
Submitted:
07 July 2024
Posted:
08 July 2024
You are already at the latest version
Abstract
The aims of this systematic review and meta-analysis were to evaluate the risk of inmates with mental disorder of being placed into disciplinary confinement (DC) and its effect on mental health. A systematic search of studies was performed in PubMed, PsycINFO, Web of Science, and Google Scholar. The meta-analysis was conducted using random-effects models. Heterogeneity among study point estimates was assessed with Q statistics and quantified with I2 index. Publication bias was assessed with Egger’s test. Quality assessment was based on the GRADE Checklist for observational studies. Guidelines from Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) were followed throughout. First, a meta-analysis of 5 articles including 27,455 inmates showed than incarcerated individuals with a mental disorder were 1.23 times (OR=1.23, CI=1.10; 1.38) more likely to be placed in DC than incarcerated individuals without a mental disorder. Particularly, having a severe mental disorder (OR=1.31, p<0.001), a personality disorder (OR=1.66, p<0.001) and having previously received mental health services (OR=1.16, p=0.024) increased the risk of being placed in DC. Secondly, a systematic review of 5 articles including 171,300 inmates showed more psychological distress, psychiatric symptoms (self-harm, thought disorders, obsessive-compulsive symptoms), need for mental health services and hospitalizations in DC than the general correctional population. Considering the increased risk of placement in DC for incarcerated persons with a mental disorder and its deleterious effect on mental state, it is essential that correction officials create new safe interventions to manage these inmates and offer them proper mental health care to limit its use.
Keywords:
correctional facilities
; disciplinary confinement
; mental health
; prevalence
; meta-analysis
; systematic review
1. Introduction
People with mental disorders are overrepresented in correctional facilities [1,2,3]. Indeed, 47.7% of individuals in an American prison in 2015 had a mental disorder; this number went up to 74.6% in a study that included 10 Canadian jails in 2017 [1,2]. Moreover, a national survey in 2004-2005 showed that in certain regions of the USA (e.g., Arizona, Nevada), a higher prevalence of individuals with a mental disorder were in correctional facilities than in psychiatric hospitals [4]. However, compared to psychiatric hospitals, correctional facilities have fewer appropriate resources and services for mental disorders, and training for correctional staff is very limited [2,5]. Thus, psychiatric symptoms may be mistaken for an intentional act of disobedience by staff [6,7]. In addition, individuals with mental disorders have more difficulty complying with regulations (e.g., strict schedules) and they adapt less well to the correctional environments (e.g., by committing auto and hetero aggressive behavior) [3,6,7]. In correctional facilities whose primary objective is to preserve institutional order and security, one of the ways to manage, prevent and control disruptive behavior is through the use of solitary confinement [7,8,9,10]
Solitary confinement exists in three forms with different objectives: 1) administrative confinement for institutional management purposes (e.g., inmates who fail to appropriately adjust in the general carceral population by violating facility rules), 2) protective confinement for the inmate’s personal safety, and 3) disciplinary confinement as punishment for failure to comply with an institutional rule [9,11]. Concerning the latter, which is within the scope of this paper, a disciplinary process governs this type of solitary. When an inmate is ticketed by a guard for a rule violation, they must appear before a disciplinary committee to determine the punishment associated with the violation. A variety of punishments are available, from a warning to the most severe disciplinary measure being disciplinary confinement [12]. Generally, inmates in solitary confinement are kept in their cells for 23 hours a day, with one hour for physical exercise and hygiene care. These cells are generally physically separated from the general correctional population. Access to programs and services (e.g., education, rehabilitation), to recreation and to other inmates is very limited [13,14,15,16]. In some cases, the cells may be lit continuously with artificial light that inmates could not control, and there may be no access to natural light [17].
This isolated and disenfranchised environment has given rise to several studies into the repercussions on inmates’ mental state leading to a few meta-analyses. A first quantitative synthesis on administrative confinement specifically found a significant small to moderate effect on anxiety (g=0.39, CI=0.08; 0.70) and general health (g=0.61, CI=0.14; 1.08) and no effect for self-harm, cognitive functioning, mood/emotion, psychosis as well as hypersentivity/hyperactivity [18]. A second meta-analysis including the 3 types of solitary confinement found numerous deleterious impacts on the mental health of incarcerated people. Inmates in solitary confinement showed a significant increase in mood symptoms (anxiety and depression) (SMD= 0.41, CI=0.19; 0.64), psychotic symptoms (SMD=0.35, CI=0.18; 0.52) and aggressivity or hostility symptoms (SMD=0.38, 0.29; 0.47) than individuals not in solitary confinement [19]. Considering that inmates with a mental disorder are more prone to disorganized behavior that can be mistaken for being resistant to regulations, as well as greater difficulty adapting to the correctional facilities environment, studies have evaluated whether they are more predisposed to being placed into solitary confinement than other inmates [20]. In 2020, a meta-analysis including 11 articles with 163,414 inmates showed that inmates with a mental disorder indeed had a 1.62 times higher probability (OR = 1.62, CI = 1.21; 2.15) of being placed in solitary confinement than other inmates without a mental disorder [21].
