
Submitted:
14 June 2024
Posted:
14 June 2024
You are already at the latest version
Abstract
The objective was to compare the color match and color stability behavior of single and multishade resin-based composites (RBCs) used for direct restorations. This review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Randomized clinical trials evaluating the shade performance of single-shade RBCs in direct restorations were included. A search of the scientific literature was performed in 5 databases (April 2024). The meta-analysis was performed using RevMan 5.4, calculating the risk difference (RD) and 95% confidence interval (CI) of the dichotomous outcome using a random effects model. Bias was assessed using the RoB 2.0 tool, and certainty of evidence was assessed using the GRADE tool. Four studies with 263 restorations analyzed were selected. The results showed comparable performance between single-shade RBCs and multishade RBCs in terms of color match and color stability over 12 months. Three studies had a low risk of bias with all expected results, and one study had some concerns. The certainty of evidence for color stability was considered low for all follow-up periods due to the small number of events and sample size. According to the United States Public Health Service Evaluation (USPHS) and the World Dental Federation (FDI), there is comparable clinical color performance between single-shade and multishade RBCs over 12 months.
Keywords:
Composite resins
; dental materials
; permanent dental restoration
; color
; color perception
; systematic review
; randomized controlled trial
1. Introduction
Resin-based composites (RBCs) have emerged as the preferred aesthetic material for dental restorations in both anterior and posterior teeth [1]. However, achieving color harmony between the composite resin and the adjacent dental substrate poses a significant challenge [2]. The effectiveness of a restoration is closely related to its surface properties and color stability [3]. Given the subjective nature of color matching, accurate shade selection remains a formidable task in recreating the natural appearance of dental elements [4]. The proposed technique for achieving color involves selecting a resin from various types of hues, chroma, and luminosity, as well as different optical properties such as opacity, translucency, and opalescence, which requires time and increased cost [5]. Consequently, there is an urgent need to continuously refine techniques that simplify the process of composite resin color selection, thereby reducing clinical protocols and chair time [6].
According to dentists, tooth color is the second most influential factor in smile preference and, along with tooth arrangement, is one of the first features noticed by patients when they smile [7]. The lighter the tooth color is, the more attractive the smile is [8]. This highlights the importance of achieving the correct shade of resin during the restorative procedure. In addition, the resin must exhibit color stability in the oral cavity; therefore, esthetic restoration failure due to discoloration is a relevant clinical issue [9]. Errors in shade selection and pigmentation are easily noticed by patients, negatively affecting their perception and leading to the need for restoration repair or replacement [10]. Replacement of restorations is costly and carries the risk of sacrificing healthy tooth structure, which may compromise tooth vitality and accelerate the destructive tooth cycle [11].
Dental materials that can adapt to human tooth color offer numerous advantages, including aesthetic enhancement, reduced reliance on shade guides and reduced risk of shade mismatch [1]. This adaptability, often referred to as the "chameleon effect" [12], has led to the emergence of single-shade RBCs equipped with "smart shade technology" [8]. This "chameleon effect" is made possible by the ability of the resin to absorb light from the surrounding tooth [5]. These materials promise to capture the adjacent coloration of restored dental elements, facilitated by particles that produce red/yellow hues that blend with the surrounding coloration, complemented by uniformly sized spherical particles that adjust the transmitted color [8]. This new ability imparted to resins means that the perceived color of a region shifts toward the color of the surrounding area, eliminating or neutralizing color discrepancies between the tooth and the restoration [5]. In addition, single-shade RBCs streamline the color selection process by eliminating the need to choose between different resin shades, as is the case with multishade RBCs, thus reducing the time lost in the clinical resin selection process [13]. These materials are able to match all the shades in the Vita Classic Shade Guide [14].
While in vitro studies indicate comparable color matching between single-shade and multishade RBCs [12,13], others indicate better color matching with single-shade RBCs [6]. In addition to comparable performance in terms of their ability to match the surrounding tooth substrate, restorations with single-shade RBCs were significantly whiter than those with the original tooth shade [15]. Single-shade RBCs have greater chroma adjustment potential than multishade resins, enabling them to match a wide range of human tooth shades. However, this ability may be compromised in deep restorations due to increased translucency and structural coloration, resulting in light reflection, even at longer wavelengths [16]. In addition, there are concerns regarding the color stability of single-shade resins. In vitro studies have shown that they are susceptible to discoloration from commonly consumed beverages such as wine, coffee and black tea [3,17,18]. Conversely, clinical studies indicate that the color stability is comparable to that of multishade resins [1,19]. Therefore, there is a need to understand the clinical color behavior of single-shade RBCs in terms of color matching and stability.
Based on current evidence from clinical and laboratory studies, there is a lack of definitive understanding of the favorable clinical color behavior of single-shade RBCs, leading to uncertainties regarding their suitability for clinical use. There is limited evidence for the in vivo color stability of single-shade RBCs, and therefore, there is an urgent need for an evidence synthesis study that merges data from multiple primary clinical investigations. Such an effort aims to provide robust and reliable scientific evidence on the color matching and color stability of this novel material. This initiative aims to provide stronger scientific support for the color match of this innovative restorative material and to either confirm or challenge its suitability for use. The aim of this systematic review was to compare the clinical color matching and stability of single and multishade RBCs in direct restorations.
2. Materials and Methods
2.1. Protocol and Registration
This systematic review was conducted following the guidelines of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [20] and was structured as follows: (1) identification of the guiding question, (2) collection of relevant studies, (3) determination of inclusion and exclusion criteria, (4) data extraction, and (5) synthesis of the results [21]. Prior to commencement, the methodology of this study was registered in PROSPERO (International Prospective Register of Systematic Reviews) with the protocol number CRD42024529670.
2.2. Eligibility Criteria
The guiding question for this review was "Do single-shade RBCs have shade performance comparable to that of multishade resin composites in direct restorations?" The population/problem, intervention/exposure, comparison, and outcome of the study were guided by the PICOS strategy. The Population/participants (P) consisted of patients with anterior or posterior restorations. The Intervention (I) analyzed was direct restoration with Single-shade RBC, and the Comparator (C) was multi-shade RBC. The evaluated Outcome (O) was color match. The study design (S) was Randomized Clinical Trial.
The study inclusion criteria were as follows: (1) randomized clinical trial; (2) evaluation of the color match of single-shade RBCs in direct restorations; (3) use of the United States Public Health Service (USPHS) criteria and World Dental Federation (FDI) criteria to evaluate the clinical color match of the RBCs; and (4) use of multishade RBCs as comparative material. The exclusion criteria were as follows: (1) studies evaluating color matching with other methods; (2) in vitro studies; (3) studies using experimental single-shade RBCs; (4) unpublished information in the scientific literature; (5) studies for which the full text was not available; and (6) retrospective studies.
