep Med 2022, 18, 1573–1581. [Google Scholar] [CrossRef] [PubMed]
- Tagetti, A.; Bonafini, S.; Zaffanello, M.; Benetti, M.V.; Vedove, F.D.; Gasperi, E.; Cavarzere, P.; Gaudino, R.; Piacentini, G.; Minuz, P.; et al. Sleep-disordered breathing is associated with blood pressure and carotid arterial stiffness in obese children. J Hypertens 2016. [Google Scholar] [CrossRef] [PubMed]
- Jennum, P.; Riha, R.L. Epidemiology of sleep apnoea/hypopnoea syndrome and sleep-disordered breathing. Eur Respir J 2009, 33, 907–914. [Google Scholar] [CrossRef] [PubMed]
- Franklin, K.A.; Lindberg, E. Obstructive sleep apnea is a common disorder in the population-a review on the epidemiology of sleep apnea. J Thorac Dis 2015, 7, 1311–1322. [Google Scholar] [CrossRef] [PubMed]
- Zaffanello, M.; Ersu, R.H.; Nosetti, L.; Beretta, G.; Agosti, M.; Piacentini, G. Cardiac Implications of Adenotonsillar Hypertrophy and Obstructive Sleep Apnea in Pediatric Patients: A Comprehensive Systematic Review. Children (Basel) 2024, 11. [Google Scholar] [CrossRef]
- Brunetti, L.; Rana, S.; Lospalluti, M.L.; Pietrafesa, A.; Francavilla, R.; Fanelli, M.; Armenio, L. Prevalence of obstructive sleep apnea syndrome in a cohort of 1,207 children of Southern Italy. Chest 2001, 120, 1930–1935. [Google Scholar] [CrossRef] [PubMed]
- Lumeng, J.C.; Chervin, R.D. Epidemiology of pediatric obstructive sleep apnea. Proc Am Thorac Soc 2008, 5, 242–252. [Google Scholar] [CrossRef]
- Tishler, P.V.; Larkin, E.K.; Schluchter, M.D.; Redline, S. Incidence of sleep-disordered breathing in an urban adult population: the relative importance of risk factors in the development of sleep-disordered breathing. Jama 2003, 289, 2230–2237. [Google Scholar] [CrossRef]
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol 2013, 177, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.T.; Lin, Y.C.; Kuan, Y.C.; Huang, Y.H.; Hou, W.H.; Liou, T.H.; Chen, H.C. Intranasal corticosteroid therapy in the treatment of obstructive sleep apnea: A meta-analysis of randomized controlled trials. Am J Rhinol Allergy 2016, 30, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Tauman, R.; Gozal, D. Obstructive sleep apnea syndrome in children. Expert Review of Respiratory Medicine 2011, 5, 425–440. [Google Scholar] [CrossRef] [PubMed]
- Mussi, N.; Forestiero, R.; Zambelli, G.; Rossi, L.; Caramia, M.R.; Fainardi, V.; Esposito, S. The First-Line Approach in Children with Obstructive Sleep Apnea Syndrome (OSA). J Clin Med 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Kuhle, S.; Hoffmann, D.U.; Mitra, S.; Urschitz, M.S. Anti-inflammatory medications for obstructive sleep apnoea in children. Cochrane Database Syst Rev 2020, 1, Cd007074. [Google Scholar] [CrossRef] [PubMed]
- Tapia, I.E.; Shults, J.; Cielo, C.M.; Kelly, A.B.; Elden, L.M.; Spergel, J.M.; Bradford, R.M.; Cornaglia, M.A.; Sterni, L.M.; Radcliffe, J. A Trial of Intranasal Corticosteroids to Treat Childhood OSA Syndrome. Chest 2022, 162, 899–919. [Google Scholar] [CrossRef] [PubMed]
- Locci, C.; Cenere, C.; Sotgiu, G.; Puci, M.V.; Saderi, L.; Rizzo, D.; Bussu, F.; Antonucci, R. Adenotonsillectomy in Children with Obstructive Sleep Apnea Syndrome: Clinical and Functional Outcomes. J Clin Med 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Pavwoski, P.; Shelgikar, A.V. Treatment options for obstructive sleep apnea. Neurol Clin Pract 2017, 7, 77–85. [Google Scholar] [CrossRef]
- Zaghi, S.; Holty, J.E.; Certal, V.; Abdullatif, J.; Guilleminault, C.; Powell, N.B.; Riley, R.W.; Camacho, M. Maxillomandibular Advancement for Treatment of Obstructive Sleep Apnea: A Meta-analysis. JAMA Otolaryngol Head Neck Surg 2016, 142, 58–66. [Google Scholar] [CrossRef]
- Pekkanen, J.; Sunyer, J.; Anto, J.M.; Burney, P. Operational definitions of asthma in studies on its aetiology. Eur Respir J 2005, 26, 28–35. [Google Scholar] [CrossRef]
