
Submitted:
18 June 2024
Posted:
18 June 2024
You are already at the latest version
Abstract
Background: C-reactive protein (CRP) is a predictive biomarker of colorectal surgery (CRS) complications but has not been evaluated by comparing patients undergoing CRS with intracorporeal anastomosis (IA) or extracorporeal anastomosis (EA). Therefore, we aimed to describe postoperative CRP values between two groups of patients who underwent laparoscopic right hemicolectomy for right-side colon cancer with IA or EA. Methods: We retrospectively reviewed the data of patients affected by right-side colon cancers who underwent laparoscopic right-hemicolectomy with ileo-colic IA or EA between January 2016 and December 2022. Results: A total of 340 patients underwent laparoscopic right hemicolectomy. EA was performed in 238 (70%) and IA in 102 (30%) cases. Patients with IA showed significantly higher values of CRP in the second, third and fourth postoperative days (15.2 mg/dL vs 9.5 mg/dL p=
Keywords:
colorectal cancer
; laparoscopy
; c-reactive protein
; anastomosis
; postoperative
1. Introduction
Colorectal cancer (CRC) is the third most common cancer globally and the second leading cause of cancer-related mortality [1,2,3]. Minimally invasive hemicolectomy for right-side CRC is a commonly performed procedure [4,5]. However, despite the introduction of different surgical techniques and enhanced recovery protocols, morbidity remains considerable [6,7]. The anastomotic leak (AL) rate in colorectal surgery (CRS) ranges between 3% and 17%, depending on the anastomosis location, and it is associated with higher morbidity, mortality, costs and worse oncological outcomes, particularly in terms of local recurrence [8,9,10,11].
Studies have investigated reliable predictive biomarkers for colorectal complications [12,13,14,15,16,17]. However, no biomarkers are considered completely reliable and error-free when making early-stage diagnoses or when complications are present. Therefore, different clinical studies are searching for ways to diagnose ALs and other complications before clinical symptoms appear [13,18].
C-reactive protein (CRP) has been reported to be an important predictor of septic complications and ALs after an elective colorectal resection [19]. ALs can typically be ruled out when CRP is below a certain level, depending on the postoperative day (POD). However, the best response to elevated CRP values is not well defined. Some physicians remeasure CRP levels in the following days [15,20], while some centres perform computed tomography in patients with CRP levels >15 mg/dL on POD 2 or 3 [12].
Recent studies have suggested that the rate of change, i.e., the trajectory, of CRP levels may be more useful than a cut-off point [15,21]. However, CRP trajectory testing via comparing patients undergoing CRS with intracorporeal (IA) or extracorporeal anastomosis (EA) has not yet been evaluated. Therefore, we aimed to describe the postoperative CRP values between two groups of patients who underwent a laparoscopic right hemicolectomy for right-side colon cancer with IA or EA.
2. Material and Methods
We reviewed 340 consecutive patients who underwent a laparoscopic right-hemicolectomy with ileo-colic IA or EA between January 2016 and December 2022 at Fondazione IRCCS San Gerardo dei Tintori Hospital (Monza, Italy). All data were obtained from a prospectively maintained database and analysed retrospectively. All patients signed an informed consent form for the anonymous use of clinical data. We collected baseline characteristics and a co-morbidity index according to the Charlson Comorbidity Index (CCI), operative time (minutes), type of suture, anastomosis (IA or EA) and postoperative data [22]. Until 31 January 2020, patients received EA. After this date, we systematically introduced IA. The first 20 IA cases were dropped from the study as they were considered to be within the learning curve [23]. Postoperative complications according to the Clavien-Dindo classification (CD), including gastrointestinal bleeding, reoperation and hospital stay duration were collected and analysed [24]. Major complications were defined as when the CD score was ≥IIIa. CRP levels (mg/dL) were measured and collected at PODs 1, 2, 3 and 4.
2.1. Surgical Technique
For the IAs, we established intestinal continuity using a side-to-side isoperistaltic suturing technique. The arms of the linear vascular cutting stapler (EchelonTM/EchelonTM Flex Endopath, Johnson and Johnson/Ethicon or EndoGIATM/EndoGIATM Ultra, Medtronic/Covidien or SIGNIATM, Medtronic/Covidien) were inserted and fired through transverse incisions on the antimesenteric side of the terminal ileum and transverse colon. The enterotomy site was closed using a double layer of barbed suture (Filbloc®, Assut Europe S.p.A or V-Loc™, Medtronic). For the EAs, we established intestinal continuity using a manual side-to-side isoperistaltic suturing technique with a double layer of 3/0 polyglactin (VicrylTM, Ethicon) or mechanically using a stapler technique, similar to the IA procedure.
