
Submitted:
18 June 2024
Posted:
18 June 2024
You are already at the latest version
Abstract
Background/Objectives: Infectious Endocarditis often requires surgical intervention, with postoperative acute kidney injury (AKI) posing a significant concern. This retrospective study aimed to investigate AKI incidence, its impact on short-term mortality, and identify modifiable factors in patients with endocarditis scheduled for valve surgery. Methods: This single center study enrolled 130 consecutive endocarditis patients from 2013 to 2021 undergoing valve surgery. Creatinine levels were monitored pre- and postoperatively, and AKI was defined by Kidney Disease: Improving Global Outcomes (KDIGO) criteria. Patient demographics, comorbidities, procedural details, and complications were recorded. Primary outcomes included AKI incidence, the relevance of creatinine levels for AKI detection, and the association of AKI with 30-, 60- and 180-day mortality. Modifiable factors contributing to AKI were explored as secondary outcomes. Results: Postoperatively, 35.4% developed AKI. The highest creatinine elevation occurred on the 2nd postoperative day. Best predictive value for AKI was a creatinine level of 1.35 mg/dl on the 2nd day (AUC: 0.901; sensitivity: 0.89, specificity: 0.79). Elevated creatinine levels on the 2nd day were robust predictors for short-term mortality at 30, 60 and 180 days postoperatively (AUC ranging from 0.708 to 0.789). CK-MB levels at 24 hours postoperatively and minimum hemoglobin during surgery were identified as independent predictors for AKI in logistic regression. Conclusions: This study highlights the crucial role of creatinine levels in predicting short-term mortality in surgical endocarditis patients. A specific threshold (1.35 mg/dl) provides a practical marker for risk stratification, offering insights for refining perioperative strategies and optimizing outcomes in this challenging patient population.
Keywords:
acute kidney injury
; endocarditis
; creatinine
; valve surgery
1. Introduction
Endocarditis, initiated by the invasion of pathogens into the bloodstream, imposes a substantial burden on the cardiovascular system [1]. Its clinical spectrum ranges from subtle to life-threatening scenarios. The implications extend beyond the cardiac realm, with systemic consequences that may necessitate prompt intervention [2,3,4].
Valvular surgery, often required for uncontrolled infection, embolic disease or severe valvular dysfunction, aims to eradicate the infectious focus, repair or replace valves, and restore cardiac function. Valvular surgery is, therefore, integral to the comprehensive management of endocarditis, aiming not only to address the acute infectious process but also to prevent long-term complications and improve overall patient outcomes [5,6,7].
While valvular surgery stands as a cornerstone in the management of endocarditis, the postoperative period introduces a distinct set of challenges, prominently featuring acute kidney injury (AKI). The kidneys, with their complex vascular network and high metabolic demands, are particularly vulnerable to the hemodynamic shifts and inflammatory responses associated with cardiac surgery [8]. Despite advancements in perioperative care, the occurrence of AKI remains a concerning complication, with the potential to influence both short-term and long-term outcomes.
AKI, defined by a sudden decline in kidney function, poses multifaceted risks to patients undergoing valvular surgery for endocarditis. Beyond its immediate impact on renal function, AKI is associated with increased morbidity and mortality, prolonged hospital stays, and potential long-term renal complications [9]. Understanding the factors contributing to AKI in this specific patient population is crucial for developing targeted interventions that may mitigate its occurrence, ultimately improving postoperative recovery and long-term prognosis.
The decision to delve into the intricate relationships between endocarditis, valvular surgery, and AKI is grounded in the clinical significance of this triad. While valvular surgery is a key component in managing endocarditis, the potential complications, especially AKI, warrant detailed exploration [8,9,10]. AKI, if not managed promptly and effectively, can significantly impact the overall trajectory of patient recovery and may contribute to adverse outcomes.
Moreover, the identification of modifiable factors associated with AKI in endocarditis patients undergoing valve surgery holds promise for informing targeted interventions [11,12]. If specific factors contributing to AKI can be pinpointed and modified, there exists an opportunity to improve renal outcomes and overall survival in this challenging patient group.
This study, therefore, seeks to unravel the complex dynamics between endocarditis, valvular surgery, and AKI, offering insights that may pave the way for tailored therapeutic approaches and enhanced patient care.
2. Materials and Methods
- Study Population
In this study, 130 patients from a single, large tertiary center in Salzburg, Austria, who were diagnosed with endocarditis and scheduled for valve surgery, were consecutively enrolled over a nine-year period (2013 to 2021). Patients with kidney failure requiring dialysis prior to surgery were excluded from the study. Data was analyzed retrospectively.
- Ethics Declaration
The study protocol was approved by the State of Salzburg Ethics Commission (EK: 1109/2023) and conducted in accordance to principles of the Declaration of Helsinki and Good Clinical Practice. Patient consent was waived due to retrospective nature of the study as determined by the State of Salzburg Ethics Commission.
- Endocarditis
All patients fulfilled the Duke criteria [13,14] for endocarditis valid at the time of the indication for surgery.
- Indication for Valve Surgery
The indication for cardiac surgical treatment of the valve(s) affected by endocarditis was made by an endocarditis team [13,14,15] consisting of cardiologists, cardiac surgeons and infectiologists.
- AKI
The study aimed to assess the incidence of acute kidney injury (AKI) in an endocarditis population by closely monitoring creatinine levels before and after surgery. The Kidney Disease: Improving Global Outcomes (KDIGO) criteria for AKI definition were utilized to quantify the occurrence of AKI [16,17]. We used the serum creatinine criteria for definition and classification of AKI because urinary excretion data were not continuously and completely available in the medical records of all patients.
- Outcomes investigated
Incidence of acute kidney injury (AKI): The study aimed to determine the frequency of postoperative AKI in endocarditis patients undergoing valve surgery.
Relevance of Creatinine Levels for AKI Detection: The investigation sought to establish a practical parameter for risk stratification by assessing the significance of creatinine levels, particularly focusing on preoperative to 7th postoperative day.
Association of AKI with short-term mortality: Primary outcomes included evaluating the relationship between AKI development and short-term mortality at specific intervals postoperatively (30, 60 and 180 days).
Exploration of modifiable factors contributing to AKI: The study aimed to identify variables amenable to modification that influence the development of AKI. Through a comprehensive assessment of various pre- and intraoperative factors, an attempt was made to uncover potential indicators up to 24 hours postoperatively, thus contributing to a more comprehensive understanding of the modifiable elements affecting AKI in patients undergoing valve surgery for endocarditis
- Statistical Analysis
The statistical analysis and graphical representation were conducted using SPSS (Version 25.0, SPSS Inc., USA). To assess the normal distribution of variables, the Kolmogorov–Smirnov–Lilliefors test was employed. Normally distributed metric data were presented as mean ± standard deviation (SD) and analyzed using an unpaired student’s t-test. For not-normally distributed metric data, the median and interquartile range (IQR) were used, and statistical analysis employed the Mann–Whitney-U-test. Categorical data were expressed as frequencies/percentages and compared using the chi-square test. Initially, a Kaplan–Meier curve, accompanied by log–rank tests and numbers at risk, was generated to examine potential differences in 30- to 180-day survival between patients with and without AKI (AKI+ vs. AKI-). To establish creatinine cut-off values at different endpoints (preoperative = D-1, at the day of surgery = D0, and postoperative D1-6), area under the receiver operator characteristics (AUROC) curves were constructed. The analysis included the area under the curve (AUC) and a separate assessment of the Youden Index (YI) based on the presence of AKI. Additional AUROC curves were calculated for predicting various creatinine cut-off values (D-1 to D3) with respect to 30-, 60- and 180-day mortality. Subsequently, a univariate binary logistic regression model was utilized to calculate the hazard ratio (HR) and 95% CI for factors influencing the presence or absence of AKI. For enhanced comparability, metric data underwent z-transformation. Following this, a multivariable binary logistic regression was conducted to identify independent predictors of AKI. Covariates associated with AKI in the univariate analysis (p < 0.050) were entered, and a backward variable elimination was performed. A p-value < 0.050 was considered statistically significant throughout the analyses.
3. Results
- Baseline Characteristics
A tabular overview of the baseline characteristics of the entire cohort, as well as the differentiation between AKI+ and AKI- patients with corresponding significance levels, is provided in Table 1. A total of 130 patients were enrolled in the study protocol. Based on KDIGO criteria, 46 of these (35.4%), exhibited AKI within the first seven post-operative days. The average age of the study population was 61.9 ± 14.4 years, with 70.8% being male. Staphylococci (36.9% of cases) and Streptococci (22.3%) were the most frequently detected germs. In 21 patients (16.2%), no sufficient pathogen evidence was found.
