
Submitted:
15 June 2024
Posted:
17 June 2024
You are already at the latest version
Abstract
Keywords: Endodontic microsurgery; Root canal treatment; Isthmus preparation; Short-term outcomes
Keywords:
Endodontic microsurgery
; Root canal treatment
; Isthmus preparation
; Short-term outcomes
1. Introduction
Non-surgical endodontic therapy is currently the most favored treatment method for clinical management of periapical periodontitis [1]. Despite positive outcomes associated with non-surgical treatments, a certain proportion of interventions fail [2,3,4,5,6] for an array of reasons including the presence of residual bacteria in difficult-to-instrument root canal systems and the presence of extra-apical infection [7]. In these cases, surgical endodontic treatment is often employed. One of the indicated surgical approaches is endodontic microsurgery (EMS) performed with a microscope, which provides higher proportions of successful outcomes than traditional root-end surgery [8]. This improved success may arise from the rigorous application of defined surgical procedures, more advanced instrumentation, improved retrograde root canal cavity preparation and filling materials, and high-resolution identification of underlying structural problems enabled by microscopy [9,10,11].
The percentage of successful outcomes following EMS is affected by several pre-treatment factors, which include root canal instrumentation prior to apicoectomy [12]. While previous instrumentation has been associated with improved outcomes, placement of a post and core restoration has been reported to negatively affect prognosis [13]. Currently, no definitive conclusions have been reached with respect to these factors. In addition, if an isthmus is present on the surgically prepared surface of the root, isthmus preparation may be performed, but the effect of this preparation on post-treatment success is not defined [14,15]. While the therapeutic value of EMS is recognized in Japan [15,16], no studies have quantified outcomes and the relative importance of the pre-treatment factors described above. Here we conducted a retrospective analysis with one year follow-up of the preoperative and intraoperative factors that affect the success of EMS in Japanese patients.
2. Materials and Methods
2.1. Study Design
This study was conducted according to the principles of the Declaration of Helsinki (2013). Written, informed consent was obtained from all patients, and the study was approved by the Tokyo Dental College Institutional Review Board (Tokyo Dental College Ethical Review No. 515). Retrospective analysis of outcomes was conducted for patients who underwent microscope-guided apicoectomy in the Department of Conservative Dentistry of the Tokyo Dental College at Chiba Hospital between March 2013 and March 2015.
2.2. Sample Selection
Based on the medical and dental histories, patients who fulfilled the following inclusion criteria were selected.
- No medical contraindications for surgical endodontic therapy (ASA-PS class I or II).
- Diagnosis of periapical periodontitis by preoperative cone-beam computed tomography (CBCT).
- Root resection and retrograde root canal filling were conducted with the aid of a surgical microscope and with specialized instruments and treatment protocols optimized for EMS.
- The patient provided informed consent for the treatment.
Patients that exhibited root perforation, advanced marginal periodontitis, or root fracture during preoperative examinations were excluded from the study.
2.3. Surgical Treatment Procedures and Follow-up
All procedures were conducted by a single, board-certified endodontist with 15 years’ experience. The same operative procedures were used for all patients enrolled in this study. Other than the performance of the incisions, procedures were conducted with a magnified view provided by a surgical microscope (OPMI PROergo, Carl Zeiss, Gottingen, Germany). Below we describe the surgical method.
Infiltration (for maxillary teeth) or block anesthesia (for mandibular teeth) was performed with 2% xylocaine with 1:80,000 epinephrine. Cognizant of the condition of the periodontal tissues and cosmetic appearance, releasing incisions were placed through the gingival sulcus and the gingival papilla. In some instances, an Ochsenbein flap design was used. A full thickness mucoperiosteal flap was reflected; low tractional forces were applied during the surgical procedure to aid visual inspection of the tooth root. If needed for improving visual access to the root apex, the labial surface of the alveolar bone was removed by ostectomy to expose the apex of the root and the lesion. A tapered fissure bur in a 45° angled-head air turbine drill was used to resect the root perpendicularly to its long axis at ~3 mm from the apex. After the apical portion had been severed from the root, the lesion was excised and immersed in 10% formalin solution. Hemostasis was conducted by applying pressure with a cotton swab soaked in 1:000 epinephrine. The cut surface was stained with methylene blue and examined under magnification. A 3 mm-deep retrograde cavity was prepared with an ultrasound tip (KIS Ultrasonic Tip, Obtura-Spartan, Fenton, MI). After enlargement, the cut surface was again stained with methylene blue and examined. Upon confirming there were no structural defects in the root, retrograde filling was conducted by inserting MTA cement (ProRoot MTA White, Dentsply Tulsa Dental, Tulsa, OK). After placement of the filling, the integrity of the MTA seal was confirmed under magnification, and by obtaining radiographs of the affected site.
The flap was replaced and closed with interrupted sutures (6-0 nylon). After application of pressure and ice packs for 10 minutes, hemostasis was confirmed. All patients received amoxicillin hydrate (250 mg every 8 h for 3 days, starting immediately after the procedure) and either an anti-inflammatory analgesic (Loxoprofen sodium hydrate 60 mg) or Acetaminophen, 500 mg) every 6 h after surgery. The excised lesion was submitted for histopathological examination by a board-certified pathologist. The wound was disinfected with chlorhexidine and the sutures were removed on day 4. Patients who underwent surgery were contacted 12 months later and re-examined for assessment of healing. Patients who could not be contacted and those who declined to undergo re-examination were considered as lost to follow-up. At the 12 months examination, the presence or absence of signs and symptoms was evaluated, and dental radiographs were obtained.
