
Submitted:
14 June 2024
Posted:
18 June 2024
You are already at the latest version
Abstract
The use of chimeric antigen receptor (CAR) in natural killer (NK) cells for cancer therapy is gaining momentum, marking a significant shift in cancer treatment. This review aims to explore the potential of CAR-NK cell therapy in cancer immunotherapy, providing a fresh perspective. It discusses the innovative approaches in CAR-NK cell design and engineering, particularly targeting refractory or recurrent cancers. By comparing CAR-NK cells with traditional therapies, the review highlights their unique ability to tackle tumor heterogeneity and immune system suppression. Additionally, it explains how novel cytokines and receptors can enhance CAR-NK cell efficacy, specificity, and functionality. The review underscores the advantages of CAR-NK cells, including reduced toxicity, lower cost, and broader accessibility compared to CAR-T cells, along with their potential in treating both blood cancers and solid tumors.
Keywords:
CAR-NK cell therapy
; Immunotherapy
; tumor heterogeneity
1. Introduction
The inception of chimeric antigen receptor (CAR) technology has revolutionized the landscape of cancer therapy. Originating from its development for T cells in the late 20th century, CAR therapy has demonstrated profound efficacy, particularly in treating hematologic malignancies [1]. CARs, engineered to augment T cell recognition and eradication of tumor cells, amalgamate external antigen recognition domains with internal signaling domains, thereby bestowing CAR-T cells with tumor-specific targeting capabilities [2]. However, despite the progress, the application of CAR-T therapy in treating solid tumors remains fraught with challenges, including severe side effects like cytokine release syndrome (CRS), targeting precision issues, and the emergence of drug resistance [3].
Natural killer (NK) cells, pivotal players in the innate immune response, exhibit cytotoxic activity against non-self-cells independently of the major histocompatibility complex (MHC) recognition, a limitation observed in T cells [4]. This distinct attribute, along with their unique cytokine profile, positions CAR-NK cell therapy as an innovative alternative, potentially circumventing the limitations of CAR-T therapy. The adaptation of CAR technology to NK cells has opened new avenues for cancer treatment, particularly in addressing the complexities of solid tumors, tumor heterogeneity, and immune escape mechanisms [5].
This review delves into the progression, advantages, and challenges of CAR-NK cell therapy, with a keen focus on its potential to overcome the hurdles in treating solid tumors. We will systematically evaluate the efficacy of CAR-NK cells in enhancing cancer treatment, their role in circumventing drug resistance, and their capacity to minimize toxic reactions. By providing a comprehensive overview of the state-of-the-art in CAR-NK therapy, this paper seeks to address the scientific queries and literature gaps within this field. Through a detailed analysis of the development, benefits, and obstacles associated with CAR-NK cell therapy, this review aims to chart the future course of this promising treatment modality. We aspire to offer a current perspective on CAR-NK cell therapy, elucidating its evolving role and prospects in the advancing frontier of cancer immunotherapy.
2. Overview of CAR-NK Cell Therapy
CAR-NK cell therapy represents a burgeoning area within cancer immunotherapy, entailing the genetic engineering of NK cells to express CARs. These receptors are meticulously designed to include an extracellular antigen-binding domain, commonly sourced from a monoclonal antibody, fused with an intracellular signaling domain. This domain typically features CD3ζ and may be augmented with one or more co-stimulatory molecules, such as CD28 or 4-1BB, to enhance the therapeutic efficacy and functionality of the CAR-NK cells [6]. The unique configuration of CAR-NK cells allows them to recognize and eliminate tumor cells that display the specific target antigen, bypassing the need for MHC recognition. Such capability represents a significant advantage, distinguishing CAR-NK cells from other immunotherapeutic approaches [7].
The flexibility of CAR-NK cell therapy is multifaceted, showcasing both the diversity in the cellular sources and the molecular intricacy of the CAR constructs themselves. Initially, this adaptability is evident in the variety of sources from which CAR-NK cells can be derived, including peripheral blood, umbilical cord blood, induced pluripotent stem cells (iPSCs), and NK cell lines [8,9]. Each source offers unique advantages in terms of availability, expansion potential, and compatibility with genetic modification. Building upon this foundational versatility, Table 1 highlights the specific molecular engineering of CAR constructs that further expands the therapeutic potential of CAR-NK cells. The table provides a curated list of some effective CARs that have been published, detailing their molecular combinations of extracellular and intracellular domains, alongside their respective target antigens. This precision in design allows for the creation of CAR-NK cells tailored to recognize and eliminate a wide array of cancer cell antigens with remarkable specificity. Among these, the NK-92 cell line stands out due to its high cytotoxic potential and ease of expansion in vitro. The NK-92 cells, once modified to express the CAR, become potent tools in targeting and destroying tumor cells [10]. A crucial aspect of CAR-NK cell therapy is its potential to be used as an "off-the-shelf" product, offering versatile and readily available treatment options. This characteristic is particularly beneficial in the clinical setting as it circumvents the need for patient-specific matching or lymphodepletion procedures [11]. It significantly simplifies the treatment process, potentially making it accessible to a broader patient population and reducing time and costs associated with therapy customization. Moreover, the manufacturing of CAR-NK cells involves a series of sophisticated steps to ensure their safety, efficacy, and consistency [4]. This includes the selection of the right target antigen, optimization of CAR design for maximum binding and activation, and fine-tuning the cultivation process to produce cells with high vitality and functional stability. In addition to their direct cytotoxicity, CAR-NK cells also exhibit an array of immunomodulatory functions [12]. They can recruit other immune cells to the tumor site, enhancing the overall anti-tumor response. This synergy between direct tumor cell killing and immune system activation is a key factor that could potentially increase the effectiveness of CAR-NK cell therapy in treating a wide range of cancers.
Furthermore, the field of CAR-NK cell therapy is rapidly evolving, particularly when compared to established CAR-T cell therapies. Researchers are keenly focused on addressing certain limitations that are more pronounced in the CAR-NK cell domain [13]. These include challenges such as the limited persistence of CAR-NK cells in vivo, a concern less prevalent in CAR-T cells due to their longer-lasting memory and proliferation capabilities. Additionally, potential off-target effects and the immunosuppressive nature of the tumor microenvironment are areas where CAR-NK cells, much like their CAR-T counterparts, require further refinement and innovation [3].

Table 1.
Specific CAR constructs and applications.
| 1st Author | Year | Cell Type | Generation | Intracellular Signaling Domains |
|---|---|---|---|---|
| P Kvacskay [14] | 2024 | CAR-T | First | CD3ζ |
| Y Wang [15] | 2024 | CAR-T | Second | CD28, 4-1BB with CD3ζ |
| Ritmeester-Loy [16] | 2024 | CAR-T | Third | CD28, 4-1BB, and CD3ζ |
| R Basar [13] | 2020 | CAR-NK | First | CD3ζ or NK cell activating domains (e.g., 2B4) |
| L Herrera [17]. | 2021 | CAR-NK | Second | DAP12, 2B4, CD3ζ, or NK cell-specific costimulatory molecules (e.g., CD137, NKG2D) |
| A Page [18]. | 2024 | CAR-NK | Third | Combinations of NK cell-specific signaling domains (e.g., DAP12, 2B4, NKG2D, CD137) |
Note. The extracellular domain is consistent, the scFv (single-chain variable fragment) sequence changes depending on the antigen, typically CD19. The most used hinge region was CD8α or IgG1, and transmembrane moieties are from CD3ζ, CD8 or CD28.
3. The Comparison of CAR-NK Cells to CAR-T Cells Therapies
CAR-NK and CAR-T therapies are powerful tools against cancers, originating primarily from research in hematological malignancies (blood cancers). However, there exist several similarities and differences between them. Below is a brief comparison of both therapies (Table 2).
3.1. Intracellular Signaling Domains
CAR-T cells are typically engineered to incorporate the CD3ζ domain along with co-stimulatory domains such as CD28 and 4-1BB [19]. The CD3ζ domain plays a pivotal role in signal transduction and is an essential component of the T cell receptor (TCR), linking antigen recognition to several intracellular signal-transduction pathways. The co-stimulatory domains, CD28 and 4-1BB, enhance the survival, proliferation, and effector functions of the CAR-T cells [20]. CD28 is known to drive high T-cell activation, which can potentially lead to exhaustion and shortened persistence. Conversely, 4-1BB enhances T cell proliferation and survival, and reduces T cell exhaustion [20].
CAR-NK cells, like CAR-T cells, can utilize NK-specific signaling domains like 2B4, DAP10, and DAP12 [21]. These NK-specific signaling domains contribute to the unique functional characteristics of CAR-NK cells. For instance, the 2B4 domain serves as a co-stimulatory domain, enhancing the cytotoxic activity of CAR-NK cells. DAP10, a major adaptor protein and the exclusive signaling intermediate of NKG2D in human NK cells, is known to enhance the cytotoxic ability of CAR-NK cells against certain tumor cells [22]. DAP12, an important adaptor molecule that is associated with multiple activating receptors, is also utilized in CAR-NK cells to improve their anti-tumor potential [22,23].
Thus, both CAR-T cells and CAR-NK cells play crucial roles in immunotherapy, they exhibit distinct differences in their intracellular signaling domains. These differences contribute to their unique functionalities in targeting and eliminating cancer cells. CAR-T cells commonly use CD28 and 4-1BB, while CAR-NK cells can utilize NK-specific signaling domains like 2B4, DAP10, DAP12 (Figure 1). These differences in intracellular signaling domains contribute to the unique functional characteristics of each cell type in cancer immunotherapy.
3.2. Cell Sources for Both CAR-T and CAR-NK Cells
CAR-T cells are typically sourced from patients themselves, a method known as autologous derivation. In this procedure, T cells are harvested from the patient, engineered to express a specific CAR, and then reintroduced into the patient [24]. This strategy has demonstrated significant success in treating hematological malignancies. Alternatively, CAR-T cells can be obtained from a donor with a compatible MHC, referred to as MHC-matched allogeneic derivation [25]. MHC comprises a group of cell surface proteins crucial for the adaptive immune system to recognize foreign entities. Ensuring MHC compatibility between the donor and the recipient is vital to avert graft-versus-host disease [25]. Allogeneic CAR-T cell therapy offers several potential benefits over the autologous approach, including the ready availability of cryopreserved batches for immediate treatment, the potential for standardizing CAR-T cell products, the opportunity for multiple genetic enhancements, the possibility of redosing or using a combination of CAR-T cells targeting different antigens, and reduced costs through an industrialized production process [24] (Figure 1).
On the other hand, CAR-NK Cells can be derived from a variety of sources. They can be autologous, like CAR-T cells, but they can also be derived from non-MHC matched allogeneic cell lines or NK cell lines [26]. NK cells do not require HLA matching, which provides more choices for possible donors and thus enhances the quality of the final product [27]. Their ability to act in an antigen-independent manner makes them a viable option for an “off-the-shelf” therapy that can be manufactured on a large scale and easily distributed to cancer patients [26]. Moreover, NK cells from allogeneic sources can also be used in immunotherapies owing to their reduced risk of alloreactivity [28]. This means that they are less likely to attack the patient’s own cells, reducing the risk of complications.
So, both CAR-T and CAR-NK cells have their unique sources and advantages; the choice between them would depend on various factors including the type of cancer, the patient’s condition, and the available resources. Both represent promising advances in the field of cancer immunotherapy.