2.3. Information Sources and Search Strategy
The PubMed, Embase, Web of Science, Scopus, and Cochrane Library databases were searched for clinical studies evaluating the color stability of single-shade RBCs in direct restorations on April 2024. The following Medical Subject Headings (MESH) or text words were used: single-shade composite, monoshade universal composite, monochromatic composite, permanent dental restoration, permanent dental filling, randomized controlled trials as topic, randomized clinical trial, clinical trial, clinical data, clinical studies as topic, medical trial, intervention study, intervention trial, interventional study, and interventional trial. The following search was performed across all databases: [("single-shade composite" OR "mono-shade universal composite" OR "monochromatic composite") AND ("restorations, permanent dental" OR "restoration permanent dental" OR "dental permanent filling" OR “dental permanent fillings”)] AND [(“Randomized Controlled Trials as Topic” OR “Clinical Trials, Randomized” OR “Trials, Randomized Clinical” OR “Controlled Clinical Trials, Randomized” OR “Randomized Controlled Trial” OR “clinical trial” OR “clinical data” OR “clinical studies as topic” OR “medical trial” OR “intervention study” OR “intervention studies” OR “intervention trial” OR “interventional studies” OR “interventional study” OR “interventional trial”)] (Table 1).
2.4. Selection Process
The studies were stored and systematically organized using an online program (Rayyan, Qatar Computing Research Institute). Duplicates were first removed, and then the titles and abstracts were read to determine whether the studies met the predefined criteria. The selection process was carried out independently by two authors (CFCL and SBM) who were previously calibrated, and discrepancies were discussed with a third author (MAJRM). The calibration process facilitated by the two authors (CFCL and SBM) involved the joint reading and assessment of 10 articles to ensure congruence in the interpretation and application of the selection criteria. This collaborative review promoted a consistent approach to article selection based on predetermined criteria. Any disagreements that arose during independent selection were resolved through discussion and consensus with the third author (MAJRM). Eligible articles were carefully read, and their data were carefully extracted.
2.5. Data Collection Process
Two authors (CFCL and SBM), who were previously calibrated, performed the data extraction using a guide table covering the main methodological characteristics of the studies. Key data included author/year, RBCs used, number of subjects and age range, number of restored teeth, type of restored tooth, finishing and polishing protocol, light curing unit, type of restoration, follow-up period, analysis criteria, and conclusion.
2.6. Assessment of Study Risk of Bias
The included trials were assessed for risk of bias by two authors (CFCL and SBM), who had been previously calibrated. The assessment used the Cochrane Risk of Bias for Randomized Trials version 2 (RoB 2) tool, which includes domains assessing bias related to the randomization process, deviations from intended interventions, missing outcome data, measurement of outcomes, and selection of reported outcomes. Each domain is accompanied by signaling questions designed to systematically request relevant information for bias assessment, with responses categorized as yes, probably yes, probably no, no, or no information. Following the completion of the signaling questions, a risk of bias judgment was made, which was categorized as low risk of bias, some concerns, or high risk of bias. The RoB 2 tool contains algorithms that connect responses to signaling questions with suggested risk of bias assessments for each domain. In cases of disagreement between the two assessors, a third assessor was consulted to reach a consensus (MAJRM).
2.7. Effect Measures and Synthesis Methods
The meta-analysis was performed using a random-effects model. Review Manager version 5.4 (Review Manager 5.4, The Cochrane Collaboration) software was used to calculate the risk difference with a 95% confidence interval. The data were dichotomized for this analysis. Acceptable restorations were those that received the Alpha and Bravo scores for the USPHS criteria and scores of 1, 2 and 3 for the FDI criteria. The unacceptable restorations were those that received Charlie score when the USPHS criteria were applied and those with scores of 4 and 5 when the FDI criteria were used to evaluate color stability. The unacceptable data were used in the meta-analysis. This analysis was performed with two subgroups according to the follow-up period: one considered the baseline (1 to 7 days), and the other considered after 12 months. Table 2 shows the USPHS and FDI grading criteria.
2.8. Certainty Assessment
The certainty of evidence for each outcome was evaluated utilizing the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) tool, accessible at http://www.gradeworkinggroup.org/. This tool evaluates the study design and considers factors such as risk of bias, imprecision, inconsistency, indirectness of evidence, and publication bias to potentially determine the quality of evidence. Each aspect is assessed as having "no limitation," "serious limitations," or "very serious limitations," allowing for the classification of evidence quality as high, moderate, low, or very low. A lower quality indicates that the estimate may differ substantially from the true effect.
3. Results
3.1. Study Selection
A total of 31 studies were extracted from the databases in the search conducted in April 2024. After removing duplicates, 22 studies remained, and their titles and abstracts were analyzed according to the predefined inclusion and exclusion criteria. The full texts of 10 potentially eligible studies were read, 4 of which met the selection criteria (Figure 1). One study was excluded for assessing color behavior on a typodont [22], another for evaluating color on a denture [23], three studies were retrospective [14,24,25], and the last study was a clinical report study [26].
3.2. Study Characteristics
The characteristics of the studies are shown in Table 3. The included articles were published between 2022 and 2024. The number of participants ranged from 20 to 70. The age of the subjects ranged from 43 to 58 years, with follow-up periods ranging from 3 days to 1 year [1, 19, 26, 27]. The countries where the trials were conducted were Egypt [1,28], Brazil [27], and India [19].
The total number of patients treated and teeth restored was 141 and 236, respectively. One study included class IV restorations [28], one study included full coronal aesthetic restorations [19], one study included noncarious cervical lesions [27], and one study included occlusal restorations [1]. The restored dental elements included permanent anterior and posterior teeth and primary anterior teeth. Of the selected studies, only Miranda et al. [27] used the FDI criteria, and the others used the USPHS. The single-shade RBCs used were Filtek Universal [28], Omnichroma [1,19], and Admira Fusion X-tra [27]. The multishade RCBs used were Filtek z350 xt [28], Tetric N Ceram [1,19], and Admira Fusion [27]. All studies reported the use of absolute isolation. The light-curing units used were an Elipar S10 [26], a Bluephase meter II [27], and a Bluephase Style [1]. One study did not report the light-curing device used [19]. All studies cured for 20 seconds per increment.