2.2. Perioperative Management
All patients were treated according to the Enhanced Recovery After Surgery (ERAS) protocol for CRS [7,25,26]. No patient received mechanical bowel preparation [7,27,28]. All patients received intravenous antibiotic prophylaxis with 2 g of cefoxitin and 500 mg of metronidazole within 60 minutes before starting surgery. In cases of allergy, 500 mg of azithromycin was administrated intravenously. At the end of each surgery, we verified the vascularisation of the anastomosis with indocyanine green [29]. Both groups followed the key points of the postoperative ERAS protocol, i.e., all patients were given oral liquid nutrition on the first POD, urinary catheters were almost always removed on the first POD, the nasogastric tube was removed at the end of the surgical procedure and patients were encouraged to initiate mobilisation from the first POD [7].
2.3. Statistical Analysis
Descriptive statistics are reported as percentages and means or medians with 25–75 interquartile ranges (IQRs) and minimum-maximum ranges. Differences between means were compared using the Mann-Whitney U test. The chi-square test and two-by-two cross tables were used to compare categorical data. Differences were statistically significant when p-values were <0.05. Statistical analyses were carried out using IBM SPSS Statistics for Macintosh, Version 27 (IBM Corp, Armonk, NY, USA).
3. Results
During the study period, 340 patients underwent laparoscopic right hemicolectomy for right-side colon cancer. IA was performed in 102 (30%) patients. Baseline patient characteristics are listed in Table 1. In total, 173 (50.9 %) patients were male, with 120 (50.4%) in the EA and 53 (52%) in the IA groups (p=0.795). Median age was the same: 73 years in both the EA and IA groups (p=0.348). No differences in patient comorbidities were found. The CCI distribution was similar in the two groups: 5 vs 6 in the EA and IA groups, respectively (p=0.522).
Operative characteristics are listed in Table 2. Manual sutures were used only in the EA group, whereas mechanical sutures were used in all IA patients and 40 (16.8%) EA patients. The median operative time was similar in both groups (172.5 minutes in the EA group vs 188 minutes in the IA group, p=0.059). Abdominal drainage was necessary for 141 (59.2%) EA patients and 27 (26.5%) IA patients (p<0.001). The number of lymph nodes harvested was similar between the two groups (20 in the EA group vs 19 in the IA group, p=0.523).
No significant differences in complication rates were found between the two groups (Table 3). Furthermore, the AL rate was similar between the two groups: 12 (5%) patients in the EA group vs 4 (3.9%) in the IA group (p=0.718). Gastrointestinal bleeding occurred in 2 (0.8%) patients in the EA group vs 6 (5.9%) in the IA group (p=0.218). Re-operation was necessary for 19 (8%) patients (10 for AL, 2 for gastrointestinal bleeding, 7 for anastomotic stenosis) in the EA group and for 6 (5.9%) patients in the IA group (3 for AL, 3 for gastrointestinal bleeding), which was not significantly different (p=0.567). There was no mortality in either group. The median hospital stay duration was 7 (IQR 6–9, p=0.236) days in the two groups.
Postoperative CRP values are reported in Table 4. As depicted in Figure 1, CRP values were 9.5 mg/dL for the EA group vs 15.2 mg/dL for the IA group (p<0.001) on POD 2, 8.7 mg/dL in the EA group vs 12.9 mg/dL in the IA group (p<0.001) on POD 3 and 5.6 mg/dL in the EA group vs 8.8 mg/dL in the IA group (p=0.006) on POD 4. Significant differences were also found considering patients without major complications: 8.7 mg/dL in the EA group vs 14.6 mg/dL in the IA group (p<0.001) on POD 2, 8.6 mg/dL in the EA group vs 12.6 mg/dL in the IA group (p<0.001) on POD 3 and 5.3 mg/dL in the EA group vs 8.4 mg/dL in the IA group (p=0.003) on POD 4. However, when we considered only patients with major complications (CD score ≥IIIa), no significant differences in CRP levels were observed postoperatively.
