
Submitted:
24 June 2024
Posted:
24 June 2024
You are already at the latest version
Abstract
Background. Epithelial ovarian cancer (EOC) is the deadliest gynecological malignancy worldwide. Brain metastasis (BM) is quite an uncommon presentation. However, the likelihood of central nervous system (CNS) metastasization should be considered in the context of disseminated disease. The therapeutic management of BMs is an unmet clinical need, to date. Case presentation. We identified across different Cancer Centers six cases of both BRCA wild-type and BRCA-mutated EOC spreading to the CNS. They presented either with a single brain lesion or with multiple lesions and most of them had intracranial-only disease. All cases received Poly-ADP ribose polymerase inhibitor (PARPi) maintenance, as by clinical practice, for a long time within a multimodal treatment approach. We also provide an insight into the available body of work regarding the management of this intriguing disease setting, with a glimpse of future therapeutic challenges. Conclusion. Despite the lack of unanimous guidelines, multimodal care pathways should be encouraged for optimal disease control of this unfortunate patient’s subset. Albeit not being directly investigated in BM patients, the PARPi maintenance is deemed to have a valuable role in this setting. Prospective research, aimed to implement worthwhile strategies in the multimodal patient journey of BMs from EOC, is eagerly awaited.
Keywords:
epithelial ovarian cancer
; brain metastases
; PARP inhibitors
; multimodal patient journey.
1. Introduction
1.1. Clinical Presentation of BMs from EOC
EOC, also referred to as “silent killer” or “whispering disease” [1], harbors the highest disease burden and mortality among gynecologic malignancies, due to earlier relapse despite optimal chemosensitivity [1,2,3]. Regarding metastatic patterns, the locoregional relapse, caused by intraperitoneal or lymphatic spread, is highly frequent within 3 years from adjuvant platinum-based therapy completion [4]. The abdominal-pelvic metastatic sites are more common than hematogenous distant sites [4]. Among them, CNS is exceedingly rare in EOC, being involved in about 0,3–11% of different series [5]. However, better clinician awareness and latest advances in the anticancer therapies as well as imaging techniques have led to an augmented incidence of unusual CNS metastases [5,6].
Evidence regarding this patient’s subset is still sparse and controversial [7]. BM is an unfavorable event, with a very poor prognosis [7]. CNS spreading in EOC patients is also a late clinical manifestation, with a time to onset of BM significantly longer than that for other recurrent sites. Strikingly, high-grade serous ovarian cancer (HGSOC) was found as the most common histotype related to BM development with a longer time interval despite more aggressive behavior [7,8]. The clinical presentation of BM includes both oligometastatic and polymetastatic lesions [9], although most patients harbor a single metastasis [10]. Most typical clinical complaints are sensory and motor disturbances, cognitive dysfunction, or intracranial hypertension symptoms [7,11]. Historically, EOC, Karnofsky performance status (KPS) >70, single brain metastasis, absence of extracranial disease, cranial surgery, cranial RT, and CHT resulted as independent favorable predictors of overall survival (OS) in multivariate analysis [9]. Recently, younger age, intracranial-only disease, single CNS site and multimodality care were established as good prognostic indicators for longer OS after BM diagnosis [7].
1.2. The Key role of Multimodal Treatment Plan for BMs from EOC
Due to the high disease burden and the heterogeneous uptake of anticancer drugs, an effective treatment of BMs is a serious unmet clinical need in the field of neuro-oncology [5,12]. Collectively, no consensus exists about the optimal treatment strategy for EOC BMs due to their rarity [7]. Only retrospective data supports clinical decision making in this subset [5]. Aggressive multimodality approach is warranted in carefully selected patients who may profit from actual intracranial disease control. The therapeutic mainstay of BM treatment consists of surgical resection, whole-brain radiotherapy (WBRT), chemotherapy (CHT), and, more recently, intensity-modulated RT (IMRT) and stereotactic radiosurgery (SRS), including gamma-knife radiosurgery [5,13]. The new techniques of CNS radiation (IMRT and SRS) should be prioritized for tumor control, due to long-term sequelae of WBRT, unless intracranial disease is widespread [5,14]. In line with this notion, SRS yields more favorable outcomes in terms of OS, neurological impairment and QoL, in highly selected patient cohorts (oligometastases, good disease control, and good KPS) [5]. A good KPS, a single disease site and good tumor accessibility are the main requirements for cranial surgery, also aimed at histological confirmation [5,15]. In the largest single-institution study of EOC BMs, post-operative RT ensured a better intracranial disease control as compared to surgery alone [9]. In lieu of current findings, the highest median OS was reported for BM patients receiving all therapeutic modalities including CHT [10,11].
1.1. Biomarkers of CNS Spread and Potential Therapeutic Targets
Presently, evidence of potential biomarkers of brain spread from EOC is almost based on small-size retrospective studies, while prospective validation is lacking [4,16,17]. The standard platinum-based regimens are the most used due to their ability to cross the blood-brain barrier (BBB) with beneficial effects based on the known platinum sensitivity of EOC. The long-term prognosis is still unsatisfactory [18]. Scant data suggests the possibly predictive role of hormone receptors as well as the multi drug reactivity 1 gene expression as possible biomarkers of BMs development, but further prospective research clarifying this finding is of great interest [4,19].
Both BRCA 1 and BRCA2 tumor suppressor genes play a key role in high-fidelity DNA repair via homologous recombination repair (HRR) pathway. A dysfunctional HRR, which is also referred to as homologous recombination deficiency (HRD) signature, is broadly identified in about half of HGSOC patients [19]. All the genetic/epigenetic defects (not limited to BRCA mutations) included in the HRD signature identify somatic mutational landscapes reflecting the BRCAness phenotype. The HRD signature may serve as a biomarker for platinum and PARPi sensitivity [20] and thus may inform prognosis and treatment decision making of BRCA-like tumors, translating into longer survival time and time to platinum-resistance [21]. Strikingly, the presence of BRCA pathogenic mutation has been currently suggested as a risk factor for brain spread from EOC [4]. BRCA1-2-mutant patients are prone to develop earlier extraperitoneal visceral metastases such as BMs, opposed to the wild-type counterpart [22,23], with a shorter median time to metastasis, a younger age without survival differences by BRCA status [23]. A limited cancer burden was reported in BRCA-related BMs partly due to known platinum sensitivity enabling durable systemic disease control [16]. To date, the functional role of BRCA deficiency in EOC brain metastasization remains unexplained [24 Ratner]. Likewise, the evidence suggesting HRD as a likely risk factor for BM [15] may explain the similar survival trend in both the BRCA wild-type and BRCA-mutant subgroups [5]. In BRCA-wild type cases, the presence of at least one mutation in alternative HRD genes acts as a risk factor for BM development thus supporting the PARPi use in this population with BMs [5].
Therefore, the data supporting the implication of BRCA and HRD signature in EOC spreading to the brain, while inconclusive, are noteworthy. The first NGS study exploring the set of actionable somatic mutations in metastatic EOC found a high number of BRCA 1/2-mutations beside other HRR defects in all sequenced BM samples [24]. These findings strongly suggest that pharmacological PARP inhibition could be an attractive targeted therapeutic for patients with BMs [24]. To date, the PARPi maintenance is thought to have a valuable role in the management of this patient's subset [5]. Given the paucity of EOC patients affected by BMs, no unanimous guidelines are yet in sight [7], thereby the therapeutic algorithm in this setting needs to be clarified [15].
Herein, we present a multi-institutional case study research highlighting the clinical outcomes of EOC patients with intracranial disease, who received PARPi maintenance during their therapeutic journey (as summarized in the Table 1, below).