3.3. CAR-T and CAR-NK Cells In Vitro Expansion
CAR-T cells are engineered by modifying T cells to express a CAR that targets cancer cells. The expansion of CAR-T cells in vitro is essential to obtain enough effector cells for therapeutic purposes [29]. This process typically involves the activation and proliferation of T cells under controlled laboratory conditions. Initially, T cells are activated using specific stimuli, such as anti-CD3 and anti-CD28 antibodies. Anti-CD3 antibodies bind to the CD3 complex on T cells, initiating their activation, while anti-CD28 antibodies provide a necessary costimulatory signal that enhances T cell proliferation and survival [30]. Following the activation, the culture is supplemented with cytokines, particularly interleukin-2 (IL-2), to support the growth and proliferation of T cells. IL-2 is a crucial growth factor for T cells, enhancing their proliferation and promoting the survival of activated cells [31]. This combined approach of activation and cytokine support enables the robust in vitro expansion of CAR-T cells, preparing them for therapeutic infusion into patients.
Like CAR-T cells, CAR-NK cells are engineered to target and eliminate cancer cells. However, NK cells represent a different lineage of lymphocytes with innate immune properties. The in vitro expansion of CAR-NK cells can be achieved using various methods, including feeder cell lines or a combination of cytokines like IL-2 and IL-15. IL-15 is particularly significant for NK cell growth, as it promotes the survival, proliferation, and activation of NK cells [32]. The feeder cells, often genetically modified to express certain ligands or to secrete growth factors, provide a nurturing environment for CAR-NK cell expansion [33]. These feeder cells can interact with NK cell receptors, delivering necessary signals that promote cell growth and functional maturation.
The in vitro expansion of CAR-T and CAR-NK cells is a crucial step in preparing these cells for therapeutic use in cancer immunotherapy. For in vitro expansion of both types of CAR cells, this process involves a combination of cell activation, growth factor supplementation, and sometimes the use of feeder cells, to produce many effector cells capable of targeting and destroying cancer cells. (Figure 2).
3.4. Pre-Expansion Prior to Transduction in CAR-T and CAR-NK Cells
Pre-expansion prior to transduction is a critical step in the production of both CAR-T and CAR-NK cells. This process involves the stimulation and expansion of T or NK cells before they are genetically modified to express the CAR. The goal of this step is to increase the number of cells available for transduction, which can enhance the efficiency of the transduction process.
For CAR-T cells, the pre-expansion process often involves the use of specific stimuli to activate the cells and promote their proliferation [34]. One study showed that functional CAR-T cells could be generated within 24 hours from T cells derived from peripheral blood without the need for T-cell activation or ex vivo expansion [34]. The efficiency of viral transduction in this process was substantially influenced by the formulation of the medium and the surface area-to-volume ratio of the culture vessel [34]. Another study described a 9-day protocol for CAR gene transduction and expansion of primary rhesus macaque peripheral blood mononuclear cells (PBMCs) [35]. The cells produced and expanded with this method showed high levels of viability, high levels of co-expression of two transduced genes, retention of the central memory phenotype, and enough for immunotherapeutic infusion [35].
For CAR-NK cells, the pre-expansion process is similar but has some unique aspects. One protocol described how to generate CAR-NK cells with transduction efficiencies greater than 15% from healthy donor ex vivo expanded NK cells using third-generation lentiviral vectors [36]. The protocol also showed how to assess CAR-NK cell anti-tumor function in vitro using a flow cytometry-based killing assay [36]. Another study developed a highly efficient method for site-specific gene insertion in NK cells using CRISPR (Cas9/RNP) and AAVs [37]. The CAR transduction was efficient, its expression remained stable after expansion, and it improved efficacy against AML targets [37].
The pre-expansion prior to transduction is a crucial step in the production of both CAR-T and CAR-NK cells. It involves the stimulation and expansion of T or NK cells before they are genetically modified to express the CAR, which helps increase the number of cells available for transduction and can enhance the efficiency of the transduction process.
3.5. Cell Killing Mechanism
CAR-T cells are engineered with CARs that specifically target and bind to antigens presented on the surface of tumor cells [38]. The external domain of these receptors, typically derived from the single-chain variable fragment (scFv) of an antibody, enables precise recognition of the antigens. Upon engaging with its target antigen, the CAR initiates a series of intracellular signals through domains such as CD3ζ and costimulatory domains like CD28 or 4-1BB [39]. This activation process propels the CAR-T cell into action, prompting it to proliferate, produce cytokines, and gear up for the targeted elimination of cancer cells. Once activated, CAR-T cells deploy cytotoxic molecules, including perforin and granzymes [40]. Perforin paves the way by forming pores in the membrane of the tumor cell, allowing granzymes to enter and induce apoptosis, ultimately leading to the destruction of the cancer cell.
In addition to their CAR-dependent capabilities, NK cells exhibit CAR-independent cytotoxicity, a crucial mechanism for targeting cancer cells. NK cells possess natural activating and inhibitory receptors that respond to stress signals and the absence of normal "self" markers on potential target cells [7]. The interplay of these signals determines the activation state of NK cells. Once activated, NK cells unleash cytotoxic granules, containing molecules like perforin and granzymes, which facilitate the direct killing of target cells, mirroring the cytotoxic approach of CAR-T cells [41]. This dual-action mechanism endows CAR-NK cells with a unique advantage, enabling them to effectively eradicate cancer cells, even those lacking the specific antigen recognized by the CAR [11]. This capability renders CAR-NK cells exceptionally effective and versatile in combating diverse tumor cell populations, enhancing their potential as a formidable tool in cancer immunotherapy [28].
The above data shows that CAR-T cells rely primarily on antigen-specific recognition for cytotoxicity, while CAR-NK cells can kill tumor cells through both CAR-dependent and independent mechanisms, offering a broader range of targets and potentially enhancing the effectiveness of cancer immunotherapy.
3.6. Cytokine Release Syndrome and Neurotoxicity
CRS and Neurotoxicity are notable side effects associated with CAR-T cell therapy, presenting significant clinical challenges. CRS is an acute systemic inflammatory response triggered by the massive release of cytokines from activated CAR-T cells [42]. This cytokine storm can lead to a spectrum of symptoms, from mild conditions like fever and fatigue to severe, potentially fatal issues such as hypotension, organ failure, and shock. Neurotoxicity, also recognized as immune effector cell-associated neurotoxicity syndrome (ICANS), manifests with neurological symptoms ranging from headache, confusion, and aphasia to more severe outcomes like seizures, cerebral edema, and coma [43].
On the other hand, the incidence and severity of these side effects are notably lower in CAR-NK cell therapies, which might be attributed to the inherent differences in the activation pathways and effector functions of NK cells compared to T cells [7]. Additionally, the engineering aspects of CAR constructs in NK cells, including the signaling domains and co-stimulatory molecules, might also contribute to the reduced toxicity profile [28].
3.7. CAR-T and CAR-NK Therapies in Hematological Malignancies and Solid Tumors
CAR-T therapy has demonstrated significant efficacy in treating hematological malignancies, particularly B-cell leukemias and lymphomas, by targeting specific antigens like CD19 [44]. However, its application in solid tumors faces challenges due to issues like identifying tumor-specific antigens, T-cell infiltration, and overcoming the immunosuppressive tumor microenvironment [45]. Conversely, CAR-NK therapy, which is emerging as a promising alternative, shows potential in both hematological malignancies and solid tumors [45]. CAR-NK cells can mediate their effects through both CAR-dependent and independent mechanisms, potentially offering broader tumor recognition and less susceptibility to the immunosuppressive effects of the tumor microenvironment [11]. Moreover, CAR-NK cells have been associated with fewer severe side effects, such as cytokine release syndrome and neurotoxicity, compared to CAR-T cells, highlighting their potential for a safer profile in cancer immunotherapy [12].
Thus, CAR-T cells have established a strong foothold in treating hematological cancers, their role in solid tumor therapy remains under intensive research to overcome existing limitations [46]. CAR-NK cells, on the other hand, represent a versatile and potentially safer option, with ongoing research indicating their broader applicability and effectiveness in treating both hematological malignancies and solid tumors [47].
3.8. Cost-Effectiveness
CAR-NK cells have several advantages over CAR-T cells that make them potentially more cost-effective:
- (1)
- Off-the-shelf availability: Unlike CAR-T cells, which are patient-specific and require a lengthy and costly manufacturing process, CAR-NK cells can be derived from healthy donors and stored for immediate use [48]. This eliminates the need for individualized cell production and reduces waiting time for patients.
- (2)
- Safety: CAR-NK cells have been associated with fewer severe side effects such as cytokine release syndrome (CRS), neurotoxicity, and graft-versus-host disease (GVHD) [49]. This could potentially lead to lower healthcare costs related to the management of these side effects.
- (3)
- Natural cytotoxicity: CAR-NK cells preserve the natural cytotoxicity of NK cells even if the expression of targeted tumor antigens is downregulated [48]. This could potentially lead to more effective treatment outcomes and, therefore, cost savings in the long run.
- (4)
- Manufacturing costs: While the exact cost of manufacturing CAR-NK cells is not specified, the cost of manufacturing CAR-T cells has been estimated to be between $48,000 and $106,000 per dose [50]. The ability to produce CAR-NK cells from healthy donors and in larger batches could potentially reduce these costs.
In conclusion, while both CAR-T and CAR-NK cells have shown promise in cancer therapy, the unique characteristics of CAR-NK cells, including their off-the-shelf availability, safety profile, and natural cytotoxicity, make them potentially more cost-effective. However, more research is needed to fully understand the cost-effectiveness of CAR-NK cells in comparison to CAR-T cells (Table 2).
4. Development of CAR-NK Cells
4.1. CAR-NK Cell Preparation Process
The manufacturing of CAR-NK cells is a complex, multistage endeavor, carefully designed to optimize their therapeutic safety, effectiveness, and uniformity. Initiation of this process requires the acquisition of initial biological materials, which may encompass peripheral blood mononuclear cells (PBMCs) obtained from donors, umbilical cord blood, or iPSCs [51].
In the generation of PBMC-derived CAR-NK cells, leukapheresis serves as the initial step to procure PBMCs, which is followed by the selective removal of CD3+ T cells and the enrichment of CD56+ NK cells [52]. These cells are then primed for activation with cytokines such as IL-2, or a synergistic cytokine blend including IL-2, IL-15, and IL-18. Subsequently, they are cultured alongside feeder cells over a span of 10 to 15 days to achieve full activation [53]. Prior to infusion into the patient, a lymphodepleting regimen is administered, and the support of IL-2 post-infusion is typically provided to promote CAR-NK cell persistence and activity [54]. In contrast, the production of CAR-NK cells from cord blood necessitates the initial isolation and amplification of CD34+ hematopoietic progenitor cells [55]. These progenitors are then guided through a differentiation process into functional NK cells by a milieu of cytokines including SCF, IL-7, IL-15, IL-1, amongst others. This differentiation phase is completed after an extended culture period with feeder cells, lasting beyond 21 days [56].
For CAR-NK cells derived from iPSCs, the protocol entails the progressive differentiation of iPSCs into hematopoietic progenitor cells through the action of SCF, vascular endothelial growth factor (VEGF), and bone morphogenetic protein 4 (BMP4) [57]. Following this, the progenitors are differentiated into NK cells using a tailored cocktail of cytokines, such as IL-15, IL-3, IL-7, SCF, and FLT3L [58]. The final maturation and expansion of these NK cells demand a 28 to 32-day cultivation with feeder cells [59]. Each of these methodologies underscores the nuanced and meticulous nature of CAR-NK cell production, a testament to the cutting-edge advances in cellular engineering that are setting new horizons in cancer immunotherapy (Figure 3).
4.2. Technological Advances and Innovations
CAR-NK cells represent a groundbreaking approach in immunotherapy, utilizing genetically engineered NK cells equipped with CARs [33]. These synthetic receptors are adept at recognizing specific tumor cell antigens, triggering the NK cells to annihilate the cancerous cells. A significant advantage of CAR-NK cells over their counterparts, CAR-T cells, lies in their derivation from allogeneic sources, like umbilical cord blood or induced pluripotent stem cells. This attribute negates the need for patient-specific manufacturing processes [6]. Moreover, CAR-NK cells present a substantially reduced risk of cytokine release syndrome and graft-versus-host disease, two severe complications often associated with CAR-T cell therapies [60].