2.4. Data Collection and Outcome Assessment
The following data were obtained from the patients’ records using the parameters identified below and recorded:
Age at surgery, sex, dental arch (maxillary or mandibular), lesion size, lesion type, preoperative root canal treatment, presence or absence of a post core, and presence or absence of an isthmus on the cut surface were recorded in the database. Preoperative and postoperative signs and symptoms (pain, and pain on percussion and palpation) and X-ray findings were also recorded in the database.
Patient assessments were conducted using postoperative dental radiographs and the criteria of healing of periapical lesions provided earlier by Rud et al. [17] and Molven et al. [18]. Based on these criteria, the status of periapical healing was classified as: complete healing, incomplete healing, uncertain healing, or unsatisfactory healing. Of these categories, complete healing and incomplete healing were assessed as “clinical success,” (Figure 1) and uncertain healing and unsatisfactory healing were considered as “clinical failure” (Figure 2). If the tooth had more than one root, the root that exhibited the least advanced healing was assessed as the overall status of healing for that tooth. Radiographs were evaluated by three calibrated, board-certified endodontists. If their assessments varied, they discussed the case until they reached a consensus assessment. The success rate was then calculated from this assessment.
If the tooth had more than one root, the root that exhibited the least advanced healing was assessed as the overall status of healing for that tooth. Radiographs were evaluated by three calibrated, board-certified endodontists. If their assessments varied, they discussed the case until they reached a consensus assessment. The success rate was then calculated from this assessment.
2.5. Statistical Analysis
A binary logistic regression model was used in which the clinical healing rate was the dependent variable, which was used to evaluate associations between independent variables and treatment outcomes (“clinical success” versus “clinical failure”). The unadjusted odds ratios were calculated to evaluate the associations between variables. The effects of different variables on healing and their associations were evaluated using odds ratios and 95% confidence intervals.
EZR (Jichi Medical University Saitama Medical Center, Japan) was used for all statistical analysis [19]. EZR is a graphical user interface (GUI) for R (The R Foundation for Statistical Computing, Vienna, Austria); more precisely, it is the improved version of R Commander, which was designed to add statistical functions that are frequently used in biological statistics. For parametric data, the results are reported as mean±standard deviation.
3. Result
A total of 55 patients underwent EMS between March 2013 and March 2015, of whom 9 were excluded from the study. In two cases this was because root fracture was diagnosed intraoperatively, and the tooth was extracted; the other seven patients could not be contacted. The re-examination rate was 86.8% (46/53), and the final analysis set included 46 teeth of 46 patients. There were more than 2.5-fold more women (n = 34) than men (n = 12). The mean age of the patients was 46.2 ± 12.5 years. According to the criteria described above for periapical healing after endodontic treatment [17,18], there was complete healing in 76.1% of cases (35/46), incomplete healing in 17.4% (8/46), uncertain healing in 2.2% (1/46), and unsatisfactory healing in 4.3% (2/46). Based on our working description of treatment success described above, clinically successful outcomes were 93.5% of cases and clinical failures comprised 6.5% of cases.
The mean lesion diameter was 5.2 ± 3.2 mm. Histopathological analysis showed that the excised lesions were of different pathological diagnoses (Table 1).
We evaluated the association between healing outcome and prognostic factors (Table 2). There were more successful outcomes for teeth in the maxillary arch than for the mandibular arch (p=0.041). Treatment success was higher (p=0.019) when previous root canal instrumentation had been conducted than when no previous instrumentation was provided. There were no significant differences (p>0.2) of treatment success with respect to age, sex, lesion size on previous radiograph, the presence or absence of a post, or the presence or absence of a root canal isthmus.
4. Discussion
We examined Japanese patients who had undergone EMS one year previously for treatment of periapical periodontitis. We assessed the effects of preoperative and intraoperative factors on the percentage of successful outcomes after EMS, which was 93.5%, a result that is similar to previous reports [20,21,22]. As these earlier reports described analyses conducted on non-Japanese populations, the data collectively indicate that are no substantial racial differences in EMS outcomes, at least with respect to Japanese populations. Further, of the pre-operative and peri-operative factors that were analyzed, only dental arch (maxillary or mandibular) and previous root canal instrumentation showed statistically significant differences with respect to the % of treatment success. The other factors that were analyzed (lesion size, lesion type, presence or absence of a post core, presence or absence of an isthmus on the cut surface) did not affect treatment success.
