
Submitted:
13 June 2024
Posted:
14 June 2024
You are already at the latest version
Abstract
Background and Objectives: Metastases are the most common tumors of the spine. As an important increase in the annual incidence of spinal metastases (SM) has been observed in the last decade, the aim of this study was to describe the epidemiology and histopathological types of SM surgically treated in the neurosurgery clinics of a regional hospital in North-Eastern Romania over a period of 5 years, in order to define a certain tumor profile that would benefit from an early screening. Materials and Methods: We retrospectively evaluated 115 adult patients, searching for demographic data (gender and age of the patients), primary tumor characteristics (location and histological type), topography and histopathological type of the spinal metastasis, and the time interval between the diagnosis of the primary tumor and the surgery for the spinal metastasis. Results: The patients were elderly (average age = 58.96 years), with a male predominance (67.82%). Main location of SM was in thoracic region (44.34%), with multiple vertebral metastases in 30.43% patients. Only 33.04% of the patients had a known cancer at the time of admission. Primary tumor was located mainly in lung (47.82%), gastrointestinal tract (15.65%), breast (11.30%), prostate (10.43%) and kidney (9.56%). SM from lung cancer mostly expressed squamous cell carcinoma (19.13%), and those from the digestive system mostly exhibited a moderately/poor colorectal adenocarcinoma (8.69%). Conclusions: Our data suggest the need for close surveillance of patients diagnosed with lung cancer and colorectal cancer because these malignancies most frequently develop spinal metastases. Smoking prevention actions and screening programs for the detection and removal of precancerous colorectal lesions must be developed and expanded.
Keywords:
spinal
; metastases
; epidemiology
; North-Eastern Romania
; histopathological types
; neurosurgery
1. Introduction
Spinal metastases (SM) are common in oncology practice as they can occur in 70%–90% of breast and prostate cancers [1]. Metastases are the most common tumors of the spine, accounting for approximately 90%-95% of the lesions identified on imaging investigations of this segment of the body [1,2].
An important increase in the annual incidence of SM has been observed in the last decade [3], especially of those with lung, breast, prostate, urological cancer as a starting point, although no significant increases were found in the incidence of the same primary cancers. More significant is the fact that in the next two decades an even more obvious increase in the incidence of cancer has been estimated, so that in 2040 almost 30 million new cases will be diagnosed [4]. On the other hand, however, the possibilities of detection and treatment of a cancer will improve, so life expectancy will increase, but the possibility of developing metastases with various locations, including bones, will also increase.
Bone is one of the most common sites where advanced solid tumors metastasize. But bone metastases greatly affect patients’ quality of life, in addition to increasing healthcare costs and mortality risk [5].
To date there are quite few data on the epidemiology and pathological diagnosis of SM [6], so that new data are needed in the conditions of the increase in the survival rate of these patients due to improving treatment option, which will lead in the coming years to an increasing number of patients who will present bone metastases at a certain moment in the tumor evolution. For this reason, the aim of this study was to describe the epidemiology and histopathological types of SM hospitalized in the neurosurgery clinics of a regional hospital in North-Eastern Romania over a period of 5 years, in order to define a certain tumor profile that would benefit from an early screening.
2. Materials and Methods
We performed a single-center, observational, descriptive, and retrospective study conducted at “Prof. Dr. N. Oblu” Emergency Clinical Hospital of Iași, which is a neurosurgical hospital of reference in Romania, which admits the most difficult cases in the North-Eastern region of the country.
The institutional database was searched to identify all patients who underwent spinal surgery for spinal metastases between January 2015 and December 2019.
We included only adult patients (≥18 years old) and only those with a well-established pathological diagnosis of a vertebral metastasis based on the specimens collected intraoperatively.
Demographic data (gender and age of the patients), primary tumor characteristics (location and histological type), topography and histological type of the spinal metastasis, and the time period between the diagnosis of the primary tumor and the surgery for the spinal metastasis were collected from electronic medical records.
Pathological findings and microscopical images of SM were obtained from the file archive and photo archive of Department of Pathology from the same hospital.
Data concerning patients’ age and gender, location and pathological diagnosis of the primary tumor as well as of the spinal metastases were included into a Microsoft Excel spreadsheet, thus obtaining absolute and percentage frequencies. The results were illustrated and compared using the up-mentioned software charting capabilities.
This study was approved by the Ethics Committee of “Prof. Dr. N. Oblu” Emergency Clinical Hospital, Iași, Romania, by Decision no: 8/05.06.2024 and written informed consent was obtained from each patient at the time of admission to hospital.
3. Results
3.1. Sociodemographic Characteristics of Patients
In the present study, 115 patients were included, of which 67.82% (n= 78) were male and 32.15% (n=37) were female, with a ratio male to female of 2.1. The average age of the entire studied group was 58.96 years (range: 27 to 84 years). The mean age of female patients was 58.56 years (range: 29 to 79 years) and the mean age of male patients was 59.15 years (range: 27 to 84 years) (Figure 1).
3.2. Topography of Spinal Metastasis
The location of the spinal metastatic tumor was at the cervical level in 10.43% cases (n=12), with a ratio M:F=1; in the thoracic region in 44.34% cases (n=51), with a ratio M:F=2.4; 39.13% of cases (n=45) were located in the lumbar region, with a ratio M:F= 2; 6.08% of all cases (n=7) were registered in the sacral region, with a ratio M:F=1.33 (Figure 2).
There were multiple vertebral metastases in 30.43% patients (n=35) (Figure 3).
In 66.95% of patients (n=77) the location of the primary tumor was established after the surgical intervention due to pathological diagnosis made on surgical specimens. In 33.04% of the patients (n=38) the diagnosis of cancer was known at the time of admission to neurosurgery clinics (Figure 4).
3.3. Formatting of Mathematical Components
From the point of view of the location of the primary tumor, vertebral bone metastases originated in a lung cancer in 47.82% patients (n=55), gastrointestinal cancer in 15.65% of patients (n=18), breast cancer in 11.30% of patients (n=13), prostate cancer in 10.43% of patients (n=12), kidney cancer in 9.56% of patients (n=11), skin melanoma in 1.73% patients (n=2), germ cell tumors in 1.73% of all patients (n=2), thyroid and endometrial carcinoma in 0.86% of all patients for each case (n=1) (Figure 5).
From a pathological point of view, SM from lung cancer expressed the following histological types: adenocarcinoma (solid, acinar, papillary, and colloid), squamous cell carcinoma (moderate/poor differentiated), neuroendocrine tumors (Small cell carcinoma and large cell neuroendocrine carcinoma), Pleomorphic carcinoma and adenosquamous carcinoma (Table 1, Figure 6).
Those SM originating from the digestive system presented various histological types depending on the location of the primary tumor, namely: squamous carcinoma (moderate/poor differentiated) from cancer of mucosa of the oral cavity, adenocarcinoma (moderate/poor differentiated) from colorectal cancer, trabecular hepatocellular carcinoma from liver cancer, cholangiocarcinoma from a biliary tree cancer (Table 2, Figure 7).
SM originating in breast cancers exhibited two histological types: infiltrating ductal carcinoma, NOS, and oncocytic carcinoma (Table 3, Figure 8).
SM originating in prostate cancer exhibited an acinar adenocarcinoma as a histologic type. When primary tumor was located in the kidney, SM presented the phenotype of a renal clear cell carcinoma. SM from cutaneous melanoma exhibited the same histological type. Microscopical exam of SM originating in germ cell tumors revealed two histological types: seminoma and embryonal carcinoma. Uterine tumors metastasing in vertebrae showed endometrial endometrioid carcinoma as the unique histological type. SM from thyroid cancer expressed follicular carcinoma as the only histological type (Table 4, Figure 9).
3.3. Time Interval between the Diagnosis of the Primary Tumor and the Appearance of the Primary Metastasis
For cases in which the primary tumor was known, the time between initial diagnosis and diagnosis of surgical intervention for SM averaged 20.06 months, with variations depending on the location of the primary tumor. Thus, the time interval between these two significant moments in the evolution of the analyzed malignancies was 17.1 months for lung cancer, 19.56 months for gastrointestinal cancer, with variation between 38 months for hepatocellular carcinoma and 8 months for squamous cell carcinoma of the oral cavity mucosa, 23 months for breast cancer, 33 months for prostate cancer, 20.75 months for kidney cancer, 26 months for cutaneous melanoma and one month for germ cell tumors (Table 5).
4. Discussion
Over time, various theories have appeared regarding the mechanisms of SM. Thus, various authors assumed that they can develop either by hematogenous, venous or arterial dissemination, by direct tumor extension, by lymphatic dissemination, and by subarachnoid and leptomeningeal seeding [7,8]. Recently, a new theory has emerged, i.e., that the center of the vertebral body is the primary niche for the development of complex interactions between metastatic cancer cells and the vertebral bone environment, with subsequent posterior dissemination via pedicles [1].
The age of SM patients varies in the literature, depending on the type of patients included in the study group. When only adults (≥18 years) are included, as in the present study, the mean age is in the seventh decade of life. Thus, Truong et al. [9] reported for their series a mean age of 60.91±9.72 years, and the male to female ratio was in favor of the male patients (1.15:1). Another study [5] also found that SM predominantly affects male patients (53.05%), mostly elderly, as 51.97% were older than 60 years. But in breast and prostate cancers, SM occur predominantly in the corresponding gender, and the incidence increases with age in prostate cancer and decreases with age in breast cancer. Also, in the case of genito-urinary cancers, SM occur mostly in females.
A similar research [10] with the present study, but conducted in Brazil on 51 consecutive patients with SM who were evaluated over a period of 3 years (2010–2012), identified a predominance of male patients (68.62%). The mean age was 61.07 ± 11.78 for women and 62.74 ± 10.17 for men. Another epidemiological study [11] that investigated the age and gender of 1196 patients with SM found out a male predominance (59.95%), with a male to female ratio of 1.50:1. Also, most patients (63.71%) were elderly, as their age ranged from 50 to 69. The mean age was 58.6 ± 11.6 (range: 13 to 89 years), and the median age was 59.0 years. The mean age of men was 59.4±11.9 (range: 16 to 89 years) and the mean age of women was 57.4±11.1 (range: 13 to 83 years), thus showing that the time of onset of SM was 2 years earlier in women than in men. These data differ from those obtained in the present paper in terms of age because those authors also included child patients (age ≤18 years).
Cerqueira et al. [2] also included both children and adults with SM in their study, so the mean age was 51.9 years, and the median age was 54 years. Anyway, also in their study, most patients (33.3%) were in their seventh decade of life (60-69 years).
A study conducted in Korea [5] identified that SM predominantly affects male patients (53.05%), mostly elderly (51.97%), aged over 60 years. However, in breast and prostate cancer, SM occur predominantly in the corresponding gender, and the incidence increases with age in prostate cancer and decreases with age in breast cancer. In cases with genitourinary cancers, SM developed mostly in female patients. Lu et al. [12] reported that their female patients presented a median age of 64 years (range: 36 to 88 years), but their male patients had a median age of 71 years (range: 26 to 92 years) at the time of SM diagnosis.
On the other hand, in a previous personal work on SM, but focused only on those with a gastrointestinal cancer starting point, we also identified an average age of the patients of 66.42 years, with variations between 35 and 80 years and a male predominance (75%) [13].
Regarding the topography of SM, there is unanimity among researchers, namely that these lesions are more frequently found in the thoracic region, followed by the lumbar and sacral regions, while the cervical region is the least frequently affected by these malignancies [1,2,9,11]. Wang et al. [11] found that the most common spinal level involved is thoracic (26.42%), followed by lumbar (23.50%), sacral (7.19%) and cervical (6.77%). A study similar to the present one [9], conducted on 191 patients aged ≥18 years, who underwent surgery for SM, reported that the lesion was predominantly located at thoracic level (50.26%), followed by the lumbar (25.13%) and cervical (24.60%) levels. Univariate analysis, however, did not identify a prognostic role of the region affected by SM, either in terms of patient survival or improvement in patient motor function after surgery.
