Submitted:
21 June 2024
Posted:
24 June 2024
You are already at the latest version
Abstract
Edvard Munch, a founder of Expressionism was pre-occupied with depicting his subjective experience and the most prolific painter of self-portraits since Rembrandt. Based on evidence that faces and self-related images are more salient than other objects it is plausible that self-portraits, in which the subject and object are the same, reflect the artist’s state of mind. Although he suffered from a variety of physical and psychological illness Munch was not diagnosed with any specificity in his lifetime. Posthumous diagnoses include schizophrenia, anxiety, bipolar and other disorders. Recent research has revealed altered visual perception in such patients. The present study empirically analysed three stylistic elements of Munch’s painted self-portraits and portraits: contrast, colour and fractal dimension and his painted productivity, to determine if variations correlate with critical life events and if so whether they indicate states of mind. It found significant increases in contrast and colour brightness and persistent high complexity during critical periods supporting the conclusion that Munch is diagnostically best described as suffering from early onset schizophrenia and comorbid social anxiety disorder.
Keywords:
Neuroaesthetics
; Neurophysiology
; Stylistics
; Psychiatry
; Schizophrenia
; Anxiety
; Bipolar Disorder
; Vision
; Perception
; Self-portraits
; Edvard Munch.
Introduction
Edvard Munch, most famous for ‘The Scream’,1 was a founder of Expressionism a major source of modern art. He experienced hallucinations beginning in childhood, anxiety, depressive episodes, and delusions including paranoia. Until treatment age 45 he abused alcohol, was a heavy smoker and suffered multiple somatic complaints. Following treatment, he became abstinent and withdrew into ascetic isolation which he maintained until his death. He suffered respiratory illness throughout his life. Although a contemporary of the founders of modern psychiatry he was not diagnosed with any specificity in his lifetime. He has been posthumously diagnosed as suffering from schizophrenia, anxiety, bipolar and other disorders. He was pre-occupied with expressing his subjective experience and the most prolific painter of self-portraits since Rembrandt. The results of this empirical study of three characteristics of style: contrast, colour and fractal dimension and of productivity support the conclusion that Munch is diagnostically best described as suffering from early onset schizophrenia and comorbid social anxiety disorder.
Hypothesis
The brain is more interested in faces than other subjects and in self-images more than non-self-referential material (Alzueta et al., 2020; Northoff 2006; Żochowska et al., 2021). In self-portraits the subject and object are the same. There are three images involved: i) the artist’s face in the mirror or photograph, ii) the artist’s internal self-representation and iii) the image on a surface. The artist’s gaze, internal and external, never leaves the self. This constitutes a unique feedback system engaging visual perception, self-reflection and motor activity. We hypothesised
that longitudinal empirical analysis of style in self-portraits would indicate the artist’s mental state and be distinct from portraits of others.
Background
Edvard Munch (1863-1944) ‘Munch’ is regarded by many as the father of Expressionism a school of art focused on conveying the artist’s subjective experience particularly using colour and distortion (Cernuschi, 2001; Chilvers, 2009). Although Munch initially painted in a naturalistic manner this began to change with the ‘The Sick Child’ an image of his older sister dying of tuberculosis. He later referred to it as his ‘breakthrough’ (Holland, 2005, p. 184; Stang, 1977, p. 60; Tøjner, 2001 p. 144; hereafter, ‘Holland’, ‘Stang’, and ‘Tøjner’). The image was so important to him that he painted it six times over several decades in addition to multiple works on paper (Bruteig & Falck, 2013; Woll 2008, 2001). This change in style became consolidated in 1889 after the death of his father. Emerging from his grief he wrote his ‘St Cloud Manifesto’ in which he committed himself to no longer painting “interiors, people who read and women who knit” but instead, “living people who breathe and feel, suffer and love” (Tøjner, p. 60).
His determination to convey his own feelings in a new style became manifest in paintings of Despair (1892), Melancholy (1892), the Scream (1893), Anxiety (1894) and Jealousy (1895). Loneliness, illness, death, and bitter erotic experience became themes which continued to preoccupy him throughout his life.2 Munch was keenly aware of the role physical and psychological illness played in his life and considered both essential to his art (Lubow, 2006).3 This may explain why he resisted treatment, like other creative people, until he had a complete breakdown in 1908 (Rothenberg, 2001). He saw his art as essentially confessional, a form of autobiography and of self-therapy (Ustvedt, 2020, hereafter, ‘Ustvedt’). This is reflected in the number of self-portraits he painted, 51, in addition to 20 lithographs, including his first, and over 100 other works on paper (Bruteig & Falck, 2013; Woll, 2008, 2001).
Munch lived in the era in which the foundations of modern psychiatry were being laid (Freud, 1900; Janet, 1907; Jaspers, 1913; Kraepelin, 1896) and he and his circle were aware of these developments (Prideaux 2005, hereafter, ‘Prideaux’). Diagnosis, while at an early stage, was recognizably in accordance with modern constructs but not contemporaneously applied to him. Munch has been retrospectively diagnosed with a variety of disorders including schizophrenia, schizoid-psychosis, bipolar disorder (BPD), mania, narcissistic personality disorder, borderline personality disorder, anxiety, depression, agoraphobia, germophobia and alcoholism (Bowen, 1988; Miranda et al., 2013; Skryabin et al., 2020; Warick & Warick, 2014; Wylie, 1980; Wylie & Wylie, 1989). This illustrates both the complexity of his condition and the difficulty of post-mortem diagnosis even if relatively recent and where, as here, there is voluminous documentation (Frigg & Howard, 2011; ter Borg & Trenité, 2012; Voskuil, 2020).4
Munch displayed a wide variety of symptoms including panic, phobias, insomnia, somatic complaints, pressured speech, strange ideas, hallucinations, delusions and paranoia. The latter was evident on several occasions when he provoked others violently. His brawls with strangers were notorious. On at least four occasions he used a firearm once injuring himself and on another nearly killing a friend. He had three brief love affairs but never established a stable intimate relationship relying on prostitutes, servants and models for sexual experience. His sometimes intense friendships did not last long. He could not tolerate the physical presence of people for any length of time including family members with whom he maintained life-long attachments (Prideaux; Howe, 2001, hereafter ‘Howe’; Heller, 1984, hereafter, ‘Heller’).
During his lifetime heavy drinking, and promiscuous ‘bohemian’ behaviour was common among artists (Eggum, 1984; Prideaux; Weir, 2023) yet despite this and his myriad symptoms, Munch was a productive and innovative artist throughout his life including during periods when he sought recovery in sanitoria and clinics. While there is some evidence of cognitive impairment he was capable of successfully pursuing his commercial self-interest in a complex and rapidly evolving art market Beginning his career in relative poverty and heavily criticised he died wealthy and internationally recognised (Bruteig & Falck, 2013; Heller; Prideaux; Stenersen).
Biography
Munch was the second of five children born within six years to an army physician and a considerably younger tubercular mother. At the time of his December birth his parents were living in rented rooms in a rural farmhouse. In his first year the family moved to the then rapidly industrialising capital city of Kristiana (now Oslo). Although from a prominent family, Munch’s father had a modest income which declined as he established his practice in poor areas of the city causing the family to move several times as it approached poverty. This trend worsened after the death of Munch’s mother from tuberculosis when he was 5. His older sister died of the same disease when he was 14. Tuberculosis was so common in Norway at the time that it was known as the national disease (Harris, 2007; Wood, 1991). In 1912, near its peak, 80% of children in Kristiana were infected by the time they started school (Teemu, 2008).
At birth Munch was so ill with respiratory disease that his father made arrangements for his immediate baptism and burial (Prideaux). Munch suffered respiratory illness throughout his life on several occasions requiring hospitalisation. He was unable to attend school for extended periods due to ill health spending entire winters confined to bed and ultimately could not continue. At the time of his mother’s death and again during an episode of tubercular-like infection age 13, he experienced vivid religious hallucinations. He blamed himself for the death of his sister in the following year as she had nursed him. In addition to his mother and sister the disease was responsible for the deaths of his maternal grandmother and maternal aunt. Despite his chronic vulnerability he survived pneumonia and the Spanish Flu ultimately dying of bronchitis.
There is evidence of mental illness in Munch’s family. His paternal grandfather died in an asylum.5 One of Munch’s younger sisters had symptoms of schizophrenia in adolescence and spent most of her adult life in an institution. His father, who came from a devout family, became depressed following his wife’s death and expressed increasing religious obsession and dependence on alcohol. His father’s preoccupation with divine punishment in the form of disease and death was such that Munch’s childhood hallucinations were terrifying audible and visual images of angels, skeletons and devils there to draw him into death (Prideaux). He often woke in the middle of the night wondering whether he was in hell (Tøjner).
Munch therefore had multiple reasons for emotional distress. His respiratory disease presented a constant threat of death, embodied in the deaths of close relatives, and anxiety reinforced by his father’s religious preoccupations. It imposed repeated periods of social isolation compounded by frequent changes in household. Soon after birth his mother put him in her sister’s care. After this initial separation he then experienced the death of his mother and older sister to whom he attached himself in the aftermath. His aunt, who he suspected of wanting to marry his father and replace his mother, became the only adult on whom he could rely although she too was tubercular (Stenersen; Tøjner). Unlike his father, who strongly disapproved, she recognised and nurtured his artistic talent and supported his ambition to be an artist (Harris, 2004). Despite her attention and affection Munch kept her at a distance even unwilling to attend her funeral (Prideaux).
Against his father’s wishes Munch left technical college to pursue an artistic career attending art school for a year and then seeking informal instruction from various local artists. He adopted a bohemian lifestyle led by local writers and political radicals. During this time his abuse of alcohol and tobacco became apparent (Prideaux; Heller). His first exhibition in 1885 attracted the attention of the local art establishment which provided him with the means to study in Paris. He postponed the trip due to ill health and had his first love affair with a woman of his mother’s age, the wife of a cousin, a military physician like his father. The experience filled him with what can be reasonably seen as Oedipal guilt and shame expressed in a painting called “Ashes”.
The end of the affair precipitated a period of mental disturbance which included heavy drinking, vertigo, agoraphobia, despair and jealousy (Prideaux). By year-end he was sufficiently recovered to visit Paris then at the height of the Impressionism wave; a style he adopted for a time. On his return to Kristiana, he began work lasting over a year on ‘The Sick Child’ exhibited in 1886. To his dismay, given the importance of the subject to him and the intense effort he had made, it was heavily criticised by critics and the public. Munch was so discouraged he left Norway beginning two decades of voluntary exile first in France in 1889 and from 1892 in Germany. While in France he was virtually destitute, often going without food, drinking heavily, visiting brothels and gambling unsuccessfully (Heller. Prideaux, Stang).
In 1889 he suffered near fatal pneumonia and in 1890 received news of his father’s death. He moved away from his bohemian circle and became deeply depressed. He painted a series of dark blue images including one evocative of his father.6 His response to depression was the manifesto declaring his purpose from then on to only paint subjective experience (Eggum, 1984). Soon thereafter he was again hospitalised with pneumonia and suffered a nervous collapse. Still unrecognised as an artist he continued to drink heavily painting for days without rest (Prideaux). An exhibition in Berlin in 1892 so disturbed the conservative establishment that it was immediately closed down. The resulting ‘succes de scandale’ made him famous and attracted the attention of patrons and critics. In 1893, he recalled and painted the hallucinatory experience depicted in The Scream in which the figure and the environment seem to be dissolving.
“The air turned to blood – with cutting veins of flame….That shrill, bloody red. On the road and the fence. The faces of my comrades became a garish yellow-white. I felt a huge scream welling up inside me – and I really did hear a huge scream. The colours in nature broke the lines in nature. The lines and the colours quivered with movement. These vibrations of light caused not only the oscillation of my eyes. My ears were also affected and began to vibrate. So I actually heard a scream. Then I painted The Scream” (Tøjner, p. 96).
In 1894 his younger sister was institutionalised in an asylum near the bridge depicted in The Scream (Prideaux). In 1896 his only brother died of pneumonia age 30, shortly after his marriage, confirming Munch’s fear of marriage, association of female intimacy with death and compounding his sense of loss (Azeem, 2015; Stenersen; Tøjner). His difficulty in maintaining relationships and intense social anxiety led to frequent impulsive travelling both to escape intimate contact, particularly with women, and to pursue commercial opportunities (Prideaux; Stang).
Munch’s abuse of alcohol was so severe that he was the subject of concern by his contemporaries (Ustvedt). He sought respite in various sanatoria for a variety of somatic complaints including insomnia, gastrointestinal and cardiac distress, vertigo, limb numbness and phobias including agoraphobia and fear of beds which he associated with illness and death (Tøjner). During this time he also took various drugs including bromides, aspirin and medication for the heart, fever and rheumatism (Prideaux).
He experienced increasing paranoia, convinced that others were speaking disparagingly of and plotting against him. A struggle with an obsessive lover involving a revolver resulted in the loss of part of a finger on his left hand. He depicted her several times as Charlotte Corday and himself as the murdered Marat encapsulating both his anxiety about women and his association of sex and death. His condition deteriorated and in 1908, experiencing vivid auditory and visual hallucinations and paranoid delusions, he was admitted to a clinic in Copenhagen where he remained for 9 months. On admission he was diagnosed as having dementia paralytica due to alcohol poisoning (Heller; Prideaux; Tøjner).
He was sedated and received mild electric treatment, massage and scented baths but the ‘therapy’ essentially consisted of enforced abstinence, regular meals and rest. He became sober and remained largely abstinent thereafter. In a self-portrait painted just before his release he appears to be emerging from dissolution. In 1909 he returned to Norway having received a national honour and the public recognition he had long sought. He purchased rural property outside of Oslo and thereafter he lived in isolation “just like a monk” (Muller-Westermann, 2005; Prideaux; Stang, p. 222; Stenersen). He was unable to tolerate the presence even of close family members (Prideaux). Several housekeepers and models with whom he had sexual relations were tolerated but only so long as those relations continued.
He occasionally allowed patrons who had commissioned portraits to visit, but none were allowed to stay the night (Stenersen). He worked in an eccentric fashion talking constantly which he described as, “a defense” preventing others from speaking and their words entering and taking him over. He glanced at his subjects and then painted his first impression. Sitters often moved or left as he continued to talk and paint. He famously said, ‘I paint not what I see but what I saw” (Heller p. 42; Prideaux; Tøjner p. 63). This was his modus operandi; to capture not the detail of the image but its immediate impact on him (Ustvedt).
Although awarded large state and private commissions he lived an ascetic life despite increasing wealth. His style noticeably changed from his pre-treatment period and included landscapes and local people. He surrounded himself with copies of portraits he had painted which he referred to as his “guardians”, “children” and his “family”. He sometimes “punished” them by leaving them outside or banishing them to an upstairs storage room (Stenersen). When indoors he continually played a radio broadcasting in languages he did not understand, or simply white noise, to drown out other sounds and exclude intrusive invisible waves which he believed encircled the world. The house was kept illuminated as he was frightened of the dark. It was surrounded by barbed wire, the gates padlocked when he was present and he kept fierce dogs. He continued to suffer insomnia, have delusions and feelings of persecution, particularly by the tax authorities, until his death (Stenersen; Tøjner).
Somatic Illness
Munch’s chronic respiratory illness brought him near to death on at least four occasions. Although never diagnosed it seems likely that he suffered from congenital tuberculosis which has non-specific presentation including respiratory distress and chronic lung disease, and it mimics a variety of conditions including pneumonia (Li et al., 2019; Tomar et al., 2008). Transmitted by the mother it can cross the blood brain barrier and cause persistent neuroinflammation (Manjesse, et al., 2021). Tuberculosis is a heterogenous disease often characterised by remission in untreated adults and closely associated with anxiety, depression, psychosis and somatic disorders including insomnia (de Araújo et al., 2014; Monistrol-Mula, 2024; Sossen et al., 2023). Although physicians attending Munch would have been familiar with tuberculosis maternal transmission was only medically described in 1935 (Saramba & Zhao, 2016).
Mental Illness
Some observers have suggested that Munch suffered from bipolar disorder (BPD) (Rothenberg, 2001, 2015); others incline toward schizophrenia as a diagnosis (Skryabin et al., 2020). Both are plausible depending on which aspects of behaviour and which periods of Munch’s life are the focus. Others have suggested disorders which encompass symptoms which can be comorbid with both schizophrenia and BPD but do not exclude either (McElroy Bowen, 1988; Wylie, 1980).
Creativity
Creative people share genetic predispositions to both BPD and schizophrenia and to dysregulation of dopamine and serotonin (Power et al., 2015; Runco et al., 2011; Zhang et al., 2014). First degree relatives of schizophrenia patients are overrepresented in the creative professions as are the offspring and first degree relatives of BPD patients. Biographic and historiological studies of creative people and their close relatives have found associations with mood disorders, BPD, schizophrenia and alcohol abuse (Andreasen, 1987; Jamison, 1989; Karksson, 1970; Ludwig, 1992; Post, 1994), however, many suffer from methodological weaknesses (Hurlow & MacCabe, 2011; Rothenberg, 2001). A study of visual art students found them at significantly higher risk of schizophrenia and BPD than healthy controls (MacCabe et al., 2018). An early study of geniuses found no association with mental illness in general but in those that were affected scientists were associated with BPD and artists with schizophrenia (Juda, 1949). Later studies of artists found BPD more highly associated (Johnson et al., 2012; Kyaga et al. 2011, 2013; Simeonova et al., 2005).
Dysregulation of dopaminergic pathways is characteristic of schizophrenia and to a lesser extent BPD (Stahl, 2018; Ashok et al., 2017). It is associated with novelty, risk seeking, being open to new experience, decreased inhibition, wider associations of thought, feelings and memories and with creativity (Acar et al., 2018; Boot et al., 2017; Carson et al., 2003; Ettinger et al., 2006; Kumari & Ettinger, 2010; Passamonti et al., 2015; Schluer et al., 2019; Zabelina et al., 2016). If moderated by protective cognitive strengths including high IQ, cognitive flexibility and increased working memory capacity, disinhibition appears to underpin creativity as opposed to pathology (Carson, 2011; Carson et al., 2003). A tendency toward psychopathology, ‘psychoticism’ combined with such ‘ego strengths’ has long been noticed in studies of creativity (Eysenek, 1995; Götz & Götz, 1979a, 1979b; Mackinnon, 1962).
There is evidence for an inverted U-shaped relationship between levels of dopamine and symptoms of schizotypy with pre-clinical patients demonstrating higher levels of creativity than healthy controls (Acar & Sen 2013; Boot et al., 2017; Carson, 2011). Schizotypal, as opposed to schizophrenic, traits are conducive to creativity despite similarly altered dopaminergic conditions (Eysenek, 1995; Holt, 2015; Nelson & Rawlings, 2010). There appears to be similar relationship in creative BPD patients where milder symptoms, elevated mood, impulsivity, openness to experience, higher levels of cognitive flexibility and positive schizotypy, are conducive and more severe symptoms discouraging, to creativity and there is a similar relationship in creative alcohol abusers (Akiskal & Akiskal 2007; Greenwood et al., 2022; Nelson & Rawkings, 2010; Richards et al. 1988). In visual artists creativity is associated with positive (delusion, hallucination), as opposed to negative (anhedonia, social isolation), symptomology (Burch et al., 2006; Nelson & Rawlings, 2010).
Bipolar Disorder
Manic depression, now BPD, was distinguished from ‘dementia praecox’, now schizophrenia, 15 years before Munch was admitted to the Copenhagen clinic (Kraepelin, 1893). This was well known to the clinic’s director and to other physicians Munch consulted but he was not diagnosed with either condition. His diagnosis on admission of dementia paralytica, usually associated with late stage syphilis, caused by alcohol poisoning was to a degree correct but no underlying cause of Munch’s alcohol dependence nor other source of his psychological distress was identified (Prideaux).
BPD, like schizophrenia, has a prevalence of approximately 1%, and shares a hereditability rate of 60-80% with onset principally in early adulthood and middle age (Cardno & Owen, 2014; Escamilla & Zavala, 2008). Fewer environmental risk factors have been identified than for schizophrenia but appear to include toxoplasmosis infection, childhood abuse and trauma, including parental loss, and alcohol dependence before age 25 (Robinson & Bergen, 2021).
The evidence for obstetric complications is weak (Scott et al. 2006).
BPD I diagnosis requires a manic episode not attributable to substance abuse preceded or followed by hypomanic or major depressive episodes. A manic episode is characterised by abnormally and persistently elevated mood, increased and persistent goal-directed activity, accompanied by at least three of: inflated self-esteem or grandiosity, decreased need for sleep, pressured speech, racing thoughts, distraction by irrelevant stimuli and high risk activities. The mood disturbance must cause impairment in social or occupational functioning, hospitalization, or psychotic features. BPD II requires a hypomanic episode and a major depressive episode but without functional impairment, hospitalization or psychotic features (APA 2022, hereafter ‘DSM 5’). Cyclothymic disorder is characterised by recurrent high and low mood states that do not meet the criteria for manic or depressive episodes (Johnson et al., 2012). Frequent BPD comorbidities include alcohol abuse, anxiety and conduct disorders (Koul, & Shetty, 2022; McElroy, 2004). Prior to entering the Copenhagen clinic Munch expressed most BPD I symptoms and several comorbid conditions.
Schizophrenia
Munch’s background and behaviour present multiple risk factors and symptoms of schizophrenia. It typically manifests in adolescence and early adulthood along a spectrum of severity from near normal to catatonic behaviour usually including psychotic symptoms. Twin studies in Scandinavian countries including Norway found heritability rates of over 50% (Cardno & Owen, 2014; Cardno et al,.1999; Cannon et al., 1998; Onstad et al., 1991; Lichtenstein et al., 2009). Meta-analysis confirms both high hereditability and the significance of environmental factors which are additive to the risk of psychosis (Clair & Lang 2012; Pries et al., 2018; Sullivan et al., 2003).
Developmental risk factors include maternal malnutrition, respiratory infection in the second trimester and mid-gestational insult (Brown et al., 2000; Insel, 2010; Radua et al., 2018; Robinson & Bergen 2021). A wide variety of maternal infections are now associated with psychosis (Lee et al., 2020; Weber-Stadlbauer, 2017). In utero exposure to influenza in the first trimester increases risk by 7 times and in the third trimester by 3 times (Brown & Derkits, 2010; Brown 2011; Cheslack-Postava, & Brown, 2022; Choudhury & Lennox, 2021). Older fathers increases risk as does birth in winter and early spring when infectious diseases are most prevalent (Davies, 2003; Miller et al., 2011; Watson et al., 1984). Urbanicity, related to air pollution, maternal smoking and secondary smoke also increase risk (Antonsen et al., 2020; Gatzke-Kopp & Beauchaine, 2007; Hunter et al. 2020; Margolis et al., 2023).
Schizophrenia is strongly associated with childhood trauma, particularly emotional abuse and neglect (Barrigón, 2015; Loewy et al. 2019; Vila-Badia et al., 2021). Over 80% of psychosis patient have experienced childhood abuse which increases psychosis risk 2.5 to 5 times based on the number of occurrences. Childhood trauma is characterised by increased striatal dopamine release and associated with positive symptoms (Brisch et al. 2014; Cancel et al. 2019). Emotional neglect and negative symptom severity are associated with less improvement over time (Stanton et al., 2020). Loss of the mother in childhood increases the odds of psychosis by a factor of 2 (Misra et al., 2019). Loss of two first-degree relatives in childhood compounds the risk (Liang et al., 2016). Loss of a sibling is comparable to the loss of a father (Clark et al., 2012).
Insecure attachment styles arising from infantile abuse or neglect, particularly anxious attachment, are correlated, with disease severity, paranoia and psychotic symptoms (Korver-Nieberg et al., 2014; Lavin, 2020; Read & Bentnall, 2012). Childhood onset is associated with disease severity and significantly higher incidence of hallucinations across the modal spectrum including the least common: tactile/somatic and olfactory (David et al., 2011). Olfactory hallucinations, which Munch experienced (Stenersen) characterise schizophrenia and to a lesser extent schizoaffective patients but not BPD or depressed patients with psychosis (Goghari & Harrow, 2016).
DSM now relies on eight specifiers: hallucinations, delusions, disorganised speech, abnormal psychomotor behaviour, negative symptoms, cognitive impairment, persistent depression and mania associated with functional impairment (DSM 5; Tandon, 2013; Valle, 2020). Cognitive, particularly attention and working memory deficits, sensory disturbance, social dysfunction and isolation are found in most patients (Bowie & Harvey, 2006; Correll & Schooler 2020; Javitt, 2009; Lysaker et al., 2021 ). Munch manifested all but one of these: abnormal psychomotor behaviour. Comorbidity is found in approximately half of cases and of these both anxiety and substance abuse, approach 50% and depression 25% (Buckley et al., 2009); Munch expressed all three.
Positive Symptoms
Disturbances in the dynamics of perception, such as hallucination and delusion, are key elements of psychosis (Sterzer et al. 2018, Adams et al., 2013) experienced by 80% of schizophrenia spectrum patients. Hallucinations are the experience of real perception where no external stimulus is present (Lim et al., 2016; Waters et al., 2014). Delusions, fixed beliefs based on inadequate grounds, not amenable to a rational argument or evidence to the contrary, including persecutory delusions are experienced by 70-80% of patients (Andreasen & Flaum, 1991). Both are often comorbid with anxiety disorders and function as foci of anxiety (Tibbo et al., 2003). They may be efforts to resolve perceptual incoherence and sensory misperception and to reduce anxiety (Postmes et al., 2014; Turetsky, 2007). Patients also demonstrate somatosensory dysfunction: tactile, visceral and olfactory (Kathirvel & Mortimer, 2013; Moberg et al.,1999).
Visual hallucinations, indicative of disease severity are present in 25% of cases (Waters et al. 2014). A large-scale Dutch study found a lifetime prevalence in non-affective psychosis of 37.0%; in schizophrenia of 36.5%. and perhaps surprisingly, of 47.5% in schizoaffective disorder, compared with healthy controls of 3.4% (Van Ommen et al., 2016). They are associated both with multimodal hallucinations, which may be experienced by over half of patients, and with delusions including paranoia and jealousy (Chouinard, 2019; McCarthy-Jones, 2017; Lim et al., 2016 ).
Hallucinations are far more common in childhood onset which is characterised by high rates of tactile, olfactory and multimodal hallucinations, which are more convincing and disturbing than unimodal hallucinations (Chouinard, 2019; David et al., 2011; Dudley et al., 2018). Religious hallucination is common (Cook, 2015). Interpersonal childhood trauma, emotional abuse and neglect, significantly increases the risk of visual hallucination in first episode patients, is predictive of disease severity and is closely related to retinal dysfunction and morphological abnormalities (Bernardin et al., 2017; Silverstein & Lai 2021; Solesvik et al., 2017).