We found no association between age or sex on the percentage of successful outcomes after EMS. A previous report indicated that successful outcomes were highest for younger patients in their 20s [23], and that the percentage or failed outcomes increased with age [13] while another report showed higher percentages of success for older patients [24]. Notably, other studies found no association with age [25,26]. With respect to the association with sex, one previous study reported that success was higher for women [27], whereas another found that successful outcomes were higher for men [13]. A study that used an insurance database to investigate treatment outcomes after apicoectomy found that the percentage of surviving teeth was higher for men than for women, and that the percentage of surviving teeth decreased continuously with the age of the patient [28]. In contrast, other studies found no significant differences with respect to age and sex [29,30,31]. Collectively, as the published literature on age and sex effects are inconsistent, these factors do not seem to influence the success of EMS.
In the current study the percentage of successful outcomes was higher for the maxillary arch than the mandibular arch, a result that may have been influenced by the relatively smaller sample size of teeth analyzed for the mandibular arch. Previous data indicated that the percentage of successful outcomes was higher for the maxillary arch than for the mandibular arch [13,32], and that success for the maxillary anterior teeth was reportedly higher than for posterior teeth in the maxilla. This difference may reflect the comparatively easier access and the less complex anatomical structure for anterior teeth [33].
In the current study, similar to previous analyses [34,35,36], the effect of lesion size was investigated by dividing lesions into two groups: radiographically detectable lesions with diameter <5 mm or lesions ≥ 5 mm. We found that mean lesion size was 5.20 mm and was not associated with any particular healing outcome one year later. Previous reports indicated the percentage of successful outcomes was positively associated with lesions of diameter <5 mm while lesions with a diameter ≥5 mm were not associated with success [37]. In contrast, longer term studies showed that lesion size did not affect the percentage of successful outcomes[17,38], which may reflect the notion that the time required for healing depends on lesion size [20]. Conceivably, healing by scarring (which we classified as “uncertain”) may exhibit periapical radiolucencies that shrink in diameter over longer time periods.
We found no effect on lesion type on the percentage of successful outcomes. Conceivably, this result may be influenced by our use of high magnification imaging during lesion removal, which is in contrast to previous studies in which this part of the procedure was conducted under none or low magnification. Previous data showed that radicular granulomas (73%) were more common than radicular cysts (15%) [39], which is similarly to the current study in which radicular granulomas (65%) were more common than radicular cysts (20%). In contrast, the opposite result was reported in another study in which chronic, non-specific inflammatory lesions and radicular cysts (47.3%) were more common than radicular granuloma (44.0%) [40]. Further, in this same study, treatment success for apicoectomy of teeth with cysts was higher than teeth with granulomas [40]. Conceivably, this outcome may reflect the notion that cysts, with epithelial cell walls, are relatively easier to remove than granulomas [41].
Previous root canal instrumentation can affect healing [7]. Similarly, we found that the percentage of successful outcomes was higher when root canal treatment was performed before EMS, a result that may reflect the reduced numbers of bacteria in the root canal system prior to initiation of EMS. In addition, previous treatment of the root canal aids can aid clinical diagnosis, thereby enabling the exclusion of teeth with root fracture or perforation, which facilitates positive treatment outcomes.
For many of the cases examined here, we found that EMS was indicated in cases exhibiting very little remaining tooth substance and in which post-core removal was challenging. But for these cases, there was no significant difference in the short-term percentage of successful outcomes, a result that is consistent with other studies [8]. In this context, when treatment was repeated for teeth requiring post-core removal, vertical root fracture occurred more frequently than when EMS was performed [42]. This result could arise because post-core removal reduced the amount of dentin in the root, further weakening its resistance to fracture. Conversely, when EMS was performed on teeth with ideally restored post-cores, the long-term survival rate was higher [43]. Accordingly, while not yet resolved, previous root canal treatment is considered higher risk, and surgical treatment should be the first choice for teeth with an existing post-core.
The amount of dentin at the apex may affect treatment outcomes. Insufficient isthmus instrumentation may be one reason for the failure of apicoectomy [44]. If an isthmus is seen, certain authors encourage prophylactic enlargement and filling [44,45]. However, one study found that the four-year survival rate of teeth in which no isthmus was present and isthmus preparation was not conducted was 87.4%. This survival rate is higher than the 61.5% when an isthmus was present and isthmus preparation was conducted [14]. In addition, eight of the nine cases of failure in this study were associated with vertical root fracture after teeth had undergone isthmus preparation. These data suggest that isthmus preparation may reduce the amount of dentin remaining postoperatively and weaken fracture resistance. Notably, a micro-CT morphological study of the maxillary first molars of Japanese individuals found that, even when no isthmus was present or only an incomplete isthmus was observed at a position 3 mm from the mesiobuccal root canal apex, microscopic morphological structures associated with the outcome of root canal treatment, including isthmuses, were present more coronally [46]. For this reason, in the current study, if an isthmus was observed during apicoectomy (n = 26/46), whatever its shape, prophylactic isthmus preparation was conducted with a 0.5-mm-diameter ultrasound tip while being careful to remove the minimum amount of dentin. The one-year percentage of successful outcomes was not affected by isthmus preparation even though the tooth substance of the root is weakened after isthmus preparation and the possibility of root fracture may be increased [38].
EMS reportedly has a higher short-term success rate than non-surgical endodontic therapy [47], which is consistent with the data reported here. However, as with traditional root end surgery, the long-term success rate of EMS is lower (albeit only slightly) than other short-term estimates of treatment success [48,49]. Factors that are not manifest during the short-term can still affect the long-term prognosis. Therefore, additional, longer-term follow-up is needed.
