
Submitted:
13 June 2024
Posted:
13 June 2024
You are already at the latest version
Abstract
Superior mesenteric artery (SMA) syndrome or Wilkie’s syndrome is a vascular compression disorder that causes abnormal compression of the third portion of the duodenum by the SMA. It has a low incidence rate, higher in young women, and is rarely associated with the Nutcracker phenomenon: a condition of compression of the left renal vein between the SMA and the aorta, which manifests as pain in the left flank and pelvis. Here we report the case of a 54-year-old woman with a history of repeated episodes of abdominal pain caused by the Nutcracker syndrome and Wilkie's syndrome.
Keywords:
Diagnosis
; Treatment
; Imaging
; Syndromes
1. Introduction
Superior mesenteric artery (SMA) syndrome is a rare disease in which, due to a lack of retroperitoneal fat, the third portion of the duodenum is compressed between the abdominal aorta and the SMA. Also known as Wilkie’s syndrome, SMA syndrome is characterized by a group of symptoms that could mimic anorexia nervosa and functional dyspepsia: nausea, vomiting, “stabbing” postprandial abdominal pain, bloating, heartburn, and reflux. Over time, this can lead to a reduced caloric intake and weight loss, with a further reduction of the retroperitoneal fat and a consequent increase in duodenal compression, creating a vicious circle. The precise incidence of Wilkie’s syndrome remains uncertain due to potential under- or over-diagnosis, but recent studies estimate it to be approximately 0.013%-0.3% among the general population [1]. When there is a suspicion of bowel obstruction, especially in the context of abundant weight loss, both these syndromes should be considered for differential diagnosis despite their rarity, especially considering their associated morbidity and mortality. Wilkie’s syndrome is usually diagnosed via computed tomography (CT) scanning, which makes it possible to evaluate the SMA-aorta angle (normal values: 38°-65°) [2]. Using this method, Unal et al. reported a cut-off value at 22° on the SMA-aorta angle and at 8 mm on a distance, with 42.8% of sensitivity and 100% of specificity, respectively [3]. The barium X-ray examination, Wilkie’s syndrome is characterized by some pathognomonic features. In particular, this condition presents dilatation of the first and second parts of the duodenum with or without gastric dilatation, abrupt vertical or oblique compression of the third part of the duodenum, reverse flow of the contrast liquid in the proximity of the obstruction, significant delay (4-6 hours) in gastroduodenal transit, and relief of obstruction after postural changes [4]. Nutcracker syndrome (NCS) is a rare disease characterized by an extrinsic compression of the left renal vein (LRV) between the aorta and SMA. This leads to impaired blood flow and congestion, and, thus, to a dilation of the first part of LRV [5]. There are two types of NCS: the anterior, the most common, in which there is a compression of LRV between the abdominal aorta and SMA; and the posterior, which occurs when the retro-aortic or circum-aortic renal vein is compressed in the narrow gap between the aorta and the vertebral body [6]. The prevalence of NCS is still unknown, due to the variability of its symptoms and the absence of agreed-upon diagnostic criteria, but it is reported a higher incidence rate in female patients [7]. The pathologies and conditions associated with NCS are pancreatic neoplasms, para-aortic lymphadenopathy, retroperitoneal tumor, abdominal aortic aneurysm, overarching testicular artery, strangulating fibro lymphatic tissue between the aorta and SMA, high disposition of LRV, left renal ptosis resulting in the stretching of LRV over the abdominal aortae lordosis, reduced retroperitoneal and mesenteric fat, pregnancy with a gravid uterus compressing the renal vasculature [8]. NCS is clinically characterized by flank and abdominal pain, varicocele, fatigue, and orthostatic intolerance [9]. Retrograde venography, which measures the renal vein pressure gradient, is the gold standard in NCS diagnosis. However, its invasive nature often makes it a secondary option. Usually, diagnostic workup starts with a Doppler ultrasound (US) of the renal veins, which can describe the compressive process caused by SMA. CT and magnetic resonance imaging (MRI) should be considered as additional methods. Diagnostic criteria for NCS include the presence of a venous pressure gradient between the LRV and the inferior vena cava ≥ 3mmHg, a maximum flow velocity five times higher than normal values in the LRV passing the SMA compared to the renal hilum, CT angiography or MRI angiography showing an angle between the aorta and the SMA of less than 45° [10]. However, the coexistence of both these two conditions can lead to difficult diagnostic and therapeutic management. For this reason, we report the case of a patient with Wilkie’s syndrome combined with Nutcracker syndrome.
