
Submitted:
08 July 2024
Posted:
09 July 2024
You are already at the latest version
Abstract
Background: Recent studies have found forward head posture (FHP) to be associated with altered physiology, however, there is a lack of research into whether FHP is associated with altered gait parameters when cognitively challenged. The current study was undertaken to investigate the changes in gait parameters in asymptomatic individuals with FHP when a cognitive dual task is introduced during walking. Methods: Ninety asymptomatic participants were recruited, 45 having FHP defined as having a craniovertebral angle (CVA) < 50, and 45 sex and age-matched controls having normal head posture (NHP) defined as CVA > 55. All participants walked along a 10 meter platform under a control condition (no cognitive load) with 3 consecutive trials while an optical motion-capture system consisting of 8 infrared cameras was used to assess gait kinematics. Secondly, participants were assessed under a dual task cognitive load condition (3 trials while performing simple addition, counting backwards, and answering yes or no questions) to identify the impact on gait kinematics compared to the control condition. Results: Under the single task condition, there were no significant differences for any gait parameter, however, under the dual task condition, 12/13 gait parameters were significantly altered for the FHP group compared to the NHP group (p < .01). A calculation of dual task cost (DTC) percentage showed significant increases in all gait parameters in participants with FHP (p < .02). Correlations between the CVA and gait parameters were not significant for the single task condition, but all gait parameters were correlated to CVA for the dual task condition (p < .01). The correlation between CVA and DTC for all gait variables were also significant (p < .04). Conclusions: This study demonstrates that FHP significantly increases the cognitive cost during walking, highlighting the importance of proper postural alignment for maintaining cognitive function under a dual task condition. Addressing FHP through targeted interventions could improve both physical and cognitive health, enhancing overall well-being and daily functioning.
Keywords:
Craniovertebral angle
; forward head posture
; cognition
; cognitive function
; gait
; dual task
1. Introduction
The debate surrounding forward head posture revolves around the question of whether it should be considered a normal variant or an abnormal condition that requires correction [1]. Forward head posture (FHP), where the head protrudes forward relative to the shoulders [2], is a common phenomenon, especially in today's digital age with increased screen time and sedentary lifestyles [3].
While pain can be a significant indicator of postural disorders [4], solely relying on pain to pathologize the FHP can be misleading. Not everyone with FHP experiences immediate pain or discomfort, some individuals may develop compensatory mechanisms to cope with their posture [5], which can temporarily mask pain but exacerbate problems in the long run. The situation of a lack of current pain might lead individuals to overlook the importance of diligently working to attain a more correct posture. It is essential to recognize that a comprehensive approach that goes beyond pain assessment ensures a more nuanced understanding of FHP and helps to uncover the underlying causes and potential risk factors associated with FHP.
In regards to asymptomatic individuals with FHP, in our previous research, we conducted a comprehensive analysis of specific physiological parameters related to the presence of FHP [6,7,8,9,10,11,12]. We focused on investigating the correlation between FHP in asymptomatic individuals and its impact on cervical spine nerve root evoked potentials [6], autonomic nervous system activity and sensorimotor control [7], central sensory processing and sensorimotor integration [8,9,10], athletic performance [10,11], and cardiopulmonary function [12]. Building upon this intriguing groundwork, our current emphasis is on the captivating exploration of the relationship between posture displacement (termed subluxation or altered alignment [1]) and cognitive function. This topic has emerged as a compelling avenue for further research and understanding with only sparse information available on how FHP might alter brain activity [13].
Although it has long been thought that cognitive function is associated with musculoskeletal disease [14,15], whether cognitive function and posture have a direct impact on each other or to what extent they affect each other is largely unknown. Recently, the relationship between posture subluxation and cognitive function has emerged as an intriguing area of research, and evidence suggests that these two factors may be interconnected [13]. Posture subluxation, which refers to the misalignment of vertebrae in the spine relative to either a defined ideal posture or a referenced range of normal values [16], can lead to altered sensory input and proprioception [7], affecting the body's postural control. This disruption in postural stability has been found to influence cognitive function [13,17]. Studies have shown that individuals with posture subluxations may experience deficits in attention, processing speed, and memory, this is especially true in older aged individuals [18]. Moreover, aberrant proprioceptive signals resulting from subluxations can impact the brain's ability to integrate sensory information effectively [19], where sagittal imbalance (altered posture) has been found to correlate to cognitive decline in older persons [20]. Thus, posture subluxations in the sagittal plane may not only be linked to musculoskeletal health [3,4] but could also hold potential benefits for cognitive function and overall brain health [13,15,20].
Neurophysiologically, it has been found that vertebral subluxation has a close link with altered somatosensory processing particularly in the prefrontal cortex (PFC) [21]. The prefrontal cortex is known to be a key structure responsible for the performance of what is known as “executive functions” [22]. The neuroanatomical connectivity of the PFC to most parts of the cortical and subcortical brain makes it well suited for participating in a number of neural networks and carrying out cognitive control operations in different functional domains [23]. Cognitive control is a term usually associated with the healthy functioning of the PFC and related regions such as the cingulate cortex [23].
In this context, dual-task gait, a method of assessment that evaluates gait performance while simultaneously performing a simplistic cognitive task, has emerged as a promising tool for predicting cognitive decline and assessing overall cognitive function [24]. As individuals age or experience cognitive impairments, the ability to perform dual tasks becomes more challenging due to increased cognitive demands [25]. Research has shown that gait performance during dual-task conditions can serve as a predictive indicator of cognitive decline and may help identify individuals at risk for developing cognitive impairments [26]. Furthermore, dual-task gait assessments can detect subtle changes in cognition that might not be evident during single-task gait evaluations [27]. The integration of cognitive and motor tasks in the dual-task paradigm provides a more ecologically valid measure of real-world functioning, making it a valuable tool for assessing cognitive function in various populations, including older adults and those with neurological conditions [28].
Despite the high prevalence of FHP, few studies have evaluated the effect it has on gait parameters during a dual task, where only one previous investigation was identified [29]. In this previous investigation, Moustafa and colleagues identified that whiplash injured populations had a greater dual-task cognitive cost during walking compared to a matched population of chronic neck pain and asymptomatic controls; this increase cognitive cost was correlated to FHP magnitude and altered sensori-motor integration as measured with the N-30 potential’s amplitude [29]. Due to the scarcity of available data on this topic, the current study was undertaken to investigate the changes in gait parameters in university students and staff with FHP when a cognitive dual task is introduced during walking. The core of our hypothesis is that individuals with forward head posture and those without will demonstrate different responses when undergoing dual-task assessment.
2. Materials and Methods
2.1. Study Design, Participants and Setting
The comparative design was used to evaluate the effect of cognitive dual task on gait parameters in participants with forward head posture compared to a group of strictly matched control participants without FHP. The study was carried out in the laboratories of the University of Sharjah and involved participants who are students and staff members of the same institution. Recruitment efforts were conducted through social media platforms. Ethical approval was received from the University of Sharjah (College of Health Sciences, University of Sharjah, UAE) (Ethical approval number: REC-21-03-11-03-S) and ensured that all participants provided informed consent in accordance with appropriate guidelines and regulations before data collection.
2.2. Inclusion and Exclustion Criteria
To classify an individual with FHP, the craniovertebral angle (CVA) measurement was utilized, and established cutoff values from previous publications were adhered to. Following the data provided by Yip et al. [30], FHP was defined as having a CVA of less than 50°. Therefore, participants were categorized as having FHP if their CVA measured less than 50°. On the other hand, the control group was defined as individuals with normal or no FHP, characterized by a CVA measurement greater than 55° for each participant. Exclusion criteria for the current investigation were as follows: (i) recent fractures; (ii) BMI > 30; (iii) a history of significant injury or primary musculo-skeletal surgical interventions; (iv) deformity of the spine or extremities; and (v) pregnancy or malignancy.
2.3. Study Tools and Outcome Measures
2.3.1. Craniovertebral Angle (CVA)
The CVA is reliable and valid for assessment of FHP [31]. To accurately measure the FHP degree, a photogrammetry method was followed measuring the CVA angle in the sagittal plane. The craniovertebral angle was measured in a standing position by using an imaginary horizontal line passing through the C7 spinous process, as well as another line from the C7 spinous process to the tragus of the ear as shown in Figure 1. The standing posture position was used to measure the CVA as recent evidence indicates a significant difference in sitting vs. standing postures where sitting overestimates the amount of FHP (reduces the CVA) [32] and our study focused on upright gait kinematics such that the standing CVA seemed more appropriate for our analysis. The angle was determined at the point where these two lines intersected. A larger CVA value indicates a more desirable alignment of the head and neck, while a smaller angle indicates a more severe degree of FHP. Participants with an angle of less than 50° were included in the study group, while a control group was selected with a craniovertebral angle greater than 55°, matched to the study group.
2.3.2. BTS GAITLAB System
The spatiotemporal and kinematic parameters of gait were evaluated using an optical motion-capture system consisting of 8 infrared cameras (Smart-D, BTS Bioengineering, Milan, Italy) operating at a frequency of 120 Hz (Figure 2).