4. Discussion
The study examined different trajectories of CRP values during the first four PODs in patients who underwent laparoscopic right-side hemicolectomy for CRC with EA or IA in a referral centre. CRP values in the second, third and fourth PODs were higher in patients with IA and without significant differences in the complication rate. Both groups had similar CRP-level trajectories.
Different studies have reported correlations between CRP values and postoperative complications, such as ALs [13,14,15,30]. In a recent study, Yeung et al. conducted a systematic review and meta-analysis of the CRP values of 6677 patients and found a higher inflammatory index value in patients with AL [13]. In particular, the study identified CRP cut-off values associated with ALs on the fourth through seventh PODs of 12.3 mg/dL, 11.5 mg/dL, 10.5 mg/dL and 9.6 mg/dL, respectively, with a sensitivity and specificity of 100%. In a large systematic review, Singh et al. reported that CRP values were a useful negative predictive test for the development of ALs following CRS [30]. In that report, the authors analysed seven studies, with a total of 2483 patients, and derived CRP cut-off values of 17.2 mg/dL on the third POD and 12.4 mg/dL on the fourth POD, corresponding to a negative predictive value of 97%.
Our results showed that absolute CRP levels on POD 2, 3 and 4 were higher in the IA group, but the trend of the curves was similar in both groups (Figure 1 and Table 4). Furthermore, the increased CRP values were not correlated with the development of major complications. This finding casts doubt on the value of considering a single postoperative CRP value as an effective indicator of complications, as opposed to the trend of CRP levels in the days following surgery.
To explain our results, we analysed the surgical procedures used in our study. We hypothesised that faecal contamination in the abdomen and the trocars site during the anastomosis procedure could modify the inflammatory response in the IA group. Alternatively, using a self-retaining ring retractor and covering the surgical site during EA could provide better asepsis and control of the operating field, resulting in lower contamination. For these reasons, a single CRP value should be considered a useful tool in predicting complications but would not be completely reliable, particularly in IA patients.
In a paper by Milone et al., the authors considered surgical stress and metabolic response after total laparoscopic right colectomies. They described a significant difference in CRP trajectories, which is in contrast to our data [31]. In their cohort, CRP on the third POD was significantly higher in the EA than in the IA group. In that study, the authors justified advocating for a total laparoscopic approach when performing a right colectomy for CRC. However, the small sample size (they analysed 50 patients) could have underestimated the role of IA in causing an increase in the inflammatory index; although, changes in this response would not alter preferentially performing an IA after laparoscopic right hemicolectomy. This conclusion has also been confirmed by Van Oostendor et al. in a systematic review and meta-analysis describing different outcomes after a laparoscopic right hemicolectomy with IA and EA [32]. That study analysed 1492 patients and found that IA procedures were associated with reduced short-term morbidity and a decreased hospital stay duration, suggesting faster recovery. In a recent meta-analysis of randomised controlled trials comparing IA versus EA in minimally invasive right hemicolectomies, Zhang et al. showed that IA reduced the risk of postoperative paralytic ileus and shortened the incision length but prolonged the operative time [33]. No significant differences in bleeding, ALs, overall peri-operative morbidity or length of hospital stay were found. Our results are partially aligned with these studies. In terms of hospital stay for both groups, we found that patients were discharged from hospital in a median of seven days. However, overall complications were greater in the IA group (35.2% vs 31.5%, respectively).
Our study was limited by its retrospective design and lacked a dedicated study protocol. However, we used a large, prospectively collected register from a single high-volume centre and included a well-trained surgeon.
5. Conclusion
In conclusion, this study shows that postoperative CRP values in patients who underwent laparoscopic right hemicolectomy significantly differed between patients with IA and EA, despite comparable complication rates and clinical outcomes. The usefulness of CRP values for detecting complications should be carefully evaluated. Future studies and randomised clinical trials are needed to further assess CRP trajectories in patients undergoing CRS with IA and EA for CRC to evaluate its reliability as a predictor of complications.
Author Contributions
Conceptualization, Lorenzo Ripamonti and Marco Ceresoli; Data curation, Lorenzo Ripamonti, Andrea Scacchi and Nicolò Tamini; Formal analysis, Marco Ceresoli; Supervision, Mauro Totis, Marco Braga and Luca Nespoli; Visualization, Nicolò Tamini; Writing – original draft, Andrea Scacchi; Writing – review & editing, Lorenzo Ripamonti, Luca Nespoli and Marco Ceresoli.
Funding
This research received no external funding.
