
Submitted:
02 July 2024
Posted:
02 July 2024
You are already at the latest version
Abstract
This longitudinal study aimed to analyze the effects of a team rowing-based training program on physical fitness and anthropometric parameters in female breast cancer survivors (n=40; 56.78±6.38 years). Participants were divided into two groups: one rowed in fixed seat rowing (FSR) boats (n=20; 56.35±4.89 years) and the other in sliding seat rowing (SSR) boats (n=20; 57.20±7.7 years). Both groups engaged in two 75-minute sessions per week for 24 weeks. Significant improvements were observed in both groups in resting heart rate (FSR: -10.65 bpm; SSR: -8.45 bpm), heart rate at the beginning of the 6-minute walk test (6MWT) (FSR: -10.7 bpm; SSR: -11.25 bpm), and heart rate at the end of the test (FSR: -13.85 bpm; SSR: -20.35 bpm). Blood pressure improved significantly in both diastolic blood pressure (FSR: -12.35 mmHg; SSR: -19.25 mmHg) and systolic blood pressure (FSR: -13 mmHg; SSR: -16.95 mmHg). Additionally, both groups increased the distance covered in the 6MWT (FSR: +63.05 m; SSR: +93.65 m). These results suggest that a rowing training program is a viable and safe activity for female breast cancer survivors, improving cardiac function, blood pressure, and cardiorespiratory capacity, particularly in sliding seat boats.
Keywords:
rowing
; breast cancer
; physical activity
; cardiac function
; exercise.
1. Introduction
The evolution of scientific knowledge is changing the paradigm of cancer from diagnosis and subsequent pharmacological treatment to a holistic and multidisciplinary approach that treats the individual through comprehensive therapeutic programs. In this regard, physical exercise has been postulated to play an important role in protecting against cancer. [(Spanoudaki et al., 2023)]. As an example, it has been noted that the risk of breast cancer-related mortality appears to be significantly lower among survivors who adopt a physically active routine, in contrast to those who lead a sedentary lifestyle [(Kim, Choi, & Jeong, 2013)].
Breast cancer represents the most prevalent type of cancer in women, with 2.3 million diagnoses in 2020 and is the leading cause of cancer-related deaths in the female population on a global scale [(World Health Organization, 2023)]. Despite this, the survival rate is close to 90% in most countries, so there is a high number of women who survive the disease for at least 5 years after initial treatment [(Hidrobo-Coello, 2020; Moro et al., 2024)]. However, despite this high survival rate, it is important to note that the side effects associated with the disease and its treatment, such as cancer-related fatigue [(Prieto-Gómez et al., 2022)], lymphedema [(Iacorossi et al., 2019)], cardiovascular disease [(Amin et al., 2024; Gonzalo-Encabo et al., 2023)], loss of bone mass [(Sturgeon et al., 2023)] or psychological problems such as anxiety or depression [(Todorov, Sherman, & Kilby, 2019)], can persist for long periods of time, ranging from months to years.
If we focus on the side effects produced or exacerbated by the treatment of oncological diseases, we find that cardiovascular diseases and breast cancer share numerous risk factors such as age, diet, family history, alcohol consumption, obesity and overweight, level of physical activity and tobacco use [(Gonzalo-Encabo et al., 2023)]. Yet, they share an even more relevant common risk factor since current breast cancer treatments, based on chemotherapy, radiotherapy and endocrine therapies, have a potentially deleterious effect related to cancer-induced cardiotoxicity and, consequently, to the development of cardiovascular disease [(Amin et al., 2024; Gonzalo-Encabo et al., 2023)]. Therefore, there is a need to examine which types of complementary non-pharmacological interventions can help to reduce the risk of developing cardiovascular disease in female breast cancer survivors.
The diagnosis of cancer is often accompanied by drastic changes in a person’s life. Taking into account that the lifestyle adopted can positively influence the chances of survival of the disease [(Harvie, Howell, & Evans, 2015)], as well as protect against the possible sequelae of treatment [(Courneya, Mackey, & Jones, 2000; Roscoe, Pringle, Chandler, Faghy, & Barratt, 2022)], scientific evidence has shown that engaging in physical exercise can reduce the onset of symptoms associated with cancer treatment and improve physical fitness and mental health [(Murri et al., 2023; Patsou, Alexias, Anagnostopoulos, & Karamouzis, 2017; Prieto-Gómez et al., 2022; Spanoudaki et al., 2023)]. This research has shown that a controlled training program can produce significant improvements in aerobic capacity, as well as an increase in muscle mass and strength, in addition to improving functionality of the upper limbs in women with breast cancer [(Mascherini et al., 2019; Parkinson et al., 2023; Rogers et al., 2023; Sousa et al., 2024)]. The majority of the studies consulted affirm that physical activity positively influences health status, mood, and body composition, positively affecting the quality of life of survivors [(Campbell et al., 2019; Murri et al., 2023; Patsou et al., 2017; Schleicher et al., 2022; Shachar et al., 2022)].
Despite the proven benefits of exercise and its positive impact on the health of women with breast cancer [(Goldschmidt, Schmidt, & Steindorf, 2023; Gonzalo-Encabo et al., 2023; Schmitz et al., 2019; Spanoudaki et al., 2023)], the level of physical activity is significantly reduced during cancer treatment [(García-Chico et al., 2023)], and remains even lower than it was before diagnosis [(Goldschmidt et al., 2023)]. Unfortunately, studies have shown that women who have been diagnosed with breast cancer decrease their physical activity by 11%, falling even further in those who are treated with chemotherapy (50%) and radiotherapy (24%), compared to untreated women [(García-Chico et al., 2023)]. Fatigue, low motivation, kinesiophobia, fear of lymphedema, and difficulties in accessing sports facilities are the main barriers to participation in physical activities in cancer patients [(Moro et al., 2024)]. Because of this, it is important to promote strategies and activities that encourage adherence to physical activity, even during treatment of the disease [(Courneya et al., 2014)].
Within this context, programs based on rowing have now emerged as a possible non-pharmacological therapy to ameliorate the side effects of cancer and to slow the decline associated with cancer and its treatment [(Asensio-García et al., 2021; Gavala-González, Torres-Pérez, & Fernández-García, 2021; Iacorossi et al., 2019; Moro et al., 2024)]. Rowing is a water sport in which a boat is propelled by the use of oars. In this discipline, rowers use the oars as second-degree levers, moving them in the opposite direction to the forward motion of the boat. Some of the benefits associated with this type of rowing-based exercise indicate an improvement in the physical condition of the participants [(Gavala-González, Gálvez-Fernández, Mercadé-Melé, & Fernández-García, 2020; Moro et al., 2024)], mental and psychological health [(Blanzola, O’Sullivan, Smith, & Nelson, 2016; McDonough, Patterson, Weisenbach, Ullrich-French, & Sabiston, 2019; Parry, 2008)], prevention of lymphedema [(Iacorossi et al., 2019; Unruh & Elvin, 2004)], and ultimately, an improvement in the quality of life of women rowers [(Asensio-García et al., 2021; Gavala-González, Torres-Pérez, et al., 2021; Moro et al., 2024)].
