
Submitted:
08 July 2024
Posted:
09 July 2024
You are already at the latest version
Abstract
: Background. Delivering bad news is a sensitive and challenging aspect of nursing healthcare, requiring a holistic approach that respects patients' preferences, cultural values, and religious beliefs to promote adaptation to the state's health. Aim: map the evidence of the dimensions present in the communication and management of bad news by nurses, with the person in a palliative situation, their caregivers, and family members. Methods: Based on Joanna Briggs Institute methodology, the search was conducted through MEDLINE Complete (EBSCOhost), CINAHL Complete (EBSCOhost), SciELO, and Open Access Scientific Repository in Portugal. From a total of 756 articles, 14 were included, published between 2018 and 2023. Results: Structure components in bad news are influenced by the characteristics of the palliative patients, their caregivers, family members; nurses; and the organizational environment. Promoting the quality of the communication process is desirable through continuous and advanced training in end-of-life; training in bad news; religiously and culturally sensitive nursing interventions centered on hope and maintaining faith; emotional management; and utilization of a checklist protocol. Conclusions: Honest communication allows people to actively participate in the decision-making process and in the trajectory of the care plan that is focused on themselves and their preferences, which has outcomes in functional capacity and readaptation.
Keywords:
Communication
; bad news
; nursing
; palliative care
; Readaptation
1. Introduction
The global need for palliative care has been growing annually, a trend that is expected to continue for decades to come, due to the ageing of the population and the increase in non-communicable diseases such as cancer or organ failure. Globally, it is estimated that approximately 56.8 million people have palliative needs, however, less than 15% have access to this type of care [1]. In Europe, a similar trend exists, with the disparity in access also evident: people living in poorer countries (whose minimum income is lower) and the distance to large cities determine a lower probability of access to palliative care [2]. Despite the current difficulties, the number of palliative care teams has grown exponentially in recent years. Currently, palliative care is explicitly recognized as a human right and the need to be provided from a person-centred perspective and integrated into the national health system is clear [3].
Palliative care is an approach to medicine that aims to provide active, organized, and global care, provided by specific multidisciplinary units and teams with specific training, in hospital or at home, to people suffering from an incurable or serious illness, in an advanced and progressive phase, as well as their families/ caregivers [4]. This approach to care allows for improving the quality of life of people in palliative situations and their families/ caregivers, faced with a life-threatening illness, whatever its stage, concomitantly with active curative treatment or not, offering a support system that allows the person to live as actively as possible until the moment of death [2].
Palliative care can be seamlessly integrated at any stage of the disease, serving a rehabilitative purpose by enabling and supporting patients in adapting to the successive losses stemming from the illness. In this way, the rehabilitation of the palliative patient is an essential component of palliative care, aiming to improve the quality of life of the person, focusing not only on controlling symptoms, relieving pain, and providing psychological, social and cultural care, but also on supporting the readaptation or recovery from the disease's sequelae, allowing the maintenance of functional status, reducing the impact of disability on the quality of life of the person, their family and caregivers, and preventing the emergence of new disabilities [5]. To this end, palliative care bases its philosophy of care on four fundamental pillars: adequate and rigorous symptomatic control, support for family members/caregivers, teamwork, and effective communication between all parties involved [6].
Communication is a process that allows people to exchange information about themselves and their surroundings, being an essential intervention in interactions between nurses and patients and an essential component of the nursing profession [7,8].
Efficient communication facilitates the interaction between nurses and patients, family/ caregivers and contributes to their trust in the team and in the care itself, allowing greater symptom control, strengthening coping strategies, facilitating treatment adherence, and guiding treatment processes and decision-making while also increasing satisfaction with the care provided and quality of life [9,10,11], which is why the nurse's competence in communication is fundamental to the care process.
Communication is a basic nursing skill [12], essential in person-centered nursing care as recommended in the Theory of Person-Centred Care by McCormack & McCance [9], especially in a scenario of particular fragility such as the progression of a serious and life-limiting illness as is the palliative care plan [13]. In this context, nurses must master specific communication techniques and strategies that enable them to effectively communicate with palliative patients as well as their families and caregivers. It is also important for nurses to communicate well with the multidisciplinary team when dealing with such complex situations [11].
Breaking bad news is often referred to in the literature as one of the most difficult and worrying actions in nursing clinical practice. It is one of the situations in which the professional's competence in using appropriate strategies to communicate acquires particular relevance and impact on the readaptation process to the successive losses [14,15].
Breaking bad news is often associated with the transmission of information regarding disease diagnoses, prognoses, or disease progression, however, bad news is more comprehensive [16,17]. When discussing bad news in the context of health, it can be defined as any news that negatively affects an individual's outlook on their future. This type of news has the power to impact hope, emotional and mental well-being, and disrupt one's lifestyle. It is not limited to the communication of medical diagnoses, results of analyses, complementary diagnostic exams, or treatments [16,18]. In everyday clinical practice, there are many situations in which nurses are responsible for breaking bad news and more often find themselves in the position of managing bad news, whether delivered by themselves or another health professional [19]. Therefore, delivering bad news should be seen as a process, not just as the moment of transmitting negative information to the palliative patient. The process of communicating and managing bad news involves the moments before and after the information is conveyed and is not limited to the moment it is verbalized [20]. This highlights the significance of, not only communicating bad news but also managing it effectively.
In most cases this issue is obvious, such as a diagnosis of a life-threatening disease (and consequent probability of reduced longevity, functional decline, and/or quality of life), however, in other cases, it may not be so obvious, the referral to the palliative care team, the need for hospitalization, the impossibility of staying at home without assistance, the decline in analytical parameters, the need for chemotherapy treatments or their suspension, among many other pieces of information are often bad news. transmitted by nurses in this area during their daily practice [14,21].
Communicating and managing bad news is a complex skill that informs the person in a palliative situation and empowers them to make decisions and plan their care trajectory, which has evolved significantly in recent years as care has advanced. focus more and more on the person, their needs, and desires [9]. However, despite the existence of several studies on the intervention of other health professionals in the breaking of bad news, few are found focused on nursing [19,22], which is why it is important to explore the available evidence on communication and bad news management in the field of nursing care.
This scoping review aims to: i) map existing knowledge regarding the dimensions present in the communication and management of bad news carried out by nurses, focus on the readaptation process in palliative patients, family members/caregivers; ii) identify gaps in scientific knowledge where more research will be needed in the future.