- Damianaki, A.; Vagiakis, E.; Sigala, I.; Pataka, A.; Rovina, N.; Vlachou, A.; Krietsepi, V.; Zakynthinos, S.; Katsaounou, P. Τhe Co-Existence of Obstructive Sleep Apnea and Bronchial Asthma: Revelation of a New Asthma Phenotype? J Clin Med 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Ojo, R.O.; Okobi, O.E.; Ezeamii, P.C.; Ezeamii, V.C.; Nwachukwu, E.U.; Gebeyehu, Y.H.; Okobi, E.; David, A.B.; Akinsola, Z. Epidemiology of Current Asthma in Children Under 18: A Two-Decade Overview Using National Center for Health Statistics (NCHS) Data. Cureus 2023, 15, e49229. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Adeloye, D.; Salim, H.; Dos Santos, J.P.; Campbell, H.; Sheikh, A.; Rudan, I. Global, regional, and national prevalence of asthma in 2019: a systematic analysis and modelling study. J Glob Health 2022, 12, 04052. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, M.; ElMallah, M.; Bailey, E.; Kremer, T.; Rhein, L.M. Pediatric Obstructive Sleep Apnea and Asthma: Clinical Implications. Pediatr Ann 2017, 46, e332–e335. [Google Scholar] [CrossRef] [PubMed]
- Garza, N.; Witmans, M.; Salud, M.; Lagera, P.G.D.; Co, V.A.; Tablizo, M.A. The Association between Asthma and OSA in Children. Children (Basel) 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Salles, C.; Terse-Ramos, R.; Souza-Machado, A.; Cruz Á, A. Obstructive sleep apnea and asthma. J Bras Pneumol 2013, 39, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Kong, D.L.; Qin, Z.; Shen, H.; Jin, H.Y.; Wang, W.; Wang, Z.F. Association of Obstructive Sleep Apnea with Asthma: A Meta-Analysis. Sci Rep 2017, 7, 4088. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.J. Inhaled Corticosteroids. Pharmaceuticals (Basel) 2010, 3, 514–540. [Google Scholar] [CrossRef] [PubMed]
- Reddel, H.K.; Bacharier, L.B.; Bateman, E.D.; Brightling, C.E.; Brusselle, G.G.; Buhl, R.; Cruz, A.A.; Duijts, L.; Drazen, J.M.; FitzGerald, J.M.; et al. Global Initiative for Asthma Strategy 2021: executive summary and rationale for key changes. Eur Respir J 2022, 59. [Google Scholar] [CrossRef]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: a systematic review. J Med Libr Assoc 2018, 106, 420–431. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. Bmj 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, R.; Choi, B.H.; Gozal, D.; Mokhlesi, B. Association of Adenotonsillectomy with Asthma Outcomes in Children: A Longitudinal Database Analysis. PLoS Medicine 2014, 11, e1001753–e1001753. [Google Scholar] [CrossRef] [PubMed]
- Kheirandish-Gozal, L.; Dayyat, E.A.; Eid, N.S.; Morton, R.L.; Gozal, D. Obstructive sleep apnea in poorly controlled asthmatic children: effect of adenotonsillectomy. Pediatr Pulmonol 2011, 46, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Alfurayh, M.A.; Alturaymi, M.A.; Sharahili, A.; Bin Dayel, M.A.; Al Eissa, A.I.; Alilaj, M.O. Bronchial Asthma Exacerbation in the Emergency Department in a Saudi Pediatric Population: An Insight From a Tertiary Hospital in Riyadh, Saudi Arabia. Cureus 2023, 15, e33391. [Google Scholar] [CrossRef] [PubMed]
- Heatley, H.; Tran, T.N.; Bourdin, A.; Menzies-Gow, A.; Jackson, D.J.; Maslova, E.; Chapaneri, J.; Skinner, D.; Carter, V.; Chan, J.S.K.; et al. Observational UK cohort study to describe intermittent oral corticosteroid prescribing patterns and their association with adverse outcomes in asthma. Thorax 2023, 78, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, S.; Teodorescu, M.C.; Gangnon, R.E.; Peterson, A.G.; Consens, F.B.; Chervin, R.D.; Teodorescu, M. Factors associated with systemic hypertension in asthma. Lung 2014, 192, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Magnoni, M.S.; Caminati, M.; Canonica, G.W.; Arpinelli, F.; Rizzi, A.; Senna, G. Asthma management among allergists in Italy: results from a survey. Clin Mol Allergy 2017, 15, 11. [Google Scholar] [CrossRef] [PubMed]
- Kheirandish-Gozal, L.; Dayyat, E.A.; Eid, N.S.; Morton, R.L.; Gozal, D. Obstructive sleep apnea in poorly controlled asthmatic children: Effect of adenotonsillectomy. Pediatric Pulmonology 2011, 46, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Teodorescu, M.; Consens, F.B.; Bria, W.F.; Coffey, M.J.; McMorris, M.S.; Weatherwax, K.J.; Palmisano, J.; Senger, C.M.; Ye, Y.; Kalbfleisch, J.D.; et al. Predictors of habitual snoring and obstructive sleep apnea risk in patients with asthma. Chest 2009, 135, 1125–1132. [Google Scholar] [CrossRef]
