Submitted:
30 June 2024
Posted:
01 July 2024
You are already at the latest version
Abstract
Background/Objectives: An age-associated increase in serum levels of sex hormone binding globulin (SHBG) is considered to be one of the factors leading to the development of male hy-pogonadism. Aim of the study: to study the relationship between the concentration of sex hor-mone-binding globulin in the blood serum and the age of the man, the level of total and free testosterone. A single-center retrospective cross-sectional study was conducted. The results of laboratory tests of 162 male patients aged from 18 to 56 years (median - 34 years) were analyzed. Methods: The level of total testosterone and sex hormone binding globulin (SHBG) was deter-mined by chemiluminescent immunoassay. The level of free testosterone was determined by the calculation method according to Vermeullen. Statistical analysis was performed using SPSS Sta-tistics v23. Results: Correlation analysis did not reveal a significant relationship between age and SHBG levels, as well as between age and total testosterone levels. Serum SHBG concentration showed a significant (p
Keywords:
sex hormone binding globulin
; SHBG
; male hypogonadism
; free testosterone
1. Introduction
An age-associated increase in serum levels of sex hormone-binding globulin (SHBG) has been considered by several authors as one of the factors leading to the development of male hypogonadism [1,2]. It is hypothesized that an increase in SHBG levels in the blood leads to a decrease in free testosterone concentration, while the total testosterone level may remain within the reference range [3]. We were unable to find convincing studies confirming this point of view. Furthermore, this opinion contradicts the most compelling current concept explaining the physiology of steroid hormones - the “free hormone hypothesis,” according to which only the free fraction of steroid hormones can penetrate cells and exert biological effects [4]. This hypothesis suggests that only free testosterone is capable of exerting an antigonadotropic effect, i.e., influencing the production of luteinizing hormone. Accordingly, the functioning of the negative feedback mechanism is directed at maintaining a stable concentration of free, rather than total testosterone. Therefore, under conditions of a normally functioning hypothalamic-pituitary-gonadal axis, the concentration of free testosterone should remain normal at any SHBG concentration. To clarify the role of SHBG in the development of male hypogonadism, we conducted our own study aimed at investigating the relationship between serum sex hormone-binding globulin concentration, age of the male, and levels of total and free testosterone in the blood.
2. Materials and Methods
A single-center retrospective cross-sectional study was conducted. The results of laboratory tests of 162 male patients aged 18 to 56 years (median age - 34 years) who were examined at the “Mother and Child Yaroslavl” clinic from April 2022 to November 2023 were analyzed. The levels of total testosterone (normal range 12-30 nmol/L) and sex hormone-binding globulin (SHBG) (normal range 16-69 nmol/L) were determined by chemiluminescent immunoassay (CLIA). The level of free testosterone (normal range 225-900 pmol/L) was calculated using the Vermeullen method [5]. Statistical analysis was performed using SPSS Statistics v23. Normality of distribution was assessed using the Kolmogorov-Smirnov test. Differences between patient subgroups were evaluated using the Mann-Whitney test (for 2 groups) and Kruskal-Wallis test (for 3 or more groups). Correlation analysis was conducted using the Spearman correlation coefficient. To build a linear regression, the distribution of the dependent variable was normalized by removing outliers. Differences were considered significant at p <0.05.
3. Results
The level of sex hormone-binding globulin in the examined men varied in the range from 5.8 to 109.7 (median 28.9, interquartile range from 21.15 to 37.85) nmol/l. The total testosterone level ranged from 4.7 to 50.4 (median 17.83, interquartile range from 13.26 to 23.44) nmol/l. The calculated free testosterone ranged from 0.342 to 0.503 nmol/l (median 0.396, interquartile range from 21.15 to 37.85) nmol/l.
Correlation analysis did not reveal significant relationships between age and SHBG levels, as well as between age and total testosterone levels, but a significant (p=0.01) negative correlation between age and free testosterone levels was found (Figure 1). The correlation coefficient was 0.205, corresponding to a very weak relationship on the Chaddock scale.
To clarify the relationship between age of men and SHBG levels, we divided patients into 7 subgroups based on age: 18-24 years (n=13), 25-29 years (n=23), 30-34 years (n=51), 35-39 years (n=40), 40-44 years (n=17), 45-49 years (n=12), and 50-56 years (n=5) and compared the values of serum SHBG concentration in these groups (Figure 2).
No significant differences in SHBG levels were found between these groups (p = 0.548), which, combined with the results of correlation analysis, indicates no association between SHBG levels and age among men aged 18-56 years.
