
Submitted:
18 June 2024
Posted:
19 June 2024
You are already at the latest version
Abstract
Acrylates and methacrylates are widely used, especially in the dental industry, but can cause adverse skin reactions. These compounds, including 2-hydroxyethyl methacrylate, triethylene glycol dimethacrylate, and bisphenol A-glycidyl methacrylate, are strong contact irritants or allergens. Found in dental prostheses, composite resins, dentin bonding materials, and glass ionomers, they pose a higher risk of exposure for dental personnel. Clinically, acrylate allergies manifest as facial rashes, eczema with cracked skin on fingers (pulpitis), nail dystrophy, and periungual dermatitis. Recently, the highest frequency of allergic reactions to acrylates has shifted from dentistry to the beauty industry due to increased use in artificial nails, eyelashes, and hair extensions. This has led to greater sensitization. Acrylates are also used in medical applications, such as bone cement for orthopedic endoprostheses, soft contact lenses, hearing aids, histological preparations, and wound dressings, which can also cause allergic reactions. Severe dermatitis from surgical glue containing acrylates has been documented, and diabetic medical devices are potential sources of allergic contact dermatitis. Given the extensive use and prolonged skin contact of products containing acrylates and methacrylates, this review aims to present current knowledge and literature on reactions to these compounds across different industries.
Keywords:
acrylates
; methacrylates
; contact reactions
; skin
; dentistry
; cosmetics
; allergy
; contact dermatitis
; nails
; sensitisation
1. Introduction
Acrylates are plastic materials obtained by polymerizing monomers derived from acrylic or methacrylic acid, where acrylate monomers contain an acrylic group obtained from acrylic and methacrylic acid [1,2,3,4,5,6,7,8]. Thus, acrylates and methacrylates (MA) are formed by the esterification of acrylic/methacrylic acid, and their reactivity varies depending on the type of acid used in the esterification process [9]. Acrylates serve as the basis for acrylic resins [10]. Due to their reactive double bonds, acrylates quickly form polymer plastic structures by polymerization at room temperature (spontaneous) or with the help of heat/ultraviolet (UV) light [11]. Acrylate monomers have many applications [11,12]. So, acrylates and MA are widespread, primarily in the dental industry. They are used in dental prostheses, composite resins, dentin bonding materials, and glass ionomers [9,10,13,14,15]. In the past, the most frequent human exposures to acrylates were related to production, especially in printing, dyeing, coating, the metallurgical industry, and dentistry [11,12]. Familiar sources of acrylates include floor waxes, floor coatings, and products for the surface treatment of leather, textile, and paper products. Today, many (meth)acrylates are mainly used in dental binders, printing inks, artificial nails, etc. Considering the impact of contact with acrylates and possible adverse reactions by profession, dental personnel are particularly exposed to the risk of developing an allergy to acrylates and MA [16]. Acrylates and MA can be irritants and allergens. Thus, acrylates and, more rarely, MA such as 2-hydroxyethyl methacrylate (2-HEMA), triethylene glycol dimethacrylate (TEGDMA), and 2,2-bis[4-(2-hydroxy-3-methacryloxypropoxy)phenyl]propane (bis-GMA) are strong contact irritants or allergens. These compounds have been found in uncured dental adhesives and cement in 50 to 90% concentrations. It is also important to mention that methyl methacrylate (MMA) can penetrate through thin, protective disposable gloves as a small molecular acrylate. While fully polymerized acrylic plastics are inert and harmless, hard-cured MA can evaporate, causing respiratory irritation, sensitization and allergic symptoms [8]. Thus, in the middle of the 20th century, many cases of allergic contact dermatitis (ACD) caused by MA were documented. In ACD, skin reactions appear 24-48 hours after repeated contact with an allergen/substance to which the skin was previously exposed and developed sensitization [17]. In addition, many papers on occupational ACD caused by (meth)acrylate monomers have also been published [11].
2. Chronological Development of the Application of Acrylates and the Appearance of Adverse Reactions
The development of methacrylate and acrylate compounds began in the 1930s, and in a short time, they found application in producing plastic glass used in aircraft, paints, coatings, and printing inks [18]. Thus, the use of acrylates in the 1930s began with the mass production of Plexiglas, a transparent and resistant replacement material for glass, obtained by the polymerization of methacrylate. Numerous other acrylates have found application in paints, adhesives, composite resins for dentistry, printing inks, artificial nails, and medical devices such as contact lenses, hearing aids, and cement for orthopaedic endoprostheses [8]. Although products containing acrylic polymers are relatively inert, sometimes active monomer particles are still released from the polymer structures and can act as haptens that stimulate allergic reactions [11,19,20]. Thus, they can cause allergic reactions, and their monomeric and dimeric forms have a high sensitization potential for developing allergies [21,22]. Since the 1950s, many cases of ACD have been documented due to MMA exposure. Numerous papers have been published on the occupational origin of ACD caused by (meth)acrylate monomers since that time [11]. Occupational allergy to (meth)acrylates is also possible, which most often occurs among dental staff. In the 1990s, dental professionals observed a significant increase in sensitization to acrylates [23]. Dental personnel are exposed to many potential contact allergens, including untreated plastic (acrylate) resins such as acrylic monomers, MA, urethane acrylates and epoxy acrylates. These have been used in dentistry in dentures, dentin bonding materials and glass ionomer materials [11,24]. Due to the frequent observation of these reactions, (meth)acrylates were designated as the "allergen of the year" in 2012 by the American Society for Contact Dermatitis [8,10]. Additionally, isobornyl acrylate (IBOA) was declared the contact allergen of the year for 2020 [11,25]. In recent decades, allergies to (meth)acrylates have been on the rise. These allergies are prevalent not only in dentistry but also in the beauty and medical device industries. For example, in cosmetics, with the popularity of permanent manicures, reactions to acrylates are observed in both manicurists and their clients. A new trend of non-occupational ACD caused by medical devices for diabetics has also been noted [11].