Also, Cerqueira et al. [2] also found that the majority of SM developed at the thoracic level (66.66%), followed by the lumbar region (38.09%) and the cervical and sacral levels, each of them being involved in 9.52% of cases.
The literature states that usually, at the time of diagnosis, SM are most often multiple, meaning that 2 or more levels are affected. Wang et al. [11] reported the presence of multiple SM in 36.12% of their cases. In the present study, multiple SM were present in two-thirds of the cases, which demonstrates that the addressability of oncological patients in neurosurgery clinics for symptoms determined by SM is delayed. This finding may be due to either a lack of medical education or a lower economic-social status, but a greater aggressiveness of primary tumors that disseminate at the spinal level must also be taken into account.
In the present research, two-thirds of the cases admitted to the neurosurgery clinic did not have the primary tumor identified before surgery. The reasons for not knowing the primary tumor location could be the relatively small size of the tumor, as can be the case of lung cancer, which can escape imaging detection, the lacking of specific symptoms, as in the case of colon cancer, liver and biliary tree cancers, thyroid or kidney cancers, or the primary tumor location in the pelvis, such as uterine or prostate cancer, for which patients usually delay seeing the doctor for personal reasons.
The identification of the primary tumor is very important in the management of SM because it is of great value in selecting the best treatment option to obtain the longest possible patient survival, especially in cases with unknown primary tumor, when the tumor is small or asymptomatic [14]. Especially in these situations, but even in cases with already known cancer, without surgery there is no therapy available and the patient’s survival is very low. As a result, the diagnosis of SM can be obtained with the help of at least one biopsy that ensures the sampling of tumor tissue. The biopsy or surgical specimen ensures the identification of the site and the histological type of primary tumor based on histopathological investigations, supplemented with immunohistochemical and possibly histochemical stainings, especially due to the fact that SM are moderately or poorly differentiated compared to the morphological appearance of the corresponding primary tumor.
Over time, there have been widely varying reports regarding the primary tumor pathology that presents the highest incidence of SM. An earlier study, from 1997 [15], analyzed 71 patients with SM to identify the importance of primary tumor location in determining preoperative prognosis. The authors found that 47.88% of the analyzed patients had thyroid cancer, 39.43% had kidney cancer, and in the remaining 12.67% of patients the site of the primary tumor was unknown at the time of surgery. The authors concluded that, when the primary tumor is unknown, the median survival period is significantly shorter than in patients with known primary tumors at the time of SM treatment.
A prospective clinical study [16], carried out in 2000 on 153 patients with SM identified the site and histology of the primary tumor as follows: breast carcinoma (37%), prostate carcinoma (28%), lung carcinoma (18%), which included non–small cell lung carcinoma in 12% of cases and small cell lung carcinoma in 6% of cases. In 17% of all cases other solid tumors were identified. An MRI study [17] performed on 280 patients identified the locations of primary tumors in patients with SM as follows: lung (25.71%), breast (23.21%), prostate (20.35%), hematological cells (8.21%), urinary tract (7.5%), gastrointestinal system (4.64%), unknown (4.28%), and others (6.07%). In their series of 134 clinically and MRI-investigated oncological patients with SM, Lu et al. [12] identified primary cancer in equal percentages (24%) at the breast and lung level, 15% of all cases were from the prostate, 10% were hematologic neoplasms, and 26% of cases had other primary locations. In the series of Chaichana et al. [18], primary cancer diagnoses for their 162 included patients were diverse, reported as follows: hematopoietic cancers (17%), lung cancer (16%), breast cancer (16%), kidney cancer (13%), and prostate cancer (12%). Botelho et al. [10] reported that, of the 51 patients with SM analyzed in their study, 23.52% were diagnosed with primary breast tumors, 23.52% with prostate cancer, 13.72% had a hematologic malignancy (lymphoma or multiple myeloma), 7.84% of patients had lung cancer and 5.88% had colon cancer. Bladder, kidney and larynx cancers were reported in 1.96% of cases each. Zhang et al. [19] used pathological examination to identify the primary tumor in patients with SM. The first three primary tumor sites were as follows: breast (26.6% of cases), lung (21.7% of cases), and prostate (19.2% of all cases), but they also found lymphoma, multiple myeloma, and kidney as less common locations.
A survey conducted in the United States on SM annually diagnosed identified that 16.3% had lung cancer as their starting point, 14% were derived from breast cancer, 13.1% from renal cancer, 6.8% from prostate cancer, 4.1% from cutaneous melanoma, and 2.3% from primary thyroid cancer [20].
Correlated with the fact that they studied both adult and child patients, but also with the fact that the analysis was performed on patients diagnosed with spinal metastases based either on clinical symptoms, radiographic examinations and/or histopathological diagnosis, and that hematologic malignancies (myeloma and lymphoma) were also included, the study realized by Wang et al. [11] reported similar, but also different data from the above studies. The most common primary tumor causing SM was lung cancer (36.54%), followed by unknown origin (16.22%), childhood cancer (6.52%), breast cancer (6.35%), liver/biliary cancer (6.27%), gastrointestinal cancer (4.43%), myeloma (4.43%), prostate cancer (4.43%), thyroid cancer (3.09%), sarcoma (2.76%), and less common primary neoplasia (8.95%), such as esophageal cancer, lymphoma, and cervical cancer.
In 2021, an author from Turkey [21] investigated 156 patients with SM and found that among the primary tumors that spread to the spine, respiratory system cancer was the first (47.44%), breast cancer was the second (21.15%), and both were followed by prostate cancer (11.54%), gastrointestinal tract cancer (10.26%), urinary tract (6.41%) and gynecological cancer (3.21%).
Although in the present series the same locations of the primary tumors leading to the onset of SM appear as in other studies, their order differs. Thus, in the present study, lung cancer was the most common primary tumor that determined SM, being identified in 47.82% of non-hematological tumor cases and representing 3 times more cases than the second primary tumor, respectively gastrointestinal cancers.
Similar aspects were identified by another study carried out in Romania by Bratu et al. [22]. These Romanian researchers retrospectively analyzed, from imaging and pathological points of view, 309 cases of SM diagnosed at a hospital in Bucharest between 2010 and 2014. In 44.33% of cases the patients presented SM from a hematological neoplasia, and 55.66% from another type of cancer. Those 171 patients with SM of non-hematological origin presented the following primary tumor: lung cancer (44.44%), breast cancer (25.14%), prostate cancer (8.18%), kidney cancer (4.09%), thyroid cancer (4.09%), gastrointestinal tract cancer (3.50%), bladder cancer (2.92%), malignant melanoma (2.92%), pancreatic cancer (2.33%), ovarian cancer (1.75%), and neck squamous cell cancer (1.16%).
In the present series, we identified the highest prevalence of lung cancers as a starting point for SM, probably because, as reported by other authors [3], lung cancer not only is the most frequent, but also presents a high risk of dissemination to vertebrae. Also, patients with non–small cell lung cancer mostly disseminate to the spinal column as this site is the most common site for bone metastasis [23].
Even though there are studies in the literature stating that patients with gastrointestinal cancer have the lowest risk of spinal dissemination [3], in the present series SM with a gastrointestinal cancer as a starting point, especially colorectal cancer, ranks second. As far as we know, this aspect has not been identified by another study. The cause may be the fact that such patients do not undergo imaging of the spine to detect SM unless clinical signs appear [24]. Also, in an earlier personal study [13], we also reported the epidemiological and pathological findings of 40 patients with gastrointestinal cancers and SM diagnosed and treated during a period of 9 years in the same hospital, among which the colorectal adenocarcinoma was the most frequent histological type (40%). These data demonstrate that the prevalence of gastrointestinal carcinomas have increased significantly in Romania in the last two decades. These data are confirmed by a recently published article [25], which studied all colorectal cancer cases reported by all hospitals to the National DRG System, during a period of 3 years (2016-2018). The authors identified a colorectal cancer mortality almost twice higher than the European average, which also means an increase in the corresponding incidence of colorectal cancer in Romania compared to the other European countries.
Although some authors found out that 21.15%–42.3% of SM originate from breast cancer [21,26], placing this primary tumor in the first or second place among all primary tumors that cause spinal dissemination, in our series breast cancer ranks third. In addition, in the case of prostate cancer, the present study identified SM with this starting point in fourth place, although this type of malignancy is the most common form of cancer affecting men. It is well known that this type of neoplasia presents a particular tropism for bone metastasis. In 2007, approximately 350,000 patients were diagnosed with bone metastases in the United States [27]. On the other hand, an autopsy study demonstrated that approximately 90% of men with metastatic prostate cancer also had bone metastases at the time of death [28]. Furthermore, more than 80% of therapeutically castrated prostate cancer patients experienced SM [29].
In the present series, new entities of malignant tumors that disseminated at the vertebral level, such as germ cell tumor, also appeared, but in a very small percentage. Some other studies have also shown the rarity of this medical condition. Jamal-Hanjani et al. [30] analyzed 2550 patients with germ cells tumors among which they found only 0.74% of cases with bone metastases, most of them (88.23%) at the vertebral level.
The data obtained in the present research are also confirmed regarding the prevalence of SM originating from a cutaneous melanoma. If in the present study this type of cancer was identified as the starting point of SM in only 1.73% of cases, the literature reports similar data (1.63%-4.1% of cases) [5,20], thus demonstrating that patients with cutaneous melanoma rarely disseminate to the vertebrae. As such, it can be concluded that this type of dissemination appears as a late event in the evolution of a melanoma [31].
All these data demonstrate that there is a great variation between studies regarding the starting point of SM, probably due to the pattern of development of primary tumors in a given population as a result of specific genetics and as a result of the temporal trends followed by each tumor type. For Romania, the fact that lung cancer ranks first among the primary tumors that cause SM demonstrates the significant increase in the incidence of this type of cancer in the last 25 years, both in women and in men. Also, the prevalence and long-term survival of gastrointestinal cancer, especially colorectal type, have increased significantly in recent years. Thus, although in previous studies it was considered that this type of cancer rarely causes SM, currently we found a representative number of cases.
Regarding the histological subtypes of lung cancers that caused SM, in the present series there were mostly squamous cell lung carcinomas and lung adenocarcinomas, the former being slightly more frequent. These aspects support previously published data regarding the histopathological types of lung cancer in Romania. Compared to other studies, from Asia or Latin America, which reported that lung adenocarcinoma was the primary origin of SM in 58.3%–69.6% of cases, and squamous cell carcinoma was associated with a much lower risk of bone metastasis, being identified only in 13%-17% of cases [32,33], statistical analyzes in Romania show that 48% of lung cancer patients have squamous cell lung carcinoma, 29% have adenocarcinoma, 7% have large cell carcinoma and 16% have small cell lung cancers [34]. These statistical data are also confirmed by the present study, in which the histological subtype of lung cancer that metastasizes at spinal level most frequently was squamous cell carcinoma. Similar aspects were identified by a study from Turkey [35], where the histopathological exam of 168 SM revealed the same hierarchy of histological types of lung cancer: squamous cell carcinoma (48%), adenocarcinoma (31%), small cell carcinoma (15%), and large cell carcinoma (6%).
In our series, SM from thyroid cancer were most often of the follicular type, an aspect also identified in other studies. Enkaoua et al. [35] reported, in addition to the follicular type, other histological types of thyroid cancer that have disseminated to the spine, such as the papillary type and, more rarely, medullary carcinoma with amyloid in the stroma.