The evaluation of the relationship between serum SHBG concentration and total and free testosterone levels revealed a significant positive correlation between SHBG concentration and both total (p <0.001) and free testosterone (p = 0.042) (Figure 3).
The correlation with total testosterone was strong (correlation coefficient of 0.61). Linear regression analysis resulted in a statistically significant model (p <0.001), indicating that a 1 nmol/L increase in SHBG concentration leads to a 0.275 nmol/L increase in total testosterone concentration. The R2 coefficient for the model was 0.358, suggesting the model is not entirely acceptable.
For free testosterone, the correlation was very weak, and the significance of the differences was close to the threshold, indicating no association between SHBG levels and free testosterone concentration. These findings suggest that an increase in blood SHBG concentration leads to an increase in total testosterone levels but does not decrease free testosterone concentration.
To assess the impact of abnormal SHBG concentrations on total and free testosterone levels, patients were divided into 3 groups: those within the reference range (16-69 nmol/L) (n=136), below 16 nmol/L (n=20), and above 69 nmol/L (n=6). No significant differences in free testosterone concentration were found between patients with normal and abnormal SHBG values (p=0.163) (Figure 4).
However, total testosterone values in these groups showed significant differences (p <0.0001) (Figure 5). Patients with low SHBG had lower total testosterone levels compared to those with normal SHBG, while those with abnormally high SHBG had higher total testosterone levels than men with normal SHBG values. These results confirm that SHBG concentration influences total but not free serum testosterone levels.
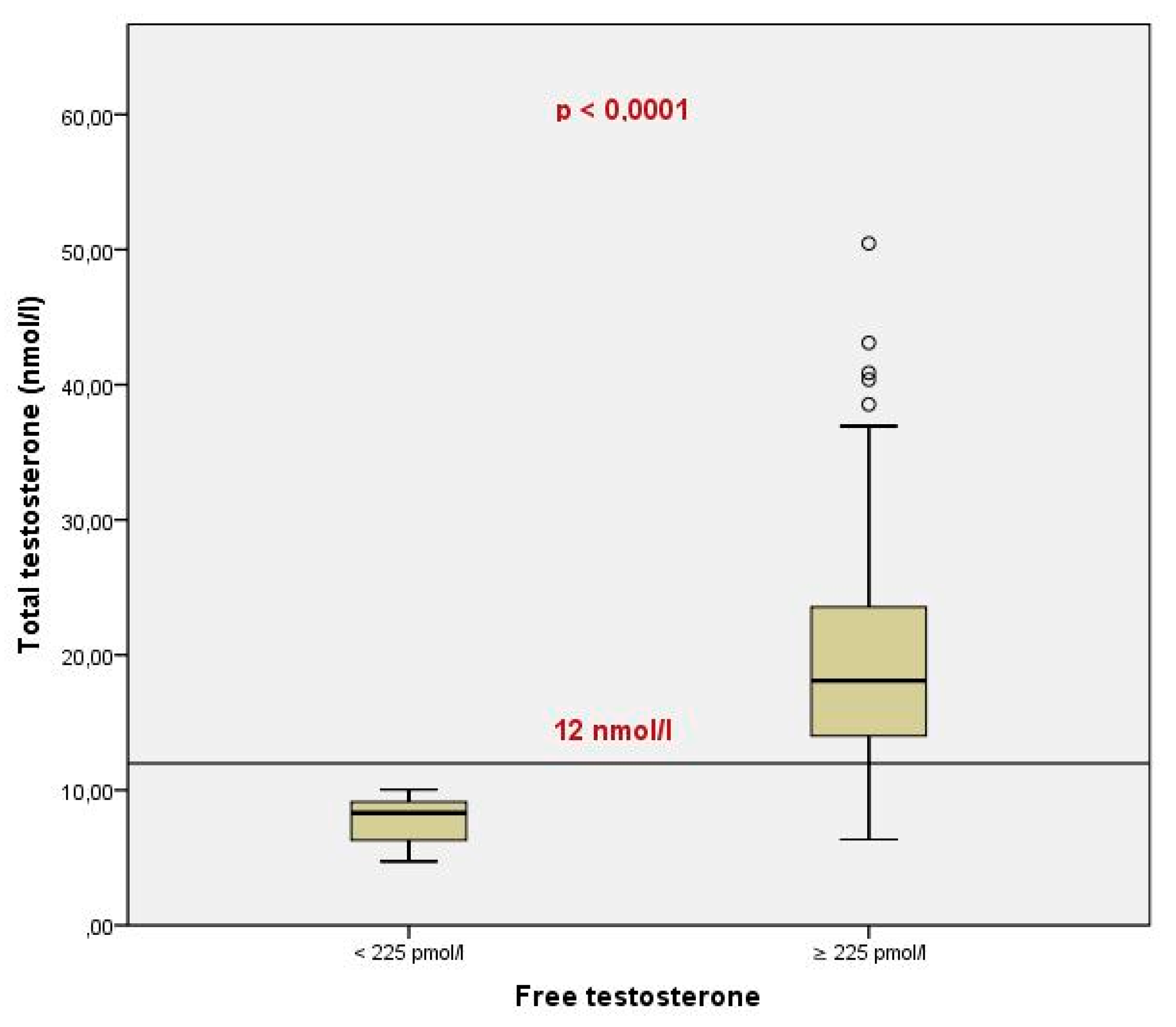
Total testosterone levels differed significantly between patients with free testosterone levels above (n=147) and below (n=7) 225 pmol/L (p<0.0001). In all patients with decreased free testosterone, total testosterone levels were below 12 nmol/L (Figure 6).
