
Submitted:
04 July 2024
Posted:
05 July 2024
You are already at the latest version
Abstract
Background and Objectives: To analyze survival in peritoneal and hemodialysis patients using chest radiography and biochemical parameters, determine dialysis etiologies and common mortality causes, reveal prognostic factors, and contribute to clinical practice. Materials and Methods: This retrospective cohort study was based on the analysis of data from 33 peritoneal dialysis and 37 hemodialysis patients who were followed and treated in our hospital between October 2018 and February 2020. Chest X-ray measurements (cardiothoracic index, pulmonary vascular pedicle width, right pulmonary artery diameter, diaphragmatic height) and biochemical parameters (urea, albumin, creatinine, parathormone, ferritin, hemoglobin, arterial blood gas, potassium) were analyzed to assess their impact on survival. Statistical analyses were performed using the Shapiro-Wilk, Wilcoxon signed rank test, Mann-Whitney U test, McNemar test, Kaplan-Meier survival analysis, Cox regression analysis, Spearman correlation test, Phi test, and ROC analysis. Results: The most common etiologies of dialysis were hypertension, type 2 diabetes mellitus, and urogenital disorders. The most common cause of death in peritoneal dialysis patients was peritonitis (38.5%), while in hemodialysis patients, it was cardiovascular diseases (47.4%). In chest X-ray measurements, pulmonary vascular pedicle width (p=0.003) and pulmonary artery diameter increased significantly (p=0.002) in hemodialysis patients, while pulmonary vascular pedicle width (p=0.028) and diaphragmatic height (p=0.004) increased significantly in peritoneal dialysis patients. No significant difference was found between the two groups in terms of biochemical parameters. Kaplan-Meier survival analysis showed that there was no significant difference in survival between peritoneal dialysis and hemodialysis methods (P>0.05). Significant correlations were found between both radiologic status and clinical status and between intact parathormone levels and pulmonary vascular pedicle width (p=0.016, p=0.024). In Cox regression analysis, age, intact parathormone levels, iPTH/PVPW ratio, and clinical status were found to be factors affecting survival (p
Keywords:
Peritoneal dialysis
; Hemodialysis
; Etiology
; Mortality
; Survival
; Chest radiography
1. Introduction
Chronic kidney disease (CKD) is defined as kidney damage that persists for at least 3 months or a glomerular filtration rate (GFR) below 60 ml/min/1.73 m² and the number of people diagnosed with CKD is increasing worldwide [1]. Therefore, it is a global public health problem. End-stage renal failure (ESRF) is the last stage of CKD, in which people with a GFR below 15 ml/min/1.73 m² require renal replacement therapies (RRT) to sustain their lives [2]. Hemodialysis (HD), Peritoneal dialysis (PD) and kidney transplantation are the most common RRT methods [3]. The prevalence of ESRD is projected to increase further in the coming years due to the increasing elderly population due to longer life expectancy and the increasing prevalence of type 2 diabetes mellitus and hypertension. According to the European Renal Association - European Dialysis and Transplantation Association (ERA-EDTA) annual report published in 2017, 83,311 new patients started RRT across Europe in 2016. By the end of the same year, the total number of patients requiring this treatment reached 564,638 [4]. Another study in 2015 estimated that by 2030, the number of people who will need RRT for ESRD will reach 5.4 million worldwide [5]. Another study predicted that CKD In 2040, it is projected to be the fifth most common cause of death worldwide [6]. These findings show the importance of both taking preventive measures for kidney health and increasing access to RRT.
HD is the most commonly used method of RRT [7]. However, the choice of RRT modality is usually made by the physician and the patient, taking into account various factors. Most studies have shown that survival rates are similar between HD and PD [8]. Routine chest radiographs in PD and HD patients play a critical role in long-term complication management by enabling early detection of pulmonary edema, cardiomegaly, pleural effusion and pulmonary infections. It also allows monitoring of pathologic changes in the lung parenchyma and conditions such as chronic obstructive pulmonary disease. By enabling the calculation of the cardiothoracic index (CTI), it helps to identify early signs of cardiovascular complications such as heart failure and vascular calcifications. Thus, treatment strategies can be guided in a timely and accurate manner [9,10,11]. PD and HD patients are routinely followed up with various biochemical parameters to monitor the efficacy of dialysis treatment, to monitor critical clinical information such as fluid balance and nutritional status, and to prevent possible complications. These parameters include serum electrolyte levels (sodium, potassium, calcium, phosphorus), urea and creatinine levels, albumin and total protein, hemogram, ferritin and parathormone (PTH) [12].
In these patients, understanding the risk factors is crucial for predicting survival time. Decreased renal function in HD patients leads to accumulation of uremic toxins. Increased levels of uremic toxins impair endothelial cell function and trigger inflammation, oxidative stress and vascular calcification processes, leading to cardiovascular diseases. Therefore, the primary cause of death in HD patients is cardiovascular disease [13]. In PD patients, infections and complications caused by infections have been accepted as the primary cause of death due to the constant connection of the peritoneal catheter with the external environment [14].
Survival analysis with chest radiography and routine biochemical parameters in PD and HD patients is of great importance to identify prognostic factors in these patients. These analyses provide clinicians with the opportunity to develop individualized treatment strategies tailored to the needs of patients, intervene early in treatment and improve long-term survival rates. However, there is no study in the current literature comparing and analyzing chest radiographs and routine biochemical parameters of PD and HD patients.
The aim of this study is to fill this gap in the literature and to contribute to clinical practice by analyzing survival in PD and HD patients with chest radiography and routine biochemical parameters and to reveal the prognostic factors in this patient group.
2. Materials and Methods
2.1. Study Design and Participants
This study is a retrospective cohort study in which the data of 33 PD and 37 HD program patients who were followed and treated in our hospital between October 2018 and February 2020 [chest radiography (once every 6 months for HD patients; once a year for PD patients), urea, albumin, creatinine, PTH, ferritin, hemoglobin, arterial blood gas, potassium, phosphate] were examined and the effect on survival was investigated. The data of HD patients enrolled in the HD unit of our hospital and PD patients (a total of 70 patients) who were followed up in the outpatient clinic of our hospital were retrospectively analyzed. Data were obtained from our hospital automation system, patients’ files and e-nabız information system. The dialysate calcium concentration used in HD patients is 1.25 to 1.50 mmol/L. PD patients included continuous peritoneal dialysis and ambulatory peritoneal dialysis patients.
For this study, patients who were previously diagnosed with ESRD based on clinical, radiologic and laboratory data and Clinical Practice Guidelines for the Evaluation and Management of CKD (KDIGO), who received PD or HD treatment for at least 1 month, whose GFR was below 15 ml/min/1.73 m², with complete data for October 2018 and February 2020, with monthly kt/v between 1.2 and 1.4 for patients receiving HD treatment and weekly kt/v between 1.7 and 2.0 for patients receiving PD treatment, aged 18 years and older were included in the study [15,16]. Patients with incomplete data, patients whose kt/v did not meet the adequacy criteria for dialysis, patients with parathyroidectomy and patients under 18 years of age were excluded from the study.
2.2. Lung Radiograph Measurement Calculations
Measurements for the evaluation of chest radiographs, CTI, heart width, pulmonary vascular pedicle width, pulmonary artery diameter, pulmonary redistribution, diaphragm height and diaphragm width are shown in Figure 1. CTI is the ratio calculated by dividing the widest diameter of the heart by the widest internal diameter of the chest cavity. For this measurement, 0.42 and 0.50 were considered normal values. Above 0.50 was defined as cardiomegaly [17]. Pulmonary vascular pedicle width (PVPW) is used to detect heart failure and volume overload. It was measured as the distance from the outer edge of the aortic arch (just below the upper border of the left main pulmonary artery) to the outermost border of the right main pulmonary artery. PVPW < 70 mm was considered normal [18]. Right pulmonary artery diameter is used to detect pulmonary hypertension, right heart failure and volume overload. The right pulmonary artery was measured closest to the midline of the pulmonary hilus. Right pulmonary artery diameter < 17 mm was considered normal [19]. Normal diaphragmatic height was generally considered to be 1.5-2.5 cm on the right and 1.0-2.0 cm on the left. This measurement is used to assess the functional status of the lungs and diaphragm. Pulmonary redistribution is the redistribution of blood flow from the lower lobes to the upper lobes of the lungs, where it is usually more concentrated. It becomes evident in diseases such as heart failure, fluid overload and pulmonary hypertension. Other lung findings evaluated are pleural fluid, pleural thickness, alveolar infiltration, aortic calcification, atelectasis. However, these parameters were not measured. Their presence or absence on chest radiography was taken into consideration. The acceptance criteria for radiologic status were as follows, improved; Reduction in the diameter of CTI and PVPW, improvement/reduction in pleural fluid, improvement in parenchymal findings (interstitial and alveolar), Stable; no change in any of these, Deterioration; no improvement in any of these. Clinical Status improved: In dialysis patients, improvement in symptoms (fatigue, muscle cramps...), improvement in laboratory results (e.g., ca, p, serum creatinine, urea...), improvement in blood gas results; Stable; no change in any of these; Deterioration; no improvement in any of these.
2.3. Ethical Approval
For this study, study permission was obtained from the scientific research ethics committee of our university with the decision number TÜTF-BAEK 2020/174 dated 04/05/2020. Written consent was obtained from the participant, A. S., for the use of the chest X-ray image in this study.
2.4. Statistical Analysis
Results were expressed as mean ± Std.Deviation or number (%). The conformity of quantitative data to normal distribution was examined by Shapiro Wilk test. Since the quantitative data did not conform to normal distribution, non-parametric test methods were used. Descriptive statistics were used for etiologic distribution of dialysis patients. Chi-Square test and Fisher’s Exact Test were used to determine the differences in the causes of death between peritoneal dialysis and HD groups. Wilcoxon signed rank test was used to compare diaphragmatic height, pulmonary artery width, vascular pedicle width, heart size and cardiothoracic ratio at baseline and 17 months later in PD and HD groups.
