
Submitted:
23 June 2024
Posted:
24 June 2024
You are already at the latest version
Abstract
Lower respiratory infections (LRI), upper respiratory infections (URI), and nutritional deficiency (ND) in under-5 children from low-middle-income countries has been at a high level for decades, despite efforts that have been realized in some countries. The study used data extracted from the global burden of diseases (GBD) to analyze the trends behavior between 1990 and 2019, and evaluate their association with maternal factors. Between 1990 and 2019, the incidence of LRI decreased between 1.2 percent and 1.3 percent (1.2-1.3%) in different female age groups, and by nearly 1 to 1.3% in those of the male gender. The incidence of URI did not decrease (0.0%) in any of their age groups. ND incidence declined around 0.7 to 4.9% in the under-5 children. LRI declined mostly in the female age groups (1.2 to 1.3%), while ND decreased more in the male gender (0.9 to 4.9%). Maternal risk factors were strongly associated to the incidence of the three conditions with over 90 percent. Maternal prevalence of HIV/AIDS and tuberculosis positively impacted the incidence of LRI, URI, and ND in Chadian under-5 children. Although the incidence of LRI and ND declined, URI incidence remained steady between 1990 and 2019 in Chadian under-5 children. To improve the health and provide a healthy growth of under-5 children, the maternal prevalence of HIV/AIDS and tuberculosis infection should be strongly addressed for a prompt accomplishment of the sustainable development goals.
Keywords:
Lower respiratory infections 1
; Upper respiratory infections 2
; Nutritional deficiency 3
; Under-5 children 4
; Maternal health and environmental risk factors 5
; Chad 6.
1. Introduction
The Lower respiratory infections (LRI) and upper respiratory infections (URI) are the two forms of medical conditions that affect the respiratory system, usually caused by a virus or bacteria [1]. In LRI, a viral agent frequently causes bronchitis or bronchiolitis, and streptococcus pneumoniae is commonly the bacterial agent [1]. When the causative agent of LRI reaches the distal airways through inhalation, aspiration or hematogenous seeding, its multiplication produces inflammation, elevated mucus secretion, unbalanced mucociliary function, necrosis, and sometimes airways obstruction causing fever, sputum production, chest pain, cough, headache, nausea, and tachypnea [1]. URI are mostly caused by viral agents such as adenovirus, coronavirus, and rhinovirus, leading to sneezing, fever, stuffy nose, tachypnea, etc. [1]. The association of recurrent respiratory infections and immune system deficiency in children has been described by previous studies [2,3]. Such association was revealed to have a long-term effect on children’s health because of the interdependence between immunoglobulin classes [2,3].
Nutrition is of great importance in the production of energy designed to promote all the processes in humans [4]. When the intake of nutrients is lower than the necessary average, nutritional inadequacy is present, and it triggers nutritional deficiency (ND) when severe [4]. ND is traduced by an important decline in nutrients, causing an abnormal performance of the body and an exposure to many diseases [4]. Conditions such as anorexia nervosa, intestinal malabsorption, food scarcity, impaired digestion, and persistent vomiting are generally associated with ND [4].
During 2019, more than 150 million of under-five (under-5) children were diagnosed with nutritional deficiency [5], and over 1 million under-5 children’s deaths were annually attributed to respiratory infections [6]. Furthermore, over 80 percent (80%) of respiratory infections are identified in low- and middle-income countries (LMICs) [6].
The republic of Chad (Chad) is classified as a low-income country during 2019 according to the world bank (WB) [7]. Thus, the country is also associated with the highest numbers of under-5 mortality caused by respiratory infections and nutritional deficiencies [5-7]. In 2018, 119 deaths per 1000 live births were recorded in Chadian under-5 children caused by different medical conditions such nutrition deficiency, respiratory diseases, malaria, etc. [8]. Moreover, another study mentioned that Chad listed nearly 18,000 under-5 deaths caused by pneumonia in 2018 [9], and three (3) children out of 1000 die from nutritional deficiencies daily during the same year (2018) [10]. Such alarming numbers demonstrate how the health of under-5 children is fragile and should be considered as a high-level public health priority in the nation.
Existing studies [11-14] have described the association between under-5 mortality and numerous maternal medical conditions and environmental factors such as maternal gynecological diseases (GD), the human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS), heath exposure, maternal disorders (MD), tuberculosis infection (TB), malaria, etc in LMICs although an accurate quantification of the interconnection degree remained challenging. Other studies [9-11] have discussed the trends of respiratory diseases and nutritional deficiency in under-5 children from Chad superficially presenting the relationship between the burden of under-5 children’s diseases and certain socioeconomic risk factors. However, there was no record of a study that discussed the trends behavior of the incidence of LRI, URI, and ND in Chadian female and male under-5 children; and measured the degree of their associations with some maternal medical and environmental risk factors.
To contribute to one of the targets of the sustainable development goals (SDGs) which is ending preventable deaths in newborns and under-5 children, with countries to reduce their mortality rates between 12 and 25 per 1000 live births across the world by 2030 [15], the present study aims to evaluate the trends of LRI, URI, and ND incidence in under-5 children from Chad by gender; and to establish the degree of their association relative to maternal health and environmental conditions.
2. Materials and Methods
2.1. Data source
The Global Burden of Diseases (GBD) provided the data extracted in this study [16]. The incidence rates of lower respiratory infections (LRI), upper respiratory infections (URI), and nutritional deficiency (ND) were evaluated per 100,000 children. The under-5 age category is divided into four age groups. The early neonates are those aged between 0-6 days, followed by the late neonates who are aged between 7 and 27 days. The post-neonates include infants aged between 28 and 364 days. The last age group is composed of children aged between 1 and 4 years, as described by the GBD [16]. The maternal health and environmental factors represented by the prevalence of the followings: gynecological diseases (GD), the human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS), tuberculosis infection (TB), maternal disorders (MD), hepatitis B (HB), malaria, nutritional deficiency (ND), alcohol use disorders (AUD), heat and cold exposure (HCE), and malaria were all downloaded from the GBD database relative to women of reproductive age (women aged between 15 and 49 years old).
The GBD database is under the Institute for Health Metrics and Evaluation (IHME) control in Seattle, Washington State, USA. Primary data sources for GBD include household surveys with complete birth histories, censuses, vital registrations, disease surveillance systems, and sample registration systems. The data utilized for the research is based on GBD data input under the Global Health Data Exchange (GHDx) section in the results tools. Further details were described on the GBD official website [16]. Ethical approval was not needed for this study because there was no direct involvement or interaction with human subjects.
