
Submitted:
27 June 2024
Posted:
29 June 2024
You are already at the latest version
Abstract
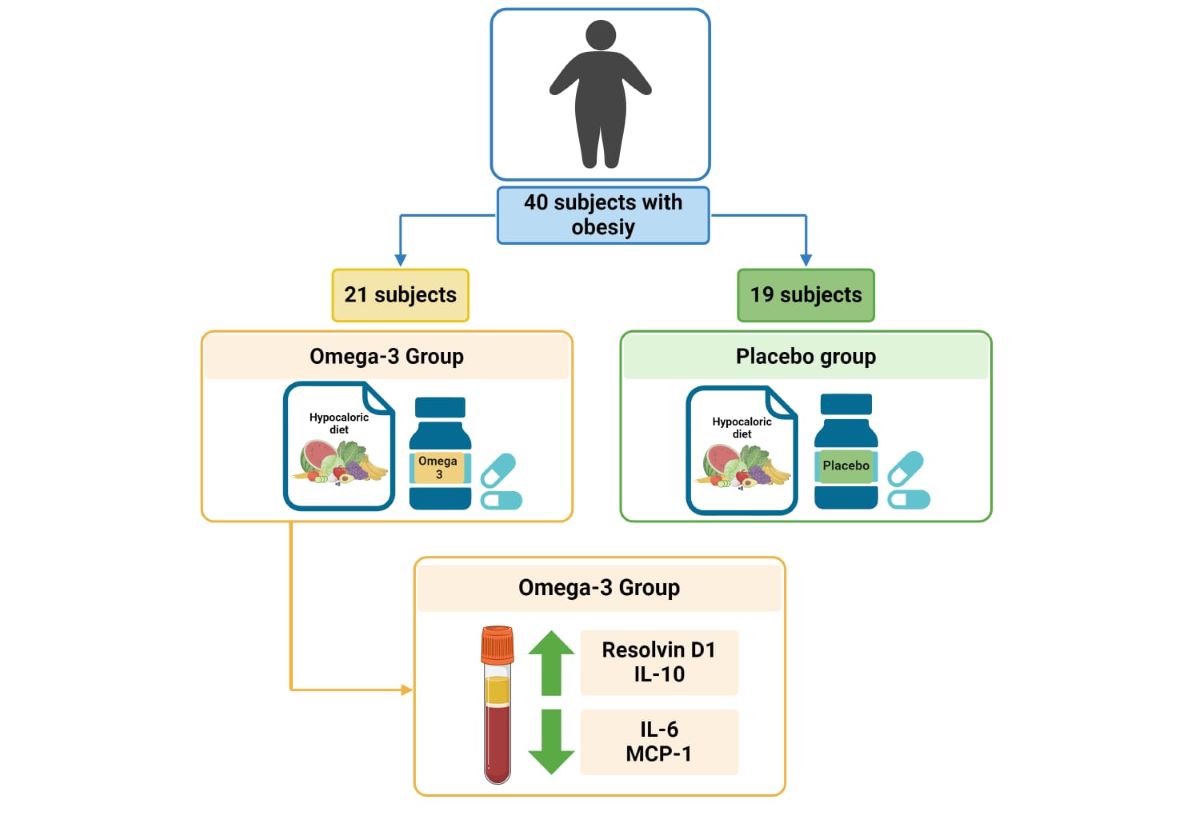
Obesity is associated with chronic low-grade inflammation. Polyunsaturated fatty ac-ids such as omega-3 (n-3), are essential in the pro-resolution of inflammation. An 8-week double-blind randomized clinical trial was conducted with a n-6:n-3, 5:1 ratio, along with daily 1.8 g of n-3 supplementation vs. placebo. A total of 40 subjects were included, 21 in omega 3 group and 19 in placebo group. The n-3 supplementation had a superior effect compared to placebo increasing levels of Resolvin D1 [129.3 (-90.1 - 193.5) vs. -16.8 (-237.8 - 92.5) pg/mL, p=0.041], IL-10 [1.4 (-0.7 - 4.6) vs. -2.0 (-5 - 0.05) pg/mL, p=0.001], and decreasing IL-6 [-0.67 (2.72 - -0.59) vs. 0.03 (-0.59 - 1.84) pg/mL p=0.015], and MCP-1 [-29.6 (-94.9 - 5.50) vs. 18.3 (-97.3 - 66.35) pg/mL, p=0.040]. In con-clusion, n-3 supplementation promoted resolution of inflammation by increasing sys-temic levels of Resolvin D1, IL-10, and decreasing IL-6 and MCP-1.
Keywords:
Diet
; Obesity
; Omega-3
; Low-grade inflammation
; Specialized pro-resolving mediators
1. Introduction
Obesity (OB) is characterized by an excessive accumulation of body fat resulting from an imbalance between daily energy intake and energy expenditure leading to excessive weight. This condition is a multifactorial disease influenced by some of genetic, cultural, and social factors. Contributing factors encompass reduced physical activity, insomnia, endocrine disorders, medication, and an imbalance in macronutrients consumption such as polyunsaturated fatty acids (PUFAs) omega-6 (n-6) and omega-3 (n-3). OB is associated with numerous comorbid and chronic medical conditions including an elevated risk of diabetes mellitus type 2, cardiovascular disease, hypertension, and dyslipidemia [1].
Currently, a low PUFAs intake, accompanied by an imbalance in their n-6:n-3 ratio has been described [2]. In Mexico, a 12:1 n-6:n-3 ratio has been reported, whereas the recommended adequacy suggests a consumption ratio no more than 5:1 [3,4]. This imbalance is strongly related with overweight comorbidities, and may contribute to the chronic low-grade inflammation [2,5].
In the other hand, the inflammatory response functions as a defense mechanism in the innate immune system to protect the host against detrimental stimuli, however, its activity must be resolved once the threat diminishes. This self-limiting process is crucial for preserving homeostasis [6]. Nevertheless, the failure to achieve resolution or continued exposure to environmental and biological factors that induce inflammatory response activation, can rise a chronic inflammatory process. This results in the extended presence of immune cells such as lymphocytes, macrophages, and plasma cells in the adipose tissue, accompanied by the secretion of proinflammatory cytokines [7,8].
Prolonged existence of chronic low-grade inflammation triggers the infiltration of immune cells and the secretion of inflammatory cytokines within the tissue environment, potentially inhibiting glucose absorption and altering lipid metabolism [9]. In recent years, attention has been focused on the investigation of the biological resolution of inflammation initiated by specific biochemical signals generated through the ingestion of n-3 PUFA. These potent bioactive molecules are collectively known as specialized pro-resolving mediators (SPMs) that include resolvins (Rv), protectins (PD), and maresins (MaR) [10]. There are few studies analyzing the anti-inflammatory effects of n-3 PUFAs in subjects with obesity.
