
Submitted:
03 July 2024
Posted:
03 July 2024
You are already at the latest version
Abstract
We conducted a retrospective evaluation of the clinical outcomes and prognostic factors in patients with non-metastatic castration-resistant prostate cancer (nmCRPC) treated with first-line androgen receptor signaling inhibitors (ARSI) in real-world clinical practice in Japan. Between 2012 and 2023, a total of 127 consecutive patients with nmCRPC received ARSI treatment. Overall survival (OS), metastatic-free survival (MFS), and prostate-specific antigen progression–free survival (PSA-PFS) from ARSI initiation were assessed using Kaplan–Meier methodology. Clinical factors associated with OS in nmCRPC were analyzed using the Cox proportional hazards model. Among the patients, 72, 26, 12, and 17 received enzalutamide (ENZ), abiraterone (ABI), apalutamide (APA), and darolutamide (DARO) as first-line therapy. The median OS and MFS for all patients were 79.0 and 42.0 months, respectively. Median PSA-PFS was 27.0, 20.0, 10.0, and 14.0 months for patients treated with ENZ, ABI, APA, and DARO, respectively (p = 0.33). Multivariate analysis revealed that a baseline PSA level ≥3.67 ng/ml at ARSI initiation was significantly associated with poorer OS (p = 0.002). ARSI demonstrated favorable efficacy in nmCRPC patients. There were no significant differences in clinical outcomes among different types of ARSI therapy for nmCRP. Elevated baseline PSA at ARSI initiation was significantly associated with poorer OS.
Keywords:
non-metastatic castration-resistant prostate cancer
; androgen receptor signaling inhibitors
; overall survival
; prostate-specific antigen
; real-world clinical practice
Introduction
Prostate cancer remains the second most common malignancy among men worldwide [1]. In localized prostate cancer, primary treatments typically include radical prostatectomy or radiation therapy. However, recurrence occurs in 15 to 30% of treated patients [2,3], who subsequently undergo androgen deprivation therapy (ADT) as a standard treatment [4]. Unfortunately, some patients progress to non-metastatic castration-resistant prostate cancer (nmCRPC), which is associated with increased risks of metastasis and mortality. Median overall survival (OS) and bone metastasis–free survival in nmCRPC patients treated with ADT have been reported as 43.5 and 31.5 months, respectively [5].
Recently, three phase Ⅲ trials—SPARTAN, ARAMIS, and PROSPER—demonstrated that apalutamide (APA), darolutamide (DARO), and enzalutamide (ENZ) significantly extend metastatic-free survival (MFS) and OS for patients with nmCRPC [6,7,8]. The NCCN guidelines recommend offering androgen receptor signaling inhibitors (ARSIs) to nmCRPC patients if their PSA doubling time (PSADT) is ≤10 months [9]. Japanese public health insurance covers ENZ, APA, DARO, and abiraterone acetate (ABI) with prednisone for nmCRPC. Real-world clinical practice shows that PSA progression–free survival (PSA-PFS) and MFS are significantly improved with ENZ and ABI compared to first-generation antiandrogen therapy like flutamide [10]. Novel ARSIs have been associated with better oncological outcomes in nmCRPC patients compared to those not receiving ARSIs [11]. However, studies on the efficacy and safety of ARSIs in nmCRPC patients and comparisons among ENZ, APA, DARO, and ABI in real-world clinical settings remain limited. Furthermore, while some reports suggest PSADT as a prognostic factor for nmCRPC, the optimal cutoff value remains unclear [5,12]. Therefore, additional effective biomarkers are needed.
In this study, we conducted a retrospective evaluation of the clinical outcomes and prognostic factors among patients with nmCRPC treated with first-line ARSIs in real-world clinical practice in Japan.
Methods
Study Population
We retrospectively reviewed consecutive patients diagnosed with nmCRPC who were treated at our institution between March 2012 and August 2023. Radiological data from computed tomography (CT), magnetic resonance imaging (MRI), or bone scintigraphy, as well as clinical information from medical records including physical and pathological examination findings and laboratory results before and during ARSI therapy, were collected based on the attending physician’s records. This study was approved by the institutional ethics committee at the Cancer Institute Hospital, Japanese Foundation for Cancer Research. Written informed consent for ARSI therapy was obtained from all patients before initiating treatment.
Treatment and Follow-Up Examination
All patients received androgen deprivation therapy (ADT) throughout the treatment period. PSA progression was defined as a greater than 25% increase in PSA levels over two consecutive measurements separated by at least 1 week [13] despite maintaining low serum testosterone concentrations below 50 ng/mL with ADT, and confirmed absence of distant metastases using CT, MRI, or bone scintigraphy prior to the initiation of ARSI therapy. Patients with a history of distant metastases were excluded. ENZ, APA, and DARO were administered every 4 weeks. ABI was administered every 2 weeks for the first 3 months, then every 4 weeks thereafter. The recommended dosages for ENZ, APA, ABI, and DARO were 160 mg/day, 240 mg/day, 1000 mg/day, and 1200 mg twice daily, respectively. Clinical information, including physical examination findings, Karnofsky Performance Status, and laboratory results before and during ARSI therapy, was collected based on the attending physician’s decision. Evaluation for distant metastases was performed using conventional imaging modalities such as CT, MRI, or bone scintigraphy, as determined by the attending physician.
Statistical Analysis
Descriptive statistics for continuous variables are presented as the median and interquartile range (IQR), while categorical variables are reported as frequencies and percentages. PSA-PFS, MFS, and OS were defined as the time from initiation of ARSI therapy to PSA progression, first evidence of a distant metastasis on conventional imaging, and death from any cause, respectively. PSA response was defined as the proportion of the lowest PSA level relative to baseline PSA at the initiation of ARSI therapy. PSA progression was defined as a ≥ 25% and ≥ 2 ng/mL increase from the PSA nadir in men who had a reduction in PSA after ARSI initiation, and a ≥ 25% and ≥ 2 ng/mL increase from the PSA on the date of ARSI initiation in men with no reduction in PSA after ARSI initiation. Data were censored on the date of the last PSA measurement during ARSI treatment [13]. Patients who remained alive without disease progression and those lost to follow-up were censored at the time of their last follow-up or contact.
PSA-PFS, MFS, and OS curves were estimated using the Kaplan–Meier method, and differences were analyzed by the log-rank test. In addition, we investigated the association between OS and several clinicopathological factors, including Gleason pattern 5 at prostate biopsy, lactate dehydrogenase (LDH), alkaline phosphatase (ALP), PSA at initiation of ARSI therapy, time to CRPC, prior docetaxel chemotherapy, presence of regional lymph nodes, treatment type (surgery, radiation therapy, or no local treatment with combined androgen blockade), and PSADT calculated using the Pound et al. method [14]. The optimal cutoff values for ALP, LDH, time to CRPC, and PSA were determined based on receiver operating characteristic (ROC) curves, and patients were stratified into higher and lower groups based on these cutoffs.
Univariate and multivariate Cox proportional hazard models were used to assess the significant associations between OS and the clinical factors. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated to quantify these associations. Statistical analyses were performed using JMP software version 13.0 (SAS Institute, Cary, NC, USA), and p values <0.05 were considered statistically significant.
