
Submitted:
18 June 2024
Posted:
20 June 2024
You are already at the latest version
Abstract
Criteria air pollutant exposure has always been a major factor that negatively impacts human health through different pathways. One of the critical concerns is adverse birth outcomes associated with criteria air pollutant exposure such as low birth weight, preterm births, neonatal mortality, etc. Recent studies show that criteria air pollutant exposures are strongly associated with the elevated risk of preterm births defined as any birth occurring before 37 weeks of gestation. Bangladesh is one of the most polluted and has the highest preterm birth rate compared to other countries of the world. Although numerous global and regional studies investigate the impacts of criteria air pollutant exposure on preterm births, limited studies are available that investigated the impacts of the major criteria air pollutants on preterm births in recent years for Bangladesh. In this study, we employ the criteria air pollution data from the MERRA-2 model and satellite-sensed data regionally scaled for Bangladesh from NASA Giovanni (version 4.38) coupled with exposure-response modeling to quantify the impacts of CO, O3, PM2.5, SO2, and NO2 exposure on preterm births in Bangladesh during the 2015-2019 period. Based on the air quality analysis, the highest CO, O3, PM2.5, SO2, and NO2 exposures were observed in 2018 up to 272.8 /m3, 88.2 ppbv, 62.9 /m3, 20.5 /m3, and 11.6 ppbv respectively. This elevated amount of criteria air pollutant exposure has had direct implications for the increased rate of preterm births in Bangladesh. During 2015-2019, CO, O3, PM2.5, SO2, and NO2 exposures from all natural and anthropogenic emissions combinedly caused from 0.18 million [95% confidence interval (95CI): 0.08 – 0.29 million] up to 0.20 million [95CI: 0.08 – 0.32 million] preterm births among 4.3 million annual total live births each year which indicated a 4.4-4.9% preterm birth rate exclusively attributable to criteria air pollutant exposure in Bangladesh. Our study is critical for the overall wellbeing of the under-represented women and children in Bangladesh as it facilitates the quantitative evidence of preterm births caused by major air pollutant exposure and advocates the reduction of countrywide air pollution and establishment of well-aware community by facilitating low-cost air quality monitoring system in each household, necessary reformation of pollution prevention policies & regulations in national level and strict as well as vigilant law enforcement on human activities that causes air pollution.
Keywords:
preterm births
; Bangladesh
; criteria air pollutants
; adverse birth outcomes.
1. Introduction
Preterm births (PTB), defined as births before 37 weeks of gestation, is a major adverse birth outcome (ABO) that has several acute and long-term health effects. PTB is a worldwide public health concern that very often results in infant morbidity and mortality as well as long-term developmental impairments such as cerebral palsy, intraventricular hemorrhage, and chronic respiratory distress (Blencowe et al., 2012, 2013). PTBs account for more than 15 million premature births per year which corresponds to around 10% of all births globally (WHO, 2022). Complications resulting from PTBs are the second biggest cause of death in children under the age of five, accounting for almost 1 million deaths in 2015 (Perin et al., 2022; WHO, 2022). PTB is a major contributor to neonatal death and morbidity and is linked to long-term health issues such as chronic lung disease and neurodevelopmental abnormalities (Beck et al., 2010; McClure et al., 2018).
The prevalence of PTB varies considerably across countries, with rates ranging from 5% in certain high-income nations to more than 15% in some low- and middle-income countries (Blencowe et al., 2013) worldwide. PTB occurrence is disproportionately high in Africa and Asia, where approximately 85% of global PTBs occur each year (Barros et al., 2010; Beck et al., 2010; WHO, 2012). The severity of PTBs in Bangladesh is worse than ever as a recent study found that Bangladesh has the highest PTB rate of 16.2% among all the other countries around the world (Ohuma et al., 2023). Previous studies have shown that the prevalence of PTBs in Bangladesh is substantially high where in 2014, the estimated national PTB rate was 19.1% (Chawanpaiboon et al., 2019). A rural cohort study on mother-live-born baby pairs in Sylhet, Bangladesh, done between 2002 and 2006, found that 19.4% of newborns were PTBs (Baqui et al., 2013). Another recent research done in the suburban northern part of Bangladesh found that the overall PTB rate among pregnant women was 14.6% of all live births (Hossain et al., 2022). All these alarming PTBs rates call for immediate investigation of the multifaceted risks associated with PTBs in Bangladesh including environmental, socioeconomic, and physiological stressors in recent years.
One of the most abundant and hard-to-control environmental stressors is air pollution. Polluted air is a complex mixture of pollutants like carbon dioxide (CO2), nitrogen oxides (NOx), ozone (O3), sulfur dioxide (SO2), and fine particulate matter with an aerodynamic diameter of less than 2.5 (PM2.5) etc., which cause chronic health issues globally, particularly among vulnerable groups such as elderly population, pregnant women and their newborns. Exposure to the polluted air can lead to an immediate infiltration of the existing pollutants into the placenta which can influence fetal growth and development (Saenen et al., 2019). Several studies have shown a significant positive association between air pollution exposure and PTBs during pregnancy (Chen et al., 2021; Dadvand et al., 2013; Gehring et al., 2011; Han et al., 2018; Partha et al., 2022). According to different epidemiological and biological research, exposure to air pollution can cause inflammation, oxidative stress, placental insufficiency, etc. which can contribute to PTBs (Ritz et al., 2007). Elevated pollutant exposure during pregnancy slightly increased the odds of PTBs in normotensive and hypertensive women, with different effect modification patterns observed based on gestational age and specific pollutants (Weber et al., 2019). Women who were exposed to carbon monoxide levels of more than 0.91 ppm during the last 6 weeks of pregnancy had an increased risk of having PTBs (Ritz et al., 2007). Exposure to PM2.5 was found to significantly increase the risk of preterm birth during all trimesters of pregnancy, with the highest risk observed in the third trimester (Cai et al., 2020; Guo et al., 2018; Sun et al., 2015). A recent study on asthmatic mothers showed a higher risk of PTBs from NOx, CO, and SO2 exposure during the weeks of 34 to 36, and from O3 in week 34 (Mendola et al., 2016). A meta-analysis also found a significant association between PTB risk and exposure to CO and PM10 (Stieb et al., 2012).
Bangladesh experiences significant air pollution from various sources such as industrial emissions, transportation, brick kilns, fossil fuels, and biomass burning (Pavel et al., 2021; Salam et al., 2021; Siddiqui et al., 2020). Bangladesh ranked top among the most air-polluted countries in 2021, but by 2022 it had dropped to fifth place, as per the World Air Quality Report (IQAir, 2022; World Bank, 2022). This level of air pollution is extremely harmful to human health, and it may be contributing significantly to the increasing PTB rates across the country. In recent years, a very limited number of studies have investigated the association between air pollution exposure and PTBs in Bangladesh. A recent study focused on the association between air pollution exposure and PTBs in Bangladesh within Dhaka city only and found linearly increasing PTB rates from 9.0% to 15.2% across the lowest and highest categories of air quality index (AQI) exposure (Nahian et al., 2023). This study was initiated to fill this gap by investigating the possible association between PTB rates and air pollution exposure across Bangladesh in terms of AQI which lacks the investigation of increased risks of PTB based on the actual air pollutant exposure assessment on a national scale. On top of that, there is still a very limited amount of knowledge on the comprehensive assessment of the effect of outdoor exposure of different criteria air pollutants on pregnant women and PTB rates across the entire country. In this study, we focused on five criteria air pollutants which are CO, O3, PM2.5, SO2, and NO2 and their nationwide quantitative exposure impacts on PTBs in Bangladesh during 2015-2019.
2. Methodology
2.1. Remotely Sensed Data Collection
We collected the global concentration dataset of five major criteria air pollutants i.e., CO, O3, PM2.5, SO2, and NO2 during the timeframe of 2015-2019 and used global country mask data to target the domain of Bangladesh to investigate the regional exposure of the criteria air pollutants and their quantitative impacts on PTBs in Bangladesh. Table 1 shows the sources of global CO, O3, PM2.5, SO2, and NO2 concentrations used in this study from various instruments and methods. For the concentration and exposure of CO, PM2.5, and SO2, we relied on the Modern-Era Retrospective Analysis for Research and Applications, Version 2 (MERRA-2) data products from the Giovanni (NASA) Earth data website (https://giovanni.gsfc.nasa.gov/giovanni/) which allows users to search and download both model and observational Earth science data products from instruments and systems like MERRA-2, Ozone Monitoring Instrument (OMI), Atmospheric Infrared Sounder (AIRS), Goddard Earth Observing System (GEOS), Global Land Data Assimilation System Version 2 (GLDAS-2) etc. for different disciplines like aerosols, atmospheric chemistry, hydrology, ocean biology, water and energy cycle etc. for any timeline between 1984 up until 2023 and a wide range of spatial and temporal resolution. The MERRA-2 model is an updated atmospheric reanalysis dataset of its previous version MERRA offered by NASA’s Global Modeling and Assimilation Office (GMAO) which includes the type of observational data exclusively not accessible to MERRA and improves the GEOS model by supplying important updates and atmospheric schemes (GMAO, 2015; Gelaro et al., 2017). It incorporates satellite radiance data from both operational and research instruments and utilizes a 3-dimensional variational data assimilation analysis algorithm. The assimilation of radiation data necessitates meticulous quality control and bias correction procedures. Using a variety of data sources, MERRA-2 incorporates aerosol and meteorological observations within GEOS-5 (Goddard Earth Observing System Model, v.5) (Buchard et al., 2015; Gelaro et al., 2017; Yao et al., 2020). Numerous recent studies have utilized MERRA-2 data products to investigate crucial atmospheric scientific problems, including the variability of meteorological factors, such as temperature and precipitation, and their influence on weather patterns (Jenwitheesuk et al., 2022; Ryu & Min, 2021; Zhao et al., 2021). For the time period between January 1, 2015, and December 31, 2019, we extracted two-dimensional, monthly time-averaged PM2.5 and SO2 total surface mass concentration products from the M2TMNXAER (v5.12.4) dataset (GMAO-M2TMNXAER, 2015), and CO surface concentration from the M2TMNXCHM (v5.12.4) dataset (GMAO-M2TMNXCHM, 2015) of MERRA-2 model. PM2.5, CO, and SO2 data were extracted with a spatial resolution of 0.5° latitude 0.625° longitude. The monthly time-averaged, level 3 O3 mole fraction data in the air during both day (ascending) and night (descending) time were downloaded with a spatial resolution of 1° latitude 1° longitude from the AIRS3STM (v7.0) dataset (GES DISC, 2019) from NASA's Atmospheric Infrared Sounder (AIRS) project available on the Giovanni portal. The AIRS is an advanced grating spectrometer installed in the Aqua satellite located at NASA’s second Earth Observing System (EOS) polar-orbiting platform that measures the infrared radiation emitted by Earth’s atmosphere to produce vertical profiles of atmospheric temperature, moisture, the concentration of trace gases, etc. and is capable of tracking the entire vertical distribution of O3, enabling the detection of O3 transport from the upper atmosphere to the lower atmosphere during specific atmospheric occurrences.