Therefore, the aim of this study was to evaluate the effect of a nutritional intervention with 5:1 (n-6:n-3) PUFAs ratio with supplemented n-3 on anthropometric, biochemical, and pro-resolution inflammation parameters in adults with obesity.
2. Materials and Methods
2.1. Study Design
A randomized placebo controlled, double-blind parallel clinical trial with 8 weeks of follow-up was carried out at the Instituto de Nutrigenética y Nutrigenómica Traslacional, between October and December 2021. This trial was approved by ethics committees of the Centro Universitario de Ciencias de la Salud, Universidad de Guadalajara (CI-03221). Moreover, this study was registered in ClinicalTrials.gov (NCT05068557) and carried out according to the Declaration of Helsinki (2013). If participants agreed, written informed consent was obtained before screening and data collection.
2.2. Study Participants
All participants were recruited through flyers and social media invitations. A virtual screening process was conducted using electronic forms to assess eligibility. Inclusion criteria included subjects aged 25 to 50 years with obesity determined by body mass index (BMI) [11] and/or abdominal obesity according ATP III criteria [12]. Individuals who were pregnant, lactating, taking either omega-3, 6, 9 supplements, or using anti-inflammatory, lipid lowering, hypoglycemic, or antihypertensive medication, with immunological or neoplastic diseases, a history of cholecystectomy, fish or shellfish allergies or intolerances, were not included. Those with current COVID-19 diagnosis or within the previous 30 days, were excluded. A total of 40 Mexican adults with obesity were recruited (Figure 1).
2.3. Randomization
The supplement assignment was accomplished using the randomly permuted blocks method to balance the number of patients assigned to each treatment group [13]. The procedure was conducted by a researcher who was not involved in the treatment nor follow up of patients and was responsible for the recording and control of double blinded intervention.
2.4. Intervention
The intervention consisted of a hypocaloric diet, which was the same for both groups, along supplementation with n-3 or placebo according to the study group.
All the participants underwent interviews with a nutritionist to obtain clinical records and sociodemographic information. Additionally, the three days dietary record was collected, using food replicas (Nasco, Fort Atkinson USA) to assist in portion size estimation in accordance with the Sistema Mexicano de Alimentos Equivalentes [14].
2.4.1. Nutritional Intervention
The nutritional intervention consisted in a caloric reduction of 200 kcal every 4 weeks, based on the basal estimated caloric expenditure using Mifflin St. equation [15]. A recipes book was developed by nutritionists, containing 20 days of 3 main meals and 2 snacks that were calculated to maintain a n-6:n-3 PUFAs ratio of 5:1. Recipes were analyzed using Nutritionist Pro™ software (Axxya Systems, Woodinville, WA, USA) according to NOM-043, NOM-037, and GPC guidelines [16,17,18].
2.4.2. Omega 3 and Placebo Intervention Group
The n-3 supplementation consisted in 3 capsules per day containing 1080 mg of Eicosapentaenoic acid (EPA) and 720 mg of Docosapentaenoic acid (DHA), meanwhile, placebo group took 1600 mg of alpha-linolenic acid (ALA). Subjects were instructed to take one capsule with each main meal in both groups.
2.5. Outcome Measurements
2.5.1. Dietetic Analyses
Data was interpreted using the Nutritionist Pro™ software (Axxya Systems, Woodinville, WA, USA). The dietary n-3 was calculated by adding the following PUFAs: alpha-linolenic acid (18:3), stearidonic acid (18:4), eicosapentaenoic acid (20:5), docosapentaenoic acid (22:5), docosahexaenoic acid (22:6), and the n-6 PUFAs with the sum of linoleic acid (18:2), and arachidonic acid (20:4). The n-6:n-3 ratio was calculated dividing the n-6 value by the n-3 in grams. The cutoff for the n-6:n-3 PUFAs ratio was 5:1 [4].
2.5.2. Adherence Analyses
For diet adherence analyses, kilocalories intake and the n-6:n-3 ratio were considered. High adherence was defined as a consumption ± 20% of established kilocalories and a n-6:n-3 ratio <10:1 [19]. High supplementation adherence was defined if >80% of capsules were taken.
When the percentages obtained were considered, >80% was defined as high adherence.
2.5.3. Anthropometric Measurements
Measurements were taken after 8 to 12 hours of fasting, barefoot, with light clothes. Height was determined using a stadiometer with a precision of 1 mm (Rochester Clinical Research, Inc., New York, USA). Waist circumference (WC) was measured according to ISAK method using a Lufkin Executive® (New Brighton, United States) thin line 2 mm measuring tape. Abdominal obesity was defined when WC was ≥88cm in women and ≥102cm in men according to ATP-III [12]. Tetrapolar body electrical bioimpedance was used to assess body fat percentage (BF%) (InBody 570, Bio space Co. Seoul, Korea). Besides, BMI was calculated as weight in kilograms divided by height in meters squared (kg/m2).
2.5.4. Biochemical Measurements
Blood sampling was performed after fasting, then centrifuged at 4 °C for 15 min at 3500 RPM to obtain serum and plasma, finally, stored at −80 ◦C for future use. Serum glucose, triglycerides (TG), total cholesterol (TC), and high-density lipoprotein cholesterol (HDL-c) were determined by dry chemistry using a Vitros 350 Analyzer (Ortho-Clinical Diagnostics, Johnson & Johnson Services Inc., Rochester, NY, USA). Very low-density-lipoprotein cholesterol (VLDL-c) was estimated by dividing total triglycerides/5, low-density lipoprotein cholesterol (LDL-c) was calculated using the Friedewald formula as long as TG levels were less than 400 mg/mL [20]. Insulin was determined by a chemiluminescent immunoassay using a Liaison® (DiaSorin S.p.A., Saluggia (VC), Italy) and insulin resistance was calculated using the homeostasis model assessment (HOMA-IR = fasting insulin (μIU/mL) × fasting glucose (mg/dL) /405] [21].
2.5.5. Inflammatory Parameters
The cytokines TNF-α (Catalog A35601), IL-6 (Catalog A35573), MCP-1 (Catalog A35598) and IL-10 (Catalog A35590), were determined in serum samples using ProQuantum High Sensibility Immunoassay kits (Invitrogen by Thermo Fisher Scientific, Carlsbad, CA, USA). High-sensitivity C-reactive protein (hs-CRP) was performed by immunofluorescence using the Getein 1100 equipment, and plasma Resolvin D1 (RvD1) was quantified with a competitive enzyme-linked immunosorbent assay (Cayman Chemical. Ann Arbor, Michigan, USA).
2.6. Statistical Analysis
Sample size was calculated using the OpenEpi v3 software using the mean difference formula for clinical trials, reference values were obtained from changes in RvD1 levels re-ported in a population with obesity that received n-3 supplementation [22]. To achieve a statistical power of 80% and an alpha of 0.05%, a sample size of 19 participants in each study group, was required.