2.2. Statistical analysis
The aims of the present research article are to evaluate the different behaviors of LRI, URI, and ND incidence trends in Chadian under-5 female and male children and identify the various degrees of their associations with certain maternal health and environmental factors. To accomplish those objectives, the study employed the following statistical analyses.
2.2.1. Trends assessment: Joinpoint regression
The behaviors of the trends from the incidence of LRI, URI, and ND from 1990 to 2019 was analyzed using Joinpoint regression. Years with significant changes in the patterns were identified, and the annual percentage change (APC) and the average annual percent change (AAPC), along with their 95% confidence interval (CI), were also estimated for each trend segment between the study period (1990-2019). The equation and algorithm for Joinpoint regression analysis calculations are described elsewhere [17]. Many studies used the same regression analysis (Joinpoint regression) to access different trends [18-21]. The study utilized Joinpoint regression software program (version 4.9.0.0, March 2021) from the Statistical Research and Application branch of the U.S. National Cancer Institute Surveillance Research Program to conduct the analysis.
2.2.2. Association and impact evaluation: LASSO regression
In the current study, the selected independent variables are all related to maternal age category (women aged between 15 and 49 years old). They include the prevalence of gynecological diseases (GD), the prevalence of the human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS), the prevalence of maternal disorders (MD), the prevalence of tuberculosis (TB), the prevalence of hepatitis B (HB), the prevalence of nutritional deficiency (ND), the prevalence of malaria, the prevalence of alcohol use disorders (AUD), and finally the prevalence of heat and cold exposure (HCE) which were found significantly high in Chad during 2019 according to GBD study findings [16]. Anterior studies [11-14] identified the association between some of those maternal conditions and under-5 children mortality, although the estimation of the different degree of association remained generally challenging.
Pearson correlation coefficients of the variables differ relative to the incidence of the diseases, as presented in Table 1. Strong statistically significant correlation coefficients could be identified among the estimates which could indicate the presence of multicollinearity [22]. Multicollinearity is commonly debated when conducting regression analyses. In the presence of multicollinearity, the regression outcome estimates could be misleading because multicollinearity can generate considerable confidence intervals and few significant likelihood values of the independent variables, making the model less reliable [23]. The origins of multicollinearity are generally attributed to data collection, physical motives, outliers, an over-defined model, and the specification of a model [24]. Therefore, the present study utilized a penalized regression known as Least absolute shrinkage and selection operator (LASSO) regression. In the presence of multicollinearity, LASSO regressions had been previously utilized to overpower collinearity. It employs penalization procedures to shrink regression estimates completely to zero (0) and automatically excludes one of the variables from the model, as illustrated in research executed in different fields [25-27]. The algorithm and the equation representing LASSO regression had been discussed elsewhere [28,29]. In our study, we utilized the optimum search for the penalty value in the regression models. RStudio 2021.09.0 Build 3.5.1 software was utilized to conduct the regression analysis.
3. Results
3.1. Joinpoint regression findings
The trends representing the incidence of lower respiratory infections (LRI), upper respiratory infections (URI), and nutritional deficiency (ND) in Chadian under-5 female and male children between 1990 to 2019 are presented in figures 1 to 3.
According to Figure 1, which displays the trend of LRI incidence in both genders, declining patterns could be observed in different trends describing each age group and the overall age category in the two genders, especially after 2000. Between 1990 and 2019, the lowest patterns were associated with females and males aged between 0 to 6 days (early neonates), and the highest was observed in those aged between 1 and 4 years. There is a similarity between the trends in the female gender and those in the male gender.
Figure 2 is the representation of the trends from URI incidence. In both females and males from different age groups, upward and downward patterns were present in the trends. An increasing phase could be noticed between 1990 and 2005, followed by a downstream segment between 2006 and 2019. Compared with the rest of the age groups, the lowest trends of URI were associated with males and females aged between 1 and 4 years. Females and males aged between 28 and 364 (post-neonates) days and those aged between 0 and 6 days (early neonates) registered the highest patterns relative to different periods. When comparing 1990 with 2019, a seemingly steady level is observed in the trends of URI in under-5 female and male children from Chad.
Based on the representation of ND incidence between 1990 and 2019, Figure 3 shows an upward and downward behaviors in the trends representing different age groups, except for the trend in males aged between 1 and 4 years that displayed an almost steady pattern. In the rest of the age groups from both genders, upward and downward behaviors were present in different trends. The lowest rates of ND incidence were identified in males and females aged between 1 and 4 years.
Table 2 displays the outcomes from Joinpoint regression. According to the average annual percent of change (AAPC) estimates, the incidence of LRI decreased significantly across different age groups in males and females. In children aged between 0 and 6 days (early neonates), 7-27 days (late neonates), and 28-364 days (post neonates), LRI incidence declined more in the age groups from the female gender in comparison to those of the male gender. Regarding infants aged between 1 and 4 years, LRI decreased equally in females and males between 1990 and 2019. Based on the study findings, the incidence of URI did not decrease in any age group in both genders from 1990 to 2019. The incidence of ND decreased in all the age groups in both females and males from 1990 to 2019. In both genders, the decline of ND incidence in early neonates and children of 1-4 years are the most and least, in contrast to the rest of the age groups during the same study period. In all age groups, the incidence of ND declined mostly in the male gender age groups compared with the female gender.
When looking at the values relative to the overall (under-5 children) in both genders, LRI incidence declined more in the female gender in contrast to the male gender. Oppositely, the overall ND incidence decreased more in the male gender than the female.
Figure 1.
Trends of lower respiratory infections (LRI) incidence in Chadian female and male under-5 children between 1990 and 2019.
Figure 1.
Trends of lower respiratory infections (LRI) incidence in Chadian female and male under-5 children between 1990 and 2019.