Moreover, among men with total testosterone less than 12 nmol/L (n = 26), 73% (n=17) had free testosterone concentrations above the lower limit of the reference interval, while 27% (n=9) had concentrations below. These findings suggest that assessing SHBG levels and calculating free testosterone is advisable only for patients with decreased total testosterone levels.
4. Discussion
In the present study, we did not find an association between serum SHBG levels and age in men aged 18-56 years, although several large studies have reported an increase in SHBG concentration with age. Muller M. et al. observed a 1.1% increase in blood SHBG concentration per year in men aged 40 to 80 years [6]. Liu P.Y. estimated an annual increase in blood SHBG of 2.3-2.5% on average in men aged 18-90 years, with a more significant annual increase in SHBG observed in older men compared to younger men [7]. In our study, more than half of the men were younger than 35 years, two-thirds were younger than 40 years, and there were no elderly men. The age structure of the sample likely explains the lack of association between SHBG and age in our study.
We found a strong positive correlation between SHBG and total testosterone levels in our study. The influence of SHBG concentration on free testosterone levels in our study was very weak, which we interpreted as a lack of association between SHBG levels and free testosterone concentration. This result is consistent with studies that have examined populations of men with high SHBG concentrations due to SHBG gene polymorphism, showing that an increase in serum SHBG concentration is associated with an increase in total testosterone concentration, but free testosterone concentration does not change significantly [8,9].
Interestingly, none of the patients with a total testosterone level above 12 nmol/l had a reduced concentration of free testosterone, while 27% of men with a total testosterone level below 12 nmol/l had reduced concentrations of free testosterone. Similar data were obtained in the European Male Ageing Study (EMAS), where an examination of 3068 men aged 40 to 79 years showed that low concentrations of free testosterone were observed in only 27.3% of men with a total testosterone level below 12 nmol/l [10]. The same study also showed that it is low concentrations of free, rather than total, testosterone that are associated with symptoms of hypogonadism [10]. In this regard, it seems advisable to recommend measuring SHBG levels and calculating free testosterone levels in patients with reduced total testosterone levels. This will help avoid overdiagnosis of hypogonadism, as not all patients with reduced total testosterone will have low concentrations of free testosterone and symptoms of hypogonadism. On the other hand, there is no need to test free testosterone in men with normal total testosterone values.
5. Conclusions
The serum level of SHBG in men aged 18-56 years is not significantly associated with age. An increase in serum SHBG concentration in men is accompanied by a rise in total testosterone levels, but it does not have a substantial impact on free testosterone concentration. It is advisable to measure SHBG levels and calculate free testosterone in patients with a total testosterone level below 12 nmol/L, as when total testosterone levels are above 12 nmol/L, the concentration of free testosterone always corresponds to normal values, whereas when total testosterone levels are below 12 nmol/L, reduced free testosterone concentration is observed in only 27% of patients.
Author Contributions
Conceptualization, Aleksei Ryzhkov and Igor Shormanov; Data curation, Alexandra Vasilyeva; Formal analysis, Alexandra Vasilyeva; Investigation, Alexandra Vasilyeva; Methodology, Aleksei Ryzhkov; Project administration, Aleksei Ryzhkov; Resources, Svetlana Sokolova; Software, Aleksei Ryzhkov; Supervision, Svetlana Sokolova; Validation, Aleksei Ryzhkov and Svetlana Sokolova; Visualization, Aleksei Ryzhkov; Writing – original draft, Aleksei Ryzhkov; Writing – review & editing, Igor Shormanov.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to retrospective type of study.
