
Submitted:
24 June 2024
Posted:
25 June 2024
You are already at the latest version
Abstract
Abstract Introduction PCa is one of the cancers that exhibits the widest disparity gaps. Geographical place of residence has been shown to be associated with healthcare access/utilization and PCa outcomes. Geographical Information Systems (GIS) are widely being utilized for PCa disparities research, however, inconsistencies in their application exist. This systematic review will summarize GIS application within PCa disparities research, highlight gaps in the literature and propose alternative approaches. Methods This paper followed the methods of the Cochrane Collaboration and the criteria set of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Articles published in peer-reviewed journals were searched through the PubMed, Embase, and Web of Science databases till December 2022. The main inclusion criteria were employing a GIS approach and examining a relationship between geographical components and PCa disparities. The main exclusion criteria were studies conducted outside the US and those that were not published in English. Results A total of 25 articles were included, 23 focused on PCa measures as outcomes: incidence, survival, and mortality while only two examined PCa management. GIS application in PCa disparities research was grouped into three main categories: mapping, processing, and analysis. GIS mapping allowed for the visualization of quantitative, qualitative, and temporal trends of PCa factors. GIS processing was mainly used for geocoding and smoothing of PCa rates. GIS analysis mainly served to evaluate global spatial autocorrelation and distribution of PCa cases, while local cluster identification techniques were mainly employed to identify locations with poorer PCa outcomes, soliciting public health interventions. Discussion Varied GIS applications and methodologies have been used in researching PCa disparities. Multiple geographical scales were adopted leading to variation in associations and outcomes. Geocoding quality varied considerably leading to less robust findings. Limitations in cluster-detection approaches were identified especially when variations were captured using the Spatial Scan Statistic. GIS approaches utilized in other diseases might be applied within PCa disparities research for more accurate inferences. A novel approach for GIS research in PCa disparities could be focusing more on geospatial disparities in procedure utilization especially when it comes to PCa screening techniques. Conclusion This systematic review summarized and described the current state and trend of GIS application in PCa disparities research. Although GIS is of crucial importance when it comes to PCa disparities research, future studies should rely on more robust GIS techniques, carefully select the geographical scale studied, and partner with GIS scientists for more accurate inferences. Such interdisciplinary approaches have the potential to bridge the gaps between GIS and cancer prevention and control to further advance cancer equity.
Keywords:
Keywords: GIS
; geographic
; prostate cancer
; disparities
; systematic review
Introduction
Prostate cancer (PCa) is the second leading cause of cancer death in American men and one of the cancers that exhibits the largest disparities [1,2]. There is a large literature documenting disparities in PCa outcomes that is robust across multiple regions and sociodemographic profiles [3]. African American (AA) men, on average, have a 78% higher incidence of developing PCa in their lifetime compared to Non-Hispanic NHWs (NHW) [1,2,4,5,6,7]. Further, AAs are also more likely to be diagnosed at a younger age, present with more aggressive disease, and possess a 2.3 times higher mortality rate than their NHW counterparts [4,5,6]. Hispanics and some Asian groups have lower PCa incidence, however, they tend to suffer from more advanced disease at diagnosis [5,6,8]. PCa disparities are not only present across racial/ethnic attributes, but they are also significantly associated with the geographical place of residence. Hispanics living in Mexico have a lower incidence of PCa than Hispanics living in the Caribbean [9] while Puerto Ricans living in Puerto Rico have a lower incidence than Puerto Ricans living in the mainland United States [10].
In 2019, a systematic review compiling results from 169 international studies presented substantial evidence that PCa outcomes and management varied according to the place of residence across different populations and geographies [11]. Although this review summarized the two most important drivers of PCa disparities, which were rurality and area deprivation, various geographical approaches were utilized across the studies including multiple geographical scales and geospatial analyses which created a wide heterogeneity for study comparison [11]. Other reviews have been published around geographical approaches for prostate cancer research, however, none have reviewed the utilization of geographic information systems (GIS) as tools to advance PCa disparities research [12,13,14,15]. In fact, Obertova and Afshar focused their reviews on inconsistencies of rural/urban designation and its utilization within PCa disparity research [13,14], while Gilbert discussed GIS approaches, however only focusing on the state of Florida [15].
According to the National Cancer Institute, health disparities research is a growing area in research, and tools to identify and eliminate disparities are growing and encouraged in aims to identify pockets of disadvantage and map priority areas [16]. Geospatial analyses provide visual insights and substantial proof of the location of disparities and demonstrate their variability by adding a dynamic layer for traditional findings of disparities [17]. A new frontier of PCa research is the utilization of spatial approaches to identify focal points for interventions and resource mitigation and help outline underlying drivers of disparities [18].
Indeed, multiple approaches have been used to examine the association between geographical places of residence and PCa outcomes. Precisely, area-level characteristics and socioeconomic (SES) profiles have been linked to multiple disparities in PCa outcomes across various geographical scales such as county, census, census tracts, and others [19,20]. SES and demographics have also been linked to healthcare access and utilization of advanced PCa procedures [21,22,23]. Further, spatial approaches combine techniques from geography, epidemiology, and public health to better understand health needs and allocate resources [24]. This is especially relevant within the context of PCa disparities research which calls for multidimensional approaches to advance cancer health equity and reduce the persisting gap in outcomes [1]. As such, GIS applications may help expose the determinants of local and sociodemographic disparities and provide information to improve health service delivery models, training for healthcare professionals, and overall health outcomes [25].
GIS is defined as any technology, software, or hardware that enables the processing, mapping, and analysis of geographical variables [26,27]. Geographic Information Systems (GIS) research in PCa has been developing throughout time and branched into multiple applications such as processing, mapping, and analysis [18]. The ultimate success of GIS is when data is transformed into a useful representation that provides disease insights [28]. Such a collaborative approach delivers prospects to examine associations and connections within health outcomes, the contextual environment, and social determinants of health to advance cancer-related equity research [29]. This allowed the advancement of such tools with time and the development of a field named the Geographic Information Science (GIScience) [26], which examines the interdisciplinary collaborations aided by GIS to provide meaningful observations that have the potential to guide public health decision-making.
Furthermore, different geographical variables and various spatial scales have been adopted in aims to conduct such analyses and provide valuable data for public health interventions [30]. As such, geographical analyses in PCa outcomes have moved from the simple stratification of rural/urban continuum to computation of composite area deprivation indices within neighborhoods and utilization of GIS for cluster identification and prediction of poorer outcomes [31,32]. Those differences in approaches invite the need for methodological standardization when performing geospatial analyses to identify appropriate applications for Geographic Information Systems (GIS) in analyzing PCa disparities.
The main goal of this comprehensive review is to compile a resource for researchers interested in conducting geographical analyses for PCa disparities. This systematic review aims to summarize the literature about geospatial disparities in PCa, describe the different GIS applications utilized in relating place of residence with disparities in PCa outcomes, and identify gaps in the literature. This review also identifies current limitations for GIS application in PCa research and proposes alternative approaches. As such, this review provides a comprehensive assessment of methods and a valuable resource for researchers joining the increasing trend of analyzing disparities from a geographical perspective.
Methods
This paper follows the methods of the Cochrane Collaboration [33] and the criteria set of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [34] to report systematic reviews and meta-analyses. Articles published in scholarly (peer-reviewed) journals in English were searched through the PubMed, EMBASE, and Web of Science databases till December 2022.
Search Method
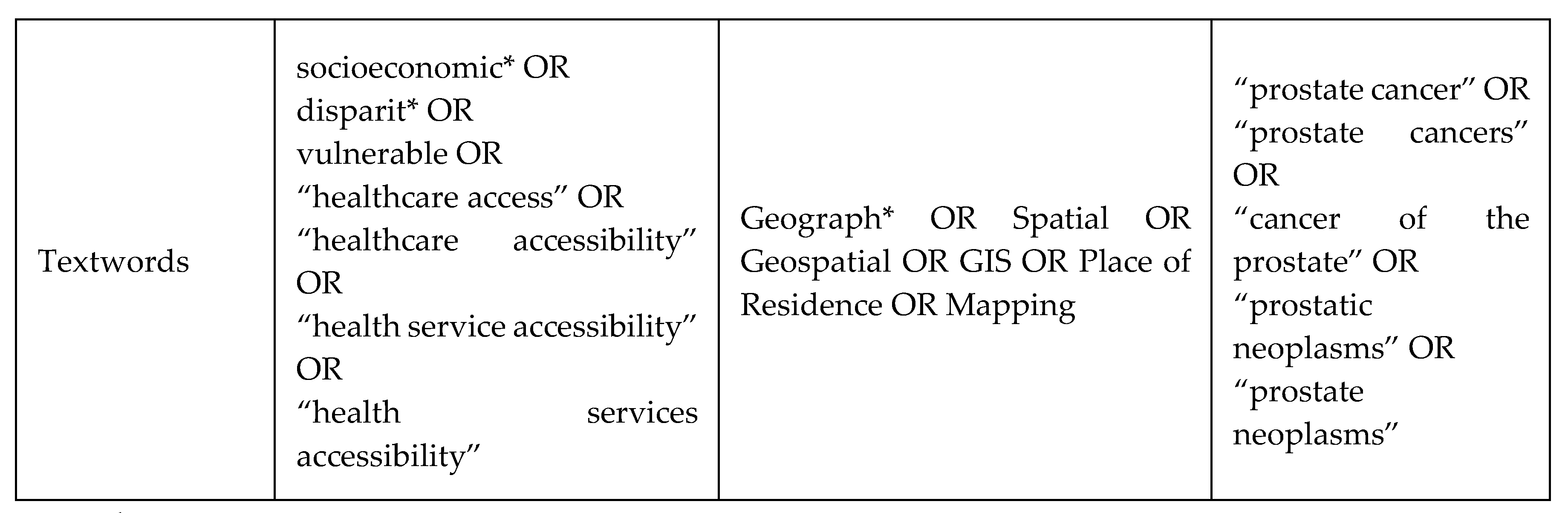
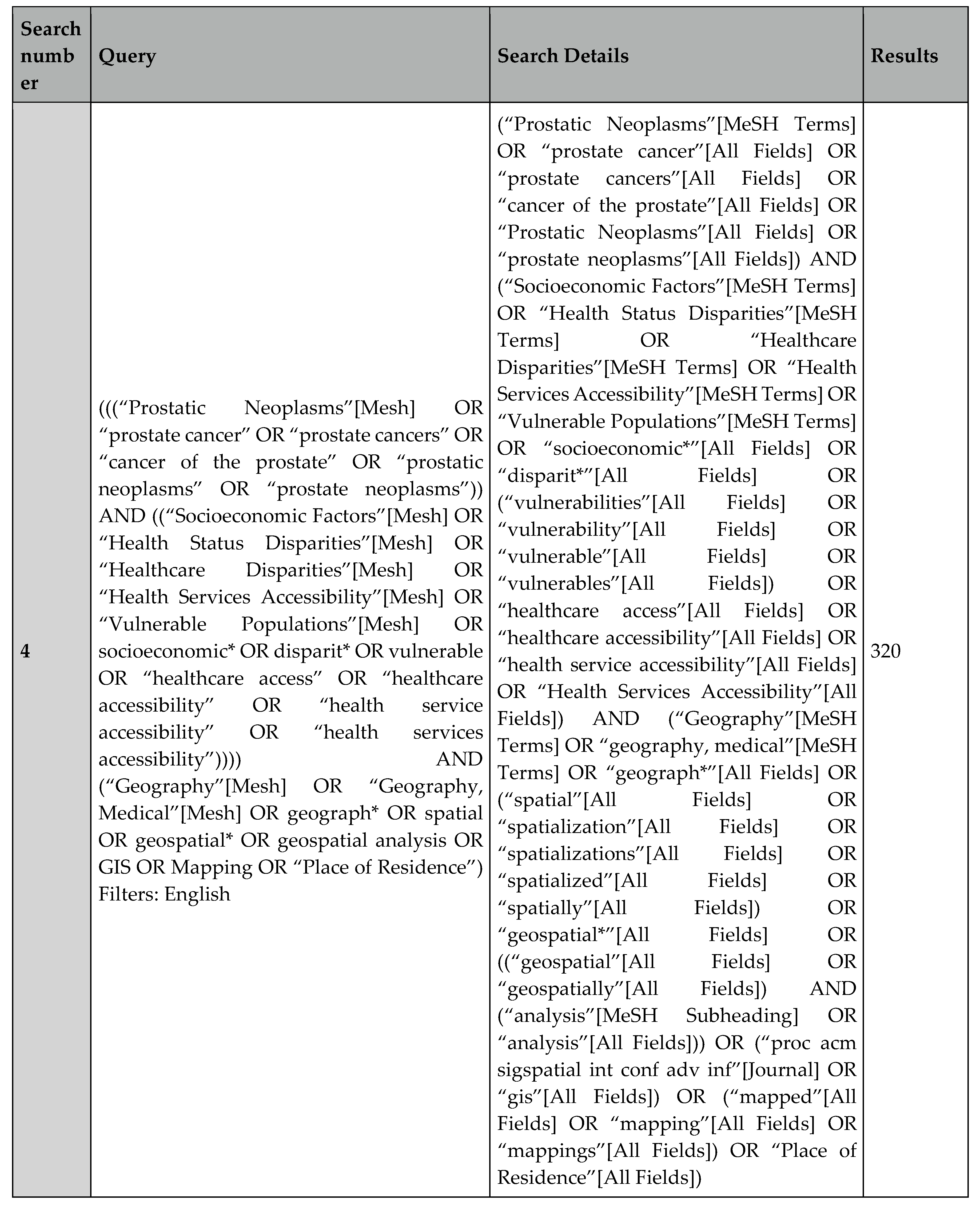
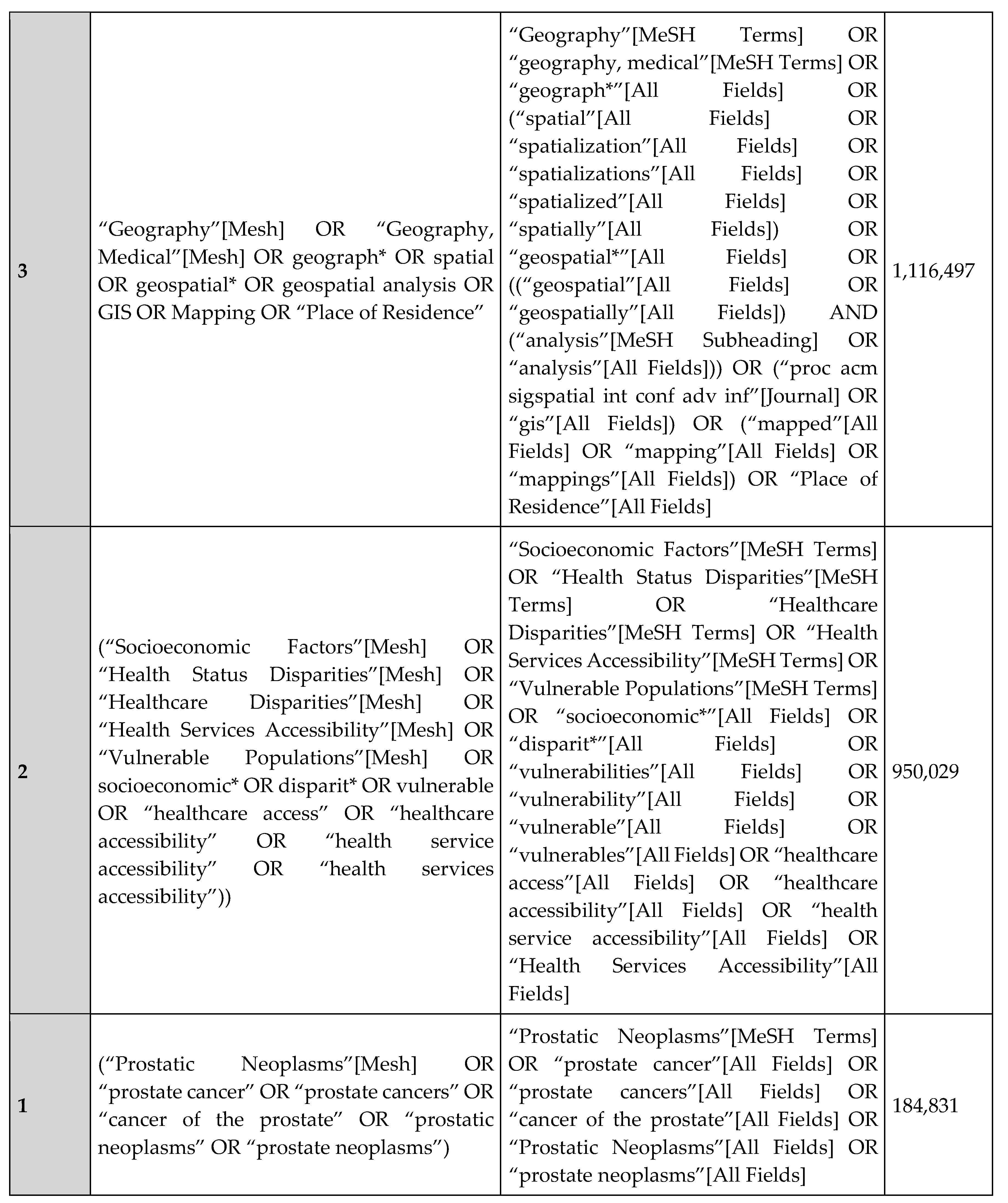
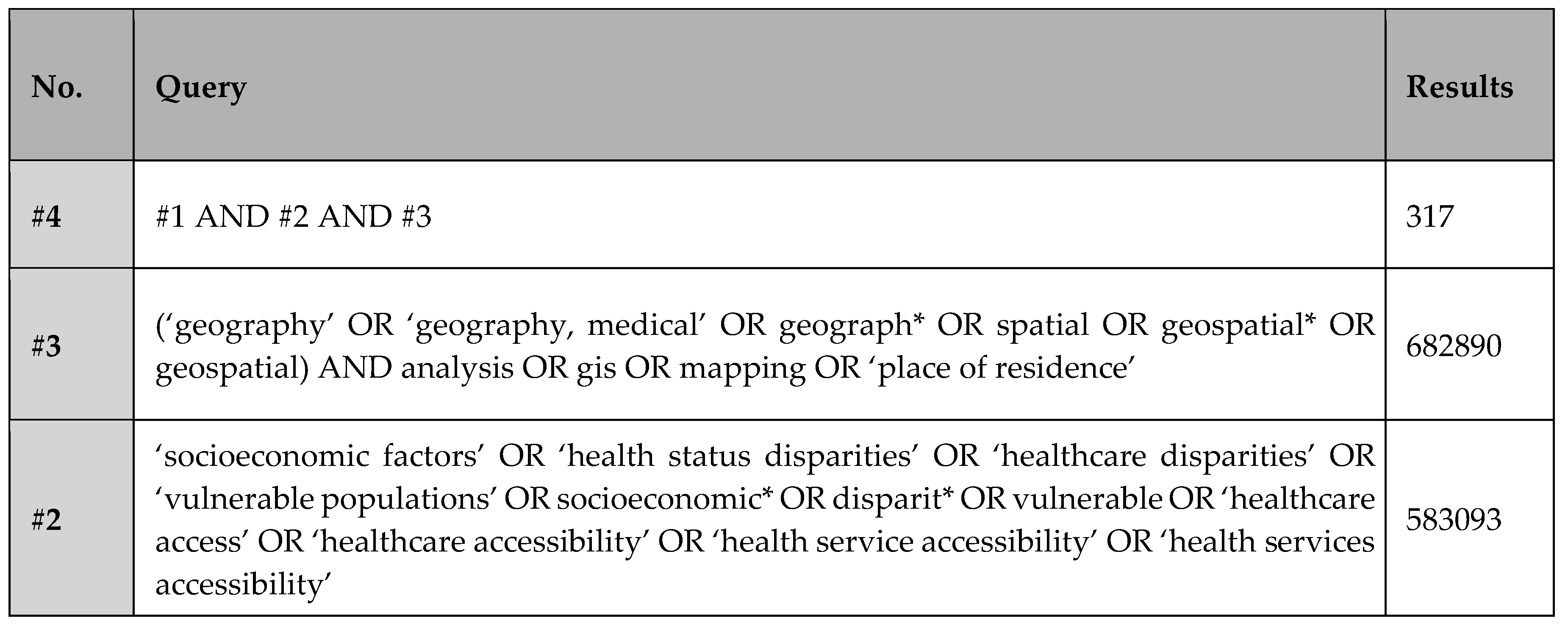
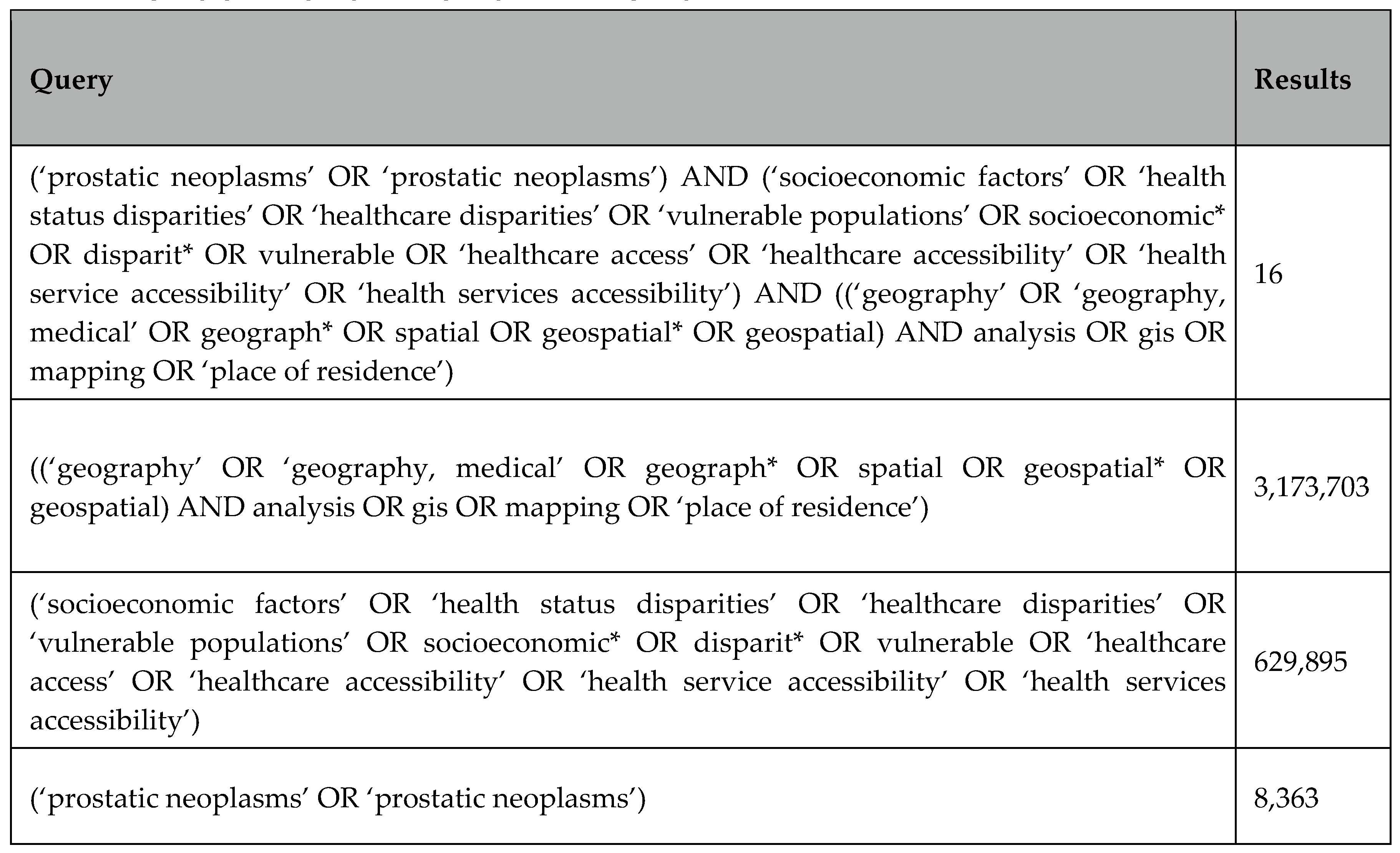
The main search terms (i.e., MeSH terms and keywords) focus on 1) GIS 2) disparities and inequities 3) prostate neoplasm. Three main databases were researched PubMed, EMBASE, and Web of Science [35,36,37], and a detailed research strategy is included in Appendix A.
Article Selection
