
Submitted:
01 July 2024
Posted:
02 July 2024
You are already at the latest version
Abstract
Cardiovascular diseases, which are the leading cause of death in Croatia, are linked to the high prevalence of hypertension. Both are associated with high salt intake which was determined almost two decades ago when Croatian Action on Salt and Health (CRASH) was launched. The main objective of the present study was to evaluate salt, potassium, and iodine intake using 24-hour urine samples in a random sample of adult Croatian population, and to analyse trends in salt consumption after the CRASH has intensively started. Methods: In this national population-based EH-UH 2 study performed in 2018-2021 (participation rate 72 %) in which we analysed a single 24-hour urine sample, 1067 adult participants (mean age 57.12 (SD 13.9), men 35%) were included. Results: Mean salt and potassium intakes were 8.6 g/day (IQR 6.2-11.2) and 2.8 g/day (IQR 2.1-3.5), respectively, with sodium-to-potassium ratio of 2.6 (IQR 1.8-3.3). We detected a decrease of 17.6% (2 g/day less) in salt consumption compared to our previous salt-mapping study. However, only 13.7%, and 8.9 % met the WHO salt and potassium recommended target of 5 g/day, and 3.5 g/day, respectively. Salt intake was higher, and potassium ingestion was lower in rural vs. urban regions, and in continental vs. Mediterranean parts of Croatia. Moderate to severe iodine insufficiency was determined in only 3% adult participants. Conclusion: In the last fifteen years, salt consumption has been significantly reduced in Croatian adult population because of intensive and broad CRASH program led by the Croatian Society of Hypertension and the Croatian Hypertension League. However, salt intake is still too high, and potassium ingestion is too low. With expected more active engagement and help of the government, obtained results could be significantly improved. Salt reduction programs are most cost-effective methods of cardiovascular disease prevention and should be considered more seriously by the government and health policy makers.
Keywords:
salt
; sodium
; potassium
; iodine
; 24-hour urine
; population-based study
1. Introduction
According to the World Health Organization (WHO) Global Report on Hypertension, high blood pressure (BP) is the main risk factor for early death worldwide [1]. High salt consumption was the major cause of hypertension and more than 3 million deaths, and 70 million disability-adjusted life years (DALYs) globally are attributed to high sodium intake [2]. The latest Global Burden Disease Study (GBDS) report states that high sodium consumption was responsible for 1.72 million deaths and 40.54 million DALYs due to cardiovascular disease (CVD), an increase of 41.08% and 33.06%, respectively, compared to 1990 [3]. The total number of deaths from chronic kidney disease (CKD) associated with increased salt intake was 45,530, while the number of DALYs was 1.32 million [4]. It was also confirmed that high salt intake increases the risk of type 2 diabetes [5]. A meta-analysis found that reduction of 100 mmol/day in 24-hour urinary sodium excretion was associated with systolic BP reduction of 5.56 mmHg which may lead to a slowing of CKD progression and a reduction in CVD risk regardless of whether the patient has diabetes or not [6,7,8]. In 2013, the WHO recommended to all Member States to reduce population salt intake by 30%, as a part of the 9 global voluntary targets to reduce premature mortality from chronic non-communicable diseases (NCD) by 25% by 2025 [9]. Since reducing salt intake is the most cost-effective interventions to reduce the burden of NCDs, it is therefore considered a priority action for all countries [10,11,12,13]. In 2022 CVDs were the main cause of death in Croatia (39.1%), and the age-standardized death rate in Croatia was significantly higher than the EU average (591/100,000 vs. 344/100,000) [14]. Ischemic heart disease was the leading cause of death (12.2% or 6925 deaths), and hypertensive disease was in the second place (9.2% or 5231 deaths), which indicates that hypertension is the main cause of death in Croatia. High BP ranks second after smoking as an important risk factor for DALYs in Croatia [15]. The crude prevalence of hypertension in Croatia is very high (50.9%), which is higher than 15 years ago [16,17]. According to the recent study, published in 2023, authors estimated that men from Croatia will have the highest age-adjusted prevalence of hypertension worldwide, reaching 41.1% in 2040 [18]. A Declaration on the importance of starting a national campaign to reduce salt intake in Croatia was accepted at the Congress of the Croatian Society for Hypertension in 2006, and in 2007 the Croatian Action on Salt and Health (CRASH) has started [19,20,21,22,23,24]. The CRASH program was prepared according to the WHO recommendations [25]. At that time, the average intake of salt determined from the sodium in 24- hour urine was 11.3 g per day (men 13.37 g, women 10.37 g) [26,27]. The education of population, healthcare workers, and patients started aiming to increase awareness of harmful effects of excessive salt intake, and negotiations started with food industry aiming to reformulate recipes. In 2015 the Ministry of Agriculture adopted the Ordinance on Cereals and Cereal Products which determined that the proportion of salt in ready-to-eat baked bread should not exceed 1.4%. and in 2022, as the second step, determined that the salt content of ready-to-eat baked bread, as well as the baked pastry, should not exceed 1.3% [27,28]. From 2010 to 2019, the intake of salt by eating bread and bakery decreased by about 14% and 28%, respectively, and most of the bakery industry was found to be compliant with the regulation (72% of breads and 66% of bakery products had a salt content <1.4%) [27,29]. The biggest Croatian meat industry PIK Vrbovec decreased content of salt in all products for an average of 25% [27]. Maintaining a balance between sodium and potassium is important for the regulation of BP and the CV health. Adequate potassium intake could alleviate harmful effects of high salt consumption on BP and CV health [30,31]. Recommendations for daily potassium intake vary among institutions, and the WHO recommended of at least 3510 mg/day which is in line with the European Food and Safety Authority which recommends adequate intake of 3500 mg for both sexes [32,33,34]. The average daily potassium intake worldwide is around 2250 mg, which is below all the recommended values [35]. According to the results from the Salt Substitute and Stroke Study (SSaSS) the most effective way to prevent CVD in communities where potassium intake is low is to use potassium-enriched salts [36]. Progressively more studies indicate that sodium-to-potassium ratio independently predicts the upcoming risk of CVD events, and the WHO recommended sodium-to-potassium ratio ≤ 1 [37,38]. Due to universal salt iodination law introduced in 1996, Croatia is nowadays iodine sufficient country. In the Republic of Croatia there is a legal regulation of mandatory iodization of all types of salt with 15-23 mg of iodine per kilogram of salt [39,40,41,42,43,44]. The question was raised whether iodine intake would be sufficient if salt intake would be reduced to recommended values of 5 g per day [45]. The objective of our study was to estimate salt, potassium and iodine intake in a random sample of the Croatian adult population by evaluating sodium, potassium and iodine excretion in 24-hour urine samples.
2. Materials and Methods
2.1. Study Design and Recruitment
This cross-sectional study was a part of the EH-UH 2 survey (Epidemiology of arterial hypertension and salt intake in Croatia), a nationally representative survey of noninstitutionalized persons in the Croatia which involved collecting anthropometric, demographic, lifestyle and biological marker data from the general adult population to assess risk factors for cardio-kidney-metabolic health, and the prevalence of major NCDs. A total of 2021 participants were included by random selection from the general population using randomization numbers obtained from the registry of the family physician (the randomization numbers represent the ordinal numbers of the archive of each family physicians’ practice). The participants selected via the randomisation list were informed about the project by telephone call from family physician and were included in the study according to the exclusion and inclusion criteria. Exclusion criteria for participation in the project were persons with terminal illness, dementia, paresis, amputation or immobilisation of a limb, acute illness, convalescent after surgery, pregnant women, lactating mothers, COVID-19 infection within the last 3 months, those who were prescribed therapy with diuretics in the last two weeks prior to the urine sample collection date, and unsigned consent to participate in the research. The inclusion criteria were age over 18 years of age and a signed consent to participate in the research. In the case the invited subject had one or more exclusion criteria, the family physician contacted the next subject from the randomization list. For iodine status analysis, subjects with thyroid disorders or known consumption of iodine supplements were also excluded. After the participants had been included in the study, the nurses, members of the mobile examination team (MET) made an appointment for home visit. The home visit started with signing the consent to participate in the study. After signing informed consent, every participant was attributed a personal identification code to allow anonymization, and the first measurements of BP and heart rate were taken. Participants were given instruction on how to properly collect and handle urine during a 24-hour period and were instructed to fast for 12 hours prior to the examination at which blood samples would be taken. At the end of the home visits, the participants were invited for outpatient examinations. Outpatient examinations were organized on Fridays and Saturdays; thus, a single 24-hour urine was collected during regularly working day (Thursday or Friday) to avoid weekend family/friends’ meetings and eating (lunch, dinner, barbecue), and not during the festive seasons. It was carried out in three steps: (a) questionnaire survey, (b) physical measurements, and (c) blood drawn, spot urine sample and 24-hour urine collections. Nurses, physicians, pharmacists, fellows, residents and medical students who were members of MET were educated to collect study and clinical data in a standardized manner.
2.2. Questionnaire
The questionnaire (face-to-face interview) was used to collect data on participant’s demographic (age, sex, place of residence), socio-economic status (SES), lifestyles (physical activity, smoking habit, alcohol consumption, diet, frequency of high salt food consumption, fruit and vegetable consumption, knowledge on dietary salt), personal and family history of cardio-kidney-metabolic diseases, and drug therapy.
2.3. Anthropometry (Physical Measurements)
The outpatient examinations of the participants included anthropometric data measurements, measurement of brachial BP, central BP and arterial stiffness (pulse wave velocity, PWV), recording of electrocardiogram (ECG), and metabolic scale measurements followed by fasting blood drawing and collecting of morning spot urine sample. Few days before the outpatient examinations, participants were reminded to collect and bring 24-hour urine from the previous day. Office BP measurements were performed according to the European Society for Hypertension guidelines and recommendations of the Croatian Society of Hypertension [46,47]. BP was measured on both hands, and if there was a difference in BP over the left or right hand, as the higher value was taken as relevant, and further BP was measured on that arm. If there was no difference in BP between left and right arm, BP was measured on the non-dominant arm. BP and heart rate were measured using oscillometric device (OMRON M6 Comfort with smart cuff). The first measurement was discarded, and an average of the last two readings was used. Hypertension was defined as BP ≥ 140/90 mm Hg or taking medication for hypertension. The persons’ weight and height were measured while they were clothed only in their underwear without shoes.