Regarding the method of resin color selection, the polychromatic technique used in the study by Hashem, Kairy and Shaalan [28] involved the application of a palatal layer of enamel resin, followed by subsequent layers of dentin and enamel resin. However, the color scale used was not reported. Miranda et al. [27] used a shade guide from the Admira Fusion kit for shade selection, using combinations of two or more shades when necessary. Zulekha et al. [19] reported color selection for the control group only but did not detail the methodology used. Anwar et al. [1] did not clarify the method of color selection. In terms of finishing and polishing techniques, Hashem, Kairy and Shaalan [28] initially used yellow-coded diamond finishing stones, Soflex discs, Perio-Bur #831, rubber cups, flames, and wheel polishing tips. Miranda et al. [27] employed fine and extrafine #2200 diamond burs and OptraPol NG. Sulekha et al. [19] did not report the specific finishing and polishing technique used. Anwar et al. [1] used low-speed fine grit diamond finishing stones supplemented with EVE DIACOMP Plus Occuflex impregnated rubber cups and impregnated brushes following a recommended sequence (coarse, medium, fine, and superfine).
3.3. Risk of Bias in Studies
The RoB 2 tool was used for the randomized clinical trials. Zulekha et al. [19] did not describe the randomization process. Hashem, Khairy and Shalaan [28] and Anwar et al. [1] used the site “randomization.com”. Miranda et al. used the site “sealenvelope.com”. Regarding the blinding of participants, examiners, and staff, Hashem, Khairy and Shalaan [28], Miranda et al. [27] used opaque sealed envelopes. Zulekha et al. [19] presented incomplete data on allocation knowledge by outcome assessors and patients. Three [1,27,28] studies exhibited a low risk of bias, with all expected results and planned analyses documented, and one [19] exhibited some concerns regarding blinding and allocation of participants/personnel/outcome assessor (Figure 2).
For the meta-analysis, studies using the United States Public Health Service (USPHS) criteria were extracted for the proportion of restorations considered with worse scores (Charlie), and studies using the World Dental Federation (FDI) were extracted for restorations with equivalent worse scores (scores 4 and 5) according to the following criteria: color match. Four studies were included. No statistically significant differences (p>0.05) were found between single-shade and multishade resins for 1 to 7 days (p= 1.0; RD= 0.00; 95% CI -0.03 - 0,03; I2= 0%) or 12 months (p=0.61; RD= -0,01; 95% CI -0.09, 0.07; I2=0%) (Figure 3).
3.4. Certainty of Evidence
Table 4 shows that the certainty of the evidence of color stability was low for all follow-up periods. Although the included studies had a low risk of bias, issues of indirectness and imprecision were deemed significant due to sample size limitations (fewer than 300 for dichotomous outcomes). Consequently, the certainty of evidence was reduced due to the small number of events and the small sample size.
4. Discussion
For direct restorations with RBCs, color selection is an important phase. Due to the characteristics of natural teeth, it is necessary to choose the right shade of composite to achieve esthetic procedures. The aim of this systematic review and meta-analysis was to investigate the shade performance of single-shade RBCs) in direct restorations. This was achieved by evaluating restorations using clinical instruments such as the USPHS and FDI criteria, taking into account scores indicating failure (Charlie, score 4, and score 5). Two follow-up periods were analyzed: one ranging from 1 to 7 days and the other after 12 months. The first follow-up period allowed us to assess the color match of the restorations, while the second period provided information on the long-term clinical color stability of the RBCs examined. The results of the meta-analysis showed that single-shade RBCs performed similarly to multishade RBCs at both time points.
The single-shade RBCs used in the studies included in this systematic review were Filtek Universal [28], Omnichroma [1-19], and Admira Fusion X-tra [27]. Table 5 shows the composition of the single-shade RBCs. The Filtek Universal RBCs feature NaturalMatch technology and offer eight designer shades and an extrawhite option that effectively covers the 19 VITA Classic and Bleach shades [29]. Omnichroma RBC features Smart Chromatic Technology, which makes it possible to reproduce the shades of the entire Vita shade range from A1 to D4 [30]. Admira Fusion X-tra is a single-shade bulk fill resin with nanohybrid particles and ORMOCER technology. Admira Fusion X-tra is a single-shade bulk-fill resin with only one shade, as the designer nanoparticles neither diffract nor refract light [31].
All single-shade RBCs tested showed comparable color matches to those of the multishade resins over the 1- to 7-day period. This is an important feature, as color is a key factor in smile preference for both dentists and patients. Errors in color selection can lead to patient dissatisfaction and the need for costly replacement restorations, putting healthy tooth structures at risk [11]. Filtek Universal has nonaggregated and nonaggregated 20 nm silica fillers, where these particles may contribute to the opacity that explains the acceptable shade matching potential found in this systematic review [28]. NaturalMatch Technology consists of nanoparticles, pigments, and low-stress monomers that contribute to the formation of "white lines" at the margins [29]. Uniform spherical Omnichroma RBCs measuring 260 nm are capable of transmitting red-to-yellow color when ambient light passes through the resin [32]. As the red-to-yellow color is produced, it blends with the surrounding tooth color in an additive color mixing process, maximizing the ability of Omnichroma to mimic the color of the dental element without the need for pigments [30], which is consistent with our results. Admira Fusion X-tra contains spherical and uniformly sized nanoparticles that prevent diffraction or refraction of light. These nanoparticles allow light to pass through them and reach the surface of the tooth. The light is then reflected to the human eye, influenced by the adjacent tooth color [31], justifying the results of this systematic review.
Studies show that the blending effect is increased by increasing the translucency, as this property allows the composite to mimic the shade of the neighboring dentin and enamel [33]. Filtek Universal RBCs contain nanoclusters, which may be responsible for translucency and light transmission [28]. The high translucency of Omnichroma is due to a specific combination of the type (uniform spherical particles) and fraction (79%) of the inorganic phase. The absence of colorants in Omnichroma reduces energy attenuation or loss in the material, which justifies its exceptional translucency [34]. The Admira Fusion X-tra shade is 45.56% more translucent than the dentin shade and 27.5% more translucent than the enamel shade [33]. These characteristics support the findings of this study regarding color matching. The translucency required to enhance color matching appears to be a concern for aesthetic restorations [1]. Miranda et al. [27] reported that color matching was achievable regardless of the degree of dentin sclerosis. It is important to note that to achieve favorable color results with multishade resin restorations, the operator must be trained to use the incremental technique with different shades, which is not necessary when using single-shade resin [27].
The evaluation of the success of restorative therapy probably depends on the durability of the restorations [19]. One of the parameters associated with durability is color stability. All the single-shade RBCs investigated showed comparable color stability to that of the multishade resins during the 12-month follow-up period. Finishing and polishing procedures for resin composite restorations are essential steps to improve the appearance, color stability and longevity of the restorations [28]. Almost all included studies mentioned the finishing and polishing techniques, except for Zulekha et al. [19], who did not mention whether this step was performed or how it was carried out. The RBCs studied have similar filler contents and contain nanospherical filler particles, which provide a smoother finish to the restoration and fewer spaces between the resin-filler interface, reducing bacterial adhesion and microleakage and consequently minimizing staining over time [19]. Another factor that may be related to color stability is the size of the particles; when they are small, they contribute to less staining and improved esthetic properties [26]. In a retrospective study, a single-shade resin-based composite (RBC) achieved a 100% acceptable color match after 4 years in previous restorations for diastema closure and contouring [14]. Color mismatch was the least common cause of restoration failure identified by Korkut et al. [26] in a retrospective study evaluating the performance of single-shade RBCs in Class IV cavities. Only one restoration had the lowest score after 4 years of follow-up [26].