It is important to note that there are two main types of rowing: sliding seat rowing (SSR), characterized by movement of the seats to facilitate leg thrust, and fixed seat rowing (FSR), in which the rowers remain in a static seat during the exercise [(Gavala-González, 2019)]. There are clear biomechanical differences in the technical movements between the two modalities, particularly with regard to the upper limbs. In FSR, overhead shoulder flexion is required to execute the necessary movements. In contrast, in SSR, the movement of the arms is performed at shoulder height, which helps to reduce the strain on the upper extremities and trunk [(Asensio-García et al., 2021)].
Rowing was chosen because it involves the muscles of both the upper and lower extremities, as well as virtually every muscle in the body. Nevertheless, the distinguishing feature that sets it apart from most other sports is the cyclic and alternating action of flexion and extension of the upper and lower extremities, as well as the involvement of the stabilizing muscles of the trunk and back during the different phases of rowing [(Volianitis, Yoshiga, & Secher, 2020; Yoshiga & Higuchi, 2003)].
Currently, limited evidence is available on the impact of rowing on cardiac function and blood pressure in breast cancer survivors [(Stefani, Galanti, Di Tante, Klika, & Maffulli, 2015)]. Therefore, the aim of the following study will be to examine the influence of a rowing-based training program on cardiac function and aerobic capacity in female breast cancer survivors, as well as to compare the influence of boat type on the possible cardiovascular adaptations.
2. Materials and Methods
2.1. Design and Participants
This research is part of concurrent clinical trials. To support this, a 24-week training regimen, conducted twice a week, was developed for use in both FSR and SSR boats (Figure 1). Various breast cancer support groups were approached and given the opportunity to participate in a free 24-week rowing program, which included physical evaluations at the beginning and conclusion of the program. The only criteria for participation were a history of breast cancer and approval from their oncologist to engage in moderate physical activity.
The participants (N=40), aged 56.78 ± 6.38 years, were recruited on the condition that they had been diagnosed with breast cancer 6.58 ± 5.72 years previously, with varying degrees of involvement and with subsequent surgery as shown in Table 1.
After the initial selection, the nature of the study was explained to the participants, indicating that their anonymity would be maintained at all times, following the ethical considerations of Sport and Exercise Science Research [(Harriss, D.; Macsween, A.; Atkinson, 2017)] and with the principles included in the Declaration of Helsinky [(Ebihara, 2000)], which define the ethical guidelines for research in humans. The University of Malaga provided the identification number registered for the Ethics Committee: 65-2020-H, and the participants (Figure 2) completed a written informed consent. Throughout the intervention and subsequently, we acted under the provisions of organic law 3/2018, of December 5, on the Protection of Personal Data and Guarantee of Digital Rights, regarding the protection of personal data under Spanish legislation.
2.2. Instruments
A Tanita model BC730 scale (Tanita Corporation, Tokyo, Japan), accuracy 0.1 kg, was used to weigh the subjects, and a SECA model 213 portable measuring rod (Seca GmbH & Co. KG, Hamburg, Germany), accuracy 0.1 cm, was used to measure height. The 6-minute walk test was used to evaluate cardiac function, which is a valid and reliable test that assesses a person’s cardiorespiratory capacity by measuring the maximum distance they can walk on a flat surface in 6 minutes. At the same time, heart rate per minute was monitored immediately before and after finishing the test using a Polar H10 chest strap (Polar Electro Oy, Kempele, Finland), which was fitted before the start of the test and transmitted the signal to the POLAR tablet application. For blood pressure measurement, the Omron M6 Comfort IT brachial blood pressure monitor (Omron Healthcare Co., Ltd., Kyoto, Japan) was used, which indicates systolic and diastolic blood pressure and pulse rate per minute.
2.3. Procedure
Among all the women who expressed interest, a series of physical fitness assessments were conducted. With equivalent anthropometric measurements (weight, height, BMI) and test results, a participant was assigned to one group (FSR or SSR). The participant with the most comparable results was assigned to the other group (SSR or FSR). The participants were thus divided into two training groups with similar characteristics (Table 2):
The 24-week rowing training program was divided into three 4-week stages. These stages progressively increased in intensity, and were adjusted through the participants’ subjective perception of effort using the Börg scale [(Börg, 1982)].
- Initial phase with mobility exercises, proprioceptive exercises and postural control exercises. Main phase with rowing training. Final phase with stretching. Börg scale 5-6.
- Intermediate phase with mobility exercises, proprioceptive exercises and postural control exercises. Main phase with rowing training. Final phase with stretching. Börg scale 6-7.
- Final phase with mobility exercises, proprioceptive exercises and postural control exercises. Main phase with rowing training. Final phase with stretching. Börg scale 7-8.
Throughout the program, there were 2 days of training per week. Each session lasted 75 minutes. These sessions were supervised by a trainer who ensured attendance, correct execution of the tasks and intensity of the sessions, in addition to excluding from the study those subjects who did not achieve at least 90% participation. Each training session had the same structure:
- Initial part performed with warm-up, mobility, proprioceptive and postural control exercises, all performed in a multipurpose room (5-10 minutes).
- Cool down: Flexibility exercises to relax the muscles and bring the body back to its initial state after the effort (10-15 minutes).
2.4. Data Analysis
All analyses were performed with the IBM SPSS Statistics 25 statistical package. The significance level was set at p 0.05. The adjustment of the different variables to the normal distribution was assessed by both graphic procedures and the Shapiro-Wilk test.
To determine whether there were differences as a result of the rowing training undertaken by the participants, the medians of each variable pre- and post-intervention were analyzed using the Wilcoxon test for related samples (paired data). In addition, the graphic analysis of the different variables was performed using boxplots or box and whisker plots. To analyze whether there were differences according to the rowing training performed by the participants, the data from the pre-test and post-test measurements were compared through the different tests. The estimated between-subject marginal means (Boat*Measurement) and the standard deviation were considered when quantifying the interaction between the variables and their longitudinal evolution through a repeated-measures ANOVA, applying the Bonferroni post hoc test.
3. Results
Table 3 shows the evolution of the results obtained after carrying out the rowing-based training protocol taking into account the measurements in both groups. There was a significant improvement in the mean values for cardiac variables, blood pressure and cardiorespiratory capacity after the intervention program.
If we look at the differences obtained according to the type of vessel used in the training program (Table 4), we see that both the subjects who performed FSR and those who performed SSR significantly improved all the parameters related to cardiac function and cardiorespiratory capacity. Furthermore, in the SSR group, better results were obtained after the intervention protocol in all the variables of the study compared to the FSR group (Initial HR, Final HR, Diastolic BP, Systolic BP and the 6-minute walk test [6MWT]), except in Rest HR, which also shows a positive evolution.
An in-depth analysis of the results is shown in Figure 3, considering the type of boat used in the training protocol, the evolution of the variables associated with cardiac function at rest, before starting the 6MWT and at the end of the test. Both groups had significant improvements in resting heart rate (FSR: Δpre-post Rest HR=-10.65; p=.000; SSR: Δpre-post Rest HR=-8.45; p=.000), initial rate before the test (FSR: Δpre-post Initial HR=-10.7; p=.000; SSR: Δpre-post Initial HR=-11.25; p=.000) and final rate after the test (FSR: Δpre-post Final HR=-13.85; p=.000; SSR: Δpre-post Final HR=-20.35; p=.000).