2. Case Presentation
2.1. Case One
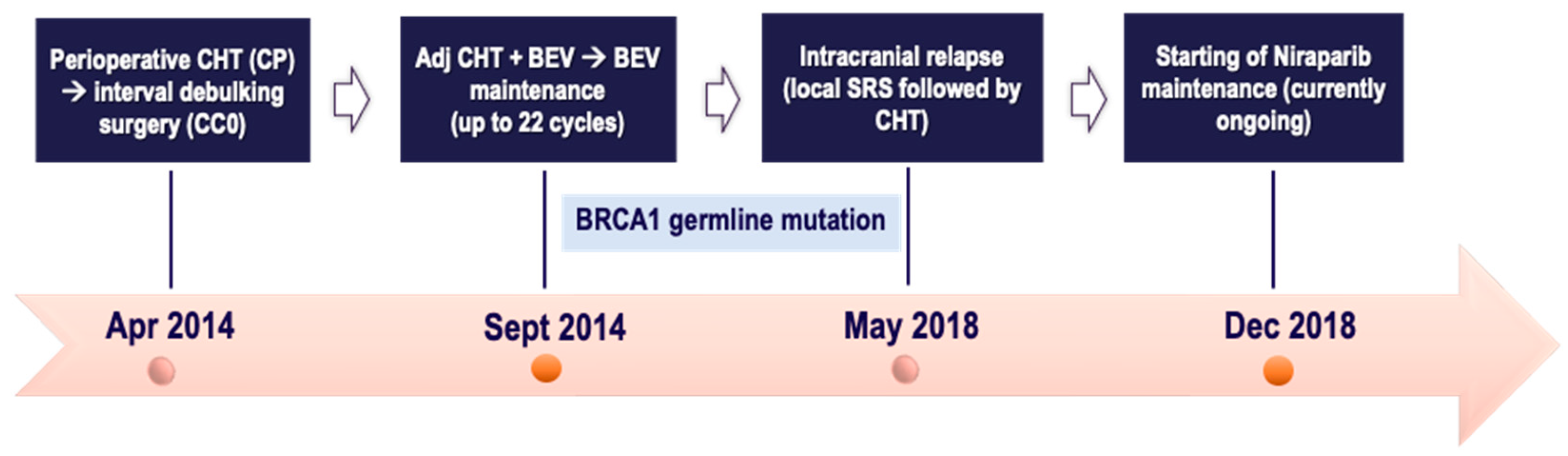
A 53-year-old postmenopausal female with an unremarkable personal medical history was diagnosed in September 2019 with advanced ovarian cancer with widespread peritoneal carcinomatosis along with bilateral pleural effusion. After diagnostic and staging laparoscopy, she underwent primary debulking surgery with optimal cytoreduction with FIGO IIIC Surgical Staging of HGSOC on histopathological exam. The baseline CA125 was 1133 U/ml. Followingly, from November 2019 to March 2020 she was offered frontline 3-weekly Carboplatin plus Paclitaxel plus Bevacizumab (6 cycles) followed by 3-weekly Bevacizumab maintenance monotherapy for up to 22 cycles. During the maintenance phase, the BRCA germline testing reported pathogenic BRCA1 deleterious mutation.
In October 2021 the patient experienced limited intracranial relapse with a single cerebellar nodule, in absence of clinical complaints. A concomitant rising of CA125 (183 U/mL) occurred. Hence, after multidisciplinary agreement, she was deemed suitable for suboccipital craniotomy with radical resection of the lesion; pathology highlighted “brain metastases from HGSOC”. Postoperatively, CA125 was normalized (18 U/ml). In December 2021 the restaging CT scan revealed an enlarged paraaortic lymph node (minimum axis of 15 mm) without other distant sites; thus, second-line treatment with carboplatin plus Pegylated liposomal doxorubicin (PLD) doublet was delivered for 6 courses, followed by complete radiological response of the target lymphadenopathy. Contemporarily, the findings on follow-up brain MRI were more suggestive for a likely residue at the surgical bed as compared to a local relapse.
Due to the diagnostic challenge of brain metastasis concomitantly with extracranial remission, after CHT completion, in June 2022 local SRS targeting all the posterior cranial fossa to a dose of 30 Gy in 10 fractions was performed. Due to intracranial-only tumor burden, despite BRCA mutation, the multidisciplinary tumor board (MTB) at the Referral Institute deemed the patient candidate for Niraparib maintenance monotherapy, which started in August 2022 and is currently ongoing. Over the time, reassessment brain MRI have shown no signs of intracranial relapse. No dose-limiting toxicity has been reported, at present. The CA125 marker has remained within the normal range.
Figure 1.
Timeline of patient treatment journey in case one. Abbreviations. CC0: completeness of cytoreduction score 0. CHT: chemotherapy. CP: Carboplatin plus Paclitaxel. BEV: Bevacizumab. SRS: stereotactic radiosurgery.
Figure 1.
Timeline of patient treatment journey in case one. Abbreviations. CC0: completeness of cytoreduction score 0. CHT: chemotherapy. CP: Carboplatin plus Paclitaxel. BEV: Bevacizumab. SRS: stereotactic radiosurgery.

2.2. Case Two
A 52-year-old postmenopausal female with an unremarkable family history was diagnosed in April 2014 with advanced EOC (diagnostic laparoscopy). At the Referral Institute, due to disease burden, she underwent perioperative chemotherapy with 3-weekly Carboplatin plus Paclitaxel regimen (three courses) followed by interval debulking surgery in July 2014, with optimal cytoreduction (no gross residual disease). Pathology confirmed FIGO IIIC HGSOC. In the adjuvant phase, from September 2014 to January 2015, the patient received further six cycles of the same platinum-based regimen combined with 3-weekly Bevacizumab at a dose of 15 mg/kg. Then Bevacizumab maintenance monotherapy was delivered until January 2016. Meanwhile, in November 2015 the BRCA germline testing was remarkable for a BRCA1 pathogenic variant.
In May 2018 CNS recurrence occurred with diagnostic work-up revealing only a right parietal lesion (of 15 mm axis); systemic CT scan excluded extracranial relapse. Following MTB discussion, intracranial SRS (27 Gy/3 fractions) was performed, followed by 6 courses of carboplatin AUC 6 monotherapy, with overall good tolerance. In December 2018, owing to platinum-sensitive relapse, despite mutational status, Niraparib maintenance was started at a dose of 200 mg once daily, based on baseline body weight and platelet count. In September 2023 the follow-up brain MRI was suggestive for complete remission of brain metastases and the repeat PET-CT scan was unremarkable for systemic disease. Concomitantly, tumor markers were unremarkable; thus 6-month radiologic reassessment was established. The Niraparib maintenance is currently ongoing with good subjective tolerance and no relevant toxicities. Therefore, the patient is experiencing a durable clinical benefit throughout Niraparib therapy.
Figure 2.
Timeline of patient treatment journey in case two. Abbreviations. CC0: completeness of cytoreduction score 0. CHT: chemotherapy. CP: Carboplatin plus Paclitaxel. BEV: Bevacizumab. SRS: stereotactic radiosurgery.
Figure 2.
Timeline of patient treatment journey in case two. Abbreviations. CC0: completeness of cytoreduction score 0. CHT: chemotherapy. CP: Carboplatin plus Paclitaxel. BEV: Bevacizumab. SRS: stereotactic radiosurgery.
2.3. Case Three
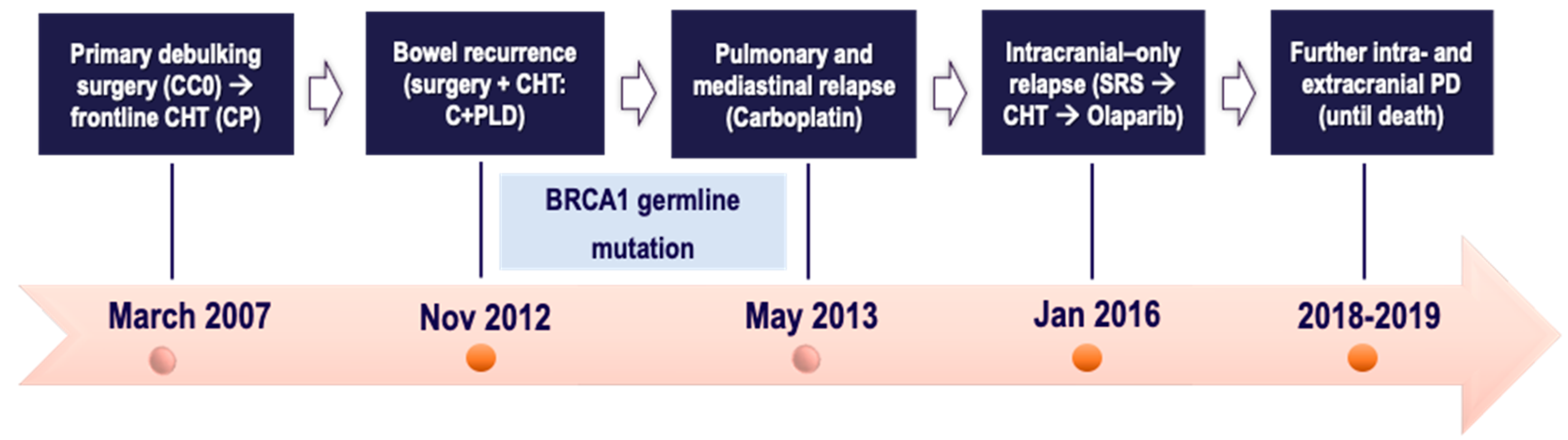
A 47-year-old postmenopausal female with an unremarkable medical history was diagnosed in March 2007 with advanced FT cancer. At the Referral Institute she underwent primary debulking surgery with optimal cytoreduction (complete response intraoperatively); pathology confirmed FIGO IIIB HGSOC. Followingly, she was given frontline Carboplatin plus Paclitaxel regimen (6 cycles) completed in September 2007. Follow-up was negative until November 2012 when a CT scan revealed a pelvic mass infiltrating the sigmoid colon, which was deemed suitable for surgical resection (sigmoidectomy along with colo-rectal anastomosis). Once bowel metastasis from HGSOC was histologically confirmed, the patient was offered Carboplatin plus PLD doublet, and then followed-up. Meanwhile, in May 2013 the patient tested positive for germline BRCA1 deleterious mutation. Then, she experienced pulmonary and mediastinal relapse, not believed suitable for locoregional approaches. Thereby, she was given Carboplatin AUC4 monotherapy (6 cycles) with partial radiological response of the disease sites.