The population-intervention-comparison-setting (PICOS) method [33] was used to determine the eligibility of studies. In our reviewed articles, the participants were “adult men in the US diagnosed with PCa”, the intervention was the GIS approach, comparative groups were men from varying demographic/socio-economic backgrounds, outcomes were PCa incidence, mortality, and survival, and/or PCa management, and finally studies included were observational. Eligible studies were all publications resulting from the database queries, referred publications known to the authors and others gathered from the reference lists of the identified publications. Out of these eligible publications, an article selection process according to specified inclusion and exclusion criteria was conducted. Included articles were those employing a GIS approach for examining the relationship between geographical components and PCa disparities and/or inequities in the United States. Studies that examined disparities in PCa outcomes using geographical elements as independent variables were included while studies conducted outside the US, those that are not published in the English language, and those that did not assess for a direct relationship between a geographical component and PCa disparities were excluded. No date restrictions were applied, and thus, the resulting articles were published through December 2022. The last date of search for relevant articles was December 31st, 2022.
Study Management
All included articles were rightfully downloaded, managed and screened using EndNote®. Six hundred and fifty-three publications were deemed eligible, all published between 1998 to 2022, including 247 duplicates. Articles were screened for eligibility based on title and abstract and 309 studies were disqualified due to the study setting not being in the US, not having an outcome of interest, and having no geographical component. After article selection according to the inclusion and exclusion criteria, 25 studies [38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62] met the requirements and were included in this review. Detailed reasons for full-text exclusions and the article selection process are represented in Figure 1. No potential biases were identified in the individual studies that met the inclusion criteria as all resulting studies were evaluated based on reproducibility, methodological quality, and credibility.
Due to the nature of the research question that aims at reviewing discovered geographical disparities in PCa, publication bias may have arisen. Likely, studies with no significant findings for disparities weren’t published and thus included publications overrepresented disparities. However, the large population-based studies in this review tend to limit this potential overrepresentation. This review followed the PRISMA checklist for evidence-based reporting and thus, principal summary measures were odds ratios, hazard ratios, relative risks, and differences in percentage along with their respective p-values.
Results
In this systematic review, a total of 25 studies were included, published from 2002 to 2022, those studies are detailed in Table 1. A total of six studies examined disparities in late-stage PC, six in incidence, four in mortality and survival, three in incidence, grade, and stage simultaneously, two in mortality-to-incidence (MIR) ratio, and two in PCa management (Table 1). GIS applications were grouped into three main application purposes: “mapping”, “processing”, and “analysis” (Table 1).
Summary of PCa Disparities Findings in GIS Studies
GIS studies that examined disparities in PCa incidence
GIS studies examining disparities in PCa mainly shared a common purpose of identifying locations of higher-than-expected incidence and examining their associations with contextual factors. For example, in Connecticut and Massachusetts, clusters of high PCa incidence were characterized by a better census-tract-level SES (less than 12 years schooling rate, below the poverty rate, renter-occupied dwellings rate, unemployment rates) mainly in NHWs as compared to AAs [40]. Similarly in Virginia, higher household income and urban residence increased the likelihood of diagnosis suggesting that better census-tract SES enhances healthcare access, especially for PCa screening [41]. Furthermore, residing in urban census tracts was associated with early-stage diagnosis, in a multi-state study conducted in Alabama, Tennessee, Georgia, and Florida [48]. Also in Georgia, Wagner et al. identified clusters of high PCa incidence that slightly differed in locations upon racial stratification suggesting the involvement of environmental predictors [53]. A novel approach was adopted by Gregorio et al., as they demonstrated that the “detection effect” through adjusting for colorectal cancer screening, accounted for all significant spatial variations in PCa incidence [54]. In Pennsylvania, the temporal decline in PCa incidence from 2000 to 2011 was suggested to illustrate the effect of the variation in PSA screening recommendations. Most notably, age at diagnosis was significantly younger in AAs as compared to NHWs, calling for increased attention in metropolitan Philadelphia areas where AAs are concentrated [56]. Mapping of PCa incidence in Alabama counties against rates of diabetes, obesity, education, and poverty, suggested an apparent association with those factors [61]. Accordingly, GIS studies examining disparities in PCa incidence suggested that higher PCa incidence may be associated with area-level racial composition, rurality, income, poverty, education, unemployment, percent renter-occupied dwellings, access to screening, and other chronic comorbidities.
GIS studies that Examined Disparities in PCa grade and Stage at Diagnosis
Having a “missing” stage and/or grade information from the tumor registry was utilized as a proxy for possible worse PCa outcomes. For example, Klassen et al. examined the relationship between missing stage and/or grade and area-level SES. As such, clusters of having a missing PCa stage or grade from the Maryland Tumor Registry were identified. Having a missing stage was associated with higher county-level household income while having a missing grade was associated with higher census block-group household income [39]. In Florida, northern and central counties exhibited the greatest racial disparities in late-stage PCa which was associated with lower census-tract income and lower college education [43]. Additionally, the late-stage proportions decreased significantly from 1981 to 2007, however, the rate of decline varied greatly based on county location and racial groups [49]. This variation was suggested to be related to geographical disparities in the implementation of the Prostate Specific Antigen (PSA) screening [52]. Upon racial stratification, more counties exhibited higher proportions of late-stage diagnosis in AAs versus NHWs. Associations were also detected on the census tract level as higher census tract income was protective while the presence of farmhouses increased the likelihood of a later stage diagnosis [49,55]. Moreover, a side-by-side mapping comparison of late-stage odds ratios (ORs) with comorbidities, income, and smoking rates at the county level, suggested that those could be associated with a later-stage diagnosis [55]. Thus, in addition to establishing relationships between later-stage diagnosis and poorer area-level SES, the temporal factor was also important to account for within this context, especially when it comes to varying PCa screening recommendations and clinical practices [63].
GIS studies that Examined Disparities in PCa Mortality and Survival
Using national data of PCa patients from 1970 to 1989, five national clusters of higher mortality in NHWs and three in AAs were detected, however, those could not be attributable to the selected county-level SES variables which included education and agricultural employment [38]. Identified geographical clusters of poorer PCa survival in Connecticut significantly diminished when individual-level variables representing age, race, and tumor severity (stage and grade) were accounted for suggesting that survival only varies in part according to the place of residence and other area-level factors might be predictors [42]. In Texas, counties with statistically significant excess mortality rates were found to be concentrated in the central state for multiple racial subgroups in a spatial and temporal analysis over a 22-year study period [44]. Meliker et al. identified survival disparities across the state of Michigan. Existing disparities identified at larger geographical scales Federal (House Legislative Districts (FHLD)) diminished and sometimes disappeared upon examination on smaller geographical scales (State House Legislative District (SHLD) and neighborhoods). This was attributed to the fact that, in smaller areas, the population at risk is more uniform in terms of modifiable SES, risk factors, and proximity to cancer screening [46]. In South Carolina, Hebert et al. mapped racially stratified MIRs across eight Department of Health and Environmental Control (DHEC) regions. Visualization on mapping presented striking differences between AAs and NHWs allowing for the localization of areas with the widest disparity gaps. MIR was also mapped per Zip Code Tabulation Area (ZCTA) in South Carolina for US Veterans where metropolitan MIR was found to be higher than non-metropolitan MIR and two clusters of higher-than-expected MIRs were detected in the Upstate region. In contrast to Hebert’s finding above, Georgantopoulos et al. found that AAs had a lower MIR than NHWs suggesting that Veterans exhibit a more uniform population for comparison and that factors causing such disparities are likely modifiable and related to healthcare access and SES [59]. Finally, PCa mortality hot spots were heavily concentrated in three major areas in Georgia. “Hot spot counties” generally had a higher proportion of AAs, older adult population, greater poverty, and more rurality [60]. Although area-level SES was shown to be associated with poorer PCa survival, including facility-level characteristics within GIS studies, as in Georgantopoulos’s study (2021) provided an additional layer for examining racial disparities in PCa.