Prior to conducting the experimental tests, anthropometric measurements such as height, weight, the distance between the anterior superior iliac spines, pelvis thickness, knee and ankle width, and leg length were obtained as (Figure 3, Figure 4 and Figure 5). As illustrated in Figure 6, 22 spherical reflective passive markers were placed on the participant's skin following the protocol outlined by Davis et al. [33].
2.3.3. Dual Task Cost (DTC) Percentage
The average performance across the three dual-task trials was used for analysis to provide a robust measure of the cognitive load’s impact on gait. The dual task cost (DTC) percentage was calculated by determining the difference between single and dual-task performance scores, dividing the result by the single-task performance score, and then multiplying by 100. For example, if the average single task walking speed was 1.2 m/s and the average dual-task walking speed was 1.0 m/s, the DTC percentage would be calculated as .
Higher DTC percentages indicate a greater impact of the cognitive task on gait performance, highlighting the extent to which cognitive load affects the ability to maintain a normal walking pattern [34]. This method allowed for a comprehensive evaluation of the interplay between cognitive demands and gait performance in individuals with and without FHP.
2.3.4. Spatiotemporal Parameters and Cognitive Performance
Participants' spatiotemporal parameters such as step length, speed, and cadence were assessed under both single-task and dual-task conditions using the BTS gait lab system. The comprehensive gait analysis included the following 13 variables and left and right sides were averaged for analysis unless there was only a specific sided difference which is then reported as side specific in the results:
- Stride time in seconds (s);
- Stance time (s);
- Swing time (s);
- Stance phase (%);
- Swing phase (%);
- Single support phase (%);
- Double support phase (%);
- Mean velocity (meters (m)/s);
- Mean velocity (%height/s);
- Cadence (steps/minute (min);
- Stride length (%height);
- Step length (m);
- Step width (m).
Cognitive performance during dual-task trials was evaluated based on the accuracy and consistency of responses to cognitive tasks, providing insights into the impact of cognitive load on gait performance. The designed pathway was equipped with the BTS gait lab system to capture gait parameters in both conditions. During the dual-task trials, participants were monitored to ensure they performed both tasks simultaneously, with gentle reminders provided if necessary to maintain dual-task engagement.
2.4. Study Procedure
Participants were instructed to walk at their self-selected pace along a 10 m walkway while the 3D trajectories of the markers were captured by the cameras under two conditions: single-task and dual-task (Figure 7). In the single-task condition, participants walked at their preferred speed without performing any additional tasks, completing at least three trials to establish baseline gait parameters. The average performance across these trails was used for subsequent analysis [35]. For the dual-task condition, participants were instructed to walk at their preferred speed while simultaneously performing various cognitive tasks, with no emphasis on prioritizing either the gait or cognitive task. These tasks included three conditions:
- (1)
- Answering yes or no questions;
- (2)
- Counting forward or backward from a 3-digit number;
- (3)
- Or performing simple mathematical calculations.
Each participant completed at least three trials for the dual-task condition, with different instructions provided for each trial. This approach ensured a comprehensive assessment of cognitive load effects [27]. A trial set was considered valid if at least 6 trials were accurately recorded, ensuring a sufficient number of gait cycles for further analysis. Rest periods between consecutive trials were allowed upon request. After completing the tests, the raw data were processed using specialized software (Smart Analyzer, BTS Bioengineering, Milan, Italy) to calculate the desired parameters.
2.5. Sample Size Determination
The required sample size was calculated based on the following parameters: an effect size of 0.5, representing a moderate effect size as per Cohen's criteria; a two-tailed significance level (α) of 0.05; and a power (1-β) of 0.80 to reduce the risk of type II errors. Using these parameters, the sample size was computed using G*Power 3.1 software. The calculations indicated that a minimum of 40 participants per group (FHP and NHP) would be needed to detect a significant difference with 80% power and a 5% level of significance. To account for potential dropouts, we added 5 participants per group, resulting in a total of 45 participants per group. Therefore, the final sample size was set at 45 participants per group, totaling 90 participants for the entire study.
2.6. Statistical Analysis
The distribution of all descriptive baseline variables was determined through the Kolmogorov-Smirnov test to ensure normalcy. Continuous data were presented as means accompanied by standard deviations (SD) in both the text and tables. To evaluate equality of variances, Levene’s test was employed at a 95% confidence level, where a p-value < 0.05 was considered significant. Descriptive statistics (means ± SD unless otherwise indicated) were reported at each time point.
To ensure group equivalence for proper case-control analysis with each demographic and clinical variable, chi-squared tests were applied for categorical variables and Student’s t-tests for continuous variables. The Student’s t-test was used to compare means of continuous variables between groups, with significance set at a p-value < 0.05. Effect size, measured using Cohen's d, indicated clinical importance with values of d ≈ 0.2, d ≈ 0.5, and d ≈ 0.8 representing negligible, moderate, and high clinical importance respectively.
Lastly, Pearson’s correlations (r) were used to examine relationships between head posture (CVA) and variables associated with spatiotemporal gait parameters during single and dual tasks, as well as between head posture and cognitive cost. Data analysis was performed using SPSS version 20.0 (SPSS Inc., Chicago, IL, USA), ensuring normality and equal variance assumptions were met prior to analysis.
3. Results
3.1. Demographics
More than 200 potential participants were primarily screened. Neck pain and shoulder pain were the most common reasons for participant exclusion. 45 participants with FHP (25 males, 20 females) and 45 age, BMI, and sex matched controls without FHP (25 males, 20 females) were recruited. Figure 8 shows Box plot for the CVA.
3.2. Single Task Detailed Results
In this study, several gait parameters were analyzed to compare individuals with FHP to those in a control group with neutral head posture (NHP) under single and dual-task conditions. Mean differences between spatiotemporal parameters in FHP and NHP groups during single task walking are shown in Table 2. No statistically significant differences between any of the gait variables were observed. Likewise, all effect sizes were small to insignificant and were not statistically significant. See Table 2.
3.3. Dual Task Detailed Results
The results, summarized in Table 3, showed that the stride time was significantly higher in the FHP group compared to the NHP group (p < 0.05), with medium to large effect sizes, indicating that participants with FHP had more difficulty maintaining stride time. Additionally, the stance time was notably longer in the FHP group (p < 0.05), suggesting that these individuals might use compensatory mechanisms to maintain balance. Similarly, the swing time was significantly lower in the FHP group (p < 0.05), likely due to altered gait mechanics associated with their FHP.
The stance phase percentage was also significantly higher in the FHP group (p < 0.05), possibly reflecting a more cautious gait pattern. The double support phase showed significant increases (p < 0.05), indicating a greater need for stability among those with FHP. Mean velocity was significantly lower in the FHP group (p < 0.05), suggesting a reduced gait speed when performing dual tasks. Stride length was shorter in the FHP group (p < 0.05), indicating compromised gait performance, and step length was similarly reduced (p < 0.05), reflecting decreased step efficiency. Lastly, a significantly wider step width (p < 0.05) was observed in the FHP group, likely as a compensatory strategy for balance issues. All these findings are detailed in Table 3.
3.4. Cognitive Cost Detailed Results
The cognitive cost results are detailed in Table 4, reveal significant findings across various gait parameters in the FHP group under dual-task conditions. For stride time (both right and left), the FHP group exhibits a significantly higher cognitive cost (p < 0.05), indicating that dual-task conditions impose a greater cognitive load on maintaining stride time. Similarly, stance time (right and left) shows a higher cognitive cost (p < 0.05) in the FHP group, reflecting increased difficulty in managing stance time. The swing time (right and left) also demands significantly more cognitive effort (p < 0.05) from the FHP group. The stance phase (right) demonstrates a higher cognitive cost (p < 0.05), suggesting greater challenges in maintaining this phase during dual tasks.
Additionally, the double support phase (right) presents an increased cognitive cost (p < 0.05) for the FHP group, indicating difficulties in managing this phase. The mean velocity also incurs a higher cognitive cost (p < 0.05), signifying that maintaining walking speed is more cognitively demanding for the FHP group under dual-task conditions. Stride length (right and left) showed a significantly higher cognitive cost (p < 0.05), reflecting compromised gait efficiency. Similarly, step length (right and left) incurs a higher cognitive cost (p < 0.05), indicating reduced step efficiency. Finally, step width (average) reveals a significantly higher cognitive cost (p < 0.05) in the FHP group, suggesting a need for a broader base of support, which is cognitively demanding. Table 4 shows each of these variables and their significance.
3.5. Correlational Results Between Variables
The correlation table for the single task condition (Table 5) reveals the relationship between head posture values and various performance parameters. The findings show no significant correlations, indicating that most correlations between head posture values measured as the CVA and the performance parameters are weak and not statistically significant. This suggests that head posture values do not have a strong influence on the performance parameters during single tasks. The lack of significant correlations indicates that head posture may not be as critical in single tasks as it is in dual tasks.
The correlation table for the dual task testing (Table 6) illustrates a relationship between head posture values and various performance parameters. Significant correlations include negative correlations with stride time (s) for both right (RT) and left (LT) sides, indicating that as the CVA decreases, both right and left stride times tend to increase. Similarly, there are negative correlations with stance time (s) for RT and LT, suggesting that lower CVA values are associated with shorter stance times. Additionally, there are positive correlations with swing time (s) for RT and LT, implying that lower CVA values correlate with longer swing times.