The patient remained free of disease progression until January 2016 when she complained of positional headaches, dizziness, blurred vision. Intracranial recurrence due to temporo-parietal and occipital lesions concomitantly with stable extracranial disease was reported on restaging CT scan. After multidisciplinary agreement, intracranial SRS was performed, followed by 6 courses of carboplatin-paclitaxel doublet, yielding partial remission on all disease sites.
In August 2016, considering platinum-sensitive relapse, Olaparib maintenance was started. She experienced 21-month disease control throughout Olaparib therapy. Following new pulmonary progression in May 2018, further carboplatin-based doublet was delivered for 6 cycles, yielding intra- and extracranial stable disease up to April 2019. Afterwards, due to systemic progression at cerebellum and supra/infra-diaphragmatic lymph nodes, the patient underwent further three chemotherapeutics, namely PLD- trabectedin doublet, carboplatin, and weekly paclitaxel, respectively. Therefore, the patient died in November 2019 after being hospitalized for pulmonary distress.
Figure 3.
Timeline of patient treatment journey in case three. Abbreviations. CC0: completeness of cytoreduction score 0. CHT: chemotherapy. CP: Carboplatin plus Paclitaxel. C+PLD: Carboplatin + Pegylated liposomal doxorubicin. SRS: stereotactic radiosurgery. PD: progressive disease.
Figure 3.
Timeline of patient treatment journey in case three. Abbreviations. CC0: completeness of cytoreduction score 0. CHT: chemotherapy. CP: Carboplatin plus Paclitaxel. C+PLD: Carboplatin + Pegylated liposomal doxorubicin. SRS: stereotactic radiosurgery. PD: progressive disease.
2.4. Case Four
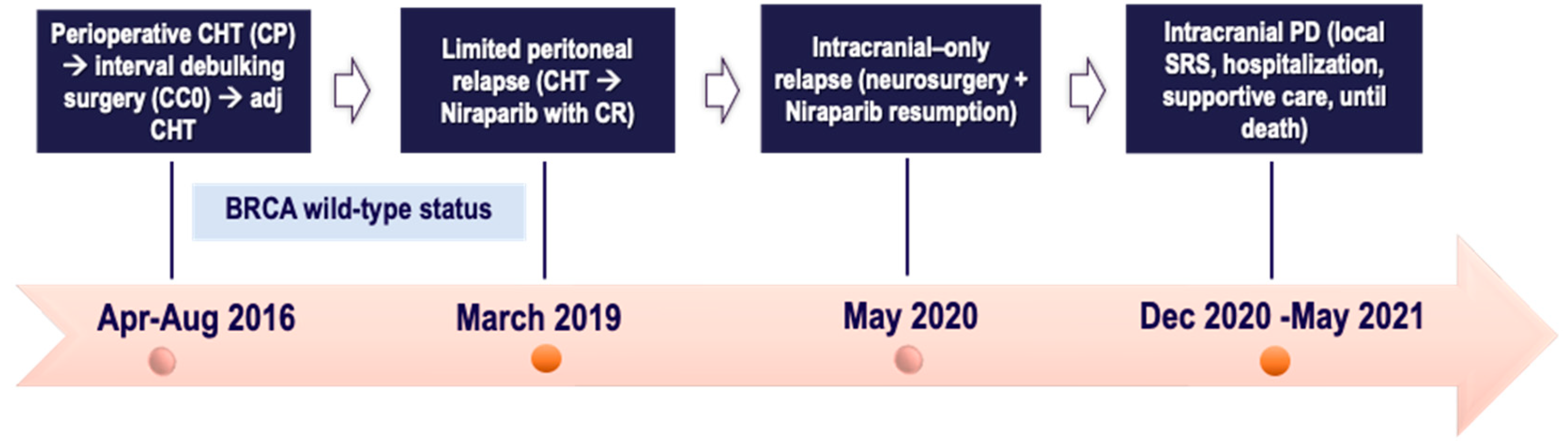
A 65-year-old postmenopausal female without comorbidities sought medical attention in April 2016 for abdominal swelling and pain, with radiological assessment of omental cake, diffuse peritoneal carcinomatosis, ascites and infradiaphragmatic lymphadenopathies. Due to the disease burden and the histological diagnosis of HGSOC on laparoscopic biopsies, at the Referral Centre the patient received neoadjuvant Carboplatin plus Paclitaxel regimen, with good radiologic response. In June 2016 she underwent interval debulking surgery comprising bilateral salpingo-adnexectomy, omentectomy, appendectomy, peritonectomy and pelvic/para-aortic lymphadenectomy, with no gross residual disease. Pathology highlighted FIGO IIIC HGSOC. Meanwhile, BRCA germline testing excluded pathogenic mutation. The subsequent follow-up remained negative until March 2019 when relapse occurred. The CT findings were peritoneal implants of Glisson’s capsule and pelvic peritoneum, in the context of mild pain. Owing to the fully platinum sensitive relapse, the patient was offered a 2nd line Carboplatin (then switched to Cisplatin due to allergy) plus Gemcitabine regimen with a complete radiological response of all disease sites. Thus, in June 2019 Niraparib maintenance monotherapy was started at the full dose of 300 mg once daily with weekly full blood count testing as per drug label. Due to recurrent grade 2 thrombocytopenia in the first 3 cycles leading to a 3-week break, Niraparib was de-escalated to 200 mg once daily without adjustments until the treatment ended.
In May 2020 neurological complaints (fasting emesis, headaches, unsteady gait) occurred. Intracranial disease was confirmed on brain MRI due to single left cerebellar metastases of 26 x 30 mm with modest vasogenic edema, along with no extracranial disease on CT scan. Following multidisciplinary agreement, the patient, after short-course anti-edema corticosteroids, underwent suboccipital craniotomy with radical resection of the single cerebellar lesion; pathology highlighted “brain metastases from HGSOC”. A postsurgical sequela (pseudomeningocele) required immediate surgical revision.
The neurological interdisciplinary care group at the Referral Centre, based on the time elapsed from neurosurgery, did not recommend adjuvant RT on surgical bed. Thus, Niraparib was resumed after surgical wound healing, given the extracranial disease control along with the low-volume intracranial disease. In November 2020 the follow-up brain MRI showed findings more suggestive for a deep residue of the resected metastasis than a local relapse, thus posing a diagnostic dilemma. Due to the clinical complaints (unsteady gait), a diagnostic lumbar puncture was performed in an inpatient setting, excluding LMs, followed by local SRS targeting all the posterior cranial fossa (25 Gy/5 fractions). Meanwhile, Niraparib was maintained, aside from a 5-day break during RT sessions. The patient experienced a sustained clinical benefit from Niraparib monotherapy with improved cenesthesia by virtue of daily functional rehabilitation and no new neurological complaints. Overall intra- and extracranial disease control on follow-up brain MRI and CT scan, respectively, was shown.