Figure 4 provides the blood pressure measurements obtained before and after the 6MWT. Both the FSR and SSR groups showed significant improvements in systolic (FSR: Δpre-post Systolic BP=-13; p=.000; SSR: Δpre-post Systolic BP=-16.25; p=.000) and diastolic (FSR: Δpre-post Diastolic BP=-12.35; p=.000; SSR: Δpre-post Diastolic BP=-19.25; p=.000) blood pressure, although these improvements were slightly greater in the women who rowed in the SSR group.
4. Discussion
In recent years, therapeutic programs based on rowing have been proposed as a type of non-pharmacological strategy that modulates adverse effects in female breast cancer survivors by involving moderate-intensity physical exercise that combines aerobic and muscle strength training [(Asensio-García et al., 2021)]. The potential of this activity lies in a viable, sustainable and safe model that can be tolerated by different age groups [(Asensio-García et al., 2021; Iacorossi et al., 2019; Stefani et al., 2015)]. Consequently, recent studies have shown, after 4 years of follow-up, that women who participated in Dragon Boat training were able to maintain their cardiac parameters within normal ranges for their age (compared to healthy active individuals), despite chemotherapy treatment, in addition to not developing any type of cardiac condition during this period [(Stefani et al., 2015) Other studies conducted over 12 weeks in this type of vessel, have reported a 30% improvement in cardiorespiratory capacity, also measured through the 6MWT [(Moro et al., 2024)]. Despite these improvements, there are no studies that verify which type of boat is more suitable when designing novel therapeutic programs based on rowing activity, since the muscle groups and exercise dynamics involved in fixed seat rowing differ from rowing on a sliding seat.
With this in mind, statistically significant improvements in cardiac function, systolic and diastolic blood pressure and cardiorespiratory capacity can be observed when analyzing the results of our study. These improvements after implementation of the intervention protocol occur in both the FSR group and the rowers who participated in the SSR. When comparing the groups, a higher rate of improvement in resting heart rate can be seen in the FSR group, while the female breast cancer survivors who participated in the SSR group had greater improvements in the variables of heart rate before and after the 6MWT, systolic and diastolic blood pressure, and distance traveled in the 6MWT (directly correlated with the cardiorespiratory capacity and VO2max of the subjects). According to the data, although the rowing activity itself can promote cardiac adaptations that optimize the functioning of the cardiovascular system, with the SSR modality, greater adaptations occur comparatively considering the same time span (12 weeks).
Cardiac function adaptations were also found after a 12-week intervention when we compared the results, focusing on the variables of our study, with previous studies that used rowing training programs in breast cancer survivors [(Gavala-González, Gálvez-Fernández, Mercadé-Melé, & Fernández-García, 2021)]. The results showed a 10% improvement in the systolic and diastolic blood pressure of the participating women. These results are consistent with other rowing studies, such as those by Stefani et al. [(Stefani et al., 2015)], which showed significant improvements in diastolic function in women breast cancer survivors treated with chemotherapy after 4 years of Dragon Boat training [(Stefani et al., 2015)] or by Serra et al. [(Serra, Ryan, Ortmeyer, Addison, & Goldberg, 2018)] who found that a 16-week resistance training program that improved systolic and diastolic blood pressure by 5% in breast cancer survivors. These results indicate the positive impact that a professionally supervised intervention program based on rowing could have on myocardial function, even in women previously treated with chemotherapy [(Stefani et al., 2015)].
This is important because one of the main problems associated with oncological treatments is chemotherapy-induced cardiotoxicity, which has direct and indirect adverse effects on the cardiovascular system [(Amin et al., 2024; Ginzac, Bernadach, Molnar, & Duclos, 2021; Howden et al., 2021)]. As an example, it has been shown that the incidence of left ventricular dysfunction among patients treated with certain anticancer drugs, such as high-dose doxorubicin (700 mg/m²), can reach 48%. The incidence of myocardial ischemia due to 5-fluorouracil (5-FU) can be as high as 10% [(Frickhofen et al., 2002; Jose Luis Zamorano, Patrizio Lancellotti, Daniel Rodriguez Muñoz, Victor Aboyans, Riccardo Asteggiano, Maurizio Galderisi, Gilbert Habib, Daniel J Lenihan, Gregory Y H Lip, Alexander R Lyon, Teresa Lopez Fernandez, Dania Mohty, Massimo F Piepoli, Juan Tam, 2016)]. Furthermore, between 26% and 93% of patients with arsenic trioxide show a prolonged QT interval, and many develop life-threatening ventricular tachyarrhythmias [(Lenihan & Kowey, 2013)]. As a result, chemotherapy-induced cardiotoxicity has been associated with cardiovascular diseases such as myocardial dysfunction, heart failure, coronary artery disease, arrhythmias, arterial hypertension, thromboembolic disease, peripheral vascular disease, pulmonary hypertension, and pericardial complications [(Amin et al., 2024; Odynets, Briskin, Ikkert, Todorova, & Yefremova, 2020)].
In this context, clinical trials in breast cancer survivors based on pharmacological strategies (e.g. beta-blockers, angiotensin-converting enzyme inhibitors, etc.) have shown some benefits in the treatment of cardiovascular disease, but also adverse effects. [(Gonzalo-Encabo et al., 2023)]. A rowing-based training program offers a non-pharmacological therapy that can safely contribute to achieving the goals proposed by the American College of Sports Medicine (ACSM), which recommends that cancer survivors perform at least 150 minutes of moderate physical activity or 75 minutes of vigorous exercise, as well as incorporating strength training twice a week [(Rock et al., 2022)]. Reviews, such as that by Sturgeon et al. [(Sturgeon et al., 2023)], suggest that aerobic exercise has a moderate effect on improving cardiac function in women with breast cancer, consistent with findings in disease-free populations. Furthermore, Gonzalo-Encabo et al. [(Gonzalo-Encabo et al., 2023)] after reviewing published studies, found that 16 weeks of aerobic and resistance training can reduce the risk of cardiovascular disease by 15% in Hispanic and Latina breast cancer survivors (at greater risk than the rest of the population of developing this type of disease).
Rowing is an activity that combines the benefits of aerobic exercise and strength training and can have a beneficial effect on cardiovascular health in female breast cancer survivors [(Gavala-González, Gálvez-Fernández, et al., 2021)]. In this study, we can see a directly proportional relationship between cardiorespiratory capacity, heart rate, and blood pressure in female rowers who participated in both training groups. Better cardiorespiratory capacity improves the heart’s ability to maintain function and pump blood with less effort. [(Ross et al., 2016)]. Exercise can also improve the regulation of the autonomic nervous system, reducing the activity of the sympathetic nervous system (which increases blood pressure and heart rate) and increasing that of the parasympathetic nervous system (which decreases heart rate) [(Amin et al., 2024; García-Chico et al., 2023)]. Our study showed an overall improvement of 9-10 beats less at rest after 12 weeks of training. In addition, exercise-induced improvement of endothelial function [(Gonzalo-Encabo et al., 2023)] may lead to improved arterial health contributing to the prevention of diseases such as hypertension. As we can see, after 24 weeks of rowing training, diastolic blood pressure decreased overall by 10%, while systolic blood pressure decreased by 15%. Moreover, these results were more prominent in the SSR group rowing on a sliding seat boat than in the FSR group, which rowed on a fixed seat boat.