In the present series, SM from renal cancer exhibited only clear cell renal carcinoma histological type and the same histological aspect was identified by Enkaoua et al. [35].
From a prognostic point of view, a recent research identified that patients with SM from small cell lung cancer have a median overall survival of only 6.3 months, in contrast to those with non-small cell lung carcinoma, which have a survival of 8.9 months. Notably, within the non-small cell lung carcinoma subgroup, patients diagnosed with adenocarcinoma showed the most prolonged survival, with a survival of 25.3 months [36].
The time interval from the diagnosis of the primary tumor to the diagnosis of SM varies widely, depending on the histological type of the primary neoplasia. A study conducted in Korea [5] evaluated the time interval from primary tumor diagnosis to bone metastasis for various primary solid malignancies. They observed that lung cancer had the shortest mean time to bone metastasis (9.0 ± 15.2 months), followed by breast cancer (14.9 months) and prostate cancer (17.4 months). Conversely, in the case of colorectal cancer they identified the longest average time to bone metastasis (28.9 ± 25.5 months). Overall, the median time from primary cancer diagnosis to surgery for bone metastasis was 18.9 months.
Van den Brand et al. [37] also reported that patients with lung cancer had the shortest time interval (about 9.0 months), while those with carcinoma of the breast and prostate have a significantly longer interval of 14.9 and 17.4 months, respectively. A group of researchers from Brazil [38] found that the time interval between the diagnosis of the primary tumor and surgery for the treatment of SM was on average 9.6 months, with minimum and maximum values between 4 days and 3183 days (8.84 years), respectively.
In the present series, the mean time interval between the diagnosis of the primary tumor and surgery for SM for the entire group of patients was similar to that reported by Hong et al. [5] in Korea (20.06 months versus 18.9 months). However, given the fact that in the present series we identified new types of primary tumors as the starting point of SM, the obtained data differ from those published by other authors [5,37,38]. The longest interval of time between those two moments in the evolution of a neoplasia was in the case of liver cancer (38 months) and the shortest was for germ cell tumors (1 month).
As demonstrated by the present study, many of the patients with SM are elderly and have neurological deficits due to involvement of several vertebral regions, with spine instability. Quantification of vertebral involvement, neurologic status, general health, and primary tumor histology are important factors to consider for surgical planning and therapeutic targeting.
Spinal metastases can be treated by chemotherapy, radiotherapy, and surgical treatment. Patients with SM are difficult to treat surgically, because the metastases represent an advanced stage of the oncological disease and therefore the postoperative prognosis can be very poor [10]. Surgical treatment aims to improve quality of life by achieving pain control and improving neurological deficits [39].
Conventional surgery in SM is highly invasive and requires a long hospital stay to stabilize the spine and remove nerve compression caused by the tumor. The most commonly used is decompression or “detachment surgery”, in which the tumor is resected so as to achieve decompression of the spinal cord [39]. Preoperative embolization can also be used to reduce the risk of hemorrhage and improve outcomes with low complication rates [40].
For patients with solitary spinal metastasis without invasion of the vertebral canal and a good general status of health, with a long life expectancy because the primary tumor has a slow growth rate, curative surgical interventions, such as metastasectomy or en bloc resection of tumors [41] or en bloc spondylectomy/total vertebrectomy), must be taken into account. Vertebral resection should be followed by spinal reconstruction and appropriate instrumentation [42]. When the prognosis is poor, local control must be obtained in the medium term, intralesional excision methods such as piecemeal excision or „eggshell” curettage can be used. For patients with the poorest prognosis, i.e., in the advanced phase of metastatic disease, palliative surgery is recommended, such as spinal cord decompression with stabilization, or only supportive care [40].
Since 2005, in Japan, minimally invasive spine stabilization with percutaneous pedicle screw fixation of the spine is used for patients with SM and advanced metastatic disease, in order to reduce pain and allow the oncological patient to be able to carry out his daily activities related to personal care. At the same time, this treatment method of SM can prevent vertebral pathological fractures [43].
A multivariate analysis of the risk factors for poor prognosis of patients with SM surgically treated [44] found out that age ≥ 65 years at surgery, presence of extraspinal metastases and poor performance scores were associated with 180-day mortality. For these reasons, the authors considered that multidisciplinary discussions about the benefits and risks of surgery in patients with these risk factors are necessary.
5. Conclusions
The present study provides a detailed description of the epidemiological and pathological characteristics of spinal metastases, which could help orthopedic surgeons understand the clinical characteristics of spinal metastases and is of great importance in guiding scientific research.
Our findings have direct implications for the allocation of resources necessary for the care of these patients, but also for health policy. In the coming years, healthcare systems will face a growing population of elderly patients with spinal metastases, for whom direct healthcare costs will be high. Moreover, our data suggests the need for close surveillance of patients diagnosed with lung cancer and colorectal cancer because these malignancies most frequently develop spinal metastases. It is becoming clear that smoking prevention actions and screening programs for the detection and removal of precancerous colorectal lesions must be developed and expanded.
Author Contributions
Conceptualization, S.S., L.E., A.S., G.F.D. and V.S.; methodology, M.T.T., L.C.D.C. and C.I.S.; software, S.S. and A.M.D.; validation, A.K, V.P. and A.S.; formal analysis, V.S.; investigation, S.S, A.S., G.F.D, M.G.D. and A.M.D.; resources, M.T.T.; data curation, C.I.S.; writing—original draft preparation, S.S, A.S., G.F.D. and A.M.D.; writing—review and editing, L.E., A.S., M.G.D, V.P., A.K., C.I.S., L.C.D.C. and M.T.T.; visualization, L.E., A.S. and V.S.; supervision, A.S, A.K. and V.S.; project administration, S.S, A.S. and V.S.; funding acquisition, S.S, A.S. and V.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Romania’s National Recovery and Resilience Plan (PNRR), Pylon III, section I5. Establishment and operationalization of Competence Centers PNRR-III-C9-2022—I5, project “Creation, Operational and Development of the National Center of Competence in the field of Cancer”, acronym CNCC, code 14.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and institutional ethical approval was obtained from the Committee of Ethics of “Prof. Dr. N. Oblu” Emergency Clinical Hospital, Iași, Romania, with decision no: 8/05.06.2024.
Informed Consent Statement
Written informed consent was obtained from each patient at the time of hospitalization. “Prof. Dr. N. Oblu” Emergency Clinical Hospital, Iași, Romania has implemented, as standard procedure, the existence of a written informed consent for all hospitalized patients, where the patients can agree and opt-in, or can disagree and opt-out from participating in certain scientific and didactic activities. This section of consent covers mainly retrospective and observational studies, where all identifiable information is carefully anonymized.
Data Availability Statement
The data can be shared upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ziu, E.; Viswanathan, V.K.; Mesfin, F.B. Spinal Metastasis. In: StatPearls [Internet]. StatPearls Publishing: Treasure Island (FL), 2024.
- Cerqueira, B.P.; dos Santos do Nascimento Carvalho, M.; de Barros Pontes, F.G. Epidemiological Characterization of Patients with Spinal Tumors in Alagoas, Brazil. J. Bras. Neurocirur. 2023, 34, 291–296. [Google Scholar] [CrossRef]
- Shakil, H.; Malhotra, A.K.; Badhiwala, J.H.; Karthikeyan, V.; Essa, A.; He, Y.; Fehlings, M.G.; Sahgal, A.; Dea, N.; Kiss, A.; Witiw, C.D.; Redelmeier, D.A.; Wilson, JR. Contemporary trends in the incidence and timing of spinal metastases: A population-based study. Neuro-Oncol. Adv. 2024, 6, vdae051. [Google Scholar] [CrossRef]
- World Health Organization. Who Report on Cancer: Setting Priorities, Investing Wesely and Providing Care for All. Geneva: World Health Organization, 2020.
- Hong, S.; Youk, T.; Lee, S.J.; Kim, K.M.; Vajdic, C.M. Bone metastasis and skeletal-related events in patients with solid cancer: A Korean nationwide health insurance database study. PLoS One. 2020, 15, e0234927. [Google Scholar] [CrossRef]
- Cortez, P.R. Spinal metastasis: diagnosis, treatment and prognosis - Integrative review from 2012 to 2017. Coluna/Columna 2020, 19, 58–66. [Google Scholar] [CrossRef]
- Esperança-Martins, M.; Roque, D.; Barroso, T.; Abrunhosa-Branquinho, A.; Belo, D.; Simas, N.; Costa, L. Multidisciplinary Approach to Spinal Metastases and Metastatic Spinal Cord Compression—A New Integrative Flowchart for Patient Management. Cancers (Basel). 2023, 15, 1796. [Google Scholar] [CrossRef]