5. Conclusions
The % of short-term successful outcomes after EMS in Japanese patients was very high (93.5%). The two factors that affected success were dental arch and previous root canal instrumentation. Age, sex, lesion size, lesion type, the presence or absence of a post core, and the presence or absence of a root canal isthmus had no significant effect on short-term success.
Author Contributions
Conceptualization, M.Y., N.K. and C.M.; Methodology, M.Y. C.M.; Data curation, S.M., N.M., R.F., S.S. and K.S.; Writing, M.Y., I.D., C.M.; Project administration, C.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by an internal award from Tokyo Dental College.
Informed Consent Statement
Written informed consent was obtained from all patients for consent to analyze and include their data in this paper.
Data Availability Statement
The data presented in this publication are available on request. from the corresponding author. The data are not publicly available due to privacy restrictions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- von Arx, T. Failed root canals: the case for apicoectomy (periradicular surgery). J Oral Maxillofac Surg 2005, 63, 832–837. [Google Scholar] [CrossRef] [PubMed]
- Akerblom, A.; Hasselgren, G. The prognosis for endodontic treatment of obliterated root canals. J Endod 1988, 14, 565–567. [Google Scholar] [CrossRef] [PubMed]
- Salehrabi, R.; Rotstein, I. Endodontic treatment outcomes in a large patient population in the USA: an epidemiological study. J Endod 2004, 30, 846–850. [Google Scholar] [CrossRef] [PubMed]
- Gorni, F.G.; Gagliani, M.M. The outcome of endodontic retreatment: a 2-yr follow-up. J Endod 2004, 30, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: systematic review of the literature - part 1. Effects of study characteristics on probability of success. Int Endod J 2007, 40, 921–939. [Google Scholar] [CrossRef] [PubMed]
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: systematic review of the literature -- Part 2. Influence of clinical factors. Int Endod J 2008, 41, 6–31. [Google Scholar] [CrossRef] [PubMed]
- Karabucak, B.; Setzer, F. Criteria for the ideal treatment option for failed endodontics: surgical or nonsurgical? Compend Contin Educ Dent 2007, 28, 391–397, quiz 398, 407. [Google Scholar] [PubMed]
- Kim, S.; Kratchman, S. Modern endodontic surgery concepts and practice: a review. J Endod 2006, 32, 601–623. [Google Scholar] [CrossRef]
- Setzer, F.C.; Shah, S.B.; Kohli, M.R.; Karabucak, B.; Kim, S. Outcome of endodontic surgery: a meta-analysis of the literature--part 1: Comparison of traditional root-end surgery and endodontic microsurgery. J Endod 2010, 36, 1757–1765. [Google Scholar] [CrossRef]
- Setzer, F.C.; Kohli, M.R.; Shah, S.B.; Karabucak, B.; Kim, S. Outcome of endodontic surgery: a meta-analysis of the literature--Part 2: Comparison of endodontic microsurgical techniques with and without the use of higher magnification. J Endod 2012, 38, 1–10. [Google Scholar] [CrossRef]
- Kohli, M.R.; Berenji, H.; Setzer, F.C.; Lee, S.M.; Karabucak, B. Outcome of Endodontic Surgery: A Meta-analysis of the Literature-Part 3: Comparison of Endodontic Microsurgical Techniques with 2 Different Root-end Filling Materials. J Endod 2018, 44, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Hepworth, M.J.; Friedman, S. Treatment outcome of surgical and non-surgical management of endodontic failures. J Can Dent Assoc 1997, 63, 364–371. [Google Scholar] [PubMed]
- Taschieri, S.; Machtou, P.; Rosano, G.; Weinstein, T.; Del Fabbro, M. The influence of previous non-surgical re-treatment on the outcome of endodontic surgery. Minerva Stomatol 2010, 59, 625–632. [Google Scholar] [PubMed]
- Kim, S.; Jung, H.; Kim, S.; Shin, S.J.; Kim, E. The Influence of an Isthmus on the Outcomes of Surgically Treated Molars: A Retrospective Study. J Endod 2016, 42, 1029–1034. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, M.; Yokoo, S.; Yamaguchi, T.; Suzuki, K.; Makiguchi, T. Factors Influencing Bone Healing after Extirpation with Endodontic Microsurgery-Microscopic Apicoectomy for Extensive Radicular Cysts. 北関東医学 2019, 69, 315–324. [Google Scholar] [CrossRef]
- Sukegawa, S.; Shimizu, R.; Sukegawa, Y.; Hasegawa, K.; Ono, S.; Fujimura, A.; Yamamoto, I.; Nakano, K.; Takabatake, K.; Kawai, H.; et al. Prognostic Factors in Endodontic Surgery Using an Endoscope: A 1 Year Retrospective Cohort Study. Materials (Basel) 2022, 15. [Google Scholar] [CrossRef] [PubMed]
