
Submitted:
20 June 2024
Posted:
21 June 2024
You are already at the latest version
Abstract
Background. Coronary artery disease (CAD) with extensive stenosis presents significant clinical challenges. This case report details the management and outcomes of a 61-year-old male with a notable history of CAD, initially treated with coronary artery bypass grafting (CABG), followed by an innovative intravenous hydrogen and oxygen nanobubble therapy due to recurrent symptoms.Case Presentation. Mr. BH was diagnosed with significant stenosis in the left anterior descending (LAD) artery and left circumflex (LCx) artery, initially managed by CABG. Recurring symptoms led to the adoption of a novel treatment involving hydrogen and oxygen nanobubbles. Following treatment initiation, Mr. BH experienced substantial improvements in physical capacity and symptomatic relief, with an ability to climb 22 flights of stairs and resolution of previous symptoms such as dyspnea and cough. Despite these improvements, subsequent imaging revealed in-stent restenosis and progression of graft disease.Discussion. The application of hydrogen and oxygen nanobubbles as a therapy in CAD is explored, highlighting potential mechanisms such as reduction of oxidative stress and improvement in endothelial function. This case contrasts the effects of conventional surgical and pharmaceutical interventions with the novel nanobubble therapy, illustrating both the benefits and complexities of managing advanced CAD with innovative treatments.Conclusion. While Mr. BH showed clinical improvement with nanobubble therapy, the development of new severe stenosis and restenosis underscores the need for further research to understand the long-term efficacy and mechanisms of nanobubble therapy in complex CAD cases. This case suggests that while innovative therapies may provide symptomatic relief and functional improvement, they do not obviate the need for ongoing surveillance and possibly further intervention.
Keywords:
coronary artery disease
; stenosis
; nanobubble
; hydrogen
; oxygen
; antioxidant
; ultrafine bubble
; nanomedicine
; anti‐inflammatory
; cardiovascular
; ischemia
; atherosclerosis
Introduction
Coronary stenosis describes the constriction or occlusion of the coronary arteries, essential for myocardial perfusion. This pathological condition predominantly arises from the progressive accumulation of atherosclerotic plaques, impeding arterial blood flow. The resultant ischemia manifests clinically as angina pectoris, dyspnea, and other symptomatic presentations of coronary artery disease (CAD). In the absence of timely and effective intervention, these stenosis may culminate in critical outcomes, including myocardial infarction or sudden cardiac death.
The development of coronary stenosis involves various factors, including lipid accumulation. Lipids play a crucial role in atherosclerosis, leading to the formation of plaques within the coronary arteries. Studies have shown that dyslipidemia, particularly high levels of LDL cholesterol and triglycerides, is associated with an increased risk of coronary artery disease (CAD)[1,2]. Furthermore, the presence and severity of coronary artery stenosis can be predicted by assessing metabolic and lipidomic profiles, providing insights into the pathogenesis of CAD [3]. Non-invasive imaging techniques like CT coronary angiography can help identify subclinical atherosclerosis and high-risk plaque features, aiding in risk stratification and treatment targets for patients with asymptomatic CAD[4]. Additionally, cardiac mechanical parameters, such as vessel myocardium strain and strain rate, have been correlated with the severity of coronary artery stenosis, offering a potential diagnostic tool for CAD[5].
Current Management of Coronary Stenosis
The management of coronary stenosis has evolved significantly, incorporating a blend of advanced interventional techniques and foundational lifestyle modifications. Among the cornerstone treatments for coronary stenosis, diet, exercise, and smoking cessation play pivotal roles in conservative management, aiming to reduce cardiovascular risks and improve patient outcomes. Smoking cessation is highlighted as a critical intervention, associated with a reduction in cardiovascular events by up to 50%, underscoring its importance in the therapeutic arsenal against coronary heart disease (CHD) [6]. Similarly, physical endurance training, as part of a comprehensive rehabilitation program, has been shown to reduce cardiac mortality in CHD patients by approximately 30%, presenting a compelling case for its inclusion as an alternative to interventional measures in selected patients [7]. Dietary modifications further contribute to the risk reduction strategy, emphasising the role of an appropriate diet in preventing cardiovascular events [8]. These lifestyle interventions are complemented by medical treatments including acetylsalicylic acid, statins, ACE-blockers, and beta-blockers, which have become the standard in medical therapy for CHD [9]. Despite the advancements in percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG), which have significantly improved the management of coronary artery disease (CAD), the importance of conservative treatment remains undiminished [10]. The integration of lifestyle modifications with medical and invasive treatments reflects a holistic approach to managing coronary stenosis. This approach is supported by advancements in diagnostic and therapeutic procedures, including the use of intravascular imaging to guide interventions [11], and the development of novel pharmacological options for refractory angina [12,13]. Moreover, the selection of treatment strategies, whether invasive or conservative, is informed by a thorough assessment of the patient’s condition, including the use of coronary computed tomography angiography (CCTA) for planning and guiding coronary interventions [13]. Diet, exercise, and smoking cessation are integral to the current treatment paradigms for coronary stenosis, serving as foundational elements that complement the advanced therapeutic options available today. These lifestyle interventions are essential for risk reduction and are pivotal in the comprehensive management of patients with coronary artery disease [14].
The management of coronary stenosis involves a multifaceted approach, incorporating antiplatelets, beta-blockers, statins, and ACE inhibitors as cornerstone therapies. Antiplatelet agents, particularly the more potent P2Y12-inhibitors like prasugrel and ticagrelor, play a critical role in acute coronary syndrome (ACS) treatment by preventing thrombotic events, although there remains a need for balancing antithrombotic efficacy against bleeding risk[15]. Beta-blockers, on the other hand, are not only pivotal in managing arrhythmias and treating angina pectoris and heart failure but also in controlling hypertension, a major risk factor in the cardiovascular continuum. Their combination with ACE inhibitors is especially beneficial due to their complementary actions on the sympathetic nervous system and renin-angiotensin-aldosterone system, offering improved cardiovascular outcomes[16]. Statins are another essential component in this regimen, known for their role in reducing plasma levels of myeloperoxidase (MPO) in patients with coronary artery disease (CAD), indicating their influence on inflammatory markers associated with atherosclerosis[17]. ACE inhibitors have shown promise in providing cardiovascular protection and reducing ischemic events and complications in cardiac surgery patients, highlighting their importance beyond blood pressure control[18]. Recent studies have also compared the efficacy of angiotensin receptor blockers (ARBs) with ACE inhibitors, each combined with statin therapy, suggesting substantial reductions in cardiovascular events and mortality in patients with newly diagnosed coronary heart disease, although these findings are subject to debate due to potential biases in study design[19]. For patients with stable angina, a combination of anti-ischemic agents including beta-blockers, nitrates, and calcium channel blockers, alongside metabolic agents and vasodilator therapies, are recommended to prevent myocardial infarction and improve quality of life[20]. In acute settings, such as ACS, the combination of antiplatelet agents and anticoagulants is crucial for preventing coronary events[13]. Furthermore, in the context of acute myocardial infarction (AMI) treated with revascularization, the combined use of beta-blockers and ACEI/ARB has been associated with the lowest incidence of all-cause mortality and heart failure hospitalisation, underscoring the synergistic benefits of these medications[21]. In summary, the current therapeutic strategy for managing coronary stenosis emphasises a comprehensive approach involving antiplatelets, beta-blockers, statins, and ACE inhibitors, each playing a unique role in mitigating the risk of cardiovascular events and improving patient outcomes[22,23].