Unfortunately, these meta-analyses included only administrative confinement or all 3 types of solitary confinement (administrative, disciplinary, and protective). A deeper understanding of solitary confinement is needed since the types of solitary confinement are used for different purposes, the duration and level of restrictions differ, and the process for each type of confinement is different [12,22,23,24]. Moreover, compared with other forms of confinement in detention, disciplinary confinement has been the most widely used [25]. In this sense, some studies have focused on disciplinary confinement. However, studies show divergent results. For instance, some studies have observed a higher prevalence of inmates with a mental disorder in disciplinary confinement [12,23,26,27], whereas other authors have observed no significantly difference [13], or results depending on the type of measure used (diagnosis, length of observation) [28,29]. Also, the type of measures used to define the presence of a mental disorder (having been hospitalized in psychiatry in the last year, diagnosis) varies from study to study, making it difficult to interpret the results [27,29]. Concerning the effects on mental health, it is possible that disciplinary confinement has a variable effect on different types of mental health symptoms (e.g., anxiety, psychotic, depression) [22,30,31]. It is also possible that the effect may differ for different inmates, and particularly, whether or not the inmate has a history of a mental disorder [31]. Consequently, this article had for aims to conduct:
- a systematic review and meta-analysis of the association between mental disorders in inmates and placement into disciplinary confinement in correctional setting compared to in inmates without any mental disorder.
- a systematic review on the effects of disciplinary confinement in correctional setting on the mental health of inmates with or without pre-existing psychiatric conditions.
2. Materials and Methods
2.1. Search Strategies
A systematic search was performed in the electronic databases of PubMed, PsycINFO, Web of Science and Google Scholar with key words that were inclusive for disciplinary confinement (e.g., disciplinary solitary, punitive segregation), psychological effect (e.g., hallucinations, depression, suicide) and mental illness (e.g., psychiatric disorder, mental health). A full electronic search strategy is available in supplementary material. Reference lists were scanned by hand to identify additional studies. Searches were completed by October 2023. Abstracts were screened and full articles by S.G and L.D. No setting, date or geographical restrictions were applied; searches were limited to English or French language sources.
2.2. Study Eligibility
Studies were included if the sample comprised adult inmates over the age of 18 in correctional settings. More specifically for the first objective (association between mental illness and placement into disciplinary confinement), the included articles had to have reported 1) any indication of a potential mental disorder (i.e., mental disorder diagnosed by mental health professionals, taking regular psychotropic medication, received mental health services from a qualified health professional, residency in an institutional mental health unit) before being place into disciplinary confinement and 2) the statistical associations were calculated/or could be calculated using odds ratios (OR). For the second objective (effects on mental health), studies were included if a measure of psychological symptomatology or self-harm was incorporated during or after being placed in solitary confinement. Disagreements on the inclusion of studies were resolved by group discussions to obtain a final consensus (see Table S1 for electronic search strategy for the systematic review and meta-analysis conducted).
2.3. Data Extraction
Data were extracted with a standardized form and double checked for consistency by the authors. Reported effect sizes with 95% confidence intervals (CI) were recorded with other key information (e.g., sample size (proportion of SMI sample, proportion of men), type of psychological symptomatology or indication of a mental disorder, adjustment for confounding factors, type of measure (administrative data, survey, clinical assessment), control group). Quality assessment was independently undertaken by S.G and L.D against a set of criteria based on the GRADE Checklist for observational studies [32]. Studies were assigned to categories of High, Moderate, and Low quality. Extracted data were independently cross-checked and any queries were resolved by discussion with A.D. To achieve a high standard of reporting, we followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (see Table S3 for PRISMA Checklist) [33].