- Rud, J.; Andreasen, J.O.; Jensen, J.E. Radiographic criteria for the assessment of healing after endodontic surgery. Int J Oral Surg 1972, 1, 195–214. [Google Scholar] [CrossRef] [PubMed]
- Molven, O.; Halse, A.; Grung, B. Observer strategy and the radiographic classification of healing after endodontic surgery. Int J Oral Maxillofac Surg 1987, 16, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software 'EZR' for medical statistics. Bone Marrow Transplant 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Rubinstein, R.A.; Kim, S. Short-term observation of the results of endodontic surgery with the use of a surgical operation microscope and super-EBA as root-end filling material. Journal of Endodontics 1999, 25, 43–48. [Google Scholar] [CrossRef]
- Chong, B.S.; Pitt Ford, T.R.; Hudson, M.B. A prospective clinical study of Mineral Trioxide Aggregate and IRM when used as root-end filling materials in endodontic surgery. 2003. Int Endod J 2009, 42, 414–420. [Google Scholar] [CrossRef]
- von Arx, T.; Hanni, S.; Jensen, S.S. Clinical results with two different methods of root-end preparation and filling in apical surgery: mineral trioxide aggregate and adhesive resin composite. J Endod 2010, 36, 1122–1129. [Google Scholar] [CrossRef]
- Song, M.; Jung, I.Y.; Lee, S.J.; Lee, C.Y.; Kim, E. Prognostic factors for clinical outcomes in endodontic microsurgery: a retrospective study. J Endod 2011, 37, 927–933. [Google Scholar] [CrossRef]
- Barone, C.; Dao, T.T.; Basrani, B.B.; Wang, N.; Friedman, S. Treatment outcome in endodontics: the Toronto study--phases 3, 4, and 5: apical surgery. J Endod 2010, 36, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Çalışkan, M.K.; Tekin, U.; Kaval, M.E.; Solmaz, M.C. The outcome of apical microsurgery using MTA as the root-end filling material: 2- to 6-year follow-up study. Int Endod J 2016, 49, 245–254. [Google Scholar] [CrossRef]
- Tawil, P.Z.; Saraiya, V.M.; Galicia, J.C.; Duggan, D.J. Periapical microsurgery: the effect of root dentinal defects on short- and long-term outcome. J Endod 2015, 41, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Liao, W.-C.; Lee, Y.-L.; Tsai, Y.-L.; Lin, H.-J.; Chang, M.-C.; Chang, S.-F.; Chang, S.-H.; Jeng, J.-H. Outcome assessment of apical surgery: A study of 234 teeth. Journal of the Formosan Medical Association 2019, 118, 1055–1061. [Google Scholar] [CrossRef]
- Raedel, M.; Hartmann, A.; Bohm, S.; Walter, M.H. Three-year outcomes of apicectomy (apicoectomy): Mining an insurance database. J Dent 2015, 43, 1218–1222. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.; Glickman, G.N.; Woodmansey, K.F.; He, J. Retrospective Analysis of Root-end Microsurgery Outcomes in a Postgraduate Program in Endodontics Using Calcium Silicate-based Cements as Root-end Filling Materials. J Endod 2020, 46, 345–351. [Google Scholar] [CrossRef]
- Zhou, W.; Zheng, Q.; Tan, X.; Song, D.; Zhang, L.; Huang, D. Comparison of Mineral Trioxide Aggregate and iRoot BP Plus Root Repair Material as Root-end Filling Materials in Endodontic Microsurgery: A Prospective Randomized Controlled Study. J Endod 2017, 43, 1–6. [Google Scholar] [CrossRef]
- Pinto, D.; Marques, A.; Pereira, J.F.; Palma, P.J.; Santos, J.M. Long-Term Prognosis of Endodontic Microsurgery-A Systematic Review and Meta-Analysis. Medicina (Kaunas) 2020, 56. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Kim, S.G.; Lee, S.J.; Kim, B.; Kim, E. Prognostic factors of clinical outcomes in endodontic microsurgery: a prospective study. J Endod 2013, 39, 1491–1497. [Google Scholar] [CrossRef] [PubMed]
- Ørstavik, D.; Pitt Ford, T.R. Essential endodontology : prevention and treatment of apical periodontitis; Blackwell Science: Oxford, UK, 1998; pp. 368–369. [Google Scholar]
- Hjorting-Hansen, E.; Andreasen, J.O. Incomplete bone healing of experimental cavities in dog mandibles. Br J Oral Surg 1971, 9, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Lustmann, J.; Friedman, S.; Shaharabany, V. Relation of pre- and intraoperative factors to prognosis of posterior apical surgery. J Endod 1991, 17, 239–241. [Google Scholar] [CrossRef] [PubMed]
