
Submitted:
03 July 2024
Posted:
04 July 2024
Read the latest preprint version here
Abstract
Dengue fever, caused by the dengue virus (DENV), presents a significant global health challenge, especially in tropical and subtropical regions. In 2024, dengue cases in Brazil are four times higher than in 2023, with a significant increase in deaths. This serves as a warning for potential new dengue outbreaks in non-tropical areas. Herein, we explored various aspects of DENV transmission, clinical manifestations, epidemiological trends, and management strategies. DENV transmission involves Aedes mosquitoes as vectors and humans as a host, influenced by temperature, humidity, and precipitation, exacerbated by climate change. Clinical manifestations range from asymptomatic to severe forms such as dengue hemorrhagic fever and dengue shock syndrome, affected by viral serotype and host factors. Common symptoms of dengue include strong headache, body and joint pain, prostration, weakness, pain behind the eyes, rash, and itchy skin. In some cases, especially in children, dengue may initially present with intense diarrhea and vomiting before progressing to more characteristic symptoms. Even patients with mild dengue fever often experience symptoms, particularly weakness, that hinder their ability to perform daily activities. These symptoms can persist for at least one week. We approached several diagnoses that combine clinical symptoms with serological and molecular tests. Prevention strategies implemented in Brazil include vector control, community engagement, and vaccination programs are described and shown to be insufficient to prevent the outbreak in 2024. Climate change drives the geographical expansion of dengue-endemic areas, with recent outbreaks in Europe highlighting the evolving epidemiological landscape. Vigilant and global collaborative efforts are crucial to decrease dengue's impact worldwide.
Keywords:
dengue
; outbreak
; vaccines
; pandemic
; epidemiology
Introduction
Dengue is a viral disease transmitted by arthropods, making it an arboviral and zoonotic disease [1]. Arboviruses, which include a diverse range of viruses, follow a transmission cycle involving arthropod vectors and vertebrate hosts [2]. These vectors include mosquitoes, ticks, sand flies, and biting midges [3,4]. The virus families that encompass arboviruses are Flaviviridae (genus Flavivirus), Bunyaviridae (genera Nairovirus, Orthobunyavirus, Phlebovirus, and Tospovirus), Togaviridae (genus Alphavirus), Rhabdoviridae (genus Vesiculovirus), Orthomyxoviridae (genus Thogotovirus), and Reoviridae (genera Orbivirus and Coltivirus) [5,6]. Among these, the most significant viruses causing diseases in humans and animals belong to the Togaviridae and Flaviviridae families [5,7].
Flaviviruses are a group of enveloped, (+)ssRNA viruses [8,9] that includes dengue virus (DENV), japanese encephalitis virus (JEV), west nile virus (WNV), zika virus (ZIKV), yellow fever virus (YFV), and tick-borne encephalitis virus (TBEV) [8]. Other virus present in the Americas are chikungunya virus (CHIKV) and mayaro virus (MAYV) that have (+)ssRNA, which belong to the Alphavirus genus of the Togaviridae family [10,11]. Another virus of concern is the Oropouche virus (OROV), a segmented (-)ssRNA virus belonging to the genus Orthobunyavirus in the Peribunyaviridae family, which causes symptoms similar to dengue fever [11,12].
Dengue is an endemic disease prevalent in over 100 countries worldwide, particularly in tropical and subtropical regions of Southeast Asia, Africa, the West Pacific, and the Americas [13,14], where temperature and humidity conditions favor the proliferation of mosquito vectors [15,16]. Additionally, cases of the disease have been observed in some regions of Europe and the United States of America [14]. It is believed that climate change and population growth will increase the incidence of dengue, especially in areas where the disease is already endemic [17,18,19]. In particular, in Brazil, dengue epidemics are intensified by temperature variations and rainy periods. Most cases of dengue fever occur after humid and hot periods, particularly in urban areas. High temperatures (26 ºC to 29 ºC) significantly influence the spread of dengue by affecting mosquito development rates, reproduction, survival, biting rates, and viral replication within the vector [20].
The dengue virus has four distinct serotypes, each exhibiting genetic diversity [21]. These serotypes are classified into various genotypes based on samples collected from different geographic regions: (1) DENV-1 includes I, II, III, and IV genotypes; (2) DENV-2 is categorized into Asian genotype I, Asian genotype II, Cosmopolitan genotype, American genotype V, and Sylvatic genotype; (3) DENV-3 comprises I, II, III, and IV genotypes; (4) DENV-4 encompasses I, II, III, and IV genotypes [22]. Recently, a fifth serotype, DENV-5, was identified in Malaysia [23,24]. Human infection occurs through the bite of a female mosquito, particularly A. aegypti [25,26] or A. albopictus [27], affecting approximately 390 million people annually. While A. aegypti is commonly associated with most infections, the geographic range of A. albopictus is steadily expanding. This species is more tolerant of cold weather (ecological plasticity), exhibits competitive feeding behavior, and lacks effective control strategies, all of which contribute to the rising number of dengue cases in colder regions [28,29,30].
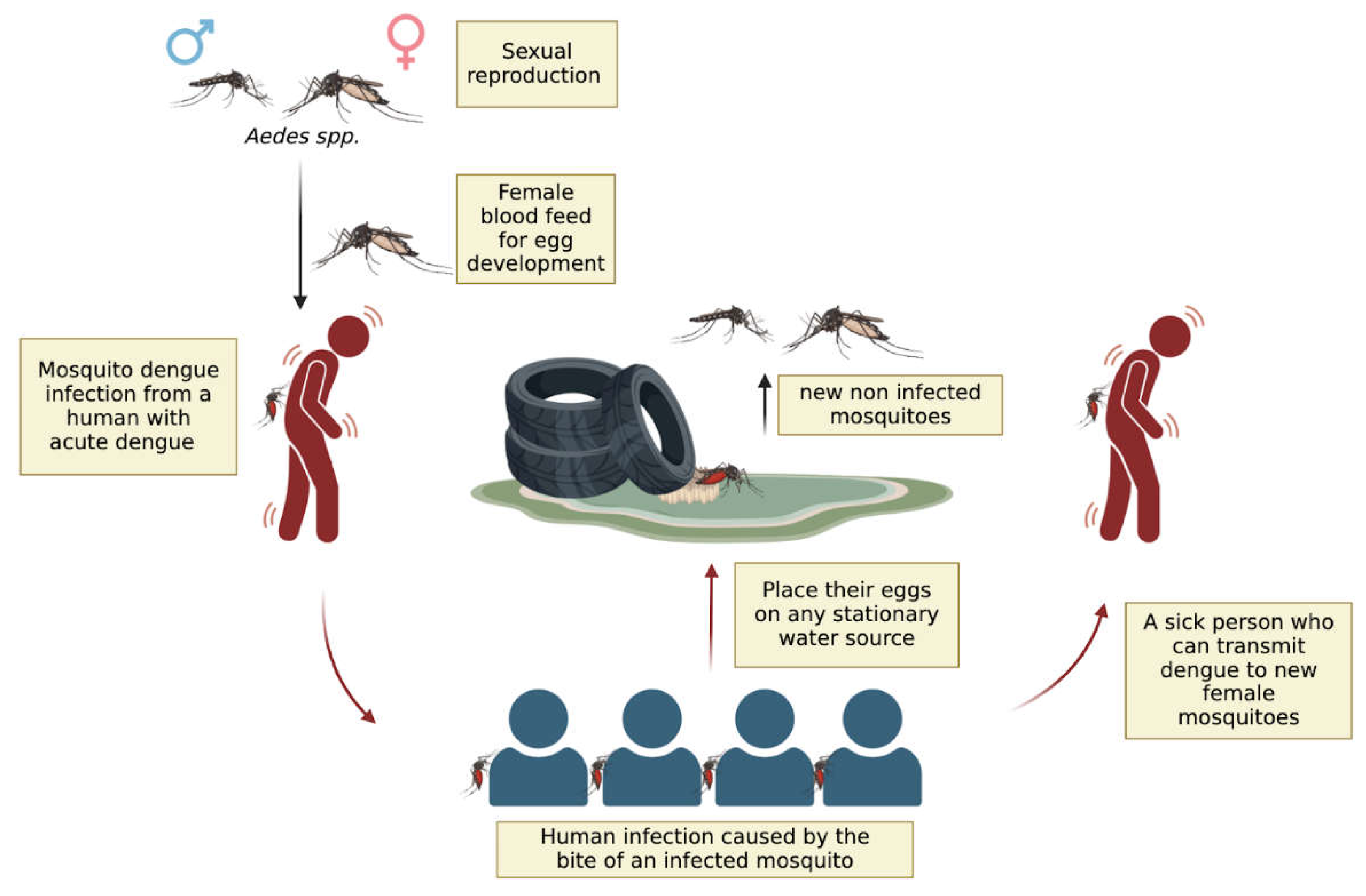
When a person infected with dengue virus (DENV) is bitten by an A. aegypti or A. albopictus, a complex sequence of events allows the virus to replicate and spread within the mosquito [27,31] (Figure 1). Inside the female mosquito, the virus infects the midgut epithelial cells, where it binds to specific receptors and replicates [32]. After replication, the virus escapes from the midgut, spreads through the haemocoel, and infects various secondary tissues, including the fat body, nervous system, and salivary glands. Infection of the salivary glands is crucial for the virus’s transmission to new hosts [33,34,35]. When the mosquito bites another person, DENV is transmitted through the saliva injected during blood feeding, introducing the virus into the new host's bloodstream and initiating infection [33]. This entire process, from ingestion of the virus to the ability to transmit it to a new host, takes approximately 8-12 days, depending on environmental factors such as temperature and humidity [31,33]. This period is known as the extrinsic incubation period [15]. Understanding these steps is crucial for developing strategies to interrupt the transmission cycle of DENV and reduce the incidence of dengue. To date, there is no evidence of human-to-human arboviral disease virus transmission
Figure 1.