2. Case Report
This is the case of a 54-year-old woman with a body mass index of 23.2 kg/m2 and a history of sub-continuous epigastric pain, not related to meals, radiating to the back, with associated retrosternal heartburn, nausea, and frequent belching for which she took antacids and prokinetics, with partial benefit. She underwent an esophagogastroduodenoscopy to have two hyperplastic gastric polyps removed. In addition, a diagnosis of diffuse atrophic gastritis with high titer anti-parietal cell antibodies (1:640) was made. Subsequently, she underwent a cholangio-MRI with no evidence of dilation of the intra- and extra-hepatic bile ducts or endoluminal stones. However, due to the persistence of symptoms, a cholecystectomy was performed. Postoperatively, the patient presented recurrent episodes of vomiting and an abdominal CT scan showed fluid overdistension of the stomach and abdominal adhesions, leading to a viscerolytic surgery. However, after discharge, abdominal discomfort persisted, though more mildly, and the patient was admitted to our center. A complete blood count with no evidence of laboratory parameters alterations, and subsequently, an upper gastrointestinal (UGI) series and a contrast-enhanced abdominal CT with contrast medium were performed. The UGI series showed a slowed-down progression of the contrast medium, which stagnated at the level of the third duodenal portion (Figure 1).
The diagnosis of Wilkie’s syndrome (Figure 2) and NCS (Figure 3) was further confirmed via CT scan, with evidence of a significant restriction of the third duodenal portion as well as a compression with proximal dilatation of LRV.
Subsequently, the patient started a fodmap-free diet in combination with a treatment of trimebutyn maleate 150mg thrice a day, simethicone 80mg twice a day, and probiotic tablets once a day. This resulted in an improvement but not a reversal of the symptomatology due to the patient’s poor therapeutic and alimentary compliance. Actually, considered the persistent symptomatology, and in particular persistent abdominal pain, the patient is under evaluation for a possible surgical approach.
3. Discussion
Considering the potentially associated life-threatening complications such as acute and chronic pancreatitis, severe malnutrition, duodenal and gastric ulcers, pneumoperitoneum and pneumomediastinum, Wilkie’s syndrome and NCS should always be taken into consideration in differential diagnosis in case of patients with obstructive bowel symptoms. Both syndromes, although well described in the literature, are rare clinical pictures, usually presenting alone, and their coexistence is rare. Evidence described in the literature are summarized in Table 1.
In summary, according to the reported evidence, the mean age at diagnosis of patients with both syndromes was 28,72 ± 12,85 (mean ± standard deviation), with a higher prevalence of males (12/22; 54%). Furthermore, these patients showed one to five clinical manifestations associated with both conditions. Regarding the patients’ management, CT scanning was the most used technique for diagnosis (16/22; 72%: Figure 4A), while nutritional therapy was the preferred treatment (11/22; 50%; Figure 4B).
Regarding the diagnosis, although the US has been proposed as a diagnostic exam, poor patient cooperation and intestinal meteorism may hinder the correct viewing of abdominal structures. Using the echo-color-Doppler modality, US is also useful for showing bright colors of high velocity due to the aliasing artifacts from the jetting flow immediately distal to the AM portion of the LRV. Thus, for both Wilkie’s syndrome and NCS, the definitive diagnosis is made with contrast-enhanced CT scanning or the MRI, which make it possible to detect the compression of the duodenum and LRV and accurately measure the SMA-aorta angle [33,34]. In terms of treatment options, the conservative one is the most widely adopted, especially because of the frequently associated benefits and the absence of related complications. Conversely, surgery is reserved for clinical cases characterized by a chronic persistence of symptoms unresponsive to conservative strategies. More specifically, surgical treatment is indicated in patients with the following clinical picture: 1) failure of the conservative treatment, 2) long-standing disease with progressive weight loss and duodenal dilatation with stasis, and 3) complicated peptic ulcer secondary to bile stasis and reflux [35]. Surgical interventions to consider include the Strong’s procedure, gastrojejunostomy, and duodenojejunostomy (even through a laparoscopic approach). Duodenojejunostomy appears to be the best procedure, with a success rate higher than 90%, while Strong’s procedure (lysis of the ligament of Treitz) showed a success rate of 25% [36]. Regarding NCS, conservative treatment must be preferred in young subjects given the higher probability of spontaneous remission, due to the increase in retroperitoneal fat and the formation of a collateral venous circulation [37]. Surgery is indicated in the presence of intolerable symptoms or after the failure of conservative treatment. Among the many surgical interventions, we mention LRV transposition, LRV transposition with patch venoplasty, patch venoplasty without LRV transposition, LRV transposition with saphenous vein cuff, gonadal vein transposition, and saphenous vein bypass. Among these, LRV transposition is the most common and effective approach [37,38]. Observational studies on large cohorts of patients are necessary to define appropriate guidelines on the subject of diagnosis, and to describe the possible treatment options to be adopted based on the clinical picture.