Patients with postoperative AKI were significantly less likely to have Streptococcus-induced endocarditis compared to those with normal renal function (8.7% vs. 29.8%; p = 0.006). Both the total surgery time, clamp time, and perfusion time were significantly prolonged in patients with AKI. The same pattern was observed for ventilation time and length of stay in the ICU. Ultimately, patients with AKI, in addition to a significantly increased preoperative EuroScore II (13.4 ± 9.6 vs. 8.8 ± 10.3; p = 0.001), also exhibited significantly higher postoperative 24-hour levels of lactate (4.6 ± 2.1 mmol/l vs. 2.4 ± 2.2 mmol/l; p = 0.023), Troponin T (1024.0 ± 3619.5 ng/l vs. 728.5 ± 798.3 ng/l; p = 0.007), and CK-MB (91.7 ± 117.1 U/l vs. 53.6 ± 28.3 U/l).
- Creatinine Levels: 2nd postoperative day as vulnerable day regarding kidney function
In order to assess the creatinine trajectory both preoperatively and postoperatively, patients underwent laboratory assessment at least once daily. The graphical and numerical representation of the respective creatinine trajectories for the entire cohort, as well as AKI- and AKI+ patients, is depicted in Figure 1 and Table 2.
In the overall population, a baseline creatinine level was observed on the day before surgery (D-1) at 1.1 ± 0.7 mg/dl. Subsequently, postoperatively, the peak was noted on the second postoperative day (D2) with a deviation to 1.6 ± 1.0 mg/dl, followed by a decline to an average of 1.2 - 1.3 mg/dl in the subsequent course. Patients who did not meet the criteria for AKI in the postoperative period started with an average creatinine of 1.1 ± 0.6 mg/dl, significantly lower than that of AKI patients (1.2 ± 0.7 mg/dl; p = 0.003). Furthermore, AKI+ patients maintained significantly higher postoperative creatinine levels compared to AKI- patients throughout the course. The peak was reached on D2 for both groups (1.3 ± 0.7 mg/dl vs. 2.2 ± 1.0 mg/dl; p < 0.001).
- Kaplan-Meier: AKI as a driving force for premature mortality
Not only were the in-hospital deaths significantly different between the AKI+ and AKI- cohorts (Table 1: 32.6% vs. 7.1%), but the influence of AKI as a driving force for premature mortality also manifested in short-term outcomes over a 180-day period. This observation is evident in the corresponding Kaplan-Meier curve, supported by log-rank tests and the numbers at risk depicted in Figure 2. Patients experiencing postoperative AKI consistently demonstrated a significantly elevated mortality throughout the follow-up period from 30 to 180 days. The 30-day mortality for AKI+ patients was already at 21.7%, rising to 39.1% after 6 months.
- AUROC-AKI: Creatinine of 1.35 mg/dl as relevant predictor for postoperative AKI
AUROC analyses were calculated to assess creatinine cut-off values on D-1 to D4 in relation to the presence of postoperative AKI (Figure 3).
The most accurate diagnostic prediction for the occurrence of AKI was achieved for the 2nd postoperative day (D2) using a creatinine cut-off of 1.35 mg/dl (AUC: 0.901; 95% CI: 0.849 — 0.953; sensitivity: 0.89; specificity: 0.79; YI: 0.68; p < 0.001). The same cut-off value of 1.35 mg/dl was observed on D0, D1, and D3, with AUC values ranging from 0.781 to 0.886 and p-values < 0.001.
- AUROC-Mortality: Creatinine of 1.35 mg/dl as relevant predictor for postoperative mortality
Further AUROC analyses were figured out to analyze creatinine cut-off values on D-1 to D3 in relation to postoperative mortality (Figure 4A: 30-day mortality; Figure 4B: 60-day mortality; Figure 4C: 180-day mortality).
Once again, the most reliable diagnostic performance was observed on the 2nd postoperative day with a creatinine cut-off of 1.35 mg and AUC values ranging from 0.708 to 0.789. Corresponding sensitivities ranged from 0.79 to 0.93, specificities from 0.61 to 0.64, YIs from 0.42 to 0.54, and p-values were ≤ 0.001.
- Binary Logistic Regression: Hemoglobin, CK-MB and renal excretion 2-3 hours after surgery as independent predictors for postoperative AKI
In order to investigate influencing factors concerning postoperative AKI, a univariate and multivariable binary logistic regression was figured out (Table 3).
For a clearer overview, only parameters with a p-value ≤ 0.050 were listed in the univariate analyses and subsequently included in the multivariable analysis. Ultimately, renal excretion 2-3 hours postoperatively, the minimally measured intraoperative hemoglobin in blood gas analysis, and the maximum CK-MB 24 hours postoperatively emerged as independent markers for the occurrence of postoperative AKI.
4. Discussion
The comprehensive analysis presented in this manuscript sheds light on critical aspects surrounding AKI in endocarditis patients undergoing valve surgery. Our findings, as outlined in the results section, highlight several key observations that warrant thoughtful consideration and further discussion.
- Postoperative frequency of AKI in patients undergoing valve surgery due to endocarditis
AKI occurs in approximately 20-30% of heart surgery cases [18,19,20]. The frequency of postoperative AKI in heart surgery varies, but it is particularly common in procedures involving cardiopulmonary bypass or valve surgeries [21]. The intricate nature of these surgeries, coupled with factors like prolonged exposure to anesthesia, inflammation, and ischemia-reperfusion injury due to reduced renal blood flow during surgery, contributes to the increased susceptibility of the kidneys to injury [22,23].
In the context of endocarditis, the risk of postoperative AKI may be heightened due to the infectious nature of the condition, potentially exacerbating the inflammatory response and contributing to renal complications [24]. The frequency of postoperative AKI in patients with endocarditis can vary depending on various factors, including the severity of the infection, the extent of cardiac involvement, and individual patient characteristics. While precise figures may vary across studies, research suggests that the incidence of AKI in patients undergoing valve surgery for endocarditis can range from 20% to 40% [13,24,25], with some studies reporting higher rates in more severe cases [9]. The incidence of postoperative AKI in our study population was substantial, with 35.4% of patients experiencing this complication. This underscores the vulnerability of patients with endocarditis to renal complications following valve surgery. In addition, the occurrence of AKI causes a significant increase in health care costs [10].
- Early detection of AKI: Overcoming the challenge of delay
Given the complexities of cardiac surgical procedures and the vulnerability especially of patients with endocarditis to perioperative kidney injury, there is a pressing need for enhanced surveillance strategies during this critical period. Implementing targeted monitoring protocols can help clinicians identify AKI promptly and intervene before irreversible damage occurs. Addressing the challenge of delayed AKI detection in cardiac surgery patients is essential for improving clinical outcomes and mitigating the impact of kidney injury on postoperative recovery [26].
Our study highlights the critical importance of overcoming this delay in AKI detection. We identified the peak in creatinine elevation on the 2nd postoperative day as a significant predictor for AKI, with a specific threshold of 1.35 mg/dl demonstrating optimal diagnostic accuracy. This finding underscores the pivotal role of early postoperative monitoring, particularly on the 2nd day, in identifying patients at risk of AKI and facilitating timely interventions.
However, the accuracy of traditional biomarkers, such as serum creatinine, can be compromised in the perioperative period, leading to delayed diagnosis and potential underestimation of AKI severity [27]. During the immediate postoperative phase, patients often undergo aggressive fluid resuscitation, which can result in dilutional effects on serum creatinine levels. This dilution may mask the true extent of kidney injury, making it challenging to identify AKI promptly [28]. Consequently, there is a risk of missing the optimal window for intervention, potentially exacerbating kidney damage and prolonging recovery time.
This fact reinforces the need for proactive measures during this critical timeframe to effectively manage and improve outcomes for patients at risk of postoperative AKI and, if necessary, to establish other biomarkers for early detection in the first two postoperative days [29].
- Consistancy of our creatinine cut-off value highlights AKI’s significance in short-term mortality prediction
Our study explored the association between creatinine, AKI and short-term mortality in endocarditis patients. The examination of creatinine cut-off values in relation to postoperative mortality provides relevant insights. The consistency of the again 1.35 mg/dl cut-off value across multiple time points (D0 to D3) and its association with short-term mortality at 30, 60 and 180 days postoperatively underscore its robust predictive value.