Reproduction cycle of Aedes spp. and dengue transmission cycle. The reproduction cycle of Aedes spp. mosquitoes and the dengue transmission cycle involve several stages. Male and female mosquitoes mate, and female mosquitoes go for blood feeding for egg development. A female mosquito then bites an infected individual, acquiring the dengue virus. This infected mosquito subsequently bites multiple healthy individuals, transmitting the virus to them. These newly infected individuals then transmit the virus to additional mosquitoes that bite them. The female mosquito lays her eggs in stagnant water sources, where the eggs hatch into larvae and develop into new mosquitoes, perpetuating the cycle.
Figure 1.
Reproduction cycle of Aedes spp. and dengue transmission cycle. The reproduction cycle of Aedes spp. mosquitoes and the dengue transmission cycle involve several stages. Male and female mosquitoes mate, and female mosquitoes go for blood feeding for egg development. A female mosquito then bites an infected individual, acquiring the dengue virus. This infected mosquito subsequently bites multiple healthy individuals, transmitting the virus to them. These newly infected individuals then transmit the virus to additional mosquitoes that bite them. The female mosquito lays her eggs in stagnant water sources, where the eggs hatch into larvae and develop into new mosquitoes, perpetuating the cycle.
Once inside the human host, the dengue virus targets various cells and tissues, including macrophages, lymphocytes, lymph nodes, peripheral blood, lungs, liver, kidneys, stomach, endothelial cells, hepatocytes, and central nervous system cells (Figure 4) [36]. Dengue infection progresses through three phases: the febrile phase, the critical phase, and the recovery phase [37]. The febrile phase of dengue lasts about a week and is characterized by high fever, severe headache, muscle and joint pain, prostration, eye pain, fatigue, nausea, vomiting, loss of appetite, and sometimes minor bleeding [38,39]. In some cases, particularly in children, dengue may initially present with intense diarrhea and vomiting before progressing to more characteristic symptoms. Even patients with mild dengue often experience symptoms, especially fatigue, that hinder their ability to perform daily activities for at least one week. The critical phase involves more severe symptoms such as plasma leakage and internal hemorrhage [2]. The recovery phase is marked by the gradual reabsorption of fluid from the extravascular compartment, improvement in general well-being, return of appetite, and stabilization of the haemodynamic state [2]. Additionally, neurological complications such as encephalopathy, myelopathy, myositis, and peripheral neuropathy are frequently identified following dengue infection [40].
Herein, we discussed dengue fever, caused by the DENV, as an increasingly significant global health challenge in tropical and subtropical regions. In particular, the explosion of cases in Latin America in 2024 is impressive, with more than 4 times higher than in 2023. We explored various aspects, including its transmission by Aedes mosquitoes, which is influenced by climate factors such as temperature and precipitation due to climate change. Clinical manifestations range widely from asymptomatic cases to severe forms such as dengue hemorrhagic fever and shock syndrome, influenced by factors such as viral serotype and host immunity. We emphasized the diagnostic approaches based on clinical symptoms and laboratory tests. Prevention efforts include strategies as vector control, community engagement, and vaccination campaigns, although challenges such as insecticide resistance persist. Lastly, we discussed the spread of dengue into new regions like Europe, highlighting the evolving epidemiological landscape and the necessity for global collaboration to implement effective mitigation strategies.
The Impact of Global Warming on Dengue Outbreaks in the Americas
As global warming becomes more evident with the increasing frequency of climate disasters, one significant impact is the intensification of rainfall [41]. The Brazilian National Institute for Space Research (INPE) reports that in 2024, the southern part of Brazil will experience up to a 30% increase in average annual rainfall compared to the last three decades [42]. This increase in rainfall will lead to more standing water in urban areas, which are the primary habitats for the main vectors of dengue [43]. The proliferation of Aedes mosquitoes is directly related to precipitation, humidity, and high temperatures, with Latin America providing an ideal environment. Global warming leads to higher temperatures in subtropical and temperate areas, which often have high urban population densities, creating ideal conditions for proliferation of mosquitoes. These observations suggest that global warming and climate change are directly influencing the spread of tropical diseases. In developing countries, which are experiencing an increase in natural disasters such as floods, tsunamis, and storms, these events exacerbate the formation of standing water in large urban areas. This, in turn, facilitates the spread of dengue and other mosquito-borne diseases.
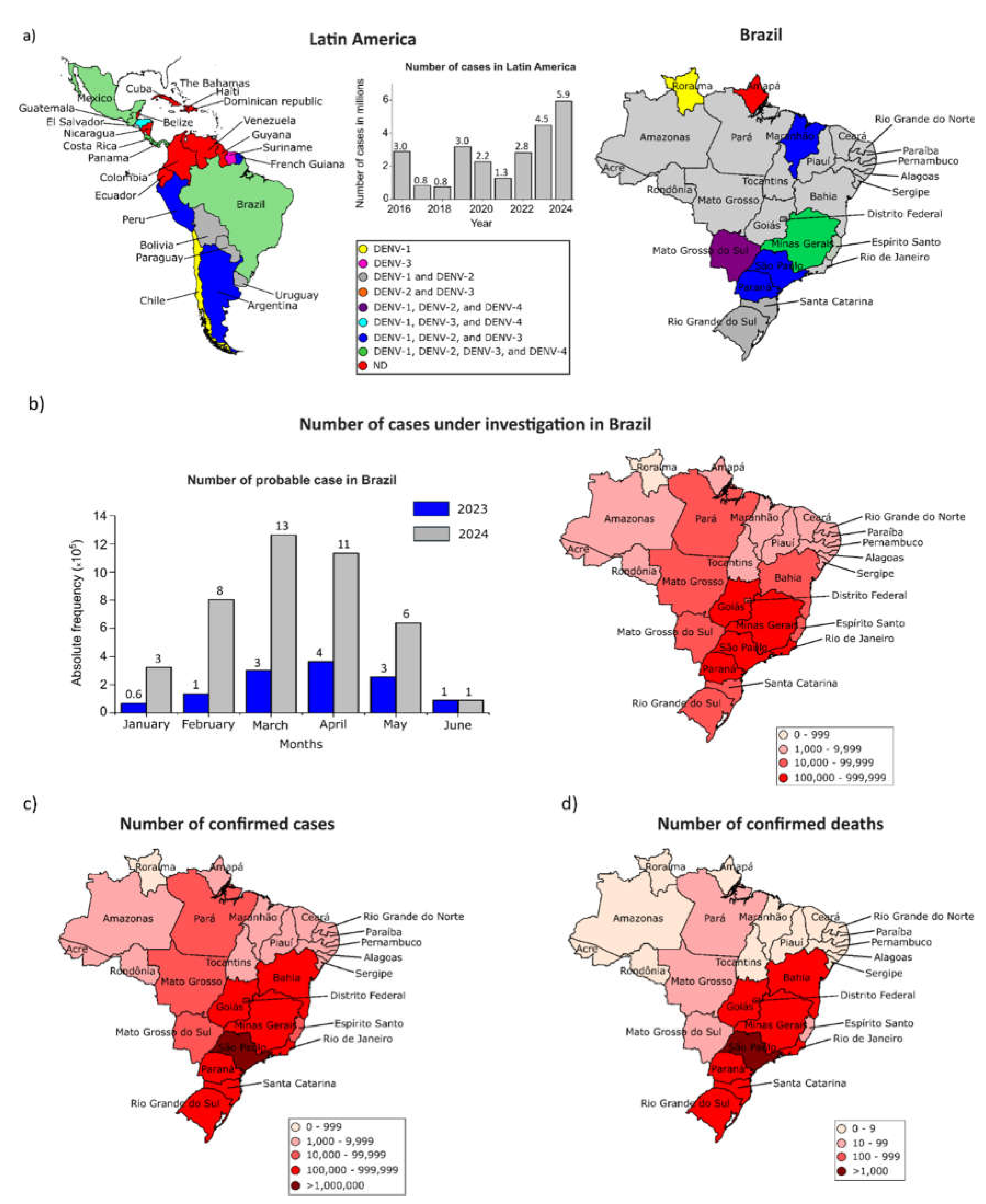
The number of dengue cases in Latin America has been increasing since 2021, reaching ~6 million cases in 2024 (Figure 2a). The four DENV serotypes have been detected in Latin America, with serotypes DENV1 and DENV-2 mainly found in Brazil, with the exception of Minas Gerais that has the four serotypes circulating. In March of 2024 the number of DENV cases under investigation in Brazil was four times higher than 2023, with higher cases and deaths in the southeast and south regions (Figure 2 b-d). The cases of DENV may be underestimated due to economic factors and limited diagnostic tests, especially in the north and northeast regions of Brazil. Until June 18, 2024, Brazil had reported a total of 4.2 million confirmed dengue cases and 3,900 deaths [44]. Additionally, 1.8 million dengue cases and over 2,000 deaths are still under investigation [44]. With the onset of autumn and winter, we expect a decrease in dengue cases in Brazil, as the cooler temperatures are less favorable to mosquito reproduction. However, continued vigilance and preventive measures remain crucial to controlling the spread of dengue.
Figure 2.
Geographic distribution of serotypes in different regions of the Americas and Brazil, 2024. a) Distribution of the serotypes by country in Latin America Latin America and the Caribbean from 2016 to April 2024 [45] and 2024 in Brazil [44]. Twenty-five countries and territories reported the circulation of dengue serotypes in the Americas. Brazil, Costa Rica, Guatemala, Honduras, Mexico, and Panama reported the simultaneous circulation of DENV-1, DENV-2, DENV-3, and DENV-4[46]. Minas Gerais reported the simultaneous circulation of DENV-1, DENV-2, DENV-3, and DENV-4 [47]. b) Number of dengue cases under investigation in Brazil [44]. c) Number of confirmed cases in Brazil [44]. d) Number of deaths caused by dengue in Brazil [44]. ND = Not divulged.