- Fomchenko, E.I.; Bayley, J.C.; Alvarez-Breckenridge, C.; Rhines, L.D.; Tatsui, C.E. Spinal Metastases and the Evolving Role of Molecular Targeted Therapy, Chemotherapy, and Immunotherapy. Neurospine 2022, 19, 978–993. [Google Scholar] [CrossRef]
- Truong, V.T.; Al-Shakfa, F.; Phan, P.; Newman, N.; Boubez, G.; Shedid, D.; Yuh, S.J.; Wang, Z. Does the Region of the Spine Involved with Metastatic Tumor Affect Outcomes of Surgical Treatments? World Neurosurg. 2021, 156, e139–e151. [Google Scholar] [CrossRef]
- Botelho, R.V.; de Oliveira, M.F.; Rotta, J.M. Quantification of Vertebral Involvement in Metastatic Spinal Disease. Open Orthop J. 2013, 7, 286–291. [Google Scholar] [CrossRef]
- Wang, F.; Zhang, H.; Yang, L.; Yang, X.; Zhang, H.; Li, J.; Qiao, R.; Hu, Y. Epidemiological Characteristics of 1196 Patients with Spinal Metastases: A Retrospective Study. Orthop. Surg. 2019, 11, 1048–1053. [Google Scholar] [CrossRef]
- Lu, C.; Gonzalez, R.G.; Jolesz, F.A; Wen, P.Y.; Talcott, J.A. Suspected spinal cord compression in cancer patients: a multidisciplinary risk assessment. J. Support. Oncol. 2005, 3, 305–312. [Google Scholar] [CrossRef]
- Selaru, S.; Sava, A.; Scripcariu, D.V.; Costea, C.F.; Dumitrescu, A.M.; Costăchescu, B.; Dumitrescu, G.F.; Ciupilan, C.; Vatavu, R.; Haba, R.M.; Poroch, V.; Dima-Cozma, L.C.; Vornicu, V.; Stan, C.I. Epidemiological and pathological characteristics of spinal metastases from gastrointestinal cancers – a series of 40 cases. Rom. J. Morphol. Embryol. 2023, 64, 225–234. [Google Scholar] [CrossRef]
- Marchi Candido, P.B.; Pinheiro, R.P.; Peria, F.M.; Nogueira Toledo, V.; Tavares Costa, H.R.; Aparecido Defino, H.L. Unknown primary tumor sites in spinal metastasis. Coluna/Columna 2021, 20, 64–67. [Google Scholar] [CrossRef]
- Enkaoua, E.A.; Doursounian, L.; Chatellier, G.; Mabesoone, F.; Aimard, T.; Saillant, G. Vertebral Metastases. A Critical Appreciation of the Preoperative Prognostic Tokuhashi Score in a Series of 71 Cases. Spine. 1997, 22, 2293–2298. [Google Scholar] [CrossRef]
- Helweg-Larsen, S.; Sorensen, P.S.; Kreiner, S. Prognostic factors in metastatic spinal cord compression: a prospective study using multivariate analysis of variables influencing survival and gait function in 153 patients. Int. J. Radiat. Oncol. Biol. Phys. 2000, 46, 1163–1169. [Google Scholar] [CrossRef]
- Husband, D.J.; Grant, K.A.; Romaniuk, C.S. MRI in the diagnosis and treatment of suspected malignant spinal cord compression. Br. J. Radiol. 2001, 74, 15–23. [Google Scholar] [CrossRef]
- Chaichana, K.L.; Pendleton, C.; Wolinsky, J.P.; Gokaslan, Z.L.; Sciubba, D.M. Vertebral compression fractures in patients presenting with metastatic epidural spinal cord compression. Neurosurg. 2009, 65, 267–274. [Google Scholar] [CrossRef]
- Zhang, Y.; Cai, F.; Liu, L.; Liu, X.D. Pathological Investigation of Vertebral Tumor Metastasis from Unknown Primaries - a Systematic Analysis. Asian Pac. J. Cancer Prev. 2015, 16, 1047–1049. [Google Scholar] [CrossRef]
- Wright, E.; Ricciardi, F.; Arts, M.; Buchowski, J.M.; Chung, C.K.; Coppes, M.; Crockard, A.; Depreitere, B.; Fehlings, M.; Kawahara, N.; Lee, C.S.; Leung, Y.; Martin-Benlloch, A.; Massicotte, E.; Mazel, C.; Oner, C.; Peul, W.; Quraishi, N.; Tokuhashi, Y.; Tomita, K.; Ulbricht, C.; Verlaan, J.J.; Wang, M.; Choi, D. Metastatic spine tumor epidemiology: comparison of trends in surgery across two decades and three continents. World Neurosurg. 2018, 114, e809–17. [Google Scholar] [CrossRef]
- Başdelioğlu, K. Features of Spinal Metastases: A Retrospective View. Int. J. Spine Surg. 2021, 15, 119–129. [Google Scholar] [CrossRef]
- Bratu, A.M.; Raica, V.P.; Sălcianu, I.A.; Zaharia, C.; Popa, V.B.; Lupu, A.R.; Ştefănescu, V.; Dobrea, C-M.; Iana, G.; Marinescu, A.N. MRI differential diagnosis: bone metastases versus bone lesions due to malignant hemopathies. Rom. J. Morphol. Embryol. 2017, 58, 1217–1228. [Google Scholar]
- Amelot, A.; Terrier, L.M.; Cristini, J.; Buffenoir, K.; Pascal-Moussellard, H.; Carpentier, A.; Bonaccorsi, R.; Le Nail, L.R.; Mathon, B. Spinal metastases from lung cancer: Survival depends only on genotype, neurological and personal status, scarcely of surgical resection. Surg. Oncol. 2020, 34, 51–56. [Google Scholar] [CrossRef]
- Portales, F.; Thézenas, S.; Samalin, E.; Assenat, E.; Mazard, T.; Ychou, M. Bone metastases in gastrointestinal cancer. Clin. Exp. Metastasis 2015, 32, 7–14. [Google Scholar] [CrossRef]
- Ionescu, E.M.; Tieranu, C.G.; Maftei, D.; Grivei, A.; Olteanu, A.O.; Arbanas, T.; Calu, V.; Musat, S.; Mihaescu-Pintia, C.; Cucu, I.C. Colorectal Cancer Trends of 2018 in Romania-an Important Geographical Variation Between Northern and Southern Lands and High Mortality Versus European Averages. J. Gastrointest. Cancer. 2021, 52, 222–228. [Google Scholar] [CrossRef]
- Zhoobasarova, D.; Sadykova, A.; Muratov, Z.; Abdraeva, F.; Aitieva, A.; Aitieva, Z.; Zheenbekova1, D.; Ismailova, F.; Tazhibaeva, U.; Kyzy, A.M.; Abdullaeva, Z.; Kochkorbaeva, Z.; Maksatbek, T.; Keneshbaev, B.; Kadyrberdieva, M.; Sherieva, N. Optimization Diagnosis of Breast Cancer Vertebral Metastases. Advances in Breast Cancer Research 2021, 10, 156–164. [Google Scholar] [CrossRef]
- Jemal, A.; Siegel, R.; Ward, E.; Murray, T.; Xu, J.; Thun, M.J. Cancer statistics, 2007. CA Cancer J. Clin. 2007, 57, 43–66. [Google Scholar] [CrossRef]
- Bubendorf, L.; Schöpfer, A.; Wagner, U.; Sauter, G.; Moch, H.; Willi, N.; Gasser, T.C.; Mihatsch, M.J. Metastatic patterns of prostate cancer: An autopsy study of 1,589 patients. Hum. Pathol. 2000, 31, 578–583. [Google Scholar] [CrossRef]
- Crnalic, S.; Lofvenberg, R.; Bergh, A.; Widmark, A.; Hildingsson, C. Predicting survival for surgery of metastatic spinal cord compression in prostate cancer: a new score. Spine (Phila Pa 1976) 2012, 37, 2168–2176. [Google Scholar] [CrossRef]
- Jamal-Hanjani, M.; Karpathakis, A.; Kwan, A.; Mazhar, D.; Ansell, W.; Shamash, J.; Harper, P.; Rudman, S.; Powles, T.; Chowdhury, S. Bone metastases in germ cell tumours: lessons learnt from a large retrospective study. BJU Int. 2013, 112, 176–181. [Google Scholar] [CrossRef]
- Zheng, D.X.; Soldozy, S.; Mulligan, K.M.; Levoska, M.A.; Cohn, E.F.; Finberg, A.; Alsaloum, P.; Cwalina, T.B.; Hanft, S.J.; Scott, J.F.; Rothermel, L.D.; Nambudirig, V.E. Epidemiology, management, and treatment outcomes of metastatic spinal melanoma. World Neurosurg. X. 2023, 18, 100–156. [Google Scholar] [CrossRef]
- dos Reis Oliveira, M.B.; Costa Souza, L.; Sampayo, E.J.G.; de Carvalho, G.S.; de Queiroz Mello, F.C.; Paschoal, M.E.M. The Impact of Lung Carcinoma Histology on the Frequency of Bone Metastases. Rev. Bras. Ortop. (Sao Paulo) 2019, 54, 524–530. [Google Scholar]
- Zhai, S.; Hu, P.; Liu, X.; Li, Z.; Wang, B.; Zhou, H.; Liu, Z.; Liu, X.; Li, Y.; Wei, F. Prognostic Analysis of Spinal Metastasis Secondary to Lung Cancer after Surgeries: A Unicentric, Large-Cohort, Retrospective Study. Orthop. Surg. 2022, 15, 70–78. [Google Scholar] [CrossRef]
- Ciuleanu, TE. Research and Standard of Care: Lung Cancer in Romania. Am. Soc. Clin. Oncol. Educ. Book. 2012, 437–41. [Google Scholar] [CrossRef]
- Aydinl, U.; Ozturk, C.; Bayram, S.; Sarihan, S.; Evrensel, T.; Yilmaz, H.S. Evaluation of lung cancer metastases to the spine. Acta Orthop. Belg. 2006, 72, 592–597. [Google Scholar]
- Groszman, L.; Hubermann, J.A.; Kooner, P.; Alamiri, N.; Bozzo, A.; Aoude, A. The Impact of Adjunct Medical Therapy on Survival after Spine Metastasis: A Systematic Review and Pooled Data Analysis. Cancers (Basel) 2024, 16, 1425. [Google Scholar] [CrossRef]
- Van den Brande, R.; Cornips, E.M.J.; Peeters, M.; Ost, P.; Billiet, C.; Van de Kelft, E. Epidemiology of spinal metastases, metastatic epidural spinal cord compression and pathologic vertebral compression fractures in patients with solid tumors: A systematic review. J. Bone Oncol. 2022, 35, 100446. [Google Scholar] [CrossRef]
- Valesin Filho, E.S.; Tardini, R.; de Abreu, L.C.; Vieira Motter, B.; Adami, F.; Miller Reis Rodrigues, L. Epidemiological study of 55 patients with symptomatic metastatic spinal disease in Santo André - SP, Brazil. Coluna/Columna 2013, 12, 32–35. [Google Scholar]
- Hong, S.H.; Chang, B.S.; Kim, H.; Kang, D.H.; Chang, S.Y. An Updated Review on the Treatment Strategy for Spinal Metastasis from the Spine Surgeon’s Perspective. Asian Spine J. 2022, 16, 799–811. [Google Scholar] [CrossRef]
- Di Perna, G.; Cofano, F.; Mantovani, C.; Badellino, S.; Marengo, N.; Ajello, M.; Comite, L.M.; Palmieri, G.; Tartara, F.; Zenga, F.; Ricardi, U.; Garbossa, D. Separation surgery for metastatic epidural spinal cord compression: a qualitative review. J Bone Oncol. 2020, 25, 100320. [Google Scholar] [CrossRef]
- Kato, S.; Demura, S.; Shinmura, K.; Yokogawa, N.; Shimizu, T.; Murakami, H.; Kawahara, N.; Tomita, K.; Tsuchiya, H. Surgical metastasectomy in the spine: a review article. Oncologist. 2021, 26, e1833–e1843. [Google Scholar] [CrossRef]
- Al Farii, H.; Aoude, A.; Al Shammasi, A.; Reynolds, J.; Weber, M. Surgical Management of the Metastatic Spine Disease: A Review of the Literature and Proposed Algorithm. Global Spine J. 2023, 13, 486–498. [Google Scholar] [CrossRef]
- Nakanishi, K.; Uchino, K.; Watanabe, S.; Misaki, K.; Iba, H. Effect of Minimally Invasive Spine Stabilization in Metastatic Spinal Tumors. Medicina 2022, 58, 358. [Google Scholar] [CrossRef]
- Knapp, B.; Govindan, A.; Patel, S.S.; Pepin, K.; Wu, N.; Devarakonda, S.; Buchowski, J.M. Outcomes in patients with spinal metastases managed with surgical intervention. Cancers (Basel). 2024, 16, 438. [Google Scholar] [CrossRef]
Figure 1.
Gender distribution of spinal metastases.