2.3. Procedures of 24-Hour Urine Collection
Participants were provided with 2.5 l plastic polyethylene containers, and clear verbal explanation was given as well as detailed written instructions on how to collect the 24-hour urine sample emphasizing the importance of collecting every drop of urine. They were asked to discard the first urine voided on the day of their collection and to collect all urine voided during the subsequent 24-hour period, ending with the first urine void the following morning. On the outpatient visit, the MET staff measured and recorded the 24-hour urine volume, thoroughly mixed the collection, and retained three 2ml aliquots which were stored at 4° C and shipped the same day: the first one to the Central Laboratory in University Hospital Centre Zagreb where urine creatinine, potassium and sodium were analysed; the second aliquot for iodine analyses was sent to the laboratory of University Hospital Centre Sestre milosrdnice, Zagreb. The third aliquot was left as back-up, if needed. The total volume of urine collected was measured using a measuring cylinder. A quality assurance to avoid inclusion of incomplete urine collections (under/ over-collected) was applied, and 24-hour urine specimens were considered incomplete if: (i) start and end time were not recorded and could not be ascertained; (ii) length of collection time was out of range of 22–26 hours; (iii) total urine volume was less than 500 ml; (iv) a female participant was menstruating; (v) a participant reported that more than a few drops of urine were missed during collection. Further predefined criteria for a high likelihood of incomplete urine collection were values of urine creatinine content referred to body weight outside 2 standard deviations of the sex-specific distribution (5.9–26.0 mmol/24 h for men and 4.0–16.4 mmol/24 h for women). Figure 1. shows stepwise procedure for the selection of valid participants according to protocol adherence, quality control and completeness of 24-hour urine collections. For iodine status analysis, further 119 subjects with thyroid disorders or known consumption of iodine supplements were also excluded. Sodium and potassium content in the urine were determined on the Abbott Alinity CC analyser using the ion-selective electrode, indirect method after dilution of the sample (method of indirect potentiometry) (Alinity, Abbott, USA). Creatinine content was determined using the enzymatic method with creatinine on the same analyser. Calibration was performed using the same company calibrators traceable to the IDMS method and NIST reference material SRM 967 (substance creatinine purity of 99.7 ± 0.3%). The content of iodine was determined by the Modified Microplate Method for the Determination of Urinary Iodine Concentration. It is a colorimetric determination method of the Sandell-Kolthoff reaction with a microplate reader. Standards and reagents were manually prepared, with a limit of detection 5 ug/L. Internal quality control data (Seronorm, Norway) from 2018 to 2021 was less than 10%. External quality control data was positively accomplished by Centres for Disease Control and Prevention (CDC), Atlanta, USA. Quality control in 2018 data were: accuracy 1.4% for sodium, 2.7% for potassium and 3.0% for creatinine with variation coefficient 2.04% for sodium, 1.43% for potassium and 2.57% for creatinine. In 2019 quality control data were: accuracy 0.91% for sodium, 1.48% for potassium, and 1.71% for creatinine with variation coefficient 1.34% for sodium, 1.69% for potassium and 2.44% for creatinine The respective data for the period 2021 were: accuracy 2.01% for sodium, 0.31% for potassium, 8.8% for iodine, and 4.41% for creatinine with variation coefficient 1.60% for sodium, 1.88% for potassium, 4.4% for iodine, and 2.08% for creatinine. Values for sodium or potassium (mmol/24 h) were converted into g/day (1 mmol = 0.023 g of sodium, 1 mmol = 0.039 g of potassium) to estimate dietary intake. The sodium value was multiplied by 2.5421 to convert dietary sodium intake into salt (NaCl) intake. Then, sodium values were multiplied by 1.05 (if approximately 95% of sodium ingested is excreted in the urine) [48]. Potassium dietary intake was calculated assuming 85% of the potassium ingested is excreted in the urine [49]. Urinary iodine was expressed in µg/l using multiplier 1.08 assuming 92% of iodine ingested is excreted in the urine. The cut-off values according to the WHO/EURO protocol were used [50]: < 5 g/24-hour for salt consumption, >9 0 mmol/24-hour for potassium consumption, for iodine consumption: insufficient (<100 µg/l) with subcategories: severe (<20 µg/l), moderate (20–49 µg/l), mild (50–99 µg/l); adequate consumption (100–199 µg/l); consumption above requirement (200–229 µg/l); excessive consumption (≥ 300 µg/l) [51].
2.4. Statistical Analysis
According to the WHO/PAHO Regional Expert Group for Cardiovascular Disease, to detect approximately 1 g reduction in salt intake over time using 24-hour urinary sodium excretion (difference ~20 mmol/24 hour), with a standard deviation of 75 mmol/day (alpha = 0.05, power = 0.80), a minimum sample of 120 individuals per stratum is recommended [48]. Thus, a minimum recommended sample size of 170 was estimated per age and sex groups and adjusted for an anticipated non-response rate of 30% (this was non-response rate in our previous survey). The population was stratified in groups by sex (men and women) and by age (A. 18–29 years; B. 30–44 years; C. 45–59 years; D 60–75 years), and urban/rural and Mediterranean/continental areas. Finally, 1942 individuals were needed to be selected (total n = 170 x 8 groups/0.7 attrition = 1942). In relation to the geographical regions of participants’ place of residence in this survey, we divided group into five different regions of Croatia: Central part (continental), North-West part (continental), Slavonia (continental), Istria, Croatian Littoral, Gorski kotar region (Mediterranean mountain), Dalmatia (Mediterranean) (Figure 3). According to the WHO recommendation, the prevalence of 24-hour sodium excretion lower than 85 mmol (corresponding to 5 g of salt) per day was calculated. All statistical analyses were carried out with IBM SPSS Statistics 28.0.0.0. (IBM Corporation, Armonk, NY, USA). For continuous variables, after testing for normal distribution (Kolmogorov-Smirnov and Shapiro-Wilk tests), either a Student’s t-test for unpaired samples or analysis of variance (ANOVA) or the Mann-Whitney test (for non-normally distributed results) was used to assess differences between group means, and the Pearson chi-square test was performed to determine associations between categorical variables. The results were reported as mean (standard deviation- SD), median (interquartile range -IQR), or percentages, as appropriate. Pearson and Spearman correlation coefficients were calculated to obtain information about the relationships between variables.
The survey was carried out in accordance with the Declaration of Helsinki and Good Clinical Practice [52]. Ethical approval for the survey was obtained from the Committee of Research Ethics of the Croatian National Institute of Public Health and participants were provided a written informed consent to sign.
3. Results
After the exclusions reported above, the final nationwide population sample included 1067 participants between 18 and 89, recruited from five Croatian regions (Central part, North-East part—Slavonia, North-West part, North part of the coast, South part of the coast—Dalmatia).
3.1. Completion of 24-Hour Urine Collection
In 2018-2021, 1765 adults aged 18 to 91 years were randomized and participated in the examination component of EH—UH 2 survey (Figure 1). Among these 1765 participants, 1342 (76%) attended the outpatient visit and were asked to participate in 24-hour urine collection examination. Out of them, 1268 (94.5%) participants (35% men) completed a 24-hour urine collection with 1067 (84.1%) participants collecting an adequate urine sample. They were included in further analyses. There were no differences between group of subjects which participated in 24-hour urine collection examination and those who refused to participate in age, BMI and diastolic BP, but in the group which did not collect 24-hour urine were more men (44% vs.35%) and they had lower systolic BP (129.9 vs. 133.6 mmHg). The response rate of enrolled subjects for the 24-hour urine collection was estimated at approximatively 72% ((94.5% (24-hour urine completion rate) × 76% (attended the EH-UH 2 outpatient visit)), and the adequate 24-hour urine collection was estimated at approximatively 63.8% (84.1% adequate 24-hour urine sample) × 76% (attended the EH-UH 2 outpatient visit)). The overall survey response rate for the 24-hour urine collection was estimated at approximately 69% (94.5 (24-hour urine completion rate) × 73% (EH-UH 2 response rate)), and the adequate survey 24-hour urine collection was 61% (84.1% (24-hour urine completion rate) × 73% (EH-UH 2 response rate)).
3.2. Characteristics of the Participants Attended the Outpatient Visit and Asked to Participate in 24-Hour Urine Examination
Table 1. shows the characteristics of the participants. The average age of the cohort was 57.2 which is higher than the average age of the general Croatian adult population which was 44.3 (men 42.5, women 45.9) according to the 2021 census [53]. Average BP values were in high-normal BP ranges, and average BMI value was in the overweight category. There were no statistically significant differences in the mean age and heart rate between men and women, however men were taller and heavier with higher BMI, and higher values of systolic and diastolic BP.
3.3. Daily Urinary Excretions of Creatinine, Sodium, Potassium, Iodine, and Estimated Salt, Potassium and Iodine Intake in the Whole Group
Results of the analyses of the 24-hour urine sample are presented in Table 2. Average urinary volume excretion was 1589.9 ml/day, being higher in men than in women. Mean urinary sodium excretion was 140.5 mmol/24-hours (IQR 101.5 g-191.3), corresponding to a mean consumption of 8.6 grams of salt per day (IQR 6.2 g-11.7 g). We observed significant difference between men and women in daily salt consumption being significantly higher in men than in women (10.5 g (IQR 7.3 g-14.0 g) vs. 8.0 g (IQR 5.8 g-10.5 g), p < 0.001), equivalent to ~2.5 grams of higher salt consumption than women did. Only 13.7% of population met the WHO criteria of less than 5 grams of salt per day (Figure 2). Significantly more women than man ingested recommended amount of salt per day (16.2% vs. 9.1%; χ 2 = 10.404; p = 0.0012). Men consumed more potassium than women (3.1 grams per day (IQR 2.3 g–3.9 g) vs. 2.6 grams per day (IQR 2.0 g-3.3 g); p < 0.001)), and more men than women met the WHO recommended levels of potassium intake of 90 mmol/day or more (χ 2 = 17.5; p= 0,000002). Higher salt and potassium intake observed in men could be explained with the fact that men in average eat more food than women. We observed significant correlation between salt and potassium consumption in both men and women (R= 0.223, R= 0.291, respectively; p< 0.001 for both) (Figure S1, S2, S3). In the whole group only 3.7% subjects had the salt-to-potassium ratio less than 1. Interestingly, women had lower sodium-to-potassium ration than men (2.5 IQR 1.8-3.3 vs. 2.8 IQR 1.9-3.8; p<0.001). Although more women than men had the ratio less than 1, the difference was not significant (4.2% vs. 2.9%; χ 2 = 1.06; p=0.303). In the whole group, overall median of urinary iodine excretion was in recommended range (131.8 µmol/l IQR 95.4-174), indicating adequate iodine intake. Men excreted significantly more iodine than women (p < 0.001) which is related to higher salt intake in men. We found significant correlation between salt and iodine intake in the whole group (R = 0.52; p < 0.001) as well as in men (R = 0.57; p < 0.001) and in women (R = 0.45; p < 0.001) (Figure S4, S5, S6). In the whole group 22.3% subjects had urinary iodine excretion below 100 µg/l (Table 3). However, most of the subjects (70.9%) had urinary iodine excretion in the “adequate” and “above requirement” category (Table 3). However, majority had mild insufficiency (86%). There were no differences between men and women in urinary iodine excretion values below 100 µg/l (χ 2 = 1.889; p = 0.203). Although more men than women were in iodine categories “above requirement” (31.7% vs. 22.2%), we failed to find statistically significant difference (χ 2 = 3.243; p = 0.07). Excessive iodine intake with urinary iodine excretion values ≥ 300 µg/l was found in 6.8% of participants.