2.4. Statistical Analysis
For the meta-analysis (objective 1), data were entered into an electronic database and analysed in R (version 4.3.2) with the metafor package [34,35]. General population inmates with and without mental disorders were compared to assess whether the risk of being placed in disciplinary confinement was higher for inmates with a mental disorder. The following qualitative descriptions of the strength of reported ORs were used [36]: small (OR = 1.0–1.5), moderate (OR = 1.6–2.5), strong (OR = 2.6–9.9) and very strong (OR = 10.0 and above). Heterogeneity among study point estimates was assessed with the Q statistics and quantified with I2 index with a value of 0% indicating no effect heterogeneity, whereas 25%, 50% and 75% suggest low, moderate and high heterogeneities, respectively [37,38]. Since substantial heterogeneity was observed (see below), we employed random-effects models that are more conservative than fixed-effects models, and appear to better address heterogeneity between studies and study samples [39]. Risk of publication bias was assessed with Egger’s test. A significative p-value can indicate publication bias since studies that do not show statistically significant effects may more likely remain unpublished (Egger et al. 1997). In order to have more precision and explain the heterogeneity between articles, sub-analyses were conducted for men and women separately and by 4 categories of mental heath statue according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR): 1) severe mental illness (e.g., psychotic disorder, mood disorder), 2) common mental disorder (e.g., anxiety, obsessive-compulsive disorder), 3) mental health services (e.g., having been hospitalized in psychiatry, prescription drug use) and 4) personality disorder [40]. Due to incompatible data, a meta-analysis was not feasible for objective 2 and therefore only results of the systematic review are presented.
3. Results
3.1. Description of Studies
This literature search identified 10,248 potential articles that were screened for eligibility after removing duplicates. With the search in google scholar and cross-referencing, 92 additional studies were identified. Among these articles, 48 full texts were assessed and 38 were then excluded. After assessment, for the first objective (association between mental illness and solitary confinement), 5 final articles were included amounting to a total of 27,455 inmates and the quality of studies as being graded mostly as moderate. One study was undertaken in correctional facilities in England, and the other four in the United State of America. Concerning the second objective (effects on mental health), 5 other final articles were included comprising 171,300 inmates. Data ranged from low to high quality of evidence. Also, 4 studies were carried out in correctional facilities in the United State of America and one in Denmark. The PRISMA flowchart for the inclusion of studies in the meta-analysis is found in Figure 1. The details of the retrieved studies are described in supplementary material (see Table S2).
3.2. Association of Mental Health in Disciplinary Confinement
Incarcerated individuals with a mental disorder were 1.23 times (OR=1.23, CI=1.10; 1.38) more likely to be placed in disciplinary confinement compared to incarcerated individuals without a mental disorder (Figure 2). The database was characterised by moderate heterogeneity (Q=30.38, p=0.016, I2=41.1 %). Egger’s test (t=0.1429, p=0.78) suggested that there was no publication bias. In both men (OR=1.34, p=0.009) and women (OR=1.24, p=0.002), a significant association between the presence of a mental disorder and placement into disciplinary confinement was observed. By category of mental disorder, there was an increase in the risk of ending up in disciplinary confinement in favor of incarcerated people with a severe mental disorder (OR=1.31, p<0.001) as well as for those with a personality disorder (OR=1.66, p<0.001) compared to incarcerated people with no mental disorder. Also, incarcerated individuals who used mental health services before incarceration had an increased risk of ending up in disciplinary confinement (OR=1.16, p=0.024) than those who never used health services. There was no significant association for common mental disorders. Of the 5 articles included, 3 controlled for offense leading to disciplinary confinement [27,28,41] and 2 articles controlled for age, gender and ethnicity [28,41]. The quality of evidence ranged from low to moderate. Evidence was particularly low for those that did not control for confounding factors, and those that used self-reported measures for diagnosis purposes. The details of the retrieved studies are described in supplementary material.
3.3. Effects of Disciplinary Confinement on Mental Health
3.3.1. Psychological Distress and Psychiatric Symptoms
Two cross-sectional studies conducted by Miller in a U.S. federal penitentiary used clinical interviews to assess psychological distress in 30 inmates who had been in disciplinary confinement (n=10), administrative confinement (n=10) or the general correctional population (n=10). The first study showed that the average distress score assessed with Brief Symptom Inventory in disciplinary confinement was significantly higher than in administrative segregation and in the general correctional population (p<0.01) [42]. The second study by Miller and Young (1997) observed more obsessive-compulsive symptoms (p=0.01), interpersonal sensitivity (p=0.02) and hostility (p=0.001) in disciplinary confinement compared to inmate in the general correctional population. No significant difference was found for depressive symptoms, anxiety or paranoid ideation [22].
Another cross-sectional study in the U.S. showed that mentally ill inmates (n=90) experienced more psychological distress score assessed by survey questionnaire in disciplinary confinement (d=1.16, p<0.001) than inmates without mental disorders (n=85). More specifically, inmates with mental disorders experienced more suicidal ideation, concentration problems, thought disorders and perceptual (visual or auditory) disorders in disciplinary confinement compared to inmates without mental disorder. In this study, a mental disorder was a classification given by mental health staff at admission or during incarceration, without further specification [30].