Figure 2.
Geographic distribution of serotypes in different regions of the Americas and Brazil, 2024. a) Distribution of the serotypes by country in Latin America Latin America and the Caribbean from 2016 to April 2024 [45] and 2024 in Brazil [44]. Twenty-five countries and territories reported the circulation of dengue serotypes in the Americas. Brazil, Costa Rica, Guatemala, Honduras, Mexico, and Panama reported the simultaneous circulation of DENV-1, DENV-2, DENV-3, and DENV-4[46]. Minas Gerais reported the simultaneous circulation of DENV-1, DENV-2, DENV-3, and DENV-4 [47]. b) Number of dengue cases under investigation in Brazil [44]. c) Number of confirmed cases in Brazil [44]. d) Number of deaths caused by dengue in Brazil [44]. ND = Not divulged.
Dengue Symptoms and Determinants for Recurrence and Disease Severity
Patients infected with dengue are asymptomatic or exhibit a range of symptoms from mild to severe, which can sometimes progress to fatal outcomes [48,49]. Dengue is considered an acute, systemic, dynamic, debilitating, and self-limiting febrile illness. While most patients recover, some can progress to severe forms and even death. Nearly all dengue-related deaths are preventable, often depending on the quality of healthcare provided [50]. Anyone presenting with a sudden onset of fever (39°C to 40°C) accompanied by at least two of the following symptoms such as strong headache, prostration, muscle and/or joint pain, and pain behind the eyes, should seek medical attention immediately to receive timely treatment [50]. However, vigilance is necessary after the febrile period. As the fever subsides (between the 3rd and 7th day of illness), warning signs may appear, indicating a potential deterioration of the patient's condition. These signs, which suggest plasma leakage from blood vessels and/or hemorrhaging, that may include severe and continuous abdominal pain, persistent vomiting, fluid accumulation in body cavities (ascites, pleural effusion, pericardial effusion), postural hypotension and/or fainting, lethargy and/or irritability, enlarged liver (hepatomegaly) > 2cm, mucosal bleeding and progressive increase in hematocrit [50]. After the critical phase of dengue, the patient enters the recovery phase. However, the disease can still progress to severe forms, characterized by significant plasma leakage, severe hemorrhages, or severe organ impairment, potentially leading to death [50]. Dengue in children can begin with severe abdominal pain, accompanied by diarrhea and vomiting, before progressing to the classic symptoms of dengue. The warning signs of dengue in infants and childrens may not be as evident, increasing the risk of severe illness. All age groups are equally susceptible to dengue. However, individuals with preexisting conditions, pregnant women, infants, young children (up to 2 years old), and people over 65 years old are at higher risk of developing complications [50].
Common symptoms for all dengue serotypes include abdominal pain, drowsiness, and bleeding mucous membranes (Figure 3) [51]. However, the presence and severity of other symptoms may vary depending on the serotype involved in the infection. While all serotypes may induce severe reactions, DENV-2 is particularly noted for its higher virulence and association with more severe disease manifestations [52].
Additionally, factors such as age, genetic variability, and alterations in the patient's immune response are significant indicators of potential disease severity [53]. Studies have demonstrated that elderly patients often require longer hospital stays and have a higher likelihood of developing severe dengue due to preexisting comorbidities and infections with specific serotypes [54,55]. Adults are at increased risk of developing dengue hemorrhagic fever, while children and teenagers are particularly susceptible to severe plasma leakage and shock [56]. These severe manifestations are associated to the elevated expression of chemokines and pro-inflammatory cytokines such as CCL-2, CCL-5, TNF-α, IFN-γ, and IL-6, which act on endothelial cells to promote plasma extravasation and the escape of pro-inflammatory factors [53,57].
Another critical aspect is that secondary dengue infections are generally more severe than primary infections. This increased severity is believed to occur because a primary infection induces permanent immunity against the initial serotype and short-term immunological memory to other serotypes. During a secondary infection by a different serotype, pre-existing antibodies form complexes with the virus that are then captured by receptors on immune cells, leading to internalization and replication of the virus within host cells [48,58]. Recent studies have also indicated that a primary infection with the zika virus followed by a subsequent dengue virus infection poses a significant risk for developing severe dengue fever, comparable to the severity observed in heterologous primary and secondary dengue infections [59].
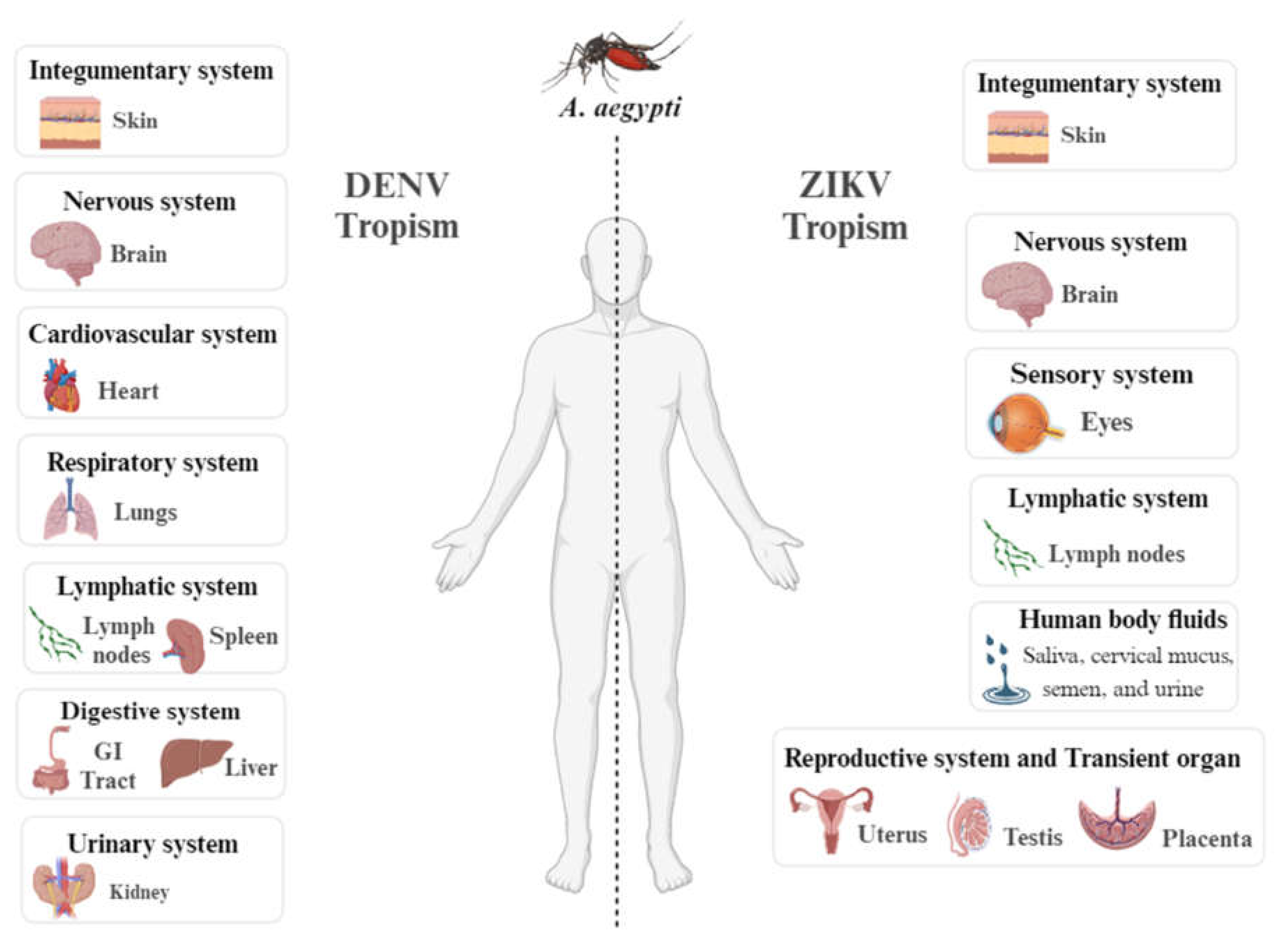
Dengue and Zika are related viruses transmitted by the same species of mosquitoes. While dengue has been well-documented and has affected people worldwide for many years, Zika has only recently caused outbreaks. Even though the virus similarities, the tropism of the viruses are different (Figure 4). Complication due to a zika virus infection is during the pregnancy that may cause microcephaly and other congenital malformations in the infant referred to as congenital Zika syndrome [60].
Another neglected arbovirus, with symptoms similar to dengue and chikungunya, is orupuche fever (OF) [12,61]. The Oropouche virus (OROV) is one of the most common orthobunyaviruses and has in recent months spread to several countries in Central and South America, alerting the Pan American Health Organization (PAHO, WHO) on February 2, 2024 [62,63]. The OROV outbreak can be divided into: (1) sylvatic, transmitted by the mosquitoes Coquilletti diavenezuelensis, Aedes serratus and, the most important, Culicoides paraenses, through various hosts, such as sloths (Bradypus tridactylus), rodents, birds, and non-human primates; (2) urban, transmitted by the mosquitoes Culicoides paraenses and Culex quinquefasciatus through humans as the amplifying host [12,61,62,64].
Symptoms include headache, high fever, arthralgia, myalgia, skin rashes, malaise, pain behind the eyes, nausea, vomiting, and mild bleeding. Symptoms usually disappear within two weeks, but in the most severe cases meningitis or encephalitis occurs [12,61,65]. To date, no deaths have been reported due to OROV [61]. As the symptoms are similar to those of other arboviruses, OROV has been gaining notoriety due to the outbreak of dengue-like symptoms in the Americas, which probably indicates an underreporting of cases of OF and causes a gap in knowledge about the disease and about OROV.