3.4. Daily Salt, Potassium and Iodine Intake According to Residency and Geographic Regions
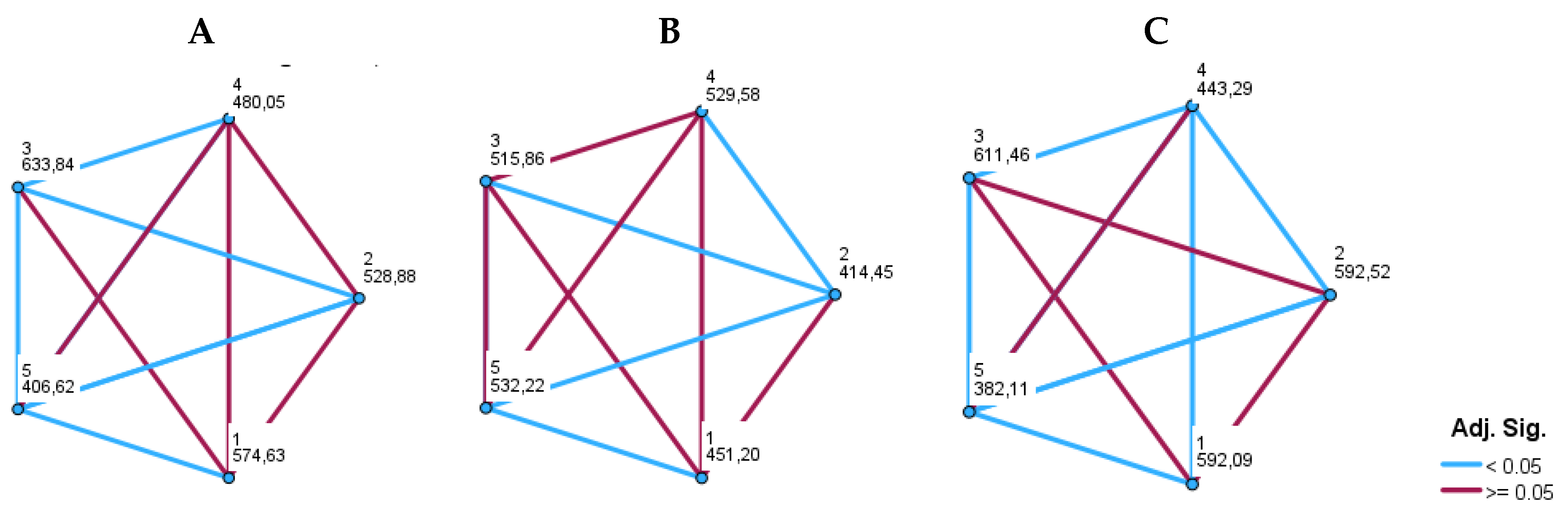
Results on salt, potassium and iodine consumption according to the residency are presented in Table 4. Salt intake was significantly higher while potassium intake was significantly lower in rural vs. urban areas (p < 0.001; p = 0.006, respectively). When we analysed geographical variability, we found that salt intake was significantly lower and potassium intake significantly higher in the Mediterranean part of Croatia compared to the continental part (p < 0.001 for both). Sodium-to-potassium ratio was significantly lower in urban vs. rural areas, and in Mediterranean vs. continental part of Croatia (p<0.001 for both). As shown in Table 5 and figures 3 and 4, daily salt intake was significantly lowest in the southern part of the Croatian coast, in Dalmatia (7.37 g) compared to all other regions including the northern part of the Croatian coast (8.46 g). However, salt intake in the northern part of the Croatian coast was lower than salt intake in all three continental regions of Croatia. The highest salt intake was observed in the North-West part of Croatia (11.0 g) compared to all other regions. Daily potassium intake was significantly higher in both Dalmatia (3.0 g) and northern part of the Croatian coast (3.0 g) than in all continental regions. The lowest potassium intake was found in the North-East part of Croatia, in Slavonia (2.4 g). Sodium-to-potassium ratio was significantly lower in both Dalmatia and northern part of the Croatian coast than in all continental regions. The highest sodium-to-potassium ratio was observed in the North-West part of Croatia. There were no significant differences among continental parts of Croatia in either potassium ingestion or sodium-to-potassium ratio.
Figure 2.
Distribution of single 24-hour salt intake estimates.
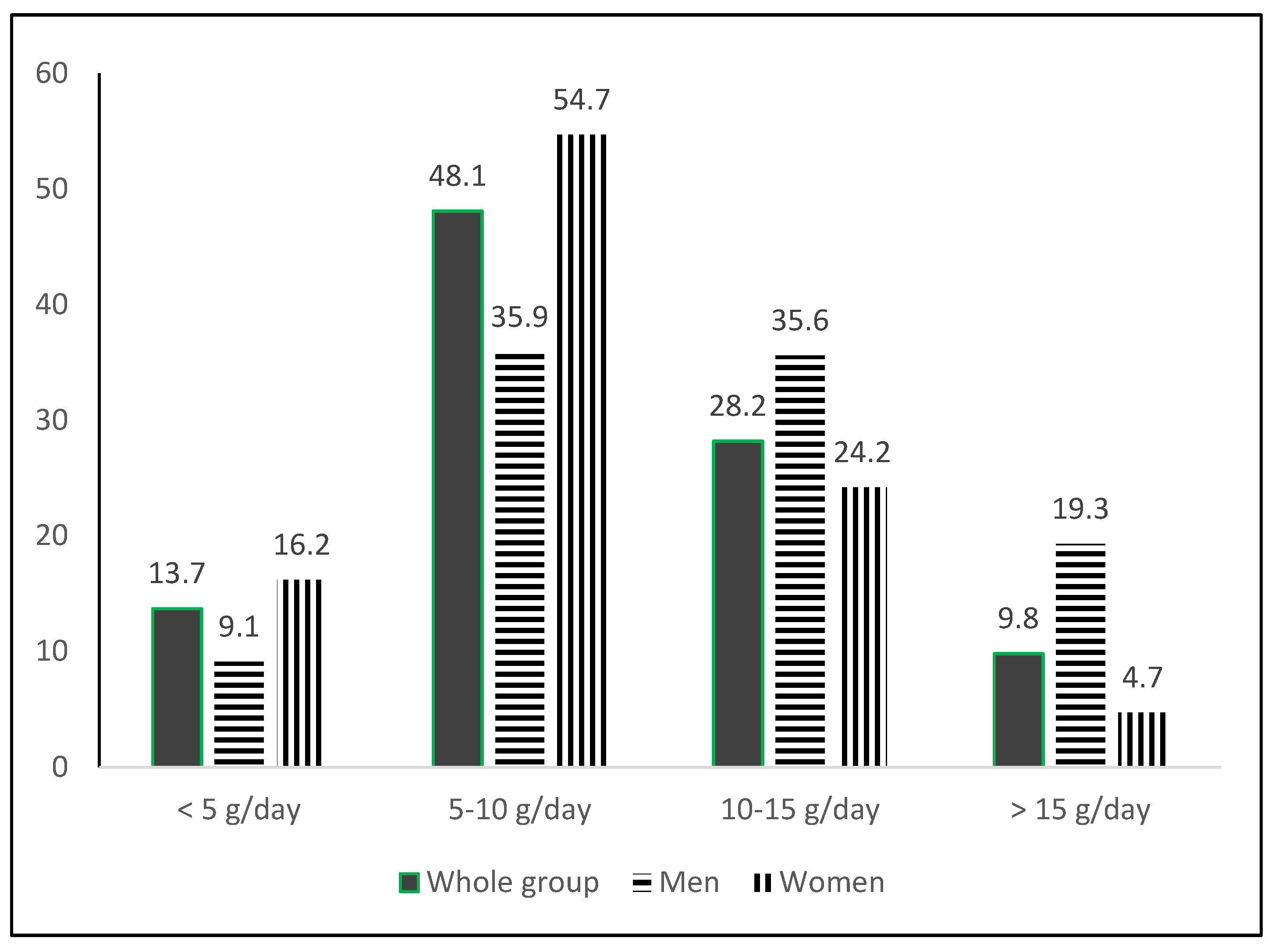
Figure 3.
Observed median 24-hour urinary sodium/salt (left) and potassium (right) excretion by region.
Figure 3.
Observed median 24-hour urinary sodium/salt (left) and potassium (right) excretion by region.
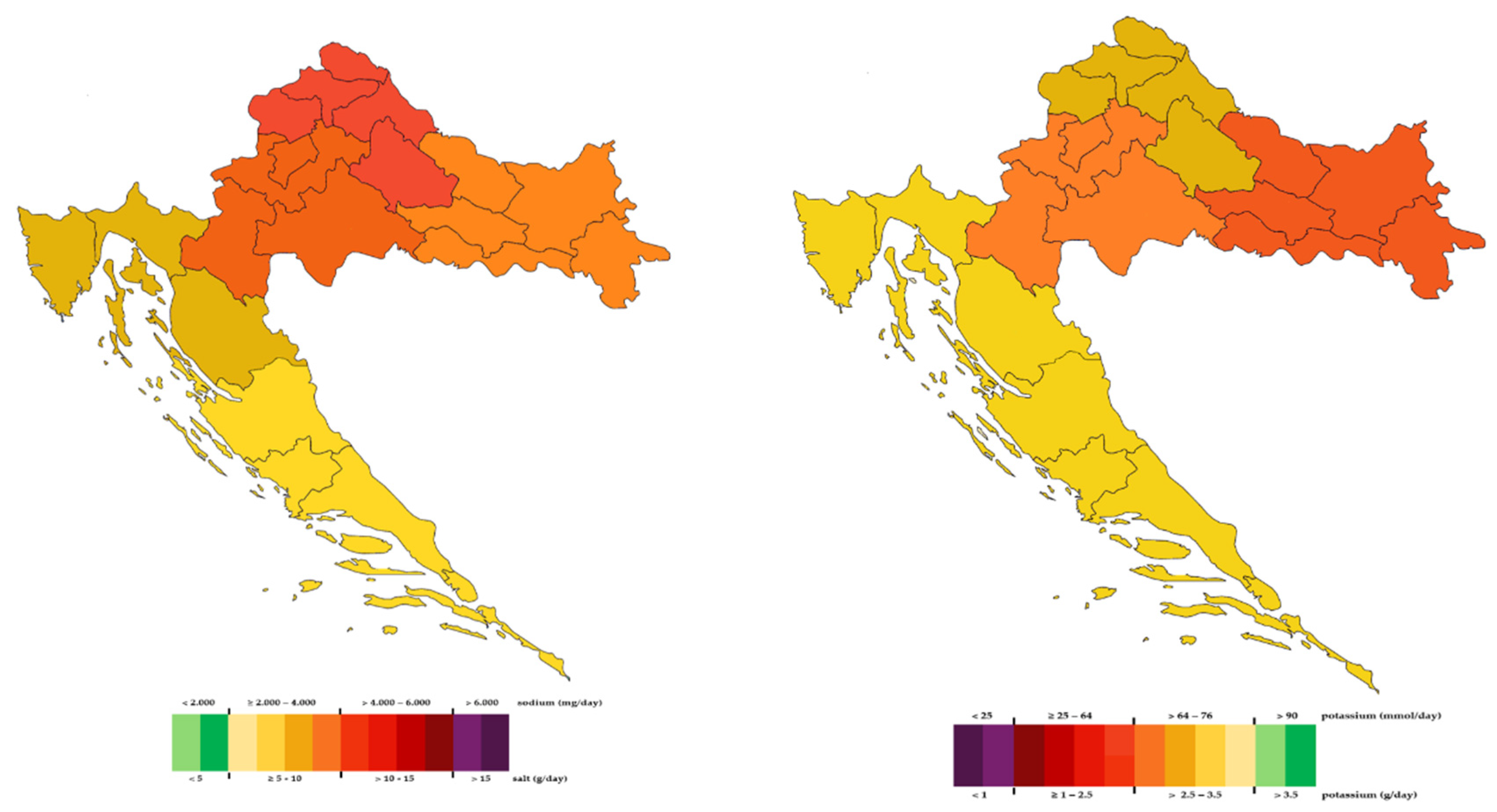
Figure 4.