- Teodorescu, M.; Xie, A.; Sorkness, C.A.; Robbins, J.; Reeder, S.; Gong, Y.; Fedie, J.E.; Sexton, A.; Miller, B.; Huard, T.; et al. Effects of inhaled fluticasone on upper airway during sleep and wakefulness in asthma: a pilot study. J Clin Sleep Med 2014, 10, 183–193. [Google Scholar] [CrossRef]
- Shen, T.C.; Lin, C.L.; Wei, C.C.; Chen, C.H.; Tu, C.Y.; Hsia, T.C.; Shih, C.M.; Hsu, W.H.; Sung, F.C.; Kao, C.H. Risk of Obstructive Sleep Apnea in Adult Patients with Asthma: A Population-Based Cohort Study in Taiwan. PLoS One 2015, 10, e0128461. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.S.S.; Chan, T.O.; To, K.W.; Chan, K.K.P.; Ngai, J.; Yip, W.H.; Lo, R.L.P.; Ko, F.W.S.; Hui, D.S.C. Continuous positive airway pressure for obstructive sleep apnoea does not improve asthma control. Respirology 2018, 23, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Henao, M.P.; Kraschnewski, J.L.; Bolton, M.D.; Ishmael, F.; Craig, T. Effects of Inhaled Corticosteroids and Particle Size on Risk of Obstructive Sleep Apnea: A Large Retrospective Cohort Study. Int J Environ Res Public Health 2020, 17. [Google Scholar] [CrossRef] [PubMed]
- Ross, K.R.; Storfer-Isser, A.; Hart, M.A.; Kibler, A.M.; Rueschman, M.; Rosen, C.L.; Kercsmar, C.M.; Redline, S. Sleep-disordered breathing is associated with asthma severity in children. J Pediatr 2012, 160, 736–742. [Google Scholar] [CrossRef] [PubMed]
- Conrad, L.A.; Nandalike, K.; Rani, S.; Rastogi, D. Associations between sleep, obesity, and asthma in urban minority children. J Clin Sleep Med 2022, 18, 2377–2385. [Google Scholar] [CrossRef] [PubMed]
- Alkhalil, M.; Schulman, E.; Getsy, J. Obstructive sleep apnea syndrome and asthma: what are the links? J Clin Sleep Med 2009, 5, 71–78. [Google Scholar] [CrossRef] [PubMed]
- di Palmo, E.; Filice, E.; Cavallo, A.; Caffarelli, C.; Maltoni, G.; Miniaci, A.; Ricci, G.; Pession, A. Childhood Obesity and Respiratory Diseases: Which Link? Children (Basel) 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Setzke, C.; Broytman, O.; Russell, J.A.; Morel, N.; Sonsalla, M.; Lamming, D.W.; Connor, N.P.; Teodorescu, M. Effects of inhaled fluticasone propionate on extrinsic tongue muscles in rats. J Appl Physiol (1985) 2020, 128, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Chmielewska, M.; Akst, L.M. Dysphonia associated with the use of inhaled corticosteroids. Curr Opin Otolaryngol Head Neck Surg 2015, 23, 255–259. [Google Scholar] [CrossRef]
- Ragnoli, B.; Pochetti, P.; Raie, A.; Malerba, M. Interrelationship Between Obstructive Sleep Apnea Syndrome and Severe Asthma: From Endo-Phenotype to Clinical Aspects. Front Med (Lausanne) 2021, 8, 640636. [Google Scholar] [CrossRef]
- Lu, H.; Fu, C.; Li, W.; Jiang, H.; Wu, X.; Li, S. Screening for obstructive sleep apnea syndrome in asthma patients: a prospective study based on Berlin and STOP-Bang questionnaires. J Thorac Dis 2017, 9, 1945–1958. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Mihaicuta, S.; Tiotiu, A.; Corlateanu, A.; Ioan, I.C.; Bikov, A. Asthma and obstructive sleep apnoea in adults and children - an up-to-date review. Sleep Med Rev 2022, 61, 101564. [Google Scholar] [CrossRef]
- Thompson, C.A.; Eslick, S.R.; Berthon, B.S.; Wood, L.G. Asthma medication use in obese and healthy weight asthma: systematic review/meta-analysis. Eur Respir J 2021, 57. [Google Scholar] [CrossRef] [PubMed]
- Alkhalil, M.; Schulman, E.S.; Getsy, J. Obstructive sleep apnea syndrome and asthma: the role of continuous positive airway pressure treatment. Ann Allergy Asthma Immunol 2008, 101, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Abdul Razak, M.R.; Chirakalwasan, N. Obstructive sleep apnea and asthma. Asian Pac J Allergy Immunol 2016, 34, 265–271. [Google Scholar] [CrossRef]
- Davies, S.E.; Bishopp, A.; Wharton, S.; Turner, A.M.; Mansur, A.H. Does Continuous Positive Airway Pressure (CPAP) treatment of obstructive sleep apnoea (OSA) improve asthma-related clinical outcomes in patients with co-existing conditions?- A systematic review. Respir Med 2018, 143, 18–30. [Google Scholar] [CrossRef]
Figure 1.
PRISMA Flow Diagram.