In delusion formation the intensity of perception is altered and inappropriately high levels of salience are attributed to sensory information which might otherwise be disregarded (Jaspers 1913; Kapur, 2003). In paranoia visual information, including facial emotion and gestures, indicators of intention, are negatively biased, as is overheard speech. Threatening inferences are drawn leading to false beliefs and inappropriate behaviour (Bucci et al. 2008; Mitrovic et al., 2020; Pawełczyk et al., 2018; Trotta et al., 2021). Changes in glutamate regulation in the course of illness, from hyper- to hypo- dysregulation, parallel the longitudinal transition from early-stage prevalence of hallucination to chronic stage prevalence of delusion (Sterzer et al. 2018; Powers et al. 2016).
Sleep disorder affects 70- 80% of patients, is predictive of psychosis and is associated with disease severity (Laskemoen et al., 2019; Reeve et al., 2018). Somatisation, the persistence of physical symptoms including limb numbness, gastrointestinal and cardiovascular distress, where there is no apparent physiological cause, is found in two-thirds of patients (Ritsner et al., 2003; Sood et al., 2023; Varsamis & Adamson, 1976). Transient symptoms indicate conversion disorder, the expression of sensory or motor dysfunction in the absence of neurologic or other medical condition, which is associated with schizophrenia (Sharma et al., 2007; Peeling et al., 2023; Ting et al., 2010).
Sexually reckless and aggressive behaviour are characteristic of people, particularly males, on the schizophrenia spectrum Grassi et al., 1999; Hodgins, 2017; Hoptman, 2015; Nettle et al., 2006; Ouzir, 2013; Whiting et al., 2022). Comorbidity with substance abuse is the most salient indicator of aggressive behaviour (Cho et al., 2019). There is also a strong relationship between schizophrenia, substance abuse and gambling (Fortgang et al. 2018).
Negative Symptoms
60-80% of patients present negative symptoms, typically at an early stage. Social withdrawal, particularly in children, characteristically precedes onset of psychotic symptoms (Cullen et al., 2011; Kretschmer,1970; Velthorst et al., 2017). In contrast to positive symptoms, they show no tendency toward spontaneous improvement (Li et al., 2020; Mosolov & Yaltonskaya, 2022). The risk of schizophrenia patients developing depressive symptoms is over 60% (Gozdzik-Zelazny et al., 2011; Samsom & Wong, 2015). It is difficult to distinguish them from depression which is experienced by 80% of first episode patients (Krynicki et al., 2018; Richter et al., 2019; Upthegrove et al., 2010).
Recognition of Self and Others
Schizophrenia is characterized and is distinguished from other disorders, including BPD, by a disturbance in the sense of self and an altered relationship with reality (Kean, 2009; Moe & Docherty, 2014; Parnas & Henriksen, 2014). Patients have difficulty recognising themselves and report feelings of strangeness when looking in the mirror (Abely, 1930; Bortolon et al., 2017; Caputo et al., 2012). Experiments confirm patients’ difficulty in recognizing oneself visually, bodily and audibly (Keromnes et al., 2019; Kozáková et al. 2020; Pan & Zhou, 2020; Rossetti et al., 2022; Sandsten et al, 2020; Waters, 2012). This may be related to temporal abnormalities in multisensory integration, essential to a sense of ‘self’. The attentional and the informational roles of the senses are disturbed thus patients see, hear, feel and smell the world differently (Gröhn et al., 2021; Javitt & Freedman, 2015; Parnas & Hendriksen 2014; Sandsten, 2020).
There is a deficit in facial emotion recognition of both self and others in patients with impairment related to symptom severity (Ruocco et al., 2014; Yun et al., 2014). Such deficits are characteristic enough as to constitute an intermediate phenotype (Fusar-poli et al., 2022). They present across a wide range of facial expression including sadness, fear, surprise, disgust, anger and happiness (Kohler et al., 2010; Liang et al., 2019; Muros et al., 2021; Rubin et al., 2022). Patients are particularly unable to recognize happy faces (Turetsky et al., 2007), are prone to interpret any facial emotion as sad or fearful (Mikhailova et al., 1996; Tsoi et al., 2008) and to attribute sadness to neutral faces (Kohler et al., 2003). Munch never painted a smile or a happy face characteristically painting faces, including his own, as sad or expressionless.
These deficits are consistent with findings of deficits in social cognition and metacognition which include an inability to grasp relationships as an intersubjective whole, a gestalt, characteristic of magnocellular dysfunction which causes a loss of the ‘frame’ of things (Lysaker et al., 2021; McGilchrist, 2009, 2021; Miller & Hou, 2004; Muros, 2021; Turetsky 2007). The mirror neuron system, which ‘maps’ others’ actions, feelings and intentions onto areas processing the self is abnormal in schizophrenia and associated with deficiencies in social cognition (Bonini et al., 2020; van der Weiden et al., 2015). Dysregulation of dopamine and cholinergic networks contributes to errors in matching sensory information with predictions as to others intentions (Diaconescu et al., 2019). Synchronisation with others, neurologically and physiologically, is required for cooperation implying that if one person in a pair, such as artist and model, has dysfunctional perception mutual understanding will be impaired (Balconi & Fronda, 2021; Muller et al., 2021; Palumbo et al., 2017).
Anxiety
Munch suffered from all major forms of anxiety: agoraphobia, closely associated with childhood trauma (Balaram & Marwaha, 2023), generalised anxiety, which affects both adolescents and adults, panic disorder, characterised by feelings of physical and psychological distress, fear of dying and separation anxiety, associated with fearful and disorganised attachment styles which have life-long debilitating effects on the ability to form intimate relationships (APA, 2022b; Bowlby,1960; Stern, 1985). Most of all he suffered from social anxiety, persistent fear of social situations threatening embarrassment or humiliation,(Aderka et al., 2012; DSM 5, Schneier et al., 1992) which causes functional impairment in relationships with family and friends and in forming and maintaining romantic relationships. Sufferers are less likely to marry and are more likely to drop out of school (Stein & Stein, 2008).
Social anxiety has relatively early onset, half of cases manifesting from age 13 and 90% by age 23 (Stein, 2006). It is associated with childhood adversity, dysfunctional parenting, including over-controlling and shaming parents, emotional neglect and abuse, childhood trauma as well as insecure attachment styles. This accounts for the lack of trust in others, fear of rejection and abandonment and anxiety about and avoidance of adult attachments (Eng et al., 2001; Elling et al., 2022; Michail & Birchwood, 2014). Sufferers maintain feelings of shame which may be antecedent to the disorder, are preoccupied with their own anxiety, demonstrate a lack of knowledge of emotions in others and themselves, tend to interpret ambiguous or neutral faces as angry or threatening and express hypervigilance, suspiciousness, paranoia and avoidance behaviour (Bögels & Mansell 2004; Gutierrez-Garcia & Calvo, 2017; Gutiérrez et al. 2017, 2018; Hofman 2010; McTeague et al. 2018; O’Toole. 2012; Peschard & Philippot, 2017; Swee et al., 2021; Wermes et al. 2018). There is a correlation with persecutory delusions (Achim et al., 2016). When comorbid with schizophrenia (15% - 36% of cases) patients present greater social avoidance but less severe cognitive disturbance as compared with those without social anxiety. Self-medication with alcohol and poorer social adjustment are common (Achim et al., 2011; Carrigan & Randall 2003; Eng et al., 2001; Pallanti et al., 2004; Roy et al., 2018). .
Substance Abuse
Alcohol dependence and smoking, are frequently comorbid with schizophrenia and BPD, (Castillo-Carniglia et al., 2019; Dickerson et al., 2013; Spoorthy et al., 2019; Kiran & Chaudhury, 2016). Both alcohol and tobacco affect sensory, emotional and cognitive function and are often abused in tandem (Castillo-Carniglia et al., 2019; Drake et al., 1990; Regier 1990; Shantna et al., 2009). There is a plausible bi-directional relationship between them (Jiang et al., 2014) and there are bi-directional relationships between both and psychosis (Degenhardt, 2018; Quigley & MacCabe 2019).
Although both are often used to ‘self-medicate’ symptoms and comorbid anxiety (Leonard et al. 2007; Turner et al., 2018; cf. Manzella et al. 2015) their use can have both exacerbating and moderating effects (Chambers et al. 2001; Krystal et al., 200). Smoking may partially normalise task performance by transiently enhancing attention but may exacerbate psychotic symptoms (Dickerson et al., 2013; Fernandes et al. 2017; Fernandes et al., 2018a; Lawrence et al., 2002; Heffner et al., 2011; Huang et al., 2019; Kelly & McCreadie, 2000) and does not normalize visual deficits (Hong et al., 2011). Alcohol abuse is a trigger of psychosis and a likely cause of depression (Boden & Fergusson, 2011; Stankewicz & Salen 2018).
Smoking and alcohol abuse share heritability rates of 50% thus environmental factors, including parental mental health and substance abuse, childhood stress, emotional abuse and depressed /neglectful parents, contribute significantly to their aetiology (Do & Maes, 2017; Enoch, 2006). Parental abuse of alcohol, particularly by fathers, is a strong indicator of substance abuse in offspring (Thor et al., 2022). Linked to childhood trauma, abuse often begins in adolescence peaking between ages 18 and 23 (De Bellis, 2002). Despite manifold effects much of the damage caused by alcohol is repaired and dysfunction reduced within 4-7 years of abstinence. Longer-term abstinence allows recovery from most cognitive deficits except deficits in visual processing including spatial processing and contrast gain control (Fein et al., 2006; Oscar-Berman & Marinkovic, 2007).
Schizoaffective Disorder
Given Munch’s symptoms a possible diagnosis is schizoaffective disorder. Those who experience psychosis and persistent mood disorder not caused by substance abuse, are now characterized as schizoaffective (DSM 5, 295.70). Symptoms are less severe and frequency of hallucination is less (Goghari & Harrow, 2016). Compared with schizophrenia little is known of the disorder’s aetiology; loss and replacement of the mother and not completing higher education appear associated (Vardaxi et al., 2018; Chouinard et al., 2019).
Patients with milder positive symptoms and occasional depressive moods, but without persistent depression, demonstrate greater creativity as compared with healthy controls; those with severe symptoms demonstrate lower creativity (Acar et al., 2018; Verhaeghen et al., 2005). Low mood due to social rejection is associated with greater creativity however anxiety, including social anxiety, is not (Alkinola & Mendes, 2008; Byron & Khazanchi, 2011; Silvia & Kimbrel, 2010). Schizoaffective patients demonstrate a tendency to interpret neutral faces as sad and have greater difficulty in recognizing facial emotions, including anger, happiness, sadness and fear, than BPD patients but less than patients with schizophrenia (Ruocco et al., 2014).
Schizophrenia and Vision
Visual deficiencies in patients are associated with functional and anatomical anomalies throughout the visual system including the occipital, temporal, parietal and prefrontal areas (Butler et al., 2008, 2005; Dima et al., 2010; Gagné et al., 2015; Silverstein & Keane, 2011). Functionally, reduced visual acuity is widely observed; in one study approaching 70%; 60% of cases demonstrate visual disturbance of some kind. (Shoham et al., 2021; Silverstein & Rosen, 2015; Smith et al., 1997; Viertiö et al., 2007). Visual perception of even simple objects is deficient as are perceptual organization and surround suppression (Butler & Javitt 2005; Chen et al. 2006; O’Donnell et al., 2006, 1996; Silverstein & Keane, 2011). Patients suffer deficits in detecting and discriminating between, coherent and biological motion with 50-80% demonstrating deviant eye-tracking control (Chen et al. 1999, 2005, 2007; Holzman et al., 1974; Kim et al., 2013; Stuve et al., 1997). Deficits also include misperception of the size, distance, colour, brightness, contrast and contour of objects, in processing spatial frequency, integration, binocular vision, depth perception and re-visualisation which are related to hallucination and delusion (Chen et al., 2008; Keri et al., 2002; Schechter et al. 2006; Silverstein et al., 2000; 2015; 2021; Slaghuis 1998; Wang et al., 2018).
Abnormality in retinal morphology and function are observed in children, adolescents, and young adults at high-risk (Hebert et al., 2010; Koethe et al., 2009; Mittal et al., 2015; Revheim et al., 2014; Schubert et al., 2005; Silverstein, 2016) and are so pervasive they may be endophenotypes of the disease (Adámek et al., 2022; Adams & Nasrallah, 2018; Gagne et al., 2015; Samani et al. 2018). This helps explain why schizophrenia does not develop in the congenitally blind and provides indirect support for the role of disturbed vision in the aetiology and experience of the disease including hallucination (Adámek et al., 2022; Landgraf & Osterheider, 2013). Optical coherence tomography (OCT) studies reveal reduced macular thickness and volume, thinning of both inner (bipolar, horizontal and amacrine cells) and outer (photoreceptor) layers and reduced thickness in the retinal nerve fibre layer (RNFL). Reductions in ganglion cell layer (GCL) and inner plexiform layer (IPL) thickness, enlarged optic cup volume, increased cup-to-disc ratios and related tissue loss are also characteristic (Celik et al., 2016; Jerotic et al., 2020; Kazakos & Karageorgiou 2020; Komatsu et al., 2022; Lizano et al., 2019. 2020; Maziade & Silverstein, 2020; Pan et al., 2018; Schoenfeld-Lecuona et al., 2016)).
Inflammation and swelling of photoreceptors and microvascular abnormalities are evident (Appaji, 2020; Jurišić, et al., 2020; Silverstein et al. 2021) as are distinctive iris pigment dots and crypts related to altered colour vision and cognition (Duan et al., 2022). These abnormalities and rod dysfunction appear to cause patients to experience colours as more vivid and are related to hallucinatory experience (Bernardin et al., 2020; Silverstein & Lai, 2021). Altered rod and cone electroretinogram (ERG) responses distinguish schizophrenia from other psychosis and from depression (Demmin et al., 2018, 2020; Hébert et al., 2020; Viertiö et al., 2007).
Both hypo and hyper dopaminergic conditions can prevail in differing systems and at different points in disease progression (Brisch et al., 2014; Vitay & Hamker, 2007). Reduced dopamine levels in the retina lead to excessively strong coupling of horizontal and amacrine cells and to cone-amacrine cell dysfunction (Bernardin et al., 2022; Dumitrescu et al., 2009; Kolb, 2005b). This causes reduced contrast sensitivity, poorer colour vision and loss of visual acuity (Bodis-Wollner, 1990; Djamgoz et al., 1997; Haug et al., 1995; Howes et al., 2017, Jackson et al., 2012; Price et al., 1992; Zemon et al., 2021). Lower contrast sensitivity at low spatial frequencies and with moving stimuli causes difficulty in discerning differing adjacent elements and the blurring of borders (Harper et al., 2020; Schallmo et al., 2015).
A second effect is to reduce interactions between neurons and rods, signalling light and dark, leading to reduced surround suppression related to hallucination (Hedden & Dowling, 1978; Maziade & Silverstein, 2020). Decreased contrast sensitivity and reduced contrast gain control are common (Butler et al., 2005; Kent et al. 2011; O’Donnell et al., 2006; Skottun & Skoyles, 2007; Slaghuis, 1998). Deficits appear in first episode patients and like contrast sensitivity, deteriorate as the disease progresses. (Feigenson et al. 2014; Silverstein & Keane, 2011; Uhlhaas & Silverstein, 2005). Both reduced contrast gain and weaker surround suppression are suggestive of reduced inhibition in the visual cortex (Tibber et al., 2013; Yoon et al., 2010). Spatial frequency processing, dependent on dopamine receptor function in the retina, is also dysregulated (Chen et al., 2003; Hwang et al., 2013; Tagliati et al.,1994).
Retinal hyperdopaminergic conditions cause malfunction in the magnocellular pathway resulting in low spatial frequency perceptual distortions. High risk and prodromal patients appear to have elevated magnocellular pathway response consistent with reports of “abnormal intensity of environmental stimuli, feelings of being flooded and inundated, and inability to focus attention to relevant details” (Keri et al., 2007, p. 183). Excess retinal dopamine leads to increased brightness and hyper-intense colour perception in first episode patients together with visual distortion (Bunney et al., 1999; Chapman, 1966; Klosterkotter et al., 2001). Excess dopamine in the limbic system is associated with positive symptoms including hallucination and may be related to structural changes in the retina (Brandies & Yehuda, 2008; Schönfeldt-Lecuona et al., 2020).
GABA receptors are found throughout the visual system (Mize et al. 1992). Increased levels of dopamine and reduced GABA levels in the visual cortex, provide a plausible account of reduced surround suppression and are indicative of over-active magnocellular pathways (Kelemen et al., 2013; Yoon et al., 2020, 2010). Hypofunction of NMDA glutamate receptors due to GABA depletion helps explain both reduced contrast perception and reduced lateral inhibition (Merritt et al. 2016; Nakazawa & Sapkota, 2020; Serrano-Pedraza et al., 2014). Resulting hyperactivity in cortical PV-positive fast spiking GABA interneurons, together with increased levels of dopamine are related to psychosis and cognitive deficits including deficits in face recognition (Heckers & Konradi, 2015; Holt et al., 2005, 2006; Lisman et al., 2008; Nakazawa et al. 2012; Swanton, T. 2020). Both environmental and genetic etiologic risk factors of schizophrenia appear to interact with these interneurons which are particularly vulnerable to exotoxicity and oxidative stress arising from maternal infection and obstetric insults (Jiang et al., 2013; Turkheimer et al., 2015, 2020).
Both the magnocellular-dorsal and parvocellular-ventral pathways express connectivity abnormalities although there appears to be a preferential dysfunction in the former (Deng et al., 2019). Consistent with magnocellular and middle temporal dysfunction patients demonstrate deficits in detection of movement and related surround suppression and deficits in facial emotion recognition (Butler et al., 2009; Chen et al., 2003; Creupelandt et al., 2019; Foisy et al., 2007; Foxe et al., 2001; Maurage et al., 2007, 2008; Petra et al., 2009; Schallmo et al., 2015; Tadin et al., 2006). These dysfunctions generate a low signal to noise ratio which propagates to and may be amplified by, cortical dysfunction and are associated with cognitive deficits, social impairment and psychosis (Adámek et al., 2022; Foxe et al., 2001; Núñez et al., 2013).
Alterations in retinal morphology and visual processing appear correlated with cortical abnormalities and clinical symptoms (Bernardin et al. 2021; Silverstein & Thompson 2015) Thinner retinal epithelium layer correlates with mania, reduced GCL and IPL volume are negatively correlated with disease severity, there are non-linear associations between RNFL thickness and acute and chronic patients and with negative and positive symptoms (Alizadeh et al., 2021 Bannai et al., 2020; Celik et al., 2016; Kalenderoglu et al., 2016; Schönfeldt-Lecuona et al., 2020). Delusions correlate with deficits in contour integration, conceptual disorganization and perceptual instability (Javitt, 2015). These correlations are consistent with changes in how the world is experienced by patients. A world literally seen as strange can be experienced as unsafe, threatening, underpinning anxiety, paranoia, hallucination and resulting responses (Grillo, 2018). Persecutory delusions, for example, are associated with increased risk of violence and social isolation (Coid et al., 2013; Fett et al., 2002).
Looking out, deficiencies in vision affect how the world appears, looking in, they seem to reveal the neurological substrate for an altered reality. McGilchrist (2021) emphasises the importance of hemispheric disconnection which isolates the dominant left hemisphere from the aspects of perception and understanding in which the right hemisphere excels. The latter is attuned to perception of context, depth, natural settings, emotional recognition and understanding. In schizophrenia perception, dominated by the left hemisphere, is substantially disabled in recognizing facial emotion, spatial depth and surrounding context. All this suggests that visual artists suffering from schizophrenic spectrum disorders will have significantly altered perception and experience of the world which will be reflected in their painting style.
In summary, someone on the schizophrenic spectrum with comorbid anxiety, alcohol and tobacco abuse is highly likely to be deficient in perceiving contrast, colour, depth, context, peripheral objects and motion, to have difficulty in recognising emotional expression both in their own and others’ faces and a negative bias when doing so. These visual impairments do not improve over time and are likely cumulative in their effects. They are indicative of and contributory to, an altered experience of reality. That reality would be more vivid in colour where attention is focused and blurred at the periphery, lacking in surrounding context and detail. Things would not be noticed or seem disorganised, people’s feelings would be unrecognised, confusing or threatening. Such perception would be a source of inappropriate behaviour and anxiety and efforts to understand and contain it and oneself would likely include hallucination, delusion, avoidance behaviour and social isolation. In contrast, BPD is characterised by sharper, more accurate, sensory experiences including more accurate vision and hearing together with heightened states of empathy and awareness of others’ states of mind (Parker, 2014; Parker et al. 2017).
Contrast
While a large majority of studies of contrast perception in schizophrenia find an overall reduction in magnocellular function (Cadenhead et al. 2013; Chieffi, 2019) studies of unmedicated patients reveal higher contrast sensitivity and hyperactivity in the pathway consistent with patient reports of vivid anomalous visual experience (Kéri & Benedek, 2007). Hypofunction may therefore be the result of antipsychotic medication (Chen et al., 2003; Kiss et al., 2010). However, medication does not explain reduced function in first degree relatives, prodromal, high risk and remitted patients and in schizotypic subjects (Cutting & Dunne 1986; Harper et al., 2020; Schubert et al., 2005). Dysfunction at low spatial frequencies in the early stages of the disease progresses to dysfunction in higher spatial frequencies as the disease develops (Adámek et al., 2022; Chieffi 2019; Silverstein, 2016). The explanation appears to lie in the progression of the disease, characterized by retinal hyperfunction in the early stage, accompanied by hallucination and hypofunction, accompanied by delusion, as it develops (Tandon et al. 2009).
Among alcohol’s most prevalent and persistent effects is visuo-spatial dysfunction (Lew et al., 2020). Alcohol reduces retinal-image quality and visual performance under scotopic conditions (Castro et al., 2014). Moderate drinking impairs contrast sensitivity at low frequencies (Galdino et al., 2011) and acute alcohol use reduces contrast sensitivity at all frequencies as well as contrast gain affecting visual processing in both the magnocellular and parvocellular pathways (Casares-López et al., 2020; Roquelaure et al., 1995; Zhuang et al., 2012). This persists despite years of abstinence (da Cruz et al., 2016). Nicotine is associated with rod dysfunction (Varghese et al. 2011).
Colour
Colour perception dysfunction appears in patients at all stages particularly in the tritan (blue-yellow) spectrum accompanied by retinal hypodopaminergic conditions (Chapman, 1966; Cutting & Dunne 1989; Fernandes et al. 2019; Huang et al., 2020; Kogata & Iidaka, 2018; Phillipson & Harris, 1985; Shuwairi et al., 2002; Young, 1974; Zhuo et al., 2021). Alcohol reduces the capacity to distinguish colours increasing the recognition threshold across the colour spectrum. Impairment in perception of colour and luminance is found in young, chronic and abstaining alcohol users (Brasil et al., 2015; Castro et al., 2009; Martins et al., 2019). Reduced colour discrimination is also found in smokers consistent with cone dysfunction (Fernandes et al., 2019, 2018a, 2018b, 2017; Gundogan et al. 2006, 2007).
Fractals
Experiments consistently demonstrate a human preference for fractal values in the mid-range of 1.3-1.5 in landscapes, buildings, urban areas, artificial and biological forms as well as in art of all categories (Hagerhall et al. 2004; Heerwagen & Orians 1993; Taylor & Sprott 2008). Natural images with mid-range values are appealing, reduce stress and stimulate calm attention (Hagerhall et. al., 2008; Taylor, 2006; Taylor et al., 2011; Ulrich, 1984). Given its frequency in the natural world at all scales it is unsurprising that humans evolved to prefer it and regard conformity with it as attractive and an element of beauty (Spehar et al., 2003; Taylor et al., 2005, 2006; Viengkham & Spehar, 2018). Artists unconsciously depict faces with fractal values in the mid-range (Redies et al., 2007a, 2007b). Spatial frequencies in art significantly higher are associated with triggering epileptic seizure and migraine in susceptible individuals and aversion in healthy subjects (Fernandez & Wilkins, 2008).
Fractals are key to physical and mental health. Numerous aspects of human physiology such as the bronchia of the lungs and the circulatory system, as well as the brain at multiple levels, demonstrate fractal structure (Di leva, 2016). Health is not characterized by linear, homeostasis and equilibrium but by complex, non-linear, ’chaotic’ fluctuations around points of attraction (Varela et al., 2010; West, 2006). Self-complexity, possessing multiple traits and the ability to move among them, provides flexibility, adaptability and resilience to environmental changes moderating both physiological and psychological stress (Brown & Rafaeli, 2007; Linville, 1987). In contrast, lack of fluctuation, rigidity, is characterized by a lack of adaptability and psychopathology (Bruzzo, 2007, Freud, 1896; Horney, 1942; James, 1890; Jung, 1916; Pincus et al., 2019).
Material
Munch’s extant work consists of 1789 paintings on canvas and wooden panels as well as over 7600 images on paper. He also produced approximately 260 photographs including self-portraits. Of his paintings on canvas and panel eight are known to have been lost, all of which he painted again and an additional 10 lost entirely. None of these were portraits or self-portraits. Of the total corpus of paintings 151 are executed entirely in media other than oil paint and excluded to ensure comparability.
Of the remaining 1638 paintings in oil and oil mixed with other materials 51 are self-portraits; 3% of his total oeuvre. He painted self-portraits throughout his career beginning with his first exhibited painting and the last completed the year before his death (Muller-Westermann, 2005). Included in this category are paintings in which his self-portrait is accompanied by another person; 120 self-portraits on paper are excluded.
Portraits examined here represent 13% of his oil paintings all of which are included except preparatory oil sketches and one for which no image is available. All of the portraits are oil on canvas, wood panel or cardboard and painted from life except four painted posthumously. The portraits include 33 images of family and friends. There are 18 images where two or more people are depicted ‘Group Portraits’ treated as single paintings two of which are included in the ‘Family and Friends’ category.
Excluded are paintings of scenes in which figures may be identified as Munch, family members or friends but which lack faces or are not detailed enough to be regarded as portraits. Images of models are excluded except where included in a self-portrait. Munch often painted two versions of commissioned portraits one of which he kept for himself. In such circumstances both versions are included. The resulting study sample of 268 paintings, amounts to 16% of his total oil painted oeuvre.
There are few difficulties in authenticating Munch’s paintings. He kept most of his work which has remained in public ownership since his death. Paintings in the city of Bergen have been in public ownership since the collector’s death. Paintings held elsewhere are well documented and their provenance is not in question. His entire extant painted oeuvre is presented in a catalogue raissone compiled by Gerd Woll (2008). It is on this work that the present study relies for the paintings’ authentication and chronology.
Methods
All of the images examined are high resolution digital images downloaded wherever possible directly from the institutions which own the original paintings. Where this was not possible the highest resolution images available were obtained from open sources. Most institutions provided images in Tag Image File Format (TIF or TIFF) which preserves image quality regardless of copying. Some images were provided in Portable Network Graphics (PNG) format which is equivalent to TIFF in all relevant respects. The remaining images were obtained in Joint Photographic Experts Group (JPEG) format. The images had varying numbers of pixels which were not standardised as test results were found to be substantially the same after rounding. Images obtained in JPEG and PNG format were converted to TIFF using a publicly available on-line service (xconvert.com) to ensure both consistency and stability of the images during processing. Several images provided by institutions included picture frames or colour reference bars which were removed using Adobe Photoshop (adobe.com/uk). TIFF images were used to measure contrast and fractals and converted to JPEG to measure colour to meet software requirements.