Pairwise comparisons of daily salt (A), potassium (B) intake, and of sodium-to-potassium ratio (C) among five Croatian regions. Each node shows the sample average rank of five different regions; 1 = Central part; 2 = North-East-Slavonia; 3 = North-West part; 4 = North part of the coast; 5 = South part of the coast-Dalmatia.
Figure 4.
Pairwise comparisons of daily salt (A), potassium (B) intake, and of sodium-to-potassium ratio (C) among five Croatian regions. Each node shows the sample average rank of five different regions; 1 = Central part; 2 = North-East-Slavonia; 3 = North-West part; 4 = North part of the coast; 5 = South part of the coast-Dalmatia.
4. Discussion
EH-UH 2 study is the first nationwide study on salt and potassium consumption in Croatian general adult population. The results showed that in both genders salt consumption was still high, and potassium intake was too low. In majority of subjects iodine excretion was in recommended ranges, and only in a very small proportion of population it was severely insufficient.
1. Salt Consumption in General Adult Population
Average population salt consumption in our adult sample of 8.6 g/day was above the WHO recommended value of 5 g/day. However, according to the systematic review of population-level intake in the WHO European region in only a few countries (Norway, Netherlands, Italy, and United Kingdom) mean salt intake was below 9 g/day [54]. In EH-UH 2 study, salt intake was significantly higher in men (10.5 g/day) than in women (8.0 g/day) which was in concordance with reports from most countries. In men, salt intake below 11 g/day was found only in Portugal (10.8 g/day), Ireland (10.4 g/day), Norway (10.4 g/day), Netherlands (10.3 g/day), Italy (9.5 g/day) and United Kingdom (9.2 g/day). In women, salt intake less than 9 g/day was found only in Israel (8.59 g/day), Lithuania (8.4 g/day), Spain (8.36 g/day), Switzerland (8.0 g/day), Netherlands (7.8 g/day), United Kingdom (7.6 g/day), Norway (7.5 g/day), Ireland (7.4 g/day), and Italy 7.2 g/day) [54]. Croatian data which were included in this study were collected in our previous salt-mapping study conducted in 2005 when salt ingestion on population level was 11.3 g/day (men 13.4 g/day, women 10.4 g/day) [26]. Significant improvement at the population level which was found in the EH-UH 2 study (2 g/day less, or 17.6% decrease of salt consumption with no gender difference) is a result of a broad and intensive CRASH program which started in 2006 [27]. In 2021, Santos et al. published a systematic review of national salt reduction initiatives. Croatia was not included in this report while at that time results of our nationwide study EH-UH 2 were not available [55]. Only fourteen countries out of 96 included in this report analysed data on program effects, and among them 9 reported a moderate decrease (1-2 g/day), 3 reported a substantial decrease (> 2 g/day), and 5 reported a slight decrease (< 1g/day). The most significant decrease (26% and 24% in men and women, respectively) was observed in Finland, in North Karelia program and in Sout-West of Finland (16% and 19% in men and women, respectively) [56,57]. In Italy salt consumption decreased by 12% and 13% in men and women, respectively [58]. According to the report from Slovenia, salt consumption decreased by 10% in men and 3% in women [59]. Argentina, Australia, Fiji, Turky and United Kingdom reported in general population decrease of salt consumption by 18%, 2%, 12%, 17% and 7%, respectively [60,61,62,63,64]. The achievements were obtained in different periods of time in different countries. Follow up period was 4, 3, 3, 5, 20, 2, 9, 5, 4, and 13 years in Argentina, Australia, Fiji, Finland North Karelia, South-West Finland, Italy, Netherlands, Slovenia, Turkey, and United Kingdom, respectively. We failed to find any association between duration of follow up with obtained results in listed countries. It seems that success mostly depends on the engagement and enthusiasm of non-governmental organizations and willingness of the food industry to participate. This was the case in Croatia where most of work was done by the Croatian Society of Hypertension and Croatian Hypertension League with help of the Croatian Society of Atherosclerosis. We have established an excellent collaboration with the meat industry. Moreover, an important contribution was done by the Ministry of Agriculture which prepared an ordinance for bakery industry which limits salt content in final bakery products to be no more than 1.3%. The Croatian Institute of Public Health and the Croatian Agency for Agriculture and Food participated and strongly supported all these activities. In EH-UH 2 study, the WHO target of 5 g/day was found in only 13.7% of population (9.1% men, 16.2% women). This is significantly better than 3.7% which was registered in our salt-mapping 15 years ago, but far away from the main WHO aim. Similar results of 11.3% and 12.5% were found in Moldova and Lithuania, respectively [65,66]. Montenegro, Hungary and Greece reported that 7%, 6.9% and 5% of population reach the WHO target, respectively [67,68]. After an average of 5 years of most intensive CRASH activities, we achieved 3.5% decrease of salt consumption per year on population level. Decrease of 4% per year was achieved only in Italy and North Karelia. Keeping in mind years when we have started with several educational activities for general population and negotiations with food industry, the real result would be that we achieved approximately 2% decrease of salt consumption per year. These results indicate that the goal of 4% per year was probably optimistically set too high.
2. Potassium Consumption in Adult Population
It is well known that low potassium intake is related to higher BP and CVD risk, and vice versa [69]. Thus, WHO recommended that potassium intake should be at least 3.5 g/day for both genders [33]. According to our results, average potassium intake in Croatian adult population of 2.9 g/day is significantly below this target, but above the average word intake of 2.3 g/day [70]. Men ingested more potassium than women, and this could be explained similarly as for salt consumption with the fact that men eat more food. Our result agrees with results obtained in Hungary (3.0 g/day), but average amount was lower than results published for Montenegro (3.2 g/day), Moldova (3.4 g/day), Greece (3.3 g/day), and Lithuania (3.3 g/day). In our cohort only 14.7% of adult population reach the WHO target of at least 3.5 g/day (90 mmol/day) what is in concordance with results reported from Montenegro (13%), but lower than results found in Lithuania (23.1%), Hungary (31.2%), Greece (33.4%) and Moldova (39%) [65,66,67,68,71].
3. Sodium-to-Potassium Ratio
In our cohort the average sodium-to potassium ratio was 2.6, which was lower than result of 3.0 found in Hungary [67], and 2.8 reported in the INTERSALT study [72], but higher than 1.3 and 2.3 observed in Greece and Lithuania, respectively [66,68]. We found sodium-to-potassium ratio to be lower in women than in men (2.6 and 3.0), which was the case in Norway (1.79 and 1.86), NHANES study (2.87 and 3.17), Finland (1.92 and 2.87), New Zealand (2.1 and 2.3), Italy (2.8 and 3.1), Hungary (2.8 and 3.2), Greece (1.32 and 1.37), and Lithuania (2.1 and 2.6) [66,73,74,75,76,77]. Beside Greece where the ratio was closest to one, in vast majority of countries, the sodium-to potassium ratio was reported to be significantly higher than the recommended one reflecting globally unhealthy eating habits with too much salt and not enough vegetables and fruits.
4. Salt and Potassium Intake According to the Residency and Geographical Difference
Salt intake and the sodium-to-potassium ratio were higher, and potassium intake was lower in rural than urban areas indicating that eating habits were worse among rural population. In studies conducted in Canada and Moldova, sodium and potassium intake were higher in rural than in urban region, but sodium-to-potassium ratio was slightly better in urban regions [65,78]. It seems that our rural population eats less vegetables and fruits than farmers in Canada and Moldova. This should be taken into consideration not only for educational plans but also for activities and national programs which should be adjusted when organized by the government. Croatia could be separated into two regions, Continental and Mediterranean which differ in geography, but even more important, in history, culture, gastronomy and lifestyle. For the first time differences between Dalmatia (Mediterranean part) and Slavonia (Continental part) were reported already in 1966 in the Seven Countries Study where it was observed that population living in Dalmatia had lower BP with less obesity than population from Slavonia [79]. Croatia is an excellent model to test and analyse, in the same population, whether Mediterranean style of living is still present. We found salt intake and sodium-to-potassium ratio to be lower, and potassium intake to be higher in Mediterranean part than in continental part. Although, these results indicated that eating habits concerning salt and potassium intake were better in the Mediterranean part, the average salt consumption was still too high, and the average consumption of potassium was still too low. We further analysed differences in salt and potassium intake among five different Croatian regions—two from the coast, and three continental regions. The lowest sodium intake and sodium-to-potassium ratio and highest potassium intake found in both Mediterranean parts of Croatia could be explained with still preserved traces of the Mediterranean way of living. Finding no differences in high sodium-to-potassium ratio among continental regions reflects equally poor eating habits in continental Croatia with too salty food and insufficient consummation of vegetables and fruits. In the MINISAL-GIRSCI programme the authors found a significant north-south pattern of sodium excretion in Italy [80]. These spatial differences and geographical variations were partly explained with socioeconomic gradient. In forthcoming paper, our plan is to determine which factors and variables could most plausibly explain geographical differences in Croatia.
5. Strenghts and Limitations
According to our knowledge this is the first study on salt, potassium and at the same time a daily iodine excretion in Croatia. Strengths of our population-based study are: (i) the enrolment of a large random sample of men and women of the Croatian adult population from different parts of the country; (ii) salt and potassium intake were measured using the gold-standard method of 24-hour urine collections; (iii) a rigorous quality control was performed, and highly standardized protocol was used enabling us to include only valid urine samples into the analyses; (iv) participation rate was very good and there were no substantial differences between group which was included in analyses and the group of subjects who either refused to participate or the group of subjects whose urine samples were inadequate. The limitation of our study is: (i) urinary sodium, potassium and iodine were only assessed once; (ii) we did not use PABA to determine the completeness of urine collection.