Despite advances in research on the relationship between physical exercise and non-pharmacological oncological therapy, there is still insufficient scientific evidence to develop an exercise prescription for most people with this disease [(Sturgeon et al., 2023)]. More research is therefore needed to understand how physical activity and sport interact with the disease, what the consequences are for the individual and what the best strategies are for oncological rehabilitation through exercise [(Campbell et al., 2019; Schmitz et al., 2019)].
The strength of this pioneering study is the data it provides on physical activity and rowing, not only demonstrating that rowing is a viable and safe sport for breast cancer survivors, but also which type of boat produces the greatest positive changes in cardiac function in the participants. However, the study also has some limitations related to the sample power of the participants. Our findings are based on a relatively small sample, due to the very specific population encompassed by the study, the complexity in its recruitment and subsequent follow-up during the intervention protocol.
5. Conclusions
The present study shows that a rowing-based therapeutic program, combining aerobic and muscular strength exercises, can be a viable and safe strategy to improve cardiovascular health in female breast cancer survivors. It has been demonstrated that 24 weeks of rowing training can significantly improve cardiac function, blood pressure and cardiorespiratory capacity, and may mitigate the adverse effects of cardiotoxicity induced by cancer treatments. These results are particularly noteworthy in the group using SSR boats, which showed greater cardiovascular adaptations compared to the group using FSR boats. This novel study highlights the importance of further exploring and validating the beneficial effects of physical exercise in cancer rehabilitation, opening the door to new non-pharmacological therapeutic strategies to improve the health and well-being of this vulnerable population.
Author Contributions
Conceptualization, J.G-G., M.R-P. and J.C.F-G.; methodology, J.G.-G. and J.G.-G.; software, M.R.-P.; validation, J.C.F.-G., J.G.-G. and J.G.-G.; formal analysis, M.R.-P.; investigation, M.R.-P. and J.G.-G.; resources, J.G.-G. and M.R.-P.; data curation, J.G.-G.; writing—original draft preparation, M.R.-P. and J.G.-G.; writing—review and editing, M.R.-P., J.G.-G. and J.C.F.-G.; visualization, J.G.-G.; supervision, J.C.F.-G.; project administration, J.G.-G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of the University of Malaga with the number 65-2020-H.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The Ethical Committee of the University of Malaga, which authorized this study, precludes ceding, showing or disclosing to third parties by any means the database of this research (personal data, medical history, interviews, physical condition tests and others) because it is considered confidential and sensitive information.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Amin, A. M., Khlidj, Y., Abuelazm, M., Ibrahim, A. A., Tanashat, M., Imran, M., … Abdelazeem, B. (2024). The efficacy and safety of exercise regimens to mitigate chemotherapy cardiotoxicity: a systematic review and meta-analysis of randomized controlled trials. Cardio-Oncology, 10(1), 1–20. [CrossRef]
- Asensio-García, M. del R., Tomás-Rodríguez, M. I., Palazón-Bru, A., Hernández-Sánchez, S., Nouni-García, R., Romero-Aledo, A. L., & Gil-Guillén, V. F. (2021). Effect of rowing on mobility, functionality, and quality of life in women with and without breast cancer: a 4-month intervention. Supportive Care in Cancer, 29(5), 2639–2644. [CrossRef]
- Blanzola, C., O’Sullivan, P., Smith, K., & Nelson, R. (2016). The Benefits of Dragon Boat Participation for Breast Cancer Survivors. Therapeutic Recreation Journal, 50(3). https://doi.org/10.18666/trj-2016-v50-i3-7511. [CrossRef]
- Börg, G. (1982). Psychophysical bases of perceived exertion. Medicine and Science in Sports and Exercise, 14(5), 377–381. [CrossRef]
- Campbell, K. L., Winters-Stone, K. M., Wiskemann, J., May, A. M., Schwartz, A. L., Courneya, K. S., … Schmitz, K. H. (2019). Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Medicine and Science in Sports and Exercise, 51(11), 2375–2390. [CrossRef]
- Courneya, K. S., Mackey, J. R., & Jones, L. W. (2000). Coping with cancer: Can exercise help? Physician and Sportsmedicine, 28(5), 49–73. [CrossRef]
- Courneya, K. S., Segal, R. J., Gelmon, K., Mackey, J. R., Friedenreich, C. M., Yasui, Y., … McKenzie, D. C. (2014). Predictors of adherence to different types and doses of supervised exercise during breast cancer chemotherapy. International Journal of Behavioral Nutrition and Physical Activity, 11(1), 85. [CrossRef]
- Ebihara, A. (2000). World medical association declaration of Helsinki. Japanese Pharmacology and Therapeutics. [CrossRef]
- Frickhofen, N., Beck, F. J., Jung, B., Fuhr, H. G., Andrasch, H., & Sigmund, M. (2002). Capecitabine can induce acute coronary syndrome similar to 5-fluorouracil. Ann Oncol, 13(5), 797-801. [CrossRef]
- García-Chico, C., López-Ortiz, S., Peñín-Grandes, S., Pinto-Fraga, J., Valenzuela, P. L., Emanuele, E., … Santos-Lozano, A. (2023). Physical Exercise and the Hallmarks of Breast Cancer: A Narrative Review. Cancers, 15(1), 324. [CrossRef]
- Gavala-González, J. (2019). Las modalidades del remo: el remo en banco fijo. Sevilla, Spain: Universidad de Sevilla.
- Gavala-González, J., Gálvez-Fernández, I., Mercadé-Melé, P., & Fernández-García, J. C. (2020). Rowing training in breast cancer survivors: A longitudinal study of physical fitness. International Journal of Environmental Research and Public Health, 17(14), 1–12. [CrossRef]
- Gavala-González, J., Gálvez-Fernández, I., Mercadé-Melé, P., & Fernández-García, J. C. (2021). Cardiac Effects of a Rowing Training Program in Breast Cancer Survivors. Sustainability (Switzerland), 13, 6805. [CrossRef]
- Gavala-González, J., Torres-Pérez, A., & Fernández-García, J. C. (2021). Impact of rowing training on quality of life and physical activity levels in female breast cancer survivors. International Journal of Environmental Research and Public Health, 18(13). [CrossRef]
- Ginzac, A., Bernadach, M., Molnar, I., & Duclos, M. (2021). Adapted Physical Activity for Breast Cancer Patients Treated with Neoadjuvant Chemotherapy and Trastuzumab Against HER2 ( APACAN2 ): A Protocol for a Feasibility Study, 11(April 2018), 1–8. [CrossRef]
- Goldschmidt, S., Schmidt, M. E., & Steindorf, K. (2023). Long-term effects of exercise interventions on physical activity in breast cancer patients: a systematic review and meta-analysis of randomized controlled trials. Supportive Care in Cancer, 31(2), 17–21. [CrossRef]
- Gonzalo-Encabo, P., Sami, N., Wilson, R. L., Kang, D.-W., Ficarra, S., & Dieli-Conwright, C. M. (2023). Exercise as Medicine in Cardio-Oncology: Reducing Health Disparities in Hispanic and Latina Breast Cancer Survivors. Current Oncology Reports, 25(11), 1237–1245. [CrossRef]
- Harriss, D.; Macsween, A.; Atkinson, G. (2017). Standards for Ethics in Sport and Exercise Science Research. International Journal of Sports Medicine, 38(14), 1126–1131.