The quality of evidence was graded as being low for these analyses due to small sample and no control for confounding factors.
3.3.2. Mental Health Services and Hospitalizations
A large-scale longitudinal study (n=36,360) in correctional facilities (e.i., closed prisons, open prisons, and jails) in Denmark found that inmates exposed to disciplinary confinement (n=4,120) were significantly (p<0.05) more likely to receive mental health care (Mental Health Contact) within 3 years of incarceration, compared with inmates who had received another type of disciplinary sanction (fines, warnings, confiscation of contraband) (n=12,483) and that no recorded disciplinary actions (n=19,757) [26]. Mental health contact was defined whether people have contact/consultancy with the general mental health care system after release reported from administrative database. These analyses were graded as being of moderate quality evidence.
A study with evidence graded as being of low quality has reported from interviews with 55 inmates with no mental disorder prior to being placed in disciplinary confinement that 40% were transferred to a psychiatric unit due to a deterioration in their mental state, suicide threat or suicide attempt during their placement in disciplinary confinement. In this analyse, there was no control group [30].
3.3.3. Self Harm
The retrospective study by Kaba et al. (2014) examined predictors of self-harm (defined as self-injurious behaviors not leading to impairment or death) and potentially fatal self-harm (high likelihood of leading to death or severe impairment) among 134,188 inmates in New York’s local detention facilities (New York Jail System). For general self-harm, disciplinary confinement was the strongest risk factor (OR = 10.15, CI=8.53; 12.08). The best predictor of potentially fatal self-harm was the combination of exposure to disciplinary confinement and having a severe mental disorder, with an almost 10-fold increase in probability (OR = 9.80, CI=5.02; 19.18). Severe mental disorders were defined based on the criteria for a psychiatric diagnosis according to the most current Diagnostic and Statistical Manual of Mental Disorders other than alcohol or drug disorders, organic brain syndromes, developmental disabilities, or social conditions and impairment in functioning due to Mental illness or reliance on psychiatric treatment, rehabilitation and supports. The data was collected from database of department of correction [31]. The quality of evidence of these analyses were graded as high.
The cross-sectional study conducted in Louisiana’s state-operated prisons by Cloud et al. (2023) with evidence evaluated as being of moderate quality compared self-harm behaviors collected by survey between inmates in disciplinary confinement (n=347) and inmates in combined administrative or protective confinement (n=170). The survey showed that self-harm was 1.97 times more likely (OR=1.97, p=0.01) to occur in disciplinary confinement than in administrative or protective. This study reported that each 90-day stay in a disciplinary confinement slightly but significantly (OR=1.03, p=0.02) increased the risk of subsequent self-harm [43].
4. Discussion
This study showed a higher risk of inmates with a mental disorder of being placed in disciplinary confinement than other inmates as well as a differential risk depending on the type of mental disorder. Moreover. being exposed to these settings has been shown to cause many adverse effects on the mental state of inmates.
Concerning the first objective, based on the 5 studies included within our meta-analysis, we found a significant higher risk of being placed into disciplinary confinement for any mental health problem within a considerable sample of 27,455 inmates in both men and women. Notably, of the 5 articles included, 3 controlled for offense leading to disciplinary confinement [27,28,41]. Quality of evidence of analyses were graded as being mainly moderate quality. The database was characterised by moderate heterogeneity and no publication bias was found. This result is in line with the meta-analysis that included the 3 types of solitary confinement having shown a positive association [21]. Since disciplinary confinement is a process comprising several stages (ie., receiving a ticket from a guard, ii. penalty decided by a disciplinary committee and iii. sanction duration), one study evaluated whether the risk for an inmate with a mental disorder differed at each of the 3 stages. The authors showed a significantly higher risk for inmates with mental disorder at each of the 3 stages, after controlling for the severity of the offence committed [12]. Therefore, inmates with mental disorders received more tickets by guards, they were granted more decisions to be placed within disciplinary confinement and the duration of confinement was moreover longer than their counterparts without mental disorders. The greatest disparity between mentally disordered and non-mentally disordered inmates was at the first stage, when guards handed out tickets [12]. This study proposes that this disproportion of the cumulative disadvantage is associated to the stigmatisation of individuals with mental illness, which supports the importance of training correctional staff in the management of this population [12,44,45]. A second study, which also controlled for offence severity, likewise showed a higher risk of mentally disordered inmates receiving the most severe form of punishment, disciplinary confinement, than another (i.e., reprimand, lose privilege, higher custody) by the disciplinary committee [41]. Notably, it was shown that a significant risk is linked with severe mental disorders, personality disorders and having a history of mental health service use. A common mental disorder does not appear to be a risk for placement in disciplinary isolation. Thus, a more pronounced level of disorganization may have increased the risk of being placed in disciplinary confinement. These results are not surprising considering the hypotheses put forward that psychiatric symptoms, such as disorganization could be perceived as a refusal to obey and would lead to greater difficulty in adapting to correctional facilities [6,7].