In December 2020, she was hospitalized due to intracranial hypertension symptomatology with subsequent clinical deterioration. MRI findings were suggestive for LMs, proven by cerebrospinal fluid cytology. Systemic CT scan excluded extracranial progression. Due to poor KPS and rapidly progressive disease, the MTB at the Referral Centre retained the patient unfit for CHT rechallenge. Supportive and palliative care with intensive rehabilitation were empowered upon discharge with clinical benefit on symptoms relief. At the end of May 2021, 61 months after diagnosis, the patient died. Hence, a multimodal care approach combining surgery, RT, and CHT has been encouraged to manage brain metastases from EOC in a fit patient with good KPS.
Figure 4.
Timeline of patient treatment journey in case four. Abbreviations. CC0: completeness of cytoreduction score 0. CHT: chemotherapy. CP: Carboplatin plus Paclitaxel. CR: complete response. PD: progressive disease. SRS: stereotactic radiosurgery.
Figure 4.
Timeline of patient treatment journey in case four. Abbreviations. CC0: completeness of cytoreduction score 0. CHT: chemotherapy. CP: Carboplatin plus Paclitaxel. CR: complete response. PD: progressive disease. SRS: stereotactic radiosurgery.
2.5. Case Five
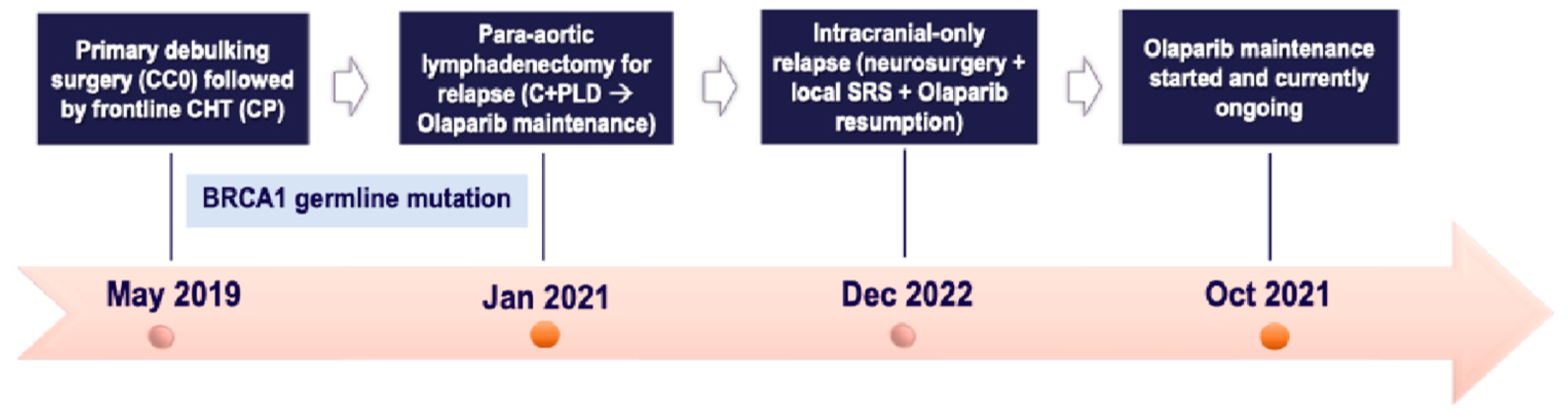
A 52-year-old postmenopausal female with an unremarkable medical history was diagnosed in May 2019 with advanced EOC. At the Referral Institute she underwent primary debulking surgery with optimal cytoreduction (no gross residual disease); pathology confirmed FIGO IIB high-grade endometrioid ovarian carcinoma. Then, she underwent frontline Carboplatin plus Paclitaxel regimen (4 cycles out of 6, due to the patient's untolerance). In April 2020 the BRCA germline testing (delayed due to patient’s willingness) resulted positive for BRCA1 deleterious mutation.
Follow-up was negative until January 2021 when a lymph node relapse was detected on restaging CT scan (para-aortic adenopathies), concomitantly with a biochemical relapse, albeit without clinical symptoms. After multidisciplinary agreement, in February 2021 the patient underwent paraaortic lymphadenectomy, with histological confirmation of “metastasis from endometrioid histotype of ovarian carcinoma”. Therefore, she was offered Carboplatin plus PLD doublet, due to residual taxane-related neurotoxicity, followed by Olaparib maintenance, which was started in October 2021. Olaparib was de-escalated (to 450 mg daily) due to anemia, without further adjustments subsequently.
In December 2022 she was hospitalized owing to an epileptic crisis without other neurological complaints, and CT scan revealed a single left parieto-occipital lesion of about 43 mm without extracranial disease sites. Due to intracranial-only disease, the MTB at the Referral Centre deemed the patient candidate for neurosurgery with radical resection of the single lesion and postoperative SRS (3 fractions). Thus, the patient was referred for Olaparib maintenance resumption (apart from 3 weeks off during the treatments). Histological report of “brain metastases from G3 endometrioid ovarian cancer” was obtained.
As of June 2024, the Olaparib maintenance is currently underway, with a 32-month disease control as the last CT scan is unremarkable for intra- and extracranial disease along with a CA125 within the normal range. Thus, the patient is experiencing a long-term clinical benefit throughout the Olaparib monotherapy, without any relevant toxicity or clinical complaint.
Figure 5.
Timeline of patient treatment journey in case five. Abbreviations. CC0: completeness of cytoreduction score 0. CHT: chemotherapy. CP: Carboplatin plus Paclitaxel. C+PLD: Carboplatin + Pegylated liposomal doxorubicin. SRS: stereotactic radiosurgery.
Figure 5.
Timeline of patient treatment journey in case five. Abbreviations. CC0: completeness of cytoreduction score 0. CHT: chemotherapy. CP: Carboplatin plus Paclitaxel. C+PLD: Carboplatin + Pegylated liposomal doxorubicin. SRS: stereotactic radiosurgery.
2.6. Case Six
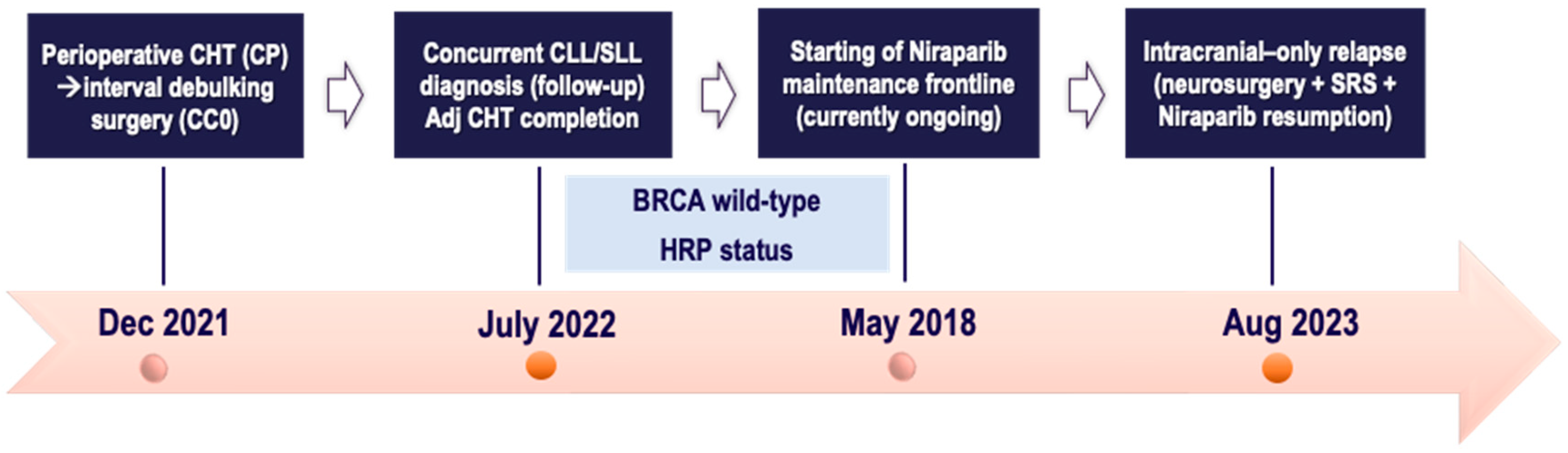
A 73-year-old female with an unremarkable family history sought medical attention in December 2021 for abdominal swelling and severe constipation. Diagnostic work-up revealed adnexal mass, ascites, peritoneal carcinomatosis, omental cake, and multiple mesenteric lymphadenopathies. Baseline Ca125 was 788 U/ml. At the Referral Centre, in February 2022 she underwent laparoscopy with histological diagnosis of HGSOC from an omental biopsy. After MTB discussion, due to the disease burden, the patient was offered neoadjuvant chemotherapy with four cycles of carboplatin plus paclitaxel doublet, gaining a favorable radiological response and complete biochemical remission (Ca125: 29 U/ml). In July 2022 she underwent interval debulking surgery, including retrograde hysterectomy, salpingo-oophorectomy, radical omentectomy, and excision of bulky and para-aortic, paracaval and iliac-obturator lymph nodes, with no gross residual disease. Final pathology confirmed FIGO IIIA (ypT3a ypN1b) HGSOC. Additionally, left obturator lymph nodes showed localization of chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL, based on WHO 2017). After hematological consultation recommending only follow-up for the newly diagnosed CLL/SLL, the patient received the last two cycles of platinum chemotherapy up to September 2022. Meanwhile, the HRD and BRCA somatic testing reported BRCA wild-type and HR proficient status. Owing to the good radiological and biochemical response, based on mutational status, Niraparib maintenance monotherapy was started in October 2022 at the dose of 200 mg once daily. The first 6-month follow-up CT scan showed no evidence of disease recurrence with concomitant increase in number and size of pelvic lymph nodes, corresponding to the disease sites of known CLL/SLL. However, PET-CT scan was unremarkable such that no specific treatment was indicated by the Consultant Hematologist. The patient has continued Niraparib maintenance without significant toxicity.
