
Submitted:
21 June 2024
Posted:
22 June 2024
You are already at the latest version
Abstract
Lipid-lowering therapy (LLT) is a cornerstone of atherosclerotic cardiovascular disease prevention. Although LLT might lead to different reductions in low-density lipoprotein cholesterol (LDL-C) levels in women and men, LLT diminishes cardiovascular risk equally effectively in both sexes. Despite similar LLT efficacy, the use of high-intensity statin, ezetimibe, and proprotein convertase subtilisin/kexin type 9 inhibitors is lower in women compared to men. Women achieve the guideline-recommended LDL-C levels less often than men. Greater cholesterol burden is particularly prominent in women with familial hypercholesterolemia. In clinical practice, women and men with dyslipidemia present with different cardiovascular risk profiles and disease manifestations. The concentrations of LDL-C, lipoprotein(a) and other blood lipids differ between women and men over a lifetime. Dissimilar levels of LLT’s target molecules partially result from sex-specific hormonal and genetic determinants of lipoprotein metabolism. Hence, to evaluate a potential need for sex-specific LLT, this comprehensive review (i) describes the impact of sex on lipoprotein metabolism and lipid profile, (ii) highlights sex differences in cardiovascular risk among patients with dyslipidemia, (iii) presents recent, up-to-date clinical trial and real-world data on LLT efficacy and safety in women, and (iv) discusses diverse medical needs of women and men with dyslipidemia and increased cardiovascular risk.
Keywords:
atherosclerotic cardiovascular disease
; cholesterol
; dyslipidemia
; lipid-lowering therapy
; women
; sex differences
1. Introduction
Atherosclerotic cardiovascular disease (ASCVD) remains the leading cause of death in women and men worldwide [1]. Given the fundamental role of blood lipoproteins in atherosclerotic plaque formation, hypercholesterolemia and hypertriglyceridemia substantially contribute to ASCVD development and progression [2]. Therefore, lipid-lowering therapy (LLT) is a mainstay of ASCVD prevention and treatment [3]. In women and men with increased low-density lipoprotein cholesterol (LDL-C) levels, according to the patient’s global cardiovascular risk, currently recommended treatment regimens comprise [high-intensity] statins, ezetimibe, bempedoic acid, and proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors [4,5]. In addition, novel therapeutic targets such as lipoprotein(a) [Lp(a)] [6], and novel drug classes, such as antisense oligonucleotides and small interfering ribonucleic acids, are intensively studied [7,8].
Real-world data demonstrate that women less often receive the guideline-recommended LLT [9,10,11,12], and thus, do not benefit from ASCVD prevention strategies equally to men. Sex differences exist in lipoprotein metabolism, most likely due to sex-specific hormonal and genetic determinants [13,14]. The potential mechanisms leading to the different female and male lipid profiles [15], especially among patients with familial hypercholesterolemia (FH) [16], are still a matter of discussion. Furthermore, women have additional risk factors related to reproductive health and psychosocial status that are not present in men [17,18]. Among patients with dyslipidemia, sex disparities are also observed in LDL-C goal attainment [19,20,21], LLT-related side effects [22], adherence to LLT [23,24], perception of dyslipidemia and cardiovascular risk, as well as patient-physician relationship [25]. Hence, sex can affect the diagnostic process, treatment course, and clinical outcome. Importantly, differences may be driven not only by biological but also psychosocial characteristics. Therefore, along with sex, the significance of gender cannot be neglected [17,18].
Aiming to evaluate a potential need for sex-specific LLT, this comprehensive review (i) describes the impact of sex on lipoprotein metabolism, (ii) considers sex differences in lipid profiles, (iii) characterizes cardiovascular risk and disease manifestation in female patients with dyslipidemia in comparison to men, (iv) discusses LLT strategies along with their efficacy and safety in women based on data from clinical trials and real-world studies, and (v) proposes solutions to overcome challenges faced in clinical practice due to diverse medical needs of women and men with dyslipidemia and increased cardiovascular risk.
2. Sex Differences in Lipoprotein Metabolism
2.1. Role of Sex Hormones
ASCVD develops 7-10 years later in women compared to men [26]. Cardiovascular risk in women increases following menopause, accompanied by a decline in the production and concentration of estrogens, the primary female sex hormones. Estrogens exert a cardioprotective effect, and hence, contribute to sex differences in cardiovascular risk [27]. Among their multi-faceted actions, estrogens seem to affect the lipid profile and its atherogenicity [13,14]. In the following sections, we will discuss the basic effects of sex hormones on molecular mechanisms found in humans, as well as tissue and animal models, which are summarized in Figure 1.
2.1.1. Estrogens and Very Low Density-Lipoproteins
Estrogens affect triglyceride-rich very low density-lipoprotein (VLDL-TG) metabolism. First, estrogen-related receptor alpha (ERRα), a downstream target of estrogen receptor alpha (ERα), upregulates apolipoprotein B-100 (apoB-100) and microsomal triglyceride transfer protein (MTP) expression. Consequently, ERRα increases VLDL-TG production and secretion in the liver [28]. Correspondingly, in the presence of cholesteryl ester transfer protein (CETP), estrogens enhance small heterodimer partner and protein disulfide isomerase expression, leading to increased VLDL-TG production. Of note, the effect of estrogens is mediated not only via ERα, but also via the G protein-coupled estrogen receptor (GPER) [29].
Women exhibit a higher VLDL-TG secretion rate, which along with a lower VLDL-apoB-100 secretion rate suggests that women secrete fewer but TG-richer VLDL of lower atherogenicity, as has been shown with stable isotope kinetic tracer studies [30,31]. Nevertheless, the potential effect on circulating VLDL-TG levels is counteracted by an accelerated clearance rate in women [32]. Considering the relationship with sex hormones, in postmenopausal women on hormone replacement therapy (HRT), the administration of oral estrogen increases VLDL-TG production, whereas oral progestin and transdermal estrogen stimulate VLDL-TG clearance [14,33]. However, no changes in VLDL-TG and VLDL-apoB-100 kinetics occur during the menstrual cycle [34].
2.1.2. Estrogens and Low Density-Lipoproteins
Estrogens play a key role in LDL-C metabolism. Estrogens increase LDL receptor (LDL-R) expression and activity on the liver surface via ERα, leading to increased LDL-C uptake and subsequent decline in circulating LDL-C levels [35,36,37].
The effect on the LDL-R is also mediated by the impact of estrogens on the expression and function of proprotein convertase subtilisin/kexin type 9 (PCSK9). Following binding to the LDL-R extracellular domain, PCSK9 triggers LDL-R endocytosis and lysosomal degradation through the clathrin trafficking pathway [38,39]. Overall, higher circulating PCSK9 levels are present in women compared to men, as well as in postmenopausal compared to premenopausal women [40]. In addition, circulating PCSK9 levels differ between menstrual cycle phases, with an inverse correlation between PCSK9 and estrogen levels [41,42]. However, this association is observed only for endogenous estrogens, as HRT has no effect on PCSK9 levels in postmenopausal women [43,44]. Furthermore, an in vitro study revealed that the phytoestrogen, resveratrol, suppresses PCSK9 proximal promoter via ERα, resulting in lower PCSK9 production [45]. Conversely, other studies suggested that the impact of estrogens on PCSK9 production through genetic signaling is nonsignificant, on the contrary to the impact on PCSK9 clearance [40,46,47].
Several studies examined functional modifications of PCSK9 on cell lines. First, estrogens inhibit the phosphorylation of secreted PCSK9, impeding its interaction with LDL-R [46]. Furthermore, estrogens block PCSK9 internalization and alter clathrin distribution, resulting in the inhibition of LDL-R endocytosis. Interestingly, estrogens additionally enhance LDL-C uptake in the presence of extracellular PCSK9. Of note, both effects are mediated via GPER [48,49]. Conversely, a complex relationship occurs between estrogens and PCSK9 distribution, as PCSK9-deficient male mice exhibit higher LDL-R levels on the liver surface compared to female mice [47]. Correspondingly, in hepatic cells treated with hyperlipidemic serum of postmenopausal women, estrogens reduce LDL-C uptake, and thus, diminish hepatic lipid accumulation. This effect is mediated by sterol regulatory element-binding protein-1 (SREBP-1), the expression of which is promoted by ERα [50].
Moreover, estrogens influence lipoprotein size, as ERRα stimulates phospholipase A2 group XII B (Pla2g12b) expression. Mutation in the Pla2g12b gene reduces the levels of apoB and large lipoproteins but significantly increases the concentration of small LDL-like particles [13,51]. Correspondingly, certain variations in the ERα gene are associated with higher levels of small LDL particles of greater atherogenicity [52,53], accompanied by increased risk of myocardial infarction (MI) [54] and aortic valve stenosis [55].
The anti-atherogenic effects of estrogens are also exerted independent of hepatic LDL-C metabolism. In the presence of estrogens, SREBP-1 reduces LDL-C uptake in cholesterol-loaded macrophages, and hence, inhibits foam cell formation. Importantly, estrogens increase the sensitivity to statin treatment, as the combination of estrogen with rosuvastatin reduces lipid accumulation in foam cells compared to statin monotherapy, as well as counteracts atherosclerotic plaque progression [50]. Estrogen-induced reduction in total cholesterol (TC) levels and inhibition of atherosclerotic plaque formation is mediated by ERα [56]. Considering other receptors, scavenger receptor class B type 1 (SR-B1) enhances LDL transcytosis in coronary endothelial cells, as investigated using a novel assay [57]. This effect is opposed by estrogens, which inhibit SR-B1 expression via GPER [58]. Noteworthy, the anti-atherogenic effect of GPER was proposed as ligand-independent, indicating its crucial role in maintaining cardiovascular health [59]. Finally, although no differences in LDL oxidation occur during the menstrual cycle [60], a protective effect of estrogens against LDL oxidation was proposed [61].
2.1.3. Estrogens and High-Density Lipoproteins
Estrogens are involved in high density-lipoprotein cholesterol (HDL-C) metabolism and reverse cholesterol transport. Estrogens reduce concentrations of hepatic SR-B1, impeding HDL-C uptake and subsequently increasing circulating HDL-C levels [62]. The effect of estrogens on hepatic SR-B1 expression is likely post-transcriptional, as authors have reported no [63] or a lower decrease [58] in the concentration of messenger ribonucleic acid for SR-B1 compared to SR-B1 protein level. Of note, the decline in SR-B1 levels was linked to an estrogen-associated increase in LDL-R activity [63].
Considering further aspects of reverse cholesterol transport, administration of oral estrogen and progestin to postmenopausal women increases the expression of adenosine triphosphate-binding cassette transporter A1 (ABCA1), a protein involved in HDL-C efflux, in leukocytes [64]. Similarly, estrogens enhance cholesterol efflux from vascular smooth muscle cells to apoA-I and HDL through the upregulation of ABCA1 and ABCG1 [65]. However, ABCA1-specific cholesterol efflux capacity increases in early menopause [66]. Furthermore, premenopausal women have higher CETP levels, which positively correlate with estrogen levels [67]. Interestingly, CETP is necessary for estrogen to enhance HDL-C efflux [68]. Moreover, the activity of lecithin:cholesterol acyltransferase (LCAT), a protein participating in HDL-C efflux, increases in postmenopausal women on HRT [69]. Estrogens also promote the synthesis of apoA-I, but not apoA-II, with the former being a cofactor for LCAT, and the latter inhibiting lipoprotein lipase activity [70,71]. In addition, estrogens inhibit hepatic lipase activity, possibly contributing to higher levels of HDL2, particles of lower density than HDL3, in women [72]. Moreover, HDL-associated estrogen fatty acyl esters enhance cholesterol efflux from macrophages via ERs and SR-B1 [73]. However, the latter results could not be confirmed in a bigger cohort of pre- and postmenopausal women and men, in which estrogens did not affect the activity of CETP, LCAT, or phospholipid transfer protein [74].
2.1.4. Estrogens and Cholesterol Metabolism
Estrogens are involved in cholesterol synthesis and absorption [14]. SREBPs promote a cholesterol synthesis pathway involving 3-hydroxy-3-methyl-glutaryl-coenzyme A (HMG-CoA) reductase, the main target of statins. As demonstrated in animal models, females have lower activity and concentrations of both SREBPs and HMG-CoA reductase than males, which is associated with the presence of estrogens [14,75]. Conversely, estrogens upregulate the expression of Niemann-Pick C1-like protein 1, a target of ezetimibe, promoting increased cholesterol absorption in the intestine [76]. In addition, ERRα enhances apoA-IV expression, and thus, participates in the regulation of intestinal lipid absorption [77].
2.2. Role of Genetics
Along with sex hormones, lipoprotein metabolism is altered by an individual’s genetic component. In hyperlipidemic mice, both gonadal and chromosomal sex affect the hepatic transcriptome and the expression of genes involved in fatty acid metabolism. Interestingly, following statin treatment, a compensatory overexpression of genes involved in cholesterol synthesis is observed only in subjects with the male XY genotype [78]. A study in obese humans identified sex differences in the hepatic methylome and gene expression on autosomes and the X-chromosome. For instance, higher HDL-C levels in women correlate with greater expression of the lysine demethylase 6A gene, the silencing of which reduces apoA-I expression and HDL-C levels [79]. In addition, certain sex-specific single nucleotide polymorphisms in CETP and apoA-V genes are related to dyslipidemia [80].
Furthermore, the presence of two X-chromosomes correlates with elevated HDL-C levels and HDL-apoA-I exchange activity. However, higher apoA-I, apoA-IV, and apoE levels were identified in subjects with the XY genotype [81]. Moreover, women with one X-chromosome exhibit higher LDL-C and TG levels, as well as smaller LDL and HDL particle sizes compared to women with two X-chromosomes [82]. Similarly, the XY genotype is associated with higher TG levels compared to the XX genotype in mice on a cholesterol-enriched diet [81]. These results would indicate a favorable impact of female genotype on lipoprotein levels. Conversely, another study reported an association between the XX genotype and greater apoB-100 synthesis, higher TC and TG levels, as well as increased expression of genes involved in intestinal lipid absorption [83].
2.3. Key Messages
Altogether, lipoprotein metabolism is affected by sex hormones via multiple molecular pathways. Estrogens appear to (i) counteract hepatic accumulation of fatty acids and lipids by promoting VLDL-TG production and secretion, thereby protect against hepatic steatosis, (ii) reduce LDL-C levels by stimulating LDL-R activity, partially due to the interaction with PCSK9, (iii) promote lipoprotein size expansion, (iv) increase HDL-C levels by impeding SR-B1 activity, (v) enhance reverse cholesterol transport, and (vi) modulate cholesterol synthesis and absorption of dietary lipids. Moreover, lipoprotein metabolism is influenced by sex-specific genetic variations and sex chromosomes.
3. Sex Differences in Lipid Profile
3.1. Lipid Profile Throughout the Lifetime
Lipid profiles vary with age and differ between women and men, which has recently been the subject of an extensive review [15,17,84]. In the general population, higher TC (median: 1.8 vs. 1.6 mmol/L, p<0.001), LDL-C (0.79 vs. 0.72 mmol/L, p<0.001), HDL-C (0.75 vs. 0.68 mmol/L, p<0.001), non-HDL-C (0.98 vs. 0.92 mmol/L, p<0.05) and apoB levels (31 vs. 29 mg/dL, p<0.001) were found in girls compared to boys in cord blood at birth, with corresponding results observed when measured in venous blood. Similar trends in TC (median: 4.0 vs. 3.7 mmol/L, for females and males, respectively, p<0.001), LDL-C (1.85 vs. 1.56 mmol/L, p<0.05), HDL-C (1.39 vs. 1.23 mmol/L, p<0.001), non-HDL-C (2.56 vs. 2.37 mmol/L, p<0.05) and apoB levels (76 vs. 71 mg/dL, p<0.05) were also reported at 2 months, but not at 14-16 months of age, as presented in Figure 2 [85].
