
Submitted:
08 July 2024
Posted:
10 July 2024
You are already at the latest version
Abstract
The objective of this study was to analyze the epidemiological links of HIV, HCV and HIV-HCV coinfections to less studied types of transmission in certain populations. We performed an observational, prospective study on 903 patients aged between 15-87 years who took part in the Open Test Project. They were divided into two subgroups: general population and individuals from prisons, and questioned about multiple risk factors. Chi-Square Independence Test was used to establish correlations between the risk factors and the results of the screening tests. Logistic regression was used to calculate the probability of a reactive screening test based on each independent risk factor and age. HIV was very strongly associated with unprotected sexual intercourse with HIV-positive partners (the strongest association), unprotected sexual intercourse with sex workers, newly diagnosed sexually transmitted diseases (STDs), intravenous drug use (IDUs) and sharing injecting materials. In the case of HCV reactive tests, very strong associations have been established with injecting drug use (the strongest association), unprotected sexual intercourse with IDUs and sharing injecting materials. Our study indicates the need for implementing targeted public health programs, tailored to the local epidemiology that can ultimately lead to micro-elimination of hepatitis and HIV infections in this area.
Keywords:
HIV
; HCV
; HIV-HCV coinfection
; micro-elimination
; inmates
; IDUs
; STDs
; strong association
1. Introduction
World Health Organization’s sustainable development goals for 2030 aim to end the epidemic of Acquired Immunodeficiency Syndrome (AIDS), combat hepatitis and other communicable and sexually transmitted diseases (STDs) by 2030 [1]. Still, a more realistic objective may be the micro-elimination of Human Immunodeficiency virus (HIV) and hepatitis C virus (HCV) from population segments with targeted strategies of prevention and treatment; the basic idea is that micro-elimination will eventually lead to macro-elimination.
Moreover, infections with HIV and HCV are frequently encountered in individuals with similar risk factors, and shared parenteral transmission routes. HIV poses a major global health challenge, worsened by rising emigrant numbers [2]. There are currently 18,015 people living with HIV in Romania, a significant proportion of them being long-term survivors from the 1990 cohort, parenterally infected during childhood [3,4]. However, only 13,759 receive effective treatment or post-exposure prophylaxis [3]. Therefore, more effort should be put into prompt and early identification and management of new cases.
On the other hand, HCV affects about 170 million people worldwide, significantly outnumbering HIV-1 infections [5]. Most HCV acute cases develop chronic hepatitis, leading to severe complications such as fibrosis, cirrhosis or hepatocellular carcinoma without diagnosis and treatment [6]. Rapid and accurate diagnosis is the key to preventing the spread of HCV infections, Romania being the country with the highest prevalence of HCV infections among the Balkan countries [7]. While serological screening and risk factors identification can reduce the risk of parenterally transmitted diseases, new cases of HCV infection still occur through dangerous practices.
The present study aims to analyze HIV and HCV infections transmission pathways in Romania, and the epidemiological links to the main novel transmission types. The study assessed the risk of a positive screening test when exposed to an extended list of predefined risk factors for HIV, and HCV infections. Assuming that individual exposure to risk factors varies, this study seeks to enhance understanding of HIV and HCV transmission dynamics for improved personalized diagnosis and treatment guidelines. Nonetheless, the decisive goal is to accurately identify up-to-date risk factors, improve screening, and promote voluntary testing.
2. Materials and Methods
We performed an observational, population oriented, prospective study on 903 patients with ages between 15-87 years, participating in the European Open Test Project, carried out in Stefan S. Nicolau Institute of Virology from Bucharest and Profilaxia Medical Centre from Timișoara, Romania, coordinated by ANLAIDS (Associazione Nazionale per la Lotta contro l’AIDS - Sezione Lombarda), Italy, with funding from Otto per Mille della Chiesa Valdese, Italy.