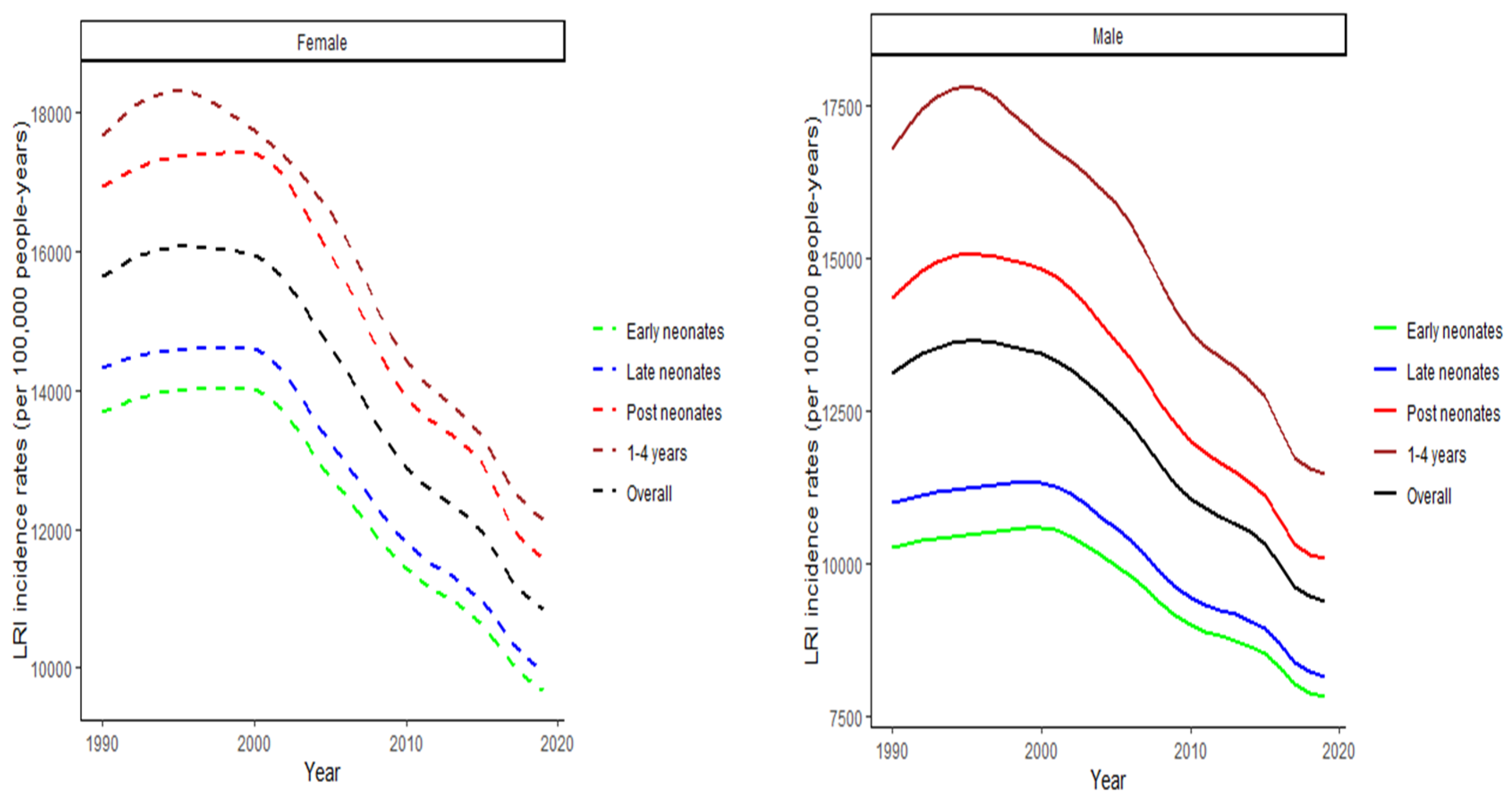
Figure 2.
Trends of upper respiratory infections (URI) incidence in Chadian female and male under-5 children between 1990 and 2019.
Figure 2.
Trends of upper respiratory infections (URI) incidence in Chadian female and male under-5 children between 1990 and 2019.
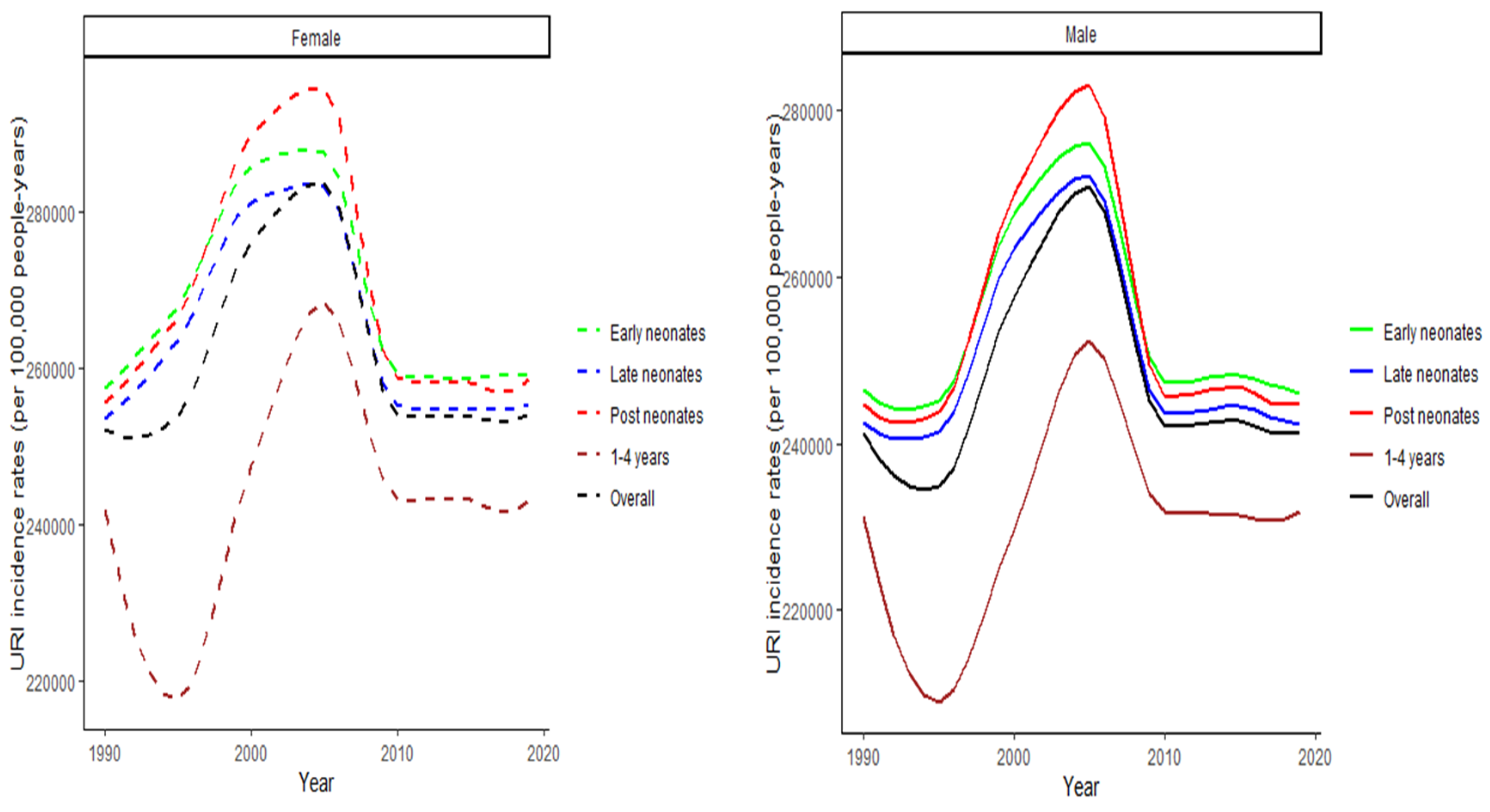
Figure 3.