Proofreading
Professional proofreading and editing services by Cambridge Proofreading LLC (343 W Wolf Point Plaza, Chicago, IL, USA).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, Ethical review and approval were waived for this study, due to retrospective and anonymous nature of the present study.
Informed Consent Statement
Patient consent was waived due to retrospective and anonymous nature of the present study.
Data availability statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to hospital policy.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Keum, N.; Giovannucci, E. Global Burden Of Colorectal Cancer: Emerging Trends, Risk Factors And Prevention Strategies. Nat Rev Gastroenterol Hepatol 2019, 16, 713–732. [Google Scholar] [CrossRef]
- Marcellinaro, R.; Spoletini, D.; Grieco, M.; Avella, P.; Cappuccio, M.; Troiano, R.; Lisi, G.; Garbarino, G.M.; Carlini, M. Colorectal Cancer: Current Updates And Future Perspectives. J Clin Med 2023, 13. [Google Scholar] [CrossRef]
- Rocca, A.; Avella, P.; Scacchi, A.; Brunese, M.C.; Cappuccio, M.; De Rosa, M.; Bartoli, A.; Guerra, G.; Calise, F.; Ceccarelli, G. Robotic Versus Open Resection For Colorectal Liver Metastases In A "Referral Centre Hub&Spoke Learning Program". A Multicenter Propensity Score Matching Analysis Of Perioperative Outcomes. Heliyon 2024, 10, E24800. [Google Scholar] [CrossRef]
- Van Leersum, N.J.; Snijders, H.S.; Henneman, D.; Kolfschoten, N.E.; Gooiker, G.A.; Ten Berge, M.G.; Eddes, E.H.; Wouters, M.W.; Tollenaar, R.A.; Bemelman, W.A.; et al. The Dutch Surgical Colorectal Audit. Eur J Surg Oncol 2013, 39, 1063–1070. [Google Scholar] [CrossRef]
- Hannan, E.; Feeney, G.; Ullah, M.F.; Ryan, C.; Mcnamara, E.; Waldron, D.; Condon, E.; Coffey, J.C.; Peirce, C. Robotic Versus Laparoscopic Right Hemicolectomy: A Case-Matched Study. J Robot Surg 2022, 16, 641–647. [Google Scholar] [CrossRef]
- Schwenk, W.; Haase, O.; Neudecker, J.; Müller, J.M. Short Term Benefits For Laparoscopic Colorectal Resection. Cochrane Database Syst Rev 2005, 2005, Cd003145. [Google Scholar] [CrossRef]
- Gustafsson, U.O.; Scott, M.J.; Hubner, M.; Nygren, J.; Demartines, N.; Francis, N.; Rockall, T.A.; Young-Fadok, T.M.; Hill, A.G.; Soop, M.; et al. Guidelines For Perioperative Care In Elective Colorectal Surgery: Enhanced Recovery After Surgery (Eras(®)) Society Recommendations: 2018. World J Surg 2019, 43, 659–695. [Google Scholar] [CrossRef] [PubMed]
- Leahy, J.; Schoetz, D.; Marcello, P.; Read, T.; Hall, J.; Roberts, P.; Ricciardi, R. What Is The Risk Of Clinical Anastomotic Leak In The Diverted Colorectal Anastomosis? J Gastrointest Surg 2014, 18, 1812–1816. [Google Scholar] [CrossRef]