As there was limited availability of remotely sensed or in-situ measured open-source NO2 surface concentration data on a global scale, we obtained user-developed monthly time-averaged global surface NO2 concentration data with a spatial resolution of 0.0083° latitude 0.0083° longitude (~1 km2) from a recent study of Anenberg et al. (2022). In that study, the authors created a new dataset of global surface annual average NO2 concentrations in 5-year temporal resolution from 1990 to 2010, and then annual temporal resolution from 2010 to 2019. The researchers utilized an already existing global NO2 concentration dataset from a land use regression (LUR) model prepared by Larkin et al. (2017) which had a spatial resolution of 100 m 100 m and covered the years 2010-2012. The study of Anenberg et al. (2022) discovered high bias in NO2 concentrations for rural areas in Larkin et al.’s datasets and made some adjustments using surface NO2 concentrations obtained from the OMI satellite. They also compared their NO2 concentration estimates in urban and rural areas to monitors in the United States, Canada, and Europe to assess the performance of the adjustments made in their study to decrease the overall uncertainty and increase the credibility of the dataset. Overall, for all the extracted concentration datasets for different air pollutants, we used a filtering algorithm to get rid of any invalid, missing, or non-arithmetic data points and modified the default resolution of each dataset to 0.1° latitude 0.1° longitude (10 km ) to be constant with other datasets like the global country mask and live birth data. All the monthly air quality data of CO, O3, PM2.5, SO2, and NO2 was compiled to prepare the 5-year-annual-average concentration data for each criteria air pollutant for the years 2015-2019 for the final analysis. All information regarding the source of remotely sensed data products of the criteria pollutants is provided in Table 1.
2.2. Evaluation of Criteria Air Pollutant Datasets
To evaluate the air quality data retrieved from remotely sensed and user-generated data sets that uses satellite observations (hereafter collectively referred as remotely-sensed data sets), we collected monthly reports of CO, O3, PM2.5, SO2, and NO2 in-situ observational data during the timeframe of 2015-2019 supplied by Department of Environment (DoE) of Government of People’s Republic of Bangladesh (http://case.doe.gov.bd) and compared them with our remotely-sensed datasets by the means of Bland-Altman plots. Based on this study’s timeframe, continuous DoE monthly reports for all five criteria air pollutants were only available for the years 2015, 2016 and 2017 so we compared the remotely sensed data sets with the in-situ data for only those specific years to avoid uncertainty. Multiple locations all over the country included air-quality stations within Dhaka like Sangshad Bhaban, Firmgate, Darus-Salam, Gazipur, and outside of Dhaka like Narayangonj; Khulshi, Chattogram; Agrabad, Chattogram; Red Crecent Campus, Sylhet; Baira, Khulna; Sopura, Rajshahi; DFO office campus, Barisal supplied the daily-averaged in-situ CO, O3, PM2.5, SO2, and NO2 data on DoE website which were later used to generate the monthly in-situ data reports and finally incorporated in this evaluation. Units and time-averaging methods are kept constant between remotely sensed and in-situ data sets and latitude and longitude indices were calculated based on the actual latitude and longitude of each physical location of air-quality stations to retrieve the accurate amount of CO, O3, PM2.5, SO2, and NO2 exposure from the remotely sensed data in the identical time format (yearly, daily, or hourly) of the in-situ measurements. Association between the remotely sensed data and the field measurements was then computed with the help of Bland-Altman plots where the y-axis shows the differences in concentrations between each pair of in-situ observations and remotely sensed data and the x-axis shows the mean of each pair of in-situ observations and remotely sensed data. Bland-Altman plots help us understand the association between the in-situ and remotely sensed data by the proximity of each point with respect to the central mean bias line and upper and lower limits of agreement (LOA) (alternative of 95% confidence interval) that denotes +1.96 and -1.96 standard deviations (SD) respectively for each criteria air pollutant.
2.3. Preterm Birth Calculation from Criteria Air Pollutant Exposure
In this study, we estimated the criteria air pollutant induced PTBs in Bangladesh from 2015 to 2019. An exposure-response model shown in Eqn. 1 is incorporated followed by recent exposure-response studies (Huang et al., 2021; Partha et al., 2022; Xiong et al., 2022) to calculate the number of PTBs (Ni,j) caused by the exposure of each criteria air pollutant in each grid box of longitude (i) and latitude (j) where BIRi,j is the gridded live births in each grid box (i, j), PTBRc is the country-level baseline of preterm birth rate (PTBRc) , and ORi,j is the Odds Ratio (OR) associated with each criteria air pollutant exposure and PTB in each horizontal model grid box of longitude (i) and latitude (j).
Poverty Mapping of the World version 2.01 supplied by the Center for International Earth Science Information Network – CIESIN (CIESIN, 2021) at horizontal resolution 2.5 min 2.5 min was used to account for the baseline of the live births, BIRi,j, in each grid box for 2015. As the actual estimate of global live births (141.6 Million) reported by the UN – World Population Prospects (https://population.un.org/wpp/) is different than the CIESIN reported global live births (127.3 Million) for 2015, scaling factors were calculated to reduce underestimation of live births based on the ratio of total global live births in each respective year from UN reports and from CIESIN data and multiplied with the CIESIN gridded live birth data to process and create the upscaled gridded live birth data for the study period (shown in supplemental Figure S1). The country mask of Bangladesh is then used to calculate the number of live births in each grid box within the domain of Bangladesh. PTBRc is derived as the ratio of the prevalence of PTBs in Bangladesh retrieved from the Global Burden of Disease 2019 dataset (GBD 2019 Risk Factors Collaborators, 2020). and the total number of live births in Bangladesh in each respective year. Eqn. (2) shows the basic expression of the OR in each grid box where γ denotes the log-linear slope between the exposure of each criteria air pollutant and the associated PTB, Ci,j, is the air pollutant concentration in each grid box to which the population is exposed and Co is the counterfactual concentration of each pollutant below which there are no health impacts associated with the exposure which is either assumed or retrieved from recent studies.
The log-linear slope γ can be derived using Eqn. (3) where OR is the measured odds of PTB with the increment of specific air pollutant concentration C. For the measured value of OR in Eqn. (3), we have incorporated the results from different recent studies that investigated the association of PTB with CO (Li et al., 2016); O3 (Rappazzo et al., 2021); PM2.5 (Sun et al., 2015); SO2 (Liu et al., 2019) and NO2 (Llop et al., 2010). Detailed equations for ORi,j and γ for each criteria air pollutant is given in the Supplemental Section S1.
3. Results & Discussion
3.1. Evaluation of Remotely Sensed Criteria Air Pollutant Exposure against In-Situ Observations
Based on our air quality analysis, the annual average CO concentration ranged from 0.031-0.033 μg/m3 with maximum estimates ranging from 240.8-272.8 μg/m3 during the 2015-2019 study period with the highest and lowest concentrations observed in 2018 and 2019 respectively. A similar peaking trend was observed for the surface concentrations of O3, PM2.5, SO2, and NO2 with the highest concentrations observed as 88.2 ppbv, 62.9 μg/m3, 20.5 μg/m3, and 11.6 ppbv respectively in the year 2018. This peaking trend in 2018 can be explained by the increase of key emissions sources in Bangladesh which mainly are brick-burning kilns, vehicle exhausts, industrial emissions, open waste burning, and large-scale construction work in that particular year. The Clean Air and Sustainable Environment project (CASE, 2020) under the Department of Environment in Bangladesh reported the number of brick kilns as around 4959 in 2013, which increased by 61.3% in 2018 up to 8000, which might have caused this increased amount of air pollutant exposure in that particular year. Furthermore, according to the CASE project, the number of total vehicles registered up to June 2018 was about 619654, indicating a 67.6% increase compared to 2013. Click or tap here to enter text.Additionally, recent construction megaprojects in Bangladesh like the Padma bridge, roads & highway projects, railway & airport expansion projects along with the alarmingly growing industrial sector also contributed to these highest concentrations of criteria air pollutants in 2018. Based on trend analysis of the surface concentration of each criteria air pollutant, CO, SO2, and PM2.5 exposure are observed to decrease by 9.4%, 10.1%, and 0.5% respectively in 2019, whereas the concentration of O3, and NO2 increased by 1.42% and 8.5% compared to 2015.