During infancy, higher TC and LDL-C levels can be found in females up to 6 months of age. Less pronounced and inconsistent sex differences might also occur in HDL-C and TG levels [86]. In childhood and early adolescence, females exhibit higher TC, LDL-C, non-HDL-C, and apoB levels [15]. Starting at the age of around 20 years, men are believed to exhibit more atherogenic lipid profiles, with elevated LDL-C and TG levels [15]. However, several studies reported higher levels of Lp(a), a molecule of 6-fold greater atherogenicity compared to LDL on a per particle basis, in women [87], especially in those diagnosed with ASCVD [88,89].
Considering patients with hereditary lipid disorders, among newborns of mothers with FH, female infants exhibit higher TC, LDL-C, HDL-C, apoB, and apoA-I levels in cord blood compared to males [90]. In children with FH, increased TC (mean difference [MD]: 0.48 mmol/l, p<0.001) LDL-C (0.39 mmol/l, p<0.001), and non-HDL-C (0.42 mmol/l, p<0.001) levels were demonstrated in girls. In the same group, higher HDL-C levels were found in girls aged <5 years (mean 1.25 vs. 1.10 mmol/L, p<0.05) or 15-19 years (1.34 vs. 1.09 mmol/L, p<0.001) compared to boys of the same age [91]. Importantly, contrary to the general population, among patients with FH, higher TC (median: 8.4 vs. 8.22 mmol/L, p=0.01 [21]; and 8.2 vs. 7.6 mmol/L, p<0.001 [92]) and LDL-C levels (6.2 vs. 6.0 mmol/L, p=0.005 [93]) were described in women.
3.2. Impact of Hormonal Status in Women
3.2.1. Menstrual Cycle
Small variations in the lipid profile have been reported during the menstrual cycle [15,84], with a non-linear association between the menstrual cycle phase and TC, LDL-C, and HDL-C levels [84,94]. Specifically, the highest TC and LDL-C levels were identified in the follicular phase, which is characterized by low estrogen levels. The median TC and LDL-C levels decrease on average by 3% and 4.9% (p<0.0001), respectively, in the luteal phase [97]. Furthermore, the highest HDL-C levels occur during ovulation with an increase of 2% compared to other phases [95]. Considering other lipid parameters, although lower TG and VLDL-C levels were described in the luteal phase, the decrease was not statistically significant [96,97]. Importantly, in a study in 259 healthy women, when measured in the late luteal phase, 10.5% of the participants had LDL-C levels above the desirable range defined as <130 mg/dL, compared to 17.8% when measured in the follicular phase, showing important clinical implications, especially when women of reproductive age are included in clinical trials [95].
3.2.2. Pregnancy
Pregnancy is associated with elevated lipoprotein levels, as lipids are crucial for fetal development [15,84]. Due to altered hepatic and adipose metabolism, TC, LDL-C, HDL-C, and TG levels continue to increase from the first trimester and peak at the end of the second trimester. Therefore, dyslipidemia is likely most pronounced during the second and third trimester. Interestingly, a similar increase in lipoprotein levels is observed in pregnant women with and without a history of dyslipidemia [98,99], whereas higher absolute LDL-C levels occur in women with FH, reaching values >8 mmol/L in the 30th gestational week [16]. In a study in 222 pregnant women, 60% of the participants reached LDL-C levels above the value recommended for non-pregnant patients [100]. In addition, LDL size decreases during pregnancy, leading to increased LDL oxidation and higher atherogenicity [101]. However, HDL-C and apoA-I levels also gradually increase, with a peak in the second trimester. Nonetheless, the greatest increase during pregnancy affects TG levels, reaching two- to fourfold higher values compared to pre-pregnancy. Postnatally, lipoprotein levels normalize within 6 weeks to 6 months [15,99]. Interestingly, these changes might be influenced by breastfeeding [15,102]. Specifically, women who breastfeed have lower LDL-C levels and experience smaller declines in HDL-C levels [103], preserving higher HDL-C values during 6 months of lactation [104].
3.2.3. Menopause
Due to a decline in estrogen production, the lipid profile becomes more atherogenic following menopause [15,84]. Elevated TC, LDL-C, and apoB levels were described within a year interval from the final menstrual period. Importantly, the increase was independent of age [105]. Furthermore, a meta-analysis revealed increased TC (MD: 0.58 mmol/L), LDL-C (0.45 mmol/L), and TG (0.27 mmol/L) levels in postmenopausal women. Although the change was partially attributable to older age [106], when adjusted for age and body mass index, postmenopausal women had higher TC levels compared to premenopausal women (mean: 5.2 vs. 4.94 mmol/L, p<0.045) [107]. In addition, higher LDL-C (mean: 2.90 vs. 2.73 mmol/L, p=0.013) and lower HDL-C levels (1.47 vs. 1.55 mmol/L, p=0.013) were found in women who experienced menopause >6 years prior compared to those who had menopause <2 years prior [108]. On the contrary, a meta-analysis found no differences in HDL-C levels between pre- and postmenopausal women [106]. Intriguingly though, inconsistent study results suggest that high HDL-C levels must not necessarily be cardioprotective in middle-aged women [109]. Finally, women experience an increase in Lp(a) levels around the age of 50 years, with even 22% higher Lp(a) levels following menopause [110], which substantially contributes to a greater atherogenicity of the lipid profile.
Considering the loss of ovarian function, women with premature ovarian insufficiency (POI), defined as menopause before the age of 40 years, are at increased cardiovascular risk [111]. An association between POI and higher TG and marginally lower HDL-C levels was found [112]. A meta-analysis confirmed these results and reported higher TC, LDL-C, and TG levels in patients with POI compared to healthy controls but did not identify any differences in HDL-C levels [113].
3.2.4. Female-Specific Comorbidities
Women with polycystic ovary syndrome (PCOS) have an increased risk of developing metabolic syndrome and dyslipidemia. PCOS is characterized by excessive androgen production [15,84]. In women, dehydroepiandrosterone negatively correlates with TC levels, whereas androstenedione is associated with lower TG and apoA levels [114]. A recent meta-analysis of 23 cohort studies found higher TC and lower HDL-C levels in women with PCOS compared to healthy controls [115]. Furthermore, another meta-analysis found no differences in HDL-C but described higher TG levels in obese women with PCOS compared to obese women without PCOS [116]. Regarding another female-specific comorbidity, endometriosis is associated with an unfavorable lipid profile. Higher levels of all lipoproteins were found in women with endometriosis compared to healthy controls, with the most pronounced increase in LDL-C levels (MD: 37%, p<0.0001) [117].
3.3. Impact of Exogenous Estrogens
3.3.1. Contraception
Contraceptives containing sex hormones affect the lipid profile [15,84]. The impact of contraception differs regarding the content of estrogen and progestin. The estrogen component is believed to reduce LDL-C levels, as well as to increase HDL-C and TG levels, whereas the progestin component exhibits an opposite effect, depending on its androgenicity [15,118]. Traditionally used ethinyl estradiol has a greater impact on hepatic lipoprotein metabolism compared to the novel estetrol [119]. A combination of ethinyl estradiol and desogestrel, a third-generation progestin, reduces LDL-C and increases HDL-C levels [120]. On the contrary, a modern combination of estetrol and drospirenone, a fourth-generation progestin, has no significant effect on TC, LDL-C, and HDL-C levels, and causes a lower increase in TG levels compared to a combination of ethinyl estradiol and drospirenone (MD: 24% vs. 65.5% [121]; and 10% vs. 61.2% [122]). Interestingly, a 29.7% decline in TG levels was observed with a combination of estetrol and levonorgestrel, a second-generation progestin [122], compared to a 28% increase in TG levels with a combination of ethinyl estradiol and levonorgestrel [121]. Regarding the form of combined contraception, no differences were found between oral contraceptives and vaginal rings [123] or dermal patches [118,124].
Considering the progestin component of contraception, more androgenic progestins increase LDL-C and decrease HDL-C levels compared to the more favorable impact of novel, less androgenic progestins [118,119]. Progesterone-only pills with drospirenone or desogestrel are associated with only statistically nonsignificant declines in TC, LDL-C, HDL-C, and TG levels, whereas a significantly stronger reduction in TG levels was reported for drospirenone (MD: 0.226 vs. 0.111 mmol/L, p=0.0351) [119]. In addition, a decline in Lp(a) levels was described in women on desogestrel-containing contraceptives, with lower Lp(a) levels found in oral contraception users compared to non-users (median: 4.5 vs. 3.8 mg/dL, p=0.008) [125]. In another study though, the overall effect of a desogestrel-only pill was comparable to levonorgestrel and was described as negligible [126]. Considering other administration routes, levonorgestrel-releasing intrauterine device reduces TC (mean: 4.94 vs. 4.66 mmol/L, p=0.037) and TG levels (0.93 vs. 0.77 mmol/L, p=0.021) within 12 months of use. Although a decline in HDL-C levels can be observed at 6 months following insertion (1.38 vs. 1.29 mmol/L, p=0.012), values at 12 months are similar to those measured before insertion. Finally, a non-hormonal intrauterine device containing copper shows no effect on the lipid profile throughout 18 months of use [127].
3.3.2. Hormone Replacement Therapy
Regarding postmenopausal women, HRT reduces TC, LDL-C [128], Lp(a) [110,128,129,130], and apoB levels [129]. A favorable impact of exogenous estrogens on the lipid profile was found among women with POI, with those on HRT having similar TC, VLDL-C, LDL-C, and TG levels compared to healthy controls. In addition, the former group had higher HDL-C levels than the latter (mean 1.45 vs. 1.34 mmol/L, p=0.03) [131]. Interestingly, although oral HRT significantly decreases LDL-C levels, it also leads to higher TG levels compared to transdermal HRT, which has a more neutral effect on TG [128,132]. However, oral HRT is more effective in reducing Lp(a) levels (MD: 20.35%; p<0.0001), whereas no differences depending on estrogen dose or progestin addition were identified [130]. Conversely, the effect of HRT on TG levels is influenced by estrogen dose, as a meta-analysis found a correlation between low-dose estrogen and lower TG levels compared to standard-dose estrogen [128]. Considering HRT formulation, a combination with progestin is associated with higher TC and LDL-C levels compared to estrogen alone [128].
3.4. Key Messages
Altogether, sex differences in the lipid profile can be found throughout life. Females exhibit elevated TC and LDL-C levels in childhood compared to males. Although the opposite is likely to be observed during adolescence in the general population, among patients with FH, higher TC and LDL-C levels are found in women. Moreover, variations in female lipid profiles occur due to changes in hormonal status. During the menstrual cycle, TC and LDL-C levels increase in the follicular phase, whereas HDL-C levels peak during ovulation. Furthermore, elevated levels of TG, followed by TC, LDL-C, and HDL-C can be found during pregnancy. After menopause, the lipid profile becomes more atherogenic due to increased LDL-C, Lp(a), and TG levels. Unfavorable changes in lipid profile are also driven by female comorbidities such as POI, PCOS, and endometriosis.
Considering exogenous sex hormones, combined hormonal contraception might favorably affect LDL-C and HDL-C levels, but also increase TG levels. A combination of novel estrogens and progestins of low androgenicity, as well as progesterone-only pills and non-hormonal contraception seem to have a more neutral effect on lipid profiles. Nevertheless, available data is inconsistent, and further studies are required to assess the impact of contraception on the lipid profile. Correspondingly, HRT reduces TC, LDL-C, and Lp(a) levels, but also increases TG levels in postmenopausal women. However, the unfavorable effect on TG levels is less pronounced with low-dose estrogens and transdermal HRT.
4. Women with Dyslipidemia In Clinical Practice
4.1. Patient Characteristics
4.1.1. Lipid Profile and Cardiovascular Risk In Women
Sex differences observed in molecular mechanisms and lipid profiles translate into differences in cardiovascular risk. First, lipoprotein levels during infancy and childhood correlate with adult concentrations. Therefore, it was hypothesized that higher lipoprotein levels observed in girls increase the lifetime cardiovascular risk in women [85]. Indeed, among patients with FH, elevated LDL-C levels observed in women throughout life contribute to a greater LDL-C burden, which is the product of LDL-C concentration and exposure. Specifically, in a study involving 438 subjects, women with FH had higher LDL-C burden at the age of 19 (111.7 vs. 100.7 mmol/l-years, p<0.001) and 30 years (175.1 vs. 156.7 mmol/l-years, p<0.05) compared to a man with FH. In addition, the threshold of 125 mmol/l-year, which was associated with an increased risk of MI, was reached by all women with FH at the age of 33 years, and by all men with FH by the age of 40 years. Correspondingly, at the age of 36 years, 43.8% of women with FH reached the threshold of 220 mmol/l-years, an average LDL-C burden at the time of MI, compared to 6.2% of men with FH [92].
Considering other blood lipids, due to an increase in Lp(a) levels during menopausal transition, elevated Lp(a) levels are more prevalent in women than men after the age of 50 years. Therefore, Lp(a) may account for increased cardiovascular risk in postmenopausal women. In addition, a stronger association between Lp(a) and ASCVD was found in women with FH, compared to men with FH regardless of age [133]. Interestingly, among patients with type 2 diabetes mellitus type 2 (DM), cardiovascular risk declines in women following adjustment for Lp(a) levels [134]. Correspondingly, an independent association between Lp(a) levels, mortality, and non-fatal MI was found in women with type 2 DM, but not in men with type 2 DM or patients without type 2 DM [135]. Hence, an increased Lp(a) level is an essential cardiovascular risk factor in women, especially in combination with elevated TC [136] or LDL-C levels [89]. Moreover, although hypertriglyceridemia was linked to increased cardiovascular risk in both sexes, non-fasting TG levels have a stronger prognostic value for predicting MI, coronary artery disease (CAD), total mortality [137], and peripheral artery disease (PAD) [138] in women compared to men. Hence, it was suggested that elevated TG level is a more potent cardiovascular risk factor in women [17].
4.1.2. Cardiovascular Risk Factors in Women
Regarding the patient’s global cardiovascular risk, women treated for ASCVD are likely to be older and have more cardiovascular risk factors than men, due to the later onset of ASCVD [17]. The prevalence of dyslipidemia, glucose intolerance, visceral adiposity, and arterial hypertension increases following menopause, leading to endothelial dysfunction and inflammation, which in turn predispose to ASCVD [27]. The cardiovascular risk profile of postmenopausal women is presented in Figure 3. Women are also more often affected by systemic autoimmune disorders, which promote ASCVD development and progression [139]. Interestingly, a greater impact of established cardiovascular risk factors, such as hypertension, DM, and smoking, on the global cardiovascular risk was reported in women [18]. For instance, a stronger association between first MI and arterial hypertension (odds ratio (OR): 2.87 vs. 2.19, p<0.001 for all), DM (3.59 vs. 1.76), and current smoking (3.28 vs. 3.25) was found in women compared to men [140].
Furthermore, sex-specific conditions accounting for increased cardiovascular risk were described and comprise obstetric and gynecological disorders, such as gestational DM or hypertension, pre-eclampsia, placental abruption, preterm delivery, stillbirth, miscarriage, premature menopause or PCOS [18,141]. Furthermore, the use of combined oral contraception was linked to negative changes in cardiovascular risk factors [142] and increased incidence of stroke [143] and MI, especially in women with hypertension or dyslipidemia [141]. Correspondingly, an association between HRT and increased cardiovascular risk was found in postmenopausal women, especially with HRT initiated years after menopause [18]. On the contrary, a favorable impact of HRT on cardiovascular risk and mortality was suggested provided HRT is started around menopausal transition [144]. Finally, increased cardiovascular risk and ASCVD-related mortality rates were found in women with breast cancer varying based on cancer treatment received [145].