Negative correlations with stance phase (%) for RT and LT show that lower CVA values are associated with shorter stance phases, while positive correlations with swing phase (%) for RT and LT indicate that lower CVA values are linked to longer swing phases. Moreover, there is a positive correlation with step length (m) for RT and LT, demonstrating that lower CVA values correlate with longer step lengths. These correlations suggest that the CVA significantly influences gait parameters during dual tasks, potentially affecting balance and stability.
4. Discussion
Our study investigated the impact of FHP on cognitive dual-task performance, revealing significant findings that contribute to the existing body of knowledge on the interplay between musculoskeletal alignment and cognitive function. The results demonstrate that individuals with FHP exhibit greater cognitive dual-task costs compared to those with normal head posture, indicating that FHP may be associated with increased cognitive demands during gait performance. These results are consistent with previous studies which have demonstrated that FHP can lead to various physiological and neurological impairments, affecting both physical and cognitive functions [36]. This aligns with cognitive load theory, which suggests that increased physical discomfort and proprioceptive inaccuracies associated with FHP can elevate cognitive load, thereby impairing cognitive performance [36,37].
4.1. Interpretation of Findings
The observed differences in dual-task performance between FHP and control groups align with existing literature that suggests postural misalignments can impact cognitive processes [13,20,29,36,37]. The increased cognitive cost in the FHP group may be attributed to altered sensory input and proprioception resulting from vertebral misalignments. Similar to how phantom limb pain develops due to maladaptive cortical reorganization in response to the loss of sensory input [38], FHP can lead to maladaptive changes in the sensory and motor cortex. These disruptions potentially lead to increased cognitive load as the brain compensates for impaired postural stability, as supported by studies indicating deficits in attention, processing speed, and memory in individuals with postural deviations [20,39]. The increased cognitive cost observed in the FHP group can be attributed to several underlying mechanisms. Firstly, FHP causes biomechanical stress on the neck and shoulders, leading to muscle fatigue and discomfort, which in turn can reduce cognitive resources available for task performance [37,40]. Secondly, FHP is associated with altered proprioceptive function, which can disrupt sensory input and integration, further increasing the cognitive load required for maintaining balance and performing tasks [7,8,9,40]. Finally, the structural changes in the cervical spine due to FHP, through alteration in the cervical lordosis, can impair blood flow to the brain [41], affecting cognitive functions such as attention and memory [20,36].
Additionally, deafferentation resulting from faulty posture may very well exacerbate cognitive impairments. Research has shown that the loss of sensory nerve signals due to poor posture may increase cognitive load and impair cognitive performance by disrupting proprioception feedback and increasing the brain’s compensatory efforts [20,29,42]. Moreover, neuroplasticity plays a critical role in the relationship between cognition and posture. Neuroplastic changes in response to altered sensory input from poor posture can lead to both adaptive and maladaptive cognitive outcomes. Studies indicate that neuroplasticity mechanisms, such as synaptogenesis and cortical reorganization, are involved in adapting to increased cognitive demands [43,44] and it is possible that these same adaptations are imposed by FHP. These changes highlight the brain’s ability to reorganize and modify its neural connections in response to environmental stimuli and experience, which is crucial for maintaining cognitive function in the face of physical impairments [44].
4.2. Implications for Clinical Practice
The significant correlations between the CVA and cognitive dual-task performance emphasizes the need for comprehensive assessment protocols that consider both musculoskeletal and cognitive parameters. Clinicians should be aware of the potential cognitive implications of FHP and incorporate strategies to address postural alignment in rehabilitation programs. This approach is particularly relevant for populations at risk of cognitive decline, such as older adults and individuals with neurological conditions [20].
Our study also supports the use of dual-task gait assessments as a valuable tool for detecting cognitive impairments. The integration of cognitive and motor tasks in these assessments provides a more ecologically valid measure of real-world functioning, which is critical for identifying subtle cognitive deficits that may not be evident in single-task evaluations [45,46]. This has significant implications for early intervention and monitoring of cognitive health in clinical settings. Clinicians should consider assessing posture as part of routine evaluations, especially for individuals presenting with cognitive complaints. Interdisciplinary approaches involving physical therapists, occupational therapists, and cognitive specialists can provide comprehensive care that addresses both the physical and cognitive challenges associated with FHP. Early intervention and education on the importance of maintaining proper posture could help prevent the development of FHP and, therefore, any associated cognitive impairments [34,35].
4.3. Practical Applications
Individuals with FHP are likely to experience increased cognitive fatigue and reduced efficiency in tasks requiring simultaneous cognitive and physical effort. This could impact daily activities, workplace productivity, and overall quality of life. For example, Jung and colleagues recently identified that office workers who adopted a forward head posture had a change in the magnitude and frequency of gamma brain waves [13]. Specifically, it was found that reducing the CVA (increasing FHP), caused brain waves to switch to gamma waves at rest. Higher gamma waves are important during cognition and mental processing and are linked to higher IQ’s, however, at rest high gamma activity is not normal and is associated with greater sympathetic demand [13]. Jung et al.[13] stated “the activity of gamma waves during rest is related to the abnormal excitatory system and hyperarousal of the sensory system and can affect the overall level of neural excitation, causing unnecessary arousal and interfering with psychological relaxation”. Furthermore, chronic FHP can lead to long-term health issues, including chronic neck pain, headaches [4,5], and potential cognitive decline [20,34,35]. To mitigate the negative effects of FHP, interventions aimed at correcting posture should be considered. These could include physical therapy, ergonomic adjustments in the workplace, and exercises designed to strengthen the cervical and upper back muscles. Incorporating regular breaks and posture checks during prolonged computer use can also help in maintaining proper alignment and reducing the risk of developing FHP [4,13].
4.4. Limitations and Future Directions
Despite the robust design and significant findings of our study, several limitations must be acknowledged. The cross-sectional nature of the study precludes causal inferences, and longitudinal studies are necessary to establish the temporal relationship between FHP and cognitive decline. Additionally, our sample was limited to university students and staff, which may not be representative of the general population; in fact, an older cohort known to have cognitive decline may show greater gait alterations with postural misalignment with a dual task cognitive challenge. Future research should include diverse populations to enhance the generalizability of the findings. Further investigation into the mechanisms underlying the relationship between posture and cognitive function is warranted. Specifically, exploring the role of different regions of the brain and their connectivity in individuals with postural deviations can provide deeper insights into the neurophysiological basis of our findings. Additionally, interventional studies examining the effects of postural correction on cognitive outcomes will be valuable in determining the efficacy of targeted therapies.
5. Conclusions
Our study demonstrates that forward head posture significantly increases the cognitive cost during walking, highlighting the importance of proper postural alignment for maintaining cognitive function. Addressing FHP through targeted interventions could improve both physical and cognitive health, enhancing overall well-being and daily functioning. Further research is needed to explore the long-term effects of FHP and the efficacy of different interventions in mitigating its cognitive impacts.
Author Contributions
SAG, IMM, AA conceived the research idea and participated in its design, data collection, and synthesis. SAG, IMM, AA, PAO, DEH contributed to the statistical analysis and interpretation of results and wrote the various drafts. All authors have read and approved the final version of the manuscript and agree with the order of presentation of the authors.
Funding
CBP NonProfit for possible funding of any associated publication fees.
Institutional Review Board Statement
The research was conducted in accordance with all applicable regulations. University of Sharjah (College of Health Sciences, University of Sharjah, UAE) Ethical approval number: REC-21-03-11-03-S.
Informed Consent Statement
The research was conducted in accordance with all applicable regulations and informed consent was provided to and received from all participants prior to data collection.
Data Availability Statement
The datasets analyzed in the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
PAO is a paid consultant for CBP NonProfit, Inc. DEH is the CEO of Chiropractic BioPhysics and lectures on rehabilitation methods, and distributes products for patient rehabilitation to physicians in the USA; none of these products were used in this manuscript. All the other authors declare that they have no competing interests.
