
Submitted:
16 June 2024
Posted:
21 June 2024
You are already at the latest version
Abstract
Viral hepatitis is currently acknowledged as a significant public health issue that necessitates a prompt and immediate response. Hepatitis is a significant worldwide health problem that causes the death of approximately 1.5 million individuals annually. The objective of this study was to ascertain the occurrence rate of hepatitis A, E, B, and C infections in the Hajjah governorate of Yemen from 2020 to 2023.A retrospective study was conducted in the Hajjah Governorate of Yemen for four years, 2020– 2023. About 41162 cases were collected from the clinical records of epidemiological surveillance in the Public Health Office of the Hajjah Governorate. All cases were diagnosed in different laboratories based on direct observation of viral hepatitis in the blood sample. The required data were obtained by using the designed questionnaire. The findings of the present investigation were summarized as follows: The current findings indicate that the prevalence rate of Hepatitis A and E was 761 (1.85%), while the prevalence rate of Hepatitis B and C was 971 (2.36%) among the participants of the study. The current findings indicate that the incidence of Hepatitis A and E was greater in 2022 (2.3%), while Hepatitis B and C had a higher rate in 2020 (2.9%). The study revealed a higher prevalence of hepatitis A and E among individuals originating from Al Miftah district 116, with a rate of 7.5%. Furthermore, the prevalence of hepatitis B and C in Hajjah city was significantly higher, reaching 579 cases (22.9%). The month with the highest incidence of hepatitis A and E viruses was September, with a rate of 85 cases (2.6%), while the lowest incidence was observed in April, with a rate of 1.3%. The prevalence of hepatitis B and C viruses was highest in October 1997, with a rate of 2.8%, followed by November 1997 with the same rate. The lowest observed incidence of 1.6% was recorded in April. In Autumn, a significant prevalence of hepatitis A and B viruses, as well as hepatitis B and C viruses, was identified at rates of 2.2% and 2.6%, respectively.The study findings indicate that the occurrence of HAV, HEV, HBV, and HCV in the study area is consistent with global trends. Although the study found a low prevalence of hepatitis viruses, these types of viruses will continue to pose a significant risk to public health. Based on this study, it is imperative for authorities to actively enhance public awareness in order to enable prompt planning and essential arrangements for an effective response to outbreaks or epidemics. This will ultimately lead to a reduction in illness, death, and economic burden.
Keywords:
Hepatitis A
; Hepatitis B
; Hepatitis C
; Hepatitis E
; Epidemiology
; Hajjah
; Yemen
Introduction
1.1.1. Hepatitis B virus
1.1.1.1. Classification
The hepatitis B virus belongs to the Orthohepadnavirus genus, along with eleven other species. The Hepadnaviridae family, which also includes the four other genera Avihepadnavirus, Herpetohepadnavirus, Metahepadnavirus, and Parahepadnavirus, is where the genus is categorized. The sole member of the viral order Blubervirales is this family of viruses. All apes, including chimpanzees, gorillas, orangutans, and Old World monkeys, have been reported to carry viruses resembling hepatitis B (Dupinay et al., 2017). ... in woolly monkeys found in the New World (the woolly monkey hepatitis B virus), pointing to the virus’s prehistoric primate origin. There are ten subgenotypes of genotype D (Hundie et al., 2017).
1.1.1.2. Morphology
A. Structure
The hepadnavirus family includes the hepatitis B virus. The viral particle, also known as a virion or Dane particle (WHO, 2015), is made up of an icosahedral nucleocapsid core made of protein and an outer lipid envelope. The viral DNA and a DNA polymerase with reverse transcriptase activity akin to that of retroviruses are enclosed in a nucleocapsid (Locarnini, 2004).
B. Components
It consists of:
- HBsAg, or hepatitis B surface antigen was the first known hepatitis B virus protein (Jaroszewicz et al., 2010).
- HBcAg (Hepatitis B core antigen) The primary structural protein of the HBV icosahedral nucleocapsid and is involved in the virus’s reproduction (Lin et al., 2012).
- HBeAg (Hepatitis B envelope antigen) is secreted and builds up in serum. The same reading frame is used to create both HBcAg and HBeAg (TSRI, 2009).
- HBx is tiny. is nonstructural, 154 amino acids long, and plays a significant part in HBV replication in HepG2 cells as well as liver illness linked to HBV (Tang et al. 2006).
C.Size
Although the circular DNA that makes up the HBV genome is uncommon, it is not completely double-stranded. The viral DNA polymerase is connected to one end of the whole strand. According to Kay and Zoulim (2007), the genome has a length of 3020–3320 nucleotides for the full length strand and 1700–2800 nucleotides for the short length strand.
1.1.1.3. Epidemiology
As of 2017, at least 391 million individuals, or 5% of the global population, were chronically infected with HBV. However, same year there were an additional 145 million instances of acute HBV infection (GBD, 2017). According to WHO (2020), regional prevalences vary from approximately 6% in Africa to 0.7% in the Americas.
The disease primarily spreads among youngsters in regions with moderate frequency, such as Eastern Europe, Russia, and Japan, where 2–7% of the population has a chronic infection. Transmission during birthing is more likely in high-prevalence areas like China and South East Asia, but it can also occur during childhood in other high-endemicity areas like Africa (Alter, 2003).
According to Komas et al. (2013), the prevalence of chronic HBV infection is at least 8% in high endemicity areas and between 10% and 15% in Africa and the Far East. China has 120 million infected persons as of 2010, followed by 40 million in India and 12 million in Indonesia. The World Health Organization (WHO) estimates that the virus claims the lives of 600,000 people annually. About 19,000 new cases were reported in the US in 2011, a nearly 90% decrease from 1990 (Schillie et al., 2013).
1.1.1.4. Transmission
Hepatitis B virus transmission occurs when an individual comes into contact with infected blood or bodily fluids that contain blood. Comparatively speaking, it is 50–100 times more contagious than the HIV virus (CDC, 2015). Sexual interaction is one way that information can spread (Fairley and Read, 2012). Reusing contaminated needles and syringes, transfusions of blood, transfusions with other human blood products, and vertical transmission from mother to child after childbirth (Buddeberg et al., 2008).
A mother who tests positive for HBsAg at birth has a 20% chance of infecting her child if treatment is not received. In the event that the mother also tests positive for HBeAg, this risk might reach 90%. Within households, family members may contract HBV from one another by coming into touch with saliva or secretions that contain the virus on non-intact skin or mucous membranes (IDEAS, 2009).
1.1.1.5. Diseases
Hepatitis B virus (HBV) continues to be a global health concern even with a vaccine to prevent it. The hepatitis B virus (HBV) is the infectious agent that causes hepatitis B, a liver-damaging illness (WHO, 2014). Acute hepatitis B can develop into chronic hepatitis B, which can cause many illnesses and ailments (Hu et al., 2019).
1.1.1.6. Signs and symptoms
Acute viral hepatitis, which starts with generalized malaise, lack of appetite, nausea, vomiting, body aches, low fever, and dark urine and develops into jaundice, is linked to acute hepatitis B virus infection. For those affected, the disease lasts a few weeks before progressively getting better (Terrault et al., 2005).
Hepatitis B virus infection can be chronic and asymptomatic, or it can be linked to a persistent liver inflammation that progresses over years to cirrhosis. An infection of this kind significantly raises the risk of hepatocellular carcinoma (HCC; liver cancer). About half of hepatocellular carcinoma cases in Europe are related to hepatitis B and C (El-Serag, 2011).
1.1.1.7. Diagnosis
Hepatitis B virus antigens and antibodies that can be found in an individual’s blood after an acute infection or in an individual who has been infected for a long time. Assays, or tests for the identification of hepatitis B virus infection, are blood or serum tests that look for antibodies made by the host or viral antigens. These assays have complicated interpretations (Bonino et al., 1987).
The most common test for this illness is the hepatitis B surface antigen (HBsAg). It is the initial detectable antigen produced by the virus following infection. But this antigen might not be present in the early stages of an infection, and it might not be noticeable in the latter stages when the host is eliminating it. The 180 or 240 copies of the core protein, also referred to as the hepatitis B core antigen, or HBcAg, make up the icosahedral core particle. Serological evidence of disease may only be IgM antibodies specific to the hepatitis B core antigen during this “window” in which the host is still infected but is effectively clearing the virus. Consequently, total anti-HBc and HBsAg are present in the majority of hepatitis B diagnostic panels (Karayiannis et al., 2009).
Hepatitis B e antigen (HBeAg) is a second antigen that appears shortly after HBsAg does. Hepatitis B virus genotypes that do not express the ‘e’ antigen challenge the conventional wisdom that increased rates of viral replication and enhanced infectivity are linked to the presence of HBeAg in a host’s serum (Liaw et al., 2010).
IgG antibodies to the hepatitis B surface antigen and core antigen (anti-HBs and anti-HBc IgG) will eventually overtake the HBsAg if the host is successful in eliminating the infection. The window period is the interval of time between the elimination of HBsAg and the emergence of anti-HBs. A person who tests positive for anti-HBs but negative for HBsAg has likely had a prior vaccination or recovered from an illness (Liaw et al., 2010).
Hepatitis B carriers are those who test positive for HBsAg for at least six months (Lok and McMahon, 2007). If virus carriers are in the immunological clearance phase of a chronic infection, they may have chronic hepatitis B, which would be indicated by high serum alanine aminotransferase levels and liver inflammation. Due to their low viral multiplication, carriers who have seroconverted to HBeAg negative status—especially those who contracted the infection as adults—may be less likely to experience long-term consequences or to infect others (Chu and Liaw, 2007). To identify and quantify the quantity of HBV DNA, often known as the viral load, in clinical specimens, PCR techniques have been developed. These examinations determine an individual’s infection status and track the effectiveness of treatment (Zoulim, 2006).
1.1.1.8. Prevention
Since 1991, the United States has consistently recommended vaccinations for babies to avoid hepatitis B (Schillie et al., 2013). It is usually advised to take the first dosage the day after birth. According to Chan et al. (2016), the hepatitis B vaccine was the first to be able to prevent cancer in general and liver cancer in particular.
In addition, the vaccine with hepatitis B immunoglobulin combo is better than the vaccine alone (Lee et al., 2006). In 86% to 99% of cases, this combination stops HBV transmission around the time of birth (Wong et al., 2014).
1.1.1.9. Treatment
Most persons who have an acute hepatitis B infection recover on their own without the need for treatment (CDC, 2017). Less than 1% of individuals with immunocompromised individuals or those whose infection progresses aggressively to fullminant hepatitis may need early antiviral treatment (Lai and Yuen, 2007).
Treatment duration varies based on medicine and genetics, ranging from six months to a year. However, the length of treatment varies greatly and is typically more than a year when medication is administered orally (Terrault et al., 2016).
As of 2018, the United States had eight approved medicines available to treat hepatitis B infection. They include two immune system modulators, PEGylated interferon alpha-2a and interferon alpha-2a, as well as antiviral drugs, such as entecavir, lamivudine, adefovir, tenofovir disoproxil, tenofovir alafenamide, telbivudine, and more. The World Health Organization suggested entecavir or tenofovir as first-line treatments in 2015. The majority of people who have cirrhosis now require therapy (WHO, 2015).
Long-acting PEGylated interferon, which is injected just once per week, has replaced the use of interferon (Dienstag, 2008). The therapy lowers the quantity of virus particles detected in the blood, or the viral load, by inhibiting viral replication in the liver (Pramoolsinsup, 2002).
1.2.2. Hepatitis C virus
1.2.2.1. Virology
According to Rosen (2011), the hepatitis C virus (HCV) is a tiny, enclosed, single-stranded, positive-sense RNA virus. According to Ray et al. (2009), it belongs to the family Flaviviridae and the genus Hepacivirus. HCV has seven main genotypes, referred to as genotypes one through seven (Nakano et al., 202 1). According to Wilkins et al. (2010), genotype 1 accounts for roughly 70% of cases in the US, genotype 2 for 20%, and each of the remaining genotypes for 1% of cases.
In Europe and South America, genotype 1 is likewise the most prevalent (Rosen, 2011). The virus particles in the serum have a half-life of roughly three hours, although they could be as brief as forty-five minutes (Lerat and Hollinger 2004; Pockros, 2011). Every day, an infected individual produces roughly 1012 virus particles (Lerat Hollinger, 2004).
1.2.2.2. Transmission
Most infections are often caused by percutaneous contact with contaminated blood; however, the mode of transmission is highly dependent on the location and economic standing of a nation (Hagan and Schinazi, 2013). In fact, injectable drug usage is the main means of transmission in the industrialized world, whereas risky medical procedures and blood transfusions are the main means in the developing world (Maheshwari and Thuluvath, 2010). In 20% of cases, the cause of transmission is still uncertain (Pondé, 2011).
A. Drug use
In many regions of the world, injection drug use (IDU) is a significant risk factor for hepatitis C. Out of the 77 countries that were examined, it was shown that between 60% and 80% of injectable drug users in 25 of them, including the US, had hepatitis C. More than 80% of the countries had these rates (Nelson et al., 2011).
Ten million intravenous drug users are thought to be hepatitis C positive; the largest absolute totals are found in China (1.6 million), the US (1.5 million), and Russia (1.3 million) (Nelson et al., 2011). Inmates in American prisons have a hepatitis C prevalence that is 10–20 times higher than that of the general population (Imperial, 2010).
B. Healthcare exposure
Significant infection risks are associated with blood transfusions, blood product transfusions, and organ donations that do not undergo HCV screening (Wilkins et al., 2010). 1992 saw the implementation of universal screening in the US (Marx, 2010). and in 1990, Canada implemented nationwide screening (Day et al., 2009).
As a result, the risk per unit of blood dropped from one in 200 (Marx, 2010) to one in 10,000–1,000,000 (Pondé, 2010). This minimal risk persists because, depending on the technique, it can take anywhere from 11 to 70 days for the blood to test positive for hepatitis C after the potential blood donor has the disease (Pondé, 2010).
According to Wilkins et al. (2010), there is a 1.8% risk that someone who was needlestick injured by an HCV positive person will go on to get the illness. If the puncture incision is deep and the needle in question is hollow, the danger is higher (Alter, 2007).
C. Sexual intercourse
Hepatitis C is not often spread through sexual contact. Very minimal risks have been observed in studies looking at the possibility of HCV transmission between heterosexual partners when one is infected and the other is not (Kim, 2016).
D. Bodymodification
Hepatitis C risk is elevated by two to three times in those who have tattoos. This may be the result of contaminated dyes or inadequately sanitized equipment (Jafari et al., 2010). According to the CDC (2012), tattoos received in a licensed establishment are rarely directly linked to HCV infection.
E. Sharedpersonalitems
Razors, toothbrushes, and tools for manicures and pedicures are examples of personal hygiene products that can get contaminated with blood. Sharing these kinds of things may expose someone to HCV. Hugging, kissing, or sharing cutlery while cooking are not examples of informal contact that can transmit HCV (CDC, 2012). additionally, it cannot be spread via food or drink (Wong and Lee, 2006).
F. Mother-to-child transmission
Less than 10% of pregnancies result in hepatitis C transmission from mother to kid. This risk cannot be changed by any means (Lam et al., 2010). Although the exact time of transmission during pregnancy is unknown, it may happen at either the gestational or delivery stages (Pondé, 2010). There is a higher chance of transmission during a prolonged labor (Alter, 2007).
1.2.2.3. Epidemiology
In a 2021 report, the World Health Organization estimated that, as of 2019, 58 million persons worldwide had chronic hepatitis C (WHO, 2021). An estimated 290,000 people die each year from hepatitis C-related illnesses, primarily cirrhosis and liver cancer, and an estimated 1.5 million people become infected each year (WHO, 2022).
Consequently, the global chronic patient population under treatment increased from approximately 950,000 in 2015 to 9.4 million in 2019. Hepatitis C mortality decreased from approximately 400,000 to 290,000 during the time (WHO 2015; WHO, 2021).
A previous study conducted in 2013 found that infection rates were low (<1.5%) in Asia-Pacific, Tropical Latin America, and North America, and high (>3.5% population infected) in Central and East Asia, North Africa, and the Middle East; intermediate (1.5–3.5%) in South and Southeast Asia, sub-Saharan Africa, Andean, Central and Southern Latin America, Caribbean, Oceania, Australasia, and Central, Eastern, and Western Europe.