The normality distribution of quantitative variables was assessed using the Shapiro–Wilk test. Quantitative variables were represented as mean ± standard deviation (SD) or as median and interquartile range (IQR). Qualitative variables were expressed in frequencies and percentages. Comparative analysis for parametric variables between two independent groups or for related samples, Student t-test was used, and for non-parametric analyses, Mann–Whitney U test, or Wilcoxon was used. Repeated measures analysis of variance (ANOVA) or Friedman test was conducted adjusted by gender as corresponded. To evaluate changes in qualitative variables in the study groups, McNemar test was used. A p value <0.05 was considered statistically significant. All statistical analyses were carried out using SPSS v25.0 software (IBM Corp., Armonk, NY, USA).
3. Results
A total of 40 subjects were included in the study, where 21 corresponded to the omega 3 group (38% (n=8) females, and 62% (n=13) males) and 19 to the placebo group (42% (n=8) females, and 58 % (n=11) males). At baseline, there were no statistically significant differences between the study variables among the groups.
Characteristics of Diet and Adherence
The analysis of dietary variables is presented in Table 1 (basaline vs. 8 weeks postintervention). It was observed a significant increase in n-3 PUFA intake in both groups. In contrast, in the omega-3 group the intake of n-6 PUFA significantly decreased compared to baseline consumption. Nonetheless, it is important to highlight that the n-6:n-3 ratio intake improved significantly in both groups, achieving an ideal proportion. Regarding adherence, both study groups exhibited a 60% at the end of the study.
Anthropometric and Biochemical Measurements
In Table 2, the results of anthropometric parameters throughout the intervention (baseline, 4 weeks, and 8 weeks) are presented. After the intervention, improvement in weight, BMI, percentage of body fat, waist circumference (WC), triglycerides (TG), VLDL-c, was observed in both groups. However, when comparing intergroup, no statistical differences were observed. Moreover, prevalence of abdominal obesity significantly decreased 35% in omega-3 group (p=0.016), meanwhile, in placebo group decreased 5.6% (p=0.978) (Table 3).
Regarding fasting insulin and HOMA index, an improvement was observed in both groups, however, no differences were found between groups. In placebo group, the basal insulin was 19.2 ± 9.3 μIU/mL vs. 15.5 ± 8.2 μIU/mL final (p=0.040). Likewise, in the omega- 3 group, a significant decrease in insulin was observed (20.0 ± 11.4 vs. 14.8 ± 11.4 μIU/mL, p=0.025). On the other hand, basal HOMA index, in the omega-3 group was 4.8 ± 2.8 vs. 3.5 ± 2.4 final (p=0.076), and in placebo group was 4.4 ± 2.1 vs. 3.62 ± 1.9 (p=0.122).
Inflammation Resolution Parameters
After intervention, TNF-α, IL-6, and MCP-1 decrease in the omega-3 group, while IL-10 and RvD1 increased. Besides, in the placebo group, a decrease in TNF-α was also observed. Moreover, in intergroup analysis IL-6, IL-10, and RvD1, remained statistically significant (Table 4).
4. Discussion
It has been shown that supplementation with n-3 PUFAs have an important role in the treatment of obesity, as they have a favorable impact on chronic low-grade inflammation. However, controversial results persist among different populations, particularly regarding the duration and consumption quantity [23]. The aim of this study was to assess the effect of a nutritional intervention with average ratio of 5:1 (n-6:n-3) supplemented with n-3, on anthropometric, biochemical, and pro-resolution of inflammation parameters in adults with obesity [19].
Given the crucial role of patients adherence in this kind of interventional projects, WHO's recommendations for chronic diseases treatments, suggests to achieve at least 50% [24], which agree with findings in this study due to 60% of adherence was found in both groups, however, more motivational strategies should be use in further studies with satisfaction surveys that leads to improving treatment.
Regarding baseline analysis of three dietary records, all subjects showed an inadequate consumption of n-6:n-3 PUFAs ratio which agree with other studies in Mexican population with obesity [3,25,26] showing an imbalance associated with higher adipose tissue percentage, WC, and higher levels of triglycerides, glucose, and insulin [3]. Additionally, it contributes to chronic low-grade inflammation in obesity by activating inflammatory pathways and interfering with the synthesis of lipid mediators in pro-resolution inflammation, such as resolvins [10].
In this study, both groups significantly increased n-3 intake and achieved a dietary n-6:n-3 consumption ratio of <5:1 at the end of the intervention. However, it is noteworthy that the omega-3 group exhibited statistically lower n-6 dietary intake compared to the placebo group. These findings could be related with better metabolic profile and pro-resolution inflammation mediators exposed above.
Analysis of anthropometric variables showed intragroup improvements in weight, body fat percentage, BMI, and waist circumference; however, when comparing these variables between groups, no statistically significant differences were found. We hypothesize that these results could be attributed to the implementation of the same dietary recommendations in the recipes book provided.
Nevertheless, prevalence of abdominal obesity significantly decreased 35% in omega-3 group compared to 5.6% in placebo group. These findings are consistent with meta-analyses that found a relationship between n-3 intake of animal source with better anthropometric measures [27,28]. However, the impact of these PUFAs on body composition has been controversial with WC reported as the anthropometric variable related to obesity that has the most significant impact after n-3 supplementation [28].
Among the biochemical variables, some lipid profile components had an improvement, such as triglycerides and VLDL-c. This could be explained by a mechanism in which n-3 PUFAs act as ligands for peroxisome proliferator-activated receptor alpha (PPAR-α), a transcription factor that promotes the expression of genes involved in β-oxidation of fatty acids [29,30], decreasing VLDL-c levels. The VLDL-c is responsible for endogenous transport of triglycerides from the liver to peripheral tissues, including visceral, mainly in the abdominal region [31]. On the other hand, no effects were observed on HDL-c and total cholesterol, consistent findings with a meta-analysis by Harrys et al., where triglycerides and VLDL-c significantly decreased while HDL-c and total cholesterol were not altered after 7 to 10 weeks of n-3 PUFA supplementation [32]. Nevertheless, other factors may be involved, such as physical activity and genetic factors related to HDL-c concentrations [33].
Regarding fasting insulin, it was observed improvements, independently of groups, following the intervention, which may be attributable to the same dietary regimen and the favorable impact of an adequate diet on insulin levels [34]. Furthermore, the HOMA index consistently displayed improved parameters in the omega-3 group throughout the intervention, indicating a beneficial effect. The correlation between omega-3 fatty acids and the free fatty acid receptor 4 (FFAR4) elucidates the potential mechanisms underlying the observed effects on glucose metabolism and insulin levels. Activation of FFAR4 by omega-3 fatty acids has been associated with enhancements in insulin sensitivity and glucose homeostasis [35,36]. Nevertheless, literature reports inconclusive n-3 effects on these variables in humans [37] might be due glucose homeostasis is influenced by other factors beyond n-3 intake, such as lifestyle, physical activity, body fat percentage, among others [34,37,38]. Given this complexity, further clinical trials with longer time, are necessary, as our intervention lasted only 8 weeks and that the activation of FFAR4 can be evaluated.