The current interventional treatments for coronary stenosis include percutaneous coronary intervention (PCI) with angioplasty and stent placement, and coronary artery bypass grafting (CABG). Both treatments have evolved significantly, offering distinct advantages based on patient-specific factors, such as the complexity of coronary artery disease (CAD) and patient comorbidities. PCI, particularly with the use of drug-eluting stents (DES), has become a widely accepted treatment for coronary stenosis, including in-stent restenosis (ISR) and severe stenosis of the left main coronary artery (LMCA). Modern DES reduces the incidence of ISR and is recommended for repeated PCI in cases of ISR. The advancements in stent technology and procedural techniques have contributed to PCI’s favourable outcomes in patients with LMCA disease, showing non-inferiority to CABG in terms of mortality and major adverse cardiac events in patients with low-to-intermediate anatomical complexities[24,25]. However, the presence of severe coronary calcium can increase the complexity of PCI, necessitating advanced plaque-modification devices and techniques, such as rotational atherectomy and lithoplasty, to prepare the lesion adequately for stent placement[6,26]. CABG, on the other hand, remains the standard of care for patients with unprotected left-main disease (ULMD) and multivessel disease (MVD), particularly in those with high anatomical complexity or specific lesion characteristics, such as proximal left anterior descending (pLAD) artery stenosis. CABG is associated with more durable revascularization and lower rates of repeat revascularization compared to PCI. However, it is also associated with a longer recovery period and, in some cases, higher rates of early stroke[8,27]. The choice between PCI and CABG is influenced by several factors, including the patient’s clinical presentation, the anatomical complexity of CAD, and the presence of comorbid conditions. Recent guidelines and clinical trials, including the ISCHEMIA study, have provided insights into the optimal management strategies for patients with chronic coronary syndromes (CCS), emphasising the role of modern conservative therapy alongside interventional treatments[7]. Moreover, the treatment of CAD in special populations, such as cancer patients, has highlighted the importance of individualised care plans, taking into consideration the unique risks and benefits of each treatment modality[10]. In conclusion, the choice between angioplasty with stent placement and CABG for the treatment of coronary stenosis is complex and must be tailored to the individual patient’s needs, based on a thorough assessment of the clinical and anatomical factors, as well as the patient’s preferences and expected outcomes[28].
Regenerative medicine, particularly through the use of stem cell therapies, has shown significant promise in addressing long-standing diseases, including those affecting the heart. The novel CRISPR-Cas9 gene editing technology has enabled precise and efficient gene manipulation, facilitating the development of cell-based therapies for incurable diseases[29]. Stem cell therapy, especially using mesenchymal stem cells (MSCs), has emerged as a breakthrough in treating cardiovascular diseases by promoting the regeneration of infarcted myocardium, which conventional treatments fail to achieve[30]. The success of cell-based therapies in treating ischemic heart disease hinges on the type of stem cells used, their delivery method, and the underlying disease[31]. The potential of stem cells in cardiology lies in their ability to regenerate myocardial tissue, offering a permanent solution beyond temporary measures like stents and medications[32]. However, the transition from somatic, non pluripotent stem or progenitor cells to induced pluripotent stem cells (iPSCs) has marked a significant advancement, moving closer to clinical trials[33]. Despite the marginal results of clinical trials to date, the integration of stem cell therapy with conventional therapies holds the potential to address the health problems of advanced cardiovascular patients[34]. The lack of guideline-based indications for stem cell-based therapy remains a challenge, highlighting the need for further research to establish appropriate criteria[35]. Efforts to improve the efficacy of somatic cardiac cell therapy include selecting specific cellular subpopulations and enhancing delivery methods[36]. The field of regenerative cardiology is rapidly evolving, with adult stem cells and iPSCs playing crucial roles in developing cell-based strategies for heart disease treatment[37]. Collaboration between biotechnology and tissue engineering has led to novel therapeutic strategies, including stem cells and nanotechnology, showing promising effects in managing CAD[38]. Together, these advancements in regenerative medicine and stem cell therapy offer hope for more effective treatments for coronary stenosis, potentially revolutionising the approach to cardiovascular disease management.
Current treatments for coronary stenosis face various challenges and limitations. Severe coronary artery calcification poses a significant obstacle to successful percutaneous coronary intervention, affecting acute and long-term outcomes [39]. In-stent restenosis remains a concern, with a failure rate of 10-15% leading to repeat procedures in about 40% of patients within a year [40]. Additionally, the prevalence of coronary artery calcification in patients with advanced age, chronic kidney disease, and diabetes complicates lesion preparation before stent deployment, often resulting in suboptimal outcomes [41]. Despite advancements like drug-eluting stents reducing in-stent restenosis rates, challenges persist due to aggressive neointimal proliferation and neoatherosclerosis, making DES-ISR treatment complex [42]. Treatment with all-trans-retinoic acid (atRA) has shown promising results in reversing coronary artery stenosis. Research conducted on a mouse model of Kawasaki disease demonstrated that atRA significantly suppressed coronary artery inflammation and reduced the incidence of stenosis by suppressing smooth muscle cell migration [43]. Additionally, a study on drug-coated balloons (DCB) for in-stent restenosis found that a new coating formulation (Agent) was non-inferior to standard DCB in reducing late lumen loss, indicating a potential treatment option for coronary stenosis [44]. Furthermore, cardiovascular medications like angiotensin converting enzyme inhibitors (ACEIs), aldosterone receptor antagonists (ARBs), statins, and calcium channel blockers (CCBs) have been associated with improved coronary flow reserve[45]. However, to the authors’ knowledge, there is not yet any non-invasive treatment that can reverse coronary stenosis.
The Use of Hydrogen and Oxygen Nanobubbles as a Novel Treatment
Hydrogen and oxygen nanobubbles represent an innovative approach to the treatment of coronary stenosis. This method involves the administration of nano-sized bubbles filled with hydrogen and oxygen gases, which have been shown to have potential therapeutic effects on various medical conditions, including inflammation, oxidative stress, and tissue ischemia—all of which are key components in the pathology of coronary artery disease. The therapy involves infusing hydrogen and oxygen nanobubbles into the bloodstream through an intravenous route. These nanobubbles are engineered to be small enough to pass through capillaries without obstructing blood flow, ensuring targeted delivery and efficient absorption.
Scientific Rationale
Hydrogen, as a molecule, has been recognized for its strong antioxidant properties due to its high reducing capability, effectively inhibiting inflammation and neutralising oxygen-derived free radicals, thereby reducing oxidative damage[46,47]. This is further supported by studies demonstrating hydrogen’s ability to decrease levels of pro-inflammatory cytokines such as interleukin-6 (IL-6) and tumour necrosis factor-α (TNF-α), while simultaneously increasing anti-oxidative markers like superoxide dismutase (SOD)[48]. Moreover, hydrogen-rich saline has been found to exert anti-inflammatory and anti-oxidative effects in models of uncontrolled hemorrhagic shock, suggesting its potential for broader therapeutic applications[49]. The anti-inflammatory and anti-oxidative effects of hydrogen are not limited to specific conditions but have also been observed in the context of viral-induced tissue damage, where reducing oxidative stress and inflammatory cytokine storms could alleviate symptoms of severe viral infections[50]. Oxygen nanobubbles, on the other hand, have been highlighted for their role in oxygenating hypoxic patients, particularly those suffering from acute hypoxemic respiratory failure due to COVID-19, showcasing a novel approach to addressing impaired respiration or blood circulation[51]. The combination of hydrogen and oxygen therapies has been explored in clinical settings, where hydrogen-oxygen therapy improved postoperative pulmonary functions, reduced pain intensity, and accelerated recovery in patients undergoing lung surgery, attributed to its anti-inflammatory and anti-oxidative effects[52]. Furthermore, hydrogen therapy’s molecular mechanisms include downregulation of proinflammatory cytokines and pro-apoptotic factors, and upregulation of angiogenic pathways, suggesting its role in promoting vasodilation and improving vascular health[53]. These findings are corroborated by research indicating hydrogen’s therapeutic potential in neurodegenerative diseases through its antioxidant and anti-inflammatory actions[54], and its protective effects against cardiovascular diseases by modulating signal transduction and gene expression to suppress proinflammatory cytokines and ROS production[55]. In summary, hydrogen and oxygen nanobubble intravenous treatments offer a multifaceted therapeutic approach, leveraging their antioxidant, anti-inflammatory, and vasodilation effects to mitigate oxidative stress, inflammation, and improve vascular and overall health.