GIS studies that Examined Disparities in PCa Management
Only two studies examined disparities in PCa management. Those mainly employed GIS mapping to identify visual associations between zip-code level factors and PCa treatment. Single institutional data was used to relate Stereotactic Body Radiation Therapy (SBRT) with zip-code level characteristics. The geospatial distance between the patient’s zip code and the facility was calculated and the geographical reach of the institution was assessed by examining the SES status for each zip code. Travel distance did not prevent uptake of prostate SBRT in AAs, elderly, or rural localized PCa cases [58]. A national GIS study examined disparities in PCa management using the National Medicare Database where PCa modalities were mapped across PCa cases county. Multivariate regression identified that practitioners of more novel modalities (i.e.,: SBRT and proton therapy) were mainly concentrated in zip codes that are more urban, while greater distance was associated with a significantly decreased probability of treatment (IMRT −3.8% per 10 miles; prostatectomy −2.1%; brachytherapy −2%; proton therapy −1.6%; and SBRT −1.1%) [62].
Application of GIS in PCa Disparities Research
All included studies shared a mutual rationale for GIS employment which was to identify geographic regions with the highest burden of PCa so that public health interventions can be prioritized. In this systematic review, three main purposes were identified for utilizing a GIS approach in studying PCa disparities: mapping, processing, and analysis. Mapping was employed in 24 studies, analysis in 16, and processing in 14 (Table 1). Those are described below and are represented in Figure 2.
Application of GIS in PCa Disparities Research: “Mapping”
All but one study [45] employed GIS techniques for mapping/visualization where PCa data were mostly translated into polygons of PCa measured in a certain geographical unit. The main purpose of creating maps was to provide a cartogenic representation of PCa rates and zones where poorer outcomes or higher disparities exist. Multiple software was utilized for mapping, however, ArcGIS remained the most utilized as it was employed by nine out of the 23 studies included and it is considered by many as the industry standard [64,65].
Mapping a Snapshot in Time: Qualitative and Quantitative Data
All studies presented maps with a single snapshot in time, mostly translating points to polygons as point data was aggregated to a certain designated geographical scale. The most common scale for mapping was “county” present in 12 studies. Remaining mapping was performed on the level of the census tract (in 3 studies )40, 41, 48]), zip codes (2 studies [58,59]), FHLD/SHLD/Neighborhoods (1 study [46]) and DHEC (1 study [47]), census block group (1 study [39]). For example, after acquiring individual-level data from the Virginia Cancer Registry, Oliver et al., geocoded data to the street level and assigned a census tract and a county for each case. As such, maps were reproduced displaying county-level and census tract-level PCa incidence. Such mapping helped to visually identify how disease rates changed from one zone to another. Consequently, PCa incidence was found to be the highest in the Eastern and Central portions of Virginia [41]. Such visual indicators can be the source of identifying locations where further analysis of contextual factors might be warranted.
Furthermore, both qualitative and quantitative PCa-related variables were represented (Figure 3). Eleven studies had both quantitative and qualitative maps while eight had only quantitative and six only qualitative. Qualitative mapping showed the spatial distribution of categorical, or nominal data such as rural/urban counties, or the presence or absence of certain outcomes, such as zones presenting significant disparities or clusters of a concentrated outcome (Figure 3). Conversely, quantitative mapping presented the spatial distribution of numeral data as most of those represented PCa rates, either for incidence, late stage, or mortality (Table 1). This kind of mapping was mainly used to identify locations with worse PCa outcomes or higher concentrations of the disease. For example, Jemal et al. mapped PCa mortality rates per county relying on the national cancer registry data. This approach was useful to identify and visualize counties with higher PCa mortality by comparing mortality rates across US counties (Figure 3A).
One of the uses for qualitative mapping was to illustrate the presence (or absence) of objective differences and/or inequities between specific subpopulations of interest. For example, Meliker et al. mapped locations with significant racial disparities in PCa survival to highlight areas of unequal PCa outcomes (Figure 3B) [46]. Qualitative mapping was also utilized to map contextual variables that help in understanding spatial circumstances under which PCa outcomes may be affected. This was especially valuable when qualitative information is visualized in parallel to PCa outcomes. For instance, Goovaerts et al., produced a qualitative map of rural/urban counties to obtain a visual representation of the associations between rural/urban places of residence and late-stage diagnosis (Figure 3C) [52].
Mapping Trends Overtime
Although mapping either qualitative or quantitative data in a time snapshot offers insightful visualization, including a temporal dimension ensured a more complete geographical analysis across the period studied. Hsu et al. included a temporal element in their mapping by reproducing maps showing excess PCa mortality across different time frames [44]. The inclusion of the temporal dimension allowed them to not only identify geographical clusters of worse PCa mortality but to also examine whether those clusters persisted over time. As such, their mapping identified three specific counties where excess mortality among Hispanics has been consistently present for over 19 years, calling public health policymakers to prioritize those areas based on spatiotemporal evidence [44]. Gooavert et al. [49, 51), furthered the inclusion of the temporal dimensions through 3-D mapping of PCa incidence and late-stage diagnosis [51]. Their three-dimensional model was created using SGeMS, the Stanford Geostatistical Modeling Software, where proportions of late-stage PCa were calculated over a 3-year moving window from 1982 to 2006 (Figure 3D). This mapping approach allowed the examination of how rates of late-stage disease responded to the 1990s introduction of Prostate Specific Antigen (PSA) testing, a blood test that facilitated PCa detection and early diagnosis. As such, including a temporal dimension while mapping PCa outcomes makes it easier to comprehend spatiotemporal relationships especially as significant approaches that affect clinical guidelines and health outcomes are continuously developing in PCa.
Application of GIS in PCa Disparities Research: “Processing”
Processing spatial data was mainly performed in 14 studies to prepare data for subsequent analyses and was grouped into geocoding and smoothing. (Table 1). Eight studies mentioned geocoding their data, six studies employed smoothing techniques, and two studies employed both (Table 1).
GIS Processing: Geocoding
Geocoding allowed the provision of geographical coordinates for participants’ addresses that were later used for mapping and allowed for individual-level variables to be represented on a location basis. Accordingly, addresses of PCa cases were geocoded into a specific location to facilitate spatial recognition patterns and allow for observational inferences. For example, Oliver et al. geocoded their PCa cases to the census tract using exact patient addresses which allowed examining associations between high PCa incidence and census-tract-level SES [41]. Another application of GIS processing is the transformation of certain point variables to aggregates which provided variable information for multiple geographical scales. For instance, Xiao et al. employed GIS processing to transform available latitude and longitudinal data into values per county to examine how county-level environmental factors affect PCa outcomes. In this case, geocoding assisted in preparing environmental data for county-level mapping and analysis by testing the relationship between county-level environmental factors and PCa stage/grade [43]. As such, GIS processing allows for scale transformation and the obtention of variables to the desired level of aggregation to be able to draw inferences between area-level characteristics and PCa outcomes.
Although geocoding enabled scaled visualization and data transformation, geocoding percentage, describing the successful conversion of addresses into a specific location, varied in between studies. Half of the studies that mentioned geocoding did not report the percentage of successful geocoding (Table 1). The geocoding success rate in the remaining half ranged between a low of 74% [41] to a high of 100% [47]. Note, geocoding success increased with the increasing size of the geographical scale as it moved from 74% upon geocoding to the census tract to 100% upon geocoding to the county [41].
GIS Processing: Smoothing
Data smoothing created an approximation function intended to capture patterns in the dataset and was mainly employed to reduce noise in the data by providing smoothed estimates (Figure 4). Goovaerts et al. performed binomial kriging to smooth rates of late-stage PCa to obtain smoother maps for late-stage diagnosis rates while Moore et al. (2022) employed the Spatial empirical Bayesian smoothing (SEBS) method to smooth mortality rates [60]. In both cases, smoothing was mainly utilized to approximate rates data and filter random noise so that clearer spatial patterns are observed.
An additional reason binomial kriging was performed is to replace missing values from the years where no PCa cases were diagnosed within specific locations in Florida [49]. Binomial kriging provided a measure of reliability called the kriging variance that allowed capitalizing on spatial autocorrelation and neighboring geographical units. This was followed by a sensitivity analysis which showed that kriging-based noise-filtering improved the fit of the joinpoint regression models (i.e., lower residual variability) compared to the modeling of raw rates. In this case, noise-filtered data also helped in providing a clearer detection of the variation in county-level late-stage diagnosis rates across racial groups and study period (Figure 4A) [49].
Moore et al. applied the SBES method to smooth PCa mortality rates and group them into quintiles. This distribution allowed for quintile-based quantitative mapping to identify and represent counties belonging to the poorest quintiles of PCa mortality (Figure 4B). Such an initial approach only provided information on how counties compare in terms of PCa outcomes, without identifying clusters or hot spots of concern [60]. On another hand, a weighted two-dimensional smoothing algorithm called “Headbanging” was performed on PCa incidence rates in Virginia (Figure 4C). This allowed for smoother mapping of PCa outcomes, allowing patterns to emerge from the data [41]. Lastly, the Inverse Distance Weighting (IDW) interpolation technique was performed to provide smoothed GIS mapping based on local odds ratios of highly aggressive PCa [57]. This technique created continuous and smoothed surfaces for the entire state of Pennsylvania based on the respondents’ addresses. This allowed the visualization of spatial patterns of the explanatory effect of the variable “race” as smoothed rates were racially stratified (Figure 4D).
Application of GIS in PCa Disparities Research: “Spatial Analysis”
Although mapping and processing may produce key visual insights, spatial associations can be examined by utilizing specific GIS analysis methods. In this systematic review, 16 studies applied GIS analysis to spatially analyze and interpret associations with PCa outcomes. Of those, four performed global spatial autocorrelation, 15 included a cluster identification approach, and one study employed a geographically weighted regression (Table 1).
GIS Analysis: Identification of Spatial autocorrelation
Spatial autocorrelation is the term used to describe the presence of systematic spatial variation in a variable and it’s the tendency for areas or sites that are close together to have similar values [66]. As Waldo Tobler’s first law of geography states: “Everything is related to everything else. But near things are more related than distant things” [67]. This was used as a key concept in geospatial research as it laid the rationale of spatial autocorrelation methods that test whether geographically closer zones have more of the same health outcomes profiles. Spatial autocorrelation indicated the presence of clustering or dispersion in a map, as such, examining the global spatial autocorrelation was used as an initial step for assessing overall geographical variability in the study area and has been performed in four out of the 25 studies included (Table 1). Three spatial tests were utilized to assess for global autocorrelation: the Global Moran’s I, Cuzick-Edwards’ k-NN, and Tango’s Maximized Excess Events Test MEET (Table 1).
Data from the Pennsylvania Cancer Registry was used to test for significant global autocorrelation using the global Moran’s I. The global Moran’s I statistics with 95% confidence intervals were calculated for each of the four time periods studied (2000-2002, 2003-2005, 2006-2008, and 2009-2011) and resulted in a non-significant negative value, indicating a non-significant negative spatial autocorrelation or a dispersed pattern in the data. As such, the authors’ interpretation included the presence of heterogenous dispersion of PCa incidence across counties which was also apparent on the quantitative mapping [56]. Similarly, a non-significant global Moran’s I (p=0.08) was also obtained upon testing for spatial autocorrelation of MIRs in South Carolina [59]. Despite the lack of statistically significant global heterogeneity, subsequent local cluster identification techniques detected two significant clusters of higher-than-expected MIRs [59]. Although examining global spatial autocorrelation was mainly utilized to test for general dispersion or clustering of the whole area of study, this approach did not eliminate the presence or absence of local PCa clusters.
A comparative study was performed to compare three different global spatial clustering techniques, utilized commonly in GIS research, to test for clustering in PCa stage and grade: Cuzick-Edwards’ k-NN, Global Moran’s I, and Tango’s Maximized Excess Events Test MEET [45]. Cuzick-Edwards’ k-NN and Moran’s I were found to be very sensitive to the population’s density, while MEET turned out to be the simplest to use as density does not need to be specified for the test. For the stage at diagnosis, all three models showed a reduction in clustering upon individual and area-level adjustments, however, some residual clustering remained. This study showed that, in addition to testing for global dispersion, those three global clustering techniques can be applied to check for residual clustering especially after adjusting for individual and area-level variables [45]. All in all, assessing for global clustering allows for identifying dispersion in overall PCa outcomes within spatial data. This initial step was important to understand the level of geographical heterogeneity of the PCa measure in question and elicited the need to adjust for underlying factors.
GIS Analysis: Cluster Identification
In addition to assessing for global spatial autocorrelation, GIS was utilized to identify clusters of concern in 14 studies, as this was often performed with the aim to identify and prioritize zones for public health interventions and/or locations that elicit further analyses (Table 1). Methods of cluster detection varied (Figure 5) as eight studies employed the Spatial Scan Statistic, two the local Moran I, two utilized a spatially weighted hierarchical cluster analysis, one performed a hot spot analysis coupled with the Spatial Scan Statistic, and another coupled with the local Moran’s I test (Table 1).
The Spatial Scan Statistic developed by Kulldorff [68] was commonly used to identify whether PCa outcomes were geographically randomly distributed or whether clusters were present. Within these studies, SatScan software was utilized to generate ellipses and/or circles of varying sizes and evaluate observed versus expected rate ratios (risk within vs outside the circles) to identify statistically significant “clusters” of disease rates [68]. Variations in the utilization of Kulldorff’s Spatial Scan Statistic were identified and described in Table 2. Six studies relied on circular scanning windows, one on both circular and elliptical, and two did not mention the scanning window shape employed. Variations in scanning window size also occurred as this was mostly dependent on the size of the population at risk (four studies) and on the study period (one study). Furthermore, the cluster delimitation approach was different among studies as five studies did not rely on geopolitical boundaries for cluster formation while three based their clusters on county and census tract boundaries (Table 2).
Although all studies utilizing the Spatial Scan Statistic shared a similar purpose, several rationales were employed. Some studies relied on racially stratifying cluster identification to highlight racial disparities in PCa outcomes. For example, four clusters of higher PCa incidence were detected in NHW while two clusters were detected in AA within the states of Connecticut and Massachusetts between 1994 and 1998 (Figure 5A) [40]. Other studies attempted to understand the underlying factors behind cluster formation by testing whether identified clusters remained after adjusting for designated factors. As an example, the number of significant clusters diminished when adjusting for individual-level variables such as race, age, and year and census-tract level SES. This approach explained the potential variables affecting cluster formation as older age, black race, and higher county-level income increased the likelihood of missing stage while older age and higher block-group income increased the likelihood of missing grade [39]. Similarly, the number of clusters of poorer PCa survival decreased in Connecticut upon adjusting for disease severity. However, the fact that some of those clusters remained demonstrated that additional factors, not accounted for in the study, were contributing to worse PCa prognosis [42]. Another approach for employing cluster identification was to profile the SES characteristics of the identified clusters in order to understand the relationship between poorer outcomes and area-level variables within those specific geographical boundaries. For example, Altekruse et al. focused on gathering clusters of higher PCa incidence to examine the relationship between high incidence within those boundaries and area-level SES utilizing the Pearson correlation test [48]. This resulted in significant associations between a higher relative risk of localized PCa and urban locations as well as a higher AA proportions [48].
The Getis-Ord-Gi technique developed by Getis and Ord in 1992 was also used to identify hot spots of concentrated disease outcomes [69]. In contrast to clusters identified by the Spatial Scan Statistic, this approach mainly identified “cooler” or “hotter” zones of the designated outcome in question. For example, in the state of Georgia, Wagner et al. analyzed county-level hotspots of PCa incidence with the Getis-Ord-Gi statistic and identified census-tract level clusters using the Spatial Scan Statistic. The rationale behind this dual cluster identification approach was primarily to identify counties with the highest PCa incidence and delineate clusters of higher incidence within smaller geographical areas [53]. Another county-level hot spot analysis was performed also in Georgia to detect counties with the highest PCa mortality (Figure 5C). Such an analysis was then racially stratified to compare racial disparities in PCa mortality. The identified hot spot counties were then analyzed for SES characteristics and found to have a higher AA proportion and lower median household income when compared with non-hot spot counties [60].