- von Arx, T.; Jensen, S.S.; Hanni, S. Clinical and radiographic assessment of various predictors for healing outcome 1 year after periapical surgery. J Endod 2007, 33, 123–128. [Google Scholar] [CrossRef] [PubMed]
- von Arx, T.; Penarrocha, M.; Jensen, S. Prognostic factors in apical surgery with root-end filling: a meta-analysis. J Endod 2010, 36, 957–973. [Google Scholar] [CrossRef] [PubMed]
- Pallares-Serrano, A.; Glera-Suarez, P.; Tarazona-Alvarez, B.; Penarrocha-Oltra, D.; Penarrocha-Diago, M.; Penarrocha-Diago, M. Healing of 295 Endodontic Microsurgery Cases After Long-Term (5-9 Years) Versus Middle-Term (1-4 Years) Follow-up. J Endod 2022, 48, 714–721. [Google Scholar] [CrossRef]
- Nair, P.N. New perspectives on radicular cysts: do they heal? Int Endod J 1998, 31, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Oginni, A.O.; Olusile, A.O. Follow-up study of apicectomised anterior teeth. SADJ 2002, 57, 136–140. [Google Scholar]
- Alantar, A.; Bloud, C.; Galéazzi, J.-M.; Baranes, M.; Lévy, G.; Chapireau, D.; Benlagha, N.; Maman, L. Success rate and recurrence frequency of periapical surgery: prospective study on 132 cases. Med Buccale Chir Buccale 2010, 16, 15–22. [Google Scholar] [CrossRef]
- Riis, A.; Taschieri, S.; Del Fabbro, M.; Kvist, T. Tooth Survival after Surgical or Nonsurgical Endodontic Retreatment: Long-term Follow-up of a Randomized Clinical Trial. J Endod 2018, 44, 1480–1486. [Google Scholar] [CrossRef] [PubMed]
- Truschnegg, A.; Rugani, P.; Kirnbauer, B.; Kqiku, L.; Jakse, N.; Kirmeier, R. Long-term Follow-up for Apical Microsurgery of Teeth with Core and Post Restorations. J Endod 2020, 46, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Shin, S.J.; Kim, E. Outcomes of endodontic micro-resurgery: a prospective clinical study. J Endod 2011, 37, 316–320. [Google Scholar] [CrossRef] [PubMed]
- von Arx, T. Frequency and type of canal isthmuses in first molars detected by endoscopic inspection during periradicular surgery. Int Endod J 2005, 38, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Matsunaga, S.; Yamada, M.; Kasahara, N.; Kasahara, M.; Odaka, K.; Fujii, R.; Miyayoshi, N.; Sekiya, S.; Sako, R.; Sugiuchi, A.; et al. Tooth Root Cross-section Variations of Significance for Endodontic Microsurgery and Predicted Risk of Concealed Canal Isthmus Based on Cross-sectional Morphology: Three-dimensional Morphological Analysis of Japanese Maxillary First Molars Using Micro-CT. Journal of Hard Tissue Biology 2019, 28, 153–158. [Google Scholar] [CrossRef]
- Del Fabbro, M.; Taschieri, S.; Testori, T.; Francetti, L.; Weinstein, R.L. Surgical versus non-surgical endodontic re-treatment for periradicular lesions. Cochrane Database Syst Rev 2007, CD005511. [Google Scholar] [CrossRef] [PubMed]
- von Arx, T.; Hanni, S.; Jensen, S.S. 5-year results comparing mineral trioxide aggregate and adhesive resin composite for root-end sealing in apical surgery. J Endod 2014, 40, 1077–1081. [Google Scholar] [CrossRef]
- Caliskan, M.K.; Tekin, U.; Kaval, M.E.; Solmaz, M.C. The outcome of apical microsurgery using MTA as the root-end filling material: 2- to 6-year follow-up study. Int Endod J 2016, 49, 245–254. [Google Scholar] [CrossRef]
Figure 1.
Representative radiographs as examples of clinical success. Complete healing (Top Row): A mandibular first molar was radiographically assessed as ‘complete healing’ 1 year after EMS. (A) immediate post-operative, (B) 1-year follow-up, (C) Diagram of the apical healing used for classification developed by Rud and Molven [17,18]. Incomplete healing (Bottom Row): A maxillary lateral incisor was radiographically assessed as ‘incomplete healing’ 1 year after EMS. (D) immediate postoperative, (E) 1-year follow-up, (F) Diagram of apical healing used for classification as described [17,18].
Figure 1.
Representative radiographs as examples of clinical success. Complete healing (Top Row): A mandibular first molar was radiographically assessed as ‘complete healing’ 1 year after EMS. (A) immediate post-operative, (B) 1-year follow-up, (C) Diagram of the apical healing used for classification developed by Rud and Molven [17,18]. Incomplete healing (Bottom Row): A maxillary lateral incisor was radiographically assessed as ‘incomplete healing’ 1 year after EMS. (D) immediate postoperative, (E) 1-year follow-up, (F) Diagram of apical healing used for classification as described [17,18].