Based on the results of this study, single-shade RBCs exhibited similar color characteristics to multishade RBCs. These findings can help clinicians support the use of dental materials that mimic and harmonize with natural tooth shades, providing color stability. The majority of the studies included in this systematic review had a low risk of bias, but the certainty of the evidence was rated as low due to the small number of events and sample size, which may not have provided sufficient evidence. Only one study [19] showed some concerns about the blinding and allocation of participants/personnel/outcome assessors. The limitations of this study are related to the length of follow-up, which was only up to one year. At least a decade of observation is required to accurately assess differences in treatment efficacy, as restorative materials may have different failure rates over time [35]. Nevertheless, this topic remains relatively unexplored in the literature, mainly due to the lack of randomized clinical trial (RCT) studies. Several studies included in the meta-analysis used the USPHS criteria, which are known for their limited sensitivity in definitively assessing the success of a restorative procedure [36]. Conversely, the FDI criteria have been shown to be more sensitive and accurate than the USPHS standards in identifying subtle differences in clinical studies [37]. The conclusions drawn from this systematic review and meta-analysis should be treated with caution due to the limited availability of clinical studies. We advocate the conduct of additional randomized clinical trials to assess the clinical performance of these resins, particularly with longer follow-up periods, as initial evaluations tend to have fewer events.
5. Conclusions
This systematic review and meta-analysis revealed that the color match and color stability of direct restorations with single-shade RBCs were similar to those of direct restorations with multishade RBCs over a 12-month period. However, these results should be considered with caution due to the low certainty of evidence regarding small events and the small sample used in the included studies.
Author Contributions
C.F.C.L. and S.B.M. contributed to the study conception and design, and C.F.C.L. and R.B.E.L., for the material preparation and data collection. A.K.M.A. performed the statistical analysis. A.K.M.A. and M.A.J.R.M. critically revised the manuscript and supervised the review process. The first draft of the manuscript was written by C.F.C.L., S.B.M. and R.B.E.L. All authors commented on previous versions of the manuscript. All the authors have read and approved the final manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All the data are available within the manuscript.
Conflitcts of Interest
The authors declare no conflicts of interest.
References
- Anwar, R.S.; Hussein, Y.F.; Riad, M. Optical behavior and marginal discoloration of a single shade resin composite with a chameleon effect: A randomized controlled clinical trial. BDJ Open (2024), 10, 11. [CrossRef]
- Barros, M.S.; Silva, P.F.D.; Santana, M.L.C.; Bragança, R.M.F.; Faria-E-Silva, A.L. Background and surrounding colors affect the color blending of a single-shade composite. Braz Oral Res (2023), 28,37:e035. [CrossRef]
- Rohym, S.; Tawfeek, H.E.M.; Kamh, R Effect of coffee on color stability and surface roughness of newly introduced single shade resin composite materials. BMC Oral Health (2023), 22, 23, 236. [CrossRef]
- Hardan, L.; Bourgi, R. Cuevas-Suárez, C.E.; Lukomska-Szymanska, M.; Monjarás-Ávila, A.J.; Zarow, M. et al Novel Trends in Dental Color Match Using Different Shade Selection Methods: A Systematic Review and Meta-Analysis. Materials (Basel) (2022), 8, 468. [CrossRef]
- Oivanen, M.; Keulemans, F.; Garoushi, S.; Vallittu, P.K.; Lassila, L. The effect of refractive index of fillers and polymer matrix on translucency and color matching of dental resin composite. Biomater Investig Dent (2021) 1,8, 48-53. [CrossRef]
- Cruz da Silva, E.T.; Charamba Leal, C.F.; Miranda, S.B.; Evangelista Santos, M.; Saeger Meireles, S.; Maciel de Andrade, A.K. et al Evaluation of Single-Shade Composite Resin Color Matching on Extracted Human Teeth. Sci World J (2023) 26, 2023:4376545. [CrossRef]
- Jouhar, R.; Ahmed, N.; Ahmed, M.A.; Faheemuddin, M.; Mosaddad, S.A.; Heboyan, A. Smile aesthetics in Pakistani population: Dentist preferences and perceptions of anterior teeth proportion and harmony. BMC Oral Health (2024), 29, 24, 401. [CrossRef]
- Ahmed, M.A.; Jouhar, R; Khurshid, Z. Smart Monochromatic Composite: A Literature Review. Int J Dent (2022), 8, 2022:2445394. [CrossRef]
- Paolone, G.; Formiga, S.; De Palma, F.; Abbruzzese, L.; Chirico, L.; Scolavino, S.; Goracci, C.; Cantatore, G.; Vichi, A. Color stability of resin-based composites: Staining procedures with liquids-A narrative review. J Esthet Restor Dent (2022), 34, 6, 865-887. Epub 2022 Apr 9. [CrossRef]
- Demarco, F.F.; Collares, K.; Correa, M.B.; Cenci, M.S.; Moraes, R.R.; Opdam, N.J. Should my composite restorations last forever? Why are they failing? Braz Oral Res (2017), 28, 31, e56. [CrossRef]
- Blum, I.R.; Özcan, M. Reparative Dentistry: Possibilities and Limitations. Curr Oral Health Rep (2018), 5, 4, 264-269. Epub 2018 Sep 15. [CrossRef]
- Altınışık, H.; Özyurt, E. Instrumental and visual evaluation of the color adjustment potential of different single-shade resin composites to human teeth of various shades. Clin Oral Investig (2023), 27, 2, 889-896. [CrossRef]
- Cubukcu, I.; Gundogdu, I.; Gul, P. Color match analysis of single-shade and multishade composite resins using spectrophotometric and visual methods after bleaching. Dent Mater J (2023) 29, 42, 6, 826-834. [CrossRef]
- Korkut, B.; Türkmen, C. Longevity of direct diastema closure and recontouring restorations with resin composites in maxillary anterior teeth: A 4-year clinical evaluation. J Esthet Restor Dent (2023), 33, 4, 590-604. [CrossRef]
- Rosa, E.D.A.R.; Silva, L.F.V.D.; Silva, P.F.D.; Silva, A.L.F.E. Color matching and color recovery in large composite restorations using single-shade or universal composites. Braz Dent J (2024) 22, 35, e245665. [CrossRef]
- Yamashita, A.; Kobayashi, S.; Furusawa, K,; Tichy, A.; Oguro, R.; Hosaka, K.; Shimada, Y. et al Does the thickness of universal-shade composites affect the ability to reflect the color of background dentin? Dent Mater J (2023), 30, 42, 2, 255-265. [CrossRef]
- Ersöz, B.; Karaoğlanoğlu, S.; Oktay, E.A.; Aydin, N. Resistance of Single-shade Composites to Discoloration. Oper Dent (2022), 1, 47, 686-692. [CrossRef]
- Chen, S.; Zhu, J.; Yu, M.; Jin, C.; Huang, C. Effect of aging and bleaching on the color stability and surface roughness of a recently introduced single-shade composite resin. J Dent (2024), 143, 104917. [CrossRef]
- Zulekha; Vinay, C.; Uloopi, K.S.; RojaRamya, K.S.; Penmatsa, C.; Ramesh, M.V. Clinical performance of one shade universal composite resin and nanohybrid composite resin as full coronal esthetic restorations in primary maxillary incisors: A randomized controlled trial. J Indian Soc Pedod Prev Dent (2022), 40, 2, 159-164. [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med (2019), 6, 7, e1000097.