Mann Whitney U test was used to compare the differences in diaphragmatic height, pulmonary artery width, pulmonary vascular pedicle width, heart size and cardiothoracic ratio between PD and HD groups at baseline and after 17 months.
McNemar test was used to compare the presence of cardiomegaly, redistribution, interstitial patern, pleural fluid, pleural thickness, alveolar infiltration and normal variables at baseline and 17 months in both PD and HD groups.
Kaplan-Meier Survival Analysis (Log-rank test) was used to analyze the survival of peritoneal and HD patients. Univariate cox regression analysis was used to examine the effects of possible factors on survival based on 2018 values. Multivariate Cox regression analysis was performed for parameters with P<0.05. The correlation between iPTH level and chest radiograph findings was analyzed by Spearman test, and the correlation between radiological status and clinical status was analyzed by Phi test. The results showed that there was a significant correlation between both radiologic status and clinical status and between iPTH and PVPW. From these correlations, backward multivariate Cox regression analysis was applied to evaluate the effect of iPTH and PVPW on survival. In line with the significant correlation found as a result of the analysis, the power of iPTH/PVPW ratio in predicting mortality was evaluated by ROC curve. SPSS 20.0 statistical package program was used for data analysis (IBM SPSS Statistics for Windows. Version 20.0. Armonk. NY: IBM Corp.). P<0.05 was accepted as the limit of statistical significance.
3. Results
How the chest radiograph measurement calculations used in the study were performed is shown in Figure 1.
The study included 33 PD patients and 37 HD patients. The mean age of PD patients was 52.1 ± 9.4 years and 63.6% were female. The mean age of HD patients was 59.9 ± 16.9 years and 62.2% were female. The distribution of etiologic causes in a total of 70 dialysis patients is shown in Table 1. Accordingly, the most common causes of dialysis were hypertension (48.6%) and type 2 diabetes mellitus (27.1%).
The rate
The distribution of causes of death in PD and HD patients is compared in Table 2.
The data revealed that the most common causes of death differed for both dialysis types. The highest cause of death in PD patients was peritonitis with 38.5%, while the highest cause of death in HD patients was other cardiovascular causes with 47.4%.
Pearson Chi-Square test results showed that there was a significant association between PD and HD groups in terms of causes of death (p=0.030). However, since the expected frequency was less than 5 in 93.8% of the cells, Fisher’s Exact Test was applied. Fisher’s Exact Test results also confirmed that there was a statistically significant difference between dialysis types in terms of causes of death (p=0.008). Fisher’s Exact Test results showed that the rate of death due to peritonitis was significantly higher in the PD group (p=0.005) and the rate of death due to other cardiovascular causes was significantly higher in the HD group (p=0.013). No significant difference was found between the groups in terms of other causes of death (Table 2, p>0.05).
In the PD group, diaphragmatic height and vascular pedicle width at 17 month were significantly higher than baseline values (p=0.004 and p=0.028, respectively). There was no significant difference between the baseline and at 17 month values of pulmonary artery width, heart size and cardiothoracic ratio (p>0.05 for all). In the HD group, the at 17 month values of pulmonary artery width and pulmonary vascular pedicle width were significantly higher than the baseline values (p=0.002 and p=0.003, respectively). There was no significant difference between the baseline and at 17 month values of diaphragmatic height, heart size and cardiothoracic ratio (p>0.05 for all; Table 3).
The diaphragmatic height difference of the PD group was significantly higher than that of the HD group (p=0.016). There was no significant difference between the PD and HD groups in terms of pulmonary artery width, vascular pedicle width, heart size, cardiothoracic ratio and biochemical parameters at baseline and 17 months (p>0.05 for all ; Table 3).
According to McNemar test, there was no significant difference in the changes of cardiomegaly, redistribution, interstitial pattern, pleural fluid, pleural thickness, alveolar infiltration variables at baseline and 17 months in both PD and HD groups (p>0.05 for all; Table 4).
Kaplan-Meier survival analysis was used to analyze the survival rates of PD and HD patients according to total dialysis time. Figure 2 shows how the survival rates changed over time for both dialysis modalities.
No significant difference in survival rates was observed between the two dialysis modalities. Although the survival rate in the HD group appeared to be lower in earlier periods, this difference was not statistically significant (p = 0.462). In both groups, the survival rate decreased with increasing dialysis duration. However, no clear method superiority emerged.
The mean survival time was 12.4 years in PD patients and 13.2 years in HD patients (p=0.462). The total duration of dialysis was 9.0 ± 4.5 in survivors and 7.5 ± 4.8 in deceased patients (p=0.067).
The effects of possible factors on survival were analyzed by univariate cox regression analysis and the results are shown in Table 5.
Univariate cox regression analysis revealed that age, albumin, hemoglobin, ferritin, potassium, intact parathyroid hormone (iPTH) levels and clinical status had significant effects on survival in PD and HD patients, while radiologic status had a borderline significant effect on survival risk. In the Ex group, mean age (Table 5, p=0.016) was higher, albumin level (Table 5, p=0.005) was lower, hemoglobin level (Table 5, p=0.04) was lower and ferritin level (Table 5, p=0.047) was higher. In addition, potassium level (Table 5, p= 0.035) was significantly lower in the ex group, while iPTH level (Table 5, p=0.013) had a statistically significant effect on survival. iPTH levels were lower in the ex group. Clinical status had a significant effect on survival (Table 5, p=0.003). This result indicates that clinical status has a positive effect on survival. Patients with radiologic deterioration had a higher survival risk than patients with stable or improving radiologic status (Table 5, p=0.055), with borderline statistical significance. No statistically significant difference was found between the other parameters (p > 0.05 for all).
The effects of the parameters that were significant in univariate cox regression analysis on survival were evaluated by multivariate cox regression analysis and the results are shown in Table 6.
According to multivariate cox regression analysis, the effects of age, albumin, hemoglobin, ferritin, iPTH, potassium levels and clinical status on survival were analyzed. The effects of age, iPTH levels and clinical status on survival were statistically significant (Table 6, P < 0.05). Other parameters were not significant (P > 0.05)
Spearman’s correlation test was performed to evaluate the correlation between iPTH level, which was found to be significant in the multivariate Cox regression analysis, and chest X-ray findings that may have an effect on survival. The results of the analysis are shown in Table 7. The relationship between radiologic status and clinical status was evaluated with the Phi test and the results are shown in Table 8.
These results showed a statistically significant correlation between radiologic status and clinical status (Tablo 8; Phi, 0.287; p = 0.016). On the other hand, there was a significant correlation between iPTH level and PVPW (Tablo7; p = 0.024). No significant correlation was found between the other variables (P > 0.05). Therefore, we calculated iPTH/PVPW and analyzed its effect on survival by multivariate cox regression analysis. The results are shown in Table 9.
Multivariate Cox regression analysis revealed that age, iPTH/PVPW and clinical status had a statistically significant effect on survival (Table 9, P < 0.05).
Receiver Operating Characteristic (ROC) analysis was performed to evaluate the effectiveness of iPTH/PVPW in mortality prediction. The results of the analysis are shown in Figure 3.
According to the ROC curve obtained, a certain accuracy in mortality prediction was achieved with the iPTH/PVPW combination. Although the area under the curve value was not statistically significant (AUC=0.606; p > 0.05), the sensitivity value for the iPTH/PVPW ratio at the cut-off value of ≤6.8 was 71.9% and the specificity value was 56.8%.
4. Discussion
In this study, we performed a retrospective comparative analysis of chest radiographs and routine biochemical parameters of PD and HD patients and analyzed these results in terms of survival in dialysis patients and prognostic parameters. Such a study is not available in the literature and our study fills this gap. Our study revealed that there was no significant difference in survival between PD and HD patients. Furthermore, our study revealed a significant correlation between radiologic status and clinical status. Early detection and management of radiological findings such as CTI, redistribution, alveolar infiltration, interstitial pattern, pleural fluid, cardiomegaly, aortic calcification due to vascular calcium deposition, diaphragmatic elevation and atelectasis, have shown to positively affect survival. These results emphasize that prospective close monitoring of the health status of patients under dialysis treatment, especially the management of cardiopulmonary complications, is important in improving survival. Age, PTH level, IPTH/PVPW and clinical status were determined as the most important prognostic factors affecting survival.
In scientific and clinical applications, the main goal of prediction is to accurately estimate the risk of an outcome using a combination of several predictors. The final predictive model created in this process is based on data relationships that are often statistically significant, but not necessarily causal [20]. Data selection plays an important role in determining the results of survival analysis of ESRD patients. Therefore, the use and identification of routine chest X-ray findings and routine biochemical parameters of dialysis patients is of great importance as well as causality analysis [21].
When the etiology of 70 dialysis patients was analyzed in our study, the most common causes were hypertension with 48.6%, type 2 diabetes mellitus with 27.1%, and urogenital disorders such as vesicourethral reflux and polycystic kidney with 11.4% (Table 1). Our findings are consistent with the existing literature. In a 2016 study, it was shown that uncontrolled hypertension may lead to progressive kidney damage and cause ESRD and is one of the important reasons for dialysis treatment [22].
In another study, hypertension was found to be a significant contributor to the development of CKD and progression of CKD to ESRD in patients and 90% of patients with CKD were affected by hypertension [23]. Diabetic nephropathy is a common microvascular complication of type 2 diabetes mellitus and usually progresses to ESRD requiring dialysis. A recent study examining the etiologic distribution of CKD showed that type 2 diabetes mellitus remains one of the most important causes of ESRD [24].
Urogenital disorders have been reported to cause permanent kidney damage and contribute to dialysis patient burden by causing impairment in renal function from childhood onwards. The association of vesicourethral reflux, which is a consequence of urogenital disorders, with CKD has been investigated in a large cohort study and it has been shown that vesicourethral reflux significantly increases the risk of developing CKD in children [25]. These results emphasize the importance of early diagnosis and treatment of hypertension, type 2 diabetes mellitus and urogenital disorders in reducing dialysis patient burden. At the same time, effective management of these diseases is very important for the survival of patients who develop ESRD, receive dialysis treatment and have one of these chronic disease diagnoses.