Along with sex, cardiovascular risk is influenced by sociological, psychological, and cultural features reflected by gender. Due to low socioeconomic status, poor education, and limited access to healthcare, women are less likely to seek medical attention and are less aware of their own cardiovascular risk. Furthermore, women suffer from greater mental stress, depression, and anxiety, which predispose to ASCVD, and affect disease manifestation and clinical outcome [146]. A stronger association between depression and first MI was found in women than in men (OR: 3.09 vs. 1.77; p<0.001), highlighting the importance of psychosocial cardiovascular risk factors in women [140].
4.1.3. Atherosclerotic cardiovascular Disease in Women
Sex differences occur in ASCVD manifestations. Women tend to have smaller atherosclerotic plaques with a lower volume of lipid-rich necrotic core and calcification in the carotid arteries [147]. Those in the coronary arteries have additionally lower volumes of fibrous tissue and fibro-fatty tissue, along with greater total plaque burden [148]. Overall, women have less vulnerable atherosclerotic plaques, and contrary to men, experience acute plaque rupture less frequently than plaque erosion [149]. Moreover, women are less likely to exhibit diffuse CAD or severe ischemia, but present with more frequent angina and microvascular disease as the underlying cause [150].
Considering clinical presentation, women with acute coronary syndrome tend to show prodromal and atypical symptoms, which might be underestimated by physicians, leading to delays in treatment [151]. Specifically, a longer time from the onset of symptoms to alarming emergency medical services and to first medical contact, along with lower rates of percutaneous coronary interventions and longer in-hospital delays, followed by worse clinical outcomes, were reported in women among patients with acute coronary syndrome [152]. Similarly, women with PAD less often experience intermittent claudication and present with atypical symptoms, resulting in lower sensitivity of ankle-brachial index measurement, a more challenging diagnostic process, and delayed diagnosis. Consequently, women with PAD present with multivessel disease and chronic limb ischemia more frequently and experience a higher rate of complications after surgery, either endovascular or open, than men [153].
4.2. Lipid-Lowering Therapy
4.2.1. Effectiveness of Lipid-Lowering Agents in Women
Reaching the guideline-recommended LDL-C levels is essential for ASCVD prevention and treatment. Currently, first-line LLT includes a statin in a maximally tolerated dose [3]. Although a study on 337 patients found lower LDL-C reduction in women after adjustment for dose and statin power (22.7 vs. 28.5%, p<0.001) [154], a meta-analysis including 174,000 patients showed that statins are similarly efficient in reducing LDL-C levels and the risk of MACE at 1-year follow-up in both women and men [155]. In addition, a higher increase in HDL-C levels was described in women compared to men on statin treatment (MD: 5.64%, p=0.001) [156].
Considering the next step of LLT, a combination of statin and ezetimibe reduces LDL-C levels and the risk of MACE equally in women and men [157]. In the cardiovascular endpoint trial IMPROVE-IT, ezetimibe decreased MACE rates similarly in women and men [158]. Although a meta-analysis revealed significantly greater changes in LDL-C (p=0.0066), non-HDL-C, TC, TG, apoA-I (p<0.0001), and apoB levels (p=0.0055) in men compared to women on statin and ezetimibe, the differences were only ≤2% [159]. Interestingly, a comparison of high-intensity statin monotherapy with a combination of moderate-intensity statin and ezetimibe found both treatment strategies equally efficient in reducing cardiovascular event rates regardless of sex. Of note, discontinuation or dose reduction rates were lower in the latter compared to the former group in both women and men [160]. Moreover, among patients with ASCVD or FH treated with statins and bempedoic acid, greater placebo-corrected reductions in LDL-C (21.2 vs. 17.4%, p=0.044), non-HDL-C (17.3 vs. 12.1%, p=0.003), TC (13.8 vs. 10.5%, p=0.012) and apoB levels (16 vs. 11.3%, p=0.004) were observed in women than men. Conversely, comparable results were reported among both sexes in patients receiving bempedoic acid along with low-dose or no statin [161]. Most importantly though, bempedoic acid reduced LDL-C levels and cardiovascular risk similarly in women and men in the cardiovascular endpoint trial Clear Outcomes [162].
Sex differences are most pronounced in LDL-C reduction with PCSK9 inhibitor treatment. A greater reduction in LDL-C levels was reported in men than in women on evolocumab (58% vs. 52%, p<0.001). Nevertheless, relative risk reductions in the primary endpoint and key secondary endpoint in the evolocumab cardiovascular endpoint trial Fourier were similar for both sexes [163]. Correspondingly, alirocumab treatment was associated with a higher LDL-C decline in men than women in placebo-controlled (60 vs. 48.3%) and ezetimibe-controlled trials (50.9 vs. 42.3%). Although only 36.5% of women compared to 58.7% of men achieved on-treatment LDL-C levels <50 mg/dL, no sex differences occurred in the risk of MACE in the alirocumab cardiovascular endpoint trial Odyssey Outcomes [164]. These results were confirmed in meta-analyses evaluating the efficacy of PCSK9 inhibitors in women [165,166], as well as in real-world registries [167,168]. The latter reported lower LDL-C reduction in women than men both among patients with (48% vs. 61%, p<0.001) and without FH (55% vs. 62%, p=0.015) [167]. Of note, despite differences in circulating PCSK9 levels, no differences in LDL-C reduction were observed between pre- and post-menopausal women on PCSK9 inhibitors [167,168].
4.2.2. Real-World Lipid-Lowering Therapy in Women
Given the comparable efficacy of lipid-lowering agents in women and men, current guidelines do not recommend sex-specific treatment regimens [3], and hence, should be followed equally regardless of sex. However, real-world data demonstrate that women are less likely than men to receive any statin (OR: 0.70, p<0.001). Even if treated, women receive lower than the guideline-recommended intensity statin more often than men (OR: 0.82, p<0.001) [9]. In addition, women with CAD treated with statins are less often evaluated by cardiologists (62 vs. 67.4%, p<0.001), whereas such an evaluation is associated with higher statin use (OR: 2.535, p<0.001) [169]. Consequently, women achieve the guideline-recommended LDL-C levels less often than men. For instance, in a recent study from Portugal, women were found to be 22% less likely to reach the LDL-C goal than men [19]. Higher LDL-C levels were found in women both in primary and secondary prevention settings (age-adjusted difference: 0.3 and 0.28 mmol/L, respectively) [20]. However, it should be pointed out that CVD risk-based LDL-C goal attainment is generally low, in both men and women varying between 20-30%, as consistently reported across Europe [170,171,172] and in the United States [173].
Similar trends were described among patients with FH, with women being on LLT less often than men (58.4 vs. 61.1%, p<0.001). If treated, women with FH take the highest statin dose (16.6 vs. 13.1%, p<0.001), ezetimibe (23.4 vs. 25.9%, p<0.0001), and PCSK9 inhibitors (2.5 vs. 3.5%, p=0.0002) less frequently than men [11]. Generally, men with FH are more likely to receive high-intensity statin (OR: 1.52, p<0.05) [12]. Consequently, women with FH have higher on-treatment LDL-C levels (125 vs. 116 mg/dL, p=0.02), especially among those with premature ASCVD (135 vs. 109 mg/dL, p=0.005) [174]. Correspondingly, women with FH less often reach LDL-C levels <100 mg/dL (20 vs. 29%, p<0.001), consistently among FH patients with ASCVD, without ASCVD, and those on statin treatment (ORs: 0.70, 0.68, and 0.74, respectively) [21]. Importantly, a significantly stronger association between higher pre-treatment LDL-C levels and not reaching the LDL-C goal was found in women compared to men with FH, both among patients with (OR: 0.35 vs. 0.64, p=0.02) or without ASCVD (OR: 0.70 vs. 0.83, p=0.013) [94].
Alarmingly, women are approximately 2.5 years older when diagnosed with FH [11] and are commenced on LLT later in life than men (42.3 vs. 37.5 years of age, p<0.0001) [175]. Furthermore, women experience an average of 2.3 year-long off-treatment periods related to conception, pregnancy, and breastfeeding, contributing to a greater total LDL-C burden [16]. Of note, maternal hypercholesterolemia is associated with higher LDL-C levels in offspring (MD: 0.04 mmol/L), and hence, might not only increase the cardiovascular risk of the mother but also of the child. Overall, women with FH suffer from greater excess cardiovascular morbidity compared to men with FH (standardized morbidity ratio: 7.55 vs. 6.83), especially among patients aged 30-50 years (15.04 vs. 10.03) [175].
Regarding other aspects of LLT, women discontinue statin treatment more often than men (10.9 vs. 6.1%, p<0.001) [9]. Side effects are the most frequent reason for stopping or switching to another statin in both sexes, but women are more likely to report them. A higher rate of new or worsening muscle symptoms as side effects of statin treatment were found in women than men (31 vs. 26%, p<0.01) [22]. Importantly, women with a history of statin use are less likely than men to try another statin [9]. Furthermore, sex differences occur in adherence to statin treatment [23], with women being less likely to take statin as prescribed (67 vs. 71%, p=0.007) but more likely to skip a dose or not to fill a prescription (35 vs. 31%, p=0.02).
Considering the patient-physician relationship, women are less likely to be informed about the risk associated with elevated LDL-C levels, which might contribute to a greater proportion of women dissatisfied with their treatment [22] and questioning statin efficacy and safety [9]. Correspondingly, lower adherence to statin treatment was also reported in women compared to men with FH [24]. Moreover, women with FH receive less frequently than men adequate information about FH (68.9 vs. 80.2%, p=0.011) and the associated risks (71.1 vs. 80.7%, p=0.033), as well as less often agree that statins are safe (44.8 vs. 60%, p=0.003). At the same time, women with FH are more concerned about their high LDL-C levels than men (67.5 vs. 56.5%, p=0.024) [25].
4.3. Key Messages
Altogether, the prevalence of cardiovascular risk factors differs in women and men. Women might have a greater burden related to LDL-C, Lp(a), and TG levels, especially among patients with FH. Women are exposed not only to traditional cardiovascular risk factors, but also those associated with reproductive health and psychosocial status. Among patients with ASCVD, women and men exhibit different plaque morphology and pathophysiology. Moreover, unusual disease manifestations in women can negatively influence the diagnostic process, treatment course, and clinical outcome. Therefore, global female cardiovascular risk might be underestimated, leading to delayed LLT initiation, as a part of ASCVD prevention.
No sex differences occur in the risk of MACE following LLT, and hence, both women and men benefit equally from LLT. Despite comparable LLT efficacy, women are less likely than men to be offered LLT, including high-intensity statins, ezetimibe, and PCSK9 inhibitors. Consequently, women have higher on-treatment LDL-C levels and achieve their risk-based LDL-C goal less often than men. A similar trend is observed among patients with FH. In addition, women with FH are diagnosed and started on LLT later in life and are exposed to pregnancy-associated off-treatment periods, which contribute to greater LDL-C burden and cardiovascular morbidity. Moreover, women are less adherent to statin treatment, mostly due to side effects, and have less satisfying patient-physician relationships compared to men.
5. Conclusions and Future Directions
Men still constitute the majority of clinical trial participants, even in recent years. For instance, trials investigating novel LDL-C-lowering inclisiran and Lp(a)-lowering olpasiran include approximately 32% of women [176,177]. Consequently, most of the available data on MACE reduction with LLTs is derived primarily from men. Female underrepresentation may partly result from a lower willingness of women to participate in trials due to greater concerns about possible harm or transportation issues. Interestingly though, more women are included in trials with female corresponding authors, indicating the important role the sex of researchers may play in resolving this conundrum [178]. To gain a better understanding of sex differences in dyslipidemia and LLT efficacy and safety, greater representation of women in clinical trials, as well as sex-specific research must be endorsed. Further studies are necessary to investigate, among others, (i) the role of sex-specific hormonal and genetic determinants in dyslipidemia and ASCVD, (ii) the relationship between menstrual cycle and lipid profile, (iii) the meaning of menopausal transition for ASCVD prevention, (iv) the burden and treatment of dyslipidemia in pregnant women, (v) the impact of contraception and HRT on dyslipidemia and cardiovascular risk, (vi) the influence of Lp(a) and TG levels on cardiovascular risk in women, or (vi) sex disparities in the response to novel lipid-lowering agents.
Based on the presented data, women with dyslipidemia could benefit from sex-specific recommendations. For instance, lipoprotein level monitoring, especially regarding TG levels, seems reasonable in women taking contraception or HRT. Given the menopause-related changes, repeated measurement of lipoprotein levels, including Lp(a), could lead to reclassification of the female cardiovascular risk after menopausal transition. Correspondingly, considering additional cardiovascular risk factors, such as those related to reproductive health or psychosocial status, along with traditional ones, can contribute to more precise cardiovascular risk stratification in women. Among patients on LLT, the use of combination treatment might prevent side effects of statin treatment, and hence, improve female adherence. In addition, due to pregnancy-associated off-treatment periods, early LLT initiation and strict follow-up to minimize time off-treatment seem rational, especially in women with FH.
Furthermore, to ensure that both women and men receive equitable LLT, there is a need to promote sex-specific research outcomes among healthcare professionals. Specifically, physicians treating patients with dyslipidemia should be educated on sex differences in lipid and cardiovascular risk profiles, and disease manifestations. More attention should also be brought to the impact of sex and gender on treatment course and adherence. Hereby, physicians must be encouraged not to delay LLT initiation in women, and to use the guideline-recommended LLT intensity regardless of sex. Treatment equality, along with a need for earlier diagnosis in women, must be advocated especially considering patients with FH. Finally, to raise female awareness of the cardiovascular risk associated with dyslipidemia, appropriate actions must be undertaken both in clinical practice and at the institutional level. Spreading the knowledge about LLT's importance, efficacy, and safety is essential to reduce the LDL-C burden in women. It is long overdue that national and international guidelines address the issue of sex differences in the prevention of cardiovascular disease and tailor their recommendation accordingly [17,84,154]. The key messages about the management of dyslipidemia in women are summarized in
Author Contributions
Conceptualization, J.M.Z. and I.G.B.; methodology, J.M.Z.; investigation, J.M.Z.; resources, J.M.Z.; data curation, J.M.Z..; writing—original draft preparation, J.M.Z.; writing—review and editing, J.M.Z., M.M., H.K.B., I.G.B.; visualization, J.M.Z., M.M., I.G.B.; supervision, H.K.B., I.G.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
None declared.
Conflicts of Interest
I.G.B. has served as a consultant and received honoraria from Akcea, Amgen, Daiichi-Sankyo, Novaritis, Sanofi-Regeneron, Ultragenyx, and Amarin. The other authors declare no conflict of interest related to the manuscript.