Furthermore, three studies employed the local Moran’s I to identify Local Indicators of Spatial Autocorrelations (LISA) (Table 1). LISA was used to identify significant clusters of Pennsylvania counties with either higher or lower PCa incidence as well as counties that differed significantly from their neighboring counties, representing either a “high-low” or “low-high” geographical cluster (Figure 5). In addition to identifying low and high-incidence counties, LISA provided information on how a specific location compared with its surroundings (Figure 5B). The analysis was repeated for four different time periods to understand the temporal variation of identified clusters [56]. Lastly, two studies employed the spatially weighted hierarchical cluster analysis using Ward’s minimum variance to group counties that have similar temporal trends of late-stage incidence rates in the state of Florida. This was mainly performed to examine the temporal and spatial clustering of late-stage proportions, especially since screening recommendations were introduced during the study period (Figure 5D) [51,52].
GIS Analysis: Geographically Weighted Regression (GWR)
Only a single study employed GWR (Table 1) which provided a spatial dimension to traditional measures of associations. A geographically weighted local logistic regression model was used to investigate how the covariate effects on PCa outcome changed spatially by considering spatial dependence. In fact, higher weight was assigned to cases that were geographically closer to each other to account for spatial dependence. This method was mainly applied to represent how associations between predictors and PCa outcomes vary geographically. For example, Goovaerts et al. identified specific areas where the risk of advanced PCa is more sensitive to the census-tract median household income [55].
Discussion
This systematic review is the first to comprehensively summarize GIS applications in prostate cancer (PCa) disparities research. Unlike previous reviews that focused on geographical variability in PCa outcomes and associations with predictors, this review emphasizes the utility of GIS [11,12,14,18]. GIS’s interdisciplinary approach is crucial for addressing disparities in PCa outcomes [6,70].
Main Themes and Findings
GIS applications in PCa disparities research fall into three main themes: mapping, processing, and analysis. Most studies (23 out of 25) utilized GIS to examine PCa incidence, mortality, and survival rather than treatment and management. The primary rationale was to visualize and statistically identify geographical areas with poorer PCa outcomes, aiding in policy and public health intervention prioritization. Policymakers could also benefit from identifying disparities in healthcare access, as disparities in procedure utilization and PCa management contribute to worse outcomes [20,21,22,71]. A clear limitation in examining PCa management outcomes in GIS research is the databases used. Including databases with procedure information, such as SEER-Medicare [72] or SPARCS [73], could enhance GIS research by visualizing healthcare access disparities and associating them with outcomes. Despite this, cancer registry data linked to census data proved valuable for examining PCa outcomes and area-level characteristics (Table 1).
Specific GIS Applications in PCa Management
Two studies focused on PCa management, using GIS for mapping and regression analyses to explore the relationship between radiation therapy uptake, travel distance, and socioeconomic status (SES) [58,62]. Aghdam et al. mapped SES clusters of patients receiving radiation therapy [58], while Tang et al. mapped PCa treatment modalities by county [62]. Other studies also examined the impact of travel distance on treatment utilization, finding that longer distances were associated with lower radiation therapy likelihood [74,75] and increased advanced-stage PCa rates among African Americans [76]. Dobbs et al. used Google Distance Matrix API to calculate transit times and their impact on clinic absenteeism, finding driving distance inversely associated with missed appointments [77]. This approach could help study the impact of distance and time on healthcare access among PCa patients. Combining procedure uptake information with analytical GIS approaches could provide insights into healthcare access for PCa patients. Such approaches have been used to study spatial variation and identify clusters in other diseases, such as malignancies and vaccine uptake [78,79,80]. For example, Zahnd et al. performed hotspot analysis and spatial lag models to detect low mammography access clusters and identify associated sociodemographic factors [80]. Translating these approaches to PCa procedure uptake, such as multiparametric MRI for advanced diagnosis and detection, could advance understanding of PCa disparities. This is crucial as PCa is a screenable and highly curable disease when appropriate screening and management are undertaken.
Multilevel Analyses in GIS Research
Four studies successfully integrated GIS with multilevel analyses, an essential approach given the complex relationship between race/ethnicity and area-level SES in PCa disparities [81,82,83]. Klassen et al. identified high PCa grade and stage clusters and evaluated variability before and after adjusting for census-level characteristics [39]. This approach helps determine the contribution of multileveled factors to spatial clusters and identifies areas for additional localized investigations. Similarly, Altekruse’s study further examined identified clusters for local associations with area-level factors [48].
Limitations and Recommendations
Several limitations and recommendations from this review are detailed in Table 3.
GIS Mapping and Scale Definition: Almost all studies (24/25) used mapping to visually represent associations between geography and PCa. However, varying geographical scales were adopted, resulting in different findings [41,43,46]. County-level data was most commonly used due to ease of access. However, multiple scales within studies introduced challenges in disentangling personal choice from contextual factors. For example, Meliker et al. observed disappearing survival disparities between NHW and AAs when moving from larger to smaller geographical scales [46]. Oliver et al. detected significant SES associations with PCa outcomes at the census tract level but not at the county level [41]. This phenomenon, known as the Modifiable Areal Unit Problem (MAUP), introduces statistical bias. The recommended geographical scale depends on the research question. Smaller scales might better capture associations with area-level indicators, while larger scales might better detect disparities between geographical areas. To mitigate MAUP, using original point data or smaller units of analysis (e.g., “County” instead of “State”) and performing sensitivity analyses for each geographical scale are suggested [86]. Luo et al. demonstrated the context-dependency of aggregation error using a Monte Carlo simulation, emphasizing the importance of population density consideration [88].
GIS Processing: Geocoding quality and data smoothing were the main GIS processing applications identified. Only eight studies reported geocoding, with success rates varying between 74% and 100% (Table 1). Standardized geocoding approaches, such as those by NAACCR, are recommended to improve outcome comparability [89]. Insufficient geocoding can lead to systematically missing data, misinforming public health interventions. This was illustrated by Oliver et al., who showed how varying geocoding quality resulted in different cluster formations for PCa patients (Figure 6) [90]. Smoothing techniques help aggregate results of adjacent areas with scarce or missing data but can introduce bias if over-applied. Proper use of smoothing techniques can fill gaps, reduce bias, and prepare data for spatial analysis.
GIS Analysis: GIS applications enable rapid spatial analysis of PCa outcomes. Spatial autocorrelation is crucial for examining the impact of space on PCa observations. Three spatial autocorrelation approaches were identified: Global Moran’s I, Tango’s MEET, and Cuzick-Edward’s k-NN. Global Moran’s I is commonly used to test for global spatial autocorrelation, but the Geary’s c test could also be employed [95]. The absence of global spatial autocorrelation does not imply the absence of localized spatial patterns. Cluster detection methods varied, with the Spatial Scan Statistic (SSS), Local Indicator of Spatial Autocorrelation (LISA), and hotspot analysis using the Getis-Ord-Gi statistic being the primary techniques. Variations in SSS model specifications highlight the need for standardization. LISA is more sensitive and specific in cluster detection but increases Type I error with more cases. Hotspot analysis provides color-scaled visual representations of cold and hot spots but is limited by pre-defined geographical boundaries. Combining multiple geospatial approaches, such as hotspot analysis and LISA, is recommended for robust findings. A table summarizing the strengths and weaknesses of the different GIS analysis methods utilized in PCa research is presented below (Table 4).
Future Recommendations for GIS Application in PCa Research
Future GIS research in PCa disparities should focus on several key areas to enhance the scope and impact of findings:
- Expanding the scope to include treatment and management outcomes is crucial. Utilizing comprehensive databases like SEER-Medicare and SPARCS for procedure-level information will provide valuable insights into healthcare access and utilization, leading to a more holistic understanding of PCa disparities.
- Incorporating both spatial and temporal dimensions in GIS research will allow for a more comprehensive assessment of the cancer burden. This can be achieved through preliminary stratification, joinpoint analysis, or detailed discussions that account for ongoing medical advancements and changes in screening recommendations.
- Ensuring racial inclusivity in study populations is also vital. Future research should extend beyond African Americans (AAs) and Non-Hispanic Whites (NHWs) to include other minority groups such as Non-Hispanic Asian/Pacific Islanders (NHAPI). This will provide a broader understanding of racial disparities in PCa outcomes.
- Combining multiple geospatial approaches for robust cluster detection and sensitivity analysis will enhance the reliability and validity of research findings. Employing techniques like Spatial Scan Statistic (SSS), Local Indicator of Spatial Autocorrelation (LISA), spatial oblique decision trees (SpODT), and hierarchical Bayesian spatial modeling (HBSM) will offer a comprehensive view of spatial patterns and their underlying causes.
- Addressing geocoding quality and the Modifiable Areal Unit Problem (MAUP) is essential. Researchers should adhere to standardized geocoding principles and report geocoding success rates. Conducting sensitivity analyses across different geographical scales and using original point data when possible will mitigate issues related to MAUP and enhance the robustness of findings.
By addressing these recommendations, future GIS research can leverage spatial analysis to design effective public health interventions, ultimately reducing disparities in PCa outcomes. Including visual aids such as tables and figures can further enhance the clarity of the discussion. For example, a table summarizing the strengths and weaknesses of different GIS methods, a visual representation of geographical scales and their impact on findings, and a flowchart of recommended GIS approaches for PCa disparities research can make the information more digestible. Following these recommendations will ensure that future GIS studies in PCa disparities are more robust, comprehensive, and impactful.
Study Strengths and Limitations
To my knowledge, this is the first systematic review of GIS applications within PCa disparities research. This review is unique as it provided a comprehensive summary of spatial analysis within this disease, highlighted the importance of specific methods in relation to PCa outcomes, and discussed potential gaps while proposing potential solutions. A GIS approach for PCa disparities is crucial for designing efficient and targeted public health interventions. Although this review contains valuable information for future researchers joining the rising trend of GIS research and disparities, few limitations were encountered. Limitations mainly include the search terms used to select the articles. Some used terms might have been new to the literature, and thus historical articles describing the same initiative might have been missed by using obsolete terminology. Also, selections have been restricted to published articles only. By doing so, valuable unpublished findings might have been missed, especially since this area of research is evolving rapidly nowadays.
Conclusions
This review highlights current trends in GIScience for PCa surveillance and epidemiology, categorizing GIS approaches into processing, mapping, and analysis. Mapping enables visualization of PCa rates and disparities, processing involves geocoding and rate smoothing, and analysis identifies clusters for public health interventions. Limitations were noted in each area, with recommendations to expand GIS research to address healthcare access disparities, justify scale selections, and combine cluster detection methods for improved accuracy. The review emphasizes interdisciplinary collaboration to enhance PCa disparity studies, guiding future public health and policy interventions effectively.
Funding
No funding was utilized for this research.
Data Availability Statement
The full search strategy is included in the appendix and can be applied for future reproducibility.
Conflicts of Interest
No conflicts of interest exist, and no disclosures are to be mentioned.
Appendix A. Research Strategy
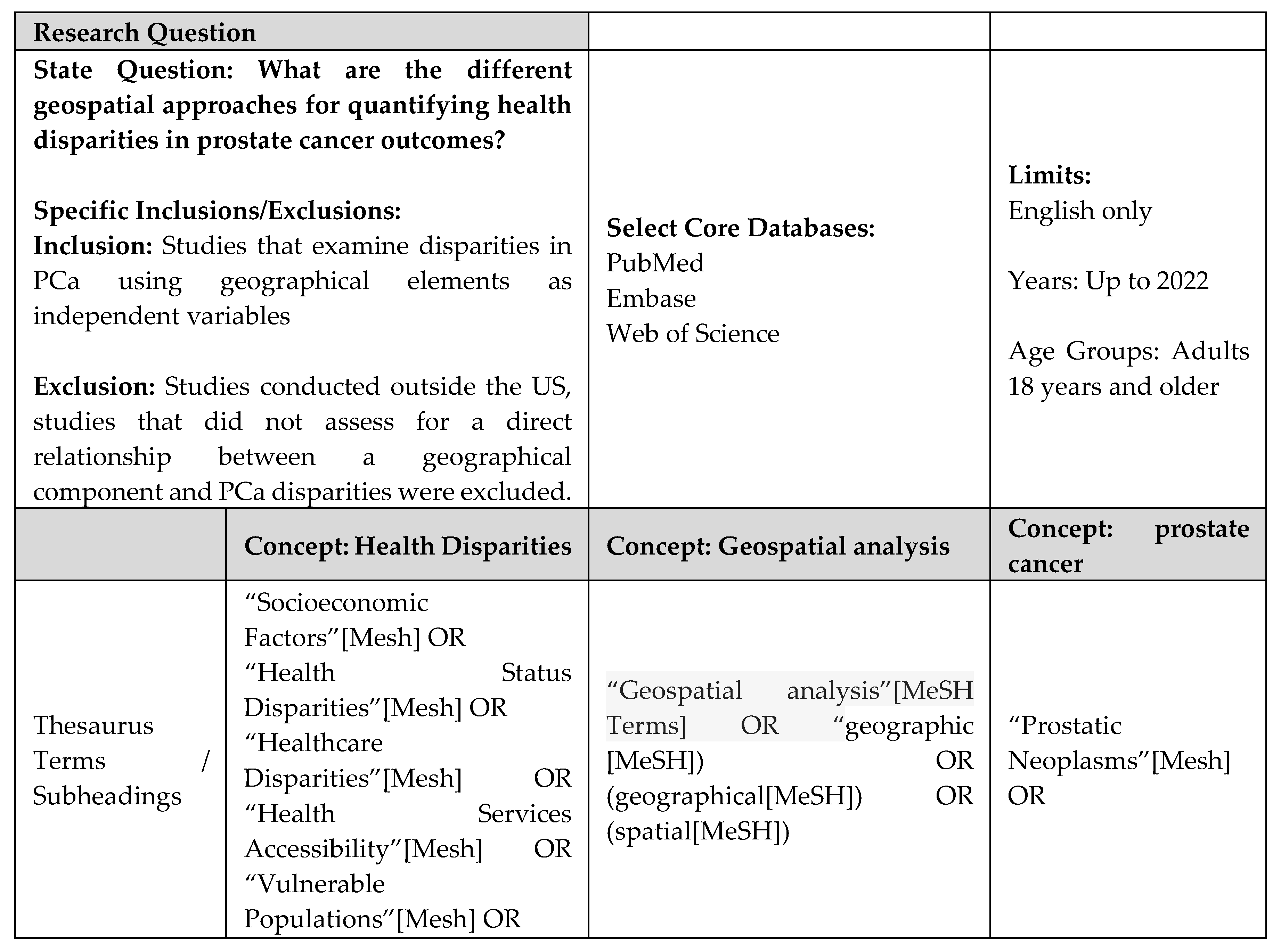
PubMED SEARCH STRATEGIES
EMBASE SEARCH STRATEGIES

WEB OF SCIENCE SEARCH STRATEGIES
References
- Zavala VA, Bracci PM, Carethers JM, Carvajal-Carmona L, Coggins NB, Cruz-Correa MR, et al. Cancer health disparities in racial/ethnic minorities in the United States. Br J Cancer. 2021;124(2):315-32. [CrossRef] [PubMed] [PubMed Central]
- Rawla P. Epidemiology of Prostate Cancer. World J Oncol. 2019;10(2):63-89. [CrossRef] [PubMed] [PubMed Central]
- Coughlin SS. A review of social determinants of prostate cancer risk, stage, and survival. Prostate Int. 2020;8(2):49-54. [CrossRef] [PubMed] [PubMed Central]
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7-30. [CrossRef] [PubMed]
- DeSantis CE, Miller KD, Goding Sauer A, Jemal A, Siegel RL. Cancer statistics for African Americans, 2019. CA Cancer J Clin. 2019;69(3):211-33. [CrossRef] [PubMed]
- Chornokur G, Dalton K, Borysova ME, Kumar NB. Disparities at presentation, diagnosis, treatment, and survival in African American men, affected by prostate cancer. Prostate. 2011;71(9):985-97. [CrossRef] [PubMed] [PubMed Central]
- Dess RT, Hartman HE, Mahal BA, Soni PD, Jackson WC, Cooperberg MR, et al. Association of Black Race With Prostate Cancer-Specific and Other-Cause Mortality. JAMA Oncol. 2019;5(7):975-83. [CrossRef] [PubMed] [PubMed Central]
- Tyson MD, 2nd, Castle EP. Racial disparities in survival for patients with clinically localized prostate cancer adjusted for treatment effects. Mayo Clin Proc. 2014;89(3):300-7. [CrossRef] [PubMed]
- Pinheiro PS, Sherman RL, Trapido EJ, Fleming LE, Huang Y, Gomez-Marin O, et al. Cancer incidence in first generation U.S. Hispanics: Cubans, Mexicans, Puerto Ricans, and new Latinos. Cancer Epidemiol Biomarkers Prev. 2009;18(8):2162-9. [CrossRef] [PubMed]
- Ho GY, Figueroa-Valles NR, De La Torre-Feliciano T, Tucker KL, Tortolero-Luna G, Rivera WT, et al. Cancer disparities between mainland and island Puerto Ricans. Rev Panam Salud Publica. 2009;25(5):394-400. [CrossRef] [PubMed]
- Dasgupta P, Baade PD, Aitken JF, Ralph N, Chambers SK, Dunn J. Geographical Variations in Prostate Cancer Outcomes: A Systematic Review of International Evidence. Front Oncol. 2019;9:238. [CrossRef] [PubMed] [PubMed Central]
- Baade PD, Yu XQ, Smith DP, Dunn J, Chambers SK. Geographic disparities in prostate cancer outcomes--review of international patterns. Asian Pac J Cancer Prev. 2015;16(3):1259-75. [CrossRef] [PubMed]
- Obertova Z, Brown C, Holmes M, Lawrenson R. Prostate cancer incidence and mortality in rural men--a systematic review of the literature. Rural Remote Health. 2012;12(2):2039. [PubMed]
- Afshar N, English DR, Milne RL. Rural-urban residence and cancer survival in high-income countries: A systematic review. Cancer. 2019;125(13):2172-84. [CrossRef] [PubMed]
- Gilbert SM, Pow-Sang JM, Xiao H. Geographical Factors Associated With Health Disparities in Prostate Cancer. Cancer Control. 2016;23(4):401-8. [CrossRef] [PubMed]
- Research NCIGPfC. Health Disparities Information. https://giscancergov/research/health_disparitieshrml.