A questionnaire was used to collect information from the study population during November 2019 and February 2023. All the participants signed an informed consent and received medical counselling before and after testing. The protocol was approved by the Ethics Commission of Institute of Virology. Our research was conducted within the Declaration of Helsinki guidelines, and under the terms of all local legislation. Patients were asked about the following risk factors: sexual intercourse with men, women or both, abstinence, condom use during sexual intercourse as a means of STDs prevention, offering sexual services in exchange of drugs and money, newly diagnosed STDs, incarceration, unprotected sexual intercourse with sex workers, intravenous drug users (IDUs), sexual intercourse with IDUs, HIV positive people and men who have sex with men (MSM), and sharing needles, syringes, spoons, filters and other injecting materials, all in the last 12 months. Patients were also evaluated for demographic factors (gender, date of birth, age, nationality, residence place -urban or rural), and previous HIV and HCV testing.
Rapid qualitative tests were used to detect antibodies for screening of HIV and HCV from blood or saliva (OraQuick HIV and HCV tests); briefly, after collecting samples from the oral cavity or peripheral blood, the samples were processed in a developer vial. The presence of antibodies in the sample is indicated by the appearance of a reddish-purple line in both Control Zone and Test Zone of the device (reactive test). All the reactive tests were confirmed using an immunoenzymatical test.
Patients’ data were processed in JASP statistic program; to establish correlations between the risk factors and the result of the screening tests we used Chi-Square Independence Test. The degree of association was evaluated with the φ (phi) association coefficient (for binary variables) and Cramer’s V coefficient (for nonbinary variables). We set a p value at 0.05 (confidence interval, CI = 95%). The degree of freedom (df value) is obtained from the contingency table. Frequencies lower than 5 needed a Yates continuity correction. Coefficients > 0.25 indicated a very strong association between the risk factor and the result of the screening test; 0.15 - 0.25 - strong association; 0.1 - 0.15 - moderate association; 0.05 - 0.1 - weak association; 0 - 0.05 - very weak or absent association. Furthermore, to calculate the probability of a reactive screening test based on each independent risk factor and age, logistic regression was used.
3. Results
903 Romanian individuals with different risk profiles were introduced in the study and subsequently divided into 2 subgroups: general population (806 persons) and individuals from prisons (97 persons). The association between individual risk factors and the screening test results for HIV, HCV and HIV-HCV coinfection were compared between the two subgroups.
3.1. General Characteristics of the Patients
The general population cohort, with a mean age of 39.37 ± 14.54 years, were predominantly women (63.89%) and mainly from urban areas: Bucharest (38.33%), and Timișoara (28.16%). 26 individuals had reactive HIV screening tests (3.22%), 22 had reactive HCV screening tests (2.73%) and 7 had reactive tests for both HIV and HCV (0.86%). The mean age for HIV reactive individuals was 36.65 ± 8.93 years, while for HCV reactive population was 43.31 ± 11.91 years, older than of the HIV group.
Prison inmates, averaged 41.66 ± 9.28 years, were mostly men (92.78%) from Jilava Penitentiary Hospital; 55 had reactive HIV tests (56.7%), 49 had reactive HCV tests (50.51%), and 30 had HIV-HCV co-infection (30.92%). The mean age for HIV reactive inmates was 41.12 ± 8.72 years, and the mean age in HCV reactive prisoners was 39.3 ± 6.78 years.
3.22% from the general population, as compared to 56.7% from the prisoners had reactive HIV screening tests; 2.73% from the people in general population and 50.51% from the imprisoned had reactive HCV screening tests, while 0.86% from the general population, and 30.92% from the prisoners had reactive tests for both HIV and HCV.
3.2. Correlations between Risk Factors and the Outcomes of the Screening
We assessed how heterosexual intercourse within the last 12 months with women influences screening results in both populations. A strong association between the risk factor and the HIV screening test result was observed only in correctional facilities populations. Other associations are detailed in Table 1, which also includes comparative data regarding the odds for positive HIV and HCV tests simultaneously or separately, alongside the Chi-square test logistic regression analysis results.
Heterosexual intercourse with men in the previous 12 months was evaluated as a potential risk factor, as well. A very strong correlation (φ = 0.32, p < 0.05) was observed for HIV among individuals in prisons. A strong association was found for HCV and HIV-HCV co-infection (φ = 0.2, p = 0.1, and φ = 0.22, p = 0.06, respectively). Within the general population, HIV showed a moderate association. HCV and coinfection are presented in Table 1, Table 2, Table 3 and Table 4, along with the relationships for sexual activity with both men and women in the last 12 months. All available results are for exposures to risk factors over the past 12 months.