Postcardiac surgery serum creatinine has been described previously, in a study involving over 6000 patients, by Hou et al. [30] as a robust and versatile outcome indicator. Furthermore, our data support what has been reported by Ye et al. [31], who also found that creatine levels on postoperative day 2, (48 hours after cardiac surgery) provided the best prediction of future mortality.
Despite the pitfalls discussed above regarding creatinine determination, these observations underscore the utility of creatinine levels, particularly on the 2nd postoperative day, not only in the detection of AKI but also in the prognosis of short-term mortality.
- How can we prevent postoperative AKI following surgery for endocarditis?
In the pursuit of understanding modifiable factors contributing to AKI, our analyses identified renal excretion 2-3 hours postoperatively, the minimum intraoperative hemoglobin, and the maximum CK-MB 24 hours postoperatively as independent markers for postoperative AKI.
Early identification and monitoring of modifiable risk factors, such as renal excretion and intraoperative hemoglobin levels, are crucial for implementing targeted interventions to prevent AKI. Renal function should be assessed promptly postoperatively, with close monitoring of urine output, serum creatinine levels, and renal excretion rates in the hours immediately following surgery. Any decline in renal function or signs of impaired renal excretion should prompt early intervention to optimize hemodynamic stability and renal perfusion [32].
Intra- and postoperatively, strategies to minimize hemodynamic instability and blood loss are essential to preserve renal function. This includes meticulous attention to fluid balance, optimizing preload, and maintaining adequate perfusion pressure to ensure optimal renal blood flow [33,34,35]. Hemoglobin levels should be closely monitored throughout the surgical procedure, with prompt intervention to address any significant declines to mitigate the risk of renal hypoperfusion and subsequent injury [36].
Avoidance of nephrotoxic agents, such as certain medications and contrast agents, is essential to prevent additional stress on the kidneys. Close collaboration between multidisciplinary teams, including anesthesiologists, nephrologists, cardiologists, and cardiac surgeons, is vital for optimizing perioperative care and minimizing the risk of AKI. Furthermore, the integration of artificial intelligence (AI), as demonstrated in the study by Kalisnik et al. [37], could revolutionize early AKI detection, thereby enhancing perioperative care outcomes in patients undergoing cardiac surgery.
While our study provides valuable insights into the association between acute kidney injury (AKI) and endocarditis patients undergoing valve surgery, several limitations should be acknowledged. The study’s retrospective design introduces potential biases and relies on existing records, limiting its control and data collection. Being single-center, its findings may lack broader applicability to diverse patient populations. Additionally, the small sample size of 130 patients could compromise statistical power and generalizability. The focus on valve surgery for endocarditis may not extend to other surgical procedures with different AKI risk profiles. Lastly, while the KDIGO criteria for AKI are widely accepted, they may not capture the full spectrum of renal dysfunction.
5. Conclusions
This retrospective study of patients with endocarditis undergoing valve surgery highlights the substantial incidence of postoperative AKI. The identification of a specific creatinine threshold (1.35 mg/dl) on the 2nd postoperative day as a robust predictor for both AKI and short-term mortality offers a practical parameter for risk stratification. These find-ings emphasize the importance of vigilant monitoring, early intervention, and the potential for targeted interventions to enhance renal outcomes and overall survival in this challenging patient population.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: title; Table S1: title; Video S1: title.
Author Contributions
Conceptualization E.B.; Statistical analysis E.B; Writing — original draft preparation C.Din., C.Die., K.G., J.S., R.H., O.D. and E.B.; Writing — review and editing C.Din., U.C.H., R.S., R.R., J.M.K. and E.B.; Data collection C.Din., N.R., M.K., A.S.K. and E.B.; Project administration C.Din. and E.B.; Language spell checking C.Die. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study protocol was approved by the State of Salzburg Ethics Commission (EK: 1109/2023) and conducted in accordance to principles of the Declaration of Helsinki and Good Clinical Practice. Patient consent was waived due to retrospective nature of the study as determined by the State of Salzburg Ethics Commission.
Informed Consent Statement
Patient consent was waived due to to retrospective nature of the study.
Data Availability Statement
The data underlying this article will be shared on reasonable request to the corresponding author.
Acknowledgments
Graphical abstract was created with BioRender.com. Selected artwork (endocarditis image) shown in the graphical abstract was used from pictures provided by Servier Medical Art (Servier; https://smart.servier.com/), licensed under a Creative Commons Attribution 4.0 Unported License. E.B. dedicates this work to her head of department, whose guidance and request for a manuscript on acute kidney injury were invaluable in shaping this work.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be constructed as a potential conflict of interest.
References
- Rajani, R.; Klein, J.L. Infective endocarditis: A contemporary update. Clin. Med. 2020, 20, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Cahill, T.J.; Prendergast, B.D. Infective endocarditis. Lancet 2016, 387, 882–893. [Google Scholar] [CrossRef] [PubMed]
- Hubers, S.A.; DeSimone, D.C.; Gersh, B.J.; Anavekar, N.S. Infective Endocarditis: A Contemporary Review. Mayo Clin. Proc. 2020, 95, 982–997. [Google Scholar] [CrossRef] [PubMed]
- Rezar, R.; Lichtenauer, M.; Haar, M.; Hödl, G.; Kern, J.M.; Zhou, Z.; Wuppinger, T.; Kraus, J.; Strohmer, B.; Hoppe, U.C.; et al. Infective endocarditis – A review of current therapy and future challenges. Hell. J. Cardiol. 2021, 62, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.; Arockiam, A.D.; Jamil, Y.; El Dahdah, J.; Honnekeri, B.; El Helou, M.C.; Kassab, J.; Wang, T.K.M. Contemporary risk models for infective endocarditis surgery: a narrative review. Ther. Adv. Cardiovasc. Dis. 2023, 17. [Google Scholar] [CrossRef] [PubMed]
- Iaccarino, A.; Barbone, A.; Basciu, A.; Cuko, E.; Droandi, G.; Galbiati, D.; Romano, G.; Citterio, E.; Fumero, A.; Scarfò, I.; et al. Surgical Challenges in Infective Endocarditis: State of the Art. J. Clin. Med. 2023, 12, 5891. [Google Scholar] [CrossRef] [PubMed]
- AATS Surgical Treatment of Infective Endocarditis Consensus Guidelines Writing Committee Chairs; Pettersson, G. B.; Coselli, J.S.; Hussain, S.T.; Griffin, B.; Blackstone, E.H.; Gordon, S.M.; LeMaire, S.A.; Woc-Colburn, L.E. 2016 The American Association for Thoracic Surgery (AATS) consensus guidelines: Surgical treatment of infective endocarditis: Executive summary. J. Thorac. Cardiovasc. Surg. 2017, 153, 1241–1258. [Google Scholar] [CrossRef] [PubMed]