- Cobb CD. Geospatial Analysis: A New Window Into Educational Equity, Access, and Opportunity. Review of Research in Education. 04/21/2020;Volume 44, Issue 1. [CrossRef]
- Adebola TM, Fennell HWW, Druitt MD, Bonin CA, Jenifer VA, van Wijnen AJ, et al. Population-Level Patterns of Prostate Cancer Occurrence: Disparities in Virginia. Curr Mol Biol Rep. 2022;8(1):1-8. [CrossRef] [PubMed] [PubMed Central]
- Freeman VL, Ricardo AC, Campbell RT, Barrett RE, Warnecke RB. Association of census tract-level socioeconomic status with disparities in prostate cancer-specific survival. Cancer Epidemiol Biomarkers Prev. 2011;20(10):2150-9. [CrossRef] [PubMed] [PubMed Central]
- Washington C, Deville C, Jr. Health disparities and inequities in the utilization of diagnostic imaging for prostate cancer. Abdom Radiol (NY). 2020;45(12):4090-6. [CrossRef] [PubMed]
- Ajayi A, Hwang WT, Vapiwala N, Rosen M, Chapman CH, Both S, et al. Disparities in staging prostate magnetic resonance imaging utilization for nonmetastatic prostate cancer patients undergoing definitive radiation therapy. Adv Radiat Oncol. 2016;1(4):325-32. [CrossRef] [PubMed] [PubMed Central]
- El Khoury CJ, Ros PR. A Systematic Review for Health Disparities and Inequities in Multiparametric Magnetic Resonance Imaging for Prostate Cancer Diagnosis. Acad Radiol. 2021;28(7):953-62. [CrossRef] [PubMed]
- Orom H, Biddle C, Underwood W, 3rd, Homish GG, Olsson CA. Racial or Ethnic and Socioeconomic Disparities in Prostate Cancer Survivors’ Prostate-specific Quality of Life. Urology. 2018;112:132-7. [CrossRef] [PubMed] [PubMed Central]
- Beale L, Abellan JJ, Hodgson S, Jarup L. Methodologic issues and approaches to spatial epidemiology. Environ Health Perspect. 2008;116(8):1105-10. [CrossRef] [PubMed] [PubMed Central]
- Seidman CS. An introduction to prostate cancer and geographic information systems. Am J Prev Med. 2006;30(2 Suppl):S1-2. [CrossRef] [PubMed]
- DM M. Geographic information science: defining the field. In: Duckham M, Goodchild MF, Worboys MF, eds Foundations of Geographic Information Science New York: Taylor & Francis; 2003:3-18. 2003.
- University Consortium for Geographic Information Science (UCGIS). UCGIS bylaws. 2016 version. Washington, DC: UCGIS; 2016 Available at: http://wwwucgisorg/assets/docs/ucgis_bylaws_march2016pdf.
- Sahar L, Foster SL, Sherman RL, Henry KA, Goldberg DW, Stinchcomb DG, et al. GIScience and cancer: State of the art and trends for cancer surveillance and epidemiology. Cancer. 2019;125(15):2544-60. [CrossRef] [PubMed] [PubMed Central]
- Elliott P, Wartenberg D. Spatial epidemiology: current approaches and future challenges. Environ Health Perspect. 2004;112(9):998-1006. [CrossRef] [PubMed] [PubMed Central]
- Lyseen AK, Nohr C, Sorensen EM, Gudes O, Geraghty EM, Shaw NT, et al. A Review and Framework for Categorizing Current Research and Development in Health Related Geographical Information Systems (GIS) Studies. Yearb Med Inform. 2014;9(1):110-24. [CrossRef] [PubMed] [PubMed Central]
- DeRouen MC, Schupp CW, Koo J, Yang J, Hertz A, Shariff-Marco S, et al. Impact of individual and neighborhood factors on disparities in prostate cancer survival. Cancer Epidemiol. 2018;53:1-11. [CrossRef] [PubMed] [PubMed Central]
- DeRouen MC, Schupp CW, Yang J, Koo J, Hertz A, Shariff-Marco S, et al. Impact of individual and neighborhood factors on socioeconomic disparities in localized and advanced prostate cancer risk. Cancer Causes Control. 2018;29(10):951-66. [CrossRef] [PubMed] [PubMed Central]
- Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare support from the Cochrane Collaboration for the development and evaluation of the tool described; they have no financial relationships with any organisations that might have an interest in the submitted work in the previous three years and no other relationships or activities that could appear to have influenced the submitted work. [CrossRef] [PubMed] [PubMed Central]
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700. [CrossRef] [PubMed] [PubMed Central]
- PubMED. https://pubmedncbinlmnihgov.
- EMBASE. https://wwwembasecom/landing?status=grey.
- Web of Science - Clarivate. https://wwwwebofsciencecom/wos/woscc/basic-search.
- Jemal A, Kulldorff M, Devesa SS, Hayes RB, Fraumeni JF, Jr. A geographic analysis of prostate cancer mortality in the United States, 1970-89. Int J Cancer. 2002;101(2):168-74. [CrossRef] [PubMed]
- Klassen AC, Kulldorff M, Curriero F. Geographical clustering of prostate cancer grade and stage at diagnosis, before and after adjustment for risk factors. Int J Health Geogr. 2005;4(1):1. [CrossRef] [PubMed] [PubMed Central]
- DeChello LM, Gregorio DI, Samociuk H. Race-specific geography of prostate cancer incidence. Int J Health Geogr. 2006;5:59. [CrossRef] [PubMed] [PubMed Central]
- Oliver MN, Smith E, Siadaty M, Hauck FR, Pickle LW. Spatial analysis of prostate cancer incidence and race in Virginia, 1990-1999. Am J Prev Med. 2006;30(2 Suppl):S67-76. [CrossRef] [PubMed]
- Gregorio DI, Huang L, DeChello LM, Samociuk H, Kulldorff M. Place of residence effect on likelihood of surviving prostate cancer. Ann Epidemiol. 2007;17(7):520-4. [CrossRef] [PubMed]
- Xiao H, Gwede CK, Kiros G, Milla K. Analysis of prostate cancer incidence using geographic information system and multilevel modeling. J Natl Med Assoc. 2007;99(3):218-25. [PubMed] [PubMed Central]
- Hsu CE, Mas FS, Miller JA, Nkhoma ET. A spatial-temporal approach to surveillance of prostate cancer disparities in population subgroups. J Natl Med Assoc. 2007;99(1):72-80, 5-7. [PubMed] [PubMed Central]
- Hinrichsen VL, Klassen AC, Song C, Kulldorff M. Evaluation of the performance of tests for spatial randomness on prostate cancer data. Int J Health Geogr. 2009;8:41. [CrossRef] [PubMed] [PubMed Central]
- Meliker JR, Goovaerts P, Jacquez GM, Avruskin GA, Copeland G. Breast and prostate cancer survival in Michigan: can geographic analyses assist in understanding racial disparities? Cancer. 2009;115(10):2212-21. [CrossRef] [PubMed] [PubMed Central]
- Hebert JR, Daguise VG, Hurley DM, Wilkerson RC, Mosley CM, Adams SA, et al. Mapping cancer mortality-to-incidence ratios to illustrate racial and sex disparities in a high-risk population. Cancer. 2009;115(11):2539-52. [CrossRef] [PubMed] [PubMed Central]
- Altekruse SF, Huang L, Cucinelli JE, McNeel TS, Wells KM, Oliver MN. Spatial patterns of localized-stage prostate cancer incidence among white and black men in the southeastern United States, 1999-2001. Cancer Epidemiol Biomarkers Prev. 2010;19(6):1460-7. [CrossRef] [PubMed] [PubMed Central]
- Goovaerts P, Xiao H. Geographical, temporal and racial disparities in late-stage prostate cancer incidence across Florida: a multiscale joinpoint regression analysis. Int J Health Geogr. 2011;10:63. [CrossRef] [PubMed] [PubMed Central]
- Xiao H, Tan F, Goovaerts P. Racial and geographic disparities in late-stage prostate cancer diagnosis in Florida. J Health Care Poor Underserved. 2011;22(4 Suppl):187-99. [CrossRef] [PubMed] [PubMed Central]
- Goovaerts P, Xiao H. The impact of place and time on the proportion of late-stage diagnosis: the case of prostate cancer in Florida, 1981-2007. Spat Spatiotemporal Epidemiol. 2012;3(3):243-53. [CrossRef] [PubMed] [PubMed Central]
- Goovaerts P. Analysis of geographical disparities in temporal trends of health outcomes using space-time joinpoint regression. Int J Appl Earth Obs Geoinf. 2013;22:75-85. [CrossRef] [PubMed] [PubMed Central]
- Wagner SE, Bauer SE, Bayakly AR, Vena JE. Prostate cancer incidence and tumor severity in Georgia: descriptive epidemiology, racial disparity, and geographic trends. Cancer Causes Control. 2013;24(1):153-66. [CrossRef] [PubMed]
- Gregorio DI, Samociuk H. Prostate cancer incidence in light of the spatial distribution of another screening-detectable cancer. Spat Spatiotemporal Epidemiol. 2013;6:1-6. [CrossRef] [PubMed]
- Goovaerts P, Xiao H, Adunlin G, Ali A, Tan F, Gwede CK, et al. Geographically-Weighted Regression Analysis of Percentage of Late-Stage Prostate Cancer Diagnosis in Florida. Appl Geogr. 2015;62:191-200. [CrossRef] [PubMed] [PubMed Central]
- Wang M, Matthews SA, Iskandarani K, Li Y, Li Z, Chinchilli VM, et al. Spatial-temporal analysis of prostate cancer incidence from the Pennsylvania Cancer Registry, 2000-2011. Geospat Health. 2017;12(2):611. [CrossRef] [PubMed] [PubMed Central]
- Wang M, Chi G, Bodovski Y, Holder SL, Lengerich EJ, Wasserman E, et al. Temporal and spatial trends and determinants of aggressive prostate cancer among Black and White men with prostate cancer. Cancer Causes Control. 2020;31(1):63-71. [CrossRef] [PubMed]
- Aghdam N, Carrasquilla M, Wang E, Pepin AN, Danner M, Ayoob M, et al. Ten-Year Single Institutional Analysis of Geographic and Demographic Characteristics of Patients Treated With Stereotactic Body Radiation Therapy for Localized Prostate Cancer. Front Oncol. 2020;10:616286. [CrossRef] [PubMed] [PubMed Central]
- Georgantopoulos P, Eberth JM, Cai B, Rao G, Bennett CL, Emrich CT, et al. A spatial assessment of prostate cancer mortality-to-incidence ratios among South Carolina veterans: 1999-2015. Ann Epidemiol. 2021;59:24-32. [CrossRef] [PubMed]
- Moore JX, Tingen MS, Coughlin SS, O’Meara C, Odhiambo L, Vernon M, et al. Understanding geographic and racial/ethnic disparities in mortality from four major cancers in the state of Georgia: a spatial epidemiologic analysis, 1999-2019. Sci Rep. 2022;12(1):14143. [CrossRef] [PubMed] [PubMed Central]
- Aladuwaka S, Alagan R, Singh R, Mishra M. Health Burdens and SES in Alabama: Using Geographic Information System to Examine Prostate Cancer Health Disparity. Cancers (Basel). 2022;14(19). [CrossRef] [PubMed] [PubMed Central]
- Tang C, Lei X, Smith GL, Pan HY, Hoffman KE, Kumar R, et al. Influence of Geography on Prostate Cancer Treatment. Int J Radiat Oncol Biol Phys. 2021;109(5):1286-95. [CrossRef] [PubMed] [PubMed Central]
- Moyer VA, Force USPST. Screening for prostate cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;157(2):120-34. [CrossRef] [PubMed]
- Maguire D. ArcGIS: General Purpose GIS Software System. . In: Shekhar, S, Xiong, H (eds) Encyclopedia of GIS Springer, Boston, MA. 2008. [CrossRef]
- Esri AP. ArcGIS Online. https://wwwesricom/en-us/landing-page/product/2019/arcgis-online/overview/.
- Griffith DA. Estimators of Spatial Autocorrelation. Encyclopedia of Social Measurement. 2005;Volume 3, p. 581.
- Tobler W. A computer movie simulating urban growth in the Detroit Region. Economic Geography. 1970;46:234–240.
- Kulldorff M, Nagarwalla N. Spatial disease clusters: detection and inference. Stat Med. 1995;14(8):799-810. [CrossRef] [PubMed]
- Arthur Getis JKO. The Analysis of Spatial Association by Use of Distance Statistics. Geographical Analysis. 1992. [CrossRef]
- Disparities UPC. https://wwwccsnwiorg/prostatecancerdisparitieshtml.
- Cackowski FC, Mahal B, Heath EI, Carthon B. Evolution of Disparities in Prostate Cancer Treatment: Is This a New Normal? Am Soc Clin Oncol Educ Book. 2021;41:1-12. [CrossRef] [PubMed]
- SEER-Medicare Linked Data Resource. https://healthcaredeliverycancergov/seermedicare/.
- Statewide Planning and Research Cooperative System (SPARCS). https://wwwhealthnygov/statistics/sparcs/.