Informed Consent Statement
Patient consent was waived due to the study is associated only with laboratory data without the ability to identify patients.
Data Availability Statement
Dataset available on request from the authors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Tishova, Y. A., Mskhalaya, G. Z., & Kalinchenko, S. Y. E. (2010). Age-related hypogonadism in men with metabolic syndrome. Diabetes mellitus, 13(1), 21-25. [CrossRef]
- Parshin AG, Eloyev RA. Our experience in examining urological patients with a high level of sex hormone-binding globulin. Experimental and Clinical Urology. 2018(2):73-7.
- Kuznetsova EA, Adamchik AS, Goncharov NP, Katsiya GV. Choice of diagnostic method for hypogonadism in obese men with metabolic syndrome. Andrology and Genital Surgery. 2015(3):10-6. [CrossRef]
- Mendel, CM. The free hormone hypothesis: a physiologically based mathematical model. Endocrine reviews. 1989;10(3):232-74.
- Vermeulen A, Verdonck L, Kaufman JM. A critical evaluation of simple methods for the estimation of free testosterone in serum. The Journal of clinical endocrinology and metabolism. 1999;84(10):3666-72. [CrossRef]
- Muller M, den Tonkelaar I, Thijssen JH, Grobbee DE, van der Schouw YT. Endogenous sex hormones in men aged 40-80 years. Eur J Endocrinol. 2003;149(6):583-9. [CrossRef]
- Liu PY, Beilin J, Meier C, Nguyen TV, Center JR, Leedman PJ, et al. Age-related changes in serum testosterone and sex hormone binding globulin in Australian men: longitudinal analyses of two geographically separate regional cohorts. The Journal of clinical endocrinology and metabolism. 2007;92(9):3599-603. [CrossRef]
- Ohlsson C, Wallaschofski H, Lunetta KL, Stolk L, Perry JR, Koster A, et al. Genetic determinants of serum testosterone concentrations in men. PLoS genetics. 2011;7(10):e1002313. [CrossRef]
- Svartberg J, Schirmer H, Wilsgaard T, Mathiesen EB, Njølstad I, Løchen ML, et al. Single-nucleotide polymorphism, rs1799941 in the Sex Hormone-Binding Globulin (SHBG) gene, related to both serum testosterone and SHBG levels and the risk of myocardial infarction, type 2 diabetes, cancer and mortality in men: the Tromsø Study. Andrology. 2014;2(2):212-8. [CrossRef]