3. Acrylates in Cosmetics and Medicine
In recent decades, the occurrence of allergy to (meth)acrylates has shifted from dentistry to the beauty industry, where the application of acrylates has become very frequent [26]. Concerning acrylates in cosmetics, the most important sources of sensitization are artificial eyelashes, hair extensions, and artificial nails [27,28]. However, artificial nail products have long been known as a source of acrylate allergies, with the first such case reported by Canizares in 1956 [11,29]. Due to the wide availability of nail techniques based on acrylates, MA, or cyanoacrylates, the use of artificial nails has increased, leading to greater sensitization [11,16,30]. Although acrylate nails composed of powder and liquid containing acrylates (applied on the nail plate without photo-hardening) were previously the most popular, their use is now rare due to long-term performance issues [11,28]. Today, the most common trend is the so-called permanent nail polish containing photo-cured acrylates (also known as "semi-permanent," "permanent nail polish" or "gel nail polish"). This product is a mixture of acrylate monomers applied to the nail plate and polymerized using fluorescent, UV or LED lamps. It is low-cost and simple to use. All types of artificial nails contain acrylates and can cause hypersensitivity in beauticians and their clients [28,31]. Also, with the use of commercial nail kits for home use, there is an even greater risk of allergy, so ACD caused by home use of artificial nails (already described in Australia, Sweden and Spain) is possible [27,31]. Sensitization can develop even after several months or years of using artificial nails [11]. Nowadays, new sources of acrylates appear [11]. For example, a case of acrylate ACD caused by a fixed hair prosthesis (in a man with scarring alopecia) was described after 4 weeks of using a capillary prosthesis fixed with a liquid adhesive containing acrylate (Ghostbond) [32]. The patient developed pruritic eczematous lesions on the scalp, and despite switching to double-sided adhesive tape, there was no improvement [32]. A patch test confirmed an allergy to hydroxypropyl methacrylate (2-HPMA), hydroxyethyl acrylate, butyl acrylate, adhesive tape and Ghostbond glue (2+). However, IBOA, previously used mainly in coatings, inks, cosmetics, and paints, is also a potential allergen, though less frequent than other (meth)acrylates [33]. Acrylates are widely used for various medical purposes, so allergies to acrylates in bone cement for orthopaedic endoprostheses, soft contact lenses, hearing aids and histological preparations are also possible [11]. Wound dressings are also cited as sources of sensitization to acrylates [12]. Cases of severe dermatitis from surgical glue containing acrylates, which many surgeons use, are also described in the surgical papers. Prolonged exposure to skin adhesives (weeks or months after application) carries a higher risk of primary sensitization, especially on inflamed skin [11]. Multiple reports also indicate that diabetic medical devices are an important cause of ACD. For example, new technologies for rapid glucose measurement have been implicated [34]. According to the results of one multicenter study, skin reactions to the Freestyle Libre, a flash glucose monitoring (FGM) system (which involves fixing the device to the skin with adhesive for two weeks) may occur directly below the adhesive part of the sensor and most patients exhibited a proven allergy to isobornyl acrylate, a component of the device [11,33,34]. In another study following 70 diabetics (type 1) with suspected contact allergy to the glucose sensor tested by patch test (exposed for an average of 6 months before the first signs of sensor-related dermatitis), allergic reactions to IBOA were found in 81% of Freestyle Libre users [33]. Also, responses to the insulin pump are possible, so recently, IBOA has been identified as responsible for them as a sensitizer in the tubeless insulin pump (OmniPod) [11,35]. Therefore, based on current observations and recommendations, manufacturers need to eliminate this allergen from these devices due to the increased prevalence of acrylate allergies [34]. Other acrylates, such as N,N-dimethylacrylamide (DMAA) and 2-ethyl cyanoacrylate, present in the CGM Platinum G4 Dexcom sensor adhesive, are also potential sensitizers in insulin infusion and glucose monitoring devices [36]. As a preventive measure, in cases of ACD caused by acrylates, patients can use special hydrocolloid plates between the skin and the adhesive part of the sensor to prevent or limit the allergic reaction [11,37,38]. Other sources of sensitization to acrylates include electrodes for transcutaneous electrical nerve stimulation (TENS) (used in treating chronic back pain) and the adhesive layer of electrocardiogram electrodes [38,39]. There are also cases of ACD to acrylates in aesthetic medicine. For example, a case was described where a patient developed ACD to polymethyl methacrylate (PMMA) after an intradermal filler injection (to correct the tip of his nose). Subsequently, an allergy to MMA (3+) was proven (in the past he already had a suspected mucosal reaction to a dental prosthesis based on polymethyl- methacrylate resins) [40].
4. Acrylates as a Cause of Allergic Contact Dermatitis and Other Disorders
Clinically, allergy to acrylates most often appears as a rash on the face and/or eyelids, eczema with cracking of the finger skin (pulpitis), nail dystrophy and periungual dermatitis (Figure 1) [5,19].
The overall clinical picture of skin allergy can also manifest as acquired leukoderma on the fingertips or sometimes with simultaneous dermatitis of the face or neck [11,16,30,41]. Nail abnormalities similar to psoriasis (due to the presence of onycholysis and severe subungual hyperkeratosis) can occur, although nail changes can exist independently without finger dermatitis. However, not all skin lesions at contact sites can be attributed to ACD alone; other manifestations, such as irritant (non-allergic) contact dermatitis, must also be considered. In differential diagnosis of skin lesions, "acne mechanica," which manifests as inflammatory papules and pustules caused by mechanical pressure, should also be considered [42]. In addition, acrylates and MA can also cause asthma [43]. A different frequency of allergy to certain acrylate haptens has been observed among dental personnel. Furthermore, comparing the frequency of contact allergy to acrylates between dentists and medical doctors showed more frequent allergic reactions in dentists than in medical doctors [17]. The most important allergens among dentists and dental nurses are 2-HEMA and MMA, while for dental technicians, it is mainly ethylene glycol dimethacrylate (EGDMA) [44]. According to the results of a study testing allergies in dental technicians and its connection with work-related ACD (patch tests conducted from 2001 to 2015 in Germany), the most common contact allergens were MA and acrylates [24]. Therefore, eczema of the hand and pulpitis of the fingertips (especially the first three fingers) were observed as typical clinical manifestations of allergies to (meth)acrylate in these dental professions, but generalized dermatitis is also possible [44,45,46,47]. The face and eyelids can sometimes be affected due to acrylate particles in the air or the transmission of allergens via contaminated tools or hands [27]. Additionally, acrylates can cause respiratory hypersensitivity, such as difficulty breathing, asthma, or rhinoconjunctivitis. Among other unwanted changes/lesions induced by acrylates, the term allergic contact stomatitis is described in the literature. This condition has been observed in some dental patients due to inadequate polymerization and the release of residual monomers from acrylate-based prosthetic replacements [48]. Patients with this condition may experience oral symptoms like burning or pain in the mouth, loss of taste, numbness, inflammation of the mucous membrane, vesicles, erosions and lichenoid reactions limited to the area of contact with dental materials [11]. Therefore, caution is recommended when working with sensitized patients who need dental procedures, as they may experience complications during dental work [49]. However, sometimes inadequately performed dental prosthetic work (which, by its impact, disrupts the biological width of the periodontium) can cause inflammation of the underlying mucosa (with hyperemia and erythema), or patients after the creation of new prosthetic work can report clinical problems (burning mouth syndrome), so often wrongly/unfairly declare it an oral allergic reaction. Therefore, clinicians need to consider these possibilities when working with patients [50,51]. It is also important to note that inflammation of the lips and perioral skin sometimes may occur due to contact irritants or allergic reactions to metals or acrylates [52]. When cheilitis results from an allergic reaction to allergens such as acrylates in contact with the lips, the lesions are limited to the affected part of the lips. Positive results from allergy tests are helpful for further monitoring the significance of confirmed allergies. Although acrylates were once considered occupational allergens specific to dental professionals, they have recently become common occupational contact allergens for beauticians and hairdressers due to the presence of acrylates in cosmetic adhesives [53]. Looking at adverse reactions when working in cosmetics, ACD caused by different types of acrylate artificial nail techniques is often unrecognized - due to the unobserved association of manicure product use with nail abnormalities [12]. In establishing the diagnosis, the clinical picture, involvement of all nails and absence of specific signs of psoriatic nails (e.g., "salmon patches") can help (a nail biopsy is usually unnecessary) [54]. According to research, acrylate allergy occurs most often in young female beauticians who suffer from hand dermatitis and sometimes facial dermatitis [27]. According to an international retrospective study [11 European Environmental Contact Dermatitis Research Groups / EEC DRG)], most cases of ACD to acrylates were caused by nail styling materials (67%): 43% of patients were users/consumers, and 56% were contractors/workers. Furthermore, most occupational ACD cases (65%) were detected during the first year on the job. Study results highlight the high sensitizing power of acrylates [8,11,28]. A positive reaction to two or more acrylates was found in most patients, with the most frequent allergens being 2-HEMA, 2-HPMA, EGDMA and ethyl cyanoacrylate [11,28]. Looking at the negative impact of acrylates on beauticians, they also described mucosal symptoms (eye, nasal and respiratory) due to their exposure to acrylates. In beauticians, there is a possible direct connection between exposure to allergens at the workplace, including (meth)acrylates, with lung function and airway inflammation [55]. Their nasal and respiratory symptoms can be associated with the strong irritating properties of acrylates [11,55]. Induced asthma or exacerbation of existing asthma, conjunctivitis, and rhinitis are also possible [49,55]. The negative influence of acrylates when performing eyelash extensions (a modern cosmetic trend) should also be mentioned, with possible unwanted reactions during the process of glueing artificial eyelashes (eyelash by eyelash on the natural eyelashes of clients) with eyelash glue that often contains cyanoacrylates. Clinically, possible unwanted manifestations in clients include eye disorders such as blepharitis and hand eczema in stylists [56]. Sometimes, the first manifestations can be conjunctivitis and rhinitis due to the local application of acrylate glue for eyelashes (which stimulates the influx of eosinophils into the tears and then into the nasal mucosa). A case was described of a beautician who used eyelash glue with acrylate to extend artificial eyelashes for two years (containing ethyl-2-cyanoacrylate, alkoxy-2-cyanoacrylate, and PMMA), leading to eye and nasal symptoms - discontinuing the use of these adhesives led to the withdrawal of symptoms [11].