- Arega MA, Yang DD, Royce TJ, Mahal BA, Dee EC, Butler SS, et al. Association Between Travel Distance and Use of Postoperative Radiation Therapy Among Men With Organ-Confined Prostate Cancer: Does Geography Influence Treatment Decisions? Pract Radiat Oncol. 2021;11(4):e426-e33. [CrossRef] [PubMed]
- Muralidhar V, Rose BS, Chen YW, Nezolosky MD, Nguyen PL. Association Between Travel Distance and Choice of Treatment for Prostate Cancer: Does Geography Reduce Patient Choice? Int J Radiat Oncol Biol Phys. 2016;96(2):313-7. [CrossRef] [PubMed]
- Holmes JA, Carpenter WR, Wu Y, Hendrix LH, Peacock S, Massing M, et al. Impact of distance to a urologist on early diagnosis of prostate cancer among black and white patients. J Urol. 2012;187(3):883-8. [CrossRef] [PubMed]
- Dobbs RW, Malhotra NR, Caldwell BM, Rojas R, Moreira DM, Abern MR. Determinants of Clinic Absenteeism: A Novel Method of Examining Distance from Clinic and Transportation. J Community Health. 2018;43(1):19-26. [CrossRef] [PubMed]
- Teshale AB, Amare T. Exploring spatial variations and the individual and contextual factors of uptake of measles-containing second dose vaccine among children aged 24 to 35 months in Ethiopia. PLoS One. 2023;18(1):e0280083. [CrossRef] [PubMed] [PubMed Central]
- Saha A, Hayen A, Ali M, Rosewell A, MacIntyre CR, Clemens JD, et al. Socioeconomic drivers of vaccine uptake: An analysis of the data of a geographically defined cluster randomized cholera vaccine trial in Bangladesh. Vaccine. 2018;36(31):4742-9. [CrossRef] [PubMed] [PubMed Central]
- Zahnd WE, McLafferty SL, Sherman RL, Klonoff-Cohen H, Farner S, Rosenblatt KA. Spatial Accessibility to Mammography Services in the Lower Mississippi Delta Region States. J Rural Health. 2019;35(4):550-9. [CrossRef] [PubMed]
- Pudrovska T, Anishkin A. Clarifying the positive association between education and prostate cancer: a Monte Carlo simulation approach. J Appl Gerontol. 2015;34(3):293-316. [CrossRef] [PubMed] [PubMed Central]
- Bostwick DG, Burke HB, Djakiew D, Euling S, Ho SM, Landolph J, et al. Human prostate cancer risk factors. Cancer. 2004;101(10 Suppl):2371-490. [CrossRef] [PubMed]
- El Khoury CJ, Sean A. P. Clouston. Racial/Ethnic Disparities in Prostate Cancer 5-Year Survival: The Role of Health-Care Access and Disease Severity. Cancers. 2023.
- Iris Hui WKTC. 3.13 - Spatial Dimensions of American Politics,. Editor(s): Bo Huang, Comprehensive Geographic Information Systems, Elsevier, Pages 181-188, ISBN 9780128047934,. 2018. [CrossRef]
- Openshaw STMAUPPI---.
- M.D. Su M-CL, T.H. Wen. Spatial Mapping and Environmental Risk Identification. Encyclopedia of Environmental Health, 2011, Pages 228-235. 2011;National Taiwan University, Taipei, Taiwan, Available online 3 March 2011.
- Grande D, Asch DA, Wan F, Bradbury AR, Jagsi R, Mitra N. Are Patients With Cancer Less Willing to Share Their Health Information? Privacy, Sensitivity, and Social Purpose. J Oncol Pract. 2015;11(5):378-83. [CrossRef] [PubMed] [PubMed Central]
- Luo L, McLafferty S, Wang F. Analyzing spatial aggregation error in statistical models of late-stage cancer risk: a Monte Carlo simulation approach. Int J Health Geogr. 2010;9:51. [CrossRef] [PubMed] [PubMed Central]
- Goldberg DW, Ballard M, Boyd JH, Mullan N, Garfield C, Rosman D, et al. An evaluation framework for comparing geocoding systems. Int J Health Geogr. 2013;12:50. [CrossRef] [PubMed] [PubMed Central]
- Oliver MN, Matthews KA, Siadaty M, Hauck FR, Pickle LW. Geographic bias related to geocoding in epidemiologic studies. Int J Health Geogr. 2005;4:29. [CrossRef] [PubMed] [PubMed Central]
- Walter SR, Rose N. Random property allocation: A novel geographic imputation procedure based on a complete geocoded address file. Spat Spatiotemporal Epidemiol. 2013;6:7-16. [CrossRef] [PubMed]
- Howlader N, Noone AM, Yu M, Cronin KA. Use of imputed population-based cancer registry data as a method of accounting for missing information: application to estrogen receptor status for breast cancer. Am J Epidemiol. 2012;176(4):347-56. [CrossRef] [PubMed] [PubMed Central]
- Henry KA, Boscoe FP. Estimating the accuracy of geographical imputation. Int J Health Geogr. 2008;7:3. [CrossRef] [PubMed] [PubMed Central]
- Sanderson M, Coker AL, Perez A, Du XL, Peltz G, Fadden MK. A multilevel analysis of socioeconomic status and prostate cancer risk. Ann Epidemiol. 2006;16(12):901-7. [CrossRef] [PubMed] [PubMed Central]
- Geary RCTCRaSMTIS, 5, 115-145. [CrossRef]
- Anselin L, Li X. Operational Local Join Count Statistics for Cluster Detection. J Geogr Syst. 2019;21(2):189-210. [CrossRef] [PubMed] [PubMed Central]
- Thatcher EJ, Camacho F, Anderson RT, Li L, Cohn WF, DeGuzman PB, et al. Spatial analysis of colorectal cancer outcomes and socioeconomic factors in Virginia. BMC Public Health. 2021;21(1):1908. [CrossRef] [PubMed] [PubMed Central]
- Moraga P, Montes F. Detection of spatial disease clusters with LISA functions. Stat Med. 2011;30(10):1057-71. [CrossRef] [PubMed]
- Esri AP. https://pro.arcgis.com/en/pro-app/latest/tool-reference/spatial-statistics/h-how-hot-spot-analysis-getis-ord-gi-spatial-stati.htm.
- Goungounga JA, Gaudart J, Colonna M, Giorgi R. Impact of socioeconomic inequalities on geographic disparities in cancer incidence: comparison of methods for spatial disease mapping. BMC Med Res Methodol. 2016;16(1):136. [CrossRef] [PubMed] [PubMed Central]
- Johnson GD. Small area mapping of prostate cancer incidence in New York State (USA) using fully Bayesian hierarchical modelling. Int J Health Geogr. 2004;3(1):29. [CrossRef] [PubMed] [PubMed Central]
- Guttmann A, Li X, Gaudart J, Gerard Y, Demongeot J, Boire JY, et al. Spatial heterogeneity of type I error for local cluster detection tests. Int J Health Geogr. 2014;13:15. [CrossRef] [PubMed] [PubMed Central]
- Walter SD. Visual and statistical assessment of spatial clustering in mapped data. Stat Med. 1993;12(14):1275-91. [PubMed]
- 2013. LABdmhmiseSENYCp.
- Alexander Fotheringham CFB, Martin Charlton Geographically Weighted Regression: The Analysis of Spatially Varying Relationships. 2002;https://www.researchgate.net/publication/27246972_Geographically_Weighted_Regression_The_Analysis_of_Spatially_Varying_Relationships.
- Kim SG, Cho SH, Lambert DM, Roberts RK. Measuring the value of air quality: application of the spatial hedonic model. Air Qual Atmos Health. 2010;3(1):41-51. [CrossRef] [PubMed] [PubMed Central]
- Iyengar S, Hall IJ, Sabatino SA. Racial/Ethnic Disparities in Prostate Cancer Incidence, Distant Stage Diagnosis, and Mortality by U.S. Census Region and Age Group, 2012-2015. Cancer Epidemiol Biomarkers Prev. 2020;29(7):1357-64. [CrossRef] [PubMed] [PubMed Central]
- Kish JK, Yu M, Percy-Laurry A, Altekruse SF. Racial and ethnic disparities in cancer survival by neighborhood socioeconomic status in Surveillance, Epidemiology, and End Results (SEER) Registries. J Natl Cancer Inst Monogr. 2014;2014(49):236-43. [CrossRef] [PubMed] [PubMed Central]
- Gourd E. New advances in prostate cancer screening and monitoring. Lancet Oncol. 2020;21(7):887. [CrossRef] [PubMed]
- Census.gov. https://www.census.gov/content/dam/Census/library/publications/2020/acs/acs_geography_handbook_2020_ch02.pdf.
- Gaudart J, Poudiougou B, Ranque S, Doumbo O. Oblique decision trees for spatial pattern detection: optimal algorithm and application to malaria risk. BMC Med Res Methodol. 2005 Jul 18;5:22. [CrossRef] [PubMed] [PubMed Central]
- Graham-Steed T, Uchio E, Wells CK, Aslan M, Ko J, Concato J. ‘Race’ and prostate cancer mortality in equal-access healthcare systems. Am J Med. 2013 Dec;126(12):1084-8. [CrossRef] [PubMed] [PubMed Central]
- Iyengar S, Hall IJ, Sabatino SA. Racial/Ethnic Disparities in Prostate Cancer Incidence, Distant Stage Diagnosis, and Mortality by U.S. Census Region and Age Group, 2012-2015. Cancer Epidemiol Biomarkers Prev. 2020 Jul;29(7):1357-1364. [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Article Selection Process.
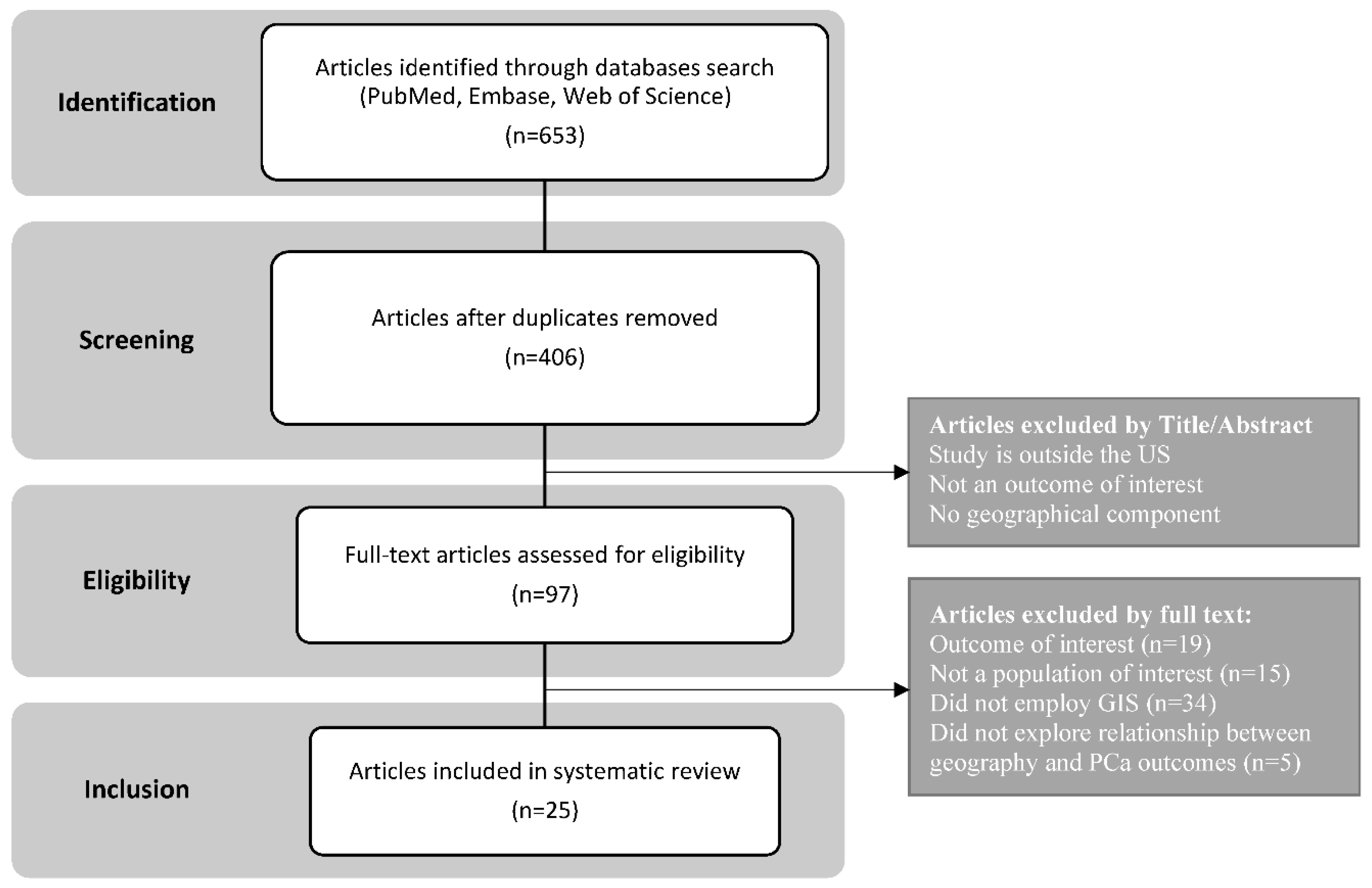
Figure 2.
GIS application in Prostate Cancer (PCa) Disparities Research.
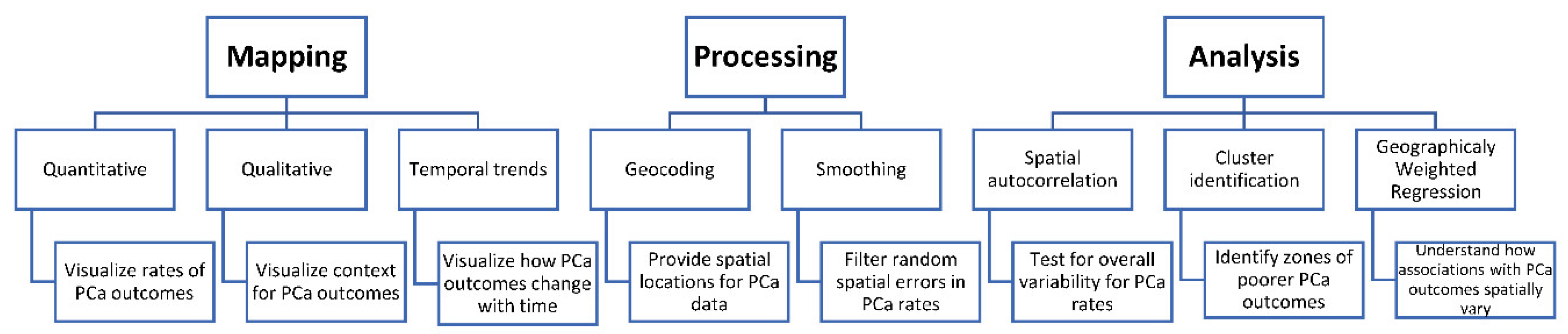
Figure 3.
Examples of different types of mapping utilized in PCa disparities research.
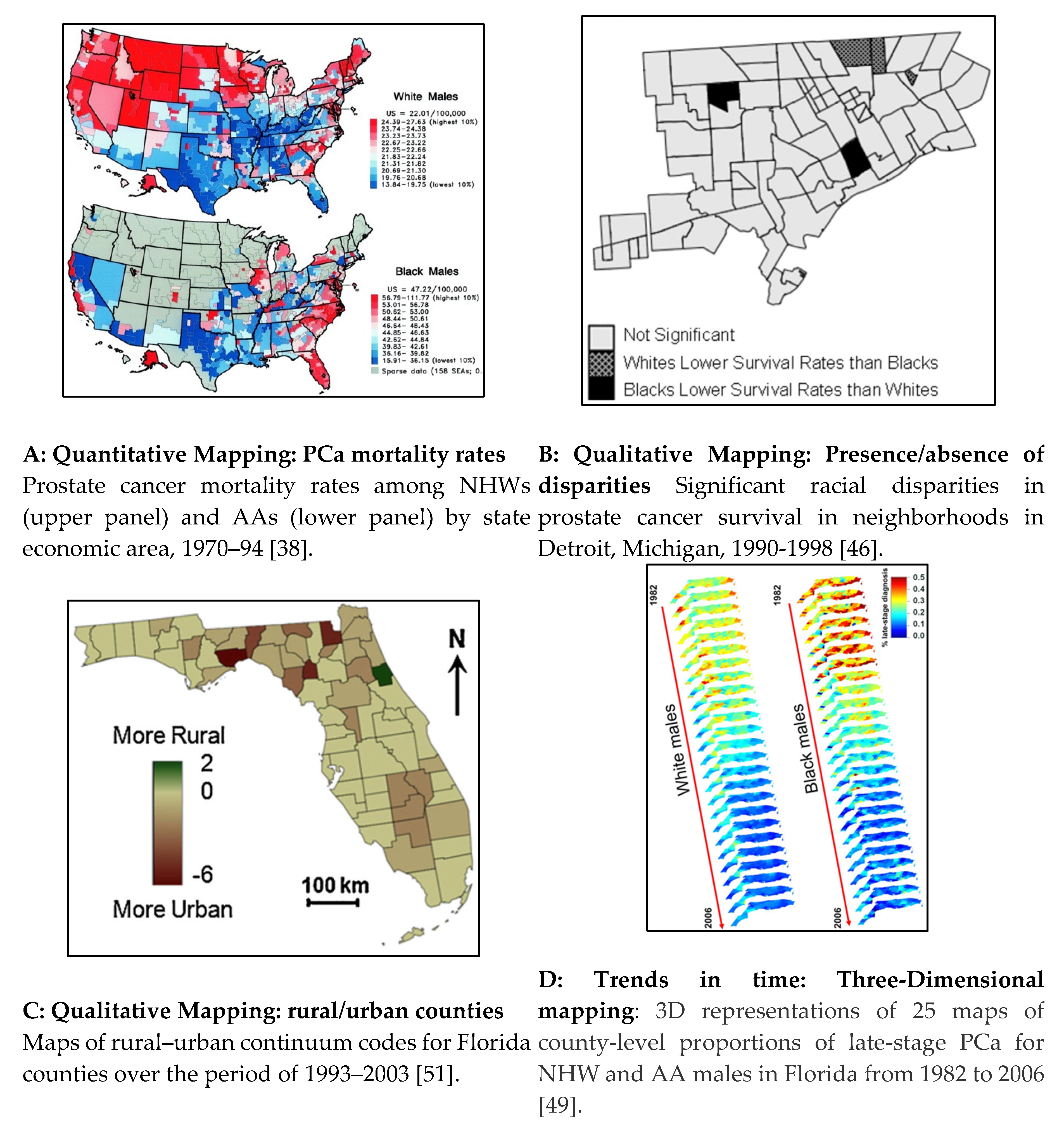
Figure 4.