- Harvie, M., Howell, A., & Evans, D. G. (2015). Can Diet and Lifestyle Prevent Breast Cancer: What Is the Evidence? American Society of Clinical Oncology Educational Book, (35), e66–e73. [CrossRef]
- Hidrobo-Coello, J. F. (2020). Actividad Física para pacientes con diagnóstico de Cáncer. Guía de prescripción deportiva para Ecuador. Revista Iberoamericana De Ciencias De La Actividad Física Y El Deporte, 9(3), 18–41. [CrossRef]
- Howden, E., Foulkes, S., Dillon, H., Bigaran, A., Wright, L., Janssens, K., … La Gerche, A. (2021). Traditional markers of cardiac toxicity fail to detect marked reductions in cardiorespiratory fitness among cancer patients undergoing anti-cancer treatment. European Heart Journal Cardiovascular Imaging, 22(4), 451–458. [CrossRef]
- Iacorossi, L., Gambalunga, F., Molinaro, S., De Domenico, R., Giannarelli, D., & Fabi, A. (2019). The effectiveness of the sport “dragon boat racing” in reducing the risk of lymphedema incidence: An observational study. Cancer Nursing, 42(4), 323–331. [CrossRef]
- Jose Luis Zamorano, Patrizio Lancellotti, Daniel Rodriguez Muñoz, Victor Aboyans, Riccardo Asteggiano, Maurizio Galderisi, Gilbert Habib, Daniel J Lenihan, Gregory Y H Lip, Alexander R Lyon, Teresa Lopez Fernandez, Dania Mohty, Massimo F Piepoli, Juan Tam, E. S. D. G. (2016). 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC. European Heart Journal, 37(36), 2768–2801. [CrossRef]
- Kim, J., Choi, W. J., & Jeong, S. H. (2013). The effects of physical activity on breast cancer survivors after diagnosis. J Cancer Prev., 18(3), 193–200. [CrossRef]
- Lenihan, D. J., & Kowey, P. R. (2013). Overview and management of cardiac adverse events associated with tyrosine kinase inhibitors. Oncologist, 18(8), 900–908. https://doi.org/10.1634/theoncologist.2012-0466. [CrossRef]
- Mascherini, G., Tosi, B., Giannelli, C., Grifoni, E., Degl’innocenti, S., & Galanti, G. (2019). Breast cancer: effectiveness of a one-year unsupervised exercise program. J Sports Med Phys Fitness, 59(3), 283–289. [CrossRef]
- McDonough, M. H., Patterson, M. C., Weisenbach, B. B., Ullrich-French, S., & Sabiston, C. M. (2019). The difference is more than floating: factors affecting breast cancer survivors’ decisions to join and maintain participation in dragon boat teams and support groups. Disability and Rehabilitation, 41(15), 1788–1796. [CrossRef]
- Moro, T., Casolo, A., Bordignon, V., Sampieri, A., Schiavinotto, G., Vigo, L., … Cerea, S. (2024). Keep calm and keep rowing: the psychophysical effects of dragon boat program in breast cancer survivors. Supportive Care in Cancer, 32(4). [CrossRef]
- Murri, A., Vitucci, D., Tranchita, E., Grazioli, E., Gori, S., Modena, A., … Cerulli, C. (2023). “OPERATION PHALCO”—Adapted Physical Activity for Breast Cancer Survivors: Is It Time for a Multidisciplinary Approach? Cancers, 15(1), 1–11. [CrossRef]
- Odynets, T., Briskin, Y., Ikkert, O., Todorova, V., & Yefremova, A. (2020). Cardiopulmonary function in breast cancer patients versus healthy control women, 28(1), 6–10.
- Parkinson, J., Bandera, A., Crichton, M., Shannon, C., Woodward, N., Hodgkinson, A., … van der Meij, B. S. (2023). Poor Muscle Status, Dietary Protein Intake, Exercise Levels, Quality of Life and Physical Function in Women with Metastatic Breast Cancer at Chemotherapy Commencement and during Follow-Up. Current Oncology, 30(1), 688–703. [CrossRef]
- Parry, D. C. (2008). The contribution of dragon boat racing to women’s health and breast cancer survivorship. Qualitative Health Research, 18(2), 222–233. [CrossRef]
- Patsou, E. D., Alexias, G. D., Anagnostopoulos, F. G., & Karamouzis, M. V. (2017). Effects of physical activity on depressive symptoms during breast cancer survivorship: A meta-analysis of randomised control trials. ESMO Open, 2(5). [CrossRef]
- Prieto-Gómez, V., Yuste-Sánchez, M. J., Bailón-Cerezo, J., Romay-Barrero, H., de la Rosa-Díaz, I., Lirio-Romero, C., & Torres-Lacomba, M. (2022). Effectiveness of Therapeutic Exercise and Patient Education on Cancer-Related Fatigue in Breast Cancer Survivors : A Randomised, Single-Blind, Controlled Trial with a 6-Month. Journal of Clinical Medicine, 11, 269. [CrossRef]