Other metabolic consequences of obesity associated with the imbalance of n-6:n-3 PUFA ratio intake, is the maintenance of chronic low-grade inflammation affecting pro-resolution inflammation processes mainly in adipose tissue [39,40]. Studies in vitro and clinical trials, have demonstrated that n-3 PUFAs, particularly EPA and DHA, decrease the number of resident macrophages in adipose tissue and crown-like structures characteristic of the M1 phenotype. In addition to the decrease in levels of MCP-1, a chemotactic protein with a key role in the initiation, development, and perpetuation of chronic low-grade inflammation in obesity [41,42], consistent with the findings of this study, where MCP-1 levels were lower in the omega-3 group both intragroup and compared between groups at the end of the intervention.
Similarly, IL-6 concentrations were lower in the omega 3 group both intra and intergroups at the end of the intervention, consistent with the study of Milutinivic et al., who evaluated the effect of n-3 supplementation (2.4 g/day) for 8 weeks on inflammatory markers, highlighting a statistically significant decrease of IL-6 [43]. Moreover, a meta-analysis published in 2021 by Wei Y. et al., including 31 studies between 2003 and 2019, aimed to study the effect of inflammatory markers and the n-6:n-3 PUFA ratio consumption in various inflammatory etiology diseases, emphasizing obesity and associated comorbidities. Omega-3 supplementation has been associated with the modulation of inflammation through the nuclear factor κB (NF-κB) pathway. Research indicates that omega-3 fatty acids can influence markers of inflammation by inhibiting the production of pro-inflammatory cytokines and regulating the NF-κB signaling pathway [44]. As in this study, they concluded that systemic levels of IL-6 and TNF-α were lower in subjects with lower n-6:n-3 consumption ratio as has been documented in the literature [45].
Regarding RvD1, which belongs to the family of lipid pro-resolution inflammation mediators, increased significantly compared to baseline in omega-3 group along with IL-10. This supports the hypothesis proposed in this study, as RvD1 is synthesized from DHA metabolism [10,46,47], and the omega-3 group had a higher total consumption compared to placebo group. Additionally, it has been reported that RvD1 promotes the synthesis of IL-10 [48] which agrees with a study by Polus et al., included 59 women with obesity provided with dietary guidelines and supplementation with 1.8 g/day of n-3 for 12 weeks. In proportion, they observed 58% of increase in RvD1 plasma levels, and an in-crease in IL-10, compared to baseline in n-3 supplemented group. Although our results are consistent, the higher increased in Polus et al. study may be due to the longer intervention (12 vs. 8 weeks) [22]. This finding suggests that the chronicity of n-3 consumption favors the incorporation of these PUFAs into the cellular membranes phospholipids [4], and as a result, the enhancement of the RvD1 synthesis involved in inflammation resolution processes by reducing the activation of the NF-κB-mediated cascade, leading to reported decreases of TNF-α, IL-6, MCP-1, and increase IL-10 [46,49,50].
Perspectives of this study, are to increase the intervention time including more sub-jects, analyze more inflammatory and pro-resolution molecules with others methodologies such as chromatographic, to allow us to corroborate data and elucidate cellular mechanisms where n-6:n-3 PUFA ratio is involved.
Moreover it is necessary that health professionals and governmental programs, pro-mote an adequate consumption of n-6:n-3 PUFA ratio intake due to their association with obesity and related disorders where a chronic low-grade inflammation is present.
5. Conclusions
After intervention, improvement in weight, BMI, percentage of body fat, waist circumference, triglycerides, VLDL-c, insulin and TNFα, were observed in both groups.
Nevertheless, the omega-3 supplemented group had improved resolution of inflammation by increasing systemic concentrations of resolvin D1, IL-10, and decreasing IL-6 and MCP-1; and the prevalence of abdominal obesity significantly decreased 35% in omega 3 group, meanwhile, in placebo group decreased only 5.6%.
Author Contributions
All authors contributed significantly to this article. J. T-V: conceptualization, data curation, investigation, methodology, development of experiments, writing—original draft and editing. R. R-E: development of experiments, investigation, super-visions. W. C-P: methodology, formal analysis, resources, supervision, writing–original draft, writing–review and editing. C. R-R: methodology, development of experiments. S.R-P: collected the data, data curation, M.P-R: writing–original draft, writing–review and editing, E.M-L: conceptualization, data curation, formal analysis, funding acquisition, methodology, project administration, resources, supervision, visualization, writing–original draft, writing–review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Fortalecimiento UdG (REC/CINV/0975/2022) to Erika Martínez-López and Fondo para proyectos de impulso a la investigación (PIN 2022-III) to Erika Martínez-López.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committees of Centro Universitario de la Salud, Universidad de Guadalajara (protocol code CI-03221 and date of approval 14 September 2021). And was registered in ClinicalTrials.gov (NCT05068557).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors would like to acknowledge the valuable collaboration of the EPICO team. Cordially thank the Universidad de Guadalajara, Instituto de Nutrigenética y Nutrigenómia Traslacional and Laboratorio de Evaluación del Estado Nutricio, to enable the development of the work, and the subjects who participated in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- González-Muniesa, P.; Mártinez-González, M.-A.; Hu, F.B.; Després, J.-P.; Matsuzawa, Y.; Loos, R.J.F.; Moreno, L.A.; Bray, G.A.; Martinez, J.A. Obesity. Nat. Rev. Dis. Primer 2017, 3, 17034. [Google Scholar] [CrossRef] [PubMed]
- Simopoulos, A.P.; DiNicolantonio, J.J. The Importance of a Balanced ω-6 to ω-3 Ratio in the Prevention and Management of Obesity. Open Heart 2016, 3, e000385. [Google Scholar] [CrossRef]
- Torres-Castillo, N.; Silva-Gómez, J.A.; Campos-Perez, W.; Barron-Cabrera, E.; Hernandez-Cañaveral, I.; Garcia-Cazarin, M.; Marquez-Sandoval, Y.; Gonzalez-Becerra, K.; Barron-Gallardo, C.; Martinez-Lopez, E. High Dietary ω-6:ω-3 PUFA Ratio Is Positively Associated with Excessive Adiposity and Waist Circumference. Obes. Facts 2018, 11, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Becerra, K.; Barron-Cabrera, E.; Muñoz-Valle, J.F.; Torres-Castillo, N.; Rivera-Valdes, J.J.; Rodriguez-Echevarria, R.; Martinez-Lopez, E. A Balanced Dietary Ratio of N-6:N-3 Polyunsaturated Fatty Acids Exerts an Effect on Total Fatty Acid Profile in RBCs and Inflammatory Markers in Subjects with Obesity. Healthcare 2023, 11, 2333. [Google Scholar] [CrossRef] [PubMed]
- Simopoulos, A.P. An Increase in the Omega-6/Omega-3 Fatty Acid Ratio Increases the Risk for Obesity. Nutrients 2016, 8, 128. [Google Scholar] [CrossRef] [PubMed]
- Hannoodee, S.; Nasuruddin, D.N. Acute Inflammatory Response. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2023. [Google Scholar]
- Chen, L.; Deng, H.; Cui, H.; Fang, J.; Zuo, Z.; Deng, J.; Li, Y.; Wang, X.; Zhao, L. Inflammatory Responses and Inflammation-Associated Diseases in Organs. Oncotarget 2017, 9, 7204–7218. [Google Scholar] [CrossRef]
- Serhan, C.N.; Brain, S.D.; Buckley, C.D.; Gilroy, D.W.; Haslett, C.; O’Neill, L.A.J.; Perretti, M.; Rossi, A.G.; Wallace, J.L. Resolution of Inflammation: State of the Art, Definitions and Terms. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2007, 21, 325–332. [Google Scholar] [CrossRef]
- Hotamisligil, G.S. Inflammation and Metabolic Disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Chiang, N.; Serhan, C.N. Specialized Pro-Resolving Mediator Network: An Update on Production and Actions. Essays Biochem. 2020, 64, 443–462. [Google Scholar] [CrossRef]
- WHO Obesidad y Sobrepeso. Available online: https://www.who.int/es/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 2 July 2019).