Preclinical and clinical investigations into hydrogen and oxygen nanobubble intravenous treatments have shown promising results across various medical applications, from mitigating oxidative stress and inflammation in obesity-related disorders to enhancing oxygen delivery in hypoxic tissues and combating hypoxia in cancer therapy. Hydrogen nanobubble water has demonstrated potential in reducing oxidative stress and adipogenesis in adipocytes, suggesting its utility in preventing metabolic disorders associated with obesity[47]. Similarly, oxygen nanobubbles have been explored for their capacity to deliver oxygen to hypoxic tissues, showing promise in mitigating ischemic conditions in the retina[56] and improving blood oxygenation, which could be beneficial in treating hypoxia, ischemic diseases, infection control, and enhancing the efficacy of anticancer chemoradiation therapies[57]. In the realm of cancer treatment, oxygen nanobubbles have been investigated for their ability to reduce tumour hypoxia, potentially improving treatment outcomes[58]. They have also been used as a novel agent for imaging and ultrasound-guided drug delivery in bladder cancer treatment, demonstrating the ability to precisely guide and propel nanobubbles to tumours, enhancing the efficacy of chemotherapy[59]. Furthermore, targeting the hypoxic tumour microenvironment with oxygen nanobubbles has shown to impact cancer epigenetics and therapeutics significantly, indicating a broad application spectrum[60]. Ozonated nanobubbles have been explored for their disinfectant properties, particularly in the context of SARS-CoV-2 in hospital wastewater treatment, highlighting their potential in pandemic response efforts[61]. Additionally, their application in aquaculture to control Vibrio parahaemolyticus and improve water quality further underscores the versatility of nanobubble technology[62,63]. Lastly, lipid-shelled oxygen nanobubbles have been synthesised to reverse hypoxic conditions in breast cancer cells, downregulating HIF-1α and improving cellular conditions, which could lead to enhanced effectiveness of chemotherapy and radiotherapy[64]. These investigations collectively underscore the potential of hydrogen and oxygen nanobubble intravenous treatments in addressing a wide range of medical challenges, from metabolic disorders and hypoxia in ischemic diseases to targeted drug delivery and cancer therapy.
Potential Advantages over Traditional Therapies
Unlike surgical interventions, this intravenous nanobubble treatment does not require any invasive procedures, potentially reducing the risk of complications and recovery time. It can also be used in conjunction with traditional therapies, potentially enhancing overall treatment efficacy. Moreover, preliminary data suggest that nanobubble therapy may have fewer side effects compared to some pharmacological treatments, which can offer a significant advantage for long-term management. This assertion is supported by various studies exploring the multifaceted applications of nanobubbles in medical therapy, particularly in cancer treatment and antibacterial applications. For instance, the biocompatibility assessment of a nanobubble formulation of chloroxylenol-based Dettol showed no notable cytotoxic effect on human keratinocytes and hemocytes, indicating a high level of biocompatibility and suggesting reduced side effects compared to harsher chemical treatments [65]. Similarly, in the realm of cancer therapy, nanobubbles loaded with paclitaxel and lecithin demonstrated reduced toxicity and increased antitumor efficacy in mice, compared to treatments with paclitaxel alone, highlighting the potential for nanobubble therapy to mitigate side effects while enhancing therapeutic outcomes [66]. Moreover, the development of multifunctional nanobubbles for tumour-targeted therapy and imaging has shown not only improved therapeutic efficacy but also selective tumour accumulation, which could potentially reduce the systemic side effects commonly associated with conventional chemotherapy [67]. This targeted approach is further exemplified by the construction of PTX-AMD070 nanobubbles for breast and cervical cancer therapy, which, when combined with ultrasound targeted nanobubble destruction, exhibited pronounced effects in inhibiting cell proliferation and promoting apoptosis, suggesting a method that could minimise adverse effects on healthy tissues [68]. Additionally, the use of nanobubbles in ultrasound imaging and photoacoustic imaging for tracking tumour growth and metastasis offers a non-invasive diagnostic tool that could reduce the need for more invasive, potentially harmful procedures [69]. The environmental and biological safety of nanobubble technology is also highlighted in water treatment applications, where nanobubble ozonation demonstrated effective water purification without the use of harmful chemicals, further underscoring the technology’s potential for safety and reduced side effects in a broad range of applications [70]. In summary, the emerging data from these studies collectively suggest that nanobubble therapy holds promise for reducing side effects compared to some traditional pharmacological treatments, offering a safer, more targeted, and potentially more effective therapeutic approach [71,72,73,74] .
Hydrogen and oxygen nanobubbles present a promising new avenue for the treatment of coronary stenosis. This innovative therapy could potentially address several fundamental pathological aspects of coronary artery disease, offering a holistic approach that might complement or even improve upon existing treatment strategies. As research progresses, this could herald a significant shift in how coronary artery disease is treated, emphasising the importance of continued investigation into novel therapeutic modalities.
Case Presentation
Mr. BH, a 61-year-old male with a significant cardiac history, initially presented on July 12, 2017, with normal transthoracic echocardiography (TTE) results. On February 6, 2018, diagnostic coronary angiography (DCA) findings indicated normal left main coronary artery (LMCA), but revealed extensive calcification and significant stenosis in the left anterior descending (LAD) artery, with 90% stenosis at the ostial, and 100% stenosis at both proximal and distal segments. Additionally, the left circumflex (LCx) artery was calcified with 90% stenosis at its ostial. Right coronary artery (RCA) appeared within normal limits (Figure 1). Collaterals from RCA were supplying the distal LAD. Mr. BH subsequently underwent coronary artery bypass grafting (CABG) with saphenous vein grafts (SVG) to the LAD and obtuse marginal (OM) branch on February 27, 2018.
By December 21, 2020, the clinical diagnosis was mild pulmonary regurgitation with normal left ventricular (LV) systolic function, grade 1 LV diastolic dysfunction, and normal right ventricular (RV) systolic function, as per TTE. On July 11, 2023, Mr. BH reported symptoms of frequent cough, absence of morning erections, dyspnea upon climbing three flights of stairs, and blurred vision. His medication regimen included vitamin D3, clopidogrel (CPG) 5 mg, aspirin (Aspillet) 5 mg, atorvastatin, and irbesartan. His blood pressure (BP) was recorded at 147/92 mmHg, and he started on intravenous (IV) therapy with 5 mL of nanobubble solution in 500 mL normal saline (NS).
Despite ongoing IV therapy, by July 15, he experienced chest pain after walking briskly for 500 metres, which was relieved by resting. Over the subsequent months, the frequency and volume of nanobubble IV therapy were increased, leading to an improvement in his vision and a decrease in the frequency of cough and dyspnea. By September 2, 2023, Mr. BH reported no symptoms, and his BP was 132/87 mmHg. He continued to show improvement and was capable of climbing 22 flights of stairs by December 4, 2023. The 50th IV session on March 1, 2024, maintained his stable condition.