The evolution of CAR-NK cell technology has been propelled by remarkable advancements in gene editing, cell engineering, and the field of cancer immunology. Pivotal developments include:
- (1)
- Enhanced CAR Designs: The initial generation of CARs featured a single-chain variable fragment (scFv) from an antibody targeting a tumor antigen, linked to a CD3ζ signaling domain for NK cell activation [61]. However, limitations in efficacy and persistence arose, with CAR-NK cells becoming exhausted or anergic after repeated activations. Addressing these drawbacks, subsequent generations of CARs now incorporate additional co-stimulatory domains, like CD28, 4-1BB, or OX40 [62]. These modifications significantly bolster the survival, proliferation, and functionality of CAR-NK cells [63]. Further, innovations have led to exploring diverse antigen recognition formats, such as NKG2D receptors, bispecific antibodies, or nanobodies, enhancing the specificity and adaptability of CAR-NK cells [64].
- (2)
- Identification of Novel Therapeutic Targets: The efficacy and safety of CAR-NK cell therapy heavily depend on the chosen tumor antigens. Ideal targets are those predominantly expressed on tumor cells, minimizing off-target effects on healthy tissues [65]. However, this is challenging since many tumor antigens also appear on normal cells at lower levels. To circumvent this, researchers have discovered more tumor-specific targets. Some target antigens are uniquely expressed in tumor-specific conditions, like HIF1α in hypoxic environments [12], while others, like CD38 or CD19, exhibit distinct glycosylation patterns in tumor cells compared to their normal counterparts [19].
- (3)
- Synergistic Combination Therapies: The integration of CAR-NK cells with other treatment modalities – such as chemotherapy, radiotherapy, checkpoint inhibitors, or cytokines – offers a promising strategy to elevate their effectiveness and safety [66]. These combinations can synergistically augment tumor infiltration, activation, persistence, and anti-tumor activity of CAR-NK cells [67]. For instance, combining CAR-NK cells with IL-15 or IL-21 can significantly enhance NK cell survival and functionality [68]. Additionally, pairing CAR-NK cells with PD-1 or PD-L1 inhibitors can disrupt the immune checkpoints that typically inhibit NK cell activity [69].
4.3. Strategies to Enhance CAR-NK Cells
One of the challenges in developing effective CAR-NK cell therapies is to overcome the tumor microenvironment, which can suppress the function and persistence of CAR-NK cells. Several strategies have been proposed to enhance the anti-tumor activity of CAR-NK cells, such as the use of specific cytokines, improving cell penetration abilities, and extending cell survival [70].
Cytokines are important mediators of immune responses and can modulate the proliferation, differentiation, activation, and survival of CAR-NK cells [6]. For example, IL-15 is a key cytokine for NK cell development and maintenance and has been shown to enhance the anti-tumor efficacy of CAR-NK cells in preclinical models [71]. IL-15 can also induce the expression of NKG2D, a natural cytotoxicity receptor that can recognize stress-induced ligands on tumor cells [72]. Other cytokines that have been explored for CAR-NK cell therapy include IL-2, IL-7, IL-12, IL-18, and IL-21 [73].
Another strategy to improve the anti-tumor activity of CAR-NK cells is to enhance their ability to penetrate solid tumors, which are often characterized by high interstitial pressure, dense extracellular matrix, and low oxygen levels [74]. One approach is to engineer CAR-NK cells with chemokine receptors that can guide them to the tumor site, such as CXCR2 or CCR2 [75]. Another approach is to co-express enzymes that can degrade the extracellular matrix, such as hyaluronidase or matrix metalloproteinases [66]. A third approach is to co-express hypoxia-inducible factors that can increase the expression of glycolytic enzymes and angiogenic factors, which can help CAR-NK cells adapt to the hypoxic tumor microenvironment [76].
A third strategy to enhance the anti-tumor activity of CAR-NK cells is to extend their survival and persistence in vivo, which can be affected by factors such as immunosuppressive cells, soluble factors, and metabolic stress [77]. One way to increase the survival of CAR-NK cells is to co-express anti-apoptotic genes, such as Bcl-2 or Bcl-xL [78]. Another way is to co-express immune checkpoint inhibitors, such as PD-1 or CTLA-4, which can prevent the exhaustion and dysfunction of CAR-NK cells [79]. A third way is to co-express metabolic regulators, such as AMPK or PGC-1α, which can enhance the mitochondrial function and oxidative phosphorylation of CAR-NK cells [80].
In the dynamic field of CAR-NK cell therapy, a multitude of cutting-edge strategies centered around novel cytokines and receptors are being pursued to surmount various challenges, including tumor heterogeneity, antigen escape, and the immunosuppressive tumor microenvironment [4]. One such innovative strategy involves leveraging CAK cells as a source for CAR-NK cells [81], offering a route to enhance their activation and cytotoxic capabilities against tumor cells. Equally significant is the exploration of the cytokine-inducible SH2-containing protein (CIS) as a regulatory mechanism in CAR-NK cell signaling [82]. CIS acts as a negative feedback regulator, aiming to finely tune the activation levels of CAR-NK cells, which could be crucial in preventing overactivation and reducing the risk of cytokine release syndrome, a common complication in cell-based therapies [83].
Further enhancing the CAR-NK cell repertoire, researchers are investigating the application of IL-15 super agonist complexes [68], which hold the potential to significantly boost the survival, persistence, and anti-tumor efficacy of CAR-NK cells. In parallel, IL-21 is being harnessed to promote the expansion and differentiation of CAR-NK cells [84], aiming to generate a more potent and diverse NK cell population capable of effectively targeting a broader spectrum of tumor antigens. Additionally, IL-12 is garnering attention for its ability to augment the anti-tumor activity of CAR-NK cells and aid in the formation of long-lasting immunological memory, an essential feature for sustained cancer remission [85].
Another groundbreaking approach involves the development of bispecific cytokine receptors [86]. These receptors are designed to broaden the specificity and versatility of CAR-NK cells, enabling them to target multiple tumor antigens simultaneously and respond more effectively to various signals within the tumor microenvironment [87]. This strategy could be pivotal in enhancing the targeting accuracy of CAR-NK cells, potentially overcoming one of the major hurdles in cancer immunotherapy – the adaptability of tumors [11].
Together, these advancements represent a significant leap forward in the quest to enhance the efficacy, durability, and safety of CAR-NK cell therapies. By addressing the current limitations and harnessing the power of innovative cytokines and receptor technologies, these strategies are laying the groundwork for more effective and tailored cancer treatments, offering hope to patients battling various malignancies (Figure 4).
4.4. Synthetic Biology Applications in CAR-NK Cells:
Synthetic biology, a cross-disciplinary field blending engineering principles with biological systems, is playing a pivotal role in advancing CAR-NK cells therapies [88]. In this innovative approach, CAR-NK cells are equipped with synthetic receptors that recognize and target specific antigens on tumor cells, initiating the NK cell's cytotoxic response. Despite their potential, CAR-NK cells face challenges such as target antigen selection, CAR expression regulation, enhancement of cell persistence and homing, and mitigation of off-target effects and immunogenicity [89]. To address these challenges, synthetic biology offers a suite of tools and strategies, particularly in modifying cytokine signaling pathways, crucial for the survival, proliferation, activation, and function of CAR-NK cells [90].
One notable application is the engineering of CAR-NK cells to express IL-15 or its receptor IL-15Rα constitutively, leveraging IL-15's role in NK cell development and maintenance. This modification aims to enhance CAR-NK cell persistence and antitumor activity in vivo [6,61]. Additionally, synthetic biology techniques are employed to create CAR-NK cells that secrete IL-12 upon antigen recognition. IL-12, a pro-inflammatory cytokine, boosts NK cell activation and cytotoxicity, thereby enhancing antitumor efficacy and countering immunosuppression in the tumor microenvironment [91]. Furthermore, to prevent NK cell exhaustion and enhance sensitivity to tumor antigens, CAR-NK cells are being engineered to lack PD-1 expression or incorporate a dominant-negative PD-1 mutant [92]. This manipulation addresses the inhibitory effects of the PD-1 pathway on NK cell function [93]. These examples illustrate some of the potential applications of synthetic biology in CAR-NK cell therapy. With its ability to provide precise and versatile modifications, synthetic biology stands as a powerful platform for designing more effective CAR-NK cell therapies, offering new avenues for cancer treatment.
5. Clinical Applications and Future Outlook
5.1. Clinical Trials of CAR-NK Cells:
CAR-NK cells are a promising immunotherapy strategy for the treatment of various cancers [12]. Several clinical trials have been conducted or are ongoing to evaluate the safety and efficacy of CAR-NK cells in different tumor types. Here, we provide an overview of some of these trials and their preliminary results. The first clinical trial of CAR-NK cells was reported by Liu et al. in 2020 [6]. They used allogeneic NK cells derived from cord blood and transduced them with a retroviral vector encoding a CD19-specific CAR. The CAR-NK cells were infused into 25 patients with relapsed or refractory B-cell malignancies, including non-Hodgkin lymphoma (NHL), chronic lymphocytic leukemia (CLL), and acute lymphoblastic leukemia (ALL) [6]. The results showed that the CAR-NK cells were well tolerated, with no cases of cytokine release syndrome (CRS) or graft-versus-host disease (GVHD). The overall response rate (ORR) was 68%, with 12 patients achieving complete remission (CR) and five achieving partial remission (PR). The median progression-free survival (PFS) was 13.8 months, and the median overall survival (OS) was not reached.
Another clinical trial of CAR-NK cells was conducted by Dai H et al. in 2020 [94]. They used NK cells derived from peripheral blood mononuclear cells (PBMCs) of healthy donors and transduced them with a lentiviral vector encoding a CD19-specific CAR. The CAR-NK cells were infused into 11 patients with relapsed or refractory B-cell malignancies, including NHL, CLL, and ALL. The results showed that the CAR-NK cells were well tolerated, with no cases of CRS or GVHD. The ORR was 73%, with eight patients achieving CR and one achieving PR. The median PFS was 8.8 months, and the median OS was not reached.
Other ongoing clinical trials of CAR-NK cells include NCT03692637, which is testing a CD19-specific CAR-NK cell product derived from iPSCs in patients with B-cell malignancies (ClinicalTrials.gov Identifier: NCT03692637); NCT04324996, which is testing a CD30-specific CAR-NK cell product derived from PBMCs in patients with Hodgkin lymphoma or anaplastic large cell lymphoma(ClinicalTrials.gov Identifier: NCT04324996); and NCT04613952, which is testing a mesothelin-specific CAR-NK cell product derived from PBMCs in patients with malignant pleural mesothelioma(ClinicalTrials.gov Identifier: NCT04613952). These trials are expected to provide more evidence on the feasibility, safety, and efficacy of CAR-NK cells in various cancer settings.
5.2. Future Research Directions and Challenges
CAR-NK cell therapy, with its significant potential in cancer treatment, particularly in hematological malignancies, faces several challenges and areas for future research to enhance its efficacy and safety. Some pivotal directions and challenges include:
- (1)
- Optimizing CAR Design and Engineering:
A key area of focus is the optimization of CAR constructs to improve their specificity, affinity, and functionality. This could involve developing bispecific or Mult specific CARs capable of targeting multiple tumor antigens, which would be particularly useful in treating cancers with high antigenic variability [95]. Incorporating costimulatory domains or cytokines into CAR designs is another strategy to modulate CAR-NK cell activation and survival, potentially improving their persistence and reducing toxicity [96]. Additionally, the integration of suicide genes or switchable receptors offers a method to control the longevity and potential adverse effects of CAR-NK cells in vivo, providing a safety switch to mitigate risks [97].