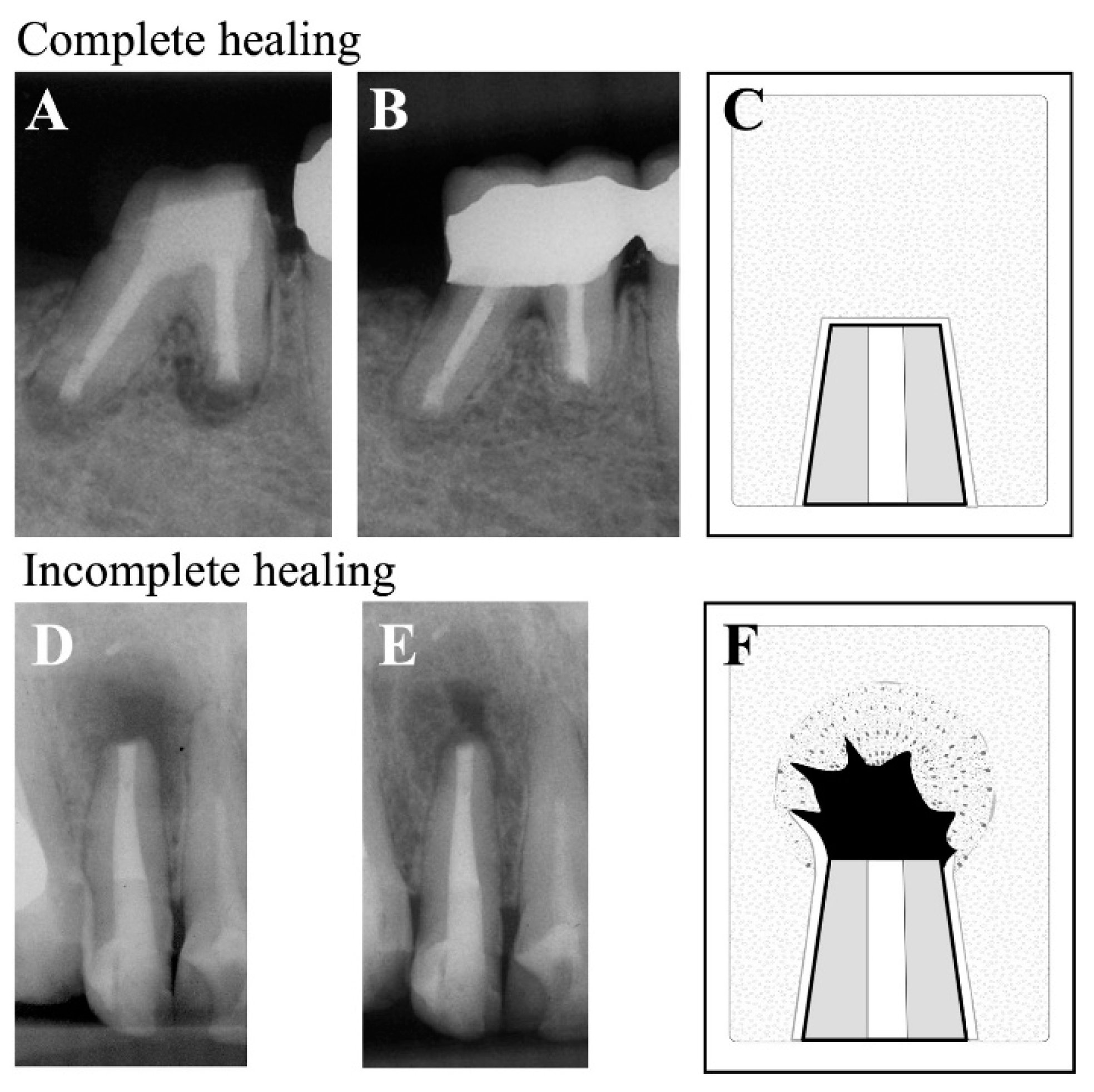
Figure 2.
Representative radiographs as examples of unsatisfactory healing. Uncertain Healing (Top Row). A maxillary central incisor was radiographically assessed as ‘uncertain healing’ 1 year after EMS. (A) Immediate post-operative, (B) 1-year follow-up, (C) Diagram of apical healing used for classification as described [17,18]. Unsatisfactory Healing (Bottom Row). A mandibular lateral incisor was radiographically assessed as ‘unsatisfactory healing’ 1 year after EMS. (D) Immediate postoperative, (E) 1-year follow-up, (F) Diagram of apical healing used for classification as described [17,18].
Figure 2.
Representative radiographs as examples of unsatisfactory healing. Uncertain Healing (Top Row). A maxillary central incisor was radiographically assessed as ‘uncertain healing’ 1 year after EMS. (A) Immediate post-operative, (B) 1-year follow-up, (C) Diagram of apical healing used for classification as described [17,18]. Unsatisfactory Healing (Bottom Row). A mandibular lateral incisor was radiographically assessed as ‘unsatisfactory healing’ 1 year after EMS. (D) Immediate postoperative, (E) 1-year follow-up, (F) Diagram of apical healing used for classification as described [17,18].