- Rubio, M.A.; Moreno, C.; Cabrerizo, L. Guías para el tratamiento de las dislipemias en el adulto: Adult Treatment Panel III (ATP-III). Endocrinol. Nutr. 2004, 51, 254–265. [Google Scholar] [CrossRef]
- Lazcano-Ponce, E.; Salazar-Martínez, E.; Gutiérrez-Castrellón, P.; Angeles-Llerenas, A.; Hernández-Garduño, A.; Viramontes, J.L. Ensayos clínicos aleatorizados: variantes, métodos de aleatorización, análisis, consideraciones éticas y regulación. Salud Pública México 2004, 46, 559–584. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Lizaur, A.B.; Gonzalez-Palacios, B.; Castro-Becerra, A. Sistema Mexicano de Alimentos Equivalentes; Cuaeta edición.; Fomento de Nutrición y Salud, A.C.: México, 2014; ISBN 978-607-00-7928-3. [Google Scholar]
- Mifflin, M.D.; St Jeor, S.T.; Hill, L.A.; Scott, B.J.; Daugherty, S.A.; Koh, Y.O. A New Predictive Equation for Resting Energy Expenditure in Healthy Individuals. Am. J. Clin. Nutr. 1990, 51, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Norma Oficial Mexicana NOM-043-SSA2-2012, Servicios básicos de salud. Promoción y educación para la salud en materia alimentaria. Criterios para brindar orientación. 2013, 35.
- Cano-Pérez, E.; Meoño-Morales, E.; Mendoza-Salazar, L. Prevención, Diagnóstico y tratamiento del sobre peso y obesidad exógena 2012.
- Morales, P.A.K. Norma Oficial Mexicana NOM-037-SSA2-2012, Para la prevención, tratamiento y control de las dislipidemias. 2012.
- Simopoulos, A.P. The Importance of the Omega-6/Omega-3 Fatty Acid Ratio in Cardiovascular Disease and Other Chronic Diseases. Exp. Biol. Med. 2008, 233, 674–688. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Homeostasis Model Assessment Insulin Resistance and β Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man.Pdf.
- Polus, A.; Zapala, B.; Razny, U.; Gielicz, A.; Kiec-Wilk, B.; Malczewska-Malec, M.; Sanak, M.; Childs, C.E.; Calder, P.C.; Dembinska-Kiec, A. Omega-3 Fatty Acid Supplementation Influences the Whole Blood Transcriptome in Women with Obesity, Associated with pro-Resolving Lipid Mediator Production. Biochim. Biophys. Acta BBA - Mol. Cell Biol. Lipids 2016, 1861, 1746–1755. [Google Scholar] [CrossRef] [PubMed]
- Kavyani, Z.; Musazadeh, V.; Fathi, S.; Hossein Faghfouri, A.; Dehghan, P.; Sarmadi, B. Efficacy of the Omega-3 Fatty Acids Supplementation on Inflammatory Biomarkers: An Umbrella Meta-Analysis. Int. Immunopharmacol. 2022, 111, 109104. [Google Scholar] [CrossRef]
- Organization, W.H. Adherence to Long-Term Therapies : Evidence for Action; World Health Organization, 2003; ISBN 978-92-4-154599-0.
- Lopez-Pentecost, M.; Hallmark, B.; Thomson, C.A.; Chilton, F.; Garcia, D.O. Association between Dietary Fatty Acid Intake and Liver Steatosis and Fibrosis in a Sample of Mexican-Origin Hispanic Adults with Overweight or Obesity. Int. J. Environ. Res. Public. Health 2023, 20, 3103. [Google Scholar] [CrossRef] [PubMed]
- Torres-Valadez, R.; Ramos-Lopez, O.; Frías Delgadillo, K.J.; Flores-García, A.; Rojas Carrillo, E.; Aguiar-García, P.; Bernal Pérez, J.A.; Martinez-Lopez, E.; Martínez, J.A.; Zepeda-Carrillo, E.A. Impact of APOE Alleles-by-Diet Interactions on Glycemic and Lipid Features– A Cross-Sectional Study of a Cohort of Type 2 Diabetes Patients from Western Mexico: Implications for Personalized Medicine. Pharmacogenomics Pers. Med. 2020, 13, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.Y.; Liu, W.; Zhao, T.Y.; Tian, H.M. EFFICACY OF OMEGA-3 POLYUNSATURATED FATTY ACIDS SUPPLEMENTATION IN MANAGING OVERWEIGHT AND OBESITY: A META-ANALYSIS OF RANDOMIZED CLINICAL TRIALS. J Nutr Health Aging.