2. Materials and Methods
This scoping review was conducted under the Joanna Briggs Institute methodology [23,24], the research strategy and analysis of articles were carried out based on the guidelines for systematic reviews and goal extension -analysis: PRISMA-ScR [25]. This review consists of three steps: identifying relevant literature, applying inclusion/exclusion criteria, and reviewing the included evidence [26]. The scoping review protocol was registered on the Open Science Framework (OSF) at https://archive.org/details/osf-registrations-jaqd2-v to prevent duplication of scientific evidence.
2.1. Selection Criteria
Eligibility criteria were determined based on Population, Context, and Concept (PCC) elements per the Joanna Briggs Institute guiding principles [23,27]. The research question was: What are the key aspects involved in the communication and management of difficult news by nurses (C) with patients in palliative care, their family members/caregivers (P), in the settings of inpatient, outpatient, and home care units (C)?
- -
- Population: Person in a palliative situation, family members/caregivers.
- -
- Concept: Dimensions of communication and management of bad news in nursing.
- -
- Context: Inpatient, outpatient, and home units.
People under the age of 19 were excluded from the analysis (in the CINHAL and MEDLINE databases, people aged 19 or over are defined as “all adults”) and pregnant women. Opinion articles or editorials were also excluded, as well as all those without correlation with the communication and management of bad news carried out by nurses, with the person in a palliative situation, family members/caregivers, and the defined objective(s).
This scoping review included the incorporation of qualitative, quantitative, mixed methods studies, and other systematic reviews conducted within the last five years, with a time limit from 01/01/2018 to 12/10/2023.
2.2. Search Strategy
To validate the novelty of the topic under study, a comprehensive search was conducted across multiple databases, including PubMed, JBI Evidence Synthesis, and PROSPERO. No similar scoping reviews were found, either completed or with a registered protocol, emphasizing the originality of the research topic.
The following electronic databases were used in the search: MEDLINE Complete (EBSCOhost) and CINAHL Complete (EBSCOhost). The descriptors were validated in the Medical Subject Headings (MeSH) accepting the term “Breaking bad news” in natural language, due to its high frequency in multiple articles/documents found in a first floating reading on the topic. Only documents written in English, Portuguese, and Spanish were analyzed to ensure high-quality data selection and extraction. The research strategy is detailed in Table 1.
SciELO and Open Access Scientific Repository databases in Portugal were also used, and the search was guided by the same temporal delimitation and descriptors previously validated in Health Sciences (DeSC).
2.3. Selection Process and Article Eligibility Criteria
The documents were selected based on their title and abstract, aligning with the defined objectives for the scoping review. Initially, the search results were exported to the Mendeley® 19.4 reference manager (Mendeley Ltd., Elsevier, Amsterdam, The Netherlands), thereby streamlining the identification and removal of duplicate articles. The full text of the selected documents/publications was meticulously evaluated against the predefined inclusion criteria by either two (T.M and A.R) or three (E.S.) independent reviewers. Data extraction and organization were conducted encompassing details such as author(s), year and country of study, research objectives, methodology, population/sample size, care context, as well as the dimensions of communication and management of difficult news by nurses in palliative care settings with patients and their family members/caregivers. The data extraction tool used in this process was developed by the reviewers. All disagreements regarding report inclusion were resolved through discussion or with a third reviewer (E.S.).
3. Results
3.1. Characteristics of Included Studies, Context, And Population
A total of 756 articles were considered after eliminating those that were repeated. Upon closer observation of the abstract, 672 were excluded and 84 were considered eligible. Of the 84 publications identified, 14 were selected for reading and were assessed in detail. These last articles and documents that were included will be discussed and systematized in this article, as illustrated in Figure 1.
The included articles were carried out in 17 different countries: Saudi Arabia (n=1); United States of America (n= 5); China (n=1); Italy (n=3); Singapore (n=1); Spain (n=3); Sweden (n=2); Australia (n=3); Japan (n=1); Iran (n=4); United Kingdom (n=7); New Zealand (n=1); Jordan (n=1); Canada (n=2); South Africa (n=1); Israel (n=1); Brazil (n=1). We had more than 10 countries included due to the inclusion of a systematic review design.
Considering the different study designs included, it is possible to verify that there are an equal number of qualitative (n=5) and quantitative (n=5) studies, followed by mixed methods (n=2) and systematic literature reviews (n=2). Concerning the care contexts observed, these include hospital inpatient units (n=6), long-term inpatient units (n=5), and, less frequently, palliative care teams (n=1). The sample consists of health professionals in general (n=4), nurses (n=8), and less frequently, caregivers and family members of people in palliative situations (n=2).
3.2. Data Presentation
To facilitate comprehension of the primary information within the included studies, Table 2 has been devised to consolidate data encompassing author/year of publication, primary objectives, methodology, sample/population under investigation, care context, and dimensions of communication and management of bad news in nursing with individuals in palliative situations and their respective caregivers/ family members.
4. Discussion
The communication and management of bad news when dealing with a person in a palliative situation and their caregivers or family members exhibits dimensions that are discernible before, during, and after the disclosure of the truth [19,28,29]. It is not possible to categorize the dimensions or separate them clearly by moments since they often occur simultaneously and continuously in the therapeutic relationship, assuming, however, different relevance throughout the process, contributing, in all circumstances, to the provision of nursing care centred on the person in palliative situations, their caregivers/family members [19,29,30,31,32,33]. To facilitate the discussion of the obtained data, it was chosen to analyse it by grouping the dimensions discovered through the structure and process of communication and management of adverse news in nursing with individuals in palliative care, along with the outcomes of effective communication and management of such news.
4.1. Dimensions of Structure of Communication and Management of Bad News
The identified dimensions related to the structure of communicating bad news in nursing were the characteristics of the person in a palliative situation and their caregivers/family members, the characteristics of the nurse, and the institutional and organizational culture.
The absence of prior information regarding diagnosis or prognosis significantly influences the reception of bad news and diminishes the individual's inclination to engage in meaningful discussions, respecting their preferences and end-of-life wishes [15,31]. Difficulties in acknowledging a poor prognosis and in comprehending the limitations and complexities of supportive treatments, conflicting care objectives between family members or the multidisciplinary team, and the reluctance to accept bad news due to the desire to maintain hope for a cure pose barriers to effective communication of bad news that are directly linked to the patient, family, and caregivers [35,36].