Figure 3.
Development and evolution of dengue symptoms in humans. Dengue progresses through three distinct clinical phases: (1) febrile phase that begins after the incubation period and is characterized by classic symptoms such as high fever, rash, myalgia, retro-orbital pain, nausea, and diarrhea (depicted on the left side of the figure). (2) Critical phase that occurs as the fever starts to subside. During this period, symptoms may worsen, indicating a potential progression to a more severe condition. Symptoms include plasma leakage through capillaries, hemorrhages, shock, and liver or kidney impairment (depicted on the right side of the figure). (3) Recovery phase, where the extravasated fluid is reabsorbed, and gastrointestinal symptoms gradually reduce. This image was created based on data from references [66,67].
Figure 3.
Development and evolution of dengue symptoms in humans. Dengue progresses through three distinct clinical phases: (1) febrile phase that begins after the incubation period and is characterized by classic symptoms such as high fever, rash, myalgia, retro-orbital pain, nausea, and diarrhea (depicted on the left side of the figure). (2) Critical phase that occurs as the fever starts to subside. During this period, symptoms may worsen, indicating a potential progression to a more severe condition. Symptoms include plasma leakage through capillaries, hemorrhages, shock, and liver or kidney impairment (depicted on the right side of the figure). (3) Recovery phase, where the extravasated fluid is reabsorbed, and gastrointestinal symptoms gradually reduce. This image was created based on data from references [66,67].
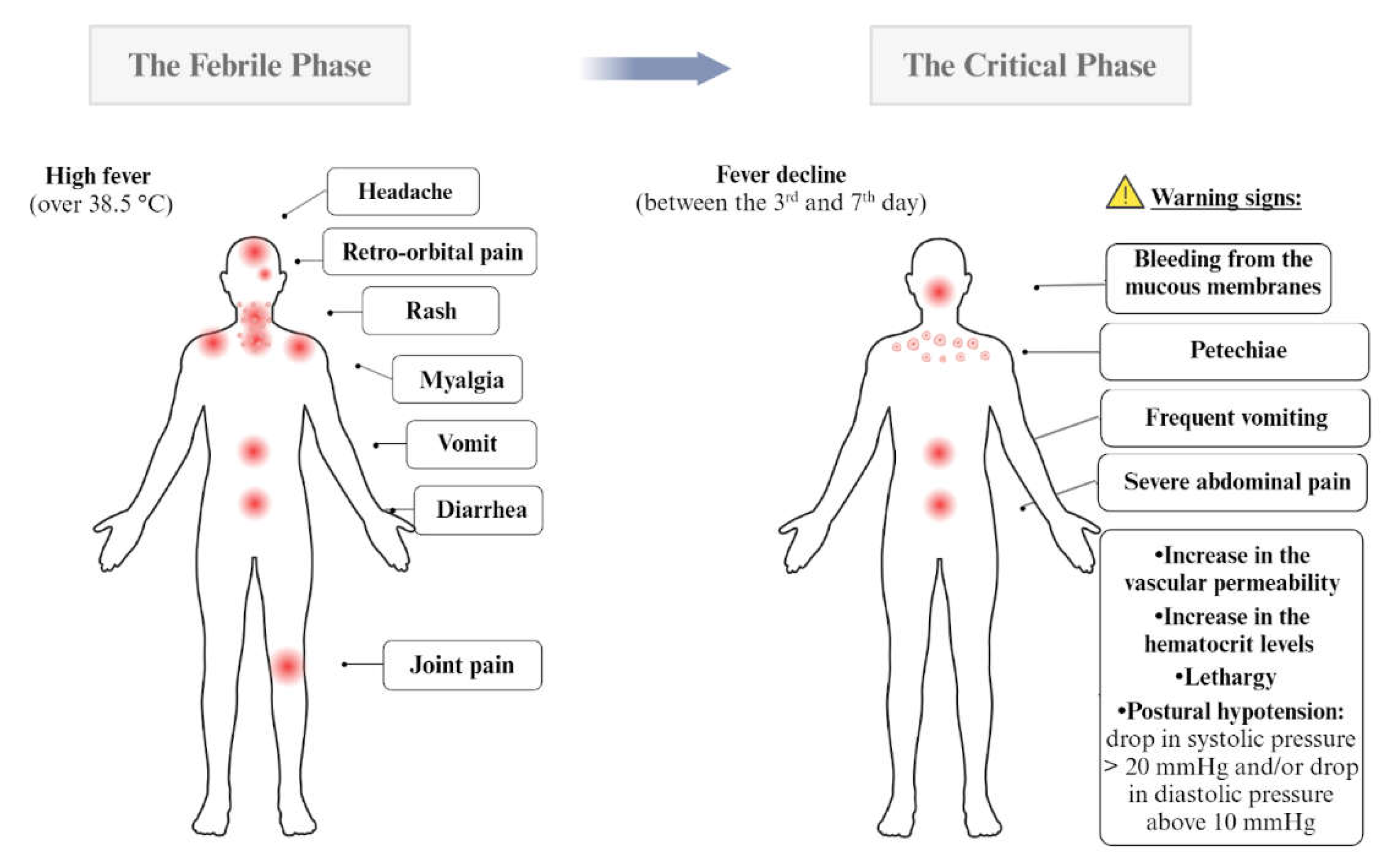
Figure 4.
Tissue tropism of dengue (DENV) and Zika (ZIKV) viruses detected in humans. The organs and body fluids where dengue virus (DENV, left side) and zika virus (ZIKV, right side) have been detected in humans bitten by A. aegypti mosquitoes carrying these viruses. The figure is based on data obtained from references [68,69,70,71].
Figure 4.
Tissue tropism of dengue (DENV) and Zika (ZIKV) viruses detected in humans. The organs and body fluids where dengue virus (DENV, left side) and zika virus (ZIKV, right side) have been detected in humans bitten by A. aegypti mosquitoes carrying these viruses. The figure is based on data obtained from references [68,69,70,71].
Clinical Management and Therapeutic Intervention in Dengue
The severity of the infection is a key factor in choosing the better treatment. The Federal Government Organization responsible for promoting, protecting, and recovering the health of the population in Brazil, the Ministério da Saúde (MS), emphasizes through the National Dengue Control Guidelines the importance of risk classification of patients for treatment and reduction of deaths. The following classification model is indicated as shown in Table 1. The classification system ensures that patients receive appropriate care based on the severity of their symptoms, aiming to reduce mortality and improve outcomes. By following these guidelines, healthcare providers can effectively manage dengue cases, prioritize resources, and deliver timely interventions to those in need. Proper adherence to this structured approach is essential for controlling the impact of dengue and safeguarding public health in Brazil.

Table 1.
Risk group classification and clinical approaches for dengue treatment. Patients with DENV are classified into distinct severity groups (Blue, Green, Yellow, and Red) based on clinical signs, hypotension, and bleeding. It guides healthcare professionals with indicators for patient management. Treatment strategies vary according to each group. Group A (Blue) receives care at Primary Health Care Units with home-based treatments, Group B (Green) is observed in Secondary Health Care Units with intensified hydration, Group C (Yellow) undergoes intravenous hydration in Tertiary Health Care Units, and Group D (Red) requires immediate intensive care [72].
Table 1.
Risk group classification and clinical approaches for dengue treatment. Patients with DENV are classified into distinct severity groups (Blue, Green, Yellow, and Red) based on clinical signs, hypotension, and bleeding. It guides healthcare professionals with indicators for patient management. Treatment strategies vary according to each group. Group A (Blue) receives care at Primary Health Care Units with home-based treatments, Group B (Green) is observed in Secondary Health Care Units with intensified hydration, Group C (Yellow) undergoes intravenous hydration in Tertiary Health Care Units, and Group D (Red) requires immediate intensive care [72].
| Signs of shock | Clinical approach | Reference | |
| Group A(Blue) | - |
|
[66,68,72,73] |
| Group B(Green) | Patients presenting two or more clinical signs of the acute phase in addition to spontaneous bleeding, which can be indicated by petechiae, gingival bleeding and ecchymosis. | The care occurs in a Secondary Health Care Unit equipped with an on-observation bed, where they are required to stay hospitalized for a minimum of 12 h. During this time, they receive oral or intravenous hydration and undergo a complete blood count to monitor their hematocrit levels. | [66,73] |
| Group C(Yellow) | Here symptoms may arise that may indicate the progression of the disease to a more serious clinical condition that includes lethargy, severe abdominal pain, postural hypotension, frequent vomiting, bleeding from the mucous membranes, progressive increase in the hematocrit levels and decrease of the platelets levels. |
|
[66,73] |
| Group D(Red) | Intended for patients presenting signs of shock: convergent blood pressure (Differential BP <20mm Hg), arterial hypotension, cyanosis, rapid pulse, and slow capillary refill. |
|
[66,72,73] |
Measures Adopted in Brazil to Mitigate the DENV Cases
Dengue fever exhibits distinct seasonal contamination patterns, with a notable surge in cases and heightened epidemic risks typically observed between October and May of the following year [74]. Factors exacerbating vector proliferation and disease incidence include inadequate basic sanitation services, unregulated urban expansion, and improper waste disposal [72,74]. In 2024, global dengue cases exploded, particularly in the Americas, where 80% of global cases are concentrated. Several countries, including Brazil, reported escalating case numbers alongside simultaneous circulation of all four dengue serotypes (Figure 2) [75]. Climate change-induced alterations have accelerated mosquito breeding and virus dissemination, contributing significantly to this scenario [76].