In August 2023, she presented to the Emergency Department with worsening vomiting, nausea, and vertigo. Brain CT highlighted a large hypodense area of 43x21mm in the left cerebellar hemisphere causing mass effect on the vermis with displacement to the right and marked compression of the ventricular system. These findings were confirmed on brain MRI and were suggestive for CNS metastases. Restaging CT scan excluded extracranial relapse, while confirming the known lymphadenopathies as unchanged. After transfer to the neurosurgery department, the patient underwent excision of the left cerebellar lesion. Histopathology highlighted: “poorly differentiated adenocarcinoma with immunophenotypic profile consistent with the primary HGSOC, with clear resection margins”. The MTB at the Referral Centre retained the patient suitable for SRS to the resection bed and Niraparib resumption (after a break during neurosurgery) under close clinical and radiological surveillance.
However, about a month later, the patient returned to the Emergency Department with spontaneous hematomas, atraumatic conjunctival and eyelid hemorrhage, revealing pancytopenia (hemoglobin 7.41g/dl, neutrophils 1.40x103/μl, platelets 6.77x103/μl). Niraparib was discontinued, and a bone marrow biopsy showed hypocellular marrow with CLL/SLL infiltration (25%). After normalization of blood parameters within 28 days, Niraparib was resumed with first-level dose de-escalation at 100 mg once daily. The subsequent blood count tests showed normal hematological values, thus allowing Niraparib continuation. Follow-up systemic CT scan performed in December 2023 revealed stable lymph nodes with no signs of progression. As of June 2024, the patient is asymptomatic and is continuing Niraparib maintenance therapy without any toxicity.
Figure 6.
Timeline of patient treatment journey in case six. Abbreviations. CC0: completeness of cytoreduction score 0. CHT: chemotherapy. CP: Carboplatin plus Paclitaxel. CLL/SLL: chronic lymphocytic leukemia/small lymphocytic lymphoma. HRP: homologous recombination proficient. SRS: stereotactic radiosurgery.
Figure 6.
Timeline of patient treatment journey in case six. Abbreviations. CC0: completeness of cytoreduction score 0. CHT: chemotherapy. CP: Carboplatin plus Paclitaxel. CLL/SLL: chronic lymphocytic leukemia/small lymphocytic lymphoma. HRP: homologous recombination proficient. SRS: stereotactic radiosurgery.
3. Discussion and Literature Review
In our multi-institutional case study research, six patients, presenting with BMs from EOC, experienced a sustained clinical benefit from PARPi maintenance, received in the context of a multimodal treatment journey. Little data is available, to date, about the treatment modalities for this intriguing disease setting, due to the rarity of BMs [15]. Findings supporting the PARPi use in this context are still anecdotal [5,15]. Our descriptive research can thus provide a valuable reference to clinical practice for this uncommon scenario. The current body of work about PARPi use in BMs is summarized in the Supplementary file (Table S1), along with the search criteria reported in the search strategy section (at the bottom of the Supplementary Table S1).
3.1. What’s the Rationale Behind the PARPi Use in BMs from EOC?
PARPi are the standard-of-care maintenance treatments licensed both in frontline and platinum-sensitive relapse settings, even regardless of BRCA and HRD mutation status [25]. Historically, the milestone of the PARPi mechanism of action has been identified as “synthetic lethality”, consisting in the loss-of-function mutation of BRCA genes coupled with synthetically inhibiting PARP1 [21]. Recently, the key role of stalled replication forks due to PARP1 blocking, which enables genomic instability and cell death, has been suggested [21].
Limited evidence supports PARPi effectiveness in BM treatment for EOC [14,15,26]. The BBB disruption in the context of intracranial metastases could enable more successful delivery and efficacy of cytotoxics, like platinum salts and PARPi [14]. Preclinical findings strongly support differential pharmacokinetic (PK) profile and antitumor activity of PARPi in intracranial xenografts [14]. A comparative PK study of PARPi highlighted the correlation between Niraparib’s favorable pharmacokinetic properties and preclinical antitumor effects in BRCA wild-type tumors [27,28]. Niraparib exhibits greater and sustained intratumoral exposure than that of Olaparib, due to higher permeability across the intact BBB [4,28]. This is consistent with the more potent tumor growth inhibition exerted by Niraparib in BRCA-mutant intracranial xenografts, opposed to Olaparib, thus supporting its broader clinical effect in patients with both BRCAmut and BRCA wild-type tumors.
In the rapidly evolving therapeutic landscape of EOC, PARPi are increasingly employed as maintenance monotherapy in BM patients, although their efficacy in platinum-sensitive brain relapse is almost completely unknown [18]. The unique body of work supporting PARPi use in this setting arises from review case series and retrospective studies, in absence of robust prospective data [5].
Interestingly, broadening the therapeutic applicability of PARPis to cancers with BRCAness phenotype, including many CNS malignancies, remains a significant challenge and an active research topic [29]. Thanks to recent preclinical studies, novel sensitivity biomarkers of BRCAness are being discovered, paving ways towards rational combinations of PARPis in neuro-oncology [29], whose feasibility and efficacy will be also informed by the ongoing clinical trials (ClinicalTrials.gov identifier: NCT03991832) [29,30]. Notably, Niraparib activity and efficacy are being tested in investigational trials for either newly diagnosed or recurrent glioblastoma patients (ClinicalTrials.gov identifier: NCT05076513 and NCT04715620) [30,31]. To the best of our knowledge, no trials on PARPi efficacy in BM patients are underway. Anyway, the PARPi maintenance is gaining a growing role in the management of BMs from EOC [5].
3.2. What are the Main Highlights for Niraparib Maintenance in BMs from EOC?
Cases one and two are emblematic for Niraparib maintenance in patients with intracranial-only recurrence, presenting with a single cerebellar lesion. From an anatomical standpoint, the cerebellum represents the most common intracranial metastatic site [9]. There is a paucity of data regarding the treatment of brain metastases with Niraparib in EOC. Among the handful of available reports [15,18,26], in the former a BRCA1 mutant patient developed a solitary fully platinum-sensitive CNS relapse from HGSOC that, nevertheless, was rapidly progressive while on platinum CHT and WBRT. After partial response to the following platinum-based regimen, maintenance Niraparib favored intracranial stable disease and systemic control, leading to symptoms’ relief and durable patient’s remission for over 17 months [26] (as reported in the Supplementary Table S1).