Figure 1 shows the spatial distribution of five year-average surface concentrations of CO, O3, PM2.5, SO2, and NO2. The figure demonstrates that CO, O3 and PM2.5 had more severe exposure in Bangladesh during the study period compared to exposure to SO2, and NO2. The massive air pollutant exposure in India also has a substantial effect on the exposure in those adjacent areas of Bangladesh, for which PM2.5 exposure is observed to be higher in the northwestern and southwestern regions near the border and O3 in the northern portion of Bangladesh. However, CO and SO2 exposure was observed to be the highest in southwestern districts of Bangladesh such as Chuadanga, Satkhira, and Jashore, Khulna whereas a dispersed NO2 exposure of moderate concentration has been observed all over the country. Specifically for Bangladesh, the major sources of PM2.5 are dust emissions from brick kilns and construction sites (The Third Pole, 2018). According to a recent study in Bangladesh, motor vehicles, power plants, and other combustions sources are the primary contributors to CO, and NO2 emissions (Haque et al., 2017), whereas combustions of sulfur containing fuels such as coal, and diesel in industrial and energy sectors are the key sources of SO2 emissions. O3 is basically formed in the atmosphere through a reaction of volatile organic compounds (VOCs) emitted from vehicle tailpipes, paints, and solvents with nitrogen oxides (NOx) from various sources, facilitated by sunlight. It is to be noted that the major industrial zones are Dhaka, Narayanganj, Gazipur, Khulna, Chittagong, and Rajshahi regions (Sabur et al., 2012), therefore the exposure of criteria air pollutants are observed to be more severe in these regions.
Figure 2 shows the validation of the remotely sensed data of surface concentrations of CO, O3, PM2.5, SO2, and NO2 used in this study against in situ observations in terms of Bland-Altman plots along with the 95% confidence interval (CI) and () 1.96 standard deviation (SD). The mean bias of the remotely sensed surface concentration of CO, O3, PM2.5, SO2 and NO2 during 2015-2019 is observed as 932.9 μg/m3, -72.6 ppbv, 10.9 μg/m3, 1.8 μg/m3 and 12.6 ppbv with a SD of 798.2 μg/m3, 4.2 ppbv, 23.9 μg/m3, 8.6 μg/m3 and 16.6 ppbv respectively.
The Bland-Altman plots in Figure 2 demonstrate a good agreement with 95% confidence between most of the in-situ and remotely sensed data points for each criteria air pollutants associated with the exact locations as majority of the data points lie within their respective limits of agreement (LOA). Even though there are some outliers, they represent a very small portion of the whole sample size. Majority of the in-situ and remotely sensed data points are in a close proximity of their respective mean bias line indicating the remotely sensed data is overall observed to be in well agreement with the in-situ data for each of the criteria air pollutants.
Despite this good agreement, in-situ O3 concentrations from DoE, Bangladesh require additional curation as they were observed to be only up to 12.3 ppb, whereas the actual and remotely sensed O3 concentrations are much higher in this region, resulting in an overestimation of the actual O3 concentrations by our remotely sensed data. This overestimation is due to the underestimation of actual O3 concentrations by the in-situ monitoring devices. A recent report published by the Department of Environment (DoE) of Bangladesh under the CASE Project (DoE, 2018) indicated that the O3 concentrations in Bangladesh were at-least above 20 ppb during the study period, indicating that the in situ O3 observation data reported in the monthly DoE reports may either be entered incorrectly or the averaging method of daily O3 concentration may be different than the remotely-sensed data averaging method. A wide variation was also observed in stationary O3 observations within each day including numerous zero values. Additionally, observation data were missing for a large number of days which resulted in a reduced estimation of in situ O3 concentration. For all these reasons, in situ O3 concentrations are observed to be lower compared to our continuous monthly-averaged remotely sensed data. We further observed estimates of O3 concentrations similar to our remotely sensed data in other studies for Bangladesh during this period and found that the 17-year (2003–2019) average O3 concentration was observed as 51.42 ± 1.82 ppbv (Pavel et al., 2021). Despite this limitation of in-situ O3 data from DoE, Bangladesh, we incorporated it to point out the reporting error in the dataset and to be consistent in terms of in-situ data source while validating the remotely sensed data. It should be noted that remotely sensed data for each air pollutant was considered for 2015, 2016, and 2017 only for which the continuous in-situ data were available.
3.2. Preterm Births in Bangladesh Associated with Criteria Pollutant Exposure
Figure 3 shows the spatial distribution of 5-year average annual total PTB attributable to long-term CO, O3, PM2.5, SO2, and NO2 exposure in Bangladesh during 2015-2019 period. The spatial distributional plots reveal that PM2.5, CO, and O3 exposure possess a serious potential of causing substantial PTBs at locations spread all over the country, especially within the central region of Dhaka, whereas the effect of SO2 and NO2 exposure are comparably low. Despite the higher impacts of CO, O3, and PM2.5 exposure on PTBs all over the country, lower impacts are still observed in Figure 3(a)-3(c) in the southern regions including the coastal and hilly districts of Bangladesh like Bagerhat, Patuakhali, Khagrachari, Rangamati, Bandarban etc. mostly due to the less numbers of emission sources like manufacturing industries and low population density in this region (Khatun et al., 2021). However, PTBs attributable to SO2 exposure are observed higher in the western districts of Bangladesh e.g., Rajshahi, Kushtia, Jhenaidah, Jessore, Satkhira along with the common hotspot, Dhaka, when compared to the rest of the districts with low to no PTBs observed in the hilly districts of Bangladesh. The western districts of Bangladesh possess moderate number of industries, moderate to higher density of population along with higher-than-average SO2 exposure which explains the elevated impacts of SO2 exposure on PTBs in this region. Impacts of NO2 exposure on PTBs in Bangladesh are observed to be more sporadic than spatial similar to its surface concentration distribution shown in Figure 1(e) that contributes to a much lesser estimate of PTBs compared to other criteria air pollutants. The site-specific PTB estimates are shown in Figure 4 for locations spread all over the country that experience higher than average air pollution and are continuously monitored by DoE, Bangladesh for major criteria air pollutant exposure throughout the year (detailed estimates shown in supplemental Table S2). Highest PTBs associated with synergistic exposure of CO, O3, PM2.5, SO2, and NO2 are observed in overly dense locations like Farmgate, Dhaka; Agrabad, Chattogram; Narayangonj; Khulshi, Chattogram ranging as 1133-1253; 984-1081; 666-732 and 411-452 respectively during the study period. Individual exposure impact analysis at these locations shows that PM2.5 exposure had the highest contribution in causing PTBs followed by O3, CO, and SO2 exposure where NO2 exposure had no impact most likely due to different locations other than the abovementioned locations being hotspots for NO2 exposure.
Figure 5 demonstrates the 5-year trend of the total annual PTBs imputable to CO, O3, PM2.5, SO2, and NO2 exposure along with 95% confidence interval error bars. The histogram indicates that PM2.5 exposure caused the highest amount of PTBs observed as 0.092 millions (95% CI: 0.028-0.134 millions) in 2018, followed by O3, CO, SO2, and NO2 exposure up to 0.056 millions (95% CI: 0.030-0.084 millions), 0.041 millions (95% CI: 0.016-0.065 millions), 0.007 millions (95% CI : 0.001-0.024 millions) and 0.003 millions (95% CI: 0.002-0.004 millions) respectively over the five year study period. The total number of live births in Bangladesh from CIESIN, 2021 data ranged from 4.29 – 4.30 M which is within the 2-factor range of live births reported as 3.13 M by UNICEF for Bangladesh (UNICEF, 2024).
Based on the 5-year trend analysis, PTBs attributable to CO, O3, PM2.5, and SO2 declined in 2019 by 7.9%, 5.9%, 7.4%, and 26.9% respectively compared to 2015, whereas NO2-induced PTB increased by 17.4%. Similar patterns of percentage changes were observed in the trends of each air pollutant exposure (shown in supplemental Table S1) over the five years, where annual average CO, O3, PM2.5, and SO2 exposure decreased by 2.4%, 0.34%, 2.7%, 15.2% but NO2 exposure increased by 0.81% in 2019 compared to 2015. Majority of the air pollution exposure and associated PTBs decreased in 2019 due to the reduction in vehicle emissions and the implementation of several air pollution control policies in Bangladesh. According to Climate and Clean Air Coalition (CCAC), Bangladesh has been reducing vehicle emissions since 2015 by importing diesel fuels with a lower sulfur content, imposing restrictions on the importation of used cars that are over four years old, and enforcing emission standards for petrol and diesel usage according to the Euro 1 and Euro 2 standardization protocol (Climate & Clean Air Coalition, Bangladesh).Additionally, the reduced estimates of PTBs in 2019 is attributable to the numerous effective air pollution controlling measures those have been adopted under the CASE project. Furthermore, the enactment of the ‘Brick Manufactures and Kiln Establishment Control Act 2013’ from July 1, 2014, aimed at controlling emissions from brick kilns, has further aided in the reduction of air pollution that ultimately contributed to the reduced impacts on PTBs.
Additionally, the total number of live births and preterm birth rate from all causes in each year over the study period was almost constant, indicating that the decrease in PTBs in 2019 is due to the reduction of air pollutant exposure. The similar patterns of reduction in both air pollutant exposure and the number of PTBs also indicate a strong association of the elevated risks of PTBs with air pollutant exposure where other variables (such as live births and preterm birth rate) were constant.
With the highest number of PTBs observed in 2018, the annual total PTBs due to the synergistic exposure of CO, O3, PM2.5, SO2, and NO2 ranged from 0.18 million (95% CI: 0.08-0.29 million) up to 0.20 million (95% CI: 0.08-0.32 million) (details in supplemental Table S3), which indicates that around 4.14-4.55% of the total live births were preterm due to synergistic exposure of CO, O3, PM2.5, SO2, and NO2 in Bangladesh during the study period. On top of that, criteria air pollutant exposure combinedly caused around 21.81-23.96% of the total PTBs from all causes in Bangladesh which indicates air pollution exposure is one of the major causes of PTBs in Bangladesh. Due to the unavailability of recent nationwide cohort studies investigating the PTBs associated with major criteria air pollutant exposure, we evaluate our findings by comparing to a recent study by Partha et al., 2022 which found similar estimates of PTBs as 0.073 M (95% CI: 0.042–0.097 M) with 5.6% live births being PTBs in Bangladesh associated to another set of air pollutant exposure i.e., benzene, toluene, ethylbenzene and xylene (BTEX) in 2015.