Contrast
To measure changes in levels of contrast an average measure of contrast was derived from each painting. In digital images the luminance of a pixel is derived from its red, green, and blue (RBG) wavelength components as 0.299R + 0.587G + 0.11. The images were analysed as a two-dimensional random process and the mean and autocorrelation function provided a value for the contrast of brightness in the portraits. The autocorrelation function quantifies the average relationship between data points in a time series and their previous data points using the Wiener–Kinchin theorem (Chatfield & Xing, 2019). Matrix transformation of luminance values was conducted using the 2-D Fourier Fast Transform and the average image contrast was characterized by the value at origin (Turkheimer et al., 2020). The calculations were performed using MATLAB (v. R2021a).
Colour
The colour median for each painting was measured in Red Green Black (RBG) and Cyan Magenta Yellow Black (CYMK) models. RGB, known as additive colour mixing, is a method of encoding the three cone receptor wavelengths. In concept, each colour is made up of red, green, and blue light that shines with varying intensities. Hexadecimal coding allows integers ranging from 0 to 255 to be represented with only two digits. The CMYK colour model is a subtractive colour model used in colour printing. It subtracts or masks colours from the white backdrop of the paper as ink decreases reflected light. The RGB and CMYK average values were calculated using MATLAB (v. R2021a).7
Fractals
Two methods of fractal analysis are used in the present study: one ‘2’ and one ‘3’ dimensional. The former was obtained from ImageJ software (http://rsbweb.nih.gov/ij/index.html) which uses “box counting” a widely used sampling and data collection process. The fundamental approach is converting the image to greyscale and placing a sequence of grids of decreasing calibre (boxes) over a picture methodically and recording data for each subsequent calibre (counting) creating grids of progressively larger sizes. FracLac generates the grey D value on the basis of the correlation between the variations in both average intensity and grid calibre due to the change in sampling process. The image type was set to 8-bit grayscale and the threshold adjusted with the “Default” algorithm which was chosen after tests using alternative binarizing functions for threshold segmentation produced outcomes within an error range of 0.03 to 0.05. Box sizes were set as 2,3,4,6,8,12,16,32 and 64 for counting and plotting. The range of D values is between 1 and 2 and the values are plotted with log(S) on the x-axis and log(N(s)) on the y-axis.
Considerable colour information is lost after conversion to greyscale which can affect the accuracy in roughness measurement. In order to reduce potential inaccuracy, a modified differential box counting approach (Nayak & Mishra, 2016) was used to determine fractal dimension values of RGB colour images. Combining the “probabilistic algorithm” method (Ivanovici & Richard, 2011) and the “box merging” method extending box counting, (Nikolaidis et al., 2011) the fractal dimension of RGB colour images was estimated using vectors in 5-dimensions (x, y, r, g, b). A greyscale image in this format generates 256 distinct shades of colour between 0 and 255. Applying this method to the 24-bit format for colour images resulted in individual RGB components calculated based on six possible combinations ranging from Ix,y (1) to Ix,y (6) which are averaged to improve accuracy of the roughness estimate. The range of D values using this method is between 2 and 3 which were plotted on the basis described above.
Results
Contrast
Analysis of Munch’s self-portraits (Figure 1) and portraits (Figure 2) reveals increases in average contrast and then maintenance at higher levels in periods of crisis.8 This is consistent with vivid or ‘florid’ episodes in psychosis. There are also intermittent declines during calmer periods. There was a statistically significant positive correlation of the Average Self-Portrait Contrast with age (Pearson Correlation R= 0.515. R^2 = 0.265, P<0.001) indicating a progressive deterioration of Munch’s condition. However there are notable singularities (point-change > 3 Std) in the years 1888, 1906, 1920, 1924 and 1926 where there are dramatic increases in brightness. All of these occur during periods of crisis and may be understood as peaks in altered perception representing high points in his distress.
Analysis of the self-portraits is confirmed by analysis of the portraits. There is again a statistically significant positive correlation of the average contrast with age (Pearson Correlation R= 0.400. P<0.001) with very similar quantitative values between the two sets and an identical rate of change: 0.003 units of positive change in contrast for every year. This consistency indicates repeatability and robustness of the analytical approach. Interestingly the mean level of contrast is higher in the portraits than in the self-portraits perhaps reflecting heightened anxiety as portraits require the presence of other people most of whom were relative strangers. Munch was almost certainly more at ease when painting self-portraits which also contain more surrounding context than the portraits. This difference in state of mind may also be reflected in the range of contrast for the portraits which is somewhat wider.
Colour
Colour analysis of the self-portraits reveals that Munch’s use of red and blue tended to increase in periods of crisis while his use of yellow generally falls suggesting dysfunction on the tritan axis (Figure 3.). His use of green rose in his first crisis period, in 1893 and then remained above the mean from 1908 to 1920 when it fell below it and then it rose again in 1925 remaining above the mean until his death.
There are statistically positive significant correlations of age with colours extracted with the RGB format from the self-portraits. There was a positive correlation with Red (Pearson R = 0.303, p=0.031), Green, (Pearson R = 0.487 p<0.0010 and Blue (Pearson R = 0.440 P<0.001). These changes likely underly a general increase in colour intensity (Pearson R = 0.413, p<0.001) but perceptual lightness, hue and saturation did not change with age. It is noteworthy that while red increased after 1906, its value was not sustained afterwards and correlation was weaker (did not survive multiple comparisons correction) which may indicate that red perception may be associated only with the acute phase of psychotic episodes. There were no associations of elements of the CMYK palette with age.
There are also similarly statistically positive significant correlations of age with colours extracted with the RGB format in the portraits. There was a positive correlation with Red (Pearson R = 0.378, p<0.001), Green, (Pearson R = 0.407 p<0.001), Blue (Pearson R = 0.379 P<0.001). These changes are likely underly a general increase in colour intensity (Pearson R = 0.440, p<0.001) but again perceptual lightness, hue and saturation did not change with age. Differently from the self-portraits, in the CMYK colour model all elements except K were negatively associated with age. The largest correlation was a negative Pearson R correlation (R=-0.397 p<0.001) for Yellow consistent with the self-portraits and disturbance on the tritan axis.
Figure 3.
Red. Mean: 113.31; SD: 36.04. Range: 34-176. Critical years: Mean: 112.86; SD: 32.90.
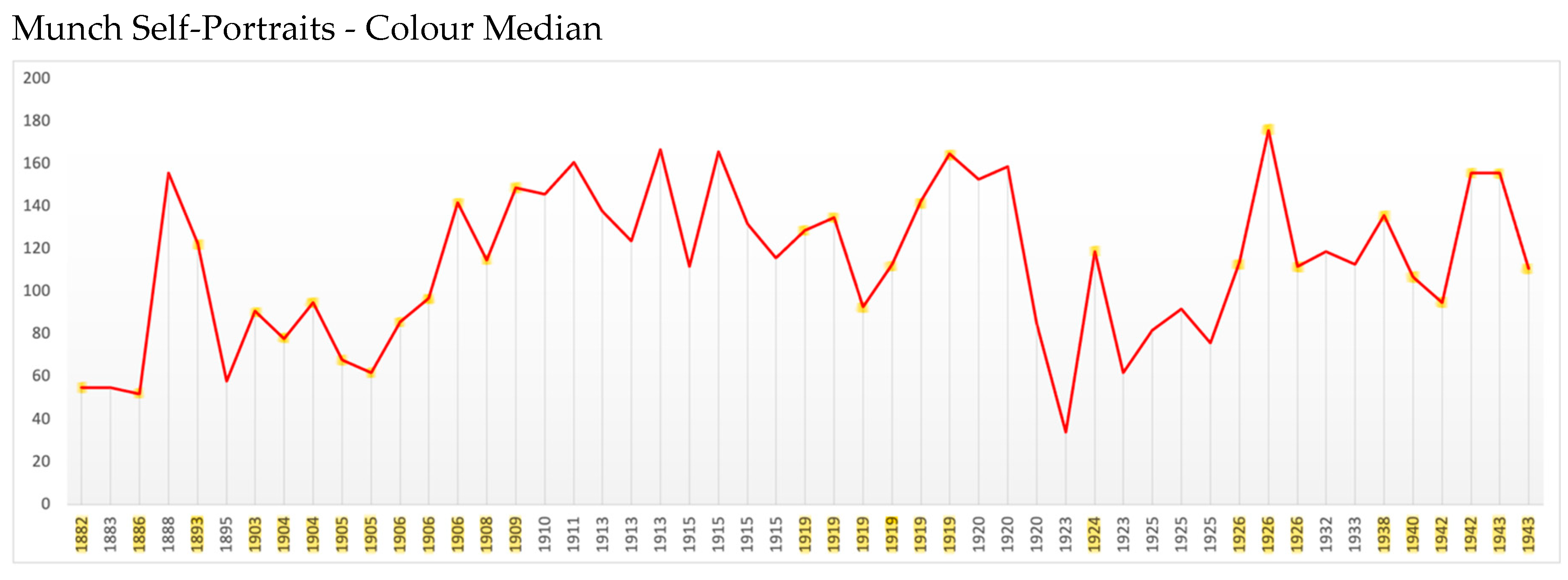
Figure 4.
Green. Mean: 106.45; SD: 31.53. Range: 42-168. Critical years: Mean: 105.00; SD: 30.80.
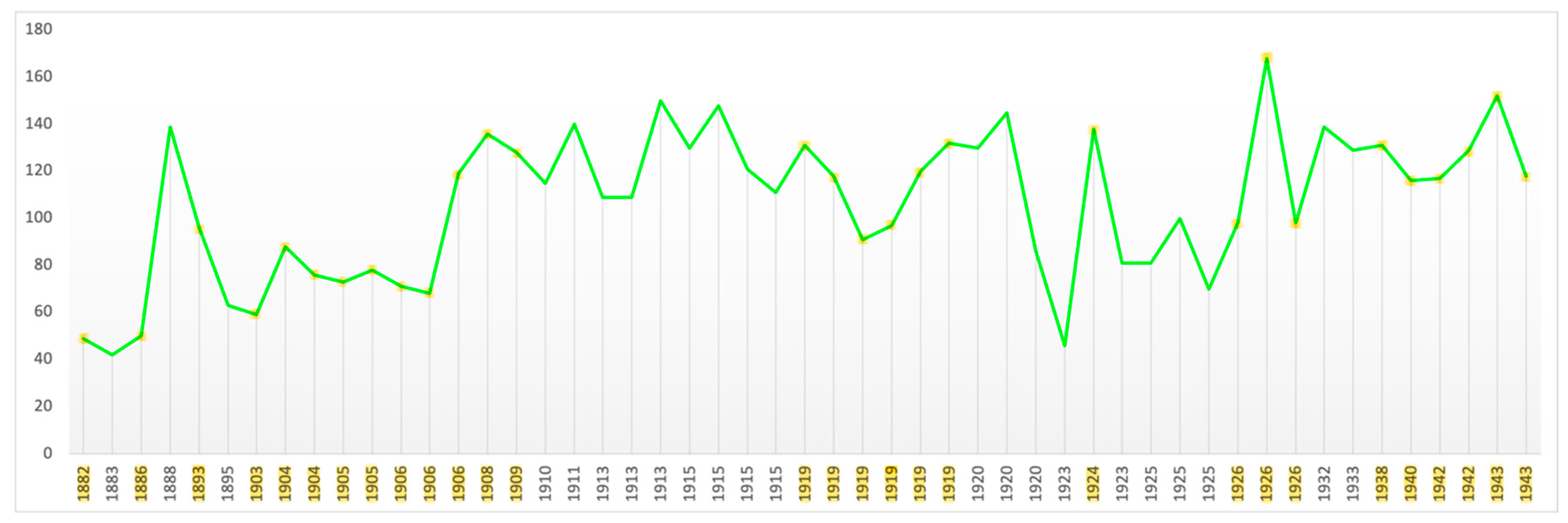
Figure 5.
Blue. Mean: 87.61; SD: 28.75. Range: 30-154. Critical years: Mean: 85.66; SD: 29.15.
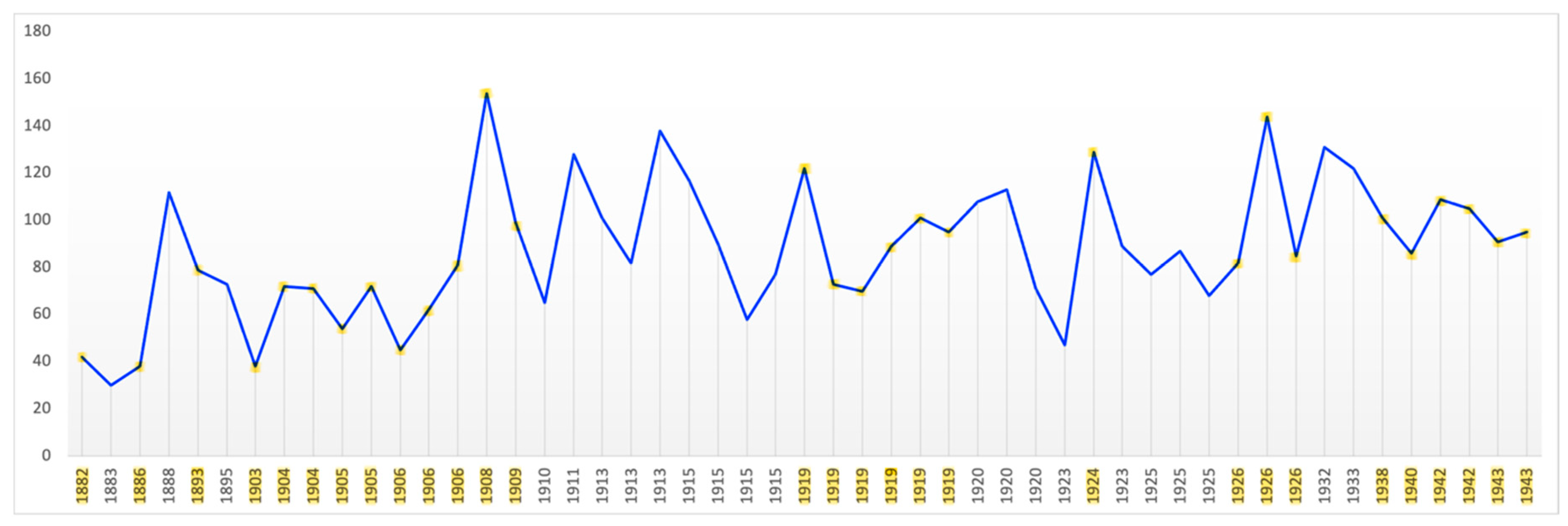
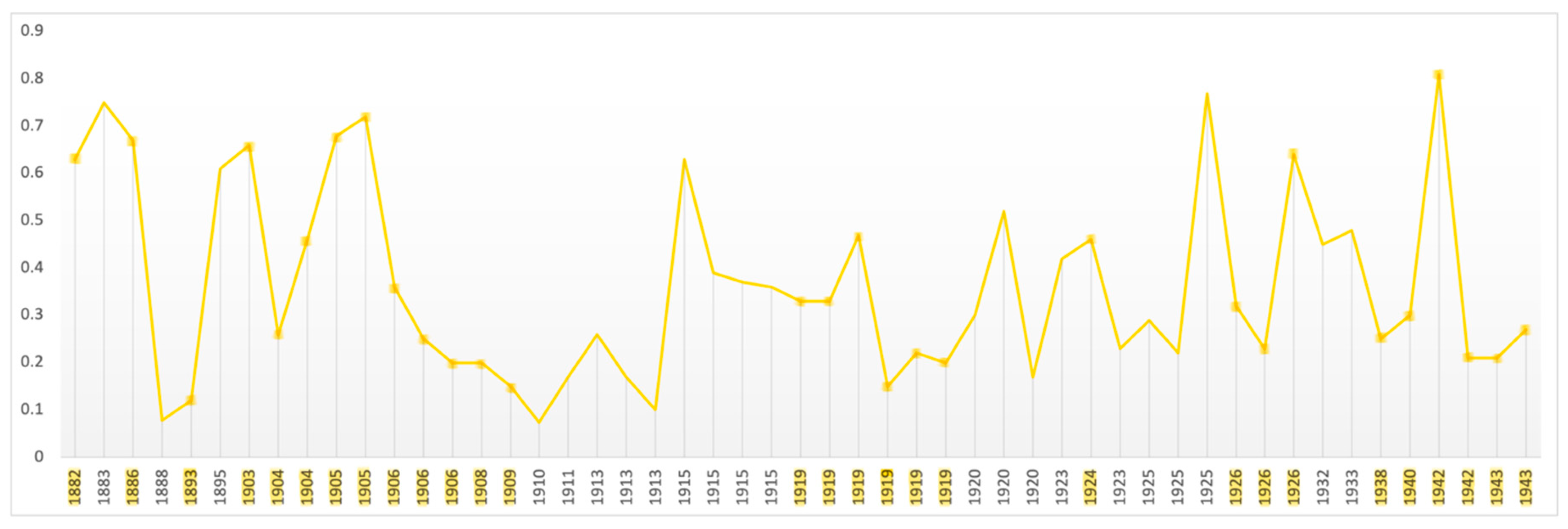
Figure 6.
Yellow. Mean: 0.364; SD: 0.203. Range: 0.073-0.81. Critical years: Mean: 0.371; SD: 0.20.
Fractals
The mean fractal value of Munch’s self-portraits is 1.78 (Figure 7) and that of his portraits 1.80 (Figure 8). These are well above the mid-range associated with attractiveness and beauty and helps explain why his paintings were disturbing to his contemporaries. The fractal values in Munch’s self-portraits are remarkably consistent. Even during his most intense period of crisis (1903-1908) there is little variation nor is there generally when crisis and non-crisis periods are compared (Figure 9).
Munch’s portrait fractal values are remarkably high throughout his career regardless of whether the subject was an individual (1.80) or a group (1.793) although the mean fractal value is noticeably lower (1.738) when he painted family members and friends (Figure 10). This, together with somewhat higher values in the portraits compared with the self-portraits, as is the case in levels of contrast, suggests he experienced greater stress when painting unrelated others consistent with social anxiety. The consistent high level of fractal values, from earliest to latest paintings and despite deliberate alterations in style both before and after treatment indicates a complex, persistent and inflexible state of mind.
Productivity
Munch was productive throughout his career with an annual average of 27 paintings.
over a 60-year career (Figure 11). His productivity rose in periods of distress the most dramatic of which was the period 1896 to 1909 reaching the second highest point in his career in 1907 the year before he entered the Copenhagen clinic; a level only reached once again in 1915. In the 9 months before he entered the clinic, as his symptoms became overwhelming, his productivity plummeted rising again during and after treatment. There were less dramatic but discernible rises in productivity in crisis periods before (1885-1895) and after (1924-1926, 1930) treatment.
The first crisis period lasted 9 years beginning with the Sick Child followed by paintings of Despair, In the Death Room, Melancholy, Anxiety, Ashes, and the Scream. In the second and longest crisis period, beginning in 1896 and peaking in 1907 he painted Self-portrait in Hell, Self-portrait with Wine Bottle, two more versions of the Death Room and of The Sick Child, two paintings of ‘Inheritance’, two versions of The Dead Mother, the Death of Marat and Separation. In 1895, the year-long interlude between the first and second crisis periods and of his brother’s death, he painted Self-portrait with Cigarette, Vampire and Jealousy. In the third period he painted several images recalling his days of heavy drinking and in 1930 painted himself suffering from an embolism as a figure reminiscent of the Scream and as sad and isolated (Eggum, 1984; Heller; Stang; Woll).
His achieved his lifetime peak in productivity in a period of feeling honoured, accepted, and prosperous. In 1916 he received public and private commissions and purchased the countryside home in which he spent the rest of his life. His productivity also noticeably rose in periods of crisis: 1924-1926 when his sister and a friend died and in 1930 when his aunt died.
The apparent exception, a drop in productivity in a period of crisis between 1936-1941 was one of physical rather than emotional disability. He had suffered deteriorating vision in both eyes and was then well into old age, when productivity may be expected to drop (Simonton, 1990). Nevertheless, once his vision recovered his productivity began to rise and he painted several important self-portraits before his death.
Discussion
Munch was, from birth, a sick child; physically and mentally. The indications are that he inherited a genetic predisposition to schizophrenia and suffered maternally transmitted infection. Physiological trauma at birth was compounded by that of separation from his preoccupied mother; both must have been sources of intense anxiety. Munch recorded the memory of his earliest experience in images of infants dying of congenital syphilis in the arms of their mothers. Titled ‘Inheritance’ they are essentially self-portraits, although not included here as such. The additional trauma of witnessing his mother’s illness and death is depicted in paintings of the ‘Dead Mother’ which show a small child in the same pose (hands over ears) as the figure in the Scream, treated here, as Munch regarded it, as a self-portrait. The unbearable horror and sadness of her death is evident.
After his mother’s death he shifted attachment to his older sister who then dies of the same disease that killed his mother. This further traumatic separation was compounded by his guilt that he had been the cause of her death. The experience was seared into his memory and expressed in the Sick Child. The impact of these deaths from tubercular-type illness, which his aunt suffered, as he did, was compounded by witnessing his father and younger sister’s increasing mental disorder. It is thus not hard to see why he wrote:
“I inherited two of humanity’s most dreaded enemies – consumption and mental illness. Sickness, madness and death were the black angels that surrounded my crib. My mother died prematurely – from her I inherited the seeds of consumption. My father was obsessively nervous and obsessively religious – to the point of madness. This had been the fate of his family for generations. From him I inherited the seeds of madness. The angels of fear – sorrow and death – had stood by my side since the day I was born. They followed me when I played -followed me everywhere. Followed me in the spring and the glory of summer. They stood by my side at bedtime when I shut my eyes -they threatened me with death, hell and eternal damnation. Often I awoke in the middle of the night – I gazed around the room in wild fear – was I in Hell?...[my] entire youth was worm eaten… tormented by doubt -fear and illness.” (Tøjner p. 203-4).
The evidence is that Munch was correct in his self-diagnosis. His chronic illness, given its immediate onset upon birth, was very likely congenital tuberculosis. There is a bidirectional relationship between tuberculosis and psychosis (Kuo et al., 2013; Monistrol-Mula et al. 2024). A first degree relative, his sister, suffered from schizophrenia and another, his father, evidenced depression, anxiety in the form of obsessive religiosity, alcohol and nicotine dependence, each of which entails a significant genetic component (Enoch, 2006; Kendall et al. 2021; Meier & Deckert 2019; Purty et al., 2019; Rakesh et al. 2021; True et al. 1999). Given the loss of not one but two primary attachments, his ambivalent relationship with his aunt, his difficulty in establishing relationships with women and association of female intimacy with death, it is reasonable to assume an anxious/avoidant attachment style which, together with trauma, is closely associated with psychosis and schizophrenia in particular (Sheinbaum et al., 2013; Velikonja et al. 2015). His inherited susceptibilities and the multiple developmental and environmental factors which made Munch’s childhood a panorama of physical and mental distress, including anxiety, grief and guilt, made the childhood onset of psychosis almost inevitable.
Munch was also increasingly isolated due to his illness, unable to attend school or complete higher education. He began drinking in adolescence and by early adulthood was abusing both alcohol and tobacco. When Munch abandoned the career chosen by his father in favour of an artistic one, his father condemned it publicly and privately causing Munch intense shame, a predicate for social anxiety (Harris, 2004). His first love affair was one of many occasions on which Munch felt deeply ashamed as was the exhibition of the Sick Child. He was intensely sensitive to criticism all his life avoiding exhibitions of his work and social occasions of all kinds. He often fled from personal, social and professional contacts (Stenersen). His need to avoid people worsened over time and was unaltered by treatment and abstinence. Before treatment his delusions became paranoid and after predominantly persecutorial.
Social anxiety is frequently comorbid with schizophrenia and joint sufferers are characterised by insecure attachment, childhood trauma, increased difficulty in mentalisation, a higher sense of shame, greater negative attribution bias and suicidality (Roy et al., 2012; Achim et al., 2016). They also evidence greater social avoidance but less severe cognitive disturbance compared to those without social anxiety. With the exception of suicidal planning Munch demonstrates all these elements. He had multiple childhood trauma, disorganised and fearful attachments to his mother, sister and aunt, and a father who was over-controlling and shaming all of which are indicative of the social, generalised and phobic anxiety he experienced (Faravelli et al., 2012; Murphy et al., 2022).
Munch experienced depression, also a frequent comorbidity of schizophrenia, but it appears to have been episodic, and related to specific events such as his father’s death rather than cyclical. He also developed a variety of somatic, conversion type, symptoms and became increasingly paranoid, hallucinatory and violent as his drinking increased. These symptoms, often found in schizophrenia, and his depressive episodes, subsided once he became abstinent which suggest they were alcohol related. His intense social anxiety, however, continued made manifest by the extraordinary avoidance measures he employed which also appear related to his persecutorial delusions. His insomnia too persisted into old age. Munch’s life thus parallels the natural history of schizophrenia: childhood pre-morbid and prodromal phases, first psychotic episodes, a florid psychotic phase, followed by stable delusions accompanied by negative symptoms and social deficits (Tandon et al., 2009).
If one focuses on the period between his first love affair and his treatment in Copenhagen Munch may be seen as suffering from BPD I with psychosis which occurs in approximately half of cases and is easily mistaken for schizophrenia (Chakrabarti & Singh, 2022). He would now not be diagnosed with BPD II given his psychotic experiences. His reckless and often aggressive behaviour including visiting prostitutes despite fear of syphilis, gambling, brawling and use of firearms can be understood as manic as can his impulsive travelling and working for days without rest, eating little, seemingly existing on cigarettes and alcohol each co-morbid with BPD as well as schizophrenia (Frye & Salloum, 2006; Heffner et al., 2011; Stang; Yakovenko et al. 2016). The restless working, however, can also be seen as periods of inspiration (Jones et al., 2014) and as efforts to process his distress by expression in art, and the travelling as avoidant behaviour associated with social anxiety. Following treatment he no longer visited prostitutes and while having affairs none of them were characterised by the violence, jealousies or mood swings evident in his pre-treatment relationships.
Munch had periods of depression such as those following the end of his first love affair and his father’s death, but these were not preceded or followed by manic or hypomanic behaviour as would be expected in BPD 1. Prior to his father’s death he had been hospitalised with pneumonia, itself a cause of depression as is alcohol abuse (Boden & Fergusson, 2011; Davydow et al., 2014). The depression following his father’s death resulted in a profound change in style which was to become characteristic of his greatest work. Self-reflective rumination typical of depressive episodes, as opposed to recurrent depression, is associated with the generation of creative ideas (Baird et al., 2012; Verhaeghen et al., 2005). His father’s death can be seen as setting him free artistically (Heller).