Moreover, once placed in disciplinary confinement, inmates may show a degradation of their mental health. The 5 included studies comprising a large sample of 171,300 inmates showed greater psychological distress and a greater likelihood of needing psychiatric services than inmates in the general correctional population. A higher risk of self-harm was also reported, and this risk was even higher if the inmates had a pre-existing mental disorder. In addition, 2 studies that compared solitary confinement to other types of confinement appear to show that disciplinary confinement is more deleterious in terms of self-harm and psychological distress. Although it was not possible to carry out a meta-analysis of disciplinary confinement alone, the results point in the same direction as the meta-analysis that included all 3 types of solitary confinement, i.e., a positive association between confinement and a deleterious effect on inmates’ mental state [19]. Indeed, the authors obtained a small association for mood (d=0.41, CI=0.19; 0.64), psychotic (d=0.35, CI=0.18; 0.52) and aggressive (d=0.38, CI=0.29; 0.47) symptoms. An effect on psychological distress, self-harm as well as the need for psychiatric services and hospitalization have also been observed. Thus, the fact that the duration is predetermined and that it is framed by a disciplinary process does not seem to mitigate the effect of the disciplinary confinement compared to other types of solitary confinement.
However, these results should be interpreted with caution, given the low quality of evidence in many studies and more studies with larger sample sizes are needed and should consider important confounding factors. Considering that the risk of being placed in disciplinary confinement is higher according to the type of mental disorder and possibly according to the severity of the disorder, it would be necessary to evaluate the effects on the mental state of the inmates in a consistent manner.
Whereas our meta-analysis shows that inmates with mental disorder are at an elevated risk of being placed into disciplinary confinement and of suffering the effects of these settings, several limitations must be considered. Firstly, few studies specifically targeting disciplinary confinement have been identified in the literature, most of which were carried out in the United State of America, thereby reducing the possibility of generalizing the results since confinement conditions may differ between institutions and jurisdictions. Moreover, due to the lack of studies we were unable to conduct a meta-analysis for the effects on mental health. Currently, we retrieved solely one to two studies per symptom (some studies comprising also small sample sizes), and only one study investigated the effects for inmates with a pre-existing disorder. Moreover, no study evaluated the possibility of developing a mental disorder following exposure to disciplinary confinement. Secondly, most of the results come from self-reported data, which may have underestimated the results for both objectives, given that inmates may lack self-awareness into their illness or be fearful of stigmatization. Several factors like the level of social isolation and privileges, availability of programming, and duration as well as number of confinements could moderate the effects of disciplinary confinement [46].
5. Conclusions
In conclusion, our meta-analytical investigation showed that mental disorders are at greater risk of being placed into disciplinary confinement. To our knowledge, this is the first meta-analysis to differentiate between different types of mental disorders. Our results also showed that the use of disciplinary confinement has a negative impact on the mental state of the inmates. Consequently, some states in the United States of America have begun to restrict the number of days allowed [47]. Also, studies have set out to find a solution to reduce its use or develop alternative programs [48,49]. However, more alternatives and policies are crucial since more individuals with mental illness enter in correctional systems and solitary confinement has been widely opted as a placement for these inmates. Indeed, changes are needed in the manner correctional facilities manage and care for their inmates with mental health problems. Intervention should not only be effective in maintaining order, but also support inmates’ mental well-being. Finally, since the primary aim of disciplinary confinement is to maintain order within correctional facilities, it would be interesting to assess whether it achieves this objective.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1. Electronic search strategy for the systematic review and meta-analysis conducted. Table S2. Details of the retrieved studies included. Table S3. PRISMA Checklist.
Author Contributions
Conceptualization, S.G., L.D. and A.D.; methodology, S.G. and L.D..; validation, S.G., L.D. and A.D.; formal analysis, S.G. and C-E. G.; writing—original draft preparation, SG.; writing—review and editing, S.G., L.D. and A.D.; supervision, A.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Acknowledgments
AD is holder of a Senior salary award from the FRQS.