- Paolone, G.; Mazzitelli, C.; Josic, U. et al Modeling Liquids and Resin-Based Dental Composite Materials-A Scoping Review. Materials (Basel) (2022) 24, 15, 11, 3759. [CrossRef]
- Rauber, G.B.; Bernardon, J.K.; Vieira, L.C.C.; Baratieri, L.N. Evaluation of a technique for color correction in restoring anterior teeth. J Esthet Restor Dent (2017), 29, 5, 309-316. Epub 2017 Jul 22. [CrossRef]
- de Abreu, J.L.B.; Sampaio, C.S.; Benalcázar Jalkh, E.B.; Hirata, R. Analysis of the color matching of universal resin composites in anterior restorations. J Esthet Restor Dent (2021), 33, 2, 269-276. [CrossRef]
- Korkut, B.; Özcan, M. Longevity of Direct Resin Composite Restorations in Maxillary Anterior Crown Fractures: A 4-year Clinical Evaluation. Oper Dent. (2022), 1, 47, 2, 138-148. PMID: 35604829. [CrossRef]
- Korkut, B.; Ünal, T.; Can, E. Two-year retrospective evaluation of monoshade universal composites in direct veneer and diastema closure restorations. J Esthet Restor Dent (2022), 35, 3, 525-537. Epub 2022 Dec 7. [CrossRef]
- Romero, M.F. Esthetic anterior composite resin restorations using a single shade: Step-by-step technique. J Prosthet Dent (2015), 114, 1, 9-12. [CrossRef]
- Miranda, A.O.; Favoreto, M.W.; Matos, T.P.; Castro, A.S.; Kunz, P.; Souza, J.L. et al. Color Match of a Universal-shade Composite Resin for Restoration of Noncarious Cervical Lesions: An Equivalence Randomized Clinical Trial. Oper Dent (2024), 1,49, 1, 20-33. [CrossRef]
- Hashem, B.B.; Khairy, M.A.; Shaalanm, O.O. Evaluation of shade matching of monochromatic versus polychromatic layering techniques in restoration of fractured incisal angle of maxillary incisors: A randomized controlled trial. J Inter Oral Health (2023), 15,1, 43-51. [CrossRef]
- 3 M. Filtek universal restorative: Technical product profile. (2019) https://multimedia.3m.com/mws/media/1651107O/3m-filtek-universal-restorative-technical-product-profile.pdf. Accessed 05 May 2024.
- Tokuyama. Omnichroma: Technical report. (2024) https://omnichroma.com/us/wp-content/uploads/sites/4/2019/01/OMNI-Tech-Report-Color-Final.pdf Accessed 05 May 2024].
- VOCO. Admira Fusion x-tra: Simplicity in one shade. (2024) https://www.voco.dental/us/portaldata/1/resources/products/folders/us/AF_x-tra_single_pages-01-2020_US_Product_Lit_FINAL_1-14-20.pdf. Accessed 05 May 2024.
- de Abreu , J.L.B.; Sampaio, C.S.; Benalcázar Jalkh, E.B.; Hirata, R. Analysis of the color matching of universal resin composites in anterior restorations. J Esthet Restor Dent (2021), 33, 2, 269-276. Epub 2020 Sep 29. [CrossRef]
- Batista, G.R.; Borges, A.B.; Zanatta, R.F.; Pucci, C.R.; Torres, C.R.G. Esthetical Properties of Single-Shade and Multishade Composites in Posterior Teeth. Int J Dent (2023), 12, 2023:7783321. [CrossRef]
- Lucena, C.; Ruiz-López, J.; Pulgar, R.; Della Bona, A.; Pérez, M.M. Optical behavior of one-shaded resin-based composites. Dent Mater (2021), 37, 5, 840-848. [CrossRef]
- Veloso, S.R.M.; Lemos, C.A.A.; de Moraes, S.L.D.; do Egito Vasconcelos, B.C.; Pellizzer, E.P.; de Melo Monteiro, G.Q. Clinical performance of bulk-fill and conventional resin composite restorations in posterior teeth: A systematic review and meta-analysis. Clin Oral Investig (2019), 23, 1, 221-233. [CrossRef]
- Arbildo-Vega, H.I.; Lapinska, B.; Panda, S. Clinical Effectiveness of Bulk-Fill and Conventional Resin Composite Restorations: Systematic Review and Meta-Analysis. Polymers (Basel) (2020), 10, 12, 8, 1786. [CrossRef]
- Azizi, F.; Ezoji, F.; Khafri, S.; Esmaeili, B. Surface Micro-Hardness and Wear Resistance of a Self-Adhesive Flowable Composite in Comparison to Conventional Flowable Composites. Front Dent (2023), 30, 20:10. [CrossRef]
Figure 1.
PRISMA Flow diagram of the literature search and selection criteria.