4. Conclusions
This case report highlights the diagnostic and therapeutic complexities associated with the coexistence of Wilkie’s syndrome and NCS. Although these conditions are usually present alone, their simultaneous occurrence presents unique challenges, underscoring the importance of considering both in differential diagnosis. The patient in this case report showed persistent gastrointestinal symptoms despite multiple interventions, leading to the ultimate diagnosis through advanced imaging techniques. CT and MRI remain the most used diagnostic tools for these syndromes, providing detailed anatomical insights necessary for accurate diagnosis. Conservative management, including dietary modifications and pharmacological therapy, often serves as the initial approach, although patient compliance can significantly impact the effectiveness of this strategy. In refractory cases or when conservative treatment fails, surgical interventions such as duodenojejunostomy for Wilkie’s syndrome and LRV transposition for NCS offer promising outcomes. The decision to proceed with surgery must be carefully weighed against the severity of symptoms, the patient’s overall health status, and the potential for spontaneous resolution, particularly in younger patients. This case report underscores the necessity for further research to establish comprehensive guidelines and optimize treatment protocols. Larger cohort studies are essential to better understand the pathophysiology, improve diagnostic accuracy, and refine both conservative and surgical treatment strategies for these complex syndromes.
Author Contributions
Conceptualization, L.A. and D.L.; methodology, F.I., V.B, and V.F., software, G.Q.; validation, F.I., V.B. and G.G.M.S.; data curation, F.I. and V.F.; writing—original draft preparation, F.I., V.B., VF., and G.G.M.S.; writing—review and editing, L.A. and D.L.; visualization, G.Q.; supervision, L.A., F.L. and D.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Ethical approval was not requested due to the observational, retrospective, and anonymized study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All of the data were included in the study.
Acknowledgments
We would like to thank Simone Scarlata for his critical review of the English language.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Claro, M.; Sousa, D.; Abreu da Silva, A.; Grilo, J.; Martins, JA. Wilkie’s Syndrome: An Unexpected Finding. Cureus 2021, 14, 13–e20413. [Google Scholar] [CrossRef]
- Oka, A.; Awoniyi, M.; Hasegawa, N.; Yoshida, Y.; Tobita, H. ; Ishimura, N., Ishihara, S. Superior mesenteric artery syndrome: Diagnosis and management. World J Clin Cases 2023, 11, 3369–3384. [Google Scholar] [CrossRef]
- Unal, B.; Aktaş, A.; Kemal, G.; Bilgili, Y.; Güliter, S.; Daphan, C.; Aydinuraz, K. Superior mesenteric artery syndrome: CT and ultrasonography findings. Diagn Interv Radiol 2005, 11, 90–5. [Google Scholar]
- Oka, A.; Awoniyi, M.; Hasegawa, N.; Yoshida, Y.; Tobita, H.; Ishimura, N.; Ishihara, S. Superior mesenteric artery syndrome: Diagnosis and management. World J Clin Cases 2023, 11, 3369–3384. [Google Scholar] [CrossRef]
- Kaur, R.; Airey, D. Nutcracker syndrome: A case report and review of the literature. Front Surg 2022, 9, 984500. [Google Scholar] [CrossRef]
- Ananthan, K.; Onida, S.; Davies, A.H. Nutcracker Syndrome: An Update on Current Diagnostic Criteria and Management Guidelines. Eur J Vasc Endovasc Surg 2017, 53, 886–894. [Google Scholar] [CrossRef]
- Kurklinsky, A.K.; Rooke, T.W. Nutcracker phenomenon and Nutcracker syndrome. Mayo Clin Proc 2010, 85, 552–9. [Google Scholar] [CrossRef]
- Ananthan, K.; Onida, S.; Davies, A.H. Nutcracker Syndrome: An Update on Current Diagnostic Criteria and Management Guidelines. Eur J Vasc Endovasc Surg 2017, 53, 886–894. [Google Scholar] [CrossRef]