References
- Harrison, D.E.; Harrison, D.D.; Troyanovich, S.J.; Harmon, S. A Normal Spinal Position: It’s Time to Accept the Evidence. J Manipulative Physiol Ther 2000, 23, 623–644. [Google Scholar] [CrossRef] [PubMed]
- Cho, C.Y. Survey of Faulty Postures and Associated Factors Among Chinese Adolescents. J Manipulative Physiol Ther 2008, 31, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Kaushal, K.; Jasrotia, S.; Singh, S.; Kaushal, K.; Jasrotia, S. Prevalence of Forward Head Posture and Its Impact on the Activity of Daily Living among Students of Adesh University – A Cross-Sectional Study. Adesh University Journal of Medical Sciences & Research 2020, 2, 99–102. [Google Scholar] [CrossRef]
- Mahmoud, N.F.; Hassan, K.A.; Abdelmajeed, S.F.; Moustafa, I.M.; Silva, A.G. The Relationship Between Forward Head Posture and Neck Pain: A Systematic Review and Meta-Analysis. Curr Rev Musculoskelet Med 2019, 12, 562–577. [Google Scholar] [CrossRef] [PubMed]
- Singla, D.; Veqar, Z. Association Between Forward Head, Rounded Shoulders, and Increased Thoracic Kyphosis: A Review of the Literature. J Chiropr Med 2017, 16, 220. [Google Scholar] [CrossRef] [PubMed]
- Kamel, M.; Moustafa, I.M.; Kim, M.; Oakley, P.A.; Harrison, D.E. Alterations in Cervical Nerve Root Function during Different Sitting Positions in Adults with and without Forward Head Posture: A Cross-Sectional Study. J. Clin. Med. 2023, 12, 1780. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, I.M.; Youssef, A.; Ahbouch, A.; Tamim, M.; Harrison, D.E. Is Forward Head Posture Relevant to Autonomic Nervous System Function and Cervical Sensorimotor Control? Cross Sectional Study. Gait Posture 2020, 77. [Google Scholar] [CrossRef] [PubMed]
- Moustafa IM, Diab AA, Hegazy F, Harrison DE. Demonstration of central conduction time and neuroplastic changes after cervical lordosis rehabilitation in asymptomatic subjects: a randomized, placebo-controlled trial. Sci Rep. 2021 Jul 28;11(1):15379. [CrossRef]
- Moustafa, I.M.; Diab, A.A.M.; Harrison, D.E. Does Forward Head Posture Influence Somatosensory Evoked Potentials and Somatosensory Processing in Asymptomatic Young Adults? J. Clin. Med. 2023, 12, 3217. [Google Scholar] [CrossRef] [PubMed]
- Moustafa I, Kim M, Harrison DE. Comparison of Sensorimotor Integration and Skill-Related Physical Fitness Components Between College Athletes With and Without Forward Head Posture. J Sport Rehabil. 2022 Jul 22;32(1):53-62. [CrossRef]
- Saad, N.; Moustafa, I.M.; Ahbouch, A.; Alsaafin, N.M.; Oakley, P.A.; Harrison, D.E. Are Rotations and Translations of Head Posture Related to Gait and Jump Parameters? J. Clin. Med. 2023, 12, 6211. [Google Scholar] [CrossRef]
- Tamim, M.; Moustafa, I.M.; Alaparthi, G.K.; Oakley, P.A.; Harrison, D.E. Translational and Rotational Postural Aberrations Are Related to Pulmonary Functions and Skill-Related Physical Fitness Components in Collegiate Athletes. J. Clin. Med. 2023, 12, 4618. [Google Scholar] [CrossRef]
- Jung, J.-Y.; Lee, Y.-B.; Kang, C.-K. Effect of Forward Head Posture on Resting State Brain Function. Healthcare 2024, 12, 1162. [Google Scholar] [CrossRef]
- Sui, S.X.; Williams, L.J.; Holloway-Kew, K.L.; Hyde, N.K.; Pasco, J.A.; Au, J.A.P. Molecular Sciences Skeletal Muscle Health and Cognitive Function: A Narrative Review. 2020. [CrossRef]
- Akinnuwesi, B.A.; Adegbite, B.A.; Adelowo, F.; Ima-Edomwonyi, U.; Fashoto, G.; Amumeji, O.T. Decision Support System for Diagnosing Rheumatic-Musculoskeletal Disease Using Fuzzy Cognitive Map Technique. Inform Med Unlocked 2020, 18, 100279. [Google Scholar] [CrossRef]
- Kent, C. Models of Vertebral Subluxation: A Review. Journal of Vertebral Subluxation Research 1996, 1(1):1-7.
- Lajoie, Y.; Teasdale, N.; Bard, C.; Fleury, M. Attentional Demands for Static and Dynamic Equilibrium. Exp Brain Res 1993, 97, 139–144. [Google Scholar] [CrossRef]
- Cohen, R.G.; Vasavada, A.N.; Wiest, M.M.; Schmitter-Edgecombe, M. Mobility and Upright Posture Are Associated with Different Aspects of Cognition in Older Adults. Front Aging Neurosci 2016, 8. [Google Scholar] [CrossRef]
- Schafer, R.C. Basic Principles of Chiropractic : The Neuroscience Foundations of Clinical Practice. 1990, 519.
- Nishimura H, Ikegami S, Uehara M, Takahashi J, Tokida R, Kato H. Detection of cognitive decline by spinal posture assessment in health exams of the general older population. Sci Rep. 2022 ;12(1):8460. 19 May. [CrossRef]
- Lelic, D.; Khan Niazi, I.; Holt, K.; Jochumsen, M.; Dremstrup, K.; Yielder, P.; Murphy, B.; Drewes, A.M.; Haavik, H. Manipulation of Dysfunctional Spinal Joints Affects Sensorimotor Integration in the Prefrontal Cortex: A Brain Source Localization Study. 2016. [CrossRef]
- Jones, D.T.; Graff-Radford, J. Executive Dysfunction and the Prefrontal Cortex. Continuum (Minneap Minn) 2021, 27, 1586–1601. [Google Scholar] [CrossRef] [PubMed]
- Friedman, N.P.; Robbins, T.W. The Role of Prefrontal Cortex in Cognitive Control and Executive Function. Neuropsychopharmacology 2022, 47, 72–89. [Google Scholar] [CrossRef]
- Ruffieux, J.; Keller, M.; Lauber, B.; Taube, W. Changes in Standing and Walking Performance Under Dual-Task Conditions Across the Lifespan. Sports Medicine 2015, 45, 1739–1758. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Woollacott, M. Attentional Demands and Postural Control: The Effect of Sensory Context. J Gerontol A Biol Sci Med Sci 2000, 55. [Google Scholar] [CrossRef]
- Fuller, R.L.; Van Winkle, E.P.; Anderson, K.E.; Gruber-Baldini, A.L.; Hill, T.; Zampieri, C.; Weiner, W.J.; Shulman, L.M. Dual Task Performance in Parkinson’s Disease: A Sensitive Predictor of Impairment and Disability. Parkinsonism Relat Disord 2013, 19, 325–328. [Google Scholar] [CrossRef]
- Oh, C. Single-Task or Dual-Task? Gait Assessment as a Potential Diagnostic Tool for Alzheimer’s Dementia. Journal of Alzheimer’s Disease 2021, 84, 1183. [Google Scholar] [CrossRef]
- Silsupadol, P.; Shumway-Cook, A.; Lugade, V.; van Donkelaar, P.; Chou, L.S.; Mayr, U.; Woollacott, M.H. Effects of Single-Task Versus Dual-Task Training on Balance Performance in Older Adults: A Double-Blind, Randomized Controlled Trial. Arch Phys Med Rehabil 2009, 90, 381. [Google Scholar] [CrossRef] [PubMed]
- Moustafa IM, Diab A, Shousha T, Raigangar V, Harrison DE. Sensorimotor integration, cervical sensorimotor control, and cost of cognitive-motor dual tasking: Are there differences in patients with chronic whiplash-associated disorders and chronic idiopathic neck pain compared to healthy controls? Eur Spine J. 2022 Dec;31(12):3452-3461. [CrossRef]
- Yip CH, Chiu TT, Poon AT. The relationship between head posture and severity and disability of patients with neck pain. Man Ther. 2008 May;13(2):148-54. [CrossRef] [PubMed]
- Singla D, Veqar Z, Hussain ME. Photogrammetric Assessment of Upper Body Posture Using Postural Angles: A Literature Review. J Chiropr Med. 2017 Jun;16(2):131-138. [CrossRef]
- Titcomb DA, Melton BF, Bland HW, Miyashita T. Evaluation of the Craniovertebral Angle in Standing versus Sitting Positions in Young Adults with and without Severe Forward Head Posture. Int J Exerc Sci. 2024 Jan 1;17(1):73-85.