His periods of creativity and increased productivity were accompanied by negative feelings of guilt, shame and jealousy not the positive or euphoric feelings associated with mania, creativity and BPD (Johnson et al., 2012). He was also prolific when in more stable moods during his ‘beach period’ in 1907 and following the end of his exile. That his depression subsided once he became abstinent and publicly acknowledged suggests that it was not inherent, as in BPD 1and cyclothymic disorder, but induced by alcohol and a sense of rejection. The presence in later years of olfactory hallucination is inconsistent with BPD (Goghari & Harrow, 2016), BPD patients are not deficient in motion detection (Chen, 2005) and at no stage do his paintings reveal the heightened accuracy of perception and empathy with others characteristic of BPD; quite the contrary.
Although it can begin at any age, BPD typically manifests itself in late adolescence and early adulthood by which time Munch already had a history of hallucination (Bolton et al., 2021). BPD accompanied by hallucination is relatively rare in comparison with schizophrenia and usually abates in the early years after onset (Chakrabarti & Singh, 2022; Goghari et al., 2013). BPD’s natural course does include childhood anxiety and insomnia, but continues, regardless of periods of remission and cyclically or not, to include persistent depression and long-term cognitive decline.
In his 35 year period of abstinence and isolation Munch is not reported by contemporaries as appearing either manic or depressed although they did notice delusions and antisocial behaviour. His journals and correspondence reveal self-absorption, sensitivity to criticism and obsessive concerns but neither the grandiosity of mania nor the futility of depression (Holland, 2005; Prideaux; Tøjner). There is also no evidence of any of the widespread neurocognitive deficits, typical in BPD, in executive functioning, verbal and spatial memory and psychomotor performance, which usually persist in non-symptomatic periods (Bauer & Gitlin, 2016; Tsitsipa & Fountoulakis, 2015). While unable to function well socially, he remained in contact with a wide circle (Cernuschi, 2001; Heller) and fully capable of managing his affairs including planning carefully for his death. There was no medication available so the absence of BPD symptoms during this period makes a diagnosis of BPD less plausible.
If one looks at Munch’s entire life history including the background of risk factors, childhood onset of insomnia and multimodal hallucination in the absence of depression or mania, the cessation of hallucination, manic behaviour and depression following abstinence from alcohol, and the transition to persistent delusions and stable mood and functioning thereafter, he appears to follow the natural course of schizophrenia as opposed to schizoaffective or bipolar disorder (Goghari & Harrow, 2016). The transition is also consistent with the long-term change in style after treatment noted by art historians. It therefore seems reasonable to conclude that his underlying disease was schizophrenia, initially exacerbated by alcohol, combined with comorbid intense social anxiety (DSM 5, Malaspina et al., 2013; Mancuso, 2015). While it is difficult to diagnose retrospectively and the overlap between BPD and schizophrenia, genetically and phenomenologically is considerable (Cardno & Owen 2014; Laursen et al., 2009) the present results support this conclusion
As discussed above, schizophrenia is characterised by visual impairment particularly deficits in contrast sensitivity, motion detection, surround suppression, perceptual organization, contour perception and facial emotion recognition (Butler et al., 2008; Dakin et al., 2005’ Silverstein & Keane, 2011; Silverstein & Rosen, 2015; Turetsky et al., 2007). Colour vision impairment, increased intensity of, or change in perception, is also evident particularly on the tritan spectrum (Vollmer-Larsen et al., 2007). These deficits are also found in heavy drinkers and smokers compounding them in individuals on the schizophrenia spectrum (Fernandes et al., 2019). The results here suggest that Munch had deficits in all these domains.
First, contrast in his paintings increased significantly during critical periods particularly in the self-portraits. This tracks the most florid of his adult hallucinatory and delusional periods. His productivity increased in the same periods and can be understood as an effort to process and express these intense experiences as he did most famously in The Scream. “When I paint sickness and suffering it is…a healthy release. It is a healthy reaction from which one can learn and carry on living” (Tøjner, p.134). That the magnocellular system was preferentially affected, typical in schizophrenia, is evidenced by the absence of surrounding context, motion, gesture or peripheral objects particularly in the portraits. While several self-portraits have contextual backgrounds, the portraits are stereotypical, rigid poses against featureless backgrounds (Ustvedt 2020, p. 123). Depth and volume are only tangentially indicated by abbreviated intersecting lines suggestive of floor and wall but there are no, or at most one, identifying ornaments or objects Significantly no source of light is evident and there are almost no shadows indicative of a lack of depth perception and a visual system deficient in peripheral vision and in recognising natural environmental cues.
Second, primary colours, red, green and blue, like contrast, increased in proportion in self-portraits painted during periods of distress but yellow declined indicative of altered vision on the tritan spectrum consistent with studies of visual disturbance in schizophrenia. The likelihood is that his retina, magnocellular and parvocellular pathways and visual system generally were altered morphologically and functionally and the evidence is that these deficits increased as his disease progressed.
Third, Munch’s self-portraits and portraits are all essentially expressionless and to the extent there is expression it is sadness. Almost all are face front; more two than three dimensional, characteristic of patient art (Cunningham-Dax, 1998; McGilchrist, 2009). Only rarely are there even slight turns of the head. Even the Sick Child, while poignant and in an identifiable space, is essentially a flat profile. The self-portraits whether painted from photographs or images in the mirror show little insight. With a few exceptions, his sisters and friends, the portraits reveal an inability to read his sitters’ emotions confirming his inability mirror or to synchronise with the feelings of others.
He never paints himself or others in a positive mood consistent with the negative bias in facial emotion recognition revealed in multiple studies of schizophrenia (Fusar-poli et al. 2022). There are no images of happiness or joy, neither among family and friends nor when painting children; perhaps a projection of his own unhappy childhood. His self-portraits depict him at times of illness, insomnia, depressed, eating, drinking, tormented and isolated and yet without expression except sadness.
This is all consistent with Munch’s manner of working which he and others described. He would glance at the subject and then paint his first impression without moving his eyes from the canvas. He didn’t notice or care if subjects moved or left (Stenersen, Tøjner). He was oblivious of the subject’s presence as it was, to him, no longer relevant. His intention was to paint not the subject but his subjective response, “the perception of [his] brain”. He famously remarked, “I do not paint what I see; I paint what I saw.” and what he saw were “the inner images of the mind. The images upon the reverse of the eye” (Tøjner, p. 131). He ignored details that did not remain in his memory of the first impression. Even when painting out of doors he closed himself off from his surroundings and concentrated on the canvas (Prideaux; Stenersen ).
This pattern of only glancing at his subjects and then painting without further reference to them takes on significance when viewed from the perspective of his afflictions. Many who sat for him noticed that he spoke incessantly and did not maintain eye contact to prevent interaction (Holland). He painted not what was before him but his first impression which he immediately and unconsciously imbued with meaning and it was that meaning he sought to convey not a likeness of what he had seen (Tøjner). The subject of Munch’s paintings was not in front of him but inside him and what was inside him was his experience and his disease.
Fractal analysis is consistent with this. The fractal dimension of his paintings is significantly above the level preferred by healthy observers, beyond that even of abstract painters such as Jackson Pollack (de la Calleja et al., 2016; Forsythe et al. 2017). It is not surprising that public and critics initially reacted as they did and it indicates that he perceived the world and himself fundamentally differently from others. Equally important and what distinguishes him from other painters who have been similarly studied, is that the high fractal dimension was maintained throughout his career. It is present in his first, ‘realistic’ self-portrait, in his impressionist phase, in his pre-treatment expressionism, post treatment painting ‘en plein air’, and in his last self-portraits. It hardly varied for six decades with only slightly reduced values when painting those close to him. The somewhat higher fractal level in portraits of unrelated others is consistent with his intense social anxiety. This all suggests an inflexible state of mind and an altered way of seeing the world that started in childhood and was so deeply implanted that neither deliberate changes in style nor experience could alter it.
Conclusions
Munch can be seen, from a psychiatric point of view, as exemplifying schizophrenia and social anxiety disorder. A diagnosis of BPD or schizoaffective disorder are inconsistent with the coincidence of mood disorder and alcohol abuse. His symptoms, following the natural course of schizophrenia, shifted from hallucination to delusion. His anxiety, particularly social anxiety, like his insomnia, never abated. His painted self-portraits and portraits, which he saw, like all his painting, as a means of expressing himself, reflect empirically the transitions in his state of mind: growing brighter, more colourful, and more numerous as his symptoms became more severe while maintaining a high, rigid measure of complexity throughout his life. This suggests that his childhood experience of both physiological and psychological distress caused him to acquire neurological traits including lasting morphological, neurobiological, and functional changes particularly affecting perception of contrast, context, motion, and facial emotion. From this perspective his illnesses and his efforts to manage them can be seen as fundamental to his art.
Limitations
The most important limitation of the present study is that it encompasses only a fraction of Munch’s paintings and none of his works on paper. Analysis of those works might reveal very different results. Second, the material examined are not the original paintings but digital images. This, at the very least, means that analysis of colour is of limited use given the difficulties which computers have of identifying colour in anything like the subtlety of the eye. Fractal and contrast analysis are more reliable but again could vary if applied to other and original works.
Acknowledgments
This work represents independent research partly funded by the NIHR Maudsley Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London.
References
- Abely, P. De signe du mriroir dans les psychoses et plus spécialement dans la demence précoce. Ann Medicopsychol 1930, 28–36. [Google Scholar]
- Acar, S.; Chen, X.; Cayirdag, N. Schizophrenia and creativity: A meta-analytic review. Schizophr. Res. 2018, 195, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Acar, S.; Sen, S. A multilevel meta-analysis of the relationship between creativity and schizotypy. Psychol. Aesthetics, Creativity, Arts 2013, 7, 214–228. [Google Scholar] [CrossRef]
- Achim, A.M.; Maziade, M.; Raymond, E.; Olivier, D.; Merette, C.; Roy, M.-A. How prevalent are anxiety disorders in schizophrenia? A meta-analysis and critical review on a significant association. Schizophr. Bull. 2009, 37, 811–821. [Google Scholar] [CrossRef] [PubMed]
- Achim, A.M.; Sutliff, S.; Samson, C.; Montreuil, T.C.; Lecomte, T. Attribution bias and social anxiety in schizophrenia. Schizophr. Res. Cogn. 2016, 4, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Adámek, P.; Langová, V.; Horáček, J. Early-stage visual perception impairment in schizophrenia, bottom-up and back again. Schizophrenia 2022, 8, 27. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.A.; Stephan, K.E.; Brown, H.R.; Frith, C.D.; Friston, K.J.; Adams, R.A.; Stephan, K.E.; Brown, H.R.; Frith, C.D.; Friston, K.J.; et al. The computational anatomy of psychosis. Front. Psychiatry 2013, 4, 47. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.A.; Nasrallah, H.A. Multiple retinal anomalies in schizophrenia. Schizophr. Res. 2018, 195, 3–12. [Google Scholar] [CrossRef]
- Aderka, I.M.; Hofmann, S.G.; Nickerson, A.; Hermesh, H.; Gilboa-Schechtman, E.; Marom, S. Functional impairment in social anxiety disorder. J. Anxiety Disord. 2012, 26, 393–400. [Google Scholar] [CrossRef]
- Akinola, M.; Mendes, W.B. The dark side of creativity: biological vulnerability and negative emotions lead to greater artistic creativity. Pers. Soc. Psychol. Bull. 2008, 34, 1677–1686. [Google Scholar] [CrossRef]
- Alizadeh, M.; Delborde, Y.; Ahmadpanah, M.; Seifrabiee, M.A.; Jahangard, L.; Bazzazi, N.; Brand, S. Non-linear associations between retinal nerve fibre layer (RNFL) and positive and negative symptoms among men with acute and chronic schizophrenia spectrum disorder. J. Psychiatr. Res. 2021, 141, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Alzueta, E.; Melcón, M.; Jensen, O.; Capilla, A. The 'Narcissus Effect': Top-down alpha-beta band modulation of face-related brain areas during self-face processing. NeuroImage 2020, 213, 116754. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th Edition, Text Revision (DSM-5-TR); American Psychiatric Publishing: Arlington (VA), 2022. [Google Scholar]
- American Psychiatric Association. Anxiety Disorders. In Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Text Revision; American Psychiatric Association, 2022; pp. 215–231. [Google Scholar]
- Andreasen, N.C.; Flaum, M. Schizophrenia: The characteristic symptoms. Schizophr. Bull. 1991, 17, 27–49. [Google Scholar] [CrossRef] [PubMed]
- Higier, R.G.; Jimenez, A.M.; Hultman, C.M.; Borg, J.; Roman, C.; Kizling, I.; Larsson, H.; Cannon, T.D.; Sachsse, U.; VON DER Heyde, S.; et al. Creativity and mental illness: prevalence rates in writers and their first-degree relatives. Am. J. Psychiatry 1987, 144, 1288–1292. [Google Scholar] [CrossRef]
- Antonsen, S.; Mok, P.L.H.; Webb, R.T.; Mortensen, P.B.; McGrath, J.J.; Agerbo, E.; Brandt, J.; Geels, C.; Christensen, J.H.; Pedersen, C.B. Exposure to air pollution during childhood and risk of developing schizophrenia: a national cohort study. Lancet Planet. Heal. 2020, 4, e64–e73. [Google Scholar] [CrossRef] [PubMed]
- Appaji, A.; Nagendra, B.; Chako, D.M.; Padmanabha, A.; Hiremath, C.V.; Jacob, A.; Varambally, S.; Kesavan, M.; Venkatasubramanian, G.; Rao, S.V.; et al. Retinal vascular abnormalities in schizophrenia and bipolar disorder: A window to the brain. Bipolar Disord. 2019, 21, 634–641. [Google Scholar] [CrossRef] [PubMed]
- År Til År, F. Edvard Munch. A Year by Year Record of Edvard Munch’s Life; Aschehoug & Co., 1961. [Google Scholar]
- Ashok, A.H.; Marques, T.R.; Jauhar, S.; Nour, M.M.; Goodwin, G.M.; Young, A.H.; Howes, O.D. The dopamine hypothesis of bipolar affective disorder: the state of the art and implications for treatment. Mol. Psychiatry 2017, 22, 666–679. [Google Scholar] [CrossRef] [PubMed]
- Azeem, H. The art of Edvard Munch: a window onto a mind. BJPsych Adv. 2015, 21, 51–53. [Google Scholar] [CrossRef]
- Baird, B.; Smallwood, J.; Mrazek, M.D.; Kam, J.W.Y.; Franklin, M.S.; Schooler, J.W. Inspired by distraction: Mind wandering facilitates creative incubation. Psychol. Sci. 2012, 23, 1117–1122. [Google Scholar] [CrossRef]
- Balaram, K.; Marwaha, R. Agoraphobia. In StatPearls [Internet]; StatPearls Publishing: Treasure Island (FL), 2023; Available online: https://www.ncbi.nlm.nih.gov/books/NBK554387/.
- Balconi, M.; Fronda, G. Intra-Brain Connectivity vs. Inter-Brain Connectivity in Gestures Reproduction: What Relationship? Brain Sci. 2021, 11, 577. [Google Scholar] [CrossRef]
- Bannai, D.; Lizano, P.; Kasetty, M.; Lutz, O.; Zeng, V.; Sarvode, S.; Kim, L.A.; Hill, S.; Tamminga, C.; Clementz, B.; et al. Retinal layer abnormalities and their association with clinical and brain measures in psychotic disorders: A preliminary study. Psychiatry Res. Neuroimaging 2020, 299, 111061–111061. [Google Scholar] [CrossRef] [PubMed]
- Barrigón, M.L.; Diaz, F.J.; Gurpegui, M.; Ferrin, M.; Salcedo, M.D.; Moreno-Granados, J.; Cervilla, J.A.; Ruiz-Veguilla, M. Childhood trauma as a risk factor for psychosis: A sib-pair study. J. Psychiatr. Res. 2015, 70, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Gitlin, M. Natural Course of Bipolar Disorder and Implications for Treatment. In The Essential Guide to Lithium Treatment; Springer: Cham, 2016. [Google Scholar] [CrossRef]
- Bernardin, F.; Schwitzer, T.; Angioi-Duprez, K.; Giersch, A.; Jansen, C.; Schwan, R.; Laprevote, V. Retinal ganglion cells dysfunctions in schizophrenia patients with or without visual hallucinations. Schizophr. Res. 2020, 219, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Bernardin, F.; Schwitzer, T.; Angioi-Duprez, K.; Giersch, A.; Ligier, F.; Bourion-Bedes, S.; Jansen, C.; Schwan, R.; Laprevote, V. Retinal ganglion cell dysfunction is correlated with disturbed visual cognition in schizophrenia patients with visual hallucinations. Psychiatry Res. 2021, 298, 113780. [Google Scholar] [CrossRef] [PubMed]
- Bernardin, F.; Schwitzer, T.; Schwan, R.; Angioi-Duprez, K.; Ligier, F.; Bourion-Bedes, S.; Jansen, C.; Giersch, A.; Laprevote, V. Altered central vision and amacrine cells dysfunction as marker of hypodopaminergic activity in treated patients with schizophrenia. Schizophr. Res. 2022, 239, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Boden, J.M.; Fergusson, D.M. Alcohol and Depression Addiction. 2011, 106, 906–914. [Google Scholar] [PubMed]
- Bodis-Wollner, I. Visual deficits related to dopamine deficiency in experimental animals and Parkinson's disease patients. Trends Neurosci. 1990, 13, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Bögels, S.M.; Mansell, W. Attention processes in the maintenance and treatment of social phobia: hypervigilance, avoidance and self-focused attention. Clin. Psychol. Rev. 2004, 24, 827–856. [Google Scholar] [CrossRef] [PubMed]
- Bonini, L.; Rotunno, C.; Arcuri, E.; Gallese, V. Mirror neurons 30 years later: implications and applications. Trends Cogn. Sci. 2022, 26, 767–781. [Google Scholar] [CrossRef]
- Boot, N.; Baas, M.; van Gaal, S.; Cools, R.; De Dreu, C.K. Creative cognition and dopaminergic modulation of fronto-striatal networks: Integrative review and research agenda. Neurosci. Biobehav. Rev. 2017, 78, 13–23. [Google Scholar] [CrossRef]
- Bortolon, C.; Capdevielle, D.; Altman, R.; Macgregor, A.; Attal, J.; Raffard, S. Mirror self-face perception in individuals with schizophrenia: Feelings of strangeness associated with one's own image. Psychiatry Res. 2017, 253, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Bowen, A.M. Munch and Agoraphobia: His Art and His Illness RACAR: revue d’art canadienne / Canadian Art Review. 1988, 15, 23–50. Available online: https://www.jstor.org/stable/42630379.
- Bowie, C.R.; Harvey, P.D. Cognitive deficits and functional outcome in schizophrenia. Neuropsychiatr. Dis. Treat. 2006, 2, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Bowlby, J. Separation Anxiety. International Journal of Psychoanalysis 1960, 41, 89–113. [Google Scholar] [PubMed]
- Brandies, R.; Yehuda, S. The possible role of retinal dopaminergic system in visual performance. Neurosci. Biobehav. Rev. 2008, 32, 611–656. [Google Scholar] [CrossRef] [PubMed]
- Brasil, A.; Castro, A.J.O.; Martins, I.C.V.S.; Lacerda, E.M.C.B.; Souza, G.S.; Herculano, A.M.; Rosa, A.A.M.; Rodrigues, A.R.; Silveira, L.C.L. Colour Vision Impairment in Young Alcohol Consumers. PLOS ONE 2015, 10, e0140169. [Google Scholar] [CrossRef] [PubMed]
- Brisch, R.; Saniotis, A.; Wolf, R.; Bielau, H.; Bernstein, H.-G.; Steiner, J.; Bogerts, B.; Braun, A.K.; Jankowski, Z.P.; Ekumaratilake, J.; et al. The role of dopamine in schizophrenia from a neurobiological and evolutionary perspective: Old fashioned, but still in vogue. Front. Psychiatry 2014, 5, 47. [Google Scholar] [CrossRef]
- Brown, A.S.; Schaefer, C.A.; Wyatt, R.J.; Goetz, R.; Begg, M.D.; Gorman, J.M.; Susser, E.S. Maternal exposure to respiratory infections and adult schizophrenia spectrum disorders: A prospective birth cohort study. Schizophr. Bull. 2000, 26, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.S. Exposure to prenatal infection and risk of schizophrenia. Front. Psychiatry 2011, 2, 63. [Google Scholar] [CrossRef]
- Brown, A.S.; Derkits, E.J.; Kendler, K.S.; Lee, Y.H.; Cherkerzian, S.; Seidman, L.J.; Papandonatos, G.D.; Savitz, D.A.; Tsuang, M.T.; Goldstein, J.M.; et al. Prenatal infection and schizophrenia: A review of epidemiologic and translational studies. Am. J. Psychiatry 2010, 167, 261–280. [Google Scholar] [CrossRef]
- Brown, G.; Rafaeli, E. Components of Self-Complexity as Buffers for Depressed Mood. J. Cogn. Psychother. 2007, 21, 310–333. [Google Scholar] [CrossRef]
- Bruteig, M.; Falck, U. K. Edvard Munch Works on Paper; Munch Museum, Yale University Press, 2013. [Google Scholar]
- Bruzzo, A. The chaotic nature of Self. Dialegesthai. Rivista telematica di filosofia 2007, 9. Available online: https://mondodomani.org/dialegesthai/>.