6. Conclusion
In last fifteen years, salt consumption has been significantly reduced in Croatian adult population because of intensive and broad CRASH program led by the Croatian Society of Hypertension and the Croatian Hypertension League. However, salt intake is still too high, and potassium ingestion is too low. Only 13.7% of population reach the WHO target of 5 grams of salt per day, and only 8.9% of population ingested at least 3.5 grams of potassium per day. Poorer sodium-to-potassium ratio observed in rural areas should be considered when future national programs will be planed. Better results found in the Mediterranean part might reflect still present rudiments of the Mediterranean way of living. However, even in Mediterranean part of Croatia salt intake is still too high.
CRASH achieved very good result which is more than proof-of-feasibility. With expected more active engagement and help of the government, obtained results could be significantly accelerated and improved. Salt reduction programs are most cost-effective methods of CVD prevention and should be considered more seriously by the government and health policy makers [81].
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
Croatian Science Foundation research grant (IP-06-2016) for supporting the project Epidemiology of hypertension and salt intake in Croatia (EH—UH 2); unrestricted research grants of the Croatian Society of Hypertension and the Croatian Hypertension League; Croatian Science Foundation program “Young Researchers’ Career Development Project—training of doctoral students” funded the work of Mihaela Marinović Glavić (PhD student), DOK-2018-09; financial and organization help from the School of Medicine University of Zagreb, and the Croatian Institute of Public Health.
Informed Consent Statement
The survey was carried out in accordance with the Declaration of Helsinki and Good Clinical Practice. Ethical approval for the survey was obtained from the Committee of Research Ethics of the National Centre of Public Health and participants provided written informed consent to take part.
Acknowledgments
We would like to thank all participants who agreed to participate, to family physicians, nurses, residents, fellows and medical students who as a members of the MET participated in field work. We would also like to thank medical directors of outpatient clinics across Croatia who allowed us to use their rooms and facilities for our filed work. Warm and special thanks to Professor Jasna Lovrić, vice-dean of the School of Medicine, and to the d8solutions company, digital partner of the Croatian Hypertension League who helped us in organization of the field work.
Conflicts of Interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
References
- World Health Organization. Global report on hypertension: the race against a silent killer. World Health Organization: Geneva, Switzerland, 2023. Available online: https://www.who.int/publications/i/item/9789240081062 (accessed on 10 April 2024).
- GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018 Nov 10;392(10159):1736-1788. [CrossRef]
- Wang, K.; Jin, Y.; Wang, M.; Liu, J.; Bu, X.; Mu, J.; Lu, J. Global cardiovascular diseases burden attributable to high sodium intake from 1990 to 2019. J. Clin. Hypertens. 2023, 25 (9), 868–879. [CrossRef]
- Liu, W.; Zhou, L.; Yin, W.; Wang, J.; Zuo, X. Global, regional, and national burden of chronic kidney disease attributable to high sodium intake from 1990 to 2019. Front. Nutr. 2023, 10. [CrossRef]
- Wang, X.; Ma, H.; Kou, M.; Tang, R.; Xue, Q.; Li, X.; Harlan, T. S.; Heianza, Y.; Qi, L. Dietary sodium intake and risk of incident type 2 diabetes. Mayo Clinic Proceedings 2023, 98 (11), 1641–1652. [CrossRef]
- Filippini, T.; Malavolti, M.; Whelton, P. K.; Naska, A.; Orsini, N.; Vinceti, M. Blood pressure effects of sodium reduction. Circulation. 2021, 143 (16), 1542–1567. [CrossRef]
- McMahon, E.; Campbell, K. L.; Bauer, J.; Mudge, D. W.; Kelly, J. Altered dietary salt intake for people with chronic kidney disease. Cochrane Library 2021, 2021 (6). [CrossRef]
- Hodson, E. M.; Cooper, T. E. Altered dietary salt intake for preventing diabetic kidney disease and its progression. Cochrane Library 2023, 2023 (1). [CrossRef]
- World Health Organization. Noncommunicable Diseases, Rehabilitation and Disability (NCD). Global action plan for the prevention and control of noncommunicable diseases 2013-2020. Available online: https://www.who.int/publica-472tions/i/item/9789241506236 (accessed on 13 May 2024).
- Cobiac, L.; Vos, T.; Veerman, L. Cost-effectiveness of interventions to reduce dietary salt intake. Heart 2010, 96 (23), 1920–1925. [CrossRef]
- Webb, M.; Fahimi, S.; Singh, G.; Khatibzadeh, S.; Micha, R.; Powles, J.; Mozaffarian, D. Cost effectiveness of a government supported policy strategy to decrease sodium intake: global analysis across 183 nations. BMJ. 2017, i6699. [CrossRef]
- Trieu, K.; Neal, B.; Hawkes, C.; Dunford, E.; Campbell, N. R. C.; Rodríguez-Fernández, R.; Legetić, B.; McLaren, L.; Barberio, A.M.; Webster, J. Salt Reduction Initiatives around the World – A Systematic Review of Progress towards the Global Target. PloS 480 One 2015, 10 (7), e0130247. [CrossRef]
- Webster, J.; Dunford, E.; Hawkes, C.; Neal, B. Salt reduction initiatives around the world. J. Hypertens. 2011, 29 (6), 1043–1050. [CrossRef]
- Croatian Institute of Public Health. Epidemiological data on cardiovascular diseases. Available online: https://www.hzjz.hr/aktualnosti/epidemioloski-podaci-o-kardiovaskularnim-bolestima/ (accessed on 11 May 2024).
- Murray, C. J. L.; Aravkin, A. Y.; Zheng, P.; Abbafati, C.; Abbas, K.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I. et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis 516 for the Global Burden of Disease Study 2019. Lancet 2020, 396 (10258), 1223–1249. [CrossRef]
- Global Burden of Disease 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 407 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: 408 a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392 (10159), 1923–1994. [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and con-411 trol from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 412 398 (10304), 957–980. [CrossRef]
- Boateng, E. B.; Ampofo, A. G. A glimpse into the future: modelling global prevalence of hypertension. BMC Public Health 2023, 23 (1). [CrossRef]
- Less Salt—More Health. Croatian Action on Salt and Health (CRASH). Available online: https://pubmed.ncbi.nlm.nih.gov/19514255/ (accessed on 10 April 2024).
- Salt—Hidden Poison in Everyday Meal. Available online: https://pubmed.ncbi.nlm.nih.gov/19642535/ (accessed on 3 March 2024).
- Less salt—More Health: Possibilities of Prevention in Croatia. Available online: https://pubmed.ncbi.nlm.nih.gov/20649071/ (accessed on 5 April 2024).
- Jelaković, B.; Vrdoljak, A.; Pećin, I.; Buzjak, V.; Karanović, S.; Ivković, V.; Dapić, K.; Domislović, V.; Reiner, Z. Less Salt—More Health. Croatian Action on Salt and Health (46). J. Hypertens Res. 2016, 2, 61–68. Available online: http://hypertens.org/contents/pdfs/jhr-201606-020203.pdf (accessed on 15 May 2024).
- Jelaković, B.; Premužić, V.; Čvorišćec, D.; Erceg, I.; Fuček, M.; Jelaković, M.; Jovanović, A.; Kaić-Rak, A.; Laganović, M.; Lederer, P. et al. Salt Mapping in Croatia. Croatian Action on Salt and Health (CRASH). Kidney Blood Press Res. 2009, 32, 323.
- Sović, S.; Vitale, K.; Keranović, A.; Dražić; Džakula, A.; Jelaković, B. Prevalence, awareness, treatment and control of hypertension and salt intake in some rural area of Sisak—Moslavina county, Croatia. Period. Biol. 2011, 113, 321–326.
- World Health Organization. Reducing salt intake in populations. Available online: https://iris.who.int/bitstream/handle/10665/43653/9789241595377_eng.pdf?sequence=1&isAllowed=y (accessed on 13 March 2024).
- Jelaković, B.; Premužić, V.; Čvorišćec, D.; Erceg, I.; Fuček, M.; Jelaković, M.; Jovanović, A.; Kaić-Rak, A.; Laganović, M.; Lederer, 531 P. et al. Salt Mapping in Croatia. Croatian Action on Salt and Health (CRASH). Kidney and Blood Press Research, 2009; 32:323, 532 2009.
- Jelaković, B.; Marinović Glavić, M.; Batinić Sermek, M. Bilajac, L.; Bubaš, M.; Buzjak Služek, V.; Capak, K.; Drenjančević, I.; Gross Bošković, A.; Jelaković, A. et al. Croatian Action on Salt and Health (CRASH): On the Road to Success – Less Salt, More Health. Nutrients 2024, 16 (10), 1518. [CrossRef]
- Ordinance on cereals and cereal products (NN 101/2022) Available online: https://narodne-novine.nn.hr/clanci/sluzbeni/2022_09_101_1495.html (accessed on 5 May 2024).
- Hrvatska agencija za poljoprivredu i hranu, HAPIH (Croatian Agency for Agriculture and Food, CAAF), 2020. Scientific report 550 on the intake of salt through the consumption of bread and bakery products. Ad hoc. Task force of the Centre for Food Safety. 551 Available online: https://www.hapih.hr/wp-content/uploads/2021/01/Znanstveno-izvjesce-o-unosu-kuhinjske-soli-konzumaci-552jom-kruha-i-pekarskih-proizvoda_compressed.pdf (accessed on 15 April 2024).
- Gonçalves, C.; Abreu, S. Sodium and potassium intake and cardiovascular disease in Older people: a systematic review. Nutrients 2020, 12 (11), 3447. [CrossRef]
- Sodium and potassium intake: Effects on chronic disease Outcomes and risks [Internet]. PubMed. https://pubmed.ncbi.nlm.nih.gov/30125063/.
- Academies of Sciences, Engineering, and Medicine. Dietary Reference Intakes for Sodium and Potassium. Washington, DC; The National Academies Press; 2019. https://ods.od.nih.gov/factsheets/Potassium-HealthProfessional/#en11.
- World Health Organization. WHO issues new guidance on dietary salt and potassium. Available online: https://www.who.int/news/item/31-01-2013-who-issues-new-guidance-on-dietary-salt-and-potassium (accessed on 11 May 2024).
- European Food Safety Authority. Dietary reference values for potassium. European Food Safety Authority. Available online: https://www.efsa.europa.eu/en/efsajournal/pub/4592 (accessed on 10 May).
- Reddin, C.; Ferguson, J.; Murphy, R.; Clarke, A.; Judge, C.; Griffith, V.; Alvarez, A.; Smyth, A.; Mente, A.; Yusuf, S. et al. Global mean potassium intake: a systematic review and Bayesian meta-analysis. European Journal of Nutrition 2023, 62 (5), 2027–2037. [CrossRef]
- Huang, L.; Li, Q.; Wu, J. H.; Tian, M.; Yin, X.; Yu, J.; Liu, Y.; Zhang, X.; Wu, Y.; Paige, E.; Trieu, K.; Marklund, M.; Rodgers, A.; Neal, B. The contribution of sodium reduction and potassium increase to the blood pressure lowering observed in the Salt Substitute and Stroke Study. Journal of Human Hypertension 2024, 38 (4), 298–306. [CrossRef]
- Yang, Y.; Wu, Q.; Lv, Q.; Li, J.; Li, L.; Wang, S. Dietary sodium, potassium intake, sodium-to-potassium ratio and risk of hypertension: a protocol for systematic review and dose–response meta-analysis of cohort studies. BMJ Open 2023, 13 (2), e065470. [CrossRef]
- Morrissey, E.; Giltinan, M.; Kehoe, L.; Nugent, A. P.; McNulty, B. A.; Flynn, A.; Walton, J. Sodium and Potassium Intakes and Their Ratio in Adults (18–90 y): Findings from the Irish National Adult Nutrition Survey. Nutrients 2020, 12 (4), 938. [CrossRef]
- Salt Ordinance, Narodne novine, number 70/2019. Available online: https://mingo.gov.hr/print.aspx?id=7930&url=print (accessed on 20 May 2024).