- Rock, C. L., Thomson, C. A., Sullivan, K. R., Howe, C. L., Kushi, L. H., Caan, B. J., … McCullough, M. L. (2022). American Cancer Society nutrition and physical activity guideline for cancer survivors. CA: A Cancer Journal for Clinicians, 72(3), 230–262. [CrossRef]
- Rogers, L. Q., Courneya, K. S., Oster, R. A., Anton, P. M., Phillips, S., Ehlers, D. K., & McAuley, E. (2023). Physical activity intervention benefits persist months post-intervention: randomized trial in breast cancer survivors. Journal of Cancer Survivorship, 17(6), 1834–1846. [CrossRef]
- Roscoe, C. M. P., Pringle, A., Chandler, C., Faghy, M. A., & Barratt, B. (2022). The Role of Physical Activity in Cancer Recovery: An Exercise Practitioner’s Perspective. International Journal of Environmental Research and Public Health, 19(6). [CrossRef]
- Ross, R., Blair, S., Arena, R., Church, T., Després, J., Franklin, B., … Wisløff, U. (2016). Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign. Circulation, 134(24), 653–699. [CrossRef]
- Schleicher, E., Mcauley, E., Anton, P., Ehlers, D. K., Phillips, S. M., & Rogers, L. Q. (2022). Moderators of Physical Activity and Quality of Life Response to a Physical Activity Intervention for Breast Cancer Survivors Trial. Research Square, 1–24. [CrossRef]
- Schmitz, K. H., Campbell, A. M., Stuiver, M. M., Pinto, B. M., Schwartz, A. L., Morris, G. S., … Matthews, C. E. (2019). Exercise is medicine in oncology: Engaging clinicians to help patients move through cancer. CA: A Cancer Journal for Clinicians, 69(6), 468–484. [CrossRef]
- Serra, M. C., Ryan, A. S., Ortmeyer, H. K., Addison, O., & Goldberg, A. P. (2018). Resistance training reduces inflammation and fatigue and improves physical function in older breast cancer survivors. Menopause, 25(2), 211–216. [CrossRef]
- Shachar, S. S., Heiling, H., Muss, H. B., Meghan, D., Wagoner, C. W., Deal, A. M., & Nyrop, K. A. (2022). Physical Activity Intervention in Patients with Metastatic Breast Cancer During Active Treatment: Quality of Life and Function. The Oncologist, (September), 1–10. [CrossRef]
- Sousa, B. L. S. C., dos Santos Rosa, T., Silvino, V. O., Barros, E. M. L., de Luca Corrêa, H., do Prado, D. M. L., … dos Santos, M. A. P. (2024). Physical and autonomic functionality in women with breast cancer pre and post chemotherapy: a case control study. BMC Sports Science, Medicine and Rehabilitation, 16(1), 1–10. [CrossRef]
- Spanoudaki, M., Giaginis, C., Karafyllaki, D., Papadopoulos, K., Solovos, E., Antasouras, G., … Papadopoulou, S. K. (2023). Exercise as a Promising Agent against Cancer: Evaluating Its Anti-Cancer Molecular Mechanisms. Cancers, 15(21), 79–82. [CrossRef]
- Stefani, L., Galanti, G., Di Tante, V., Klika, R. J., & Maffulli, N. (2015). Dragon Boat training exerts a positive effect on myocardial function in breast cancer survivors. Physician and Sportsmedicine, 43(3), 307–311. [CrossRef]
- Sturgeon, K. M., Kok, D. E., Kleckner, I. R., Guertin, K. A., McNeil, J., Parry, T. L., … Winters-Stone, K. (2023). Updated systematic review of the effects of exercise on understudied health outcomes in cancer survivors. Cancer Medicine. [CrossRef]
- Todorov, N., Sherman, K. A., & Kilby, C. J. (2019). Self-compassion and hope in the context of body image disturbance and distress in breast cancer survivors. Psycho-Oncology, 28(10), 2025–2032. [CrossRef]
- Unruh, A. M., & Elvin, N. (2004). In the Eye of the Dragon: Women’s Experience of Breast Cancer and the Occupation of Dragon Boat Racing. Canadian Journal of Occupational Therapy, 71(3), 138–149. [CrossRef]
- Volianitis, S., Yoshiga, C. C., & Secher, N. H. (2020). The physiology of rowing with perspective on training and health. European Journal of Applied Physiology, 120(9), 1943–1963. [CrossRef]
- World Health Organization. (2023). Cancer. Retrieved August 26, 2023, from https://www.who.int/es/news-room/fact-sheets/detail/cancer.
- Yoshiga, C. C., & Higuchi, M. (2003). Rowing performance of female and male rowers. Scandinavian Journal of Medicine & Science in Sports, 13(5), 317–321. [CrossRef]
Figure 1.
Time line of the study. 6MWT: 6-minute walk test; AM: anthropometric measurements.
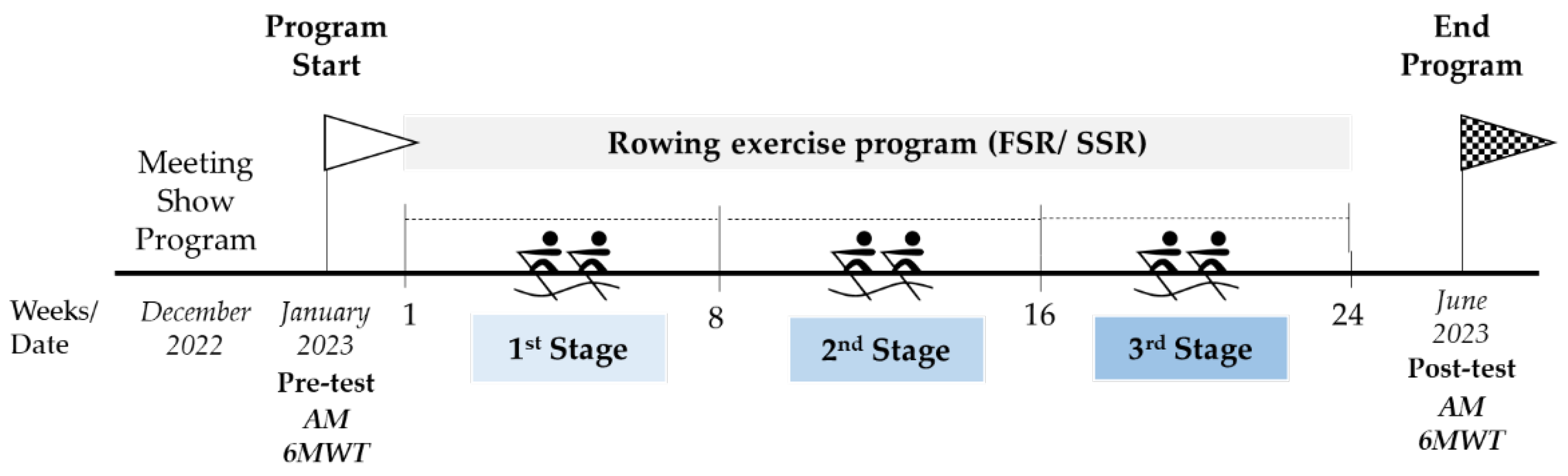
Figure 2.
A flow diagram of the sample selected for this study.
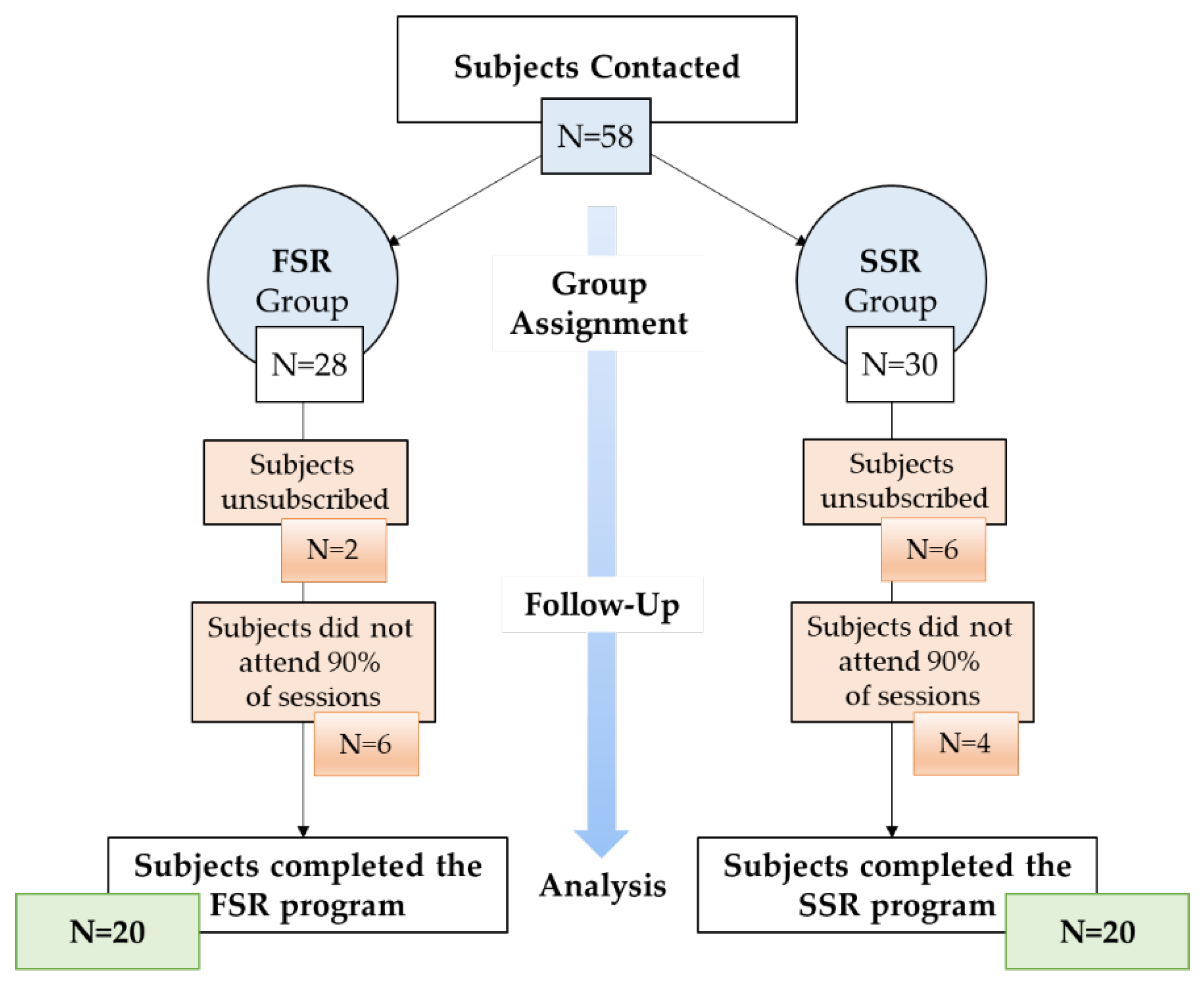
Figure 3.