- Gulleroglu, K.; Gulleroglu, B.; Baskin, E. Nutcracker syndrome. World J Nephrol 2014, 3, 277–81. [Google Scholar] [CrossRef]
- de Macedo, G.L. , Dos Santos, M.A., Sarris, A.B., Gomes, R.Z. Diagnosis and treatment of the Nutcracker syndrome: a review of the last 10 years. J Vasc Bras 2018, 17, 220–228. [Google Scholar]
- Barsoum, M.K. , Shepherd, R.F., Welch, T.J. Patient with both Wilkie syndrome and Nutcracker syndrome. Vasc Med 2008, 13, 247–50. [Google Scholar] [CrossRef]
- Vulliamy, P. , Hariharan, V., Gutmann, J., Mukherjee, D. Superior mesenteric artery syndrome and the ‘Nutcracker phenomenon’. BMJ Case Rep 2013, 2013, bcr2013008734. [Google Scholar] [CrossRef]
- Inal, M. , Unal Daphan, B., Karadeniz Bilgili, MY. Superior mesenteric artery syndrome accompanying with Nutcracker syndrome: a case report. Iran Red Crescent Med J 2014, 16, e14755. [Google Scholar] [CrossRef]
- Alenezy, A. , Obaid, AD., Qattan, A.A., Hamad, A. Superior mesenteric artery syndrome and Nutcracker phenomenon. Saudi J Med Med Sci 2014, 2, 223–5. [Google Scholar]
- Nunn, R. , Henry, J., Slesser, A.A.P., Fernando, R., Behar, N. A model example: coexisting superior mesenteric artery syndrome and the Nutcracker phenomenon. Case Rep Surg 2015, 2015, 649469. [Google Scholar]
- Iqbal, S. , Siddique, K., Saeed, U., Khan, Z., Ahmad, S. Nutcracker Phenomenon With Wilkie’s Syndrome in a Patient With Rectal Cancer. J Med Cases, 2016; 7, 282–285. [Google Scholar]
- Heidbreder, R. Co-occurring superior mesenteric artery syndrome and Nutcracker syndrome requiring Roux-en-Y duodenojejunostomy and left renal vein transposition: a case report and review of the literature. J Med Case Rep 2018, 12, 214. [Google Scholar] [CrossRef]
- Al-Zoubi, N.A. Nutcracker Syndrome Accompanying With Superior Mesenteric Artery Syndrome: A Case Report. Clin Med Insights Case Rep 2019, 12, 1179547619855383. [Google Scholar] [CrossRef]
- Shi, Y. , Shi, G., Li, Z., Chen, Y., Tang, S., Huang, W. Superior mesenteric artery syndrome coexists with Nutcracker syndrome in a female: a case report. BMC Gastroenterol 2019, 19, 15. [Google Scholar] [CrossRef]
- Diab, S.; Hayek, F. Combined Superior Mesenteric Artery Syndrome and Nutcracker Syndrome in a Young Patient: A Case Report and Review of the Literature. Am J Case Rep 2020, 21, e922619. [Google Scholar] [CrossRef]
- Lin, T.H. , Lin, C.C., Tsai, J.D. Superior mesenteric artery syndrome and Nutcracker syndrome. Pediatr Neonatol 2020, 61, 351–352. [Google Scholar] [CrossRef]
- Farina, R. , Iannace, F.A., Foti, P.V., Conti, A., Inì, C., Libra, F., Fanzone, L., Coronella, M.E., Santonocito, S., Basile, A. A Case of Nutcracker Syndrome Combined with Wilkie Syndrome with Unusual Clinical Presentation. Am J Case Rep 2020, 21, e922715. [Google Scholar] [CrossRef]
- Wang, C. , Wang, F., Zhao, B., Xu, L., Liu, B., Guo, Q., Yang, X., Wang, R. Coexisting Nutcracker phenomenon and superior mesenteric artery syndrome in a patient with IgA nephropathy: A case report. Medicine (Baltimore) 2021, 100, e26611. [Google Scholar] [CrossRef]
- Suárez-Correa, J. , Rivera-Martínez, W.A., González-Solarte, K.D., Guzmán-Valencia, C.F., Zuluaga-Zuluaga, M.V.S., Juan, C. Nutcracker Syndrome Combined with Wilkie Syndrome: Case Report. Rev. colomb. Gastroenterol 2022, 37, 306–310. [Google Scholar]
- Laskowski, T. , Tihonov, N., Richard, M., Katz, D., d’Audiffret, A., Lim, S. Concurrent Nutcracker syndrome and superior mesenteric artery syndrome requiring duodenojejunal bypass and left renal vein transposition. Ann Vasc Surg 2022, 2, 100099. [Google Scholar]
- Khan, H. , Al-Jabbari, E., Shroff, N., Barghash, M., Shestopalov, A., Bhargava, P. Coexistence of superior mesenteric artery syndrome and Nutcracker phenomenon. Radiol Case Rep 2022, 17, 1927–1930. [Google Scholar] [CrossRef]