- Davis, R.B.; Õunpuu, S.; Tyburski, D.; Gage, J.R. A Gait Analysis Data Collection and Reduction Technique. Hum Mov Sci 1991, 10, 575–587. [Google Scholar] [CrossRef]
- Bahureksa, L.; Najafi, B.; Saleh, A.; Sabbagh, M.; Coon, D.; Mohler, M.J.; Schwenk, M. The Impact of Mild Cognitive Impairment on Gait and Balance: A Systematic Review and Meta-Analysis of Studies Using Instrumented Assessment. Gerontology 2017, 63, 67–83. [Google Scholar] [CrossRef] [PubMed]
- MacAulay, R.K.; Wagner, M.T.; Szeles, D.; Milano, N.J. Improving Sensitivity to Detect Mild Cognitive Impairment: Cognitive Load Dual-Task Gait Speed Assessment. J Int Neuropsychol Soc 2017, 23, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Gong, W.; Jeon, J. Correlations between Forward Head Posture, Range of Motion of Cervicospinal Area, Resting State, and Concentrations of the Brain. J Phys Ther Sci 2011, 23, 481–484. [Google Scholar] [CrossRef]
- Oh, H.J.; Song, G. Bin Effects of Neurofeedback Training on the Brain Wave of Adults with Forward Posture. J Phys Ther Sci 2016, 28, 2938. [Google Scholar] [CrossRef] [PubMed]
- Flor, H.; Birbaumer, N. Phantom Limb Pain: Cortical Plasticity and Novel Therapeutic Approaches. Curr Opin Anaesthesiol 2000, 13, 561–564. [Google Scholar] [CrossRef] [PubMed]
- Baione, V.; Ferrazzano, G.; Celletti, C.; De Rosa, M.; Belvisi, D.; Fabbrini, G.; Galli, M.; Camerota, F.; Conte, A. Attention-Demanding Cognitive Tasks Worsen Postural Control in Patients With Cervical Dystonia: A Case-Control Study. Front Neurol 2021, 12, 666438. [Google Scholar] [CrossRef] [PubMed]
- Yong, M.S.; Lee, H.Y.; Lee, M.Y. Correlation between Head Posture and Proprioceptive Function in the Cervical. J Phys Ther Sci 2016, 28, 857. [Google Scholar] [CrossRef]
- Katz EA, Katz SB, Fedorchuk CA, Lightstone DF, Banach CJ, Podoll JD. Increase in cerebral blood flow indicated by increased cerebral arterial area and pixel intensity on brain magnetic resonance angiogram following correction of cervical lordosis. Brain Circ. 2019 Jan-Mar;5(1):19-26. [CrossRef]
- Makin, T.R.; Flor, H. Brain (Re)Organisation Following Amputation: Implications for Phantom Limb Pain. Neuroimage 2020, 218. [Google Scholar] [CrossRef]
- Greenwood, P.M.; Parasuraman, R. Neuronal and Cognitive Plasticity: A Neurocognitive Framework for Ameliorating Cognitive Aging. Front Aging Neurosci 2010, 2. [Google Scholar] [CrossRef] [PubMed]
- Marzola, P.; Melzer, T.; Pavesi, E.; Gil-Mohapel, J.; Brocardo, P.S. Exploring the Role of Neuroplasticity in Development, Aging, and Neurodegeneration. Brain Sciences 2023, Vol. 13, Page 1610 2023, 13, 1610. [Google Scholar] [CrossRef] [PubMed]
- Parsons, T.D. Virtual Reality for Enhanced Ecological Validity and Experimental Control in the Clinical, Affective and Social Neurosciences. Front Hum Neurosci 2015, 9, 146520. [Google Scholar] [CrossRef] [PubMed]
- Faria, A.L.; Latorre, J.; Silva Cameirão, M.; Bermúdez i Badia, S.; Llorens, R. Ecologically Valid Virtual Reality-Based Technologies for Assessment and Rehabilitation of Acquired Brain Injury: A Systematic Review. Front Psychol 2023, 14. [Google Scholar] [CrossRef]
Figure 1.
The craniovertebral angle (CVA) measured in a standing, neutral, upright posture position. The CVA (angle A) is measured by a line connecting the tragus of the ear to the C7 vertebral prominence and then measuring the intersection of this line to a horizontal line passing through C7 prominence, where the acute angle side is measured.
Figure 1.
The craniovertebral angle (CVA) measured in a standing, neutral, upright posture position. The CVA (angle A) is measured by a line connecting the tragus of the ear to the C7 vertebral prominence and then measuring the intersection of this line to a horizontal line passing through C7 prominence, where the acute angle side is measured.
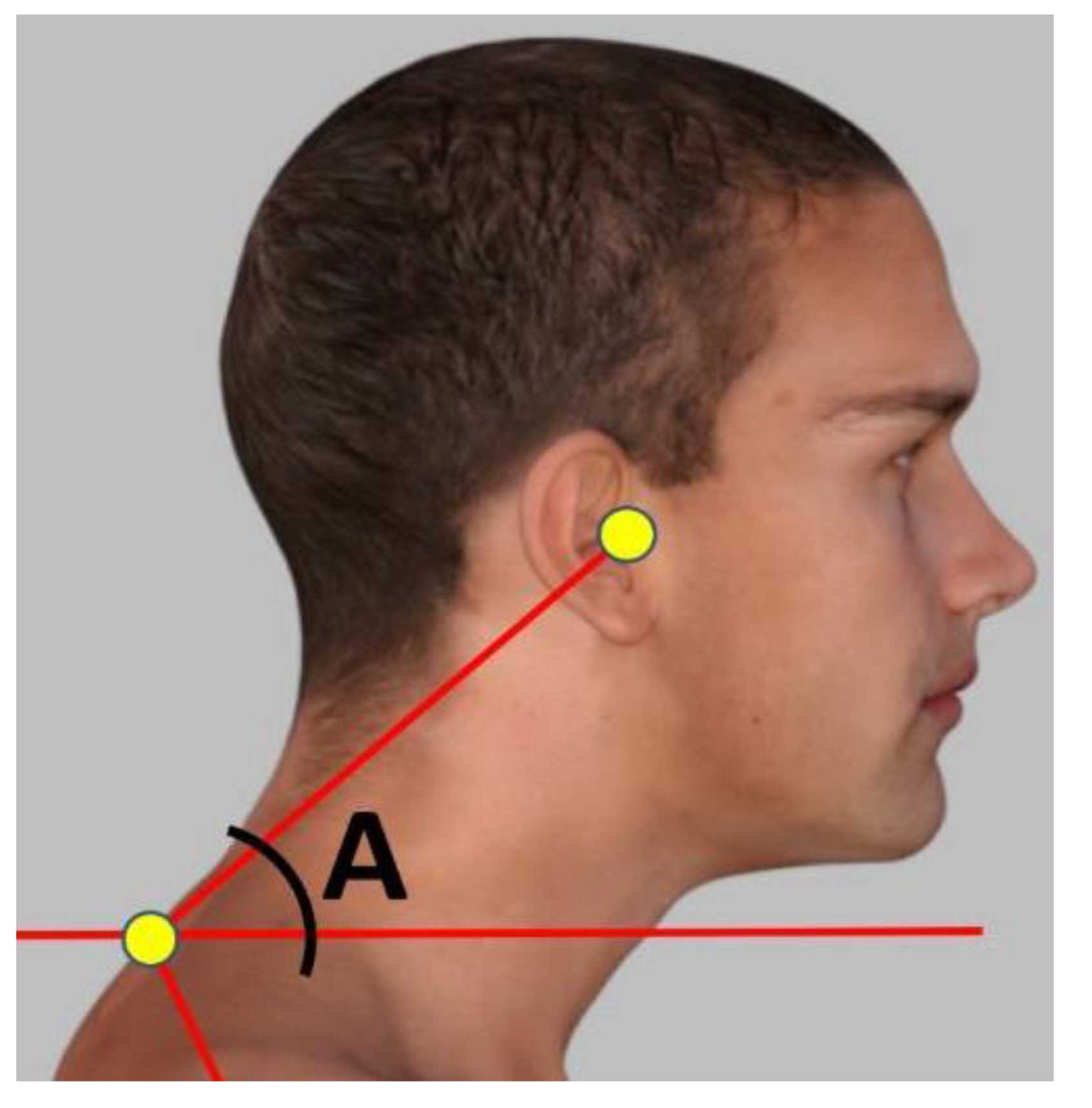
Figure 2.
The optical motion-capture system consisting of 8 infrared cameras was used to assess gait kinematics while participants walked along the 10 meter platform. .
Figure 2.
The optical motion-capture system consisting of 8 infrared cameras was used to assess gait kinematics while participants walked along the 10 meter platform. .

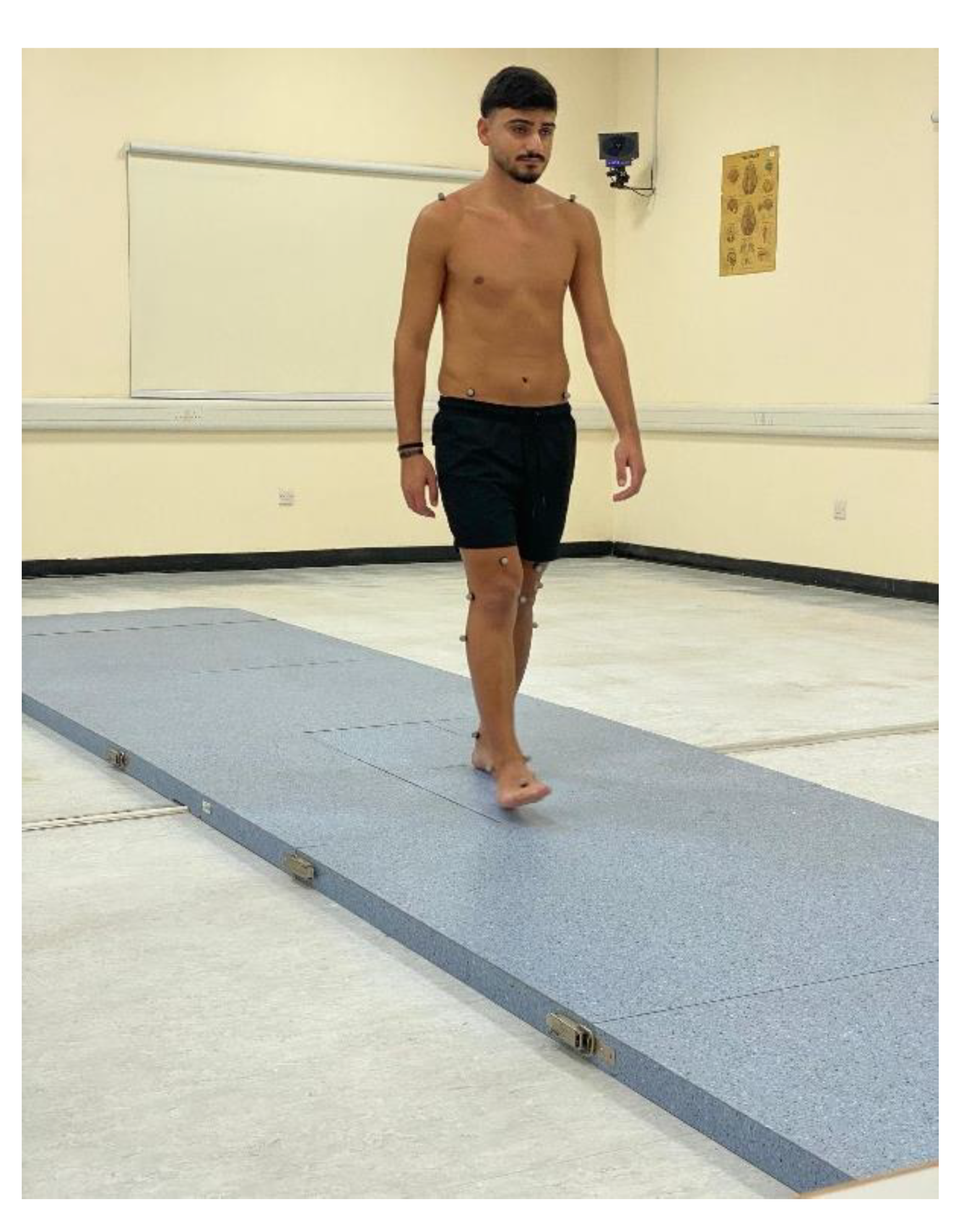
Figure 3.