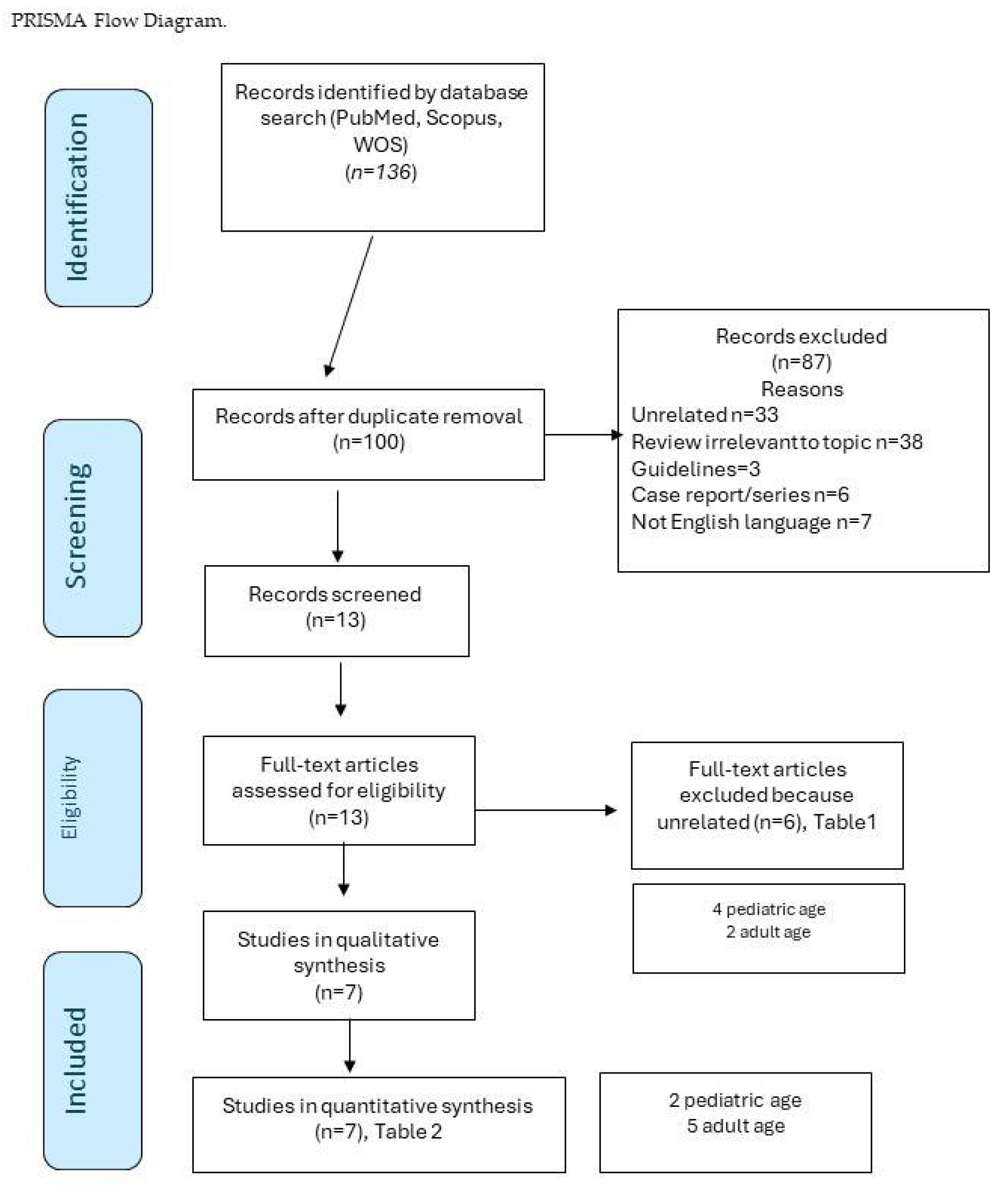
Figure 2.
Risk-of-bias plots ROBINS-E.
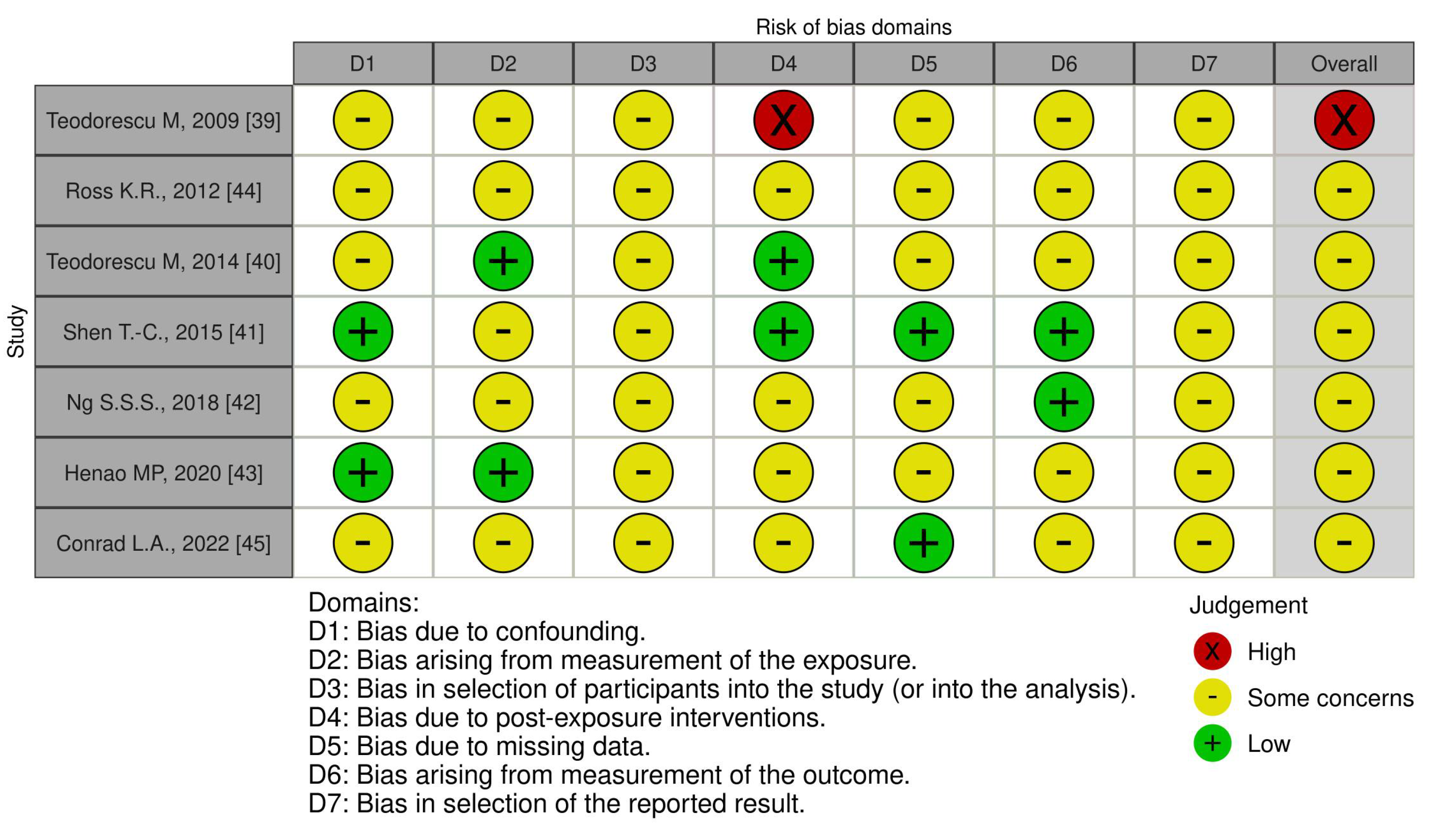

Table 1.
Excluded studies from the review.
| First Author, Year | Aim of the Study | Subjects and methods | Asthma | ICS | OSA or SDB | Conclusions | Reasons of exclusion |
|---|---|---|---|---|---|---|---|
| CHILDREN | |||||||
| Kheirandish-Gozal L, 2011 [38] | Prevalence of OSA in asthmatic PCA children. Effect of A&T on AAE frequency |
92/135 children (age 6.58 ± 1.8 years) with PCA; PSG. A&T was performed in the case of OSA. oAHI ≥5/ora TST (n.58) |
AAE (n. 92), 3.27 ± 1.13/year AAE: OSA+ (n. 58) 3.57 ± 1.37/years OSA- (n.34) 3.12 ± 1.40/years (p<0.05) |
β-rescue agonists (4.1 ± 2.4/week) β-Rescue agonists (/week): OSA+: 4,7 ± 2,9 versus OSA- 3,6 ± 2,1 (p<0,04) |
β-Rescue agonists (/week): Before T&A OSA+ (No. 35) 4.3 ± 1.8 vs. after T&A 2.1 ± 1.5 (p<0.001) Before PSG OSA- (n.24) 4.2 ± 1.9 against after PSG 3.9 ± 2.2 (p=NS) AAE (/year): Before T&A OSA+ (No. 35) 4.1 ± 1.3 vs. after T&A 1.8 ± 1.4 (p<0.001) Prima di PSG OSA- (n.24) 3,5 ± 1,5 versus dopo PSG 3,7 ± 1,7 (p=NS) |
The prevalence of OSA is higher in children with PCA Treatment of OSA by A&T is associated with improvements |
Effect of A&T on AAE Frequency in Children With PCA and Associated OSA |
| Bhattacharjee R, 2014 [32] | A&T+ Comparison with Controls, SDB, and Asthma Control | ATH A&T n.5,942 (44%) vs controls n.537 (2%) |
AAE decreased from 2,243 (30%) pre-A&T to 1,566 (2%) post-A&T in children (p<0.0001) Annual reduction in the incidence of hissing by 40.3% in A&T vs. 0% in controls |
Reduction in ICS prescription 21.5% A&T vs -2.0% controls (p<0.001) ICS/LABA −2.2% A&T vs −20.1% controld (p<0.001) Reduction of continuous inhalation for the first hour by 30% in A&T vs. 0% in controls (p<0.001) |
Reduction of OSA, snoring, and/or sleep disturbances: A&T n.3603 (27%) vs controlli n.1099 (1%) |
Children A&T: 30% reduction in AAE 1 year before A&T versus 1 year after 37.9% reduction in ASAs and 35.8% reduction in asthma-related hospitalizations |
Efficacy of A&T in Improving Asthma Symptoms and Reducing SDBs |
| Alfurayh, MA, 2022 [34] | Exacerbation of Bronchial Asthma in the ED in a Paediatric Population | Cohort study: Children in ED due to asthma exacerbation. Data collection: demographics, comorbidities, and asthma-related variables. |
Visits to the ED: yes (33.9%) vs no (66.1%) Of the 123 patients who used steroids, 74% (91) had no nocturnal symptoms (p < 0.001) |
Of the 363 asthma patients (age 4.9 ± 2.5 years; 68.8% male), 33.9% (n.123) used steroids for asthma | 1.9% with FBO (n.7). Number of patients hospitalized with OSA 4.5% (p=0.203). |
Association Between Steroid Use in Asthmatic Patients, Number of ED Visits, and Nocturnal Symptoms | Steroid Use in Asthmatic Patients, Number of ED Visits, and Nocturnal Symptoms |
| Heatley H, 2023 [35] | Intermittent prescribing of OCS in asthmatic patients and the association with adverse outcomes | Cohort study. Primary Care Medical Records (ages 4–<12, 12–<18, 18–<65 and ≥65 years) received intermittent OCS Categories: prescription: single, least frequent (≥90 day range), frequent (<90 day interval) Controls: patients not treated with OCS, matched 1:1 |