The probability of cirrhosis among chronically infected individuals after 20 years is estimated to be approximately 10-15% for men and 1-2%) for women, however it varies according on the study. It’s unknown why there is this difference. Hepatocellular carcinoma can develop at a rate of 1-4 percent annually if cirrhosis is established (Yu and Chuang, 2009). Egypt achieved a significant reduction in Hepatitis C infection rates from 22% in 2011 to just 2% in 2021 by implementing Egypt’s 2030 Vision (Egypt Today, 2021).
About 2% of Americans suffer from chronic hepatitis C (Wilkins et al., 2010). According to estimates, there were 30,500 new cases of acute hepatitis C in 2014 (0.7 cases per 100,000 people), up between 2010 and 2012. (CDC, 2016). In 2008, there were 15,800 hepatitis C-related fatalities (CDC, 2014). surpassing HIV/AIDS as the leading cause of death in the United States in 2007. (Nrw York Time, 2012). According to estimates, between 0.13 and 3.26% of people in Europe suffer from chronic infections (Blachier et al., 2013).
According to Hepatitis C, 2017, around 118,000 individuals in the UK had a chronic infection in 2019. There are more cases of this virus overall in a few Asian and African nations (Holmberg et al., 2011). Pakistan (4.8%) and China (3.2%) are two nations with exceptionally high infection rates (WHO, 2011).
Since 2014, most people can eradicate the condition in 8–12 weeks with the use of incredibly powerful medication. Overall, the number of HCV cases increased in 2015, with around 950,000 new infections and 1.7 million treatment cases (Lombardi and Mondelli, 2019).
A. HCV in children and pregnancy
Global estimates place the prevalence of hepatitis C virus infection in infants and pregnant women at 0.05–5% and 1-8%, respectively (Arshad et al., 2011). An estimated 3–5% of cases are vertically transmitted, and children have a high probability of spontaneous clearance (25–50%). Higher rates of occurrence in children (15%) as well as vertical transmission (18%, 6–36%, and 41%) have been documented (Fischler, 2007).
HCV infection is now most commonly caused via transmission around the time of birth in affluent countries. Transmission appears to be uncommon when there is no virus in the mother’s blood (Thomas et al., 1998). According to Indolfi and Resti (2009), procedures that expose the newborn to maternal blood and membrane rupture occurring more than six hours prior to birth are factors linked to an elevated likelihood of infection.
1.2.2.4. Signs and symptoms
Hepatitis C can take two weeks to six months to incubate. After the initial infection, almost 80% of individuals show no symptoms at all. When symptoms are severe, a person may have fever, lethargy, nausea, vomiting, abdominal discomfort, pale stools, dark urine, joint pain, and jaundice (yellowing of the skin and whites of the eyes). About 20–30% of infected individuals experience acute symptoms (WHO, 2016; CDC, 2020).
1.2.2.5. Diagnosis
Hepatitis C can be diagnosed using many methods such as quantitative HCV RNA polymerase chain reaction (PCR), recombinant immunoblot assay, and HCV antibody enzyme immunoassay (ELISA) (Wilkins et al., 2010). While antibodies can take a significant amount longer to develop and become detectable, HCV RNA can usually be found by PCR one to two weeks after infection (Ozaras and Tahan, 2009).
Patients with acute illnesses typically come with mild, nonspecific flu-like symptoms, making diagnosis difficult. In contrast, the transition from acute to chronic illness is often sub-clinical (Westbrook and Dusheiko, 2014). According to Kanwal and Bacon (2011), chronic hepatitis C is defined as a viral infection that lasts longer than six months and is detected by the presence of its RNA.
A. Serology
The first step in the testing process for hepatitis C usually involves blood work to look for HCV antibodies using an enzyme immunoassay. In the event that this test yields positive results, an additional test is run to confirm the immunoassay results and ascertain the viral load. HCV RNA polymerase chain reaction is employed to measure the viral load, and recombinant immunoblot assay is utilized to validate the immunoassay (Wilkins et al., 2010). Although there are hazards associated with the process, liver biopsies are utilized to assess the level of liver damage that is present (Rosen, 2011).
1.2.2.6. Prevention
As of 2016 (Abdelwahab and Said, 2018), there is no vaccination that is authorized to prevent getting hepatitis C. The risk of hepatitis C in injecting drug users is reduced by around 75% when harm reduction tactics, such as providing fresh needles and syringes and treating substance abuse, are combined (Hagan et al., 2011). Both blood donor screening and following standard operating procedures in medical facilities are critical on a nationwide scale (Ray and Thomas, 2009).
1.2.2.7. Treatment
Alcohol and liver-toxic drugs should be avoided by those with chronic hepatitis C (Wilkins et al., 2010). Given the higher risk of infection if they also have hepatitis A and hepatitis B, they should also receive vaccinations against those diseases (Wilkins et al., 2010). At lower dosages, acetaminophen use is usually regarded as safe (Kim, 2016).
A. Medications
About 90% of chronic cases with ribavirin resolve with therapy (WHO, 2016). For those with confirmed chronic hepatitis C who do not have a significant risk of dying from other causes, antiviral drug treatment is advised (AASLD/IDSA, 2015). When given medicine, almost 90% of patients with persistent infections can be cured (CDC, 2019). Nevertheless, it may be costly to obtain these medicines (WHO, 2016).
For patients who have not responded to prior treatment with sofosbuvir or other NS5A inhibitors, a combination of sofosbuvir, velpatasvir, and voxilaprevir may be utilized. Treatments up until 2011 involved a 24- or 48-week course of pegylated interferon alpha and ribavirin, contingent on the genotype of the HCV (Wilkins et al., 2010).
Cure rates from this treatment range from 45 to 70% for genotypes 1 and 4, and from 70 to 80% for genotypes 2 and 3. Treatment works best while hepatitis C is in its acute stage, which lasts for six months, as opposed to when it has progressed into the chronic stage (Ozaras and Tahan, 2009). About 25% of those with chronic hepatitis B experience reactivation of hepatitis B after receiving therapy for hepatitis C (Mücke et al., 2018).
1.2.3. Hepatitis A virus
Hepatovirus A (HAV) is the infectious agent that causes hepatitis A, a form of viral hepatitis. Many cases, especially in the younger population, show few or no symptoms. For individuals who experience symptoms, the interval between infection and symptoms is two to six weeks (Connor, 2005; Matheny and Kingery, 2012).
When they do, symptoms including nausea, vomiting, diarrhea, jaundice, fever, and abdominal discomfort usually linger for eight weeks. Ten to fifteen percent of patients had a symptom recurrence within six months of the original illness. Rarely, acute liver failure can happen; older people are more likely to have this (Matheny and Kingery, 2012).
Typically, consuming food or drinking water tainted with diseased excrement spreads the infection. Shellfish that is uncooked or undercooked is a very common source. Additionally, it can spread through intimate contact with an infected individual. Even while children who are infected frequently show no symptoms, they can still spread the infection to others. A person is immune for the remainder of their lives following just one infection. Blood testing is necessary for the diagnosis because the symptoms can be mistaken for those of several different illnesses. Out of the five recognized hepatitis viruses, there are A, B, C, D, and E. Bellou and associates (2013); Matheny and Kingery, 2012).
As a preventative measure, the hepatitis A vaccine works well. Certain nations regularly advise against it for young people and others who are more vulnerable and have never received a vaccination. It seems to work for eternity. Proper meal preparation and hand cleaning are two other protective strategies. There isn’t a set course of therapy; rest and over-the-counter drugs for nausea or diarrhea are advised as needed. Most of the time, infections end fully and don’t cause persistent liver damage. Liver transplantation is the treatment of choice for acute liver failure, should it arise. (WHO, 2013; Irving et al., 2012; Matheny and Kingery, 2012).
Annually, there are around 114 million infections (including symptomatic and asymptomatic) and 1.4 million symptomatic cases worldwide. It is more prevalent in parts of the world where there is a shortage of clean water and inadequate sanitation. Ninety percent of children in underdeveloped countries are immune by maturity, having been infected by the age of ten. In moderately developed nations, when vaccination rates are low and children are not exposed at an early age, it frequently happens during outbreaks. 11,200 people died from acute hepatitis A in 2015. Every year on July 28, the world observes World Hepatitis Day to raise awareness of viral hepatitis (Matheny and Kingery, 2012; WHO, 2013).
1.2.3.1. Transmission
The fecal–oral pathway is how the virus spreads, and crowded, unsanitary environments are common places for infections to happen. Parenterally administered hepatitis A can seldom be contracted from blood or blood products. Food-borne illnesses frequently occur, and eating shellfish raised in contaminated water carries a significant risk of infection. HAV is responsible for about 40% of cases of acute viral hepatitis. Ten days after infection, or before symptoms appear, infected people are contagious. According to Murray et al. (2005), the virus is resistant to drying, detergent, acid (pH 1), solvents (such as ether and chloroform), and temperatures as high as 60 °C.
Both fresh and salt water can support it for several months. Epidemics from common sources (restaurants, water, etc.) are common. In developing nations, the prevalence of infection in children can exceed 100%; yet, once an infection occurs, a lifetime immunity develops. Drinking water treated with chlorine, formalin (0.35%, 37 °C, 72 hours), peracetic acid (2%, 4 hours), beta-propiolactone (0.25%, 1 hour), and UV light can all inactivate HAV. Sexual intercourse, particularly oroanal sexual behaviors, can also transmit HAV (Brundage and Fitzpatrick, 2006).
This virus is very contagious in underdeveloped nations and areas with low standards of hygiene, and the sickness is typically first discovered in early childhood. The frequency of HAV falls as wages grow and more people have access to clean water. However, in industrialized nations, young adults who are susceptible to infection are the main carriers of the virus. Most of these individuals become infected while traveling to nations where the illness is common or by coming into contact with infected individuals. The virus’s sole natural reservoir is humans. There are no known insect or animal vectors that can spread the virus. There have been no reports of a chronic HAV condition (Connor, 2005).
1.2.3.2. Epidemiology
About 1.4 million persons worldwide are thought to get symptomatic HAV infections each year. In total, there were about 114 million infections in 2015, both symptomatic and asymptomatic. 11,200 people died from acute hepatitis A in 2015. The amount of hepatovirus A in circulation is lower in developed nations than it is in underdeveloped nations. Since the majority of adults and adolescents in poor nations have already experienced the illness, they are immune. There is a chance that adults in middle-income nations will be exposed to diseases (Jacobsen and Wiersma, 2010; Matheny and Kingery, 2012).
In 1997, the US CDC received reports of almost 30,000 cases of hepatitis A; however, throughout the years, the number of cases reported every year has decreased to less than 2,000. The state of Kentucky experienced the largest-scale hepatitis A outbreak in US history in 2018. It is thought that the outbreak began in November 2017. As of July 2018, there had been at least one case of hepatitis A recorded in 48 percent of the state’s counties; there had been 969 suspected cases overall, with six fatalities (482 instances in Louisville, Kentucky). The outbreak peaked in July 2019 with 5,000 cases and 60 fatalities, but it thereafter tapered off to a few new cases per month (Wymer, 2019).
In late 2003, there was another large-scale outbreak in the US: the 2003 US hepatitis outbreak, which struck at least 640 persons in northeastern Ohio and southwest Pennsylvania (resulting in four fatalities). A Monaca, Pennsylvania restaurant’s poisoned green onions were identified as the cause of the outbreak (Wheeler et al., 2005).
After consuming clams from a tainted river in Shanghai, China, more than 300,000 people contracted HAV in 1988. A recall of frozen berries was issued in June 2013 after at least 158 persons—69 of whom required hospitalization—were infected with HAV after the US retailer Costco sold the product to over 240,000 consumers. A recall of Costco’s frozen berries was announced in April 2016, following at least 13 cases of HAV infection in Canada, three of which resulted in hospitalization. A recall of frozen berries was announced in Australia in February 2015 after the product was consumed by at least 19 persons who became ill. Hepatitis A outbreaks in 2017 were recorded in Utah, Michigan, and California (especially in the San Diego area), resulting in over 800 hospital admissions and 40 fatalities (Ramseth, 2017).
1.2.3.3. Structure
Hepatovirus A is a picornavirus, meaning it has a single strand of positive-sense RNA encased in a protein shell. It is not enclosed. The virus has been identified as having only one serotype, but several genotypes. The genome uses codons in a biased way that is unusually different from that of its host. Its internal ribosome entrance site is also not very good. Highly conserved clusters of uncommon codons limit antigenic diversity in the area encoding the HAV capsid (Aragonès et al., 2008).
| Genus | Structure | Symmetry | Capsid | Genomic arrangement | Genomic segmentation |
| Hepatovirus | Icosahedral | Pseudo T=3 | Nonenveloped | Linear | Monopartite |
1.2.3.4. Taxonomy
Hepatovirus A is a type of virus belonging to the genus Hepatovirus, family Picornaviridae, order Picornavirales. Natural hosts include vertebrates such as humans. There are nine known Hepatovirus members. Shrews, hedgehogs, rodents, and bats are all infected by this species. Hepatitis A may have originated in rodents, according to phylogenetic study (Anthony et al., 2015).
Electron micrograph of Hepatovirus A virions.
From a seal, a member virus of hepatovirus B, or Phopivirus, has been isolated. About 1800 years ago, this virus and Hepatovirus A had a common ancestor. The woodchuck Marmota himalayana has been found to harbor another hepatovirus, known as the Marmota himalayana hepatovirus. It suggests that approximately a millennium ago, this virus and the one that infects primates had an ancestor (Yu et al., 2016).
1.2.3.2.1. Genotypes
There has been a description of one serotype and seven distinct genetic groups (three simian and four human). I through III are the human genotype numbers. There are six known subtypes: IA, IB, IIA, IIB, IIIA, and IIIB. The genotypes of simian have been assigned numbers IV–VI. Additionally, a single human isolate of genotype VII has been reported. It has been possible to isolate humans and owl monkeys with genotype III. Most isolates from humans belong to genotype I. Subtype IA makes up the majority of type I isolates (Ching et al., 2002).
According to estimates, the genome experiences 1.73–9.76 × 10−4 nucleotide substitutions per site annually for each mutation. It seems that approximately 3600 years ago, the human strains separated from the simian strains. It has been estimated that the mean age of the IIIA and III genotype strains is 202 years and 592 years, respectively (Kulkarni et al., 2009).
1.2.3.5. Pathogenesis
The host immunological reaction to HAV results in hepatic damage. Human leukocyte antigen-restricted, HAV-specific CD8+ T lymphocytes and natural killer cells mediate hepatocellular damage and the elimination of infected hepatocytes; viral replication takes place in the cytoplasm of hepatocytes. It seems that interferon-gamma plays a major part in encouraging the removal of infected hepatocytes. Severe hepatitis is linked to an overreaction by the host, as evidenced by a significant decrease in HAV ribonucleic acid (RNA) in the bloodstream after acute infection (CDC, 2009).
1.2.3.6. Signs and symptoms
Early signs of hepatitis virus Although an infection can be mistaken for influenza, some individuals—particularly children—don’t show any symptoms at all. It usually takes 2-4 weeks (the incubation period) for symptoms to manifest following the initial infection. Ninety percent of kids do not exhibit any symptoms. For individuals who experience symptoms, the interval between infection and onset is typically 2–6 weeks, with an average of 28 days (Connor, 2005).
Age is a crucial factor in the likelihood of symptomatic infection; over 80% of adults have symptoms consistent with acute viral hepatitis, but most children have infections that are either silent or go undiagnosed. Although some patients may experience symptoms for up to six months, the majority of patients experience symptoms such as fatigue, fever, nausea, appetite loss, jaundice, a yellowing of the skin or whites of the eyes due to hyperbilirubinemia, diarrhea, light or clay-colored stools (acholic faeces), and abdominal discomfort (Ciocca, 2000; CDC, 2009). Bile is removed from the bloodstream and excreted in the urine, giving it a dark amber color.
1.2.3.7. Extrahepatic manifestations
Extrahepatic symptoms include pancreatitis, red cell aplasia, joint discomfort, and widespread lymphadenopathy. Pericarditis with kidney failure are extremely rare conditions. If they materialize, they have an abrupt start and end when the illness resolves (Mauss et al., 2012).