In our study, peritonitis was found to be the most common cause of PD-related deaths, accounting for 38.5% (Table 2). This result is consistent with a study in which 267 PD patients were included and PD-related peritonitis was investigated [26]. The most common causes of death in HD patients were cardiovascular causes (47.4%) and myocardial infarction (10.5%) (Table 2), which is in line with the recent literature which found that 57.9% of HD patients suffered from cardiovascular diseases and almost half of HD patients died due to cardiovascular diseases [27]. Accordingly, regular patient follow-up and infection management, along with continuous patient education and compliance with strict hygiene rules, may contribute to improved survival rates in PD patients. In HD patients, identification, regular follow-up and management of cardiovascular risk factors are important in terms of contributing to increased survival rates for this group.
When the at 17 month changes in the chest radiographs of PD patients were analyzed, it was found that PVPW and diaphragmatic height increased significantly (Table 3). In PD, the peritoneum, which is a serous membrane consisting of visceral and parietal leaves with a surface area of approximately 1-2 m2 in adults, is used [28]. During PD, dialysate is delivered daily through a catheter into the peritoneal cavity, which is performed on a daily basis, and due to inadequate ultrafiltration, a certain amount of fluid accumulates in the peritoneal cavity each time, resulting in volume overload. This results in increased pressure in the pulmonary circulation and dilation of the pulmonary vascular pedicle. At the same time, hypertension due to increased volume and heart failure also contribute to the increase in PVPW [29]. Dialysate fluid introduced into the peritoneal cavity increases intra-abdominal pressure and elevates the diaphragm [30]. Our findings are consistent with the existing literature.
When chest radiographs of HD patients were compared 17 months apart, it was found that PVPW and pulmonary artery diameter increased significantly (Table 3). HD is usually administered in treatment sessions 2-3 times a week, each lasting at least 4 hours. Between these sessions, patients are expected to pay attention to fluid intake and interdialytic weight gain should not exceed 4-4.5% of their dry weight [31]. If patients do not pay attention to fluid intake, volume overload occurs, resulting in increased pulmonary artery pressure and enlargement of the pulmonary vascular pedicle. Patients may develop heart failure due to chronic volume overload, which increases pulmonary artery pressure and leads to enlargement of both the pulmonary vascular pedicle and pulmonary artery diameter. Arterio-venous fistulas used in HD patients increase pulmonary artery pressure by increasing cardiac output. For all these reasons, pulmonary hypertension is also common in HD patients. And this is seen as an increase in PVPW and pulmonary artery diameter on chest radiography [32]. Our results are in parallel with these findings reported in the literature. The urea, albumin, ferritin, iPTH, arterial blood gas, hemoglobin, creatinine and potassium values of HD and PD patients at baseline and 17 months later were compared both within and between groups and no significant difference was found (Table 3; P > 0.05). The main reason for this result is that both HD and PD show similar efficacy in the removal of metabolic wastes and maintenance of electrolyte balance. Other important factors are the optimal level of dialysis adequacy of the patients since the start of our study (October 2018), implementation of current treatment protocols, and control of nutrition and drug therapy. These factors led to stable biochemical parameters and minimal changes throughout the duration of the study, thus no significant differences were observed.
In our study, chest radiographic findings of PD and HD patients were compared. A statistically significant difference was found between the two groups in terms of diaphragmatic height (Table 3; P=0.016). This may be related to the fact that PD and HD applications are different techniques [30]. On the other hand, no significant difference was observed between PD and HD patients in terms of cardiomegaly, redistribution, interstitial pattern, pleural fluid, pleural thickness and alveolar infiltration variables on chest radiographs taken 17 months apart (Table 4; P > 0.05). Furthermore, it is likely that both HD and PD patients experienced similar rates of pulmonary redistribution due to increased pulmonary venous pressure due to fluid imbalance. Moreover, both treatment modalities cause interstitial edema and thickening of the lungs, predisposing to the formation of an interstitial pattern on chest radiographs. Therefore, since similar etiologic factors lead to similar chest X-ray findings, no significant difference was found between these parameters.
In our study, total dialysis times and survival rates for HD and PD methods were analyzed; no significant difference was found between them in terms of survival (Figure 2, P = 0.462). In a prospective cohort study conducted in 2023 with 65 PD and HD patients matched by propensity score matching method, patients were followed up for survival and no significant difference was found between the two dialysis methods in terms of survival [33]. This result is consistent with our findings.
Univariate Cox regression analysis revealed that age, serum albumin, hemoglobin, ferritin, iPTH and potassium levels and clinical status parameters had significant effects on survival (Table 5; P < 0.05 for all).
PTH is an 84 amino acid protein that targets various organs such as bone, kidney and intestine. PTH is also known as a uremic toxin; serum levels increase as CKD progresses and have many systemic side effects, including cardiovascular disease [34,35,36]. iPTH refers to the biologically active PTH molecule that detects full-length 1-84 bio-PTH and 7-84 PTH fragments [37]. iPTH tests accurately assess the activity of the parathyroid gland in patients with kidney disease and dialysis by measuring the active portion of parathyroid hormone. Conventional PTH tests can overestimate results by measuring biologically inactive PTH fragments, so iPTH tests give more specific and accurate results.
It has been shown that a steady increase in PTH levels occurs as GFR starts to decrease in Chronic Kidney Patients [38]. In patients with ESRD, PTH levels are frequently monitored to assess parathyroid function. This is necessary to manage disorders of bone and mineral metabolism.
Increased iPTH levels in dialysis patients are closely associated with secondary hyperparathyroidism. In the kidneys, 25-hydroxy vitamin D is converted to its active form 1,25-dihydroxy vitamin D by the action of PTH. The resulting 1,25-dihydroxy vitamin D suppresses PTH production through a negative feedback mechanism. FGF-23 production in bone osteocytes is controlled by phosphate, 1,25-dihydroxy vitamin D and PTH. Increased FGF-23 levels decrease PTH production by acting on the FGFR1-αKlotho receptor complex in parathyroid glands [39]. However, in ESRD, inhibitory feedback mechanisms become inadequate due to down-regulation of Ca2+ sensitive, vitamin D and FGF23 / Klotho receptors in the parathyroid gland. In addition, end organ ineffectiveness of PTH due to ESRD also contributes to the gradual increase in PTH synthesis and release [40]. Parathyroid glands undergo nodular hyperplasia as a result of negative feedback mechanisms that are constantly stimulated and disrupted to maintain calcium, phosphate and vitamin D balance. Secondary hyperparathyroidism develops. Parathyroidectomy is required in severe and medically refractory patients [41,42,43,44]. In our study, iPTH levels were found to be lower in the ex group compared to the survivors (Table 5). This may be related to changes in PTH metabolism in critical illness or severe inflammation, impaired parathyroid function due to malnutrition and poor general health, and excessive suppression of iPTH due to overuse of drugs that lower iPTH levels such as calcimimetics, vitamin D analogs and phosphate binders. In particular, a 2021 study emphasized that the use of vitamin D analogs is not neutral in the development of hypercalcemia [45]. This finding suggests that vitamin D analogs may cause suppression of PTH release, increasing the risk of hypercalcemia. Considering all these factors, it can be concluded that the lower iPTH levels in the ex group may be due to a multifactorial effect, especially the overuse of iPTH-suppressing drugs. In a study conducted in 2017 and similar to our study, the relationship between iPTH levels of 115 HD patients within 1 year and mortality was investigated and it was found that low iPTH levels were associated with mortality [46]. The results of our study are consistent with these literatures.
Control of albumin, ferritin, hemoglobin, potassium levels and clinical status have a positive impact on survival time. These findings emphasize that close monitoring and management of biochemical and clinical parameters is vital to improve patient prognosis.
Multivariate Cox regression analysis was used to evaluate the independent effects of age, albumin, hemoglobin, ferritin, iPTH, potassium levels and clinical status on survival. Age, iPTH levels and clinical status were found to be prognostic factors affecting survival (Table 6). Increasing age was found to negatively affect survival (Table 6, p = 0.007). Studies have shown that survival of dialysis patients decreases with age due to the emergence of new comorbidities (infection, cardio vascular diseases) or deterioration of existing morbidities (hypertension, type 2 diabetes mellitus), malnutrition, decrease in physiological reserves, decrease in muscle mass and functions due to decrease in physical activities, mood disorders, difficulties in adaptation to treatment and decrease in social life support [47,48]. Our results are consistent with these literatures. It was found that a decrease in iPTH levels negatively affected survival (Table 6, p < 0.040). This result contradicts some studies in the literature. PTH levels are not a clear indicator of mortality in dialysis patients. Although only long-term studies have found that increased PTH levels are associated with mortality, the specific PTH values for this association are quite different [49,50,51]. Molecules that affect PTH such as calcium, phosphorus and vitamin D show a more consistent relationship with mortality. Increases in calcium levels above 10.5 mg/dL and, more importantly, increases in calcium and phosphorus together and exceeding the limit value (Ca*P) of 55 mg²/dL² increase the risk of calcification, especially in vessels and soft tissues. Due to calcified vascular structures, vascular walls harden, their elasticity decreases and this increases the risk of mortality by increasing the development of cardiovascular events, myocardial infarction and cerebrovascular events [52,53]. Keeping PTH levels under control at optimum levels in dialysis patients is an important goal for improving survival rates. However, while achieving this control, drugs that lower iPTH levels are used. Over time, changes in iPTH levels can occur for reasons such as patients not following their diet. In the COSMOS study conducted in 2015, higher iPTH increase in patients with low baseline iPTH levels was associated with lower mortality [54]. In another study conducted in 2015 and similar to our study, low iPTH levels were found to be associated with high mortality [46]. Although both studies differ from our study in that they included only HD patients and focused on iPTH levels, our results are compatible. A large cohort study conducted in 2017 to determine mortality rates only in HD patients found that low and intermediate iPTH levels (<75 pg/ml, 75-150 pg/ml) were associated with a high mortality risk. However, high iPTH levels (300-600 pg/ml or more) did not show an increased mortality risk [55].