Dose-response relationship between cumulative annual exposure to OCS and risk of adverse outcomes | ICS prescriptions (0, 1–3, 4–6, 7–9, 10–12, and ≥13 administrations) 12 months prior to initial OCS prescriptions: received 1–2 administrations of SABA and ≤3 of ICS Proportion of patients receiving ≥3 administrations of SABA and ≥4 of ICS at baseline increased with more frequent OCS prescriptions Higher number of ICS prescriptions in those who had more frequent OCS prescriptions |
Higher risks of adverse outcomes related to OCS, pneumonia, and OSA | Patients with asthma who received intermittent OCS have frequent prescription. Prescribing more frequent OCS associated with higher risk of adverse outcomes |
Association Between Intermittent OCS Prescribing in Asthmatic Patients and Adverse Outcomes, Such as Pneumonia and OSA |
| ADULTS | |||||||
| Ferguson S, 2014 [36] | Association Between Lower Airway Caliber, OSA, and Other Asthma-Related Factors With HTN | Multicenter study; 812 asthmatics (ages 46 ± 14) OSA scale of the SA-SDQ Medical records: HTN, OSA, spirometry and medications |
Subjects with asthma, use of ICS n.631 (78%): low dose n.189 (23%), medium dose n.235 (29%), high dose n.207 (25%) | Associations of HTN: Low-dose ICS (OR 0.86, CI 0.50-1.45), medium doses (OR 1.1, CI 0.75-1.95), and high-dose (OR 2.18, CI 1.37-3.48) |
Association of HTN with history of OSA (OR= 5.18, CI 3.66-7.32; p<0.0001) and high risk of OSA according to SA-SDQ (OR 5.18 CI 3.66-7.32, p<0.001) | Concomitant OSA has been associated with HTN | Association Between OSA and ICS, with Hypertension in Asthmatic Patients |
| Magnoni M.S., 2017 [37] | How Italian allergists deal with asthma patients | 174 questionnaires, 16 questions: epidemiology, risk factors, therapeutic approaches and adherence to therapy |
Follow-up visits at 56.5%, worsening of symptoms for 41%, percentage of visits due to adverse effects of drugs 3% |
ICS combined with LABA were considered the treatment of choice | Sleep apnea and obesity were assessed as the most important comorbidities/risk factors of PCA | Recognizing and managing OSA could be key to improving asthma control in patients | Survey or a questionnaire exploring how Italian allergists manage asthma patients, including their treatment approaches and asthma management |
Legend: AAE, esacerbazioni asmatiche acute; ACT, punteggio del Test di Controllo dell'Asma; AO, adverse outcomes; ATH, Hypertrophy of tonsils and adenoids; A&T, adenotonsillectomy; ; ED, emergency department; ESS, Epworth Sleepiness Scale; HTN, systemic hypertension; ICS, corticosteroidi per via inalatoria; LABA, long-acting beta-agonists; oAHI, obstructive apnea hypopnea index; OCS, Oral corticosteroids; OSA, obstructive sleep apnea; PCA, poor controlled asthma; PSA, polysomnography; TST, total sleep time.
Table 2.
Included studies from the review.
| First Author, Year | Aim of the Study | Subjects and methods | Inhaled corticosteroid | Asthma | OSA o SDB | Conclusion |
|---|---|---|---|---|---|---|
| ADULTS | ||||||
| Teodorescu M, 2009 [39] | Risk Factors Associated with Habitual Snoring and OSA Risk in Asthmatic Patients | Survey 284 asthmatics (age 46 ± 13, range 18–75 years) N.143/284 (50%) had SDB or met the criteria for high OSA risk Valutazione SDB: Self-Reported OSA Symptom, SA-SDQ |