Regarding the characteristics of nurses, it was found that those who are more experienced, with a greater number of years of professional experience in a given context, generally experience fewer difficulties in communicating and managing bad news with the person in a palliative situation/ family members/ caregivers [15,32]. However, not only does the number of years of clinical practice contribute to the acquisition of skills, as training in the area of end-of-life communication significantly increases the confidence of health professionals, in their ability to have difficult conversations, in addition to increasing their skills to communicate with families in crises, manage emotional needs arising from bad news, manage family and professional conflicts and manage the communication of bad news at the end of life in general [15,19,32,37].
Organizational and institutional factors also often impede nurses' ability to have meaningful conversations with the person in palliative situations and their caregivers/ family members. The high workload and inadequate professional/ patient ratio often cause a lack of time for nurses to get to know the participants in-depth, building therapeutic relationships so that they can discuss clinical situations as a team, as well as conveniently and adequately inform people [30,35,38]. The lack of materials such as brochures or other informative documents and treatment protocols; lack of home support structures; insufficient hospitalization spaces when there is a need for symptomatic control or caregiver overload and the lack of a private place for communication also negatively affect the quality of communication and the revelation of the truth [35].
Teamwork is mentioned as a factor that facilitates the quality of communicating bad news, promoting reflection on positive and negative interactions and occurrences; facilitating the management of feelings, emotions, and complex situations; facilitating the management of time spent on communication, and allowing caregivers and family members to prepare for death [28,38]. To facilitate the communication of bad news, it is important that the team shares relevant information, such as prognosis and treatment and care objectives. The possibility for the reference nurse to be present when the truth is revealed and bad news is communicated, becoming aware of the information shared and the way in which it was shared, facilitates the subsequent management of communication by the remaining members of the multidisciplinary team. This sharing makes it possible to improve the quality of care provided; contributes to improving communication skills within the team itself; increases the satisfaction of the person/caregivers/family regarding the care received and allows for better management of the emotions of everyone involved [28,32,33,35]. However, there are documented situations in which the multidisciplinary team could become a barrier to communicating bad news. Situations in which there is an inability of the multidisciplinary team to reach a consensus regarding the treatment trajectory and objectives of care, the inability to achieve diagnostic certainty, or poor communication between team members are examples of this occurrence [35].
Nurses experience greater difficulties in communicating with members of the medical team, especially concerning the assessment of the person in a palliative situation, attributing these difficulties to the lack of collaboration between members of the multidisciplinary team, when providing end-of-life care [32].
There are, in general, no conflicts regarding the scope of intervention of each group as each one has its theoretically well-defined role [35], nonetheless, some feelings of devaluation or minimization of the scope of intervention of each group may arise [28,38], which corroborates the fact that the multidisciplinary team can either be a barrier or a facilitating factor in communication, depending on its functioning and dynamics.
4.2. Dimensions of Process of Communication and Management of Bad News
The dimensions related to the process of communicating bad news in nursing with the person in a palliative situation and their caregivers/ family members identified were: continuous and advanced training in end-of-life care; training in communication and breaking bad news; religiously and culturally sensitive nursing interventions; nursing interventions to promote hope and maintain faith; emotional management; therapeutic relationships; use of a bad news communication protocol; respect for autonomy, needs and preferences.
Communicating bad news effectively requires that nurses acquire, through pre- and postgraduate training, as well as reflective practice, a set of communication tools and structures that allow them to reveal the truth, answer difficult questions, and gather complex information with security, sensitivity, and empathy [30,32,35,39]. Although nurses feel prepared to provide care to people at the end of life, they often do not feel comfortable communicating bad news with the person in a palliative situation and their caregivers/ family members. This situation derives from the lack of communication skills that give them the confidence necessary to address complex topics as well as to manage the emotions that arise from these conversations [15,19,36].
Studies indicate that caregivers and family members supported by professionals trained in the area of communicating bad news recognize the good work and the positive repercussions that adequate communication and information have on themselves and on the person in a palliative situation, thus reinforcing the relevance of training and communication skills training [37,39].
Providing training in communicating bad news based on the application of a model (COMFORT, SPIKES, ABCDE, or others] is effective in improving the quality of communication perceived not only by the person in a palliative situation and their caregivers/ family members but also by the professionals themselves, increasing their confidence to approach difficult topics, to manage bad news and family crises and topics related to the end of life in general [37]. The use of a protocol when communicating bad news is associated with greater skills and experience in this area, however, studies indicate that the majority of nurses do not anchor the communication of bad news in any specific model [15]. It is also important that nurses' training includes the acquisition of communication skills that are culturally sensitive, as communication needs and ways of approaching bad news and the end of life are different between cultures and/or religions. For this reason, it is particularly important to acquire communication skills that allow them to effectively address the psychological and spiritual aspects of death so that they can reveal bad news while maintaining the hope of the patient and their caregivers/family members and avoiding cultural and religious conflicts [15,36]. Also, the felt need to reveal the truth, as well as the way professionals’ approach bad news and the end of life are different between cultures and/or religions. Despite the widespread trend towards greater and more detailed revelation of the truth at the end of life, cultural and religious differences continue to exist, particularly those related to diagnoses and prognoses of illness. In various cultures/religions, family pressure is common so that the truth is not revealed to the person in a palliative situation (conspiracy of silence) since knowledge could cause hopelessness or lack of faith. In some cultures, such as Asian cultures, there is a tendency for people in palliative situations not to be informed, nor to participate in the decision-making process regarding their end of life. This situation often occurs at the request of the person in palliative situations, not necessarily the result of the professional's lack of communication skills or their reluctance to address difficult topics. However, studies have demonstrated the existence of significant differences between truth-telling practices on the part of health professionals, between cultures, namely Asian and Eastern, when compared to those of Western countries, especially concerning diagnoses and prognoses [36,40]. Religious health professionals may experience greater difficulties in communicating and managing bad news with the person in a palliative situation/family/caregivers [32].