- Pronio, A.; Di Filippo, A.; Narilli, P.; Mancini, B.; Caporilli, D.; Piroli, S.; Vestri, A.; Montesani, C. [Anastomotic Dehiscence In Colorectal Surgery. Analysis Of 1290 Patients]. Chir Ital 2007, 59, 599–609. [Google Scholar] [PubMed]
- Khan, A.A.; Wheeler, J.M.; Cunningham, C.; George, B.; Kettlewell, M.; Mortensen, N.J. The Management And Outcome Of Anastomotic Leaks In Colorectal Surgery. Colorectal Dis 2008, 10, 587–592. [Google Scholar] [CrossRef]
- Marcellinaro, R.; Grieco, M.; Spoletini, D.; Troiano, R.; Avella, P.; Brachini, G.; Mingoli, A.; Carlini, M. How To Reduce The Colorectal Anastomotic Leakage? The Miracle Protocol Experience In A Cohort In A Single High-Volume Centre. Updates Surg 2023, 75, 1559–1567. [Google Scholar] [CrossRef]
- Leourier, P.; Pellegrin, A.; Regimbeau, J.M.; Sabbagh, C. Is Early Ct In Cases Of Elevated Postoperative Crp The Best Option For The Diagnosis Of Colorectal Anastomotic Leakage? Int J Colorectal Dis 2023, 38, 278. [Google Scholar] [CrossRef] [PubMed]
- Yeung, D.E.; Peterknecht, E.; Hajibandeh, S.; Torrance, A.W. C-Reactive Protein Can Predict Anastomotic Leak In Colorectal Surgery: A Systematic Review And Meta-Analysis. Int J Colorectal Dis 2021, 36, 1147–1162. [Google Scholar] [CrossRef]
- Tamini, N.; Bernasconi, D.; Ripamonti, L.; Lo Bianco, G.; Braga, M.; Nespoli, L. Clinical Validation Of The Comprehensive Complication Index In Colon Cancer Surgery. Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef]
- Stephensen, B.D.; Reid, F.; Shaikh, S.; Carroll, R.; Smith, S.R.; Pockney, P. C-Reactive Protein Trajectory To Predict Colorectal Anastomotic Leak: Predict Study. Br J Surg 2020, 107, 1832–1837. [Google Scholar] [CrossRef]
- Giaccaglia, V.; Salvi, P.F.; Antonelli, M.S.; Nigri, G.; Pirozzi, F.; Casagranda, B.; Giacca, M.; Corcione, F.; De Manzini, N.; Balducci, G.; et al. Procalcitonin Reveals Early Dehiscence In Colorectal Surgery: The Predics Study. Ann Surg 2016, 263, 967–972. [Google Scholar] [CrossRef] [PubMed]
- Perrella, A.; Giuliani, A.; De Palma, M.; Castriconi, M.; Molino, C.; Vennarecci, G.; Antropoli, C.; Esposito, C.; Calise, F.; Frangiosa, A. C-Reactive Protein But Not Procalcitonin May Predict Antibiotic Response And Outcome In Infections Following Major Abdominal Surgery. Updates Surg 2022, 74, 765–771. [Google Scholar] [CrossRef]
- Platt, J.J.; Ramanathan, M.L.; Crosbie, R.A.; Anderson, J.H.; Mckee, R.F.; Horgan, P.G.; Mcmillan, D.C. C-Reactive Protein As A Predictor Of Postoperative Infective Complications After Curative Resection In Patients With Colorectal Cancer. Ann Surg Oncol 2012, 19, 4168–4177. [Google Scholar] [CrossRef] [PubMed]
- Welsch, T.; Müller, S.A.; Ulrich, A.; Kischlat, A.; Hinz, U.; Kienle, P.; Büchler, M.W.; Schmidt, J.; Schmied, B.M. C-Reactive Protein As Early Predictor For Infectious Postoperative Complications In Rectal Surgery. Int J Colorectal Dis 2007, 22, 1499–1507. [Google Scholar] [CrossRef]