In a different situation, a patient with CNS relapse received Niraparib monotherapy, in the ambit of a multimodal treatment plan (with WBRT and CHT), yielding an almost complete radiological response (on MRI) of brain lesions after 9 months of administration. The tolerability profile was manageable with transient asymptomatic myelosuppression favoring treatment resumption and continuation, without further events [18]. Strikingly, a very atypical presentation of a cerebellar metastasis from EOC at initial diagnosis has been recently reported [10]. A personalized multimodal therapeutic approach including neurosurgery, frontline CHT and Niraparib maintenance led to intracranial complete clinical response and good patient’s quality of life [10] (as detailed in the Supplementary Table S1). Notably, in a more recent retrospective cohort, BM patients receiving Niraparib as part of their multimodal treatment plan gained good disease control irrespective of their BRCA mutational status [5] (as detailed in the Supplementary Table S1). In another case study, the administration of Niraparib maintenance monotherapy, following surgical debulking of a single brain metastasis, yielded long-term clinical benefit (PFS of about 29 months) in a patient who was unfit for other systemic and locoregional approaches (CHT and brain RT, respectively) [32]. Strikingly, the successful outcome of Niraparib in a BRCA1-mutant patient with BM from high-grade serous endometrial cancer was highlighted [33] (as reported in the Supplementary Table S1).
3.3. What Evidence Supports Olaparib Maintenance in Patients with Intracranial Relapse?
Case three reflects the clinical setting of Olaparib maintenance in a BRCA-mutated patient after intra-/extracranial recurrence. There is scant evidence supporting Olaparib effectiveness in BM treatment for EOC [14]. We are aware of two case reports showing intracranial responses to olaparib in EOC/FT/PP cancers, the former with leptomeningeal metastases (LMs) in a BRCA2-mutant patient with HGSOC and the latter with multiple brain metastases in a BRCA1-mutated patient with PP cancer, respectively [34,35] (as summarized in the Supplementary Table S1). Recently, a monocenter case series, dealing with BRCA1-2 mutant patients affected by oligometastatic EOC to the brain, highlighted durable benefit with olaparib maintenance continued after local therapy (even combined with bevacizumab) [36]. In another retrospective series of BRCA-mutated patients with BMs, OS benefit from multimodal approaches including PARPi maintenance was reported, although the prognosis remains poor [37].
Interestingly, in a case study a BRCA1-mutated patient with late isolated CNS relapse yielded a long-term response to Olaparib exceeding 4 years after WBRT completion and 42 months following olaparib onset. A meaningful intracranial response, with further shrinkage of multiple BMs reported on follow-up MRI, is being maintained along with durable systemic disease control and good QoL, without relevant toxicities [14] (as detailed in the Supplementary Table S1). Of note, Olaparib, given as maintenance regimen in a BRCA2-mutant heavily pretreated patient with platinum-sensitive intracranial relapse, yielded a 14-month disease control intra-and extra-cranially despite CNS metastases with carcinomatous meningitis [38] (as reported in the Supplementary Table S1). Patients with LMs harbor a very dismal prognosis [39]. This is the first report highlighting the efficacy of a PARPi on meningeal disease of a gBRCA-mut carrier, likely due to the Olaparib ability to cross the leptomeningeal barrier [38].
A peculiar setting regards the development of BMs arising from a primary FT cancer, whose incidence is only 0.21% according to the SEER database. In detail, median time to onset of BMs from FT cancers is about 3 years (range 3–52 months). Of note, sites of CNS metastasis encompass supratentorial and infratentorial compartments as well as the skull base [40]. Among the available reports, a woman diagnosed with a BRCA1-related FT presented with an incidentally discovered left frontoparietal mass, whose pathology was consistent with “metastasis from HGSOC of Mullerian origin”. The adjuvant SRS performed due to the relatively young age, good KPS and the limited tumor volume, yielded sustained benefit. This case is demonstrative of the importance of screening for CNS disease in metastatic gynecologic malignancies, especially in patients harboring BRCA mutations and disseminated disease [40].
3.4. What is the Rationale for Continuing PARPi Beyond Intracranial Progression in EOC?
Cases four, five and six reflect the continuation of PARPi maintenance, both in frontline (case six) and relapsed (cases four-five) setting, beyond intracranial oligometastatic recurrence without extracranial disease. In detail, they report the Niraparib (cases four-six) and Olaparib (case five) continuation beyond intracranial-only relapse (oligometastases) treated with local therapy. Despite the strong prognostic impact of PARPi in platinum-sensitive recurrence, many patients will eventually progress on maintenance therapy [41]. Compelling evidence from the updated analysis of the phase III ENGOT-OV16/NOVA trial highlights the extended benefit (primary endpoint PFS) of Niraparib monotherapy beyond first disease progression in both the gBRCA-mut and BRCA wild-type cohorts, respectively [42]. This final data supports the safe long-term use of Niraparib in the platinum-sensitive relapsed setting [41]. However, none of the prospective registration trials addressed PARPi efficacy in BM patients, albeit those with stable metastases being eligible [15]. Supporting evidence from case reports show prolonged intracranial responses with PARPi [15] (as reported in Supplementary Table S1). In a recent mono-institutional experience, about one-third of patients on Olaparib maintenance experienced oligo-progression, defined as limited to ≤3 sites, involving CNS at a 5% rate. These patients may benefit from local consolidation therapy, albeit being rarely employed in EOC. No survival differences in patients with and without oligo-progression were found [41] (as detailed in the Supplementary Table S1). Prospective validation of these findings is mandated to address the value of local therapy for these patients [41].
Strikingly, case six is the first clinical report on the continuation of frontline Niraparib maintenance beyond CNS oligometastatic recurrence. There are no available clinical trials or other case studies regarding this context, probably due to the recent implementation of Niraparib in frontline setting and the known rarity of CNS relapse. In fact, only a clinical case highlighted the use of frontline Niraparib maintenance in a patient presenting with EOC-related BM at time of initial diagnosis, with no progressive disease [10] (as detailed in the Supplementary Table S1). Hence, albeit considering the limitations associated with our descriptive case study, especially the low generalizability of these findings, in absence of high-quality supporting evidence, our experience may add to routine practice for this highly rare scenario and foster further research.
Overall, indirect encouraging results from trials designed in other tumors, such as non-small cell lung cancer receiving targeted therapies following local ablation, may add to potential clinical utility of PARPi in intracranial disease control even after oligoprogression [15]. Further consideration should be given to continuing PARPi beyond localized disease control in extracranial oligoprogression [15]. Collectively, evidence directly ensuring the continuation or not of PARPi after locoregional therapies for CNS progression in EOC is lacking as of yet [15]. Further prospective validation is needed to address the role of local therapy for this patient’s subset [41].
4. Concluding Remarks and Future Challenges
Owing to the prolonged survival times, uncommon presentations like BMs from EOC are expected to increase. Shared multidisciplinary and supportive care pathways should be ensured for a personalized treatment plan. The gynecologic oncology community will require growing experience with the PARPi use in this rare scenario [15]. To our knowledge, EOC patients harboring untreated or symptomatic BMs were excluded from known registration trials [15]. No trials addressing PARPi efficacy in this population are underway [15]. Clinically relevant issues for EOC patients with intracranial relapse are emerging, like the continuation of PARPi beyond isolated CNS progression after local therapy [15]. Thus, clinical trials including BM patients even in the post-progression setting, are strongly awaited given their durable response to PARPi ever reported before [15]. In summary, prospective research, aimed to identify predictive biomarkers and implement individualized strategies for BM patients, is strongly needed [15].
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Summary of the available evidence about PARPi use in patients with BMs from EOC, according to the search criteria reported in the search strategy section.
Author Contributions
Conceptualization, S.F., A.B.; methodology, S.F..; resources, S.F, G.T., L.B., G.A., A.F., A.M., A.B.; writing—original draft preparation, S.F.; writing—review and editing, A.B., G.T.; visualization and correction, S.F., A.B.; supervision, A.B.; project administration, S.F., A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The case study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Obtained
Data Access Statement
All relevant data are within the paper and its Supporting Information files. .
Conflicts of Interest declaration
The authors declare no conflicts of interest for this work.