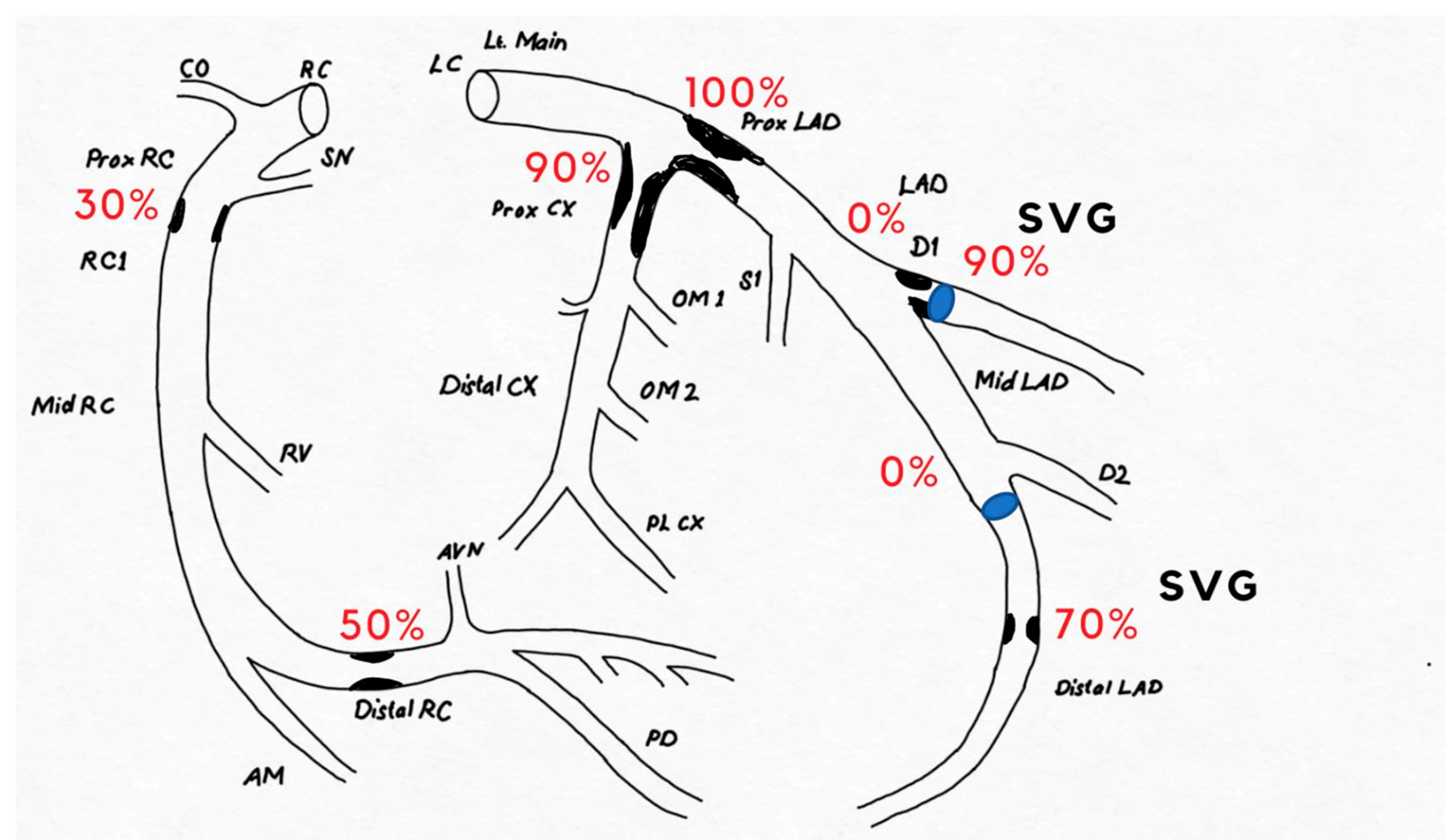
On March 14, 2024, TTE indicated normal end-diastolic volume (EDV), absence of left ventricular hypertrophy (LVH), and preserved left ventricular systolic function with an ejection fraction of 70%. However, a computed tomography angiography (CTA) conducted on March 26, 2024, revealed in-stent restenosis (ISR) with subtotal occlusion at the stent in the ostial LM extending to the proximal LCx, and heavy calcification with total occlusion at the proximal segment of LAD. There was also 90% stenosis at the SVG to diagonal branch (D1) anastomotic site and 70% stenosis at the SVG to distal LAD anastomotic site (Figure 2).
As of March 27, 2024, Mr. BH reported no symptoms, demonstrated the capability of having a morning erection, and maintained a BP of 139/83 mmHg while continuing his IV therapy regimen.
Discussion
Mr. BH, a cardiac patient, presented with complex coronary artery disease which was initially managed by coronary artery bypass grafting (CABG). Over the years, his management included medication and a novel intervention using intravenous nanobubble solution therapy, which showed variable clinical results. The initial treatment with CABG using saphenous vein grafts (SVG) to bypass occluded segments of the left anterior descending (LAD) and left circumflex (LCx) arteries was a standard and effective approach for managing significant stenosis. Post-surgery medications such as clopidogrel, aspirin, atorvastatin, and irbesartan were prescribed to manage risk factors and prevent thrombosis, which are conventional post-CABG management strategies. The effectiveness of this approach was initially positive as evidenced by normal left ventricular function and lack of symptoms up until complications arose noted on later evaluations.
The novel intravenous nanobubble treatment was introduced later in Mr. BH’s management plan due to the recurrence of symptoms and subsequent diagnostic findings suggesting in-stent restenosis and progression of graft disease. Improvement in symptoms such as reduced dyspnea, cough, and enhanced physical capacity (climbing 22 flights of stairs) post nanobubble therapy indicates a possible beneficial effect. However, the role of nanobubble therapy in directly influencing coronary artery disease progression or stenosis is unclear and not well established in current medical literature.
The hypothesised scientific rationale for how hydrogen and oxygen nanobubbles might reverse coronary stenoses involves several interconnected mechanisms, primarily focusing on the reduction of oxidative stress, modulation of endothelial function, and potential direct effects on atherosclerotic plaques. Firstly, hydrogen nanobubbles have been shown to possess significant antioxidant properties, effectively removing cytotoxic reactive oxygen species (ROS) such as •OH, ClO–, and ONOO– from water, which are known contributors to oxidative stress within the vascular system. This reduction in ROS can mitigate the oxidative damage to endothelial cells, a key factor in the progression of coronary stenosis[75]. Similarly, oxygen nanobubbles, by ensuring enhanced oxygen delivery to hypoxic tissues, could improve cellular metabolism and reduce ischemic conditions that exacerbate endothelial dysfunction and atherosclerosis[76]. Moreover, the delivery of hydrogen sulphide (H2S) via ultrasound-targeted microbubble destruction has been demonstrated to attenuate myocardial ischemia-reperfusion injury, suggesting that nanobubbles could be used as vehicles for therapeutic agents, potentially offering a novel approach to directly treat or reverse the pathological processes underlying coronary stenosis[77]. This is further supported by the observation that inhaling hydrogen gas reduces myocardial ischemic/reperfusion injury by attenuating endoplasmic reticulum stress and down-regulating autophagy, mechanisms that could also be relevant in the context of coronary stenosis[78]. The application of nanoparticles in coronary artery disease treatment, including the use of rapamycin-loaded nanoparticles, has shown promise in reducing intimal thickening and modulating the expression of factors involved in vascular remodelling, such as matrix metalloproteinases (MMPs) and tissue inhibitors of metalloproteinases (TIMPs)[79]. This suggests that nanobubbles, possibly loaded with therapeutic agents, could directly influence the cellular and molecular pathways involved in the development of coronary stenosis. In summary, the combined antioxidant effects of hydrogen nanobubbles, the potential for improved oxygen delivery with oxygen nanobubbles, and the capability of nanobubbles to serve as vehicles for therapeutic agents offer a multifaceted approach to potentially reverse coronary stenoses by reducing oxidative stress, improving endothelial function, and directly affecting the atherosclerotic process[80,81,82,83,84].
The reversal of coronary stenosis in our patient after serial intravenous hydrogen oxygen nanobubble treatment presents an intriguing case that aligns with emerging research on novel therapies for coronary heart disease (CHD). Related studies offer insights into the potential mechanisms and comparative efficacy of similar interventions. Hydrogen gas inhalation (HI) has been shown to reduce infarct size and mitigate adverse left ventricular remodelling in a rat model of acute myocardial infarction (AMI), suggesting a cardioprotective role of hydrogen in the context of coronary artery disease [85]. This is supported by the broader understanding that molecular hydrogen can exert antioxidant, anti-inflammatory, and antiapoptotic effects, leading to cardioprotective benefits [86]. These properties could potentially explain the observed reversal of coronary stenosis in our patient, as hydrogen’s ability to reduce oxidative stress and inflammation may contribute to the improvement of vascular health and the regression of atherosclerotic lesions. Comparatively, the Lifestyle Heart Trial demonstrated that intensive lifestyle changes could lead to regression of coronary atherosclerosis after 5 years, highlighting the potential for non-pharmacological interventions to reverse coronary disease [87]. This suggests a multifaceted approach to managing CHD, where both lifestyle modifications and innovative treatments like hydrogen therapy could be beneficial. Furthermore, the use of intracoronary Ad-HGF administration for treating severe diffuse coronary disease has shown long-term safety and efficacy in improving ejection fraction, indicating that gene therapy could be another avenue for reversing coronary stenosis [88]. While the direct comparison of hydrogen oxygen nanobubble treatment to these interventions is not available, the underlying principles of reducing oxidative stress, improving myocardial function, and promoting vascular health are consistent across studies. Our patient’s response to hydrogen oxygen nanobubble treatment may reflect these mechanisms at play, aligning with the broader research efforts aimed at reversing coronary stenosis through various innovative therapies [89,92].
Conclusions
While CABG and conventional pharmacotherapy initially managed Mr. BH’s cardiac condition effectively, the introduction of nanobubble therapy potentially contributed to symptom management. However, the presence of new severe stenosis and restenosis raises concerns about the long-term effectiveness of this therapy. Further evaluation through controlled studies is necessary to understand the role and mechanism of nanobubble therapy in cardiac disease, especially in patients with complex histories like Mr. BH. Continued monitoring and possibly additional revascularization procedures may be necessary given the recent findings of stent and graft stenosis.