Communicating bad news brings about emotions and feelings that nurses often do not feel prepared to deal with, often avoiding moments of revealing the truth to self-protect. Managing bad news at an emotional level is reported to be as challenging or more challenging as revealing bad news, and it is common for ill-prepared nurses to withdraw from contact with the person in a palliative situation, their caregivers/family members after the moment of revelation. the bad news for not being able to deal with other people's emotions [19,30,32,36,38]. This emotional barrier in managing bad news becomes even more complex in situations in which the person in a palliative situation/ family/ caregivers expresses negative reactions to the news received [32,33] or when the people in a palliative situation are younger [15]. Situations in which the professional identifies with the experiences of the patient, caregivers, or family members are especially likely to cause emotional suffering for nurses [33].
Nurses also experience difficulties in maintaining the balance between revealing the truth and promoting hope, stating that, if on the one hand, they must reveal the truth, on the other they feel that they should not do so in a way that causes feelings of hopelessness and despair; This balance is fragile and causes difficulties in the emotional management of all communication participants [15,32,33,36].
Open and honest communication allows the therapeutic relationship with health professionals and promotes a caring environment based on truth and respect for the autonomy of the person being cared for [39], also contributing to reducing suffering, anxiety, and feelings of loss of control and insecurity related to the disease process [28].
4.3. Dimensions of Outcome of Communication and Management of Bad News
The dimensions related to the outcome of the process of breaking bad news in nursing with the person in a palliative situation and their caregivers/ family members found were adaptation to the disease process and decision-making capacity of the person in a palliative situation and their caregivers/ family members.
Communicating bad news effectively allows the person and their caregivers/ family members to have the information necessary to make informed decisions, thus promoting active and appropriate participation in decisions about their care or treatment plan. As a two-way channel, by communicating in a truly open way, and promoting the establishment of therapeutic relationships, nurses better understand the needs, desires, and preferences of the people they care for [31,40].
Insufficient communication or failure to address bad news can cause distress for the person and their caregivers/family members. The fact of not being informed about your diagnosis or prognosis makes it difficult to adapt to the disease process and makes it impossible to satisfy your last wishes and desires [28,39,40].
The pact, or conspiracy, of silence, is a dynamic often established to spare the person in a palliative situation from greater suffering. Evidence suggests that failure to reveal, or deny, the truth often leads to feelings of isolation and complicated grief [39]. In this way, open communication, with family involvement in communicating bad news and revealing the truth, often leads to the person in a palliative situation maintaining a more positive attitude towards death and being more willing to discuss preferences and care in end-of-life [40], contributing to the provision of holistic care focused on the needs and preferences of the person, as well as their caregivers and family members.
4.4. Limitations and Suggestions
As limitations present in the scoping review, the restriction of included studies to the time limit of the previous 5 years stands out, as well as the fact that studies in other languages, in addition to English, Portuguese, and Spanish, were excluded, which may have led to relevant studies may not have been subject to analysis. The scoping methodology only informs clinical practice about which dimensions interfere in the communication and management of bad news, since it does not have the scope to provide guidelines/recommendations. Future effectiveness studies are considered necessary to clarify the results of nurses communicating and managing bad news on the well-being of individuals and their families, as well as demonstrate whether interventions require adaptations depending on the care environments.
5. Conclusions
The communication and management of bad news in nursing with people in palliative situations and their caregivers/ family members present dimensions that become evident before the moment of revealing the truth, during and after the revelation of truth, assuming different relevance throughout the communication process of bad news, but crucially contributing to communication centered on the person, their preferences, desires, and needs.
Interacting with family and caregivers adds complexity to care and emotional weight to the relationship, especially when there are unrealistic and inappropriate expectations, making the balance between the relational dynamics and the values of the person in a palliative situation complex (30,32]. Given the impact that the therapeutic relationship in palliative care seems to have on the multidisciplinary team, in general, and on nurses in particular, as well as its potential for burnout, institutions should recognize such ramifications and provide conditions for professionals to process situations with complex experiences, promoting a culture of collective care open to joint reflection and personal, professional and team growth.
Supporting patients and their family members as they approach the end of life, helping to rehabilitate sequelae and adapt to successive losses resulting from the disease process, requires ongoing professional development and the recognition of communication as a vital skill to ensure the provision of quality holistic care. We suggest future studies of effectiveness to make clear the component of nursing intervention in communicating and managing the bad news in palliative care.
Author Contributions
Conceptualization, T.M, A.R. and E.S; methodology, T.M, A.R. and E.S.; software, T.M, A.R., and E.S.; validation, T.M, A.R., E.S, C.F. and L.P..; formal analysis, T.M, A.R., and E.S; investigation, T.M, A.R., and E.S resources, C.F and L.P..; writing—original draft preparation, T.M, A.R., and E.S; writing—review and editing, T.M, A.R. and E.S; supervision, A.R. and E.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and The PRISMA 2020 statement.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. Palliative Care factsheets [Internet]. 2020 [cited 2023 Nov 2]. Available online: https://www.who.int/news-room/fact-sheets/detail/palliative-care.
- World Health Organization. Palliative Care Key Facts [Internet]. 2023 [cited 2023 Nov 3]. Available online: https://www.who.int/europe/news-room/fact-sheets/item/palliative-care.
- Ezer T, Lohman D, de Luca GB. Palliative Care and Human Rights: A Decade of Evolution in Standards. J Pain Symptom Manage [Internet]. 2018, 55, S163–9. [CrossRef]
- Lei 52/2012. Lei de Bases dos Cuidados Paliativos [Internet]. Assembleia da Republica, Serie I; 2012 p. 5119–24. Available online: https://data.dre.pt/eli/lei/52/2012/09/05/p/dre/pt/html.
- Harding Z, Hall C, Lloyd A. Rehabilitation in palliative care: a qualitative study of team professionals. BMJ Support Palliat Care [Internet]. 2022, 12, 28–38. [CrossRef]
- Silva R, Paiva M, Vital F, Moura MJ, Lourenço J, Lopes JM. Plano Estratégico para o Desenvolvimento dos Cuidados Paliativos 2021-2022 2 Comissão Nacional de Cuidados Paliativos: Com o contributo dos Coordenadores Regionais: Ordem dos Médicos Ordem dos Enfermeiros Ordem dos Psicólogos [Internet]. 2021. Available online: https://www.acss.min-saude.pt/wp-content/uploads/2017/01/PEDCP-2021_2022.pdf.