References
- Jiri Hatina, Maximilian Boesch, Sieghart Sopper, Michaela Kripnerova, Dominik Wolf, Daniel Reimer, Christian Marth, and Alain G. Zeimet. (2021). Ovarian cancer stem cell heterogeneity. In A. Birbrair (Ed.), Stem Cells Heterogeneity in Cancer (pp. 201–216).
- Ledermann, J. A., Matias-Guiu, X., Amant, F., Concin, N., Davidson, B., Fotopoulou, C., González-Martin, A., Gourley, C., Leary, A., Lorusso, D., Banerjee, S., Chiva, L., Cibula, D., Colombo, N., Croce, S., Eriksson, A. G., Falandry, C., Fischerova, D., Harter, P., … Fagotti, A. (2024). ESGO–ESMO–ESP consensus conference recommendations on ovarian cancer: pathology and molecular biology and early, advanced and recurrent disease. Annals of Oncology. [CrossRef]
- National Comprehensive Cancer Network, Ovarian cancer including fallopian tube cancer and primary peritoneal cancer. NCCN Practice Guidelines, Version 1, 2023.
- Scotto, G., Borella, F., Turinetto, M., Tuninetti, V., Valsecchi, A. A., Giannone, G., Cosma, S., Benedetto, C., & Valabrega, G. (2021). Biomarkers of central nervous system involvement from epithelial ovarian cancer. Cells (Basel, Switzerland), 10(12), 3408. [CrossRef]
- Alizzi, Z., Roxburgh, P., Cartwright, D., McLaren, A., Park, S., Jones, R., Greening, S., Hudson, E., Green, C., Gray, S., Khalique, S., Karteris, E., & Hall, M. (2023). Description of a retrospective cohort of epithelial ovarian cancer patients with brain metastases: Evaluation of the role of PARP inhibitors in this setting. Journal of Clinical Medicine, 12(7), 2497. [CrossRef]
- Kolomainen, D. F., Larkin, J. M. G., Badran, M., A’Hern, R. P., King, D. M., Fisher, C., Bridges, J. E., Blake, P. R., Barton, D. P. J., Shepherd, J. H., Kaye, S. B., & Gore, M. E. (2002). Epithelial ovarian cancer metastasizing to the brain: a late manifestation of the disease with an increasing incidence. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology, 20(4), 982–986. [CrossRef]
- Marchetti, C., Ferrandina, G., Cormio, G., Gambino, A., Cecere, S., Lorusso, D., De Giorgi, U., Bogliolo, S., Fagotti, A., Mammoliti, S., Narducci, F., Bergamini, A., Scollo, P., Biglia, N., Breda, E., Tamberi, S., Marinaccio, M., Angioli, R., Salerno, L., … Panici, P. B. (2016). Brain metastases in patients with EOC: Clinico-pathological and prognostic factors. A multicentric retrospective analysis from the MITO group (MITO 19). Gynecologic Oncology, 143(3), 532–538. [CrossRef]
- Madariaga, A. (2020). Manage wisely: poly(ADP-ribose) polymerase inhibitor (PARPi) treatment and adverse events. Int J of Gynecol Cancer, 30, 903–915. [CrossRef]
- Nasu, K., Satoh, T., Nishio, S., Nagai, Y., Ito, K., Otsuki, T., Hongo, A., Hirashima, Y., Ogura, T., & Shimada, M. (2013). Clinicopathologic features of brain metastases from gynecologic malignancies: a retrospective study of 139 cases (KCOG-G1001s trial). Gynecologic Oncology, 128(2), 198–203. [CrossRef]
- Cabitza, E., Pirola, M., Baldessari, C., Bernardelli, G., Zunarelli, E., Pipitone, S., Vitale, M. G., Nasso, C., Molinaro, E., Oltrecolli, M., D’Agostino, E., Mandato, V. D., Palicelli, A., Dominici, M., & Sabbatini, R. (2023). Cerebellar metastasis of ovarian cancer: a case report. Journal of Medical Case Reports, 17(1), 553. [CrossRef]
- Pakneshan, S., Safarpour, D., Tavassoli, F., & Jabbari, B. (2014). Brain metastasis from ovarian cancer: a systematic review. Journal of Neuro-Oncology, 119(1), 1–6. [CrossRef]
- Kim M. et al: Barriers to Effective Drug Treatment for Brain Metastases: A Multifactorial Problem in the Delivery of Precision Medicine. Pharm Res; 35(9): 177. [CrossRef]
- Limon, D., Shachar, E., Wolf, I., Adar, L., Peleg Hasson, S., Ferro, L., & Safra, T. (2022). Brain metastases in patients with ovarian cancer. Acta Oncologica (Stockholm, Sweden), 61(6), 757–763. [CrossRef]
- Gallego, A. (2021). Long-term response to olaparib in BRCA 1-related ovarian cancer with brain metastases. Int J Gynecol Cancer, 31, 1292–1296. [CrossRef]
- Kasherman, L., Madariaga, A., Rouzbahman, M., Murphy, K., Shultz, D., Stockley, T., & Oza, A. M. (2021). Across barriers: poly ADP-ribose polymerase inhibitors beyond progression in high grade serous ovarian cancer with brain metastases. International Journal of Gynecological Cancer: Official Journal of the International Gynecological Cancer Society, 31(1), 139–143. [CrossRef]
- Stasenko, M., Cybulska, P., Feit, N., Makker, V., Konner, J., O’Cearbhaill, R. E., Alektiar, K. M., Beal, K., Gardner, G. J., Long Roche, K. C., Sonoda, Y., Chi, D. S., Zivanovic, O., Leitao, M. M., Jr, Cadoo, K. A., & Tew, W. P. (2019). Brain metastasis in epithelial ovarian cancer by BRCA1/2 mutation status. Gynecologic Oncology, 154(1), 144–149. [CrossRef]
- Kwon, J.-W., Yoon, J. H., Lim, M. C., Joo, J., Yoo, H., Shin, S.-H., Park, S. Y., Lee, S. H., Kim, Y.-J., Kim, J.-Y., & Gwak, H.-S. (2018). Treatment results and prognostic factors of brain metastases from ovarian cancer: A single institutional experience of 56 patients. International Journal of Gynecological Cancer: Official Journal of the International Gynecological Cancer Society, 28(8), 1631–1638. [CrossRef]
- Tao, Mengyu, Cheng, J., & Wu, X. (2020). Niraparib as maintenance therapy in germline ATM-mutated and somatic BRCA2-mutated ovarian cancer with brain metastases: A case report and literature review. OncoTargets and Therapy, 13, 12979–12986. [CrossRef]
- Matsuo, K., Eno, M. L., Ahn, E. H., Shahzad, M. M. K., Im, D. D., Rosenshein, N. B., & Sood, A. K. (2011). Multidrug resistance gene (MDR-1) and risk of brain metastasis in epithelial ovarian, fallopian tube, and peritoneal cancer. American Journal of Clinical Oncology, 34(5), 488–493. [CrossRef]
- Le Page, C., Amuzu, S., Rahimi, K., Gotlieb, W., Ragoussis, J., & Tonin, P. N. (2021). Lessons learned from understanding chemotherapy resistance in epithelial tubo-ovarian carcinoma from BRCA1and BRCA2 mutation carriers. Seminars in Cancer Biology, 77, 110–126. [CrossRef]
- Vergote, I., González-Martín, A., Ray-Coquard, I., Harter, P., Colombo, N., Pujol, P., Lorusso, D., Mirza, M. R., Brasiuniene, B., Madry, R., Brenton, J. D., Ausems, M. G. E. M., Büttner, R., Lambrechts, D., & European experts’ consensus group. (2022). European experts’ consensus: BRCA/homologous recombination deficiency testing in first-line ovarian cancer. Annals of Oncology, 33(3), 276–287. [CrossRef]
- Jernigan, A. M., Mahdi, H., & Rose, P. G. (2015). Epithelial ovarian cancer metastatic to the central nervous system and a family history concerning hereditary breast and ovarian cancer--A potential relationship. International Journal of Gynecological Cancer: Official Journal of the International Gynecological Cancer Society, 25(7), 1232–1238. [CrossRef]
- Ratner, Elena, Bala, M., Louie-Gao, M., Aydin, E., Hazard, S., & Brastianos, P. K. (2019). Increased risk of brain metastases in ovarian cancer patients with BRCA mutations. Gynecologic Oncology, 153(3), 568–573. [CrossRef]