References
- Ralapanawa, U.; Sivakanesan, R. Epidemiology and the Magnitude of Coronary Artery Disease and Acute Coronary Syndrome: A Narrative Review. J Epidemiol Glob Health 2021, 11, 169–177. [Google Scholar] [CrossRef]
- Libby, P. The Changing Landscape of Atherosclerosis. Nature 2021, 592, 524–533. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; Cosyns, B.; Crawford, C.; Davos, C.H.; Desormais, I.; Di Angelantonio, E.; Franco, O.H.; Halvorsen, S.; Hobbs, F.D.R.; Hollander, M.; Jankowska, E.A.; Michal, M.; Sacco, S.; Sattar, N.; Tokgozoglu, L.; Tonstad, S.; Tsioufis, K.P.; van Dis, I.; van Gelder, I.C.; Wanner, C.; Williams, B. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur Heart J, 2022; 29, 5–115. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A. 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias: Lipid Modification to Reduce Cardiovascular Risk. Eur Heart J 2020, 41, 111–188. [Google Scholar] [CrossRef]
- Banach, M.; Penson, P.E.; Farnier, M.; Fras, Z.; Latkovskis, G.; Laufs, U.; Paneni, F.; Parini, P.; Pirro, M.; Reiner, Ž. Bempedoic Acid in the Management of Lipid Disorders and Cardiovascular Risk. 2023 Position Paper of the International Lipid Expert Panel (ILEP). Prog Cardiovasc Dis 2023, 79, 2–11. [Google Scholar] [CrossRef]
- Kronenberg, F.; Mora, S.; Stroes, E.S.G.; Ference, B.A.; Arsenault, B.J.; Berglund, L.; Dweck, M.R.; Koschinsky, M.; Lambert, G.; Mach, F.; McNeal, C.J.; Moriarty, P.M.; Ntarajan, P.; Nordestgaard, B.G.; Parhofer, K.G.; Virani, S.S.; von Eckardstein, A.; Watts, G.F.; Stock, J.K.; Ray, K.K.; Tokgözoǧlu, L.S.; Catapano, A.L. Lipoprotein(a) in Atherosclerotic Cardiovascular Disease and Aortic Stenosis: A European Atherosclerosis Society Consensus Statement. Eur Heart J 2022, 43, 3925–3946. [Google Scholar] [CrossRef] [PubMed]
- Gouni-Berthold, I.; Schwarz, J.; Berthold, H.K. PCSK9 Monoclonal Antibodies: New Developments and Their Relevance in a Nucleic Acid–Based Therapy Era. Curr Atheroscler Rep 2022, 24, 779–790. [Google Scholar] [CrossRef] [PubMed]
- Katsiki, N.; Vrablik, M.; Banach, M.; Gouni-Berthold, I. Inclisiran, Low-Density Lipoprotein Cholesterol and Lipoprotein (a). Pharmaceuticals 2023, 16, 577. [Google Scholar] [CrossRef]
- Nanna, M.G.; Wang, T.Y.; Xiang, Q.; Goldberg, A.C.; Robinson, J.G.; Roger, V.L.; Virani, S.S.; Wilson, P.W.F.; Louie, M.J.; Koren, A. Sex Differences in the Use of Statins in Community Practice: The Patient and Provider Assessment of Lipid Management (PALM) Registry. , Circ Cardiovasc Qual Outcomes 2019, 12, e005562. [Google Scholar] [CrossRef]
- Peters, S.A.E.; Colantonio, L.D.; Zhao, H.; Bittner, V.; Dai, Y.; Farkouh, M.E.; Monda, K.L.; Safford, M.M.; Muntner, P.; Woodward, M. Sex Differences in High-Intensity Statin Use Following Myocardial Infarction in the United States. J Am Coll Cardiol 2018, 71, 1729–1737. [Google Scholar] [CrossRef]
- Vallejo-Vaz, A.J.; Stevens, C.A.T.; Lyons, A.R.M.; Dharmayat, K.I.; Freiberger, T.; Hovingh, G.K.; Mata, P.; Raal, F.J.; Santos, R.D.; Soran, H. Global Perspective of Familial Hypercholesterolaemia: A Cross-Sectional Study from the EAS Familial Hypercholesterolaemia Studies Collaboration (FHSC). Lancet 2021, 398, 1713–1725. [Google Scholar] [CrossRef]
- März, W.; Schmidt, N.; an Haack, I.; Dressel, A.; Grammer, T.B.; Kleber, M.E.; Baessler, A.; Beil, F.U.; Gouni-Berthold, I.; Julius, U. The German CaRe High Registry for Familial Hypercholesterolemia – Sex Differences, Treatment Strategies, and Target Value Attainment. Atherosclerosis Plus 2023, 53, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Conlon, D.M.; Welty, F.K.; Reyes-Soffer, G.; Amengual, J. Sex-Specific Differences in Lipoprotein Production and Clearance. Arterioscler Thromb Vasc Biol 2023, 43, 1617–1625. [Google Scholar] [CrossRef] [PubMed]
- Palmisano, B.T.; Zhu, L.; Stafford, J.M. Role of Estrogens in the Regulation of Liver Lipid Metabolism. Adv Exp Med Biol 2017, 1043, 227–256. [Google Scholar] [CrossRef]
- Holven, K.B.; Roeters van Lennep, J. Sex Differences in Lipids: A Life Course Approach. Atherosclerosis 2023, 384, 117270. [Google Scholar] [CrossRef]
- Klevmoen, M.; Mulder, J.W.C.M.; Roeters van Lennep, J.E.; Holven, K.B. Sex Differences in Familial Hypercholesterolemia. Curr Atheroscler Rep 2023, 25, 861–868. [Google Scholar] [CrossRef] [PubMed]
- Roeters Van Lennep, J.E.; Tokgözoǧlu, L.S.; Badimon, L.; Dumanski, S.M.; Gulati, M.; Hess, C.N.; Holven, K.B.; Kavousi, M.; Kaylkçloǧlu, M.; Lutgens, E. Women, Lipids, and Atherosclerotic Cardiovascular Disease: A Call to Action from the European Atherosclerosis Society. Eur Heart J 2023, 44, 4157–4173. [Google Scholar] [CrossRef]
- Vogel, B.; Acevedo, M.; Appelman, Y.; Bairey Merz, C.N.; Chieffo, A.; Figtree, G.A.; Guerrero, M.; Kunadian, V.; Lam, C.S.P.; Maas, A.H.E.M. The Lancet Women and Cardiovascular Disease Commission: Reducing the Global Burden by 2030. Lancet 2021, 397, 2385–2438. [Google Scholar] [CrossRef]
- Gavina, C.; Araújo, F.; Teixeira, C.; Ruivo, J.A.; Corte-Real, A.L.; Luz-Duarte, L.; Canelas-Pais, M.; Taveira-Gomes, T. Sex Differences in LDL-C Control in a Primary Care Population: The PORTRAIT-DYS Study. Atherosclerosis 2023, 384, 117148. [Google Scholar] [CrossRef]
- Rachamin, Y.; Grischott, T.; Rosemann, T.; Meyer, M.R. Inferior Control of Low-Density Lipoprotein Cholesterol in Women Is the Primary Sex Difference in Modifiable Cardiovascular Risk: A Large-Scale, Cross-Sectional Study in Primary Care. Atherosclerosis 2021, 324, 141–147. [Google Scholar] [CrossRef]
- Amrock, S.M.; Duell, P.B.; Knickelbine, T.; Martin, S.S.; O’Brien, E.C.; Watson, K.E.; Mitri, J.; Kindt, I.; Shrader, P.; Baum, S.J. Health Disparities among Adult Patients with a Phenotypic Diagnosis of Familial Hypercholesterolemia in the CASCADE-FHTM Patient Registry. Atherosclerosis 2017, 267, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Karalis, D.G.; Wild, R.A.; Maki, K.C.; Gaskins, R.; Jacobson, T.A.; Sponseller, C.A.; Cohen, J.D. Gender Differences in Side Effects and Attitudes Regarding Statin Use in the Understanding Statin Use in America and Gaps in Patient Education (USAGE) Study. J Clin Lipidol 2016, 10, 833–841. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, K.M.; Zullig, L.L.; Bastian, L.A.; Bosworth, H.B. Statin Adherence: Does Gender Matter? Curr Atheroscler Rep 2016, 18, 63. [Google Scholar] [CrossRef] [PubMed]
- Zamora, A.; Ramos, R.; Comas-Cufi, M.; García-Gil, M.; Martí-Lluch, R.; Plana, N.; Alves-Cabratosa, L.; Ponjoan, A.; Rodríguez-Borjabad, C.; Ibarretxe, D. Women with Familial Hypercholesterolemia Phenotype Are Undertreated and Poorly Controlled Compared to Men. Sci Rep 2023, 13, 1492. [Google Scholar] [CrossRef]
- Alshibani, B.; Iatan, I.; Guerin, A.; Ruel, I.; Cermakova, L.; Ramanakumar, A. V.; Pilote, L.; Coutinho, T.; Brunham, L.R.; Genest, J. Sex Differences in the Perception of Cardiovascular Risk in Familial Hypercholesterolemia. J Clin Lipidol 2023, 18, e97–e104. [Google Scholar] [CrossRef] [PubMed]
- Maas, A.H.; Appelman, Y.E. Gender differences in coronary heart disease. Neth Heart J. 2010, 18, 598–602. [Google Scholar] [CrossRef] [PubMed]
- Ryczkowska, K.; Adach, W.; Janikowski, K.; Banach, M.; Bielecka-Dabrowa, A. Menopause and Women’s Cardiovascular Health: Is It Really an Obvious Relationship? Arch Med Sci 2023, 19, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Liu, Q.; Huang, T.; Tan, W.; Qu, L.; Chen, T.; Pan, H.; Chen, L.; Liu, J.; Wong, C.W. Dysfunction of Estrogen-Related Receptor Alpha-Dependent Hepatic VLDL Secretion Contributes to Sex Disparity in NAFLD/NASH Development. Theranostics 2020, 10, 10874–10891. [Google Scholar] [CrossRef]
- Palmisano, B.T.; Le, T.D.; Zhu, L.; Lee, Y.K.; Stafford, J.M. Cholesteryl Ester Transfer Protein Alters Liver and Plasma Triglyceride Metabolism through Two Liver Networks in Female Mice. J Lipid Res 2016, 57, 1541–51. [Google Scholar] [CrossRef]
- Magkos, F.; Patterson, B.W.; Mohammed, B.S.; Klein, S.; Mittendorfer, B. Women Produce Fewer but Triglyceride-Richer Very Low-Density Lipoproteins than Men. J Clin Endocrinol Metab 2007, 92, 1311–1318. [Google Scholar] [CrossRef]
- Wang, X.; Magkos, F.; Mittendorfer, B. Sex Differences in Lipid and Lipoprotein Metabolism: It’s Not Just about Sex Hormones. J Clin Endocrinol Metab 2011, 96, 885–893. [Google Scholar] [CrossRef]
- Matthan, N.R.; Jalbert, S.M.; Barrett, P.H.R.; Dolnikowski, G.G.; Schaefer, E.J.; Lichtenstein, A.H. Gender-Specific Differences in the Kinetics of Nonfasting TRL, IDL, and LDL Apolipoprotein B-100 in Men and Premenopausal Women. Arterioscler Thromb Vasc Biol 2008, 28, 1838–43. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.I.; Reeds, D.N.; Okunade, A.L.; Patterson, B.W.; Mittendorfer, B. Systemic Delivery of Estradiol, but Not Testosterone or Progesterone, Alters Very Low Density Lipoprotein-Triglyceride Kinetics in Postmenopausal Women. J Clin Endocrinol Metab 2014, 99, 1306–10. [Google Scholar] [CrossRef] [PubMed]
- Magkos, F.; Patterson, B.W.; Mittendorfer, B. No Effect of Menstrual Cycle Phase on Basal Very-Low-Density Lipoprotein Triglyceride and Apolipoprotein B-100 Kinetics. Am J Physiol Endocrinol Metab 2006, 291, E1243–E1249. [Google Scholar] [CrossRef] [PubMed]
- Ndzie Noah, M.L.; Adzika, G.K.; Mprah, R.; Adekunle, A.O.; Adu-Amankwaah, J.; Sun, H. Sex–Gender Disparities in Cardiovascular Diseases: The Effects of Estrogen on ENOS, Lipid Profile, and NFATs During Catecholamine Stress. Front Cardiovasc Med 2021, 8, 639946. [Google Scholar] [CrossRef] [PubMed]
- Ma, P.T.S.; Yamamoto, T.; Goldstein, J.L.; Brown, M.S. Increased MRNA for Low Density Lipoprotein Receptor in Livers of Rabbits Treated with 17α-Ethinyl Estradiol. Proc Natl Acad Sci U S A 1986, 83, 792–796. [Google Scholar] [CrossRef] [PubMed]
- Owen, A.J.; Roach, P.D.; Abbey, M. Regulation of Low-Density Lipoprotein Receptor Activity by Estrogens and Phytoestrogens in a HepG2 Cell Model. Ann Nutr Metab 2004, 48, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Gouni-Berthold, I.; Berthold, H.K. PCSK9 Antibodies for the Treatment of Hypercholesterolemia. Nutrients 2014, 6, 5517–5533. [Google Scholar] [CrossRef] [PubMed]
- Seidah, N.G.; Awan, Z.; Chrétien, M.; Mbikay, M. PCSK9: A Key Modulator of Cardiovascular Health. Circ Res 2014, 114, 1022–1036. [Google Scholar] [CrossRef]
- Ooi, T.C.; Raymond, A.; Cousins, M.; Favreau, C.; Taljaard, M.; Gavin, C.; Jolly, E.E.; Malone, S.; Eapen, L.; Chretien, M. Relationship between Testosterone, Estradiol and Circulating PCSK9: Cross-Sectional and Interventional Studies in Humans. Clin Chim Acta 2015, 446, 97–104. [Google Scholar] [CrossRef]
- Ghosh, M.; Gälman, C.; Rudling, M.; Angelin, B. Influence of Physiological Changes in Endogenous Estrogen on Circulating PCSK9 and LDL Cholesterol. J Lipid Res 2015, 56, 463–469. [Google Scholar] [CrossRef]
- Persson, L.; Henriksson, P.; Westerlund, E.; Hovatta, O.; Angelin, B.; Rudling, M. Endogenous Estrogens Lower Plasma PCSK9 and LDL Cholesterol but Not Lp(a) or Bile Acid Synthesis in Women. Arterioscler Thromb Vasc Biol 2012, 32, 810–814. [Google Scholar] [CrossRef] [PubMed]
- Lakoski, S.G.; Lagace, T.A.; Cohen, J.C.; Horton, J.D.; Hobbs, H.H. Genetic and Metabolic Determinants of Plasma PCSK9 Levels. J Clin Endocrinol Metab 2009, 94, 2537–2543. [Google Scholar] [CrossRef]
- Ooi, T.C.; Raymond, A.; Cousins, M.; Favreau, C.; Taljaard, M.; Gavin, C.; Jolly, E.E.; Malone, S.; Eapen, L.; Chretien, M. Relationship between Testosterone, Estradiol and Circulating PCSK9: Cross-Sectional and Interventional Studies in Humans. Clin Chim Acta 2015, 446, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Jing, Y.; Hu, T.; Lin, C.; Xiong, Q.; Liu, F.; Yuan, J.; Zhao, X.; Wang, R. Resveratrol Downregulates PCSK9 Expression and Attenuates Steatosis through Estrogen Receptor α-Mediated Pathway in L02 cells. Eur J Pharmacol 2019, 855, 216–22. [Google Scholar] [CrossRef]
- Starr, A.E.; Lemieux, V.; Noad, J.; Moore, J.I.; Dewpura, T.; Raymond, A.; Chrétien, M.; Figeys, D.; Mayne, J. β-Estradiol Results in a Proprotein Convertase Subtilisin/Kexin Type 9-Dependent Increase in Low-Density Lipoprotein Receptor Levels in Human Hepatic HuH7 Cells. FEBS Journal 2015, 282, 2682–2696. [Google Scholar] [CrossRef]