- Querido A, Salazar H, Neto IG. Comunicação. In: Barbosa A, Pina PR, Tavares F, Neto IG, editors. Manual de Cuidados Paliativos. 3rd ed. Lisboa: Faculdade de Medicina de Lisboa; 2016. p. 815–31.
- Kwame A, Petrucka PM. A literature-based study of patient-centered care and communication in nurse-patient interactions: barriers, facilitators, and the way forward. BMC Nurs. 2021, 20, 1–11.
- McCormack B, McCance T. Person-centred Practice in Nursing and Health Care: Theory and Practice. 2nd ed. Wiley Blackwell; 2017.
- Alfriyie, D. Effective Communication between nurses and patients: an evolutionary concept analysis. Brittish J Community Nurs. 2020, 7, 505–512. [Google Scholar]
- Mehnert A, Koranyi S. Kommunikation mit schwerstkranken Patienten – mehr als nur Breaking Bad News. Ther Umschau [Internet]. 2022, 79, 29–35. [CrossRef]
- Pontes AC, Leitão IMTA, Ramos IC. Comunicação terapêutica em Enfermagem: instrumento essencial do cuidado. Rev Bras Enferm. 2008, 61, 312–318.
- Wittenberg-Lyles E, Goldsmith J V., Ferrell BR, Ragan SL, Oxford University Press. Communication in Palliative Nursing. Druk: Oxford University Press; 2017.
- Dahlin C, Wittenberg E. Communication in Palliative Care. In: Ferrell BR, Paice JA, editors. Oxford Textbook of Palliative Nursing. 5th ed. Oxford: Oxford University Press; 2020. p. 55–77.
- Sánchez AR, Beltrán MJM, Arribas Marín JM, de la Torre-Montero JC, Gil BB, García M del CM, et al. The Communication of Bad News in Palliative Care: The View of Professionals in Spain. Am J Hosp Palliat Med. 2023, 1–12.
- Al-Johani WM, Alshamlan NA, Alghamdi MF, Alabdulkader AM, Aljohani WM, Alghamdi RF, et al. Breaking Bad News of a Cancer Diagnosis: A Mixed-Methods Study of Patients’ Perspectives. Patient Prefer Adherence. 2022, 16, 3357–3369.
- Kumar V, Sarkhel S. Clinical practice guidelines on breaking bad news. Indian J Psychiatry. 2023;65(2):238.
- Arber A, Gallagher A. Breaking bad news revisited: the push for negotiated disclosure and changing practice implications. Int J Palliat Nurs. 2003, 9, 166–172.
- Wahyuni S, Gautama MSN, Simamora TY. A Literature Review of Nurses Challenges and Barriers in Assisting Patients and Families Facing Breaking Bad News. Indian J Palliat Care. 2023, 29, 243–249.
- Ptacek JT, Ptacek JJ, N. M. E. I’m sorry to tell you..." - Physicians’ reports of breaking bad news. J Behav Med [Internet]. 2001, 24, 205–217. [CrossRef]
- Koch A, Mantzouris S. Nurses’ Role in Providing Comprehensive Communication, Prognostication, and Palliative Care During the COVID-19 Pandemic. J Hosp Palliat Nurs [Internet]. 2020, 22, 442–446, Available online: https://search.ebscohost.com/login.aspx?direct=true&AuthType=ip,shib&db=mdc&AN=32947392&lang=pt-pt&site=ehost-live.
- Hernández-Marrero P, Fradique E, Pereira SM. Palliative care nursing involvement in end-of-life decision-making: Qualitative secondary analysis. Nurs Ethics [Internet]. 2019, 26, 1680–1695, Available online: https://search.ebscohost.com/login.aspx?direct=true&AuthType=ip,shib&db=mdc&AN=29807491&lang=pt-pt&site=ehost-live.
- Peters MDJ, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. 2020, 18, 2119–2126.
- Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis [Internet]. JBI; 2020. [CrossRef]
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann Intern Med. 2018, 169, 467–473.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021, 372.
- Aromataris E, Munn Z. JBI Manual for Evidence Synthesis. 2020.
- Rylander A, Fredriksson S, Stenwall E, Gustafsson LK. Significant aspects of nursing within the process of end-of-life communication in an oncological context. Nord J Nurs Res [Internet]. 2018, 39, 85–91, Available online: https://search.ebscohost.com/login.aspx?direct=true&AuthType=ip,shib&db=ccm&AN=136876626&lang=pt-pt&site=ehost-live.
- Yazdanparast E, Arasteh A, Ghorbani SH, Davoudi M. The effectiveness of communication skills training on nurses’ skills and participation in the breaking bad news. Iran J Nurs Midwifery Res. 2021, 26, 337–341.
- Kerr D, Milnes S, Ammentorp J, McKie C, Dunning T, Ostaszkiewicz J, et al. Challenges for nurses when communicating with people who have life-limiting illness and their families: A focus group study. J Clin Nurs [Internet]. 2019, 29, 416–428, Available online: https://search.ebscohost.com/login.aspx?direct=true&AuthType=ip,shib&db=ccm&AN=141095716&lang=pt-pt&site=ehost-live.
- Gonella S, Basso I, Clari M, Dimonte V, Di Giulio P. A qualitative study of nurses’ perspective about the impact of end-of-life communication on the goal of end-of-life care in nursing home. Scand J Caring Sci [Internet]. 2020, 35, 502–511, Available online: https://search.ebscohost.com/login.aspx?direct=true&AuthType=ip,shib&db=ccm&AN=150251590&lang=pt-pt&site=ehost-live.
- Toh SW, Hollen VT, Ang E, Lee YM, Devi MK. Nurses’ communication difficulties when providing end-of-life care in the oncology setting: a cross-sectional study. Support Care Cancer [Internet]. 2020, 29, 2787–2794, Available online: https://search.ebscohost.com/login.aspx?direct=true&AuthType=ip,shib&db=mdc&AN=32997186&lang=pt-pt&site=ehost-live.
- Francis L, Robertson N. Healthcare practitioners’ experiences of breaking bad news: A critical interpretative meta synthesis. Patient Educ Couns. 2023, 107, 107574.
- Lukewich JA, Tranmer JE, Kirkland MC, Walsh AJ. Exploring the utility of the Nursing Role Effectiveness Model in evaluating nursing contributions in primary health care: A scoping review. Nurs Open. 2019, 6, 685–697.