5. Diagnosis and Proof of Allergy to Acrylates
Patch testing is the gold standard for confirming the diagnosis of allergy to acrylates and metals (Figure 2 and Figure 3) [11].
Therefore, acrylic monomers are included in several commercial patch tests, including dental materials for dental patients, dental staff, artificial nails, and printing [44]. Polyvalent allergy to acrylates is also common in the test results (multiple positive reactions in the patch test), although the patients were probably not exposed to all of these substances. This may be due to cross-reactions between acrylic monomers (allergic sensitization caused by one acrylic compound extends to one or more other acrylic compounds) and accompanying allergies due to their simultaneous presence in some products [8,44]. According to the results of a study on the occurrence of cross-reactivity of acrylic compounds, most people sensitized to (meth)acrylates were allergic to more than one of the tested compounds (66.3%), which points to the need for preventive measures [10]. According to the results of a study conducted on 67 patients allergic to (meth)acrylates, reactions to one or two (meth)acrylates were proven in 42% of them, while allergies to ≥ 5 (meth)acrylates in 33% [24]. According to the study by Raposo et al., positive patch tests to HEMA acrylates were observed in more than 90% of patients with an allergy to acrylates [21]. In comparison, 64.1% were positive for 2-HPMA, so they can be considered a good screening marker [21]. Therefore, it is proposed that 2-HEMA and HPMA should be added to the European basic patch test series [11,30]. Also, since acrylic monomers often cause cross-reactions, sensitized persons should not be exposed to any of these compounds [10,58]. Following the results of allergy tests to nail acrylates and the results of patch tests to them ("European Baseline Series and Acrylate Series Nails Artificial" and 10% ethyl cyanoacrylate), significant contact allergies to tri ethylene glycol diacrylate were observed [22]. Previous sensitization to nail acrylates can lead to eczematous reactions after exposure to dental fillings, bone cement, hearing aids, surgical adhesives or insulin devices containing acrylates. Therefore, clinicians and patients/clients who are in contact with acrylates should be adequately informed about possible adverse reactions and their recognition and proof [11,48]. According to research by Lyapina, more than two-thirds of all dentistry workers/students who reported skin symptoms (61.9%) were third- and fourth-year students and practitioners (most often without skin symptoms were dental professionals) [10]. According to these results, the general sensitization rates to MA in the studied population are relatively high: from 25.9% (for MMA) to 31.7% (for TEGDMA). In addition, a significantly higher frequency of sensitization to MMA and TEGDMA in third- and fourth-year students compared to dental professionals was also observed. A significantly higher frequency of sensitization to EGDMA, BIS-GMA, 2-HEMA, and tetrahydrofuryl methacrylate was recorded in patients compared to dental professionals. Therefore, greater awareness of the possible adverse effects of exposure to MA is needed [10]. Regarding diagnostics of potential oral manifestations to acrylates, although the patch test is a standard method for confirmation of contact allergies, the correct interpretation of the results and their clinical importance for oral mucosal lesions (histologically different from the skin) can be complex. Differences in the concentration of haptens in the oral mucosa compared to standard substances and differences in pH values are essential for the patch test results, which can lead to false positive/negative results or non-specific irritant reactions [59]. Also, sometimes inadequately made prosthetic works can imitate allergic reactions, and assessing the clinical importance of haptens in dental materials is difficult.
6. Allergy to Acrylates and Methacrylates in Dental Workers and Students
Many acrylic monomers are used in dentistry, so dental workers can become sensitized (dentists, dental technicians, patients, or dental students) when it's necessary to examine the possibility of adverse reactions to dental preparations based on acrylates to which they are exposed. Numerous studies confirm the high frequency of sensitization to (meth)acrylates in dental professionals and their patients (who are exposed to resin-based materials during dental treatments) [10]. In their daily activities, dental professionals and dental students are exposed to numerous chemical substances, primarily from various dental materials and drugs. Thus, dental products contain numerous allergens and irritants that can cause health problems for dental professionals (during their professional exposure), dental students (during their education) and patients to whom they are applied. According to the literature data, the most common positive allergens among dentists and dental nurses were 2-HEMA, ethyl acrylate (EA), TEGDMA, and bis-GMA [10]. At the same time, 2-HEMA is considered the most critical allergen for dentists and dental nurses, while MMA and EGDMA are significant for dental technicians. The relevance of the positive reaction is also crucial, as positive patch test reactions to bis-GMA, diethylene glycol diacrylate (DEGDA), TEGDMA, ethyl methacrylate (EMA), and EA were relevant in some patients [10,44,58,60]. In the study population, overall sensitization rates to MA were relatively high, varying from 25.9% for MMA to 31.7% for TEGDMA. The lowest frequency of sensitization was in dental professionals, while the highest rates varied (depending on the allergens and examined groups). There was significantly more frequent sensitization to MMA and TEGDMA in third- and fourth-year students than in dental professionals, likely related to their recent and intensive exposure to these substances during the second year of training [10]. Due to the occupational nature of the exposure, a patch test for contact allergens is required for the complete diagnosis and evaluation of professional skin allergy to MA in dental staff [9]. Numerous studies confirm the high frequency of sensitization to (meth)acrylates in dental professionals, as well as in patients who undergo dental treatment and are exposed to resin-based materials [14,61,62]. Several other studies have been conducted to assess the frequency of sensitization to acrylates in various populations (Table 1) [1,2,3,4,5,6,7,13,14,19,63,64].
Due to the frequent use of acrylic monomers in dentistry, dental workers (dental staff, patients, or dental students) sometimes become sensitized (with a positive patch test), when is essential to identify these individuals and determine the relevance of their allergies. In addition to proving sensitization to allergens by patch test, it is necessary to examine the relevance of these reactions [65]. It is also crucial that product declarations of dental acrylate materials list all acrylic compounds present in the products, including acrylic monomers/impurities with concentrations lower than 1%. This could help select a product that a sensitized person could use.