References
- Masuda, D.; Yamashita, S. Enhanced Intestinal Absorption of Cholesterol along with Increased Chylomicron Remnants for De novo Progression of Coronary Stenosis. J. Atheroscler. Thromb. 2017, 24, 120–122. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Wang, Z.; Qin, M.; Zhang, B.; Lin, L.; Ma, Q.; Liu, C.; Chen, X.; Li, H.; Lai, W.; et al. Comprehensive Metabolomics Identified the Prominent Role of Glycerophospholipid Metabolism in Coronary Artery Disease Progression. Front. Mol. Biosci. 2021, 8, 632950. [Google Scholar] [CrossRef] [PubMed]
- Thai, P.V.; Tien, H.A.; Van Minh, H.; Valensi, P. Triglyceride glucose index for the detection of asymptomatic coronary artery stenosis in patients with type 2 diabetes. Cardiovasc. Diabetol. 2020, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Graby, J.; Sellek, J.; Khavandi, A.; Loughborough, W.; Hudson, B.J.; Shirodaria, C.; Downie, P.; Antoniades, C.; Rodrigues, J.C.L. Coronary CT angiography derived pericoronary inflammation and bespoke cardiovascular risk prediction in the lipid clinic: beyond the calcium score. Eur. Hear. J. 2022, 43. [Google Scholar] [CrossRef]
- Chaichuum, S.; Chiang, S.-J.; Daimon, M.; Chang, S.-C.; Chan, C.-L.; Hsu, C.-Y.; Chen, H.-H.; Tseng, C.-L. Segmental Tissue Speckle Tracking Predicts the Stenosis Severity in Patients With Coronary Artery Disease. Front. Cardiovasc. Med. 2022, 8, 832096. [Google Scholar] [CrossRef] [PubMed]
- Cubero-Gallego, H.; Tizón-Marcos, H.; Vaquerizo, B.; Valero, I.M.C.; Pinel, a.A.C.; Borrego, J.C.; Blanco, B.J.M.S.; Martína, R.G.D.M. Current options for the management of calcified lesions. REC: Interv. Cardiol. (English Ed. 2020; 2, 129–139. [Google Scholar] [CrossRef]
- Bershtein, L.L.; Zbyshevskaya, E.V.; Gumerova, V.E. Optimum Treatment Strategy in Chronic Coronary Syndromes: the New Trials vs the Current Guidelines. Ration. Pharmacother. Cardiol. 2021, 17, 761–770. [Google Scholar] [CrossRef]
- Laricchia, A.; Colombo, A. New interventional solutions in calcific coronary atherosclerosis: drill, laser, shock waves. Eur. Hear. J. Suppl. 2020, 22, L49–L52. [Google Scholar] [CrossRef]
- Iannaccone, G.; Scarparo, P.; Wilschut, J.; Daemen, J.; Dekker, W.D.; De Jaegere, P.; Zijlstra, F.; Van Mieghem, N.M.; Diletti, R. Current approaches for treatment of coronary chronic occlusions. Expert Rev. Med Devices 2019, 16, 941–954. [Google Scholar] [CrossRef] [PubMed]
- Doenst, T.; Thiele, H.; Haasenritter, J.; Wahlers, T.; Massberg, S.; Haverich, A. The Treatment of Coronary Artery Disease Current Status Six Decades After the First Bypass Operation. Dtsch. Aerzteblatt Online 2022, 119, 716–723. [Google Scholar] [CrossRef]
- Predescu, L.M.; Zarma, L.; Platon, P.; Postu, M.; Bucsa, A.; Croitoru, M.; Deleanu, D.E.; Ginghina, C. Current treatment of left main coronary artery disease. Cor et Vasa 2016, 58, e328–e339. [Google Scholar] [CrossRef]
- Bertolone, D.T.; Gallinoro, E.; Esposito, G.; Paolisso, P.; Bermpeis, K.; De Colle, C.; Fabbricatore, D.; Mileva, N.; Valeriano, C.; Munhoz, D.; et al. Contemporary Management of Stable Coronary Artery Disease. High Blood Press. Cardiovasc. Prev. 2022, 29, 207–219. [Google Scholar] [CrossRef] [PubMed]
- Tekin, G. , & Tekin, A. (2015). Current Medical Treatment of Stable Coronary Artery Disease. Arşiv Kaynak Tarama Dergisi, 24(4), 592-613.
- Desch, S.; Schuler, G.; Niebauer, J. [Conservative treatment of coronary heart disease--current options]. . 2005, 147, 45–7. [Google Scholar] [PubMed]
- Zwart, B.; Parker, W.A.E.; Storey, R.F. New Antithrombotic Drugs in Acute Coronary Syndrome. J. Clin. Med. 2020, 9, 2059. [Google Scholar] [CrossRef] [PubMed]
- Correale, M.; Tricarico, L.; Iacoviello, M.; Brunetti, N.D. SGLT2 Inhibitors: Statins or ACE-Inhibitors of the 21st Century? J. Clin. Med. 2023, 12, 2695. [Google Scholar] [CrossRef] [PubMed]
- Strauss, M.H.; Hall, A.S.; Narkiewicz, K. The Combination of Beta-Blockers and ACE Inhibitors Across the Spectrum of Cardiovascular Diseases. Cardiovasc. Drugs Ther. 2023, 37, 757–770. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.-Z.; Cao, L.-H.; Liu, H. ACE inhibitors in cardiac surgery: current studies and controversies. Hypertens. Res. 2011, 34, 15–22. [Google Scholar] [CrossRef]
- Ndrepepa, G.; Braun, S.; Schömig, A.; Kastrati, A. Impact of therapy with statins, beta-blockers and angiotensin-converting enzyme inhibitors on plasma myeloperoxidase in patients with coronary artery disease. Clin. Res. Cardiol. 2011, 100, 327–333. [Google Scholar] [CrossRef]
- Smith, S.M.; Lee, J.; Lee, S. ARB Superiority Over ACE Inhibitors in Coronary Heart Disease: An Alternative Viewpoint. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2019, 39, 204–206. [Google Scholar] [CrossRef]
- Shin, E.-S. Current Status of Coronary Stent. Korean J. Med. 2015, 89, 282–290. [Google Scholar] [CrossRef]
- Choi, B. R. , & Hong, M. K. ( 2006). Medical Treatment of Coronary Artery Disease. Hanyang Medical Reviews, 39–51.
- Sim, H.W.; Zheng, H.; Richards, A.M.; Chen, R.W.; Sahlen, A.; Yeo, K.-K.; Tan, J.W.; Chua, T.; Tan, H.C.; Yeo, T.C.; et al. Beta-blockers and renin-angiotensin system inhibitors in acute myocardial infarction managed with inhospital coronary revascularization. Sci. Rep. 2020, 10, 15184. [Google Scholar] [CrossRef] [PubMed]
- Ullrich, H.; Olschewski, M.; Münzel, T.; Gori, T. Coronary In-Stent Restenosis: Predictors and Treatment. Dtsch. Aerzteblatt Online 2021, 118, 637. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.-C.; Park, D.-W.; Park, S.-J. Percutaneous Coronary Intervention and Coronary Artery Bypass Grafting for the Treatment of Left Main Coronary Artery Disease. Korean Circ. J. 2019, 49, 369–383. [Google Scholar] [CrossRef] [PubMed]
- Towashiraporn, K.; Krittayaphong, R. Current Perspectives on Antithrombotic Therapy for the Treatment of Acute Coronary Syndrome. Int. J. Gen. Med. 2022, 15, 2397–2414. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Klusewitz, S.; Elefteriades, J.; Prescher, L. The Current State of Coronary Revascularization: Percutaneous Coronary Intervention versus Coronary Artery Bypass Graft Surgery. Int. J. Angiol. 2021, 30, 228–241. [Google Scholar] [CrossRef]
- Pushparaji, B. , Donisan, T. ( 25(6), 143–158. [PubMed]
- Garg, D. Regenerative Medicine and its Potential in Cardiovascular Disease. J. Stud. Res. 2022, 11. [Google Scholar] [CrossRef]
- Arjmand, B.; Abedi, M.; Arabi, M.; Alavi-Moghadam, S.; Rezaei-Tavirani, M.; Hadavandkhani, M.; Tayanloo-Beik, A.; Kordi, R.; Roudsari, P.P.; Larijani, B. Regenerative Medicine for the Treatment of Ischemic Heart Disease; Status and Future Perspectives. Front. Cell Dev. Biol. 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Litwinowicz, R. , Kapelak, B., Sadowski, J., Kędziora, A., & Bartus, K. (2018). The use of stem cells in ischemic heart disease treatment. Kardiochirurgia i Torakochirurgia Polska/Polish Journal of Thoracic and Cardiovascular Surgery, 15(3), 196-199.