- Roubtsova, A.; Chamberland, A.; Marcinkiewicz, J.; Essalmani, R.; Fazel, A.; Bergeron, J.J.; Seidah, N.G.; Prat, A. PCSK9 Deficiency Unmasks a Sex- And Tissue-Specific Subcellular Distribution of the LDL and VLDL Receptors in Mice. J Lipid Res 2015, 56, 2133–2142. [Google Scholar] [CrossRef]
- Fu, W.; Gao, X.P.; Zhang, S.; Dai, Y.P.; Zou, W.J.; Yue, L.M. 17β-Estradiol Inhibits PCSK9-Mediated LDLR Degradation Through GPER/PLC Activation in HepG2 Cells. Front Endocrinol (Lausanne) 2020, 10, 930. [Google Scholar] [CrossRef] [PubMed]
- Jia, F.; Fei, S.F.; Tong, D.B.; Xue, C.; Li, J.J. Sex Difference in Circulating PCSK9 and Its Clinical Implications. Front Pharmacol 2022, 13, 953845. [Google Scholar] [CrossRef]
- Xie, F.; Li, X.; Xu, Y.; Cheng, D.; Xia, X.; Lv, X.; Yuan, G.; Peng, C. Estrogen Mediates an Atherosclerotic-Protective Action via Estrogen Receptor Alpha/SREBP-1 Signaling. Front Cardiovasc Med 2022, 9, 895916. [Google Scholar] [CrossRef]
- Thierer, J.H.; Ekker, S.C.; Farber, S.A. The LipoGlo Reporter System for Sensitive and Specific Monitoring of Atherogenic Lipoproteins. Nat Commun 2019, 10, 3426. [Google Scholar] [CrossRef]
- Demissie, S.; Cupples, L.A.; Shearman, A.M.; Gruenthal, K.M.; Peter, I.; Schmid, C.H.; Karas, R.H.; Housman, D.E.; Mendelsohn, M.E.; Ordovas, J.M. Estrogen Receptor-α Variants Are Associated with Lipoprotein Size Distribution and Particle Levels in Women: The Framingham Heart Study. Atherosclerosis 2006, 185, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Shearman, A.M.; Demissie, S.; Cupples, L.A.; Peter, I.; Schmid, C.H.; Ordovas, J.M.; Mendelsohn, M.E.; Housman, D.E. Tobacco Smoking, Estrogen Receptor α Gene Variation and Small Low Density Lipoprotein Level. Hum Mol Genet 2005, 14, 2405–2413. [Google Scholar] [CrossRef] [PubMed]
- Shearman, A.M.; Cupples, L.A.; Demissie, S.; Peter, I.; Schmid, C.H.; Karas, R.H.; Mendelsohn, M.E.; Housman, D.E.; Levy, D. Association Between Estrogen Receptor Gene Variation and Cardiovascular Disease, JAMA 2003, 290, 2263–2270. [CrossRef]
- Nordström, P.; Glader, C.A.; Dahlén, G.; Birgander, L.S.; Lorentzon, R.; Waldenström, A.; Lorentzon, M. Oestrogen Receptor α Gene Polymorphism Is Related to Aortic Valve Sclerosis in Postmenopausal Women. J Intern Med 2003, 254, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Billon-Galés, A.; Fontaine, C.; Douin-Echinard, V.; Delpy, L.; Berges, H.; Calippe, B.; Lenfant, F.; Laurell, H.; Guéry, J.C.; Gourdy, P. Endothelial Estrogen Receptor-α Plays a Crucial Role in the Atheroprotective Action of 17β-Estradiol in Low-Density Lipoprotein Receptor-Deficient Mice. Circulation 2009, 120, 2567–2576. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, S.M.; Sugiyama, M.G.; Fung, K.Y.Y.; Gao, Y.; Wang, C.; Levy, A.S.; Azizi, P.; Roufaiel, M.; Zhu, S.N.; Neculai, D. A Novel Assay Uncovers an Unexpected Role for SR-BI in LDL Transcytosis. Cardiovasc Res 2015, 108, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari, S.; Nabi, F.N.; Sugiyama, M.G.; Lee, W.L. Estrogen Inhibits LDL (Low-Density Lipoprotein) Transcytosis by Human Coronary Artery Endothelial Cells via GPER (G-Protein-Coupled Estrogen Receptor) and SR-BI (Scavenger Receptor Class B Type 1). Arterioscler Thromb Vasc Biol 2018, 38, 2283–2294. [Google Scholar] [CrossRef]
- Meyer, M.R.; Fredette, N.C.; Howard, T.A.; Hu, C.; Ramesh, C.; Daniel, C.; Amann, K.; Arterburn, J.B.; Barton, M.; Prossnitz, E.R. G Protein-Coupled Estrogen Receptor Protects from Atherosclerosis. Sci Rep 2014, 4, 7564. [Google Scholar] [CrossRef]
- Ruiz-Sanz, J.I.; Navarro, R.; Martínez, R.; Hernández, M.L.; Matorras, R.; Ruiz-Larrea, M.B. No Effect of Menstrual Cycle on LDL Oxidizability and Particle Size. Maturitas 2007, 57, 253–260. [Google Scholar] [CrossRef]
- Koh, K.K. Effects of Estrogen on the Vascular Wall: Vasomotor Function and Inflammation Cardiovasc Res. 2002, 55, 714–726. [CrossRef]
- Landschulz, K.T.; Pathak, R.K.; Rigotti, A.; Krieger, M.; Hobbs, H.H. Regulation of Scavenger Receptor, Class B, Type I, a High Density Lipoprotein Receptor, in Liver and Steroidogenic Tissues of the Rat. J Clin Invest. 1996, 98, 984–995. [Google Scholar] [CrossRef]
- Stangl, H.; Graf, G.A.; Yu, L.; Cao, G.; Wyne, K. Effect of Estrogen on Scavenger Receptor BI Expression in the Rat . J Endocrinol. 2002, 175, 663–672. [Google Scholar] [CrossRef]
- Darabi, M.; Rabbani, M.; Ani, M.; Zarean, E.; Panjehpour, M.; Movahedian, A. Increased Leukocyte ABCA1 Gene Expression in Post-Menopausal Women on Hormone Replacement Therapy. Gynecol Endocrinol. 2011, 27, 701–705. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Liu, Y.; Zhu, L.; Wang, W.; Wan, Z.; Chen, F.; Wu, Y.; Zhou, J.; Yuan, Z. 17β-Estradiol Promotes Cholesterol Efflux from Vascular Smooth Muscle Cells through a Liver X Receptor α-Dependent Pathway. Int J Mol Med 2014, 33, 550–558. [Google Scholar] [CrossRef] [PubMed]
- El Khoudary, S.R.; Hutchins, P.M.; Matthews, K.A.; Brooks, M.M.; Orchard, T.J.; Ronsein, G.E.; Heinecke, J.W. Cholesterol Efflux Capacity and Subclasses of HDL Particles in Healthy Women Transitioning through Menopause. J Clin Endocrinol Metab 2016, 101, 3419–3428. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Zhuang, Y.; Qiang, H.; Liu, X.; Xu, R.; Wu, Y. Relationship between Endogenous Estrogen Concentrations and Serum Cholesteryl Ester Transfer Protein Concentrations in Chinese Women. Clin Chim Acta 2001, 314, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Cazita, P.M.; Berti, J.A.; Aoki, C.; Gidlund, M.; Harada, L.M.; Nunes, V.S.; Quintão, E.C.R.; Oliveira, H.C.F. Cholesteryl Ester Transfer Protein Expression Attenuates Atherosclerosis in Ovariectomized Mice. J Lipid Res 2003, 44, 33–40. [Google Scholar] [CrossRef]
- Ulioa, N.; Verdugo, C.; Rios, M.; Sep01veda, J.; Sepolveda, S.; Naveas, R.; Calvo, C. Increased Activity of Lecithin:Cholesterol Acyltransferase During Short-Term Oral Estrogen Progestin Replacement Therapy in a Group of Postmenopausal Women Metabolism 1998, 47, 297–300. [CrossRef]
- Brinton, E.A. Oral Estrogen Replacement Therapy in Postmenopausal Women Selectively Raises Levels and Production Rates of Lipoprotein A-I and Lowers Hepatic Lipase Activity Without Lowering the Fractional Catabolic Rate. Arterioscler Thromb Vasc Biol 1996, 16. [Google Scholar] [CrossRef] [PubMed]
- Jin, F.Y.; Kamanna, V.S.; Kashyap, M.L. Estradiol Stimulates Apolipoprotein A-I- but Not A-II-Containing Particle Synthesis and Secretion by Stimulating MRNA Transcription Rate in Hep G2 Cells. Arterioscler Thromb Vasc Biol 1998, 18. [Google Scholar] [CrossRef]
- Gardner, C.D.; Tribble, D.L.; Young, D.R.; Ahn, D.; Fortmann, S.P. Population Frequency Distributions of HDL, HDL2, and HDL3 Cholesterol and Apolipoproteins A-I and B in Healthy Men and Women and Associations with Age, Gender, Hormonal Status, and Sex Hormone Use: The Stanford Five City Project. Prev Med (Baltim) 2000, 31, 335–345. [Google Scholar] [CrossRef]
- Badeau, R.M.; Metso, J.; Wähälä, K.; Tikkanen, M.J.; Jauhiainen, M. Human Macrophage Cholesterol Efflux Potential Is Enhanced by HDL-Associated 17β-Estradiol Fatty Acyl Esters. Journal of Steroid Biochemistry and Molecular Biology 2009, 116, 44–49. [Google Scholar] [CrossRef]
- Badeau, R.M.; Metso, J.; Kovanen, P.T.; Lee-Rueckert, M.; Tikkanen, M.J.; Jauhiainen, M. The Impact of Gender and Serum Estradiol Levels on HDL-Mediated Reverse Cholesterol Transport. Eur J Clin Invest 2013, 43, 3177–323. [Google Scholar] [CrossRef]
- De Marinis, E.; Martini, C.; Trentalance, A.; Pallottini, V. Sex Differences in Hepatic Regulation of Cholesterol Homeostasis. J Endocrinol 2008, 198, 635–643. [Google Scholar] [CrossRef]
- Duan, L.P.; Wang, H.H.; Ohashi, A.; Wang, D.Q.H. Role of Intestinal Sterol Transporters Abcg5, Abcg8, and Npc111 in Cholesterol Absorption in Mice: Gender and Age Effects. Am J Physiol Gastrointest Liver Physiol 2006, 290, G269–G276. [Google Scholar] [CrossRef]
- Carrier, J.C.; Deblois, G.; Champigny, C.; Levy, E.; Giguère, V. Estrogen-Related Receptor α (ERRα) Is a Transcriptional Regulator of Apolipoprotein A-IV and Controls Lipid Handling in the Intestine. J Biol Chem 2004, 279, 52052–52058. [Google Scholar] [CrossRef] [PubMed]
- Wiese, C.B.; Agle, Z.W.; Zhang, P.; Reue, K. Chromosomal and Gonadal Sex Drive Sex Differences in Lipids and Hepatic Gene Expression in Response to Hypercholesterolemia and Statin Treatment. Biol Sex Differ 2022, 13, 63. [Google Scholar] [CrossRef] [PubMed]
- García-Calzón, S.; Perfilyev, A.; de Mello, V.D.; Pihlajamäki, J.; Ling, C. Sex Differences in the Methylome and Transcriptome of the Human Liver and Circulating HDL-Cholesterol Levels. J Clin Endocrinol Metab 2018, 103, 4395–4408. [Google Scholar] [CrossRef]
- Lee, G.; Jeon, H.K.; Yoo, H.Y. Sex-Related Differences in Single Nucleotide Polymorphisms Associated with Dyslipidemia in a Korean Population. Lipids Health Dis 2022, 21. [Google Scholar] [CrossRef]
- Link, J.C.; Chen, X.; Prien, C.; Borja, M.S.; Hammerson, B.; Oda, M.N.; Arnold, A.P.; Reue, K. Increased High-Density Lipoprotein Cholesterol Levels in Mice with XX versus XY Sex Chromosomes. Arterioscler Thromb Vasc Biol 2015, 35, 1778–1786. [Google Scholar] [CrossRef]
- Van, P.L.; Bakalov, V.K.; Bondy, C.A. Monosomy for the X-Chromosome Is Associated with an Atherogenic Lipid Profile. J Clin Endocrinol Metab 2006, 91, 2867–2870. [Google Scholar] [CrossRef]
- AlSiraj, Y.; Chen, X.; Thatcher, S.E.; Temel, R.E.; Cai, L.; Blalock, E.; Katz, W.; Ali, H.M.; Petriello, M.; Deng, P. XX Sex Chromosome Complement Promotes Atherosclerosis in Mice. Nat Commun 2019, 10, 2631. [Google Scholar] [CrossRef] [PubMed]
- Gouni-Berthold, I.; Laufs, U. Special Aspects of Cholesterol Metabolism in Women. Dtsch Arztebl Int 2024, 121, 401–406. [Google Scholar] [CrossRef]
- Nielsen, S.T.; Lytsen, R.M.; Strandkjær, N.; Rasmussen, I.J.; Sillesen, A.S.; B. Vøgg, R.O.; Raja, A.A.; Nordestgaard, B.G.; Kamstrup, P.R.; Iversen, K. Significance of Lipids, Lipoproteins, and Apolipoproteins during the First 14–16 Months of Life. Eur Heart J 2023, 44, 178–183. [Google Scholar] [CrossRef]
- Felzer-Kim, I.T.; Visker, J.R.; Ferguson, D.P.; Hauck, J.L. Infant Blood Lipids: A Systematic Review of Predictive Value and Influential Factors. Expert Rev Cardiovasc Ther 2020, 18, 381–394. [Google Scholar] [CrossRef] [PubMed]
- Enkhmaa B, Berglund L. Non-genetic influences on lipoprotein(a) concentrations. Atherosclerosis, 202; 349, 53–62. [CrossRef]
- Frohlich, J.; Dobiášová, M.; Adler, L.; Francis, M. Gender Differences in Plasma Levels of Lipoprotein (a) in Patients with Angiographically Proven Coronary Artery Disease. Physiol Res 2004, 53, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Nenseter, M.S.; Lindvig, H.W.; Ueland, T.; Langslet, G.; Ose, L.; Holven, K.B.; Retterstøl, K. Lipoprotein(a) Levels in Coronary Heart Disease-Susceptible and -Resistant Patients with Familial Hypercholesterolemia. Atherosclerosis 2011, 216. [Google Scholar] [CrossRef]
- Øyri, L.K.L.; Bogsrud, M.P.; Christensen, J.J.; Ulven, S.M.; Brantsæter, A.L.; Retterstøl, K.; Brekke, H.K.; Michelsen, T.M.; Henriksen, T.; Roeters van Lennep, J.E. Novel Associations between Parental and Newborn Cord Blood Metabolic Profiles in the Norwegian Mother, Father and Child Cohort Study. BMC Med 2021, 19, 91. [Google Scholar] [CrossRef] [PubMed]
- Holven, K.B.; Narverud, I.; van Lennep, J.R.; Versmissen, J.; Øyri, L.K.L.; Galema-Boers, A.; Langslet, G.; Ulven, S.M.; Veierød, M.B.; Retterstøl, K. Sex Differences in Cholesterol Levels from Birth to 19 Years of Age May Lead to Increased Cholesterol Burden in Females with FH. J Clin Lipidol 2018, 12, 748–755. [Google Scholar] [CrossRef] [PubMed]
- Johansen, A.K.; Bogsrud, M.P.; Christensen, J.J.; Rundblad, A.; Narverud, I.; Ulven, S.; Langslet, G.; Retterstøl, K.; Holven, K.B. Young Women with Familial Hypercholesterolemia Have Higher LDL-Cholesterol Burden than Men: Novel Data Using Repeated Measurements during 12-Years Follow-Up. Atherosclerosis Plus 2023, 51, 28–34. [Google Scholar] [CrossRef]