1.2.3.8. Diagnosis
After hepatovirus A infection, serum IgG, IgM, and ALT levels. HAV is eliminated in the feces at the conclusion of the incubation period, but the identification of HAV-specific IgM antibodies in the blood allows for a precise diagnosis. The blood only contains IgM antibodies after an acute hepatitis A infection. It appears 1-2 weeks following the original illness and lasts for up to 14 weeks. IgG antibodies in the blood indicate that the sickness has progressed past its acute phase and that the patient is no longer susceptible to infection. After vaccination, IgG antibodies to HAV are also detected in the blood, and the presence of these antibodies serves as the basis for testing to determine a person’s immunity to the virus (Musana et al., 2004).
The liver enzyme alanine transferase (ALT) is significantly more prevalent in the blood than usual during the acute stage of the infection. The virus-damaged liver cells produce the enzyme. Up to two weeks before a clinical sickness manifests, hepatovirus A can be found in the blood (viremia) and feces of infected individuals (Musana et al., 2004).
1.2.3.9. Prevention
a. Vaccination
Hepatovirus A, either inactivated or attenuated, is contained in the two vaccination forms. Both offer proactive defense against upcoming infections. For almost 25 years, the vaccine offers protection against HAV in over 95% of instances. The vaccination Maurice Hilleman and his colleagues produced was approved in 1995 and administered to children in high-risk areas for the first time in 1996. In 1999, the vaccine was expanded to places where infection rates were rising (CDC, 2006).
1.2.3.10. Treatment
Hepatitis A does not currently have a specific treatment. After an infection, symptoms may be slow to go away and may take weeks or months. It’s critical to stay away from needless drugs. Avoid using acetaminophen, paracetamol, and antiemetic medications if you have vomiting (WHO, 2022). Hospitalization is not required if acute liver failure is not present. The goal of therapy is to preserve comfort and a healthy nutritional balance, which includes replenishing fluids lost due to diarrhea and vomiting (WHO, 2022).
1.3. Objective of this study
1.3.1. General objectives
The aim of the present investigation was designed to determine the prevalence of hepatitis A, E, B and C viruses in Hajjah governorate between 2020-2023, Yemen.
1.3.2. Specific objectives
- To determine the prevalence of viral hepatitis in Hajjah governorate between 2020-2023.
- To evaluate the demographic factors influencing the prevalence of viral hepatitis infection in Hajjah governorate between 2020-2023.
2. Materials and Methods
2.1. Study Design and Area
The Hajjah Governorate in Yemen hosted this retrospective study for four years, from 2020 to 2023. The Hajjah Governorate is situated around 123 kilometers northwest of Sana’a, the capital of Yemen. It is connected to the Red Sea and a portion of Al Hudaydah governorate from the west, the Sa’ada governorate and the Kingdom of Saudi Arabia from the north, the Amran governorate from the east, the Al Mahwit and Al Hudaydah governorates from the south, and the Red Sea from the east. The governorate has a population of 2,782,000 people and a land area of roughly 10,141 km2 (3,915 sq mi). While the coastal plains regions experience hot, humid tropical summers and mild winters, the highland regions of the Hajjah governorate experience mild summers and chilly winters. The Hajjah Governorate is separated into the 31 districts listed below. Villages are created by further subdividing these districts into sub-districts.
2.2. Study Population
Data were collected from the clinical records of epidemiological surveillance in the Public Health Office of the Hajjah Governorate. All cases were diagnosed in different laboratories based on direct observation of hepatitis A, E, B, and C in the blood sample.
2.3. Data Collection
The data required in this study included information such year of infection, weekly number, district name, month, and season,
2.4. Statistical Analysis
The information was divided into quantitative variables and shown in tables and figures as frequencies and percentages. In addition, the probability (P) value that was deemed statistically significant at ≤ 0.05 was determined using the statistical package for social sciences (SPSS) program.
3. Results
3.1. Socio-Demographic Characteristics
A total of 41162 cases were collected between 2020 and 2023 in patients from different districts belong to Hajjah governorate. The majority of specimens were more in years of 2023 at 12673 (30.8%) and the lower in year of 2020 at 3499 (8.5%), as summarized in Table 1 and Figure 1.
Table 2 shows that the most specimens were collected from Bani Qais at 2635 (6.5%) and the lower was from Hayran 36 (0.1%) as summarized Figure 2.
3.2. Prevalence of Hepatitis A, E, B, and C Viruses
3.2. Distribution of Hepatitis A, E, B, and C Viruses
The present results showed that the higher rate of HAV and HEV was in 2022 (2.3%) whereas Hepatitis B and C was in 2020 (2.9%) (Table 6 and Figure 6).
This finding showed that a higer rate of HAV and HEV was detected among individuals who come from Al Miftah district 116 (7.5%). In addition, a higher rate of hepatitis B and C was Hajjah city at 579(22.9%) as shown in Table 7 and Figure 7.
Regarding the month of the incident, the highest rate of HAV and HEV viruses were recorded at 85(2.6%) in September while the hepatitis B and C viruses were higher in the October 97 (2.8%) and November 115 (2.8%). Additionally, the lowest rate was 1.6%% observed for hepatitis A and E and hepatitis B and C in April (Table 8 and Figure 8).
4. Discussion
Furthermore, the hepatitis B and C viruses were higher in the October 97 (2.8%) and November 115 (2.8%) and the lower rate was 1.6%% observed in April. The high rate of hepatitis A and B and hepatitis B and C viruses were observed in Autumn at 2.2% and 2.6%, respectively.
The current findings indicate that the prevalence rate of HAV and HEV was 761 (1.85%). The prevalence of both Hepatitis A virus (HAV) and Hepatitis E virus (HEV) in patients with acute viral hepatitis was found to be 11.5% according to a study conducted by Joon et al. in 2015. The occurrence of HAV and HEV was determined to be 15.4% and 29.7%, respectively, according to Chandni et al. (2020). The occurrence of Hepatitis A virus (HAV) and Hepatitis E virus (HEV) in India was documented at 6.7% and 8.5%, respectively, according to Palewar et al. (2022).
This study found a 2.36% prevalence of combined HBV and HCV in Hajjah governorate from 2020 to 2023. The overall prevalence of hepatitis B surface antigen (HBsAg) is 2.5% and the prevalence of anti-hepatitis C virus (HCV) is 4.8% (Qureshi et al., 2010). The worldwide collective seroprevalence was found to be 5.8% for HBs-antigen and 10.3% for HCV-antibodies. The highest prevalence of HBV was seen in the WHO African Region, with a pooled prevalence of 7.8%. Similarly, the WHO European Region had the highest prevalence of HCV, with a pooled prevalence of 17.5% (Olaru et al., 2023). Egypt has a high prevalence rate of 20% due to iatrogenic contamination, as reported by Rutherford et al. in 2016.
In 2016/2017, OCHA reported that 71% of households in Hajjah lacked access to safe drinking water. The city of Hajjah is currently maintaining its water and sanitation facilities, but only at a minimal level, primarily due to assistance from external organizations such as the Berghof Foundation (2023).
The current findings indicate that the incidence of Hepatitis A and E was greater in 2022 (2.3%), while Hepatitis B and C had a higher rate in 2020 (2.9%). The study revealed a higher prevalence of hepatitis A and E among individuals originating from Al Miftah district, with a rate of 7.5%. Furthermore, Hajjah city exhibited a significantly elevated prevalence of hepatitis B and C, with a rate of 579 cases (22.9%).
The month with the highest incidence of hepatitis A and E viruses was September, with a rate of 85 cases (2.6%), while the lowest incidence was observed in April, with a rate of 1.3%. A study conducted by Palewar et al. (2022) revealed that the incidence of infection was higher between June and October, namely during the monsoon and post-monsoon periods. Furthermore, the study period observed occurrences of both HAV and HEV cases, with notable increases in the months of June, July, and August, which coincide with the monsoon season (Chandni et al., 2020). According to Chen et al. (2019), the highest number of confirmed HAV patients occurred between May and July 2016.
Hepatitis A virus (HAV) and Hepatitis E virus (HEV) infections are spread through the ingestion of fecal matter. This can occur due to a lack of clean drinking water during the summer or when sewage contaminates the water supply during the monsoon season. These factors increase the likelihood of contracting these illnesses (Palewar et al., 2022).
In the viral hepatitis Surveillance-India (2011–2013) study, Kumar et al. (2017) found that there was a 17% rise in the overall number of reported hepatitis cases between June and September. Joon et al. (2015) found that HAV and HEV were both widespread throughout the year, with a higher occurrence observed towards the conclusion of the monsoon season and the onset of winter. According to Chandni et al. (2020), there is a fluctuation in the spread of acute viral hepatitis during different seasons. This variation may be caused by the introduction of polluted soil into wells and rivers when there are significant rains or floods.
In addition, the prevalence of hepatitis B and C viruses was greater in October 1997 (2.8%) and November 2015 (2.8%), while the lowest rate of 1.6% was reported in April. In Autumn, a significant prevalence of hepatitis A and B viruses at a rate of 2.2% and hepatitis B and C viruses at a rate of 2.6% was reported.
5. Conclusion and Recommendatios
5.1. Conclusion
- The present result revealed that the prevalence rate of Hepatitis A and E was 761 (1.85%) while the Hepatitis B and C was 971 (2.36%) among study subjects.
- The present results showed that the higher rate of Hepatitis A and E was in 2022 (2.3%) whereas Hepatitis B and C was in 2020 (2.9%).
- This finding showed that a higer rate of hepatitis A and E was detected among individuals who come from Al Miftah district 116 (7.5%). In addition, a higher rate of hepatitis B and C was Hajjah city at 579 (22.9%).
- Regarding the month of the incident, the highest rate of hepatitis A and E viruses were recorded in September at 85(2.6%) while the lowest was in April (1.3%)
- The hepatitis B and C viruses were higher in the October 97 (2.8%) and November 115 (2.8%) and the lower rate was 1.6%% observed in April
- The high rate of hepatitis A and B and hepatitis B and C viruses were observed in Autumn at 2.2% and 2.6%, respectively.
5.2. Recommendation
- The implementation and timing of interventions, such as universal children vaccination programs, must be done carefully.
- Hence, it is imperative to ensure the continuous and long-term availability of diagnostic kits of all kinds at healthcare facilities.
- The need for sectors to collaborate in order to ensure the provision of safe water and sewage disposal.
- This study highlights the significance of screening all hepatitis viral markers (A, B, C, E) for early detection and prevention of outbreaks and epidemics by the public health sector, thereby reducing illness and death rates.
- This data will be crucial for the development of future immunization tactics and improvement of sanitation programs in this region.
- It is advisable to administer HAV immunization to individuals at high risk and to maintain ongoing monitoring to monitor control actions during community-wide outbreaks of HAV.
- Ensuring the quality of public water supplies and implementing proper sewage disposal systems at the community level can effectively reduce the transmission of Hepatitis A virus (HAV) and Hepatitis E virus (HEV).
- Individuals can decrease their risk of infection by practicing good hygiene, such as washing their hands with clean water and avoiding consuming food and water that may be contaminated.
- The authorities should strive to enhance public awareness in order to permit prompt preparation and required arrangements for an effective response to outbreaks or epidemics, therefore reducing illness, death, and economic cost.
References
- Aaron D, Nagu TJ, Rwegasha J, Komba E(2017). Hepatitis B vaccination coverage among healthcare workers at national hospital in Tanzania: how much, who and why? BMC Infect Dis.17(1):1–7. [CrossRef]
- AASLD/IDSA HCV Guidance Panel (2015). Hepatitis C guidance: AASLD-IDSA recommendations for testing, managing, and treating adults infected with hepatitis C virus. Hepatology. 62 (3): 932–954. [CrossRef]
- Abdelwahab KS, Said ZN (2016). Status of hepatitis C virus vaccination: Recent update. World Journal of Gastroenterology. 22 (2): 862–873. [CrossRef]
- Abdullah QY, et al., (2020). Seroprevalence of dengue fever virus among suspected patients in Taiz Governorate-Yemen. Universal J Pharm Res., 2020; 5(5):21-26. [CrossRef]
- Abebaw W, Kibret M, Abera B (2014). Prevalence and risk factors of H. pylori from dyspeptic patients in Northwest Ethiopia: a hospital based cross-sectional study. Asian Pac J Cancer Prev. 15(11): 4459–4463. [CrossRef]
- Akbulut A: HAV Infection. Tekeli E, Balık İ (eds.): Viral Hepatit 2003. Roche, İstanbul, 2003; 57–84 [in Turkish].
- Al-Aomary NM, et al., (2023). The Rate of Asymptomatic Throat Carriage of Streptococcus pyogenes and Its Associated Risk Factors among Medical Students of Queen Arwa University in Sana’a City, Yemen. Electron. J. Univ. Aden Basic Appl. Sci. 4(3). [CrossRef]
- Al-Awar MS, et al., (2022). Job satisfaction at clinical laboratories in Sana’a hospitals, Yemen, using the application of Herzberg’s two-factor theory of motivation. Al-Razi Univ J Med Sci. 2022; 6 (1): 17-29. [CrossRef]
- Al-Hadheq AA, et al., (2023). Prevalence of Intestinal Parasitic Infections among Children Attending Some Schools in Amran Governorate, Yemen. J. Amr. Uni. 3(6), 10. 03 (2023): 279- 288. [CrossRef]
- Al-Haik MW, et al., (2017). Antimicrobial activities for hadhrami honey on growth of some pathogenic bacteria. Universal J Pharm Res., 2017: 2(6), 7-12. [CrossRef]
- Al-Haik WM, et al., (2023). Bacterial Conjunctivitis in Hadhramout Governorate-Yemen”, Electron. J Univ. Aden Basic Appl Sci. 4(4): 338-346. [CrossRef]
- Al-Halani AA, et al., (2023). Prevalence of intestinal parasites, malnutrition, anemia and their risk factors among orphaned children in Sana’a City, Yemen. Universal J Pharm Res. 2023; 8(2):32-39. [CrossRef]
- Alhlale FM, et al., (2019) The inhibitory effect of Euphorbia hirta extracts against some wound bacteria isolated from Yemeni patients. COPS. 2019; 3(2): 780-786.
- Alhlale FM, et al., (2020). Effect of most common antibiotics against bacteria isolated from surgical wounds in Aden Governorate hospitals, Yemen. Universal J Pharm Res 2020; 5(1): 21-24. [CrossRef]
- Al-Khawlany RS, et al., (2021). Prevalence of methicillin-resistant Staphylococcus aureus and antibacterial susceptibility among patients with skin and soft tissue infection at Ibb City, Yemen. PSM Microbiol, 2021: 6(1): 1-11.
- Almezgagi M, et al., (2020). Prevalence of hepatitis B virus and hepatitis C virus and associated risk factors among hemodialysis patients in Ibb city-Yemen. PSM Microbiol. 5(2): 32-40.
- Al-Munkari IM, et al., (2022). Hepatitis B, hepatitis C, and HIV infection: Prevalence, knowledge, practice, and attitude among medical waste handlers working in some hospitals at Sana’a City-Yemen. Bachelor Thesis, Medical Laboratory Dep. Queen Arwa University. 2022; Pp; 25-67.
- Al-Ofairi, et al., (2024). “Gram-negative bacteria in some clinical specimens and their antibiotics resistance profiles, Sana’a, Yemen”, Electron. J. Univ. Aden Basic Appl. Sci., vol. 5, no. 1, pp. 86-94, March. [CrossRef]
- Alsaifi AG, et al., (2021). Distribution and risk factors for intestinal parasitic infections among primary schoolchildren in Sana’a city, Yemen. Bachelor Thesis, Medical Laboratory, Queen Arwa University. 2021; Pp; 20-40.
- Alshafli A, Al-Zain A, Faydi I, et al. (2022). Seroprevalence and risk factors of Helicobacter pylori Infection among school children presenting at schools in Sana’a city, Yemen. Bachelor Thesis, Medical Laboratory Dep., Yemen and Gulf University for Science and Technology. 2022; Pp; 27-49.
- Alshahethi MA, et al., (2020). Distribution and risk factors for Giardia lamblia among children at Amran Governorate, Yemen. Universal J Pharm Res., 2020; 5(3):34-37. [CrossRef]
- Alshahethi MA, et al., (2020). Prevalence of Entamoeba histolytica among children attending healthcare centres at Amran governorate, Yemen. PSM Biol Res., 2020; 5(3): 98-105.