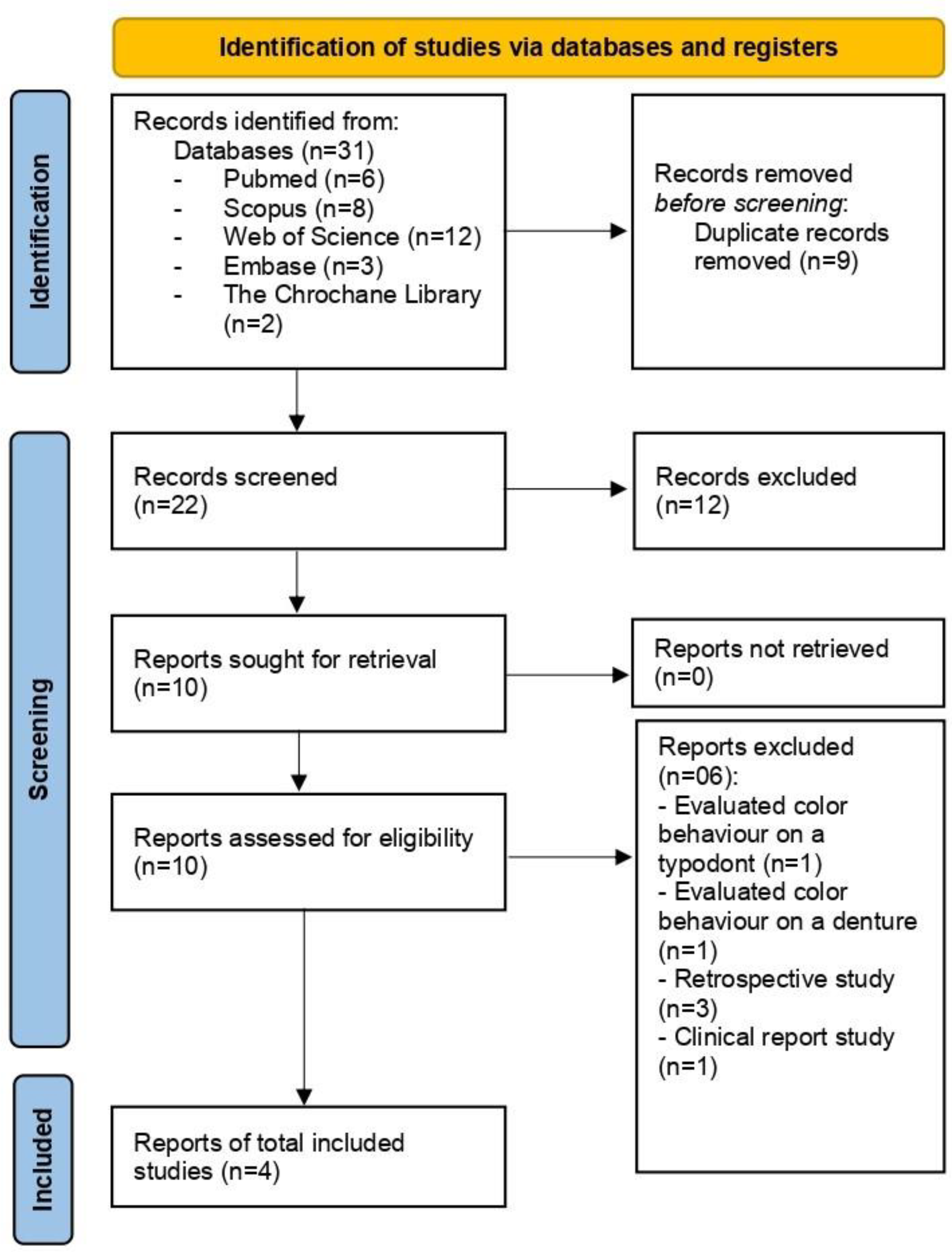
Figure 2.
Risk of bias analysis for the randomized clinical trials.
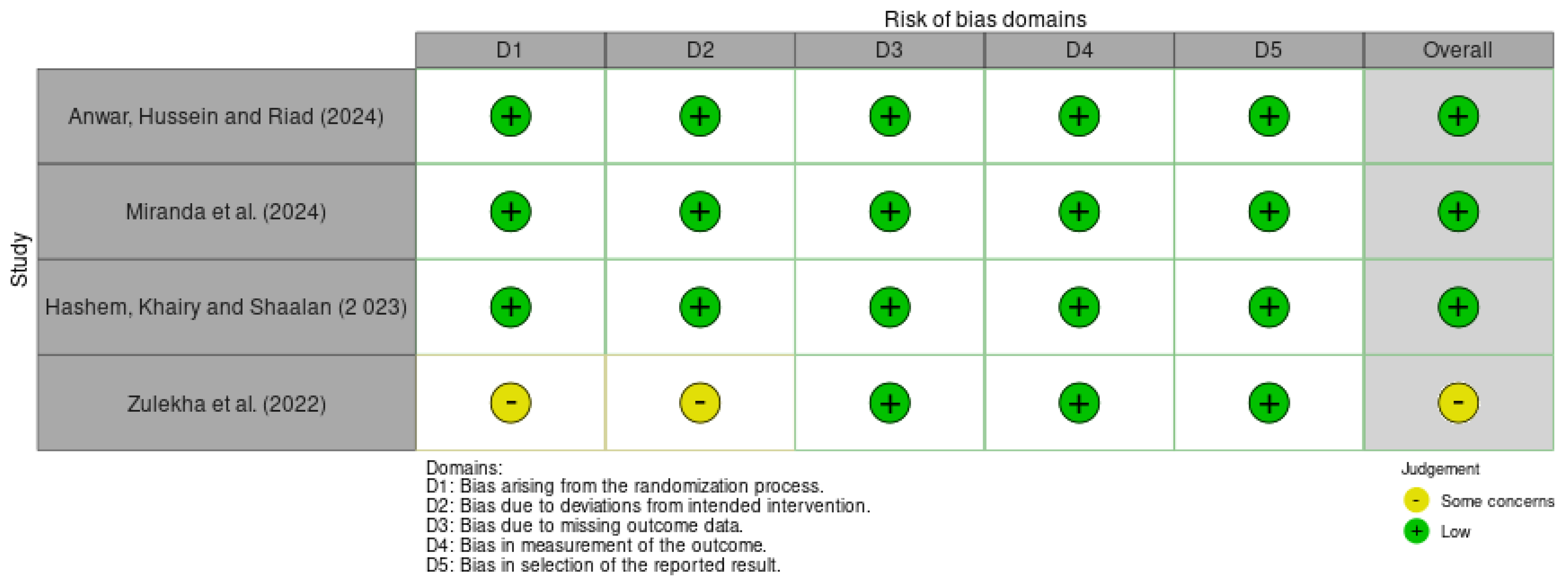
Figure 3.
Forest plot of color behavior.