Application of smoothing techniques in GIS studies examining PCa disparities. *Yearly kriging estimates were averaged over the period 1982-2006 and weighted according to the inverse of the binomial kriging standard deviations to assign more importance to more reliable estimates. For black males (BM), results are expressed as the ratio of average proportions for black versus white males (WM) to facilitate the visualization of racial disparities.
Figure 4.
Application of smoothing techniques in GIS studies examining PCa disparities. *Yearly kriging estimates were averaged over the period 1982-2006 and weighted according to the inverse of the binomial kriging standard deviations to assign more importance to more reliable estimates. For black males (BM), results are expressed as the ratio of average proportions for black versus white males (WM) to facilitate the visualization of racial disparities.
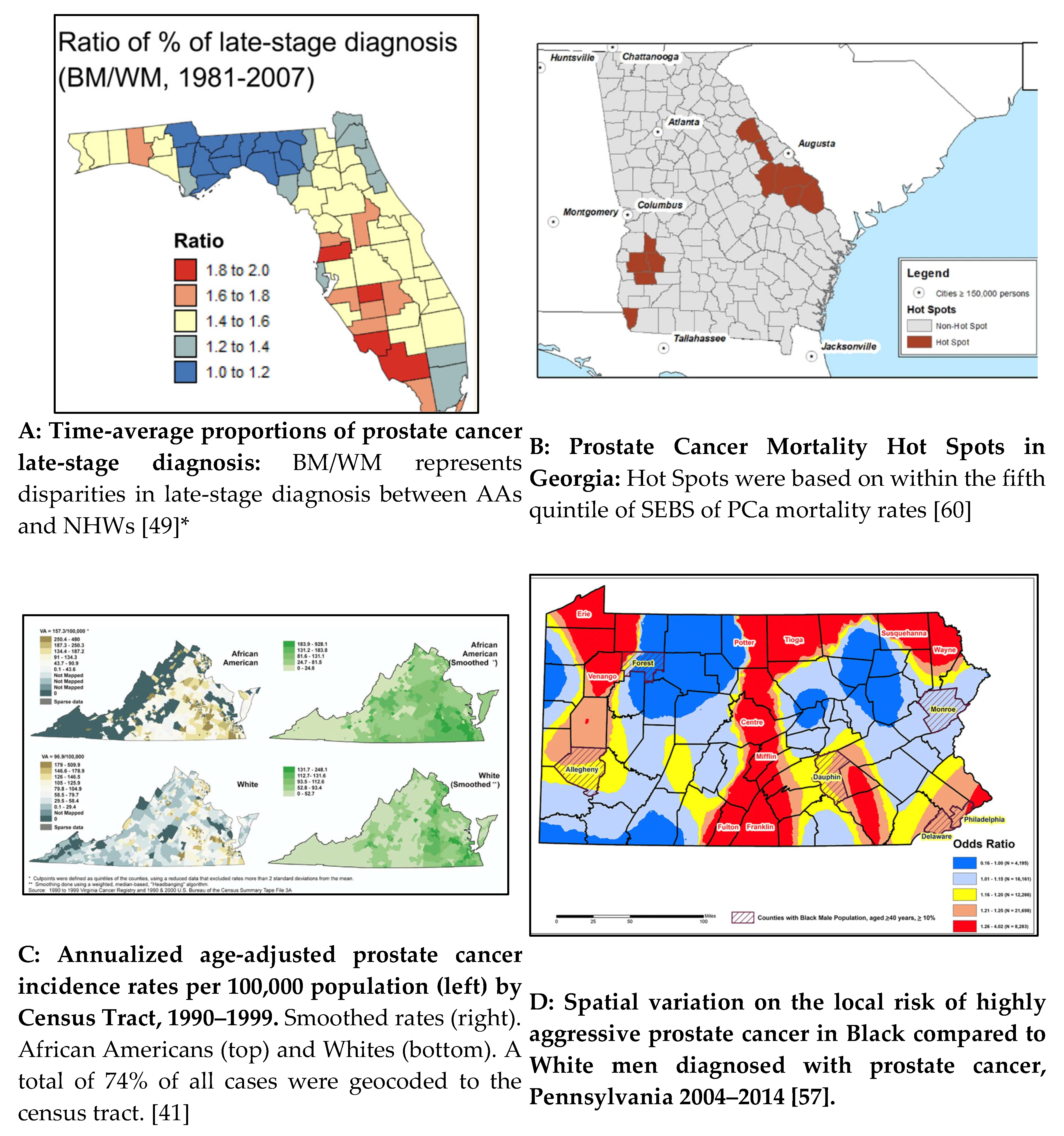
Figure 5.
Application of GIS Analysis in PCa Disparities Research.
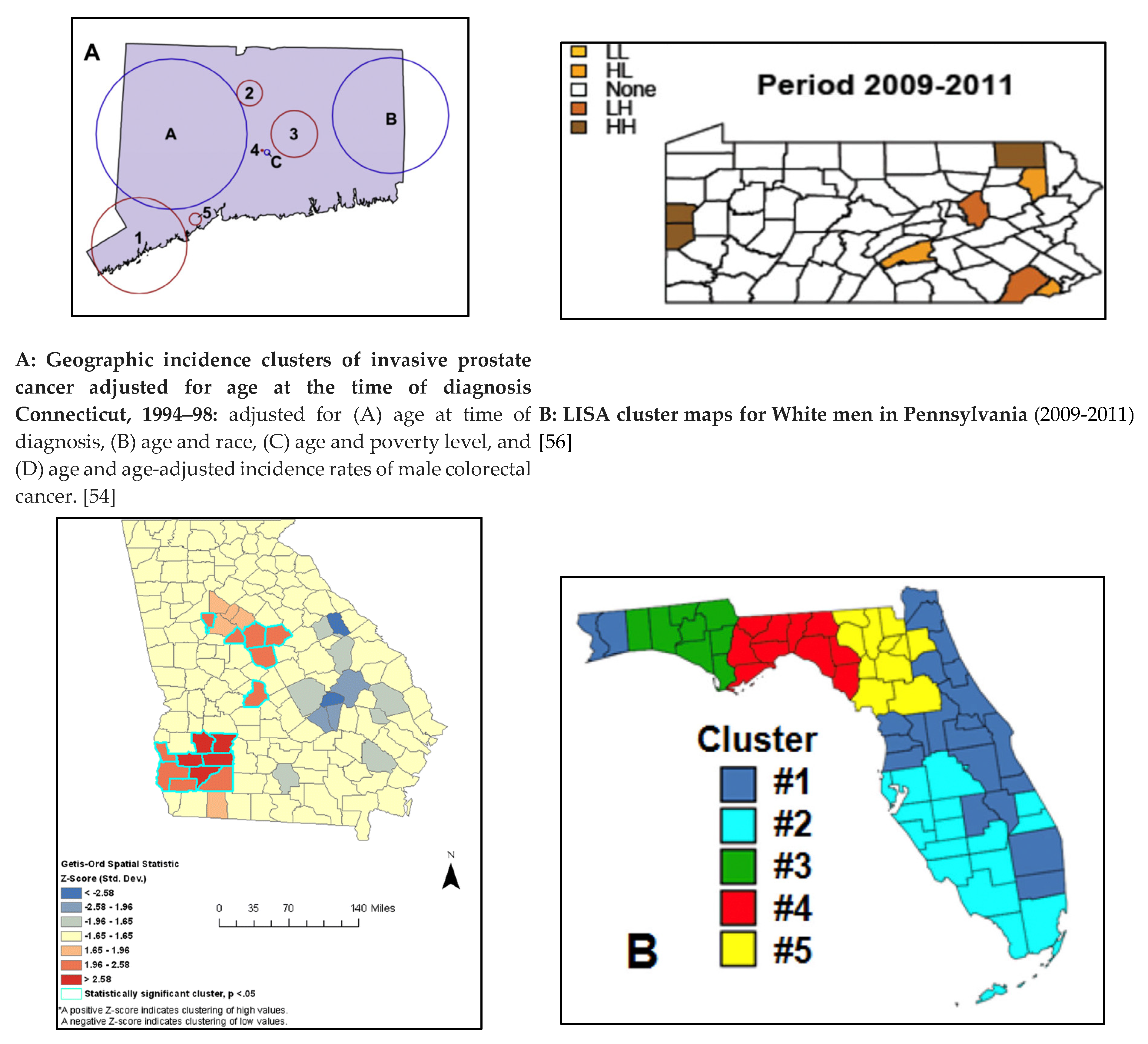

Figure 6.
Variation in clusters of PCa incidence based on Geocoding Quality (Virginia 1990-1999) [90].
Figure 6.
Variation in clusters of PCa incidence based on Geocoding Quality (Virginia 1990-1999) [90].


Table 1.
Summary of Studies Included In This Systematic Review.
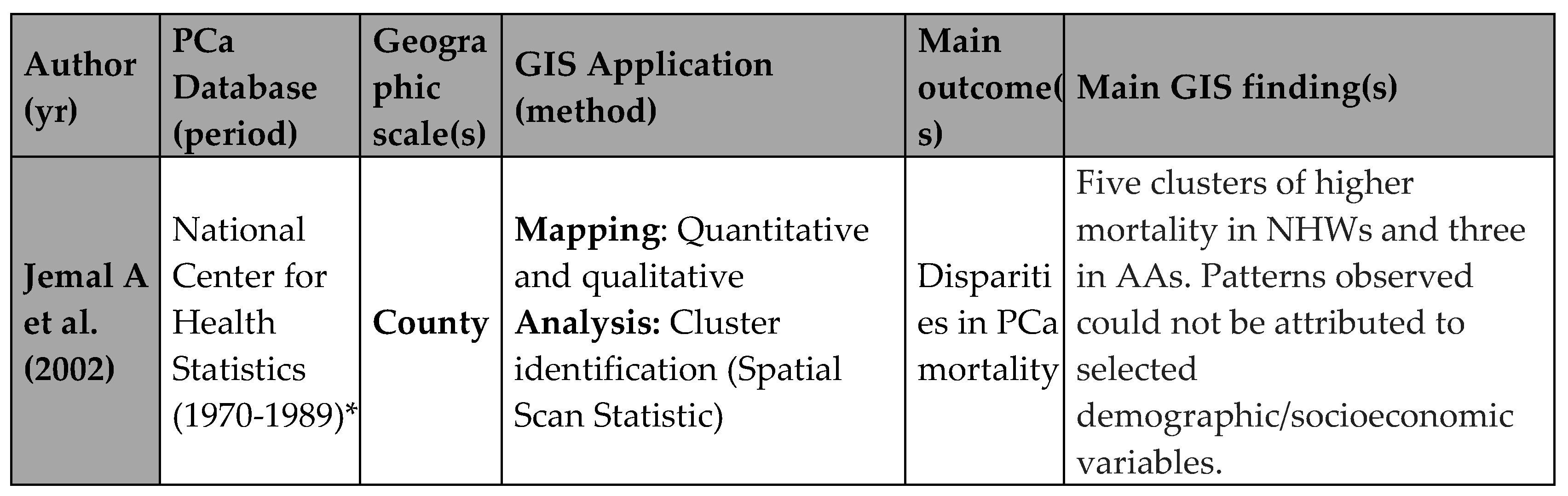

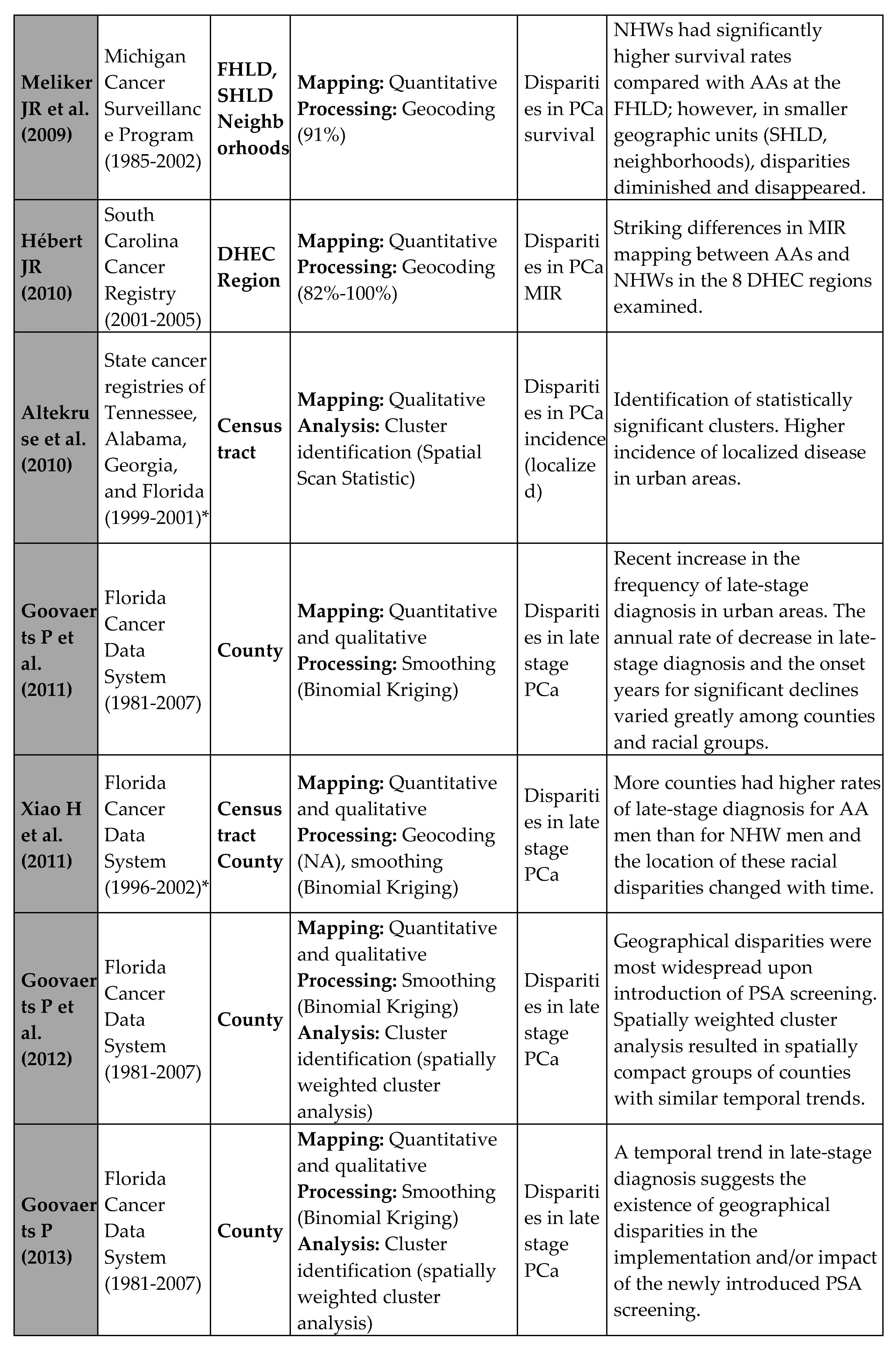
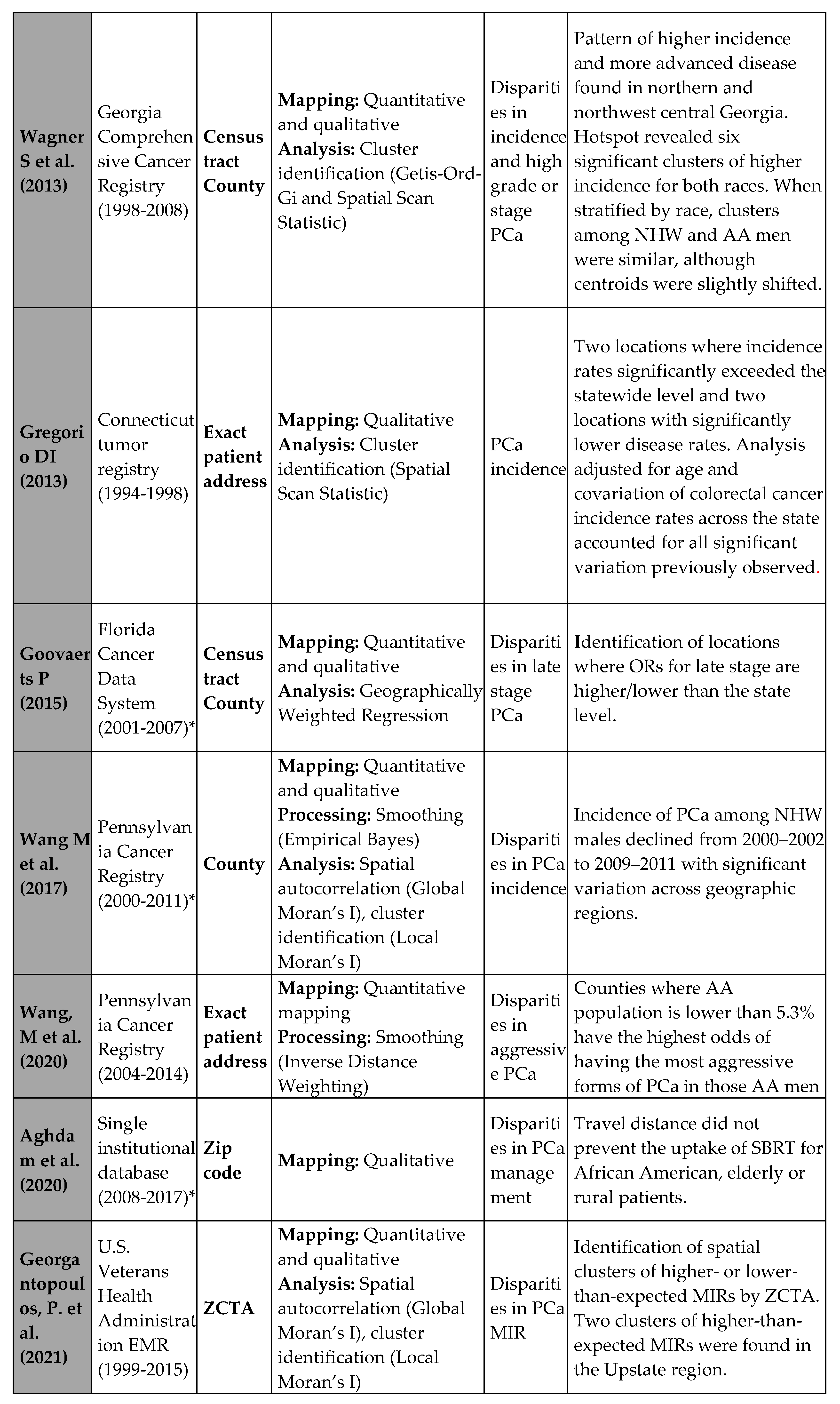

*PCa database linked to census data.