- Amrutha, M.; Monaza, A.; Rithika, P.; Surya, S.; Kochoradze-Margishvili, T. Use of Stem Cells In Regenerative Cardiovascular Medicine (Review Article). Exp. Clin. Med. Ga. 2022. [Google Scholar] [CrossRef]
- Duran, A.G.; Reidell, O.; Stachelscheid, H.; Klose, K.; Gossen, M.; Falk, V.; Röll, W.; Stamm, C. Regenerative Medicine/Cardiac Cell Therapy: Pluripotent Stem Cells. Thorac. Cardiovasc. Surg. 2018, 66, 053–062. [Google Scholar] [CrossRef]
- Masumoto, H.; Sakata, R. Cardiovascular surgery for realization of regenerative medicine. Gen. Thorac. Cardiovasc. Surg. 2012, 60, 744–755. [Google Scholar] [CrossRef] [PubMed]
- Behjati, M. Suggested indications of clinical practice guideline for stem cell-therapy in cardiovascular diseases: A stepwise appropriate use criteria for regeneration therapy. 2013, 9, 306–310.
- Nazari-Shafti, T.Z.; Kempfert, J.; Falk, V.; Röll, W.; Stamm, C. Regenerative Medicine/Cardiac Cell Therapy: Adult/Somatic Progenitor Cells. Thorac. Cardiovasc. Surg. 2018, 66, 042–052. [Google Scholar] [CrossRef] [PubMed]
- Bolli, R.; Hare, J. Introduction to a Compendium on Regenerative Cardiology. Circ. Res. 2018, 123, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Kandaswamy, E.; Zuo, L. Recent Advances in Treatment of Coronary Artery Disease: Role of Science and Technology. Int. J. Mol. Sci. 2018, 19, 424. [Google Scholar] [CrossRef] [PubMed]
- Aleksandric, S.; Banovic, M.; Beleslin, B. Challenges in Diagnosis and Functional Assessment of Coronary Artery Disease in Patients With Severe Aortic Stenosis. Front. Cardiovasc. Med. 2022, 9, 849032. [Google Scholar] [CrossRef] [PubMed]
- Hennessey, B.; Pareek, N.; Macaya, F.; Yeoh, J.; Shlofmitz, E.; Gonzalo, N.; Hill, J.; Escaned, J. Contemporary percutaneous management of coronary calcification: current status and future directions. Open Hear. 2023, 10, e002182. [Google Scholar] [CrossRef]
- Alghrairi, M.; Sulaiman, N.; Mutashar, S. Health Care Monitoring and Treatment for Coronary Artery Diseases: Challenges and Issues. Sensors 2020, 20, 4303. [Google Scholar] [CrossRef]
- Mekala, K.; Mehta, R.H.; Joumaa, M.; Yamasaki, H. Treatment of heavily calcified coronary artery stenosis using 3.5 mm peripheral intravascular lithotripsy balloon: case series. Eur. Hear. J. - Case Rep. 2020, 4, 1–5. [Google Scholar] [CrossRef]
- Suganuma, E.; Sato, S.; Honda, S.; Nakazawa, A. All trans retinoic acid alleviates coronary stenosis by regulating smooth muscle cell function in a mouse model of Kawasaki disease. Sci. Rep. 2021, 11, 1–11. [Google Scholar] [CrossRef]
- Hamm, C.W.; Dörr, O.; Woehrle, J.; Krackhardt, F.; Ince, H.; Zeus, T.; Berland, J.; Piot, C.; Roubille, F.; Schult, I.; et al. A multicentre, randomised controlled clinical study of drug-coated balloons for the treatment of coronary in-stent restenosis. EuroIntervention 2020, 16, e328–e334. [Google Scholar] [CrossRef]
- Yong, J.; Tian, J.; Yang, X.; Xing, H.; He, Y.; Song, X. Effects of Oral Drugs on Coronary Microvascular Function in Patients Without Significant Stenosis of Epicardial Coronary Arteries: A Systematic Review and Meta-Analysis of Coronary Flow Reserve. Front. Cardiovasc. Med. 2020, 7, 580419. [Google Scholar] [CrossRef] [PubMed]
- Afshari, R.; Akhavan, O.; Hamblin, M.R.; Varma, R.S. Review of Oxygenation with Nanobubbles: Possible Treatment for Hypoxic COVID-19 Patients. ACS Appl. Nano Mater. 2021, 4, 11386–11412. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L. , & Miwa, N. (2021). Hydrogen nano-bubble water suppresses ROS generation, adipogenesis, and interleukin-6 secretion in hydrogen-peroxide-or PMA-stimulated adipocytes and three-dimensional subcutaneous adipose equivalents. Cells, 10(3), 626.
- Kurokawa, H., Matsui, H., Ito, H., Taninaka, A., Shigekawa, H., Dodbiba, G., ... & Fujita, T. (2019). Antioxidant effect of hydrogen nanobubble contributes to suppression of tumor cell growth. Biomed. J. Sci. Tech. Res, 19, 14592-14594.
- Si, Y.; Tian, H.; Dong, B.; Zhang, Y.; Wen, Y.; Jia, X.; Li, Y.; Zhang, A.; Qin, S. Effects of hydrogen as adjuvant treatment for unstable angina. Exp. Biol. Med. 2021, 246, 1981–1989. [Google Scholar] [CrossRef] [PubMed]
- DU, Z.; Jia, H.; Liu, J.; Zhao, X.; Wang, Y.; Sun, X. Protective effects of hydrogen-rich saline in uncontrolled hemorrhagic shock. Exp. Ther. Med. 2014, 7, 1253–1258. [Google Scholar] [CrossRef]
- Yang, M. , Zhang, Z., Gao, B., Liu, L., & Hu, T. (2017). Hydrogen medicine therapy: an effective and promising novel treatment for multiple organ dysfunction syndrome (MODS) induced by influenza and other viral infections diseases. SOJ Microbiol Infect Dis, 5, 1-6.
- LeBaron, T.W.; Kura, B.; Kalocayova, B.; Tribulova, N.; Slezak, J. A New Approach for the Prevention and Treatment of Cardiovascular Disorders. Molecular Hydrogen Significantly Reduces the Effects of Oxidative Stress. Molecules 2019, 24, 2076. [Google Scholar] [CrossRef]
- Yang, W. C. , Zhang, Y. R., Yu, J. X., Yang, Y., Liu, X. N., Zhang, X.,... & Wang, Q. S. (2022). Hydrogen-oxygen therapy improves postoperative pulmonary functions and accelerates recovery through attenuating inflammatory reactions and oxidative stress in patients undergoing lung surgery.
- Zhang, J.H.; Matei, N.; Camara, R. Emerging mechanisms and novel applications of hydrogen gas therapy. Med Gas Res. 2018, 8, 98–102. [Google Scholar] [CrossRef]
- Rahman, M.H.; Bajgai, J.; Fadriquela, A.; Sharma, S.; Trinh Thi, T.; Akter, R.; Goh, S.H.; Kim, C.-S.; Lee, K.-J. Redox Effects of Molecular Hydrogen and Its Therapeutic Efficacy in the Treatment of Neurodegenerative Diseases. Processes 2021, 9, 308. [Google Scholar] [CrossRef]
- Nghia, N.H.; Nguyen, N.T.; Binh, P.T.; May, L.T.; Huy, T.T.; Giang, P.T.; St-Hilaire, S.; Van, P.T. Effect of nanobubbles (oxygen, ozone) on the Pacific white shrimp (Penaeus vannamei), Vibrio parahaemolyticus and water quality under lab conditions. Fish. Aquat. Sci. 2022, 25, 429–440. [Google Scholar] [CrossRef]
- Bluemke, E.; Young, L.A.J.; Owen, J.; Smart, S.; Kinchesh, P.; Bulte, D.P.; Stride, E. Determination of oxygen relaxivity in oxygen nanobubbles at 3 and 7 Tesla. Magn. Reson. Mater. Physics, Biol. Med. 2022, 35, 817–826. [Google Scholar] [CrossRef]
- Messerschmidt, V.; Ren, W.; Tsipursky, M.; Irudayaraj, J. Characterization of Oxygen Nanobubbles and In Vitro Evaluation of Retinal Cells in Hypoxia. Transl. Vis. Sci. Technol. 2023, 12, 16–16. [Google Scholar] [CrossRef]
- Verinda, S. B. , Yulianto, E., Gunawan, G., & Nur, M. (2021). Ozonated nanobubbles-a potential hospital waste water treatment during the COVID-19 outbreak in Indonesia to eradicate the persistent SARS-CoV-2 in HWWs. Ann. Trop. Med. Public Health, 24, 24-197.