Trends of nutritional deficiency (ND) incidence in under-5 Chadian female and male children between 1990 and 2019.
Figure 3.
Trends of nutritional deficiency (ND) incidence in under-5 Chadian female and male children between 1990 and 2019.
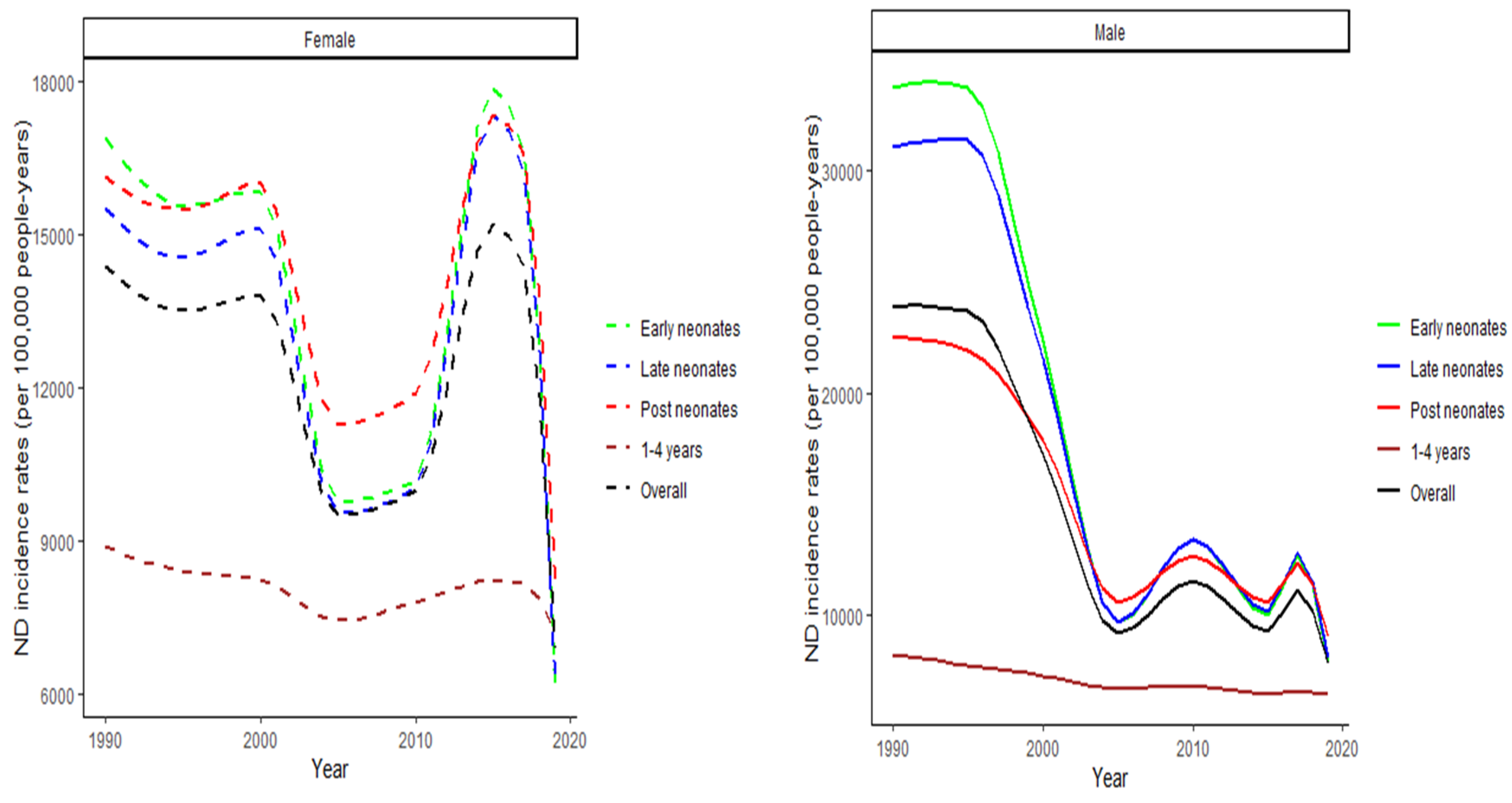

Table 2.
Average annual percent of change (AAPC) values.
| LRI | URI | ND | ||
| Variables | Period | AAPC (95% CI) | AAPC (95% CI) | AAPC (95% CI) |
| Female | ||||
| Early neonates (0-6 days) | 1990-2019 | -1.2* (-1.3, -1.1) | 0.0 (0.0, 0.1) | -3.1* (-3.8, -2.3) |
| Late neonates (7-27 days) | 1990-2019 | -1.3* (-1.3, -1.2) | 0.0 (0.0, 0.1) | -2.8* (-3.5, -2.0) |
| Post neonates (28-364 days) | 1990-2019 | -1.3* ( -1.5, -1.2) | 0.0 (-0.1, 0.1) | -2.1* (-2.7, -1.5) |
| 1-4 years | 1990-2019 | -1.3* ( -1.4, -1.2) | 0.0 (-0.1, 0.1) | -0.7* (-0.8, -0.6) |
| Overall | 1990-2019 | -1.3* (-1.4, -1.2) | 0.0 (-0.0, 0.1) | -2.2* (-2.9, -1.6) |
| Male | ||||
| Early neonates (0-6 days) | 1990-2019 | -1.0* (-1.0, -0.9) | 0.0 (-0.1, 0.1) | -4.9* (-6.1, -3.6) |
| Late neonates (7-27 days) | 1990-2019 | -1.0* (-1.1, -1.0) | 0.0 (-0.1, 0.1) | -4.5* (-5.7, -3.3) |
| Post neonates (28-364 days) | 1990-2019 | -1.2* (-1.4, -1.1) | 0.0 (-0.1, 0.2) | -3.1* (-3.8, -2.4) |
| 1-4 years | 1990-2019 | -1.3* (-1.5, -1.2) | 0.0 (-0.1, 0.1) | -0.9* (-0.9, -0.8) |
| Overall | 1990-2019 | -1.2* (-1.4, -1.0) | 0.0 (-0.1, 0.2) | -3.8* (-4.7, -2.8) |
**, statistically significant values at alpha=0.05; CI, confidence interval; LRI, lower respiratory infections; URI, upper respiratory infections; ND, nutritional deficiency.