In our study, there was a correlation between radiologic status and clinical status (Table 8, Phi, 0.287, p = 0.016). This correlation suggests that evaluating both types of status together will increase survival. Spearman’s correlation test to evaluate the relationship between iPTH levels and chest X-ray findings showed a significant correlation between iPTH levels and PVPW (Table 7, p = 0.024). This finding suggests that there may be a relationship between iPTH levels and the width of pulmonary vascular structures.
Multivariate Cox regression analysis revealed that iPTH/PVPW ratio had a significant negative effect on survival [Table 9, β= - 0.073, p=0.035, HR=0.930, 95% CI (0.869 - 0.995)]. This correlation indicates that iPTH/PVPW has a significant and positive effect on survival. Each unit increase in this ratio increases the probability of survival by approximately 7.5%. This finding suggests that a higher iPTH/PVPW ratio is associated with longer expected survival in dialysis patients. This emphasizes the importance of the balance between bone metabolism and vascular health and may offer a potential therapeutic target. It also suggests that the iPTH/PVPW ratio may be a clinically important prognostic indicator and should be considered in predicting survival or mortality. To further explore this relationship, we evaluated the potential of the iPTH/PVPW ratio to predict mortality. ROC curve analysis revealed that the iPTH/PVPW ratio performed moderately well in predicting mortality (AUC=0.606, p > 0.05), although not statistically significant, which may be due to the small size of our study group. Using ≤6.8 as cut-off value, the sensitivity and specificity were 71.9% and 56.8%, respectively. These findings suggest that mortality is higher when the iPTH/PVPW ratio is ≤6.8. It is likely to be statistically significant in future studies to be conducted with larger sample groups.
Increased PVPW is closely associated with parameters such as volume overload, pulmonary artery pressure, heart failure, pulmonary edema, vascular stiffness and elasticity. These biological mechanisms suggest that increased vascular stiffness and decreased vascular elasticity may be associated with cardiovascular complications and thus reduced survival. An iPTH/PVPW ratio of less than 6.8 suggests that these vascular complications may be higher and thus associated with higher mortality rates. However, more comprehensive and large-scale studies are needed to establish this relationship more precisely.
The most important limitations of our study are that it was retrospectively designed, conducted in a single center and the sample group was small.
5. Conclusions
This is the first study to evaluate the effects of chest radiography and biochemical parameters on survival in PD and HD patients and aims to contribute to a better understanding of prognostic factors in dialysis patients. Routine radiologic examinations and biochemical monitoring enable clinical follow-up of treatment efficacy. Furthermore, these findings provide information to help develop individualized treatment strategies in the follow-up of dialysis patients.
Prevention of chronic diseases such as hypertension and type 2 diabetes mellitus and effective treatment management in individuals diagnosed with these diseases will play an important role in improving survival. Ensuring infection control and regular patient education in PD patients and regular follow-up for cardiovascular diseases, especially myocardial infarction, in HD patients is a critical factor in improving survival rates.
The results of our study revealed that the combined evaluation of chest radiography findings and biochemical parameters in the management of HD and PD patients is important in terms of improving survival rates. Another important conclusion is that uncontrolled suppression of iPTH levels may increase mortality; therefore, caution should be exercised in the use of drugs while controlling iPTH. Another important conclusion is that calculation of iPTH/PVPW values from chest radiographs and routine biochemical parameters during routine follow-up of PD and HD patients and evaluation of iPTH/PVPW values with other clinical parameters and biomarkers in cases where they are less than 6.8 may increase survival by determining the risks of patients in terms of mortality and monitoring them more closely and carefully.
In future prospective studies and clinical applications, chest radiographs and routine biochemical parameters should be evaluated together. In the management of HD and PD patients, careful control of age and iPTH levels may play a critical role to increase survival rates and iPTH/PVPW may play a critical role to determine mortality risk.
Author Contributions
Conceptualization, N.T.T. and O.N.H.; methodology, N.T.T.; software, N.T.T.; validation, N.T.T. and O.N.H.; formal analysis, N.T.T.; investigation, N.T.T.; resources, N.T.T.; data curation, N.T.T.; writing—original draft preparation, N.T.T. and O.N.H.; writing—review and editing, N.T.T. and O.N.H.; visualization, N.T.T.; supervision, N.T.T and O.N.H.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no funding.
Institutional Review Board Statement
Ethics committee approval for this study was obtained from the Ethics Committee of the Faculty of Medicine of our University with the decision number and protocol code TÜTF-BAEK 2020/174 dated 04/05/2020., and all procedures in this study were performed under the Declaration of Helsinki and its subsequent amendments. Written consent was obtained from the participant, A. S., for the use of the chest X-ray image in this study.
Informed Consent Statement
This study was conducted retrospectively as a file review.
Data Availability Statement
Our study data contain personal information of patients, and therefore, are not available for sharing due to the ‘Personal Data Protection Law’ and ethical reasons.
Acknowledgments
We would like to thank Ahmet Sezgin for his contributions to our study and Necdet Süt and Sedat Üstündağ for their support in conducting this study.
Conflicts of Interest
The authors declare no conflicts of interest
References
- Scott, I.A.; Scuffham, P.; Gupta, D.; Harch, T.M.; Borchi, J.; Richards, B. Going digital: a narrative overview of the effects, quality and utility of mobile apps in chronic disease self-management. Aust. Health Rev. 2018, 44, 62-82. [CrossRef]
- Acosta-Ochoa, I.; Bustamante-Munguira, J.; Mendiluce-Herrero, A.; Bustamante-Bustamante, J.; Coca-Rojo, A. Impact on outcomes across KDIGO-2012 AKI criteria according to baseline renal function. J. Clin. Med. 2019, 8, 1323. [CrossRef]
- Ebrahimi, V.; Khademian, M.H.; Masoumi, S.J.; Morvaridi, M.R.; Ezzatzadegan Jahromi, S. Factors influencing survival time of hemodialysis patients; time to event analysis using parametric models: a cohort study, BMC Nephrol. 2019, 20, 1-9. [CrossRef]