Results
Patient Characteristics
During the study period, 193 patients received ARSI therapy for nmCRPC. Among them, 19 patients with distant metastases at the initial diagnosis and 47 patients who received ARSI therapy as the second- or later line therapy for nmCRPC were excluded from the study. After excluding ineligible patients, a total of 127 patients who received ARSI therapy as the first-line treatment for nmCRPC comprised the cohort for this study.
The median follow-up period was 37.0 months (IQR, 18.0–61.1) after initiation of ARSI therapy. Disease progression resulted in the deaths of 23 patients (18.1%), while 12 patients (9.4%) died from disease progression and other causes. Distant metastases were evaluated in 109 patients using CT or bone scintigraphy. Patient characteristics are summarized in Table 1. Docetaxel chemotherapy was administered to six patients (4.7%) for the treatment of nmCRPC. The number of patients with Gleason Score (GS) ≥8, clinical T stage (cT) ≥3, and PSADT <6 months were 87 (69%), 82 (65%), and 99 (78%), respectively. Local treatment included surgery in 57 patients (45%) and radiation therapy in 46 patients (36%), while 24 patients (19%) did not undergo local treatment. ARSI therapy consisted of DARO in 17 patients (13%), APA in 12 patients (10%), ABI in 26 patients (20%), and ENZ in 72 patients (57%).
Efficacy of ARSI Therapy
During the follow-up period, 69 patients (54%) experienced PSA progression. The median PSA-PFS, 1-year, 3-year, and 5-year PSA-PFS for all 127 patients were 21.0 months, 61.9%, 33.8%, and 23.8%, respectively (Figure 1). A total of 62 (86.1%), 15 (57.7%), 9 (75.0%), and 12 patients (75.0%) achieved a ≥50% decrease in PSA; and 34 (47.2%), 11 (42.3%), 5 (41.7%), and 3 patients (17.6%) achieved a ≥90% decrease in PSA among patients treated with ENZ, ABI, APA, and DARO, respectively (Figure 2).
The median PSA-PFS and 1-year PSA-PFS rates with ENZ, ABI, APA, and DARO were 27.0, 20.0, 10.0, and 14.0 months, and 63.7%, 64.9%, 50.0% and 60.5% (p = 0.33), respectively (Figure 3). The median MFS, 1-year, 3-year, and 5-year MFS rates were 42.0 months, 79.2%, 60.9%, and 30.4%, respectively (Figure 4). The median OS, 1-year, 3-year, and 5-year OS rate were 79.0 months, 99.1%, 81.5%, and 64.4%, respectively (Figure 5).
Safety of ARSI Therapy
Forty-one patients (32%) experienced adverse events (AEs), with 4 (3.1%) classified as severe AEs (≥ grade 3), as detailed in Table 2. AEs were reported in 23 (31.9%), 6 (23.1%), 9 (75.0%), and 2 (17.6%) patients treated with ENZ, ABI, APA, and DARO, respectively. Although APA showed the highest proportion of AEs among all ARSIs (p = 0.005), there was no significant difference in severe AEs (p = 0.531).
The most common AEs associated with ENZ, ABI, APA, and DARO were fatigue (n = 11, 15.3 %), fatigue (n = 2, 7.7 %), rash (n = 6, 50.0 %), and fatigue (n = 2, 11.8 %), respectively. There was no significant difference in the proportion of fatigue among patients treated with ENZ, ABI, and DARO (p = 0.566). Eighteen patients (14.2 %) discontinued ARSI therapy due to AEs (ABI: n = 5, APA: n = 4, DARO: n = 2, and ENZ: n = 7).
Predictors of Prognosis in ARSI Therapy
We investigated possible prognostic factors in ARSI therapy based on pre-treatment variables. According to the ROC curve, the optimal cutoff values for LDH, ALP, time to CRPC, and PSA were 192 U/l, 271 U/l, 54 months, and 3.67 ng/mL, respectively. In multivariate analysis, PSA ≥3.67 at the initiation of first-line ARSI therapy emerged as the strongest predictor of poor prognosis for OS (p = 0.002; HR: 2.93, 95% CI: 1.46, 6.26) (Table 3).
When patients were stratified based on PSAs, differences were observed in the OS curves between those with PSA <3.67 and PSA ≥3.67 (Figure 6, p = 0.002). The median OS was not reached for patients with PSA <3.67, with a 5-year OS rate of 80.9%. For patients with PSA ≥3.67, the median OS was 60.0 months, with a 5-year OS rate of 48.0%.
Discussion
This study of nmCRPC patients receiving ARSI revealed three key findings. First, ARSI demonstrated favorable efficacy for nmCRPC patients. Second, there were no significant differences in clinical outcomes among different types of ARSI therapy for nmCRPC. Third, a high baseline PSA at the initiation of ARSI was significantly associated with poor prognosis for OS.
Recent three phase Ⅲ clinical trials, such as SPARTAN, ARAMIS, and PROSPER, have demonstrated that ARSIs significantly improve OS and MFS in nmCRPC [6,7,8]. The phase Ⅱ IMAAGEN study demonstrated that ABI resulted in a significant ≥50% PSA reduction in nmCRPC [15]. Real-world settings have also shown that ENZ and APA are effective and safe, with nmCRPC patients starting ENZ treatment in Japan experiencing a median time to PSA progression of 27.0 months [16], and an 86% PSA ≥50% reduction reported in nmCRPC patients initiating APA treatment [17].
Recent multi-institutional real-world studies have indicated that ARSI treatment, including ENZ, APA, DARO, and ABI, significantly improves oncological outcomes compared to conventional hormonal treatments for nmCRPC patients [11]. Our single-institutional study also supports the favorable oncological outcomes of novel ARSIs in real-world clinical settings.
A systematic review and network meta-analysis focusing on OS and AEs associated with APA, ENZ, and DARO ranked DARO as the most effective OS benefit related to ADT, followed by ENZ and APA, in that order. DARO also showed the most favorable profile regarding Grade ≥3 AEs [18]. There were no significant differences in PSA-PFS among the four novel ARSIs (APA, ENZ, DARO, ABI) in our cohort. While more patients experienced AEs with APA compared to the other ARSIs, the proportion of severe AEs did not significantly differ among all ARSIs.
A multivariate network meta-analysis suggested that AEs associated with novel ARSI therapy do not significantly differ, except for ENZ being ranked as more toxic regarding hypertension and headache [19]. However, the comparative oncological outcomes and safety profiles among ARSIs for nmCRPC patients remain unclear. Therefore, additional studies involving larger cohorts of nmCRPC patients treated with ARSIs are needed.
Some risk factors affecting metastasis and survival outcomes in nmCRPC patients have been analyzed. Higher PSA concentrations at diagnosis, shorter PSADT, higher Gleason score, a history of primary intervention, and a shorter interval from ADT initiation to the diagnosis of CRPC have all been associated with shorter time to metastasis [20]. Another study found that metastasis was associated with higher PSA levels at diagnosis, nadir PSA after ADT, rapid ALP rise, and shorter PSADT [21]. Shorter bone metastatic–free survival was observed as PSADT decreased below 8 months [22]. Trials like SPARTAN, PROSPER, and ARAMIS used 6 months as a cutoff point for PSADT in subgroup analyses [6,7,8]. However, while PSADT <3 months was associated with the highest risk of metastasis and poorer survival outcomes, the optimal PSADT cutoff for predicting oncological outcomes and risk stratification in nmCRPC patients remains unclear [12].