Conflicts of Interest
The authors declare no conflicts of interest
References
- Al-Rousan, T.; et al. Inside the nation’s largest mental health institution: a prevalence study in a state prison system. BMC Public Health 2017, 17, 342. [Google Scholar] [CrossRef]
- Butler, A.; et al. Prevalence of Mental Health Needs, Substance Use, and Co-occurring Disorders Among People Admitted to Prison. Psychiatr Serv 2022, 73, 737–744. [Google Scholar] [CrossRef]
- Bennion, E. Banning the bing: Why extreme solitary confinement is cruel and far too usual punishment. Ind. LJ 2015, 90, 741. [Google Scholar]
- Torrey, E.F.; Kennard, A.D.; Eslinger, D.; Lamb, R.; Pavle, J. More mentally ill persons are in jails and prisons than hospitals: A survey of the states; Treatment Advocacy Center: Arlington, VA, 2010. [Google Scholar]
- Fazel, S.; et al. Mental health of prisoners: prevalence, adverse outcomes, and interventions. Lancet Psychiatry 2016, 3, 871–81. [Google Scholar] [CrossRef]
- O’keefe, M.L.; Schnell, M.J. Offenders with mental illness in the correctional system. Journal of Offender Rehabilitation 2007, 45, 81–104. [Google Scholar] [CrossRef]
- Fellner, J. A corrections quandary: Mental illness and prison rules. Harv. CR-CLL Rev. 2006, 41, 391. [Google Scholar]
- Craig, S.C. Rehabilitation versus control: An organizational theory of prison management. The Prison Journal 2004, 84 4_suppl, 92S–114S. [Google Scholar] [CrossRef]
- Shalev, S. Supermax: Controlling risk through solitary confinement; Willan, 2013. [Google Scholar]
- Mears, D.P.; Castro, J.L. Wardens’ views on the wisdom of supermax prisons. Crime & Delinquency 2006, 52, 398–431. [Google Scholar]
- Shames, A.; Wilcox, J.; Subramanian, R. Solitary confinement: Common misconceptions and emerging safe alternatives; ERA Institute: New York, 2015. [Google Scholar]
- Simes, J.T.; Western, B.; Lee, A. Mental health disparities in solitary confinement. Criminology 2022, 60, 538–575. [Google Scholar] [CrossRef]
- Butler, H.D.; Steiner, B. Examining the use of disciplinary segregation within and across prisons. Justice Quarterly 2017, 34, 248–271. [Google Scholar] [CrossRef]
- Butler, H.D.; et al. An examination of the influence of exposure to disciplinary segregation on recidivism. Crime & Delinquency 2020, 66, 485–512. [Google Scholar]
- Morris, R.G. Exploring the effect of exposure to short-term solitary confinement among violent prison inmates. Journal of Quantitative Criminology 2016, 32, 1–22. [Google Scholar] [CrossRef]
- Woo, Y.; et al. Disciplinary segregation’s effects on inmate behavior: Institutional and community outcomes. Criminal Justice Policy Review 2020, 31, 1036–1058. [Google Scholar] [CrossRef]
- Lucas, J.W.; Jones, M.A. An analysis of the deterrent effects of disciplinary segregation on institutional rule violation rates. Criminal Justice Policy Review 2019, 30, 765–787. [Google Scholar] [CrossRef]
- Morgan, R.D.; et al. Quantitative syntheses of the effects of administrative segregation on inmates’ well-being. Psychology, Public Policy, and Law 2016, 22, 439. [Google Scholar] [CrossRef]
- Luigi, M.; et al. Shedding light on “the hole”: A systematic review and meta-analysis on adverse psychological effects and mortality following solitary confinement in correctional settings. Frontiers in Psychiatry 2020, 11, 840. [Google Scholar] [CrossRef]
- Houser, K.; Belenko, S. Disciplinary responses to misconduct among female prison inmates with mental illness, substance use disorders, and co-occurring disorders. Psychiatr Rehabil J 2015, 38, 24–34. [Google Scholar] [CrossRef]
- Dellazizzo, L.; et al. Is mental illness associated with placement into solitary confinement in correctional settings? A systematic review and meta-analysis. International journal of mental health nursing 2020, 29, 576–589. [Google Scholar] [CrossRef]
- Miller, H.A.; Young, G.R. Prison segregation: Administrative detention remedy or mental health problem? Criminal Behaviour and Mental Health 1997, 7, 85–94. [Google Scholar] [CrossRef]
- Labrecque, R.M.; Mears, D.P.; Smith, P. Gender and the effect of disciplinary segregation on prison misconduct. Criminal Justice Policy Review 2020, 31, 1193–1216. [Google Scholar] [CrossRef]
- Frost, N.A.; Monteiro, C.E. Administrative segregation in US prisons. Restrictive housing in the US: Issues, challenges, and future directions, 2016: p. 1-48.