Use of ICS: n.201 (82%): Low-dose 31 Medium-dose 87 High dose 83 No. 65 patients with grade 1 asthma: n.13 (20%) with high doses of ICS n.20 (31%) senza ICS N.77 patients with grade 4 asthma => n.12 (16%) non-use of ICS n.43 (56%) high doses of ICS |
Recent spirometry data collected to assess asthma severity step: Predictors of Habitual Snoring in 244 Asthma Patients was Asthma severity step aOR 1.22 (95% CI 0.94-1.60), p=0.14 Predictors of High Risk OSA in 244 Asthma Patients was Asthma severity step aOR 1.59 (95% CI 1.23-2.06), p<0.001 |
+129% risk of OSA with low-dose ICS (OR, 2.29; C.I.95% = 0.66-7.96); +267% with mid-dose ICS (OR, 3.67; C.I.95% = 1.34-10.03) +443% with high-dose ICS (OR, 5.43; 95% C.I. = 1.96-15.05) compared to no use of ICS Dose-dependent relationship between habitual snoring and ICS dose (overall p = 0.004) Dose-dependent relationship between high OSA risk and ICS dose (overall p < 0.001) |
Increased risk of OSA associated with ICS use. Proportional increase in risk based on the dosage of ICS used. |
| Teodorescu M, 2014 [40] | Effects of Orally Inhaled FP on UAW During Sleep and Wakefulness in Asthmatic Subjects | Prospective, single group and center study Baseline: 18 participants with asthma (age 25.9 ± 6.3 years). 16-week ICS (FP) treatment Asthma duration: 14.4 ± 10.2 years. Pcrit; MRI (Fat Fraction and Volume Around the Upper Airway) Valutazione SDB: Self-Reported OSA Symptom, SA-SDQ |
High dose inhaled FP (1,760 mcg/day). Dose adherence of FP was 91.2% ± 1.7%. |
FEV1 % pretreatment 88.8 ± 1.9, post treatment 94.1 ± 0.1 (p=0.001) | AHI baseline (events/h) = 1.2 ± 2.0, improved n.8 (0.51 ± 0.48), unchanged n.8 (1.64 ± 0.79), worsened n.2 (2.40 ± 2.40) SA-SDQ baseline score = n. 18 (21.2 ± 3.9), Improved No.8 (19.38 ± 0.98) invariato n.8 (22.00 ± 1.40) Worsened No. 2 (25.00 ± 4.00) Pcrit: improved n.8 (-8.16 ± 1.36), unchanged n.8 (-8.51 ± 2.18), worsened n.2 (-7.35 ± 0.85) Changes in tongue strength with fluticasone inhaled treatment, in the anterior (p=0.02) and posterior (p=0.002) positions |
High-dose FP led to improvements in lung function (FEV1%). Improved Pcrit in some participants. No significant impact on AHI after FP treatment. No reduction in overall AHI. High-dose FP appears to be associated with an increase in fat fraction and total fat volume in surrounding upper airway structures |
| Shen T.-C., 2015 [41] | Factors Associated with Habitual Snoring and OSA Risk in Asthmatic Patients | Retrospective cohort study. With asthma: 38,840 (age 52.8 ± 18.1 years) Asthma-free: 155,347 (age 53.3 ± 18.0 years) Follow-up period: with asthma 6.95 ± 3.33 years control 6.51 ± 3.44 years SDB Rating: PSG |
OSA Risk Ratio Among Asthma Patients Based on Different Treatments ICS 11,214 (15.3 per 1000 persons/year). No ICS 13,792 (10.6 per 1000 persons/year). |
aHR +2.51 (95% CI (1.61, 2.17) of OSA in the asthmatic cohort compared to control (12.1 vs 4.84 per 1,000 person-years). OSA development during follow-up: aHR +1.87 (95% CI = 1.61-2.17) for the asthma cohort compared to the non-asthma cohort |
OSA in asthma patients: Non-steroid aHR 1 (reference) Inhaled steroid aHR 1.33 (95% CI 1.01 - 1.76) |
Overall incidence of OSA is higher in the asthmatic cohort than in the control cohort. ICS appears to be associated with an even higher incidence of OSA among asthmatic patients. |