The correlation between abstinence from sexual intercourse in the last 12 months and the screening tests results for HIV and HCV in the prison population was very strong (Cramer’s V coefficient = 0.28, p = 0.01 and 0.3, p = 0.01, respectively) and strong in the case of coinfection (Cramer’s V coefficient = 0.23, p = 0.07). Abstinence reduced the chances of reactive HIV and HCV tests in inmates, especially among young patients.
When evaluating unprotected sexual intercourse with penetration within the last 12 months as a risk factor, it was observed that 451 individuals from the general population and 69 individuals from prisons engaged in this risky behavior, while 8 individuals from the second population were unable to recall exposure. Only 5.32% of individuals from the exposed general population presented a HIV reactive screening test, while 57.97% of exposed individuals from the prison population had reactive HIV screening tests. 50% of individuals who reported not remembering exposure also had reactive HIV screening tests. In the case of HCV reactive tests, a strong association was established (Cramer’s V coefficient = 0.23, p = 0.07) among individuals in prisons. Other correlations are detailed in Table 1, Table 2, Table 3 and Table 4.
The participants were asked whether they had been involved in sexual services in exchange for drugs or money in the last 12 months. In the general population, we noticed a prevalence of 42.85% of reactive HIV tests and 71.42% of reactive HCV tests among individuals exposed to this risk factor. The identified association was strong (φ = 0.21, p < 0.001) for HIV and very strong for HCV and coinfection (φ = 0.39, p < 0.001, and φ = 0.42, p < 0.001, respectively). Among individuals in prisons, only the associations with HIV and coinfection were strong (φ = 0.2, p = 0.1 and φ = 0.17, p = 0.21). The correlations between unprotected penetrating sexual intercourse with sex workers are presented in Table 1, Table 2, Table 3 and Table 4.
Individuals diagnosed with STDs in the last 12 months were much more likely to have reactive HIV (OR = 2.77, p = 0.3) and HCV (OR = 1.95, p = 0.52) screening tests among individuals in prisons. Newly diagnosed STDs were strongly associated with reactive HIV screening tests in both populations (general population: Cramer’s V coefficient = 0.33, p < 0.001, prison: φ = 0.3, p < 0.05). Additionally, in the general population, the odds of obtaining a positive screening test for exposed individuals compared to the odds of obtaining a positive one for individuals not recalling exposure were higher for HIV (OR = 7.5, p = 0.03). The association with HCV was strong in both populations (general population: Cramer’s V coefficient = 0.19, p < 0.001, prison: φ = 0.24, p = 0.02).
The association between unprotected penetrating sexual intercourse with HIV+ individuals in the last 12 months and the results of HIV screening tests was one of the strongest in both groups. In the general population, 60% of exposed individuals presented with a reactive test, while only 2.52% of unexposed individuals did. Among individuals in prisons, 92.3% of those who did not recall their exposure were presented with a reactive HIV screening test. Thus, very strong correlations (Cramer’s V coefficient = 0.36, p < 0.001) were established in the general population, as well as among individuals in prisons (Cramer’s V coefficient = 0.33, p < 0.05).
In the case of HCV, the identified correlation was strong (Cramer’s V coefficient = 0.2, p = 0.13) only among individuals in prisons. In the case of HIV-HCV coinfections, a very strong association was also established among individuals in prisons (Cramer’s V coefficient = 0.28, p = 0.02).
A strong association (Cramer’s V coefficient = 0.15, p < 0.001 in the general population and φ = 0.16, p = 0.1 among individuals in prisons) was observed between sexual intercourses with men who have sex with men (MSM) and the results of the HIV screening tests in both tested populations. In general population, 25% of exposed individuals subsequently had a reactive HIV test. Other correlations are presented in Table 1, Table 2, Table 3 and Table 4.
In general population, intravenous drug users showed one of the strongest associations with screening tests for HIV, HCV, and HIV-HCV coinfection (HIV: Cramer’s V coefficient = 0.32, p < 0.001, HCV: Cramer’s V coefficient = 0.59, p < 0.001, co-infection: Cramer’s V coefficient = 0.57, p < 0.001). On the other hand, in the prison population, a very strong association was only established for HCV (φ = 0.46, p < 0.05). The association with the coinfection was strong (φ = 0.17, p = 0.09). Comparative data for the two populations are presented in Figure 1.