7. Preventive Procedures
Health professionals should recognize possible occupational hazards and reactions like contact dermatitis to acrylates and apply preventive measures to avoid contact dermatitis [9]. Preventive measures should include the correct use of personal protective equipment, such as protective gloves, goggles, masks and disposable aprons. Non-contact techniques are also important to avoid skin exposure to these chemicals [66]. When choosing gloves, nitrile rubber gloves provide better protection against MA penetration, with higher penetration resistance and lower monomer penetration rates. Nitrile gloves are more effective than latex gloves, but only for a short exposure (15–20 minutes), as demonstrated by a patch test on glove fragments [11]. Gloves should also be changed frequently. Morgado et al. suggest using nitrile gloves for 30 minutes and changing them if the procedure is not completed [67]. It has been observed that during prolonged exposure, (meth)acrylates likely diffuse from the nail gel and cause dermatitis. In case of contact with the allergen for longer than 30 minutes, it is recommended to use 4H (ethylene-vinyl alcohol-polyethylene) finger covers under classic protective gloves or complete 4H gloves (although they are less comfortable and limit the sense of touch) [11,28,40,48]. Applying basic preventive measures is helpful in preventing new cases of contact dermatitis that could lead to a change of occupation [9]. Adequate personal protection among students is also essential [10]. Since the awareness of the sensitizing properties of acrylates has increased in recent years and due to the application of personal protection, as well as the popularity of non-contact techniques, the number of dental staff allergic to MA has somewhat decreased [11,68]. Looking at the prevention of reactions to acrylates in cosmetics, many irritating reactions of the mucous membranes and skin of beauticians could be prevented and avoided by using effective ventilation systems as well as personal protective equipment (such as goggles and masks) when exposed to volatile substances or dust [11,55]. The risk of sensitization also depends on the correct use of quality UV devices and the appropriate curing time of the gel, which is higher when applied at home by people who are not sufficiently trained and educated about the risks when handling acrylates. Additionally, "home beauticians" sometimes neglect necessary protective measures or change artificial nails too often, causing their skin to come into contact with nail polish more frequently and increasing the risk of sensitization [11,31]. Career counselling for a person with an adverse reaction to acrylates, including a potential allergy to acrylates, is also an important issue. Allergy to acrylates can significantly influence the choice of future profession and determine the ability to work [28]. The literature describes the case of a manicurist who developed an allergic skin reaction to acrylates after three months of work, presenting with bullous lesions on the fingertips and eczema of the hands and ears. Due to the lack of retraining counselling, she began working as a dental nurse [11]. Shortly after re-exposure to acrylates in dental materials, her skin manifestations recurred and patch tests showed positive reactions to several acrylates (2-HEMA, 2-HPMA, EGDMA, etc.) and she had to change her job. It should be known that re-exposure to acrylates at a new job can cause a recurrence of skin lesions [11,69]. Therefore, for successful retraining of people allergic to acrylates, it is crucial to consider the presence of these chemicals in different workplaces (e.g., dentistry, beauty salons, the printing industry and the construction industry) [11,28,40,48,70,71]. Clinicians should be appropriately educated and trained to provide suitable patient care. For example, if a medical procedure is planned, patients allergic to acrylates require cementless arthroplasty and dental materials that do not release acrylates.
8. Conclusions
Acrylates have become integral to many industries, from their initial applications to today's widespread use in various medical and cosmetic products that come into direct contact with the user's skin and tissues. While their usage offers numerous advantages, the risk of undesired, including allergic reactions, should not be ignored. Acrylates as a cause of ACD and other disorders highlight that allergic responses to acrylates, especially ACD, pose a significant problem. Skin tests and laboratory analyses are crucial for identifying and confirming allergic reactions, enabling targeted treatment and prevention. Due to frequent exposure to acrylates, dentists, dental technicians and students face an increased risk of developing allergic reactions, necessitating special preventive measures and adaptations in the work environment. Utilizing protective equipment, modifying work procedures and providing employee education are vital to safeguard the health of users and professionals who work with acrylates daily.
Author Contributions
Conceptualization, L.L.-M.; methodology, L.L.-M.; software, E.F., V.V. and L.P.; validation, L.L.-M., E.P. and B.Š.; formal analysis, L.L.-M., E.P. and B.Š.; investigation, L.L.-M., E.F., V.V., L.P., E.P. and B.Š.; resources, L.L.-M.; data curation, R.T. and E.B.; writing—original draft preparation, L.L.-M., E.F., V.V. and L.P.; writing—review and editing, L.L.-M., E.P., R.T., E.V. and B.Š.; visualization, L.L.-M.; supervision, L.L.-M.; project administration, E.P., R.T., E.V. and B.Š. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- de Groot, A.C.; Rustemeyer, T. 2-Hydroxyethyl methacrylate (HEMA): A clinical review of contact allergy and allergic contact dermatitis. Part 2. Cross- and co-sensitization, other skin reactions to HEMA, position of HEMA among (meth)acrylates, sensitivity as screening agent, presence of HEMA in commercial products and practical information on patch test procedures. Contact Dermatitis 2024, 90, 1–16. [Google Scholar] [PubMed]
- Havmose, M.; Thyssen, J.P.; Zachariae, C.; Johansen, J.D. Contact allergy to 2-hydroxyethyl methacrylate in Denmark. Contact Dermatitis 2020, 82, 229–231. [Google Scholar] [CrossRef] [PubMed]