- Kimura Y, Hosoya M, Toju K, Shimizu C, Morita T. Barriers to end-of-life discussion with advanced cancer patient as perceived by oncologists, certified/specialized nurses in cancer nursing and medical social workers. Jpn J Clin Oncol [Internet]. 2020, 50, 1426–1433, Available online: https://search.ebscohost.com/login.aspx?direct=true&AuthType=ip,shib&db=mdc&AN=32844993&lang=pt-pt&site=ehost-live.
- Alshammari F, Sim J, Lapkin S, McErlean G. Registered Nurses’ attitudes towards end-of-life care: A sequential explanatory mixed method study. J Clin Nurs [Internet]. 2023, 32, 7162–7174, Available online: https://search.ebscohost.com/login.aspx?direct=true&AuthType=ip,shib&db=ccm&AN=172046230&lang=pt-pt&site=ehost-live.
- Fuoto A, Turner KM. Palliative Care Nursing Communication: An Evaluation of the COMFORT Model. J Hosp Palliat Nurs [Internet]. 2019, 21, 124–130, Available online: https://search.ebscohost.com/login.aspx?direct=true&AuthType=ip,shib&db=ccm&AN=135343052&lang=pt-pt&site=ehost-live.
- Gonella S, Conti A, Albanesi B, Antal A, Dimonte V, Di Giulio P. Lived experiences of end-of-life communication among nursing home staff: An interpretive phenomenological study. J Adv Nurs [Internet]. 2022, 79, 698–710, Available online: https://search.ebscohost.com/login.aspx?direct=true&AuthType=ip,shib&db=ccm&AN=161474312&lang=pt-pt&site=ehost-live.
- Ibañez-Masero O, Carmona-Rega IM, Ruiz-Fernández MD, Ortiz-Amo R, Cabrera-Troya J, Ortega-Galán ÁM. Communicating Health Information at the End of Life: The Caregivers’ Perspectives. Int J Environ Res Public Health [Internet]. 2019, 16, 2469, Available online: https://search.ebscohost.com/login.aspx?direct=true&AuthType=ip,shib&db=mdc&AN=31336698&lang=pt-pt&site=ehost-live.
- Tang, Y. Death attitudes and truth disclosure: A survey of family caregivers of elders with terminal cancer in China. Nurs Ethics [Internet]. 2018, 26, 1968–1975, Available online: https://search.ebscohost.com/login.aspx?direct=true&AuthType=ip,shib&db=mdc&AN=30428754&lang=pt-pt&site=ehost-live. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flowchart of the article selection process.
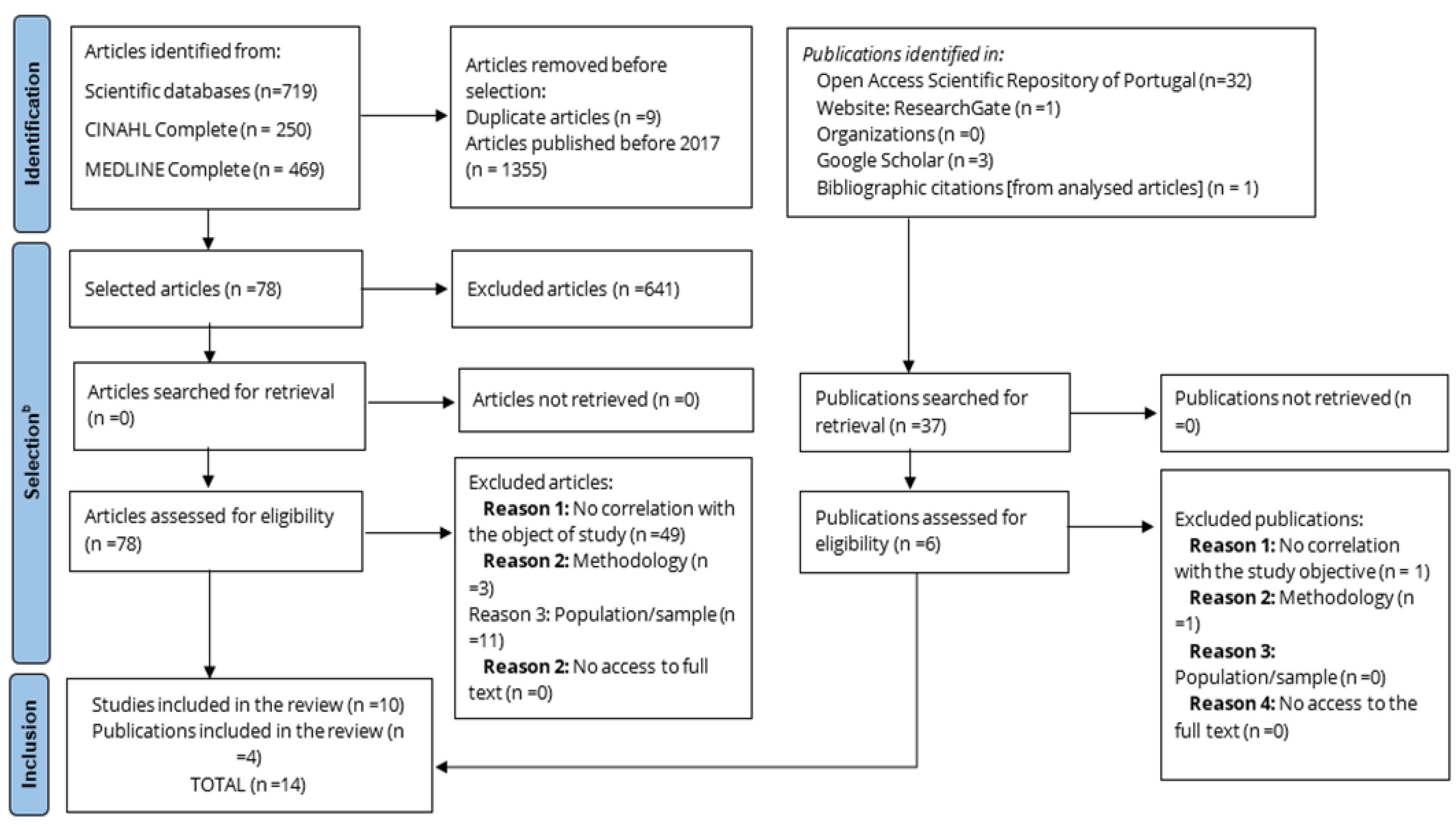

Table 1.