3.1. LASSO regression outcomes
The Least absolute shrinkage and selection operator (LASSO) regression yielded the following outcomes. The different degrees of the association of the maternal health and environmental factors and the incidence of the under-5 children’s medical conditions (LRI, URI and ND) represented by the R-square values indicated the presence of a strong association estimated over 90 percent (90%). The mean square error (MSE) of each model were alternatively low.
In the female gender, β1 represent the prevalence of GD meanwhile β2 and β4 indicating the prevalence of HIV/AIDS and TB showed positive estimates (positif effect) across the incidence of LRI, URI and ND in all the age groups of Chadian under-5 children. β3 that stands for the prevalence of MD and β6 that illustrates the prevalence of malaria have negative values (negative impact) regarding the incidence of ND in the different age groups. The prevalence of HCE represented by β9 is associated to positive values in the incidence of URI and ND in Chadian under-5 children. β3 and β8 displayed negative values concerning the incidence of URI and ND across all the different age groups.
When observing the values of the β estimates in the male gender, only β4 had positive impact throughout the incidence of LRI, URI and ND in different composed age groups. β3 and β6 showed negative values in the incidence of ND meanwhile β9 presented negative estimates during the incidence of LRI. Although the values of β1 and β5 were randomly positive and negative in the incidence of LRI, they were homogeneously negative in the incidence of URI and positive for the incidence of ND in all the age groups. β2 and β7 were only negative in the incidence of URI. β8 values were all negative for the incidence of URI and ND in all the male age groups.
Table 3.
LASSO regression estimates.
| Variables | β1 | β2 | β3 | β4 | β5 | β6 | β7 | β8 | β9 | R2 (%) | MSE |
| Female | |||||||||||
| LRI | |||||||||||
| Early neonates | -0.01 | 0.14 | 0.29 | 0.60 | N/A | N/A | 0.10 | N/A | -0.01 | 99.90 | 0.006 |
| Late neonates | -0.01 | 0.14 | 0.34 | 0.57 | N/A | N/A | 0.09 | N/A | -0.00 | 99.90 | 0.007 |
| Post neonates | -0.08 | 0.07 | 0.43 | 0.53 | N/A | N/A | 0.01 | N/A | -0.04 | 99.90 | 0.006 |
| 1-4 years | -0.07 | 0.24 | 0.52 | 0.10 | N/A | 0.09 | N/A | -0.07 | 99.91 | 0.006 | |
| Overall | -0.08 | 0.02 | 0.24 | 0.62 | N/A | N/A | 0.11 | N/A | -0.06 | 99.91 | 0.005 |
| URI | |||||||||||
| Early neonates | -0.92 | 0.06 | 0.17 | 0.51 | -0.54 | 0.33 | N/A | -0.29 | 0.23 | 99.90 | 0.007 |
| Late neonates | -0.92 | 0.05 | 0.19 | 0.49 | -0.54 | 0.33 | -0.01 | -0.29 | 0.22 | 99.90 | 0.007 |
| Post neonates | -0.89 | N/A | 0.26 | 0.32 | -0.61 | 0.48 | -0.05 | -0.32 | 0.17 | 99.87 | 0.008 |
| 1-4 years | -0.44 | N/A | 0.09 | 0.16 | -1.33 | 1.13 | -0.39 | -.058 | 0.37 | 99.49 | 0.036 |
| Overall | -0.88 | N/A | 0.11 | 0.42 | -0.87 | 0.67 | -0.08 | -0.42 | 0.26 | 99.84 | 0.011 |
| ND | |||||||||||
| Early neonates | -1.30 | 0.14 | -1.83 | 2.80 | -0.70 | -1.64 | 0.22 | -1.71 | 0.57 | 99.05 | 0.068 |
| Late neonates | -1.33 | 0.21 | -1.55 | 2.73 | -0.65 | -1.77 | 0.00 | -1.69 | 0.60 | 98.93 | 0.077 |
| Post neonates | -1.42 | 0.16 | -1.97 | 3.35 | -0.62 | -1.95 | 0.01 | -1.65 | 0.68 | 99.05 | 0.068 |
| 1-4 years | -0.28 | 0.25 | -0.69 | 1.98 | -0.17 | -1.29 | N/A | -0.72 | 0.43 | 99.71 | 0.020 |
| Overall | -1.29 | 0.18 | -1.57 | 2.83 | -0.61 | -1.78 | 0.01 | -1.61 | 0.60 | 99.04 | 0.069 |
(a) N/A, not applicable; LRI, lower respiratory infection; URI, upper respiratory infection; ND, nutritional deficiency; MSE, mean square error. (b)
| Variables | β1 | β2 | β3 | β4 | β5 | β6 | β7 | β8 | β9 | R2 (%) | MSE |
| Male | |||||||||||
| LRI | |||||||||||
| Early neonates | -0.10 | 0.05 | 0.34 | 0.64 | -0.02 | N/A | N/A | N/A | -0.06 | 99.91 | 0.006 |
| Late neonates | -0.08 | 0.08 | 0.40 | 0.57 | N/A | N/A | N/A | N/A | -0.04 | 99.90 | 0.006 |
| Post neonates | -0.08 | N/A | 0.07 | 0.68 | 0.00 | 0.00 | 0.19 | N/A | -0.10 | 99.90 | 0.006 |
| 1-4 years | 0.04 | N/A | 0.26 | N/A | 0.08 | 0.26 | 0.38 | N/A | -0.22 | 99.82 | 0.011 |
| Overall | -0.08 | 0.02 | 0.24 | 0.62 | N/A | N/A | 0.11 | N/A | -0.06 | 99.91 | 0.005 |
| URI | |||||||||||
| Early neonates | -1.09 | -0.17 | 0.14 | 0.72 | -0.93 | 0.50 | -0.33 | -0.47 | 0.30 | 99.77 | 0.016 |
| Late neonates | -1.08 | -0.17 | 0.16 | 0.70 | -0.93 | 0.51 | -0.33 | -0.47 | 0.30 | 99.77 | 0.020 |
| Post neonates | -0.92 | -0.04 | 0.24 | 0.27 | -0.90 | 0.74 | -0.24 | -0.55 | 0.27 | 99.71 | 0.020 |
| 1-4 years | -0.47 | -0.11 | 0.34 | N/A | -1.04 | 1.00 | -0.73 | -0.51 | 0.39 | 99.49 | 0.036 |
| Overall | -0.90 | -0.09 | 0.23 | 0.37 | -1.03 | 0.79 | -0.39 | -0.56 | 0.33 | 99.68 | 0.022 |
| ND | |||||||||||
| Early neonates | 0.41 | 0.37 | -0.16 | 0.32 | 0.49 | -0.32 | 0.55 | 0.00 | 0.11 | 99.73 | 0.018 |
| Late neonates | 0.43 | 0.43 | -0.39 | 0.47 | 0.45 | -0.31 | 0.65 | -0.04 | 0.15 | 99.73 | 0.019 |
| Post neonates | 0.18 | 0.26 | -0.76 | 1.21 | 0.30 | -0.51 | 0.64 | -0.04 | 0.23 | 99.76 | 0.016 |
| 1-4 years | 0.31 | N/A | N/A | 0.28 | 0.11 | N/A | 0.53 | N/A | N/A | 99.69 | 0.022 |
| Overall | 0.37 | 0.18 | -1.57 | 2.83 | -0.61 | -1.78 | 0.01 | -1.61 | 0.60 | 99.04 | 0.069 |
4. Discussion
In this study, the trends from the incidence of upper and lower respiratory infections, and nutritional deficiency in Chadian female and male under-5 children between the period of 1990 and 2019 were assessed in this study using Joinpoint regression. Furthermore, the research used the least absolute shrinkage and selection operator (LASSO) regression to evaluate the degree of the associations between the incidence of those medical conditions in Chadian under-5 female and male children with numerous maternal health and environmental factors.