Within the same risk group, behaviors associated with intravenous drug use, such as sharing needles, syringes, spoons, filters, and other equipment in the past 12 months, were also evaluated. For needles and syringes, among the general population a very strong association was established between the risk factor and the screening test results (HIV: Cramer’s V coefficient = 0.32, p < 0.001; HCV: 0.42, p < 0.001; coinfection: 0.54, p < 0.001).
In the case of individuals in correctional facilities, a very strong association was only established for HCV (Cramer’s V coefficient = 0.27, p = 0.02). For HIV and coinfection, strong associations were identified (Cramer’s V coefficient = 0.21, p = 0.11; 0.21, p = 0.1, respectively). 68.42% of those who shared needles or syringes had reactive HCV screening tests. Comparisons regarding sharing needles and syringes between the two populations are presented in Figure 2.
Likewise, 17.02% of individuals in the general population who shared the second category of objects had reactive HIV tests (Table 1, Table 2, Table 3 and Table 4).
Unprotected sexual intercourse with intravenous drug users in the past 12 months was evaluated as a potential risk factor. The results of its association with the screening test results are presented in Figure 3. 30.76% of individuals in the general population and 54.54% in correctional facilities who adopted this behavioral pattern had reactive HIV tests.
In the general population, the risk factor was strongly associated with HCV (Cramer’s V coefficient = 0.41, p < 0.001) and HIV-HCV coinfection (Cramer’s V coefficient = 0.41, p < 0.001), and moderately associated with HIV (Cramer’s V coefficient = 0.2, p < 0.001). In contrast, among incarcerated individuals, the association was very strong only in the case of HCV (Cramer’s V coefficient = 0.37, p < 0.05).
HIV reactive tests in the general population was strongly associated with unprotected sex with HIV-positive partners (strongest association), sex workers, new STDs, IDUs and sharing injecting materials (syringes/needles). Among inmates, the strongest association was also unprotected sexual intercourse with HIV+ partners, followed by new STDs. Very strong connections were also established with heterosexual intercourse with men and abstinence in the prisons, while these connections were weak in the general population.
HCV reactive tests showed very strong associations with intravenous drug use (strongest association in both populations), unprotected sex with IDUs and sharing injecting materials (syringes/needles/spoons/filters/water) in both populations and very strong associations with trading sexual services in the general population. In inmates, abstinence was very strongly associated with HCV screening tests, while this association was weak in the general population. HIV-HCV coinfection patterns mirrored HCVs in the general population, but among inmates, it was very strongly associated with unprotected sexual intercourse with HIV-positive partners. A general overview of the association between HIV, HCV and HIV-HCV reactivity and various reported risk factors is presented in Figure 4.
4. Discussion
Our study reports an extremely strong association between intravenous drug use and the results of the HIV, HCV, and HIV-HCV coinfection screening tests in the general population. Since 2011, Romania has faced an HIV epidemic among intravenous drug users, reported in patients exposed to heroin abuse who recently started using psychostimulant drugs too. One third of intravenous drug users were then reported with HIV infection while in detention [8]. In 2015, Romania launched two programs aimed to improve prevention and medical and social care for drug users [9]. These programs also targeted the inmates from Jilava Penitentiary in Bucharest, a population included in this study, as well. Prisoners had significantly higher rates of positive screening tests. However, the 2020 report from Romania’s National Anti-Drug Agency’s Report highlighted a decrease in newly diagnosed HIV infections among IDUs from 32.2% in 2013 to 11% in 2019 [10].
Evidence-based interventions should be integrated and brought to scale, while upcoming programs should focus on the underlying structural drivers of HIV transmission [11]. In the need to put an end to outbreaks in these risk groups, other issues such as homelessness and poverty should also be addressed in an integrative manner, so that not only IDUs are spared of an endless cycle of HIV transmission, but also their communities.
Around 10 million people are incarcerated or in pretrial detention worldwide, with the United States, China, and Russia accounting for half of them, and one in four prisoners has HCV infection [12]. Incarceration increases the risk of HIV and HCV due to associated risky behaviors like unprotected sex, tattooing, intravenous drug use, sexual violence and sharing injection equipment [13]. The risk is amplified by the scarcity of treatment services in prisons, as only 28 countries worldwide provide condoms in prisons [12].