ALP has also been suggested as a significant prognostic marker for MFS in nmCRPC patients, although these patients were treated with not only ARSIs, but also antineoplastic therapies such as docetaxel and cabazitaxel. Elevated ALP is thought to indicate pre-existing activated micro-metastases [23]. Our study indicated that a baseline PSA ≥3.67 ng/mL at the initiation of first-line ARSI for nmCRPC patients was the strongest predictor of poor OS in multivariate analysis. Previous reports have associated baseline PSA with survival outcomes [5,24,25,26], as PSA levels reflect tumor volume. High baseline PSA and a short PSADT in nmCRPC may be the most important factors to predict progression to metastatic disease and reduced OS [20,22,25,26,27]. Therefore, preventing or delaying metastatic progression using these prognostic biomarkers should be a primary therapeutic goal for treating nmCRPC [28]. To the best of our knowledge, this is the first report to demonstrate that higher baseline PSA levels are associated with poorer survival outcomes in nmCRPC patients treated with ARSIs. Baseline PSA level as a risk factor has been previously reported in nmCRPC patients undergoing ADT therapy.
We acknowledge several limitations in our study. First, it was retrospective with a relatively small cohort from a single institution, potentially introducing bias. The small sample size may have impacted the robustness of the results, especially in comparing efficacy and safety among different ARSI therapies. Moreover, our cohort included patients diagnosed with nmCRPC based on PSA levels ≤2.0 ng/mL at the start of ARSI therapy, despite the conventional definition of CRPC requiring a PSA rise of ≥2.0 ng/mL [15]. In our real-world setting, PSADT took precedence over absolute PSA levels in 31 patients (24%). This inclusion of patients with baseline PSA <2.0 ng/mL might have influenced survival outcomes and prognostic factors. Lastly, we defined nmCRPC using conventional imaging like CT and bone scintigraphy. Whole-body diffusion-weighted MRI (WBMRI) has been reported to have better sensitivity and similar specificity compared to bone scintigraphy completed with targeted x-rays (sensitivity: 98–100% vs. 86%, specificity: 98% vs. 98-100%) for detecting bone metastases [29]. Additionally, another retrospective study indicated that prostate -specific membrane antigen (PSMA)-PET showed positivity in 196 out of 200 patients with nmCRPC, revealing pelvic disease in 44% and metastatic disease in 55% of patients despite negative conventional imaging [30]. This suggests that some nmCRPC patients may have already progressed to metastatic CRPC detectable by PSMA-PET scan or WBMRI. However, the availability of WBMRI remains limited, and PSMA-PET scans have not yet been introduced in Japan. Therefore, external validation will be necessary after the introduction of these new imaging techniques in the future.
Conclusion
ARSI demonstrated favorable efficacy in nmCRPC patients. There were no significant differences in clinical outcomes among different types of ARSI therapy for nmCRPC. High baseline PSA at ARSI initiation was significantly associated with poor prognosis for OS. Given the preliminary nature of our small study, further investigations are necessary.
Author Contributions
Conception and design: RF, SY; administrative support: JY; collection and assembly of data: RF, TY; data analysis and interpretation: RF; manuscript writing: RF. All authors provided final approval of the manuscript.
Funding
None
Institutional review board statement
This study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the institutional ethics committee of the Cancer Institute Hospital, Japanese Foundation for Cancer Research (Ethical IRB number is 2012-1008).
Informed consent statement
Before the initial treatment, all patients provided written informed consent for ARSI therapy.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author. Due to privacy considerations and ethical restrictions, the data are not publicly available as they contain information that could compromise the privacy of research participants.
Conflicts of interest
T. Yuasa received remuneration for a lecture from Ono Pharma (Osaka, Japan) and Bristol-Myers Squibb Japan (Tokyo, Japan). The other authors have declared no conflicts of interest.
References
- Bergengren O; Pekala KR; Matsoukas K; Fainberg J; Mungovan SF; Bratt O; Bray F; Brawley O; Luckenbaugh AN; Mucci L; et al. 2022 update on prostate cancer epidemiology and risk factors-A systematic review. Eur Urol. 2023, Aug;84(2), 191-206. [CrossRef]
- Zumsteg ZS; Spratt DE; Romesser PB; Pei X; Zhang Z; Polkinghorn W; McBride S; Kollmeier M; Yamada Y; Zelefsky MJ. The natural history and predictors of outcome following biochemical relapse in the dose escalation era for prostate cancer patients undergoing definitive external beam radiotherapy. Eur Urol. 2015, Jun;67(6), 1009–1016. [CrossRef]
- Boorjian SA; Thompson RH; Tollefson MK; Rangel LJ; Bergstralh EJ; Blute ML; Karnes RJ. Long-term risk of clinical progression after biochemical recurrence following radical prostatectomy: The impact of time from surgery to recurrence. Eur Urol. 2011, Jun;59(6), 893–899. [CrossRef]
- Kluth LA; Shariat SF; Kratzik C; Tagawa S; Sonpavde G; Rieken M; Scherr DS; Pummer K. The hypothalamic-pituitary-gonadal axis and prostate cancer: Implications for androgen deprivation therapy. World J Urol. 2014, Jun;32(3), 669–676. [CrossRef]
- Aly M; Hashim M; Heeg B; Liwing J; Leval A; Mehra M; Lawson J; Brookman-May SD; Akre O. Time-to-event outcomes in men with nonmetastatic castrate-resistant prostate cancer-A systematic literature review and pooling of individual participant data. Eur Urol Focus. 2019, Sep;5(5), 788–798. [CrossRef]
- Smith MR; Saad F; Chowdhury S; Oudard S; Hadaschik BA; Graff JN; Olmos D; Mainwaring PN; Lee JY; Uemura H; et al. Apalutamide and overall survival in prostate cancer. Eur Urol. 2021, Jan;79(1), 150–158.
- Fizazi K; Shore N; Tammela TL; Ulys A; Vjaters E; Polyakov S; Jievaltas M; Luz M; Alekseev B; Kuss I; et al. ARAMIS Investigators. Nonmetastatic, castration-resistant prostate cancer and survival with darolutamide. N Engl J Med. 2020, Sep 10, 383(11), 1040–1049.
- Sternberg CN; Fizazi K; Saad F; Shore ND; De Giorgi U; Penson DF; Ferreira U; Efstathiou E; Madziarska K; Kolinsky MP; et al. Enzalutamide and survival in nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2020, Jun 4, 382(23), 2197–2206.
- Schaeffer EM; Srinivas S; Adra N; An Y; Barocas D; Bitting R; Bryce A; Chapin B; Cheng HH; D’Amico AV; et al. Prostate Cancer, Version 4.2023, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2023, Oct;21(10), 1067–1096.
- Miyake H; Matsushita Y; Watanabe H; Tamura K; Motoyama D; Ito T; Sugiyama T; Otsuka A. Comparative assessment of prognostic outcomes between first-generation antiandrogens and novel androgen-receptor-axis-targeted agents in patients with non-metastatic castration-resistant prostate cancer. Int J Clin Oncol. 2019, Jul;24(7), 842–847.