Comparison of cardiac variables before and after rowing training according to boat type. HR=Heart Rate; FSR=Fixed Seat Rowing; SSR=Sliding Seat Rowing. *p<.05; **p<.001.
Figure 3.
Comparison of cardiac variables before and after rowing training according to boat type. HR=Heart Rate; FSR=Fixed Seat Rowing; SSR=Sliding Seat Rowing. *p<.05; **p<.001.
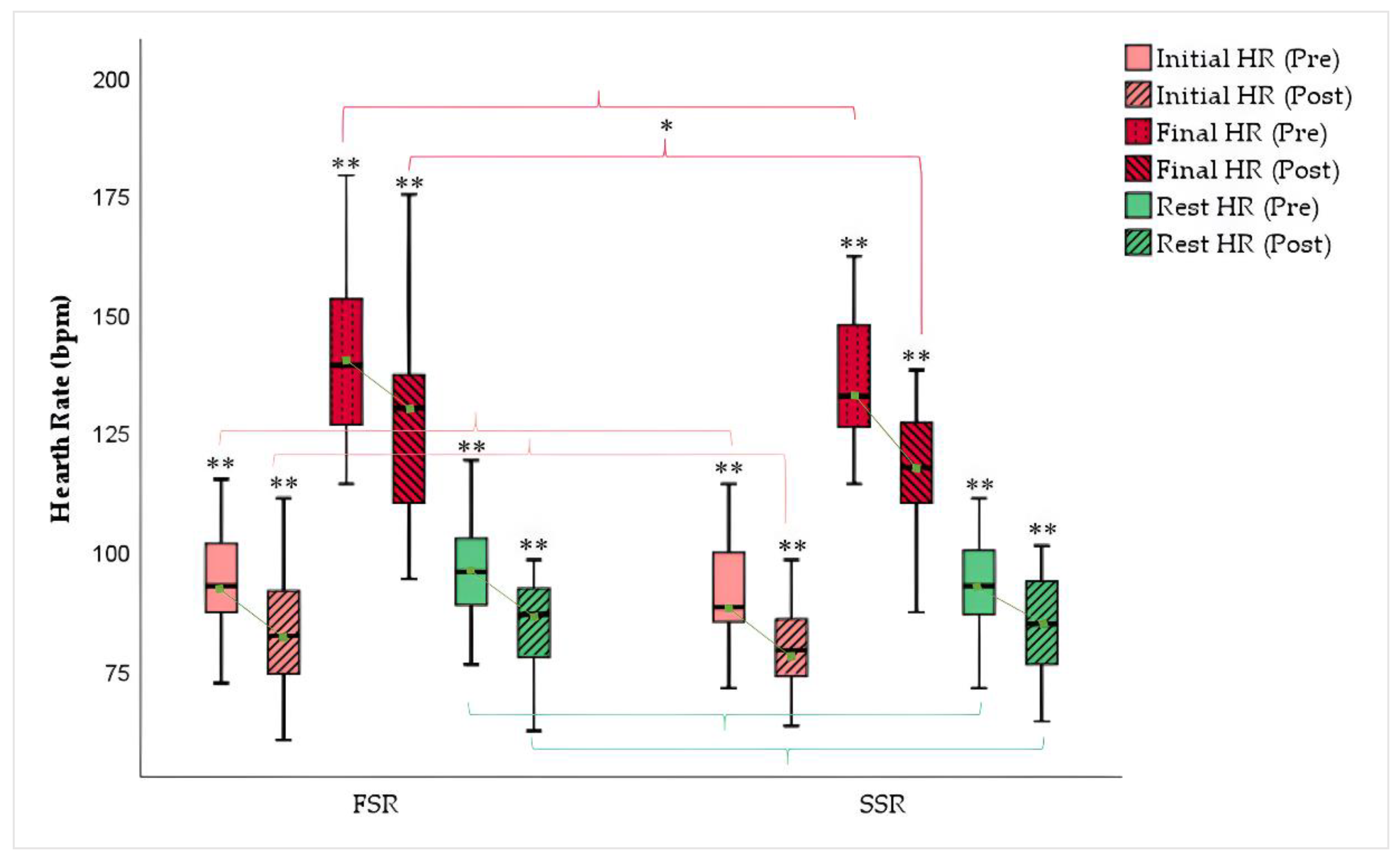
Figure 4.
Comparison of blood pressure before and after rowing training according to boat type. BP=Blood Pressure; FSR= Fixed Seat Rowing; SSR=Sliding Seat Rowing. *p<.05; **p<.001.
Figure 4.
Comparison of blood pressure before and after rowing training according to boat type. BP=Blood Pressure; FSR= Fixed Seat Rowing; SSR=Sliding Seat Rowing. *p<.05; **p<.001.