Sexual partners of IDUs face a significant infection risk, which increases with multiple partners [14]. We identified a strong association in the general population. Though underreporting may exist, similar data are also reported in the case of HCV [15,16]. In our study a very strong association with HCV was identified in both groups. Furthermore, the association between intravenous drug use and HCV is well-known and the risk is even higher when sharing needles and injecting tools [17]. This can be attributed to the common behavioral patterns of intravenous drug users.
Therefore, despite the decreasing trends of HIV and HCV infections incidence rates in Romania, the risk of HIV and HCV transmission persists, and require further studies, especially considering the dynamic changes in drug consumption behaviors in favor of new psychoactive substances which comprises 6.3% of all drugs used in Romania in 2019 [10].
Unprotected sex with known HIV-positive individuals in the past year was a major risk factor for HIV infection in our study, showing strong associations with HIV reactive tests and even stronger with HCV and coinfection, particularly among prisoners. Interestingly, inmates unaware of their exposure still had a high positivity rate in screening tests, with 92.3% of tested prisoners being positive.
Unprotected homosexual intercourse significantly raises HIV infection risk, anal sexual intercourse posing the highest risk [15]. Our study identified a strong association with HIV, but not HCV in both populations, which is consistent with other reported studies, reporting its uncommon transmission through unprotected sexual intercourse. A recent study from Mexico suggested an association between drug use during sexual activities (“chemsex”) and HCV transmission, especially following the use of ethyl chloride [18]. Following this pattern, the data from the current study should be extended, considering the lack of information regarding additional sexual practices of the individuals in this study.
The current study indicates a strong association between heterosexual activity with women and HIV screening test results in prisons and a moderate association in the general population. In the case of intercourse with men, the prison group had a higher transmission risk, with very strong associations for HIV and strong for HCV and HIV-HCV coinfection. Research on 563 heterosexual couples across 9 European countries indicated higher transmission rates from men to women, with 12% of men and 20% of women contracting HIV from their opposite-sex partners [19].
Individuals engaged in commercial sex show a high prevalence of STDs: HIV, chlamydia, gonorrhea, syphilis, including HCV, likely due to multiple risk factors [20]. Our study showed a very strong link between unprotected sexual activity with sex workers and HIV test results in the general population, but a weak association in prisons and with HCV both groups, similar with a study from Zimbabwe, attributing this result to the multiplicity of risk factors or underreporting of this behavior [21]. Likewise, the last HIV/AIDS surveillance report in Europe from 2023 indicate that the HIV new cases in Eastern Europe are associated mostly with heterosexual transmission (men 38.3%, women: 33.1%) [22]. Our study found STDs history to be a potent risk factor for HIV and HCV, with meta-analyses supporting this association, particularly emphasizing population variability, and highlighting the possibility of association between various past non-viral STDs and the HIV acquisition [23,24,25]. Moreover, other coinfections also influence the risk of HIV acquisition as well as the course of the disease; the Epstein-Barr virus (EBV) coinfection lowers gamma-interferon (IGN-γ) levels which leads to important pathogenic consequences [26]. However, analyzing these results is challenging because of the possible overlapping sexual behaviors and other risk factors [24].
Our study’s limitation lies in the cohort composition, which isn’t entirely representative of the general population, given the significantly higher prevalence of women in the general population (63.89% vs. 36.1%). The prison sample, with a higher male prevalence (92.78% vs 7.21%), aligns more closely with Romania’s detention demographics as of January 31, 2020 (95.5% men and 4.5% women in correctional facilities) [25]. The limited number of MSM participants from both populations also hinders broad generalization.
However, to our knowledge, this is the first study to compare the risk factors in incarcerated people with the ones from general population in Romania, and although a decreasing trend in HIV and HCV incidence rates are reported in this country, the risk of transmission persists, requiring innovative studies to achieve the micro-elimination of the two infections in this area.