Table 2.
Variations in the Spatial Scan Statistic Technique for Cluster Identification.
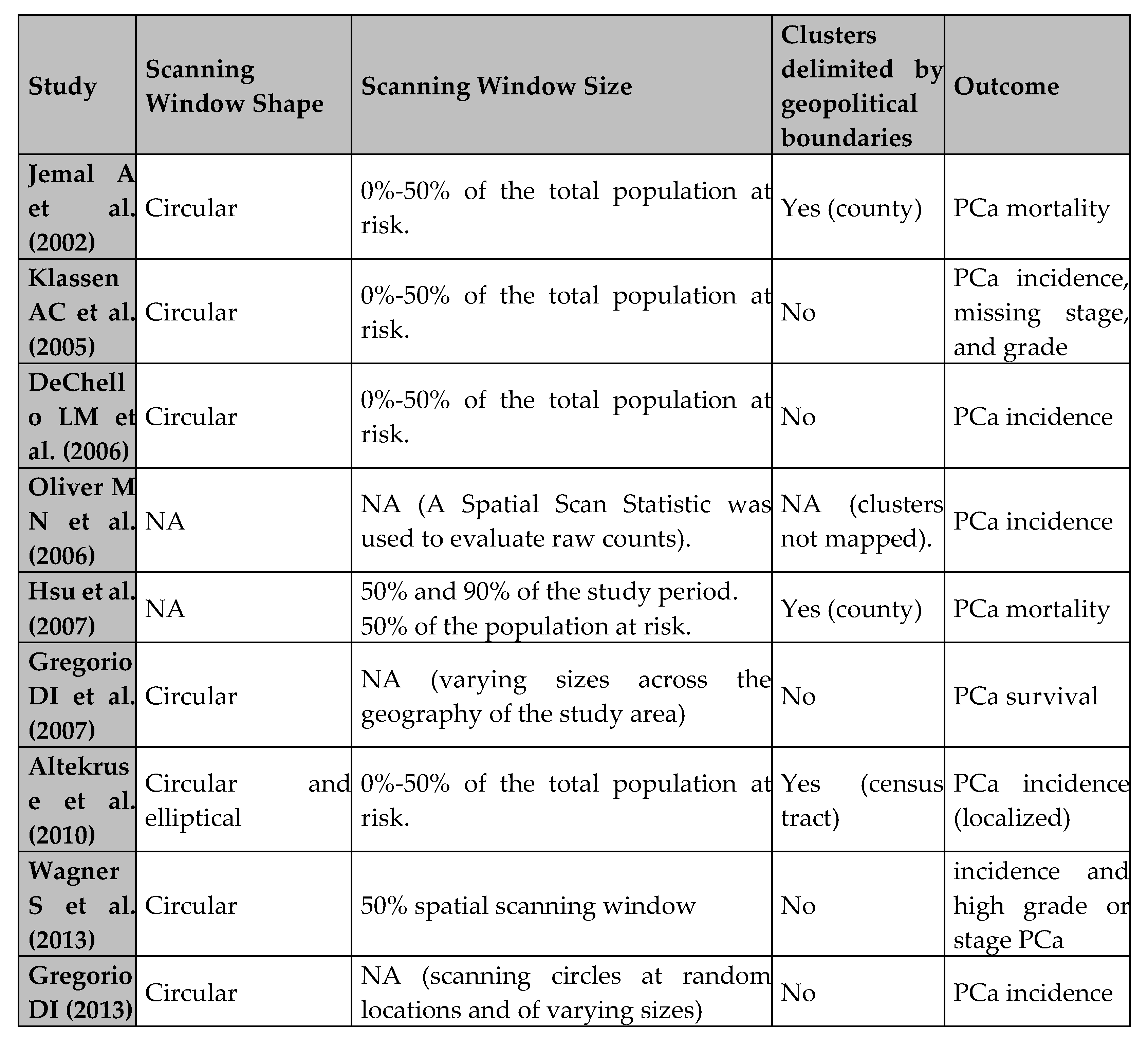
*NA= Not Available.
Table 3.
Summary of GIS Applications, Limitations, and Proposed Recommendations in PCa Research.
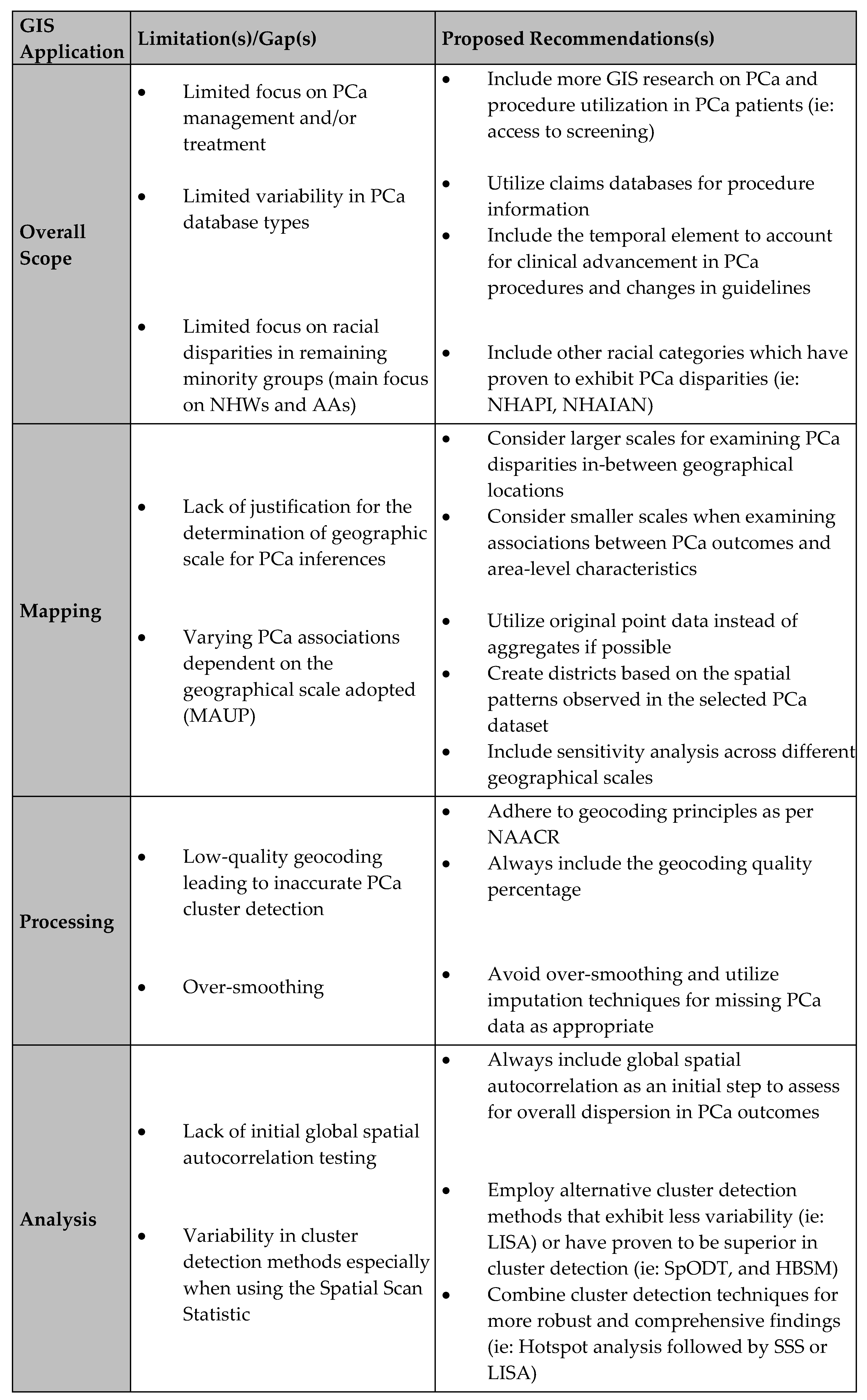
* NHAPI: Non-Hispanic Asian Pacific Islander, NHAIAN: Non-Hispanic American Indian/Alaskan Native, MAUP: Modifiable Areal Unit Problem, LISA: Local Indicator of Spatial Autocorrelation, SpODT: spatial oblique decision tree, HBSM: hierarchical Bayesian spatial modeling.
Table 4.
Summary of strengths and weaknesses of GIS analyses methods applied in PCa research.
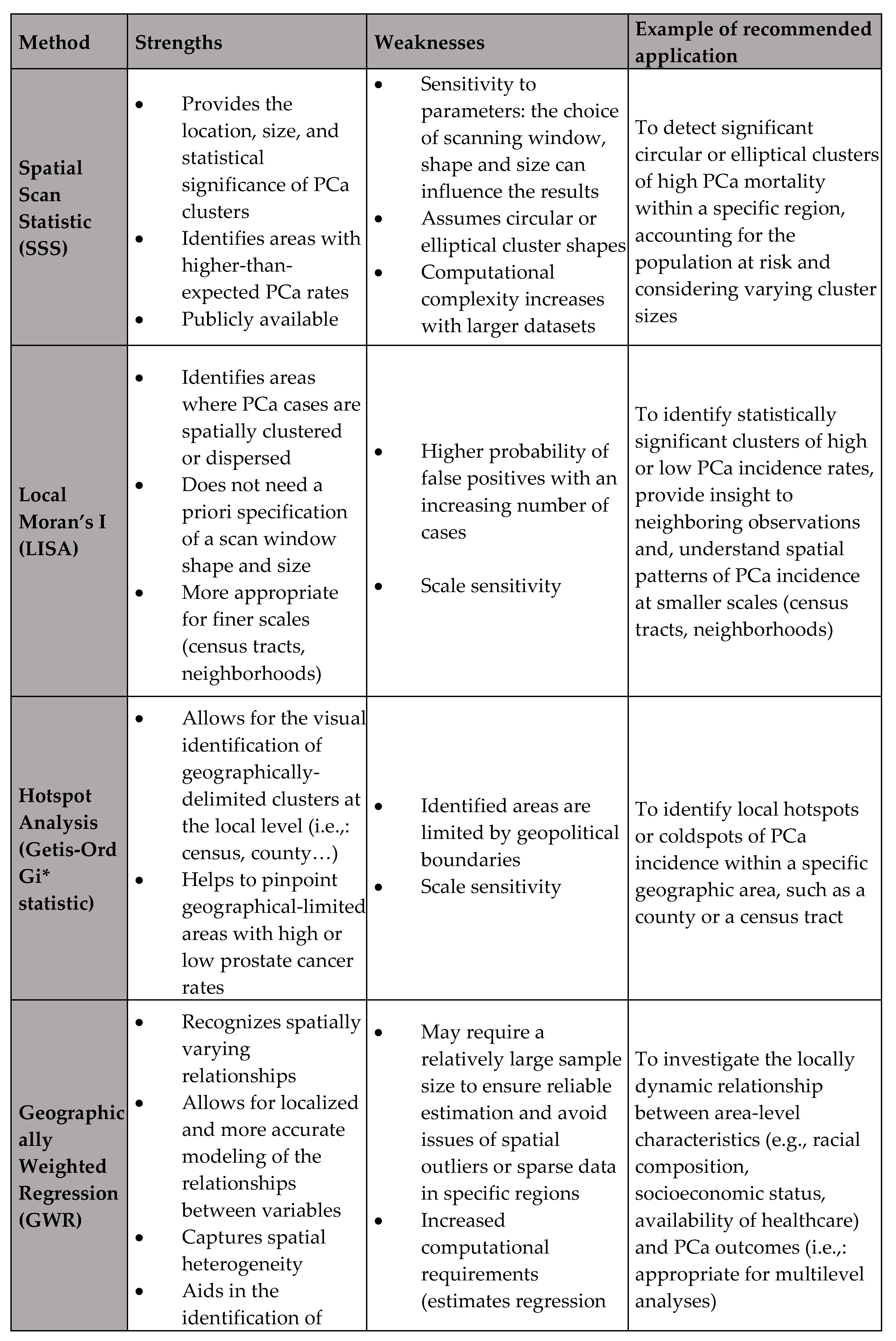
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