- Opalińska, S.; Opalińska, M.; Rudnicka, L.; Czuwara, J. Contact eczema induced by hybrid manicure. The role of acrylates as a causative factor. Postepy Dermatol. Alergol. 2022, 39, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Isaksson, M.; Zimerson, E.; Svedman, C. Occupational airborne allergic contact dermatitis from methacrylates in a dental nurse. Contact Dermatitis 2007, 57, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Ramos, L.; Cabral, R.; Gonçalo, M. Allergic contact dermatitis caused by acrylates and methacrylates—a 7-year study. Contact Dermatitis 2014, 71, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Gregoriou, S.; Tagka, A.; Velissariou, E.; Tsimpidakis, A.; Hatzidimitriou, E.; Platsidaki, E.; Kedikoglou, S.; Chatziioannou, A.; Katsarou, A.; Nicolaidou, E.; et al. The rising incidence of allergic contact dermatitis to acrylates. Dermatitis 2020, 31, 140–143. [Google Scholar] [CrossRef] [PubMed]
- Geukens, S.; Goossens, A. Occupational contact allergy to (meth)acrylates. Contact Dermatitis 2001, 44, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Sasseville, D. Acrylates in contact dermatitis. Dermatitis 2012, 23, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Cameli, N.; Silvestri, M.; Mariano, M.; Messina, C.; Nisticò, S.P.; Cristaudo, A. Allergic contact dermatitis, an important skin reaction in diabetes device users: a systematic review. Dermatitis 2022, 33, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Lyapina, M.; Dencheva, M.; Krasteva, A.; Tzekova, M.; Kisselova-Yaneva, A. Concomitant contact allergy to formaldehyde and methacrylic monomers in students of dental medicine and dental patients. Int. J. Occup. Med. Environ. Health 2014, 27, 797–807. [Google Scholar] [CrossRef]
- Kucharczyk, M.; Słowik-Rylska, M.; Cyran-Stemplewska, S.; Gieroń, M.; Nowak-Starz, G.; Kręcisz, B. Acrylates as a significant cause of allergic contact dermatitis: new sources of exposure. Postepy Dermatol. Alergol. 2021, 38, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Spencer, A.; Gazzani, P.; Thompson, D.A. Acrylate and methacrylate contact allergy and allergic contact disease: a 13-year review. Contact Dermatitis 2016, 75, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Wrangsjö, K.; Swartling, C.; Meding, B. Occupational dermatitis in dental personnel: contact dermatitis with special reference to (meth)acrylates in 174 patients. Contact Dermatitis 2001, 45, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Goon, A.T.; Isaksson, M.; Zimerson, E.; Goh, C.L.; Bruze, M. Contact allergy to (meth)acrylates in the dental series in southern Sweden: simultaneous positive patch test reaction patterns and possible screening allergens. Contact Dermatitis 2006, 55, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Fugolin, A.P.; Dobson, A.; Mbiya, W.; Navarro, O.; Ferracane, J.L.; Pfeifer, C.S. Use of (meth)acrylamides as alternative monomers in dental adhesive systems. Dent. Mater. 2019, 35, 686–696. [Google Scholar] [CrossRef] [PubMed]
- Rolls, S.; Rajan, S.; Shah, A.; Bourke, J.; Chowdhury, M.; Ghaffar, S.; Green, C.; Johnston, G.; Orton, D.; Reckling, C.; et al. (Meth)acrylate allergy: Frequently missed? Br. J. Dermatol. 2018, 178, 980–981. [Google Scholar] [CrossRef] [PubMed]
- Japundžić-Rapić, I.; Macan, J.; Babić, Ž.; Vodanović, M.; Salarić, I.; Prpić-Mehičić, G.; Gabrić, D.; Pondeljak, N.; Lugović-Mihić, L. Work-related and personal predictors of hand eczema in physicians and dentists: results from a field study. Dermatitis 2024, 35, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Piirilä, P.; Kanerva, L.; Keskinen, H.; Estlander, T.; Hytönen, M.; Tuppurainen, M.; Nordman, H. Occupational respiratory hypersensitivity caused by preparations containing acrylates in dental personnel. Clin. Exp. Allergy 1998, 28, 1404–1411. [Google Scholar] [CrossRef] [PubMed]
- Muttardi, K.; White, I.R.; Banerjee, P. The burden of allergic contact dermatitis caused by acrylates. Contact Dermatitis 2016, 75, 180–184. [Google Scholar] [CrossRef]
- Uter, W.; Geier, J. Contact allergy to acrylates and methacrylates in consumers and nail artists – data of the Information Network of Departments of Dermatology, 2004–2013. Contact Dermatitis 2015, 72, 224–228. [Google Scholar] [CrossRef]
- Raposo, I.; Lobo, I.; Amaro, C.; Lobo, M.L.; Melo, H.; Parente, J.; Pereira, T.; Rocha, J.; Cunha, A.P.; Baptista, A.; et al. Allergic contact dermatitis caused by (meth)acrylates in nail cosmetic products in users and nail technicians – a 5-year study. Contact Dermatitis 2017, 77, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Dudek, W.; Wittczak, T.; Swierczyńska-Machura, D.; Kręcisz, B.; Nowakowska-Świrta, E.; Kieć-Świerczyńska, M.; Pałczyński, C. Allergic blepharoconjunctivitis caused by acrylates promotes allergic rhinitis response. Ann. Allergy Asthma Immunol. 2014, 113, 492–494. [Google Scholar] [CrossRef] [PubMed]
- Kanerva, L.; Alanko, K.; Estlander, T.; Jolanki, R.; Lahtinen, A.; Savela, A. Statistics on occupational contact dermatitis from (meth)acrylates in dental personnel. Contact Dermatitis 2000, 42, 175–176. [Google Scholar] [PubMed]
- Heratizadeh, A.; Werfel, T.; Schubert, S.; Geier, J.; IVDK. Contact sensitization in dental technicians with occupational contact dermatitis. Data of the Information Network of Departments of Dermatology (IVDK) 2001–2015. Contact Dermatitis 2018, 78, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Splete, H.; Dermatologists name isobornyl acrylate contact allergen of the year. AT ACDS. 2019. Available online: https://www.mdedge.com/dermatology/article/195656/contact-dermatitis/dermatologists-name-isobornyl-acrylate-contact. (Accessed on 6 June 2024).
- Lin, Y.; Tsai, S.; Yang, C.; Tseng, Y.; Chu, C. Allergic contact dermatitis caused by acrylates in nail cosmetic products: case reports and review of the literature. Dermatol. Sin. 2018, 36, 218–221. [Google Scholar] [CrossRef]
- Gatica-Ortega, M.E.; Pastor-Nieto, M.A.; Mercader-García, P.; Silvestre-Salvador, J. Allergic contact dermatitis caused by (meth)acrylates in long-lasting nail polish – are we facing a new epidemic in the beauty industry? Contact Dermatitis 2017, 77, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Gonçalo, M.; Pinho, A.; Agner, T.; Andersen, K.E.; Bruze, M.; Diepgen, T.; Foti, C.; Giménez-Arnau, A.; Goossens, A.; Johanssen, J.D.; et al. Allergic contact dermatitis caused by nail acrylates in Europe. An EECDRG study. Contact Dermatitis 2018, 78, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Canizares, O. Contact dermatitis due to the acrylic materials used in artificial nails. AMA Arch. Derm. 1956, 74, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Gonçalo, M. Nail acrylate allergy: the beauty, the beast and beyond. Br. J. Dermatol. 2019, 181, 663–664. [Google Scholar] [CrossRef] [PubMed]