- Fujita N; Hatakeyama S; Tabata R; Okita K; Kido K; Hamano I; Tanaka T; Noro D; Tokui N; Suzuki Y; et al. Real-world effects of novel androgen receptor axis-targeted agents on oncological outcomes in non-metastatic castration-resistant prostate cancer: A multi-institutional retrospective study. Prostate Int. 2024, Mar;12(1), 46–51.
- Howard LE; Moreira DM; De Hoedt A; Aronson WJ; Kane CJ; Amling CL; Cooperberg MR; Terris MK; Freedland SJ. Thresholds for PSA doubling time in men with non-metastatic castration-resistant prostate cancer. BJU Int. 2017, Nov;120(5B), E80–E86.
- Scher HI; Morris MJ; Stadler WM; Higano C; Basch E; Fizazi K; Antonarakis ES; Beer TM; Carducci MA; Chi KN; et al. Prostate Cancer Clinical Trials Working Group 3. Trial design and objectives for castration-resistant prostate cancer: Updated recommendations from the Prostate Cancer Clinical Trials Working Group 3. J Clin Oncol. 2016, Apr 20, 34(12), 1402–18.
- Pound CR; Partin AW; Eisenberger MA; Chan DW; Pearson JD; Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA. 1999, May 5, 281(17), 1591–7.
- Ryan CJ; Crawford ED; Shore ND; Underwood W 3rd; Taplin ME; Londhe A; Francis PSJ; Phillips J; McGowan T; Kantoff PW. The IMAAGEN Study: Effect of abiraterone acetate and prednisone on prostate specific antigen and radiographic disease progression in patients with nonmetastatic castration resistant prostate cancer. J Urol. 2018, Aug;200(2), 344–352.
- Yokomizo A; Yonese J; Egawa S; Fukuhara H; Uemura H; Nishimura K; Nagata M; Saito A; Lee T; Yamaguchi S; et al. Correction to: Real-world use of enzalutamide in men with nonmetastatic castration-resistant prostate cancer in Japan. Int J Clin Oncol. 2022, Mar;27(3), 633–634.
- Lowentritt B; Brown G; Pilon D; Ellis L; Germain G; Rossi C; Lefebvre P; Kernen K; Sieber P; Shore N. Real-world prostate-specific antigen response and treatment adherence of apalutamide in patients with non-metastatic castration-resistant prostate cancer. Urology. 2022, Aug;166, 182–188.
- Wenzel M; Nocera L; Collà Ruvolo C; Würnschimmel C; Tian Z; Shariat SF; Saad F; Tilki D; Graefen M; Kluth LA; et al. Overall survival and adverse events after treatment with darolutamide vs. apalutamide vs. enzalutamide for high-risk non-metastatic castration-resistant prostate cancer: A systematic review and network meta-analysis. Prostate Cancer Prostatic Dis. 2022, Feb;25(2), 139–148.
- Cao B; Kim M; Reizine NM; Moreira DM. Adverse events and androgen receptor signaling inhibitors in the treatment of prostate cancer: A systematic review and multivariate network meta-analysis. Eur Urol Oncol. 2023, Jun;6(3), 237–250.
- Moreira DM; Howard LE; Sourbeer KN; Amarasekara HS; Chow LC; Cockrell DC; Hanyok BT; Aronson WJ; Kane CJ; Terris MK; et al. Predictors of time to metastasis in castration-resistant prostate cancer. Urology. 2016, Oct;96, 171–176.
- Metwalli AR; Rosner IL; Cullen J; Chen Y; Brand T; Brassell SA; Lesperance J; Porter C; Sterbis J; McLeod DG. Elevated alkaline phosphatase velocity strongly predicts overall survival and the risk of bone metastases in castrate-resistant prostate cancer. Urol Oncol. 2014, Aug;32(6), 761–768.
- Smith MR; Saad F; Oudard S; Shore N; Fizazi K; Sieber P; Tombal B; Damiao R; Marx G; Miller K; et al. Denosumab and bone metastasis-free survival in men with nonmetastatic castration-resistant prostate cancer: Exploratory analyses by baseline prostate-specific antigen doubling time. J Clin Oncol. 2013, Oct 20, 31(30), 3800–3806.
- Mori K; Kimura T; Fukuokaya W; Iwatani K; Sakanaka K; Kurokawa G; Yanagisawa T; Sasaki H; Miki J; Shimomura T; et al. Values of alkaline phosphatase at the diagnosis of castration resistance and response to primary androgen deprivation therapy as predictors of subsequent metastasis in non-metastatic castration-resistant prostate cancer. Int J Clin Oncol. 2020, Mar;25(3), 479–485.
- Madan RA; Gulley JL; Schlom J; Steinberg SM; Liewehr DJ; Dahut WL; Arlen PM. Analysis of overall survival in patients with nonmetastatic castration-resistant prostate cancer treated with vaccine, nilutamide, and combination therapy. Clin Cancer Res. 2008, Jul 15, 14(14), 4526–4531.
- Smith MR; Cook R; Lee KA; Nelson JB. Disease and host characteristics as predictors of time to first bone metastasis and death in men with progressive castration-resistant nonmetastatic prostate cancer. Cancer. 2011, May 15, 117(10), 2077–2085.
- Smith MR; Kabbinavar F; Saad F; Hussain A; Gittelman MC; Bilhartz DL; Wynne C; Murray R; Zinner NR; Schulman C; et al. Natural history of rising serum prostate-specific antigen in men with castrate nonmetastatic prostate cancer. J Clin Oncol. 2005, May 1, 23(13), 2918–2925.
- Nørgaard M; Jensen AØ; Jacobsen JB; Cetin K; Fryzek JP; Sørensen HT. Skeletal related events, bone metastasis and survival of prostate cancer: A population based cohort study in Denmark (1999 to 2007). J Urol. 2010, Jul;184(1), 162–167.
- Scher HI; Solo K; Valant J; Todd MB; Mehra M. Prevalence of prostate cancer clinical states and mortality in the United States: Estimates using a dynamic progression model. PLoS One. 2015, Oct 13, 10(10), e0139440.
- Lecouvet FE; El Mouedden J; Collette L; Coche E; Danse E; Jamar F; Machiels JP; Vande Berg B; Omoumi P; Tombal B. Can whole-body magnetic resonance imaging with diffusion-weighted imaging replace Tc 99m bone scanning and computed tomography for single-step detection of metastases in patients with high-risk prostate cancer? Eur Urol. 2012, Jul;62(1), 68–75.
- Fendler WP; Weber M; Iravani A; Hofman MS; Calais J; Czernin J; Ilhan H; Saad F; Small EJ; Smith MR; et al. Prostate-specific membrane antigen ligand positron emission tomography in men with nonmetastatic castration-resistant prostate cancer. Clin Cancer Res. 2019, Dec 15, 25(24), 7448–7454.
Figure 1.
PSA-PFS curve of ARSI for all patients with nmCRPC (n = 127).