3.3. Significance, Uncertainties, and Limitations
Our study is the first approach in Bangladesh to quantify the number of total PTBs attributable to major criteria air pollutant exposure at the country level in recent years. Our study presents the scientific evidence of how CO, O3, PM2.5, SO2, and NO2 exposures negatively cause adverse birth outcomes in terms of quantitative estimation of the total PTBs attributable to each of these air pollutants both individually and synergistically. The study emphasizes on the harmful impacts of criteria air pollution exposure on adverse birth outcomes in a least-developed and overpopulated country like Bangladesh, and specifies which criteria air pollutant exposure is more likely to cause PTBs along with spatially analyzing the possible hotspots for major air pollutant exposure and the associated PTBs. By circulating such key information, this study will facilitate a robust foundation for policymakers and governments to identify and control the specific criteria air pollutants with elevated risks of PTBs as well as to develop tailored pollution prevention policies for pregnant women at the identified hotspot locations to reduce the maternal exposure as well as the preterm birth occurrence. However, one of the main gaps in our study is the uncertainty of the odds ratios for each of the criteria air pollutant exposure incorporated from different cohort studies since there have been a very limited amount of cohort studies investigating the odds ratio associating air pollutant exposure and preterm birth, particularly for Bangladesh. To overcome this limitation, our study has considered cohort studies within close geographical proximity mostly done in Asian countries to match the socioeconomical, behavioral, and lifestyle statuses along with pollution-control policies and accessibility to information and health services. Additionally, no other factors other than air pollutant exposure were considered while calculating PTBs in our study although we acknowledge that other important factors such as maternal age, number of previous births, mental and physical health status, behavioral traits, parity, marital status, employment status, education level, etc. play a very critical role in the occurrence of PTBs. Furthermore, additional uncertainties may remain as our study does not take the date of conception into consideration and does not analyze the trimester-specific pollution exposure and its impacts on the odds of PTBs which is more of an epidemiological research concern. The principal purpose of this study is to investigate the quantitative occurrence PTBs in Bangladesh considering the five criteria air pollutant exposure, live births, PTB rate and prevalence of PTBs during 2015-2019.
4. Conclusions
In this study, we have employed five major criteria air pollutant exposure data from the MERRA-2 model and satellite-sensed data regionally scaled for Bangladesh from NASA Giovanni (version 4.38) coupled with exposure-response modeling to quantify the total number of PTBs associated with the stand-alone as well as synergistic exposure of CO, O3, PM2.5, SO2, and NO2 in Bangladesh during the 2015-2019 period. During this study period, the highest exposure of CO, O3, PM2.5, SO2, and NO2 were observed in 2018 up to 272.8 /m3 , 88.2 ppbv, 62.9 /m3, 20.5 /m3, and 11.6 respectively. These elevated pollutant exposures combinedly caused from 0.18 million (95% CI: 0.08-0.29 million) PTBs up to 0.20 million (95% CI: 0.08-0.32 million) PTBs over 5 years of the study period which attributes to 4.14% to 4.55% of total live births, and 21.81% to 23.96% of total preterm birth in Bangladesh from all causes. Despite this alarming statistics, the number of PTBs attributable to majority of the criteria air pollutant exposure, specifically CO, O3, PM2.5, and SO2, decreased by 7.9%, 5.9%, 7.4%, and 26.9% where the number of PTBs attributable to NO2 exposure increased 17.4% in 2019 compared to the year 2015 which is supported by the declining trend of annual average CO, O3, PM2.5, and SO2 exposure by 2.4%, 0.34%, 2.7%, 15.2% and inclining trend of annual average NO2 exposure by 0.81% in 2019. These declining trends of PTBs associated with reductions in criteria air pollutants exposure suggest solid association between criteria air pollutant exposure and the associated preterm births. Our study also reveals the hotspots of PTBs attributable to criteria air pollutant exposure through spatial mapping & analysis and concluded that the most densely populated city, Dhaka, experienced the highest number of PTBs along with other major hotspots like Rajshahi, Rangpur, Khulna, Jessore, Chittagong, and Comilla. Our study also indicated that hilly and coastal districts of Bangladesh e.g., Khagrachari, Bandarban, Rangamati, Patuakhali, Bagerhat experienced lesser impacts of criteria air pollutant exposure on the occurrence of PTBs.
The implications of the findings of this study emphasize the urgent need for the implementation of effective air pollution prevention policies to reduce the risks and occurrence of PTBs all over the country and to promote better neonatal health. Although the primary focus of this study is to quantify preterm birth associated with criteria air pollutant exposure only, we acknowledge that other important factors, such as maternal age, marital status, health status, number of previous babies, behavioral aspects, employment status, parity, education level, etc. contributes significantly to the elevated risk of PTBs. Therefore, further analysis and comprehensive studies can be carried out in establishing a quintessential model to best predict the association between criteria air pollutants exposure including all the above-mentioned factors and their corresponding PTBs in Bangladesh. This study also necessitates the urgent need for a complete and thorough epidemiological study analyzing the odds of PTBs associated with five major criteria air pollutant (i.e., CO, O3, PM2.5, SO2, and NO2) exposure expanded all over the country of Bangladesh.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org., Figure S1.
Acknowledgments
We would like to thank the Grid supercomputer at Wayne State University for providing necessary computational resources for the data analysis.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Anenberg, S. C., Mohegh, A., Goldberg, D. L., Kerr, G. H., Brauer, M., Burkart, K., Hystad, P., Larkin, A., Wozniak, S., & Lamsal, L. (2022). Long-term trends in urban NO2 concentrations and associated paediatric asthma incidence: estimates from global datasets. The Lancet Planetary Health, 6(1), e49–e58. [CrossRef]
- Ashraful Haque, H., Huda, N., Zaman Tanu, F., Sultana, N., Shahid Hossain, M. A., & Hasinur Rahman, M. (2017). AMBIENT AIR QUALITY SCENARIO IN AND AROUND DHAKA CITY OF BANGLADESH. Barisal University Journal Part (Vol. 1).
- Bangladesh | Climate & Clean Air Coalition. (n.d.). Available online: https://www.ccacoalition.org/en/partners/bangladesh (accessed on 2 July 2023).
- Baqui, A. H., Rosen, H. E., Lee, A. C. C., Applegate, J. A., El Arifeen, S., Rahman, S. M., Begum, N., Shah, R., Darmstadt, G. L., & Black, R. E. (2013). Preterm birth and neonatal mortality in a rural Bangladeshi cohort: implications for health programs. Journal of Perinatology, 33(12), 977–981. [CrossRef]
- Barros, F. C., Bhutta, Z. A., Batra, M., Hansen, T. N., Victora, C. G., & Rubens, C. E. (2010). Global report on preterm birth and stillbirth (3 of 7): evidence for effectiveness of interventions. BMC Pregnancy and Childbirth, 10(S1), S3. [CrossRef]
- Beck, S., Wojdyla, D., Say, L., Pilar Bertran, A., Meraldi, M., Harris Requejo, J., Rubens, C., Menon, R., & Van Look, P. (2010). The worldwide incidence of preterm birth: a systematic review of maternal mortality and morbidity. Bulletin of the World Health Organization, 88(1), 31–38. [CrossRef]
- Blencowe, H., Cousens, S., Chou, D., Oestergaard, M., Say, L., Moller, A.-B., Kinney, M., & Lawn, J. (2013). Born Too Soon: The global epidemiology of 15 million preterm births. Reproductive Health, 10(S1), S2. [CrossRef]
- Blencowe, H., Cousens, S., Oestergaard, M. Z., Chou, D., Moller, A.-B., Narwal, R., Adler, A., Vera Garcia, C., Rohde, S., Say, L., & Lawn, J. E. (2012). National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. The Lancet, 379(9832), 2162–2172. [CrossRef]
- Buchard, V., da Silva, A. M., Colarco, P. R., Darmenov, A., Randles, C. A., Govindaraju, R., Torres, O., Campbell, J., & Spurr, R. (2015). Using the OMI aerosol index and absorption aerosol optical depth to evaluate the NASA MERRA Aerosol Reanalysis. Atmospheric Chemistry and Physics, 15(10), 5743–5760. [CrossRef]
- Cai, J., Zhao, Y., Kan, J., Chen, R., Martin, R., van Donkelaar, A., Ao, J., Zhang, J., Kan, H., & Hua, J. (2020). Prenatal Exposure to Specific PM 2.5 Chemical Constituents and Preterm Birth in China: A Nationwide Cohort Study. Environmental Science & Technology, 54(22), 14494–14501. [CrossRef]
- CASE Project: Clean Air and Sustainable Environemnt. (2020). Available online: http://case.doe.gov.bd/ (accessed on 2 July 2023).
- Chawanpaiboon, S., Vogel, J. P., Moller, A.-B., Lumbiganon, P., Petzold, M., Hogan, D., Landoulsi, S., Jampathong, N., Kongwattanakul, K., Laopaiboon, M., Lewis, C., Rattanakanokchai, S., Teng, D. N., Thinkhamrop, J., Watananirun, K., Zhang, J., Zhou, W., & Gülmezoglu, A. M. (2019). Global, regional, and national estimates of levels of preterm birth in 2014: a systematic review and modelling analysis. The Lancet Global Health, 7(1), e37–e46. [CrossRef]
- Chen, Q., Ren, Z., Liu, Y., Qiu, Y., Yang, H., Zhou, Y., Wang, X., Jiao, K., Liao, J., & Ma, L. (2021). The Association between Preterm Birth and Ambient Air Pollution Exposure in Shiyan, China, 2015–2017. International Journal of Environmental Research and Public Health, 18(8), 4326. [CrossRef]
- CIESIN. (2021). Center for International Earth Science Information Network - CIESIN - Columbia University. 2021. Global Subnational Infant Mortality Rates, Version 2.01. Palisades, New York: NASA Socioeconomic Data and Applications Center (SEDAC).