- Ober, M.C. , Lazăr, F.L., Achim, A., Tirinescu, D.C., Leibundgut, G., Homorodean, C., Olinic, M., Onea, H.L., Spînu, M., Tătaru, D., et al. Interventional Management of a Rare Combination of Nutcracker and Wilkie Syndromes. J Pers Med 2022, 12, 1461. [Google Scholar] [CrossRef]
- Güngörer, V. , Öztürk, M., Arslan, Ş. A rare cause of recurrent abdominal pain; the coexistence of Wilkie’s syndrome and Nutcracker syndrome. Arch Argent Pediatr 2023, 121, e202102373. [Google Scholar]
- Castro, B.N. , Ferreira, A.R., Graça, S., Oliveira, M. Combined superior mesenteric artery syndrome and nutcraker syndrome presenting as acute pancreatitis: a case report. J Vasc Bras 2023, 22, e20220161. [Google Scholar] [CrossRef]
- Pacheco, T.B.S. , Chacon, A.C.M., Brite, J., Sohail, A.H., Gangwani, M.K., Malgor, R.D., Levine, J., do Amaral Gurgel, G. Nutcracker phenomenon secondary to superior mesenteric artery syndrome. J Surg Case Rep 2023, 2023, rjac622. [Google Scholar] [CrossRef]
- Alonso-Canal, L. , Santos-Rodríguez, A., Gil-Fournier-Esquerra, N., García-Centeno, P. Wilkie’s and Nutcracker’s syndromes overlapping a case of functional dyspepsia. Rev Gastroenterol Peru 2023, 43, 74–6. [Google Scholar] [CrossRef]
- Brogna, B. , La Rocca, A., Giovanetti, V., Ventola, M., Bignardi, E., Musto, L.A. An interesting presentation of a rare association of the Wilkie and Nutcracker syndromes. Radiol Case Rep 2023, 18, 2677–2680. [Google Scholar] [CrossRef]
- Forte, A.; Santarpia, L.; Venetucci, P.; Barbato, A. Aorto-mesenteric compass syndrome (Wilkie’s syndrome) in the differential diagnosis of chronic abdominal pain. BMJ Case Rep 2023, 16, e254157. [Google Scholar] [CrossRef]
- Kim, S.H. Doppler US and CT Diagnosis of Nutcracker Syndrome. Korean J Radiol 2019, 20, 1627–1637. [Google Scholar] [CrossRef]
- Makam, R.; Chamany, T.; Potluri, V.K.; Varadaraju, P.J.; Murthy, R. Laparoscopic management of superior mesentric artery syndrome: A case report and review of literature. J Minim Access Surg 2008, 4, 80–2. [Google Scholar] [CrossRef]
- Fromm, S.; Cash, J.M. Superior mesenteric artery syndrome: an approach to the diagnosis and management of upper gastrointestinal obstruction of unclear etiology. South Dakota Journal of Medicine 1990, 43, 5–10. [Google Scholar]
- Muheilan, M.; Walsh, A.; O’Brien, F.; Tuite, D. Nutcracker syndrome, conservative approach: a case report. J Surg Case Rep 2022, 2022, rjac423. [Google Scholar]
- Velasquez, C.A.; Saeyeldin, A.; Zafar, M.A.; Brownstein, A.J.; Erben, Y. A systematic review on management of Nutcracker syndrome. J Vasc Surg Venous Lymphat Disord 2018, 6, 271–278. [Google Scholar] [CrossRef]
Figure 1.
Antero-posterior projection of the UGI series showed a slowed gastric emptying time in later scans.
Figure 1.
Antero-posterior projection of the UGI series showed a slowed gastric emptying time in later scans.

Figure 2.
(A) Contrast-enhanced CT scan in axial projection showed the narrowing of the third duodenal portion between the aorta and the SMA, as indicated by red arrow (aorto-mesenteric distance of approximately 3 mm). (B) Contrast-enhanced CT scan in sagittal projection showed the narrowing of the third duodenal portion between the aorta and the SMA, with reduction of the aorto-mesenteric angle of approximately 13°, as indicated by red arrow (normal values: 28-65°).
Figure 2.
(A) Contrast-enhanced CT scan in axial projection showed the narrowing of the third duodenal portion between the aorta and the SMA, as indicated by red arrow (aorto-mesenteric distance of approximately 3 mm). (B) Contrast-enhanced CT scan in sagittal projection showed the narrowing of the third duodenal portion between the aorta and the SMA, with reduction of the aorto-mesenteric angle of approximately 13°, as indicated by red arrow (normal values: 28-65°).