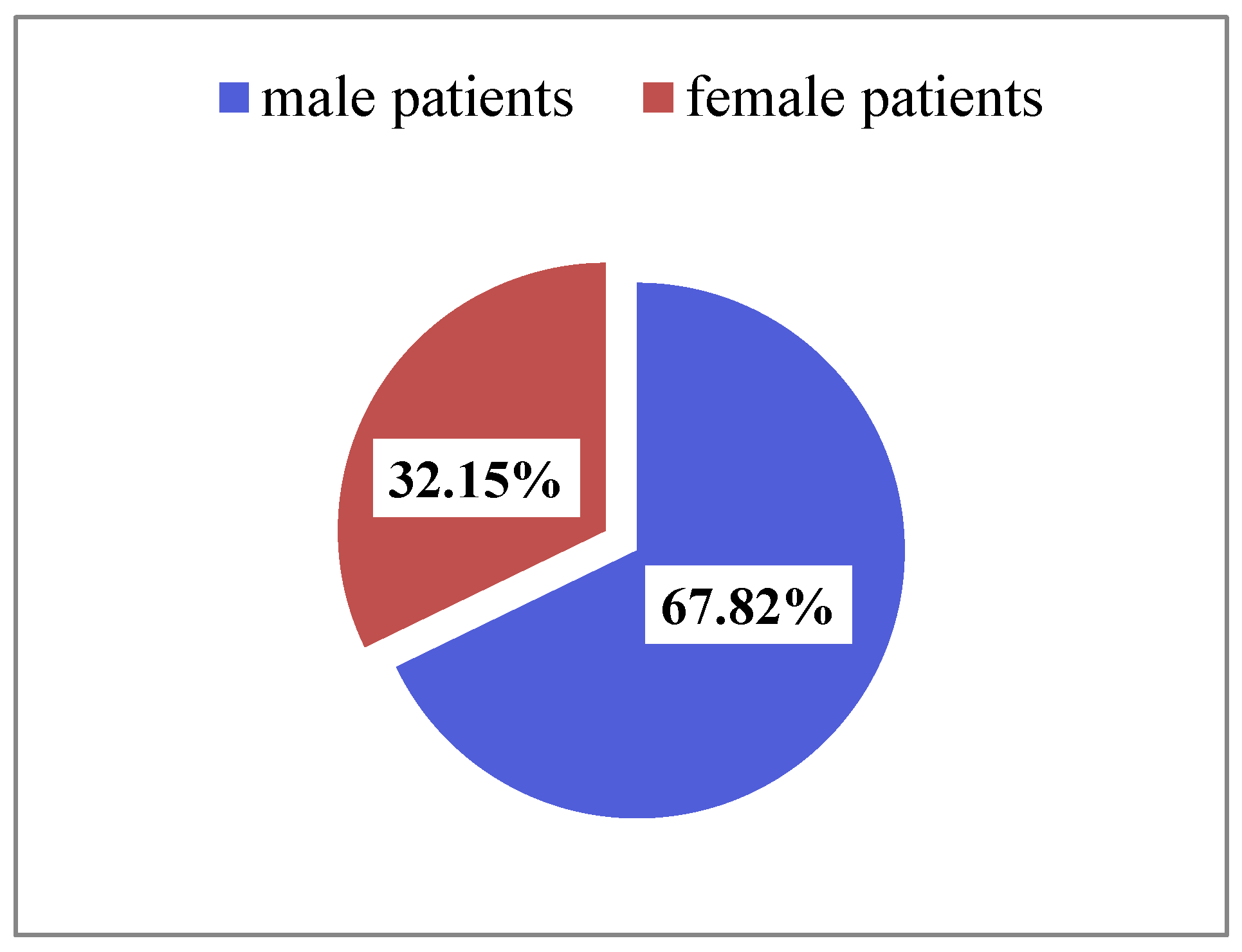
Figure 2.
Topography of spinal metastases.
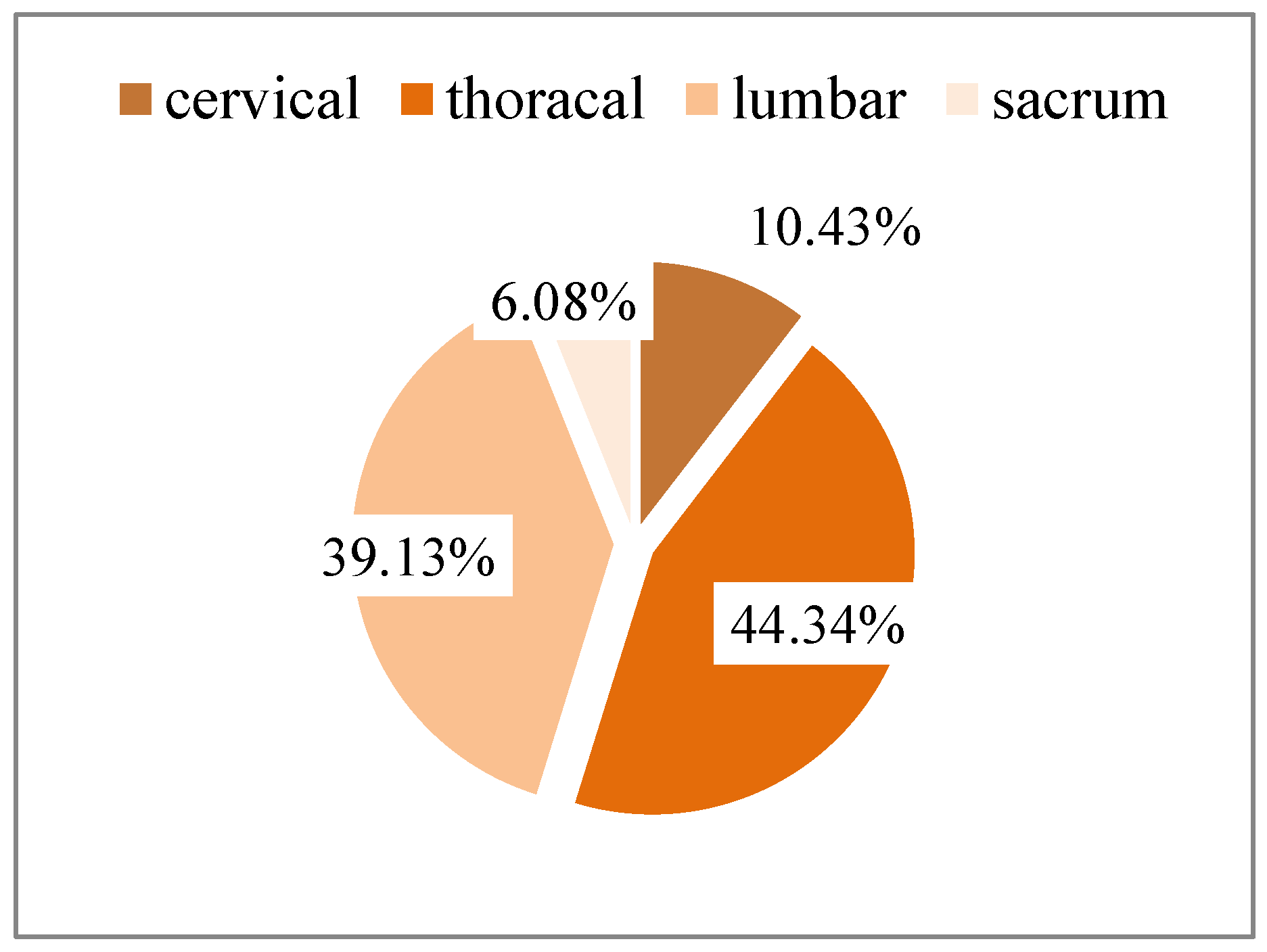
Figure 3.
Patients’ distribution according to number of spinal metastases.
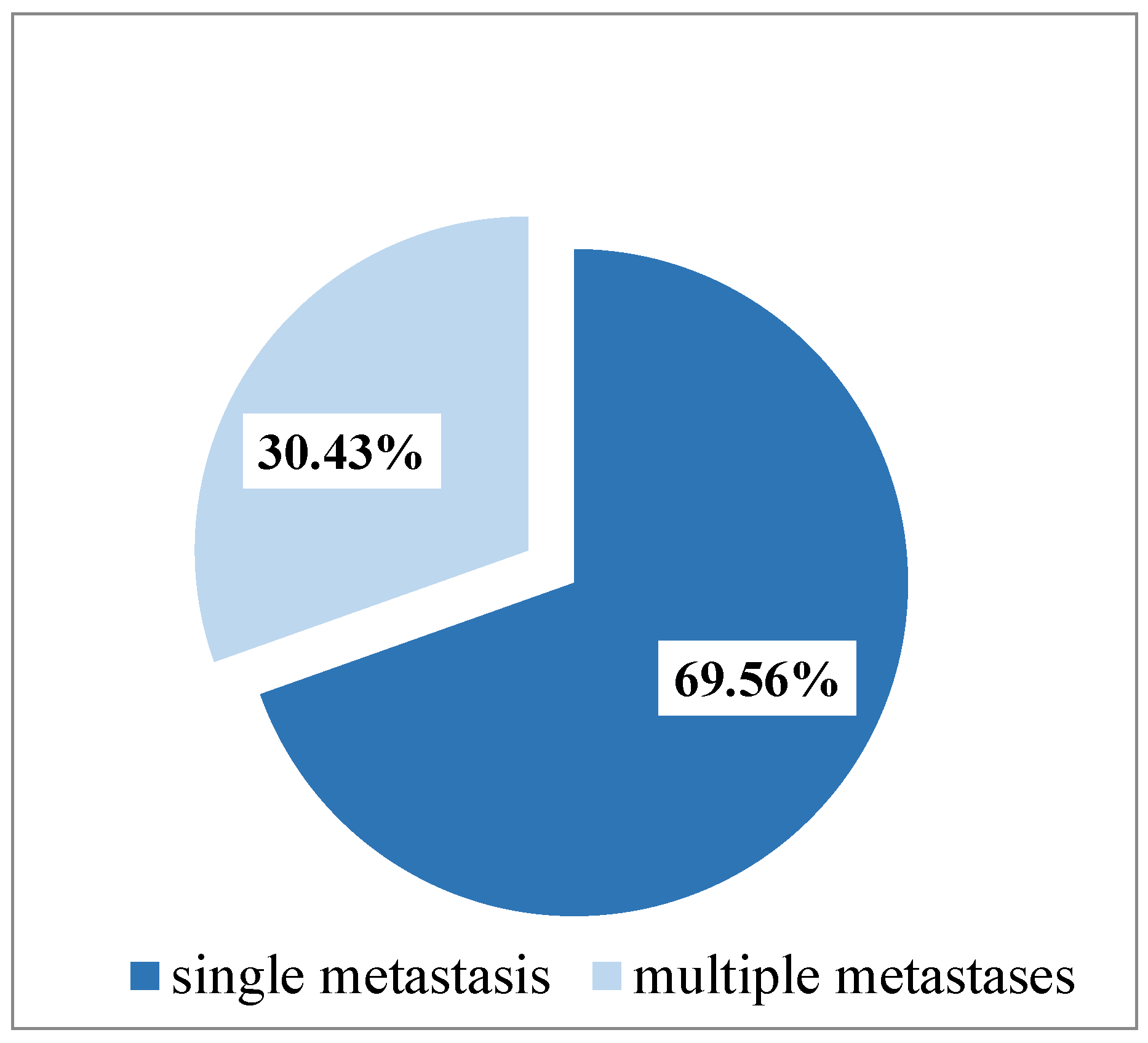
Figure 4.
Patients’ distribution according to known/unknown pathological diagnosis of primary tumor.
Figure 4.
Patients’ distribution according to known/unknown pathological diagnosis of primary tumor.