- Clean Air And Sustainable Environment Project (Case), Department of Environment Ministry of Environment, Forest and Climate Change Government of the People’s Republic of Bangladesh, AMBIENT AIR QUALITY IN BANGLADESH AMBIENT AIR QUALITY IN BANGLADESH. (2020).
- Clean Air And Sustainable Environment Project (Case), Department of Environment Ministry of Environment, Forest and Climate Change Government of the People’s Republic of Bangladesh, SOURCES OF AIR POLLUTION IN BANGLADESH (BRICK KILN & VEHICLE EMISSION SCENARIO. (2020).
- Dadvand, P., Parker, J., Bell, M. L., Bonzini, M., Brauer, M., Darrow, L. A., Gehring, U., Glinianaia, S. V., Gouveia, N., Ha, E., Leem, J. H., van den Hooven, E. H., Jalaludin, B., Jesdale, B. M., Lepeule, J., Morello-Frosch, R., Morgan, G. G., Pesatori, A. C., Pierik, F. H., … Woodruff, T. J. (2013). Maternal Exposure to Particulate Air Pollution and Term Birth Weight: A Multi-Country Evaluation of Effect and Heterogeneity. Environmental Health Perspectives, 121(3), 267–373. [CrossRef]
- Dhaka chokes on air pollution. (n.d.). Available online: https://www.ecohubmap.com/hot-spot/dhaka-chokes-on-air-pollution/ead5j3ml975szfa (accessed on 2 July 2023).
- GMAO. (2015). Modern-Era Retrospective analysis for Research and Applications, Version 2.
- GMAO-M2TMNXAER. (2015). MERRA-2 monthly mean PM2.5 & SO2 collections. [CrossRef]
- GMAO. (2015). Modern-Era Retrospective analysis for Research and Applications, Version 2.
- GMAO-M2TMNXCHM. (2015). MERRA-2 monthly mean CO collections. [CrossRef]
- GBD 2019 Risk Factors Collaborators, 2020; hereafter referred to GBD2019. (2020). Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet, 396(10258), 1223–1249. [CrossRef]
- Gehring, U., Wijga, A. H., Fischer, P., de Jongste, J. C., Kerkhof, M., Koppelman, G. H., Smit, H. A., & Brunekreef, B. (2011). Traffic-related air pollution, preterm birth and term birth weight in the PIAMA birth cohort study. Environmental Research, 111(1), 125–135. [CrossRef]
- Gelaro, R., McCarty, W., Suárez, M. J., Todling, R., Molod, A., Takacs, L., Randles, C. A., Darmenov, A., Bosilovich, M. G., Reichle, R., Wargan, K., Coy, L., Cullather, R., Draper, C., Akella, S., Buchard, V., Conaty, A., da Silva, A. M., Gu, W., … Zhao, B. (2017). The Modern-Era Retrospective Analysis for Research and Applications, Version 2 (MERRA-2). Journal of Climate, 30(14), 5419–5454. [CrossRef]
- GES DISC. (2019). AIRS project, Aqua/AIRS L3 Monthly Standard Physical Retrieval (AIRS-only) 1 degree x 1 degree V7.0, Greenbelt, MD, USA, Goddard Earth Sciences Data and Information Services Center (GES DISC). [CrossRef]
- Giorgis-Allemand, L., Pedersen, M., Bernard, C., Aguilera, I., Beelen, R. M. J., Chatzi, L., Cirach, M., Danileviciute, A., Dedele, A., van Eijsden, M., Estarlich, M., Fernández-Somoano, A., Fernández, M. F., Forastiere, F., Gehring, U., Grazuleviciene, R., Gruzieva, O., Heude, B., Hoek, G., … Slama, R. (2017). The Influence of Meteorological Factors and Atmospheric Pollutants on the Risk of Preterm Birth. American Journal of Epidemiology. [CrossRef]
- Guo, T., Wang, Y., Zhang, H., Zhang, Y., Zhao, J., Wang, Q., Shen, H., Wang, Y., Xie, X., Wang, L., Xu, Z., Zhang, Y., Yan, D., He, Y., Yang, Y., Xu, J., Peng, Z., & Ma, X. (2018). The association between ambient PM2.5 exposure and the risk of preterm birth in China: A retrospective cohort study. Science of The Total Environment, 633, 1453–1459. [CrossRef]
- Han, Y., Jiang, P., Dong, T., Ding, X., Chen, T., Villanger, G. D., Aase, H., Huang, L., & Xia, Y. (2018). Maternal air pollution exposure and preterm birth in Wuxi, China: Effect modification by maternal age. Ecotoxicology and Environmental Safety, 157, 457–462. [CrossRef]
- Hossain, M. A., Al Mamun, A. S. M., Aik, S., Karim, M. R., Zeshan, M. H. L., Sabiruzzaman, M., Islam, M. S., Ahmed, S., & Hossain, M. G. (2022). Preterm delivery and its associated factors among mothers in Bangladesh: survey in Rajshahi district. BMJ Open, 12(10), e061920. [CrossRef]
- Huang, Y., Partha, D. B., Harper, K., & Heyes, C. (2021). Impacts of global solid biofuel stove emissions on ambient air quality and human health. GeoHealth, 5, e2020GH000362. [CrossRef]
- IQAir. (2022). Interactive global map of 2022 PM2.5 concentrations by city. Available online: https://www.iqair.com/us/world-air-quality-report.
- Jenwitheesuk, K., Peansukwech, U., & Jenwitheesuk, K. (2022). Predictive MERRA-2 aerosol diagnostic model for oral, oropharyngeal and laryngeal cancer caused by air pollution in Thai population. Toxicology Reports, 9, 970–976. [CrossRef]
- Khatun, H., Sumiya, N. N., & Ali, A. A. Bin. (2021). Achieving Sustainable Development Goals in Bangladesh: Does Population Density Matter? The Dhaka University Journal of Earth and Environmental Sciences, 8(2), 1–15. [CrossRef]
- Kristen M. Rappazzo *, Jennifer L. Nichols, R. Byron Rice, Thomas J. Luben, Ozone exposure during early pregnancy and preterm birth: A systematic review and meta-analysis,. [CrossRef]
- Larkin, A., Geddes, J. A., Martin, R. V., Xiao, Q., Liu, Y., Marshall, J. D., Brauer, M., & Hystad, P. (2017). Global Land Use Regression Model for Nitrogen Dioxide Air Pollution. Environmental Science & Technology, 51(12), 6957–6964. [CrossRef]
- Li, S., Guo, Y., & Williams, G. (2016). Acute impact of hourly ambient air pollution on preterm birth. Environmental Health Perspectives, 124(10), 1623–1629. [CrossRef]
- Liu, Y., Xu, J., Chen, D., Sun, P., & Ma, X. (2019). The association between air pollution and preterm birth and low birth weight in Guangdong, China. BMC Public Health, 19(1). [CrossRef]
- Llop, S., Ballester, F., Estarlich, M., Esplugues, A., Rebagliato, M., & Iñiguez, C. (2010). Preterm birth and exposure to air pollutants during pregnancy. Environmental Research, 110(8), 778–785. [CrossRef]
- McClure, E. M., Saleem, S., Goudar, S. S., Dhaded, S., Guruprasad, G., Kumar, Y., Tikmani, S. S., Kadir, M., Raza, J., Yasmin, H., Moore, J. L., Kim, J., Bann, C., Parlberg, L., Aceituno, A., Carlo, W. A., Silver, R. M., Lamberti, L., Patterson, J., & Goldenberg, R. L. (2018). The project to understand and research preterm pregnancy outcomes and stillbirths in South Asia (PURPOSe): a protocol of a prospective, cohort study of causes of mortality among preterm births and stillbirths. Reproductive Health, 15(S1), 89. [CrossRef]
- Mendola, P., Wallace, M., Hwang, B. S., Liu, D., Robledo, C., Männistö, T., Sundaram, R., Sherman, S., Ying, Q., & Grantz, K. L. (2016). Preterm birth and air pollution: Critical windows of exposure for women with asthma. Journal of Allergy and Clinical Immunology, 138(2), 432-440.e5. [CrossRef]
- Nahian, M. Al, Ahmad, T., Jahan, I., Chakraborty, N., Nahar, Q., & Streatfield, P. K. (2023). Air pollution and pregnancy outcomes in Dhaka, Bangladesh. The Journal of Climate Change and Health, 9, 100187. [CrossRef]
- Ohuma, E. O., Moller, A.-B., Bradley, E., Chakwera, S., Hussain-Alkhateeb, L., Lewin, A., et al. (2023). National, regional, and global estimates of preterm birth in 2020, with trends from 2010: a systematic analysis. [CrossRef]
- Partha, D. B., Cassidy-Bushrow, A. E., & Huang, Y. (2022). Global preterm births attributable to BTEX (benzene, toluene, ethylbenzene, and xylene) exposure. Science of the Total Environment, 838. [CrossRef]
- Pavel, M. R. S., Zaman, S. U., Jeba, F., Islam, M. S., & Salam, A. (2021). Long-Term (2003–2019) Air Quality, Climate Variables, and Human Health Consequences in Dhaka, Bangladesh. Frontiers in Sustainable Cities, 3, 681759. [CrossRef]
- Perin, J., Mulick, A., Yeung, D., Villavicencio, F., Lopez, G., Strong, K. L., Prieto-Merino, D., Cousens, S., Black, R. E., & Liu, L. (2022). Global, regional, and national causes of under-5 mortality in 2000–19: an updated systematic analysis with implications for the Sustainable Development Goals. The Lancet Child & Adolescent Health, 6(2), 106–115. [CrossRef]
- Rappazzo, K. M., Nichols, J. L., Rice, R. B., & Luben, T. J. (2021, July 1). Ozone exposure during early pregnancy and preterm birth: A systematic review and meta-analysis. Environmental Research. Academic Press Inc. [CrossRef]
- Ritz, B., Wilhelm, M., Hoggatt, K. J., & Ghosh, J. K. C. (2007). Ambient Air Pollution and Preterm Birth in the Environment and Pregnancy Outcomes Study at the University of California, Los Angeles. American Journal of Epidemiology, 166(9), 1045–1052. [CrossRef]
- Ryu, Y.-H., & Min, S.-K. (2021). Long-term evaluation of atmospheric composition reanalyses from CAMS, TCR-2, and MERRA-2 over South Korea: Insights into applications, implications, and limitations. Atmospheric Environment, 246, 118062. [CrossRef]
- Sabur, M. A., Khan, A. A., & Safiullah, S. (2012). Treatment of Textile Wastewater by Coagulation Precipitation Method. Journal of Scientific Research, 4(3), 623–633. [CrossRef]
- Saenen, N. D., Martens, D. S., Neven, K. Y., Alfano, R., Bové, H., Janssen, B. G., Roels, H. A., Plusquin, M., Vrijens, K., & Nawrot, T. S. (2019). Air pollution-induced placental alterations: an interplay of oxidative stress, epigenetics, and the aging phenotype? Clinical Epigenetics, 11(1), 124. [CrossRef]
- Salam, A., Andersson, A., Jeba, F., Haque, M. I., Hossain Khan, M. D., & Gustafsson, Ö. (2021). Wintertime Air Quality in Megacity Dhaka, Bangladesh Strongly Affected by Influx of Black Carbon Aerosols from Regional Biomass Burning. Environmental Science & Technology, 55(18), 12243–12249. [CrossRef]
- Shanshan Li, Yuming Guo, and Gail Williams, Acute Impact of Hourly Ambient Air Pollution on Preterm Birth. [CrossRef]
- Siddiqui, S. A., Jakaria, M., Amin, M. N., Al Mahmud, A., & Gozal, D. (2020). Chronic air pollution and health burden in Dhaka city. European Respiratory Journal, 56(2), 2000689. [CrossRef]
- Stieb, D. M., Chen, L., Eshoul, M., & Judek, S. (2012). Ambient air pollution, birth weight and preterm birth: A systematic review and meta-analysis. Environmental Research, 117, 100–111. [CrossRef]
- Sun, X., Luo, X., Zhao, C., Chung Ng, R. W., Lim, C. E. D., Zhang, B., & Liu, T. (2015). The association between fine particulate matter exposure during pregnancy and preterm birth: a meta-analysis. BMC Pregnancy and Childbirth, 15(1), 300. [CrossRef]
- UNICEF. (2024). Maternal and Newborn Health Disparities - Bangladesh. Available online: https://data.unicef.org/country/bgd/.