Anthropometric measurement of the distance between the anterior superior iliac spines.

Figure 4.
Anthropometric measurement of the pelvis thickness.
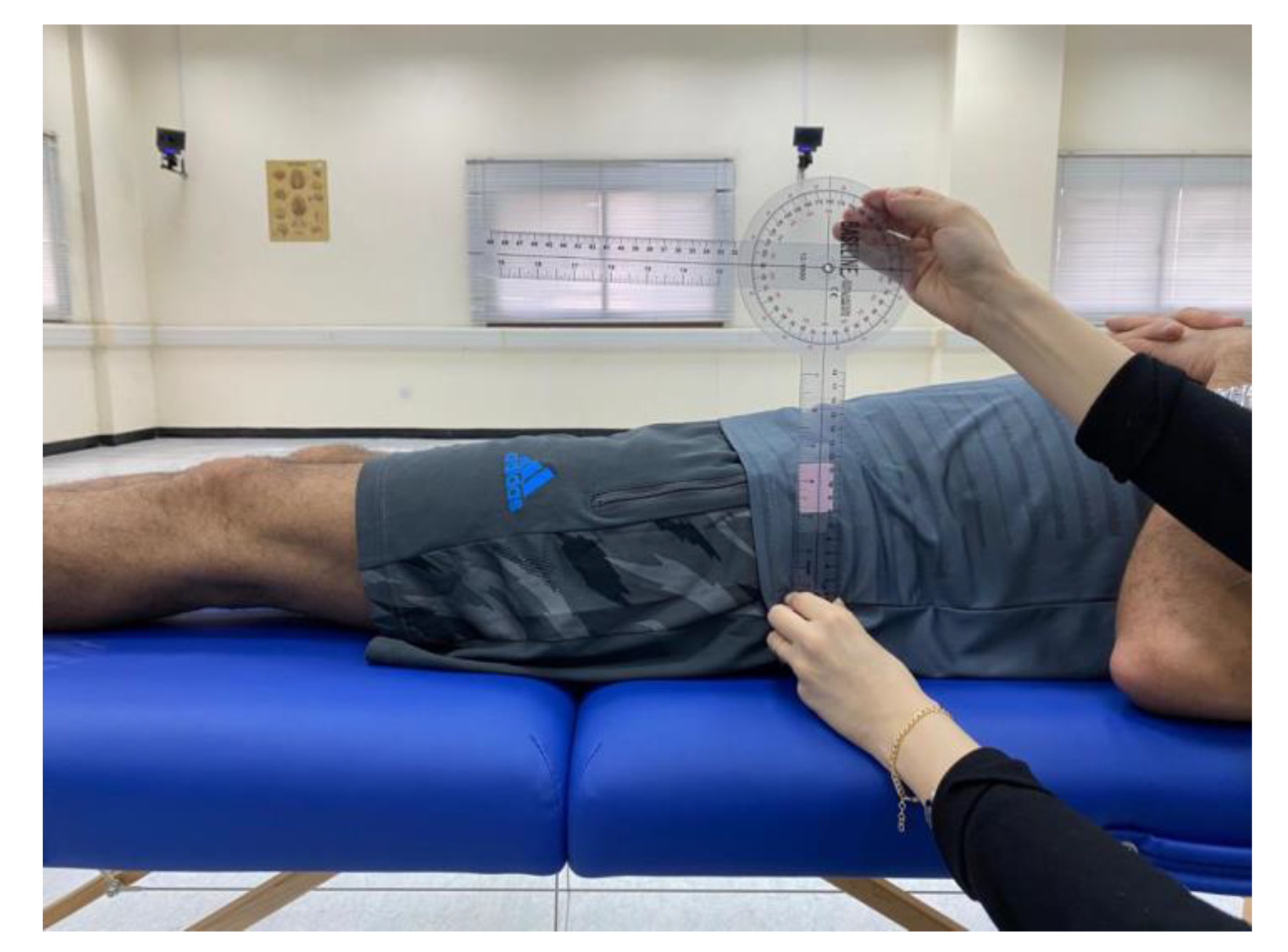
Figure 5.
Anthropometric measurement of leg lengths were obtained bilaterally from the anterior superior iliac spine to the medial maleolus.
Figure 5.
Anthropometric measurement of leg lengths were obtained bilaterally from the anterior superior iliac spine to the medial maleolus.
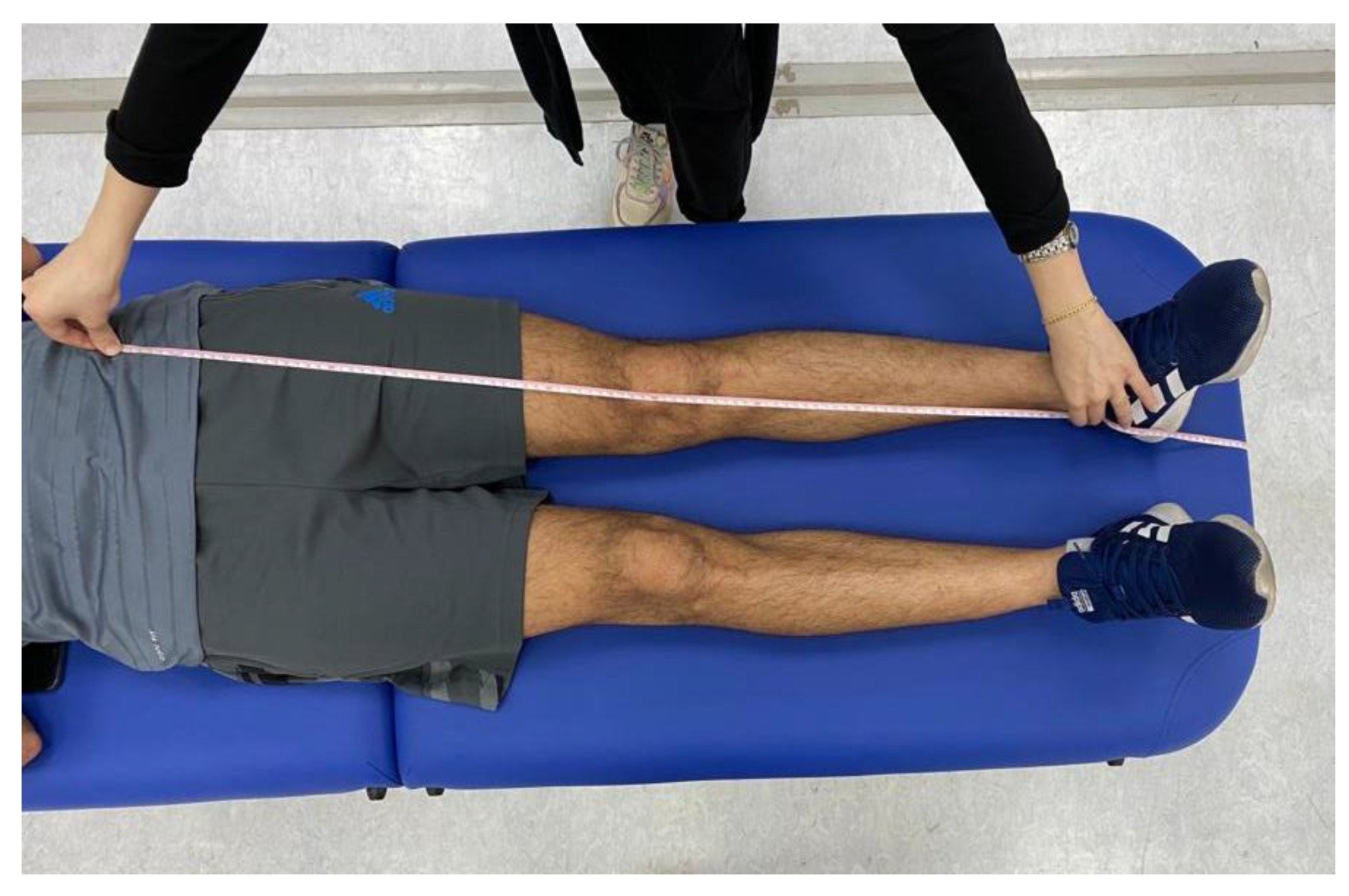
Figure 6.