- Thomé, F.S.; Sesso, R.C.; Lopes, A.A.; Lugon, J.R.; Martins, C.T. Brazilian chronic dialysis survey 2017. Braz. J. Nephrol. 2019, 41, 208-214. [CrossRef]
- Liyanage, T.; Ninomiya, T.; Jha, V.; Neal, B.; Patrice, H.M.; Okpechi, I.; Zhao, M.; Lv, J.; Garg, A.X.; Knight, J.; Rodgers, A.; Gallagher, M.; Kotwal, S.; Cass, A.; Perkovic, V. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet 2015, 385, 1975-1982. [CrossRef]
- Wetmore, J.B.; Collins, A.J. Global challenges posed by the growth of end-stage renal disease. Ren. Replace. Ther. 2016, 2, 1-7. [CrossRef]
- Kainz, A.; Berner, C.; Ristl, R.; Simon, A.; Stamm, T.; Zitt, E.; Kramar, R.; Antlanger, M.; Kautzky-Willer, A.; Schmaldienst, S.; Schernhammer, E.; Port, F.K.; Carrero, J.J.; Jager, K.J.; Hecking, M. Sex-specific analysis of haemodialysis prevalence, practices and mortality over time: the Austrian Dialysis Registry from 1965 to 2014. Nephrol. Dial. Transplant. 2019, 34, 1026-1035. [CrossRef]
- Naeem, A.; Ahmed, A.R.; Khan, K.; Khan, M.E.; Ali, B.; Banaras, F. Comparison of patient survival between hemodialysis and peritoneal dialysis among patients eligible for both modalities. J. Popul. Ther. Clin. Pharmacol. 2023, 30, 1773-1778. [CrossRef]
- Gao, N.; Kwan, B.C.; Chow, K.M.; Chung, K.Y.; Leung, C.B.; Li, P.K.; Szeto, C.C. Measurements on the routine chest radiograph as prognostic markers in Chinese peritoneal dialysis patients. Clin. Nephrol. 2011, 76, 16-22. [CrossRef]
- Zandieh, S.; Muin, D.; Bernt, R.; Krenn List, P.; Mirzaei, S.; Haller, J. Radiological diagnosis of dialysis-associated complications. Insights Imaging 2014, 5, 603-617. [CrossRef]
- Degrassi, F.; Quaia, E.; Martingano, P.; Cavallaro, M.; Cova, M.A. Imaging of haemodialysis: renal and extrarenal findings. Insights Imaging 2015, 6, 309-321. [CrossRef]
- Levin, A.; Ahmed, S.B.; Carrero, J.J.; Foster, B.; Francis, A.; Hall, R.K.; Herrington, W.G.; Hill, G.; Inker, L.A.; Kazancıoğlu, R.; Lamb, E.; Lin, P.; Madero, M.; McIntyre, N.; Morrow, K.; Roberts, G.; Sabanayagam, D.; Schaeffner, E.; Shlipak, M.; Shroff, R.; Tangri, N.; Thanachayanont, T.; Ulasi, I.; Wong, G.; Yang, C.-W.; Zhang, L.; Robinson, K.A.; Wilson, L.; Wilson, R.F.; Kasiske, B.L.; Cheung, M.; Earley, A.; Stevens, P.E. Executive summary of the KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease: Known knowns and known unknowns. Kidney Int. 2024, 105, 684-701. [CrossRef]
- Liu, J.; Zhang, H.; Diao, Z.; et al. Epidemiological analysis of death among patients on maintenance hemodialysis: results from the Beijing Blood Purification Quality Control and Improvement Center. BMC Nephrol. 2023, 24, 236. [CrossRef]
- Bitar, W.; Helve, J.; Kanerva, M.; Honkanen, E.; Rauta, V.; Haapio, M., et al. Severe infections in peritoneal dialysis and home hemodialysis patients: An inception cohort study. PLoS One. 2023, 18, e0286579. [CrossRef]
- Chen, C.H.; Teitelbaum, I. Peritoneal dialysis adequacy: a paradigm shift. Kidney Res. Clin. Pract. 2022, 41, 150. [CrossRef]
- Daugirdas, J.T.; Depner, T.A.; Inrig, J.; Mehrotra, R.; Rocco, M.V.; Suri, R.S.; Weiner, D.E.; Greer, N.; Ishani, A.; MacDonald, R.; Olson, C.; Rutks, I.; Slinin, Y.; Wilt, T.J.; Rocco, M.; Kramer, H.; Choi, M.J.; Samaniego-Picota, M.; Scheel, P.J.; Willis, K.; Joseph, J.; Brereton, L. KDOQI clinical practice guideline for hemodialysis adequacy: 2015 update. Am. J. Kidney Dis. 2015, 66, 884-930. [CrossRef]
- Elasan, S.; Yilmaz, O. Cardiothoracic ratio and left ventricular ejection fraction relationship: A meta-analysis study. Saudi Med. J. 2023, 44, 529. [CrossRef]
- Wang, H.; Shi, R.; Mahler, S.; Gaspard, J.; Gorchynski, J.; D’Etienne, J.; Arnold, T. Vascular pedicle width on chest radiograph as a measure of volume overload: meta-analysis. West. J. Emerg. Med. 2011, 12, 426-432. [CrossRef]
- Nguyen, E.T.; Silva, C.I.; Seely, J.M.; Chong, S.; Lee, K.S.; Müller, N.L. Pulmonary artery aneurysms and pseudoaneurysms in adults: findings at CT and radiography. AJR Am. J. Roentgenol. 2007, 188, W126-134. [CrossRef]
- Van Diepen, M.; Ramspek, C.L.; Jager, K.J.; Zoccali, C.; Dekker, F.W. Prediction versus aetiology: common pitfalls and how to avoid them. Nephrol. Dial. Transplant. 2017, 32 (suppl_2), ii1-ii5. [CrossRef]
- Van Geloven, N.; Swanson, S.A.; Ramspek, C.L.; Luijken, K.; van Diepen, M.; Morris, T.P.; Groenwold, R.H.H.; van Houwelingen, H.C.; Putter, H.; le Cessie, S. Prediction meets causal inference: the role of treatment in clinical prediction models. Eur. J. Epidemiol. 2020, 35, 619-630. [CrossRef]
- Olsen, M.H.; Angell, S.Y.; Asma, S.; Boutouyrie, P.; Burger, D.; Chirinos, J.A.; Damasceno, A.; Delles, C.; Gimenez-Roqueplo, A.-P.; Hering, D.; López-Jaramillo, P.; Martinez, F.; Perkovic, V.; Rietzschel, E.R.; Schillaci, G.; Schutte, A.E.; Scuteri, A.; Sharman, J.E.; Wachtell, K.; Wang, J.G. A call to action and a lifecourse strategy to address the global burden of raised blood pressure on current and future generations: the Lancet Commission on hypertension. Lancet, 2016, 388, 2665-2712. [CrossRef]
- Habas, E.; Habas, E.; Khan, F.Y.; Rayani, A.; Habas, A.; Errayes, M.; Farfar, K.L.; Elzouki, A.N.Y. Blood Pressure and Chronic Kidney Disease Progression: An Updated Review. Cureus, 2022, 14, e24244. [CrossRef]
- Xue, M.Y.; Shao, X.; Qin, H.; Yin, P.; Lin, Y.; Wu, J.; Ren, J.; Zheng, Y. Disease burden and epidemiological trends of chronic kidney disease at the global, regional, national levels from 1990 to 2019. Nephron, 2024, 148, 113-123. [CrossRef]
- Lee, S.Y.; Lai, J.N.; Haw, Y.; Chiu, L.T.; Huang, S.M.; Cheng, K.L.; Chew, F.Y. Vesicoureteral reflux is associated with increased risk of chronic kidney disease: A nationwide cohort study. Medicine, 2023, 102, e34867. [CrossRef]
- Nardelli, L.; Scalamogna, A.; Ponzano, F.; Sikharulidze, A.; Tripodi, F.; Vettoretti, S.; Alfieri, C.; Castellano, G. Peritoneal dialysis related peritonitis: insights from a long-term analysis of an Italian center. BMC Nephrol. 2024, 25, 163. [CrossRef]
- Thompson, S.; James, M.; Wiebe, N.; Hemmelgarn, B.; Manns, B.; Klarenbach, S.; Tonelli, M. Cause of death in patients with reduced kidney function. J. Am. Soc. Nephrol. 2015, 26, 2504-2511. [CrossRef]
- Andreoli, M.C.C.; Totoli, C. Peritoneal dialysis. Rev. Assoc. Med. Bras. 2020, 66, s37-s44. [CrossRef]
- Zheng, S.; Auguste, B.L. Five things to know about volume overload in peritoneal dialysis. Can. J. Kidney Health Dis. 2023, 10, 20543581221150590. [CrossRef]
- Almeida, C.P.; Ponce, D.; de Marchi, A.C.; Balbi, A.L. Effect of peritoneal dialysis on respiratory mechanics in acute kidney injury patients. Perit. Dial. Int. 2014, 34, 544-549. [CrossRef]
- Rocco, M.V.; Rigaud, M.; Ertel, C.; Russell, G.; Zemdegs, J.; Vecchio, M. Fluid intake management in maintenance hemodialysis using a smartphone-based application: a pilot study. Kidney Med. 2023, 5, 100703. [CrossRef]