- Bucci, S.; Startup, M.; Wynn, P.; Heathcote, A.; Baker, A.; Lewin, T.J. Referential delusions of communication and reality discrimination deficits in psychosis. Br. J. Clin. Psychol. 2008, 47, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Buckley, P.F.; Miller, B.J.; Lehrer, D.S.; Castle, D.J. Psychiatric Comorbidities and Schizophrenia. Schizophr. Bull. 2009, 35, 383–402. [Google Scholar] [CrossRef] [PubMed]
- Bunney, W.E.; Hetrick, W.P.; Bunney, B.G.; Patterson, J.V.; Jin, Y.; Potkin, S.G.; Sandman, C.A. Structured Interview for Assessing Perceptual Anomalies (SIAPA). Schizophr. Bull. 1999, 25, 577–592. [Google Scholar] [CrossRef] [PubMed]
- Burch, G.S.J.; Pavelis, C.; Hemsley, D.R.; Corr, P.J. Schizotypy and creativity in visual artists. Br. J. Psychol. 2006, 97, 177–190. [Google Scholar] [CrossRef] [PubMed]
- Butler, P.D.; Silverstein, S.M.; Dakin, S.C. Visual Perception and Its Impairment in Schizophrenia Biol Psychiatry. 2008, 64, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Butler, P.D.; Abeles, I.Y.; Weiskopf, N.G.; Tambini, A.; Jalbrzikowski, M.; Legatt, M.E.; Zemon, V.; Loughead, J.; Gur, R.C.; Javitt, D.C. Sensory contributions to impaired emotion processing in schizophrenia. Schizophr. Bull. 2009, 35, 1095–1107. [Google Scholar] [CrossRef] [PubMed]
- Butler, P.D.; Zemon, V.; Schechter, I.; Saperstein, A.M.; Hoptman, M.J.; Lim, K.O.; Revheim, N.; Silipo, G.; Javitt, D.C. Early-Stage Visual Processing and Cortical Amplification Deficits in Schizophrenia. ARCH GEN PSYCHIATRY/VOL 2005, 62. [Google Scholar] [CrossRef]
- Butler, P.D.; Javitt, D.C. Early-stage visual processing deficits in schizophrenia. Curr. Opin. Psychiatry 2005, 18, 151–157. [Google Scholar] [CrossRef]
- Byron, K.; Khazanchi, S. A meta-analytic investigation of the relationship of state and trait anxiety to performance on figural and verbal creative tasks. Pers. Soc. Psychol. Bull. 2011, 37, 269–283. [Google Scholar] [CrossRef] [PubMed]
- Cadenhead, K.S.; Dobkins, K.; McGovern, J.; Shafer, K. Schizophrenia spectrum participants have reduced visual contrast sensitivity to chromatic (red/green) and luminance (light/dark) stimuli: new insights into information processing, visual channel function, and antipsychotic effects. Front. Psychol. 2013, 4, 535. [Google Scholar] [CrossRef] [PubMed]
- Cancel, A.; Dallel, S.; Zine, A.; El-Hage, W.; Fakra, E. Understanding the link between childhood trauma and schizophrenia: A systematic review of neuroimaging studies. Neurosci. Biobehav. Rev. 2019, 107, 492–504. [Google Scholar] [CrossRef] [PubMed]
- Cannon, T.D.; Kaprio, J.; Lönnqvist, J.; Huttunen, M.; Koskenvuo, M. The genetic epidemiology of schizophrenia in a Finnish twin cohort. A population-based modeling study. Arch. Gen. Psychiatry 1998, 55, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Caputo, G.B.; Ferrucci, R.; Bortolomasi, M.; Giacopuzzi, M.; Priori, A.; Zago, S. Visual perception during mirror gazing at one's own face in schizophrenia. Schizophr. Res. 2012, 140, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Cardno, A.G.; Owen, M.J. Genetic relationships between schizophrenia, bipolar disorder, and schizoaffective disorder. Schizophr. Bull. 2014, 40, 504–515. [Google Scholar] [CrossRef] [PubMed]
- Cardno, A.G.; Marshall, E.J.; Coid, B.; Macdonald, A.M.; Ribchester, T.R.; Davies, N.J.; Venturi, P.; Jones, L.A.; Lewis, S.W.; Sham, P.C.; et al. Heritability estimates for psychotic disorders: the Maudsley twin psychosis series. Arch. Gen. Psychiatry 1999, 56, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Carrigan, M.H.; Randall, C.L. Self-medication in social phobia: A review of the alcohol literature. Addictive Behaviors 2003, 28, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Carson, S.H.; Peterson, J.B.; Higgins, D.M. Decreased latent inhibition is associated with increased creative achievement in high-functioning individuals. J. Pers. Soc. Psychol. 2003, 85, 499–506. [Google Scholar] [CrossRef]
- Carson, S.H. Creativity and Psychopathology: A Shared Vulnerability Model. Can. J. Psychiatry 2011, 56, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Casares-López, M.; Castro-Torres, J.J.; Martino, F.; Ortiz-Peregrina, S.; Ortiz, C.; Anera, R.G. Contrast sensitivity and retinal straylight after alcohol consumption: effects on driving performance. Sci. Rep. 2020, 10, 13599. [Google Scholar] [CrossRef]
- Castillo-Carniglia, A.; Keyes, K.M.; Hasin, D.S.; Cerdá, M. Psychiatric comorbidities in alcohol use disorder. Lancet Psychiatry 2019, 6, 1068–1080. [Google Scholar] [CrossRef] [PubMed]
- Castro, A.J.d.O.; Rodrigues, A.R.; Côrtes, M.I.T.; Silveira, L.C.d.L. Impairment of color spatial vision in chronic alcoholism measured by psychophysical methods. Psychol. Neurosci. 2009, 2, 179–187. [Google Scholar] [CrossRef]
- Castro, J.J.; Pozo, A.M.; Rubiño, M.; Anera, R.G.; del Barco, L.J. Retinal-image quality and night-vision performance after alcohol consumption. J. Ophthalmol. 2014, 2014, 704823. [Google Scholar] [CrossRef] [PubMed]
- Celik, M.; Kalenderoglu, A.; Karadag, A.S.; Egilmez, O.B.; Han-Almis, B.; Şimşek, A. Decreases in ganglion cell layer and inner plexiform layer volumes correlate better with disease severity in schizophrenia patients than retinal nerve fiber layer thickness: Findings from spectral optic coherence tomography. Eur. Psychiatry 2016, 32, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Cernuschi, C. Sex and Psyche, Nature and Nurture. In The Personal and the Political: Edvard Munch and German Expressionism; Howe, J., Ed.; Edvard Munch, Psyche, Symbol and Expressionism. Boston College, 2001. [Google Scholar]
- Chakrabarti, S.; Singh, N. Psychotic symptoms in bipolar disorder and their impact on the illness: A systematic review. World J. Psychiatry 2022, 12, 1204–1232. [Google Scholar] [CrossRef] [PubMed]
- Chambers, R.; Krystal, J.H.; Self, D.W. A neurobiological basis for substance abuse comorbidity in schizophrenia. Biol. Psychiatry 2001, 50, 71–83. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J. The Early Symptoms of Schizophrenia. Br. J. Psychiatry 1966, 112, 225–251. [Google Scholar] [CrossRef] [PubMed]
- Chase, H.W.; Loriemi, P.; Wensing, T.; Eickhoff, S.B.; Nickl-Jockschat, T. Meta-analytic evidence for altered mesolimbic responses to reward in schizophrenia. Hum. Brain Mapp. 2018, 39, 2917–2928. [Google Scholar] [CrossRef]
- Chatfield, C.; Xing, H. The Analysis of Time Series: An Introduction with R; Chapman and Hall/CRC: New York, 2019. [Google Scholar]
- Chen, Y.; Nakayama, K.; Levy, D.; Matthysse, S.; Holzman, P. Processing of global, but not local, motion direction is deficient in schizophrenia. Schizophr. Res. 2003, 61, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Levy, D.L.; Sheremata, S.; Nakayama, K.; Matthysse, S.; Holzman, P.S. Effects of typical, atypical, and no antipsychotic drugs on visual contrast detection in schizophrenia. Am. J. Psychiatry 2003, 160, 1795–1801. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Bidwell, L.; Holzman, P.S. Visual motion integration in schizophrenia patients, their first-degree relatives, and patients with bipolar disorder. Schizophr. Res. 2005, 74, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Bidwell, L.C.; Norton, D. Trait vs. State Markers for Schizophrenia: Identification and Characterization Through Visual Processes. Curr. Psychiatry Rev. 2006, 2, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Norton, D.; McBain, R. Can persons with schizophrenia appreciate visual art? Schizophr. Res. 2008, 105, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Cheslack-Postava, K.; Brown, A.S. Prenatal infection and schizophrenia: A decade of further progress. Schizophr. Res. 2022, 247, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Chieffi, S. Dysfunction of magnocellular/dorsal processing stream in schizophrenia. Curr. Psychiatry Res. Rev. 2019, 15, 26–36. [Google Scholar] [CrossRef]
- Chilvers, I. Oxford Dictionary of Art & Artists, 4th ed.; Oxford University Press, 2009. [Google Scholar]
- Cho, W.; Shin, W.-S.; An, I.; Bang, M.; Cho, D.-Y.; Lee, S.-H. Biological Aspects of Aggression and Violence in Schizophrenia. Clin. Psychopharmacol. Neurosci. 2019, 17, 475–486. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, Z.; Lennox, B. Maternal Immune Activation and Schizophrenia-Evidence for an Immune Priming Disorder. Front. Psychiatry 2021, 12, 585742. [Google Scholar] [CrossRef]
- Chouinard, V.-A.; Shinn, A.K.; Valeri, L.; Chouinard, P.A.; Gardner, M.E.; Asan, A.E.; Cohen, B.M.; Öngür, D. Visual hallucinations associated with multimodal hallucinations, suicide attempts and morbidity of illness in psychotic disorders. Schizophr. Res. 2019, 208, 196–201. [Google Scholar] [CrossRef]
- Clarke, M.C.; Tanskanen, A.; Huttunen, M.O.; Cannon, M. Sudden death of father or sibling in early childhood increases risk for psychotic disorder. Schizophr. Res. 2013, 143, 363–366. [Google Scholar] [CrossRef] [PubMed]
- Coid, J.W.; Ullrich, S.; Kallis, C.; Keers, R.; Barker, D.; Cowden, F.; Stamps, R. The relationship between delusions and violence: Findings from the East London first episode psychosis study. JAMA Psychiatry 2013, 70, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Cook, C.C. Religious psychopathology: The prevalence of religious content of delusions and hallucinations in mental disorder. Int. J. Soc. Psychiatry 2015, 61, 404–425. [Google Scholar] [CrossRef] [PubMed]
- Correll, C.U.; Schooler, N.R. Negative Symptoms in Schizophrenia: A Review and Clinical Guide for Recognition, Assessment, and Treatment. Neuropsychiatr. Dis. Treat. 2020, 16, 519–534. [Google Scholar] [CrossRef] [PubMed]
- Creupelandt, C.; D'Hondt, F.; Maurage, P. Towards a Dynamic Exploration of Vision, Cognition and Emotion in Alcohol-Use Disorders. Curr. Neuropharmacol. 2019, 17, 492–506. [Google Scholar] [CrossRef] [PubMed]
- Cullen, K.; Guimaraes, A.; Wozniak, J.; Anjum, A.; Schulz, S.; White, T. Trajectories of social withdrawal and cognitive decline in the schizophrenia prodrome. Clin. Schizophr. Relat. Psychoses 2011, 4, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Cunnigham Dax, E. The Cunnigham Dax Collection: Selected Works of Psychiatric Art; Melbourne University Press: Melbourne, 1998. [Google Scholar]
- Cutting, J.; Dunne, F. Subjective experience of schizophrenia. Schizophr. Bull. 1989, 15, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Cutting, J.; Dunne, F. The Nature of the Abnormal Perceptual Experiences at the Onset of Schizophrenia. Psychopathology 1986, 19, 347–352. [Google Scholar] [CrossRef] [PubMed]
- da Cruz, D.N.; de Andrade, M.J.O.; Cavalcanti-Gaudino, M.K.; Nogueira, R.M.T.B.L.; dos Santos, N.A. Effects of chronic alcoholism in the sensitivity to luminance contrast in vertical sinusoidal gratings. Psicol. E Crit. 2016, 29, 729. [Google Scholar] [CrossRef]
- Dakin, S.; Carlin, P.; Hemsley, D. Weak suppression of visual context in chronic schizophrenia. Curr. Biol. 2005, 15, R822–R824. [Google Scholar] [CrossRef]
- David, C.N.; Greenstein, D.; Clasen, L.; Gochman, P.; Miller, R.; Tossell, J.W.; Mattai, A.A.; Gogtay, N.; Rapoport, J.L. Childhood onset schizophrenia: High rate of visual hallucinations. J. Am. Acad. Child Adolesc. Psychiatry 2011, 50, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Davies, G.; Welham, J.; Chant, D.; Torrey, E.F.; McGrath, J. A Systematic Review and Meta-analysis of Northern Hemisphere Season of Birth Studies in Schizophrenia. Schizophr. Bull. 2003, 29, 587–593. [Google Scholar] [CrossRef] [PubMed]
- Daviet, R.; Aydogan, G.; Jagannathan, K.; Spilka, N.; Koellinger, P.D.; Kranzler, H.R.; Nave, G.; Wetherill, R.R. Associations between alcohol consumption and gray and white matter volumes in the UK Biobank. Nat. Commun. 2022, 13, 1175. [Google Scholar] [CrossRef] [PubMed]
- De Bellis, M.D. Developmental traumatology: a contributory mechanism for alcohol and substance use disorders. Psychoneuroendocrinology 2002, 27, 155–170. [Google Scholar] [CrossRef] [PubMed]
- De Araújo, G.S.; Pereira, S.M.; Dos Santos, D.N.; Marinho, J.M.; Rodrigues, L.C.; Barreto, M.L. Common mental disorders associated with tuberculosis: A matched case-control study. PLOS ONE 2014, 9, e99551. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, L.; Saha, S.; Lim, C.C.W.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Alonso, J.; Andrade, L.H.; Bromet, E.J.; Bruffaerts, R.; Caldas-De-Almeida, J.M.; et al. The associations between psychotic experiences and substance use and substance use disorders: findings from the World Health Organization World Mental Health surveys. Addiction 2018, 113, 924–934. [Google Scholar] [CrossRef] [PubMed]
- de la Calleja, E.; Cervantes, F.; de la Calleja, J. Order-fractal transitions in abstract paintings. Ann. Phys. 2016, 371, 313–322. [Google Scholar] [CrossRef]
- Demmin, D.L.; Davis, Q.; Roché, M.; Silverstein, S.M. Electroretinographic anomalies in schizophrenia. J. Abnorm. Psychol. 2018, 127, 417–428. [Google Scholar] [CrossRef] [PubMed]
- Demmin, D.L.; Netser, R.; Roché, M.W.; Thompson, J.L.; Silverstein, S.M. People with current major depression resemble healthy controls on flash Electroretinogram indices associated with impairment in people with stabilized schizophrenia. Schizophr. Res. 2020, 219, 69–76. [Google Scholar] [CrossRef]
- Deng, Y.; Liu, K.; Cheng, D.; Zhang, J.; Chen, H.; Chen, B.; Li, Y.; Wang, W.; Kong, Y.; Wen, G. Ventral and dorsal visual pathways exhibit abnormalities of static and dynamic connectivities, respectively, in patients with schizophrenia. Schizophr. Res. 2019, 206, 103–110. [Google Scholar] [CrossRef]
- Diaconescu, A.O.; Hauke, D.J.; Borgwardt, S. Models of persecutory delusions: a mechanistic insight into the early stages of psychosis. Mol. Psychiatry 2019, 24, 1258–1267. [Google Scholar] [CrossRef] [PubMed]
- Dima, D.; Dietrich, D.E.; Dillo, W.; Emrich, H.M. Impaired top-down processes in schizophrenia: A DCM study of ERPs. NeuroImage 2010, 52, 824–832. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, F.; Stallings, C.R.; Origoni, A.E.; Vaughan, C.; Khushalani, S.; Schroeder, J.; Yolken, R.H. Cigarette smoking among persons with schizophrenia or bipolar disorder in routine clinical settings, 1999–2011. Psychiatr. Serv. 2013, 64, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Di leva, A. The Fractal Geometry of the Brain; Springer-Verlag New York Inc., 2016; ISBN 9781493981489. [Google Scholar] [CrossRef]
- Djamgoz, M.; Hankins, M.; Hirano, J.; Archer, S. Neurobiology of retinal dopamine in relation to degenerative states of the tissue. Vis. Res. 1997, 37, 3509–3529. [Google Scholar] [CrossRef] [PubMed]
- Do, E.K.; Maes, H.H. Genotype × Environment Interaction in Smoking Behaviors: A Systematic Review. Nicotine Tob. Res. 2017, 19, 387–400. [Google Scholar] [CrossRef] [PubMed]
- Döges, J. The Famed Painting The Scream Holds a Hidden Message. Sci. Am. 2021, 32, 6. [Google Scholar] [CrossRef]
- Drake, R.E.; Osher, F.C.; Noordsy, D.L.; Hurlbut, S.C.; Teague, G.B.; Beaudett, M.S. Diagnosis of Alcohol Use Disorders in Schizophrenia. Schizophr. Bull. 1990, 16, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Duan, L.; Tian, C.; Fu, C.; He, J.; Dai, J.; Shao, X.; Zhu, G. Analysis of color vision and cognitive function in first-episode schizophrenia before and after antipsychotic treatment. J. Psychiatr. Res. 2022, 152, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Dudley, R.; Aynsworth, C.; Cheetham, R.; McCarthy-Jones, S.; Collerton, D. Prevalence and characteristics of multi-modal hallucinations in people with psychosis who experience visual hallucinations. Psychiatry Res. 2018, 269, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Dumitrescu, O.N.; Pucci, F.G.; Wong, K.Y.; Berson, D.M. Ectopic retinal ON bipolar cell synapses in the OFF inner plexiform layer: Contacts with dopaminergic amacrine cells and melanopsin ganglion cells. J. Comp. Neurol. 2009, 517, 226–244. [Google Scholar] [CrossRef]
- Duth, P.S.; Deepa, M.M. Color detection in RGB-modeled images using MAT LAB. Int. J. Eng. Technol. 2018, 7, 29–33. [Google Scholar] [CrossRef]
- Eggum, A. Edvard Munch Paintings, Sketches and Studies; Thames & Hudson: London, 1984. [Google Scholar]
- Elling, C.; Forstner, A.J.; Seib-Pfeifer, L.-E.; Mücke, M.; Stahl, J.; Geiser, F.; Schumacher, J.; Conrad, R. Social anxiety disorder with comorbid major depression – why fearful attachment style is relevant. J. Psychiatr. Res. 2022, 147, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Eng, W.; Heimberg, R.G.; Hart, T.A.; Schneier, F.R.; Liebowitz, M.R. Attachment in individuals with social anxiety disorder: The relationship among adult attachment styles, social anxiety, and depression. Emotion 2001, 1, 365–380. [Google Scholar] [CrossRef] [PubMed]
- Enoch, M. Genetic and environmental influences on the development of alcoholism: Resilience vs. risk. Ann. New York Acad. Sci. 2006, 1094, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Escamilla, M.A.; Zavala, J.M. Genetics of bipolar disorder. Dialog- Clin. Neurosci. 2008, 10, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, U.; Joober, R.; DE Guzman, R.; O’driscoll, G.A. Schizotypy, attention deficit hyperactivity disorder, and dopamine genes. Psychiatry Clin. Neurosci. 2006, 60, 764–767. [Google Scholar] [CrossRef] [PubMed]
- Eysenck, H.J. Creativity as a Product of lntelligence and Personality. In International Handbook of Personality and Intelligence; Saklofske, D.H., Zeidner, M., Eds.; Plenum Press, 1995. [Google Scholar]
- Faravelli, C.; Sauro, C.L.; Godini, L.; Lelli, L.; Benni, L.; Pietrini, F.; Lazzeretti, L.; Talamba, G.A.; Fioravanti, G.; Ricca, V. Childhood stressful events, HPA axis and anxiety disorders. World J. Psychiatry 2012, 2, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Feigenson, K.A.; Keane, B.P.; Roché, M.W.; Silverstein, S.M. Contour integration impairment in schizophrenia and first episode psychosis: State or trait?. Schizophr. Res. 2014, 159, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Fein, G.; Torres, J.; Price, L.J.; Di Sclafani, V. Cognitive performance in long-term abstinent alcoholic individuals. Alcohol. Clin. Exp. Res. 2006, 30, 1538–1544. [Google Scholar] [CrossRef]
- Fernandes, T.M.d.P.; de Almeida, N.L.; dos Santos, N.A. Effects of smoking and smoking abstinence on spatial vision in chronic heavy smokers. Sci. Rep. 2017, 7, 1690. [Google Scholar] [CrossRef]
- Fernandes, T.M.P.; Andrade, S.M.; de Andrade, M.J.O.; Nogueira, R.M.T.B.L.; Santos, N.A. Colour discrimination thresholds in type 1 Bipolar Disorder: a pilot study. Sci. Rep. 2017, 7, 16405. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, T.M.d.P.; de Almeida, N.L.; dos Santos, N.A. Effects of smoking and smoking abstinence on spatial vision in chronic heavy smokers. Sci. Rep. 2017, 7, 1690. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, T.M.P.; de Andrade, M.J.O.; Santana, J.B.; Nogueira, R.M.T.B.L.; dos Santos, N.A. Tobacco Use Decreases Visual Sensitivity in Schizophrenia. Front. Psychol. 2018, 9, 288. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, T.M.P.; Silverstein, S.M.; de Almeida, N.L.; dos Santos, N.A. Psychophysical evaluation of contrast sensitivity using Gabor patches in tobacco addiction. J. Clin. Neurosci. 2018, 57, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, T.M.P.; Silverstein, S.M.; Butler, P.D.; Kéri, S.; Santos, L.G.; Nogueira, R.L.; Santos, N.A. Color vision impairments in schizophrenia and the role of antipsychotic medication type. Schizophr. Res. 2019, 204, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, T.P.; Silverstein, S.M.; Almeida, N.L.; Santos, N.A. Visual impairments in tobacco use disorder. Psychiatry Res. 2019, 271, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, D.; Wilkins, A.J. Uncomfortable images in art and nature. Perception 2008, 37, 1098–1113. [Google Scholar] [CrossRef] [PubMed]
- Ferri, F.; Venskus, A.; Fotia, F.; Cooke, J.; Romei, V. Higher proneness to multisensory illusions is driven by reduced temporal sensitivity in people with high schizotypal traits. Conscious. Cogn. 2018, 65, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Fett, A.-K.J.; Hanssen, E.; Eemers, M.; Peters, E.; Shergill, S.S. Social isolation and psychosis: an investigation of social interactions and paranoia in daily life. Eur. Arch. Psychiatry Clin. Neurosci. 2022, 272, 119–127. [Google Scholar] [CrossRef]
- Foisy, M.-L.; Kornreich, C.; Petiau, C.; Parez, A.; Hanak, C.; Verbanck, P.; Pelc, I.; Philippot, P. Impaired emotional facial expression recognition in alcoholics: Are these deficits specific to emotional cues? Psychiatry Res. 2007, 150, 33–41. [Google Scholar] [CrossRef]
- Forsythe, A.; Williams, T.; Reilly, R.G. What paint can tell us: A fractal analysis of neurological changes in seven artists. Neuropsychology 2017, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Forteller, V. Edvard Munch Som Vi Kjente Ham: Vennene. 22ip il Dreyers Forlag. 1946. [Google Scholar]
- Fortgang, R.G.; Hoff, R.A.; Potenza, M.N. Problem and Pathological Gambling in Schizophrenia: Exploring Links with Substance Use and Impulsivity. J. Gambl. Stud. 2018, 34, 673–688. [Google Scholar] [CrossRef] [PubMed]
- Foxe, J.J.; Doniger, G.M.; Javitt, D.C. Early visual processing deficits in schizophrenia: impaired P1 generation revealed by high-density electrical mapping. NeuroReport 2001, 12, 3815–3820. [Google Scholar] [CrossRef] [PubMed]
- Freud, S. Further Remarks on the Neuro-Psychoses of Defence. The Standard Edition of the Complete Psychological Works of Sigmund Freud 1896, 3, 157–185. [Google Scholar]
- Freud, S. The Interpretation of Dreams. The Standard Edition of the Complete Psychological Works of Sigmund Freud 1900, 4, ix-627. [Google Scholar]
- Frigg, R.; Howard, C. Fact and Fiction in the Neuropsychology of Art. In The Aesthetic Mind: Philosophy and Psychology; Schellekens, E., Goldie, P, Eds.; Oxford University Press, Scholarship on Line, 2011. [Google Scholar] [CrossRef]
- A Frye, M.; Salloum, I.M. Bipolar disorder and comorbid alcoholism: prevalence rate and treatment considerations. Bipolar Disord. 2006, 8, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, L.; Pries, L.-K.; van Os, J.; Erzin, G.; Delespaul, P.; Kenis, G.; Luykx, J.J.; Lin, B.D.; Richards, A.L.; Akdede, B.; et al. Examining facial emotion recognition as an intermediate phenotype for psychosis: Findings from the EUGEI study. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2022, 113, 110440. [Google Scholar] [CrossRef] [PubMed]
- Gagné, A.-M.; Hébert, M.; Maziade, M. Revisiting visual dysfunctions in schizophrenia from the retina to the cortical cells: A manifestation of defective neurodevelopment. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2015, 62, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Galdino, M.K.C.; Mendes, L.C.; Vieira, J.G.; Simas, M.L.d.B.; dos Santos, N.A. Visual perception of radial sine-wave grating after the alcohol consumption. Psicol. USP 2011, 22, 99–115. [Google Scholar] [CrossRef]
- Gatzke-Kopp, L.M.; Beauchaine, T.P. Direct and passive prenatal nicotine exposure and the development of externalizing psychopathology. Child Psychiatry Hum. Dev. 2007, 38, 255–269. [Google Scholar] [CrossRef]
- Goghari, V.M.; Harrow, M.; Grossman, L.S.; Rosen, C. A 20-year multi-follow-up of hallucinations in schizophrenia, other psychotic, and mood disorders. Psychol. Med. 2013, 43, 1151–1160. [Google Scholar] [CrossRef] [PubMed]
- Goghari, V.M.; Harrow, M. Twenty year multi-follow-up of different types of hallucinations in schizophrenia, schizoaffective disorder, bipolar disorder, and depression. Schizophr. Res. 2016, 176, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Götz, K.O.; Götz, K. Personality characteristics of professional artists. Percept. Mot. Ski. 1979, 49, 327–334. [Google Scholar] [CrossRef]
- Götz, K.O.; Götz, K. Personality Characteristics of Successful Artists. 1979, 49, 919–924. [Google Scholar] [CrossRef]
- Gozdzik-Zelazny, A.; Borecki, L.; Pokorski, M. Depressive symptoms in schizophrenic patients. Eur. J. Med Res. 2011, 16, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Grassi, L.; Pavanati, M.; Cardelli, R.; Ferri, S.; Peron, L. HIV-risk behaviour and knowledge about HIV/AIDS among patients with schizophrenia. Psychol. Med. 1999, 29, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Grillo, L. A Possible Link between Anxiety and Schizophrenia and a Possible Role of Anhedonia. Schizophr. Res. Treat. 2018, 2018, 5917475. [Google Scholar] [CrossRef] [PubMed]
- Gröhn, C.; Norgren, E.; Eriksson, L. A systematic review of the neural correlates of multisensory integration in schizophrenia. Schizophr. Res. Cogn. 2021, 27, 100219. [Google Scholar] [CrossRef] [PubMed]
- Gundogan, F.C.; Durukan, A.H.; Mumcuoglu, T.; Sobacı, G.; Bayraktar, M.Z. Acute effects of cigarette smoking on pattern electroretinogram. Doc. Ophthalmol. 2006, 113, 115–121. [Google Scholar] [CrossRef]
- Gutiérrez-García, A.; Calvo, M.G. Social anxiety and trustworthiness judgments of dynamic facial expressions of emotion. J. Behav. Ther. Exp. Psychiatry 2016, 52, 119–127. [Google Scholar] [CrossRef]
- Gutiérrez-García, A.; Calvo, M.G. Social anxiety and threat-related interpretation of dynamic facial expressions: Sensitivity and response bias. Pers. Individ. Differ. 2017, 107, 10–16. [Google Scholar] [CrossRef]
- Hagerhall, C.M.; Purcell, T.; Taylor, R. Fractal dimension of landscape silhouette outlines as a predictor of landscape preference. J. Environ. Psychol. 2004, 24, 247–255. [Google Scholar] [CrossRef]
- Hagerhall, C.M.; Laike, T.; Taylor, R.P.; Küller, M.; Küller, R.; Martin, T.P. Investigations of human EEG response to viewing fractal patterns. Perception 2008, 37, 1488–1494. [Google Scholar] [CrossRef] [PubMed]
- Hansson, A.C.; Gründer, G.; Hirth, N.; Noori, H.R.; Spanagel, R.; Sommer, W.H. Dopamine and opioid systems adaptation in alcoholism revisited: Convergent evidence from positron emission tomography and postmortem studies. Neurosci. Biobehav. Rev. 2019, 106, 141–164. [Google Scholar] [CrossRef] [PubMed]
- Harper, L.; Spencer, E.; Davidson, C.; Hutchinson, C.V. Selectively reduced contrast sensitivity in high schizotypy. Exp. Brain Res. 2020, 238, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.C. Anxiety (Angst). Arch. Gen. Psychiatry 2004, 61, 15–16. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.C. Spring. Arch. Gen. Psychiatry 2007, 64, 996–997. [Google Scholar] [CrossRef]
- Haug, B.A.; Kolle, R.U.; Trenkwalder, C.; Oertel, W.H.; Paulus, W. Predominant affection of the blue cone pathway in Parkinson's disease. Brain 1995, 118, 771–778. [Google Scholar] [CrossRef]
- Heckers, S.; Konradi, C. GABAergic mechanisms of hippocampal hyperactivity in schizophrenia. Schizophr. Res. 2014, 167, 4–11. [Google Scholar] [CrossRef]
- Hedden, W.L.; Dowling, J.E. The interplexiform cell system. II. Effects of dopamine on goldfish retinal neurones. Proc. R. Soc. London. Ser. B. Biol. Sci. 1978, 201, 27–55. [Google Scholar] [CrossRef]
- Heerwagen, J. H.; Orians, G. H. Humans, habitats, and aesthetics. In The biophilia hypothesis; Kellert, S. R., Wilson, E. O., Eds.; Island Press: Covelo, CA, 1993; pp. 138–172. ISBN 9781559631471. [Google Scholar]
- Heffner, J.L.; Strawn, J.R.; DelBello, M.P.; Strakowski, S.M.; Anthenelli, R.M. The co-occurrence of cigarette smoking and bipolar disorder: phenomenology and treatment considerations. Bipolar Disord. 2011, 13, 439–453. [Google Scholar] [CrossRef] [PubMed]
- Heller, R. Munch, His Life and Work; University of Chicago Press, 1984; ISBN 100226326438. [Google Scholar]
- Hodgins, S. Aggressive Behavior Among Persons With Schizophrenia and Those Who Are Developing Schizophrenia: Attempting to Understand the Limited Evidence on Causality. Schizophr. Bull. 2017, 43, 1021–1026. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, S.G.; Asnaani, M.A.; Hinton, D.E. Cultural aspects in social anxiety and social anxiety disorder. Depression Anxiety 2010, 27, 1117–1127. [Google Scholar] [CrossRef] [PubMed]
- Holland, J. G. (2005) (trans.) The Private Journals of Edvard Munch; We Are Flames Which Pour Out Of The Earth. University of Wisconsin Press. ISBN: 0-299-19810-3.
- Holt, N. J. (2015) Schizotypy: A creative advantage? In: Schizotypy: New Dimensions (eds) Editors: Mason, O. and Claridge, G.) Routledge. ISBN 9780815356981.