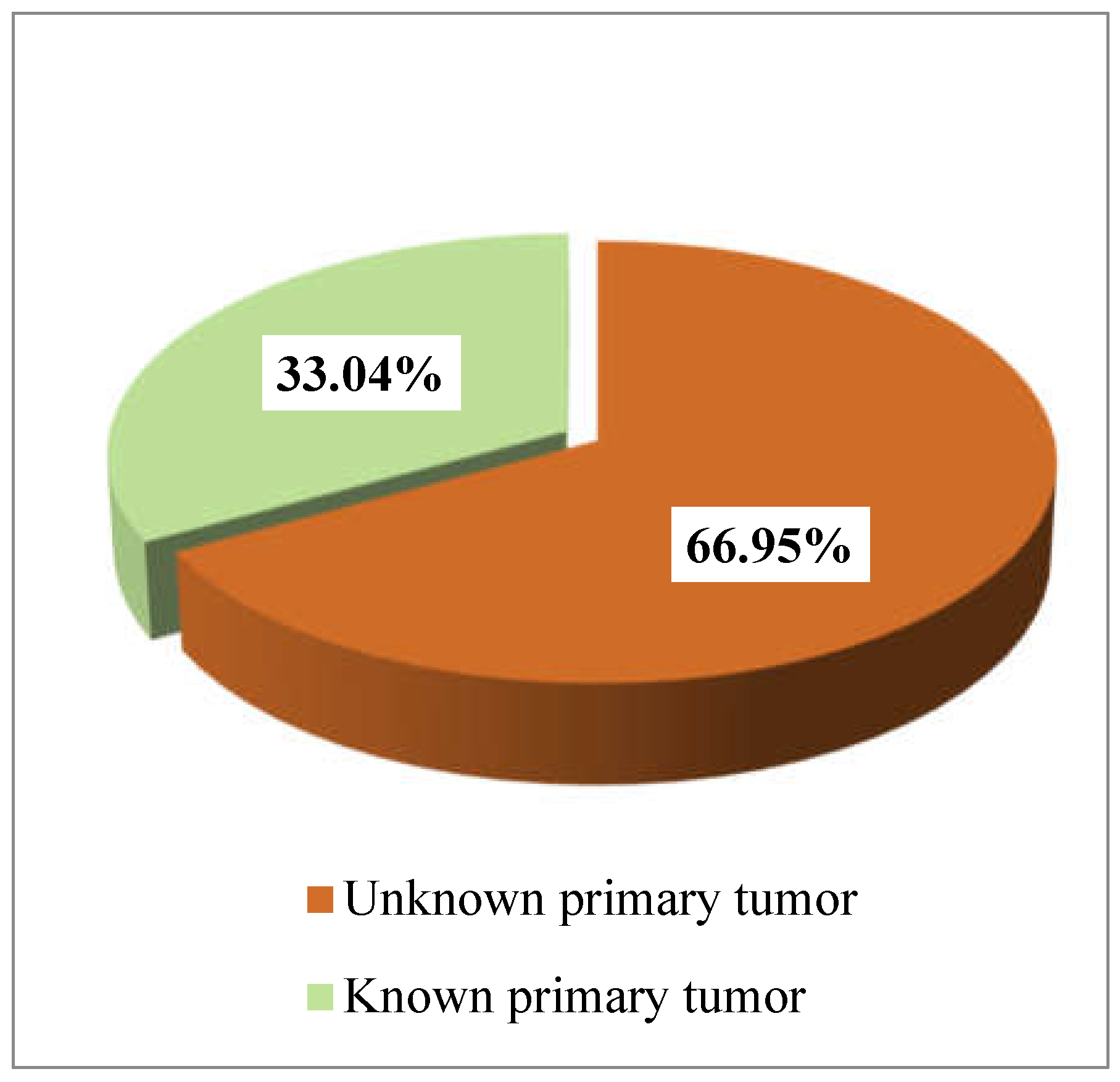
Figure 5.
Location of the primary tumor among the patients with a known histopathological diagnosis.
Figure 5.
Location of the primary tumor among the patients with a known histopathological diagnosis.
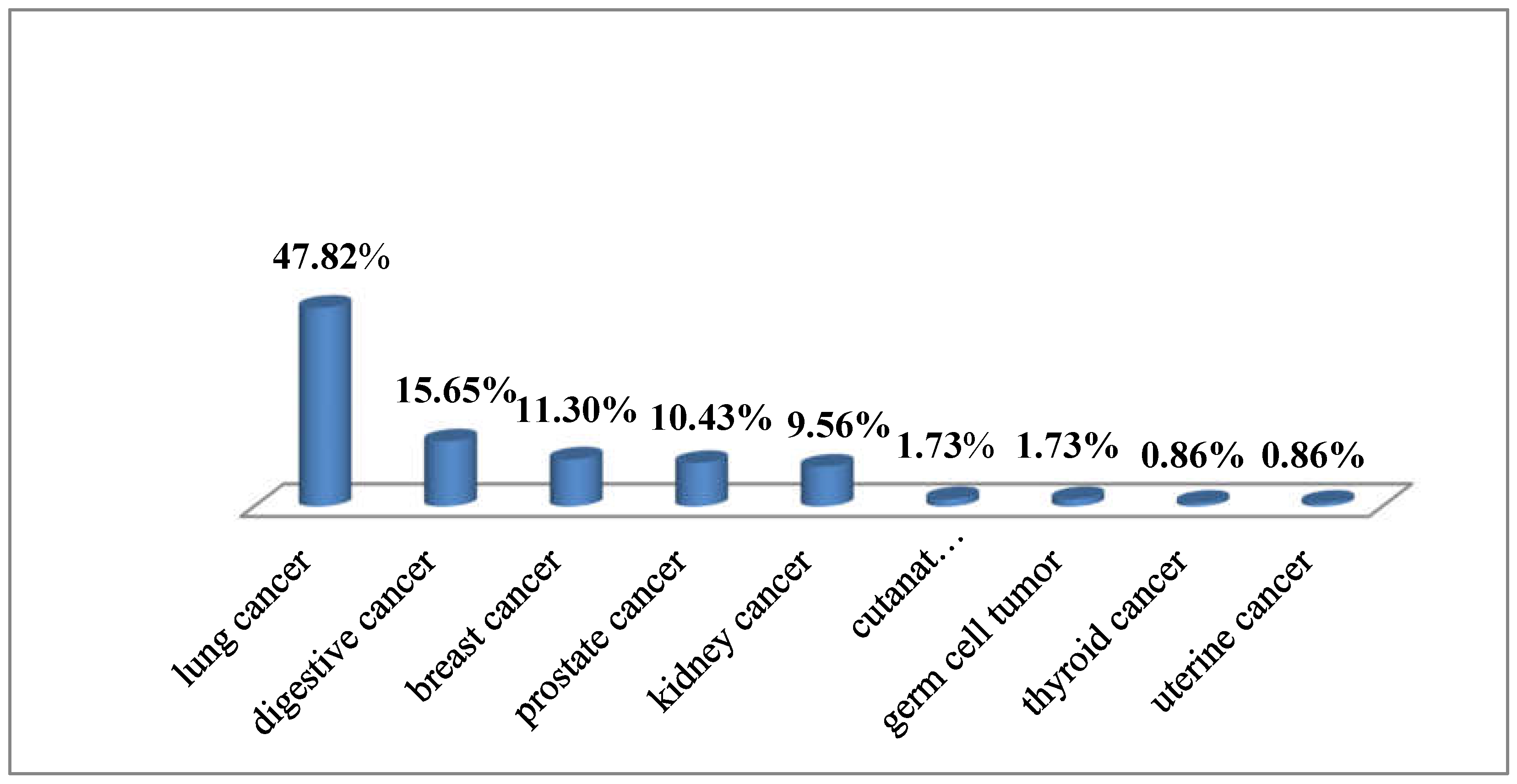
Figure 6.
Microscopic view of a spinal metastasis from a solid adenocarcinoma of the lung: (a) & (b) Tumor was made of solid small nests of poorly differentiated non-small cells, with abundant cytoplasm, well defined cell borders, vesicular nuclei, and prominent nucleoli; there were osteosclerotic changes of the vertebral bone (arrows) (Hematoxylin-Eosin, x20); (c) Tumor cells showed strong cytoplasmic positivity for CK AE1/AE3 (anti-Cytokeratin AE1/AE3 antibody, x10); (d) Tumor cells showed strong cytoplasmic positivity for CK7 (anti-Cytokeratin7 antibody, x10); (e) Tumor cells showed strong nuclear TTF-1 immunoreactivity (anti-TTF1 antibody, x10); (f) There were numerous reticulin fibers around small islands of tumor cells (silver impregnation, x20).
Figure 6.
Microscopic view of a spinal metastasis from a solid adenocarcinoma of the lung: (a) & (b) Tumor was made of solid small nests of poorly differentiated non-small cells, with abundant cytoplasm, well defined cell borders, vesicular nuclei, and prominent nucleoli; there were osteosclerotic changes of the vertebral bone (arrows) (Hematoxylin-Eosin, x20); (c) Tumor cells showed strong cytoplasmic positivity for CK AE1/AE3 (anti-Cytokeratin AE1/AE3 antibody, x10); (d) Tumor cells showed strong cytoplasmic positivity for CK7 (anti-Cytokeratin7 antibody, x10); (e) Tumor cells showed strong nuclear TTF-1 immunoreactivity (anti-TTF1 antibody, x10); (f) There were numerous reticulin fibers around small islands of tumor cells (silver impregnation, x20).

Figure 7.
Microscopic view of a spinal metastasis from a moderately adenocarcinoma of the right colon: (a) At the edge of the vertebral tumor there were small areas of carcinoma made of moderately differentiated gland with marked desmoplasia, osteolytic changes of the vertebral bone in the upper right corner (arrow) (HE, x10); (b) In the center of the tumor there were sheets of cells with a cribriform pattern; small gland lumen were filled with necrotic debris (dirty necrosis) (arrow) (HE, x20); (c) Tumor cells exhibited strong cytoplasmic positivity for Cytokeratin AE1/AE3 (anti-CK AE1/AE3 antibody, x40); (d) Tumor cells exhibited strong cytoplasmic positivity for Cytokeratin 20 (anti-CK20 antibody,x10); (e) Tumor cells exhibited strong nuclear positivity for p53 (anti-p53 antibody, x40); (f) Tumor cells exhibited a very high Ki67 Labeling Index demonstrating an aggressive evolution (anti-Ki67 antibody, x40).
Figure 7.
Microscopic view of a spinal metastasis from a moderately adenocarcinoma of the right colon: (a) At the edge of the vertebral tumor there were small areas of carcinoma made of moderately differentiated gland with marked desmoplasia, osteolytic changes of the vertebral bone in the upper right corner (arrow) (HE, x10); (b) In the center of the tumor there were sheets of cells with a cribriform pattern; small gland lumen were filled with necrotic debris (dirty necrosis) (arrow) (HE, x20); (c) Tumor cells exhibited strong cytoplasmic positivity for Cytokeratin AE1/AE3 (anti-CK AE1/AE3 antibody, x40); (d) Tumor cells exhibited strong cytoplasmic positivity for Cytokeratin 20 (anti-CK20 antibody,x10); (e) Tumor cells exhibited strong nuclear positivity for p53 (anti-p53 antibody, x40); (f) Tumor cells exhibited a very high Ki67 Labeling Index demonstrating an aggressive evolution (anti-Ki67 antibody, x40).