- Alıcı, G.; Waberi, M.M.; Mohamud, M.A.; Bashir, A.M.; Genç, Ö. Pulmonary hypertension among maintenance hemodialysis patients in Somalia: a hospital-based observational study. Egypt. Heart J. 2022, 74, 24. [CrossRef]
- Miyazaki, M.; Sasaki, K.; Nakashima, A.; Takahashi, A.; Ishiuchi, N.; Tamura, R.; Osaki, Y.; Doi, S.; Masaki, T. Comparison of survival rates between incident hemodialysis patients and peritoneal dialysis patients: a 5-year prospective cohort study with propensity score matching. Clin. Exp. Nephrol. 2023, 27, 419-426. [CrossRef]
- Moradi, H.; Sica, D.A.; Kalantar-Zadeh, K. Cardiovascular burden associated with uremic toxins in patients with chronic kidney disease. Am. J. Nephrol. 2013, 38, 136-148. [CrossRef]
- Neves, K.R.; Graciolli, F.G.; dos Reis, L.M.; Graciolli, R.G.; Neves, C.L.; Magalhães, A.O.; Custódio, M.R.; Batista, D.G.; Jorgetti, V.; Moysés, R.M.A. Vascular calcification: contribution of parathyroid hormone in renal failure. Kidney Int. 2007, 71, 1262-1270. [CrossRef]
- Levin, A.; Bakris, G.L.; Molitch, M.; Smulders, M.; Tian, J.; Williams, L.A.; Andress, D.L. Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: results of the study to evaluate early kidney disease. Kidney Int. 2007, 71, 31-38. [CrossRef]
- Kakuta, T.; Ishida, M.; Fukagawa, M. Critical governance issue of parathyroid hormone assays and its selection in the management of chronic kidney disease mineral and bone disorders. Ther. Apher. Dial. 2018, 22, 220-228. [CrossRef]
- Habas, E. S.; Eledrisi, M.; Khan, F.; Elzouki, A.Y. Secondary hyperparathyroidism in chronic kidney disease: pathophysiology and management. Cureus. 2021, 13, e16388. [CrossRef]
- Ben-Dov, I.Z.; Galitzer, H.; Lavi-Moshayoff, V.; Goetz, R.; Kuro-o, M.; Mohammadi, M.; Sirkis, R.; Naveh-Many, T.; Silver, J. The parathyroid is a target organ for FGF23 in rats. J. Clin. Invest. 2007, 117, 4003-4008. [CrossRef]
- Evenepoel, P.; Bover, J.; Torres, P.U. Parathyroid hormone metabolism and signaling in health and chronic kidney disease. Kidney Int. 2016, 90, 1184-1190. [CrossRef]
- Lau, W.L.; Obi, Y.; Kalantar-Zadeh, K. Parathyroidectomy in the management of secondary hyperparathyroidism. Clin. J. Am. Soc. Nephrol. 2018, 13, 952-961. [CrossRef]
- Cunningham, J.; Locatelli, F.; Rodriguez, M. Secondary hyperparathyroidism: pathogenesis, disease progression, and therapeutic options, Clin. J. Am. Soc. Nephrol. 2011, 6, 913-921. [CrossRef]
- Wheeler, D.C.; Winkelmayer, W.C. KDIGO 2017 clinical practice guideline update for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease-mineral and bone disorder (CKD-MBD) foreword. Kidney Int. Suppl. 2017, 7, 1-59. [CrossRef]
- Brandenburg, V.; Ketteler, M. Vitamin D and secondary hyperparathyroidism in chronic kidney disease: a critical appraisal of the past, present, and the future. Nutrients 2022, 14, 3009. [CrossRef]
- Cozzolino, M.; Bernard, L.; Csomor, P.A. Active vitamin D increases the risk of hypercalcaemia in non-dialysis chronic kidney disease patients with secondary hyperparathyroidism: a systematic review and meta-analysis. Clin. Kidney J. 2021, 14, 2437-2443. [CrossRef]
- Villa-Bellosta, R.; Rodriguez-Osorio, L.; Mas, S.; Abadi, Y.; Rubert, M.; de la Piedra, C.; Gracia-Iguacel, C.; Mahillo, I.; Ortiz, A.; Egido, J.; González-Parra, E. A decrease in intact parathyroid hormone (iPTH) levels is associated with higher mortality in prevalent hemodialysis patients. PLoS One 2017, 12, e0173831. [CrossRef]
- Chen, X.; Han, P.; Song, P.; Zhao, Y.; Zhang, H.; Niu, J.; Yu, C.; Ding, W.; Zhao, J.; Zhang, L.; Qi, H.; Shao, X.; Su, H.; Guo, Q. Mediating effects of malnutrition on the relationship between depressive symptoms clusters and muscle function rather than muscle mass in older hemodialysis patients. J. Nutr. Health Aging 2022, 26, 461-468. [CrossRef]
- Sánchez-Tocino, M.L.; Miranda-Serrano, B.; López-González, A.; Villoria-González, S.; Pereira-García, M.; Gracia-Iguacel, C.; González-Ibarguren, I.; Ortíz-Arduan, A.; Mas-Fontao, S.; González-Parra, E. Sarcopenia and mortality in older hemodialysis patients. Nutrients 2022, 14, 2354. [CrossRef]
- Natoli, J.L.; Boer, R.; Nathanson, B.H.; Miller, R.M.; Chiroli, S.; Goodman, W.G.; Belozeroff, V. Is there an association between elevated or low serum levels of phosphorus, parathyroid hormone, and calcium and mortality in patients with end stage renal disease? A meta-analysis. BMC Nephrol. 2013, 14, 1-16. [CrossRef]
- Streja, E.; Wang, H.Y.; Lau, W.L.; Molnar, M.Z.; Kovesdy, C.P.; Kalantar-Zadeh, K.; Park, J. Mortality of combined serum phosphorus and parathyroid hormone concentrations and their changes over time in hemodialysis patients. Bone 2014, 61, 201-207. [CrossRef]
- Al Salmi, I.; Bieber, B.; Al Rukhaimi, M.; AlSahow, A.; Shaheen, F.; Al-Ghamdi, S.M.G.; Al Wakeel, J.; Al Ali, F.; Al-Aradi, A.; Hejaili, F.A.; Maimani, Y.A.; Fouly, E.; Robinson, B.M.; Pisoni, R.L. for the GCC-DOPPS Study Group. Parathyroid hormone serum levels and mortality among hemodialysis patients in the Gulf Cooperation Council countries: Results from the DOPPS (2012-2018). Kidney360 2020, 1, 1083-1090. [CrossRef]
- Ghonimi, T.; Hamad, A.; Fouda, T.; AlAli, F.; Ezzat, M.; Awad, M.; Ibrahim, R.; Amin, M.; Alkadi, M.; Al-Malki, H.A. Cardiovascular calcification in hemodialysis patients: A Qatar-based prevalence and risk factors study. Qatar Med. J. 2024, 1,18. [CrossRef]
- Kim, G.H.; Choi, B.S.; Cha, D.R.; Chee, D.H.; Hwang, E.; Kim, H.W.; Chang, J.H.; Kim, J.K.; Noh, J.W.; Joo, K.W.; Lee, S.C.; Han, S.W.; Kim, S.; Kim, S.W.; Shin, S.K.; Park, W.; Kim, W.; Huh, W.; Kwon, Y.J.; Kang, Y.S. Serum calcium and phosphorus levels in patients undergoing maintenance hemodialysis: A multicentre study in Korea. Kidney Res. Clin. Pract. 2014, 33, 52-57. [CrossRef]
- Fernández-Martín, J.L.; Martínez-Camblor, P.; Dionisi, M.P.; Floege, J.; Ketteler, M.; London, G.; Locatelli, F.; Gorriz, J.L.; Rutkowski, B.; Ferreira, A. Improvement of mineral and bone metabolism markers is associated with better survival in haemodialysis patients: the COSMOS study. Nephrol. Dial. Transplant. 2015, 30, 1542-1551. [CrossRef]
- Li, D.; Zhang, L.; Zuo, L.; Jin, C.G.; Li, W.G.; Chen, J.B. Association of CKD-MBD markers with all-cause mortality in prevalent hemodialysis patients: a cohort study in Beijing. PLoS One 2017, 12, e0168537. [CrossRef]
Figure 1.
Chest radiograph measurements. Orange line: cardio-thoracic index; green line: pulmonary vascular pedicle width; yellow line: right pulmonary artery diameter; blue line: diaphragmatic height; gray arrows: pulmonary redistribution.
Figure 1.
Chest radiograph measurements. Orange line: cardio-thoracic index; green line: pulmonary vascular pedicle width; yellow line: right pulmonary artery diameter; blue line: diaphragmatic height; gray arrows: pulmonary redistribution.
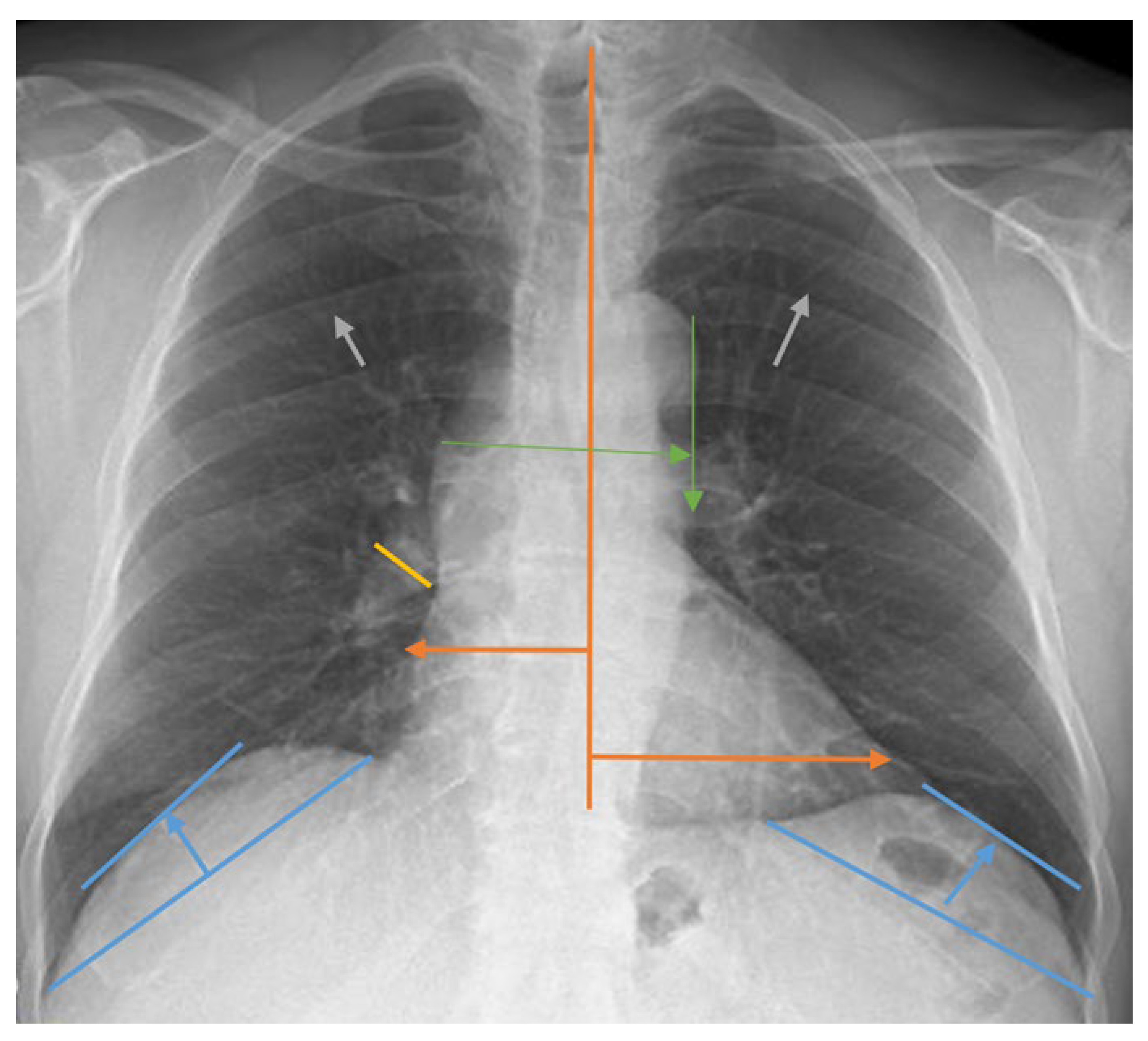
Figure 2.
Survival Rate According to Total Dialysis Duration in PD and HD Patients.
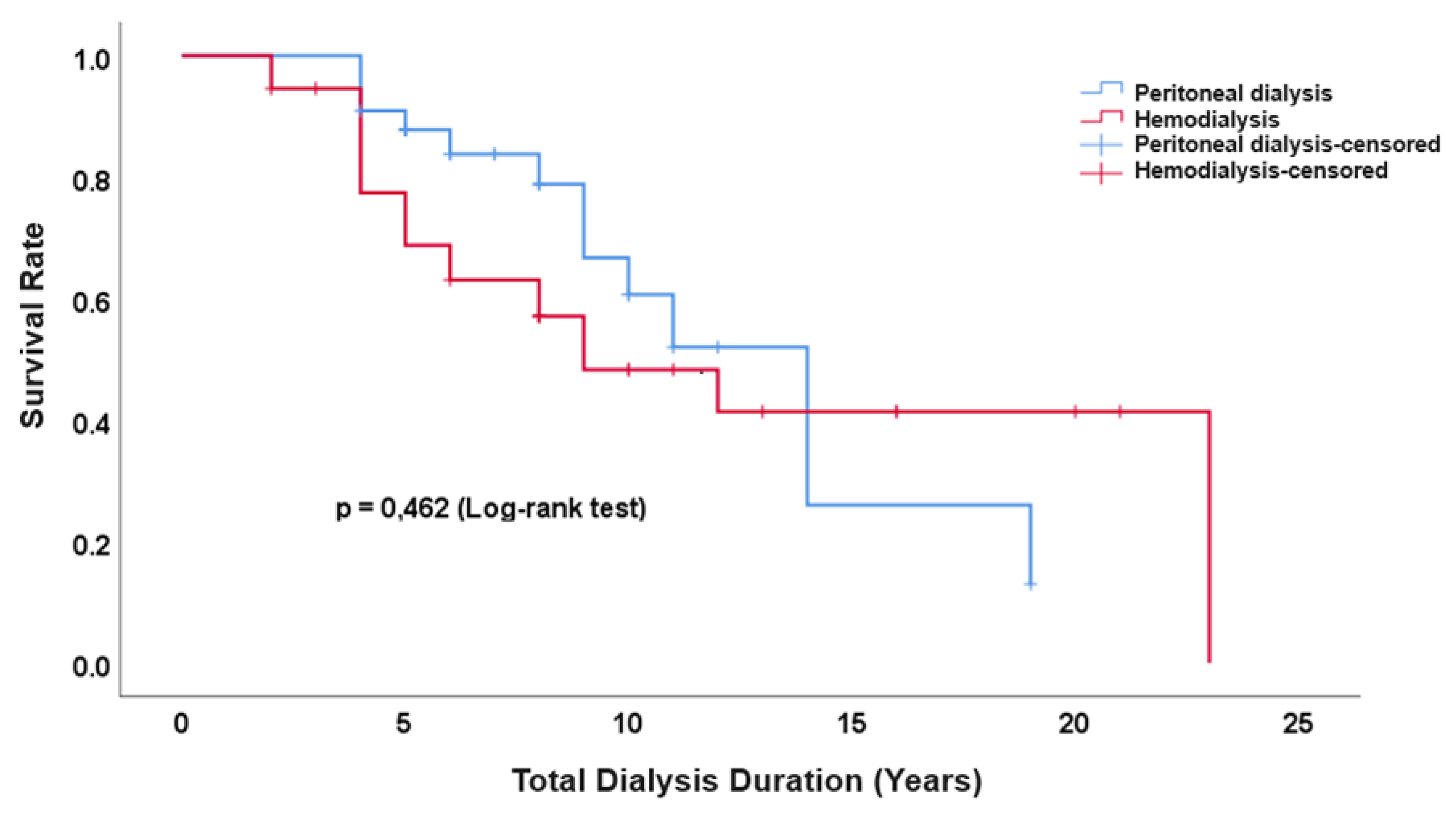
Figure 3.