- Holt, D.J.; Weiss, A.P.; Rauch, S.L.; Wright, C.I.; Zalesak, M.; Goff, D.C.; Ditman, T.; Welsh, R.C.; Heckers, S. Sustained activation of the hippocampus in response to fearful faces in schizophrenia. Biol. Psychiatry 2005, 57, 1011–1019. [Google Scholar] [CrossRef] [PubMed]
- Holt, D.J.; Kunkel, L.; Weiss, A.P.; Goff, D.C.; Wright, C.I.; Shin, L.M.; Rauch, S.L.; Hootnick, J.; Heckers, S. Increased medial temporal lobe activation during the passive viewing of emotional and neutral facial expressions in schizophrenia. Schizophr. Res. 2006, 82, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Holzman, P.S.; Proctor, L.R.; Levy, D.L.; Yasillo, N.J.; Meltzer, H.Y.; Hurt, S.W. Eye-Tracking Dysfunctions in Schizophrenic Patients and Their Relatives. Arch. Gen. Psychiatry 1974, 31, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Hong, L.E.; Schroeder, M.; Ross, T.J.; Buchholz, B.; Salmeron, B.J.; Wonodi, I.; Thaker, G.K.; Stein, E.A. Nicotine enhances but does not normalize visual sustained attention and the associated brain network in schizophrenia. Schizophr. Bull. 2009, 37, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Hoptman, M.J. Impulsivity and aggression in schizophrenia: a neural circuitry perspective with implications for treatment. CNS Spectrums 2015, 20, 280–286. [Google Scholar] [CrossRef]
- Horney, K. Self-analysis; W. W. Norton: New York, 1942. [Google Scholar]
- Howe, J. (ed) (2001) Edvard Munch: Psyche, Symbolism and Expression. Boston: McMullen Museum of Art. ISBN-1892850-02-8.
- Howes, O.D.; McCutcheon, R.; Owen, M.J.; Murray, R.M. The Role of Genes, Stress, and Dopamine in the Development of Schizophrenia. Biol. Psychiatry 2017, 81, 9–20. [Google Scholar] [CrossRef]
- Huang, H.; Dong, M.; Zhang, L.; Zhong, B.-L.; Ng, C.H.; Ungvari, G.S.; Yuan, Z.; Meng, X.; Xiang, Y.-T. Psychopathology and extrapyramidal side effects in smoking and non-smoking patients with schizophrenia: Systematic review and meta-analysis of comparative studies. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2019, 92, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Hunter, A.; Murray, R.; Asher, L.; Leonardi-Bee, J. The Effects of Tobacco Smoking, and Prenatal Tobacco Smoke Exposure, on Risk of Schizophrenia: A Systematic Review and Meta-Analysis. Nicotine Tob. Res. 2020, 22, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Hurlow, J.; MacCabe, J. Paradoxes in creativity and psychiatric conditions. In The Paradoxical Brain; Pascual-Leone, A., Ramachandran, V., Cole, J., Della Sala, S., Manly, T., Mayes, A., et al., Eds.; Cambridge University Press: Cambridge, 2011; pp. 289–300. [Google Scholar] [CrossRef]
- Hwang, C.K.; Chaurasia, S.S.; Jackson, C.R.; Chan, G.C.-K.; Storm, D.R.; Iuvone, P.M. Circadian rhythm of contrast sensitivity is regulated by a dopamine-neuronal PAS-domain protein 2-adenylyl cyclase 1 signaling pathway in retinal ganglion cells. J. Neurosci. 2013, 33, 14989–14997. [Google Scholar] [CrossRef] [PubMed]
- Insel, T.R. Rethinking schizophrenia. Nature 2010, 468, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.R.; Ruan, G.-X.; Aseem, F.; Abey, J.; Gamble, K.; Stanwood, G.; Palmiter, R.D.; Iuvone, P.M.; McMahon, D.G. Retinal dopamine mediates multiple dimensions of light-adapted vision. J. Neurosci. 2012, 32, 9359–9368. [Google Scholar] [CrossRef] [PubMed]
- Janet, P. The major symptoms of hysteria; Macmillan Publishing, 1907. [Google Scholar]
- James, W. The principles of psychology; Holt: New York, 1890. [Google Scholar]
- Jamison, K.R. Mood disorders and patterns of creativity in British writers and artists. Psychiatry 1989, 52, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Jaspers, K. (1913/1997) Allgemeine Psychopathologie. Berlin: Springer; English translation of the 7th edition: General Psychopathology. Baltimore: Johns Hopkins University Press.
- Javitt, D.C. Sensory processing in schizophrenia: neither simple nor intact. Schizophr. Bull. 2009, 35, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Javitt, D.C. Meeting overview: Sensory perception and schizophrenia, Lausanne, Switzerland June 31–July 1, 2014. Schizophr. Res. Cogn. 2015, 2, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Javitt, D.C.; Freedman, R. Sensory processing dysfunction in the personal experience and neuronal machinery of schizophreni. Am. J. Psychiatry 2015, 172, 17–31. [Google Scholar] [CrossRef]
- Jerotic, S.; Ristic, I.; Pejovic, S.; Mihaljevic, M.; Pavlovic, Z.; Britvic, D.; Ignjatovic, Z.; Silverstein, S.M.; Maric, N.P. Retinal structural abnormalities in young adults with psychosis spectrum disorders. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2019, 98, 109825. [Google Scholar] [CrossRef]
- Jiang, N.; Lee, Y.O.; Ling, P.M. Association between tobacco and alcohol use among young adult bar patrons: a cross-sectional study in three cities. BMC Public Heal. 2014, 14, 500. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.; Cowell, R.M.; Nakazawa, K. Convergence of genetic and environmental factors on parvalbumin-positive interneurons in schizophrenia. Front. Behav. Neurosci. 2013, 7, 116. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.L.; Murray, G.; Fredrickson, B.; Youngstrom, E.A.; Hinshaw, S.; Bass, J.M.; Deckersbach, T.; Schooler, J.; Salloum, I. Creativity and bipolar disorder: touched by fire or burning with questions? Clin. Psychol. Rev. 2012, 32, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Juda, A. The relationship between highest mental capacity and psychic abnormalities. Am. J. Psychiatry 1949, 106, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Jurisic, D.; Cavar, I.; Sesar, A.; Sesar, I.; Vukojevic, J.; Curkovic, M. New Insights into Schizophrenia: a Look at the Eye and Related Structures. Psychiatr. Danub. 2020, 32, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Kalenderoglu, A.; Çelik, M.; Sevgi-Karadag, A.; Egilmez, O.B. Optic coherence tomography shows inflammation and degeneration in major depressive disorder patients correlated with disease severity. J. Affect. Disord. 2016, 204, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Kapur, S. Psychosis as a state of aberrant salience: a framework linking biology, phenomenology, and pharmacology in schizophrenia. Am. J. Psychiatry 2003, 160, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, J.L. Genetic association of giftedness and creativity with schizophrenia. Hereditas 2009, 66, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Kathirvel, N.; Mortimer, A. Causes, diagnosis and treatment of visceral hallucinations. Progress in Neurology and Psychiatry January/February. 2013. [Google Scholar]
- Kean, C. Silencing the Self: Schizophrenia as a Self-disturbance. Schizophr. Bull. 2009, 35, 1034–1036. [Google Scholar] [CrossRef]
- Kelemen, O.; Kiss, I.; Benedek, G.; Kéri, S. Perceptual and cognitive effects of antipsychotics in first-episode schizophrenia: The potential impact of GABA concentration in the visual cortex. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2013, 47, 13–19. [Google Scholar] [CrossRef]
- Kelly, C.; McCreadie, R. Cigarette smoking and schizophrenia. Adv. Psychiatr. Treat. 2000, 6, 327–331. [Google Scholar] [CrossRef]
- Kendall, K.M.; Van Assche, E.; Andlauer, T.F.M.; Choi, K.W.; Luykx, J.J.; Schulte, E.C.; Lu, Y. The genetic basis of major depression. Psychol. Med. 2021, 51, 2217–2230. [Google Scholar] [CrossRef] [PubMed]
- Kéri, S.; Antal, A.; Szekeres, G.; Benedek, G.; Janka, Z. Spatiotemporal visual processing in schizophrenia. The Journal of neuropsychiatry and clinical neurosciences 2002, 14, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Kéri, S.; Benedek, G. Visual contrast sensitivity alterations in inferred magnocellular pathways and anomalous perceptual experiences in people at high-risk for psychosis. Vis. Neurosci. 2007, 24, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Keromnes, G.; Chokron, S.; Celume, M.-P.; Berthoz, A.; Botbol, M.; Canitano, R.; Du Boisgueheneuc, F.; Jaafari, N.; Lavenne-Collot, N.; Martin, B.; et al. Exploring Self-Consciousness From Self- and Other-Image Recognition in the Mirror: Concepts and Evaluation. Front. Psychol. 2019, 10, 719. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Norton, D.; McBain, R.; Ongur, D.; Chen, Y. Deficient biological motion perception in schizophrenia: results from a motion noise paradigm. Front. Psychol. 2013, 4, 46070. [Google Scholar] [CrossRef] [PubMed]
- Kiss, I.; Fábián, A.; Benedek, G.; Kéri, S. When doors of perception open: Visual contrast sensitivity in never-medicated, first-episode schizophrenia. J. Abnorm. Psychol. 2010, 119, 586–593. [Google Scholar] [CrossRef]
- Klosterkötter, J.; Hellmich, M.; Steinmeyer, E.M.; Schultze-Lutter, F. Diagnosing schizophrenia in the initial prodromal phase. Arch. Gen. Psychiatry 2001, 58, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Koethe, D.; Kranaster, L.; Hoyer, C.; Gross, S.; Neatby, M.A.; Schultze-Lutter, F.; Ruhrmann, S.; Klosterkötter, J.; Hellmich, M.; Leweke, F.M. Binocular depth inversion as a paradigm of reduced visual information processing in prodromal state, antipsychotic-naïve and treated schizophrenia. Eur. Arch. Psychiatry Clin. Neurosci. 2009, 259, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Kogata, T.; Iidaka, T. A review of impaired visual processing and the daily visual world in patients with schizophrenia. Nagoya journal of medical science 2018, 80, 317–328. [Google Scholar] [CrossRef]
- Kogata, T.; Iidaka, T. Lateralization of Color Discrimination Performance and Lexical Effects in Patients With Chronic Schizophrenia. Front. Hum. Neurosci. 2021, 15, 702086. [Google Scholar] [CrossRef] [PubMed]
- Kohler, C.G.; Turner, T.H.; Bilker, W.B.; Brensinger, C.M.; Siegel, S.J.; Kanes, S.J.; Gur, R.E.; Gur, R.C. Facial emotion recognition in schizophrenia: intensity effects and error pattern. Am J Psychiatry 2003, 160, 1768–1774. [Google Scholar] [CrossRef] [PubMed]
- Kohler, C.G.; Walker, J.B.; Martin, E.A.; Healey, K.M.; Moberg, P.J. Facial emotion perception in schizophrenia: a meta-analytic review. Schizophr. Bull. 2010, 36, 1009–1019. [Google Scholar] [CrossRef] [PubMed]
- Korver-Nieberg, N.; Berry, K.; Meijer, C.J.; de Haan, L. Adult attachment and psychotic phenomenology in clinical and non-clinical samples: A systematic review. Psychol. Psychother. Theory, Res. Pr. 2014, 87, 127–154. [Google Scholar] [CrossRef] [PubMed]
- Koul, A.; Shetty, A. Frequency of psychiatric comorbid symptoms in bipolar disorder patients in remission. Ind. Psychiatry J. 2022, 31, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Kozáková, E.; Bakštein, E.; Havlíček, O.; Bečev, O.; Knytl, P.; Zaytseva, Y.; Španiel, F. Disrupted Sense of Agency as a State Marker of First-Episode Schizophrenia: A Large-Scale Follow-Up Study. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Kraepelin. E. (1896/1971) Dementia Praecox and Paraphrenia. (8th ed.) (trans Barclay, R.M.) Huntington, NY: Krieger Publishing.
- Kretschmer, E. (1970) Physique and Character: An Investigation of the Nature of Constitution and of the Theory of Temperament. (Trans. Miller. E.) New York: Cooper Square Publishers, Inc. ISBN 9781138875401.
- Krynicki, C.R.; Upthegrove, R.; Deakin, J.F.W.; Barnes, T.R.E. The relationship between negative symptoms and depression in schizophrenia: a systematic review. Acta Psychiatr. Scand. 2018, 137, 380–390. [Google Scholar] [CrossRef] [PubMed]
- Krystal, J.H.; D’souza, D.C.; Gallinat, J.; Driesen, N.; Abi-Dargham, A.; Petrakis, I.; Heinz, A.; Pearlson, G. The vulnerability to alcohol and substance abuse in individuals diagnosed with schizophrenia. Neurotox. Res. 2006, 10, 235–252. [Google Scholar] [CrossRef] [PubMed]
- Kumari, V., & Ettinger, U. (2010) Latent inhibition in schizophrenia and schizotypy: a review of the empirical literature Chap. 17. In Latent Inhibition Cognition, Neuroscience and Applications to Schizophrenia (R. and Weiner, I. eds) Cambridge University Press. ISBN: 9780521517331.
- Kuo, S.-C.; Chen, Y.-T.; Li, S.-Y.; Lee, Y.-T.; Yang, A.C.; Chen, T.-L.; Liu, C.-J.; Chen, T.-J.; Su, I.-J.; Fung, C.-P. Incidence and outcome of newly-diagnosed tuberculosis in schizophrenics: a 12-year, nationwide, retrospective longitudinal study. BMC Infect. Dis. 2013, 13, 351–351. [Google Scholar] [CrossRef] [PubMed]
- Kyaga, S.; Lichtenstein, P.; Boman, M.; Hultman, C.; Långström, N.; Landén, M. Creativity and mental disorder: Family study of 300 000 people with severe mental disorder. Br. J. Psychiatry 2011, 199, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Kyaga, S.; Landén, M.; Boman, M.; Hultman, C.M.; Långström, N.; Lichtenstein, P. Mental illness, suicide and creativity: 40-Year prospective total population study. J. Psychiatr. Res. 2013, 47, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Laskemoen, J.F.; Simonsen, C.; Büchmann, C.; Barrett, E.A.; Bjella, T.; Lagerberg, T.V.; Vedal, T.J.; Andreassen, O.A.; Melle, I.; Aas, M. Sleep disturbances in schizophrenia spectrum and bipolar disorders – a transdiagnostic perspective. Compr. Psychiatry 2019, 91, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Laursen, T.M.; Agerbo, E.; Pedersen, C.B. Bipolar disorder, schizoaffective disorder, and schizophrenia overlap: a new comorbidity index. J. Clin. Psychiatry 2009, 70, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Lavin, R.; Bucci, S.; Varese, F.; Berry, K. The relationship between insecure attachment and paranoia in psychosis: A systematic literature review. Br. J. Clin. Psychol. 2020, 59, 39–65. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, N.S.; Ross, T.J.; A Stein, E. Cognitive Mechanisms of Nicotine on Visual Attention. Neuron 2002, 36, 539–548. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Cherkerzian, S.; Seidman, L.J.; Papandonatos, G.D.; Savitz, D.A.; Tsuang, M.T.; Goldstein, J.M.; Buka, S.L. Maternal Bacterial Infection During Pregnancy and Offspring Risk of Psychotic Disorders: Variation by Severity of Infection and Offspring Sex. Am. J. Psychiatry 2020, 177, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Leonard, S.; Mexal, S.; Freedman, R. Smoking, Genetics and Schizophrenia: Evidence for Self Medication. J. Dual Diagn. 2007, 3, 43–59. [Google Scholar] [CrossRef] [PubMed]
- Lew, B.J.; I Wiesman, A.; Rezich, M.T.; Wilson, T.W. Altered neural dynamics in occipital cortices serving visual-spatial processing in heavy alcohol users. J. Psychopharmacol. 2020, 34, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Liu, L.; Tao, Y. Diagnosis and treatment of congenital tuberculosis: a systematic review of 92 cases. Orphanet J. Rare Dis. 2019, 14, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Yang, Y.; An, F.-R.; Zhang, L.; Ungvari, G.S.; Jackson, T.; Yuan, Z.; Xiang, Y.-T. Prevalence of comorbid depression in schizophrenia: A meta-analysis of observational studies. J. Affect. Disord. 2020, 273, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Olsen, J.; Yuan, W.; Cnattingus, S.; Vestergaard, M.; Obel, C.; Gissler, M.; Li, J. Early Life Bereavement and Schizophrenia: A Nationwide Cohort Study in Denmark and Sweden. Medicine 2016, 95, e2434–e2434. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.; Chen, S.; Zhao, L.; Miao, D. Categorization of emotional faces in schizophrenia patients: An ERP study. Neurosci. Lett. 2019, 713, 134493. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, P.; Yip, B.H.; Björk, C.; Pawitan, Y.; Cannon, T.D.; Sullivan, P.F.; Hultman, C.M. Common genetic determinants of schizophrenia and bipolar disorder in Swedish families: a population-based study. Lancet 2009, 373, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Lim, A.; Hoek, H.W.; Deen, M.L.; Blom, J.D.; Bruggeman, R.; Cahn, W.; de Haan, L.; Kahn, R.S.; Meijer, C.J.; Myin-Germeys, I.; et al. Prevalence and classification of hallucinations in multiple sensory modalities in schizophrenia spectrum disorders. Schizophr. Res. 2016, 176, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Linville, P.W. Self-complexity as a cognitive buffer against stress-related illness and depression. Journal of personality and social psychology, 1987; 52, 663–676. [Google Scholar]
- Lisman, J.E.; Coyle, J.T.; Green, R.W.; Javitt, D.C.; Benes, F.M.; Heckers, S.; Grace, A.A. Circuit-based framework for understanding neurotransmitter and risk gene interactions in schizophrenia. Trends Neurosci. 2008, 31, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Lizano, P.; Lutz, O.; Ling, G.; Lee, A.M.; Eum, S.; Bishop, J.R.; Kelly, S.; Pasternak, O.; Clementz, B.; Pearlson, G.; et al. Association of Choroid Plexus Enlargement With Cognitive, Inflammatory, and Structural Phenotypes Across the Psychosis Spectrum. Am. J. Psychiatry 2019, 176, 564–572. [Google Scholar] [CrossRef] [PubMed]
- Lizano, P.; Bannai, D.; Lutz, O.; A Kim, L.; Miller, J.; Keshavan, M. A Meta-analysis of Retinal Cytoarchitectural Abnormalities in Schizophrenia and Bipolar Disorder. Schizophr. Bull. 2020, 46, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Loewy, R.L.; Corey, S.; Amirfathi, F.; Dabit, S.; Fulford, D.; Pearson, R.; Hua, J.P.; Schlosser, D.; Stuart, B.K.; Mathalon, D.H.; et al. Childhood trauma and clinical high risk for psychosis. Schizophr. Res. 2019, 205, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Lubow, A. (2006) Edvard Munch: Beyond the Scream. Smithsonian Magazine; March.
- https://www.smithsonianmag.com/arts-culture/edvard-munch-beyond-the-scream-111810150/.
- Ludwig, A.M. Creative achievement and psychopathology: comparison among professions. Am. J. Psychother. 1992, 46, 330–354. [Google Scholar] [CrossRef] [PubMed]
- Lysaker, P.H.; Hasson-Ohayon, I.; Wiesepape, C.; Huling, K.; Musselman, A.; Lysaker, J.T. Social Dysfunction in Psychosis Is More Than a Matter of Misperception: Advances From the Study of Metacognition. Front. Psychol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- MacCabe, J.H.; Sariaslan, A.; Almqvist, C.; Lichtenstein, P.; Larsson, H.; Kyaga, S. Artistic creativity and risk for schizophrenia, bipolar disorder and unipolar depression: a Swedish population-based case–control study and sib-pair analysis. Br. J. Psychiatry 2018, 212, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Mackinnon, D.W. The nature and nurture of creative talent. Am. Psychol. 1962, 17, 484–495. [Google Scholar] [CrossRef]
- Malaspina, D.; Owen, M.J.; Heckers, S.; Tandon, R.; Bustillo, J.; Schultz, S.; Barch, D.M.; Gaebel, W.; Gur, R.E.; Tsuang, M.; et al. Schizoaffective Disorder in the DSM-5. Schizophr. Res. 2013, 150, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, S.G.; Morgan, V.A.; Mitchell, P.B.; Berk, M.; Young, A.; Castle, D.J. A comparison of schizophrenia, schizoaffective disorder, and bipolar disorder: Results from the Second Australian national psychosis survey. J. Affect. Disord. 2015, 172, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Manjeese, W.; Mvubu, N.E.; Steyn, A.J.C.; Mpofana, T. Mycobacterium tuberculosis causes a leaky blood-brain barrier and neuroinflammation in the prefrontal cortex and cerebellum regions of infected mice offspring. Int. J. Dev. Neurosci. 2021, 81, 428–437. [Google Scholar] [CrossRef] [PubMed]
- Manzella, F.; E Maloney, S.; Taylor, G.T. Smoking in schizophrenic patients: A critique of the self-medication hypothesis. World J. Psychiatry 2015, 5, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Margolis, A.E.; Lee, S.H.; Liu, R.; Goolsby, L.; Champagne, F.; Herbstman, J.; Beebe, B. Associations between prenatal exposure to second hand smoke and infant self-regulation in a New York city longitudinal prospective birth cohort. Environ. Res. 2023, 227, 115652. [Google Scholar] [CrossRef] [PubMed]
- Martins, I.C.V.d.S.; Souza, G.d.S.; Brasil, A.; Herculano, A.M.; Lacerda, E.M.d.C.B.; Rodrigues, A.R.; Rosa, A.A.M.; Ventura, D.F.; Castro, A.J.d.O.; Silveira, L.C.d.L. Psychophysical Evaluation of Visual Functions of Ex-Alcoholic Subjects After Prolonged Abstinence. Front. Neurosci. 2019, 13, 179. [Google Scholar] [CrossRef] [PubMed]
- Maurage, P.; Philippot, P.; Verbanck, P.; Noel, X.; Kornreich, C.; Hanak, C.; Campanella, S. Is the P300 deficit in alcoholism associated with early visual impairments (P100, N170)? An oddball paradigm. Clin. Neurophysiol. 2007, 118, 633–644. [Google Scholar] [CrossRef] [PubMed]
- Maurage, P.; Campanella, S.; Philippot, P.; de Timary, P.; Constant, E.; Gauthier, S.; Miccichè, M.-L.; Kornreich, C.; Hanak, C.; Noel, X.; et al. Alcoholism leads to early perceptive alterations, independently of comorbid depressed state: An ERP study. Neurophysiol. Clin. 2008, 38, 83–97. [Google Scholar] [CrossRef]
- Maziade, M.; Bureau, A.; Jomphe, V.; Gagné, A. Retinal function and preclinical risk traits in children and adolescents at genetic risk of schizophrenia and bipolar disorder. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2022, 112. [Google Scholar] [CrossRef] [PubMed]
- Maziade, M.; Silverstein, S.M. The place of the retina in psychiatry: Uniting neurobiological and neurodevelopmental research with clinical research in psychiatric disorders. Schizophr. Res. 2020, 219, 1–4. [Google Scholar] [CrossRef] [PubMed]
- McCarthy-Jones, S.; Smailes, D.; Corvin, A.; Gill, M.; Morris, D.W.; Dinan, T.G.; Murphy, K.C.; O′Neill, F.A.; Waddington, J.L.; et al. Occurrence and co-occurrence of hallucinations by modality in schizophrenia-spectrum disorders, Australian Schizophrenia Research Bank, Donohoe, G., Dudley, R. Psychiatry Res. 2017, 252, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Bowen, A.M. Munch and Agoraphobia: His Art and His Illness. RACAR : Revue d’art canadienne / Canadian Art Review. 1988, 15, 23–50. [Google Scholar] [CrossRef]
- McElroy, S.L. Diagnosing and treating comorbid (complicated) bipolar disorder. 2004, 65, 35–44. [Google Scholar] [PubMed]
- McGilchrist, I. (2009/2019). The Master and his Emissary. The Divided Brain and the Making of the Western World. Yale University Press. ISBN-10 0300188374.
- McGilchrist, I. (2021) The Matter with Things. Our Brains Our Delusions and the Unmaking of the World. Vol. 1 Perspectiva. ISBN-10 1914568060.
- McTeague, L.M.; Laplante, M.-C.; Bulls, H.W.; Shumen, J.R.; Lang, P.J.; Keil, A. Face Perception in Social Anxiety: Visuocortical Dynamics Reveal Propensities for Hypervigilance or Avoidance. Biol. Psychiatry 2018, 83, 618–628. [Google Scholar] [CrossRef] [PubMed]
- Meier, S.M.; Deckert, J. Genetics of Anxiety Disorders. Curr. Psychiatry Rep. 2019, 21, 16. [Google Scholar] [CrossRef] [PubMed]
- Merritt, K.; Egerton, A.; Kempton, M.J.; Taylor, M.J.; McGuire, P.K. Nature of Glutamate Alterations in Schizophrenia. JAMA Psychiatry 2016, 73, 665–74. [Google Scholar] [CrossRef] [PubMed]
- Michail, M.; Birchwood, M. Social anxiety in first-episode psychosis: The role of childhood trauma and adult attachment. J. Affect. Disord. 2014, 163, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Millan, M.J.; Fone, K.; Steckler, T.; Horan, W.P. Negative symptoms of schizophrenia: Clinical characteristics, pathophysiological substrates, experimental models and prospects for improved treatment. Eur. Neuropsychopharmacol. 2014, 24, 645–692. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.; Messias, E.; Miettunen, J.; Alaräisänen, A.; Järvelin, M.-R.; Koponen, H.; Räsänen, P.; Isohanni, M.; Kirkpatrick, B. Meta-analysis of Paternal Age and Schizophrenia Risk in Male Versus Female Offspring. Schizophr. Bull. 2011, 37, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Mittal, V.A.; Gupta, T.; Keane, B.P.; Silverstein, S.M. Visual context processing dysfunctions in youth at high risk for psychosis: Resistance to the Ebbinghaus illusion and its symptom and social and role functioning correlates. J. Abnorm. Psychol. 2015, 124, 953–960. [Google Scholar] [CrossRef] [PubMed]
- C, M.M.; C, E.M.; D, M.M. Edvard Munch: enfermedad y genialidad en el gran artista noruego [Edvard Munch: disease and genius of the great Norwegian artist]. Rev. Medica De Chile 2013, 141, 774–779. [Google Scholar] [CrossRef]
- Misra, S.; Gelaye, B.; Koenen, K.C.; Williams, D.R.; Borba, C.P.; Quattrone, D.; Di Forti, M.; La Cascia, C.; La Barbera, D.; Tarricone, I.; et al. Early Parental Death and Risk of Psychosis in Offspring: A Six-Country Case-Control Study. J. Clin. Med. 2019, 8, 1081. [Google Scholar] [CrossRef] [PubMed]
- Mitrovic, M.; Ristic, M.; Dimitrijevic, B.; Pesic, M.H. Facial Emotion Recognition and Persecutory Ideation in Paranoid Schizophrenia. Psychol. Rep. 2020, 123, 1099–1116. [Google Scholar] [CrossRef] [PubMed]
- Mize, R.R., Marc, R.E., Sillito, A.M. (1992) Gaba in the Retinal and Central Visual System. Elsevier Science Publishers. ISBN: 0-444-81446-9.