| Henao MP, 2020 [43] | Effects of ICS on the diagnosis of OSA, with sub-analysis by particle size of ICS. |
Cohort study. 29,816 asthmatics (age 42.8 ± 21.1 years). ACT, PFT [A diagnosis of OSA was determined by ICD-9 or ICD-10 codes reported during the study period] |
Higher likelihood of OSA in ICS users with standard particle sizes (aOR +1.56, 95% CI 1.45–1.69) than in non-users There was no increased risk of OSA in users of ICS with extra-fine particles compared to asthmatics who did not use ICS (aOR 1.11, 95% CI 0.78–1.58). |
Patients with uncontrolled asthma showed a higher likelihood of receiving a diagnosis of OSA ACT score (aOR +1.60, 95% CI 1.32–1.94) among n.1380 uncontrolled asthma versus 3288 controlled asthma PFT score (aOR +1.45, 95% CI 1.19–1.77) among 1,229 uncontrolled asthma versus 1,199 controlled asthma. ICS users were more likely to have OSA, regardless of asthma control (aOR 1.58, 95% CI 1.47–1.70). |
Probability of having a diagnosis of OSA with normal-sized particle ICS (OR 1.55, 95% CI 1.11-2.16) compared to those with extra-fine particles. Increased odds of having OSA in BMI patients ≥ 25 users of normal-sized particle ICS compared to users of extra-fine particles (aOR 1.70, 95% CI 1.15-2.50). Increased odds of receiving a diagnosis of OSA in male BMI ≥ 25 users of normal-sized particle ICS compared to users of extra-fine particles (aOR 2.45, 95% CI 1.22-4.93). |
Increased risk of OSA among users of ICS with standard-sized particles, compared to non-users of ICS. No increased risk of OSA was observed among users of ICS with extra-fine particles. Patients with PCA showed a higher likelihood of OSA. The association between ICS and OSA might vary based on asthma control and individual patient characteristics, such as BMI |
| Ng S.S.S., 2018 [42] | cPAP Effect on: Asthma Control, Airway Responsiveness, Daytime Sleepiness, and Health Status in Asthmatic Patients With Nocturnal Symptoms and OSAS | Prospective, randomized controlled trial. Baseline 122 asthmatic subjects (age 50.5 ± 12.0 years). SDB Rating: PSG Patients with AHI ≥ 10 (n = 41) Patients with AHI < 10 (n = 81) CPAP group (n = 17) and control group (n = 20) |
Beclomethasone 500 μg or more per day within the last 3 months Baseline High-dose inhaled steroids 90.1% Medium-dose inhaled steroids 9.9% |
Baseline FEV1 (% predetto) 79.2 ± 20.5 No significant difference in the change of the ACT score between n.17 CPAP group 15.9 ± 2.6 vs n.20 control group 21.7 ± 10.1 (P = 0.145) |
AHI correlates with BMI (r = 0.255, P = 0.008) and neck circumference (r = 0.247, P = 0.007). No significant difference in the change of the AHI score between n.17 CPAP group 19.1 ± 11.4 vs n.20 control group 21.7 ± 10.1 (P = 0.474) |
Asthma control did not improve significantly despite taking at least a moderate dose of ICS. This therapy may not be effective in improving asthmatic symptoms in patients with concomitant asthma and OSA |
| CHILDREN | ||||||
| Ross K.R., 2012 [44] | Relationships Between Obesity, SDB, and Asthma Severity in Children | Prospective observational study, comparative study Baseline 108 (82%) asthmatic children (age 9.1 ± 3.4 years). Valutazione SDB: overnight finger pulse oximetry monitoring No SDB (n.76) età 9.3 ± 3.4 years SDB (n.32) età 8.7 ± 3.3 years Predicted FEV1 %: No SDB 98.7 ± 17.7 With SDB 90.9 ± 17.1 Associations between SDB, obesity and asthma severity at follow-up. |