ROC Curve for iPTH/Pulmonary Vascular Pedicle Width.
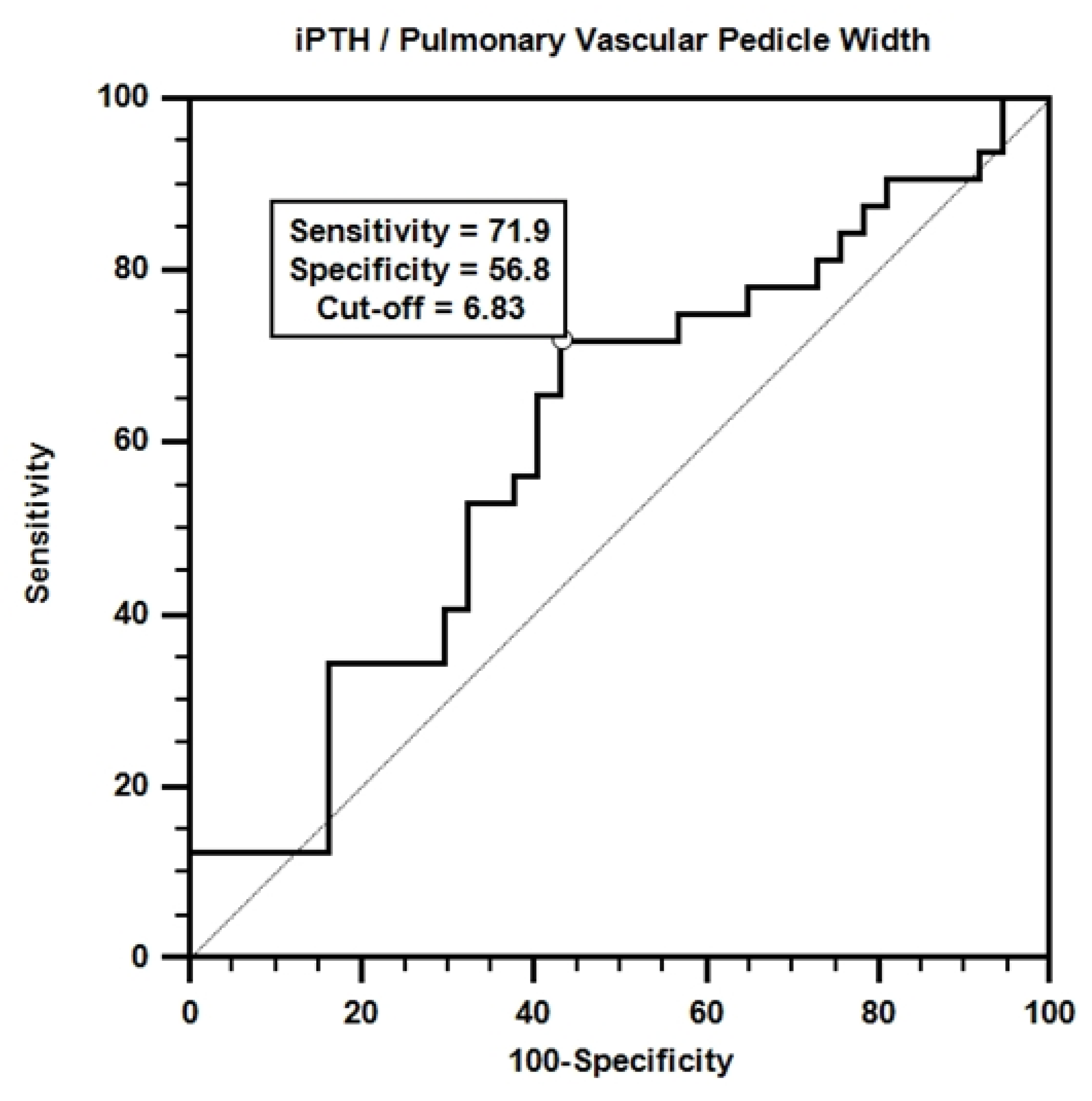

Table 1.
Etiologic Distribution of Dialysis Patients.
| Dialysis Etiology | n | n% |
|---|---|---|
| Type 1 Diabetes Mellitus | 1 | 1.4% |
| Type 2 Diabetes Mellitus | 19 | 27.1% |
| Hypertension | 34 | 48.6% |
| Glomerulonephritis | 6 | 8.6% |
| Urogenital Disorders | 8 | 11.4% |
| Pyelonephritis | 1 | 1.4% |
| Amyloid Nephropathy | 1 | 1.4% |
| Total | 70 | 100% |
Table 2.
Causes of Mortality in Patients Undergoing PD and HD.
| Ex Cause | PD (n=33) | HD (n=37) | P* | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Pneumonia | 1 | 7.7% | 3 | 15.8% | 0.590 |
| Heart failure | 2 | 15.4% | 1 | 5.3% | 0.567 |
| Aortic dissection | 1 | 7.7% | 0 | 0.0% | 0.410 |
| Dialysis complications | 2 | 15.4% | 2 | 10.5% | 1.000 |
| Peritonitis | 5 | 38.5% | 0 | 0.0% | 0.005 |
| Myocardial Infarction | 1 | 7.7% | 2 | 10.5% | 1.000 |
| Other cardiovascular causes | 1 | 7.7% | 9 | 47.4% | 0.013 |
| Malignancy | 0 | 0.0% | 2 | 10.5% | 0.506 |
| Total | 13 | 100% | 19 | 100% | 0.008 |
P*= Fisher’s Exact Test; n (%).
Table 3.
Comparison of diaphragmatic height, pulmonary artery width, pulmonary vascular pedicle width, heart size and cardiothoracic index, biochemical parameters at baseline and after 17 months in PD and HD groups.
Table 3.
Comparison of diaphragmatic height, pulmonary artery width, pulmonary vascular pedicle width, heart size and cardiothoracic index, biochemical parameters at baseline and after 17 months in PD and HD groups.
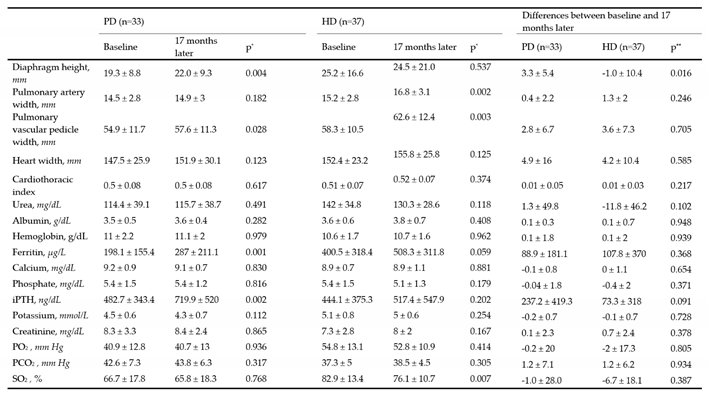
* Wilcoxon signed rank test,** Mann Whitney U test. iPTH, intact parathormone; PO2 , partial oxygen pressure; PCO2 , partial carbon dioxide pressure; SO2 , oxygen saturation.
Table 4.
Comparison of the presence of cardiomegaly, redistribution, interstitial pattern, pleural fluid, pleural thickness, alveolar infiltration variables at baseline and at the end of the first year in PD and HD groups.
Table 4.
Comparison of the presence of cardiomegaly, redistribution, interstitial pattern, pleural fluid, pleural thickness, alveolar infiltration variables at baseline and at the end of the first year in PD and HD groups.
| Baseline | PD (n=33) | HD (n=37) | ||||||
|---|---|---|---|---|---|---|---|---|
| 17 months Later | p* | 17 months Later | p* | |||||
| No | Yes | No | Yes | |||||
| Cardiomegaly | No | 14 | 6 | 0.508 | 11 | 4 | 0.125 | |
| Yes | 3 | 10 | 0 | 20 | ||||
| Redistribution | No | 14 | 1 | 0.219 | 12 | 2 | 1.000 | |
| Yes | 5 | 13 | 1 | 21 | ||||
| Interstitial pattern | No | 18 | 2 | 0.453 | 13 | 4 | 1.000 | |
| Yes | 5 | 8 | 5 | 15 | ||||
| Pleural fluid | No | 20 | 5 | 1.000 | 28 | 5 | 0.219 | |
| Yes | 5 | 3 | 1 | 3 | ||||
| Pleural thickness | No | 26 | 1 | 1.000 | 25 | 0 | 1.000 | |
| Yes | 0 | 6 | 0 | 11 | ||||
| Alveolar infiltration | No | 30 | 2 | 0.500 | 33 | 1 | 1.000 | |
| Yes | 0 | 1 | 2 | 1 | ||||
| Atelectasis | No | 30 | 1 | 1.000 | 37 | 0 | - | |
| Yes | 1 | 1 | 0 | 0 | ||||
*McNemar.