- Kusić, Z.; Lechpammer, S.; Labar, Ž.; Rončević, S.; Lukinac, Lj.; Notig-Hus, D.; Đaković, N.; Đokić, D.; Staničić, A.; Kaić-Rak, A. et al. Endemska gušavost i jodna profilaksa u Hrvatskoj / Znanstveni skup Nedostatak joda i gušavnost u Hrvatskoj - epidemiologija i jodna profilaksa : Gušavost u Hrvatskoj : prošireni zbornik / Kusić, Zvonko (ur.). Zagreb: Hrvatska akademija znanosti i umjetnosti ; : Klinička bolnica Sestre milosrdnice, 2000. str. 69-95.
- Kusić, Z.; Jukić, T.; Rogan SA, Juresa ,V.; Dabelić, N.; Stanicić, J.; Borić, M.; Lukinac, L.; Mihaljević, I.; Punda, A. et al. Current status of iodine intake in Croatia –the results of 2009 survey. Coll Antropol. 2012;36(1):123–128. https://pubmed.ncbi.nlm.nih.gov/22816208/.
- Kusić, Z.; Novosel, SA.; Dabelić, N.; Punda, M.; Roncević, S.; Labar Z, Lukinac, Lj.; Nothig-Hus, D.; Staničić, A.; Kaić-Rak, A. et al. Croatia has reached iodine sufficiency. J Endocrinol Invest. 2003; 26:738–742. https://link.springer.com/article/10.1007/BF03347356.
- Vidranski, V. (2019) Povezanost koncentracije joda u mokraći, antropoloških obilježja i fizičke aktivnosti djece u dobi od 6 do 12 godina . Doktorski rad. Osijek: Sveučilište J.J. Strossmayera, Medicinski fakultet Osijek. Available online: https://repozitorij.mefos.hr/islandora/object/mefos:1084 (accessed on 5 May 2024).
- Gharib H. Does iodine cause thyroid cancer? Acta Endocrinol (Buchar). 2018;14(4):525-526. [CrossRef]
- Vasiljev, V.; Subotić, A.; Marinović Glavić, M.; Jurga, D.; Bilajac, L.; Jelaković, B.; Rukavina, T. Overview of iodine intake. SEEMEDJ 2022, Vol 6, No 1.
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D. L.; Coca, A.; de Simone, G.; Dominiczak, A. et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension. Journal of Hypertension 2018, 36 (10), 1953–2041. [CrossRef]
- Vrdoljak, A.; Željković Vrkić, T.; Kos, J.; Vitale, K.; Premužić, V.; Laganović, M.; Jelaković, B. Blood pressure measurement – do not sweat the small stuff and it is all small stuff?!. Liječ Vjesn. 2014. https://hrcak.srce.hr/file/254652.
- World Health Organization. Protocol for population level sodium determination in 24-hour urine samples. Available online: https://www3.paho.org/hq/dmdocuments/2013/24h-urine-Protocol-eng.pdf (accessed on 29 May 2024).
- World Health Organization World Health Organization Guideline: Potassium Intake for Adults and Children. 2012.Available online: https://www.who.int/publications/i/item/9789241504829 (accessed on 1 June 2024).
- Turck, D.; Castenmiller, J.; De Henauw, S.; Hirsch-Ernst, K.-I.; Kearney, J.; Knutsen, H. K.; Maciuk, A.; Mangelsdorf, I.; McArdle, H. J.; Pelaez, C. et al. Dietary reference values for sodium. EFSA Journal 2019, 17 (9). [CrossRef]
- World Health Organization. United Nations Children’s Fund & International Council for the Control of Iodine Deficiency Disorders. Assessment of iodine deficiency disorders and monitoring their elimination. 3rd ed. Geneva, Switzerland: WHO, 2007). Available online: https://iris.who.int/bitstream/handle/10665/43781/9789241595827_eng.pdf (accessed on 2 June 2024).
- WMA - the World Medical Association-WMA Declaration of Helsinki – Ethical principles for medical research involving human subjects. WMA - the World Medical Association-WMA Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects. https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects.
- Croatian Bureau of Statistics. Population estimate of Republic of Croatia, 2021. Available online: https://podaci.dzs.hr/2022/hr/29032 (accessed on 3 June 2024).
- Kwong, E. J. L.; Whiting, S.; Bunge, A. C.; Leven, Y.; Breda, J.; Rakovac, I.; Cappuccio, F. P.; Wickramasinghe, K. Population-level salt intake in the WHO European Region in 2022: a systematic review. Public Health Nutrition 2022, 26 (S1), s6–s19. [CrossRef]
- Santos, J. A.; Tekle, D.; Rosewarne, E.; Flexner, N.; Cobb, L.; Al-Jawaldeh, A.; Kim, W. J.; Breda, J.; Whiting, S.; Campbell, N.; Neal, B.; Webster, J.; Trieu, K. A Systematic Review of Salt Reduction Initiatives around the world: A midterm evaluation of progress towards the 2025 Global Non-Communicable Diseases Salt Reduction Target. Advances in Nutrition 2021, 12 (5), 1768–1780. [CrossRef]
- McLaren, L.; Sumar, N.; Barberio, A. M.; Trieu, K.; Lorenzetti, D. L.; Tarasuk, V.; Webster, J.; Campbell, N. R. Population-level interventions in government jurisdictions for dietary sodium reduction. Cochrane Library 2016, 2017 (3). [CrossRef]
- Laatikainen, T.; Pietinen, P.; Valsta, L.; Sundvall, J.; Reinivuo, H.; Tuomilehto, J. Sodium in the Finnish diet: 20-year trends in urinary sodium excretion among the adult population. European Journal of Clinical Nutrition 2006, 60 (8), 965–970. [CrossRef]
- Donfrancesco, C.; Lo Noce, C.; Russo, O.; Minutoli, D.; Di Lonardo, A.; Profumo, E.; Buttari, B.; Iacone, R.; Vespasiano, F.; Vannucchi, S. et al. Trend of salt intake measured by 24-h urine collection in the Italian adult population between the 2008 and 2018 CUORE project surveys. NMCD. Nutrition Metabolism and Cardiovascular Diseases 2021, 31 (3), 802–813. [CrossRef]
- World Health Organization Regional Office for Europe. Meeting of the WHO action network on salt reduction in the population in the European region (ESAN): meeting report 2–10 May 2017, Dublin, Ireland. Copenhagen (Denmark): World Health Organization Regional Office for Europe; 2017. Available online: https://www.who.int/publications/i/item/WHO-EURO-2017-3289-43048-60245 (accessed on 18 May 2024).
- International Food Policy Research Institute. Global nutrition report 2016: from promise to impact: ending malnutrition by 2030. Washington (DC): International Food Policy Research Institute; 2016. Available online: https://wedocs.unep.org/20.500.11822/9677 (accessed on 15 May 2024).
- Nowson, C.; Lim, K.; Grimes, C.; O’Halloran, S.; Land, M.; Webster, J.; Shaw, J.; Chalmers, J.; Smith, W.; Flood, V. et al. Dietary salt intake and discretionary salt use in two general population samples in Australia: 2011 and 2014. Nutrients 2015, 7 (12), 10501–10512. [CrossRef]
- Pillay, A.; Trieu, K.; Santos, J.; Sukhu, A.; Schultz, J.; Wate, J.; Bell, C.; Moodie, M.; Snowdon, W.; Ma, G.; Rogers, K.; Webster, J. Assessment of a salt reduction intervention on adult population salt intake in Fiji. Nutrients 2017, 9 (12), 1350. [CrossRef]
- World Health Organization Regional Office for Europe. Progress in reducing salt consumption in Turkey [Internet]. World Health Organization Regional Office for Europe; 2013. Available online: http://www.euro.who.int/en/countries/turkey/news/news/2013/04/progress-in-reducing-salt-consumption-in-turkey (accessed on 1 June 2024).
- Public Health England. National diet and nutrition survey: assessment of salt intake from urinary sodium in adults (aged 19 to 64 years) in England, 2018 to 2019. London (UK): Public Health England; 2020. Available online: https://assets.publishing.service.gov.uk/media/5e7cd9cdd3bf7f133ed1b6a1/Report_England_Sodium_Survey_2018-to-2019__3_.pdf (accessed on 1 June 2024).