Severe asthma: children using high dose ICS alone or in combination with other drugs Not severe asthma: low to moderate dose ICS |
Asthma Severity at 12-month follow-up: Mild/Mod (n.79) Severe (n.29) Asthmatic children with BMI z-score=2 and SDB had a +6.7-fold risk (OR 1.74; 95% C.I.: 25.55) of having severe asthma compared to those without SDB. Children with asthma, BMI z-score 0 and SDB did not have an increased risk (OR +1.40; CI 95% 0.31 - 6.42) of having severe asthma compared to those without SDB |
32 children (29.6%) with SDB Children with prevalent SDB (OR 4.85, 95% CI 1.94 - 12.10) in severe asthma (55.2%) vs mild/mod asthma (20.3%, p <0.01); Children with SDB had OR 5.02 (95% CI 1.88 -13.44) to have severe asthma at follow-up (12 months), after adjustment for BMI z-score (p=0.001) |
Children who are asthmatic, obese, and with SDB: Higher risk of having severe asthma than those without SDB. Asthmatic, normal-weight, and SDB children using high doses of ICS alone or in combination with other medications: There was no significant association between SDB and asthma severity |
| Conrad L.A., 2022 [45] | Associations Between Sleep, Obesity and Asthma in Urban Minority Children | Retrospective review of medical records 448 children with asthma (ages 10.2 ± 4.1 years) who performed PSG. Association between spirometry variables, BMI and PSG parameters, adjusting for asthma and anti-allergy medications. |
Inhaled steroids: Obese asthmatics n.214 (74.1%), Normal weight asthmatics n.125 (81.2%) (p=0.09). [Montelukast: asma obesa n.174 (60,2%) versus n.92 (59,7%), p=0,92] [Steroidi nasali: Asma obesi n.89 (30,8%) versus Asma normopeso n.44 (28,6%); p= 0,63] |
FEV1: Obese asthmatics 83.1 ± 16.5, Normal weight asthmatics 86.4 ± 18.7 (p=0.05) FEF25%–75%: Obese asthmatics 74.8 ± 26.5 Normal weight asthmatics 76.8 ± 28.2 (p=0.4) |
289 obese asthmatics 5.9 ± 12.1 versus 154 normal-weight asthmatics 3.1 ± 5.7 (p=0.009) | In obese asthmatic children, both ICS and montelukast are associated with lower AHI. Neither ICS nor montelukast are associated with sleep respiratory parameters in children with asthma of normal weight. |
Legend: AAE, acute asthma exacerbation; ACT, Asthma Control Test Scores; AHI, apnoea–hypopnoea index ; aHR, adjusted HR; aOR, adjusted Odds Ratio; AT, adenotonsillectomy; ASA, acute status asthmaticus; ARERs, asthma-related emergency room visits; ARHs, asthma-related hospitalizations; BMI, body mass index; CPAP, continuous positive airway pressure; ER, emergency room; FP, fluticasone proprionato; GER, gastroesophageal reflux; GINA, Global Initiative for Asthma 2020; HR, Hazard Ratio; HTN, ipertensione sistemica; ICS, corticosteroidi inalati; LABA, long acting beta agonists; MRI, risonanza magnetica nucleare; OCS, corticosteroidi orali; OSAS, obstructive sleep apnoea syndrome; PCA, poor controlled asthma; Pcrit, passive critical closing pressure; PFT, Pulmonary Function Test; PSG, polysomnography; SABA, beta2-agonisti a breve durata d'azione; SA-SDQ, Questionario sui Disturbi del Sonno; SDB, sleep disordered breathing; UAW, collassabilità delle vie aeree superiori.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