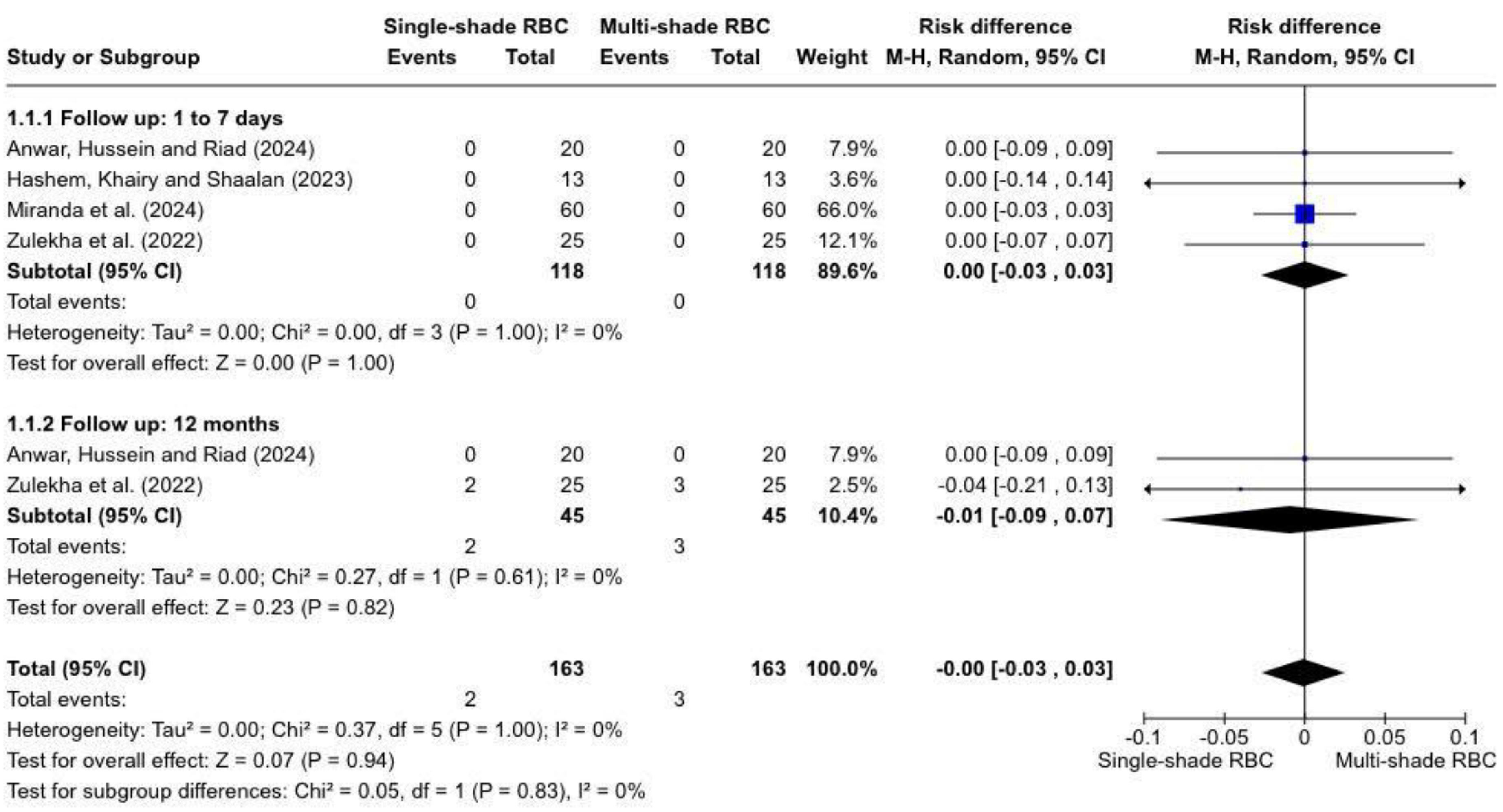

Table 1.
Search strategy.
| Database | Search strategy | Hits |
|---|---|---|
| Pubmed | (Single-shade [All Fields] AND (composite [All Fields] OR composites [All Fields])) OR (monoshade [All Fields] AND universal [All Fields] AND (composite [All Fields] OR composites [All Fields])) OR ((monochromatic [All Fields]) AND (composite [All Fields] OR composites [All Fields])) AND (dental restoration, permanent [MeSH Terms] OR dental restoration, permanent [MeSH Terms] OR dental restoration, permanent [MeSH Terms] OR dental restoration, permanent [MeSH Terms]) AND (Randomized controlled trials as topic [MeSH Terms] OR randomized controlled trials as topic [All Fields] OR clinical trials randomized [All Fields] OR clinical trials randomised [All Fields] OR trials randomized clinical [All Fields] OR trials randomised clinical [All Fields] OR controlled clinical trials randomized [All Fields] OR controlled clinical trials randomised [All Fields] OR randomized controlled trial [All Fields] OR randomised controlled trial [All Fields] OR clinical trial [All Fields] OR (clinical [All Fields] AND data [All fields]) OR clinical studies as topic [MeSH Terms] OR clinical studies as topic [All Fields] OR (Medical [All Fields] AND trial [All Fields]) OR intervention study [All Fields] OR (intervention [All Fields] AND trial [All Fields]) OR (interventional [All Fields] AND trial [All Fields]) OR (Interventional [All Fields] and Study [All Fields]) OR intervention studies [All Fields]) |
6 |
| Embase | ‘Single-shade composite’ OR ‘monoshade universal composite’ OR ‘monochromatic composite’ AND ‘dental restoration’/exp OR ‘dental restoration’ OR ‘Restorations, Permanent Dental’ OR ‘Restoration, Permanent Dental’ OR ‘Dental Permanent Fillings’ OR ‘Dental Permanent Filling’ AND ‘Randomized Controlled Trials as Topic’ OR ‘Clinical Trials, Randomized’ OR ‘Trials, Randomized Clinical’ OR ‘Controlled Clinical Trials, Randomized’ OR ‘Randomized Controlled Trial’ OR ‘clinical trial’ OR ‘clinical data’ OR ‘clinical studies as topic’ OR ‘medical trial’ OR ‘intervention study’ OR ‘intervention studies’ OR ‘intervention trial’ OR ‘interventional studies’ OR ‘interventional study’ OR ‘interventional trial’ |
3 |
| Web of Science | TS= (“Single-shade composite” OR “monoshade universal composite” OR “monochromatic composite”) AND TS= (“Restorations, Permanent Dental” OR “Restoration, Permanent Dental” OR “Dental Permanent Fillings” OR “Dental Permanent Filling”) AND TS= (“Randomized Controlled Trials as Topic) OR (Clinical Trials, Randomized” OR (Trials, Randomized Clinical) OR (Controlled Clinical Trials, Randomized) OR (Randomized Controlled Trial) OR (clinical trial) OR (clinical data) OR (clinical studies as topic) OR (medical trial) OR (intervention study) OR (intervention studies) OR (intervention trial) OR (interventional studies) OR (interventional study) OR (interventional trial)) |
12 |
| The Chrochane Library | (Single-shade composite) OR (monoshade universal composite) OR (monochromatic composite) AND (Restorations, Permanent Dental OR Restoration, Permanent Dental OR Dental Permanent Fillings OR Dental Permanent Filling) AND (Randomized Controlled Trials as Topic) OR (Clinical Trials, Randomized) OR (Trials, Randomized Clinical) OR (Controlled Clinical Trials, Randomized) OR (Randomized Controlled Trial) OR (clinical trial) OR (clinical data) OR (clinical studies as topic) OR (medical trial) OR (intervention study) OR (intervention studies) OR (intervention trial) OR (interventional studies) OR (interventional study) OR (interventional trial) |
2 |
| Scopus | ‘Restorations, AND permanent AND dental' OR 'restoration, AND permanent AND dental' OR 'dental AND permanent AND fillings' OR 'dental AND permanent AND filling' AND ‘Single-shade and composite’ OR ‘monoshade and universal and composite’ OR ‘monochromatic and composite’ AND ‘Randomized Controlled Trials as Topic’ OR ‘Clinical Trials, Randomized’ OR ‘Trials, Randomized Clinical’ OR ‘Controlled Clinical Trials, Randomized’ OR ‘Randomized Controlled Trial’ OR ‘clinical trial’ OR ‘clinical data’ OR ‘clinical studies as topic’ OR ‘medical trial’ OR ‘intervention study’ OR ‘intervention studies’ OR ‘intervention trial’ OR interventional studies’ OR ‘interventional study’ OR ‘interventional trial’ |
8 |
Table 2.