MEDLINE Complete (EBSCOhost) AND CINAHL Complete (EBSCOhost) search strategy conducted on December 10, 2023.
Table 1.
MEDLINE Complete (EBSCOhost) AND CINAHL Complete (EBSCOhost) search strategy conducted on December 10, 2023.
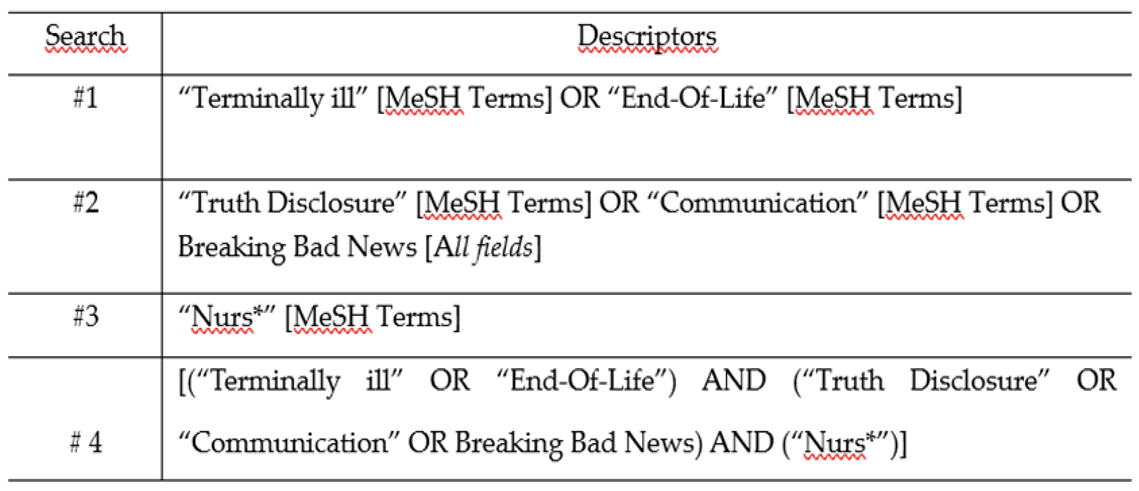 |
Table 2.
Systematisation of articles and publications included in the Scoping Review.
| Author(s)/ Publication year/ Country |
Objective/ Aim |
Methods |
Population under study Sample composition Context of care |
Dimensions of communication and management of bad news carried out by nurses, to the readaptation in palliative care |
|---|---|---|---|---|
| Alshammari et al. (2023) [28] Saudi Arabia |
To examine nurses' attitudes towards end-of-life care and explore barriers and facilitating factors that influence the provision of quality end-of-life care. | Mixed methods. (Data collection instruments: questionnaire and semi-structured interviews) |
1293 nurses in a hospital context Inpatient services: internal medicine, surgery, cardiology, oncology and palliative care in five major hospitals. |
Research indicates that nurses exhibit confidence and readiness in administering end-of-life care, yet they express a lack of preparedness in effectively communicating about end-of-life matters and managing associated emotions. Their deficient communication skills present a notable barrier to delivering high-quality end-of-life care. Furthermore, there is a demonstrable absence of experience and assurance in initiating nuanced conversations that navigate the delicate balance between fostering optimism and conveying challenging realities. |
| Fuoto & Turner (2019) [29] United Satates of America) |
Implement the COMFORT communication model to increase nurses' confidence and satisfaction in end-of-life communication and improve patient-family satisfaction with the care provided after implementing the COMFORT model. |
Mixed methods. (Data collection instrument: questionnaire) |
19 nurses working in a long-term palliative care inpatient unit. 50 family members of people living in an inpatient unit who had died, within a certain time limit. |
Training nurses in communication using the COMFORT model has been shown to increase their confidence and satisfaction when interacting with end-of-life clients. The potential of the COMFORT model extends beyond end-of-life care and could be utilized in other areas of nursing to develop skills necessary for facilitating care approaches. |
| Tang (2018) [30] China |
Describe the attitudes of family caregivers towards death and revealing the truth. | Quantitative study (Data collection instrument: questionnaire survey) |
140 caregivers/ family members of elderly people with terminal cancer admitted to long-term care units | Ineffective communication of content related to the end of life results from the lack of discussion with family caregivers about this topic as well as their difficulty in managing bad news related to the end of life of their family members. Family caregivers perceive the training of health professionals in communicating and managing bad news as being fundamental; They also understand that training in this area influences how each health professional approaches bad news situations in their daily practice. |
| Gonella et al. (2020) [31] Italy |
Explore nurses’ perspectives on how communication influences end-of-life care planning in long-term care. | Qualitative descriptive study (Data collection instrument: semi-structured interviews) |
14 nurses working in different long-term care institutions and involved in caring for residents during their last week of life. | Factors that influence the quality of communication at the end of life: life crises/transitions (physical deterioration; social problems, multiple hospitalisations and warning shots); person-centred environment; occasion of addressing the possibility of death, quality of relationships and culture of care. |
| Gonella et al. (2022) [32] Italy |
Explore and understand experiences about end-of-life communication among professionals in long-term care institutions. | Qualitative study (Data collection instrument: semi-structured interviews) |
21 multidisciplinary team members involved in end-of-life communication in long-term care institutions. |
Factors that hinder communication at the end of life: difficulty in managing feelings and emotions (of oneself and of family members/caregivers); high workload and inadequate professional/institutionalized individual ratio. Teamwork as a facilitator of the quality of communication at the end of life: promotes reflection on the quality of communication; facilitates the management of feelings, emotions and complex situations; facilitates time management for communication and allows families/caregivers to prepare for death. |
| Toh et al. (2020) [33] Singapore |
Examine communication difficulties experienced by nurses when providing end-of-life care; establish a correlation between communication difficulties and the participants and determine the impact of sociodemographic factors on the communication difficulties experienced. | Quantitative study (Data collection instrument: cross-sectional questionnaire survey) |
124 nurses working in four oncology inpatient units of a hospital. | Nurses experience greater difficulties in communicating with the person in a palliative situation/ family/ caregiver than with the multidisciplinary team, however, when difficulties are experienced in communicating with the multidisciplinary team, these are even more evident in communicating with the person in a palliative situation/ family/caregiver. Nurses who experience greater difficulty in communication are: younger, more inexperienced, have less academic training, have no training in end-of-life care and have religious practices. |
| Ibañez-Masero et al. (2019) [34] Spain |
Understand the experiences of caregivers in relation to health information and communication through the course of illness and death of family members. | Phenomenological qualitative study (Data collection instruments: unstructured interviews) |
123 caregivers accompanying people at the end of life for more than 2 months and less than 2 years | Inadequate communication of bad news causes distress for the person and their family/caregivers. Training in communicating bad news is recognized by caregivers as important and has positive repercussions on the process of illness and death. Conspiracy/Pact of silence: greater suffering, isolation and complicated grief. Society's secrecy attitude towards death makes it difficult to normalize it and prepare each person for death. |
| Rylander et al. (2018) [35] Sweden |