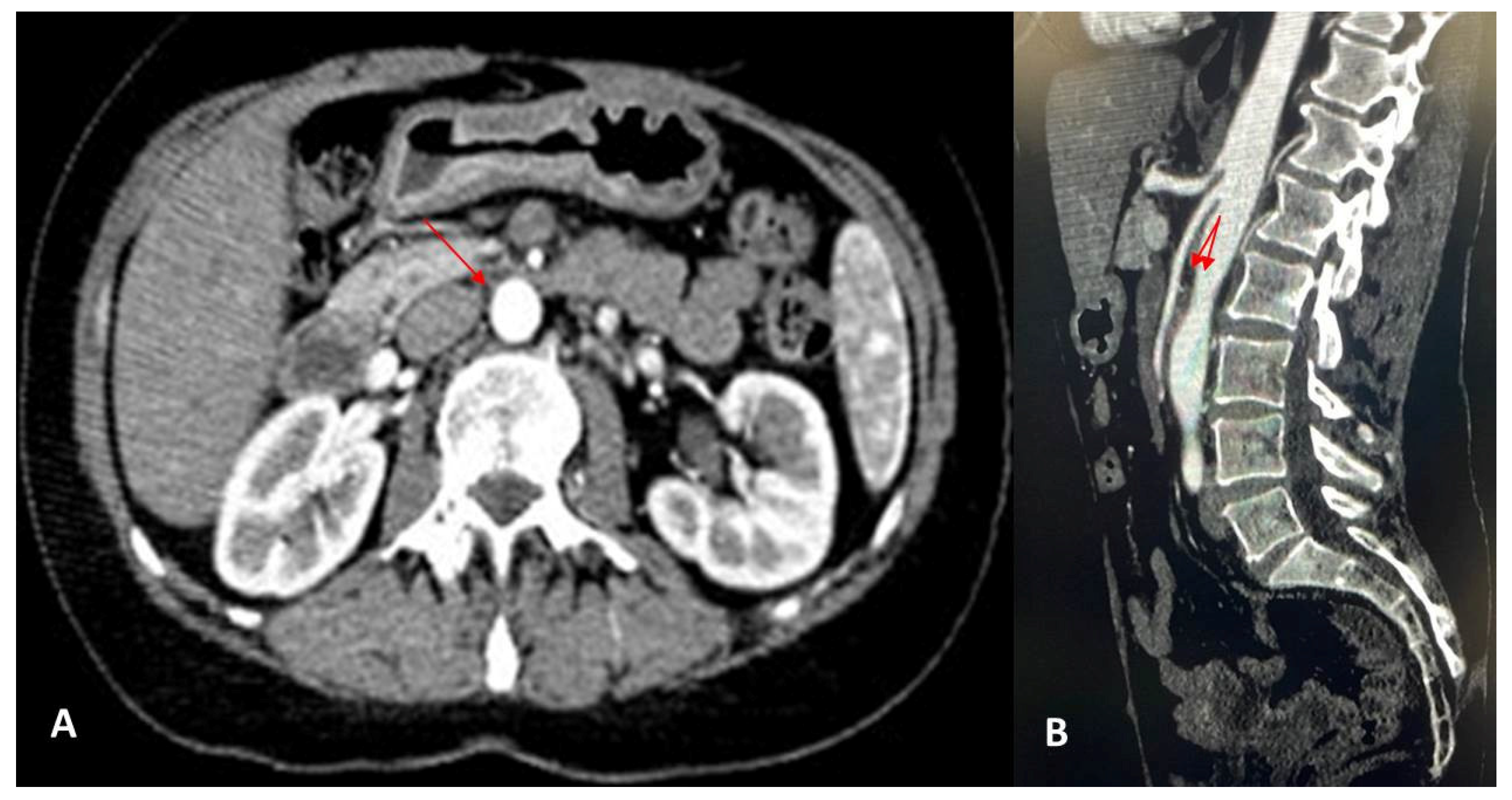
Figure 3.
(A and B) Contrast-enhanced CT scan, in axial projection, showed the compression of the LRV. (C) Reversal flow from the left gonadal vein in a coronal projection.
Figure 3.
(A and B) Contrast-enhanced CT scan, in axial projection, showed the compression of the LRV. (C) Reversal flow from the left gonadal vein in a coronal projection.