- Weber, K. A., Yang, W., Lurmann, F., Hammond, S. K., Shaw, G. M., & Padula, A. M. (2019). Air pollution, maternal hypertensive disorders, and preterm birth. Environmental Epidemiology, 3(5), e062. [CrossRef]
- WHO. (2012). The Partnership for Maternal, Newborn & Child Health. Born too soon: the global action report on preterm birth. Available online: http://whqlibdoc.who.int/publications/2012/9789241503433_eng.pdf.
- WHO. (2022). Preterm birth. Available online: https://www.who.int/news-room/fact-sheets/detail/preterm-birth.
- World Bank. (2022). The Global Health Cost of PM2. 5 Air Pollution: A Case for Action Beyond 2021. The World Bank. Available online: https://documents.worldbank.org/en/publication/documents-reports/documentdetail/455211643691938459/the-global-health-cost-of-pm-2-5-air-pollution-a-case-for-action-beyond-2021.
- Xiong, Y., Partha, D., Prime, N., Smith, S. J., Mariscal, N., Salah, H., & Huang, Y. (2022). Long-term trends of impacts of global gasoline and diesel emissions on ambient PM2.5 and O3 pollution and the related health burden for 2000-2015. Environmental Research Letters, 17(10). [CrossRef]
- Yao, W., Che, H., Gui, K., Wang, Y., & Zhang, X. (2020). Can MERRA-2 Reanalysis Data Reproduce the Three-Dimensional Evolution Characteristics of a Typical Dust Process in East Asia? A Case Study of the Dust Event in May 2017. Remote Sensing, 12(6), 902. [CrossRef]
- Ying Liu, Jihong Xu, Dian Chen, Pei Sun and Xu Ma, The association between air pollution and preterm birth and low birth weight in Guangdong, China 2019, . [CrossRef]
- Zhao, Q., Zhao, W., Bi, J., & Ma, Z. (2021). Climatology and calibration of MERRA-2 PM2.5 components over China. Atmospheric Pollution Research, 12(2), 357–366. [CrossRef]
Figure 1.
Regional spatial distribution of 5-year average surface concentrations of criteria air pollutants in Bangladesh during 2015-2019 for (a) CO, (b) O3, (c) PM2.5, (d) SO2, and (e) NO2 respectively.
Figure 1.
Regional spatial distribution of 5-year average surface concentrations of criteria air pollutants in Bangladesh during 2015-2019 for (a) CO, (b) O3, (c) PM2.5, (d) SO2, and (e) NO2 respectively.
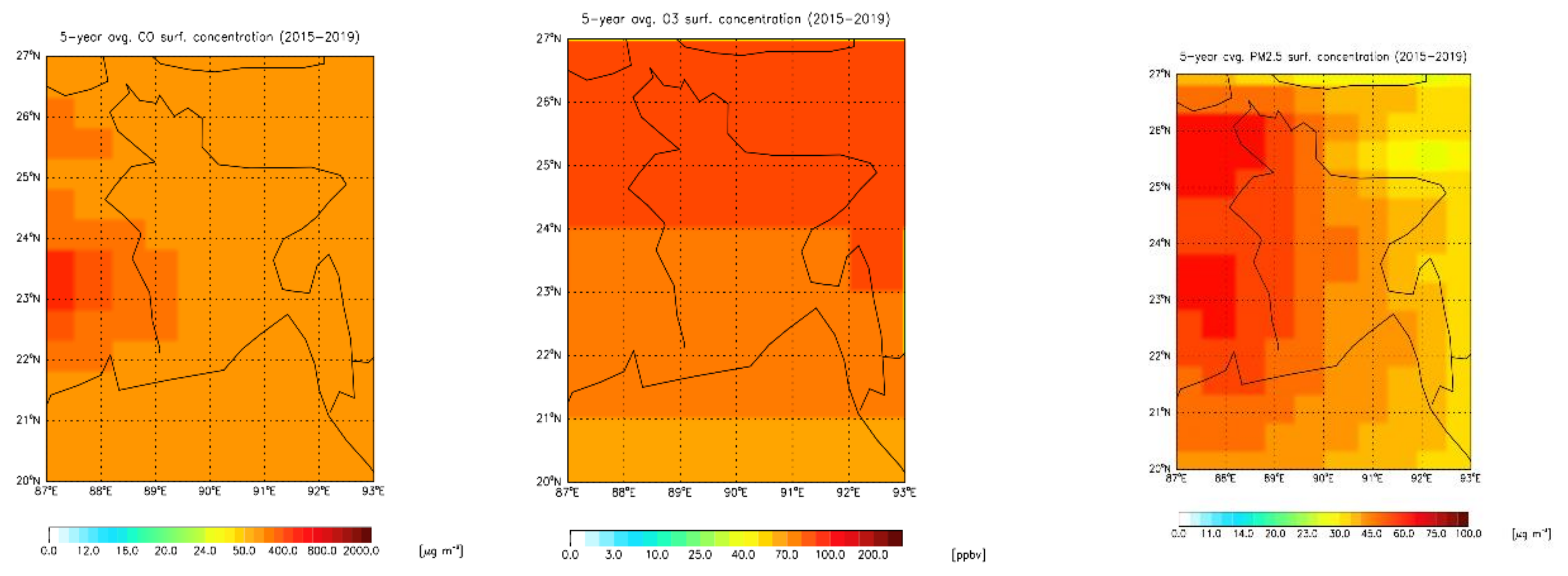
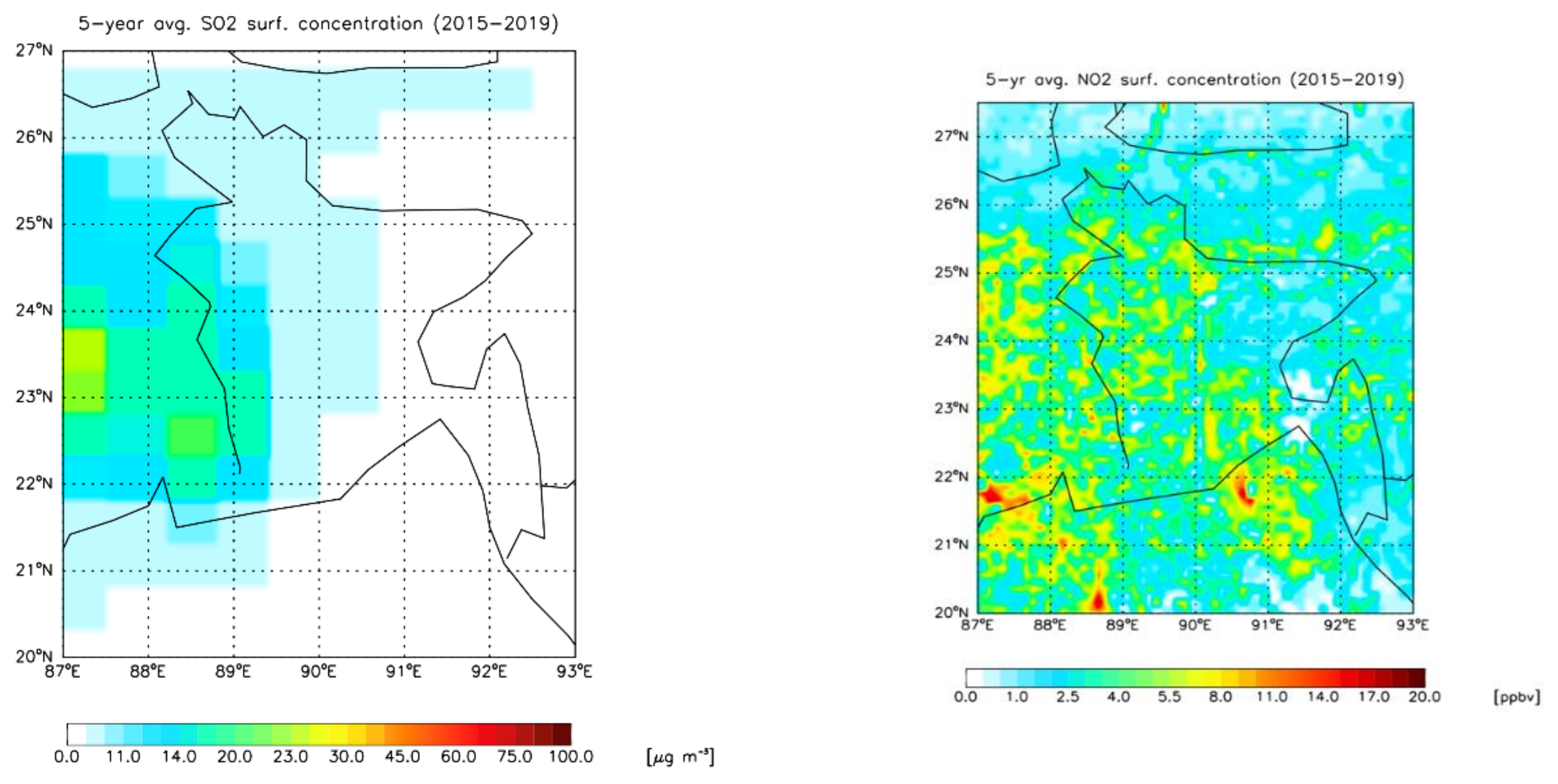
Figure 2.