- Moberg, P. J.; Agrin, R.; Gur, R. E.; Gur, R. C.; Turetsky, B. I.; Doty, R. L. Olfactory dysfunction in schizophrenia: a qualitative and quantitative review. Neuropsychopharmacology 1999, 21, 325–340. [Google Scholar] [CrossRef] [PubMed]
- Moe, A.M.; Docherty, N.M. Schizophrenia and the sense of self. Schizophr. Bull. 2013, 40, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Monistrol-Mula, A.; Felez-Nobrega, M.; Oh, H.; Haro, J.M.; Koyanagi, A. Association between tuberculosis and psychotic experiences: Mediating factors and implications for patient care in low- and middle-income countries. J. Glob. Heal. 2024, 14, 04005. [Google Scholar] [CrossRef] [PubMed]
- Mosolov, S.N.; Yaltonskaya, P.A. Primary and Secondary Negative Symptoms in Schizophrenia. Front. Psychiatry 2022, 12, 766692. [Google Scholar] [CrossRef] [PubMed]
- Müller, V.; Ohström, K.-R.P.; Lindenberger, U. Interactive brains, social minds: Neural and physiological mechanisms of interpersonal action coordination. Neurosci. Biobehav. Rev. 2021, 128, 661–677. [Google Scholar] [CrossRef] [PubMed]
- Müller-Westermann (2005) Munch by Himself. Royal Academy of Arts. ISBN 1-903973-64-3.
- Murphy, F.; Nasa, A.; Cullinane, D.; Raajakesary, K.; Gazzaz, A.; Sooknarine, V.; Haines, M.; Roman, E.; Kelly, L.; O'Neill, A.; et al. Childhood Trauma, the HPA Axis and Psychiatric Illnesses: A Targeted Literature Synthesis. Front. Psychiatry 2022, 13, 748372. [Google Scholar] [CrossRef] [PubMed]
- Muros, N.I.; García, A.S.; Forner, C.; López-Arcas, P.; Lahera, G.; Rodriguez-Jimenez, R.; Nieto, K.N.; Latorre, J.M.; Fernández-Caballero, A.; Fernández-Sotos, P. Facial Affect Recognition by Patients with Schizophrenia Using Human Avatars. J. Clin. Med. 2021, 10, 1904. [Google Scholar] [CrossRef] [PubMed]
- Nakazawa, K.; Zsiros, V.; Jiang, Z.; Nakao, K.; Kolata, S.; Zhang, S.; Belforte, J.E. GABAergic interneuron origin of schizophrenia pathophysiology. Neuropharmacology 2012, 62, 1574–1583. [Google Scholar] [CrossRef] [PubMed]
- Nakazawa, K.; Sapkota, K. The origin of NMDA receptor hypofunction in schizophrenia. Pharmacol. Ther. 2020, 205, 107426–107426. [Google Scholar] [CrossRef] [PubMed]
- Nayak, S.R.; Mishra, J. An improved method to estimate the fractal dimension of colour images. Perspect. Sci. 2016, 8, 412–416. [Google Scholar] [CrossRef]
- Nelson, B.; Rawlings, D. Relating schizotypy and personality to the phenomenology of creativity. Schizophr. Bull. 2010, 36, 388–399. [Google Scholar] [CrossRef] [PubMed]
- Nettle, D.; Clegg, H. Schizotypy, creativity and mating success in humans. Proc. R. Soc. B: Biol. Sci. 2006, 273, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Northoff, G.; Heinzel, A.; de Greck, M.; Bermpohl, F.; Dobrowolny, H.; Panksepp, J. Self-referential processing in our brain—A meta-analysis of imaging studies on the self. NeuroImage 2006, 31, 440–457. [Google Scholar] [CrossRef] [PubMed]
- Núñez, D.; Rauch, J.; Herwig, K.; Rupp, A.; Andermann, M.; Weisbrod, M.; Resch, F.; Oelkers-Ax, R. Evidence for a magnocellular disadvantage in early-onset schizophrenic patients: A source analysis of the N80 visual-evoked component. Schizophr. Res. 2013, 144, 16–23. [Google Scholar] [CrossRef] [PubMed]
- O'Donnell, B.F.; Swearer, J.M.; Smith, L.T.; Nestor, P.G.; E Shenton, M.; McCarley, R.W. Selective deficits in visual perception and recognition in schizophrenia. Am. J. Psychiatry 1996, 153, 687–692. [Google Scholar] [CrossRef] [PubMed]
- O'Donnell, B.F.; Bismark, A.; Hetrick, W.P.; Bodkins, M.; Vohs, J.L.; Shekhar, A. Early stage vision in schizophrenia and schizotypal personality disorder. Schizophr. Res. 2006, 86, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Onstad, S.; Skre, I.; Torgersen, S.; Kringlen, E. Twin concordance for DSM-III-R schizophrenia. Acta Psychiatr. Scand. 1991, 83, 395–401. [Google Scholar] [CrossRef] [PubMed]
- O’toole, M.; Hougaard, E.; Mennin, D. Social anxiety and emotion knowledge: A meta-analysis. J. Anxiety Disord. 2013, 27, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Ouzir, M. Impulsivity in schizophrenia: A comprehensive update. Aggress. Violent Behav. 2013, 18, 247–254. [Google Scholar] [CrossRef]
- Pallanti, S.; Quercioli, L.; Hollander, E. Social anxiety in outpatients with schizophrenia: a relevant cause of disability. Am. J. Psychiatry 2004, 161, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, R.V.; Marraccini, M.E.; Weyandt, L.L.; Wilder-Smith, O.; McGee, H.A.; Liu, S.; Goodwin, M.S. Interpersonal Autonomic Physiology: A Systematic Review of the Literature. Pers. Soc. Psychol. Rev. 2017, 21, 99–141. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.C.; Zhou, A.B. Altered Auditory Self-recognition in People with Schizophrenia. Span. J. Psychol. 2020, 23, e52. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Zhou, Y.; Xiang, Y.; Yu, J. Retinal nerve fiber layer thickness changes in Schizophrenia: A meta-analysis of case–control studies. Psychiatry Res. 2018, 270, 786–791. [Google Scholar] [CrossRef]
- Parker, G. The suprasensory world of bipolar II disorder. Am. J. Psychiatry 2014, 171, 614–615. [Google Scholar] [CrossRef]
- Parker, G.; Paterson, A.; Romano, M.; Graham, R. Altered Sensory Phenomena Experienced in Bipolar Disorder. Am. J. Psychiatry 2017, 174, 1146–1150. [Google Scholar] [CrossRef] [PubMed]
- Parnas, J.; Henriksen, M.G. Disordered Self in the Schizophrenia Spectrum. Harv. Rev. Psychiatry 2014, 22, 251–265. [Google Scholar] [CrossRef] [PubMed]
- Pawełczyk, A.; Kotlicka-Antczak, M.; Łojek, E.; Ruszpel, A.; Pawełczyk, T. Schizophrenia patients have higher-order language and extralinguistic impairments. Schizophr. Res. 2018, 192, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Peeling, J.L, Muzio, M.R. (2023) Conversion Disorder. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551567/.
- Peschard, V.; Philippot, P. Overestimation of threat from neutral faces and voices in social anxiety. J. Behav. Ther. Exp. Psychiatry 2017, 57, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Vlamings, P.H.J.M.; Goffaux, V.; Kemner, C. Is the early modulation of brain activity by fearful facial expressions primarily mediated by coarse low spatial frequency information? J. Vis. 2009, 9, 12–12. [Google Scholar] [CrossRef] [PubMed]
- Phillipson, O.T.; Harris, J.P. Perceptual changes in schizophrenia: a questionnaire survey. Psychol. Med. 1985, 15, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Pincus, D.; Cadsky, O.; Berardi, V.; Asuncion, C.M.; Wann, K. Fractal Self-Structure and Psychological Resilience. Nonlinear dynamics, psychology, and life sciences 2019, 23, 57–78. [Google Scholar] [PubMed]
- Post, F. Creativity and psychopathology: a study of 291world-famous men. Br. J. Psychiatry 1994, 165, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Postmes, L.; Sno, H.; Goedhart, S.; van der Stel, J.; Heering, H.; de Haan, L. Schizophrenia as a self-disorder due to perceptual incoherence. Schizophr. Res. 2014, 152, 41–50. [Google Scholar] [CrossRef] [PubMed]
- A Power, R.; Steinberg, S.; Bjornsdottir, G.; A Rietveld, C.; Abdellaoui, A.; Nivard, M.M.; Johannesson, M.; E Galesloot, T.; Hottenga, J.J.; Willemsen, G.; et al. Polygenic risk scores for schizophrenia and bipolar disorder predict creativity. Nat. Neurosci. 2015, 18, 953–955. [Google Scholar] [CrossRef] [PubMed]
- Powers, A.R.; Kelley, M.; Corlett, P.R. Hallucinations as Top-Down Effects on Perception. Biol. Psychiatry: Cogn. Neurosci. Neuroimaging 2016, 1, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Prideaux S. (2005) Edvard Munch: Behind the Scream. New Haven, Conn: Yale University Press. ISBN 978-0-300-25000.
- Price, M.J.; Feldman, R.G.; Adelberg, D.; Kayne, H. Abnormalities in color vision and contrast sensitivity in Parkinson's disease. Neurology 1992, 42, 887–887. [Google Scholar] [CrossRef] [PubMed]
- Pries, L.-K.; Guloksuz, S.; Have, M.T.; de Graaf, R.; van Dorsselaer, S.; Gunther, N.; Rauschenberg, C.; Reininghaus, U.; Radhakrishnan, R.; Bak, M.; et al. Evidence That Environmental and Familial Risks for Psychosis Additively Impact a Multidimensional Subthreshold Psychosis Syndrome. Schizophr. Bull. 2018, 44, 710–719. [Google Scholar] [CrossRef] [PubMed]
- Viswanath, B.; Purty, A.; Nestadt, G.; Samuels, J. Genetics of obsessive-compulsive disorder. Indian J. Psychiatry 2019, 61, 37–S42. [Google Scholar] [CrossRef] [PubMed]
- Quigley, H.; MacCabe, J.H. The relationship between nicotine and psychosis. Ther. Adv. Psychopharmacol. 2019, 9. [Google Scholar] [CrossRef] [PubMed]
- Radua, J.; Ramella-Cravaro, V.; Ioannidis, J.P.; Reichenberg, A.; Phiphopthatsanee, N.; Amir, T.; Thoo, H.Y.; Oliver, D.; Davies, C.; Morgan, C.; et al. What causes psychosis? An umbrella review of risk and protective factors. World Psychiatry 2018, 17, 49–66. [Google Scholar] [CrossRef] [PubMed]
- Rakesh, K.; Arvind, S.; Dutt, B.P.; Mamta, B.; Bhavneesh, S.; Kavita, M.; Navneet, K.; Shrutika, G.; Priyanka, B.; Arun, K.; et al. The Role of Religiosity and Guilt in Symptomatology and Outcome of Obsessive Compulsive Disorder. Psychopharmacology bulletin 2021, 51, 38–49. [Google Scholar]
- Redies, C.; Hänisch, J.; Blickhan, M.; Denzler, J. Artists portray human faces with the Fourier statistics of complex natural scenes. Network: Comput. Neural Syst. 2007, 18, 235–248. [Google Scholar] [CrossRef] [PubMed]
- Redies, C.; Hasenstein, J.; Denzler, J. Fractal-like image statistics in visual art: similarity to natural scenes. Spat. Vis. 2007, 21, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Read, J.; Bentall, R.P. Negative childhood experiences and mental health: theoretical, clinical and primary prevention implications. Br. J. Psychiatry 2012, 200, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Reeve, S.; Nickless, A.; Sheaves, B.; Freeman, D. Insomnia, negative affect, and psychotic experiences: Modelling pathways over time in a clinical observational study. Psychiatry Res. 2018, 269, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Regier, D.A.; Farmer, M.E.; Rae, D.S.; Locke, B.Z.; Keith, S.J.; Judd, L.L.; Goodwin, F.K. Comorbidity of Mental Disorders With Alcohol and Other Drug Abuse. JAMA 1990, 264, 2511–2518. [Google Scholar] [CrossRef] [PubMed]
- Revheim, N.; Corcoran, C.M.; Dias, E.; Hellmann, E.; Martinez, A.; Butler, P.D.; Lehrfeld, J.M.; DiCostanzo, J.; Albert, J.; Javitt, D.C. Reading Deficits in Schizophrenia and Individuals at High Clinical Risk: Relationship to Sensory Function, Course of Illness, and Psychosocial Outcome. Am. J. Psychiatry 2014, 171, 949–959. [Google Scholar] [CrossRef] [PubMed]
- Richards, R.; Kinney, D.K.; Lunde, I.; Benet, M.; Merzel, A.P. Creativity in manic-depressives, cyclothymes, their normal relatives, and control subjects. J. Abnorm. Psychol. 1988, 97, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J. (1991) A life of Picasso Vol. 1 1881-1906. Jonathan Cape. ISBN-100394531922.
- Richter, J.; Hölz, L.; Hesse, K.; Wildgruber, D.; Klingberg, S. Measurement of negative and depressive symptoms: Discriminatory relevance of affect and expression. Eur. Psychiatry 2019, 55, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Ritsner, M. The attribution of somatization in schizophrenia patients: a naturalistic follow-up study. J. Clin. Psychiatry 2003, 64, 1370–1378. [Google Scholar] [CrossRef] [PubMed]
- Robinson, N.; Bergen, S.E. Environmental Risk Factors for Schizophrenia and Bipolar Disorder and Their Relationship to Genetic Risk: Current Knowledge and Future Directions. Front. Genet. 2021, 12, 686666. [Google Scholar] [CrossRef] [PubMed]
- Roquelaure, Y.; LE Gargasson, J.F.; Kupper, S.; Girre, C.; Hispard, E.; Dally, S. Alcohol consumption and visual contrast sensitivity. Alcohol Alcohol. 1995, 30, 681–685. [Google Scholar] [CrossRef] [PubMed]
- Rossetti, I.; Repossi, M.; Florio, V.; Demartini, B.; Conca, A.; Gambini, O.; Maravita, A. Sense of body ownership and body agency in schizophrenia. Sci. Rep. 2022, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Rothenberg, A. Bipolar Illness, Creativity, and Treatment. Psychiatr. Q. 2001, 72, 131–147. [Google Scholar] [CrossRef] [PubMed]
- Rothenberg, A. (2015) Creativity and Mental Illness II: The Scream. Psychology Today, 24 March. https://www.psychologytoday.com/gb/blog/creative-explorations/201503/creativity-and-mental-illness-iithe-scream.
- Roy, M.-A.; Demers, M.-F.; Achim, A.M. Social anxiety disorder in schizophrenia: a neglected, yet potentially important comorbidity. J. Psychiatry Neurosci. 2018, 43, 287–288. [Google Scholar] [CrossRef] [PubMed]
- Roy, A.; Roy, M.; Berman, J.; Gonzalez, B. Blue cone electroretinogram amplitudes are related to dopamine function in cocaine-dependent patients. Psychiatry Res. 2003, 117, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Rubin, L.H.; Han, J.; Coughlin, J.M.; Hill, S.K.; Bishop, J.R.; Tamminga, C.A.; Clementz, B.A.; Pearlson, G.D.; Keshavan, M.S.; Gershon, E.S.; et al. Real-time facial emotion recognition deficits across the psychosis spectrum: A B-SNIP Study. Schizophr. Res. 2022, 243, 489–499. [Google Scholar] [CrossRef] [PubMed]
- Runco, M.A.; Noble, E.P.; Reiter-Palmon, R.; Acar, S.; Ritchie, T.; Yurkovich, J.M. The genetic basis of creativity and ideational fluency. Creativity Res. J. 2011, 23, 376–380. [Google Scholar] [CrossRef]
- Ruocco, A.C.; Reilly, J.L.; Rubin, L.H.; Daros, A.R.; Gershon, E.S.; Tamminga, C.A.; Pearlson, G.D.; Hill, S.K.; Keshavan, M.S.; Gur, R.C.; et al. Emotion recognition deficits in schizophrenia-spectrum disorders and psychotic bipolar disorder: Findings from the Bipolar-Schizophrenia Network on Intermediate Phenotypes (B-SNIP) study. Schizophr. Res. 2014, 158, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Samani, N.N.; A Proudlock, F.; Siram, V.; Suraweera, C.; Hutchinson, C.; Nelson, C.P.; Al-Uzri, M.; Gottlob, I. Retinal Layer Abnormalities as Biomarkers of Schizophrenia. Schizophr. Bull. 2018, 44, 876–885. [Google Scholar] [CrossRef] [PubMed]
- Samsom, J.N.; Wong, A.H.C. Schizophrenia and Depression Co-Morbidity: What We have Learned from Animal Models. Front. Psychiatry 2015, 6, 13–13. [Google Scholar] [CrossRef] [PubMed]
- Sandsten, K.E.; Nordgaard, J.; Kjaer, T.W.; Gallese, V.; Ardizzi, M.; Ferroni, F.; Petersen, J.; Parnas, J. Altered self-recognition in patients with schizophrenia. Schizophr. Res. 2020, 218, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Sandyk, R.; Kay, S.R.; Merriam, A.E. Atrophy of the cerebellar vermis: relevance to the symptoms of schizophrenia. Int. J. Neurosci. 1991, 57, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Saramba, M.I.; Zhao, D. A Perspective of the Diagnosis and Management of Congenital Tuberculosis. J. Pathog. 2016, 2016, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Schallmo, M.-P.; Sponheim, S.R.; Olman, C.A. Reduced Contextual Effects on Visual Contrast Perception in Schizophrenia and Bipolar Affective Disorder. Psychol. Med. 2015, 45, 3527–3537. [Google Scholar] [CrossRef] [PubMed]
- Schechter, I.; Butler, P.D.; Jalbrzikowski, M.; Pasternak, R.; Saperstein, A.M.; Javitt, D.C. A new dimension of sensory dysfunction: stereopsis deficits in schizophrenia. Biol. Psychiatry 2006, 60, 1282–1284. [Google Scholar] [CrossRef] [PubMed]
- Schneier, F.R.; Johnson, J.; Hornig, C.D.; Liebowitz, M.R.; Weissman, M.M. Social phobia: comorbidity and morbidity in an epidemiological sample. Arch Gen Psychiatry, 1992; 55, 322–331. [Google Scholar]
- Schönfeldt-Lecuona, C.; Kregel, T.; Schmidt, A.; Kassubek, J.; Dreyhaupt, J.; Freudenmann, R.W.; Connemann, B.J.; Gahr, M.; Pinkhardt, E.H. Retinal single-layer analysis with optical coherence tomography (OCT) in schizophrenia spectrum disorder. Schizophr. Res. 2020, 219, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Schönfeldt-Lecuona, C.; Kregel, T.; Schmidt, A.; Pinkhardt, E.H.; Lauda, F.; Kassubek, J.; Connemann, B.J.; Freudenmann, R.W.; Gahr, M. From Imaging the Brain to Imaging the Retina: Optical Coherence Tomography (OCT) in Schizophrenia. Schizophr. Bull. 2016, 42, sbv073–14. [Google Scholar] [CrossRef] [PubMed]
- Schubert, E.W.; Henriksson, K.M.; McNeil, T.F. A prospective study of offspring of women with psychosis: visual dysfunction in early childhood predicts schizophrenia-spectrum disorders in adulthood. Acta Psychiatr. Scand. 2005, 112, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Schuler, A.-L.; Tik, M.; Sladky, R.; Luft, C.D.B.; Hoffmann, A.; Woletz, M.; Zioga, I.; Bhattacharya, J.; Windischberger, C. Modulations in resting state networks of subcortical structures linked to creativity. NeuroImage 2019, 195, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.; McNeill, Y.; Cavanagh, J.; Cannon, M.; Murray, R. Exposure to obstetric complications and subsequent development of bipolar disorder. Br. J. Psychiatry 2006, 189, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Pedraza, I.; Romero-Ferreiro, V.; Read, J.C.A.; Diã©Guez-Risco, T.; Bagney, A.; Caballero-Gonzã¡Lez, M.; Rodrã guez-Torresano, J.; Rodriguez-Jimenez, R. Reduced visual surround suppression in schizophrenia shown by measuring contrast detection thresholds. Front. Psychol. 2014, 5, 1431–1431. [Google Scholar] [CrossRef] [PubMed]
- Shantna, K.; Chaudhury, S.; Verma, A.; Singh, A. Comorbid psychiatric disorders in substance dependence patients: A control study. Ind. Psychiatry J. 2009, 18, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Sorrell, J.H.; Peralta, N.R. A Protracted Case of Psychosis, Motor Abnormalities, and Agitation. Prim. Care Companion J. Clin. Psychiatry 2007, 9, 151–152. [Google Scholar] [CrossRef] [PubMed]
- Sheinbaum, T.; Bedoya, E.; Ros-Morente, A.; Kwapil, T.R.; Barrantes-Vidal, N. Association between attachment prototypes and schizotypy dimensions in two independent non-clinical samples of Spanish and American young adults. Psychiatry Res. 2013, 210, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Shoham, N.; Eskinazi, M.; Hayes, J.F.; Lewis, G.; Theodorsson, M.; Cooper, C. Associations between psychosis and visual acuity impairment: A systematic review and meta-analysis. Acta Psychiatr. Scand. 2021, 144, 6–27. [Google Scholar] [CrossRef]
- Shuwairi, S.M.; Cronin-Golomb, A.; McCarley, R.W.; O'Donnell, B.F. Color discrimination in schizophrenia. Schizophr. Res. 2002, 55, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Silva, G.M.; Souto, J.J.; Fernandes, T.P.; Bonifacio, T.A.; Almeida, N.L.; Gomes, G.H.; Felisberti, F.M.; Santos, N.A. Impairments of facial detection in tobacco use disorder: baseline data and impact of smoking duration. Rev. Bras. de Psiquiatr. 2021, 43, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, S.M.; Keane, B.P. Perceptual Organization Impairment in Schizophrenia and Associated Brain Mechanisms: Review of Research from 2005 to 2010. Schizophr. Bull. 2011, 37, 690–699. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, S.M.; Rosen, R. Schizophrenia and the eye. Schizophr. Res. Cogn. 2015, 2, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, S. M. (2016). Visual perception disturbances in schizophrenia: A unified model. In M. Li & W. D. Spaulding (Eds.), The neuropsychopathology of schizophrenia: Molecules, brain systems, motivation, and cognition (pp. 77–132). Springer International Publishing AG.
- Silverstein, S.M.; Kovács, I.; Corry, R.; Valone, C. Perceptual organization, the disorganization syndrome, and context processing in chronic schizophrenia. Schizophr. Res. 2000, 43, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, S.M.; Lai, A. The Phenomenology and Neurobiology of Visual Distortions and Hallucinations in Schizophrenia: An Update. Front. Psychiatry 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, S.M.; Lai, A.; Green, K.M.; Crosta, C.; I Fradkin, S.; Ramchandran, R.S. Retinal Microvasculature in Schizophrenia. Eye Brain 2021, 13, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Silvia, P.J.; Kimbrel, N.A. A dimensional analysis of creativity and mental illness: Do anxiety and depression symptoms predict creative cognition, creative accomplishments, and creative self-concepts? Psychol. Aesthetics, Creativity, Arts 2010, 4, 2–10. [Google Scholar] [CrossRef]
- Silverstein, S.M.; Thompson, J.L. A vision science perspective on schizophrenia. Schizophr. Res. Cogn. 2015, 2, 39–41. [Google Scholar] [CrossRef] [PubMed]
- Simeonova, D.; Chang, K.; Strong, C.; Ketter, T. Creativity in familial bipolar disorder. J. Psychiatr. Res. 2005, 39, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Simonton, D.K. Creativity in the Later Years: Optimistic Prospects for Achievement. Gerontol. 1990, 30, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Skryabin, V.Y.; Skryabina, A.A.; Torrado, M.V.; Gritchina, E.A. Edvard Munch: the collision of art and mental disorder. Ment. Heal. Relig. Cult. 2020, 23, 570–578. [Google Scholar] [CrossRef]
- Slaghuis, W.A. Contrast sensitivity for stationary and drifting spatial frequency gratings in positive- and negative-symptom schizophrenia. J. Abnorm. Psychol. 1998, 107, 49–62. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.; Pantelis, C.; McGrath, J.; Tangas, C.; Copolov, D. Ocular Abnormalities in Chronic Schizophrenia: Clinical Implications. Aust. New Zealand J. Psychiatry 1997, 31, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Soares-Weiser, K.; Maayan, N.; Bergman, H.; Davenport, C.; Kirkham, A.J.; Grabowski, S.; E Adams, C. First rank symptoms for schizophrenia. Cochrane Database Syst. Rev. 2015, 2015, CD010653. [Google Scholar] [CrossRef]
- Solesvik, M.; Joa, I.; Larsen, T.K.; Langeveld, J.; Johannessen, J.O.; Bjørnestad, J.; Anda, L.G.; Gisselgård, J.; Hegelstad, W.T.V.; Brønnick, K. Visual Hallucinations in First-Episode Psychosis: Association with Childhood Trauma. PLOS ONE 2016, 11, e0153458–e0153458. [Google Scholar] [CrossRef] [PubMed]
- Sood, M.; Ganesh, R.; Mahapatra, A.; Verma, R.; Chadda, R.K. Somatic symptoms in schizophrenia: Association with socio-demographic and clinical characteristics, disability and quality of life. Indian J. Psychiatry 2023, 65, 749–754. [Google Scholar] [CrossRef] [PubMed]
- Sossen, B.; Richards, A.S.; Heinsohn, T.; Frascella, B.; Balzarini, F.; Oradini-Alacreu, A.; Odone, A.; Rogozinska, E.; Häcker, B.; Cobelens, F.; et al. The natural history of untreated pulmonary tuberculosis in adults: a systematic review and meta-analysis. Lancet Respir. Med. 2023, 11, 367–379. [Google Scholar] [CrossRef] [PubMed]
- Spehar, B.; Clifford, C.W.; Newell, B.R.; Taylor, R.P. Universal aesthetic of fractals. Comput. Graph. 2003, 27, 813–820. [Google Scholar] [CrossRef]
- Clair, D.S.; Lang, B. Schizophrenia: a classic battle ground of nature versus nurture debate. Sci. Bull. 2021, 66, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Stahl, S.M. Beyond the dopamine hypothesis of schizophrenia to three neural networks of psychosis: dopamine, serotonin, and glutamate. CNS Spectrums 2018, 23, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Stang, R. (1977). Edvard Munch: The Man and His Art (trans. Culverwell, G.). Abbeville Press. ISBN: 0-89659-025-9.
- Stankewicz HA, Salen P. (2018) Alcohol related psychosis. Treasure Island, FL: StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK459134/.