- Bender, N.; Portmann, M.; Heg, Z.; Hofmann, K.; Zwahlen, M.; Egger, M. Fish or N3-PUFA Intake and Body Composition: A Systematic Review and Meta-Analysis: Fish and Body Composition. Obes. Rev. 2014, 15, 657–665. [Google Scholar] [CrossRef]
- Tahri-Joutey, M.; Andreoletti, P.; Surapureddi, S.; Nasser, B.; Cherkaoui-Malki, M.; Latruffe, N. Mechanisms Mediating the Regulation of Peroxisomal Fatty Acid Beta-Oxidation by PPARα. Int. J. Mol. Sci. 2021, 22, 8969. [Google Scholar] [CrossRef]
- Bays, H.E.; Tighe, A.P.; Sadovsky, R.; Davidson, M.H. Prescription Omega-3 Fatty Acids and Their Lipid Effects: Physiologic Mechanisms of Action and Clinical Implications. Expert Rev. Cardiovasc. Ther. 2008, 6, 391–409. [Google Scholar] [CrossRef] [PubMed]
- Christofides, A.; Konstantinidou, E.; Jani, C.; Boussiotis, V.A. The Role of Peroxisome Proliferator-Activated Receptors (PPAR) in Immune Responses. Metabolism. 2021, 114, 154338. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.S. N-3 Fatty Acids and Serum Lipoproteins: Human Studies. Am. J. Clin. Nutr. 1997, 65, 1645S–1654S. [Google Scholar] [CrossRef] [PubMed]
- Stein, R.; Ferrari, F.; Scolari, F. Genetics, Dyslipidemia, and Cardiovascular Disease: New Insights. Curr. Cardiol. Rep. 2019, 21, 68. [Google Scholar] [CrossRef] [PubMed]
- Papakonstantinou, E.; Oikonomou, C.; Nychas, G.; Dimitriadis, G.D. Effects of Diet, Lifestyle, Chrononutrition and Alternative Dietary Interventions on Postprandial Glycemia and Insulin Resistance. Nutrients 2022, 14, 823. [Google Scholar] [CrossRef] [PubMed]
- Hilgendorf, K.I.; Johnson, C.T.; Mezger, A.; Rice, S.L.; Norris, A.M.; Demeter, J.; Greenleaf, W.J.; Reiter, J.F.; Kopinke, D.; Jackson, P.K. Omega-3 Fatty Acids Activate Ciliary FFAR4 to Control Adipogenesis. Cell 2019, 179, 1289–1305.e21. [Google Scholar] [CrossRef]
- Cheshmehkani, A.; Senatorov, I.S.; Kandi, P.; Singh, M.; Britt, A.; Hayslett, R.; Moniri, N.H. Fish Oil and Flax Seed Oil Supplemented Diets Increase FFAR4 Expression in the Rat Colon. Inflamm. Res. 2015, 64, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Akinkuolie, A.O.; Ngwa, J.S.; Meigs, J.B.; Djoussé, L. Omega-3 Polyunsaturated Fatty Acid and Insulin Sensitivity: A Meta-Analysis of Randomized Controlled Trials. Clin. Nutr. Edinb. Scotl. 2011, 30, 702–707. [Google Scholar] [CrossRef]
- Brown, T.J.; Brainard, J.; Song, F.; Wang, X.; Abdelhamid, A.; Hooper, L. Omega-3, Omega-6, and Total Dietary Polyunsaturated Fat for Prevention and Treatment of Type 2 Diabetes Mellitus: Systematic Review and Meta-Analysis of Randomised Controlled Trials. BMJ 2019, l4697. [Google Scholar] [CrossRef]
- D’Angelo, S.; Motti, M.L.; Meccariello, R. ω-3 and ω-6 Polyunsaturated Fatty Acids, Obesity and Cancer. Nutrients 2020, 12, 2751. [Google Scholar] [CrossRef]
- Siriwardhana, N.; Kalupahana, N.S.; Cekanova, M.; LeMieux, M.; Greer, B.; Moustaid-Moussa, N. Modulation of Adipose Tissue Inflammation by Bioactive Food Compounds. J. Nutr. Biochem. 2013, 24, 613–623. [Google Scholar] [CrossRef]
- Spencer, M.; Yao-Borengasser, A.; Unal, R.; Rasouli, N.; Gurley, C.M.; Zhu, B.; Peterson, C.A.; Kern, P.A. Adipose Tissue Macrophages in Insulin-Resistant Subjects Are Associated with Collagen VI and Fibrosis and Demonstrate Alternative Activation. Am. J. Physiol.-Endocrinol. Metab. 2010, 299, E1016–E1027. [Google Scholar] [CrossRef] [PubMed]
- Spencer, M.; Finlin, B.S.; Unal, R.; Zhu, B.; Morris, A.J.; Shipp, L.R.; Lee, J.; Walton, R.G.; Adu, A.; Erfani, R.; et al. Omega-3 Fatty Acids Reduce Adipose Tissue Macrophages in Human Subjects With Insulin Resistance. Diabetes 2013, 62, 1709–1717. [Google Scholar] [CrossRef]
- Rasic-Milutinovic, Z.; Perunicic, G.; Pljesa, S.; Gluvic, Z.; Sobajic, S.; Djuric, I.; Ristic, D. Effects of N-3 PUFAs Supplementation on Insulin Resistance and Inflammatory Biomarkers in Hemodialysis Patients. Ren. Fail. 2007, 29, 321–329. [Google Scholar] [CrossRef]
- Salsinha, A.S.; Socodato, R.; Rodrigues, A.; Vale-Silva, R.; Relvas, J.B.; Pintado, M.; Rodríguez-Alcalá, L.M. Potential of Omega-3 and Conjugated Fatty Acids to Control Microglia Inflammatory Imbalance Elicited by Obesogenic Nutrients. Biochim. Biophys. Acta BBA - Mol. Cell Biol. Lipids 2023, 1868, 159331. [Google Scholar] [CrossRef]
- Wei, Y.; Meng, Y.; Li, N.; Wang, Q.; Chen, L. The Effects of Low-Ratio n-6/n-3 PUFA on Biomarkers of Inflammation: A Systematic Review and Meta-Analysis. Food Funct. 2021, 12, 30–40. [Google Scholar] [CrossRef]
- Serhan, C.N.; Clish, C.B.; Brannon, J.; Colgan, S.P.; Chiang, N.; Gronert, K. Novel Functional Sets of Lipid-Derived Mediators with Antiinflammatory Actions Generated from Omega-3 Fatty Acids via Cyclooxygenase 2–Nonsteroidal Antiinflammatory Drugs and Transcellular Processing. J. Exp. Med. 2000, 192, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- López-Vicario, C.; Rius, B.; Quiles, J.; Alonso, V.; Lopategi, A.; Titos, E.; Claria, J. Pro-Resolving Mediators Produced from EPA and DHA: Overview of the Pathways Involved and Their Mechanisms in Metabolic Syndrome and Related Liver Diseases. Eur. J. Pharmacol. 2015, 785. [Google Scholar] [CrossRef] [PubMed]
- Su, C.-J.; Zhang, J.-T.; Zhao, F.-L.; Xu, D.-L.; Pan, J.; Liu, T. Resolvin D1/N-Formyl Peptide Receptor 2 Ameliorates Paclitaxel-Induced Neuropathic Pain through the Activation of IL-10/Nrf2/HO-1 Pathway in Mice. Front. Immunol. 2023, 14, 1091753. [Google Scholar] [CrossRef]
- Serhan, C.N.; Chiang, N.; Dalli, J. The Resolution Code of Acute Inflammation: Novel Pro-Resolving Lipid Mediators in Resolution. Semin. Immunol. 2015, 27, 200–215. [Google Scholar] [CrossRef]
- Clària, J.; López-Vicario, C.; Rius, B.; Titos, E. Pro-Resolving Actions of SPM in Adipose Tissue Biology. Mol. Aspects Med. 2017, 58, 83–92. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram of subjects included in the study.