Effective year-round prevention hinges on intersectoral policies involving community engagement and healthcare professionals as pivotal actors. Strategies encompass mechanical, biological, legal, and chemical control methods [68,72,77]. Individual responsibilities include eliminating stagnant water reservoirs (containers, gutters, open reservoirs), managing debris, and employing endorsed repellents registered with Agência Nacional de Vigilância Sanitária (ANVISA), containing active ingredients such as DEET, Icaridin, EBAAP, or Citronella [78,79]. Endemic Disease Control (EDC) professionals and Community Health Agents (CHA) complement these efforts by educating residents and overseeing preventive measures [72].
Chemical control entails World Health Organization (WHO)-approved insecticides, including aerosol sprays "fumacê", such as Prallethrin and Imidacloprid, targeting larval and adult stages, but with environmental impact concerns and potential resistance development [72,80]. Biological alternatives include Bacillus thuringiensis israelensis (Bti), effective against A. aegypti larvae, and the Wolbachia method, utilizing bacteria-infected mosquitoes to hinder arbovirus transmission, with successful implementations in Brazilian cities as in Belo Horizonte [81,82].
Legal measures enforce cleanliness norms on vacant or abandoned properties, facilitating access for health agents in inactive or resistant premises [72]. Brazil's Unified Health System (SUS) integrated the dengue vaccine (Qdenga) into its national schedule in December 2023, targeting initial doses for children and teenagers aged 10-14 across 521 municipalities starting February 2024 [83]. Despite supply challenges, subsequent vaccine shipments are ongoing, with nearly 1 million doses distributed by late May 2024 to 405 municipalities [76,84]. To meet nationwide demand, the MS is advancing a single-dose tetravalent Brazilian vaccine, nearing completion of clinical trials at Instituto Butantan [76,84].
In general, combating dengue fever in Brazil requires a multiple approach that integrates community involvement, robust healthcare strategies, and coordinated efforts across various sectors. Addressing the environmental, social, and health-related determinants of dengue transmission is essential for reducing the DENV circulation. Despite implementing various measures, Brazil has seen only incremental progress in eradicating dengue, indicating the need for additional strategies. To prevent a new outbreak during the upcoming seasonal cycle of the disease, expected between December and March, further proactive measures must be implemented.
Diagnosis Test Available in Brazil for Dengue Disease
Different strategies are employed for dengue diagnosis depending on the stage of the disease and the clinical history of the infection [85] (Table 2). Despite the significant advancements in biomolecular approaches and lateral flow rapid tests, simpler techniques such as the tourniquet test (TT) are widely used in regions with a high incidence of cases and in poor areas where these methods are not affordable or laboratories cannot achieve the demand [86,87]. A positive TT (≥10 petechiae per square inch) is usually observed in patients with dengue hemorrhagic fever and severe forms of the disease due to capillary fragility and thrombocytopenia [88]. However, due to its low sensitivity and specificity, the TT alone is not accepted as a diagnostic criterion and must complement other biomolecular, antigenic, and immunogenic assays [89,90].
When deciding which test to use, previous exposure to Flaviviridae viruses must be considered. In primary infections, longer viremia and an extended presence of non-structural protein (NS1) in the bloodstream and body fluids are found. IgM typically emerges around the third day of symptom onset, while IgG is absent until the tenth day. In contrast, immunological memory from past infections allows early production of IgG, creating an effective antiviral response that limits the circulating amount of NS1[36,91,92,93,94]. Reverse-transcriptase polymerase chain reaction (RT-PCR) is a powerful tool to confirm the presence of viral particles, capable of differentiating flavivirus species and even the five DENV subtypes [36,95]. For RT-PCR, samples should be stored at 4-8 °C for no more than 24 h to avoid false-negative results due to the fast degradation of viral RNA in vitro [96].
For NS1 detection using Enzyme-Linked Immunosorbent Assay (ELISA), samples can be stored at 4-8 °C for 24 h and at -30 °C or -70 °C for 15 days or longer periods [37,96]. NS1 is a conserved glycoprotein produced by flaviviruses and found in serum and body fluids, making it an interesting target for diagnostic tests. However, saliva and urine samples have shown much lower sensitivity and specificity compared to plasma samples [97,98,99,100].
Serological tests are essential for interpreting disease progression and differentiating between primary and secondary infections. These tests can vary significantly depending on infection history and are susceptible to cross-reactions in individuals previously infected by other flaviviruses, such as a secondary zika virus infection in patients once exposed to dengue virus [101]. Positive IgM and negative IgG during the first week of infection indicates a recent primary infection, while positive IgM and IgG in a 1.10 ratio reveals a recent secondary infection (Se = 100 % and Sp = 97.4 %) [102]. Negative IgM and positive IgG results indicate an infection from the past few months [36,38]. Combining two or more tests (e.g., NS1 + IgM or NS1 + IgM/IgG detection) is strongly recommended to improve sensitivity and specificity (up to 100%), thereby providing a more reliable diagnosis.
In addition to the aforementioned techniques, some older methods, though largely replaced by new technological systems for clinical diagnosis, still hold importance for specific investigations. For example, the plaque reduction neutralization test (PRNT) and virus cultivation require specialized laboratories capable of growing the virus in cell tissues, often taking more than a week to obtain results. PRNT provides information about the presence of antibodies in the patient's serum that can inactivate specific virus species, while virus cultivation allows for the laboratory culture of viruses from different sources, including autopsy tissues [103,104,105].
Overall, accurate dengue fever diagnosis requires a combination of diagnostic strategies tailored to the disease stage and patient history. Advanced biomolecular techniques and rapid tests have improved diagnostic capabilities, but simpler methods like the tourniquet test are still vital in resource-limited settings. Biomolecular assays, such as RT-PCR and NS1 detection, confirm viral presence and differentiate dengue subtypes, though careful management is needed to ensure accuracy. Serological tests distinguish between primary and secondary infections, despite potential cross-reactions with other flaviviruses. Combining multiple diagnostic methods enhances reliability. Older techniques such as plaque reduction neutralization tests and virus cultivation remain important for specific research. An integrated approach using both advanced and traditional methods is crucial for effective dengue management, with ongoing innovation and improved accessibility key to controlling the disease globally. Table 2 shows the suggested diagnostic test to be used in dengue disease based on days after symptoms onset and time to obtain the result.
Table 2.
Diagnostic tests based on days after symptom onset. Primary infection (PI) refers to a patient experiencing their first dengue infection, while secondary infection (SI) pertains to a patient who has had a previous dengue infection. DF stands for dengue fever, DHF for dengue hemorrhagic fever, Se for sensitivity, Sp for specificity, and RDT for rapid diagnostic test.
Table 2.
Diagnostic tests based on days after symptom onset. Primary infection (PI) refers to a patient experiencing their first dengue infection, while secondary infection (SI) pertains to a patient who has had a previous dengue infection. DF stands for dengue fever, DHF for dengue hemorrhagic fever, Se for sensitivity, Sp for specificity, and RDT for rapid diagnostic test.
| Diagnostic test timeline (days after symptom onset) | |||||
|---|---|---|---|---|---|
| Method principle | Primary Infection (PI) | Secondary Infection (SI) | Time to obtain the result | ||
| Capillary fragility | Tourniquet Test |
|
min | ||
| Virus or virus product detection | Virus isolation |
|
≥ one week | ||
|
|
||||
| RT-PCR or RT-qPCR |
|
around one day | |||
| NS1 protein detection | ELISA (serum) | - from 0 to 7 days
|
- from 0 to 3 days
|
around one day | |
| RDT (serum) | min | ||||
- from 0 to 3 days
| |||||
| Antibody detection | IgM detection | ELISA (serum) |
|
|
around one day |
| RDT (serum) | - from 0 to 3 days - from 4 days onwards | min | |||
| IgG detection | RDT (serum) |
|
|
min | |
Dengue's Emergence in Europe: a Changing Epidemiological Landscape
As described in this study, dengue outbreaks in tropical countries are increasing, while outbreaks in colder regions were previously unexpected. The majority of dengue cases are travel-related [114], although this trend is gradually changing. Global warming has facilitated the adaptation and establishment of invasive mosquito species in regions where they could not survive a few years ago. Since May 2024, non-native Aedes mosquitoes (such as A. aegypti, A. albopictus, A. atropalpus, A. japonicus, and A. koreicus) have been reported as well-established in most European countries [115]. Moreover, there is concern that local European Aedes mosquitoes could potentially adapt to become new vectors for dengue and other arboviruses. For instance, the chikungunya virus has already been found in A. geniculatus, a native European mosquito [116]. Once these viruses adapt to native mosquitoes [117], diseases caused by these viruses could become established in these new regions.
Considering the species-specific establishment trends, A. aegypti and A. albopictus emerge as the primary vectors of DENV. Consequently, A. albopictus is expected to be the predominant vector contributing to the presence of dengue in Europe [118]. The northward expansion of their presence, particularly into the southernmost areas of Sweden, raises significant concerns. The well-established populations of A. albopictus in Mediterranean areas signify a potential endemic precursor, as these regions are increasingly conducive to Aedes spp. proliferation due to changing climates.