- Rastrelli G, O’Neill TW, Ahern T. Symptomatic androgen deficiency develops only when both total and free testosterone decline in obese men who may have incident biochemical secondary hypogonadism: Prospective results from the EMAS. 2018;89(4):459-69. [CrossRef]
Figure 1.
The results of the correlation analysis between the age and the serum level of SHBG (a), total testosterone (b) and free testosterone (c).
Figure 1.
The results of the correlation analysis between the age and the serum level of SHBG (a), total testosterone (b) and free testosterone (c).
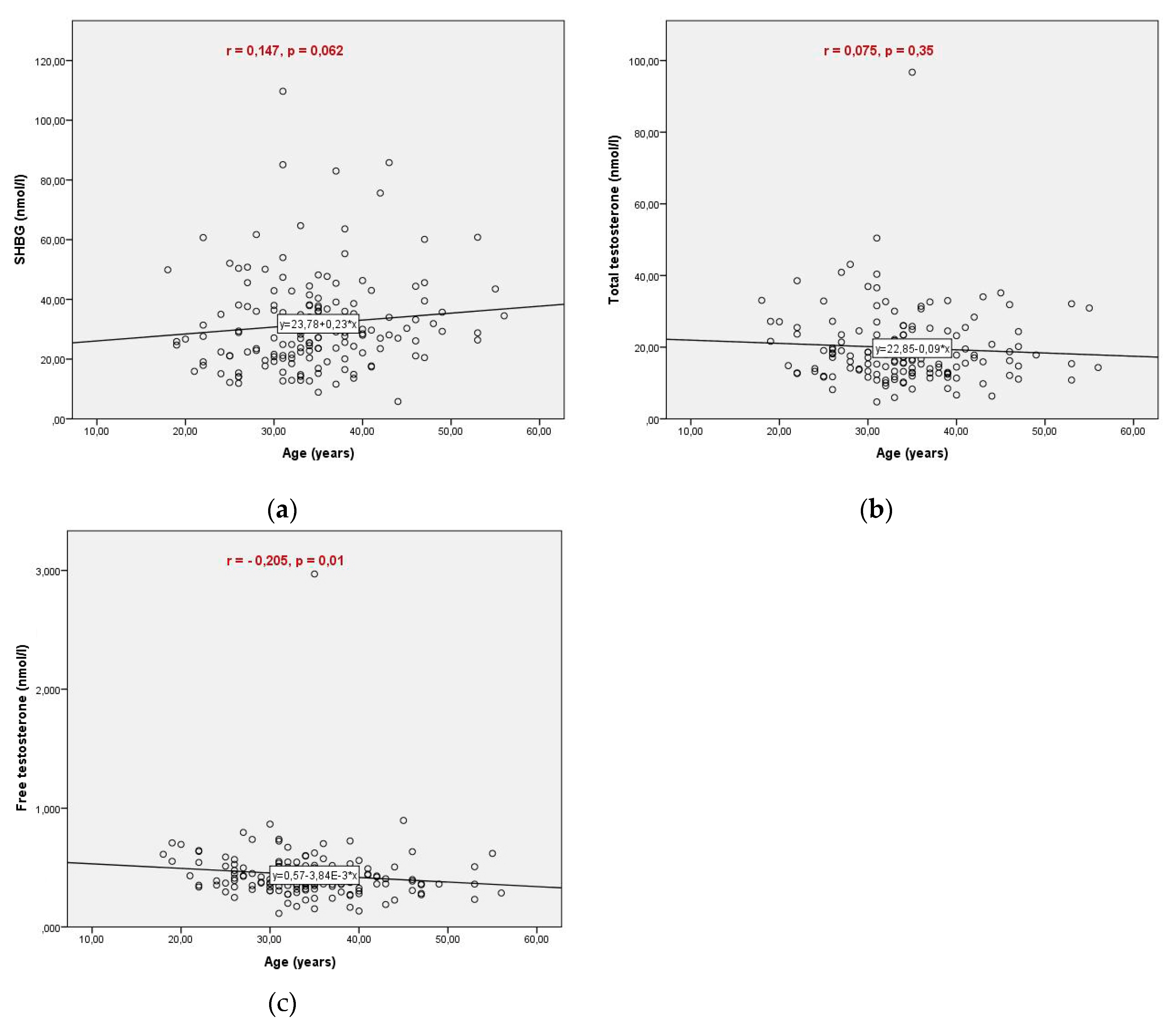
Figure 2.
Values of blood SHBG levels in different age groups.
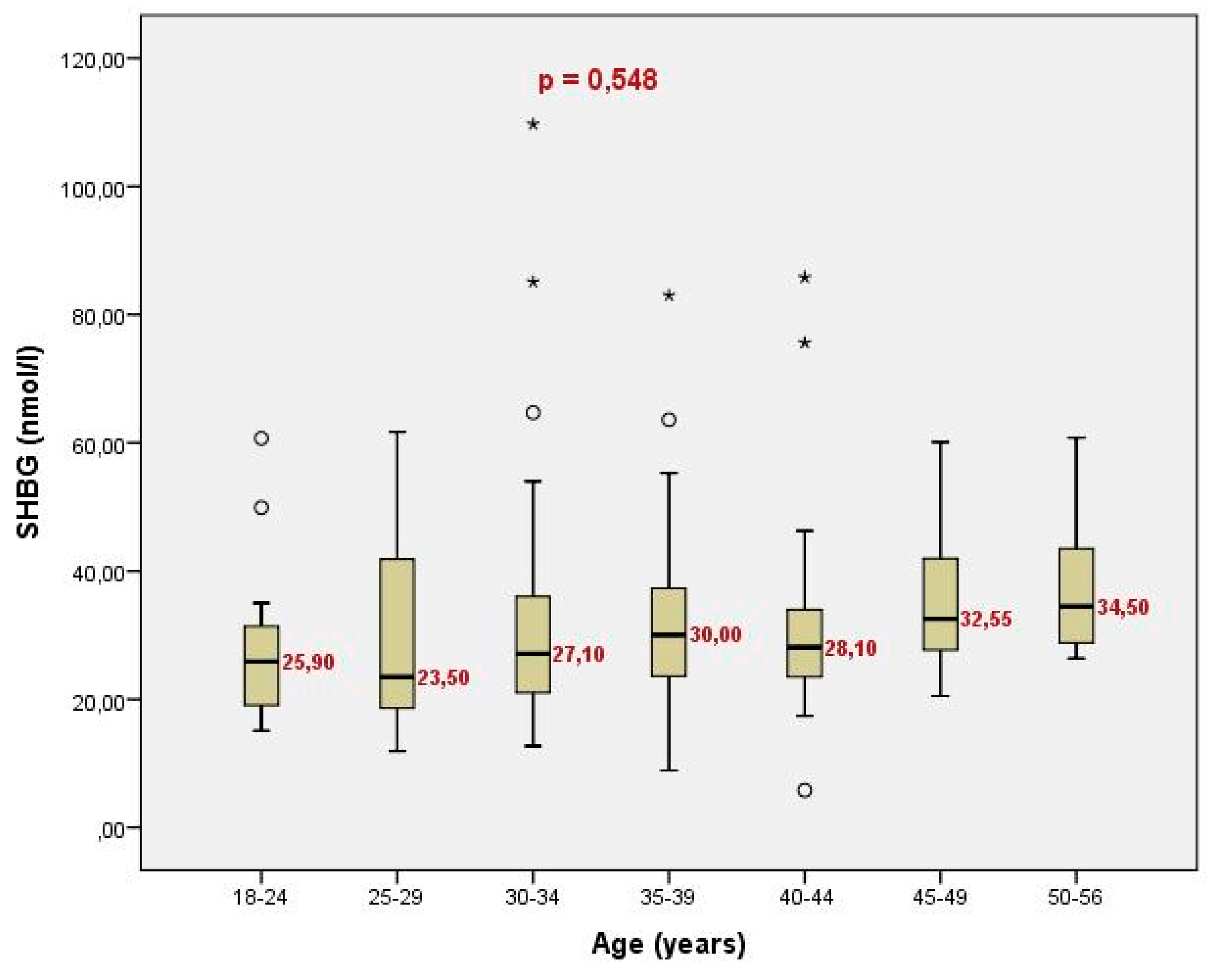
Figure 3.
Correlation between serum SHBG concentration and total (a) and free (b) testosterone levels.
Figure 3.
Correlation between serum SHBG concentration and total (a) and free (b) testosterone levels.
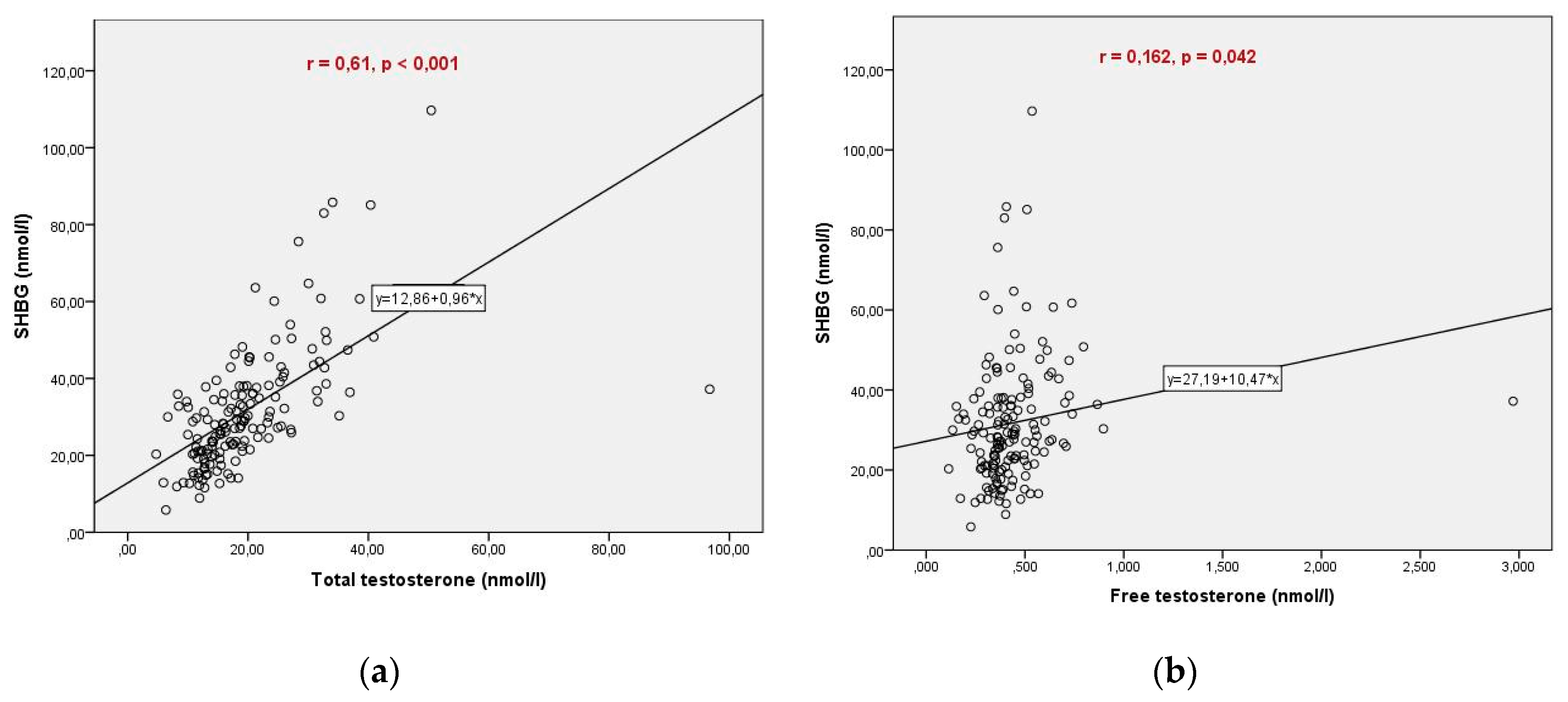
Figure 4.