- Wooldredge, J.; et al. Disparities in Segregation for Prison Control: Comparing Long Term Solitary Confinement to Short Term Disciplinary Restrictive Housing. Justice Quarterly 2023, 1–24. [Google Scholar] [CrossRef]
- Wildeman, C.; Andersen, L.H. Long-term consequences of being placed in disciplinary segregation. Criminology 2020, 58, 423–453. [Google Scholar] [CrossRef]
- Henry, B.F. Disparities in use of disciplinary solitary confinement by mental health diagnosis, race, sexual orientation and sex: Results from a national survey in the United States of America. Criminal behaviour and mental health 2022, 32, 114–123. [Google Scholar] [CrossRef]
- Severson, R.E. Gender differences in mental health, institutional misconduct, and disciplinary segregation. Criminal Justice and Behavior 2019, 46, 1719–1737. [Google Scholar] [CrossRef]
- Coid, J.; et al. Psychiatric morbidity in prisoners and solitary cellular confinement, I: Disciplinary segregation. Journal of Forensic Psychiatry & Psychology 2003, 14, 298–319. [Google Scholar]
- Wynn, J.R. Psychopathology in supermax prisons: A New York state study; City University of New York, 2007. [Google Scholar]
- Kaba, F.; et al. Solitary confinement and risk of self-harm among jail inmates. American journal of public health 2014, 104, 442–447. [Google Scholar] [CrossRef]
- Guyatt, G.H.; et al. GRADE guidelines: 4. Rating the quality of evidence—study limitations (risk of bias). Journal of clinical epidemiology 2011, 64, 407–415. [Google Scholar]
- Page, M.J.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev 2021, 10, 89. [Google Scholar] [CrossRef]
- Team, R.D.C. R: A language and environment for statistical computing. (No Title), 2010.
- Viechtbauer, W. Conducting meta-analyses in R with the metafor package. Journal of statistical software 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Rosenthal, R.; DiMatteo, M.R. Meta-analysis: Recent developments in quantitative methods for literature reviews. Annual review of psychology 2001, 52, 59–82. [Google Scholar] [CrossRef]
- Higgins, J.P.; et al. Measuring inconsistency in meta-analyses. Bmj 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Lipsey, M.W.; Wilson, D.B. Practical meta-analysis; SAGE publications, Inc, 2001. [Google Scholar]
- Cooper, H.; Hedges, L.V.; Valentine, J.C. The handbook of research synthesis and meta-analysis; Russell Sage Foundation, 2019. [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders : dsm-5-tr (Fifth edition, text revision); American Psychiatric Association Publishing, 2022. [Google Scholar]
- Clark, K. The effect of mental illness on segregation following institutional misconduct. Criminal Justice and Behavior 2018, 45, 1363–1382. [Google Scholar] [CrossRef]
- Miller, H.A. Reexamining psychological distress in the current conditions of segregation. Journal of Correctional Health Care 1994, 1, 39–53. [Google Scholar] [CrossRef]
- Cloud, D.H.; et al. Self-injury and the embodiment of solitary confinement among adult men in Louisiana prisons. SSM-Population Health 2023, 22, 101354. [Google Scholar] [CrossRef]
- Parker, G.F. Impact of a mental health training course for correctional officers on a special housing unit. Psychiatric Services 2009, 60, 640–645. [Google Scholar] [CrossRef]
- Lavoie, J.A.; Connolly, D.A.; Roesch, R. Correctional officers’ perceptions of inmates with mental illness: The role of training and burnout syndrome. International Journal of Forensic Mental Health 2006, 5, 151–166. [Google Scholar] [CrossRef]
- Haney, C. The psychological effects of solitary confinement: A systematic critique. Crime and Justice 2018, 47, 365–416. [Google Scholar] [CrossRef]
- Ahalt, C.; et al. Reducing the use and impact of solitary confinement in corrections. International Journal of Prisoner Health 2017, 13, 41–48. [Google Scholar] [CrossRef]
- Glowa-Kollisch, S.; et al. From Punishment to Treatment: The “Clinical Alternative to Punitive Segregation” (CAPS) Program in New York City Jails. Int J Environ Res Public Health 2016, 13, 182. [Google Scholar] [CrossRef]
- Zarzar, T.R.; et al. Effect of Clozapine on Time Assigned to Restrictive Housing in a State Prison Population. The Journal of the American Academy of Psychiatry and the Law 2021, 49, 581–589. [Google Scholar]
Figure 1.