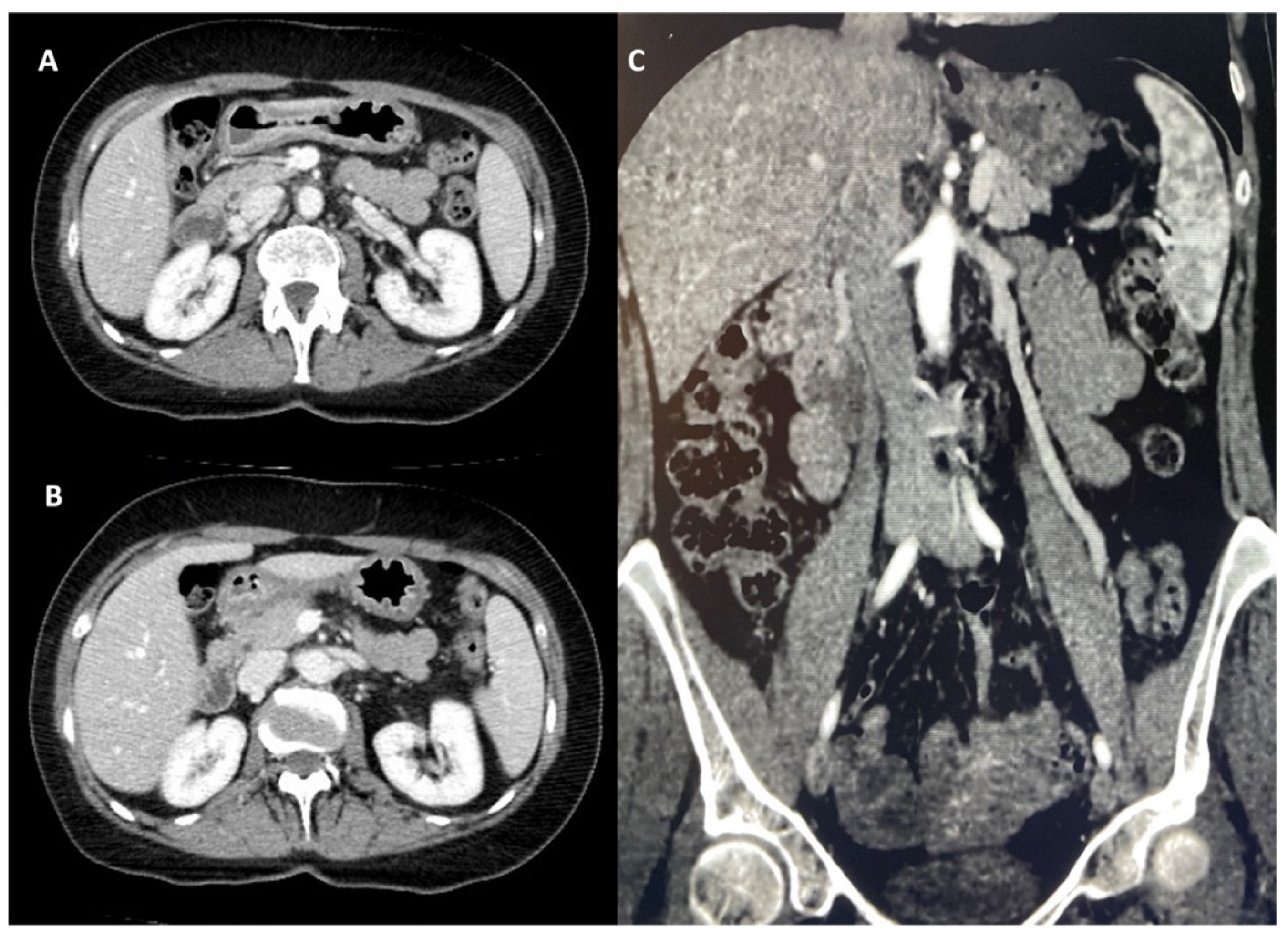
Figure 4.
Different (A) diagnostic approaches, and (B) treatment according to the studies in the literature.
Figure 4.
Different (A) diagnostic approaches, and (B) treatment according to the studies in the literature.
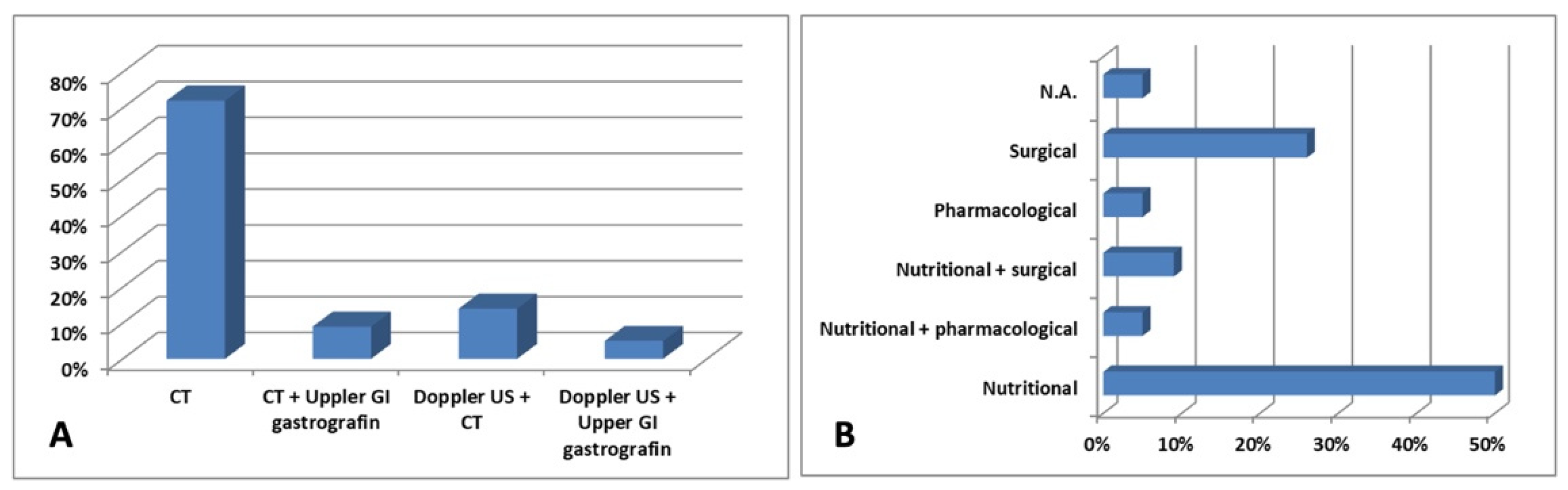

Table 1.