- (2)
- Developing Novel Sources and Production Methods:
The search for new sources and methods for generating CAR-NK cells is crucial. Utilizing iPSCs or umbilical cord blood (UCB) as alternative NK cell sources opens possibilities for a more readily available and versatile cell supply [98]. Advances in gene delivery, using either viral or non-viral vectors, and innovative ex vivo expansion or in vivo proliferation techniques, are essential to produce CAR-NK cells in sufficient quantities and qualities [99].
- (3)
- Overcoming Tumor Microenvironment Barriers:
The tumor microenvironment (TME) presents significant barriers that can impair the function and homing of CAR-NK cells [100]. Combination therapies that include immune checkpoint inhibitors, cytokines, or chemotherapeutic agents could help modulate the immunosuppressive nature of the TME [101]. Additionally, employing nanoparticles or antibodies to enhance CAR-NK cell delivery and penetration into solid tumors, along with using advanced imaging techniques or biomarkers to track their distribution and effectiveness, are promising approaches to overcome these challenges [102,103].
- (4)
- Addressing Off-Target Effects and Adverse Events:
The potential for off-target effects and adverse events remains a concern in CAR-NK cell therapy. Research focused on antigen-specific, or antigen-loss relapse models is vital to evaluate risks associated with on-target/off-tumor toxicity [4]. Preclinical animal models and clinical trials are essential for assessing the safety and feasibility of CAR-NK cell therapy across different cancer types and stages [104]. Additionally, the development and standardization of protocols and guidelines for managing adverse events such as CRS or neurotoxicity are crucial for the safe implementation of this therapy [105].
- (5)
- Enhancing Surgical Oncology Outcomes through CAR-NK Cell Therapy Integration
In the evolving landscape of oncological treatment, the advent of CAR-NK cell therapy presents a promising synergy with surgical interventions, particularly in the multimodal management of cancer [106]. The strategic integration of CAR-NK cells could enhance the efficacy of surgical resection and provide a comprehensive approach to cancer care.
Preoperative CAR-NK Cell Therapy: Prior to surgical intervention, CAR-NK cell therapy could be deployed to reduce tumor burden. The cytotoxic activity of CAR-NK cells against tumor cells can potentially decrease tumor size, rendering previously inoperable tumors amenable to surgery [12]. Additionally, this reduction in tumor mass may lead to less extensive surgeries, diminishing the risk of postoperative complications and preserving more of the patient's healthy tissue [107].
Adjuvant CAR-NK Cell Therapy: Post-surgical application of CAR-NK cells could play a pivotal role in eradicating residual malignant cells that evade surgical excision [108]. This could be particularly beneficial in the context of microscopic residual disease, which often contributes to cancer recurrence. Administering CAR-NK cell therapy following surgery might decrease the likelihood of relapse, offering a proactive approach to sustain the disease-free interval [109].
Combination Therapy for Comprehensive Care: The incorporation of CAR-NK cell therapy into the broader oncological treatment paradigm, alongside surgical resection, radiation, and chemotherapy, reflects a comprehensive strategy that could maximize therapeutic outcomes [110]. By providing a targeted immunotherapeutic intervention, CAR-NK cells can complement the direct physical removal of tumor mass, potentially preventing local and systemic relapse, a key concern in surgical oncology [111].
By harnessing the specificity and cytotoxic potential of CAR-NK cells, we can envision a collaborative model where immunotherapy and surgery work in concert to tackle the complex nature of cancer. This approach aligns with the journal's commitment to fostering innovations that support the surgeon's role in cancer care, advocating for a holistic and patient-centered approach to treatment.
- (6)
- Ethical Considerations in CAR-NK Cell Therapy:
In advancing CAR-NK cell therapy, addressing ethical challenges is paramount for patient safety, public trust, and equitable treatment access [112]. Essential considerations include obtaining informed consent, where patients must be thoroughly educated about the therapy's complexities, potential risks, and long-term implications to ensure informed decisions [4]. Additionally, the genetic modifications central to CAR-NK therapy heighten privacy concerns, necessitating robust measures to protect sensitive patient data and maintain confidentiality [77]. Beyond the clinical trial phase, post-trial care and monitoring are crucial for assessing long-term effects and ensuring the ongoing welfare of patients [4]. Together, these ethical practices underscore the commitment to patient autonomy, privacy, and sustained care, forming the backbone of responsible CAR-NK cell therapy deployment.
6. Summary
CAR-NK cells, derived from various sources like peripheral blood, umbilical cord blood, and induced pluripotent stem cells, offer a promising alternative due to their inherent advantages such as reduced risk of cytokine release syndrome and the ability to target both hematological malignancies and solid tumors without the need for human leukocyte antigen (HLA) matching. As CAR-NK cells have shown efficacy and safety in treating hematological malignancies, with ongoing research into their use for solid tumors, refining their design, manufacturing processes, and delivery mechanisms remains a priority. The integration of advancements in synthetic biology, gene editing, and immunology holds promise for enhancing the effectiveness of CAR-NK cell therapies. Ethical considerations, including patient autonomy and privacy, are paramount as we navigate the complexities of this evolving field, ensuring that the new wave of immunotherapy not only achieves clinical success but also aligns with broader health economic and ethical standards. Thus, CAR-NK cell therapy represents a significant shift in cancer immunotherapy, with the potential to redefine oncological care and offer new avenues for treatment.
In conclusion, CAR-NK cell therapy emerges as a promising and innovative approach in the realm of immunotherapy, offering a compelling alternative to CAR-T cells with its potential for reduced toxicity and broader applicability. Given the current stage of CAR-NK cell therapy, which has not yet been widely applied in clinical settings, it is premature to conclusively assess its cost-effectiveness compared to CAR-T cell therapies. The lack of large-scale clinical application limits the availability of comprehensive economic data, highlighting the need for future research to conduct detailed cost analyses. Such studies are essential to understand the economic implications fully and to ensure the sustainability and accessibility of these therapies as they progress toward broader clinical adoption.
Author Contributions
Conceptualization, A.U.R.A. and D.W.; Data curation, W.L. and A.U.R.A.; Writing - original draft, W.L. and A.U.R.A.; Writing - review and editing, X.W. and X.Z.; Funding acquisition, W.L. and D.W.; Project administration, A.U.R.A. and D.W. All authors have read and approved the final manuscript for publication.
Funding
This study was supported by the Dalian City Outstanding Young Science and Technology Talent Program, No.2023RY020(W.L.); Dalian City High-Level Innovative Talent Team Project, No. 2023RG011(D.W.).
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare that they have no competing interests.
References
- Mitra, A.; Barua, A.; Huang, L.; Ganguly, S.; Feng, Q.; He, B. From bench to bedside: the history and progress of CAR T cell therapy. Front Immunol 2023, 14, 1188049. [Google Scholar] [CrossRef] [PubMed]
- Maus, M.V. A decade of CAR T cell evolution. Nat Cancer 2022, 3, 270–271. [Google Scholar] [CrossRef] [PubMed]
- Pan, K.; Farrukh, H.; Chittepu, V.; Xu, H.; Pan, C.X.; Zhu, Z. CAR race to cancer immunotherapy: from CAR T, CAR NK to CAR macrophage therapy. J Exp Clin Cancer Res 2022, 41, 119. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.; Wen, Q.; Zhang, X. CAR-NK cell therapy for hematological malignancies: recent updates from ASH 2022. J Hematol Oncol 2023, 16, 35. [Google Scholar] [CrossRef] [PubMed]
- Ghazvinian, Z.; Abdolahi, S.; Tokhanbigli, S.; Tarzemani, S.; Piccin, A.; Reza Zali, M.; Verdi, J.; Baghaei, K. Contribution of natural killer cells in innate immunity against colorectal cancer. Front Oncol 2022, 12, 1077053. [Google Scholar] [CrossRef]
- Liu, E.; Marin, D.; Banerjee, P.; Macapinlac, H.A.; Thompson, P.; Basar, R.; Nassif Kerbauy, L.; Overman, B.; Thall, P.; Kaplan, M.; et al. Use of CAR-Transduced Natural Killer Cells in CD19-Positive Lymphoid Tumors. N Engl J Med 2020, 382, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Rezvani, K.; Rouce, R.; Liu, E.; Shpall, E. Engineering Natural Killer Cells for Cancer Immunotherapy. Mol Ther 2017, 25, 1769–1781. [Google Scholar] [CrossRef]
- Zhang, C.; Wang, Z.; Yang, Z.; Wang, M.; Li, S.; Li, Y.; Zhang, R.; Xiong, Z.; Wei, Z.; Shen, J.; et al. Phase I Escalating-Dose Trial of CAR-T Therapy Targeting CEA(+) Metastatic Colorectal Cancers. Mol Ther 2017, 25, 1248–1258. [Google Scholar] [CrossRef]
- Glienke, W.; Esser, R.; Priesner, C.; Suerth, J.D.; Schambach, A.; Wels, W.S.; Grez, M.; Kloess, S.; Arseniev, L.; Koehl, U. Advantages and applications of CAR-expressing natural killer cells. Front Pharmacol 2015, 6, 21. [Google Scholar] [CrossRef]
- Klingemann, H. The NK-92 cell line-30 years later: its impact on natural killer cell research and treatment of cancer. Cytotherapy 2023, 25, 451–457. [Google Scholar] [CrossRef]
- Li, T.; Niu, M.; Zhang, W.; Qin, S.; Zhou, J.; Yi, M. CAR-NK cells for cancer immunotherapy: recent advances and future directions. Front Immunol 2024, 15, 1361194. [Google Scholar] [CrossRef] [PubMed]