- Matsuki, N.; Ishikawa, T.; Ichiba, S.; Shiba, N.; Ujike, Y.; Yamaguchi, T. Oxygen supersaturated fluid using fine micro/nanobubbles. Int. J. Nanomed. 2014, 9, 4495–4505. [Google Scholar] [CrossRef]
- Bhandari, P.; Novikova, G.; Goergen, C.J.; Irudayaraj, J. Ultrasound beam steering of oxygen nanobubbles for enhanced bladder cancer therapy. Sci. Rep. 2018, 8, 1–10. [Google Scholar] [CrossRef]
- Bhandari, P.N.; Cui, Y.; Elzey, B.D.; Goergen, C.J.; Long, C.M.; Irudayaraj, J. Oxygen nanobubbles revert hypoxia by methylation programming. Sci. Rep. 2017, 7, 1–14. [Google Scholar] [CrossRef]
- Nghia, N. H., Van, P. T., Giang, P. T., Hanh, N. T., St-Hilaire, S., & Domingos, J. A. (2021). Control of Vibrio parahaemolyticus (AHPND strain) and improvement of water quality using nanobubble technology. Aquaculture Research, 52(6), 2727-2739.
- Khan, M.S.; Hwang, J.; Seo, Y.; Shin, K.; Lee, K.; Park, C.; Choi, Y.; Hong, J.W.; Choi, J. Engineering oxygen nanobubbles for the effective reversal of hypoxia. Artif. Cells Nanomed. Biotechnol. 2018, 46 (Suppl. 3), S318–S327. [Google Scholar] [CrossRef] [PubMed]
- Cavalli, R.; Marano, F.; Argenziano, M.; Varese, A.; Frairia, R.; Catalano, M.G. Combining Drug-Loaded Nanobubbles and Extracorporeal Shock Waves for Difficult-to-Treat Cancers. Curr. Drug Deliv. 2017, 15, 752–754. [Google Scholar] [CrossRef]
- Senthilkumar, G.; Kumar, J.A. Nanobubbles: a promising efficient tool for therapeutic delivery of antibacterial agents for the Staphylococcus aureus infections. Appl. Nanosci. 2023, 13, 6177–6190. [Google Scholar] [CrossRef]
- Li, T. , Zhou, J., Zhang, C., Zhi, X., Niu, J., Fu, H.,... & Cui, D. (2018). Surface-engineered nanobubbles with pH-/light-responsive drug release and charge-switchable behaviors for active NIR/MR/US imaging-guided tumor therapy. NPG Asia Materials, 10(11), 1046-1060.
- Tiwari, S.P. Nanobubbles as theranostic platforms for tumour-specific imaging and therapy. Int. J. Heal. Sci. 2022, 10944–10954. [Google Scholar] [CrossRef]
- Pellow, C.; Abenojar, E.C.; Exner, A.A.; Zheng, G.; Goertz, D.E. Concurrent visual and acoustic tracking of passive and active delivery of nanobubbles to tumors. Theranostics 2020, 10, 11690–11706. [Google Scholar] [CrossRef]
- Liu, C. F. , Zhou, J., Chen, X. R., & Yu, J. (2018). Drug-loaded nanobubbles for ultrasound-mediated antitumor treatment. Journal of Biological Regulators and Homeostatic Agents, 32(4), 923-929.
- Pal, P.; Joshi, A.; Anantharaman, H. Nanobubble ozonation for waterbody rejuvenation at different locations in India: A holistic and sustainable approach. Results Eng. 2022, 16. [Google Scholar] [CrossRef]
- Peng, Y.; Zhu, L.; Wang, L.; Liu, Y.; Fang, K.; Lan, M.; Shen, D.; Liu, D.; Yu, Z.; Guo, Y. Preparation Of Nanobubbles Modified With A Small-Molecule CXCR4 Antagonist For Targeted Drug Delivery To Tumors And Enhanced Ultrasound Molecular Imaging. Int. J. Nanomed. 2019, ume 14, 9139–9157. [Google Scholar] [CrossRef]
- Lu, S.; Zhao, P.; Deng, Y.; Liu, Y. Mechanistic Insights and Therapeutic Delivery through Micro/Nanobubble-Assisted Ultrasound. Pharmaceutics 2022, 14, 480. [Google Scholar] [CrossRef]
- Lan, M.; Zhu, L.; Wang, Y.; Shen, D.; Fang, K.; Liu, Y.; Peng, Y.; Qiao, B.; Guo, Y. Multifunctional nanobubbles carrying indocyanine green and paclitaxel for molecular imaging and the treatment of prostate cancer. J. Nanobiotechnology 2020, 18, 1–18. [Google Scholar] [CrossRef]
- Rigatelli, G.; Zuin, M.; Bilato, C.; Nguyen, T. Coronary artery cavitation as a trigger for atherosclerotic plaque progression: a simplified numerical and computational fluid dynamic demonstration. Rev. Cardiovasc. Med. 2022, 23, 58. [Google Scholar] [CrossRef]
- McDowell, G.; Slevin, M.; Krupinski, J. Nanotechnology for the treatment of coronary in stent restenosis: a clinical perspective. Vasc. Cell 2011, 3, 8–8. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Yang, L.; Zhong, L.; Kutty, S.; Wang, Y.; Cui, K.; Xiu, J.; Cao, S.; Huang, Q.; Liao, W.; et al. Delivery of Hydrogen Sulfide by Ultrasound Targeted Microbubble Destruction Attenuates Myocardial Ischemia-reperfusion Injury. Sci. Rep. 2016, 6, 30643. [Google Scholar] [CrossRef]
- Fetuga, I.A.; Olakoyejo, O.O.; Oluwatusin, O.; Adelaja, A.O.; Gbegudu, J.K.; Aderemi, K.S.; Adeyemi, E.A. Computational model of nano-pharmacological particles for the clinical management of stenotic and aneurysmatic coronary artery in the human body. Niger. J. Technol. Dev. 2023, 20, 79–90. [Google Scholar] [CrossRef]
- Liu, S.; Oshita, S.; Thuyet, D.Q.; Saito, M.; Yoshimoto, T. Antioxidant Activity of Hydrogen Nanobubbles in Water with Different Reactive Oxygen Species both in Vivo and in Vitro. Langmuir 2018, 34, 11878–11885. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Yang, H.; Chi, J.; Xu, Q.; Zhao, L.; Yang, W.; Liu, W.; Yang, W. Hydrogen Gas Attenuates Myocardial Ischemia Reperfusion Injury Independent of Postconditioning in Rats by Attenuating Endoplasmic Reticulum Stress-Induced Autophagy. Cell. Physiol. Biochem. 2017, 43, 1503–1514. [Google Scholar] [CrossRef]
- Zhang, Y.; Fan, W.; Li, X.; Wang, W.-X.; Liu, S. Enhanced Removal of Free Radicals by Aqueous Hydrogen Nanobubbles and Their Role in Oxidative Stress. Environ. Sci. Technol. 2022, 56, 15096–15107. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y. Advances and applications of Nanotechnology to solve Coronary Heart Disease. Highlights Sci. Eng. Technol. 2023, 36, 517–521. [Google Scholar] [CrossRef]
- Katsumata, Y.; Sano, F.; Abe, T.; Tamura, T.; Fujisawa, T.; Shiraishi, Y.; Kohsaka, S.; Ueda, I.; Homma, K.; Suzuki, M.; et al. The Effects of Hydrogen Gas Inhalation on Adverse Left Ventricular Remodeling After Percutaneous Coronary Intervention for ST-Elevated Myocardial Infarction ― First Pilot Study in Humans ―. Circ. J. 2017, 81, 940–947. [Google Scholar] [CrossRef] [PubMed]
- Miao, L.F.; Yin, Y.P.; Cui, Y.L.; Chen, L.F.; Zeng, Y.; Huang, C.L.; Zhu, W.L.; Song, C.X.; Zhang, H.; She, M.P.; et al. [Efficacy and mechanism of local delivery of rapamycin and rapamycin-loaded poly(lactic-co-glycolic) acid nanoparticles on coronary restenosis of injury-stenosis model of minipigs]. . 2016, 96, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Ilic, I.; Timcic, S.; Odanovic, N.; Otasevic, P.; Collet, C. Serial stenosis assessment—can we rely on invasive coronary physiology. Front. Cardiovasc. Med. 2023, 10, 1172906. [Google Scholar] [CrossRef] [PubMed]
- Katsumata, Y.; Sano, F.; Abe, T.; Tamura, T.; Fujisawa, T.; Shiraishi, Y.; Kohsaka, S.; Ueda, I.; Homma, K.; Suzuki, M.; et al. The Effects of Hydrogen Gas Inhalation on Adverse Left Ventricular Remodeling After Percutaneous Coronary Intervention for ST-Elevated Myocardial Infarction ― First Pilot Study in Humans ―. Circ. J. 2017, 81, 940–947. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Guo, Z.; Jia, G.; Ma, R.; Li, M. Influencing factors of coronary artery stenosis in patients with stable coronary heart disease and a correlation analysis. 2021, 13, 9522–9529.