Table 5.
Results of univariate cox regression analysis of the effects of possible factors on survival.
Table 5.
Results of univariate cox regression analysis of the effects of possible factors on survival.
| Survived (n=38) | Ex (n=32) | p | Hazard Ratio (95% Confidence Interval) |
|||
|---|---|---|---|---|---|---|
| Age, year | 52.2 ± 12.7 | 63.5 ± 10.8 | 0.016 | 1.034 (1.006 - 1.062) | ||
| Diaphragm height, mm | 21.6 ± 11.4 | 23.5 ± 16.4 | 0.599 | 1.007 (0.980 - 1.036) | ||
| Pulmonary artery diameter, mm | 14.5 ± 2.8 | 15.3 ± 2.8 | 0.302 | 1.070 (0.941 - 1.218) | ||
| Pulmonary Vascular Pedicle Width, mm | 56.5 ± 11.9 | 57 ± 10.2 | 0.140 | 1.024 (0.992 - 1.056) | ||
| Width of the heart, mm | 147.8 ± 23.1 | 152.8 ± 26.1 | 0.156 | 1.011 (0.996 - 1.025) | ||
| CTI | 0.5 ± 0.1 | 0.5 ± 0.1 | 0.478 | 5.169 (0.055 - 484.6) | ||
| Urea, mg/dL | 129.3 ± 43.4 | 128.7 ± 34.1 | 0.831 | 1.001 (0.991 - 1.011) | ||
| Albumin, g/dL | 3.7 ± 0.4 | 3.4 ± 0.6 | 0.005 | 0.339 (0.159 - 0.726) | ||
| Hemoglobin, g/dL | 11.1 ± 2 | 10.4 ± 1.9 | 0.040 | 0.810 (0.662 - 0.990) | ||
| Ferritin, µg/L | 229.7 ± 180.1 | 394.6 ± 334.3 | 0.047 | 1.001 (1.000 - 1.002) | ||
| Calcium, mg/dL | 9.1 ± 0.8 | 9 ± 0.8 | 0.546 | 0.878 (0.575 - 1.340) | ||
| Phosphate, mg/dL | 5.4 ± 1.6 | 5.5 ± 1.4 | 0.650 | 1.059 (0.826 - 1.359) | ||
| iPTH, ng/dL | 524.8 ± 380.1 | 388 ± 321.3 | 0.013 | 0.998 (0.997 - 1.000) | ||
| Potassium, mmol/L | 4.9 ± 0.7 | 4.7 ± 0.8 | 0.035 | 0.630 (0.410 - 0.968) | ||
| Creatinine, mg/dL | 7.4 ± 3.3 | 8.2 ± 2.6 | 0.505 | 0.957 (0.842 - 1.088) | ||
| PO2, mm Hg | 47.3 ± 13.4 | 49.4 ± 16.1 | 0.955 | 0.999 (0.976 - 1.023) | ||
| PCO2 , mm Hg | 39.8 ± 5.7 | 39.8 ± 7.7 | 0.919 | 1.003 (0.949 - 1.060) | ||
| SO %2, | 74.5 ± 16.3 | 76.2 ± 19 | 0.793 | 1.003 (0.982 - 1.024) | ||
| Gender |
Woman | 26 (68.4) | 18 (56.3) | 1 (Reference) | ||
| Male | 12 (31.6) | 14 (43.8) | 0.159 | 1.665 (0.819 - 3.387) | ||
| Dialysis Type |
PD | 20 (52.6) | 13 (40.6) | 1 (Reference) | ||
| HD | 18 (47.4) | 19 (59.4) | 0.481 | 1.293 (0.633 - 2.642) | ||
| Cardiomegaly |
No | 23 (60.5) | 13 (40.6) | 1 (Reference) | ||
| Yes | 15 (39.5) | 19 (59.4) | 0.154 | 1.693 (0.820 - 3.492) | ||
| Aortic calcification |
No | 13 (34.2) | 3 (9.4) | 1 (Reference) | ||
| Yes | 25 (65.8) | 29 (90.6) | 0.252 | 2.010 (0.608 - 6.639) | ||
| Redistribution |
No | 14 (36.8) | 15 (46.9) | 1 (Reference) | ||
| Yes | 24 (63.2) | 17 (53.1) | 0.680 | 1.166 (0.563 - 2.415) | ||
| Interstitial pattern |
No | 20 (52.6) | 17 (53.1) | 1 (Reference) | ||
| Yes | 18 (47.4) | 15 (46.9) | 0.714 | 1.143 (0.559 - 2.338) | ||
| Pleural fluid |
No | 29 (76.3) | 29 (90.6) | 1 (Reference) | ||
| Yes | 9 (23.7) | 3 (9.4) | 0.362 | 0.572 (0.173 - 1.898) | ||
| Pleural thickness |
No | 30 (78.9) | 22 (71) | 1 (Reference) | ||
| Yes | 8 (21.1) | 9 (29) | 0.624 | 0.812 (0.354 - 1.865) | ||
| Alveolar infiltration |
No | 36 (94.7) | 30 (93.8) | 1 (Reference) | ||
| Yes | 2 (5.3) | 2 (6.3) | 0.530 | 1.587 (0.376 - 6.709) | ||
| Atelectasis |
No | 37 (97.4) | 31 (96.9) | 1 (Reference) | ||
| Yes | 1 (2.6) | 1 (3.1) | 0.910 | 1.123 (0.152 - 8.321) | ||
| Radiological Status |
Deterioration | 7 (18.4) | 17 (53.1) | 1 (Reference) | ||
| Stable or İmproved |
31 (81.6) | 15 (46.9) | 0.055 | 0.500 (0.246 - 1.015) | ||
| Family history |
No | 28 (73.7) | 24 (75) | 1 (Reference) | ||
| Yes | 10 (26.3) | 8 (25) | 0.730 | 0.866 (0.382 - 1.961) | ||
| Clinical Status | Deterioration | 7 (18.4) | 17 (53.1) | 1 (Reference) | ||
| Stable or İmproved | 31 (81.6) | 15 (46.9) | 0.003 | 0.118 (0.028-0.495) | ||
Mean ± Standard deviation, n (%); CTI, cardio thoracic index; iPTH, intact parathormone; PO2, partial oxygen pressure; PCO2, partial carbon dioxide pressure; SO2, oxygen saturation.
Table 6.
Results of multivariate cox regression analysis of the effects of possible factors on survival.
Table 6.
Results of multivariate cox regression analysis of the effects of possible factors on survival.
| Beta | p | Hazard Ratio (95% Confidence Interval) |
||
|---|---|---|---|---|
| Age, year | 0.044 | 0.007 | 1.045 (1.012 - 1.078) | |
| Albumin, g/dL | -0.501 | 0.213 | 0.606 (0.275 - 1.334) | |
| Hemoglobin, g/dL | -0.166 | 0.129 | 0.847 (0.683 - 1.050) | |
| Ferritin, µg/L | 0.001 | 0.255 | 1.001 (1.000 - 1.001) | |
| iPTH, ng/dL | -0.002 | 0.040 | 0.998 (0.997 - 1.000) | |
| Potassium, mmol/L | -0.455 | 0.071 | 0.635 (0.387 - 1.040) | |
| Clinical status | -1.933 | 0.009 | 0.145 (0.034 - 0.621) |
iPTH, intact parathormone.
Table 7.
Spearman Correlation Test Results between iPTH level and Chest X-ray Findings.
| Diaphragm Height | Pulmonary Artery Diameter | Pulmonary Vascular Pedicle Width | CTI | ||
|---|---|---|---|---|---|
| iPTH | r | 0.112 | -0.156 | -0.272 | -0.070 |
| p | 0.360 | 0.201 | 0.024 | 0.567 | |
r, Spearman correlation coefficient; p, Significance value of correlation; CTI, Cardio thoracic index; iPTH, intact parathormone.
Table 8.
Phi Test Results of the Relationship Between Radiological and Clinical Status in PD and HD Patients.
Table 8.
Phi Test Results of the Relationship Between Radiological and Clinical Status in PD and HD Patients.
| Clinical Status | Phi | p | ||||
|---|---|---|---|---|---|---|
| Deterioration | Stable or İmproved | |||||
| PD and HD | Radiological Status | Deterioration | 20 | 4 | 0.287 | 0.016 |
| Stable or İmproved | 25 | 21 | ||||
Table 9.
Multivariate cox regression analysis results of the effect of iPTH/PVPW on survival.
| Beta | p | Hazard Ratio (95% Confidence Interval) |
||
|---|---|---|---|---|
| Age, year | 0.040 | 0.016 | 1.040 (1.008 - 1.074) | |
| iPTH/ PVPW | -0.073 | 0.035 | 0.930 (0.869 - 0.995) | |
| Albumin, g/dL | -0.500 | 0.214 | 0.606 (0.275 - 1.335) | |
| Hemoglobin, g/dL | -0.160 | 0.141 | 0.852 (0.689 - 1.054) | |
| Ferritin, µg/L | 0.000 | 0.354 | 1.000 (1.000 - 1.001) | |
| Potassium, mmol/L | -0.440 | 0.083 | 0.644 (0.391 - 1.059) | |
| Clinical Status | -1.985 | 0.008 | 0.137 (0.032 - 0.589) |
iPTH, intact Parathormone; PVPW, Pulmonary vascular pedicle width.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