- D’Elia, L.; Obreja, G.; Ciobanu, A.; Breda, J.; Jewell, J.; Cappuccio, F. P. Sodium, potassium and iodine intake, in a national adult population sample of the Republic of Moldova. Nutrients 2019, 11 (12), 2896. [CrossRef]
- Zakauskiene, U.; Macioniene, E.; Zabuliene, L.; Sukackiene, D.; Linkeviciute-Dumce, A.; Banys, V.; Bratcikoviene, N.; Karosiene, D.; Slekiene, V. et al. Sodium, potassium and iodine intake in an adult population of Lithuania. Nutrients 2022, 14 (18), 3817. [CrossRef]
- Sarkadi-Nagy, E.; Horváth, A.; Varga, A.; Zámbó, L.; Török, A.; Guba, G.; Szilfai, N.; Zentai, A.; Bakacs, M. Dietary Sodium and Potassium Intake in Hungarian Elderly: Results from the Cross-Sectional Biomarker2019 Survey. International Journal of Environmental Research and Public Health/International Journal of Environmental Research and Public Health 2021, 18 (16), 8806. [CrossRef]
- Vasara, E.; Marakis, G.; Breda, J.; Skepastianos, P.; Hassapidou, M.; Kafatos, A.; Rodopaios, N.; Koulouri, A.; Cappuccio, F. Sodium and potassium intake in healthy adults in Thessaloniki Greater Metropolitan Area—The salt intake in Northern Greece (SING) study. Nutrients 2017, 9 (4), 417. [CrossRef]
- Palaniveloo, L.; Ambak, R.; Othman, F.; Zaki, N. A. M.; Baharudin, A.; Aziz, N. S. A.; Salleh, R. Low potassium intake and its association with blood pressure among adults in Malaysia: findings from the MyCoSS (Malaysian Community Salt Survey). Journal of Health, Population and Nutrition 2021, 40 (S1). [CrossRef]
- Reddin, C.; Ferguson, J.; Murphy, R.; Clarke, A.; Judge, C.; Griffith, V.; Alvarez, A.; Smyth, A.; Mente, A.; Yusuf, S. et al. Global mean potassium intake: a systematic review and Bayesian meta-analysis. European Journal of Nutrition 2023, 62 (5), 2027–2037. [CrossRef]
- D’Elia, L.; Brajović, M.; Klisic, A.; Breda, J.; Jewell, J.; Cadjenović, V.; Cappuccio, F. P. Sodium and potassium intake, knowledge attitudes and behaviour towards salt consumption amongst adults in Podgorica, Montenegro. Nutrients 2019, 11 (1), 160. [CrossRef]
- Stamler, J.; Rose, G.; Stamler, R.; Elliott, P.; Dyer, A.; Marmot, M. INTERSALT study findings. Public health and medical care implications. Hypertension 1989, 14 (5), 570–577. [CrossRef]
- Meyer, H. E.; Johansson, L.; Eggen, A. E.; Johansen, H.; Holvik, K. Sodium and potassium intake assessed by spot and 24-H urine in the Population-Based Tromsø Study 2015–2016. Nutrients 2019, 11 (7), 1619. [CrossRef]
- Cogswell, M. E.; Loria, C. M.; Terry, A. L.; Zhao, L.; Wang, C.-Y.; Chen, T.-C.; Wright, J. D.; Pfeiffer, C. M.; Merritt, R.; Moy, C. S. et al. Estimated 24-Hour urinary sodium and potassium excretion in US adults. JAMA 2018, 319 (12), 1209. [CrossRef]
- Vasara, E.; Marakis, G.; Breda, J.; Skepastianos, P.; Hassapidou, M.; Kafatos, A.; Rodopaios, N.; Koulouri, A.; Cappuccio, F. Sodium and potassium intake in healthy adults in Thessaloniki Greater Metropolitan Area—The salt intake in Northern Greece (SING) study. Nutrients 2017, 9 (4), 417. [CrossRef]
- McLean, R.; Edmonds, J.; Williams, S.; Mann, J.; Skeaff, S. Balancing Sodium and Potassium: Estimates of Intake in a New Zealand Adult Population Sample. Nutrients 2015, 7, 8930–8938. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4663567/.
- Donfrancesco, C.; Ippolito, R.; Lo Noce, C.; Palmieri, L.; Iacone, R.; Russo, O.; Vanuzzo, D.; Galletti, F.; Galeone, D.; Giampaoli, S. et al. Excess dietary sodium and inadequate potassium intake in Italy: Results of the MINISAL study. NMCD. Nutrition Metabolism and Cardiovascular Diseases 2013, 23 (9), 850–856. [CrossRef]
- Christoforou, A.; Ng, A.; Bernstein, J.; L’Abbe, M. Estimating usual sodium intake and Sodium-to-Potassium molar ratios from urine excretion among Canadian adults: An analysis of the Canadian Health Measures Survey. Current Developments in Nutrition 2021, 5, 1020. [CrossRef]
- Buzina, R.; Keys, A.; Mohaček, I.; Hahn, A.; Brozek, J.; Blackburn, H. C3. Rural men in Dalmatia and Slavonia, Yugoslavia. Acta Medica Scandinavica 1966, 180 (s460), 147–168. [CrossRef]
- Cappuccio, F. P.; Ji, C.; Donfrancesco, C.; Palmieri, L.; Ippolito, R.; Vanuzzo, D.; Giampaoli, S.; Strazzullo, P. Geographic and socioeconomic variation of sodium and potassium intake in Italy: results from the MINISAL-GIRCSI programme. BMJ Open 2015, 5 (9), e007467. [CrossRef]
- Shoaibi, A.; Ghandour, R.; Khatib, R.; Mason, H.; O’Flaherty, M.; Capewell, S.; Husseini, A. Salt reduction as a population-based intervention for the prevention of coronary heart diseases: an economic assessment. Lancet 2013, 382, S33. [CrossRef]
Figure 1.
Final number of the participants included in the study.*Ranges for the adequate urine creatinine (5.9–26.0 mmol/24 h for men; 4.0–16.4 mmol/24 h women).
Figure 1.
Final number of the participants included in the study.*Ranges for the adequate urine creatinine (5.9–26.0 mmol/24 h for men; 4.0–16.4 mmol/24 h women).
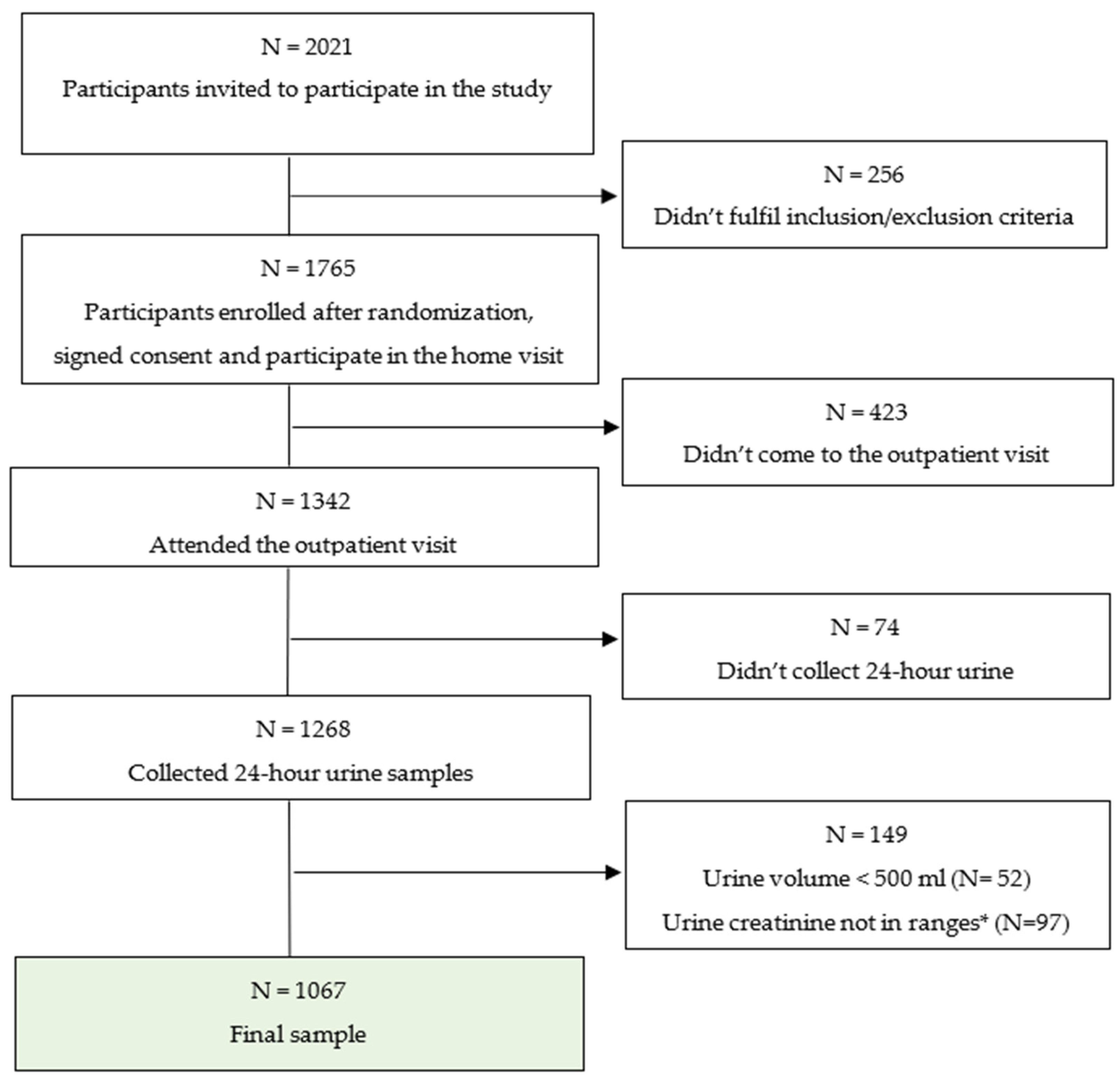

Table 1.
Characteristics of the participants.
| Whole group | Men | Women | P | |
| N | 1067 | 374 | 693 | |
| Age (years) | ||||
| Mean (SD) | 57.2 (13.9) | 57.2 (13.8) | 56.4 | 0.352 |
| S.E. | 0.37 | 0.75 | 0.55 | |
| Median (IQ range) |
59.0 (48.0-67.0) |
59.0 (48-68) |
59.0 (48-66) |
|
| Systolic BP (mmHg) | ||||
| Mean (SD) | 133.7 (19.0) | 137.9 (18.3) | 131.4 (19.2) | < 0.001 |
| S.E. | 0.5 | 0.99 | 0.77 | |
| Median (IQ range) |
132 (120.0-145.0) |
137.0 (124.5-149.0) |
130.0 (117.0-133.8) |
|
| Diastolic BP (mmHg) | ||||
| Mean (SD) | 82.5 (10.2) | 83.9 (10.2) | 81.5 (10.0) | < 0.001 |
| S.E. | 0.2 | 0.55 | 0.4 | |
| Median (IQ range) |
82.0 (76.0-89.0) |
84.0 (77.5-90.5) |
81.0 (75.1-87.5) |
|
| Heart rate (bpm) | ||||
| Mean (SD) | 75.7 (12.2) | 75.1 (13.0) | 76.4 (12.0) | 0.084 |
| S.E. | 0.3 | 0.71 | 0.48 | |
| Median (IQ range) |
75.0 (67.0-83.0) |
73.0 (65-0-83.3) |
75.6 (68.0-83.0) |
|
| Height (cm) | ||||
| Mean (SD) | 169.1 (16.7) | 178.4 (7.7) | 165.3 (6.8) | < 0.001 |
| S.E. | 0.4 | 0.42 | 0.27 | |
| Median (IQ range) |
168 (162-175) |
178.0 (174.0-183.0) |
165.0 (161.0-170.0) |
|
| Weight (kg) | ||||
| Mean (SD) | 81.4 (16.7) | 92.4 (16.1) | 76.6 (14.5) | < 0.001 |
| S.E. | 0.4 | 0.88 | 0.58 | |
| Median (IQ range) |
80.0 (69.0-91.0) |
90.0 (82.0-100.7) |
75.5 (66.0-85.8) |
|
| Body mass index (kg/m2) | ||||
| Mean (SD) | 28.3 (5.0) | 28.0 (4,6) | 28.0 (5.3) | < 0.001 |
| S.E. | 0.1 | 0.25 | 0.21 | |
| Median (IQ range) |
27.9 (24.8-31.2) |
28.4 (26.0-31,4) |
27.4 (24.0-31.1) |
Table 2.
Daily urinary excretions of sodium, potassium, and creatinine and estimates of salt, potassium and iodine intake.
Table 2.