- Al-Shamahy H (2000). Prevalence of hepatitis B surface antigen and risk factors of HBV infection in a sample of healthy mothers and their infants in Sana’a, Yemen. Ann Saudi Med . 20(5-6):464-466. [CrossRef]
- Al-Shamahy HA, Jaadan BM, Al-Madhaji AG, et al. (2019). Prevalence and potential risk factors of hepatitis B virus in a sample of children in two selected areas in Yemen. UJPR . 4(3): 17-21. [CrossRef]
- Al-Shamahy HA, Rabbad IA, Al-Hababy A (2003). Hepatitis B virus serum markers among pregnant women in Sana’a, Yemen. Ann Saudi Med. 23:87−89. [CrossRef]
- Al-Shami HZ, Al-Mutawakal ZAM, Al-Kholani AIM, et al. (2021). Prevalence of hepatitis A virus, hepatitis B virus, and hepatitis C virus, among patients with hepatic jaundice in Sana’a city, Yemen: Ahospital based study. Universal Journal of Pharmaceutical Research. 6(6):12-17. [CrossRef]
- Al-Shehari WA, et al., (2023). Cryptosporidium parvum among Cancer and Hemodialysis Patients in Ibb City, Yemen: Prevalence and Risk Factors. Al-Razi Univ J Med Sci. 2023; 7(1):15-22. [CrossRef]
- Alter MJ (2003). Epidemiology and prevention of hepatitis B. Seminars in Liver Disease. 23 (1): 39–46. [CrossRef]
- Alter MJ (2007). Epidemiology of hepatitis C virus infection. World Journal of Gastroenterology. 13 (17): 2436–2441.
- Amsalu A, Worku M, Tadesse E, Shimelis T (2016). The exposure rate to hepatitis B and C viruses among medical waste handlers in three government hospitals, southern Ethiopia. Epidemiol Health. 38:e2016001-e. [CrossRef]
- Anagaw B, Shiferaw Y, Anagaw B, Belyhun Y, Erku W, Biadgelegn F, et al., (2012). Seroprevalence of hepatitis B and C viruses among medical waste handlers at Gondar town health institutions, Northwest Ethiopia. BMC Res Notes . 5:55. [CrossRef]
- Ansa V, Udoma E, Umoh M, Anah M (2002). Occupational risk of infection by human immunodeficiency and hepatitis B viruses among health workers in South-eastern, Nigeria. East Afr Med J. 79:25-27. [CrossRef]
- Anthony SJ, St Leger JA, Liang E, et al. (2015). Discovery of a novel hepatovirus (Phopivirus of seals) related to human hepatitis A virus. mBio. 6 (4): e01180–15. [CrossRef]
- Aragonès L, Bosch A, Pintó RM (2008). Hepatitis A virus mutant spectra under the selective pressure of monoclonal antibodies: codon usage constraints limit capsid variability. J. Virol. 82 (4): 1688–700. [CrossRef]
- Arshad M, El-Kamary SS, Jhaveri R (2011). Hepatitis C virus infection during pregnancy and the newborn period are they opportunities for treatment . Journal of Viral Hepatitis. 18 (4): 229–236. [CrossRef]
- Banafa AM, et al., (2022). Prevalence of hepatitis B surface antigen among orphans children living in orphanage in Sana’a city, Yemen. PSM Microbiol 2022; 7(1): 19-26.
- Banafa MA, et al., (2020). Haemosiderosis, liver and renal diseases among Thalassemia patients in Sana’a city – Yemen. Al-Razi Univ J Med Sci. 2022; 6(2):1-10. [CrossRef]
- Bellou, M.; Kokkinos, P.; Vantarakis, A. (2013). Shellfish-borne viral outbreaks: a systematic review. Food Environ Virol. 5 (1): 13–23. [CrossRef]
- Berghof Foundation. Local Governance in Hajjah, Yemen – maps, data and resources. (2023). Local Governance in Yemen: Resource Hub.
- Blachier M, Leleu H, Peck-Radosavljevic M, Valla DC, Roudot-Thoraval F (2013). The burden of liver disease in Europe: A review of available epidemiological data. Journal of Hepatology. 58 (3): 593–608. [CrossRef]
- Blenkharn I, Odd C (2008). Sharps injuries in healthcare waste handlers. Ann Occup Hyg . 52:281-286. [CrossRef]
- Bonino F, Chiaberge E, Maran E, Piantino P (1987). Serological markers of HBV infectivity. Ann. Ist. Super. Sanità. 24 (2): 217–223.
- Brundage SC, Fitzpatrick AN (2006). Hepatitis A. Am Fam Physician. 73 (12): 2162–8. Archived from the original on 2014-03-09.
- Budak GG, Gülenç N, Özkan E, Bülbül R, et al. (2017). Seroprevalences of hepatitis B and hepatitis C among healthcare workers in Tire State Hospital. Dicle Med J. 44(3):267–270. [CrossRef]
- Buddeberg F, Schimmer BB, Spahn DR (2008). Transfusion-transmissible infections and transfusion-related immunomodulation (PDF). Best Practice and Research. Clinical Anaesthesiology. 22 (3): 503–517. [CrossRef]
- Centers for Disease Control and Prevention (CDC) (2012). Hepatitis C FAQs for health professionals. Centers for Disease Control and Prevention (CDC). Archived from the original on 4 January 2012.
- Centers for Disease Control and Prevention (CDC) (2012). Hepatitis C (PDF). Archived (PDF) from the original on 5 January 2012.
- Centers for Disease Control and Prevention (CDC) (2014). Number and rate of deaths with hepatitis C listed as a cause of death, by demographic characteristic and year – United States, 2004–2008”. Viral Hepatitis on the CDC web site. Atlanta, GA. Archived from the original on 9 March 2014.
- Centers for Disease Control and Prevention (CDC) (2015). Hepatitis B FAQs for the Public. Archived from the original on 20 August 2015.
- Centers for Disease Control and Prevention (CDC) (2016). U.S. 2014 Surveillance data for viral hepatitis, statistics and surveillance, Division of Viral Hepatitis.
- Centers for Disease Control and Prevention (CDC) (2017). Men who have sex with men | populations and settings division of viral hepatitis CDC. www.cdc.gov. 31 May 2015.
- Centers for Disease Control and Prevention (CDC) (2020). Q and A for health professionals. Viral Hepatitis.
- Centers for Disease Control and Prevention (CDC, 2021). Epidemiology and Prevention of Vaccine-Preventable Diseases: Chapter 9 Hepatitis A. Washington D.C. Public Health Foundation; 2021 [cited 2022 Jun 22] Available from: https://www.cdc.gov/vaccines/pubs/pinkbook/hepa.html.
- Central Disease Control and Prevention (CDC), (2015). Men Who Have Sex with Men Populations and Settings Division of Viral Hepatitis CDC. www.cdc.gov AABB (PDF). Archived from the original (PDF) on 2020-10-30.
- Central Diseases Control and Prevention (CDC) (2009). Archived from the original on 2011-05-22. Retrieved 2022-09-08.
- Chan SL, Wong VW, Qin S, Chan HL (2016). Infection and cancer: The case of hepatitis B. Journal of Clinical Oncology. 34 (1): 83–90. [CrossRef]
- Chandni, D., Sidhu, D., Singh, D.K., Oberoi, D.L., & Malhotra, D.S. (2020). Prevalence of Hepatitis A & E in the Patients Presenting with Acute Viral Hepatitis in a Tertiary Care Hospital. International Journal of Science and Research (IJSR); 9(2): 1494-1497. [CrossRef]
- Chen, W. C., Chiang, P. H., Liao, Y. H., Huang, L. C., Hsieh, Y. J., Chiu, C. M., Lo, Y. C., Yang, C. H., & Yang, J. Y. (2019). Outbreak of hepatitis A virus infection in Taiwan, June 2015 to September 2017. Eurosurveillance, 24(14). [CrossRef]
- Ching KZ, Nakano T, Chapman LE, Demby A, Robertson BH (2002). Genetic characterization of wild-type genotype VII hepatitis A virus. J. Gen. Virol. 83 (Pt 1): 53–60. [CrossRef]
- Chu CM, Liaw YF (2007). Predictive factors for reactivation of hepatitis B following hepatitis B e antigen seroconversion in chronic hepatitis B. Gastroenterology. 133 (5): 1458–65. [CrossRef]
- Chung GE, Yim JY, Kim D, et al. Seroprevalence of hepatitis a and associated socioeconomic factors in young healthy korean adults. Gut Liver. 2011;5:88-92. [CrossRef]
- Ciocca M. (2000). Clinical course and consequences of hepatitis A infection. Vaccine. 18: 71–74. [CrossRef]
- Coker A, Sangodoyin A, Sridhar M, Booth C, Olomolaiye P, Hammond F (2009). Medical waste management in Ibadan, Nigeria: Obstacles and prospects. Waste Manag. 29:804-811. [CrossRef]
- Connor BA (2005). Hepatitis A vaccine in the last-minute traveler. Am. J. Med. 118 (Suppl 10A): 58S–62S. [CrossRef]
- Daniels D, Grytdal S, Wasley A, (2009). Surveillance for acute viral hepatitis United States, 2007 (PDF). MMWR Surveill Summ. 58 (3): 1–27. Archived (PDF) from the original on 2012-05-19.
- Dattoli G, Guiot C, Delsanto PP, et al. (2009). Cancer metabolism and the dynamics of metastasis. Journal of Theoretical Biology. 256, pp. 305–310. [CrossRef]
- Day RA, Paul P, Williams B (2009). Brunner and Suddarth’s textbook of Canadian medical-surgical nursing (Canadian 2nd ed.). Philadelphia, PA: Lippincott Williams and Wilkins. p. 1237.
- Dienstag JL (2008). Hepatitis B virus infection. New England Journal of Medicine. 359 (14): 1486–1500. [CrossRef]
- Diestag JL, Szmuness W, Stevens CE, et al. “Hepatitis A Virus infection: new insight from seroepidemiologic studies” . J Infect Dis. 1998; 137:328-340. [CrossRef]
- Douek DC, Roederer M, Koup RA (2009). Emerging concepts in the immunopathogenesis of AIDS. Annual Review of Medicine. 60: 471–84. [CrossRef]
- Dupinay T, et al. (2013). Discovery of naturally occurring transmissible chronic hepatitis B virus infection among Macaca fascicularis from Mauritius Island. Hepatology. [CrossRef]
- Edrees WH (2021). Antibacterial susceptibility and Sider honey activity against isolated bacteria from wound patients attending at Al-Gmohori hospital in Hajja City, Yemen. Al-Razi Univ J Med Sci 2021; 5 (2):1-8. [CrossRef]
- Edrees WH (2022). Seroprevalence and risk factors for Helicobacter pylori infection among school students in Sana’a City, Yemen. Universal J Pharm Res 2022; 7(2):67-73. [CrossRef]
- Edrees WH, Al-Awar SM (2020). Bacterial contamination of mobile phones of medical laboratory workers at Sana’a city, Yemen and their antimicrobial susceptibility. JPPRes. 2020; 8 (6): 591-599.
- Edrees WH, Al-Ofairi BA, Alrahabi LM, et al., (2022). Seroprevalence of the viral markers of Hepatitis B, Hepatitis C, and HIV among medical waste handlers in some hospitals in Sana’a city- Yemen. Universal J Pharm Res. 7(3):12-19. [CrossRef]
- Edrees WH, Alshahethi MA, Al-Awar MS (2022). Factors associated with prevalence of intestinal parasitic infection among schoolchildren in Amran city, Yemen. Al-Razi Univ J Med Sci. 2022; 6(2):1-10. [CrossRef]
- Edrees WH, Alshwmi M, Al-Ofairi AB (2021). Prevalence and antifungal susceptibility of Candida species causing vaginitis among pregnant women in Hajjah Governorate, Yemen. Al-Razi Univ J Med Sci, 2021; 5;(1): 1-8. [CrossRef]
- Edrees WH, Anbar AA (2020). Prevalence and antibacterial susceptibility of bacterial uropathogens isolated from pregnant women in Sana’a, Yemen. PSM Biol Res., 2020; 5(4): 157-165.
- Edrees WH, Anbar AM (2021). Prevalence and antibiotic susceptibility of Streptococcus pyogenes isolated from schoolchildren in Sana’a City, Yemen. PSM Vet. Res., 2021; 6(2): 22-30.
- Edrees WH, Banafa AM (2021). Antibacterial susceptibility of isolated bacteria from wound infection patients presenting at some government hospitals at Sana’a city, Yemen. Al-Razi Univ J Med Sci., 2021; 5(1): 1-13. [CrossRef]
- Edrees WH, Banafa AM, Al-Awar MS (2022). Risk factors and seroprevalence of hepatitis B virus antigen among university students in the Sana’a City, Yemen. Al-Razi Univ J Med Sci. 6(1):8-16. [CrossRef]
- Edrees WH, Banafa AM, Al-Awar MS (2022). Risk factors and seroprevalence of hepatitis B virus antigen among university students in the Sana’a City, Yemen. Al-Razi Univ J Med Sci. 2022; 6(1):8-16. [CrossRef]
- Edrees WH, et al., (2020). Vulvovaginal candidiasis prevalence among pregnant women in different hospitals in Ibb, Yemen. Universal J Pharm Res, 2020; 5(4):1-5. [CrossRef]
- Edrees WH, et al., (2021). Detection of intestinal parasites of some fresh vegetables and their consumers in Sana’a City, Yemen. Al-Razi Univ J Med Sci. 2021; 5 (2):19-25. [CrossRef]
- Edrees WH, et al., (2023). Hepatitis A Virus and Helicobacter pylori among schoolchildren at Sana’a-Yemen: Seroprevalence and risk factors. Al-Razi Univ J Med Sci. 2023; 7(1):34-45. [CrossRef]
- Edrees WH, et al., (2023). Seroprevalence of Helicobacter pylori and hepatitis A virus among orphanage children in Sana’a, Yemen. Universal J Pharm Res. 2023; 8(2):53-60. [CrossRef]
- Edrees WH, et al.,(2022). Seroprevalence of the viral markers of hepatitis B, hepatitis C, and HIV among medical waste handlers in some hospitals in Sana’a city- Yemen. Universal J Pharm Res. 7(3):12-19. [CrossRef]
- Edrees WH, Mogalli NM, Alabdaly KW (2021). Assessment of some clinical and laboratory profiles among dengue fever patients in Hajjah Government, Yemen. Universal J Pharm Res 2021; 6(2):38-41. [CrossRef]
- Edrees, W.H., et al., (2022). Prevalence of intestinal parasitic infections among asymptomatic primary schoolchildren at Al-Sabeen district in Sana’a city, Yemen. PSM Biol. Res., 7(1): 34-45.
- Egypt Today (2021). Hepatitis C prevalence in Egypt drops from 7% to 2% thanks to Sisi’s initiative.
- El-Serag HB (2011). Hepatocellular carcinoma. New England Journal of Medicine. 365 (12): 1118–27.
- Fairley CK, Read TR (2012). Vaccination against sexually transmitted infections. Current Opinion in Infectious Diseases. 25 (1): 66–72. [CrossRef]
- Ferlay J, Shin HR, Bray F, et al. (2008). Estimates of worldwide burden of cancer in 2008: GLOBOCAN. Int J Cancer., 2010; 127: 2893-917. [CrossRef]
- Fiaccadore FS et al. (2006). Prevalence of hepatitis A infection in Goiânia, Goiás, Brazil, by molecular and serological procedures, 1995 - 2002. Mem Inst Oswaldo Cruz 2006; 4: 423-426. [CrossRef]
- Fischler B (June 2007). Hepatitis C virus infection. Seminars in Fetal and Neonatal Medicine. 12 (3): 168–73. [CrossRef]
- Franka E, El-Zoka AH, Hussein AH, Elbakosh MM, Arafa AK, Ghenghesh KS (2009). Hepatitis B virus and hepatitis C virus in medical waste handlers in Tripoli, Libya. J Hosp Infect. 72:258-261. [CrossRef]
- Gafer A, et al., (2023). Socio-demographic profile of patients admitted in Thalassemia center, Sana’a, Yemen. Al-Razi Univ J Med Sci. 2023; 7(1):8-14. [CrossRef]
- Gobara’a AA, et al., (2020). Prevalence of Rubella IgG antibodies among productive -age women in Al-Mahweet Governorate, Yemen. Universal J Pharm Res 2020; 5(4):28-32. [CrossRef]
- Gomes AM, Ferreira AS, Silva AA, de Souza ER (2011). Hepatitis A: seroprevalence and associated factors among schoolchildren of São Luís (MA), Brazil. Rev Bras Epidemiol, 14(4): 548-555. [CrossRef]
- Gunn RA, Murray PJ, Ackers ML, Hardison WG, Margolis HS (2001). Screening for chronic hepatitis B and C viruses infections in an urban sexually transmitted disease clinic-rationale for integrating services. Sex Transm Dis. 28:166-170. [CrossRef]
- Hagan H, Pouget ER, Des Jarlais DC (2011). A systematic review and meta-analysis of interventions to prevent hepatitis C virus infection in people who inject drugs. The Journal of Infectious Diseases. 204 (1): 74–83. [CrossRef]
- Hagan LM, Schinazi RF (2013). Best strategies for global HCV eradication. Liver International. 33 1 (s1): 68–79. [CrossRef]
- Hastings EV, Yasui Y, Hanington P, Goodman KJ (2014). Community-driven research on environmental sources of H. pylori infection in arctic Canada. Gut Microbes. 5, Taylor and Francis. pp. 606–17.