- Schreuder, M. M. , Hamkour, S., Siegers, K. E., Holven, K. B., Johansen, A. K., van de Ree, M. A., Imholz, B., Boersma, E., Louters, L., Bogsrud, M. P., Retterstøl, K., Visseren, F. L. J., Roeters van Lennep, J. E., & Koopal, C. (2023). LDL cholesterol targets rarely achieved in familial hypercholesterolemia patients: A sex and gender-specific analysis. Atherosclerosis 2023, 384, 117117. [Google Scholar] [CrossRef]
- MacGregor, K.A.; Ho, F.K.; Celis-Morales, C.A.; Pell, J.P.; Gallagher, I.J.; Moran, C.N. Association between Menstrual Cycle Phase and Metabolites in Healthy, Regularly Menstruating Women in UK Biobank, and Effect Modification by Inflammatory Markers and Risk Factors for Metabolic Disease. BMC Med 2023, 21, 488. [Google Scholar] [CrossRef]
- Mumford, S.L.; Schisterman, E.F.; Siega-Riz, A.M.; Browne, R.W.; Gaskins, A.J.; Trevisan, M.; Steiner, A.Z.; Daniels, J.L.; Zhang, C.; Perkins, N.J. A Longitudinal Study of Serum Lipoproteins in Relation to Endogenous Reproductive Hormones during the Menstrual Cycle: Findings from the BioCycle Study. J Clin Endocrinol Metab 2010, 95, E80–E85. [Google Scholar] [CrossRef]
- Barnett, J.B.; Woods, M.N.; Lamon-Fava, S.; Schaefer, E.J.; McNamara, J.R.; Spiegelman, D.; Hertzmark, E.; Goldin, B.; Longcope, C.; Gorbach, S.L. Plasma Lipid and Lipoprotein Levels during the Follicular and Luteal Phases of the Menstrual Cycle. J Clin Endocrinol Metab 2004, 89, 776–782. [Google Scholar] [CrossRef]
- Vashishta, S.; Gahlot, S.; Goyal, R. Effect of Menstrual Cycle Phases on Plasma Lipid and Lipoprotein Levels in Regularly Menstruating Women. J Clin Diagn Res 2017, 11, CC05–CC07. [Google Scholar] [CrossRef]
- Bartels, Ä.; O’Donoghue, K. Cholesterol in Pregnancy: A Review of Knowns and Unknowns. Obstet Med 2011, 4, 147–151. [Google Scholar] [CrossRef]
- Lewek, J.; Banach, M. Dyslipidemia Management in Pregnancy: Why Is It Not Covered in the Guidelines? Curr Atheroscler Rep 2022, 24, 547–556. [Google Scholar] [CrossRef]
- Bartels, Ä.; Egan, N.; Broadhurst, D.I.; Khashan, A.S.; Joyce, C.; Stapleton, M.; O’Mullane, J.; O’Donoghue, K. Maternal Serum Cholesterol Levels Are Elevated from the 1st Trimester of Pregnancy: A Cross-Sectional Study. J Obstet Gynaecol (Lahore) 2012, 32, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Belo, L.; Caslake, M.; Santos-Silva, A.; Castro, E.M.B.; Pereira-Leite, L.; Quintanilha, A.; Rebelo, I. LDL Size, Total Antioxidant Status and Oxidised LDL in Normal Human Pregnancy: A Longitudinal Study. Atherosclerosis 2004, 177, 391–399. [Google Scholar] [CrossRef]
- Stuebe, A.M.; Rich-Edwards, J.W. The Reset Hypothesis: Lactation and Maternal Metabolism. Am J Perinatol 2009, 26, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Gunderson, E.P.; Lewis, C.E.; Wei, G.S.; Whitmer, R.A.; Quesenberry, C.P.; Sidney, S. Lactation and Changes in Maternal Metabolic Risk Factors. Obstet Gynecol 2007, 109, 729–738. [Google Scholar] [CrossRef] [PubMed]
- Kallio, M.J.T.; Siimes, M.A.; Perheentupa, J.; Salmenperä, L.; Miettinen, T.A. Serum Cholesterol and Lipoprotein Concentrations in Mothers during and after Prolonged Exclusive Lactation. Metabolism 1992, 41, 1327–1330. [Google Scholar] [CrossRef]
- Matthews, K.A.; Crawford, S.L.; Chae, C.U.; Everson-Rose, S.A.; Sowers, M.F.; Sternfeld, B.; Sutton-Tyrrell, K. Are Changes in Cardiovascular Disease Risk Factors in Midlife Women Due to Chronological Aging or to the Menopausal Transition? J Am Coll Cardiol 2009, 54, 2366–2372. [Google Scholar] [CrossRef]
- Ambikairajah, A.; Walsh, E.; Cherbuin, N. Lipid Profile Differences during Menopause: A Review with Meta-Analysis. Menopause 2019, 26, 1327–1333. [Google Scholar] [CrossRef] [PubMed]
- Song, D.K.; Hong, Y.S.; Sung, Y.A.; Lee, H. The Effect of Menopause on Cardiovascular Risk Factors According to Body Mass Index in Middle-Aged Korean Women. PLoS One 2023, 18, e0283393. [Google Scholar] [CrossRef] [PubMed]
- Lou, Z.; Huang, Y.; Lan, Y.; Li, C.; Chu, K.; Chen, P.; Xu, W.; Ma, L.; Zhou, J. Relationship between Years since Menopause and Lipid Variation in Postmenopausal Women: A Cross-Sectional Study. Medicine (United States) 2023, 102, E32684. [Google Scholar] [CrossRef] [PubMed]
- El Khoudary, S.R. HDL and the Menopause. Curr Opin Lipidol 2017, 28, 328–336. [Google Scholar] [CrossRef]
- Simony, S.B.; Mortensen, M.B.; Langsted, A.; Afzal, S.; Kamstrup, P.R.; Nordestgaard, B.G. Sex Differences of Lipoprotein(a) Levels and Associated Risk of Morbidity and Mortality by Age: The Copenhagen General Population Study. Atherosclerosis 2022, 355, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Roeters Van Lennep, J.E.; Heida, K.Y.; Bots, M.L.; Hoek, A. Cardiovascular Disease Risk in Women with Premature Ovarian Insufficiency: A Systematic Review and Meta-Analysis. Eur J Prev Cardiol 2016, 23, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Knauff, E.A.H.; Westerveld, H.E.; Goverde, A.J.; Eijkemans, M.J.; Valkenburg, O.; Van Santbrink, E.J.P.; Fauser, B.C.J.M.; Van Der Schouw, Y.T. Lipid Profile of Women with Premature Ovarian Failure. Menopause 2008, 15, 919–923. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Fang, L.; Wu, Z.; Li, Y.; Jia, Q.; Cheng, J.C.; Sun, Y.P. A Meta-Analysis of Serum Lipid Profiles in Premature Ovarian Insufficiency. Reprod Biomed Online 2022, 44, 539–547. [Google Scholar] [CrossRef]
- Liang, J.; Zhang, B.; Hu, Y.; Na, Z.; Li, D. Effects of Steroid Hormones on Lipid Metabolism in Sexual Dimorphism: A Mendelian Randomization Study. Front Endocrinol (Lausanne) 2023, 13, 1119154. [Google Scholar] [CrossRef]
- Wekker, V.; Van Dammen, L.; Koning, A.; Heida, K.Y.; Painter, R.C.; Limpens, J.; Laven, J.S.E.; Van Lennep, J.E.R.; Roseboom, T.J.; Hoek, A. Long-Term Cardiometabolic Disease Risk in Women with PCOS: A Systematic Review and Meta-Analysis. Hum Reprod Update 2020, 26, 942–960. [Google Scholar] [CrossRef]
- Fu, L.; Xie, N.; Qu, F.; Zhou, J.; Wang, F. The Association Between Polycystic Ovary Syndrome and Metabolic Syndrome in Adolescents: A Systematic Review and Meta-Analysis. Reprod Sci 2023, 30, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Melo, A.S.; Rosa-E-Silva, J.C.; De Sá Rosa-E-Silva, A.C.J.; Poli-Neto, O.B.; Ferriani, R.A.; Vieira, C.S. Unfavorable Lipid Profile in Women with Endometriosis. Fertil Steril 2010, 93, 2433–2436. [Google Scholar] [CrossRef] [PubMed]
- Dragoman, M.; Curtis, K.M.; Gaffield, M.E. Combined Hormonal Contraceptive Use among Women with Known Dyslipidemias: A Systematic Review of Critical Safety Outcomes. Contraception 2016, 94, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Palacios, S.; Colli, E.; Regidor, P.A. Metabolic and Laboratory Effects of a Progestin-Only Pill Containing Drospirenone 4 Mg in Comparison to Desogestrel 75 Μg: A Double-Blind, Double-Dummy, Prospective, Randomised Study Eur J Contracept Reprod Health Care 2021, 26, 454–461. [CrossRef]
- Lobo, R.A.; Skinner, J.B.; Lippman, J.S.; Cirillo, S.J. Plasma Lipids and Desogestrel and Ethinyl Estradiol: A Meta-Analysis. Fertil Steril 1996, 65, 1100–1109. [Google Scholar] [CrossRef] [PubMed]
- Klipping, C.; Duijkers, I.; Mawet, M.; Maillard, C.; Bastidas, A.; Jost, M.; Foidart, J.M. Endocrine and Metabolic Effects of an Oral Contraceptive Containing Estetrol and Drospirenone. Contraception 2021, 103, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Mawet, M.; Maillard, C.; Klipping, C.; Zimmerman, Y.; Foidart, J.M.; Bennink, H.J.T.C. Unique Effects on Hepatic Function, Lipid Metabolism, Bone and Growth Endocrine Parameters of Estetrol in Combined Oral Contraceptives. Eur J Contracept Reprod Health Care 2015, 20, 463–475. [Google Scholar] [CrossRef]
- Guazzelli, C.A.F.; Barreiros, F.A.; Barbosa, R.; Torloni, M.R.; Barbieri, M. Extended Regimens of the Contraceptive Vaginal Ring versus Hormonal Oral Contraceptives: Effects on Lipid Metabolism. Contraception 2012, 85, 389–393. [Google Scholar] [CrossRef]
- Creasy, G.W.; Fisher, A.C.; Hall, N.; Shangold, G.A. Transdermal Contraceptive Patch Delivering Norelgestromin and Ethinyl Estradiol: Effects on the Lipid Profile. J Reprod Med 2003, 48, 179–186. [Google Scholar] [PubMed]
- Porkka, K.V.K.; Erkkola, R.; Taimela, S.; Raitakari, O.T.; Dahlen, G.H.; Viikari, J.S.A. Influence of Oral Contraceptive Use on Lipoprotein (a) and Other Coronary Heart Disease Risk Factors. Ann Med 1995, 27, 193–198. [Google Scholar] [CrossRef]
- Barkfeldt, J.; Virkkunen, A.; Dieben, T. The Effects of Two Progestogen-Only Pills Containing Either Desogestrel (75 Μg/Day) or Levonorgestrel (30 Μg/Day) on Lipid Metabolism. Contraception 2001, 64, 295–299. [Google Scholar] [CrossRef]
- Ng, Y.W.; Liang, S.; Singh, K. Effects of Mirena (Levonorgestrel-Releasing Intrauterine System) and Ortho Gynae T380 Intrauterine Copper Device on Lipid Metabolism-a Randomized Comparative Study. Contraception 2009, 79, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Nie, G.; Yang, X.; Wang, Y.; Liang, W.; Li, X.; Luo, Q.; Yang, H.; Liu, J.; Wang, J.; Guo, Q.; Yu, Q.; Liang, X. The Effects of Menopause Hormone Therapy on Lipid Profile in Postmenopausal Women: A Systematic Review and Meta-Analysis. Front Pharmacol 2022, 13, 850815. [Google Scholar] [CrossRef] [PubMed]
- Gregersen, I.; Høibraaten, E.; Holven, K.B.; Løvdahl, L.; Ueland, T.; Mowinckel, M.C.; Dahl, T.B.; Aukrust, P.; Halvorsen, B.; Sandset, P.M. Effect of Hormone Replacement Therapy on Atherogenic Lipid Profile in Postmenopausal Women. Thromb Res 2019, 184, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Anagnostis, P.; Galanis, P.; Chatzistergiou, V.; Stevenson, J.C.; Godsland, I.F.; Lambrinoudaki, I.; Theodorou, M.; Goulis, D.G. The Effect of Hormone Replacement Therapy and Tibolone on Lipoprotein (a) Concentrations in Postmenopausal Women: A Systematic Review and Meta-Analysis. Maturitas 2017, 99, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Rezende, G.P.; Dassie, T.; Gomes, D.A.Y.; Benetti-Pinto, C.L. Cardiovascular Risk Factors in Premature Ovarian Insufficiency Using Hormonal Therapy. Revista Brasileira de Ginecologia e Obstetricia 2022, 45, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Goldštajn, M.Š.; Mikuš, M.; Ferrari, F.A.; Bosco, M.; Uccella, S.; Noventa, M.; Török, P.; Terzic, S.; Laganà, A.S.; Garzon, S. Effects of Transdermal versus Oral Hormone Replacement Therapy in Postmenopause: A Systematic Review. Arch Gynecol Obstet 2023, 307, 1727–1745. [Google Scholar] [CrossRef] [PubMed]
- Allard, M.D.; Saeedi, R.; Yousefi, M.; Frohlich, J. Risk Stratification of Patients with Familial Hypercholesterolemia in a Multi-Ethnic Cohort. Lipids Health Dis 2014, 13, 65. [Google Scholar] [CrossRef] [PubMed]
- Markus, M.R.P.; Ittermann, T.; Schipf, S.; Bahls, M.; Nauck, M.; Völzke, H.; Santos, R.D.; Peters, A.; Zeller, T.; Felix, S.B. Association of Sex-Specific Differences in Lipoprotein(a) Concentrations with Cardiovascular Mortality in Individuals with Type 2 Diabetes Mellitus. Cardiovasc Diabetol 2021, 20, 168. [Google Scholar] [CrossRef] [PubMed]
- Pino, B.D.; Gorini, F.; Gaggini, M.; Landi, P.; Pingitore, A.; Vassalle, C. Lipoprotein(a), Cardiovascular Events and Sex Differences: A Single Cardiological Unit Experience. J Clin Med 2023, 12, 764. [Google Scholar] [CrossRef]
- Cook, N.R.; Mora, S.; Ridker, P.M. Lipoprotein(a) and Cardiovascular Risk Prediction Among Women. J Am Coll Cardiol 2018, 72, 287–296. [Google Scholar] [CrossRef]
- Nordestgaard, B.G.; Benn, M.; Schnohr, P.; Tybjærg-Hansen, A. Nonfasting Triglycerides and Risk of Myocardial Infarction, Ischemic Heart Disease, and Death in Men and Women. JAMA 2007, 298, 299–308. [Google Scholar] [CrossRef]
- Wadström, B.N.; Wulff, A.B.; Pedersen, K.M.; Jensen, G.B.; Nordestgaard, B.G. Elevated Remnant Cholesterol Increases the Risk of Peripheral Artery Disease, Myocardial Infarction, and Ischaemic Stroke: A Cohort-Based Study. Eur Heart J 2022, 43, 3258–3269. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.K.; Levit, R.D.; Wood, M.J.; Aggarwal, N.; O’Donoghue, M.L.; Lim, S.S.; Lindley, K.; Gaignard, S.; Quesada, O.; Vatsa, N. Chronic Rheumatologic Disorders and Cardiovascular Disease Risk in Women Am Heart J Plus 2023, 27, 100267. [CrossRef]
- Lu, Y.; Li, S.X.; Liu, Y.; Rodriguez, F.; Watson, K.E.; Dreyer, R.P.; Khera, R.; Murugiah, K.; D’Onofrio, G.; Spatz, E.S. Sex-Specific Risk Factors Associated With First Acute Myocardial Infarction in Young Adults. JAMA Netw Open 2022, E229953. [Google Scholar] [CrossRef]