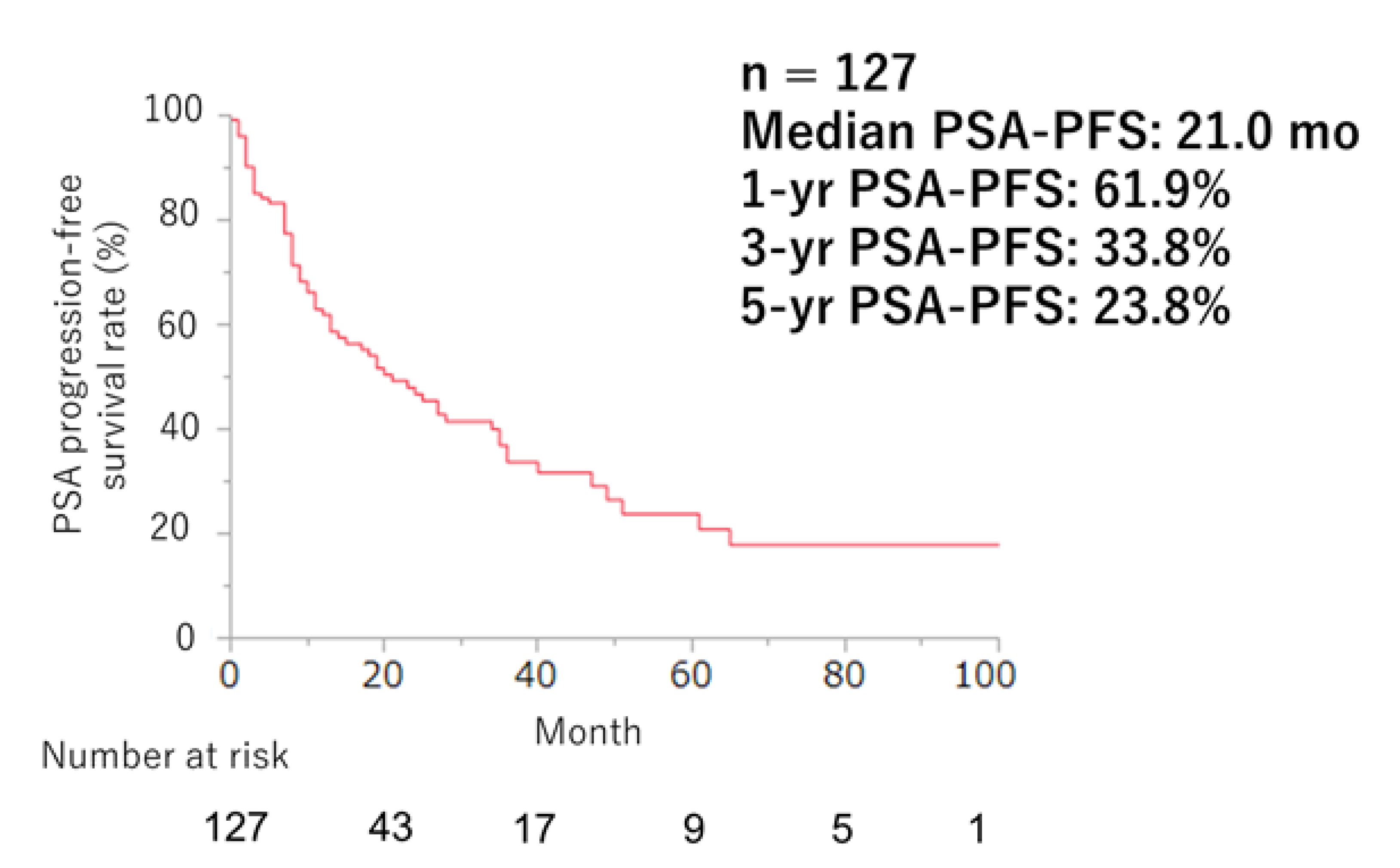
Figure 2.
Waterfall plots of the PSA response to ARSI (yellow: ENZ [n = 72], red: ABI [n = 26], green: APA [n = 12], blue: DARO [n = 17]) .
Figure 2.
Waterfall plots of the PSA response to ARSI (yellow: ENZ [n = 72], red: ABI [n = 26], green: APA [n = 12], blue: DARO [n = 17]) .
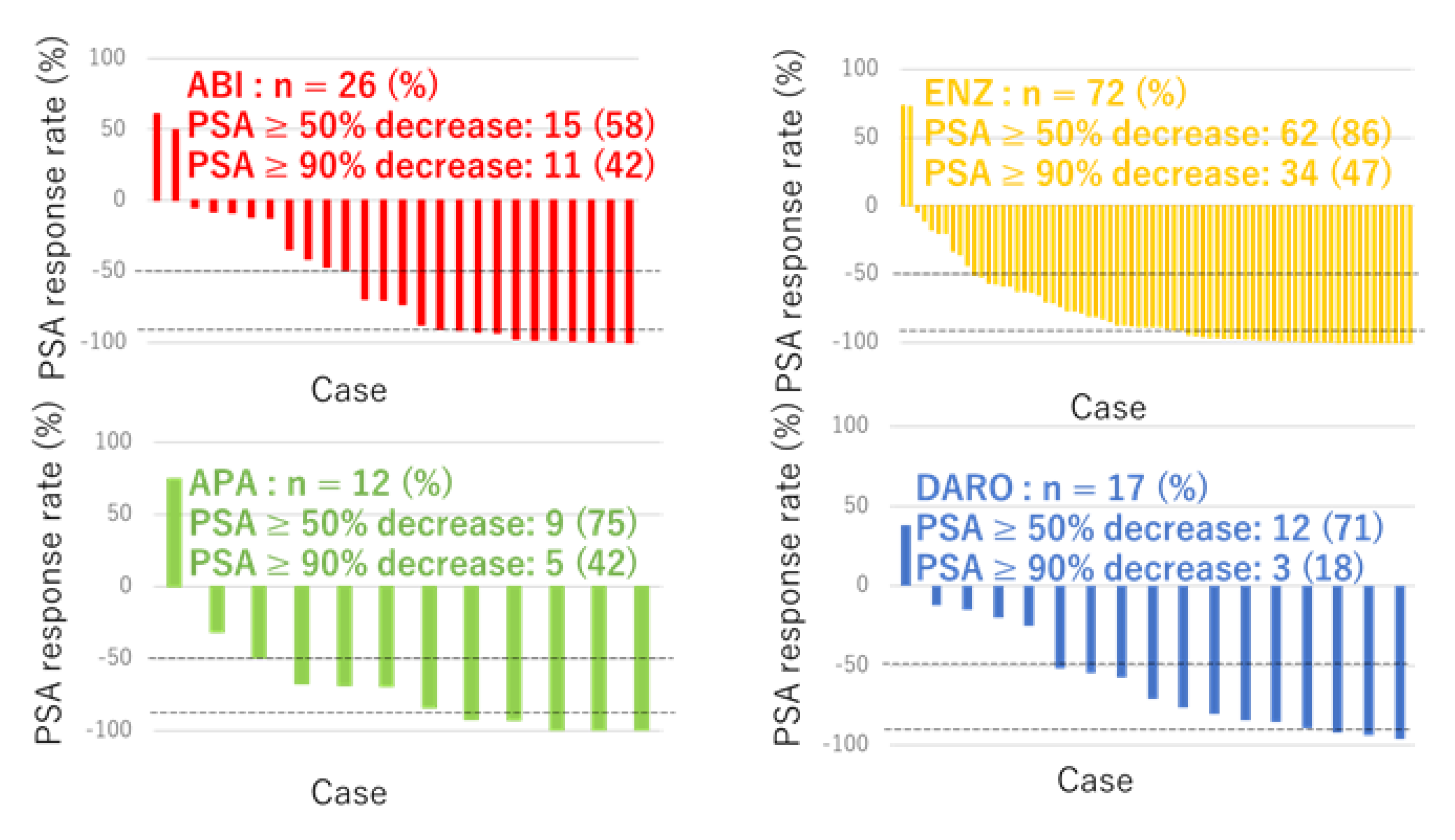
Figure 3.