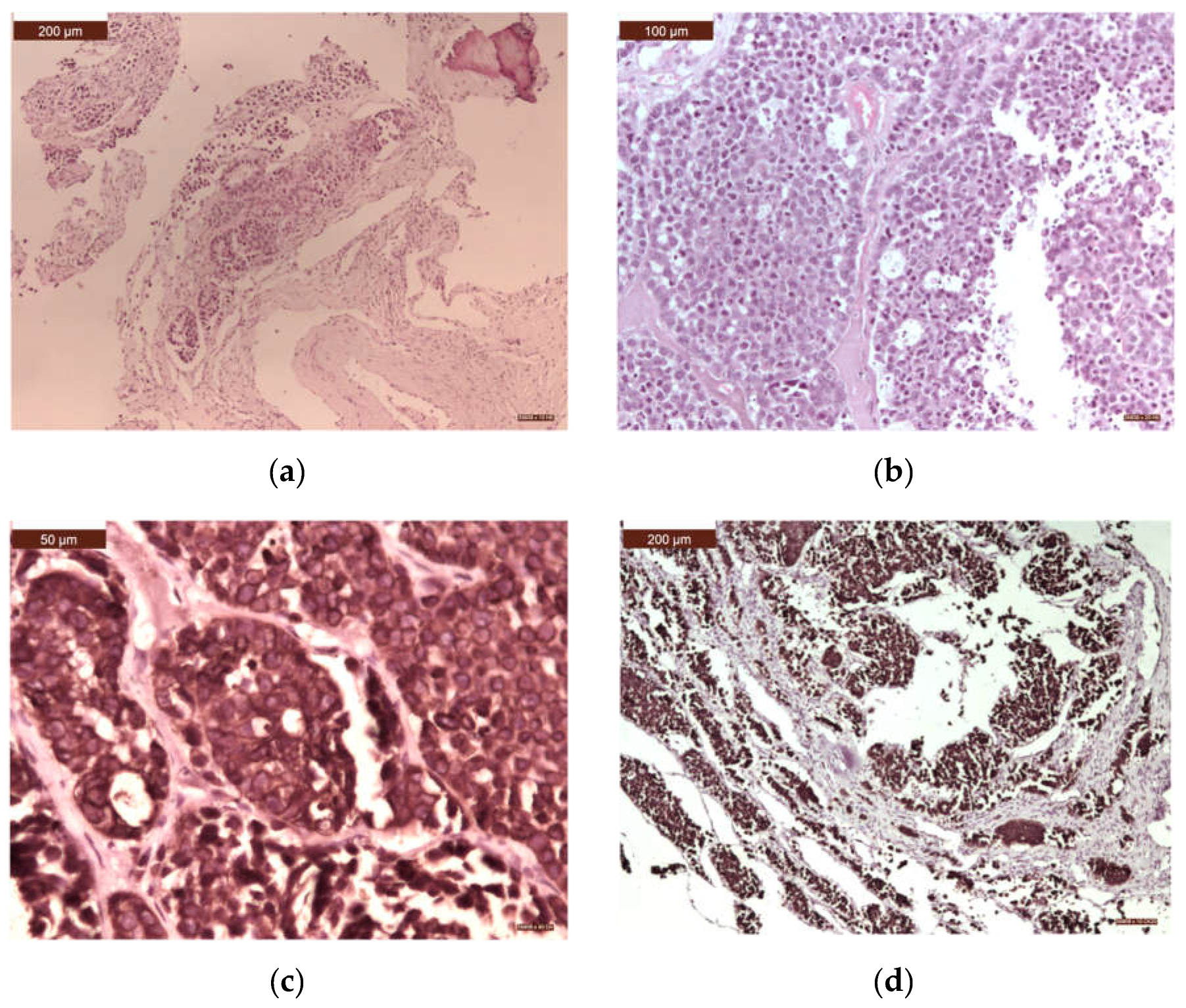
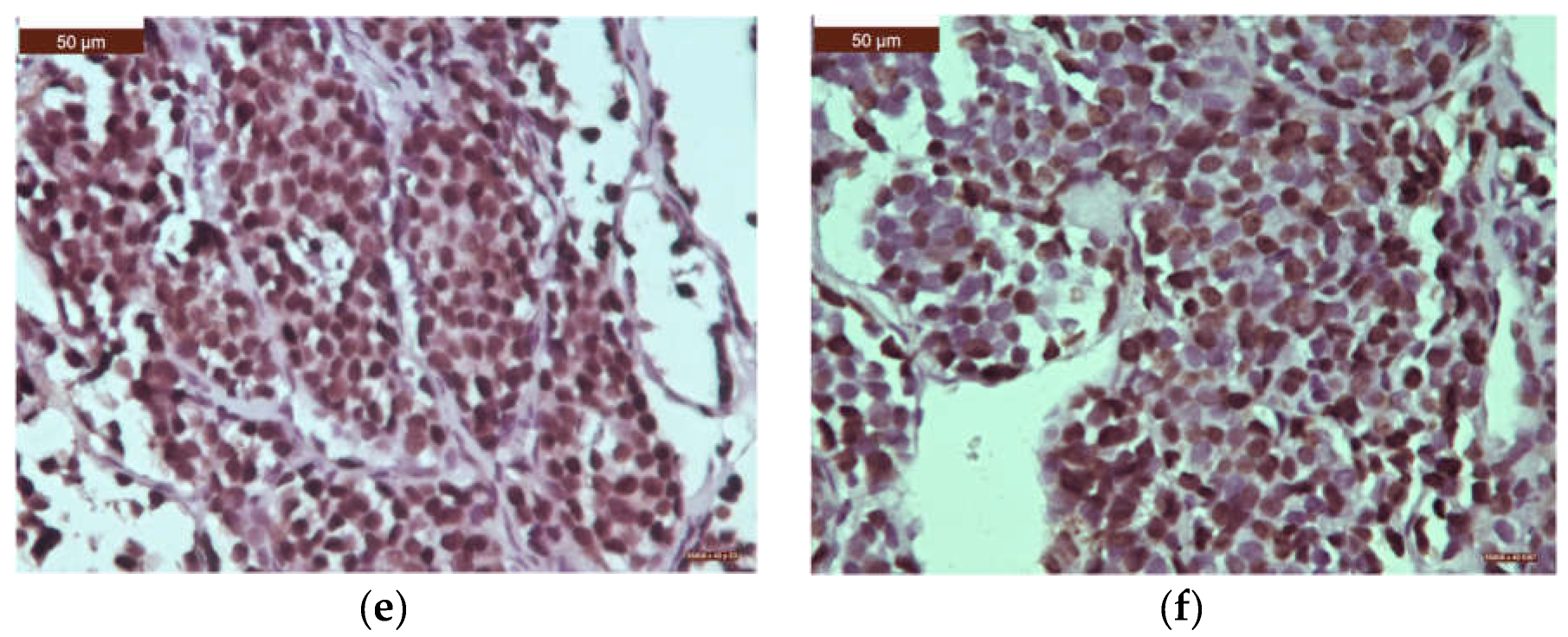
Figure 8.
Microscopic view of a spinal metastasis from an adenocarcinoma of the breast: (a) Mostly infiltrative large and solid nests of cells with tubule formation in 30% to 40% of the tumor. Tumor cells showed moderately enlarged nuclei. There is an osteoid matrix with new osteoid production, which was partially mineralization, due to osteolytic metastasis (arrow) (Hematoxylin-Eosin, x10); (b) Tumor cell exhibited strong nuclear positivity for GATA3 (anti-GATA3 antibody, x10); (c) Tumor cell exhibited strong cytoplasmic positivity for CK7 (anti-CK7 antibody, x20); (d) Tumor cell exhibited strong cytoplasmic positivity for CK19 (anti-CK19 antibody, x20); (e) Tumor cell exhibited strong nuclear positivity for Progesteron Receptor (anti-Progesteron Receptor antibody,x20); (f) Tumor cell exhibited strong nuclear positivity for Estrogen Receptor (anti- Estrogen Receptor antibody, x20).
Figure 8.
Microscopic view of a spinal metastasis from an adenocarcinoma of the breast: (a) Mostly infiltrative large and solid nests of cells with tubule formation in 30% to 40% of the tumor. Tumor cells showed moderately enlarged nuclei. There is an osteoid matrix with new osteoid production, which was partially mineralization, due to osteolytic metastasis (arrow) (Hematoxylin-Eosin, x10); (b) Tumor cell exhibited strong nuclear positivity for GATA3 (anti-GATA3 antibody, x10); (c) Tumor cell exhibited strong cytoplasmic positivity for CK7 (anti-CK7 antibody, x20); (d) Tumor cell exhibited strong cytoplasmic positivity for CK19 (anti-CK19 antibody, x20); (e) Tumor cell exhibited strong nuclear positivity for Progesteron Receptor (anti-Progesteron Receptor antibody,x20); (f) Tumor cell exhibited strong nuclear positivity for Estrogen Receptor (anti- Estrogen Receptor antibody, x20).
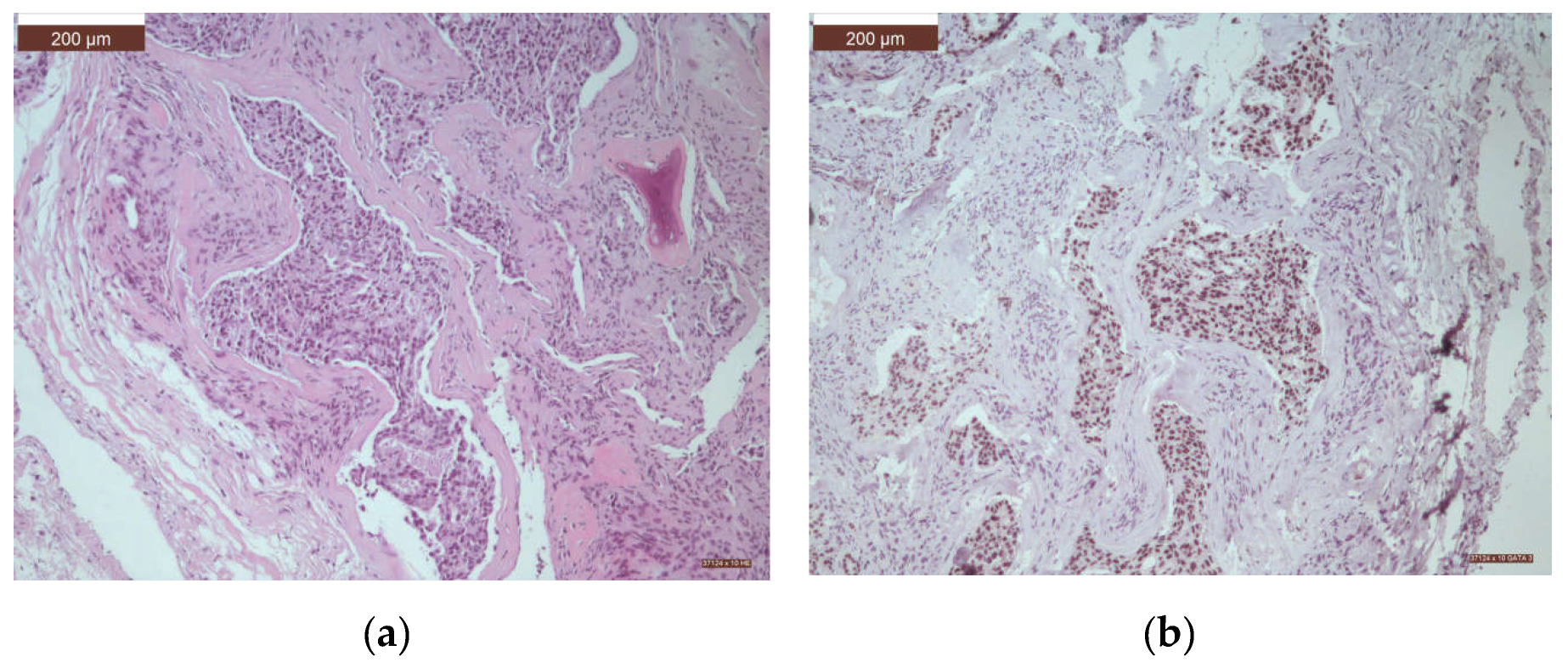
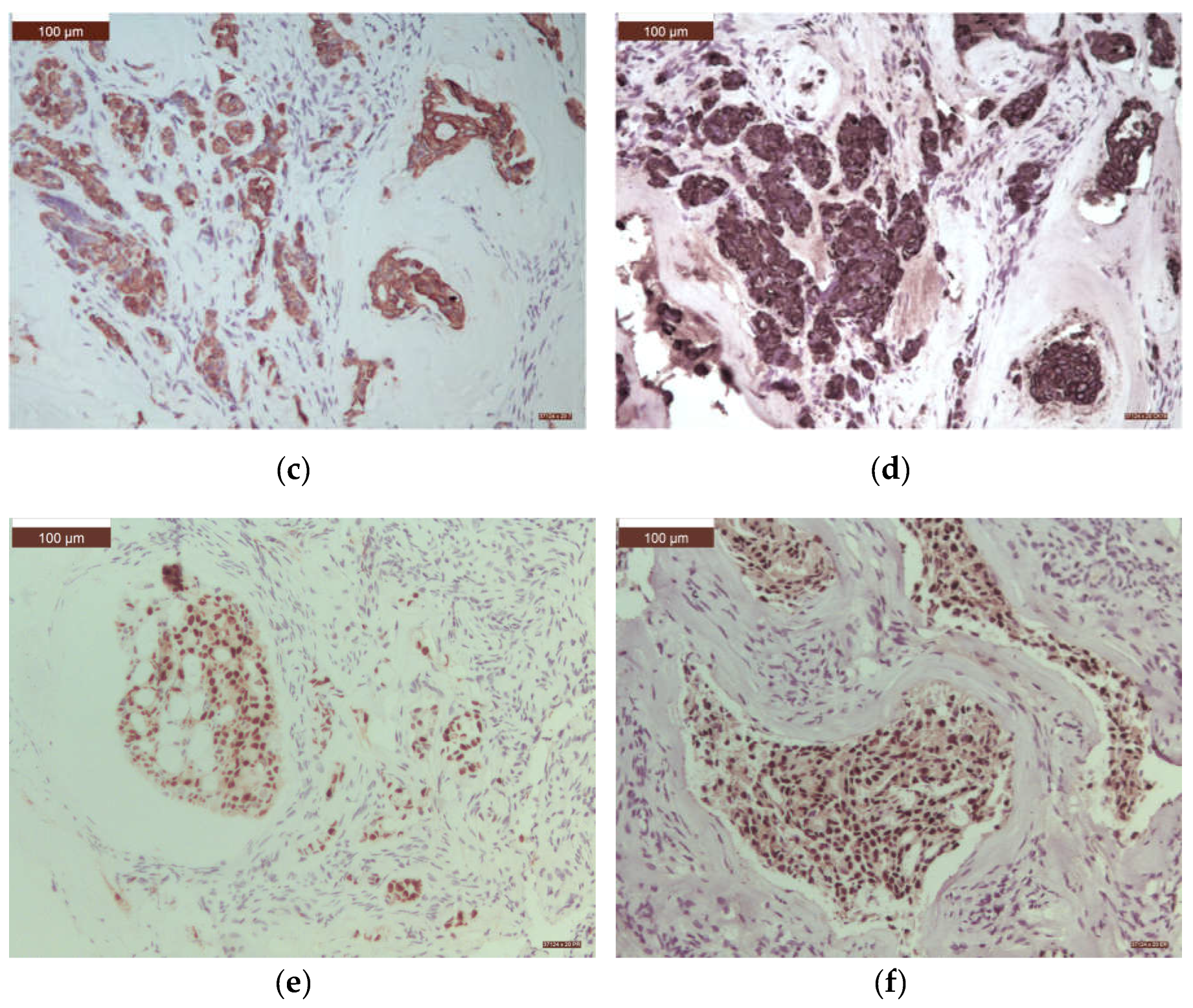
Figure 9.