- Xie, G.; Dong, H.; Liang, Y.; Ham, J.D.; Rizwan, R.; Chen, J. CAR-NK cells: A promising cellular immunotherapy for cancer. EBioMedicine 2020, 59, 102975. [Google Scholar] [CrossRef] [PubMed]
- Basar, R.; Daher, M.; Rezvani, K. Next-generation cell therapies: the emerging role of CAR-NK cells. Hematology Am Soc Hematol Educ Program 2020, 2020, 570–578. [Google Scholar] [CrossRef]
- Kvacskay, P.; Merkt, W. CD19.CAR T cells versus obinutuzumab—who will win the race for use in deep B cell depletion therapy in systemic autoimmunity? Rheumatology 2024. [CrossRef]
- Wang, Y.; Rousset, X.; Prunier, C.; Dosda, E.; Gutierrez-Guerrero, A.; Abrial, P.; Menkova, I.; Viallet, J. Abstract 4018: An innovative in vivo model for CAR-T cell therapy development: Tolerability and efficacy evaluation of CD19-targeting CAR-T cells on human lymphoma using the chicken CAM assay. Cancer Research 2024, 84, 4018–4018. [Google Scholar] [CrossRef]
- Ritmeester-Loy, S.A.; Draper, I.H.; Bueter, E.C.; Lautz, J.D.; Zhang-Wong, Y.; Gustafson, J.A.; Wilson, A.L.; Lin, C.; Gafken, P.R.; Jensen, M.C.; et al. Differential protein-protein interactions underlie signaling mediated by the TCR and a 4-1BB domain–containing CAR. 2024, 17, eadd4671. [Google Scholar] [CrossRef] [PubMed]
- Herrera, L.; Santos, S.; Vesga, M.A.; Carrascosa, T.; Garcia-Ruiz, J.C.; Perez-Martinez, A.; Juan, M.; Eguizabal, C. The Race of CAR Therapies: CAR-NK Cells for Fighting B-Cell Hematological Cancers. Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Page, A.; Chuvin, N.; Valladeau-Guilemond, J.; Depil, S. Development of NK cell-based cancer immunotherapies through receptor engineering. Cellular & Molecular Immunology 2024, 21, 315–331. [Google Scholar] [CrossRef]
- Zhang, L.; Meng, Y.; Feng, X.; Han, Z. CAR-NK cells for cancer immunotherapy: from bench to bedside. Biomarker research 2022, 10, 12. [Google Scholar] [CrossRef]
- Flemming, A. CD3ε tunes CAR T cell anticancer activity. Nature Reviews Immunology 2020, 20, 520–521. [Google Scholar] [CrossRef]
- Singh, R.; Kim, Y.H.; Lee, S.J.; Eom, H.S.; Choi, B.K. 4-1BB immunotherapy: advances and hurdles. Exp Mol Med 2024, 56, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Cappell, K.M.; Kochenderfer, J.N. A comparison of chimeric antigen receptors containing CD28 versus 4-1BB costimulatory domains. Nat Rev Clin Oncol 2021, 18, 715–727. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Zhang, R.; Nie, X.; Yang, Y.; Hua, Y.; Lu, P. 4-1BB Targeting Immunotherapy: Mechanism, Antibodies, and Chimeric Antigen Receptor T. Cancer Biother Radiopharm 2023, 38, 431–444. [Google Scholar] [CrossRef] [PubMed]
- Depil, S.; Duchateau, P.; Grupp, S.A.; Mufti, G.; Poirot, L. 'Off-the-shelf' allogeneic CAR T cells: development and challenges. Nat Rev Drug Discov 19, 185-199. [CrossRef]
- Caimi, P.F.; Melenhorst, J.J. Allogeneic CAR T Cells: Complex Cellular Therapy Designs Test the Limits of Our Preclinical Models. Cancer Immunology Research 2024, 12, 385–386. [Google Scholar] [CrossRef] [PubMed]
- Heipertz, E.L.; Zynda, E.R.; Stav-Noraas, T.E.; Hungler, A.D.; Boucher, S.E.; Kaur, N.; Vemuri, M.C. Current Perspectives on "Off-The-Shelf" Allogeneic NK and CAR-NK Cell Therapies. Front Immunol 2021, 12, 732135. [Google Scholar] [CrossRef]
- Barnes, S.A.; Trew, I.; de Jong, E.; Foley, B. Making a Killer: Selecting the Optimal Natural Killer Cells for Improved Immunotherapies. Front Immunol 2021, 12, 765705. [Google Scholar] [CrossRef] [PubMed]
- Khawar, M.B.; Sun, H. CAR-NK Cells: From Natural Basis to Design for Kill. Front Immunol 2021, 12, 707542. [Google Scholar] [CrossRef] [PubMed]
- Si, X.; Xiao, L.; Brown, C.E.; Wang, D. Preclinical Evaluation of CAR T Cell Function: In Vitro and In Vivo Models. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef]
- Hwu, P.; Rosenberg, S.A. The genetic modification of T cells for cancer therapy: an overview of laboratory and clinical trials. Cancer Detect Prev 1994, 18, 43–50. [Google Scholar]
- Rosenberg, S.A.; Restifo, N.P. Adoptive cell transfer as personalized immunotherapy for human cancer. 2015, 348, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Roddie, C.; O'Reilly, M.; Dias Alves Pinto, J.; Vispute, K.; Lowdell, M. Manufacturing chimeric antigen receptor T cells: issues and challenges. Cytotherapy 2019, 21, 327–340. [Google Scholar] [CrossRef] [PubMed]
- Rezvani, K.; Rouce, R.H. The Application of Natural Killer Cell Immunotherapy for the Treatment of Cancer. Front Immunol 2015, 6, 578. [Google Scholar] [CrossRef] [PubMed]
- Ghassemi, S.; Durgin, J.S.; Nunez-Cruz, S.; Patel, J.; Leferovich, J.; Pinzone, M.; Shen, F.; Cummins, K.D.; Plesa, G.; Cantu, V.A.; et al. Rapid manufacturing of non-activated potent CAR T cells. Nat Biomed Eng 2022, 6, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Wrona, E.; Borowiec, M.; Potemski, P. CAR-NK Cells in the Treatment of Solid Tumors. Int J Mol Sci 2021, 22. [Google Scholar] [CrossRef] [PubMed]
- Portillo, A.L.; Hogg, R.; Ashkar, A.A. Production of human CAR-NK cells with lentiviral vectors and functional assessment in vitro. STAR Protoc 2021, 2, 100956. [Google Scholar] [CrossRef] [PubMed]
- Naeimi Kararoudi, M.; Likhite, S.; Elmas, E.; Yamamoto, K.; Schwartz, M.; Sorathia, K.; de Souza Fernandes Pereira, M.; Sezgin, Y.; Devine, R.D.; Lyberger, J.M.; et al. Optimization and validation of CAR transduction into human primary NK cells using CRISPR and AAV. Cell reports methods 2022, 2, 100236. [Google Scholar] [CrossRef] [PubMed]
- Tomasik, J.; Jasinski, M.; Basak, G.W. Next generations of CAR-T cells - new therapeutic opportunities in hematology? Front Immunol 2022, 13, 1034707. [Google Scholar] [CrossRef] [PubMed]
- Sadelain, M.; Rivière, I.; Riddell, S. Therapeutic T cell engineering. Nature 2017, 545, 423–431. [Google Scholar] [CrossRef]
- Schaible, P.; Bethge, W.; Lengerke, C.; Haraszti, R.A. RNA Therapeutics for Improving CAR T-cell Safety and Efficacy. Cancer Res 2023, 83, 354–362. [Google Scholar] [CrossRef]
- Shin, E.; Bak, S.H.; Park, T.; Kim, J.W.; Yoon, S.R.; Jung, H.; Noh, J.Y. Understanding NK cell biology for harnessing NK cell therapies: targeting cancer and beyond. Front Immunol 2023, 14, 1192907. [Google Scholar] [CrossRef] [PubMed]
- Neelapu, S.S.; Tummala, S.; Kebriaei, P.; Wierda, W.; Gutierrez, C.; Locke, F.L.; Komanduri, K.V.; Lin, Y.; Jain, N.; Daver, N.; et al. Chimeric antigen receptor T-cell therapy - assessment and management of toxicities. Nat Rev Clin Oncol 2018, 15, 47–62. [Google Scholar] [CrossRef] [PubMed]
- Brudno, J.N.; Kochenderfer, J.N. Toxicities of chimeric antigen receptor T cells: recognition and management. Blood 2016, 127, 3321–3330. [Google Scholar] [CrossRef] [PubMed]
- Roschewski, M.; Longo, D.L.; Wilson, W.H. CAR T-Cell Therapy for Large B-Cell Lymphoma — Who, When, and How? 2022, 386, 692-696. [CrossRef]
- Fang, F.; Xiao, W.; Tian, Z. NK cell-based immunotherapy for cancer. Seminars in immunology 2017, 31, 37–54. [Google Scholar] [CrossRef] [PubMed]
- Yan, T.; Zhu, L.; Chen, J. Current advances and challenges in CAR T-Cell therapy for solid tumors: tumor-associated antigens and the tumor microenvironment. Exp Hematol Oncol 2023, 12, 14. [Google Scholar] [CrossRef]
- Lee, M.Y.; Robbins, Y.; Sievers, C.; Friedman, J.; Abdul Sater, H.; Clavijo, P.E.; Judd, N.; Tsong, E.; Silvin, C.; Soon-Shiong, P.; et al. Chimeric antigen receptor engineered NK cellular immunotherapy overcomes the selection of T-cell escape variant cancer cells. J Immunother Cancer 2021, 9. [Google Scholar] [CrossRef]
- Lu, H.; Zhao, X.; Li, Z.; Hu, Y.; Wang, H. From CAR-T Cells to CAR-NK Cells: A Developing Immunotherapy Method for Hematological Malignancies. 2021, 11. [CrossRef]
- Zhang, X.W.; Wu, Y.S.; Xu, T.M.; Cui, M.H. CAR-T Cells in the Treatment of Ovarian Cancer: A Promising Cell Therapy. Biomolecules 2023, 13. [Google Scholar] [CrossRef]
- Katy Spink; Steinsapir, A. The long road to affordability: a cost of goods analysis for an autologous CAR-T process. Cell Gene Therapy Insights 2018, 4, 1105–1116. [CrossRef]
- Fang, F.; Xie, S.; Chen, M.; Li, Y.; Yue, J.; Ma, J.; Shu, X.; He, Y.; Xiao, W.; Tian, Z. Advances in NK cell production. Cell Mol Immunol 2022, 19, 460–481. [Google Scholar] [CrossRef] [PubMed]
- Elahi, R.; Heidary, A.H.; Hadiloo, K.; Esmaeilzadeh, A. Chimeric Antigen Receptor-Engineered Natural Killer (CAR NK) Cells in Cancer Treatment; Recent Advances and Future Prospects. Stem Cell Rev Rep 2021, 17, 2081–2106. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Meng, Y.; Zhang, L.; Han, Z.; Feng, X. High-efficient generation of natural killer cells from peripheral blood with preferable cell vitality and enhanced cytotoxicity by combination of IL-2, IL-15 and IL-18. Biochem Biophys Res Commun 2021, 534, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Rafei, H.; Daher, M.; Rezvani, K. Chimeric antigen receptor (CAR) natural killer (NK)-cell therapy: leveraging the power of innate immunity. Br J Haematol 2021, 193, 216–230. [Google Scholar] [CrossRef] [PubMed]
- Wen, W.; Chen, X.; Shen, X.-Y.; Li, H.-Y.; Zhang, F.; Fang, F.-Q.; Zhang, X.-B. Enhancing cord blood stem cell-derived NK cell growth and differentiation through hyperosmosis. Stem Cell Research & Therapy 2023, 14, 295. [Google Scholar] [CrossRef]
- Bozhilov, Y.K.; Hsu, I.; Brown, E.J.; Wilkinson, A.C. In Vitro Human Haematopoietic Stem Cell Expansion and Differentiation. Cells 2023, 12. [Google Scholar] [CrossRef]
- Hsu, L.J.; Liu, C.L.; Kuo, M.L.; Shen, C.N.; Shen, C.R. An Alternative Cell Therapy for Cancers: Induced Pluripotent Stem Cell (iPSC)-Derived Natural Killer Cells. Biomedicines 2021, 9. [Google Scholar] [CrossRef]
- Montazersaheb, S.; Fathi, E.; Farahzadi, R. Cytokines and signaling pathways involved in differentiation potential of hematopoietic stem cells towards natural killer cells. Tissue Cell 2021, 70, 101501. [Google Scholar] [CrossRef] [PubMed]
- Moseman, J.E.; Foltz, J.A.; Sorathia, K.; Heipertz, E.L.; Lee, D.A. Evaluation of serum-free media formulations in feeder cell–stimulated expansion of natural killer cells. Cytotherapy 2020, 22, 322–328. [Google Scholar] [CrossRef]