- Hoek, V.T.; Sparreboom, C.L.; Wolthuis, A.M.; Menon, A.G.; Kleinrensink, G.J.; D'hoore, A.; Komen, N.; Lange, J.F. C-Reactive Protein (Crp) Trajectory As A Predictor Of Anastomotic Leakage After Rectal Cancer Resection: A Multicentre Cohort Study. Colorectal Dis 2022, 24, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.R.; Pockney, P.; Holmes, R.; Doig, F.; Attia, J.; Holliday, E.; Carroll, R.; Draganic, B. Biomarkers And Anastomotic Leakage In Colorectal Surgery: C-Reactive Protein Trajectory Is The Gold Standard. Anz J Surg 2018, 88, 440–444. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; Mackenzie, C.R. A New Method Of Classifying Prognostic Comorbidity In Longitudinal Studies: Development And Validation. J Chronic Dis 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Ishizaki, T.; Mazaki, J.; Kasahara, K.; Udo, R.; Tago, T.; Nagakawa, Y. Learning Curve Of Intracorporeal Anastomosis In Laparoscopic Colectomy For Right Side Colon Cancer: A Cumulative Sum Analysis. Anticancer Res 2023, 43, 3341–3348. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification Of Surgical Complications: A New Proposal With Evaluation In A Cohort Of 6336 Patients And Results Of A Survey. Ann Surg 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- The Impact Of Enhanced Recovery Protocol Compliance On Elective Colorectal Cancer Resection: Results From An International Registry. Ann Surg 2015, 261, 1153–1159. [CrossRef] [PubMed]
- Ceresoli, M.; Pedrazzani, C.; Pellegrino, L.; Muratore, A.; Ficari, F.; Polastri, R.; Scatizzi, M.; Totis, M.; Tamini, N.; Ripamonti, L.; et al. Early Postoperative Low Compliance To Enhanced Recovery Pathway In Rectal Cancer Patients. Cancers (Basel) 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Greco, M.; Capretti, G.; Beretta, L.; Gemma, M.; Pecorelli, N.; Braga, M. Enhanced Recovery Program In Colorectal Surgery: A Meta-Analysis Of Randomized Controlled Trials. World J Surg 2014, 38, 1531–1541. [Google Scholar] [CrossRef] [PubMed]
- Irani, J.L.; Hedrick, T.L.; Miller, T.E.; Lee, L.; Steinhagen, E.; Shogan, B.D.; Goldberg, J.E.; Feingold, D.L.; Lightner, A.L.; Paquette, I.M. Clinical Practice Guidelines For Enhanced Recovery After Colon And Rectal Surgery From The American Society Of Colon And Rectal Surgeons And The Society Of American Gastrointestinal And Endoscopic Surgeons. Surg Endosc 2023, 37, 5–30. [Google Scholar] [CrossRef] [PubMed]
- Keller, D.S.; Ishizawa, T.; Cohen, R.; Chand, M. Indocyanine Green Fluorescence Imaging In Colorectal Surgery: Overview, Applications, And Future Directions. Lancet Gastroenterol Hepatol 2017, 2, 757–766. [Google Scholar] [CrossRef]