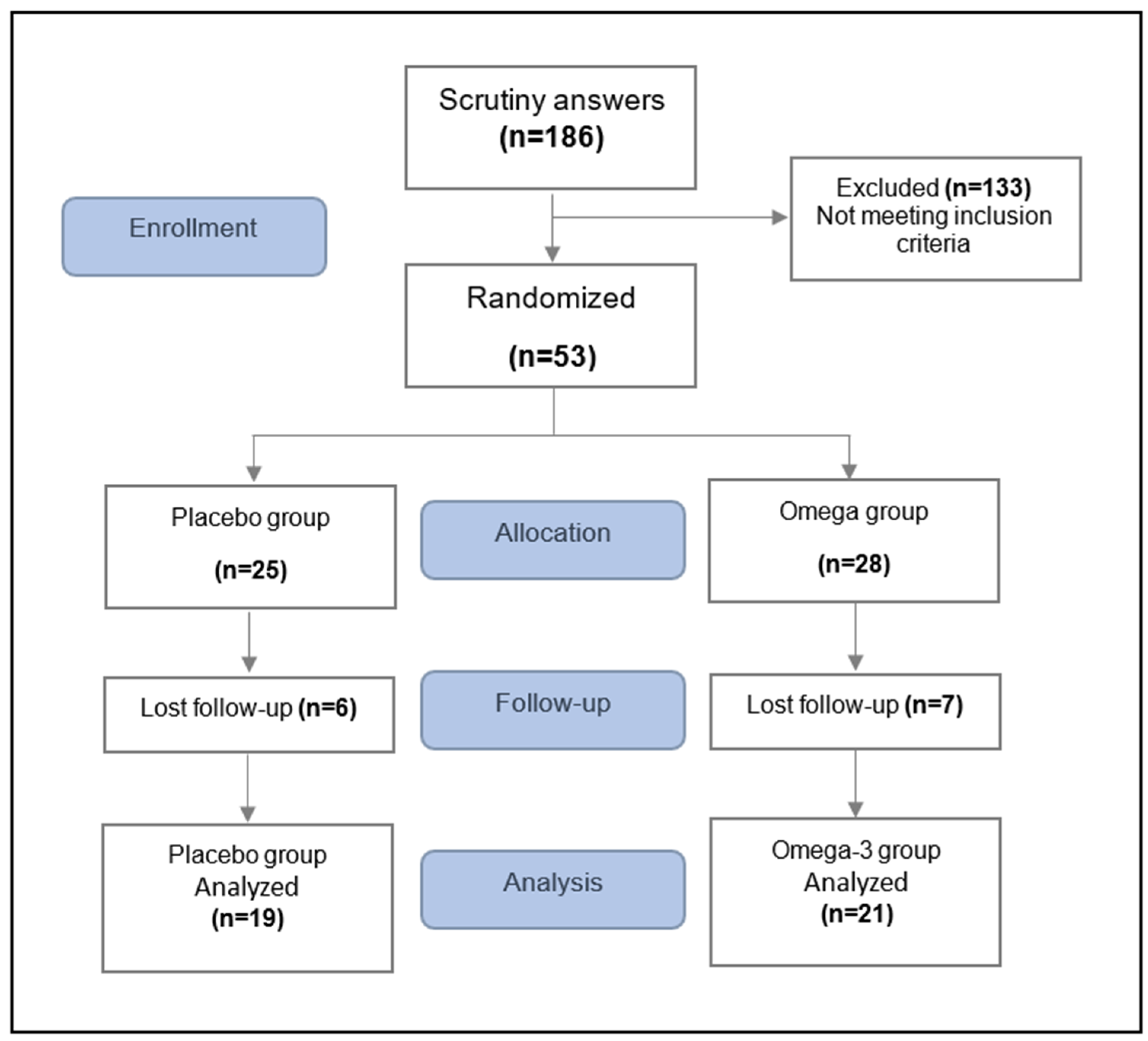

Table 1.
Nutritional variables in the study groups.
| Placebo group (n=19) | Omega-3 group (n=21) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | Baseline | Final | ∆ | Baseline | Final | ∆ | p1 | p2 | p∆ |
| Energy (kcal) | 2138 (1822–2324) | 1616 (1271–1838) | -548.2 (-822.8– -149) | 1928 (1706-3075) | 1271 (1046-1713) | -358.41 (-1311 - 42) | 0.038 | 0.060 | 0.964 |
| n-3 PUFAs (g) | 1 (0.7–1.6) | 2.9 (1.4–4.8) | 2.0 (0.62-3.31) | 1.2 (0.8–1.9) | 1.8 (1.1–4.4) | 2.0 (0.03-3.41) | 0.012 | 0.023 | 0.649 |
| n-6 PUFAs (g) | 10.9 (6.4–17.4) | 8.9 (7.7–11.9) | -1.9 (-10.5 – 2.9) | 11.4 (8.9–17.1) | 6.6 (5.3–7.7) | -3.3 (-5.9- -1.41) | 0.307 | 0.012 | 0.698 |
| n-6:n-3 ratio | 9.9 (7.5–13.1) | 3.4 (2.3–5.2) | -7.0 (-11.0- -3.1) | 9 (7.6–13.3) | 2.8 (1.7–5.2) | -5.6 (-10.9- -4.12) | 0.019 | 0.003 | 0.677 |
Data represented as median and interquartile range. Mann-Whitney U test and Wilcoxon test were used. Values of p <0.05 were considered statistically significant. ∆: Final - Baseline, p1 value represents the comparison between final and baseline in the placebo group, p2 value denotes the comparison between final and baseline in the omega-3 group, and p∆ values are the differences intergroup, Kcal: Kilocalories, g: gram, n-6: n-3 ratio: grams of omega-6 per 1 gram of omega-3.
Table 2.