The location of the 22 spherical reflective passive markers were placed on each participant's skin following the protocol outlined by Davis et al. [33].
Figure 6.
The location of the 22 spherical reflective passive markers were placed on each participant's skin following the protocol outlined by Davis et al. [33].

Figure 7.
Participants were instructed to walk at their self-selected pace along a 10 m walkway while the 3D trajectories of the markers were captured by the cameras under two conditions: single-task and dual-task.
Figure 7.
Participants were instructed to walk at their self-selected pace along a 10 m walkway while the 3D trajectories of the markers were captured by the cameras under two conditions: single-task and dual-task.

Figure 8.
The box plot for the craniovertebral angle (CVA) in the forward head posture (FHP) and control or normal head posture (NHP) group. The CVA is on the vertical axis shown as ‘head posture value’ (degrees) while the two groups are on the horizontal axis.
Figure 8.
The box plot for the craniovertebral angle (CVA) in the forward head posture (FHP) and control or normal head posture (NHP) group. The CVA is on the vertical axis shown as ‘head posture value’ (degrees) while the two groups are on the horizontal axis.
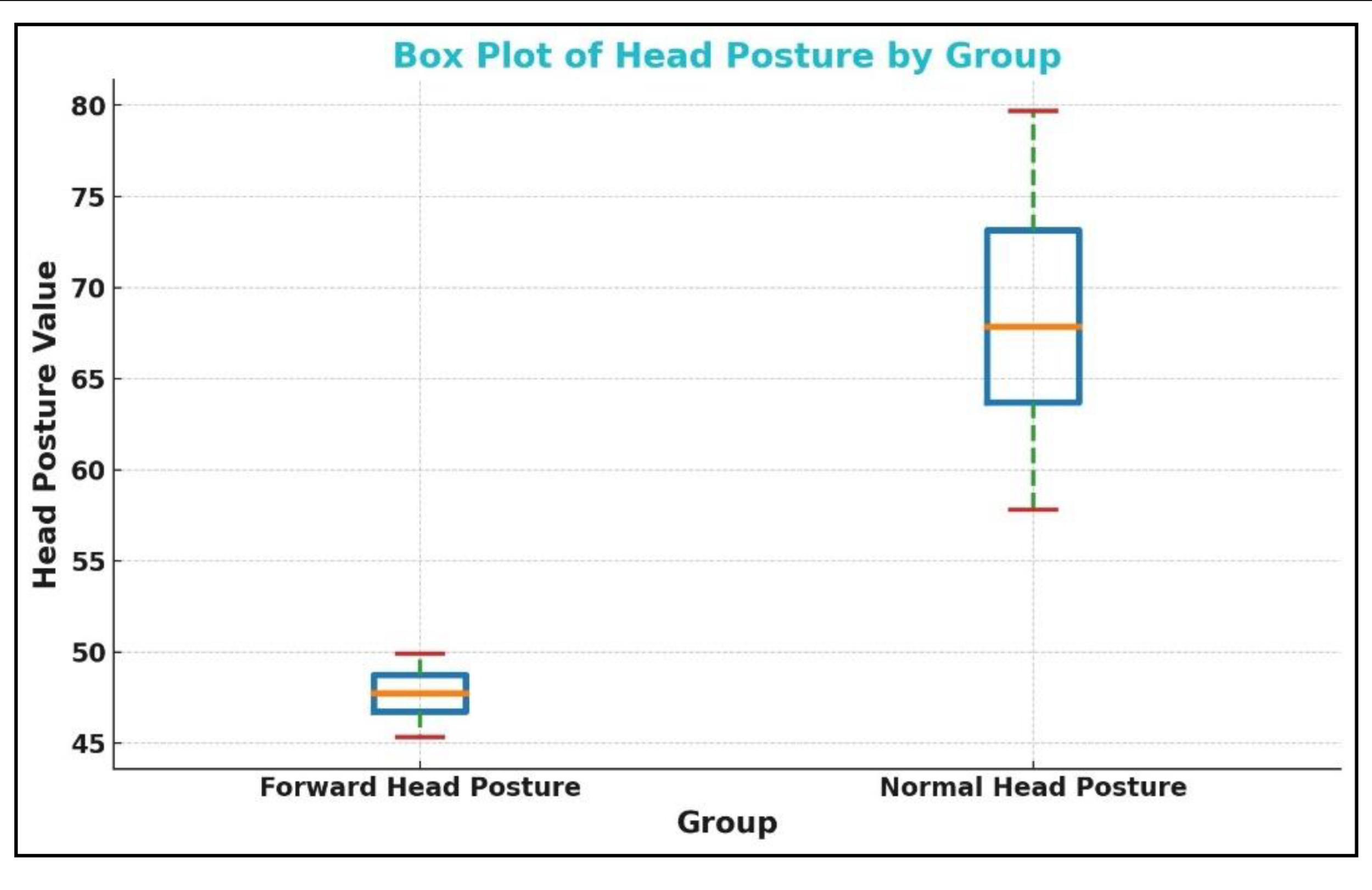

Table 1.
Baseline demographic characteristics and clinical variables. FHP: forward head posture group; NHP: normal head posture group; BMI: body mass index; CVA: craniovertebral angle.
Table 1.
Baseline demographic characteristics and clinical variables. FHP: forward head posture group; NHP: normal head posture group; BMI: body mass index; CVA: craniovertebral angle.
| Variable | FHP (n=45) | NHP (n=45) | |
|---|---|---|---|
| Age (years) | 20.5 ± 2 | 20 ± 3 | |
| BMI (kg/m2) | 21.5 ± 1.7 | 21.4 ± 1.8 | |
| Gender (%) | |||
| Male | 25 (55.5%) | 25 (55.5%) | |
| Female | 20 (44.5%) | 20 (44.5%) | |
| CVA (°) | 46.64 ± 3.23 | 67.9 5 ± 7.89 | |
Table 2.
Mean differences between spatiotemporal parameters in forward head posture (FHP) and neutral head posture (NHP) groups during single task walking are shown.
Table 2.
Mean differences between spatiotemporal parameters in forward head posture (FHP) and neutral head posture (NHP) groups during single task walking are shown.
| Variable | Group | Mean ± SD | 95% CI | Effect Size (d) | p-value |
|---|---|---|---|---|---|
| Stride time |
FHP | 1.12 ± 0.08 | [-0.061 , 0.041] |
-0.11 | 0.60 |
| NHP | 1.13 ± 0.12 | ||||
| Stance time |
FHP | 0.67 ± 0.07 | [-0.074 , 0.014] | -0.29 | 0.30 |
| NHP | 0.70 ± 0.11 | ||||
| Swing time |
FHP | 0.43 ± 0.05 | [-0.025 , 0.025] | 0.06 | 0.30 |
| NHP | 0.43 ± 0.05 | ||||
| Stance phase |
FHP | 60.19 ± 3.99 | [-2.59 , 1.69] | -0.11 | 0.20 |
| NHP | 60.64 ± 4.12 | ||||
| Double support phase |
FHP | 10.81 ± 2.19 | [-1.60 , 0.54] |
-0.25 | 0.20 |
| NHP | 11.34 ± 2.07 | ||||
| Mean velocity |
FHP | 1.16 ± 0.13 | [-0.11 , 0.054] | -0.21 | 0.15 |
| NHP | 1.19 ± 0.17 | ||||
| Mean velocity height |
FHP | 70.62 ± 8.29 | [-5.90 , 3.24] | -0.13 | 0.26 |
| NHP | 71.95 ± 10.91 | ||||
| Cadence |
FHP | 108.12 ± 7.91 | [-4.25 , 5.79] | 0.08 | 0.60 |
| NHP | 107.35 ± 9.93 | ||||
| Stride length |
FHP | 78.46 ± 7.50 | [-5.27 , 2.31] | -0.19 | 0.40 |
| NHP | 79.94 ± 7.51 | ||||
| Step length |
FHP | 0.64 ± 0.06 | [-0.036 , 0.036] |
0.13 | 0.80 |
| NHP | 0.64 ± 0.08 | ||||
| Step width average |
FHP | 0.08 ± 0.03 | [-0.047 , 0.027] | -0.24 | 0.90 |
| NHP | 0.09 ± 0.06 | ||||
| Swing Phase (%) | FHP | 38.91 ± 2.83 | [-1.51 , 0.39] | 0.20 | 0.40 |
| NHP | 38.35 ± 2.74 | ||||
| Single Support Phase (%) | FHP | 39.45 ± 2.52 | [-0.62 , 1.075] | -0.08 | 0.72 |
| NHP | 39.67 ± 2.77 |
Table 3.