- Legrand, M.; Pirracchio, R.; Rosa, A.; Petersen, M.L.; Van der Laan, M.; Fabiani, J.-N.; Fernandez-Gerlinger, M.-P.; Podglajen, I.; Safran, D.; Cholley, B.; et al. Incidence, risk factors and prediction of post-operative acute kidney injury following cardiac surgery for active infective endocarditis: an observational study. Crit. Care 2013, 17, R220–10. [Google Scholar] [CrossRef] [PubMed]
- Von Tokarski, F.; Lemaignen, A.; Portais, A.; Fauchier, L.; Hennekinne, F.; Sautenet, B.; Halimi, J.-M.; Legras, A.; Patat, F.; Bourguignon, T.; et al. Risk factors and outcomes of early acute kidney injury in infective endocarditis: A retrospective cohort study. Int. J. Infect. Dis. 2020, 99, 421–427. [Google Scholar] [CrossRef]
- Ortiz-Soriano, V.; Donaldson, K.; Du, G.; Li, Y.; Lambert, J.; Rudy, M.; Cleland, D.; Thornton, A.; Fanucchi, L.C.; Huaman, M.A.; et al. Incidence and Cost of Acute Kidney Injury in Hospitalized Patients with Infective Endocarditis. J. Clin. Med. 2019, 8, 927. [Google Scholar] [CrossRef]
- Ritchie, B.M.; Hirning, B.A.; Stevens, C.A.; Cohen, S.A.; DeGrado, J.R. Risk factors for acute kidney injury associated with the treatment of bacterial endocarditis at a tertiary academic medical center. J. Chemother. 2017, 29, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Gagneux-Brunon, A.; Pouvaret, A.; Maillard, N.; Berthelot, P.; Lutz, M.; Cazorla, C.; Tulane, C.; Fuzellier, J.; Verhoeven, P.; Frésard, A.; et al. Acute kidney injury in infective endocarditis: A retrospective analysis. Med. Et Mal. Infect. 2019, 49, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.-P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef] [PubMed]
- Delgado, V.; Delgado, V.; Marsan, N.A.; Marsan, N.A.; de Waha, S.; de Waha, S.; Bonaros, N.; Bonaros, N.; Brida, M.; Brida, M.; et al. 2023 ESC Guidelines for the management of endocarditis. Eur. Hear. J. 2023, 44, 3948–4042. [Google Scholar] [CrossRef] [PubMed]
- Davierwala, P.M.; Marin-Cuartas, M.; Misfeld, M.; Borger, M.A. The value of an “Endocarditis Team”. Ann. Cardiothorac. Surg. 2019, 8, 621–629. [Google Scholar] [CrossRef]
- Khwaja, A. KDIGO Clinical Practice Guidelines for Acute Kidney Injury. Nephron Clin. Pr. 2012, 120, c179–c184. [Google Scholar] [CrossRef] [PubMed]
- Machado, M.N.; Nakazone, M.A.; Maia, L.N. Acute Kidney Injury Based on KDIGO (Kidney Disease Improving Global Outcomes) Criteria in Patients with Elevated Baseline Serum Creatinine Undergoing Cardiac Surgery. Rev. Bras. de Cir. Cardiovasc. 2014, 29, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Vives, M.; Hernandez, A.; Parramon, F.; Estanyol, N.; Pardina, B.; Muñoz, A.; Alvarez, P.; Hernandez, C. Acute kidney injury after cardiac surgery: prevalence, impact and management challenges. Int. J. Nephrol. Renov. Dis. 2019, 12, 153–166. [Google Scholar] [CrossRef]
- Schurle, A.; Koyner, J.L. CSA-AKI: Incidence, Epidemiology, Clinical Outcomes, and Economic Impact. J. Clin. Med. 2021, 10, 5746. [Google Scholar] [CrossRef]
- O’Neal, J.B.; Shaw, A.D.; Billings F.T., IV. Acute kidney injury following cardiac surgery: current understanding and future directions. Crit. Care 2016, 20, 187. [Google Scholar] [CrossRef]
- Ramos, K.A.; Dias, C.B. Acute Kidney Injury after Cardiac Surgery in Patients Without Chronic Kidney Disease. Rev. Bras. de Cir. Cardiovasc. 2018, 33, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Conrad, C.; Eltzschig, H.K. Disease Mechanisms of Perioperative Organ Injury. Obstet. Anesthesia Dig. 2020, 131, 1730–1750. [Google Scholar] [CrossRef] [PubMed]
- Nadim, M.K.; Forni, L.G.; Bihorac, A.; Hobson, C.; Koyner, J.L.; Shaw, A.; Arnaoutakis, G.J.; Ding, X.; Engelman, D.T.; Gasparovic, H.; et al. Cardiac and Vascular Surgery–Associated Acute Kidney Injury: The 20th International Consensus Conference of the ADQI (Acute Disease Quality Initiative) Group. J. Am. Hear. Assoc. 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Hermanns, H.; Alberts, T.; Preckel, B.; Strypet, M.; Eberl, S. Perioperative Complications in Infective Endocarditis. J. Clin. Med. 2023, 12, 5762. [Google Scholar] [CrossRef] [PubMed]
- Mir, T.; Uddin, M.; Qureshi, W.T.; Regmi, N.; Tleyjeh, I.M.; Saydain, G. Predictors of Complications Secondary to Infective Endocarditis and Their Associated Outcomes: A Large Cohort Study from the National Emergency Database (2016–2018). Infect. Dis. Ther. 2022, 11, 305–321. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.K.; Shaw, A.D.; Mythen, M.G.; Guzzi, L.; Reddy, V.S.; Crisafi, C.; Engelman, D.T. PeriOperative Quality Initiative and the Enhanced Recovery After Surgery Cardiac Workgroup. Adult Cardiac Surgery-Associated Acute Kidney Injury: Joint Consensus Report. J. Cardiothorac. Vasc. Anesthesia 2023, 37, 1579–1590. [Google Scholar] [CrossRef] [PubMed]
- Najafi, M. Serum creatinine role in predicting outcome after cardiac surgery beyond acute kidney injury. World J. Cardiol. 2014, 6, 1006–21. [Google Scholar] [CrossRef] [PubMed]
- Makris K (2018) The role of the clinical laboratory in the detection and monitoring of acute kidney injury. J Lab Precis Med. 3:4454. Accessed , 2024. https://jlpm.amegroups.org/article/view/4454.
- Cheruku, S.R.; Raphael, J.; Neyra, J.A.; Fox, A.A. Acute Kidney Injury after Cardiac Surgery: Prediction, Prevention, and Management. Anesthesiology 2023, 139, 880–898. [Google Scholar] [CrossRef]
- Hou, J.; Shang, L.; Huang, S.; Ao, Y.; Yao, J.; Wu, Z. Postoperative Serum Creatinine Serves as a Prognostic Predictor of Cardiac Surgery Patients. Front. Cardiovasc. Med. 2022, 9, 740425. [Google Scholar] [CrossRef]
- Ye, M.; Dai, Q.; Zheng, J.; Jiang, X.; Wang, H.; Lou, S.; Yu, K. The Significance of Post-operative Creatinine in Predicting Prognosis in Cardiac Surgery Patients. Cell Biochem. Biophys. 2014, 70, 587–591. [Google Scholar] [CrossRef]
- Kashani, K.; Rosner, M.H.; Haase, M.; Lewington, A.J.; O'Donoghue, D.J.; Wilson, F.P.; Nadim, M.K.; Silver, S.A.; Zarbock, A.; Ostermann, M.; et al. Quality Improvement Goals for Acute Kidney Injury. Clin. J. Am. Soc. Nephrol. 2019, 14, 941–953. [Google Scholar] [CrossRef] [PubMed]
- Suarez, J.; Busse, L.W. New strategies to optimize renal haemodynamics. Curr. Opin. Crit. Care 2020, 26, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Fellahi, J.-L.; Futier, E.; Vaisse, C.; Collange, O.; Huet, O.; Loriau, J.; Gayat, E.; Tavernier, B.; Biais, M.; Asehnoune, K.; et al. Perioperative hemodynamic optimization: from guidelines to implementation—an experts’ opinion paper. Ann. Intensiv. Care 2021, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kayilioglu, S.I.; Dinc, T.; Sozen, I.; Bostanoglu, A.; Cete, M.; Coskun, F. Postoperative fluid management. World J. Crit. Care Med. 2015, 4, 192–201. [Google Scholar] [CrossRef]
- Gumbert, S.D.; Kork, F.; Jackson, M.L.; Vanga, N.; Ghebremichael, S.J.; Wang, C.Y.; Eltzschig, H.K. Perioperative Acute Kidney Injury. Anesthesiology 2020, 132, 180–204. [Google Scholar] [CrossRef]
- Kalisnik, J.M.; Bauer, A.; Vogt, F.A.; Stickl, F.J.; Zibert, J.; Fittkau, M.; Bertsch, T.; Kounev, S.; Fischlein, T. Artificial intelligence-based early detection of acute kidney injury after cardiac surgery. Eur. J. Cardio-Thoracic Surg. 2022, 62. [Google Scholar] [CrossRef]
Figure 1.
Creatinine levels in the pre- and postoperative course after endocarditis-related valve surgery; 1A: Overall Cohort; 1B: AK- Patients; 1C: AK+ Patients.
Figure 1.
Creatinine levels in the pre- and postoperative course after endocarditis-related valve surgery; 1A: Overall Cohort; 1B: AK- Patients; 1C: AK+ Patients.