- Okoth, K.; Chandan, J.S.; Marshall, T.; Thangaratinam, S.; Thomas, G.N.; Nirantharakumar, K.; Adderley, N.J. Association between the Reproductive Health of Young Women and Cardiovascular Disease in Later Life: Umbrella Review. The BMJ 2020, 371, m3502. [Google Scholar] [CrossRef] [PubMed]
- Fabunmi, O.A.; Dludla, P. V.; Nkambule, B.B. Investigating Cardiovascular Risk in Premenopausal Women on Oral Contraceptives: Systematic Review with Meta-Analysis. Front Cardiovasc Med 2023, 10, 1127104. [Google Scholar] [CrossRef] [PubMed]
- Yoon, C.W.; Bushnell, C.D. Stroke in Women: A Review Focused on Epidemiology, Risk Factors, and Outcomes. J Stroke 2023, 25, 2–15. [Google Scholar] [CrossRef]
- Hodis, H.N.; Mack, W.J. Menopausal Hormone Replacement Therapy and Reduction of All-Cause Mortality and Cardiovascular Disease: It Is about Time and Timing. Cancer J 2022, 28, 208–223. [Google Scholar] [CrossRef]
- Greenlee, H.; Iribarren, C.; Rana, J.S.; Cheng, R.; Nguyen-Huynh, M.; Rillamas-Sun, E.; Shi, Z.; Laurent, C.A.; Lee, V.S.; Roh, J.M. Risk of Cardiovascular Disease in Women With and Without Breast Cancer: The Pathways Heart Study. J Clin Oncol 2022, 40, 1647–1658. [Google Scholar] [CrossRef] [PubMed]
- Regitz-Zagrosek, V.; Gebhard, C. Gender Medicine: Effects of Sex and Gender on Cardiovascular Disease Manifestation and Outcomes. Nat Rev Cardiol 2023, 20, 236–247. [Google Scholar] [CrossRef]
- Van Dam-Nolen, D.H.K.; Van Egmond, N.C.M.; Koudstaal, P.J.; Van Der Lugt, A.; Bos, D. Sex Differences in Carotid Atherosclerosis: A Systematic Review and Meta-Analysis. Stroke 2023, 54, 315–326. [Google Scholar] [CrossRef]
- ten Haaf, M.; Rijndertse, M.; Cheng, J.; de Boer, S.; Garcia-Garcia, H.; van Geuns, R.-J.; Regar, E.; Lenzen, M.; Appelman, Y.; Boersma, E. Sex Differences in Plaque Characteristics by Intravascular Imaging in Patients with Coronary Artery Disease. EuroIntervention 2017, 13, 320–328. [Google Scholar] [CrossRef]
- Kerkhof, P.L.M.; Tona, F. Sex Differences in Diagnostic Modalities of Atherosclerosis in the Macrocirculation. Atherosclerosis 2023, 384, 117275. [Google Scholar] [CrossRef]
- Reynolds, H.R.; Shaw, L.J.; Min, J.K.; Spertus, J.A.; Chaitman, B.R.; Berman, D.S.; Picard, M.H.; Kwong, R.Y.; Bairey-Merz, C.N.; Cyr, D.D. Association of Sex with Severity of Coronary Artery Disease, Ischemia, and Symptom Burden in Patients with Moderate or Severe Ischemia: Secondary Analysis of the ISCHEMIA Randomized Clinical Trial. JAMA Cardiol 2020, 5, 773–78. [Google Scholar] [CrossRef]
- Gasecka, A.; Zimodro, J.M.; Appelman, Y. Sex Differences in Antiplatelet Therapy: State-of-the Art. Platelets 2023, 34, 2176173. [Google Scholar] [CrossRef]
- Zhou, S.; Zhang, Y.; Dong, X.; Zhang, X.; Ma, J.; Li, N.; Shi, H.; Yin, Z.; Xue, Y.; Hu, Y. Sex Disparities in Management and Outcomes among Patients with Acute Coronary Syndrome. JAMA Netw Open 2023, 6, E2338707. [Google Scholar] [CrossRef] [PubMed]
- Kavurma, M.M.; Boccanfuso, L.; Cutmore, C.; Passam, F.; Patel, S.; Hennessy, A.; Loa, J.; Figtree, G.A.; Golledge, J.; Robinson, D.A. A Hidden Problem: Peripheral Artery Disease in Women. Eur Heart J Qual Care Clin Outcomes 2023, 9, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, G.; Bosisio, R.; Calabresi, L.; Magni, P.; Pavanello, C.; Pazzucconi, F.; Sirtori, C.R. Gender-Related Lipid and/or Lipoprotein Responses to Statins in Subjects in Primary and Secondary Prevention. J Clin Lipidol 2015, 9. [Google Scholar] [CrossRef]
- Fulcher, J.; O’Connell, R.; Voysey, M.; Emberson, J.; Blackwell, L.; Mihaylova, B.; Simes, J.; Collins, R.; Kirby, A.; Colhoun, H. Efficacy and Safety of LDL-Lowering Therapy among Men and Women: Meta-Analysis of Individual Data from 174 000 Participants in 27 Randomised Trials. The Lancet 2015, 385, 1397–1405. [Google Scholar] [CrossRef]
- Hunt, N.B.; Emmens, J.E.; Irawati, S.; de Vos, S.; Bos, J.H.J.; Wilffert, B.; Hak, E.; de Boer, R.A. Sex Disparities in the Effect of Statins on Lipid Parameters The PharmLines Initiative. Medicine (United States) 2022, 101, e28394. [Google Scholar] [CrossRef]
- Kato, E.T.; Cannon, C.P.; Blazing, M.A.; Bohula, E.; Guneri, S.; White, J.A.; Murphy, S.A.; Park, J.G.; Braunwald, E.; Giugliano, R.P. Efficacy and Safety of Adding Ezetimibe to Statin Therapy among Women and Men: Insight from IMPROVE-IT (Improved Reduction of Outcomes: Vytorin Efficacy International Trial). J Am Heart Assoc 2017, 6, e006901. [Google Scholar] [CrossRef]
- Cannon, C.P.; Blazing, M.A.; Giugliano, R.P.; McCagg, A.; White, J.A.; Theroux, P.; Darius, H.; Lewis, B.S.; Ophuis, T.O.; Jukema, J.W. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. N Engl J Med 2015, 372, 2387–2397. [Google Scholar] [CrossRef] [PubMed]
- Abramson, B.L.; Benlian, P.; Hanson, M.E.; Lin, J.; Shah, A.; Tershakovec, A.M. Response by Sex to Statin plus Ezetimibe or Statin Monotherapy: A Pooled Analysis of 22,231 Hyperlipidemic Patients. Lipids Health Dis 2011, 10, 146. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.G.; Lee, S.J.; Lee, Y.J.; You, S.C.; Hong, S.J.; Yun, K.H.; Hong, B.K.; Heo, J.H.; Rha, S.W.; Hong, S.J. Effect of Moderate-Intensity Statin with Ezetimibe Combination vs. High-Intensity Statin Therapy According to Sex in Patients with Atherosclerosis. Sci Rep 2023, 13, 972–98. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, A.C.; Banach, M.; Catapano, A.L.; Duell, P.B.; Leiter, L.A.; Hanselman, J.C.; Lei, L.; Mancini, G.B.J. Evaluation of the Efficacy and Safety of Bempedoic Acid in Women and Men: Pooled Analyses from Phase 3 Trials. Atherosclerosis 2023, 384, 117192. [Google Scholar] [CrossRef]
- Cho, L.; Plutzky, J.; Brennan, D.; Louie, M.J.; Lei, L.; Robinson, P.; Powell, H.A.; Nicholls, S.J.; Lincoff, A.M.; Nissen, S.E. Impact of Bempedoic Acid on Cardiovascular Outcomes by Sex. Circulation 2024, 149, 1775–1777. [Google Scholar] [CrossRef]
- Sever, P.; Gouni-Berthold, I.; Keech, A.; Giugliano, R.; Pedersen, T.R.; Im, K.A.; Wang, H.; Knusel, B.; Sabatine, M.S.; O’donoghue, M.L. LDL-Cholesterol Lowering with Evolocumab, and Outcomes According to Age and Sex in Patients in the FOURIER Trial. Eur J Prev Cardiol 2021, 28, 805–812. [Google Scholar] [CrossRef]
- Vallejo-Vaz, A.J.; Ginsberg, H.N.; Davidson, M.H.; Eckel, R.H.; Cannon, C.P.; Lee, L.V.; Bessac, L.; Pordy, R.; Letierce, A.; Ray, K.K. Lower On-Treatment Low-Density Lipoprotein Cholesterol and Major Adverse Cardiovascular Events in Women and Men: Pooled Analysis of 10 ODYSSEY Phase 3 Alirocumab Trials. J Am Heart Assoc 2018, 7, e009221. [Google Scholar] [CrossRef]
- Myasoedova, V.A.; Rimbert, A.; Camera, M.; Le May, C.; Capoulade, R.; Cariou, B.; Poggio, P. LDL Lowering Effect of PCSK9 Inhibition Is Reduced in Women. Eur Heart J Cardiovasc Pharmacother 2023, 9, 337–342. [Google Scholar] [CrossRef]
- Rivera, F.B.; Cha, S.W.; Aparece, J.P.; Rocimo, A.; Ong, B.A.; Golbin, J.M.; Alfonso, P.G.; Enkhmaa, B.; Khan, S.U.; Cainzos-Achirica, M. Sex Differences in Cardiovascular Outcomes and Cholesterol-Lowering Efficacy of PCSK9 Inhibitors: Systematic Review and Meta-Analysis. JACC: Advances 2023, 2. [Google Scholar] [CrossRef]
- Galema-Boers, A.M.H.; Mulder, J.W.C.M.; Steward, K.; Roeters van Lennep, J.E. Sex Differences in Efficacy and Safety of PCSK9 Monoclonal Antibodies: A Real-World Registry. Atherosclerosis 2023, 384, 117108. [Google Scholar] [CrossRef]
- Paquette, M.; Faubert, S.; Saint-Pierre, N.; Baass, A.; Bernard, S. Sex Differences in LDL-C Response to PCSK9 Inhibitors: A Real World Experience. J Clin Lipidol 2023, 17, 142–149. [Google Scholar] [CrossRef]
- Zhang, H.; Plutzky, J.; Shubina, M.; Turchin, A. Drivers of the Sex Disparity in Statin Therapy in Patients with Coronary Artery Disease: A Cohort Study. PLoS One 2016, 11, e0155228. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Molemans, B.; Marieke Schoonen, W.; Giovas, P.; Bray, S.; Kiru, G.; Murphy, J.; Banach, M.; Servi, S. De; Gaita, D. EU-Wide Cross-Sectional Observational Study of Lipid-Modifying Therapy Use in Secondary and Primary Care: The DAVINCI Study. Eur J Prev Cardiol 2021, 28, 1279–1289. [Google Scholar] [CrossRef] [PubMed]
- Vrablik, M.; Seifert, B.; Parkhomenko, A.; Banach, M.; Jóźwiak, J.J.; Kiss, R.G.; Gaita, D.; Rašlová, K.; Zachlederova, M.; Bray, S. Lipid-Lowering Therapy Use in Primary and Secondary Care in Central and Eastern Europe: DA VINCI Observational Study. Atherosclerosis 2021, 334, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Gouni-Berthold, I.; Schaper, F.; Schatz, U.; Tabbert-Zitzler, A.; Fraass, U.; Sauer, S.; Ray, K.K. Low-Density Lipoprotein Cholesterol Goal Attainment in Germany: Results from the DA VINCI Study: LDL-C Goal Attainment in Germany. Atherosclerosis Plus 2022, 50, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Cannon, C.P.; De Lemos, J.A.; Rosenson, R.S.; Ballantyne, C.M.; Liu, Y.; Gao, Q.; Palagashvilli, T.; Alam, S.; Mues, K.E.; Bhatt, D.L. Use of Lipid-Lowering Therapies over 2 Years in GOULD, a Registry of Patients with Atherosclerotic Cardiovascular Disease in the US. JAMA Cardiol 2021, 6, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Agarwala, A.; Deych, E.; Jones, L.K.; Sturm, A.C.; Aspry, K.; Ahmad, Z.; Ballantyne, C.M.; Goldberg, A.C. Sex-Related Differences in Premature Cardiovascular Disease in Familial Hypercholesterolemia. J Clin Lipidol 2023, 17, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Iyen, B.; Qureshi, N.; Weng, S.; Roderick, P.; Kai, J.; Capps, N.; Durrington, P.N.; McDowell, I.F.; Soran, H.; Neil, A. Sex Differences in Cardiovascular Morbidity Associated with Familial Hypercholesterolaemia: A Retrospective Cohort Study of the UK Simon Broome Register Linked to National Hospital Records. Atherosclerosis 2020, 315. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Raal, F.J.; Kallend, D.G.; Jaros, M.J.; Koenig, W.; Leiter, L.A.; Landmesser, U.; Schwartz, G.G.; Lawrence, D.; Friedman, A. Inclisiran and Cardiovascular Events: A Patient-Level Analysis of Phase III Trials. Eur Heart J 2023, 44, 129–138. [Google Scholar] [CrossRef]
- O’Donoghue, M.L.; G. López, J.A.; Knusel, B.; Gencer, B.; Wang, H.; Wu, Y.; Kassahun, H.; Sabatine, M.S. Study Design and Rationale for the Olpasiran Trials of Cardiovascular Events And LipoproteiN(a) Reduction-DOSE Finding Study (OCEAN(a)-DOSE). Am Heart J 2022, 251, 61–69. [Google Scholar] [CrossRef]
- Van DIemen, J.; Verdonk, P.; Chieffo, A.; Regar, E.; Mauri, F.; Kunadian, V.; Sharma, G.; Mehran, R.; Appelman, Y. The Importance of Achieving Sex- And Gender-Based Equity in Clinical Trials: A Call to Action. Eur Heart J 2021, 42, 2990–2994. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Impact of estrogens on hepatic lipoprotein metabolism. The arrows indicate the activation or inhibition of selected molecular processes involved in hepatic lipoprotein metabolism. Apo – apolipoprotein; E – estrogens, ERα – estrogen receptor alpha; ERRα – estrogen-related receptor alpha; GPER – G protein-coupled estrogen receptor; HDL – high-density lipoprotein; HMG-CoA – 3-hydroxy-3-methyl-glutaryl-coenzyme A; LDL – low-density lipoprotein; LDL-R – low-density lipoprotein receptor; MTP – microsomal triglyceride transfer protein; PCSK9 – proprotein convertase subtilisin/kexin type 9; Pla2g12b – phospholipase A2 group XII B; SREBPs – sterol regulatory element-binding proteins; VLDL – very low-density lipoprotein. Created with BioRender.com.
Figure 1.
Impact of estrogens on hepatic lipoprotein metabolism. The arrows indicate the activation or inhibition of selected molecular processes involved in hepatic lipoprotein metabolism. Apo – apolipoprotein; E – estrogens, ERα – estrogen receptor alpha; ERRα – estrogen-related receptor alpha; GPER – G protein-coupled estrogen receptor; HDL – high-density lipoprotein; HMG-CoA – 3-hydroxy-3-methyl-glutaryl-coenzyme A; LDL – low-density lipoprotein; LDL-R – low-density lipoprotein receptor; MTP – microsomal triglyceride transfer protein; PCSK9 – proprotein convertase subtilisin/kexin type 9; Pla2g12b – phospholipase A2 group XII B; SREBPs – sterol regulatory element-binding proteins; VLDL – very low-density lipoprotein. Created with BioRender.com.