Bland-Altman plots of surface concentrations of criteria air pollutants during 2015-2017 between observations and remotely sensed data (observations minus remotely sensed data) in Bangladesh for (a) CO, (b) O3, (c) PM2.5, (d) SO2, and (e) NO2 respectively.
Figure 2.
Bland-Altman plots of surface concentrations of criteria air pollutants during 2015-2017 between observations and remotely sensed data (observations minus remotely sensed data) in Bangladesh for (a) CO, (b) O3, (c) PM2.5, (d) SO2, and (e) NO2 respectively.
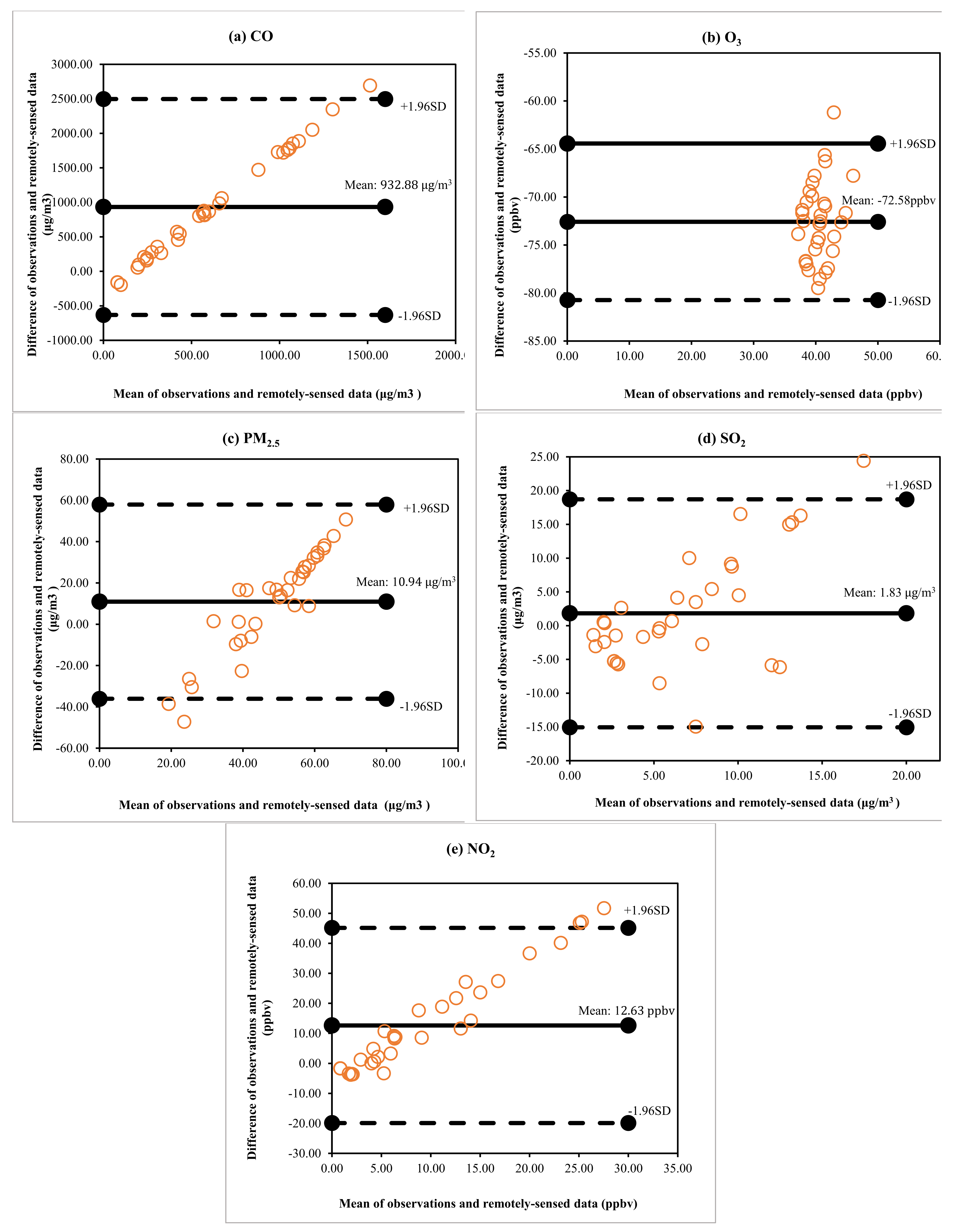
Figure 3.
Regional spatial distribution of 5-year average annual total PTB attributable to long-term (a) CO, (b) O3, (c) PM2.5, (d) SO2, and (e) NO2 exposure respectively during 2015-2019 for Bangladesh.
Figure 3.
Regional spatial distribution of 5-year average annual total PTB attributable to long-term (a) CO, (b) O3, (c) PM2.5, (d) SO2, and (e) NO2 exposure respectively during 2015-2019 for Bangladesh.
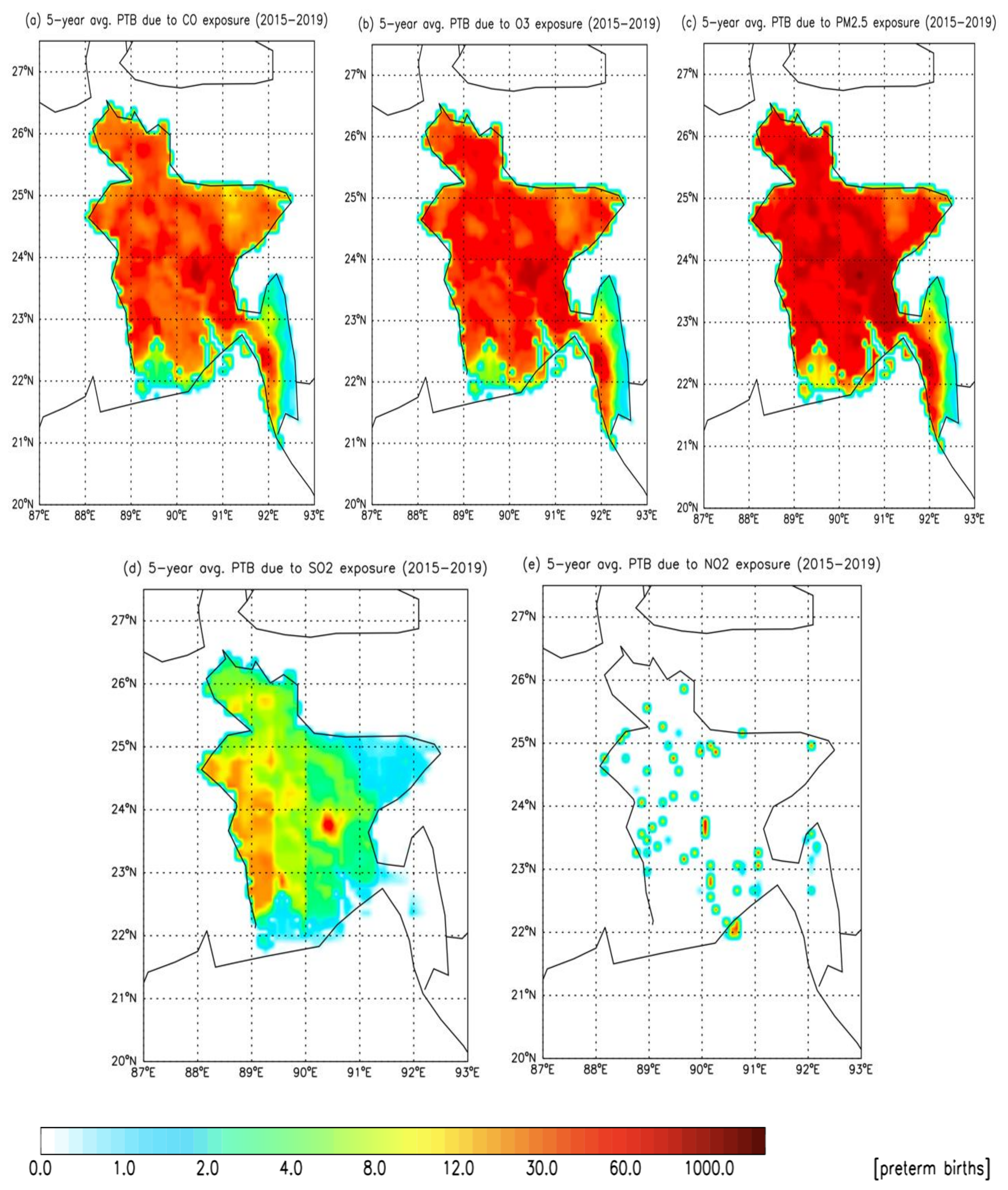
Figure 4.