Between 1990 and 2019, downward patterns could be noticed in the trends representing the incidence of lower respiratory infections (LRI) and nutritional deficiency (ND), and steady trends were observed in the temporal representation of the upper respiratory infection (URI) incidence in different age groups of under-5 Chadian children, as displayed in figures 1 to 3. This unequal behavior of the different trends was evaluated using a Joinpoint regression.
According to Joinpoint regression analysis findings, LRI incidence decreased more in the female children aged between 0 and 364 days (early neonates, late neonates, and post neonates). In children aged between 1 and 4 years, LRI decreased equally in females and males during the same period, as presented in Table 2. The outcome of the regression analysis presented in the same table (table 2) also demonstrated that the incidence of URI did not decline in any of the age groups in both genders between 1990 and 2019. Oppositely, the incidence of ND declined in all age groups in both females and males. In the two genders, the decline of ND incidence in children aged 0 to 6 days and 1 to 4 years are alternatively the highest and least in contrast to other age groups. Furthermore, the incidence of ND declined mostly in the male gender across all the age groups. The government of Chad and different stakeholders designed numerous strategies [30-32]. They employed different policies towards ameliorating the health status of under-5 children, the life conditions of the population, and the healthcare system as described previously in previous studies [30-32]. Therefore, all the declining patterns in different trends and age groups might be associated with the existing efforts realized in these few decades. However, the efforts might not impact all conditions, which could interpret the steady behavior observed in the patterns of URI incidence in the different age group from both genders. Extra efforts and commitments should be established by addressing more efficient policies to improve lifestyle and healthcare conditions for Chadian under-5 children in consequence. As identified in our study, the different behaviors in the trends of respiratory system infections and nutritional deficiency were demonstrated in existing studies [5, 33]. Furthermore, many factors, such as socioeconomic and demographic factors, were demonstrated to be associated with URI burden in LMICs, as presented in previous research [34,35]. Thus, the steady trends of URI incidence in different age groups of Chadian under-5 children might be resulting from poverty, lifestyle, occupational and environmental conditions (biomass fuel, tobacco smoking, sulfur, and nitrogen dioxide, dust), as well as the pediatric population and specialized pediatricians [7,34,35]. Moreover, the lack of sanitation, mercury, inadequate local waste disposal, dirty floors, and access to safe water sources was described to have a relationship with nutrition in childhood at varying levels [35]. A necessity for an amelioration of environmental and lifestyle factors and a more efficient national nutritional program might significantly contribute to considerably decline the burden of numerous diseases in under-5 children, as nutrition plays an important role in healthcare [35].
The degree of the association between the incidence of LRI, URI and ND in Chadian under-5 children, and maternal health and environmental conditions as risk factors was investigated in this study using least absolute shrinkage and selection operator (LASSO) regression. The regression estimates demonstrated a strong association of over 90 percent (90%). Beside this strong association, the beta coefficients (β) that represent the degree on the impact from each independent variable (maternal health and environmental factors) on the incidence of LRI, URI, and ND separately demonstrated that the prevalence of tuberculosis (TB) had a positive impact in the association in both female and male under-5 children. Furthermore, the impact of the prevalence of HIV/AIDS was positive in all female age groups. As for the rest of the maternal health and environmental conditions defined as risk factors, they were randomly impacting positively or negatively the incidence of LRI, URI and ND in Chadian under-5 children. Previous studies have identified the relationship between maternal and under-5 children’s medical conditions [11-14]. For example, a study conducted in 2017 described the effect of maternal malnutrition and its consequences on child growth in Pakistan [36]. Maternal heat and cold exposure, excessive alcohol, hepatitis B (HB), malaria and the burden of maternal HIV/AIDS and tuberculosis (TB) on under-5 children had been described as risk factors that deteriorate under-5 children health [11-14,36-40]. Thus, negatively impacting the accomplishment of the sustainable development goals regarding the health growth and the decline of under-5 mortality in the world by 2030. Strong strategies, laws and public health policies should be systematically established and rigorously followed by the country’s government and international partners to ameliorate maternal health and lifestyle conditions, and healthcare structures and services for a safer and healthier development of under-5 infants across the country.
There were some limitations in the present research. First, the study did not analyze the overall under-5 children for both genders together, but it did take into consideration the overall separately relative to the two genders. The second limitation is relative to the employment of LASSO regression which is an algorithm designed for large-scale data but used in the current study to overcome multicollinearity with datasets of 30 points and 9 independent variables. Therefore, future studies with a larger number of variables will be conducted to support our findings.