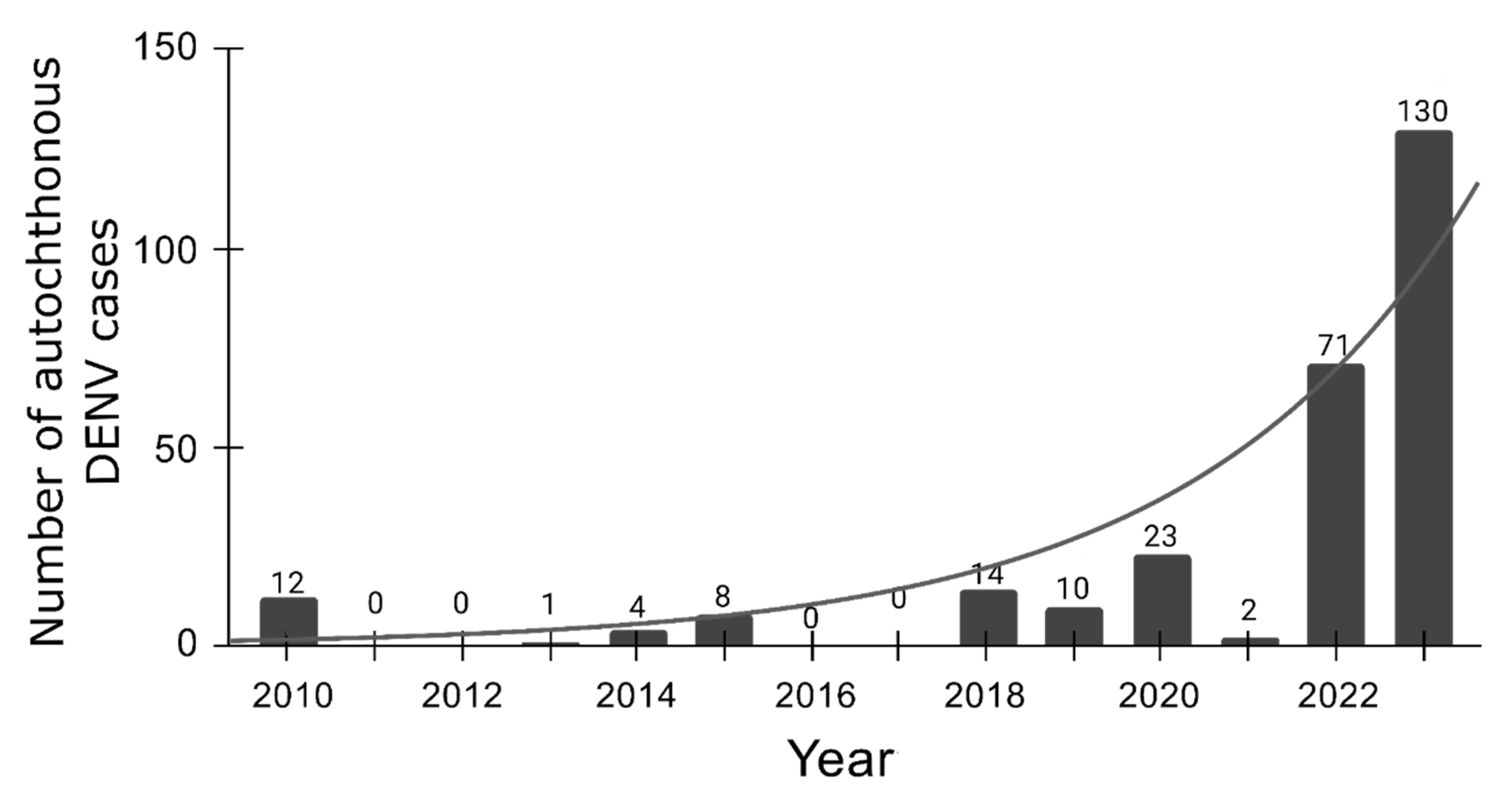
The increasing dengue outbreaks globally, including in colder regions, underscore a significant public health challenge exacerbated by global warming facilitating the spread of invasive mosquito species like Aedes into new territories. In Europe, the establishment of non-native Aedes mosquitoes raises concerns about their potential as new vectors for dengue and other arboviruses, necessitating urgent preparedness within healthcare systems and communities. The European Centre for Disease Prevention and Control [118] reports the evolution of autochthonous dengue cases in Europe over the years [115]. The exponential profile in DENV native cases is alarming, suggesting a significant increase in cases in Europe (Figure 5). This underscores the urgent need for European lifestyles and healthcare systems to prepare for managing large numbers of arbovirus cases. With intensifying climate change, proactive measures are crucial to address the presence of A. albopictus in Europe before dengue and other tropical diseases become endemic in temperate regions.
Figure 5.
Annual count of total autochthonous cases in Europe. Annual count of total autochthonous cases in Europe. The curve represents the exponential regression, showing an increase in total autochthonous cases in Europe in function of time (in year).
Figure 5.
Annual count of total autochthonous cases in Europe. Annual count of total autochthonous cases in Europe. The curve represents the exponential regression, showing an increase in total autochthonous cases in Europe in function of time (in year).
Conclusions
Dengue fever, a significant arboviral disease transmitted by Aedes mosquitoes, poses a growing public health challenge globally. The disease spreading is conducted by factors such as climate change, urbanization, and globalization, which facilitate the proliferation of mosquito vectors and the movement of infected individuals across borders. This phenomenon is evident in Latin America, where rising temperatures and increased rainfall create ideal conditions for mosquito proliferation. Moreover, the escalation of dengue cases in Brazil underscores the urgent need for improved surveillance and diagnostic capabilities, especially in economically disadvantaged regions.
Overall, this study underscores the changing epidemiological scenario of dengue, exemplified by its emergence in traditionally non-endemic regions like Europe. The establishment of A. albopictus and other invasive species in new territories signals a critical shift in DENV transmission dynamics, enhanced by climate changes and vector adaptation. The presence of these vectors in temperate zones raises significant public health concerns, necessitating coordinated surveillance, vector control strategies, and preparedness efforts. Addressing these challenges requires interdisciplinary approaches and international collaboration to mitigate the spread of dengue and other arboviruses worldwide.
Informed Consent Statement
not applicable.
Data Availability Statement
not applicable.
Acknowledgment
The authors acknowledge the National Council for Scientific and Technological Development (CNPq), the Coordination for the Improvement of Higher Education Personnel (CAPES, grant 88887.374931/2019-00 and 88887.600105/2021-00, Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Finance Code 01), and the São Paulo Research Foundation (FAPESP, 2021/10577-0, 2022/08730-7, 2021/05262-0, 2023/13894-1, 2023/07366-2), FINEP grant 29794 (FINEP/UFMG/PRPQ/CT VACINAS/SARS-CoV-2), for financial support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- FAO-WHO Expert Committee on Zoonoses. Zoonoses: Report of the FAO-WHO Expert Committee on Zoonoses, 3rd, Geneva, 1966. (1967).
- Harapan, H., Michie, A., Sasmono, R. T. & Imrie, A. Dengue: A Minireview. Viruses 12, (2020).
- Arthropod-borne and rodent-borne viral diseases. Report of a WHO Scientific Group. World Health Organ. Tech. Rep. Ser. 719, 1–116 (1985).
- Young, P. R. Arboviruses: A Family on the Move. Adv. Exp. Med. Biol. 1062, 1–10 (2018).
- Go, Y. Y., Balasuriya, U. B. R. & Lee, C.-K. Zoonotic encephalitides caused by arboviruses: transmission and epidemiology of alphaviruses and flaviviruses. Clin. Exp. Vaccine Res. 3, 58–77 (2014).
- Hollidge, B. S., González-Scarano, F. & Soldan, S. S. Arboviral encephalitides: transmission, emergence, and pathogenesis. J. Neuroimmune Pharmacol. 5, 428–442 (2010).
- Weaver, S. C. & Reisen, W. K. Present and future arboviral threats. Antiviral Res. 85, 328–345 (2010). [CrossRef]
- Liu, Y., Guan, W. & Liu, H. Subgenomic Flaviviral RNAs of Dengue Viruses. Viruses 15, (2023).
- Murugesan, A. & Manoharan, M. Dengue Virus. in Emerging and Reemerging Viral Pathogens 281–359 (Elsevier, 2020). [CrossRef]
- Drugs targeting structural and nonstructural proteins of the chikungunya virus: A review. Int. J. Biol. Macromol. 262, 129949 (2024). [CrossRef]
- Caicedo, E.-Y. et al. The epidemiology of Mayaro virus in the Americas: A systematic review and key parameter estimates for outbreak modelling. PLoS Negl. Trop. Dis. 15, e0009418 (2021).
- Martins-Filho, P. R., Soares-Neto, R. F., de Oliveira-Júnior, J. M. & Alves Dos Santos, C. The underdiagnosed threat of oropouche fever amidst dengue epidemics in Brazil. Lancet Reg Health Am 32, 100718 (2024).
- Cattarino, L., Rodriguez-Barraquer, I., Imai, N., Cummings, D. A. T. & Ferguson, N. M. Mapping global variation in dengue transmission intensity. Sci. Transl. Med. 12, (2020).
- Kularatne, S. A. & Dalugama, C. Dengue infection: Global importance, immunopathology and management. Clin. Med. 22, 9–13 (2022).
- Ferreira-de-Lima, V. H. & Lima-Camara, T. N. Natural vertical transmission of dengue virus in Aedes aegypti and Aedes albopictus: a systematic review. Parasit. Vectors 11, 77 (2018).
- Tauil, P. L. [Critical aspects of dengue control in Brazil]. Cad. Saude Publica 18, 867–871 (2002).
- Paz-Bailey, G., Adams, L. E., Deen, J., Anderson, K. B. & Lc., K. Website. Lancet 403, 667–682 (2024).
- Xu, Z. et al. Projecting the future of dengue under climate change scenarios: Progress, uncertainties and research needs. PLoS Negl. Trop. Dis. 14, e0008118 (2020).
- Morin, C. W., Comrie, A. C. & Ernst, K. Climate and dengue transmission: evidence and implications. Environ. Health Perspect. 121, 1264–1272 (2013).
- Combined effects of hydrometeorological hazards and urbanisation on dengue risk in Brazil: a spatiotemporal modelling study. The Lancet Planetary Health 5, e209–e219 (2021).
- Dengue overview: An updated systemic review. J. Infect. Public Health 16, 1625–1642 (2023).