- Hepatitis A Vaccine: Central Diseases Control and Prevention (CDC) (2006). What you need to know (PDF). Vaccine Information Statement. CDC. 2006-03-21. Archived (PDF) from the original on 2007-11-20. Retrieved 2007-03-12.
- Hepatitis Death Rate Creeps past AIDS (2017). New York Times. 27 February 2012. Archived from the original on 30 June 2017.
- Hofmeister MG, Yin S, Aslam MV, Teshale EH, Spradling PR. Hepatitis A Hospitalization Costs, United States, 2017. Emerg Infect Dis. 2020; 26(5):1040-1041. [CrossRef]
- Holmberg S (2011). Brunette GW, Kozarsky PE, Magill AJ, Shlim DR, Whatley AD (eds.). CDC health information for international travel 2012. New York: Oxford University Press. p. 231.
- Hu J, Protzer U, Siddiqui A (2019). Revisiting hepatitis B virus: Challenges of curative therapies. Journal of Virology. [CrossRef]
- Hundie GB, Stalin Raj V, Gebre Michael D, Pas SD, Koopmans MP, Osterhaus AD, et al. (2017). A novel hepatitis B virus subgenotype D10 circulating in Ethiopia. Journal of Viral Hepatitis. [CrossRef]
- IDEAS (2009). Hepatitis B – the facts: –Victorian Government Health Information, Australia”. State of Victoria. 28 July 2009.
- Imperial JC (2010). Chronic hepatitis C in the state prison system: insights into the problems and possible solutions. Expert Review of Gastroenterology and Hepatology. 4 (3): 355–64. [CrossRef]
- Indolfi G, Resti M (2009). Perinatal transmission of hepatitis C virus infection. Journal of Medical Virology. 81 (5): 836–43. [CrossRef]
- International Committee on Taxonomy of Viruses (ICTV) (2002). 61. Retroviridae. National Institutes of Health.
- Irving GJ, Holden J, Yang R, Pope D (2012). Hepatitis A immunisation in persons not previously exposed to hepatitis A. Cochrane Database Syst Rev. 7 (7): CD009051. [CrossRef]
- Ishizaki A, Bouscaillou J, Luhmann N, Liu S, Chua R, Walsh N, et al. (2017). Survey of programmatic experiences and challenges in delivery of hepatitis B and C testing in low- and middle-income countries. BMC Infect Dis. 17(1): 130–140. [CrossRef]
- Jacobsen KH, Koopman JS (2005). The effects of socioeconomic development on worldwide hepatitis A virus seroprevalence patterns. Int J Epidemiol. 34 (3): 600–9. [CrossRef]
- Jacobsen, KH; Wiersma, ST (2010). Hepatitis A virus seroprevalence by age and world region, 1990 and 2005. Vaccine. 28 (41): 6653–6657. [CrossRef]
- Jafari S, Copes R, Baharlou S, Etminan M, Buxton J (2010). Tattooing and the risk of transmission of hepatitis C: A systematic review and meta-analysis. International Journal of Infectious Diseases. 14 (11): e928-40. [CrossRef]
- Jaroszewicz J, Calle Serrano B, Wursthorn K, Deterding K, Schlue J, Raupach R, et al. (2010). Hepatitis B surface antigen (HBsAg) levels in the natural history of hepatitis B virus (HBV)-infection: A European perspective. Journal of Hepatology. [CrossRef]
- Joon, A., Rao, P., Shenoy, S., & Baliga, S. (2015). Prevalence of Hepatitis A virus (HAV) and Hepatitis E virus (HEV) in the patients presenting with acute viral hepatitis. Indian Journal of Medical Microbiology, 33, S102–S105. [CrossRef]
- Kangethe JM, Komu JG, Muturi DN, et al. (2019). Hepatitis B virus infections and associated risk factors among medical waste handlers at the Kenyatta National Hospital, Nairobi Kenya. JMSCR. 07(03):499-506. [CrossRef]
- Kanwal F, Bacon BR (2011). Does treatment alter the natural history of chronic HCV. In Schiffman ML. Chronic Hepatitis C Virus Advances in Treatment, Promise for the Future. Springer Verlag. pp. 103–04.
- Karayiannis P, Thomas HC (2009). Mahy BW, van Regenmortel MH (eds.). Desk Encyclopedia of human and medical virology. Boston: Academic Press. p. 110.
- Kay A, Zoulim F (2007). Hepatitis B virus genetic variability and evolution. Virus Research. [CrossRef]
- Kim A (2016). Hepatitis C virus. Annals of Internal Medicine (Review). 165 (5): ITC33–ITC48. [CrossRef]
- Komas NP, Vickos U, Hübschen JM, Béré A, Manirakiza A, Muller CP, Le Faou A (2013). Cross-sectional study of hepatitis B virus infection in rural communities, Central African Republic. BMC Infectious Diseases. 13: 286. [CrossRef]
- Kulkarni MA, Walimbe AM, Cherian S, Arankalle VA (2009). Full length genomes of genotype IIIA Hepatitis A Virus strains (1995–2008) from India and estimates of the evolutionary rates and ages. Infect. Genet. Evol. 9 (6): 1287–94. [CrossRef]
- Kumar M, Kumar R, Sharma AK, Kumari S. Prevalence of Hepatitis A Virus (HAV) and Hepatitis E Virus (HEV) in the Patients Presenting with Acute Viral Hepatitis (AVH) in a Tertiary Care Hospital. Int J Med Res Prof. 2017; 3(1):297-301. [CrossRef]
- Kury CM et al. (2016). Hepatitis A seroprevalence in public school children in Campos dos Goytacazes, Rio de Janeiro State, Brazil, prior to the introduction of the hepatitis A universal childhood vaccination. Cad. Saúde Pública 2016; 32(11):e00175614. [CrossRef]
- Lai CL, Yuen MF (2007). The natural history and treatment of chronic hepatitis B: a critical evaluation of standard treatment criteria and end points. Annals of Internal Medicine. 147 (1): 58–61. [CrossRef]
- Lam NC, Gotsch PB, Langan RC (2010). Caring for pregnant women and newborns with hepatitis B or C (PDF). American Family Physician. 82 (10): 1225–1259.
- Le Pont F, Hatungimana V, Guiguet M (2003). Assessment of occupational exposure to human immunodeficiency virus and hepatitis C virus in a referral hospital in Burundi, Central Africa. Infect Control Hosp Epidemiol. 24:717-718. [CrossRef]
- Lee C, Gong Y, Brok J, Boxall EH, Gluud C (2006). Hepatitis B immunisation for newborn infants of hepatitis B surface antigen-positive mothers. The Cochrane Database of Systematic Reviews. (2): CD004790. [CrossRef]
- Lerat H, Hollinger FB (2004). Hepatitis C virus (HCV) occult infection or occult HCV RNA detection. The Journal of Infectious Diseases. 189 (1): 3–6. [CrossRef]
- Liaw YF, Brunetto MR, Hadziyannis S (2010). The natural history of chronic HBV infection and geographical differences. Antiviral Therapy. 15: 25–33. [CrossRef]
- Lin YJ, Wu HL, Chen DS, Chen PJ (2012). Hepatitis B virus nucleocapsid but not free core antigen controls viral clearance in mice. Journal of Virology. [CrossRef]
- Locarnini S (2004). Molecular virology of hepatitis B virus”. Seminars in Liver Disease. [CrossRef]
- Lok AS, McMahon BJ (2007). Chronic hepatitis B. Hepatology. 45 (2): 507–39.
- Lombardi A, Mondelli MU (2019). Hepatitis C: Is eradication possible. Liver International. 39 (3): 416–426. [CrossRef]
- Ma Q, Zhang C, Fang S, Zhong P, et al. (2017). Primary esophageal mucosa-associated lymphoid tissue lymphoma: A case report and review of literature. Medicine. 96 (13): e6478. [CrossRef]
- Maheshwari A, Thuluvath PJ (2010). Management of acute hepatitis C. Clinics in Liver Disease. 14 (1): 169–76. [CrossRef]
- Markowski AR, Markowska A, Guzinska-Ustymowicz K (2016). Pathophysiological and clinical aspects of gastric hyperplastic polyps. World Journal of Gastroenterology. 22 (40): 8883–8891. [CrossRef]
- Marx J (2010). Rosen’s emergency medicine: concepts and clinical practice . Philadelphia, PA: Mosby/Elsevier. p. 1154.
- Matheny, SC; Kingery, JE (2012). Hepatitis A. Am Fam Physician. 86 (11): 1027–34, quiz 1010–1012.
- Matsumoto C, Tadokoro K, Fujimura K, Hirakawa S, Mitsunaga S, Juji T (2001). Analysis of HBV infection after blood transfusion in Japan through investigation of a comprehensive donor specimen repository. Transfusion. 41(7):878–884. [CrossRef]
- Mauss, Stefan; Berg, Thomas; Rockstroh, Juergen; Sarrazin, Christoph (2012). Hepatology: A clinical textbook. Germany: Flying publisher. pp. 29–30.
- Mengiste DA, Dirbsa AT, Behailu Hawulte Ayele BH, Hailegiyorgis TT (2021). Hepatitis B virus infection and its associated factors among medical waste collectors at public health facilities in eastern Ethiopia: a facility-based cross-sectional study. BMC Infect Dis. 21:233. [CrossRef]
- Michod RE, Bernstein H, Nedelcu AM (2008). Adaptive value of sex in microbial pathogens”. Infection, Genetics and Evolution. 8 (3): 267–85. [CrossRef]
- Minalyan A, Gabrielyan L, Scott D, Jacobs J, Pisegna JR (2017). The gastric and intestinal microbiome: Role of Proton Pump Inhibitors”. Current Gastroenterology Reports. 19 (8): 42. [CrossRef]
- Mishra RK, Tiwari YK, Pundir S, Saraf G, et al. (2017). A comparison of rapid card test with enzyme-linked immunosorbent assay for the detection of hepatitis B surface antigen [HBsAg] in tertiary care hospital. Research and reviews: A Journal of Microbiology and Virology. 7(3):27-31.
- Mogalli NM, Edrees WH, Al-Awar MS, Alshahethi MA, Al-Shehari WA (2020). Prevalence of intestinal parasitic infections among primary schoolchildren in Kohlan district at Hajjah governorate, Yemen. Al-Razi Univ J Med Sci. 4 (2):34-39.
- Mohd Hanafiah K, Groeger J, Flaxman AD, Wiersma ST (2013). Global epidemiology of hepatitis C virus infection: new estimates of age-specific antibody to HCV seroprevalence. Hepatology. 57 (4): 1333–42. [CrossRef]
- Mücke MM, Backus LI, Mücke VT, Coppola N, Preda CM, Yeh ML, et al. (2018). Hepatitis B virus reactivation during direct-acting antiviral therapy for hepatitis C: a systematic review and meta-analysis. The Lancet. Gastroenterology and Hepatology. 3 (3): 172–180. [CrossRef]
- Murphy TV, Feinstone SM, Bell BP (2013). Hepatitis A vaccines. In: Plotkin SA, OrensteinWA, Offit PA, editors. Vaccines (Sixth Edition). London: W.B. Saunders. p. 183–204.
- Nakano T, Lau GM, Lau GM, Sugiyama M, Mizokami M (2012). An updated analysis of hepatitis C virus genotypes and subtypes based on the complete coding region. Liver International. 32 (2): 339–45. [CrossRef]
- Navvabi N, Khadem Ansari MH, Navvabi A, Chalipa HR, Zitricky F (2021). Comparative assessment of immunochromatography and ELISA diagnostic tests for HBsAg detection in PCR-confirmed HBV infection. Rev Gastroenterol Méx. RGMXEN-741.
- Nelson PK, Mathers BM, Cowie B, Hagan H, Des Jarlais D, Horyniak D, Degenhardt L (2011). Global epidemiology of hepatitis B and hepatitis C in people who inject drugs: results of systematic reviews. Lancet. 378 (9791): 571–83. [CrossRef]
- Nocturne G, Pontarini E, Bombardieri M, Mariette X (2019). Lymphomas complicating primary Sjögren’s syndrome: from autoimmunity to lymphoma”. Rheumatology. Oxford, UK. 60 (8): 3513–3521.
- Obyyah A, et al., (2023). Hepatitis A virus and Helicobacter pylori Infections: Prevalence, knowledge, and preventative practices among school children in Sana’a capital of Yemen. Bachelor Thesis, Medical Laboratory Dep., Al-Razi University. 2023; Pp 22-55.
- Olaru, I. D., Beliz Meier, M., Mirzayev, F., Prodanovic, N., Kitchen, P. J., Schumacher, S. G., & Denkinger, C. M. (2023). Global prevalence of hepatitis B or hepatitis C infection among patients with tuberculosis disease: systematic review and meta-analysis. eClinicalMedicine, 58, 101938. [CrossRef]
- Ozaras R, Tahan V (2009). Acute hepatitis C: prevention and treatment. Expert Review of Anti-Infective Therapy. 7 (3): 351–61. [CrossRef]
- Palewar MS, Joshi S, Choudhary G, Das R, Sadafale A, Karyakarte R. Prevalence of Hepatitis A virus (HAV) and Hepatitis E virus (HEV) in patients presenting with acute viral hepatitis: A 3-year retrospective study at a tertiary care Hospital in Western India. J Family Med Prim Care. 2022 Jun;11(6):2437-2441. Epub 2022 Jun 30. PMCID: PMC9480694. [CrossRef] [PubMed]
- Pepin J, Abou Chakra CN, Pépin E, Nault V, Valiquette L (2014). Evolution of the global burden of viral infections from unsafe medical injections, 2000-2010. PLoS ONE. 9: e99677. [CrossRef]
- Pirinççioğlu AG, Adıgüzel S, Özekinci T (2018). Seropositivity of Hepatitis A in Children Aged 7–14 Years in Diyarbakir Province Center. Med Sci Monit, 2018; 24: 936-943. [CrossRef]
- Pockros P (2011). Novel and combination therapies for Hepatitis C Virus, An Issue of Clinics in Liver Disease. p. 47. [CrossRef]
- Pondé RA (2011). Hidden hazards of HCV transmission. Medical Microbiology and Immunology. 200 (1): 7–11. [CrossRef]
- Pramoolsinsup C (2002). Management of viral hepatitis B. Journal of Gastroenterology and Hepatology. 17 (Suppl): S125–45. [CrossRef]
- Qasem EA, et al., (2022). Occurrence and risk factors of Cryptosporidium parvum among immunocompromised patients in Ibb city-Yemen. Universal J Pharm Res. 2022;6 (3):66-78. [CrossRef]
- Qasem et al., (2020). Frequency of intestinal parasitic infections among schoolchildren in Ibb city-Yemen. Universal J Pharm Res., 2020; 5(2):42-46. [CrossRef]
- Qureshi H, Bile KM, Jooma R, Alam SE, Afridi HU. Prevalence of hepatitis B and C viral infections in Pakistan: findings of a national survey appealing for effective prevention and control measures. East Mediterr Health J. 2010;16 Suppl: S15-23. [CrossRef]
- Ray SC, Thomas DL (2009). Chapter 154: Hepatitis C. In Mandell GL, Bennett, Dolin R (eds.). Mandell, Douglas, and Bennett’s principles and practice of infectious diseases (7th ed.). Philadelphia, PA: Churchill Livingstone.