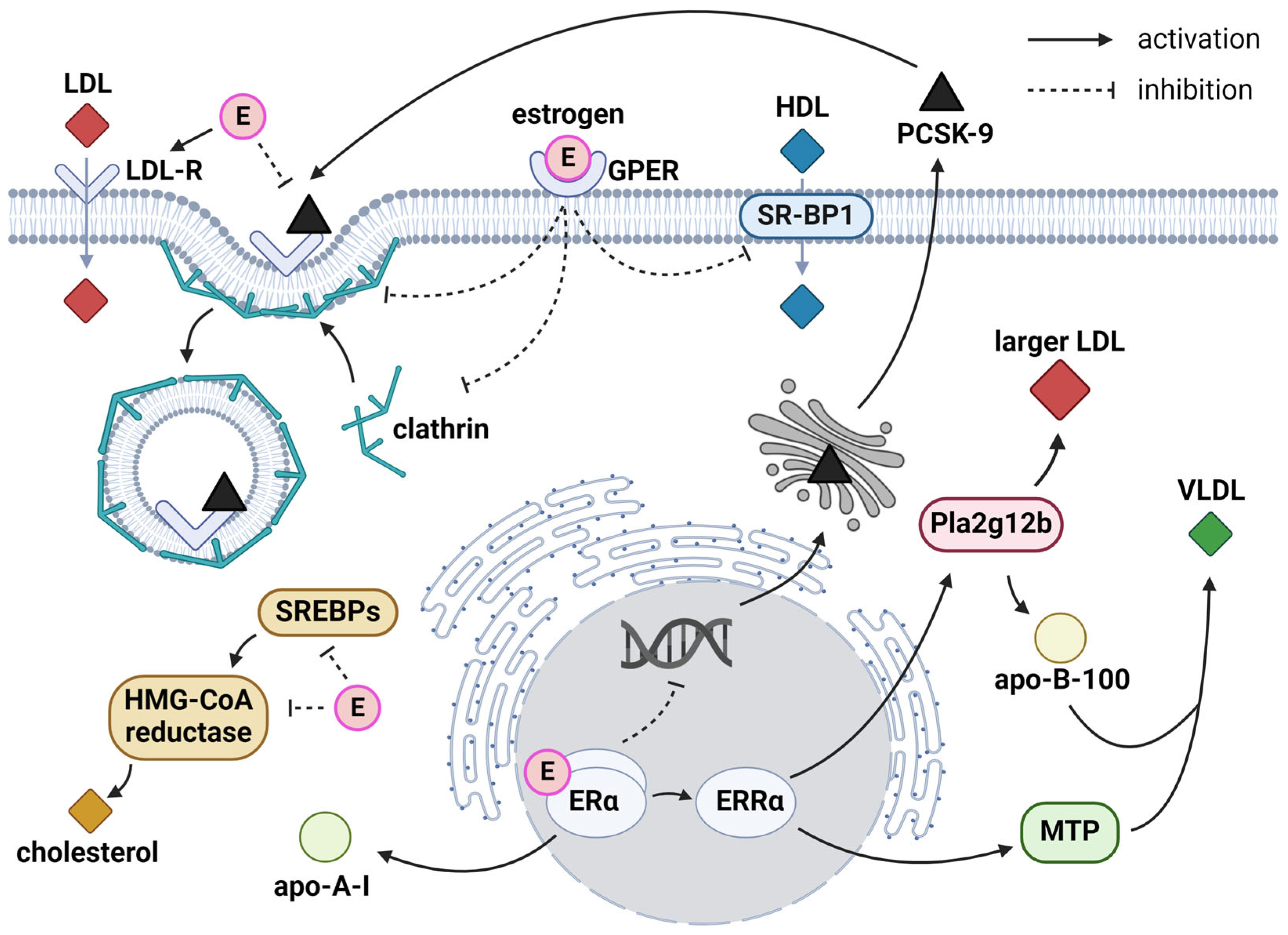
Figure 2.
Sex differences in lipid profiles early in life. The median concentrations presented were derived from [89]. Apo – apolipoprotein; HDL-C – high-density lipoprotein cholesterol; LDL-C - low-density lipoprotein cholesterol; TC – total cholesterol.
Figure 2.
Sex differences in lipid profiles early in life. The median concentrations presented were derived from [89]. Apo – apolipoprotein; HDL-C – high-density lipoprotein cholesterol; LDL-C - low-density lipoprotein cholesterol; TC – total cholesterol.
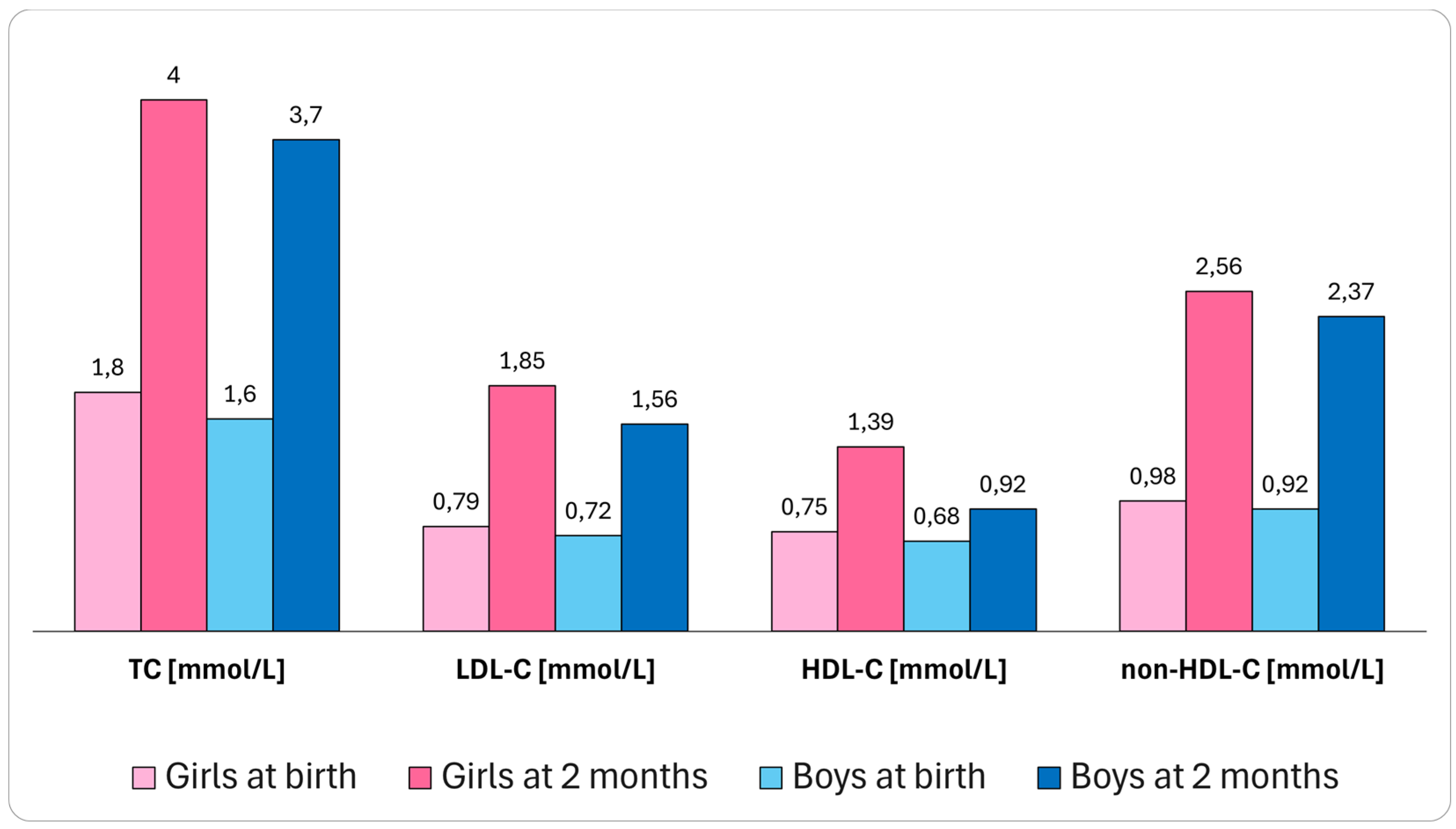
Figure 3.
Cardiovascular risk factors in postmenopausal women. The arrows indicate an increase or a decline in the prevalence of cardiovascular risk factors after menopausal transition. Apo – apolipoprotein; BP – blood pressure; LDL-C – low-density lipoprotein cholesterol; Lp(a) – lipoprotein (a); TC – total cholesterol. Created with BioRender.com.
Figure 3.
Cardiovascular risk factors in postmenopausal women. The arrows indicate an increase or a decline in the prevalence of cardiovascular risk factors after menopausal transition. Apo – apolipoprotein; BP – blood pressure; LDL-C – low-density lipoprotein cholesterol; Lp(a) – lipoprotein (a); TC – total cholesterol. Created with BioRender.com.
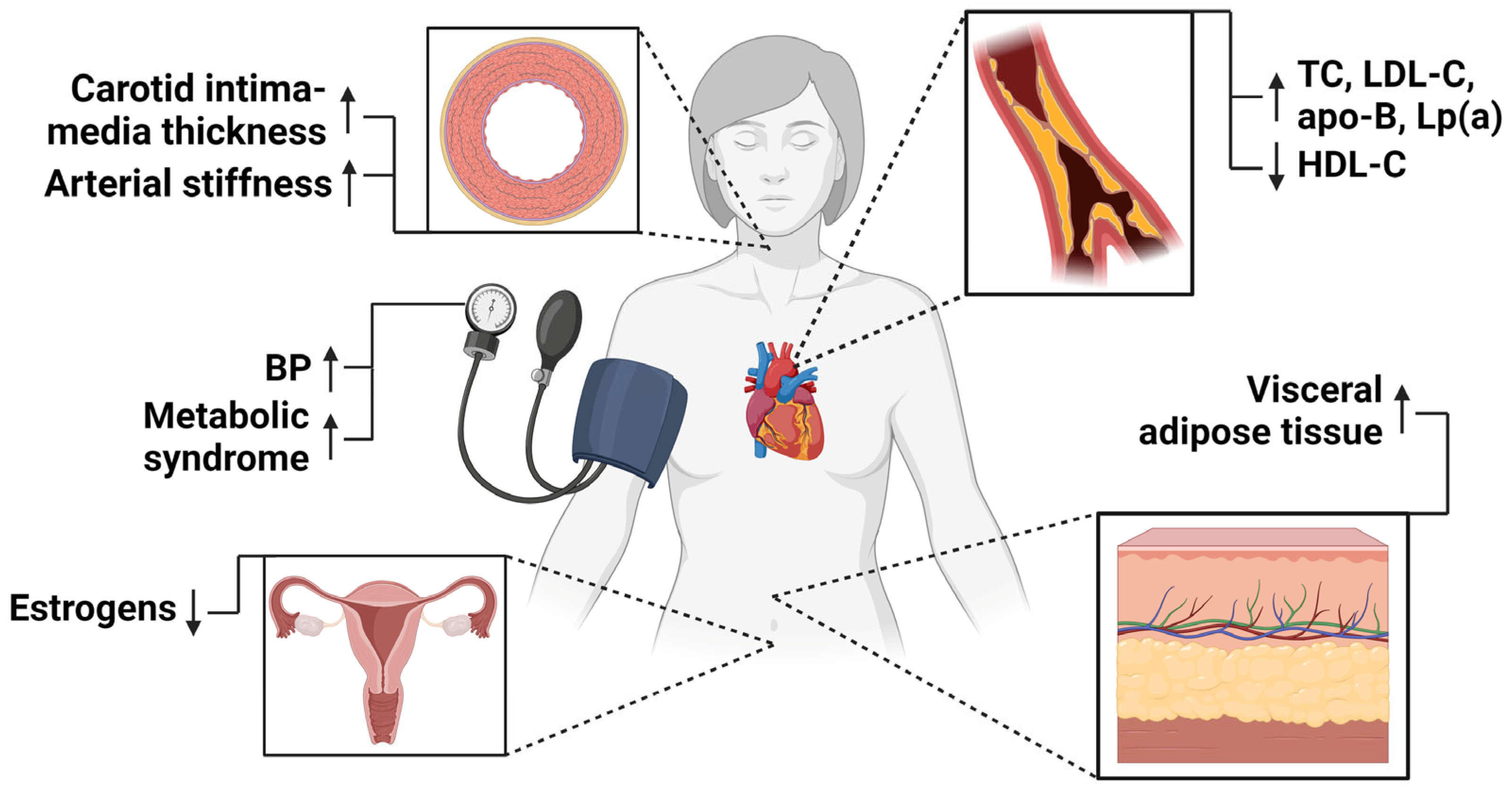
Figure 4.
Key messages about the management of dyslipidemia in women. HRT – hormone replacement therapy; LLT – lipid-lowering therapy; PCSK9 – proprotein convertase subtilisin/kexin type 9. Created with BioRender.com.
Figure 4.
Key messages about the management of dyslipidemia in women. HRT – hormone replacement therapy; LLT – lipid-lowering therapy; PCSK9 – proprotein convertase subtilisin/kexin type 9. Created with BioRender.com.
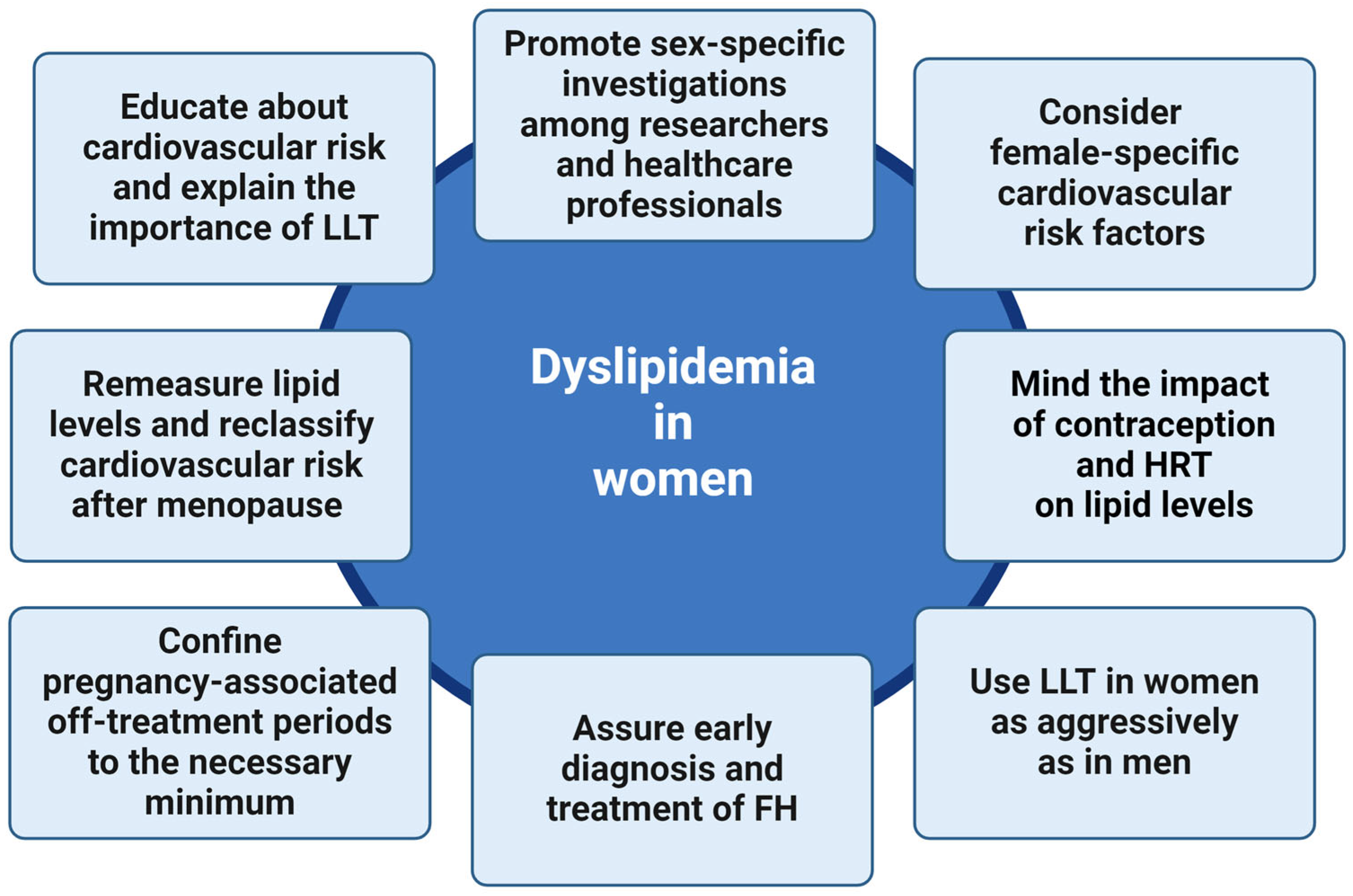
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