USPHS and FDI criteria for color behavior.
| The USPHS criteria |
|---|
|
Color match Alpha (A): The restoration matches the adjacent tooth tissue in color, shade, or translucency. Bravo (B): There is a slight mismatch in color, shade, or translucency, but within the normal range of adjacent tooth structure. Charlie (C): There is a slight mismatch in color, shade, or translucency, but outside of the normal range of adjacent tooth structure. |
| FDI Criteria |
|
Color stability or translucency
Score 1: Good coloration and translucency compared to neighboring teeth. Score 2: Minimal color and translucency deviation. Score 3: Clear deviation, but without affecting aesthetics. Score 4: Localized clinical deviation that can be corrected by repair. Score 5: Unacceptable, replacement necessary. |
Table 3.
Data extracted.
| Author, year | Study design | RBCs | No. of subjects (mean age) |
No. of rest. | Tooth | Finish and polish | Light curing | Type of rest. | Follow-up | Analysis criteria | Conclusion |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Hashem, Khairy and Shaalan (2022) |
RCT |
Filtek universal Filtek Z3250 XT |
26 (13-30) years |
26 |
Permanent Incisors |
Yellow-coded diamond finishing stones, soflex discs, perio-bur #831, and rubber cup, flame, and wheel polishing tips |
Elipar S10 - 20 sec | Class IV | 3 days | USPHS | Single-resin RBC showed satisfactory shade matching potential when compared to polychromatic RBCs. |
| Zulekha et al. (2022) |
RCT |
Omnichroma Tetric N Ceram |
25 (3-5 years) |
50 | Primary anterior teeth |
NM | NM |
Full coronal esthetic | 12 months | USPHS | Single-shade RBC performed similarly to multi-shade in terms of the color match and color stability for both 6- and 12-month intervals. |
| Miranda et al. (2024) |
RCT |
Admira Fusion Admira Fusion X-tra |
70 (40-58 years) |
120 | Anterior or posterior |
Fine and extra-fine #2200 diamond burs along with OptraPol NG | Bluephase meter II - 20 sec |
NCCL | 7 days | FDI | The single-shade RBCused achieves the same color match when compared to a multi-shade composite resin after 7 |
| Anwar, Hussein and Riad (2024) |
RCT |
Omnichroma Tetric N Ceram |
20 (20-45 years) |
40 | Molar or premolar |
Low-speed fine-grit diamond finishing stones, EVE DIACOMP Plus Occuflex-impregnated rubber cups and impregnated brushes | Bluephase Style - 20 sec. |
Oclusal cavities | 12 months | USPHS | Single-shade RBC exhibited comparable performance to a multi-shade RBC regarding color match and color stability |
Legend: RCT= Randomized Clinical Trial; RBCs= Resins Based Composites; No= Number; Rest= Restorations; NM= Not mentioned; NCCL= Non-Carious Cervical Lesion; FDI= World Dental Federation; USPHS= United States Public Health Service. Results of syntheses.
Table 4.
Evidence certainty assessment with grading of recommendations, assessment, development, and evaluation (GRADE).
Table 4.
Evidence certainty assessment with grading of recommendations, assessment, development, and evaluation (GRADE).
| Parameter | No Of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Certainty |
|---|---|---|---|---|---|---|---|---|
| Color stability (1 to 7 days) | 4 | RCT | Not seriousa | Not seriousb | Seriousc | Seriousd | None | ⊕⊕OO Low |
| Color stability (12 months) | 4 | RCT | Not seriousa | Not seriousb | Seriousc | Seriousd | None | ⊕⊕OO Low |
GRADE Working Group grades of evidence. High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. RCT: Randomized Clinical Trial. aAll included studies presented low risk of bias and just one study some concerns for blinding and alloocation of participants/personnel/outcome assessor. bThere was not presence of substantial heterogeneity. cIndirectness judged based on population, intervention, comparison, and outcome across studies, where the population did not present sufficiently direct evidence. d The evidence was downgraded because the number of events and sample are considered small.
Table 5.
Materials’ specifications and composition of Single-shade RBCs.
| Single-shade RBC | Manufacturer | Composition |
|---|---|---|
| Filtek Universal | 3 M ESPE, St. Paul, MN, USA | Fillers are a combination of a non-agglomerated/non-aggregated 20nm silica filler, a non-agglomerated/non-aggregated 4 to 11nm zirconia filler, an aggregated zirconia/silica cluster filler (comprised of 20nm silica and 4 to 11nm zirconia particles), and a ytterbium trifluoride filler. The inorganic filler loading is about 76.5% by weight (58.4% by volume). Matrix: AUDMA, AFM, diurethane-DMA, and 1,12-dodecane-DMA. |
| Omnichroma | Tokuyama Dental, Tokio, Japan | Matrix: TEGDMA, UDMA, Dibutyl hydroxyl toluene and UV absorber, Mequinol. Filler system: SiO2, ZrO2 (68 vol.-%; 79 wt%; 0.2–0.4 μm) |
| Admira Fusion X-tra | Voco GmbH, Cuxhaven, Germany |
Organically modified ceramic ORMOCER. Matrix: aromatic and aliphatic dimethacrylates, methacrylatefunctionalized polysiloxane. Filler: barium aluminum borosilicate glass ceramic filler (median: 1 mm) and silicon dioxide nanoparticles (0.02 to 0.04 μm). Filler 84 wt%. Camphorquinone Pigments: ironoxide and titanium dioxide |
Legend: AUDMA= Aromatic Urethane Dimethacrylate; AFM= Addition-Fragmentation Monomer; TEGDMA= Tetraethylene glycol dimethacrylate ; UDMA= Urethane Dimethacrylate.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