- Rosen HR (2011). Clinical practice. Chronic hepatitis C infection. The New England Journal of Medicine. 364 (25): 2429–38. [CrossRef]
- Rutherford A, Dienstag JL Greenberger NJ, Blumberg RS, Burakoff R. Viral hepatitis. Current diagnosis & treatment:gastroenterology, hepatology, & endoscopy. 3rd ed. NewYork, NY: McGraw-Hill; 2016.
- Ryan, Kenneth (2010). Sherris Medical Microbiology. McGraw-Hill. pp. 573, 576.
- Sajib S, Zahra FT, Lionakis MS, German NA, Mikelis CM (2018). Mechanisms of angiogenesis in microbe-regulated inflammatory and neoplastic conditions”. Angiogenesis. 21 (1): 1–14. [CrossRef]
- Schillie S, Murphy TV, Sawyer M, Ly K, Hughes E, Jiles R, et al. (2013). CDC guidance for evaluating health-care personnel for hepatitis B virus protection and for administering postexposure management. MMWR. Recommendations and Reports. 62 (RR-10): 1–19.
- Schubert ML, Peura DA (2008). Control of gastric acid secretion in health and disease. Gastroenterology. 134 (7): 1842–60. [CrossRef]
- Sharma M, Golia S, Mehra SK, Jani MV (2019). A comparative evaluation of rapid card test with enzyme-linked immunosorbent assay for the detection of HBsAg among pregnant women in a tertiary care hospital. Int Arch Bio Med Clin Res. 5(1):31-33.
- Shiferaw Y, Abebe T, Mihret A (2011). Hepatitis B virus infection among medical aste handlers in Addis Ababa, Ethiopia. BMC Res Notes. 4:479. [CrossRef]
- Shiukhi S, Elikaei A, Sharifi Z. The Prevalence of Hepatitis A Among Blood Donors in Golestan Province in the Northeast of Iran. Hepat Mon. 2018;18(11):e81609. [CrossRef]
- Smedby KE, Ponzoni M (2017). The aetiology of B-cell lymphoid malignancies with a focus on chronic inflammation and infections”. Journal of Internal Medicine. 282 (5): 360–370. [CrossRef]
- Smith JA, Daniel R (2006). Following the path of the virus: The exploitation of host DNA repair mechanisms by retroviruses. ACS Chemical Biology. 1 (4): 217–26. [CrossRef]
- Tang H, Oishi N, Kaneko S, Murakami S (2006). Molecular functions and biological roles of hepatitis B virus x protein. Cancer Science. [CrossRef]
- Tarantola A, Abiteboul D, Rachline A (2006). Infection risks accidental exposure to blood or body fluids in health care workers: a review of pathogens transmitted in published cases. Am J Infect Control. 34:367-375. [CrossRef]
- Terrault NA, Bzowej NH, Chang KM, Hwang JP, Jonas MM, Murad MH (2016). AASLD guidelines for treatment of chronic hepatitis B. Hepatology. 63 (1): 261–83. [CrossRef]
- Thomas SL, Newell ML, Peckham CS, Ades AE, Hall AJ (February 1998). A review of hepatitis C virus (HCV) vertical transmission: risks of transmission to infants born to mothers with and without HCV viraemia or human immunodeficiency virus infection. International Journal of Epidemiology. 27 (1): 108–17. [CrossRef]
- TSRI - News and Publications (2009). Retrieved 3 January 2009.
- Uddin MS, Islam MN, Khan MEU, Yeasmin S, Ahmed F, Amiruzzaman M (2017). Frequency of hepatitis B and C viral infection among the medical waste handlers. Bangladesh J Infect Dis. 4(1):3-9. [CrossRef]
- Vitral CL, Ospina FL, Solange Artimos S, et al. (2012) Declining prevalence of hepatitis A virus antibodies among children from low socioeconomic groups reinforces the need for the implementation of hepatitis A vaccination in Brazil. Mem Inst Oswaldo Cruz, Rio de Janeiro. 107(5): 652-658. [CrossRef]
- Wagner AD, Syn NL, Moehler M, et al. (2017). Chemotherapy for advanced gastric cancer. The Cochrane Database of Systematic Reviews. 8: CD004064. [CrossRef]
- Westbrook RH, Dusheiko G (2014). Natural history of hepatitis C. Journal of Hepatology. 61 (1): S58-68. [CrossRef]
- Westermann C, Peters C, Lisiak B, Lamberti M, Nienhaus A (2015). The prevalence of hepatitis C among healthcare workers: a systematic review and meta-analysis. Occup Environ Med. 72(12):880–888. [CrossRef]
- Wheeler C, Vogt TM, Armstrong GL, et al. (2005). An outbreak of hepatitis A associated with green onions. N. Engl. J. Med. 353 (9): 890–897. [CrossRef]
- Wilkins T, Malcolm JK, Raina D, Schade RR (2010). Hepatitis C: diagnosis and treatment (PDF). American Family Physician. 81 (11): 1351–1357.
- Wong F, Pai R, Van Schalkwyk J, Yoshida EM (2014). Hepatitis B in pregnancy: a concise review of neonatal vertical transmission and antiviral prophylaxis. Annals of Hepatology. 13 (2): 187–95. [CrossRef]
- Wong T, Lee SS (2006). Hepatitis C: A review for primary care physicians. CMAJ. 174 (5): 649–59. [CrossRef]
- World Health Organization (WHO) (2011). Hepatitis C. June 2011. Archived from the original on 2011-07-12.
- World Health Organization (WHO) (2012). Prevention and control of viral hepatitis infection: framework for global action; 2012. Available from: http://www.who.int/hiv/pub/hepatitis/Framework/en/.
- World Health Organization (WHO) (2013). Fact Sheet: Hepatitis C. www.who.int.
- World Health Organization (WHO) (2014). Hepatitis B Fact sheet N°204. who.int. July 2014. Archived from the original on 9 November 2014.
- World Health Organization (WHO) (2014). Hepatitis B Archived 9 November 2014 at the Wayback Machine.
- World Health Organization (WHO) (2015). Hepatitis B. www.who.int. Archived from the original on 10 July 2015.
- World Health Organization (WHO) (2016). Hepatitis C fact sheet N°164. July 2015. Archived from the original on 31 January 2016.
- World Health Organization (WHO) (2019). Hepatitis C questions and answers for health professionals. www.cdc.gov. 2 July 2019.
- World Health Organization (WHO) (2019). Hepatitis C. Archived from the original on 2020-05-26.
- World Health Organization (WHO) (2021). Global progress report on HIV, viral hepatitis and sexually transmitted infections, 2021. www.who.int.
- World Health Organization (WHO) (2022). Hepatitis A. https://www.who.int/news-room/fact-sheets/detail/hepatitis-a.
- World Health Organization (WHO). Hepatitis B”. www.who.int.
- World Health Organization, (2013). Archived from the original on 21 February 2014. Retrieved 20 February 2022.
- Wymer G (2019). Hepatitis A numbers down in Kentucky; health officials still urge vaccination”. WKYT.
- Yu JM, Li LL, Zhang CY, Lu S, et al., (2016) A novel hepatovirus identified in wild woodchuck Marmota himalayana. Sci Rep. 6:22361. [CrossRef]
- Yu ML, Chuang WL (2009). Treatment of chronic hepatitis C in Asia: when East meets West. Journal of Gastroenterology and Hepatology. 24 (3): 336–45. [CrossRef]
- Zajacova A, Dowd JB, Aiello AE (2009). Socioeconomic and race/ethnic patterns in persistent infection burden among US adults. Journals of Gerontology Series A: Biomedical Sciences and Medical Sciences. 64(2): 272-279. [CrossRef]
- Zoulim F (2006). New nucleic acid diagnostic tests in viral hepatitis. Semin. Liver Dis. 26 (4): 309–317. [CrossRef]
Figure 1.
Distribuation of collecetd samples from study area concerining years.
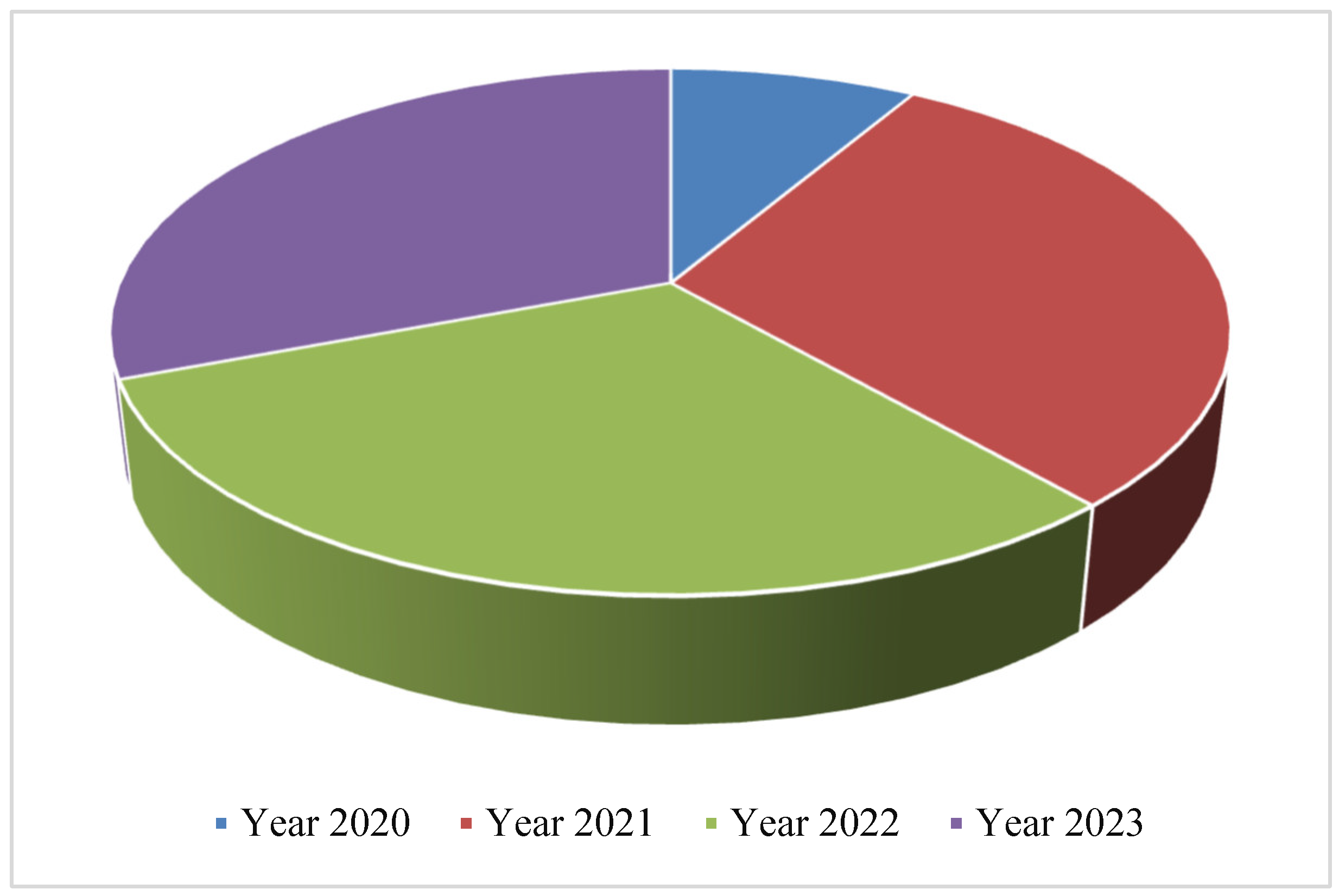
Figure 2.
Distribuation of collecetd samples from study area concerining districts.
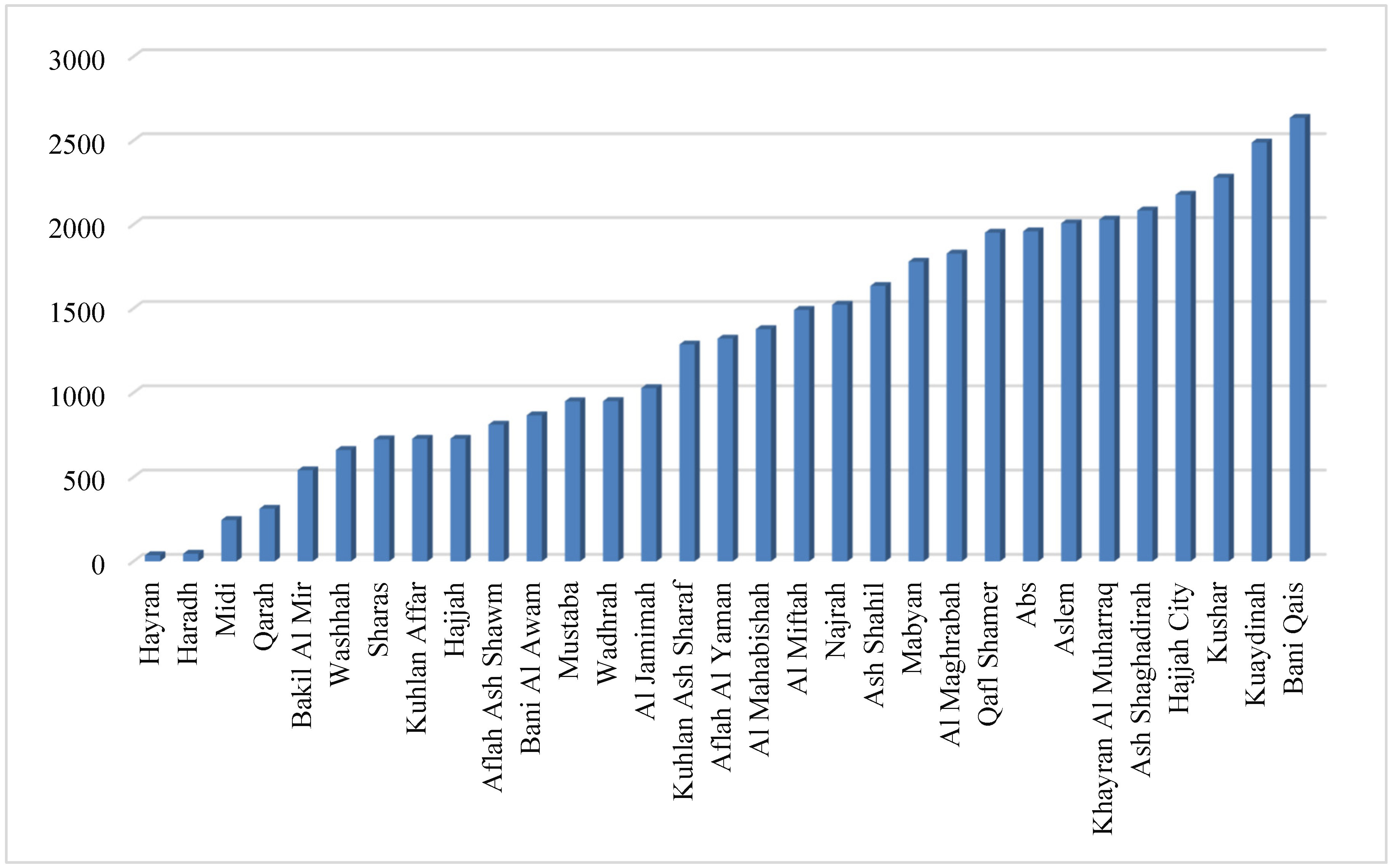
Figure 3.
Distribuation of collecetd samples from study area concerining months.