Free testosterone levels in patients with normal and abnormal SHBG values.
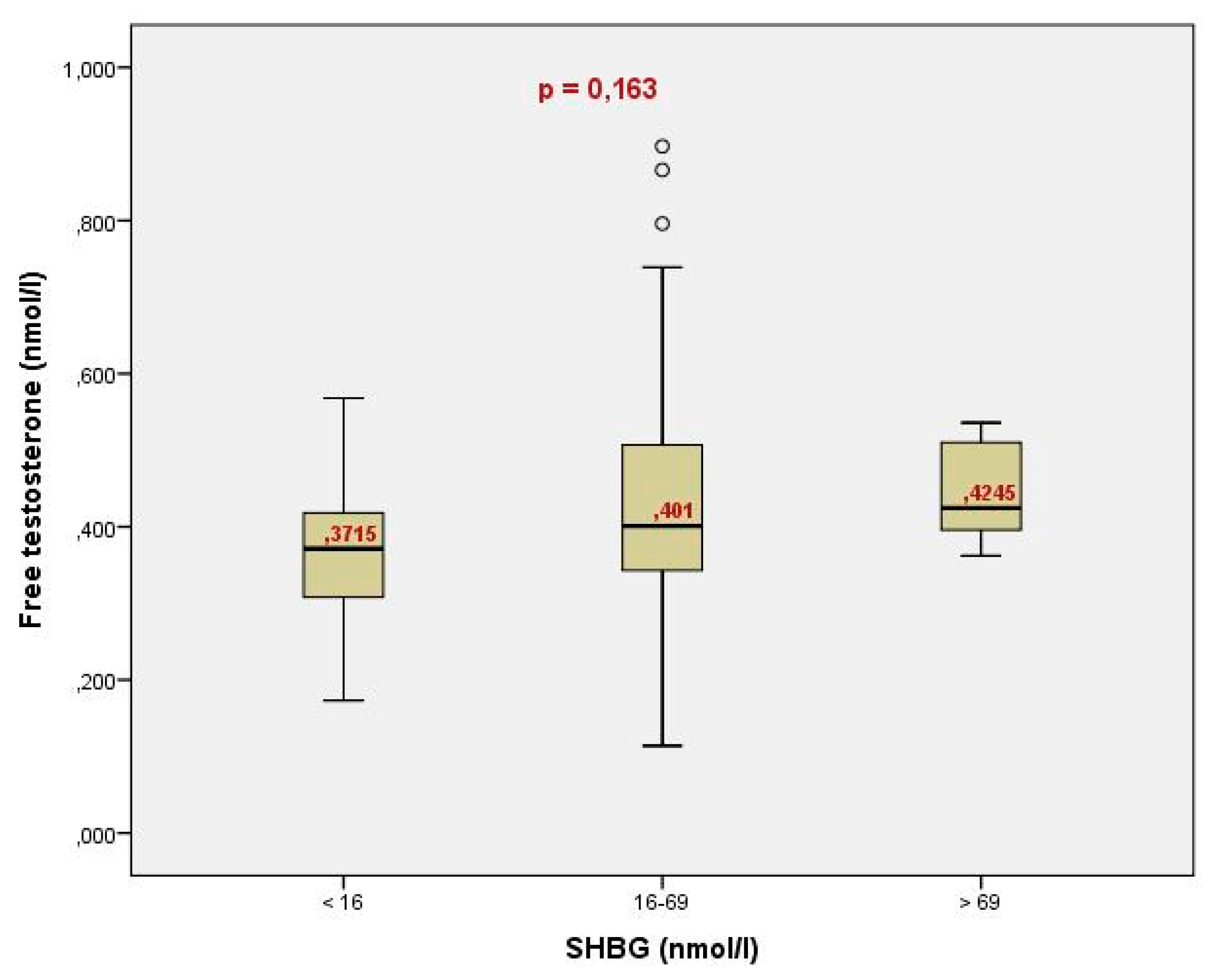
Figure 5.