- Chen, R. & Vasilakis, N. Dengue--quo tu et quo vadis? Viruses 3, 1562–1608 (2011).
- Bashyam, H. S., Green, S. & Rothman, A. L. Dengue virus-reactive CD8+ T cells display quantitative and qualitative differences in their response to variant epitopes of heterologous viral serotypes. J. Immunol. 176, 2817–2824 (2006).
- Parveen, S. et al. Dengue hemorrhagic fever: a growing global menace. J. Water Health 21, 1632–1650 (2023).
- Brathwaite Dick, O. et al. The history of dengue outbreaks in the Americas. Am. J. Trop. Med. Hyg. 87, 584–593 (2012).
- Juan, C. Dengue Fever: Strategies for Preventing Dengue and Bite Transmission Via Mosquitoes. (Independently Published, 2024).
- Cristodulo, R. et al. Dengue Myocarditis: A Case Report and Major Review. Glob. Heart 18, 41 (2023).
- Aedes albopictus - current known distribution: October 2023. European Centre for Disease Prevention and Control https://www.ecdc.europa.eu/en/publications-data/aedes-albopictus-current-known-distribution-october-2023 (2023).
- Schaefer, T. J., Panda, P. K. & Wolford, R. W. Dengue Fever. in StatPearls (StatPearls Publishing, Treasure Island (FL), 2024).
- Gamez, S., Antoshechkin, I., Mendez-Sanchez, S. C. & Akbari, O. S. The Developmental Transcriptome of , a Major Worldwide Human Disease Vector. G3 10, 1051–1062 (2020).
- Weerakoon, K. G. et al. Histopathological diagnosis of myocarditis in a dengue outbreak in Sri Lanka, 2009. BMC Res. Notes 4, 268 (2011).
- Sinha, S. et al. Dengue virus pathogenesis and host molecular machineries. J. Biomed. Sci. 31, 43 (2024).
- Madhry, D. et al. Role of non-coding RNAs in Dengue virus-host interaction. Front. Biosci. 13, 44–55 (2021).
- Guzman, M. G., Gubler, D. J., Izquierdo, A., Martinez, E. & Halstead, S. B. Dengue infection. Nature Reviews Disease Primers 2, 1–25 (2016).
- Gubler, D. J., Ooi, E. E., Vasudevan, S. & Farrar, J. Dengue and Dengue Hemorrhagic Fever, 2nd Edition. (CABI, 2014).
- Kok, B. H. et al. Dengue virus infection - a review of pathogenesis, vaccines, diagnosis and therapy. Virus Res. 324, 199018 (2023).
- Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control: New Edition. (World Health Organization, Geneva, 2009).
- Zerfu, B., Kassa, T. & Legesse, M. Epidemiology, biology, pathogenesis, clinical manifestations, and diagnosis of dengue virus infection, and its trend in Ethiopia: a comprehensive literature review. Trop. Med. Health 51, 11 (2023).
- Kalayanarooj, S. Clinical Manifestations and Management of Dengue/DHF/DSS. Trop. Med. Health 39, 83–87 (2011).
- Verma, R. et al. Neurological complications of dengue fever: Experience from a tertiary center of north India. Ann. Indian Acad. Neurol. 14, 272–278 (2011).
- Marengo, J. A. Água e mudanças climáticas. Estud. av. 22, 83–96 (2008).
- Southern Brazil has seen an increase of up to 30% in average annual rainfall over the last three decades. Planalto https://www.gov.br/planalto/en/latest-news/2024/05/southern-brazil-has-seen-an-increase-of-up-to-30-in-average-annual-rainfall-over-the-last-three-decades (2024).
- Diallo, D. et al. Dengue vectors in Africa: A review. Heliyon 8, e09459 (2022).
- BRASIL. Painel de Monitoramento das Arboviroses. Ministério da Saúde https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/a/aedes-aegypti/monitoramento-das-arboviroses/painel (2024).
- Statistica. Dengue cases in Latin America & the Caribbean 2016-2024. Statista https://www.statista.com/statistics/1099801/latin-america-number-dengue-cases/ (2024).
- PAHO. Situation Report No 20 - Dengue Epidemiological Situation in the Region of the Americas - Epidemiological Week 20, 2024. Pan American Health Organization (PAHO) https://www.paho.org/en/documents/situation-report-no-20-dengue-epidemiological-situation-region-americas-epidemiological (2024).
- BRASIL. Centro de Operações de Emergências (COE). Ministério da Saúde https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/a/arboviroses/informe-semanal/informe-semanal-no-02-coe (2024).
- Khanam, A., Gutiérrez-Barbosa, H., Lyke, K. E. & Chua, J. V. Immune-Mediated Pathogenesis in Dengue Virus Infection. Viruses 14, (2022).
- Waickman, A. T. et al. Evolution of inflammation and immunity in a dengue virus 1 human infection model. Sci. Transl. Med. 14, eabo5019 (2022).
- Dengue. Ministério da Saúde https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/d/dengue/dengue.
- Yung, C.-F. et al. Dengue serotype-specific differences in clinical manifestation, laboratory parameters and risk of severe disease in adults, singapore. Am. J. Trop. Med. Hyg. 92, 999–1005 (2015).
- Begam, N. N. et al. Management of dengue with co-infections: an updated narrative review. Drug Discov. Ther. 15, 130–138 (2021).
- Henrique Ferreira Sucupira, P. et al. Serotype-associated immune response and network immunoclusters in children and adults during acute Dengue virus infection. Cytokine 169, 156306 (2023).
- Rowe, E. K. et al. Challenges in dengue fever in the elderly: atypical presentation and risk of severe dengue and hospital-acquired infection [corrected]. PLoS Negl. Trop. Dis. 8, e2777 (2014).
- Lin, C.-H. et al. Dengue outbreaks in high-income area, Kaohsiung City, Taiwan, 2003-2009. Emerg. Infect. Dis. 18, 1603–1611 (2012).
- Paz-Bailey, G. et al. Predominance of Severe Plasma Leakage in Pediatric Patients With Severe Dengue in Puerto Rico. J. Infect. Dis. 226, 1949–1958 (2022).
- Hober, D. et al. Serum levels of tumor necrosis factor-alpha (TNF-alpha), interleukin-6 (IL-6), and interleukin-1 beta (IL-1 beta) in dengue-infected patients. Am. J. Trop. Med. Hyg. 48, 324–331 (1993).
- Soo, K.-M., Khalid, B., Ching, S.-M. & Chee, H.-Y. Meta-Analysis of Dengue Severity during Infection by Different Dengue Virus Serotypes in Primary and Secondary Infections. PLoS One 11, e0154760 (2016).
- Estofolete, C. F. et al. Influence of previous Zika virus infection on acute dengue episode. PLoS Negl. Trop. Dis. 17, e0011710 (2023).
- Musso, D., Ko, A. I. & Baud, D. Zika Virus Infection - After the Pandemic. N. Engl. J. Med. 381, 1444–1457 (2019).
- Zhang, Y. et al. Oropouche virus: A neglected global arboviral threat. Virus Res. 341, 199318 (2024).
- Mohapatra, R. K., Mishra, S., Satapathy, P., Kandi, V. & Tuglo, L. S. Surging Oropouche virus (OROV) cases in the Americas: A public health challenge. New Microbes New Infect 59, 101243 (2024).
- Public Health risk assessment related to Oropouche virus (OROV) in the region of the Americas, 9 February 2024. ReliefWeb https://reliefweb.int/report/world/public-health-risk-assessment-related-oropouche-virus-orov-region-americas-9-february-2024.
- Febre do Oropouche. Ministério da Saúde https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/f/febre-do-oropouche.
- Sakkas, H., Bozidis, P., Franks, A. & Papadopoulou, C. Oropouche Fever: A Review. Viruses 10, (2018).
- B A Seixas, J., Giovanni Luz, K. & Pinto Junior, V. [Clinical Update on Diagnosis, Treatment and Prevention of Dengue]. Acta Med. Port. 37, 126–135 (2024).
- Rajapakse, S., de Silva, N. L., Weeratunga, P., Rodrigo, C. & Fernando, S. D. Prophylactic and therapeutic interventions for bleeding in dengue: a systematic review. Trans. R. Soc. Trop. Med. Hyg. 111, 433–439 (2017).
- Jasamai, M., Yap, W. B., Sakulpanich, A. & Jaleel, A. Current prevention and potential treatment options for dengue infection. J. Pharm. Pharm. Sci. 22, 440–456 (2019).
- Silva, N. M., Santos, N. C. & Martins, I. C. Dengue and Zika Viruses: Epidemiological History, Potential Therapies, and Promising Vaccines. Trop Med Infect Dis 5, (2020).
- Miner, J. J. & Diamond, M. S. Zika Virus Pathogenesis and Tissue Tropism. Cell Host Microbe 21, 134–142 (2017).
- Begum, F., Das, S., Mukherjee, D., Mal, S. & Ray, U. Insight into the Tropism of Dengue Virus in Humans. Viruses 11, (2019).
- BRASIL. Diretrizes nacionais para a prevenção e controle de epidemias de dengue. Brasília, DF: MS, 2009. Ministério da Saúde http://bvsms.saude.gov.br/bvs/publicacoes/diretrizes_nacionais_prevencao_controle_dengue (2024).
- Stanley, S. M., Khera, H. K., Chandrasingh, S., George, C. E. & Mishra, R. K. A comprehensive review of dengue with a focus on emerging solutions for precision and timely detection. Int. J. Biol. Macromol. 254, 127613 (2024).
- BRASIL. Ministério da Saúde-Saúde de A a Z-Dengue. Ministério da Saúde https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/d/dengue/dengue (2024).