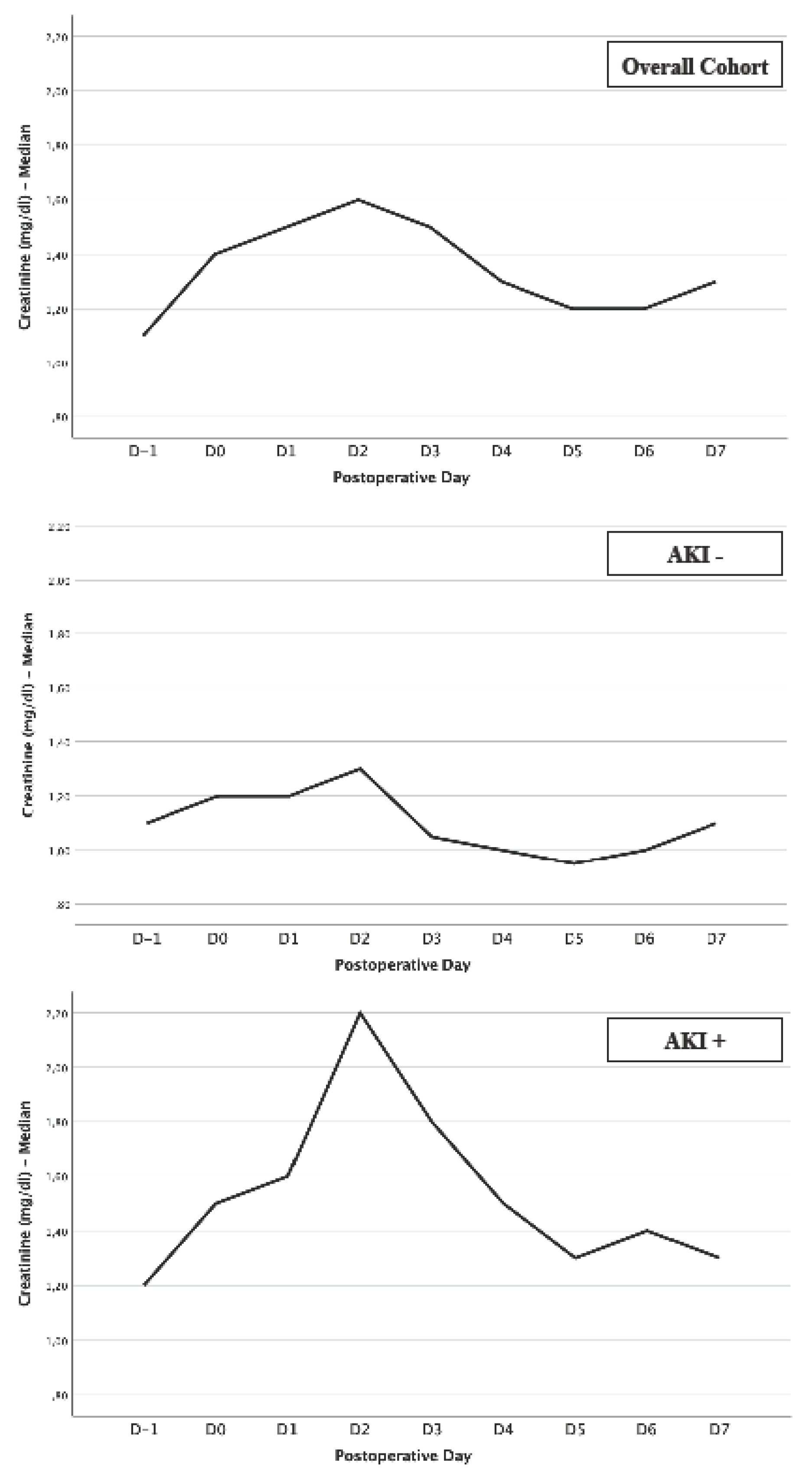
Figure 2.
Kaplan-Meier curve with corresponding numbers at risk and log-rank tests for detection of 30- to 180-day mortality in dependence of presence or absence regarding AKI.
Figure 2.
Kaplan-Meier curve with corresponding numbers at risk and log-rank tests for detection of 30- to 180-day mortality in dependence of presence or absence regarding AKI.
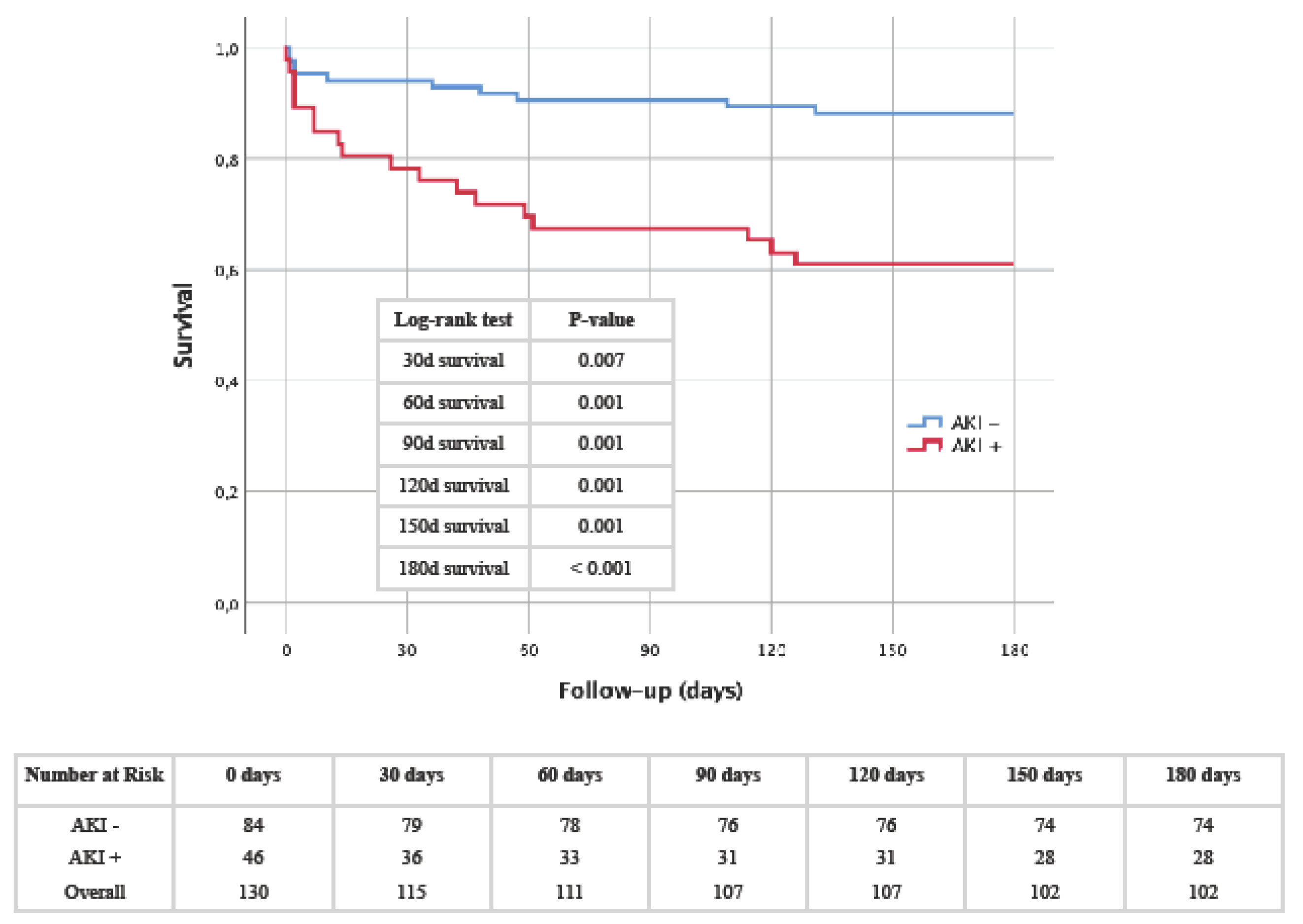
Figure 3.
AUROC analyses of perioperative (D-1 to D4) creatinine values for prediction of AKI with concerning cut-off values, Youden Index, sensitivity and specificity.
Figure 3.
AUROC analyses of perioperative (D-1 to D4) creatinine values for prediction of AKI with concerning cut-off values, Youden Index, sensitivity and specificity.