- Gatica-Ortega, M.E.; Pastor-Nieto, M.A.; Gil-Redondo, R.; Martínez-Lorenzo, E.R.; Schöendorff-Ortega, C. Non-occupational allergic contact dermatitis caused by long-lasting nail polish kits for home use: ‘the tip of the iceberg’. Contact Dermatitis 2018, 78, 261–265. [Google Scholar] [CrossRef]
- Ródenas-Herranz, T.; Navarro-Triviño, F.J.; Linares-González, L.; Ruiz-Villaverde, R.; Brufau-Redondo, C.; Mercader-García, P. Acrylate allergic contact dermatitis caused by hair prosthesis fixative. Contact Dermatitis 2020, 82, 62–64. [Google Scholar] [CrossRef] [PubMed]
- Hyry, H.S.I.; Liippo, J.P.; Virtanen, H.M. Allergic contact dermatitis caused by glucose sensors in type 1 diabetes patients. Contact Dermatitis 2019, 81, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Herman, A.; de Montjoye, L.; Tromme, I.; Goossens, A.; Baeck, M. Allergic contact dermatitis caused by medical devices for diabetes patients: a review. Contact Dermatitis 2018, 79, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Raison-Peyron, N.; Mowitz, M.; Bonardel, N.; Aerts, O.; Bruze, M. Allergic contact dermatitis caused by isobornyl acrylate in OmniPod, an innovative tubeless insulin pump. Contact Dermatitis 2018, 79, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Mowitz, M.; Herman, A.; Baeck, M.; Isaksson, M.; Antelmi, A.; Hamnerius, N.; Pontén, A.; Bruze, M. N,N-dimethylacrylamide – a new sensitizer in the FreeStyle Libre glucose sensor. Contact Dermatitis 2019, 81, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Oppel, E.; Kamann, S. Hydrocolloid blister plaster decreases allergic contact dermatitis caused by Freestyle Libre and isobornyl acrylate. Contact Dermatitis 2019, 81, 380–381. [Google Scholar]
- Dittmar, D.; Dahlin, J.; Persson, C.; Schuttelaar, M.L. Allergic contact dermatitis caused by acrylic acid used in transcutaneous electrical nervous stimulation. Contact Dermatitis 2017, 77, 409–412. [Google Scholar] [CrossRef] [PubMed]
- Foti, C.; Lopalco, A.; Stingeni, L.; Hansel, K.; Lopedota, A.; Denora, N.; Romita, P. Contact allergy to electrocardiogram electrodes caused by acrylic acid without sensitivity to methacrylates and ethyl cyanoacrylate. Contact Dermatitis 2018, 79, 118–121. [Google Scholar] [CrossRef] [PubMed]
- Shah, V.; Chaubal, T.V.; Bapat, R.A.; Shetty, D. Allergic contact dermatitis caused by polymethylmethacrylate following intradermal filler injection. Contact Dermatitis 2017, 77, 407–408. [Google Scholar] [CrossRef] [PubMed]
- Marrero-Alemán, G.; Sabater-Abad, J.; Miquel, F.J.; Boix-Vilanova, J.; Mestre Bauzá, F.; Borrego, L. Allergic contact dermatitis to (meth)acrylates involving nail technicians and users: prognosis and differential diagnosis. Allergy 2019, 74, 1386–1389. [Google Scholar] [CrossRef]
- Parać, E.; Špiljak, B.; Lugović-Mihić, L.; Bukvić Mokos, Z. Acne-like eruptions: disease features and differential diagnosis. Cosmetics 2023, 10, 89. [Google Scholar] [CrossRef]
- Walters, G.I.; Robertson, A.S.; Moore, V.C.; Burge, P.S. Occupational asthma caused by acrylic compounds from SHIELD surveillance (1989–2014). Occup. Med. 2017, 67, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Aalto-Korte, K.; Alanko, K.; Kuuliala, O.; Jolanki, R. Methacrylate and acrylate allergy in dental personnel. Contact Dermatitis 2007, 57, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Rustemeyer, T.; Frosch, P.J. Occupational contact dermatitis in dental personnel. In Kanerva’s Occupational Dermatology, John, S., Johansen, J., Rustemeyer, T., Elsner, P., Maibach, H., Eds.; Springer: Cham, Germany, 2019; pp. 1–12. ISBN 978-3-319-40221-5. [Google Scholar]
- Lugović-Mihić, L.; Ferček, I.; Duvančić, T.; Bulat, V.; Ježovita, J.; Novak-Bilić, G.; Šitum, M. Occupational contact dermatitis amongst dentists and dental technicians. Acta Clin. Croat. 2016, 55, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Japundžić, I.; Bembić, M.; Špiljak, B.; Parać, E.; Macan, J.; Lugović-Mihić, L. Work-related hand eczema in healthcare workers: etiopathogenic factors, clinical features, and skin care. Cosmetics 2023, 10, 134. [Google Scholar] [CrossRef]
- Alamri, A.; Lill, D.; Summer, B.; Thomas, P.; Thomas, B.; Oppel, E. Artificial nail wearing: unexpected elicitor of allergic contact dermatitis, oral lichen planus and risky arthroplasty. Contact Dermatitis 2019, 81, 210–211. [Google Scholar] [CrossRef] [PubMed]
- Lazarov, A. Sensitization to acrylates is a common adverse reaction to artificial fingernails. J. Eur. Acad. Dermatol. Venereol. 2007, 21, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Okada, K.; Kondo, M.; Matsushita, T.; Nakazawa, S.; Yamazaki, Y. Oral health for achieving longevity. Geriatr. Gerontol. Int. 2020, 20, 526–538. [Google Scholar] [CrossRef] [PubMed]
- Savage, N.W.; Boras, V.V.; Barker, K. Burning mouth syndrome: clinical presentation, diagnosis and treatment. Aust. J. Dermatol. 2006, 47, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Lugović-Mihić, L.; Špiljak, B.; Blagec, T.; Delaš Aždajić, M.; Franceschi, N.; Gašić, A.; Parać, E. Factors participating in the occurrence of inflammation of the lips (cheilitis) and perioral skin. Cosmetics 2023, 10, 9. [Google Scholar] [CrossRef]
- Symanzik, C.; Weinert, P.; Babić, Ž.; Hallmann, S.; Havmose, M.S.; Johansen, J.D.; Kezic, S.; Macan, M.; Macan, J.; Strahwald, J.; et al. Allergic contact dermatitis caused by 2-hydroxyethyl methacrylate and ethyl cyanoacrylate contained in cosmetic glues among hairdressers and beauticians who perform nail treatments and eyelash extension as well as hair extension applications: A systematic review. Contact Dermatitis 2022, 86, 480–492. [Google Scholar]
- Mattos Simoes Mendonca, M.; LaSenna, C.; Tosti, A. Severe onychodystrophy due to allergic contact dermatitis from acrylic nails. Skin Appendage Disord. 2015, 1, 91–94. [Google Scholar] [CrossRef]
- Kieć-Świerczyńska, M.; Świerczyńska-Machura, D.; Chomiczewska-Skóra, D.; Kręcisz, B.; Walusiak-Skorupa, J. Screening survey of ocular, nasal, respiratory and skin symptoms in manicurists in Poland. Int. J. Occup. Med. Environ. Health. 2017, 30, 887–896. [Google Scholar] [CrossRef]
- Pesonen, M.; Kuuliala, O.; Henriks-Eckerman, M.L.; Aalto-Korte, K. Occupational allergic contact dermatitis caused by eyelash extension glues. Contact Dermatitis 2012, 67, 307–308. [Google Scholar] [CrossRef]
- Japundžić, I. The impact of working conditions and constitutional factors on the onest of contact dermatitis of the hands in dental medicine doctors and medical doctors. Doctoral Dissertation, University of Zagreb, School of Dental Medicine, Zagreb, Croatia, 2020. Available online: https://repozitorij.sfzg.unizg.hr/islandora/object/sfzg:708 (accessed on 12 June 2024).