Mean differences between spatiotemporal parameters in forward head posture (FHP) and neutral head posture (NHP) groups during dual task.
Table 3.
Mean differences between spatiotemporal parameters in forward head posture (FHP) and neutral head posture (NHP) groups during dual task.
| Variable | Group | Mean ± SD | 95% CI | Effect Size (d) | p-value |
|---|---|---|---|---|---|
|
Stride time |
FHP | 1.40 ± 0.32 | [0.118 , 0.322] | 0.88 | < .001 |
| NHP | 1.18 ± 0.14 | ||||
|
Stance time |
FHP | 0.72 ± 0.06 | [0.051 , 0.109] | 1.14 | < .001 |
| NHP | 0.64 ± 0.08 | ||||
|
Swing time |
FHP | 0.44 ± 0.04 | [-0.074 , -0.026] | -0.95 | < .001 |
| NHP | 0.49 ± 0.06 | ||||
|
Stance phase |
FHP | 65.01 ± 5.97 | [2.044 , 5.656] | 0.83 | 0.01 |
| NHP | 61.16 ± 2.33 | ||||
|
Double support phase |
FHP | 12.29 ± 1.41 | [1.232 , 1.628] | 0.94 | < .001 |
| NHP | 10.86 ± 1.61 | ||||
|
Mean velocity |
FHP | 1.08 ± 0.12 | [-0.304 , -0.116] | -0.96 | < .001 |
| NHP | 1.29 ± 0.30 | ||||
|
Mean velocity height |
FHP | 60.86 ± 7.92 | [-14.45 , -7.25] | -1.25 | < .001 |
| NHP | 71.71 ± 9.46 | ||||
|
Cadence |
FHP | 103.18 ± 10.13 | [-5.29 , 2.99] | -0.18 | 0.30 |
| NHP | 104.83 ± 7.56 | ||||
|
Stride length |
FHP | 73.08 ± 7.37 | [-11.03 , -4.57] | -1.00 | < .001 |
| NHP | 80.88 ± 8.19 | ||||
|
Step length |
FHP | 0.58 ± 0.06 | [-0.105 , -0.035] | -1.10 | < .001 |
| NHP | 0.65 ± 0.08 | ||||
|
Step width average |
FHP | 0.15 ± 0.23 | [0.013 , 0.147] | 0.48 | < .001 |
| NHP | 0.07 ± 0.02 | ||||
| Swing Phase (%) | FHP | 38.36 ± 1.83 | [0.88 , 3.37] | -0.90 | 0.0008 |
| NHP | 40.69 ± 3.17 | ||||
| Single Support Phase (%) | FHP | 39.37 ± 2.16 | [0.68 , 4.35 ] | -0.65 | 0.01 |
| NHP | 41.96 ± 5.18 |
Table 4.
The mean difference in cognitive cost (CC) between forward head posture (FHP) and normal head posture (NHP). CC is calculated as the difference in parameter values from single to dual task divided by the single task value, multiplied by 100%.
Table 4.
The mean difference in cognitive cost (CC) between forward head posture (FHP) and normal head posture (NHP). CC is calculated as the difference in parameter values from single to dual task divided by the single task value, multiplied by 100%.
| Variable | Group | Mean ± SD | 95% CI | Effect size (d) | p-value |
|---|---|---|---|---|---|
| CC Stride time |
FHP | 25.79 ± 29.76 | [10.90 , 30.30] |
0.87 | < .001 |
| NHP | 5.19 ± 14.72 | ||||
| CC Stance time |
FHP | 8.43 ± 19.25 | [8.20 , 22.16] | 0.89 | < .001 |
| NHP | -6.75 ± 14.09 | ||||
| CC Swing time |
FHP | 2.78 ± 10.64 | [-19.34 , -5.16} | -0.72 | < .001 |
| NHP | 15.03 ± 21.86 | ||||
| CC Stance phase |
FHP | 8.49 ± 12.79 | [2.56 , 11.62] | 0.64 | 0.01 |
| NHP | 1.40 ± 8.74 | ||||
| CC Double support phase |
FHP | 19.87 ± 37.99 | [5.85 , 31.67] |
0.66 | 0.01 |
| NHP | 1.11 ± 22.62 | ||||
| CC Mean velocity |
FHP | 12.36 ± 34.86 |
[-5.20 , 16.22] |
-0.75 | 0.02 |
| NHP | 6.85 ± 11.41 | ||||
| CC Mean velocity height |
FHP | 13.34 ± 13.09 | [1.60 , 18.72] | -0.80 | < .001 |
| NHP | 3.18 ± 26.27 | ||||
| CC Cadence |
FHP | 4.49 ± 8.01 | [-1.16 , 7.22] |
-0.30 | < .001 |
| NHP | 1.46 ± 11.93 | ||||
| CC Stride length |
FHP | 6.84 ± 8.54 | [-0.35 , 9.21] | -0.81 | 0.01 |
| NHP | 2.41 ± 14.00 | ||||
| CC Step length |
FHP | 9.98 ± 10.65 | [0.33 , 10.85] |
-1.13 | 0.01 |
| NHP | 4.39 ± 14.51 | ||||
| CC Step width average |
FHP | 12.43 ± 340.60 | [0.31 , 4.73] |
0.49 | 0.01 |
| NHP | 9.91 ± 40.58 | ||||
| Swing Phase (%) | FHP | 15.79 ± 3.7 | [6.51 , 10.87] | 2.03 | < .001 |
| NHP | 7.1 ± 4.8 | ||||
| Single Support Phase (%) | FHP | 17.36 ± 1.86 | [6.22 , 10.90] | 1.51 | < .001 |
| NHP | 8.8 ± 7.8 |
Table 5.
Correlation between the craniovertebral angle (CVA) and gait parameters during single task conditions. s: seconds; m: meters.
Table 5.
Correlation between the craniovertebral angle (CVA) and gait parameters during single task conditions. s: seconds; m: meters.
| Parameter | Pearson’s r | p-value |
|---|---|---|
| Stride time (s) | 0.02 | 0.86 |
| Stance Time (s) | 0.08 | 0.52 |
| Swing Time (s) | 0.1 | 0.98 |
| Stance Phase (%) | 0.04 | 0.77 |
| Swing Phase (%) | -0.03 | 0.98 |
| Single Support Phase (%) | 0.06 | 0.61 |
| Double Support Phase (%) | 0.12 | 0.29 |
| Mean Velocity (m/s) | 0.08 | 0.49 |
| Mean Velocity (%height/s) | 0.05 | 0.67 |
| Cadence (steps/min) | -0.02 | 0.90 |
| Stride Length (%height) | 0.05 | 0.60 |
| Step Length (m) | -0.03 | 0.70 |
| Step Width (m) | 0.03 | 0.80 |
Table 6.
Correlation between the craniovertebral angle (CVA) and gait parameters during dual task. s: seconds; m: meters.
Table 6.
Correlation between the craniovertebral angle (CVA) and gait parameters during dual task. s: seconds; m: meters.
| Parameter | Pearson’s r | p-value |
|---|---|---|
| Stride time (s) | -0.68 | < .001 |
| Stance Time (s) | -0.56 | < .001 |
| Swing Time (s) | 0.31 | < .001 |
| Stance Phase (%) | -0.56 | < .001 |
| Swing Phase (%) | 0.53 | < .001 |
| Single Support Phase (%) | 0.40 | < .001 |
| Double Support Phase (%) | -0.55 | < .001 |
| Mean Velocity (m/s) | 0.28 | < .001 |
| Mean Velocity (%height/s) | 0.49 | < .001 |
| Cadence (steps/min) | 0.20 | < .001 |
| Stride Length (%height) | 0.39 | < .001 |
| Step Length (m) | 0.60 | < .001 |
| Step Width (m) | -0.40 | < .001 |
Table 7.
Correlation between the craniovertebral angle (CVA) and cognitive cost (CC) per each parameter. s: seconds; m: meters.
Table 7.
Correlation between the craniovertebral angle (CVA) and cognitive cost (CC) per each parameter. s: seconds; m: meters.
| Parameter | Pearson’s r | p-value |
|---|---|---|
| CC Stride time (s) | -0.61 | < .001 |
| CC Stance Time (s) | -0.41 | < .001 |
| CC Swing Time (s) | -0.35 | < .001 |
| CC Stance Phase (%) | -0.35 | < .001 |
| CC Swing Phase (%) | -0.45 | < .001 |
| CC Single Support Phase (%) | -0.23 | 0.04 |
| CC Double Support Phase (%) | -0.21 | 0.04 |
| CC Mean Velocity (m/s) | -0.37 | 0.01 |
| CC Mean Velocity (%height/s) | -0.30 | 0.01 |
| CC Cadence (steps/min) | -0.22 | 0.01 |
| CC Stride Length (%height) | -0.32 | 0.01 |
| CC Step Length (m) | -0.55 | < .001 |
| CC Step Width (m) | -0.50 | < .001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