- Tang, Y. Advances and applications of Nanotechnology to solve Coronary Heart Disease. Highlights Sci. Eng. Technol. 2023, 36, 517–521. [Google Scholar] [CrossRef]
- Li, S.; Yuan, Y.; Zhao, L.; Lv, T.; She, F.; Liu, F.; Xue, Y.; Zhou, B.; Xie, Y.; Geng, Y.; et al. Coronary stenosis is a risk marker for impaired cardiac function on cardiopulmonary exercise test. BMC Cardiovasc. Disord. 2022, 22, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Meng, H.; Du, Y.; Chen, B.; Toorabally, M.B.; Wang, Z.M.; Zhou, N.; Xu, Z.; Zhang, D.; Tao, Z.; Wang, L.; et al. Safety and Efficacy of Intracoronary Ad-HGF Administration for Treating Severe Coronary Disease: Results From Long-Term Follow-Up of a Phase I Clinical Trial. J. Clin. Trials 2017, 7. [Google Scholar] [CrossRef]
- Page, B.J.; Young, R.F.; Suzuki, G.; Fallavollita, J.A.; Canty, J.M. The physiological significance of a coronary stenosis differentially affects contractility and mitochondrial function in viable chronically dysfunctional myocardium. Basic Res. Cardiol. 2013, 108, 354. [Google Scholar] [CrossRef]
- Ornish, D.; Scherwitz, L.W.; Billings, J.H.; Gould, K.L.; Merritt, T.A.; Sparler, S.; Armstrong, W.T.; Ports, T.A.; Kirkeeide, R.L.; Hogeboom, C.; et al. Intensive Lifestyle Changes for Reversal of Coronary Heart Disease. JAMA 1998, 280, 2001–2007. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Precatheterization schematic illustrating the baseline anatomical structure and condition of the cardiovascular system prior to any surgical interventions.
Figure 1.
Precatheterization schematic illustrating the baseline anatomical structure and condition of the cardiovascular system prior to any surgical interventions.
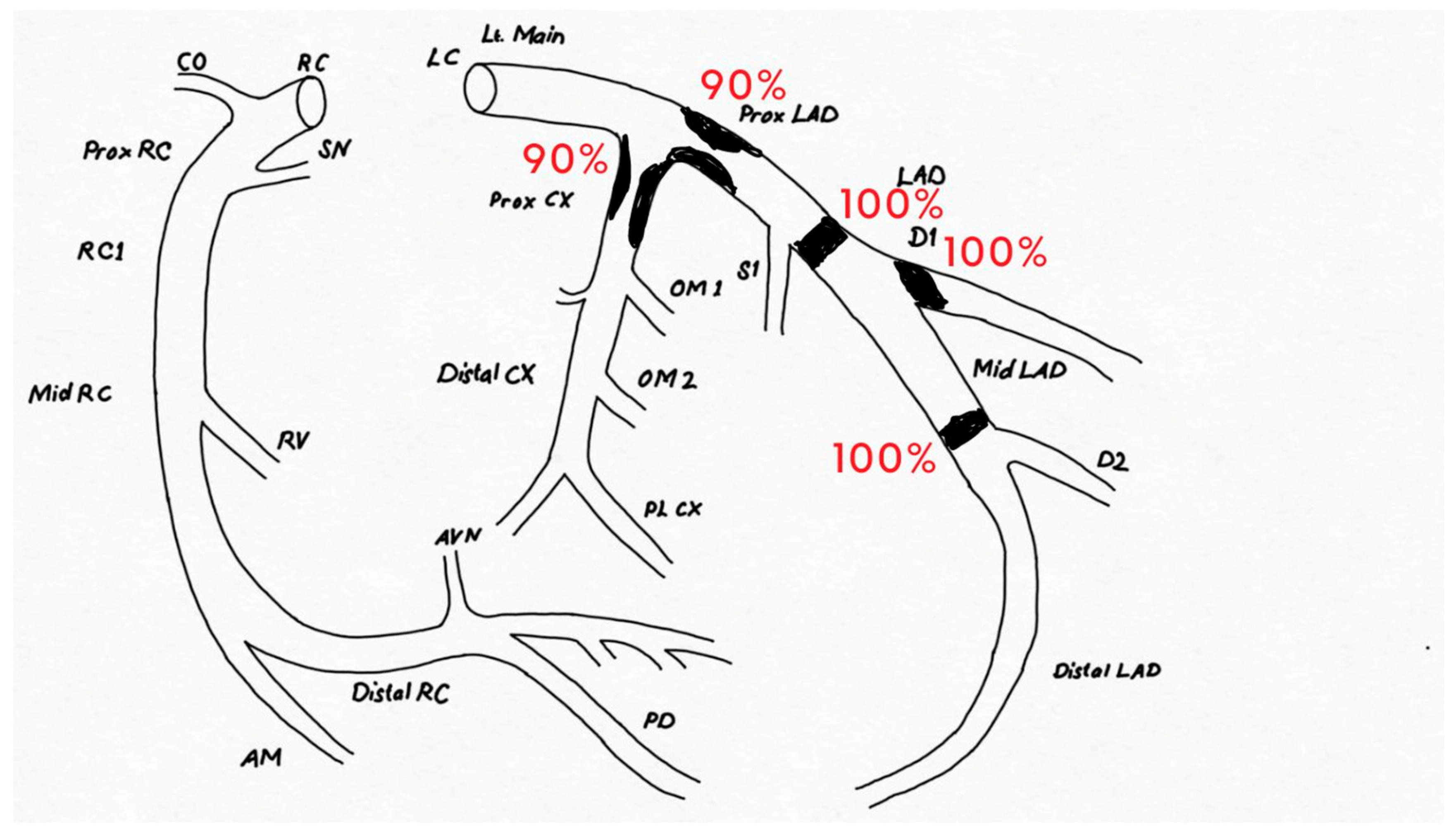
Figure 2.
Postcatheterization, post-CABG (Coronary Artery Bypass Grafting), and post-PCI (Percutaneous Coronary Intervention) schematic. The blue area highlights the anastomotic site from the aorta using a saphenous vein graft (SVG). Red numbers indicate the new state of stenosis, showing the changes in vessel narrowing following the procedures.
Figure 2.
Postcatheterization, post-CABG (Coronary Artery Bypass Grafting), and post-PCI (Percutaneous Coronary Intervention) schematic. The blue area highlights the anastomotic site from the aorta using a saphenous vein graft (SVG). Red numbers indicate the new state of stenosis, showing the changes in vessel narrowing following the procedures.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