- Drucker, A.M.; Pratt, M.D. Acrylate contact allergy: patient characteristics and evaluation of screening allergens. Dermatitis 2011, 22, 98–101. [Google Scholar] [CrossRef]
- Minciullo, P.L.; Paolino, G.; Vacca, M.; Gangemi, S.; Nettis, E. Unmet diagnostic needs in contact oral mucosal allergies. Clin. Mol. Allergy 2016, 14, 10. [Google Scholar] [CrossRef]
- Aalto-Korte, K.; Henriks-Eckerman, M.L.; Kuuliala, O.; Jolanki, R. Occupational methacrylate and acrylate allergy—cross-reactions and possible screening allergens. Contact Dermatitis 2010, 63, 301–312. [Google Scholar] [CrossRef]
- Tillberg, A.; Stenberg, B.; Berglund, A. Reactions to resin-based dental materials in patients-type, time to onset, duration, and consequence of the reaction. Contact Dermatitis 2009, 61, 313–319. [Google Scholar] [CrossRef]
- Prasad Hunasehally, R.Y.; Hughes, T.M.; Stone, N.M. Atypical pattern of (meth)acrylate allergic contact dermatitis in dental professionals. Br. Dent. J. 2012, 213, 223–224. [Google Scholar] [CrossRef]
- Kieć-Świerczyńska, M.K. Occupational allergic contact dermatitis due to acrylates in Lodz. Contact Dermatitis 1996, 34, 419–422. [Google Scholar] [CrossRef]
- Kanerva, L.; Estlander, T.; Jolanki, R.; Tarvainen, K. Occupational allergic contact dermatitis caused by exposure to acrylates during work with dental prostheses. Contact Dermatitis 1993, 28, 268–275. [Google Scholar] [CrossRef]
- Budimir, J.; Mravak-Stipetić, M.; Bulat, V.; Ferček, I.; Japundžić, I.; Lugović-Mihić, L. Allergic reactions in oral and perioral diseases-what do allergy skin test results show? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 40–48. [Google Scholar] [CrossRef]
- Thomas, S.; Padmanabhan, T.V. Methyl methacrylate permeability of dental and industrial gloves. N. Y. State Dent. J. 2009, 75, 40–42. [Google Scholar]
- Morgado, F.; Batista, M.; Gonçalo, M. Short exposures and glove protection against (meth)acrylates in nail beauticians – thoughts on a rising concern. Contact Dermatitis 2019, 81, 62–63. [Google Scholar] [CrossRef]
- Aalto-Korte, K.; Pesonen, M. The additive value of patch testing non-commercial test substances and patients' own products in a clinic of occupational dermatology. Contact Dermatitis 2023, 88, 27–34. [Google Scholar] [CrossRef]
- Kieć-Świerczyńska, M.; Krecisz, B.; Chomiczewska-Skóra, D. Occupational contact dermatitis to acrylates in a manicurist. Occup. Med. (Lond.) 2013, 63, 380–382. [Google Scholar] [CrossRef]
- Luo, S.; Liu, F.; He, J. Preparation of low shrinkage stress dental composite with synthesized dimethacrylate oligomers. J. Mech. Behav. Biomed. Mater. 2019, 94, 222–228. [Google Scholar] [CrossRef]
- Rodrigues, S.B.; Petzhold, C.L.; Gamba, D.; Leitune, V.C.B.; Collares, F.M. Acrylamides and methacrylamides as alternative monomers for dental adhesives. Dent. Mater. 2018, 34, 1634–1644. [Google Scholar] [CrossRef]
Figure 1.
Skin lesions in the person who works as a manicurist (Image from the archive of the main author, Prof. Dr. Lugović Mihić).
Figure 1.
Skin lesions in the person who works as a manicurist (Image from the archive of the main author, Prof. Dr. Lugović Mihić).

Figure 2.
Positive patch test to contact allergens - standard testing procedure (Image from the archive of the main author, Prof. Dr. Lugović Mihić).
Figure 2.
Positive patch test to contact allergens - standard testing procedure (Image from the archive of the main author, Prof. Dr. Lugović Mihić).
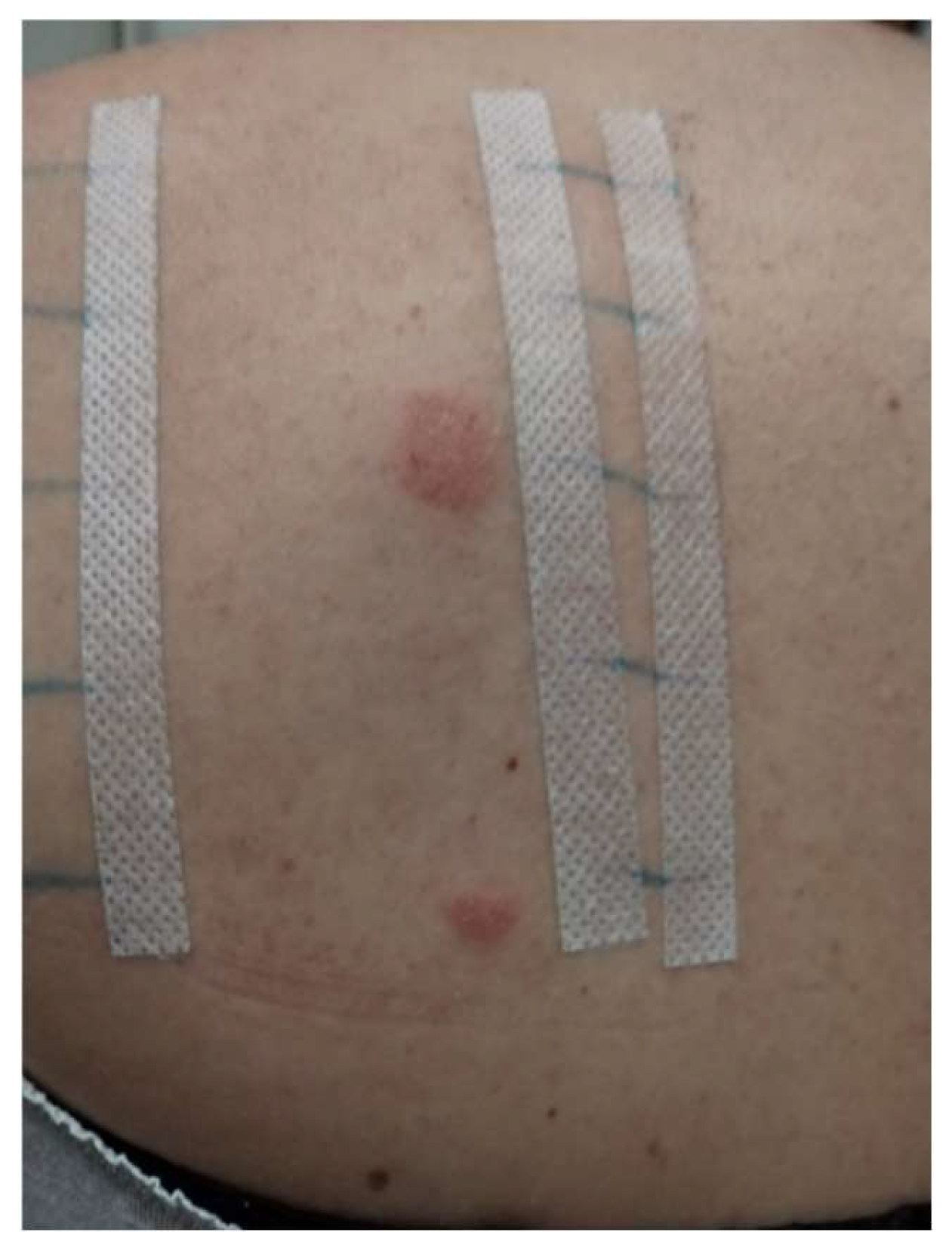
Figure 3.
Positive patch test to acrylates and MA in a dentist (Image taken from the doctoral dissertation of Dr. Iva Japundžić [57], courtesy of Dr. Iva Japundžić Rapić).
Figure 3.
Positive patch test to acrylates and MA in a dentist (Image taken from the doctoral dissertation of Dr. Iva Japundžić [57], courtesy of Dr. Iva Japundžić Rapić).


Table 1.