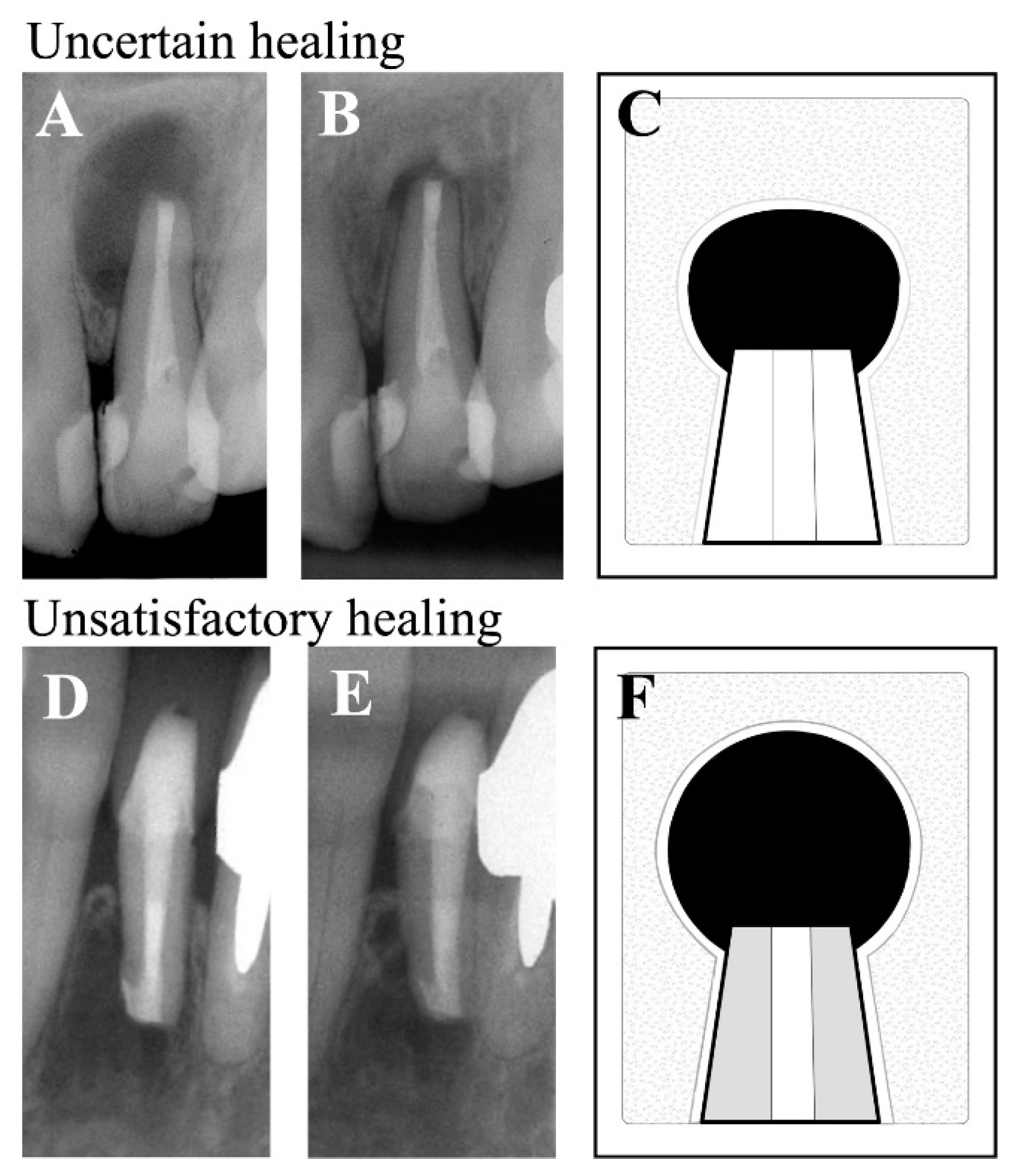

Table 1.
Types of lesions removed during EMS.
| Pathological diagnosis | n (%) |
|---|---|
| Radicular cyst | 26 (65) |
| Radicular granuloma | 8 (20) |
| Inflammatory granulation tissue | 6 (7.5) |
| Not collected | 6 (7.5) |
Table 2.
Distribution of Cases by Factor and Bivariate Analysis.
| Variable/Factor (n) | Clinical success (%) | Clinical failure (%) | OR (95%CI) | P value | |
|---|---|---|---|---|---|
| Sex (46) | Female | 31 (67.4) | 3 (6.5) | 0 (0-7.012) |
0.557 |
| Male | 12 (26.1) | 0 (0) | |||
| Age, y (46) | < 45 | 29 (63.1) | 2 (4.3) | 1.035 (0.02.-21.50) |
1 |
| ≥ 45 | 14 (30.4) | 1 (2.2) | |||
| Arch (46) | Maxillary | 39 (84.8) | 1 (2.2) | 17.08 (0.75-1165.82) |
0.041* |
| Mandibular | 4 (8.7) | 2 (4.3) | |||
| Lesion size, mm (46) | < 5 | 17 (37) | 0 (0) | Inf (0.11-Inf) |
0.524 |
| ≥ 5 | 27 (58.7) | 2 (4.3) | |||
| Lesion type (34) | Granuloma | 24 (70.6) | 2 (5.9) | 3.27 (0.04 -279.35) |
0.432 |
| Cyst | 7 (20.6) | 1 (2.9) | |||
| Pre-RCT (46) | Yes | 33 (71.8) | 0 (0) | Inf (1.14-Inf) |
0.019* |
| No | 10 (21.7) | 3 (6.5) | |||
| Post core (46) | Yes | 17 (37) | 2 (4.3) | 0.561 (0.01- 6.91) |
0.561 |
| No | 26 (56.5) | 1 (2.2) | |||
| Isthmus (46) | Yes | 18 (39.1) | 2 (4.3) | 0.368 (0.01- 7.58) |
0.572 |
| No | 25 (54.4) | 1 (2.2) |
*Indicates significance (P<0.05); CI, 95% confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