Daily urinary excretions of sodium, potassium, and creatinine and estimates of salt, potassium and iodine intake.
| 24- hour urine | Whole group | Men | Women | p |
| N | 1067 | 374 | 693 | |
| Volume (ml) | ||||
| Mean (SD) | 1589.9 (628.5) | 1670 (613.2) | 1546 (632.9) | <0.001 |
| S.E. | 19.24 | 31.7 | 24.0 | |
| Median (IQ range) |
1500 (1100-1950) |
1590 (1215-2000) |
1500 (1100-1900) |
|
| Creatinine (g/l) | ||||
| Mean (SD) | 0.8 (0.4) | 1.0 (0.5) | 0.8 (0.4) | <0.001 |
| S.E. | 0.01 | 0.02 | 0.01 | |
| Median (IQ range) |
0.7 (0.5-0.1) |
0.9 (0.6-1.3) |
0.7 (0.5-0,9) |
|
| Sodium (dU) | ||||
| Mean (SD) | 151.8 (68.8) | 179.1 (74.9) | 137.1 (60.4) | <0.001 |
| S.E. | 2.14 | 3.8 | 2.29 | |
| Median (IQ range) |
140.5 (101.5-191.3) |
170.9 (119.7-229.7) |
130.6 (96.7-171.4) |
|
| Potassium (dU) | ||||
| Mean (SD) | 58.5 (22.3) | 64.5 (24.8) | 55.3 (20.1) | <0.001 |
| S.E. | 0.68 | 1.2 | 0.76 | |
| Median (IQ range) |
56.0 (43.0-71.0) |
62.0 (47.0-78.0) |
53 (41-66.5) |
|
| NaCl intake (g/day) |
||||
| Mean (SD) | 9.3 (4.2) | 10.9 (4.5) | 8.4 (3.7) | <0.001 |
| S.E. | 0.12 | 0.23 | 0.14 | |
| Median (IQ range) |
8.6 (6.2-11.7) |
10.5 (7.3-14.0) |
8.0 (5.8-10.5) |
|
| Potassium intake (g/day) |
||||
| Mean (SD) | 2.9 (1.1) | 3.3 (1.2) | 2.8 (1.0) | <0.001 |
| S.E. | 0.03 | 0.06 | 0.03 | |
| Median (IQ range) |
2.8 (2.1-3.5) |
3.1 (2.3-3.9) |
2.6 (2.0-3.3) |
|
| Na-to-K ratio |
||||
| Mean (SD) | 2.8 (1.4) | 3.0 (1.6) | 2.6 (1.2) | <0.001 |
| S.E. | 0.04 | 0.08 | 0.04 | |
| Median (IQ range) |
2.6 (1.8-3.5) |
2.8 (1.9-3.8) |
2.5 (1.8-3.3) |
|
| Urinary iodine excretion (µg/l) | N=577 | N= 208 | N=369 | |
| Mean (SD) | 156.2 (142.19) | 172.6 (144.9) | 147.3 (139.9) | <0.001 |
| S.E. | 7.0 | 10.2 | 7.2 | |
| Median (IQ range) |
131.8 (95.4-174) |
145.9 (108.58-191.6) |
121.7 (91.4-167.1) |
Table 3.
Distribution of participants’ iodine status according to the WHO criteria based on 24-hour urinary iodine concentrations (µg/l).
Table 3.
Distribution of participants’ iodine status according to the WHO criteria based on 24-hour urinary iodine concentrations (µg/l).
| Iodine status |
Iodine concentration (µg/l)) |
Whole group N= 577 |
Men N=208 |
Women N=369 |
|||
| Insufficient Severe Moderate Mild |
N | % | N | % | N | % | |
| < 20 | 2 | 0.3 | 1 | 0.5 | 1 | 0.3 | |
| 20-49 | 16 | 2.8 | 8 | 3.7 | 8 | 2.2 | |
| 50-99 | 111 | 19.2 | 31 | 14.5 | 80 | 21.7 | |
| Adequate consumption | 100-199 | 298 | 51.7 | 100 | 46.7 | 198 | 53.7 |
| Above requirement | 200-299 | 111 | 19.2 | 54 | 25.2 | 57 | 15.4 |
| Excessive consumption | >300 | 39 | 6.8 | 14 | 6.5 | 25 | 6.8 |
Table 4.
Differences in daily estimates of salt, potassium and iodine intake between rural and urban areas, and between continental and Mediterranean part of Croatia.
Table 4.
Differences in daily estimates of salt, potassium and iodine intake between rural and urban areas, and between continental and Mediterranean part of Croatia.
| 24- hour urine | Urban | Rural | p | Mediterranean | Continental | P |
| N | 608 | 376 | 434 | 473 | ||
| NaCl intake (g/day) |
||||||
| Mean (SD) | 8.8 (3.9) | 9.9 (4.4) | < 0.001 | 8.0 (3.6) | 10.3 (4.4) | <0.001 |
| S.E. | 0.16 | 0.23 | 0.17 | 0.23 | ||
| Median (IQ range) |
8.3 (5.8-11.2) |
9.4 (6.5-12.8) |
7.4 (5.3-10.2) |
9.9 (7.2 -13.3) |
||
| Potassium intake (g/day) |
||||||
| Mean (SD) | 3.0 (1.1) | 2.8 (1.0) | 0.006 | 3.0 (1.2) | 2.8 (1.0) | <0.001 |
| S.E. | 0.04 | 0.09 | 0.05 | 0.04 | ||
| Median (IQ range) |
2.9 (2.1-3.7) |
2.7 (2.0-3.4) |
2.9 (2.2-3.8) |
2.6 (2.0-3.3) |
||
| Na-to-K ratio | ||||||
| Mean (SD) | 2.6 (1.4) | 3.0 (1.4) | < 0.001 | 2.4 (1.4) | 3.0 (1.3) | <0.001 |
| S.E. | 0.05 | 0.07 | 0.06 | 0.06 | ||
| Median (IQ range) |
2.3 (1.6-3.1) |
2.9 (2.1-3.7) |
2.0 (1.5-2.9) |
3.0 (2.3-3.8) |
||
| Urinary iodine excretion (µg/l) |
N= 183 | N= 334 | N= 219 | N= 251 | ||
| Mean (SD) | 168.9 (133.1) | 146.4 (130.0) | 0.007 | 145.8 (116.5) | 161.5 (124.3) | 0.012 |
| S.E. | 9.84 | 7.1 | 7.9 | 7.8 | ||
| Median (IQ range) |
127.7 (103.2-193.2) |
119.8 (92.6-109.2) |
124.9 (90.3-171.2) |
141.2 (103.9-183.0) |
Table 5.
Daily urinary excretions of volume, sodium, potassium, and creatinine and estimates of salt, potassium and iodine intake across different regions of Croatia.
Table 5.
Daily urinary excretions of volume, sodium, potassium, and creatinine and estimates of salt, potassium and iodine intake across different regions of Croatia.
| Continental |
Coast | ||||
| Central part |
North-East part |
North-West Part |
North part |
South part |
|
| N | 143 | 234 | 154 | 102 | 434 |
| 24-hour urine volume (ml) | |||||
| Mean (SD) |
1631.3 (667.3) | 1621.6 (652.5) |
1515.7 (579.4) |
1764.6 (840.2) |
1544.3 (564.1) |
| S.E. | 58.9 | 44.0 | 48.9 | 101.8 | 27.2 |
| Median (IQ range) |
1500.0 (1200-1972.5) |
1560.0 (1152-5-1987.9) |
1400.0 (1100.0-1800.0) |
1500.0 (1180.0-2100.0) |
1500.0 (1100.0-1900.0) |
| Urine creatinine (g/l) | |||||
| Mean (SD) |
0.7 (0.3) |
0.91 (0.414) |
0.6 (0.3) |
0.6 (0.3) |
0.9 (0.4) |
| S.E. | 0.02 | 0.02 | 0.02 | 0.03 | 0.02 |
| Median (IQ range) |
0.71 (0.52-0.93) |
0.81 (0.61-1.11) |
0.6 0.42-0.87) |
0.5 (0.42-0.79) |
0.9 (0.6-1.2) |
| 24- hour sodium (dU) | |||||
| Mean (SD) |
169.0 (69.8) |
160.2 (75.3) |
182.3 (66.7) |
147.0 (63.4) |
130.5 (59.6) |
| S.E. | 6.1 | 5.1 | 5.6 | 7.6 | 2.8 |
| Median (IQ range) |
158.2 (119.7-216.3) |
146.9 (109.0-204.0) |
179.5 (133.3-220.8) |
137.8 (98.8-185.0) |
120.1 (87.0-163.2) |
| 24-hour potassium (dU) | |||||
| Mean (SD) |
55.6 (20.1) |
52.2 (20.0) |
59.4 (18.8) |
61.2 (21.4) |
62.4 (25.0) |
| S.E. | 1.7 | 1.3 | 1.5 | 2.5 | 1.2 |
| Median (IQ range) |
52.0 (41.0-66.8) |
49.0 (38.0-66.0) |
58.0 (46.0-71.7) |
59.5 (47.0-74.5) |
60.0 (45-0-76.0) |
| NaCl intake (g/day) | |||||
| Mean (SD) |
10.3 (4.2) |
9.8 (4.6) |
11.1 (4.0) |
9.0 (3.8) |
8.0 (3.6) |
| S.E. | 0.3 | 0.3 | 0.3 | 0.4 | 0.1 |
| Median (IQ range) |
9.7 (7.3-13.2) |
9.0 (6.7-12.6) |
11.0 (8.1-13.5) |
8.4 (6.0-11.3) |
7.3 (5.3-9.9) |
| Potassium intake (g/day) | |||||
| Mean (SD) |
2.8 (1.0) |
2.6 (1.0) |
3.0 (0.9) |
3.1 (1.0) |
3.1 (1.2) |
| S.E. | 0.09 | 0.06 | 0.08 | 0.13 | 0.06 |
| Median (IQ range) |
2.6 (2.1-3.4) |
2.4 (1.9-3.3) |
2.9 (2.3-3.6) |
3.0 (2.3-3.7) |
3.0 (2.3-3.8) |
| Na-to-K ratio | |||||
| Mean (SD) |
3.1 (1.2) |
3.2 (1.5) |
3.1 (1.1) |
2.4 (0.8) |
2.3 (1.4) |
| S.E. | 0.1 | 0.1 | 0.09 | 0.1 | 0.07 |
| Median (IQ range) |
2.9 (2.2-3.9) |
2.9 (2.2-3.9) |
3.1 (2.4-3.7) |
2.3 (1.7-3.0) |
2.0 (1.4-2.9) |
| Urinary iodine excretion (µg/l) |
114 | 60 | 78 | 43 | 223 |
| Mean (SD) | 169.1 (164.4) | 157.3 (83.5) | 153.4 (64.2) | 110.9 (147.3) | 146.1 (136.7) |
| S.E. | 15.5 | 10.7 | 7.3 | 22.4 | 9.2 |
| Median (IQ range) |
140.5 (105.8-181.2) |
138.6 (99.9-196.1) |
146.6 (111.3-179.5) |
126.7 (79.0-169.3) |
122.3 (90.4-171.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