Selected data on unwanted reactions to acrylates obtained by different studies.
| Author, Year [Reference number] | Examinees/Patients | Analysed Factors - Methods | Results | Conclusions |
| Kanerva L et al., 1993 [64] | 4 patients (an orthodontist, 2 dental technicians, and an in-house trained dental worker) | Patch testing for allergens in dental prostheses | All patients had positive allergic patch test reactions to MMA. | Dental personnel working with prostheses - higher risk of sensitization. Patients working with dental prostheses should be patch-tested with MMA, 2-HEMA, dimethacrylates, epoxy acrylates, and urethane acrylates to detect occupational ACD. |
| Kiec-Swierczynska MK, 1996 [63] |
1619 patients suspected of occupational CD (examined during 1990-1994) | Patch testing to acrylates and methacrylates including EGDMA, MMA, 2-HEMA and TEGDMA | The most frequent sensitizers were: EGDMA (5 positive patch tests), MMA (4), 2-HEMA (4) and TEGDMA (4). Sensitivity to acrylates was diagnosed in 9 patients (4 dental technicians, 4 dentists, 1 textile printer). |
Dentists more sensitive to (meth)acrylate allergens and other allergens (metals and rubber additives). Dental techniques mainly sensitive to methacrylates. The textile printer was only sensitive to acrylates. |
| Geukens S and Goossens A, 2001 [7] |
3,833 patients suspect of CD (during 1978-1999) | Patients were tested by patch test | The top three sensitizers were EGDMA (17 positive patch tests), 2-HEMA, (14), and TEGDMA (6). Almost the half of the examinees (14/31) were affected by (meth)acrylate-containing dental materials (including dentists and dental technology students). |
An increasing trend in dermatological issues associated with the expanding use of (meth)acrylates, particularly in dental professions. |
| Wrangsjö K et al., 2001 [13] | 174 dental personnel referred as patients to the Department of Occupational and Environmental Dermatology, Stockholm (1995- 1998) | Patch testing to the Swedish standard series and a dental screening series. Testing for IgE-mediated allergy to natural rubber latex (NRL). |
Hand eczema affected 63% participants; 67% ICD, and 33% ACD. 59% of participants had positive reactions to standard series substances and 40% to the dental series. 22% had positive reactions to (meth)acrylates, primarily to multiple test preparations, including HEMA, EGDMA, and MMA. Allergy to NRL was recorded in 10% of patients. |
Irritant hand dermatitis was the predominant diagnosis among dental personnel. Contact allergy to (meth)acrylate in around 20% of the tested patients, mostly to 3 test substances; HEMA, EGDMA and MMA. (Meth)acrylate allergy often coexisted with atopy and/or other contact allergies. |
| Goon AT et al., 2006 [14] |
1639 subjects were patch-tested at the Department of Occupational and Environmental Dermatology, Malmo, Sweden | Patch tests to to either dental patient series or dental personnel series including (meth)acrylate allergens: identification of common allergens and their prevalence in each group. | Positive patch tests to (meth)acrylate allergens were seen in 2.3% (30/1322) of the dental patients and 5.8% (18/310) of the dental personnel. The most common allergens for both groups were 2-HEMA, EGDMA, and MMA. |
2-HEMA is important screening allergen to detect contact allergy to (meth)acrylates used in the dental profession. |
| Isaksson M et al., 2007 [4] | A case report (dental nurse with facial eczema allegedly caused by airborne methacrylates in the workplace) | Patch testing with serial dilutions of several methacrylates and work provocations in methacrylate environments | High reactivity to patch testing. Repeated exposure to methacrylates at work led to facial eczema; resolved when away. Efforts to collect the sensitizers using air pumps and filters failed. |
Facial dermatitis may be associated with airborne methacrylate exposure, which may involve allergy to ≥1 allergens. |
| Ramos L et al., 2014 [5] |
An observational and retrospective study (January 2006–April 2013) | Evaluation and correlation of epidemiological and clinical parameters and positive patch test results with (meth)acrylates. | 37/122 patients show a positive patch test with an extended (meth)acrylate series. 25 cases (67.6%) were occupational. Hand eczema with pulpitis in 32 patients: 28 related to artificial nails, 3 to dental materials, and 2 to industrial work. Oral lesions associated with dental prostheses in 4 patients. 31/37 positive to >1 (meth)acrylate. Beauty technicians with artificial nails accounted for 80% of occupational cases. |
HEMA detected 80.6% of cases and it may serve as a reliable screening allergen. A broader range of allergens is advisable for accurate diagnosis. |
| Muttardi K et al., 2016 [19] |
A retrospective study of 241 patients were patch tested with meth(acrylates) and cyanoacrylates (January 2012 – February 2015) | Patch testing with the mini-acrylate or extended acrylate series. | 16/241 patients had positive patch test reactions to (meth)acrylate or cyanoacrylate. Female predominance (M/F ratio of 1:15). |
(Meth)acrylate allergy is mainly occupational, but more common in younger women, especially beauticians and nail technicians. |
| Havmose M et al., 2020 [2] | 1293 female patients patch-tested with HEMA | Two groups of patients based on their positive/negative patch test reactions to HEMA. MOAHLFA characteristics analyzed for both groups. |
31 (2.4%) of the tested examinees were positive to HEMA. | Sensitization and elicitation of ACD to HEMA primarily from artificial nail modeling systems; a significant health issue for consumers and certain professions. |
| Gregoriou S et al., 2020 [6] | 156 female patients with ACD - using/performing cosmetic nail procedures (January 2009 – December 2018) | The incidence of positive sensitization to (meth)acrylates assessed using patch tests. | Contact allergy to ≥1 (meth)acrylates in 74.4%: 88.5% occupationally exposed, and 11.5% consumers. A statistically significant increase in (meth)acrylate ACD during 2014-2018 (79%) compared to 2009–2013 (55%). EGDMA was the most common sensitizer positive in 72.4%. Among acrylate-positive patients, the rate was 97.4%. |
A global trend of increasing (meth)acrylate sensitization among nail technicians and users of nail products with ACD. Enhancing preventive measures is essential. |
| Opaliñska S et al., 2022 [3] | 8 women with CD related to acrylates found in hybrid varnishes | Manicure using a home acrylic nail kit and a non-professional UV lamp. Clinical and dermoscopic features were assessed. |
Allergen contact areas (skin and nails) were affected. Severity correlated with exposure duration. Common findings: subungual hyperkeratosis and onycholysis (8/8 patients), eczematous finger pulp fissuring (2/8 patients) (more specific). |
Nail changes from hybrid manicures may resemble onychomycosis or nail psoriasis (patch tests in uncertain cases) - ACD was suspected. Confirmed acrylate allergies require patient awareness and avoidance. |
| de Groot AC, Rustemeyer T, 2024 [1] |
24 studies presenting case series and 168 case reports on patients with ACD attributed to HEMA | Review of cross- and co-sensitization, atypical contact allergy manifestations, HEMA versus other (meth)acrylates, HEMA's screening sensitivity, and its presence in commercial products. | Strong cross-allergy exists between HEMA, EGDMA, and HPMA. Reactions to EGDMA often from primary HEMA sensitization. Rare atypical manifestations of HEMA allergy include lichen planus, lymphomatoid papulosis, systemic CD, leukoderma post-positive patch tests, and systemic side effects (nausea, diarrhea, malaise, palpitations). |
HEMA is the most common patch test-positive methacrylate; an effective screening agent for other (meth)acrylates allergies. Sensitization to HEMA 2% pet. in patch tests is exceedingly rare. |
Abbreviations: ACD – allergic contact dermatitis; CD – contact dermatitis; EGDMA – ethylene glycol dimethacrylate; F – female; HEMA – hydroxyethyl methacrylate; HPMA – hydroxypropyl methacrylate; ICD – irritant contact dermatitis; M – male; MMA – methyl methacrylate; MOAHLFA – male, occupational relevance, a history of atopic dermatitis, hand eczema, leg dermatitis, and facial dermatitis, age > 40 years; TEGDMA – triethylene glycol dimethacrylate; 2-HEMA – 2-hydroxyethyl methacrylate.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