5. Conclusion
The incidence of LRI and ND declined in Chadian under-5 children, although the incidence of URI remained steady from 1990 to 2019. The present study also revealed a strong association between maternal health and environmental risk factors and the incidence of respiratory infections and nutritional deficiency in under-5 children. With such statistics that are not in favor to the accomplishment of the sustainable development goals (SDGs) regarding under-5 children’s health and life, the Chadian government and international organizations should reinforce and establish strategies and policies that should directly aim at improving maternal health, environmental and lifestyle.
Author Contributions
“Conceptualization, N.T.M., N.N.N.; methodology, N.T.M., N.N.N., I.A.K., L.M., A.G., S.K., O.A.M.; software, N.T.M.; validation, N.T.M., N.N.N.; formal analysis, N.T.M.; investigation, N.T.M., N.N.N., I.A.K., L.M., A.G., S.K., O.A.M.; resources, N.T.M., N.N.N., I.A.K., L.M., A.G., S.K., O.A.M.; data curation, N.T.M., N.N.N.; writing—original draft preparation, N.T.M., N.N.N.; writing—review and editing, N.T.M., N.N.N.; visualization, N.T.M.; supervision, N.T.M., N.N.N., I.A.K., L.M., A.G., S.K., O.A.M.; project administration, N.T.M., N.N.N., I.A.K., L.M., A.G., S.K., O.A.M. All authors have read and agreed to the published version of the manuscript.”
Funding
Please add: “This research received no external funding.”
Institutional Review Board Statement
“Not applicable.”
Informed Consent Statement
“Not applicable.”
Data Availability Statement
The datasets analyzed in the current study are available in the Global Burden of Diseases repository under results tools from the Global Health Data Exchange, Available from http://ghdx.healthdata.org/gbd-results-tool. [16]
Acknowledgments
“We thank the Global Burden of Diseases (GBD) for making the data available for this study.”
Conflicts of Interest
“The authors declare no conflicts of interest.”
Abbreviations
| AAPC | average annual percent change |
| AUD | alcohol usage disorders |
| APC | annual percentage of change |
| CI | confidence interval |
| GBD | global burden of disease |
| GD | gynecological diseases |
| GHDx | global health data exchange |
| HB | hepatitis B |
| HCE | heat and cold exposure |
| HIV/AIDS | human immunodeficiency virus/acquired immunodeficiency syndrome |
| IHME | institute of health metrics and evaluation |
| LASSO | least absolute shrinkage and selection operator |
| LMIC | low- and middle-income countries |
| LRI | lower respiratory infections |
| M | malaria |
| MD | maternal disorders |
| N/A | not applicable |
| ND | nutritional deficiency |
| SDGs | sustainable development goals |
| TB | tuberculosis infection |
| URI | upper respiratory infections |
| USA | united states of America |
| VIF | variance inflation factors |
| WB | world bank |
References
- Dasaraju PV, Liu C. Infections of the Respiratory System. In: Baron S, editor. Medical Microbiology. 4th edition. Galveston (TX): University of Texas Medical Branch at Galveston; 1996. Chapter 93.
- Lewandowicz-Uszyńska A, Pasternak G, Pentoś K. Immunoglobulin G deficiency in children with recurrent respiratory infections with and without history of allergy. Adv Exp Med Biol. 2021;1289:63–70. [CrossRef]
- Pasternak G, Lewandowicz-Uszyńska A, Pentoś K. Disorders of humoral immunity in children with IgG subclass deficiency and recurrent respiratory infections. Adv Exp Med Biol. (2018) 1108:99–106. [CrossRef]
- Kiani AK, Dhuli K, Donato K, Aquilanti B, Velluti V, Matera G, Iaconelli A, Connelly ST, Bellinato F, Gisondi P, Bertelli M. Main nutritional deficiencies. J Prev Med Hyg 2022;63(suppl.3):E93-E101. [CrossRef]
- Yue, T., Zhang, Q., Li, G., & Qin, H. (2022). Global Burden of Nutritional Deficiencies among Children under 5 Years of Age from 2010 to 2019. Nutrients, 14(13), 2685. [CrossRef]
- Tazinya, A.A., Halle-Ekane, G.E., Mbuagbaw, L.T. et al. Risk factors for acute respiratory infections in children under five years attending the Bamenda Regional Hospital in Cameroon. BMC Pulm Med 18, 7 (2018). [CrossRef]
- Ahinkorah, B.O., Seidu, AA., Budu, E. et al. Proximate, intermediate, and distal predictors of under-five mortality in Chad: analysis of the 2014–15 Chad demographic and health survey data. BMC Public Health 20, 1873 (2020). [CrossRef]
- World Bank. New World Bank country classifications by income level: 2022-2023. (2022). Retrieved in May 2023 from https://blogs.worldbank.org/opendata/new-world-bank-country-classifications-income-level-2022-2023.
- Save the Children, United Nations Children’s Fund (UNICEF), Chaque Souffle compte. A bout de souffle au Tchad. (2020) (Accessed in May 2023) from https://stoppneumonia.org/wp-content/uploads/2020/06/CHAD-FRENCH-2020.pdf.
- Nations Unies. Organization des Nations Unies (ONU) Info. Le taux de malnutrition des enfants alarmant dans l’ouest du Tchad. (2008). Retrieved in May 2023 from https://news.un.org/fr/story/2008/11/143522#:~:text=L'OCHA%20se%20fonde%20sur,sur%2010.000%20meurent%20de%20malnutrition (Accessed May 2023).
- Warr, A. J., Pintye, J., Kinuthia, J., Drake, A. L., Unger, J. A., McClelland, R. S., Matemo, D., Osborn, L., & John-Stewart, G. (2019). Sexually transmitted infections during pregnancy and subsequent risk of stillbirth and infant mortality in Kenya: a prospective study. Sexually transmitted infections, 95(1), 60–66. [CrossRef]
- Arunda, M. O., Choudhry, V., Ekman, B., & Asamoah, B. O. (2016). Under-five mortality and maternal HIV status in Tanzania: analysis of trends between 2003 and 2012 using AIDS Indicator Survey data. Global health action, 9, 31676. [CrossRef]
- Yaya, S., Bishwajit, G., Okonofua, F., & Uthman, O. A. (2018). Under five mortality patterns and associated maternal risk factors in sub-Saharan Africa: A multi-country analysis. PloS one, 13(10), e0205977. [CrossRef]
- Marais B. J. (2011). Impact of tuberculosis on maternal and child health. The Journal of infectious diseases, 203(3), 304–305. [CrossRef]
- United Nations Economic Commission for Europe (UNECE). Indicator 3.2. 1 (b). Under-five mortality rate, deaths per 1,000 live births. Retrieved in May 2023 from https://w3.unece.org/SDG/en/Indicator?id=91.