- Stanton, K.J.; Denietolis, B.; Goodwin, B.J.; Dvir, Y. Childhood Trauma and Psychosis. Child Adolesc. Psychiatr. Clin. North Am. 2020, 29, 115–129. [Google Scholar] [CrossRef] [PubMed]
- Stein, M.B. An epidemiologic perspective on social anxiety disorder. . 2006, 3–8. [Google Scholar]
- Stein, M.B.; Stein, D.J. Social anxiety disorder. Lancet 2008, 371, 1115–1125. [Google Scholar] [CrossRef]
- Stenersen, R. (1944/1969) Edvard Munch – Close-Up of a Genius. Stockholm: Sem & Stenersen A/S. ISBN 82-7046-057-5.
- Stern, D.N. The Interpersonal World of the Infant. Basic Books. ISBN-10185575200X. 1985. [Google Scholar]
- Sterzer, P.; Adams, R.A.; Fletcher, P.; Frith, C.; Lawrie, S.M.; Muckli, L.; Petrovic, P.; Uhlhaas, P.; Voss, M.; Corlett, P.R. The Predictive Coding Account of Psychosis. Biol. Psychiatry 2018, 84, 634–643. [Google Scholar] [CrossRef] [PubMed]
- Stuve, T.A.; Friedman, L.; Jesberger, J.A.; Gilmore, G.C.; Strauss, M.E.; Meltzer, H.Y. The relationship between smooth pursuit performance, motion perception and sustained visual attention in patients with schizophrenia and normal controls. Psychol. Med. 1997, 27, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, P.F.; Kendler, K.S.; Neale, M.C. Schizophrenia as a Complex Trait. Arch. Gen. Psychiatry 2003, 60, 1187–1192. [Google Scholar] [CrossRef] [PubMed]
- Swanton, T. The dopamine, glutamate, and GABA hypotheses of schizophrenia: Glutamate may be the key. ANU Undergraduate Research Journal, 2020; 10, 88–96. [Google Scholar]
- Swee, M.B.; Hudson, C.C.; Heimberg, R.G. Examining the relationship between shame and social anxiety disorder: A systematic review. Clin. Psychol. Rev. 2021, 90, 102088. [Google Scholar] [CrossRef] [PubMed]
- Tadin, D.; Kim, J.; Doop, M.L.; Gibson, C.; Lappin, J.S.; Blake, R.; Park, S. Weakened Center-Surround Interactions in Visual Motion Processing in Schizophrenia. J. Neurosci. 2006, 26, 11403–11412. [Google Scholar] [CrossRef] [PubMed]
- Tagliati, M.; Bodis-Wollner, I.; Kovanecz, I.; Stanzione, P. Spatial frequency tuning of the monkey pattern erg depends on d2 receptor-linked action of dopamine. Vis. Res. 1994, 34, 2051–2057. [Google Scholar] [CrossRef] [PubMed]
- Tandon, R.; Gaebel, W.; Barch, D.M.; Bustillo, J.; Gur, R.E.; Heckers, S.; Malaspina, D.; Owen, M.J.; Schultz, S.; Tsuang, M.; et al. Definition and description of schizophrenia in the DSM-5. Schizophr. Res. 2013, 150, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Tandon, R.; Nasrallah, H.A.; Keshavan, M.S. Schizophrenia,“Just the Facts” 6. Moving ahead with the schizophrenia concept: from the elephant to the mouse. Schizophrenia Res. 2009, 110, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R., Newell, B., Spehar, B. (2005) Fractals: A Resonance between Art and Nature Mathematics and Culture II, ISBN : 978-3-540-21368-0. [CrossRef]
- Taylor, R. Reduction of Physiological Stress Using Fractal Art and Architecture. Leonardo 2006, 39, 245–251. [Google Scholar] [CrossRef]
- Taylor, R.P.; Sprott, J.C. Biophilic fractals and the visual journey of organic screen-savers. . 2008, 12, 117–29. [Google Scholar] [PubMed]
- Taylor, R.P.; Spehar, B.; Van Donkelaar, P.; Hagerhall, C.M. Perceptual and Physiological Responses to Jackson Pollock's Fractals. Front. Hum. Neurosci. 2011, 5, 10034. [Google Scholar] [CrossRef] [PubMed]
- Ryymin, T. “Tuberculosis-threatened Children”: The Rise and Fall of a Medical Concept in Norway, c.1900–1960. Med Hist. 2008, 52, 347–364. [Google Scholar] [CrossRef] [PubMed]
- ter Borg, M.; Trenité, D.K.-N. The cultural context of diagnosis: The case of Vincent van Gogh. Epilepsy Behav. 2012, 25, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Thor, S.; Hemmingsson, T.; Danielsson, A.-K.; Landberg, J. Fathers’ alcohol consumption and risk of substance-related disorders in offspring. Drug Alcohol Depend. 2022, 233, 109354. [Google Scholar] [CrossRef] [PubMed]
- Tibber, M.S.; Anderson, E.J.; Bobin, T.; Antonova, E.; Seabright, A.; Wright, B.; Carlin, P.; Shergill, S.S.; Dakin, S.C. Visual Surround Suppression in Schizophrenia. Front. Psychol. 2013, 4, 88. [Google Scholar] [CrossRef] [PubMed]
- Tibbo, P.; Swainson, J.; Chue, P.; LeMelledo, J.-M. Prevalence and relationship to delusions and hallucinations of anxiety disorders in schizophrenia. Depression Anxiety 2003, 17, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Ting, J. H.; Zainal, N.; Kanagasundram, S.; Mohamed, S. Conversion Symptoms In Schizophrenia: A Case Report. Malaysian Journal Of Psychiatry 2010, 18, 18. [Google Scholar]
- Tomar, R.; Gupta, A.; Prasad, T.; Bhalla, P.; Murthy, G. Congenital Tuberculosis. Med J. Armed Forces India 2008, 64, 78–80. [Google Scholar] [CrossRef] [PubMed]
- Tøjner, P. E. (2001) Munch in His Own Words. Prestel, Munich. ISBN: 3-7913-2494-2.
- Trotta, A.; Kang, J.; Stahl, D.; Yiend, J. Interpretation Bias in Paranoia: A Systematic Review and Meta-Analysis. Clin. Psychol. Sci. 2021, 9, 3–23. [Google Scholar] [CrossRef]
- True, W.R.; Xian, H.; Scherrer, J.F.; Madden, P.A.F.; Bucholz, K.K.; Heath, A.C.; Eisen, S.A.; Lyons, M.J.; Goldberg, J.; Tsuang, M. Common Genetic Vulnerability for Nicotine and Alcohol Dependence in Men. Arch. Gen. Psychiatry 1999, 56, 655–661. [Google Scholar] [CrossRef]
- Tsitsipa, E.; Fountoulakis, K.N. The neurocognitive functioning in bipolar disorder: a systematic review of data. Ann. Gen. Psychiatry 2015, 14, 1–29. [Google Scholar] [CrossRef]
- Tsoi, D.T.; Lee, K.-H.; Khokhar, W.A.; Mir, N.U.; Swalli, J.S.; Gee, K.A.; Pluck, G.; Woodruff, P.W. Is facial emotion recognition impairment in schizophrenia identical for different emotions? A signal detection analysis. Schizophr. Res. 2008, 99, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Turetsky, B.I.; Kohler, C.G.; Indersmitten, T.; Bhati, M.T.; Charbonnier, D.; Gur, R.C. Facial emotion recognition in schizophrenia:When and why does it go awry? Schizophr. Res. 2007, 94, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Turkheimer, F.E.; Fagerholm, E.D.; Vignando, M.; Dafflon, J.; Da Costa, P.F.; Dazzan, P.; Leech, R. A GABA Interneuron Deficit Model of the Art of Vincent van Gogh. Front. Psychiatry 2020, 11, 685. [Google Scholar] [CrossRef] [PubMed]
- Turkheimer, F.E.; Leech, R.; Expert, P.; Lord, L.-D.; Vernon, A.C. The brain's code and its canonical computational motifs. From sensory cortex to the default mode network: A multi-scale model of brain function in health and disease. Neurosci. Biobehav. Rev. 2015, 55, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Turner, S.; Mota, N.; Bolton, J.; Sareen, J. Self-medication with alcohol or drugs for mood and anxiety disorders: A narrative review of the epidemiological literature. Depression Anxiety 2018, 35, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Uhlhaas, P.J.; Silverstein, S.M. Perceptual Organization in Schizophrenia Spectrum Disorders: Empirical Research and Theoretical Implications. Psychol. Bull. 2005, 131, 618–632. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, R.S. View through a window may influence recovery from surgery. Science 1984, 224, 420–421. [Google Scholar] [CrossRef] [PubMed]
- Upthegrove, R.; Birchwood, M.; Ross, K.; Brunett, K.; McCollum, R.; Jones, L. The evolution of depression and suicidality in first episode psychosis. Acta Psychiatr. Scand. 2010, 122, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Ustvedt, O. (2020) Edvard Munch: An Inner Life. London: Thames & Hudson. ISBN 978-0-500-29576-2.
- Vardaxi, C.C.; Gonda, X.; Fountoulakis, K.N. Life events in schizoaffective disorder: A systematic review. J. Affect. Disord. 2018, 227, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Valle, R. Schizophrenia in ICD-11: Comparison of ICD-10 and DSM-5. Span. J. Psychiatry Ment. Heal. 2020, 13, 95–104. [Google Scholar] [CrossRef]
- van der Weiden, A.; Prikken, M.; van Haren, N.E. Self–other integration and distinction in schizophrenia: A theoretical analysis and a review of the evidence. Neurosci. Biobehav. Rev. 2015, 57, 220–237. [Google Scholar] [CrossRef] [PubMed]
- van Ommen, M.M.; van Beilen, M.; Cornelissen, F.W.; Smid, H.G.O.M.; Knegtering, H.; Aleman, A.; van Laar, T. ; GROUP Investigators The prevalence of visual hallucinations in non-affective psychosis, and the role of perception and attention. Psychol. Med. 2016, 46, 1735–1747. [Google Scholar] [CrossRef] [PubMed]
- Vardaxi, C.C.; Gonda, X.; Fountoulakis, K.N. Life events in schizoaffective disorder: A systematic review. J. Affect. Disord. 2018, 227, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Varela, M.; Chaos, Ruiz-Esteban, R.; Mestre De Juan, M.J. Fractals, and Our Concept of Disease. Perspectives in Biology and Medicine 2010, 53, 584–595. [Google Scholar]
- Varghese, S.B.; Reid, J.C.; Hartmann, E.E.; Keyser, K.T. The Effects of Nicotine on the Human Electroretinogram. Investig. Opthalmology Vis. Sci. 2011, 52, 9445–9451. [Google Scholar] [CrossRef] [PubMed]
- Varsamis, J.; Adamson, J.D. Somatic Symptoms in Schizophrenia. Can. Psychiatr. Assoc. J. 1976, 21, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Velikonja, T.; Fisher, H.L.; Mason, O.; Johnson, S. Childhood trauma and schizotypy: a systematic literature review. Psychol. Med. 2015, 45, 947–963. [Google Scholar] [CrossRef] [PubMed]
- Velthorst, E.; Fett, A.-K.J.; Reichenberg, A.; Perlman, G.; van Os, J.; Bromet, E.J.; Kotov, R. The 20-Year Longitudinal Trajectories of Social Functioning in Individuals With Psychotic Disorders. Am. J. Psychiatry 2017, 174, 1075–1085. [Google Scholar] [CrossRef] [PubMed]
- Verhaeghen, P.; Joorman, J.; Khan, R. Why We Sing the Blues: The Relation Between Self-Reflective Rumination, Mood, and Creativity. Emotion 2005, 5, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Viengkham, C.; Spehar, B. Preference for Fractal-Scaling Properties Across Synthetic Noise Images and Artworks. Front. Psychol. 2018, 9, 1439. [Google Scholar] [CrossRef] [PubMed]
- Viertiö, S.; Laitinen, A.; Perälä, J.; Saarni, S.I.; Koskinen, S.; Lönnqvist, J.; Suvisaari, J. Visual impairment in persons with psychotic disorder. Chest 2007, 42, 902–908. [Google Scholar] [CrossRef] [PubMed]
- Vila-Badia, R.; Butjosa, A.; Del Cacho, N.; Serra-Arumí, C.; Esteban-Sanjusto, M.; Ochoa, S.; Usall, J. Types, prevalence and gender differences of childhood trauma in first-episode psychosis. What is the evidence that childhood trauma is related to symptoms and functional outcomes in first episode psychosis? A systematic review. Schizophr. Res. 2021, 228, 159–179. [Google Scholar] [CrossRef] [PubMed]
- Vitay J. & Hamker F.H. (2007) On the Role of Dopamine in Cognitive Vision. In: Paletta L., Rome E. (eds) Attention in Cognitive Systems. Theories and Systems from an Interdisciplinary Viewpoint. LNAI 4840, pp. 352–366 WAPCV. Lecture Notes in Computer Science, vol 4840. Springer, Berlin, Heidelberg.
- Vollmer-Larsen, A.; Handest, P.; Parnas, J. Reliability of Measuring Anomalous Experience: The Bonn Scale for the Assessment of Basic Symptoms. Psychopathology 2007, 40, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Voskuil, P. Vincent van Gogh and his illness. A reflection on a posthumous diagnostic exercise. Epilepsy Behav. 2020, 111, 107258. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Yu, Z.; Pan, Z.; Zhao, K.; Zhao, Q.; Zhou, D.; Shen, H.-W.; Wu, X. Impaired Binocular Depth Perception in First-Episode Drug-Naive Patients With Schizophrenia. Front. Psychol. 2018, 9, 850. [Google Scholar] [CrossRef] [PubMed]
- Warick, L., & Warick, E., (2014) Edvard Munch A Study of Loss, Grief and Creativity 22 Nov. https://www.msu.edu/course/ha/446/panter.htm.
- Waters, F.; Collerton, D.; Ffytche, D.H.; Jardri, R.; Pins, D.; Dudley, R.; Blom, J.D.; Mosimann, U.P.; Eperjesi, F.; Ford, S.; et al. Visual Hallucinations in the Psychosis Spectrum and Comparative Information From Neurodegenerative Disorders and Eye Disease. Schizophr. Bull. 2014, 40, S233–S245. [Google Scholar] [CrossRef] [PubMed]
- Waters, F.; Woodward, T.; Allen, P.; Aleman, A.; Sommer, I. Self-recognition Deficits in Schizophrenia Patients With Auditory Hallucinations: A Meta-analysis of the Literature. Schizophr. Bull. 2010, 38, 741–750. [Google Scholar] [CrossRef] [PubMed]
- Watson, C.G.; Kucala, T.; Tilleskjor, C.; Jacobs, L. Schizophrenic Birth Seasonality in Relation to the Incidence of Infectious Diseases and Temperature Extremes. Arch. Gen. Psychiatry 1984, 41, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Weber-Stadlbauer, U. Epigenetic and transgenerational mechanisms in infection-mediated neurodevelopmental disorders. Transl. Psychiatry 2017, 7, e1113–e1113. [Google Scholar] [CrossRef] [PubMed]
- Weir, David (2023) Bohemians: A Very Short Introduction. Oxford University Press. ISBN: 9780197538296.
- Wermes, R.; Lincoln, T.M.; Helbig-Lang, S. Anxious and alert? Hypervigilance in social anxiety disorder. Psychiatry Res. 2018, 269, 740–745. [Google Scholar] [CrossRef] [PubMed]
- West, B.J. Where Medicine Went Wrong - Rediscovering the Path to Complexity; World Scientific Publishing, 2006; ISBN 9789810213770. [Google Scholar]
- Whitfield, C.L.; Dube, S.R.; Felitti, V.J.; Anda, R.F. Adverse childhood experiences and hallucinations. Child Abus. Negl. 2005, 29, 797–810. [Google Scholar] [CrossRef] [PubMed]
- Whiting, D.; Gulati, G.; Geddes, J.R.; Fazel, S. Association of Schizophrenia Spectrum Disorders and Violence Perpetration in Adults and Adolescents From 15 Countries. JAMA Psychiatry 2022, 79, 120–132. [Google Scholar] [CrossRef] [PubMed]
- Woll, G. (2001) Edvard Munch, The Complete Graphic Works. Abrams, New York. ISBN-100810908743.
- Woll, G. (2008) Edvard Munch Complete Paintings, Catalogue Raissone. London: Thames & Hudson. ISBN 13: 9780500093450.
- Wylie, H.W., Jr. Edvard Munch. American Imago , Winter 1980, 37, 413–443. [Google Scholar]
- Wylie, M.L.; Wylie, H.W., Jr. The Creative Relationship of Internal and External Determinants in the Life of an Artist. Annual of Psychoanalysis 1989, 17, 73–128. [Google Scholar]
- Yakovenko, I.; Clark, C.M.; Hodgins, D.C.; Goghari, V.M. A qualitative analysis of the effects of a comorbid disordered gambling diagnosis with schizophrenia. Schizophr. Res. 2016, 171, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.H.; Maddock, R.J.; Rokem, A.; Silver, M.A.; Minzenberg, M.J.; Ragland, J.D.; Carter, C.S. GABA Concentration Is Reduced in Visual Cortex in Schizophrenia and Correlates with Orientation-Specific Surround Suppression. J. Neurosci. 2010, 30, 3777–3781. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.H.; Maddock, R.J.; Cui, E.D.; Minzenberg, M.J.; Niendam, T.A.; Lesh, T.; Solomon, M.; Ragland, J.D.; Carter, C. Reduced in vivo visual cortex GABA in schizophrenia, a replication in a recent onset sample. Schizophr. Res. 2020, 215, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Young, B.G. A phenomenological comparison of LSD and schizophrenic states. Br J Psychiatry 1974, 124, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.-Y.; Hur, J.-W.; Jung, W.H.; Jang, J.H.; Youn, T.; Kang, D.-H.; Park, S.; Kwon, J.S. Dysfunctional role of parietal lobe during self-face recognition in schizophrenia. Schizophr. Res. 2014, 152, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.; Lu, Z.; Li, Y.; Cowart, L.A.; Lopes-Virella, M.F.; Huang, Y. Docosahexaenoic acid antagonizes the boosting effect of palmitic acid on LPS inflammatory signaling by inhibiting gene transcription and ceramide synthesis. PLoS One 2016, 11, e0193343. [Google Scholar] [CrossRef] [PubMed]
- Zemon, V.; Herrera, S.; Gordon, J.; Revheim, N.; Silipo, G.; Butler, P.D. Contrast sensitivity deficits in schizophrenia: A psychophysical investigation. Eur. J. Neurosci. 2021, 53, 1155–1170. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Zhang, M.; Zhang, J. Association of COMT and COMT-DRD2 interaction with creative potential. Front. Hum. Neurosci. 2014, 8, 216. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, X.; King, A.; McNamara, P.; Pokorny, J.; Cao, D. Differential effects of alcohol on contrast processing mediated by the magnocellular and parvocellular pathways. J. Vis. 2012, 12, 16–16. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, C.; Fang, T.; Chen, C.; Chen, M.; Sun, Y.; Ma, X.; Li, R.; Tian, H.; Ping, J. Brain imaging features in schizophrenia with co-occurring auditory verbal hallucinations and depressive symptoms—Implication for novel therapeutic strategies to alleviate the reciprocal deterioration. Brain Behav. 2020, 11, e01991. [Google Scholar] [CrossRef]
- Żochowska, A.; Nowicka, M.M.; Wójcik, M.J.; Nowicka, A. Self-face and emotional faces—are they alike? Soc. Cogn. Affect. Neurosci. 2021, 16, 593–607. [Google Scholar] [CrossRef]
| 1 | The Scream is among the most famous paintings in the world ((https://edition.cnn.com/style/article/most-famous-paintings/index.html). On the reverse Munch wrote: “Can only have been painted by a madman” (Döges, 2021). |
| 2 | For images of his work in chronological order:https://en.wikipedia.org/wiki/List_of_paintings_by_Edvard_Munch. |
| 3 | “My fear of life is necessary to me, as is my illness. Without anxiety and illness, I am a ship without a rudder. My art is grounded in reflections over being different from others. My sufferings are part of my self and my art. They are indistinguishable from me, and their destruction would destroy my art. I want to keep those sufferings.” (Prideaux, 2005, 251; Tøjner, 2001, hereafter respectively ‘Prideaux’ and ‘Tøjner’). |
| 4 | Munch left several thousand pages of journals, correspondence, poetry, and fiction. His exhibitions are well documented, there are numerous contemporary reviews of his art and a significant number of people he knew wrote memoires of him (for translated materials see: https://www.emunch.no/english.xhtml; for memoires see: Stang; Är Til Är, 1961 and Stenersen, 1944 (hereafter, ‘Stenersen’). |
| 5 | Although a consequence of spinal tuberculosis, it was a source of Munch’s belief in his hereditary madness (Prideaux; Tøjner). |
| 6 | This may be compared to Picasso’s Blue Period precipitated by death of a close friend (Richardson 1991). |
| 7 | For a detailed explanation of colour extraction using MatLab (see: Duth & Deepa, 2018). |
| 8 | Paintings completed in periods of crisis in his life ‘Critical Years’ are highlighted. |
Figure 1.
Mean: 0.221; SD: 0.085. Range: 0.056 – 0.405. Critical years: Mean: 0.216, SD: 0.084.
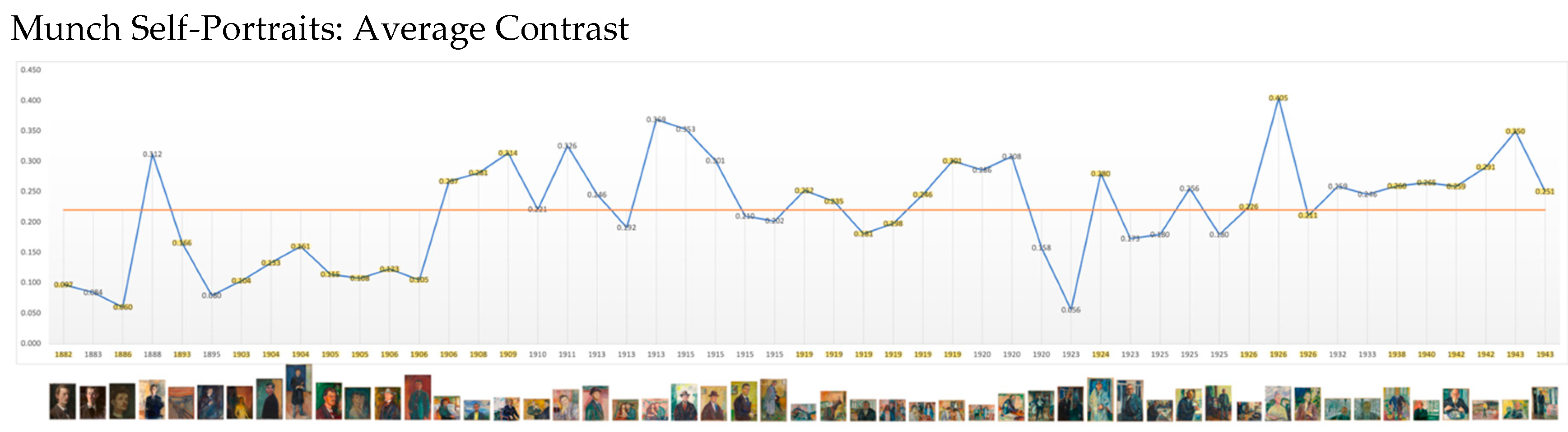
Figure 2.
Mean: 0.258, SD: 0.11, Range: 0.025 – 0.596. Critical years: Mean 0.256, SD. 0.110.

Figure 7.
Mean: 1.786; SD: 0.089; Range: 1.547 – 1.956. Critical years: Mean: 1.769; SD: 0.081.

Figure 8.
Mean: 1.80, SD: 0.106. Range: 1.292 – 1.968. Critical years: Mean: 1.810, SD: 0.091.

Figure 9.
Critical and Non-Critical Periods.

Figure 10.
Mean: 1.738; SD: 0.132. Range: 1.314-1.887. Critical years: Mean: 1.791; SD: 0.067.
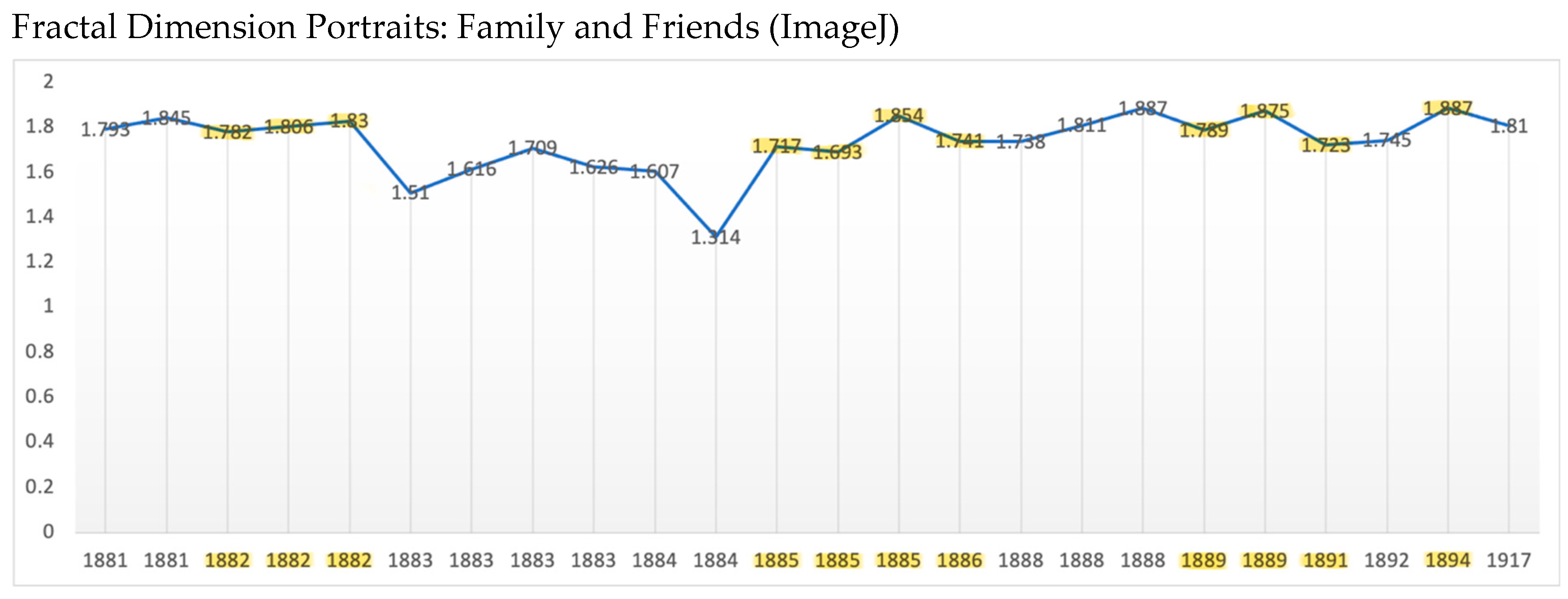
Figure 11.
Mean: 27.4.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