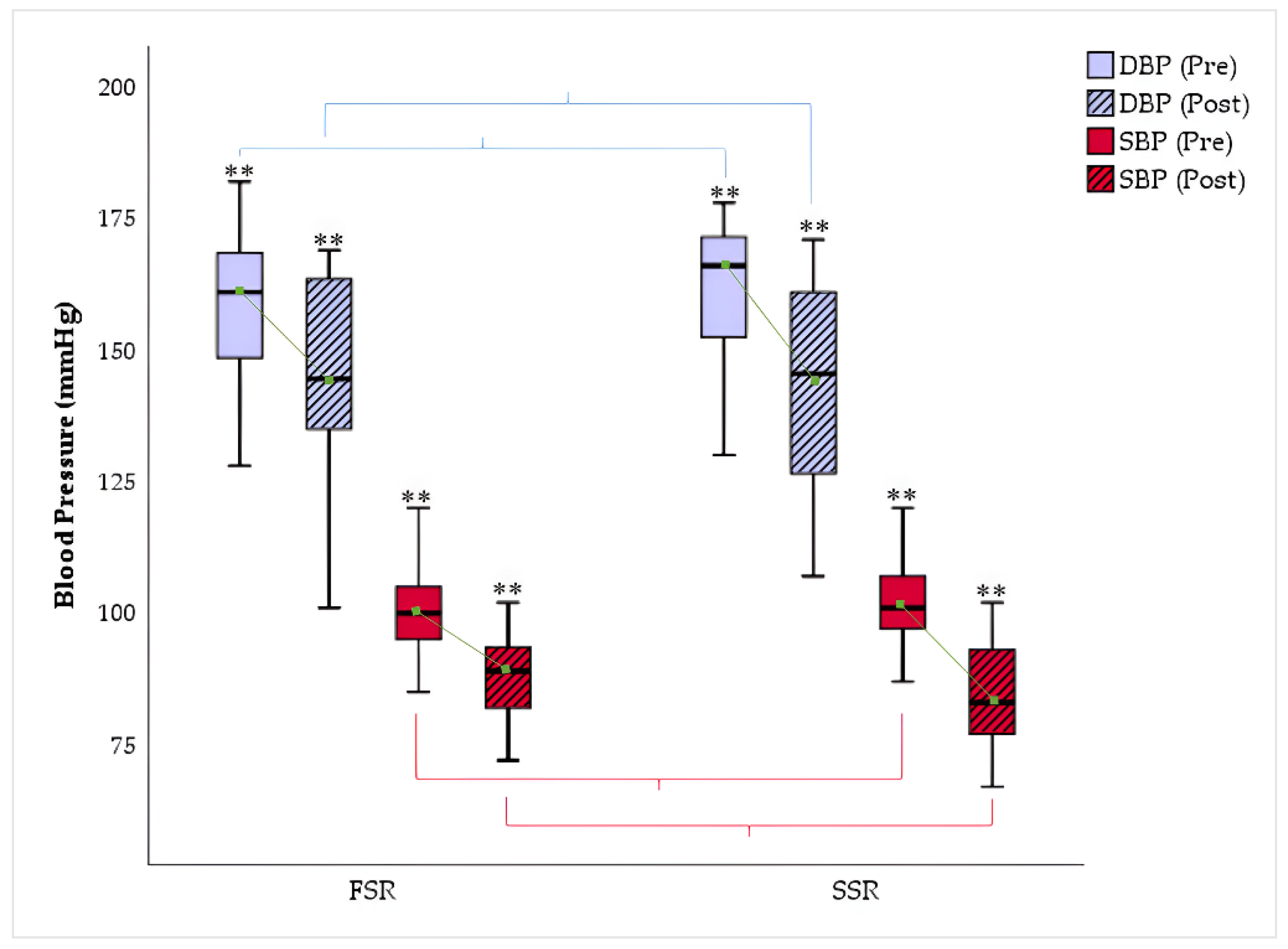

Table 1.
Characteristics of the sample.
| Breast (%) | |||||
| Right: 37.5 | Left: 57.5 | Both: 5.0 | |||
| Stage (%) | |||||
| I: 7.5 | II: 37.5 | III: 40.0 | IV: 15.0 | ||
| Surgery (%) | |||||
| Preservation: 50.0 |
Total Mastectomy: 42.5 | Double Mastectomy: 7.5 | |||
Table 2.
Descriptive analysis of study subjects according to training group.
| TOTAL (SSR + FSR) |
Fixed-Seat Rowing (FSR) | Sliding-Seat Rowing (SSR) | Difference of Means (FSR-SSR) | p | |
|---|---|---|---|---|---|
| Age (years) (SD) | 56.78 (6.38) | 56.35 (4.89) | 57.20 (7.7) | −0.85 (2.04) | 0.679 |
| Height (cm) (SD) | 162.05 (5.59) | 161.90 (4.91) | 162.20 (6.33) | −0.3 (1.79) | 0.868 |
| Weight (kg) (SD) | 69.49 (9.8) | 72.05 (8.11) | 66.92 (10.85) | 3.22 (3.11) | 0.307 |
| BMI (kg/m2) (SD) | 26.48 (3.58) | 27.48 (2.73) | 25.47 (4.09) | 1.50 (1.18) | 0.215 |
Table 3.
Within-subject analysis of the study variables after the intervention program.
| Pre-test (SD) | Post-test (SD) | ΔPre-Post (SD) | Student’s t | Effect size | p | ||
| Rest HR (ppm) | 94.33 (11.81) | 84.78 (11.27) | -9.55 (7.29) | 8.275 | 1.154 | .000** | |
| Initial Test HR (ppm) | 92.83 (12.76) | 81.85 /11.35) | -10.97 (7.59) | 9.145 | 1.2 | .000** | |
| Final Test HR (ppm) | 139.5 (18.44) | 122.4 (19.17) | -17.1 (15.69) | 6.891 | 2.481 | .000** | |
| Diastolic BP (mmHg) | 160.03 (13.37) | 144.23 (18.6) | -15.8 (16.36) | 6.109 | 2.587 | .000** | |
| Systolic BP (mmHg) | 100.78 (10.19) | 85.8 (9.8) | -14.97 (10.86) | 8.716 | 1.718 | .000** | |
| 6MWT (m) | 784.78 (103.64) | 863.13 (108.75) | +78.35 (62.57) | -7.92 | 9.893 | .000** | |
| **p<.001 |
Table 4.
Within-subject analysis of the study variables according to boat type.
| Fixed Seat Rowing (FSR) | Sliding Seat Rowing (SSR) | Interaction Effect Boat Measurement | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre-test (SD) | Post-test (SD) | ΔPre-Post | Pre-test (SD) | Post-test (SD) | ΔPre-Post | MS | F | p | |
| Rest HR (ppm) | 96.1 (11.54) | 85.45 (11.28) | -10.65 | 92.55 (11.51) | 84.1 (10.93) | -8.45 | 126.05 | .9 | .000** |
| Initial test HR (ppm) | 94.1 (14.21) | 83.4 (12.86) | -10.7 | 91.55 (10.58) | 80.3 (8.99) | -11.25 | 65.02 | .39 | .000** |
| Final test HR (ppm) | 141,75 (18.67) | 127.9 (22.38) | -13.85 | 137.25 (17.44) | 116.9 (12.47) | -20.35 | 202.5 | .59 | .000** |
| Diastolic BP (mmHg) | 158.25 (12.8) | 145.9 (17.32) | -12.35 | 161.8 (13.35) | 142.55 (19.2) | -19.25 | 126.05 | .7 | .000** |
| Systolic BP (mmHg) | 100.55 (10.51) | 87.55 (8.11) | -13 | 101 (9.59) | 84.05 (10.73) | -16.95 | 2.02 | .02 | .000** |
| 6MWT (m) | 817.25 (51.1) | 880.3 (69.96) | +63.05 | 752.3 (127.37) | 845.95 (132.58) | +93.65 | 42185.02 | 4.25 | .000** |
Interaction Effect Boat*Measurement refers to the influence of the type of boat used according to the training group on the variables; **p < 0.001.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