- Klingemann, H.; Boissel, L.; Toneguzzo, F. Natural Killer Cells for Immunotherapy - Advantages of the NK-92 Cell Line over Blood NK Cells. Front Immunol 2016, 7, 91. [Google Scholar] [CrossRef]
- Zhang, C.; Oberoi, P.; Oelsner, S.; Waldmann, A.; Lindner, A.; Tonn, T.; Wels, W.S. Chimeric Antigen Receptor-Engineered NK-92 Cells: An Off-the-Shelf Cellular Therapeutic for Targeted Elimination of Cancer Cells and Induction of Protective Antitumor Immunity. Front Immunol 2017, 8, 533. [Google Scholar] [CrossRef] [PubMed]
- Chu, J.; Deng, Y.; Benson, D.M.; He, S.; Hughes, T.; Zhang, J.; Peng, Y.; Mao, H.; Yi, L.; Ghoshal, K.; et al. CS1-specific chimeric antigen receptor (CAR)-engineered natural killer cells enhance in vitro and in vivo antitumor activity against human multiple myeloma. Leukemia 2014, 28, 917–927. [Google Scholar] [CrossRef] [PubMed]
- Imai, C.; Iwamoto, S.; Campana, D. Genetic modification of primary natural killer cells overcomes inhibitory signals and induces specific killing of leukemic cells. Blood 2005, 106, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Schonfeld, K.; Sahm, C.; Zhang, C.; Naundorf, S.; Brendel, C.; Odendahl, M.; Nowakowska, P.; Bonig, H.; Kohl, U.; Kloess, S.; et al. Selective inhibition of tumor growth by clonal NK cells expressing an ErbB2/HER2-specific chimeric antigen receptor. Mol Ther 2015, 23, 330–338. [Google Scholar] [CrossRef] [PubMed]
- St-Pierre, F.; Bhatia, S.; Chandra, S. Harnessing Natural Killer Cells in Cancer Immunotherapy: A Review of Mechanisms and Novel Therapies. Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Yan, Y.; Zhang, J.; Wei, Z.; Li, H.; Xing, L. Synergistic treatment strategy: combining CAR-NK cell therapy and radiotherapy to combat solid tumors. Front Immunol 2023, 14, 1298683. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Hu, Y.; Shi, C. Targeting Natural Killer Cells for Tumor Immunotherapy. Front Immunol 2020, 11, 60. [Google Scholar] [CrossRef] [PubMed]
- Romee, R.; Rosario, M.; Berrien-Elliott, M.M.; Wagner, J.A.; Jewell, B.A.; Schappe, T.; Leong, J.W.; Abdel-Latif, S.; Schneider, S.E.; Willey, S.; et al. Cytokine-induced memory-like natural killer cells exhibit enhanced responses against myeloid leukemia. Sci Transl Med 2016, 8, 357ra123. [Google Scholar] [CrossRef] [PubMed]
- Jia, L.; Zhang, Q.; Zhang, R. PD-1/PD-L1 pathway blockade works as an effective and practical therapy for cancer immunotherapy. Cancer biology & medicine 2018, 15, 116–123. [Google Scholar] [CrossRef]
- Valeri, A.; Garcia-Ortiz, A.; Castellano, E.; Cordoba, L.; Maroto-Martin, E.; Encinas, J.; Leivas, A.; Rio, P.; Martinez-Lopez, J. Overcoming tumor resistance mechanisms in CAR-NK cell therapy. Front Immunol 2022, 13, 953849. [Google Scholar] [CrossRef]
- Li, H.; Zhao, Y. Increasing the safety and efficacy of chimeric antigen receptor T cell therapy. Protein Cell 2017, 8, 573–589. [Google Scholar] [CrossRef]
- Lanier, L.L. Up on the tightrope: natural killer cell activation and inhibition. Nat Immunol 2008, 9, 495–502. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhou, W.; Yang, J.; Yang, J.; Wang, W. Chimeric antigen receptor engineered natural killer cells for cancer therapy. Exp Hematol Oncol 2023, 12, 70. [Google Scholar] [CrossRef]
- Liu, G.; Rui, W.; Zheng, H.; Huang, D.; Yu, F.; Zhang, Y.; Dong, J.; Zhao, X.; Lin, X. CXCR2-modified CAR-T cells have enhanced trafficking ability that improves treatment of hepatocellular carcinoma. European journal of immunology 2020, 50, 712–724. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Wang, Y.; Miao, L.; Liu, Q.; Musetti, S.; Li, J.; Huang, L. Combination Immunotherapy of MUC1 mRNA Nano-vaccine and CTLA-4 Blockade Effectively Inhibits Growth of Triple Negative Breast Cancer. Mol Ther 2018, 26, 45–55. [Google Scholar] [CrossRef]
- Doedens, A.L.; Phan, A.T.; Stradner, M.H.; Fujimoto, J.K.; Nguyen, J.V.; Yang, E.; Johnson, R.S.; Goldrath, A.W. Hypoxia-inducible factors enhance the effector responses of CD8(+) T cells to persistent antigen. Nat Immunol 2013, 14, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Kilgour, M.K.; Bastin, D.J.; Lee, S.-H.; Ardolino, M.; McComb, S.; Visram, A. Advancements in CAR-NK therapy: lessons to be learned from CAR-T therapy. 2023, 14. [CrossRef]
- Pattingre, S.; Tassa, A.; Qu, X.; Garuti, R.; Liang, X.H.; Mizushima, N.; Packer, M.; Schneider, M.D.; Levine, B. Bcl-2 antiapoptotic proteins inhibit Beclin 1-dependent autophagy. Cell 2005, 122, 927–939. [Google Scholar] [CrossRef] [PubMed]
- Cherkassky, L.; Morello, A.; Villena-Vargas, J.; Feng, Y.; Dimitrov, D.S.; Jones, D.R.; Sadelain, M.; Adusumilli, P.S. Human CAR T cells with cell-intrinsic PD-1 checkpoint blockade resist tumor-mediated inhibition. J Clin Invest 2016, 126, 3130–3144. [Google Scholar] [CrossRef]
- Dillon, L.M.; Rebelo, A.P.; Moraes, C.T. The role of PGC-1 coactivators in aging skeletal muscle and heart. IUBMB Life 2012, 64, 231–241. [Google Scholar] [CrossRef]
- Denman, C.J.; Senyukov, V.V.; Somanchi, S.S.; Phatarpekar, P.V.; Kopp, L.M.; Johnson, J.L.; Singh, H.; Hurton, L.; Maiti, S.N.; Huls, M.H.; et al. Membrane-bound IL-21 promotes sustained ex vivo proliferation of human natural killer cells. PLoS One 2012, 7, e30264. [Google Scholar] [CrossRef]
- Delconte, R.B.; Kolesnik, T.B.; Dagley, L.F.; Rautela, J.; Shi, W.; Putz, E.M.; Stannard, K.; Zhang, J.G.; Teh, C.; Firth, M.; et al. CIS is a potent checkpoint in NK cell-mediated tumor immunity. Nat Immunol 2016, 17, 816–824. [Google Scholar] [CrossRef] [PubMed]
- Chen, S. Releasing the brake in CAR natural killer cells. Blood 2021, 137, 579–581. [Google Scholar] [CrossRef] [PubMed]
- Imamura, M.; Shook, D.; Kamiya, T.; Shimasaki, N.; Chai, S.M.; Coustan-Smith, E.; Imai, C.; Campana, D. Autonomous growth and increased cytotoxicity of natural killer cells expressing membrane-bound interleukin-15. Blood 2014, 124, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, R.; Baker, J.; Beilhack, A.; Zeiser, R.; Olson, J.A.; Sega, E.I.; Karimi, M.; Negrin, R.S. In vivo trafficking and survival of cytokine-induced killer cells resulting in minimal GVHD with retention of antitumor activity. Blood 2008, 112, 2563–2574. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Yang, Y.; Wang, G.; Liu, M. Current landscape and future directions of bispecific antibodies in cancer immunotherapy. Front Immunol 2022, 13, 1035276. [Google Scholar] [CrossRef] [PubMed]
- Basar, R.; Daher, M.; Rezvani, K. Next-generation cell therapies: the emerging role of CAR-NK cells. Blood Adv 2020, 4, 5868–5876. [Google Scholar] [CrossRef] [PubMed]
- Clubb, J.D.; Gao, T.A.; Chen, Y.Y. Synthetic Biology in the Engineering of CAR-T and CAR-NK Cell Therapies: Facts and Hopes. Clin Cancer Res 2023, 29, 1390–1402. [Google Scholar] [CrossRef]
- Zhang, C.; Hu, Y.; Xiao, W.; Tian, Z. Chimeric antigen receptor- and natural killer cell receptor-engineered innate killer cells in cancer immunotherapy. Cell Mol Immunol 2021, 18, 2083–2100. [Google Scholar] [CrossRef]
- Cienfuegos-Jimenez, O.; Vazquez-Garza, E.; Rojas-Martinez, A. CAR-NK Cells for Cancer Therapy: Molecular Redesign of the Innate Antineoplastic Response. Curr Gene Ther 2022, 22, 303–318. [Google Scholar] [CrossRef]
- Jiang, H.; Zhang, W.; Shang, P.; Zhang, H.; Fu, W.; Ye, F.; Zeng, T.; Huang, H.; Zhang, X.; Sun, W.; et al. Transfection of chimeric anti-CD138 gene enhances natural killer cell activation and killing of multiple myeloma cells. Mol Oncol 2014, 8, 297–310. [Google Scholar] [CrossRef]
- Yang, L.; Shen, M.; Xu, L.J.; Yang, X.; Tsai, Y.; Keng, P.C.; Chen, Y.; Lee, S.O. Enhancing NK cell-mediated cytotoxicity to cisplatin-resistant lung cancer cells via MEK/Erk signaling inhibition. Sci Rep 2017, 7, 7958. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Chen, C.; Guo, Y.; Hu, S.; Sun, Z. Effect of CRISPR/Cas9-Edited PD-1/PD-L1 on Tumor Immunity and Immunotherapy. Front Immunol 2022, 13, 848327. [Google Scholar] [CrossRef] [PubMed]
- Dai, H.; Wu, Z.; Jia, H.; Tong, C.; Guo, Y.; Ti, D.; Han, X.; Liu, Y.; Zhang, W.; Wang, C.; et al. Bispecific CAR-T cells targeting both CD19 and CD22 for therapy of adults with relapsed or refractory B cell acute lymphoblastic leukemia. J Hematol Oncol 2020, 13, 30. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Nishikawa, H. Engineering strategies for broad application of TCR-T- and CAR-T-cell therapies. Int Immunol 2021, 33, 551–562. [Google Scholar] [CrossRef] [PubMed]
- Duan, Y.; Chen, R.; Huang, Y.; Meng, X.; Chen, J.; Liao, C.; Tang, Y.; Zhou, C.; Gao, X.; Sun, J. Tuning the ignition of CAR: optimizing the affinity of scFv to improve CAR-T therapy. Cell Mol Life Sci 2021, 79, 14. [Google Scholar] [CrossRef] [PubMed]
- Brudno, J.N.; Lam, N.; Vanasse, D.; Shen, Y.W.; Rose, J.J.; Rossi, J.; Xue, A.; Bot, A.; Scholler, N.; Mikkilineni, L.; et al. Safety and feasibility of anti-CD19 CAR T cells with fully human binding domains in patients with B-cell lymphoma. Nature medicine 2020, 26, 270–280. [Google Scholar] [CrossRef] [PubMed]
- Themeli, M.; Kloss, C.C.; Ciriello, G.; Fedorov, V.D.; Perna, F.; Gonen, M.; Sadelain, M. Generation of tumor-targeted human T lymphocytes from induced pluripotent stem cells for cancer therapy. Nat Biotechnol 2013, 31, 928–933. [Google Scholar] [CrossRef] [PubMed]
- Knorr, D.A.; Ni, Z.; Hermanson, D.; Hexum, M.K.; Bendzick, L.; Cooper, L.J.; Lee, D.A.; Kaufman, D.S. Clinical-scale derivation of natural killer cells from human pluripotent stem cells for cancer therapy. Stem Cells Transl Med 2013, 2, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Melaiu, O.; Lucarini, V.; Cifaldi, L.; Fruci, D. Influence of the Tumor Microenvironment on NK Cell Function in Solid Tumors. Front Immunol 2019, 10, 3038. [Google Scholar] [CrossRef]
- Vitale, M.; Cantoni, C.; Pietra, G.; Mingari, M.C.; Moretta, L. Effect of tumor cells and tumor microenvironment on NK-cell function. European journal of immunology 2014, 44, 1582–1592. [Google Scholar] [CrossRef]
- Murugan, D.; Murugesan, V.; Panchapakesan, B.; Rangasamy, L. Nanoparticle Enhancement of Natural Killer (NK) Cell-Based Immunotherapy. 2022, 14, 5438.