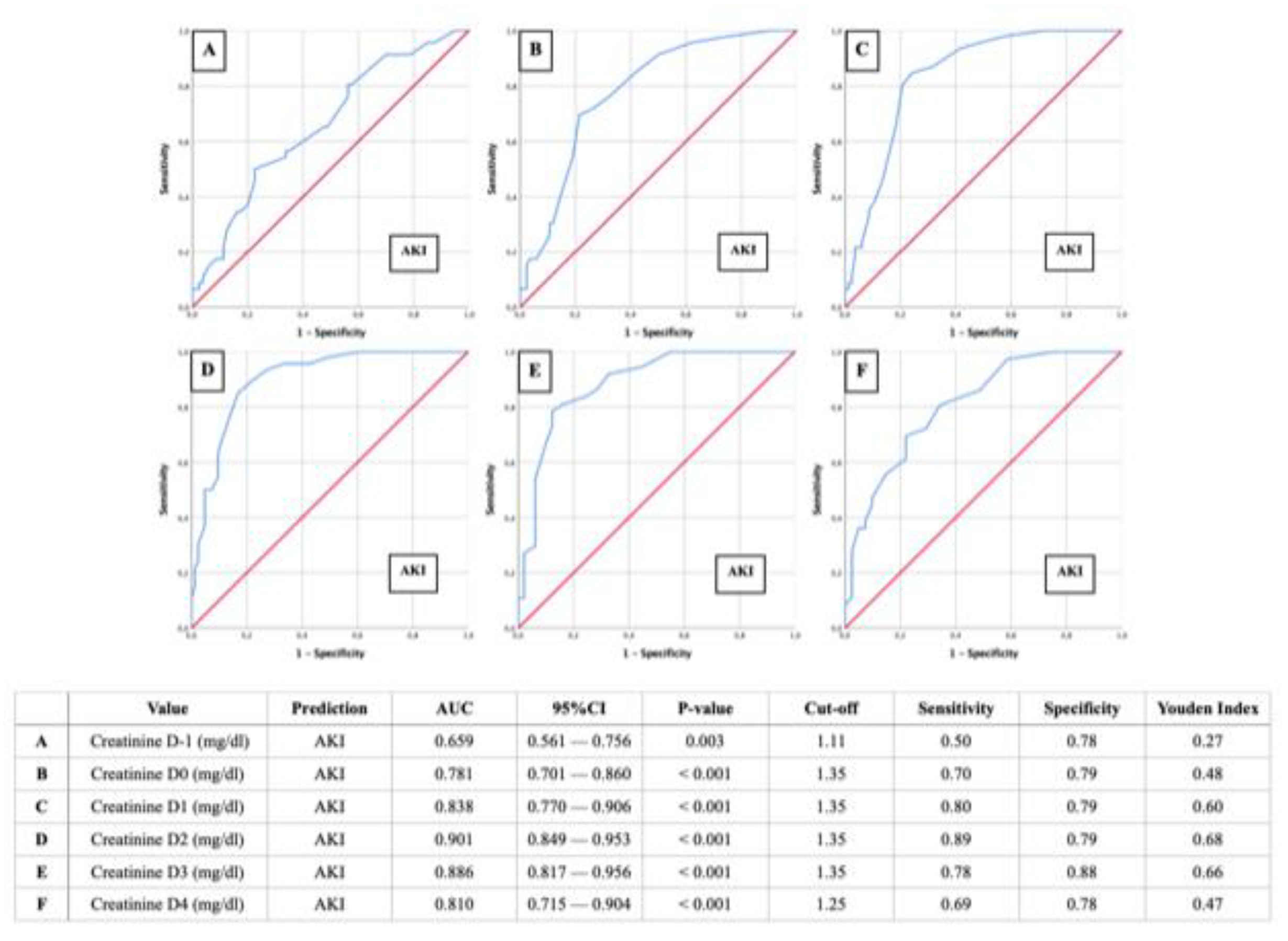
Figure 4.
AUROC analyses of perioperative (D-1 to D3) creatinine values for prediction of short-term mortalities with concerning cut-off values, Youden Index, sensitivity and specificity; 4A: 30-day mortality; 4B: 60-day mortality; 4C: 180-day mortality.
Figure 4.
AUROC analyses of perioperative (D-1 to D3) creatinine values for prediction of short-term mortalities with concerning cut-off values, Youden Index, sensitivity and specificity; 4A: 30-day mortality; 4B: 60-day mortality; 4C: 180-day mortality.
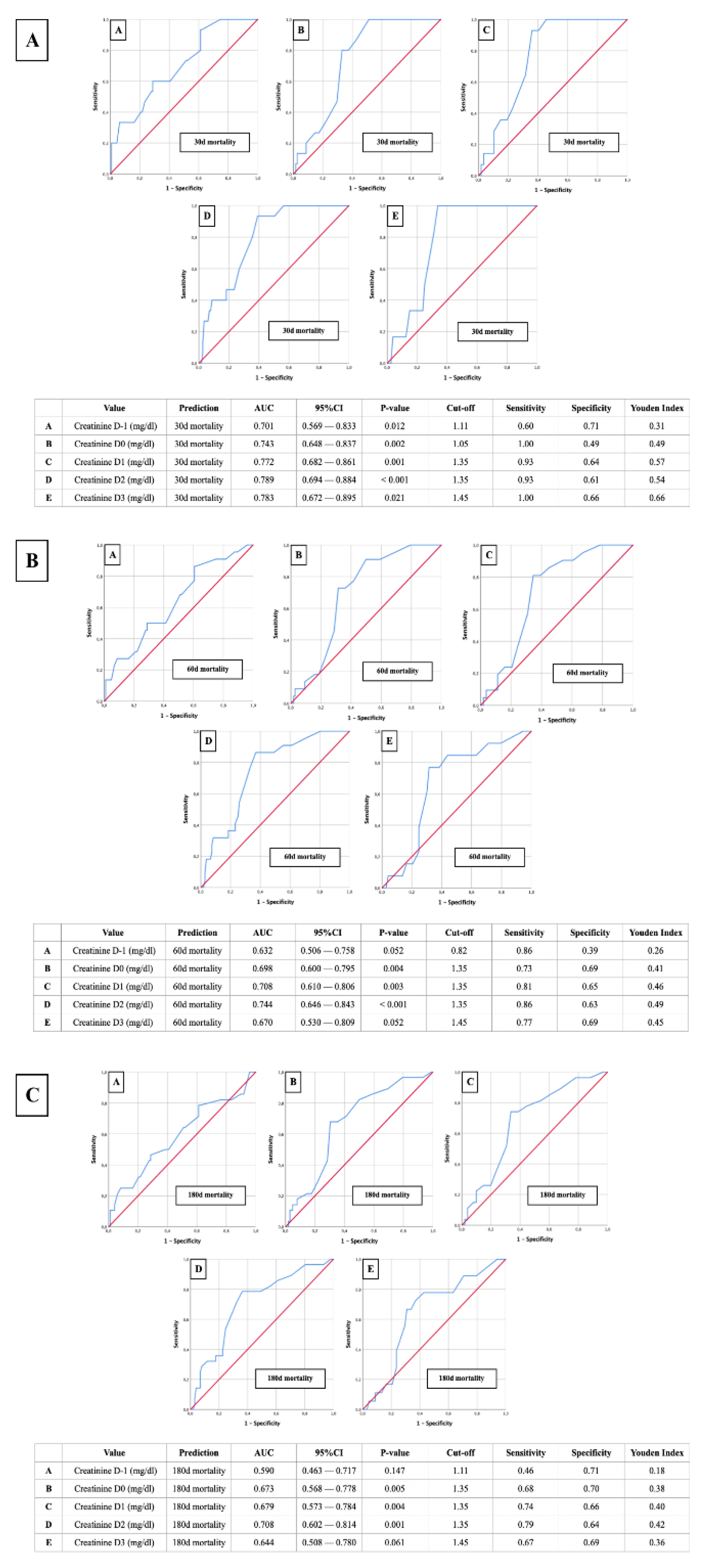

Table 1.