- Balendran, S., Liebmann-Reindl, S., Berghoff, A. S., Reischer, T., Popitsch, N., Geier, C. B., Kenner, L., Birner, P., Streubel, B., & Preusser, M. (2017). Next-Generation Sequencing-based genomic profiling of brain metastases of primary ovarian cancer identifies a high number of BRCA-mutations. Journal of Neuro-Oncology, 133(3), 469–476. [CrossRef]
- O’Malley, D. M., Krivak, T. C., Kabil, N., Munley, J., & Moore, K. N. (2023). PARP inhibitors in ovarian cancer: A review. Targeted Oncology, 18(4), 471–503. [CrossRef]
- Gray, S., Khor, X. Y., & Yiannakis, D. (2019). Niraparib as maintenance therapy in a patient with ovarian cancer and brain metastases. BMJ Case Reports, 12(8), e230738. [CrossRef]
- Sun K, Mikule K, Wang Z, et al. A comparative pharmacokinetic study of PARP inhibitors demonstrates favorable properties for niraparib efficacy in preclinical tumor models. Oncotarget 2018;9:37080–96. [CrossRef]
- Mikule, K., & Wilcoxen, K. (2015). Abstract B168: The PARP inhibitor, niraparib, crosses the blood brain barrier in rodents and is efficacious in a BRCA2-mutant intracranial tumor model. Molecular Cancer Therapeutics, 14(12_Supplement_2), B168–B168. [CrossRef]
- Ning, J., & Wakimoto, H. (2020). Therapeutic application of PARP inhibitors in neuro-oncology. Trends in Cancer, 6(2), 147–159. [CrossRef]
- Wang, X., Ellenbogen, Y., Mojica, C., Matos, G. D. R., Alsajjan, R., Ramos, R., Climans, S. A., Voisin, M., Patil, V., Baker, S., Chan, Y.-L., Pimentel Muniz, T., Gao, A., Wang, B. X., Zadeh, G., Mason, W. P., & Chen, E. X. (2024). A phase II trial of olaparib and durvalumab in patients with recurrent IDH-mutated gliomas. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology, 42(16_suppl), 2013–2013. [CrossRef]
- Sanai, N., Umemura, Y., Margaryan, T., Molloy, J., Zhang, H., Knight, W., Harmon, J., Hong, A., Wanebo, J., Braun, K., Kennedy, W. R., Garcia, M. A., Barani, I. J., Yoo, W., Tien, A.-C., Tovmasyan, A., & Mehta, S. (2024). Niraparib efficacy in patients with newly-diagnosed glioblastoma: Clinical readout of a phase 0/2 “trigger” trial. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology, 42(16_suppl), 2002–2002. [CrossRef]
- Zhang, Z., Xu, M., Sakandar, A., Du, X., He, H., He, W., Li, D., & Wen, Q. (2022). Successful treatment of a patient with brain metastasis from ovarian cancer with BRCA wild type using niraparib: A case report and review of the literature. Frontiers in Oncology, 12, 873198. [CrossRef]
- Wang, Q., Zhang, F., Gao, H., & Xu, Y. (2021). Successful treatment of a patient with brain metastases from endometrial cancer using Niraparib: a case report. Annals of Palliative Medicine, 10(1), 818–827. [CrossRef]
- Bangham, M., Goldstein, R., Walton, H., & Ledermann, J. A. (2016). Olaparib treatment for BRCA-mutant ovarian cancer with leptomeningeal disease. Gynecologic Oncology Reports, 18, 22–24. [CrossRef]
- Sakamoto, I., Hirotsu, Y., Nakagomi, H., Ikegami, A., Teramoto, K., & Omata, M. (2019). Durable response by olaparib for a Japanese patient with primary peritoneal cancer with multiple brain metastases: A case report: Durable response by olaparib. The Journal of Obstetrics and Gynaecology Research, 45(3), 743–747. [CrossRef]
- Mohler, A., Salinas, B., Nazur, K., Odia, Y., & Lambrou, N. (2021). THER-02. PARP inhibitor tolerability and impact on progression-free survival in patients with high-grade, ovarian carcinoma with brain metastasis: A case-series. Neuro-Oncology Advances, 3(Supplement_3), iii12–iii13. [CrossRef]
- Magdalena Sliwinska, Malgorzata Cieslak-Stec, Izabela Laprus, Rafal Tarnawski. 482 Brain metastases in patients with advanced BRCA-associated ovarian cancer receiving systemic treatment and adjuvant maintenance Olaparib therapy according to the criteria of study 19 clinical trial–single-centre experience (2023). [CrossRef]
- Favier, L., Truc, G., Boidot, R., & Bengrine-Lefevre, L. (2020). Long-term response to Olaparib in carcinomatous meningitis of a BRCA2 mutated ovarian cancer: A case report. Molecular and Clinical Oncology, 13(1), 73–75. [CrossRef]
- Yano, H., Nagao, S., & Yamaguchi, S. (2020). Leptomeningeal metastases arising from gynecological cancers. International Journal of Clinical Oncology, 25(2), 391–395. [CrossRef]
- Jang, A. I., Bernstock, J. D., Segar, D. J., Distasio, M., Matulonis, U., & Bi, W. L. (2021). Case report: Frontoparietal metastasis from a primary Fallopian tube carcinoma. Frontiers in Surgery, 8. [CrossRef]
- Cerda, V. R., Lu, D., Scott, M., Kim, K. H., Rimel, B. J., & Kamrava, M. (2022). Evaluation of patterns of progression on poly (ADP-ribose) polymerase inhibitor (PARPi) maintenance in ovarian cancer: a cross-sectional study. International Journal of Gynecological Cancer: Official Journal of the International Gynecological Cancer Society, 32(2), 153–158. [CrossRef]
- Matulonis, U., Herrstedt, J., Oza, A., Mahner, S., Redondo, A., Berton, D., Berek, J., Lund, B., Marmé, F., González-Martín, A., Tinker, A., Ledermann, J., Benigno, B., Lindahl, G., Colombo, N., Li, Y., Gupta, D., Monk, B., & Mirza, M. (2021). Long-term safety and secondary efficacy endpoints in the ENGOT-OV16/NOVA phase III trial of niraparib in recurrent ovarian cancer. Gynecologic Oncology, 162, S24–S25. [CrossRef]

Table 1.
Summary of baseline characteristics and treatment outcomes of the patients included in our case study research with BMs from EOC.
Table 1.
Summary of baseline characteristics and treatment outcomes of the patients included in our case study research with BMs from EOC.
|
Case ID |
Age |
BRCA mutation status |
CNS site(s) |
PARPi agent and duration |
PARPi setting at time of BMs |
Extra- cranial site(s) |
Local therapies for BMs |
CNS BOR and survival time with BMs |
| 1 | 53 | BRCA1 PV |
Single (cerebellar) BM |
Niraparib 18 m (ongoing) |
PSR | Para-aortic lymph node |
Surgery RT (SRS) |
CR 32 m (alive) |
| 2 | 52 | BRCA1 PV |
Single (right parietal) BM | Niraparib 64 m (ongoing) |
PSR | No | Surgery RT (SRS) |
CR 72 m (alive) |
| 3 | 47 | BRCA1 PV |
Multiple (parietal, occipital) BMs | Olaparib 21 m |
PSR | Lung; media-stinum |
RT (SRS) | PR 46 m (dead) |
| 4 | 65 | BRCA1-2 wild-type | Single (cerebellar) BM | Niraparib 18 m |
PSR (beyond CNS oligo-recurrence) |
No |
Surgery RT (SRS) |
PR 12 m (dead) |
| 5 | 52 | BRCA1 PV |
Single (single left parieto-occipital) BM | Olaparib 30 m (ongoing) |
PSR (beyond CNS oligo-recurrence) |
No | Surgery RT (SRS) |
CR 18 m (alive) |
| 6 | 73 | BRCA1-2 wild-type | Single (cerebellar) BM | Niraparib 18 m (ongoing) |
Frontline (beyond CNS oligo-recurrence) |
No | Surgery RT (SRS) |
CR 10 m (alive) |
Abbreviations. PV: pathogenic variant. CNS: central nervous system. PSR: platinum-sensitive relapse. BMs: brain metastases. BOR: best overall response. CR: complete response. PR: partial response. PD: progressive disease. m: months.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