- El-Mayta, R.; Zhang, Z.; Hamilton, A.G.; Mitchell, M.J. Delivery technologies to engineer natural killer cells for cancer immunotherapy. Cancer Gene Ther 2021, 28, 947–959. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Song, W.; Li, Z.; Zhang, M. Preclinical and clinical studies of CAR-NK-cell therapies for malignancies. Front Immunol 2022, 13, 992232. [Google Scholar] [CrossRef]
- Santomasso, B.D.; Nastoupil, L.J.; Adkins, S.; Lacchetti, C.; Schneider, B.J.; Anadkat, M.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; et al. Management of Immune-Related Adverse Events in Patients Treated With Chimeric Antigen Receptor T-Cell Therapy: ASCO Guideline. J Clin Oncol 2021, 39, 3978–3992. [Google Scholar] [CrossRef]
- Gong, Y.; Klein Wolterink, R.G.J.; Wang, J.; Bos, G.M.J.; Germeraad, W.T.V. Chimeric antigen receptor natural killer (CAR-NK) cell design and engineering for cancer therapy. Journal of Hematology & Oncology 2021, 14, 73. [Google Scholar] [CrossRef]
- He, J.; Yan, Y.; Zhang, J.; Wei, Z.; Li, H.; Xing, L. Synergistic treatment strategy: combining CAR-NK cell therapy and radiotherapy to combat solid tumors. 2023, 14. [CrossRef]
- Zhu, C.; Wu, Q.; Sheng, T.; Shi, J.; Shen, X.; Yu, J.; Du, Y.; Sun, J.; Liang, T.; He, K.; et al. Rationally designed approaches to augment CAR-T therapy for solid tumor treatment. Bioact Mater 2024, 33, 377–395. [Google Scholar] [CrossRef]
- Wang, W.; Liu, Y.; He, Z.; Li, L.; Liu, S.; Jiang, M.; Zhao, B.; Deng, M.; Wang, W.; Mi, X.; et al. Breakthrough of solid tumor treatment: CAR-NK immunotherapy. Cell death discovery 2024, 10, 40. [Google Scholar] [CrossRef]
- Sadeghi, S.; Chen, P.-C.; Jewett, A.; Kaur, K. Chapter 14 - Combination of NK cell immunotherapy with chemotherapy and radiation enhances NK cell therapy and provides improved prognosis in cancer patients and in humanized BLT mouse model system. In NK Cells in Cancer Immunotherapy: Successes and Challenges, Jewett, A., Fong, Y., Eds.; Academic Press: 2023; pp. 301-320.
- Fares, J.; Davis, Z.B.; Rechberger, J.S.; Toll, S.A.; Schwartz, J.D.; Daniels, D.J.; Miller, J.S.; Khatua, S. Advances in NK cell therapy for brain tumors. npj Precision Oncology 2023, 7, 17. [Google Scholar] [CrossRef]
- Kennedy, P.R.; Felices, M.; Miller, J.S. Challenges to the broad application of allogeneic natural killer cell immunotherapy of cancer. Stem Cell Res Ther 2022, 13, 165. [Google Scholar] [CrossRef]
Figure 1.
CAR-T and CAR-NK Cell Therapy Mechanisms Against Tumor Cells: The left side of the image represents CAR-NK cells, which recognize target antigens on the surface of tumor cells through CAR. These cells have 2B4 and DAP10/DAP12 as activating ligands and can secrete cytokines such as IFN-γ, IL-3, and GM-CSF. The right side represents CAR-T cells, which also recognize and bind to target antigens on tumor cells through the chimeric antigen receptor. CAR-T cells signaling molecules such as CD3ζ, CD28, and 4-1BB, and can secrete cytokines like IFN-γ, TNF-α, IL-1, and IL-6; the tumor cells in the center show their target antigens, which are the targets for recognition and binding by CAR-T and CAR-NK cells.
Figure 1.
CAR-T and CAR-NK Cell Therapy Mechanisms Against Tumor Cells: The left side of the image represents CAR-NK cells, which recognize target antigens on the surface of tumor cells through CAR. These cells have 2B4 and DAP10/DAP12 as activating ligands and can secrete cytokines such as IFN-γ, IL-3, and GM-CSF. The right side represents CAR-T cells, which also recognize and bind to target antigens on tumor cells through the chimeric antigen receptor. CAR-T cells signaling molecules such as CD3ζ, CD28, and 4-1BB, and can secrete cytokines like IFN-γ, TNF-α, IL-1, and IL-6; the tumor cells in the center show their target antigens, which are the targets for recognition and binding by CAR-T and CAR-NK cells.
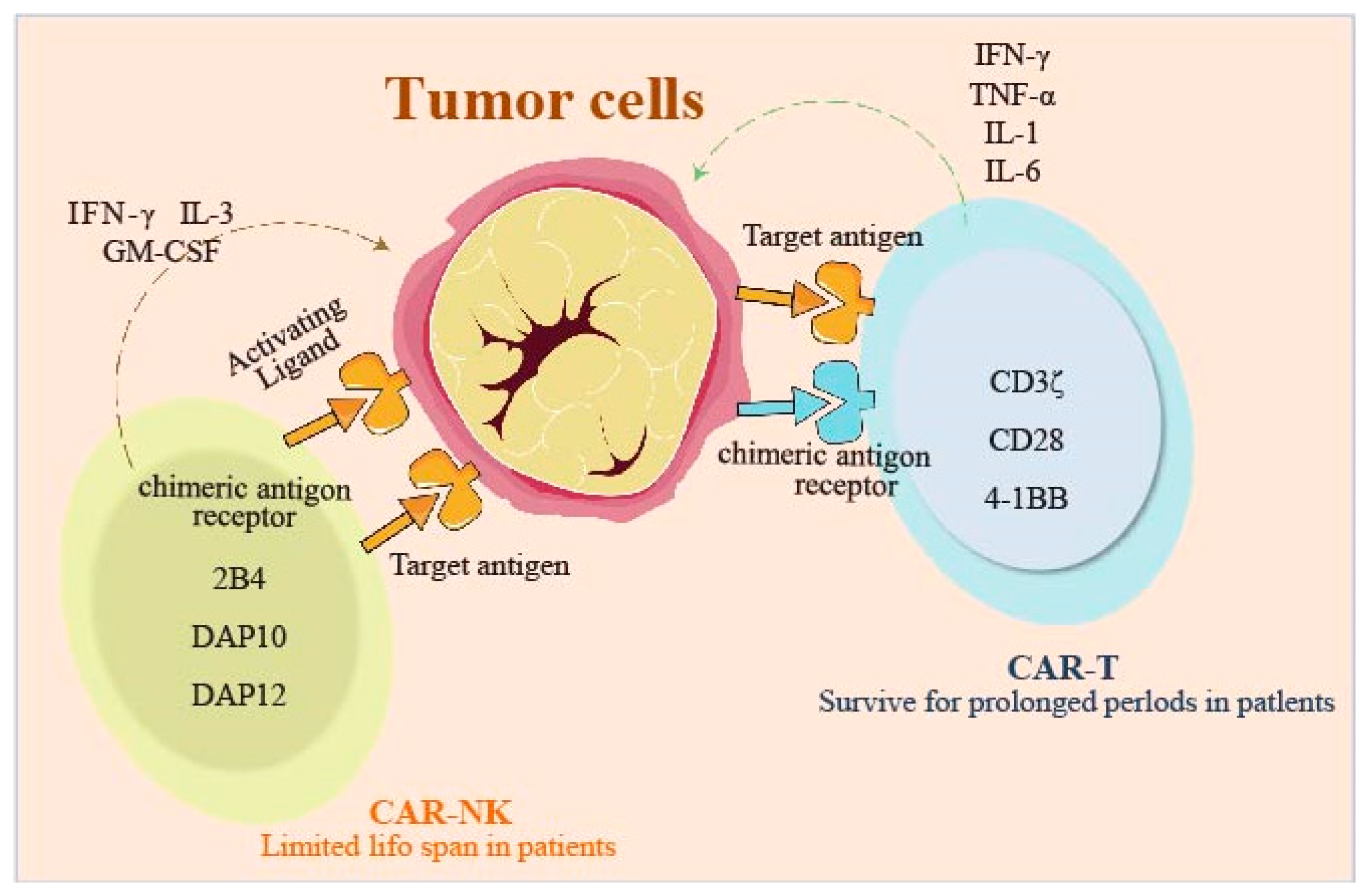
Figure 2.
Comparison of CAR T-cell and CAR NK-cell therapy processes. Figure illustrates the entire process from cell acquisition to disease targeting for both CAR T and CAR NK cell therapies. For CAR T cells, MHC matching is required to prevent rejection. For CAR NK cells, there is no need for MHC matching, simplifying the preparation process. Both undergo engineering, expansion, and are reintroduced into the patient to combat disease.
Figure 2.
Comparison of CAR T-cell and CAR NK-cell therapy processes. Figure illustrates the entire process from cell acquisition to disease targeting for both CAR T and CAR NK cell therapies. For CAR T cells, MHC matching is required to prevent rejection. For CAR NK cells, there is no need for MHC matching, simplifying the preparation process. Both undergo engineering, expansion, and are reintroduced into the patient to combat disease.
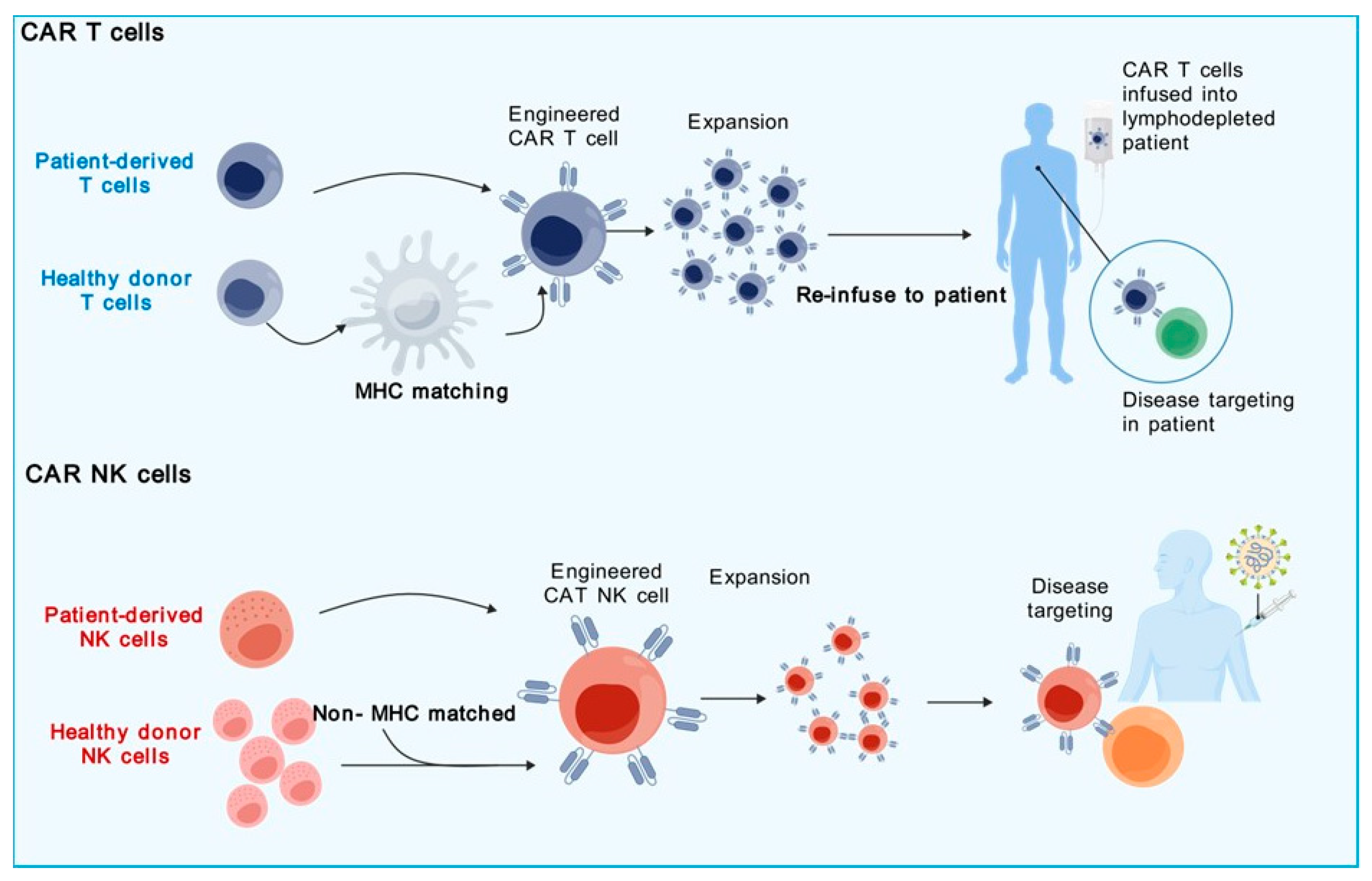
Figure 3.