- OPAS. Alerta Epidemiológico-Aumento de casos de dengue na Região das Américas. Organização Pan-Americana da Saúde (OPAS) https://www.paho.org/pt/documentos/alerta-epidemiologico-aumento-casos-dengue-na-regiao-das-americas-16-fevereiro-2024 (2024).
- BRASIL. Ministério da Saúde entrega nova remessa de vacinas da dengue. Ministério da Saúde https://www.gov.br/saude/pt-br/assuntos/noticias/2024/maio/ministerio-da-saude-entrega-nova-remessa-de-vacinas-da-dengue (2024).
- BRASIL. Ministério da Saúde elabora plano para enfrentamento da dengue 2024/2025. Ministério da Saúde https://www.gov.br/saude/pt-br/assuntos/noticias/2024/maio/ministerio-da-saude-elabora-plano-para-enfrentamento-da-dengue-2024-2025 (2024).
- BRASIL. Combate ao mosquito. Ministério da Saúde https://www.gov.br/saude/pt-br/campanhas-da-saude/2023/combate-ao-mosquito/combate-ao-mosquito (2023).
- Conselho Federal de Farmácia. Orientações sobre o uso de repelentes. Conselho Federal de Farmácia https://site.cff.org.br/noticia/noticias-do-cff/01/03/2024/orientacoes-sobre-o-uso-de-repelentes (2024).
- BRASIL. Saiba como é utilizado o fumacê no combate ao mosquito da dengue. Ministério da Saúde https://www.gov.br/saude/pt-br/assuntos/noticias/2024/marco/saiba-como-e-utilizado-o-fumace-no-combate-ao-mosquito-da-dengue (2024).
- BRASIL. Você sabe o que é o Método Wolbachia? Ministério da Saúde https://www.gov.br/saude/pt-br/assuntos/saude-com-ciencia/noticias/2024/maio/voce-sabe-o-que-e-o-metodo-wolbachia (2024).
- World Mosquito Program. Sobre o Método Wolbachia. World Mosquito Program https://www.worldmosquitoprogram.org/sobre-o-metodo-wolbachia (2024).
- BRASIL. Ministério da Saúde incorpora vacina contra a dengue no SUS. Ministério da Saúde https://www.gov.br/saude/pt-br/assuntos/noticias/2023/dezembro/ministerio-da-saude-incorpora-vacina-contra-a-dengue-no-sus (2023).
- Butantan, I. Instituto Butantan-Portal do Butantan. Tira Dúvida- Vacina da dengue deve proteger de todos os subtipos da doença; entenda a complexidade do ensaio clínico. https://butantan.gov.br/covid/butantan-tira-duvida/tira-duvida-noticias/vacina-da-dengue-deve-proteger-de-todos-os-subtipos-da-doenca--entenda-a-complexidade-do-ensaio-clinico (2022).
- Muller, D. A., Depelsenaire, A. C. I. & Young, P. R. Clinical and Laboratory Diagnosis of Dengue Virus Infection. J. Infect. Dis. 215, S89–S95 (2017).
- Gregory, C. J. et al. Utility of the tourniquet test and the white blood cell count to differentiate dengue among acute febrile illnesses in the emergency room. PLoS Negl. Trop. Dis. 5, e1400 (2011).
- Kalayanarooj, S. et al. Early clinical and laboratory indicators of acute dengue illness. J. Infect. Dis. 176, 313–321 (1997).
- Montes y Gómez, M., Escalante, H. J., Segura, A. & de Dios Murillo, J. Advances in Artificial Intelligence - IBERAMIA 2016: 15th Ibero-American Conference on AI, San José, Costa Rica, November 23-25, 2016, Proceedings. (Springer, 2016).
- Furlan, N. B., Tukasan, C., Estofolete, C. F., Nogueira, M. L. & da Silva, N. S. Low sensitivity of the tourniquet test for differential diagnosis of dengue: an analysis of 28,000 trials in patients. BMC Infect. Dis. 16, 627 (2016).
- Mayxay, M. et al. Predictive diagnostic value of the tourniquet test for the diagnosis of dengue infection in adults. Trop. Med. Int. Health 16, 127–133 (2011).
- St John, A. L. & Rathore, A. P. S. Adaptive immune responses to primary and secondary dengue virus infections. Nat. Rev. Immunol. 19, 218–230 (2019).
- Tang, K. F. & Ooi, E. E. Diagnosis of dengue: an update. Expert Rev. Anti. Infect. Ther. 10, 895–907 (2012).
- Avrami, S., Hoffman, T., Meltzer, E., Lustig, Y. & Schwartz, E. Comparison of clinical and laboratory parameters of primary vs secondary dengue fever in travellers. J. Travel Med. 30, (2023).
- Fisher, R., Lustig, Y., Sklan, E. H. & Schwartz, E. The Role of NS1 Protein in the Diagnosis of Flavivirus Infections. Viruses 15, (2023).
- Lanciotti, R. S., Calisher, C. H., Gubler, D. J., Chang, G. J. & Vorndam, A. V. Rapid detection and typing of dengue viruses from clinical samples by using reverse transcriptase-polymerase chain reaction. J. Clin. Microbiol. 30, 545–551 (1992).
- Iani, F. C. de M. et al. Dengue diagnostics: serious inaccuracies are likely to occur if pre-analytical conditions are not strictly followed. Mem. Inst. Oswaldo Cruz 115, e200287 (2021).
- Cecchetto, J., Fernandes, F. C. B., Lopes, R. & Bueno, P. R. The capacitive sensing of NS1 Flavivirus biomarker. Biosens. Bioelectron. 87, 949–956 (2017).
- Rastogi, M., Sharma, N. & Singh, S. K. Flavivirus NS1: a multifaceted enigmatic viral protein. Virol. J. 13, 131 (2016).
- Peeling, R. W. et al. Evaluation of diagnostic tests: dengue. Nat. Rev. Microbiol. 8, S30–8 (2010).
- Andries, A.-C. et al. Evaluation of the performances of six commercial kits designed for dengue NS1 and anti-dengue IgM, IgG and IgA detection in urine and saliva clinical specimens. BMC Infect. Dis. 16, 1–9 (2016).
- Lanciotti, R. S. et al. Genetic and serologic properties of Zika virus associated with an epidemic, Yap State, Micronesia, 2007. Emerg. Infect. Dis. 14, 1232–1239 (2008).
- Changal, K. H. et al. Differentiating secondary from primary dengue using IgG to IgM ratio in early dengue: an observational hospital based clinico-serological study from North India. BMC Infect. Dis. 16, 1–7 (2016).
- Bäck, A. T. & Lundkvist, A. Dengue viruses - an overview. Infect. Ecol. Epidemiol. 3, (2013).
- Ayukekbong, J. A., Oyero, O. G., Nnukwu, S. E., Mesumbe, H. N. & Fobisong, C. N. Value of routine dengue diagnosis in endemic countries. World J Virol 6, 9–16 (2017).
- Thomas, S. J. et al. Dengue plaque reduction neutralization test (PRNT) in primary and secondary dengue virus infections: How alterations in assay conditions impact performance. Am. J. Trop. Med. Hyg. 81, 825–833 (2009).
- Antunes, A. C. et al. Evaluation of the diagnostic value of the tourniquet test in predicting severe dengue cases in a population from Belo Horizonte, State of Minas Gerais, Brazil. Rev. Soc. Bras. Med. Trop. 46, 542–546 (2013).
- Grande, A. J., Reid, H., Thomas, E., Foster, C. & Darton, T. C. Tourniquet Test for Dengue Diagnosis: Systematic Review and Meta-analysis of Diagnostic Test Accuracy. PLoS Negl. Trop. Dis. 10, (2016).
- Jarman, R. G. et al. Factors Influencing Dengue Virus Isolation by C6/36 Cell Culture and Mosquito Inoculation of Nested PCR-Positive Clinical Samples. Am. J. Trop. Med. Hyg. 84, 218 (2011).
- Monitoring and improving the sensitivity of dengue nested RT-PCR used in longitudinal surveillance in Thailand. J. Clin. Virol. 63, 25–31 (2015).
- Tricou, V. et al. Comparison of two dengue NS1 rapid tests for sensitivity, specificity and relationship to viraemia and antibody responses. BMC Infect. Dis. 10, 1–8 (2010).
- Luvira, V. et al. Diagnostic Performance of Dengue NS1 and Antibodies by Serum Concentration Technique. Tropical Medicine and Infectious Disease 8, (2023).
- Laboratory diagnosis of primary and secondary dengue infection. J. Clin. Virol. 31, 179–184 (2004).
- Jang, W. S. et al. Comparative evaluation of three dengue duo rapid test kits to detect NS1, IgM, and IgG associated with acute dengue in children in Myanmar. PLoS One 14, e0213451 (2019).
- Dengue- Global situation. https://www.who.int/emergencies/disease-outbreak-news/item/2023-DON498#:~:text=Dengue%20is%20not%20endemic%20in,%2C%20Italy%2C%20Portugal%20and%20Spain.
- Aedes invasive mosquitoes - current known distribution: October 2023. European Centre for Disease Prevention and Control https://www.ecdc.europa.eu/en/publications-data/aedes-invasive-mosquitoes-current-known-distribution-october-2023 (2023).
- Prudhomme, J. et al. The native European mosquito species can transmit chikungunya virus. Emerg. Microbes Infect. 8, 962–972 (2019).
- LaTourrette, K. & Garcia-Ruiz, H. Determinants of Virus Variation, Evolution, and Host Adaptation. Pathogens 11, (2022).
- Autochthonous vectorial transmission of dengue virus in mainland EU/EEA, 2010-present. European Centre for Disease Prevention and Control https://www.ecdc.europa.eu/en/all-topics-z/dengue/surveillance-and-disease-data/autochthonous-transmission-dengue-virus-eueea (2023).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