Describe important nursing aspects in the end-of-life communication process in the context of oncological palliative care. | Qualitative, descriptive and exploratory study (Data collection instrument: semi-structured interviews) |
10 nurses working in an oncology inpatient service (acute and chronic both in active and palliative treatment) at a university hospital. | Nurses have a crucial role in all phases of the process of revealing the truth/communicating and managing bad news, having the ability to reduce anxiety and the suffering resulting from it for the person in a palliative situation, family and/or caregivers. Members of the multidisciplinary team must bring clarity to care, being interconnected in a unidirectional flow of care aimed at the person's well-being. Barriers to communicating and managing bad news: lack of information about the person's prior knowledge; single-minded focus on medical issues despite poor prognosis; revelation of the truth controlled by the medical team and lack of cooperation; non-existent or weak therapeutic relationships. |
| Kerr et al. (2019) [36] Australia |
List the communication problems that nurses consider challenging when caring for people with life-limiting illnesses | Qualitative study (Data collection instrument: focus group) |
39 nurses working in three hospital inpatient units. |
Communication problems identified: Deficit in skills for communicating bad news/complex conversations; complexity in the interaction between the professional and the families and caregivers of the person in a palliative situation; Organizational factors impede nurses' ability to have meaningful conversations with the person in a palliative situation and their caregivers/family members. |
| Kimura et al. (2020) [37] Japan |
Identify barriers to discussing the end of life with people with advanced cancer/ family members perceived by oncologists, oncology nurses and social workers; Clarify views on effective strategies to facilitate end-of-life discussion. |
Quantitative study (Data collection instrument: questionnaires) |
4354 healthcare professionals in the field of medical oncology working in 402 hospitals (494 oncologists, 993 nurses and 387 social workers) |
Barriers related to the person/family/caregivers: acceptance of a bad prognosis; understanding the limitations and complications of supportive treatments; conflicting care goals; difficulty accepting bad news as it affects previous expectations. Organizational barriers: lack of treatment protocols; lack of informative documents; lack of time for clinical discussion; lack of home support and back-up facilities; lack of private place for communication. Barriers related to healthcare professionals: lack of training in carrying out difficult conversations/ communicating bad news; lack of agreement between team members regarding the objectives of care/treatment; diagnostic uncertainty; poor communication between team members. |
| Sánchez et al. (2023) [15] Spain |
Identify the aspects associated with communicating bad news in the context of palliative care. | Descriptive cross-sectional quantitative study (Data collection instrument: online questionnaire) |
206 health professionals (102 nurses, 88 doctors and 16 psychologists) working in palliative care teams. | Referrals to palliative care teams are often initiated without adequately informing individuals in palliative situations about their diagnoses or prognoses. Barriers to effectively communicating bad news by health professionals include a lack of specific training in this area, inadequate training in the use and management of a bad news reporting protocol, challenges in maintaining a delicate balance between honesty and promoting hope, and the implications for individuals in palliative situations, as well as their caregivers and young family members. |
| Wahyuni et al. (2023) [19] Iran (n=3) USA (n=3) United Kingdom (n=4) New Zealand (n=1) Jordan (n=1) |
Understanding the role, methods, obstacles, and challenges nurses face when communicating bad news in healthcare settings. | Systematic literature review | 12 articles were included, out of a total of 1075 articles. | Nursing intervention in the process of delivering bad news includes essential steps such as preparing the individual to receive distressing information, effectively communicating the news, managing the subsequent reactions, fostering interpersonal relationships, engaging in therapeutic communication, and providing emotional support. The barriers and challenges faced by nurses in this context are primarily attributed to a lack of skills and preparedness in handling the emotional reactions of others, as well as difficulties in managing their own emotional responses and those of others. The acquisition of skills through education and training is imperative for overcoming these existing barriers and elevating the overall quality of care provided in such situations. |
| Francis & Robertson (2023) [38] USA (n=1) United Kingdom (n=3) Sweden (n=1) Canada (n=2) South Africa (n=1) Israel (n=1) Australia (n=2) Brazil (n=1) Spain (n=1) Italy (n=1 |
Provide an overview of healthcare professionals' experiences in communicating bad news. | Systematic literature review | 14 articles were included, out of a total of 1723. | Experiences in communicating and managing bad news often involve discomfort, challenging emotional regulation, and physiological responses to the delivery of negative information. Healthcare professionals may also experience emotional distress due to their empathic connection with the situations of the sick individuals and their caregivers/family members. Furthermore, inadequate communication, fear of committing errors, and a prevailing culture of invulnerability that undervalues professional self-care can exacerbate these challenges. Revealing the truth can precipitate a challenging dialogue, potentially evoking feelings of professional isolation. Failing to acknowledge this difficulty, often associated with a culture of invulnerability that discourages the open expression of emotions, can elevate the risk of burnout and exhaustion among healthcare professionals. |
| Davoudi et al. (2021) [39] Iran |
Evaluate the effect of communication training on the level of skills and participation of nurses in communicating bad news. | Semi-experimental quantitative study (Data collection instrument: questionnaires |
60 nurses working in university hospitals in a city. | Barrier to communication/participation in communicating bad news: lack of skills and knowledge. To enhance nurses' involvement in breaking bad news, it is essential for them to acquire communication skills through training. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