Production Process of CAR-NK Cells from Various Starting Materials. The workflow begins with leukapheresis for PBMC collection, followed by CD3+ T cell depletion and activation with IL-2, IL-15, and IL-18. NK cells are isolated, cultured, and expanded. CD34+ cells are selected, expanded, and differentiated into NK cells using SCF, IL-7, and IL-15. The process concludes with cell culturing and patient infusion preparation, including lymphodepletion and IL-2 administration. An alternative pathway for CAR-NK cell derivation from iPSCs involves growth factors like SCF, VEGF, and BMP4.
Figure 3.
Production Process of CAR-NK Cells from Various Starting Materials. The workflow begins with leukapheresis for PBMC collection, followed by CD3+ T cell depletion and activation with IL-2, IL-15, and IL-18. NK cells are isolated, cultured, and expanded. CD34+ cells are selected, expanded, and differentiated into NK cells using SCF, IL-7, and IL-15. The process concludes with cell culturing and patient infusion preparation, including lymphodepletion and IL-2 administration. An alternative pathway for CAR-NK cell derivation from iPSCs involves growth factors like SCF, VEGF, and BMP4.
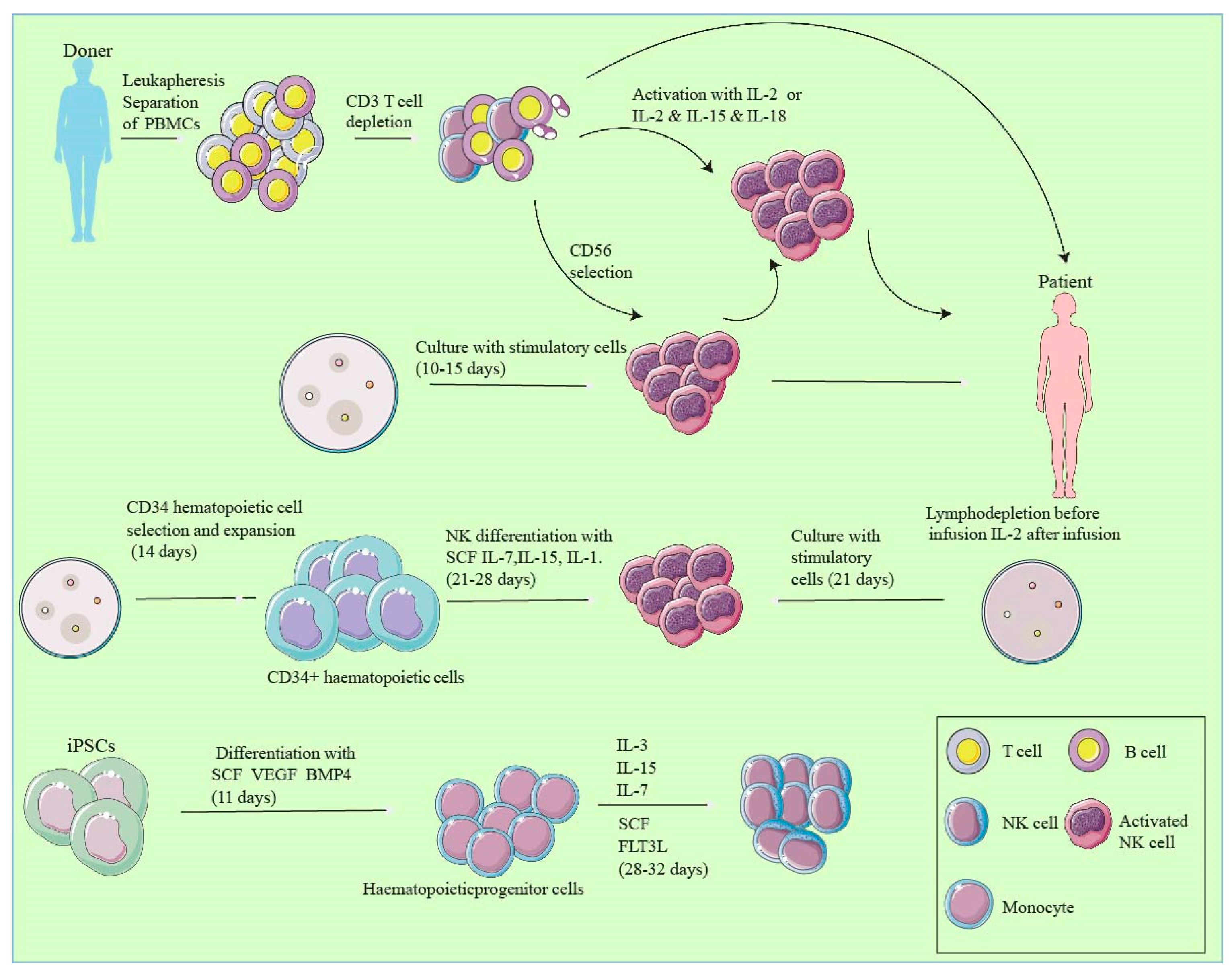
Figure 4.
Multifaceted Mechanisms of CAR-NK Cell Therapy in the Tumor Microenvironment. This illustration demonstrates key advancements such as genetic disruption of immune checkpoints in monocytes, ectopic expression of chemokine receptors for improved NK cell trafficking, and neutralization of extracellular GM-CSF to increase safety. Also depicted are metabolic reprogramming techniques to prevent functional exhaustion, cytokine preconditioning for NK cell memory enhancement, and the targeted ablation of endogenous NK cell proteins to optimize combination therapy efficacy.
Figure 4.
Multifaceted Mechanisms of CAR-NK Cell Therapy in the Tumor Microenvironment. This illustration demonstrates key advancements such as genetic disruption of immune checkpoints in monocytes, ectopic expression of chemokine receptors for improved NK cell trafficking, and neutralization of extracellular GM-CSF to increase safety. Also depicted are metabolic reprogramming techniques to prevent functional exhaustion, cytokine preconditioning for NK cell memory enhancement, and the targeted ablation of endogenous NK cell proteins to optimize combination therapy efficacy.
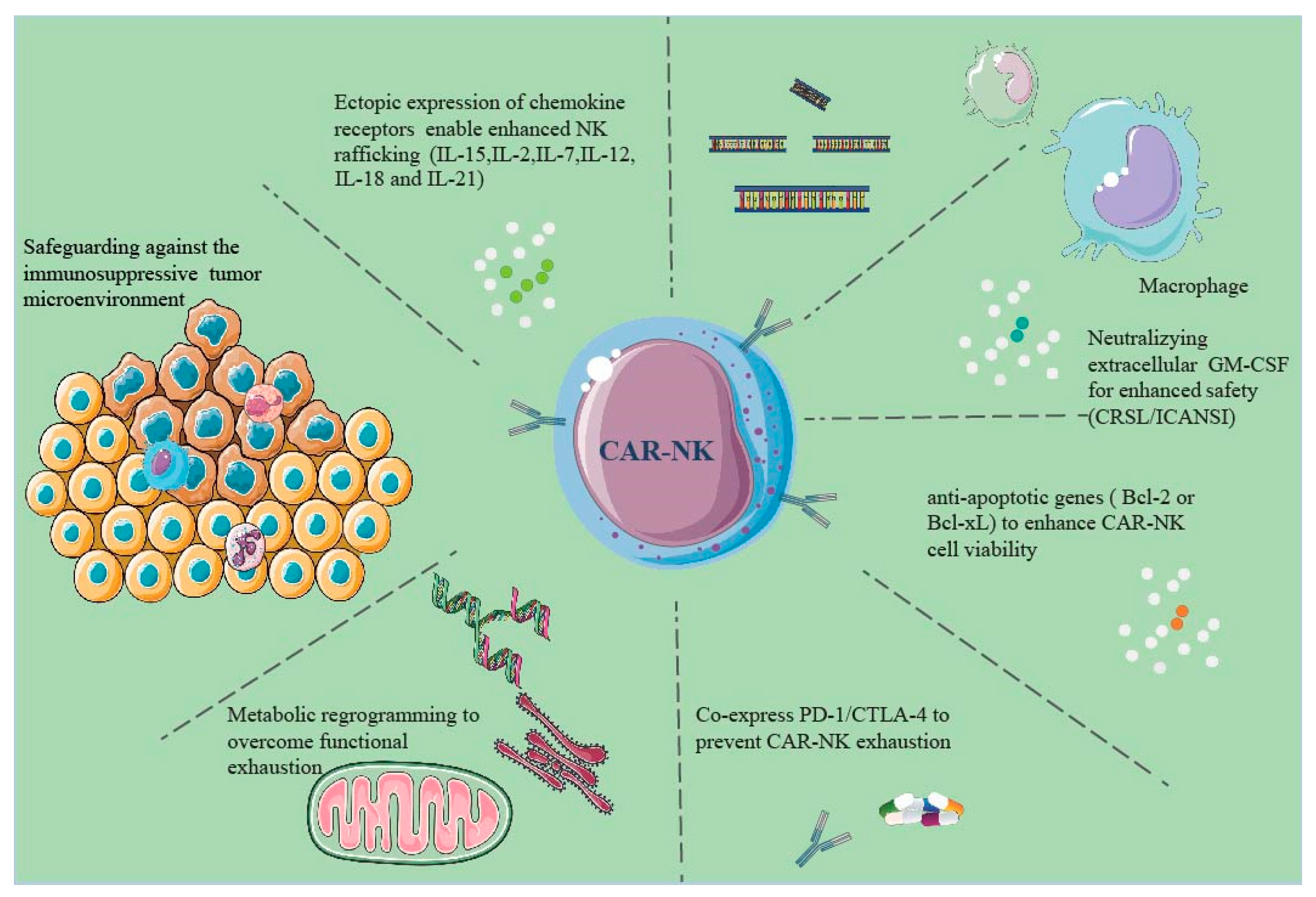
Table 2.
Comparison between CAR-T and CAR-NK Cells.
| Parameter | CAR-T Cells | CAR-NK Cells |
|---|---|---|
| Intracellular Signaling Domains | CD3ζ with co-stimulatory domains such as CD28 and 4-1BB | Like CAR-T structure but can utilize NK-specific signaling domains like 2B4, DAP10, DAP12. |
| Cell Source | Autologous or MHC-matched allogeneic | Autologous, non-MHC matched allogeneic cell lines, or NK cell lines |
| Off-the-shelf Ready-to-use CAR Product | Typically, autologous, or MHC-matched allogeneic CAR-T cells | NK cell lines. Allogeneic NK cells possible, but with poor recovery rate post-cryopreservation |
| In Vitro Expansion Capability | Yes | Yes Pre-Expansion Prior to Transduction |
| Cell Killing Mechanism | CAR-dependent cellular cytotoxicity | Both CAR-dependent and CAR-independent NK cell-mediated cytotoxicity |
| Cytokine Release Syndrome and Neurotoxicity | Common and usually severe | Less common |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