Baseline characteristics of overall study cohort and presence or absence of AKI.
| Total | AKI+ | AKI- | P-value | |
|---|---|---|---|---|
| No. (%) | ||||
| Total | 130 (100) | 46 (35.4) | 84 (64.6) | |
| Gender (male) | 92 (70.8) | 31 (67.4) | 61 (72.6) | 0.531 |
|
Age < 20 20 - 39 40 - 59 60 - 79 ≥ 80 |
1 (0.8) 14 (10.8) 29 (22.3) 81 (62.3) 5 (3.8) |
0 (0.0) 3 (6.5) 6 (13.0) 35 (76.1) 2 (4.3) |
1 (1.2) 11 (13.1) 23 (27.4) 46 (54.8) 3 (3.6) |
0.458 0.248 0.060 0.016 0.826 |
|
BMI < 18.5 18.5 - 24.9 25.0 - 29.9 30.0 - 34.9 35.0 - 39.9 ≥ 40.0 |
2 (1.5) 50 (38.5) 55 (42.3) 17 (13.1) 6 (4.6) 0 (0.0) |
0 (0.0) 14 (30.4) 21 (45.7) 7 (15.2) 4 (8.7) 0 (0.0) |
2 (2.4) 36 (42.9) 34 (40.5) 10 (11.9) 2 (2.4) 0 (0.0) |
0.292 0.164 0.568 0.592 0.101 - |
|
NYHA NYHA I NYHA II NYHA III NYHA IV |
78 (60.0) 29 (22.3) 12 (9.2) 11 (8.5) |
25 (54.3) 8 (17.4) 8 (17.4) 5 (10.9) |
53 (63.1) 21 (25.0) 4 (4.8) 6 (7.1) |
0.330 0.319 0.017 0.465 |
|
Microbiology Staphylococcus spp. - Staphylococcus aureus - Staphylococcus epidermidis Streptococcus spp. - Streptococcus mitis/oralis - Streptococcus sanguis/parasanguis Enterococcus spp. - Enterococcus faecalis HACEK group Candida spp. Mixed Infection Others Negative Blood Cultures and PCRs |
48 (36.9) 37 (28.5) 6 (4.6) 29 (22.3) 10 (7.7) 9 (6.9) 17 (13.1) 16 (12.3) 1 (0.8) 1 (0.8) 8 (6.2) 5 (3.8) 21 (16.2) |
22 (47.8) 18 (39.1) 2 (4.3) 4 (8.7) 2 (4.3) 1 (2.2) 7 (15.2) 7 (15.2) 0 (0.0) 0 (0.0) 4 (8.7) 0 (0.0) 9 (19.6) |
26 (31.0) 19 (22.6) 4 (4.8) 25 (29.8) 8 (9.5) 8 (9.5) 10 (11.9) 9 (10.7) 1 (1.2) 1 (1.2) 4 (4.8) 5 (6.0) 12 (14.3) |
0.057 0.046 0.914 0.006 0.290 0.114 0.592 0.455 0.458 0.458 0.372 0.458 0.434 |
|
Pre-existing Conditions Diabetes mellitus Arterial Hypertension CVD Previous Myocardial Infarction Atrial fibrillation Previous Aortocoronary Bypass Pacemaker (before Endocarditis) COPD Nicotine Consumption Hyperlipidemia Stroke (before Endocarditis) PAOD Chronic Kidney Disease Chronic Heart Failure |
19 (14.6) 66 (50.8) 40 (30.8) 8 (6.2) 35 (26.9) 15 (11.5) 9 (6.9) 8 (6.2) 15 (11.5) 53 (40.8) 11 (8.5) 8 (6.2) 18 (13.8) 22 (16.9) |
5 (10.9) 26 (56.5) 14 (30.4) 3 (6.5) 16 (34.8) 7 (15.2) 3 (6.5) 6 (13.0) 4 (8.7) 22 (47.8) 5 (10.9) 3 (6.5) 6 (13.0) 5 (10.9) |
14 (16.7) 40 (47.6) 26 (31.0) 5 (6.0) 19 (22.6) 8 (9.5) 6 (7.1) 2 (2.4) 11 (13.1) 31 (36.9) 6 (7.1) 5 (6.0) 12 (14.3) 17 (20.2) |
0.371 0.332 0.951 0.897 0.135 0.331 0.894 0.016 0.453 0.226 0.465 0.897 0.845 0.173 |
|
Premedication Beta-Blocker Diuretics ACEI/ARB/ARNI Statins |
58 (44.6) 56 (43.1) 36 (27.7) 33 (25.4) |
23 (50.0) 25 (54.3) 17 (37.0) 16 (34.8) |
35 (41.7) 31 (36.9) 19 (22.6) 17 (20.2) |
0.361 0.055 0.081 0.068 |
|
Preoperative Conditions Elective Surgery Urgent Surgery Emergency Surgery Prosthetic Valve Endocarditis Cardiogenic shock |
9 (6.9) 97 (74.6) 24 (18.5) 35 (26.9) 1 (0.8) |
2 (4.3) 35 (76.1) 9 (19.6) 16 (34.8) 1 (2.2) |
7 (8.3) 62 (73.8) 15 (17.9) 19 (22.6) 0 (0.0) |
0.392 0.775 0.810 0.135 0.175 |
|
Intraoperative Conditions Endocarditis of One Heart Valve Endocarditis of Two Heart Valves Endocarditis of Three Heart Valves One Surgically Repaired Heart Valve Two Surgical Repaired Heart Valves Three Surgical Repaired Heart Valves Additional aortocoronary bypass Cardioplegia Blood Products |
111 (85.4) 19 (14.6) 0 (0.0) 79 (60.8) 43 (33.1) 8 (6.2) 11 (8.5) 124 (95.4) 94 (72.3) |
38 (82.6) 8 (17.4) 0 (0.0) 23 (50.0) 18 (39.1) 5 (10.9) 5 (10.9) 44 (95.7) 40 (87.0) |
73 (86.9) 11 (13.1) 0 (0.0) 54 (66.7) 25 (29.8) 3 (3.6) 6 (7.1) 80 (95.2) 54 (64.3) |
0.507 0.525 - 0.063 0.278 0.098 0.465 0.914 0.006 |
|
Postoperative Conditions ECMO Bleeding/Tamponade Stroke Valvular Complications Complicated Pneumonia Wound Healing Disorder Third-Degree Atrioventricular Block Sepsis Tracheostomy In-Hospital Death |
5 (3.8) 15 (11.5) 4 (3.1) 1 (0.8) 5 (3.8) 6 (4.6) 15 (11.5) 2 (1.5) 4 (3.1) 21 (16.2) |
3 (6.5) 6 (13.0) 2 (4.3) 1 (0.8) 4 (8.7) 4 (8.7) 4 (8.7) 0 (0.0) 2 (4.3) 15 (32.6) |
2 (2.4) 9 (10.7) 2 (2.4) 0 (0.0) 1 (1.2) 2 (2.4) 11 (13.1) 2 (2.4) 2 (2.4) 6 (7.1) |
0.240 0.691 0.535 0.175 0.033 0.101 0.453 0.292 0.535 < 0.001 |
| Mean ± SD | ||||
| Age (years) | 61.9 ± 14.4 | 65.7 ± 12.2 | 59.8 ± 15.1 | 0.023 |
| Height (cm) | 172.9 ± 7.8 | 171.9 ± 7.4 | 173.5 ± 8.0 | 0.265 |
| Weight (kg) | 79.4 ± 15.6 | 82.2 ± 15.5 | 77.9 ± 15.5 | 0.135 |
| BMI (kg/m2) | 26.5 ± 4.5 | 27.8 ± 4.6 | 25.8 ± 4.3 | 0.016 |
| BSA (m2) | 1.9 ± 0.2 | 1.9 ± 0.2 | 1.9 ± 0.2 | 0.403 |
| ACEF 2 | 3.1 ± 1.6 | 3.3 ± 1.5 | 3.0 ± 1.6 | 0.300 |
| EuroScore II | 10.4 ± 10.2 | 13.4 ± 9.6 | 8.8 ± 10.3 | 0.013 |
| Surgery Time (min) | 271.8 ± 114.8 | 316.4 ± 117.0 | 247.3 ± 106.6 | 0.001 |
| Clamping Time (min) | 104.0 ± 53.9 | 125.6 ± 58.9 | 92.1 ± 47.3 | 0.001 |
| Perfusion Time (min) | 158.4 ± 86.2 | 194.0 ± 96.5 | 138.9 ± 73.6 | < 0.001 |
| Hospitalization Days (d) | 20.6 ± 20.3 | 23.7 ± 22.6 | 19.0 ± 18.9 | 0.208 |
| Postoperative Days (d) | 24.5 ± 21.7 | 27.2 ± 24.8 | 23.1 ± 19.9 | 0.302 |
| Ventilation Period (h) | 55.5 ± 87.7 | 91.7 ± 99.9 | 35.7 ± 73.6 | 0.001 |
| ICU stay (h) | 240.8 ± 390.5 | 353.4 ± 493.8 | 179.1 ± 306.5 | 0.033 |
| Red Blood Cell Concentrates (No.) | 1.9 ± 2.7 | 2.2 ± 1.8 | 1.7 ± 3.1 | 0.402 |
| Platelet Concentrate (No.) | 0.4 ± 0.8 | 0.6 ± 0.9 | 0.3 ± 0.8 | 0.060 |