PSA-PFS curve in nmCRPC patients divided by type of ARSI (yellow: ENZ [n = 72], red: ABI [n = 26], green: APA [n = 12], blue: DARO [n = 17]).
Figure 3.
PSA-PFS curve in nmCRPC patients divided by type of ARSI (yellow: ENZ [n = 72], red: ABI [n = 26], green: APA [n = 12], blue: DARO [n = 17]).
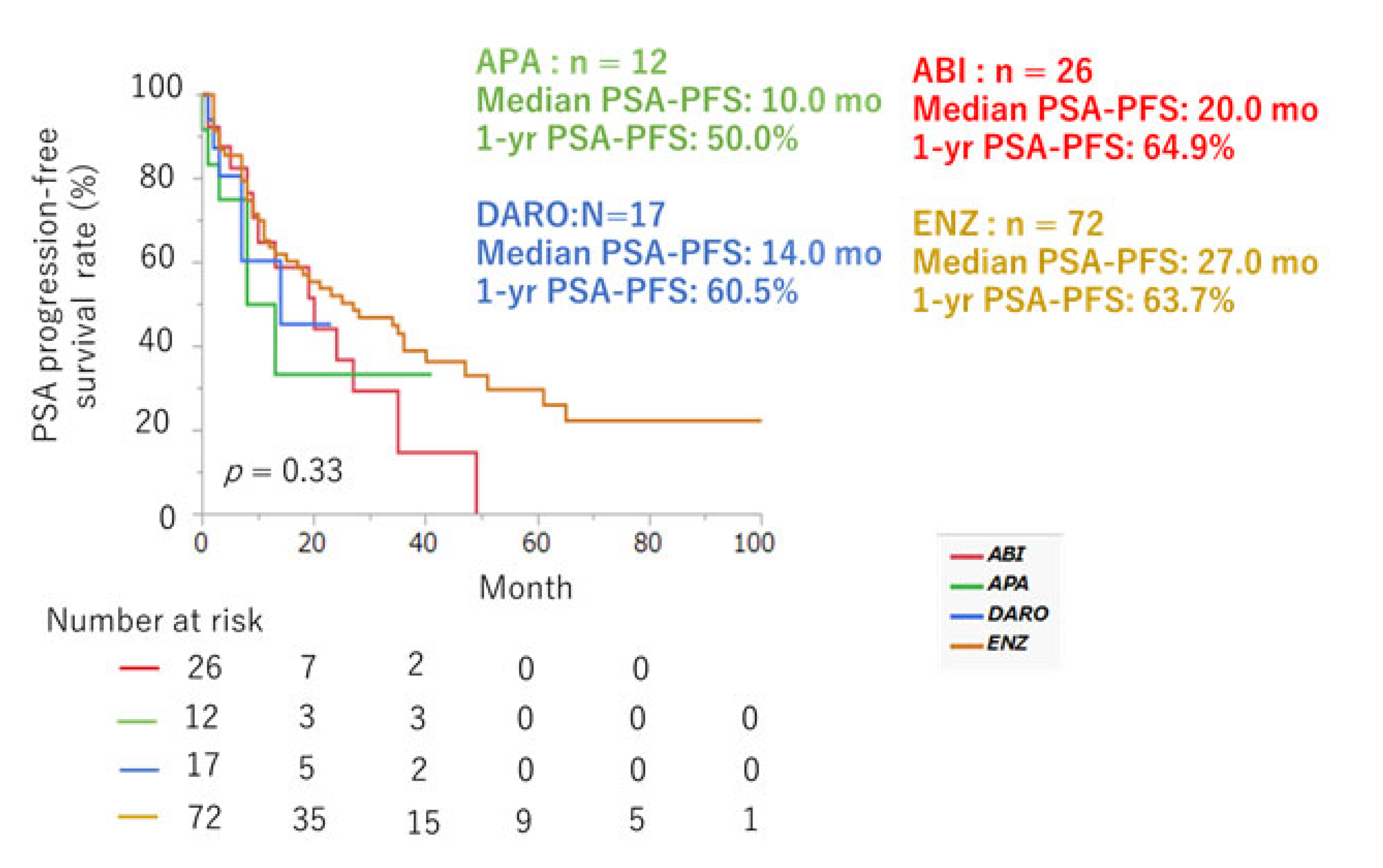
Figure 4.
MFS curve of ARSI for all nmCRPC patients (n=127).
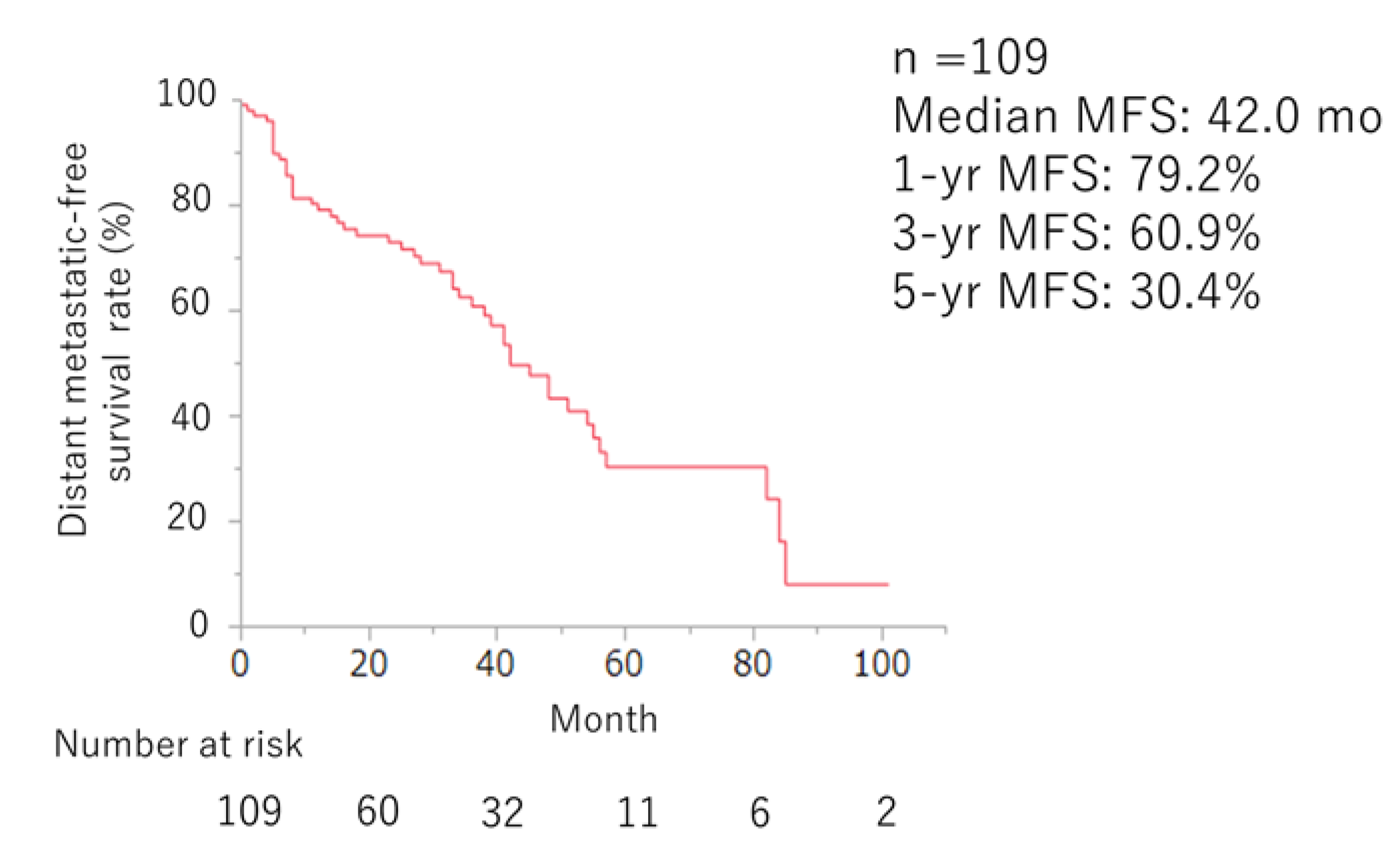
Figure 5.