- Singh, P.P.; Zeng, I.S.; Srinivasa, S.; Lemanu, D.P.; Connolly, A.B.; Hill, A.G. Systematic Review And Meta-Analysis Of Use Of Serum C-Reactive Protein Levels To Predict Anastomotic Leak After Colorectal Surgery. Br J Surg 2014, 101, 339–346. [Google Scholar] [CrossRef]
- Milone, M.; Desiderio, A.; Velotti, N.; Manigrasso, M.; Vertaldi, S.; Bracale, U.; D'ambra, M.; Servillo, G.; De Simone, G.; De Palma, F.D.E.; et al. Surgical Stress And Metabolic Response After Totally Laparoscopic Right Colectomy. Sci Rep 2021, 11, 9652. [Google Scholar] [CrossRef] [PubMed]
- Van Oostendorp, S.; Elfrink, A.; Borstlap, W.; Schoonmade, L.; Sietses, C.; Meijerink, J.; Tuynman, J. Intracorporeal Versus Extracorporeal Anastomosis In Right Hemicolectomy: A Systematic Review And Meta-Analysis. Surg Endosc 2017, 31, 64–77. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Sun, Y.; Mao, W. Meta-Analysis Of Randomized Controlled Trials Comparing Intracorporeal Versus Extracorporeal Anastomosis In Minimally Invasive Right Hemicolectomy: Upgrading The Level Of Evidence. Int J Colorectal Dis 2023, 38, 147. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
C-Reactive-Protein trend in all patients.
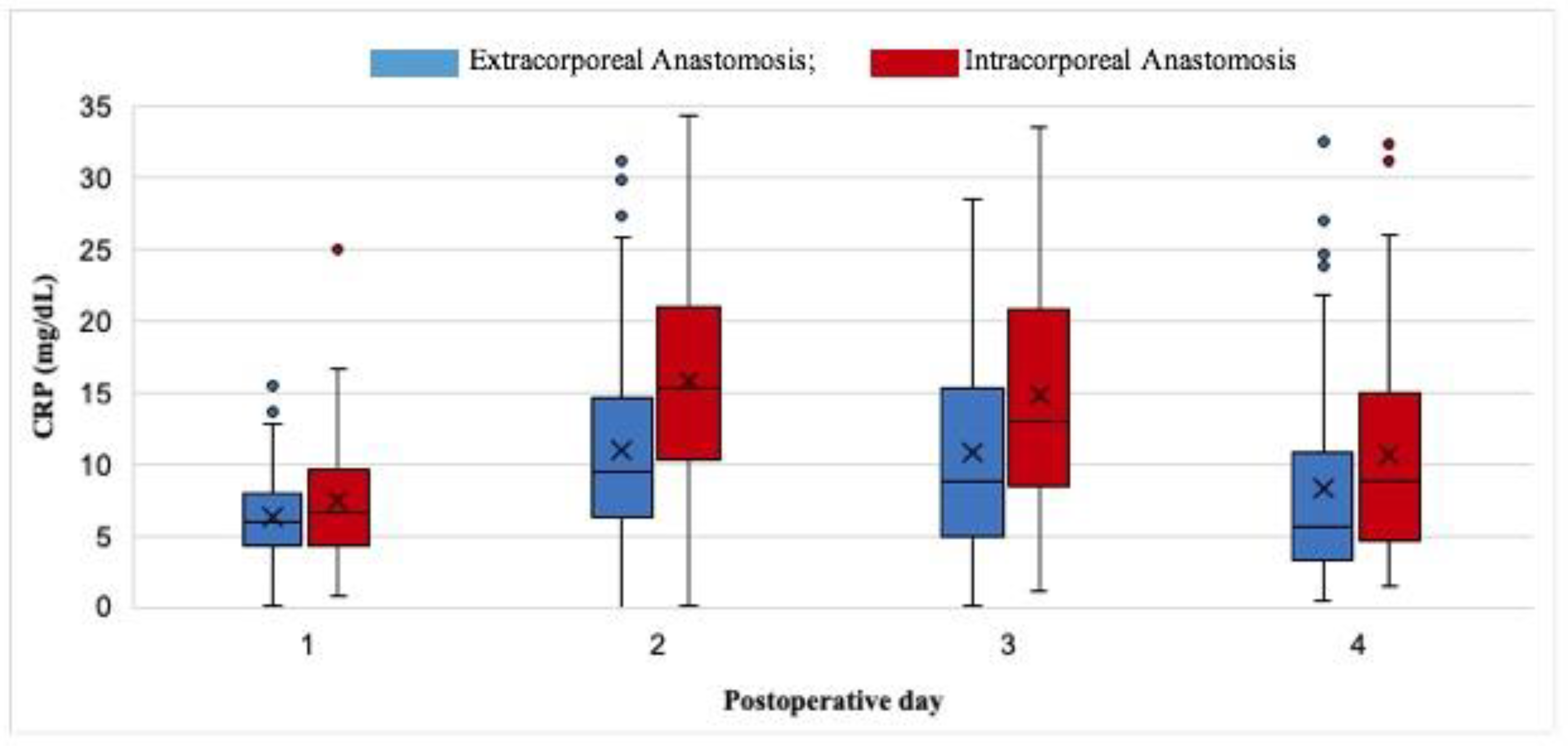

Table 1.
Baseline characteristics.
| CHARACTERISTICS | Overall | EA | IA | p-value |
|---|---|---|---|---|
| n (%) | 340 (100) | 238 (70) | 102 (30) | |
| Median age, years (IQR) | 73 (64-80) | 73 (63-79) | 73 (65-81) | 0.348 |
| Sex, Male, n (%) | 173 (50.9) | 120 (50.4) | 53 (52) | 0.795 |
| Previous surgery, n (%) | 107 (31.5) | 63 (26.5) | 44 (43.1) | 0.333 |
| Diabetes mellitus, n (%) | 49 (14.4) | 35 (14.7) | 14 (13.7) | 0.031 |
| CKD, n (%) | 24 (7.1) | 16 (6.7) | 8 (7.8) | 0.232 |
| Arterial Hypertension, n (%) | 122 (35.9) | 59 (24.8) | 63 (61.8) | 0.600 |
| COPD, n (%) | 16 (4.7) | 8 (3.4) | 8 (7.8) | 0.702 |
| Charlson Comorbidity Index, median (IQR) | 5 (4-7) | 5 (4-7) | 6 (5-7) | 0.522 |
CKD: Chronic Kidney Disease; COPD: Chronic Obstructive Pulmonary Disease; IQR: Interquartile range; IA: intracorporeal anastomosis; EA: extracorporeal anastomosis.
Table 2.
Operative outcomes.
| OPERATIVE CHARACTERISTICS | TOTAL | EA (n=238) | IA (n=102) | p-value |
|---|---|---|---|---|
| Operative time, min, median (IQR) | 179 (141.5-215) | 172.5 (140-210) | 188 (150-228) | 0.059 |
| Manual sutures, n (%) | 198 (58.2) | 198 (83.2) | 0 (0) | <0.001 |
| Mechanical sutures, n (%) | 142 (41.8) | 40 (16.8) | 102 (100) | <0.001 |
| Abdominal drainage, n (%) | 168 (49.4) | 141 (59.2) | 27 (26.5) | <0.001 |
| Lymph nodes, median (IQR) | 20 (15-26) | 20 (15-26) | 19 (15-25) | 0.523 |
IQR = Interquartile range; IA: intracorporeal anastomosis; EA: extracorporeal anastomosis.