Summary of the different studies regarding the co-existence of Wilkie’s syndrome and NCS.
| Reference | Patient | Clinical manifestations | Diagnosis | Treatment |
|---|---|---|---|---|
| Barsoum et al., 2008 [11] | 29-year-old female | Early satiety and post-prandial epigastric abdominal pain |
CT Upper GI gastrografin |
Enteral nutrition |
| Vulliamy et al., 2013 [12] | 55-year-old male | Vomiting, epigastric pain and bloating | CT | N.A. |
| Inal et al., 2014 [13] | 28-year-old male | Cachexia and intermittent abdominal pain | CT | Enteral nutrition |
| Alenezy et al., 2014 [14] | 17-year-old male | Abdominal pain and intermittent vomiting | CT | Fluid and electrolytes replacement and nasogastric tube decompression |
| Nunn et al., 2015 [15] | 19-year-old female | Severe epigastric pain associated with emesis and anorexia | CT | Enteral nutrition |
| Iqbal et al., 2016 [16] | 62-year-old male | Cachexia | CT | Enteral nutrition |
| Heidbreder; 2018 [17] | 20-year-old female | Severe left flank and lower left quadrant pain, abdominal pain, nausea, and vomiting | CT | Roux-en-Y duodenojejunostomy and LRV transposition |
| Al-Zoubi; 2019 [18] | 38-year-old female | Intermittent left-sided loin pain | CT | LRV transposition |
| Shi et al., 2019 [19] | 32-year-old female | Severe bloating, epigastric pain, left flank ache, nausea and occasional vomiting | CT | Fluid resuscitation with parenteral and enteral nutritional support, plus mosapride citrate dispersible tablets 5 mg thrice a day |
| Diab et al., 2020 [20] | 18-year-old male | Crampy post-prandial abdominal pain associated with bilious vomiting, and signs of varicocele | CT | Regular assumption of a liquid diet |
| Lin et al., 2020 [21] | 15-year-old male | Postprandial discomfort, nausea, and vomiting | CT | Enteral and parenteral nutrition |
| Farina et al., 2020 [22] | 27-year-old male | Painful post-prandial crises at the sub-acute onset, located at the epigastrium | Doppler US CT |
Endovascular stent grafting |
| Wang et al., 2021[23] | 15-year-old male | Hematuria, fatigue, anorexia, nausea, and recurrent abdominal distension | Doppler US Upper GI gastrografin |
Pulse dose of methylprednisolone 500 mg daily for 3 days, followed by 1 mg/kg orally and mycophenolate mofetil 0.75 g twice a day |
| Suarez-Correa et al., 2022 [24] | 25-year-old male | Postprandial abdominal pain and distension, nausea, vomiting, and distension | CT Upper GI gastrografin |
Enteral nutrition and surgery |
| Laskowski et al., 2022 [25] | 40-year-old female | Nausea, early satiety and diffuse abdominal pain | CT | LRV transposition |
| Khan et al., 2022 [26] | 25-year-old female | Abdominal pain associated with nausea, bilious emesis, and diarrhea | CT | Surgery and conservative therapy |
| Ober et al., 2022 [27] | 45-year-old female | Macroscopic hematuria, intermittent pain in the left flank and hypogastric region, postprandial nausea, and cachexia | Doppler US CT |
Stent implantation in the LRV |
| Gungorer et al., 2022 [28] | 17-year-old male | Abdominal pain, nausea, and vomiting | Doppler US CT |
Surgery |
| Castro et al., 2023 [29] | 18-year-old female | Epigastric pain and emesis | CT | Dietary changes |
| Pacheco et al., 2023 [30] | 26-year-old male | GI obstructive symptoms | CT | Enteral nutrition |
| Alonso-Canal et al., 2023 [31] | 24-year-old male | Functional dyspepsia | CT | Dietary changes |
| Brogna et al., 2023 [32] | 37-year-old female | Abdominal pain with sub-occlusive episodes, nausea, and vomiting | CT | Periodic insertion of a nasogastric tube to decompress the stomach, along with a high-protein diet and parenteral nutritional supplements |
Abbreviations: CT: computed tomography; GI: gastrointestinal; N.A: not available; LRV: left renal vein; US: ultrasound.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