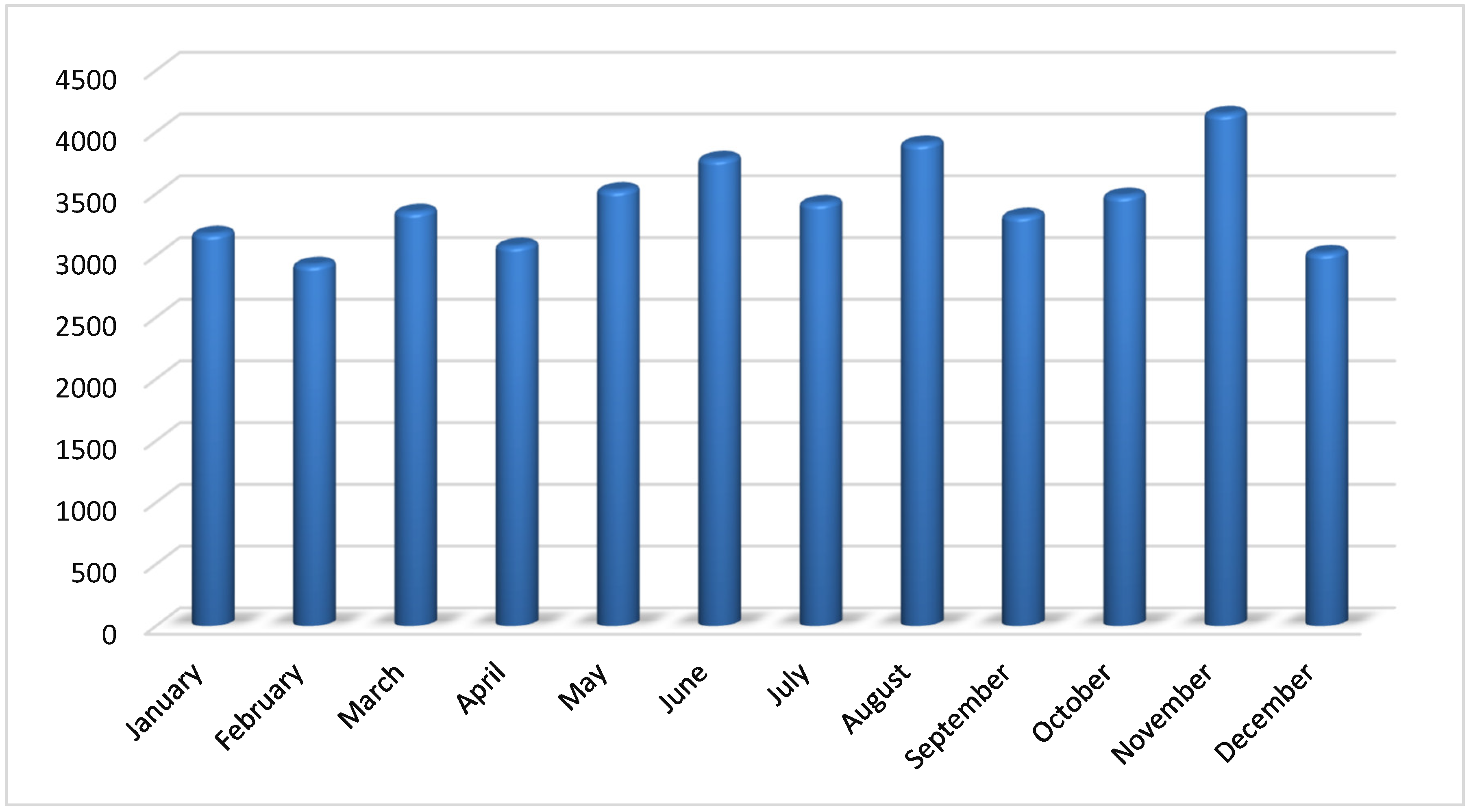
Figure 4.
Distribuation of collecetd samples from study area concerining season.
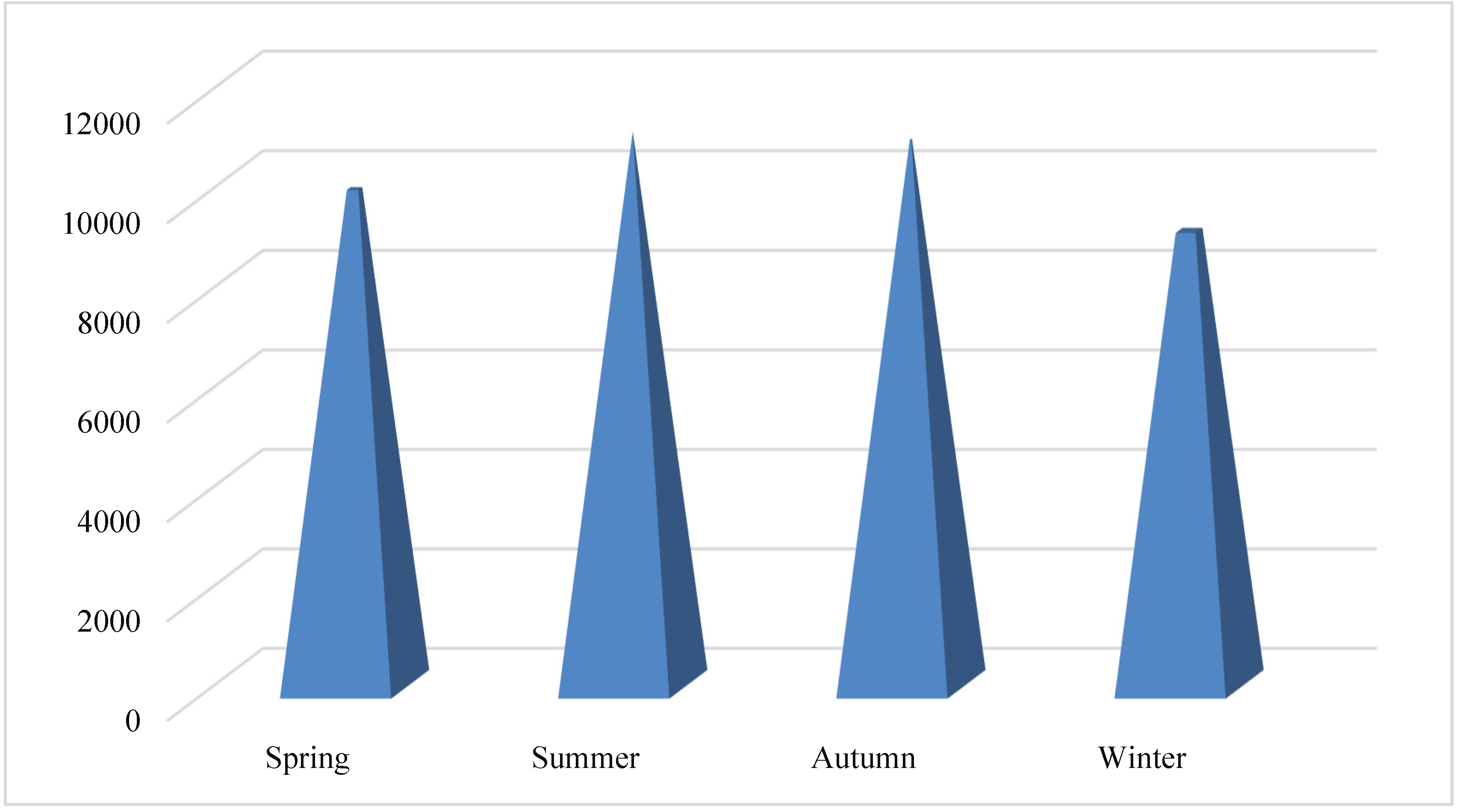
Figure 5.
Frequency of Hepatitis A, E, B, C in Hajjah governorate between 2020-2023.
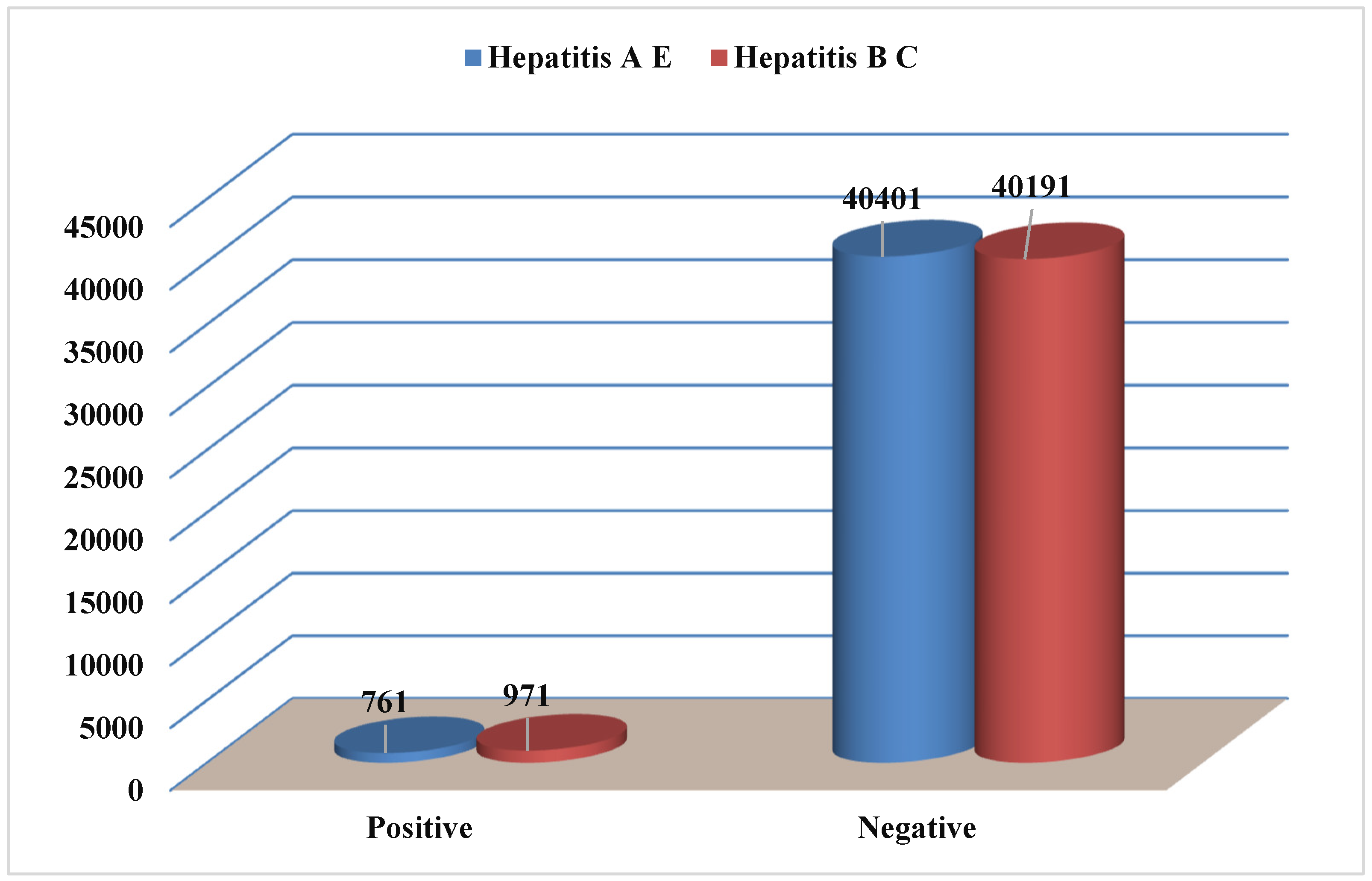
Figure 6.
Frequency of Hepatitis A, E, B, C concerining years of infection.
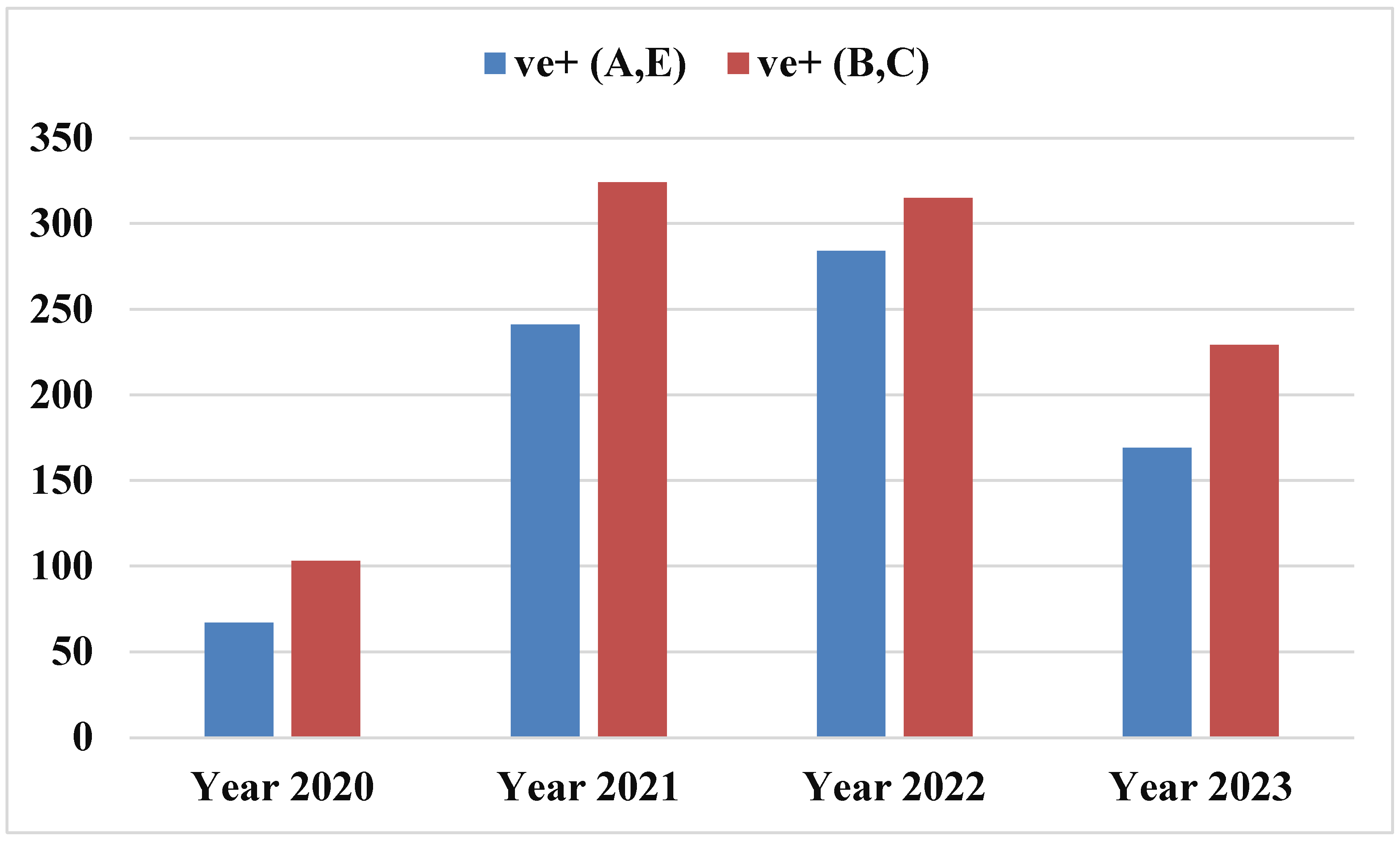
Figure 7.
Frequency of Hepatitis A, E, B, C concerining district name.