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) Results; Institute for Health Metrics and Evaluation (IHME): Seattle, WA, USA, 2020; Available online: Retrieved in April 2023 from http://ghdx.healthdata.org/gbd-results-tool.
- Terán JM, Sánchez-García E, Martínez-Carrión JM, Bogin B, Varea C. Use of Joinpoint regressions to evaluate changes over time in conscript height. Official Journal of the Human Biology Council. 2022, 34(1), e23572. [CrossRef]
- Zhang, Y., Liu, J., Han, X., Jiang, H., Zhang, L., Hu, J., Shi, L., & Li, J. (2022). Long-term trends in the burden of inflammatory bowel disease in China over three decades: A joinpoint regression and age-period-cohort analysis based on GBD 2019. Frontiers in public health, 10, 994619. [CrossRef]
- Zhu, B., Wang, Y., Zhou, W., Jin, S., Shen, Z., Zhang, H., Zhang, X., Ding, X., & Li, Y. (2022). Trend dynamics of gout prevalence among the Chinese population, 1990-2019: A joinpoint and age-period-cohort analysis. Frontiers in public health, 10, 1008598. [CrossRef]
- Qiu, H., Cao, S., & Xu, R. (2021). Cancer incidence, mortality, and burden in China: a time-trend analysis and comparison with the United States and United Kingdom based on the global epidemiological data released in 2020. Cancer communications (London, England), 41(10), 1037–1048. [CrossRef]
- Liu, X., Yu, C., Bi, Y., & Zhang, Z. J. (2019). Trends and age-period-cohort effect on incidence and mortality of prostate cancer from 1990 to 2017 in China. Public health, 172, 70–80. [CrossRef]
- Shrestha N. Detecting Multicollinearity in Regression Analysis. American Journal of Applied Mathematics and Statistics, 2020.
- Daoud JI. Multicollinearity and Regression Analysis. Journal of Physics: Conference Series. 2018, 949(1). [CrossRef]
- Murray L, Nguyen H, Lee YF, Remmenga MD, Smith DW. (2012). Variance Inflation Factors in Regression Models with Dummy Variables. Conference on Applied Statistics in Agriculture, 2012 (pp. 1-18).
- Cule E, Vineis P, De Iorio M. Significance testing in ridge regression for genetic data. BMC Bioinformatics. 2011, 12, 372. [CrossRef]
- Gelman A. Scaling regression inputs by dividing by two standard deviations. Statistics in Medicine. 2008, 27(15), 2865–2873. [CrossRef]
- Weaving D, Jones B, Ireton M, Whitehead S, Till K, Beggs CB. Overcoming the problem of multicollinearity in sports performance data: A novel application of partial least squares correlation analysis. PloS One. 2019, 14(2), e0211776.
- van Egmond MB, Spini G, van der Galien O, IJpma A, Veugen T, Kraaij W, Sangers A, Rooijakkers T, Langenkamp P, Kamphorst B, van de L'Isle N, Kooij-Janic M. Privacy-preserving dataset combination and Lasso regression for healthcare predictions. BMC Medical Informatics and Decision Making. 2021, 21(1), 266. [CrossRef]
- Tibshirani R. Regression Shrinkage and Selection via the Lasso. Journal of the Royal Statistical Society: Series B (Methodological). 1996, 58, 267-288. [CrossRef]
- United Nations Children’s Fund (UNICEF). UNICEF Chad Humanitarian Situation Report No. 3 for 1 July to September 2022. (2022). Retrieved in June 2023 from https://reliefweb.int/report/chad/unicef-chad-humanitarian-situation-report-no-3-1-july-30-september-2022?gclid=Cj0KCQjwkqSlBhDaARIsAFJANkhoafrw0kO7wZMOsjr2mx0dk2YvUPgc0LiqlH-eh_AwCgjX1D13rPYaApoVEALw_wcB.
- D. Manoufi, W.C. Kabore, C.N. Yahannon, A. Dumont, V. Ridde, Amélioration de l’offre et de la demande de soins de santé maternelle et infantile au Tchad : une étude quasi-expérimentale, Revue d'Épidémiologie et de Santé Publique, Volume 69, Issue 4, 2021,Pages 193-203, ISSN 0398-7620. [CrossRef]
- Simen-Kapeu, A., Bogler, L., Weber, A. C., Ntambi, J., Zagre, N. M., Vollmer, S., & Ekpini, R. E. (2021). Prevalence of diarrhoea, acute respiratory infections, and malaria over time (1995-2017): A regional analysis of 23 countries in West and Central Africa. Journal of global health, 11, 13008. [CrossRef]
- Hammond, A., Halliday, A., Thornton, H. V., & Hay, A. D. (2021). Predisposing factors to acquisition of acute respiratory tract infections in the community: a systematic review and meta-analysis. BMC infectious diseases, 21(1), 1254. [CrossRef]
- Cortes-Ramirez, J., Wilches-Vega, J.D., Paris-Pineda, O.M., Ayurzana, L., & Sly, P.D. (2021). Environmental risk factors associated with respiratory diseases in children with socioeconomic disadvantage. Heliyon, 7(4), e06820. [CrossRef]
- Vilcins, D., Sly, P.D., & Jagals, P. (2018). Environmental risk factors associated with child stunting: A systematic Review of the literature. Annals of Global Health, 84(4), 551-562. [CrossRef]
- Khalid N, Aslam Z, Kausar F, Irshad H, Anwer P (2017) Maternal Malnutrition and Its Kick on Child Growth: An Alarming Trim for Pakistan. J Food Nutr Popul Health Vol.1 No.3:24.
- Kim, S., Choe, SA. & Cho, SI. Harmful alcohol use among mothers of under-five child: findings from the Panel Study on Korean Children. BMC Women's Health 21, 159 (2021). [CrossRef]
- Colleen O’Leary, David Lawrence, Katherine Hafekost, Stephen R. Zubrick, Carol Bower; Maternal Alcohol-Use Disorder and Child Outcomes. Pediatrics March 2020; 145 (3): e20191574. 10.1542/peds.2019-1574.
- Tse, K. Y., Ho, L. F., & Lao, T. (2005). The impact of maternal HBsAg carrier status on pregnancy outcomes: a case-control study. Journal of hepatology, 43(5), 771–775. [CrossRef]
- Kuehn, L., & McCormick, S. (2017). Heat Exposure and Maternal Health in the Face of Climate Change. International journal of environmental research and public health, 14(8), 853. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