Microscopic view of a spinal metastasis from an acinar adenocarcinoma of the prostate: (a) Metastatic tumor showed proliferation of small, compact, malignant glands without the basal layer and with an infiltrative pattern among osseous lamellae (arrow) (Hematoxylin-Eosin, x20); (b) With a higher objective it could be seen a complicated glandular proliferations made of tumor cells with amphophilic cytoplasm and round, monomorphic, nuclei with prominent nucleoli (Hematoxylin-Eosin, x40); (c) Metastatic tumor expressed luminal Prostate-Specific Antigen immunopositivity (anti-Prostate-Specific Antigen antibody, x40); (d) Tumor cell exhibited strong cytoplasmic positivity for CK8/18 (x20); (e) Tumor cell exhibited strong cytoplasmic positivity for CK19 (x40); (f) Tumor cells exhibited a very high Ki67 Labeling Index demonstrating an aggressive evolution (anti-Ki67 antibody, x20).
Figure 9.
Microscopic view of a spinal metastasis from an acinar adenocarcinoma of the prostate: (a) Metastatic tumor showed proliferation of small, compact, malignant glands without the basal layer and with an infiltrative pattern among osseous lamellae (arrow) (Hematoxylin-Eosin, x20); (b) With a higher objective it could be seen a complicated glandular proliferations made of tumor cells with amphophilic cytoplasm and round, monomorphic, nuclei with prominent nucleoli (Hematoxylin-Eosin, x40); (c) Metastatic tumor expressed luminal Prostate-Specific Antigen immunopositivity (anti-Prostate-Specific Antigen antibody, x40); (d) Tumor cell exhibited strong cytoplasmic positivity for CK8/18 (x20); (e) Tumor cell exhibited strong cytoplasmic positivity for CK19 (x40); (f) Tumor cells exhibited a very high Ki67 Labeling Index demonstrating an aggressive evolution (anti-Ki67 antibody, x20).
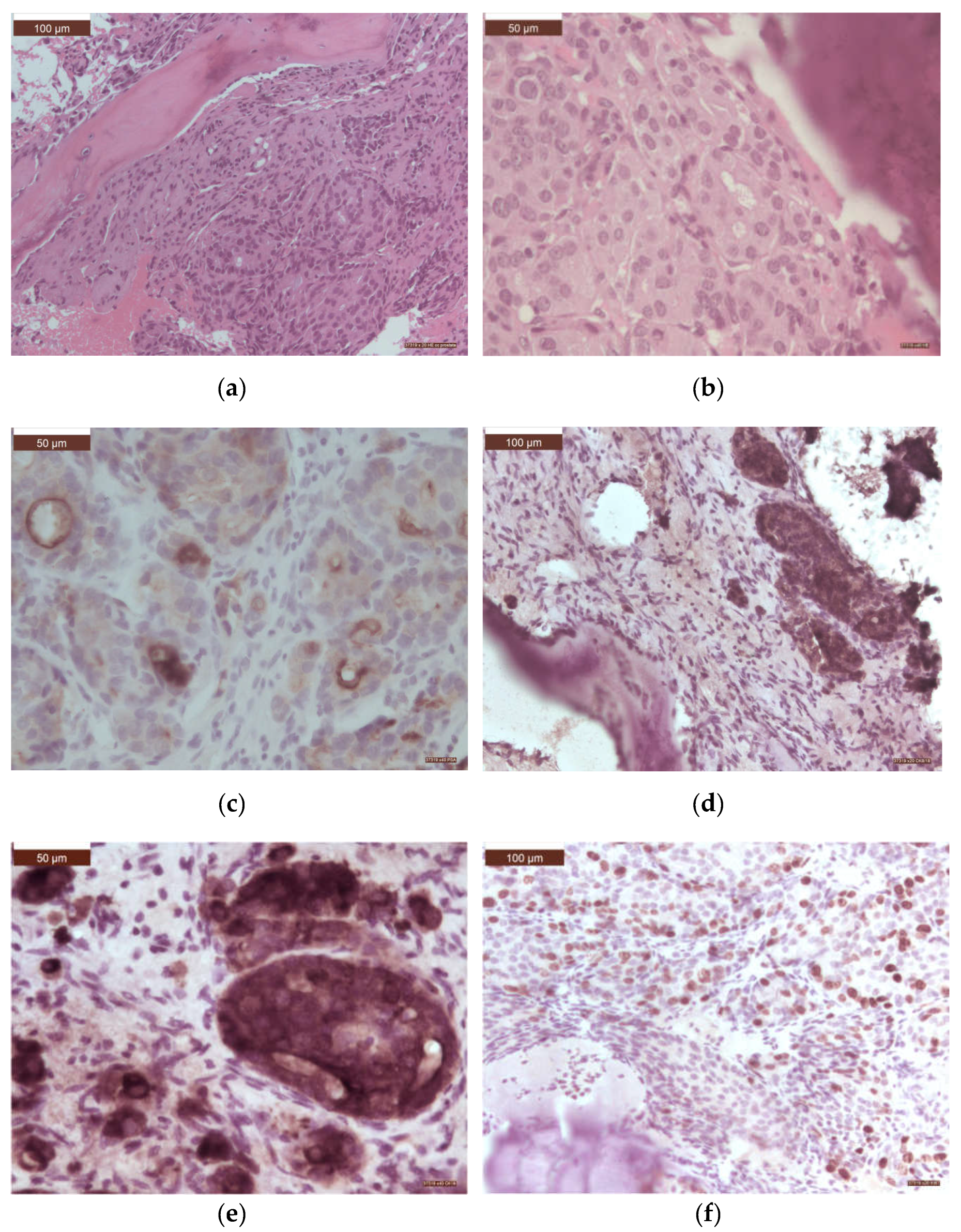

Table 1.
Histopathological types of spinal metastases starting from lung cancer.
| Histological type | n | % |
|---|---|---|
| Adenocarcinoma | 20 | 17.39 |
| solid | 9 | 7.82 |
| acinar | 7 | 6.08 |
| papillary | 3 | 2.60 |
| colloid | 1 | 0.86 |
| Squamous cell carcinoma (moderate/poor differentiated) |
22 | 19.13 |
| Neuroendocrine tumors | 11 | 9.56 |
| Small cell carcinoma | 8 | 6.95 |
| Large cell neuroendocrine carcinoma | 3 | 2.60 |
| Pleomorphic carcinoma | 1 | 0.86 |
| Adenosquamous carcinoma | 1 | 0.86 |
| Total | 55 | 47.82 |
Table 2.
Histopathological types of spinal metastases originating in gastrointestinal cancer.
| Location | Histological type | n | % |
|---|---|---|---|
| Mucosa of the oral cavity | Squamous carcinoma (moderate/poor differentiated) |
2 | 1.73 |
| Stomach | Signet-ring cell carcinoma | 1 | 0.86 |
| Colorectal | Adenocarcinoma (moderate/poor differentiated) | 10 | 8.69 |
| Liver | Trabecular hepatocellular carcinoma (moderate differentiated) | 4 | 3.47 |
| Biliary tree | Cholangiocarcinoma | 1 | 0.86 |
| Total | 18 | 15.65 |
Table 3.
Histopathological types of spinal metastases starting from breast cancer.
| Histological type | n | % |
|---|---|---|
| Infiltrating ductal carcinoma, NOS | 12 | 10.43 |
| Oncocytic carcinoma | 1 | 0.86 |
| Total | 13 | 11.30 |
Table 4.
Histopathological types of spinal metastases with other starting points.
| Location | Histological type | n | % |
|---|---|---|---|
| Prostate | Acinar adenocarcinoma | 12 | 10.43 |
| Kidney | Renal clear cell carcinoma | 11 | 9.56 |
| Skin cancer | Melanoma | 2 | 1.73 |
| Germ cell | Embryonar carcinoma | 1 | 0.86 |
| Seminoma | 1 | 0.86 | |
| Uterus | Endometrial endometrioid carcinoma | 1 | 0.86 |
| Thyroid | Follicular carcinoma | 1 | 0.86 |
| Total | 29 | 25.21 |
Table 5.
Time interval (months) between the initial diagnosis and the diagnosis of spinal metastasis according to the location of the primary tumor.
Table 5.
Time interval (months) between the initial diagnosis and the diagnosis of spinal metastasis according to the location of the primary tumor.
| Location of primary tumor | Time interval (months) |
|---|---|
| Lung | 17.1 |
| Gastrointestinal system | 19.56 |
| colon | 22.2 |
| liver/biliary tree | 38 |
| pancreas | unknown |
| the mucosa of the oral cavity | 8 |
| Breast | 23 |
| Prostate | 33 |
| Kidney | 20.75 |
| Cutaneous melanoma | 26 |
| Germ cell tumors | 1 |
| Thyroid | unknown |
| Uterus | unknown |
| Total | unknown |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