Flow-chart depicting the search strategy employed to find the studies to include in this review.
Figure 1.
Flow-chart depicting the search strategy employed to find the studies to include in this review.
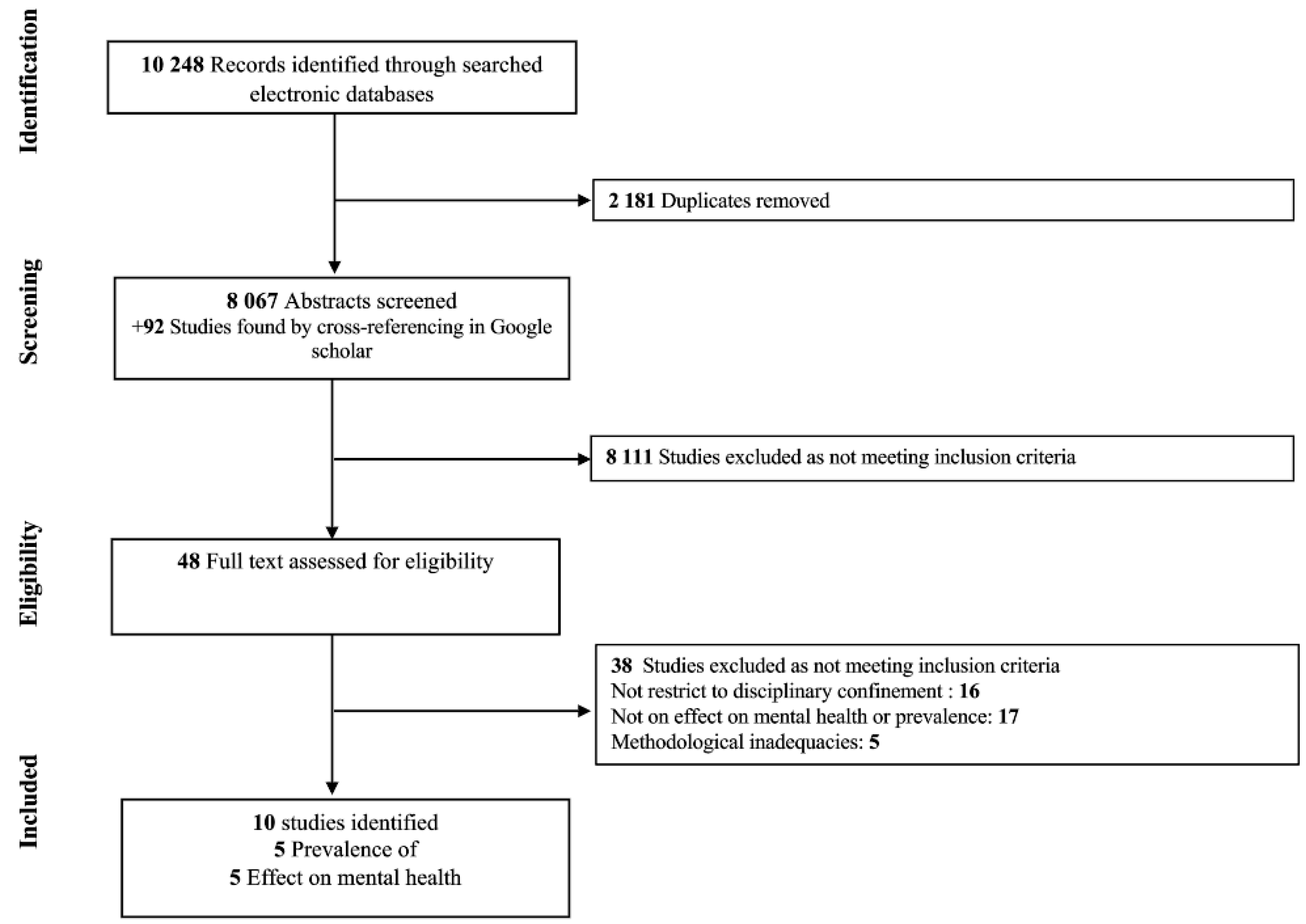
Figure 2.
Forest plot of the association between mental illness and placement into disciplinary confinement in inmates. SMD: severe mental disorder, CMD: common mental disorder, MHS, mental health services, PD: personality disorder.
Figure 2.
Forest plot of the association between mental illness and placement into disciplinary confinement in inmates. SMD: severe mental disorder, CMD: common mental disorder, MHS, mental health services, PD: personality disorder.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