| FFPs (No.) | 1.1 ± 2.1 | 1.9 ± 2.5 | 0.7 ± 1.7 | 0.004 |
| Median ± IQR | ||||
| LVEF (%) | 55.0 ± 5.0 | 55.0 ± 4.5 | 55.0 ± 5.0 | 0.746 |
| Min. Hb — intraop. (g/dl) | 7.5 ± 1.0 | 7.4 ± 1.1 | 7.6 ± 1.3 | 0.056 |
| Min. Hb — 6h postop. (g/dl) | 9.1 ± 1.7 | 8.4 ± 1.3 | 9.5 ± 1.7 | 0.077 |
| Min. Hb — 24h postop. (g/dl) | 8.7 ± 1.5 | 7.9 ± 1.1 | 8.9 ± 1.2 | 0.075 |
| Max. Lactate — 6h postop. (mmol/l) | 2.6 ± 2.5 | 3.8 ± 3.3 | 2.3 ± 1.4 | 0.006 |
| Max. Lactate — 24h postop. (mmol/l) | 2.9 ± 2.8 | 4.6 ± 2.1 | 2.4 ± 2.2 | 0.023 |
| Max. Troponin T — 24h postop. (ng/l) | 800.0 ± 1380.5 | 1024.0 ± 3619.5 | 728.5 ± 798.3 | 0.007 |
| Max. CK-MB - 24h postop (U/l) | 57.8 ± 54.8 | 91.7 ± 117.1 | 53.6 ± 28.3 | < 0.001 |
| Min. MAP — intraop. (mmHg) | 47.0 ± 7.1 | 47.0 ± 7.1 | 49.0 ± 7.5 | 0.439 |
| Max. NOR — intraop. (ml/min/kg) | 0.3 ± 0.2 | 0.3 ± 0.2 | 0.3 ± 0.2 | 0.149 |
| ⌀ NOR — intraop. (ml/min/kg) | 0.2 ± 0.1 | 0.2 ± 0.2 | 0.2 ± 0.1 | 0.282 |
| Renal Excretion 1 - 2h (ml) | 40.0 ± 65.0 | 30.0 ± 22.5 | 45.0 ± 103.8 | 0.001 |
| Renal Excretion 2 - 3h (ml) | 40.0 ± 52.5 | 20.0 ± 30.0 | 50.0 ± 70.0 | < 0.001 |
| Drainage Volume — 6h postop. (ml) | 230.0 ± 285.0 | 350.0 ± 215.0 | 150.0 ± 145.0 | < 0.001 |
| Drainage Volume — 12h postop. (ml) | 270.0 ± 350.0 | 350.0 ± 287.5 | 150.0 ± 312.5 | < 0.001 |
| Drainage Volume — 24h postop. (ml) | 550 ± 587.5 | 800.0 ± 512.5 | 400 ± 548.8 | 0.008 |
| Fluide Volume — intraop. (l) | 3.2 ± 1.6 | 3.2 ± 1.6 | 3.2 ± 1.6 | 0.134 |
BMI: body mass index; CVD: cardiovascular disease; COPD: chronic obstructive pulmonary disease; PAOD: peripheral arterial occlusive disease; ACEI: angiotensin-converting-enzyme inhibitor; ARB: angiotensin receptor blocker; ARNI: angiotensin receptor-neprilysin inhibitor; ECMO: extracorporeal membrane oxygenation; BSA: body surface area; ICU: intensiv care unit; FFP: fresh frozen plasma; LVEF: left ventricular ejection fraction; Hb: hemoglobin; CK-MB: creatine phosphokinase-MB; MAP: mean arterial pressure; NOR: noradrenaline.
Table 2.
Overview of the perioperative creatinine courses (D-1 to D7) in the entire cohort and depending on the presence of AKI.
Table 2.
Overview of the perioperative creatinine courses (D-1 to D7) in the entire cohort and depending on the presence of AKI.
| Total | AKI- | AKI+ | P-value | |
|---|---|---|---|---|
| Median ± IQR | ||||
| Creatinine D-1 (mg/dl) | 1.1 ± 0.7 | 1.1 ± 0.6 | 1.2 ± 0.7 | 0.003 |
| Creatinine D0 (mg/dl) | 1.4 ± 0.8 | 1.2 ± 0.7 | 1.5 ± 0.9 | < 0.001 |
| Creatinine D1 (mg/dl) | 1.5 ± 0.8 | 1.2 ± 0.6 | 1.6 ± 0.9 | < 0.001 |
| Creatinine D2 (mg/dl) | 1.6 ± 1.0 | 1.3 ± 0.7 | 2.2 ± 1.0 | < 0.001 |
| Creatinine D3 (mg/dl) | 1.5 ± 1.0 | 1.1 ± 0.7 | 1.8 ± 1.0 | < 0.001 |
| Creatinine D4 (mg/dl) | 1.3 ± 0.9 | 1.0 ± 0.7 | 1.5 ± 1.0 | < 0.001 |
| Creatinine D5 (mg/dl) | 1.2 ± 0.7 | 1.0 ± 0.7 | 1.3 ± 0.9 | < 0.001 |
| Creatinine D6 (mg/dl) | 1.2 ± 1.0 | 1.0 ± 0.7 | 1.4 ± 1.2 | < 0.001 |
| Creatinine D7 (mg/dl) | 1.3 ± 0.8 | 1.1 ± 0.7 | 1.3 ± 1.6 | 0.003 |
Table 3.
Univariate and multivariable binary logistic regression analysis detecting AKI in patients with endocarditis undergoing valve surgery.
Table 3.
Univariate and multivariable binary logistic regression analysis detecting AKI in patients with endocarditis undergoing valve surgery.
| AKI Binary Logistic Regression | Univariate | Multivariable | ||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-value | Hazard Ratio (95% CI) | p-value | |
| Age | 1.601 (1.057 — 2.423) | 0.026 | 0.656 (0.062 — 6.982) | 0.727 |
| BMI | 1.572 (1.079 — 2.291) | 0.019 | 2.035 (0.579 — 7.149) | 0.268 |
| EuroScore II | 1.564 (1.080 — 2.265) | 0.018 | 1.329 (0.636 — 2.775) | 0.449 |
| Renal Excretion 0 - 1h (postoperative) | 0.331 (0.117 — 0.942) | 0.038 | 0.445 (0.073 — 2.703) | 0.379 |
| Renal Excretion 2 - 3h (postoperative) | 0.324 (0.141 — 0.744) | 0.008 | 0.003 (0.000 — 0.275) | 0.012 |
| Hb minimal (intraoperative) | 0.437 (0.212 — 0.900) | 0.025 | 0.203 (0.044 — 0.926) | 0.039 |
| Surgery Time | 1.873 (1.268 — 2.766) | 0.002 | 0.225 (0.007 — 7.564) | 0.405 |
| Clamping Time | 1.964 (1.292 — 2.985) | 0.002 | 0.220 (0.019 — 2.499) | 0.222 |
| Perfusion Time | 2.003 (1.316 — 3.048) | 0.001 | 1.260 (0.447 — 3.552) | 0.662 |
| Ventilation Time | 1.954 (1.285 — 2.972) | 0.002 | 3.096 (0.118 — 81.191) | 0.498 |
| Intensive Care Unit Time | 1.660 (1.036 — 2.660) | 0.035 | 0.421 (0.023 — 7.817) | 0.561 |
| Blood Products (intraoperative) | 3.704 (1.408 — 9.743) | 0.008 | 0.094 (0.006 — 1.524) | 0.096 |
| FFP (intraoperative) | 1.795 (1.232 — 2.616) | 0.002 | 2.388 (0.945 — 6.030) | 0.066 |
| Lactate maximum (6h postoperative) | 1.607 (1.058 — 2.441) | 0.026 | 00.461 (0.158 — 1.344) | 0.156 |
| Troponin T maximum (24h postoperative) | 2.722 (1.381 — 5.365) | 0.004 | 1.193 (0.050 — 28.343) | 0.913 |
| CK-MB maximum (24h postoperative) | 5.483 (1.965 — 15.300) | 0.001 | 10.671 (1.733 — 65.723) | 0.011 |
| Quantity of Surgically Treated Heart Valves | 1.885 (1.045 — 3.400) | 0.035 | 0.629 (0.045 — 8.755) | 0.730 |
BMI: body mass index; Hb: hemoglobin; FFP: fresh frozen plasma; CK-MB: creatine phosphokinase-MB.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