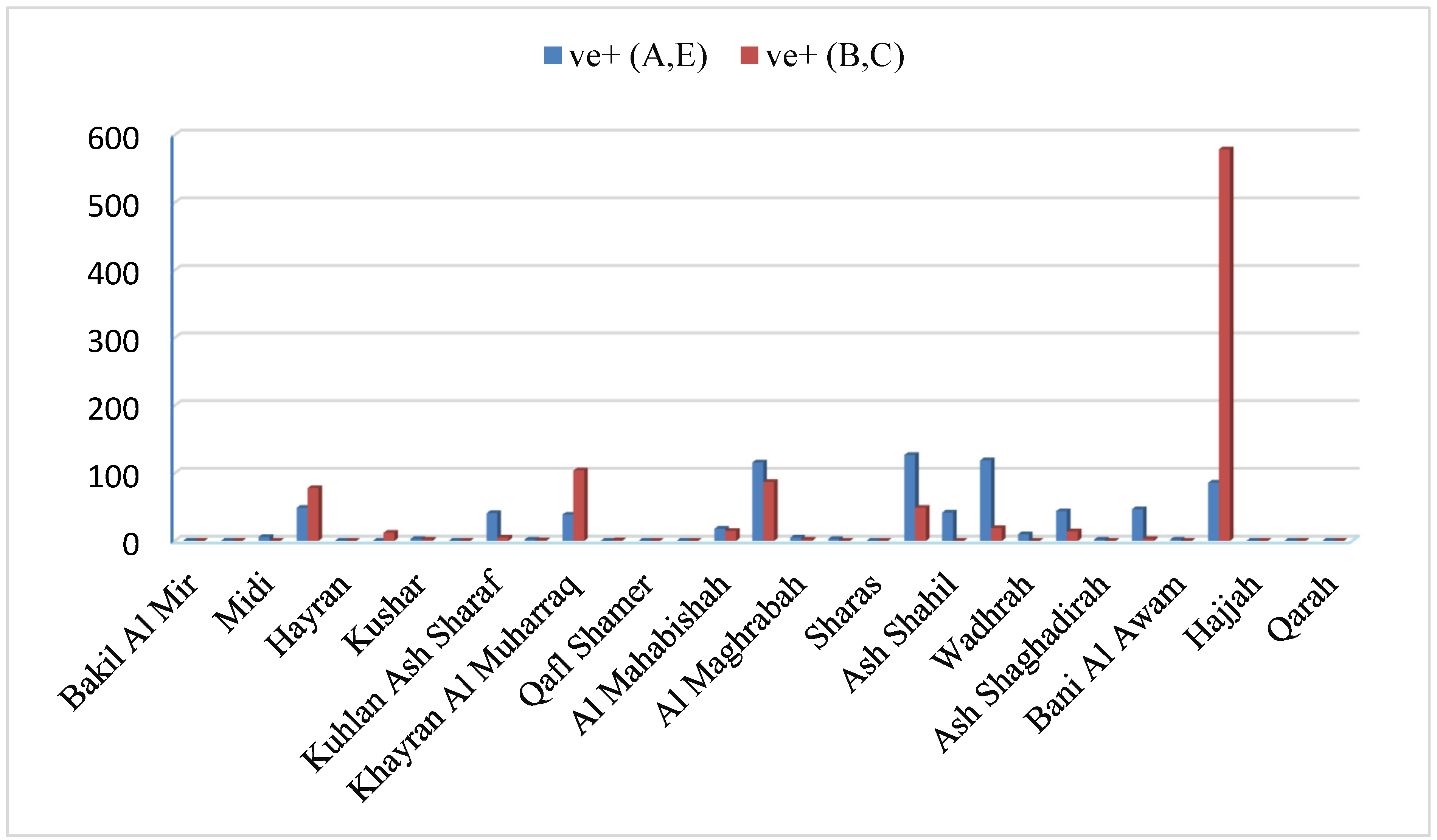
Figure 8.
Frequency of Hepatitis A, E, B, C concerining months.
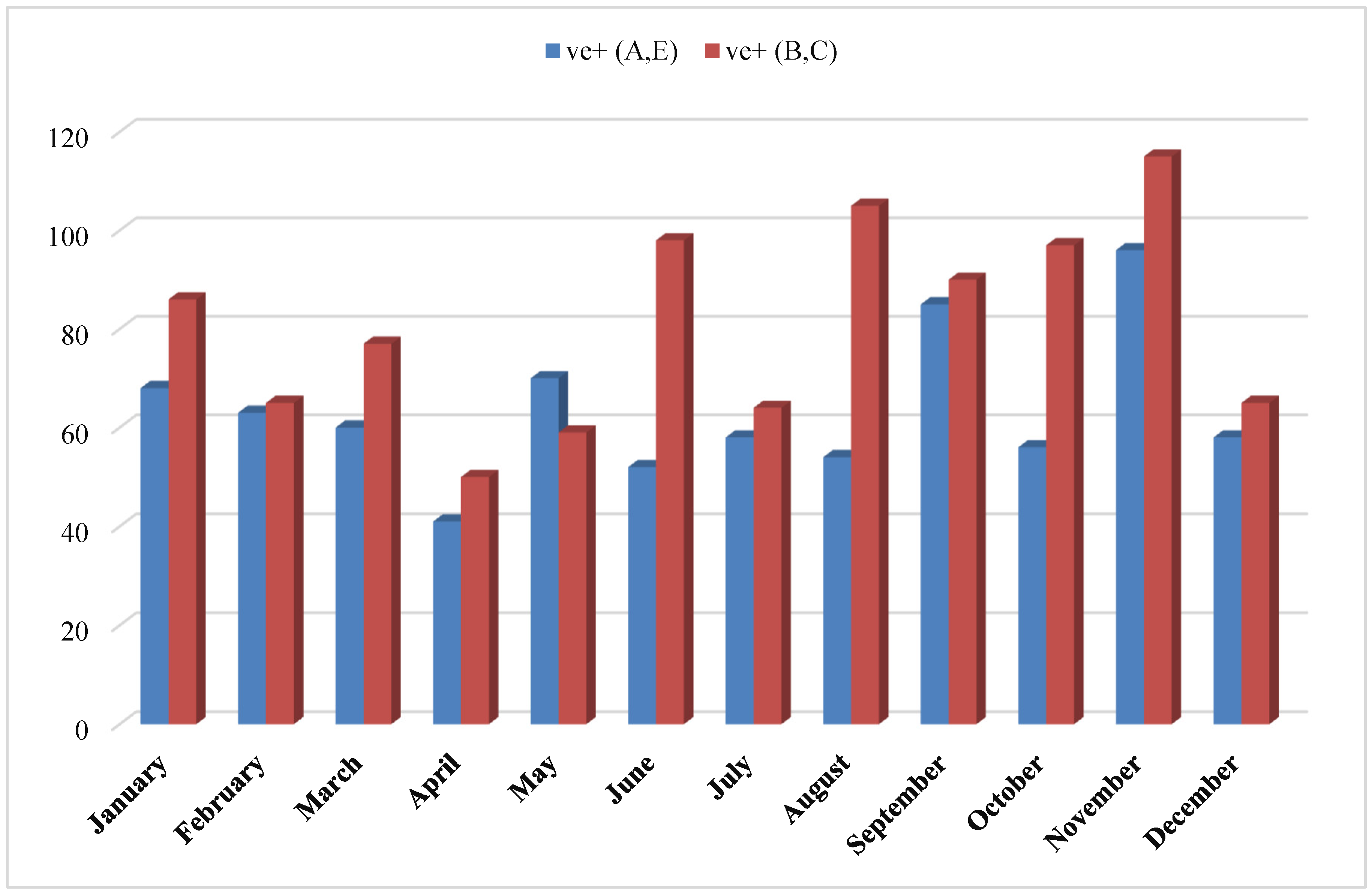
Figure 9.
Frequency of Hepatitis A, E, B, C concerining season.


Table 1.
Distribuation of collecetd samples from study area concerining years.
| Years | No. | Rate (%) |
|---|---|---|
| 2020 | 3499 | 8.5 |
| 2021 | 12380 | 30.1 |
| 2022 | 12610 | 30.6 |
| 2023 | 12673 | 30.8 |
| Total | 41162 | 100 |
Table 2.
Distribuation of collecetd samples from study area concerining districts.
| No. | Rate (%) | |
|---|---|---|
| Hayran | 36 | 0.1 |
| Haradh | 45 | 0.1 |
| Midi | 245 | 0.6 |
| Qarah | 312 | 0.8 |
| Bakil Al Mir | 540 | 1.3 |
| Washhah | 660 | 1.6 |
| Sharas | 723 | 1.8 |
| Kuhlan Affar | 727 | 1.8 |
| Hajjah | 727 | 1.8 |
| Aflah Ash Shawm | 811 | 2.0 |
| Bani Al Awam | 866 | 2.1 |
| Mustaba | 949 | 2.3 |
| Wadhrah | 950 | 2.3 |
| Al Jamimah | 1027 | 2.5 |
| Kuhlan Ash Sharaf | 1286 | 3.2 |
| Aflah Al Yaman | 1321 | 3.3 |
| Al Mahabishah | 1377 | 3.4 |
| Al Miftah | 1491 | 3.7 |
| Najrah | 1522 | 3.8 |
| Ash Shahil | 1634 | 4.0 |
| Mabyan | 1778 | 4.4 |
| Al Maghrabah | 1827 | 4.5 |
| Qafl Shamer | 1951 | 4.8 |
| Abs | 1959 | 4.8 |
| Aslem | 2007 | 5.0 |
| Khayran Al Muharraq | 2029 | 5.0 |
| Ash Shaghadirah | 2083 | 5.1 |
| Hajjah City | 2177 | 5.4 |
| Kushar | 2279 | 5.6 |
| Kuaydinah | 2488 | 6.1 |
| Bani Qais | 2635 | 6.5 |
Table 3.
Distribuation of collecetd samples from study area concerining months.
| Month | No. | Rate (%) |
|---|---|---|
| January | 3177 | 7.7 |
| February | 2926 | 7.1 |
| March | 3355 | 8.2 |
| April | 3080 | 7.5 |
| May | 3530 | 8.6 |
| June | 3783 | 9.2 |
| July | 3425 | 8.3 |
| August | 3908 | 9.5 |
| September | 3323 | 8.1 |
| October | 3486 | 8.5 |
| November | 4148 | 10.1 |
| December | 3021 | 7.3 |
Table 4.
Distribuation of collecetd samples from study area concerining season.
| Season | No. | Rate (%) |
|---|---|---|
| Spring | 9965 | 24.2 |
| Summer | 11116 | 27.0 |
| Autumn | 10957 | 26.6 |
| Winter | 9124 | 22.2 |
Table 5.
Frequency of Hepatitis A, E, B, C in Hajjah governorate between 2020-2023.
| Hepatitis type | Positive (ve+) | Negative (ve-) | Total | ||
|---|---|---|---|---|---|
| No, | % | No. | % | ||
| Hepatitis A and E | 761 | 1.85 | 40401 | 98.15 | 41162 |
| Hepatitis B and C | 971 | 2.36 | 40191 | 97.64 | 41162 |
Table 6.
Frequency of Hepatitis A, E, B, C concerining year of infection.
| Years | No. (%) | HAV and HEV | P value | Hepatitis B and C | P value | ||
|---|---|---|---|---|---|---|---|
| ve+ | ve- | ve+ | ve- | ||||
| 2020 | 3499(8.5) | 67(1.9) | 3432(98.1) | 0.000 | 103(2.9) | 3432(97.1) | 0.000 |
| 2021 | 12380(30.1) | 241(1.9) | 12139(98.1) | 324(2.6) | 12139(97.4) | ||
| 2022 | 12610(30.6) | 284(2.3) | 12326(97.7) | 315(2.5) | 12326(97.5) | ||
| 2023 | 12673(30.8) | 169(1.3) | 12504(98.7) | 229(1.8) | 12504(98.2) | ||
Table 7.
Frequency of Hepatitis A, E, B, C concerining distirict name.
| District name | Hepatitis A and E | P value | Hepatitis B and C | P value | ||
|---|---|---|---|---|---|---|
| ve+ | ve- | ve+ | ve- | |||
| Bakil Al Mir | 0(0.0) | 540(100) | 0.000 | 0(0.0) | 540(100) | 0.000 |
| Haradh | 0(0.0) | 45(100) | 0(0.0) | 45(100) | ||
| Midi | 6(2.4) | 242(97.6) | 0(0.0) | 248(100) | ||
| Abs | 49(2.5) | 1940(97.5) | 78(3.9) | 1911(96.1) | ||
| Hayran | 0(0.0) | 36(100) | 0(0.0) | 36(100) | ||
| Mustaba | 0(0.0) | 952(100) | 12(1.3) | 940(98.7) | ||
| Kushar | 3(0.1) | 2277(99.9) | 2(0.1) | 2278(99.9) | ||
| Al Jamimah | 0(0.0) | 1027(100) | 0(0.0) | 1027(100) | ||
| Kuhlan Ash Sharaf | 41(3.2) | 1257(96.8) | 5(0.4) | 1293(99.6) | ||
| Aflah Ash Shawm | 2(0.2) | 809(99.8) | 1(0.1) | 810(99.9) | ||
| Khayran Al Muharraq | 39(1.9) | 2030(98.1) | 104(5.0) | 1965(95) | ||
| Aslem | 0(0.0) | 2007(100) | 1(0.01) | 2006(99.09) | ||
| Qafl Shamer | 0(0.0) | 1951(100) | 0(0.0) | 1951(100) | ||
| Aflah Al Yaman | 0(0.0) | 1321(100) | 0(0.0) | 1321(100) | ||
| Al Mahabishah | 18(1.3) | 1365(98.7) | 15(1.1) | 1368(98.9) | ||
| Al Miftah | 116(7.5) | 1433(92.5) | 87(5.6) | 1462(94.4) | ||
| Al Maghrabah | 5(0.3) | 1822(99.7) | 2(0.1) | 1825(99.9) | ||
| Kuhlan Affar | 3(0.4) | 726(99.6) | 0(0.0) | 729(100) | ||
| Sharas | 0(0.0) | 723(100) | 0(0.0) | 723(100) | ||
| Mabyan | 127(6.9) | 1712(93.1) | 49(2.7) | 1790(97.3) | ||
| Ash Shahil | 42(2.5) | 1607(97.5) | 0(0.0) | 1649(100) | ||
| Kuaydinah | 119(4.7) | 2420(95.3) | 19(0.7) | 2520(99.3) | ||
| Wadhrah | 10(1.1) | 942(98.9) | 0(0.0) | 952(100) | ||
| Bani Qais | 44(1.6) | 2630(98.9) | 14(0.5) | 2660(99.5) | ||
| Ash Shaghadirah | 2(0.1) | 2081(99.9) | 0(0.0) | 2083(100) | ||
| Najrah | 47(3.0) | 1500(97) | 3(0.2) | 1544(99.8) | ||
| Bani Al Awam | 2(0.2) | 864(99.8) | 0(0.0) | 866(100) | ||
| Hajjah city | 86(3.4) | 2443(96.6) | 579(22.9) | 1950(77.1) | ||
| Hajjah | 0(0.0) | 727(100) | 0(0.0) | 727(100) | ||
| Washhah | 0(0.0) | 660(100) | 0(0.0) | 660(100) | ||
| Qarah | 0(0.0) | 312(100) | 0(0.0) | 312(100) | ||
Table 8.
Frequency of Hepatitis A, E, B, C concerining months.
| Month | No. (%) | Hepatitis A E | P value | Hepatitis B C | P value | ||
|---|---|---|---|---|---|---|---|
| ve+ | ve- | ve+ | ve- | ||||
| January | 3177(7.7) | 68(2.1) | 3109(97.9) | 0.000 | 86(2.7) | 3091(97.3) | 0.000 |
| February | 2926(7.1) | 63(2.2) | 2863(97.8) | 65(2.2) | 2861(97.8) | ||
| March | 3355(8.2) | 60(1.8) | 3295(98.2) | 77(2.3) | 3278(97.7) | ||
| April | 3080(7.5) | 41(1.3) | 3039(98.7) | 50(1.6) | 3030(98.4) | ||
| May | 3530(8.6) | 70(2.0) | 3460(98.0) | 59(1.7) | 3471(98.3) | ||
| June | 3783(9.2) | 52(1.4) | 3731(98.6) | 98(2.6) | 3685(97.4) | ||
| July | 3425(8.3) | 58(1.7) | 3367(98.3) | 64(1.9) | 3361(98.1) | ||
| August | 3908(9.5) | 54(1.4) | 3854(98.6) | 105(2.7) | 3803(97.3) | ||
| September | 3323(8.1) | 85(2.6) | 3238(97.4) | 90(2.7) | 3233(97.3) | ||
| October | 3486(8.5) | 56(1.6) | 3430(98.4) | 97(2.8) | 3389(97.2) | ||
| November | 4148(10.1) | 96(2.3) | 4052(97.7) | 115(2.8) | 4033(97.2) | ||
| December | 3021(7.3) | 58(1.9) | 2963(98.1) | 65(2.2) | 2956(97.8) | ||
P value < 0.05 (statistically significant).
Table 9.
Frequency of Hepatitis A, E, B, C concerining season.
| Season | No. | Rate (%) | Hepatitis A E | P value | Hepatitis B C | P value | ||
|---|---|---|---|---|---|---|---|---|
| ve+ | ve- | ve+ | ve- | |||||
| Spring | 9965 | 24.2 | 171(1.7) | 9794(98.3) | 0.000 | 186(1.9) | 9779(98.1) | 0.000 |
| Summer | 11116 | 27.0 | 164(1.5) | 10952(98.5) | 267(2.4) | 10849(97.6) | ||
| Autumn | 10957 | 26.6 | 237(2.2) | 10720(97.8) | 302(2.6) | 10655(97.2) | ||
| Winter | 9124 | 22.2 | 189(2.1) | 8935(97.9) | 216(2.4) | 8908(97.6) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