Anthropometric and biochemical variables in the study groups.
| Placebo group (n=19) | Omega 3 group (n=21) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Baseline | 4 weeks | Final | ∆ | Baseline | 4 weeks | Final | ∆ | p1 | p2 | p∆ |
| Anthropometric | |||||||||||
| Weight (kg) | 103.0 ± 20.0 | 101.5 ± 19.5 | 100.8 ± 19.2 | -2.24 ± 3.4 | 96.7 ± 16.1 | 93.4 ± 15.4 | 92.3 ± 15.2 | -3.76 ± 3.5 | 0.004 | 0.001 | 0.157† |
| BMI (kg/m2) | 36.0 ± 4.7 | 35.7 ± 5.1 | 35.5 ± 4.9 | -0.50 ± 1.3 | 33.6 ± 3.4 | 32.9 ± 3.1 | 32.5 ± 3.0 | -1.24 ± 1.2 | 0.049* | 0.001* | 0.111† |
| Body fat (%) | 44.9 ± 5.8 | 44.7 ±6.1 | 43.6 ± 7.2 | -1.32 ± 2.4 | 41.7 ± 5.1 | 41.7 ± 5.2 | 41.1 ± 5.5 | -1.10 ±1.8 | 0.043 | 0.010 | 0.752 |
| WC (cm) | 108.6 ± 14.1 | 107.4 ± 14.6 | 104.6 ± 13.3 | -3.63 ± 2.4 | 104.2 ± 11.8 | 100.9 ± 10.5 | 98.7 ± 11 | -5.03 ± 3.3 | 0.001 | 0.001 | 0.158 |
| Biochemical | |||||||||||
| TC (mg/mL) | 160.4 ± 32.0 | 155.1 ± 35.3 | 160.2 ± 34.9 | -1.05 ± 12.4 | 171.1 ± 26.6 | 163.0 ± 23.9 | 166.4 ± 31.5 | -3.63 ± 18.8 | 0.213 | 0.230 | 0.629 |
| TGs (mg/mL)* | 167.3 ± 73.3 | 139.8 ± 62.1 | 146.5 ± 65.4 | -17.94 ± 47.3 | 195.3 ± 77.7 | 155.5 ± 63.8 | 155.0 ± 99.5 | -42.15 ± 85.3 | 0.019* | 0.003* | 0.494† |
| HDL-c (mg/mL) | 35.3 ± 7.1 | 34.1 ± 7.2 | 33.4 ± 6.5 | -2.61 ± 4.71 | 35.3 ± 6.4 | 33.5 ± 7.4 | 33.1 ± 8.0 | -2.52 ± 4.0 | 0.090 | 0.050 | 0.953 |
| LDL-c (mg/mL) | 91.7 ± 24.7 | 93.1 ± 25.8 | 97.9 ± 25.2 | 5.38 ± 16.0 | 97.3 ± 21.0 | 98.2 ± 21.4 | 102.2 ± 27.0 | 7.15 ± 17.8 | 0.346 | 0.216 | 0.754 |
| VLDL-c(mg/mL)* | 33.5 ± 14.6 | 27.8 ± 12.5 | 29.3 ± 13.0 | -3.55 ± 9.4 | 39.0 ± 15.5 | 31.1 ± 12.7 | 30.8 ± 19.9 | -8.57 ± 17.0 | 0.014* | 0.005* | 0.369† |
| Glucose (mg/mL) | 94.0 ± 9.4 | 95.1 ± 7.2 | 98.3 ± 9.6 | 4.27 ± 9.27 | 96.4 ± 10.8 | 95.0 ± 9.1 | 97.8 ± 10.7 | 1.89 ± 13.3 | 0.154 | 0.272 | 0.534 |
Data presented as mean ± standard deviation, analyzed by repeated measures ANOVA (adjusted by gender), and t test (p∆). *Friedman test, †Mann-Whitney U test, p values <0.05 considered statistically significant, ∆: Final - Baseline, p1 represents the comparison between final and baseline in placebo group, p2 denotes the comparison between final and baseline in the omega-3 group, and p∆ are the differences intergroup. BMI: Body mass index, WC: Waist circumference, TC: total cholesterol, HDL-c: High-density lipoprotein cholesterol, LDL-c: Low-density lipoprotein cholesterol, VLDL-c: Very-low-density lipoprotein cholesterol.
Table 3.
Prevalence of abdominal obesity in study groups.
| Baseline (%) | Final (%) | p value | ||
|---|---|---|---|---|
|
Placebo group (n=19) |
88.9 | 83.3 | 0.978 | |
|
Omega-3 group (n=21) |
95 | 60 | 0.016 | |
Data represented as percentages, McNemar test, p < 0.05, statistically significant.
Table 4.
Inflammatory variables in the study groups.
| Placebo group (n=19) | Omega-3 group (n=21) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | Baseline | Final | ∆ | Baseline | Final | ∆ | p1 | p2 | p∆ |
| Inflammatory | |||||||||
| TNF-α(pg/mL) | 0.52 (0.4-0.8) | 0.07 (0.05-0.11) | -1.85 (-4.52- -0.71) | 0.61 (0.4-1.6) | 0.07 (0.04-0.17) | -1.82 (-5.74- -0.59) | 0.002 | 0.001 | 0.745 |
| IL-6 (pg/mL) | 2.9 (0.9-7.8) | 4.7 (0.6-7.7) | 0.03 (-0.59-1.84) | 2.3 (0.7-6.4) | 2.0 (0.3-4.4) | -0.67 (-2.72- -0.01) | 0.407 | 0.010 | 0.015 |
| hs-CRP (mg/L) | 3.4 (2.7-5.7) | 2.7 (2.7-6.6) | -0.7 (-1.30-0.30) | 4.5 (2.0-10.1) | 2.4 (1.5-8.2) | -0.5 (-3.07-0.87) | 0.296 | 0.271 | 0.603 |
| IL-10 (pg/mL) | 5.9 (3.8-8.0) | 4.58 (3.3-5.1) | -2.0 (-5.0-0.05) | 5.3 (4.5-7.2) | 7.02 (4.3-12.1) | 1.4 (-0.7-4.6) | 0.081 | 0.035 | 0.001 |
| MCP-1 (pg/mL) | 233 (204-337) | 277 (234-313) | 18.3 (-97.3-66.35) | 266 (215-295) | 235 (174-274) | -29.6(-94.9-5.50) | 0.758 | 0.040 | 0.064 |
| RvD1 (pg/mL) | 443.3 (358-545) | 403 (264-567) | -16.8 (-237.8-92.50) | 466 (392-563) | 562 (473-779) | 129.3 (-90.1-193.5) | 0.586 | 0.048 | 0.041 |
Data are presented as median and interquartile range, Mann-Whitney U test and Wilcoxon test. Values of p <0.05 considered statistically significant. ∆: Final - Baseline, p1 value represents the comparison between final and baseline in the placebo group, p2 value denotes the comparison between final and baseline in the omega-3 group, and p∆ values are the differences intergroup. TNF-α: Tumor Necrosis Factor Alpha, IL-6: Interleukin 6, hs-CRP: High-Sensitivity C-Reactive Protein, IL-10: Interleukin 10, MCP-1: Monocyte Chemoattractant Protein 1, RvD1: Resolvin D1.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