Table 3.
Postoperative outcomes.
| POSTOPERATIVE OUTCOMES | Overall | EA (n=238) | IA (n=102) | p-value |
|---|---|---|---|---|
| Overall morbidity, n (%) | 94 (27.6) | 75 (31.5) | 36 (35.2) | 0.464 |
| Major complications, n (%) | 26 (7.6) | 20 (8.4) | 6 (5.9) | 0.475 |
| Clavien-Dindo grade | ||||
| IIIB, n (%) | 15 (4.4) | 13 (5.5) | 2 (2) | 0.167 |
| IVA, n (%) | 6 (1.8) | 5 (2.1) | 1 (1) | 0.496 |
| IVB, n (%) | 5 (1.5) | 2 (0.8) | 3 (2.9) | 0.127 |
| V, n (%) | 0 | 0 | 0 | |
| Gastrointestinal bleeding, n (%) | 8 (2.3) | 2 (0.8) | 6 (5.9) | 0.218 |
| Anastomotic leak, n (%) | 16 (4.6) | 12 (5) | 4 (3.9) | 0.718 |
| Superficial SSI, n (%) | 18 (5.3) | 12 (5) | 6 (5.9) | 0.677 |
| Deep SSI, n (%) | 12 (3.6) | 10 (4.2) | 2 (2) | 0.338 |
| Reoperation, n (%) | 25 (7.3) | 19 (8) | 6 (5.9) | 0.567 |
| LOS, days, median (IQR) | 7 (6-9) | 7 (6-9) | 7 (5-9) | 0.236 |
SSI: Surgical Site Infection; LOS: length of stay; IQR: Interquartile range; IA: intracorporeal anastomosis; EA: extracorporeal anastomosis.
Table 4.
CRP (mg/dL) trends.
| CRP LEVELS, OVERALL | ||||
|---|---|---|---|---|
| POSTOPERATIVE DAY | Overall | EA (n=238) | IA (n=102) | p-value |
| I median (IQR) | 6.2 (4.3-8.4) | 6 (4.4-8) | 6.7 (4.3-9.5) | 0.122 |
| II median (IQR) | 11.4 (6.8-16.7) | 9.5 (6.3-14.6) | 15.2 (10.5-20.9) | <0.001 |
| III median (IQR) | 11 (6.5-17.7) | 8.7 (5-15) | 12.9 (8.5-20.7) | <0.001 |
| IV median (IQR) | 7 (4.1-13.1) | 5.6 (3.3-10.6) | 8.8 (4.6-15) | 0.006 |
| CRP LEVELS IN PATIENTS WITH MAJOR COMPLICATIONS (CD≥IIIa) | ||||
| I median (IQR) | 7.5 (6.5-11.1) | 7.9 (6.6-10.8) | 7.5 (4.8-11.9) | 0.968 |
| II median (IQR) | 16.6 (15.1-23.1) | 15.9 (14.8-21) | 22.5 (19-31.9) | 0.142 |
| III median (IQR) | 19.2 (13.2-27.9) | 18.3 (7.4-26.7) | 24.4 (18.9-31.9) | 0.153 |
| IV median (IQR) | 14 (9.6-24.7) | 14 (8.5-24.7) | 16.8 (11.9-31.1) | 0.733 |
| CRP LEVELS IN PATIENTS WITHOUT MAJOR COMPLICATIONS | ||||
| I median (IQR) | 6 (4.2-8.2) | 5.8 (4.2-7.7) | 6.6 (4.1-9.3) | 0.068 |
| II median (IQR) | 10.9 (6.5-16.4) | 8.7 (6.1-13.3) | 14.6(10.1-20.5) | <0.001 |
| III median (IQR) | 9.8 (6-16.6) | 8.6 (4.6-13) | 12.6 (8.1-20.4) | <0.001 |
| IV median (IQR) | 6.1 (4-12.3) | 5.3 (3.2-9.3) | 8.4 (4.6-14.3) | 0.003 |
IQR: Interquartile range; IA: intracorporeal anastomosis; EA: extracorporeal anastomosis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