OS curve of ARSI for all nmCRPC patients (n=127).
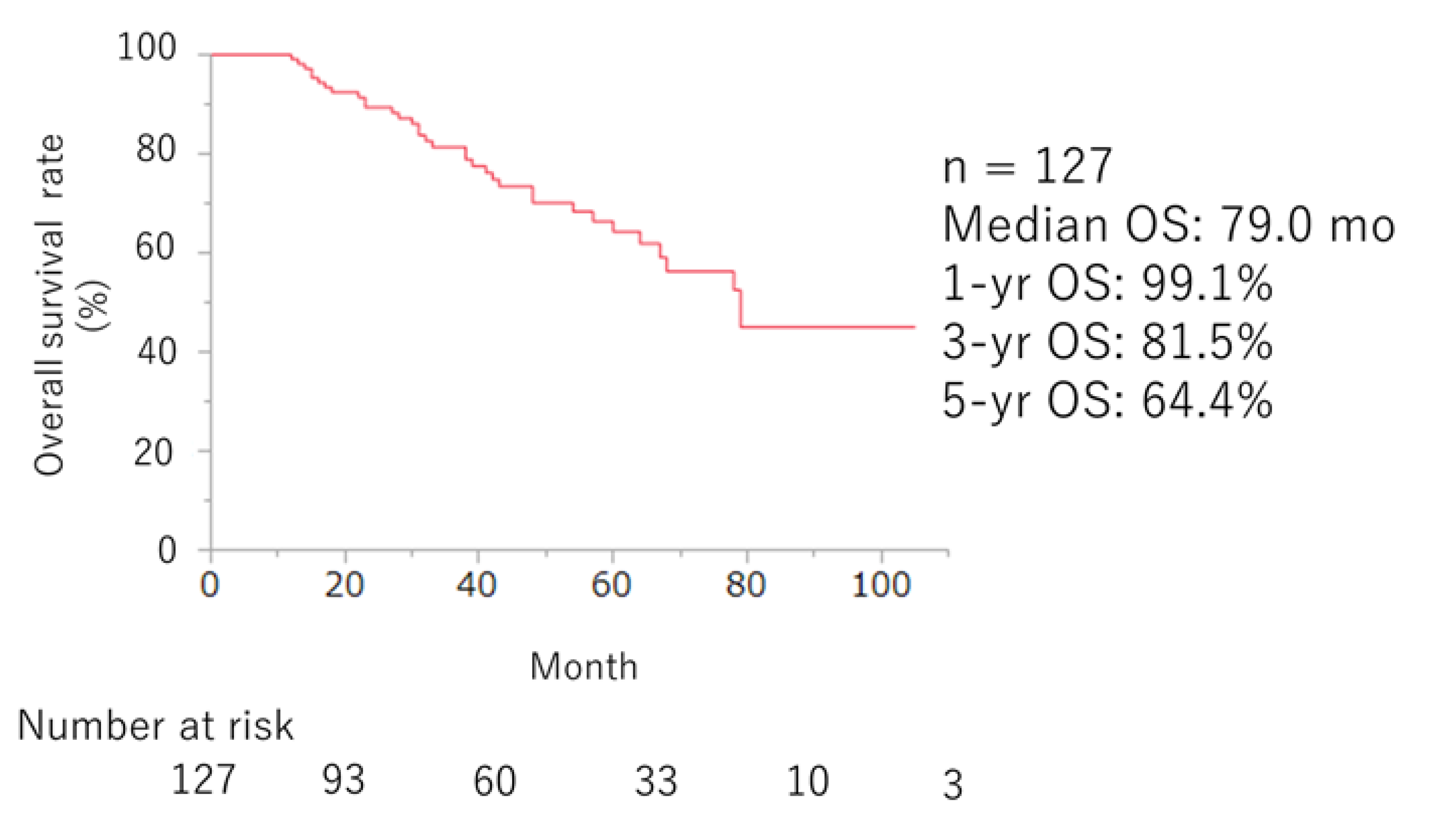
Figure 6.
OS curves divided by baseline PSA at initiation of ARSI ≥3.67 (n = 64) and <3.67 (n = 63) ng/mL (p = 0.002).
Figure 6.
OS curves divided by baseline PSA at initiation of ARSI ≥3.67 (n = 64) and <3.67 (n = 63) ng/mL (p = 0.002).