Total testosterone levels in patients with normal and abnormal SHBG values.
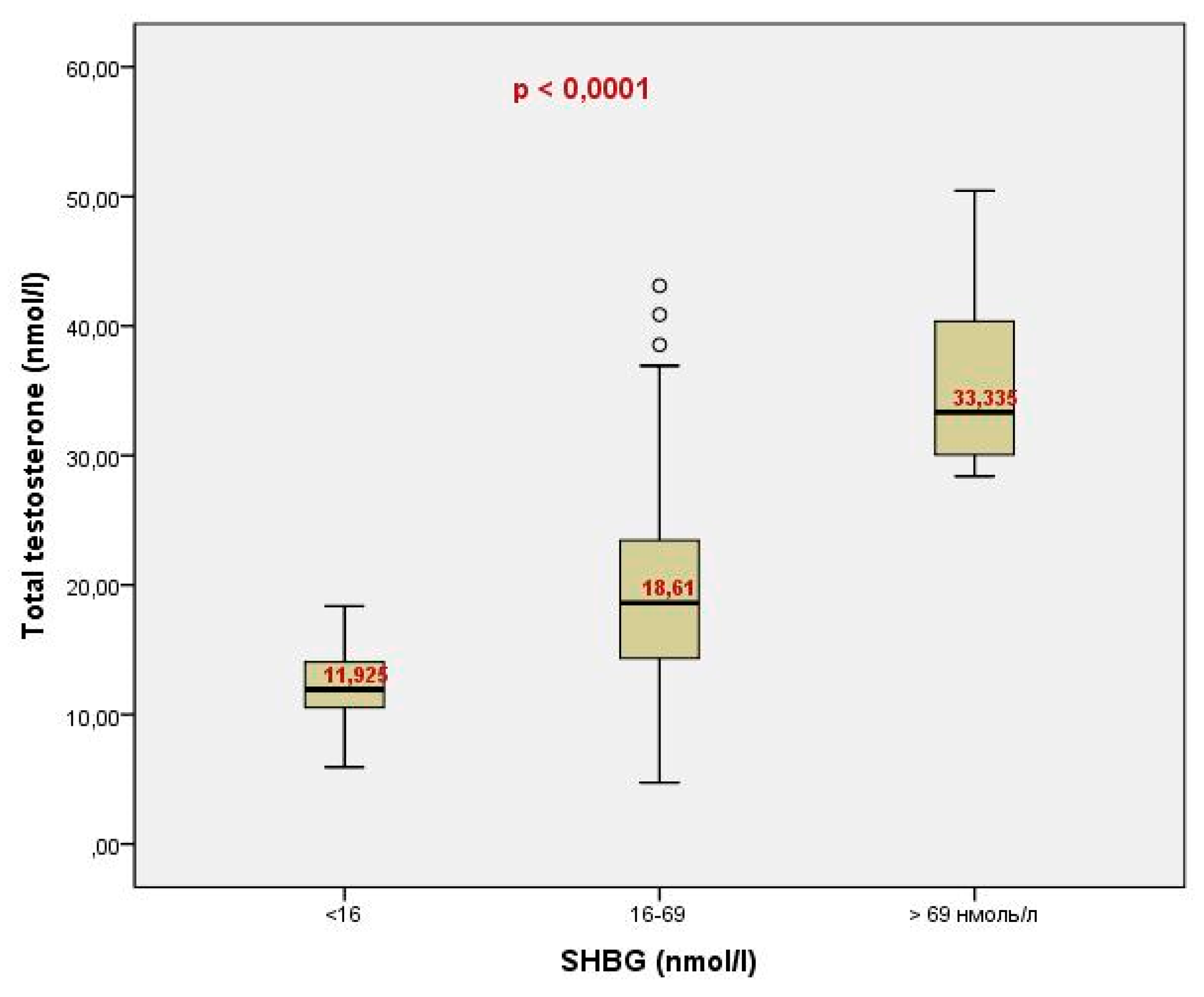
Figure 6.
Total testosterone levels in patients with free testosterone levels above and below 225 pmol/L.
Figure 6.
Total testosterone levels in patients with free testosterone levels above and below 225 pmol/L.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