Number of total PTBs at specific locations attributable to long-term CO, O3, PM2.5, SO2, and NO2 exposure during 2015-2019 for Bangladesh.
Figure 4.
Number of total PTBs at specific locations attributable to long-term CO, O3, PM2.5, SO2, and NO2 exposure during 2015-2019 for Bangladesh.
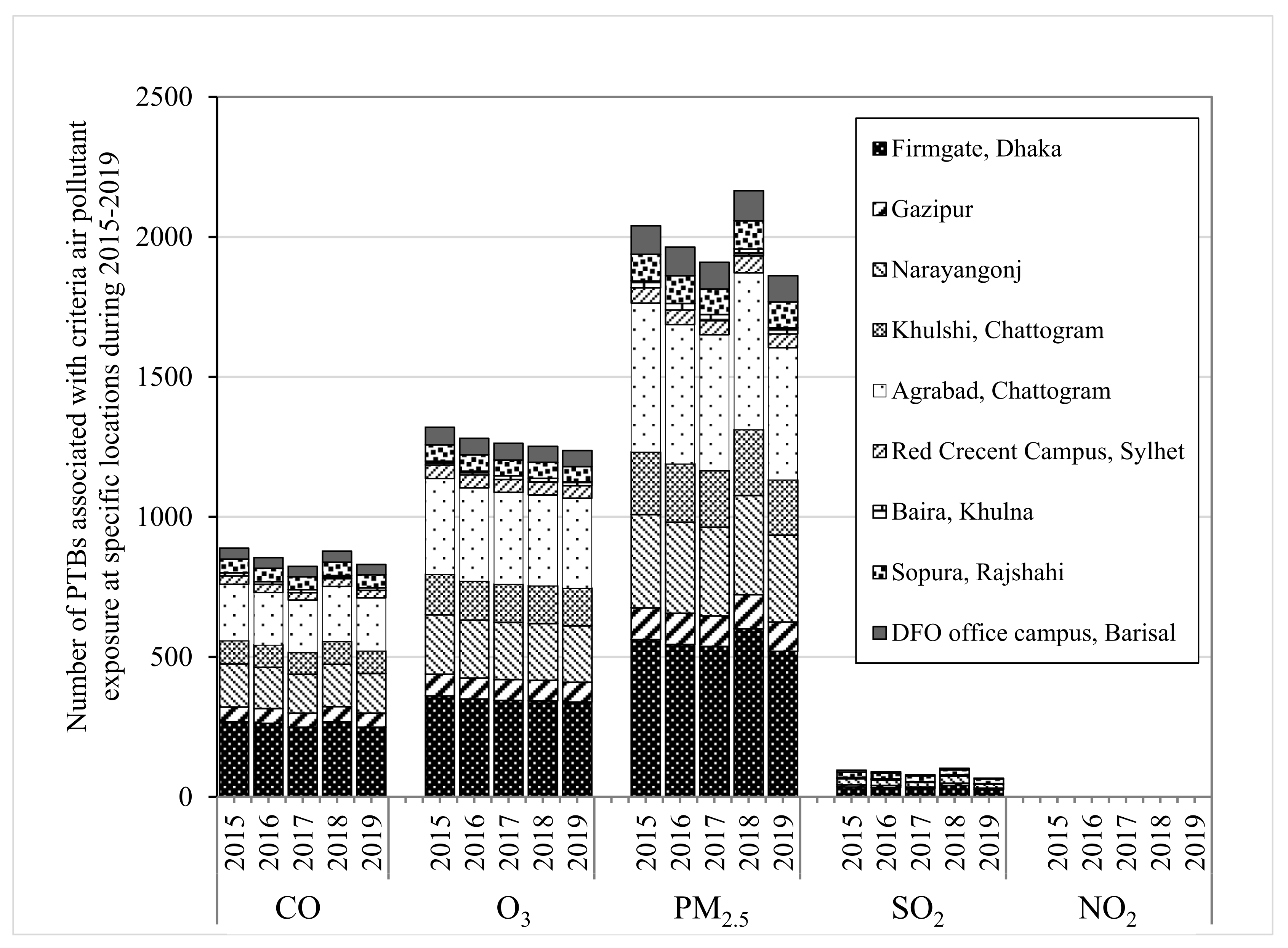
Figure 5.
Regional annual total PTB attributable to long-term CO, O3, PM2.5, SO2, and NO2 exposure respectively during 2015-2019 for Bangladesh. Error bars represent 95% confidence intervals.
Figure 5.
Regional annual total PTB attributable to long-term CO, O3, PM2.5, SO2, and NO2 exposure respectively during 2015-2019 for Bangladesh. Error bars represent 95% confidence intervals.
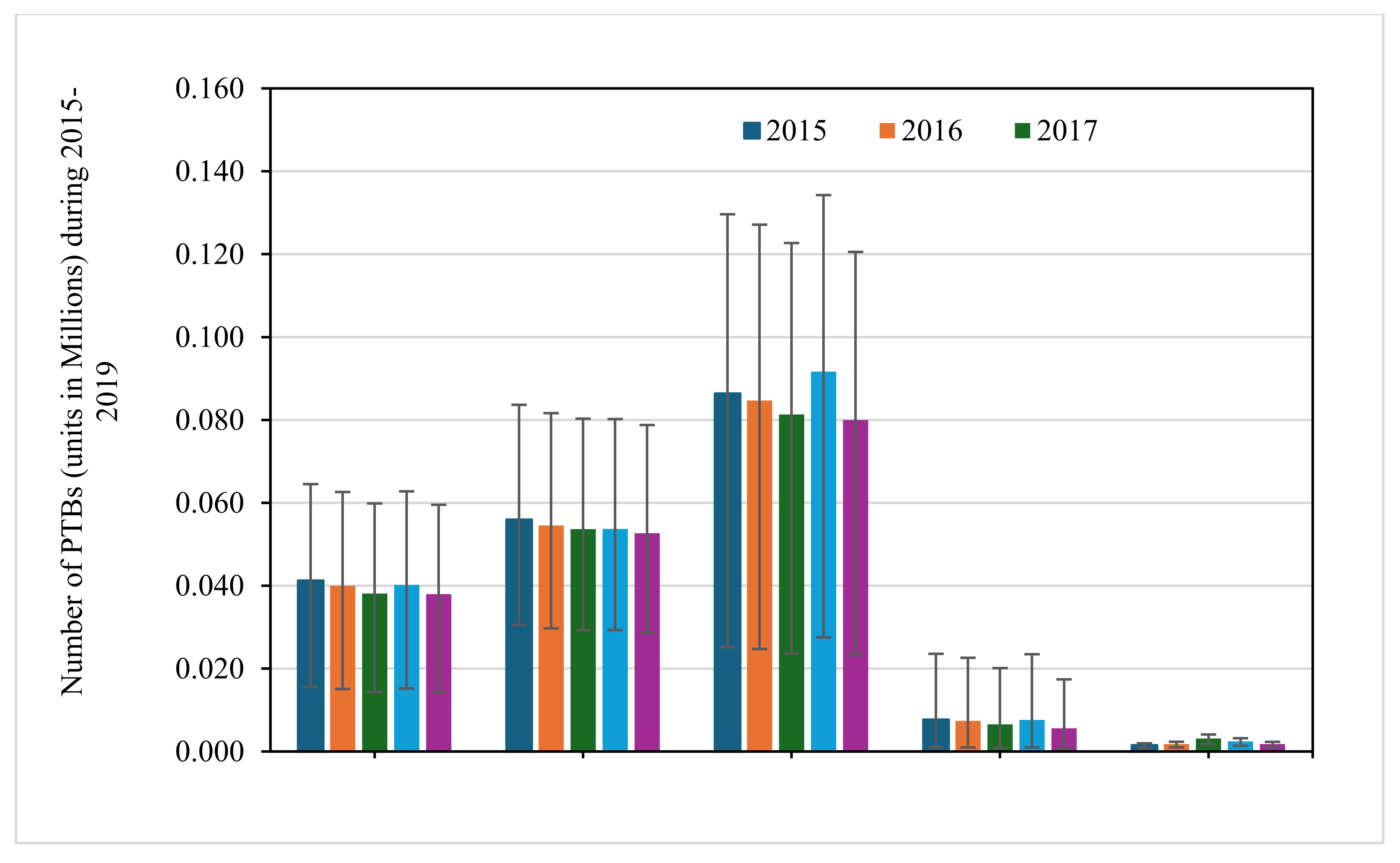

Table 1.
Sources of remotely sensed datasets of gaseous pollutants for this study.
| Criteria Pollutants | Model/Instrument/Study | Dataset/Product | Spatial Resolution (latitude longitude) |
| CO | MERRA-2 | M2TMNXCHM (v5.12.4) | 0.5° 0.625° |
| O3 | AIRS | AIRS3STM (v7.0) | 1° 1° |
| PM2.5 | MERRA-2 | M2TMNXAER (v5.12.4) | 0.5° 0.625° |
| SO2 | MERRA-2 | M2TMNXAER (v5.12.4) | 0.5° 0.625° |
| NO2 | Anenberg et al. (2022) | 0.0083° 0.0083° |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