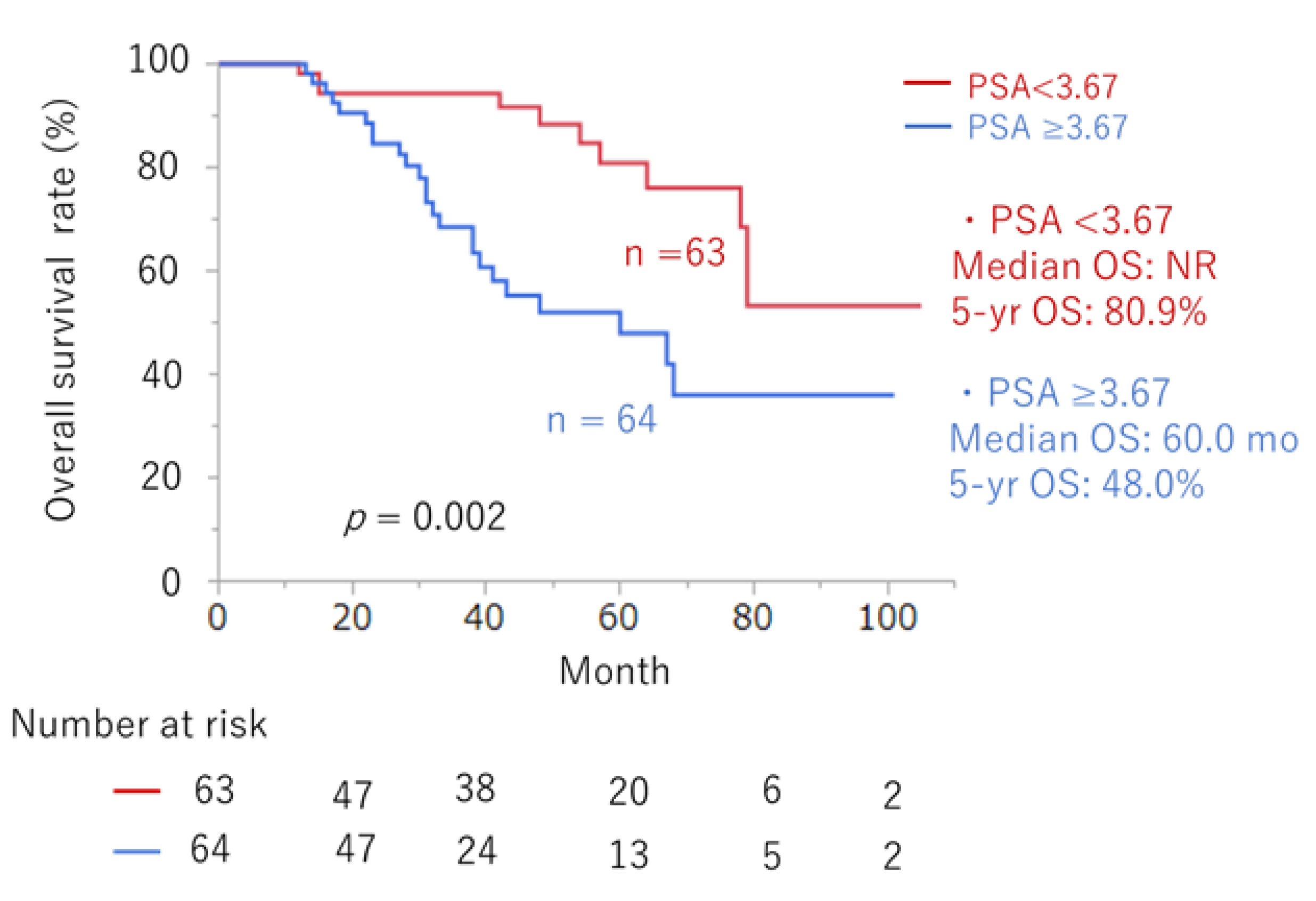

Table 1.
Patient characteristics (n = 127).
| Clinical factors | Number | |
| Median age at the time of CRPC, years (IQR) | 76 (70–81) | |
| Median initial PSA, ng/mL (IQR) | 17 (10-59) | |
| Gleason Score (%) | <8 | 40 (31) |
| ≥8 | 87 (69) | |
| Clinical T Stage | 1-2 | 44 (35) |
| 3-4 | 82 (65) | |
| Unknown | 1 (1) | |
| Clinical N Stage | 0 | 103 (81) |
| 1 | 24 (19) | |
| Local therapy (%) | Surgery | 57 (45) |
| Radiation | 46 (36) | |
| No local treatment | 24 (19) | |
| Previous docetaxel therapy (%) | Yes | 6 (5) |
| No | 121 (95) | |
| PSA doubling time, month (%) | <6 | 99 (78) |
| ≥6 | 27 (21) | |
| Unknown | 1 (1) | |
| First-line ARAT agent (%) | Darolutamide | 17 (13) |
| Apalutamide | 12 (10) | |
| Abiraterone | 26 (20) | |
| Enzalutamide | 72 (57) |
CRPC: castration-resistant prostate cancer, IQR: interquartile range, PSA: prostate-specific antigen, ARAT: androgen receptor-axis-targeted.
Table 2.
Adverse events for each ARSI agent (n = 127).
| ENZ (n = 72) | ABI (n = 26) | APA (n = 12) | DARO (n = 17) | |||||
| Any grade (%) | ≥ Grade 3 (%) | Any grade (%) | ≥ Grade 3 (%) | Any grade (%) | ≥ Grade 3 (%) | Any grade (%) | ≥ Grade 3 (%) | |
| Rash | 1 (1) | 0 | 0 | 0 | 6 (50) | 1 (4) | 0 | 0 |
| Neuropathy | 2 (3) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Fatigue | 11 (15) | 1 (2) | 2 (8) | 2 (17) | 0 | 2 (12) | 1 (6) | |
| Decreased appetite | 4 (6) | 0 | 0 | 0 | 0 | 0 | 0 | |
| Nausea | 1 (1) | 0 | 0 | 1 (8) | 0 | 0 | 0 | |
| Dysesthesia | 2 (3) | 0 | 0 | 1 (8) | 0 | 0 | 0 | |
| Dysgeusia | 1 (1) | 1 (4) | 1 (8) | 0 | 0 | 0 | ||
| Edema | 1 (1) | 1 (4) | 0 | 0 | 0 | 0 | ||
| Dizziness | 2 (3) | 0 | 0 | 0 | 0 | 0 | 0 | |
| Neutropenia | 1 (1) | 0 | 0 | 0 | 0 | 0 | 0 | |
| Hepatic dysfunction | 0 | 0 | 2 (8) | 0 | 0 | 1 (6) | 0 | |
| Hypokalemia | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Hypertension | 0 | 0 | 1 (4) | 1 (4) | 0 | 0 | 0 | 0 |
CRPC: castration-resistant prostate cancer, IQR: interquartile range, PSA: prostate-specific antigen, ARAT: androgen receptor-axis-targeted.
Table 3.
Predictors of overall survival in nmCRPC patients treated with ARSI therapy.
| Variables | Univariate | Multivariate | |||
| HR (95% CI) | p value | HR (95% CI) | p value | ||
| Gleason pattern 5 at biopsy | Yes vs. No | 1.75 (0.89, 3.56) | 0.107 | ||
| LDH (U/l) at first-line ARSI | ≥192 vs. <192 | 1.58 (0.79, 3.31) | 0.200 | ||
| ALP (U/l) at first-line ARSI | ≥271 vs. <271 | 1.87 (0.89, 3.75) | 0.097 | NS | |
| Time to CRPC (months) | ≤54 vs. >54 | 1.78 (0.82, 4.43) | 0.172 | ||
| PSA (ng/mL) at initiation of ARSI | >3.67 vs. ≤3.67 | 2.93 (1.46, 6.26) | 0.002 | 2.93 (1.46, 6.26) | 0.002 |
| Previous Docetaxel chemotherapy | Yes vs. No | 1.15 (0.28, 3.24) | 0.817 | ||
| Presence of regional lymph node | Yes vs. No | 2.31 (0.59, 8.15) | 0.215 | ||
| Treatment | 0.084 | NS | |||
| Surgery vs. CAB | 0.47 (0.19, 1.22) | 0.118 | |||
| Radiation vs. CAB | 1.04 (0.46, 2.59) | 0.914 | |||
| Surgery vs. Radiation | 2.22 (1.04, 4.92) | 0.040 | |||
| PSA-DT | ≤6 mo vs. >6 mo | 1.64 (0.59, 6.82) | 0.383 | ||
ALP: alkaline phosphatase; ARAT: androgen receptor-axis-targeted; CAB: complete androgen blockade; CI: confidence interval; CRPC: castration-resistant prostate cancer; HR: hazard ratio; LDH: lactate dehydrogenase; mo: month; NS: not significant; PSA: prostate-specific antigen.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