5. Conclusions
Our study underscores the importance of local, targeted and comprehensive public health programs to enhance HIV and HCV diagnosis and management. Key findings include a very strong association between unprotected sexual intercourse with HIV positive individuals and positive HIV tests in both populations. Trading sex for money or drugs had a strong HIV association in both populations, but for HCV this was very strong in the general population, but weak among inmates. Sharing injection equipment was highly associated with HIV, HCV and co-infection in both groups. Unprotected sex with IDUs was very strongly associated with HCV in both populations, with HIV in the general population, but weakly in the inmate’s population. Our study indicates the need for implementing targeted public health programs, tailored to the local epidemiology that can ultimately lead to micro-elimination of hepatitis and HIV infections in this area.
Author Contributions
Conceptualization, C.S.; methodology, C.S. and G.C.; validation, C.F. and A.G.; formal analysis, C.S. and L.I.; investigation, G.C., C.G., A.I. and D.C.; resources, C.F.; data curation, L.I.; writing—original draft preparation, L.I.; writing—C.S. and L.I.; visualization, C.S.; supervision, C.S. and A.G.; project administration, C.F., G.C. and C.S.; funding acquisition, C.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Otto per Mille della Chiesa Valdese, Italy, grant number Ref. OPM/2018/01274 and the APC was funded by Associazione Nazionale per la Lotta contro l’AIDS - SEZIONE LOMBARDA (ANLAIDS), Italy. This research is to be submitted for evaluation with a 50% discount of the APC.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Virology (protocol code 2537 / 12.05.2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Research data is available on request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. SDG target 3.3 communicable diseases; https://www.who.int/data/gho/data/themes/topics/sdg-target-3_3-communicable-diseases.
- Mărdărescu M, Streinu-Cercel A, Popa M. Infecția cu HIV/SIDA: o actualizare a datelor din țara noastră. Infectio.ro 2018; 4 (52): 5-10.
- CNLAS, Romania. https://www.cnlas.ro/images/doc/2023/PREZENTARE-30 iunie-2023-site -07.08.2023.pdf.
- Sultana C, Erscoiu SM, Grancea C, Ceaușu E, Ruță S. Predictors of Chronic Hepatitis C Evolution in HIV Co-Infected Patients From Romania. Hepat Mon 2013; 13(2). [CrossRef]
- Kim AY, Onofrey S, Church DR. An epidemiologic update on hepatitis C infection in persons living with or at risk of HIV infection. J Infect Dis 2013; 207 (Suppl 1): S1-6. [CrossRef]
- Lingala S, Ghany MG. Natural History of Hepatitis C. Gastroenterol Clin North Am 2015; 44(4): 717-34. [CrossRef]
- Huiban L, Stanciu C, Muzica CM, Cuciureanu T, Chiriac S., Zenovia S, et al. Hepatitis C Virus Prevalence and Risk Factors in a Village in Northeastern Romania - A Population-Based Screening - The First Step to Viral Micro-Elimination. Healthcare (Basel) 2021; 9(6): 651. [CrossRef]
- Niculescu I, Paraschiv S, Paraskevis D, Abagiu A, Batan I, Banica L, et al. Recent HIV-1 Outbreak Among Intravenous Drug Users in Romania: Evidence for Cocirculation of CRF14_BG and Subtype F1 Strains. AIDS Res Hum Retroviruses 2015; 31(5): 488-95.
- Guvernul României 2022. The Government has approved two programs in the field of prevention, and psychological, social and medical care provided to drug users; https://www.gov.ro/en/government/cabinet-meeting/the-government-has-approved-two-programs-in-the-field-of-prevention-and-psychological-social-and-medical-care-provided-to-drug-users.
- AGENȚIA NAȚIONALĂ ANTIDROG, ROMÂNIA; http://ana.gov.ro/raportul-national-privind-situatia-drogurilor-in-romania-2020/.
- Strathdee SA, Kuo I, El-Bassel N, Hodder S, Smith LR, Springer SA. Preventing HIV outbreaks among people who inject drugs in the United States: plus ça change, plus ça même chose. AIDS 2020; 34(14): 1997-2005.
- Valera P, Chang Y, Lian Z. HIV risk inside U.S. prisons: a systematic review of risk reduction interventions conducted in U.S. prisons. AIDS Care 2017; 29(8): 943-952.
- Cdc.gov 2021. HIV Among People Who Inject Drugs | HIV by Group | HIV/AIDS | CDC; https://www.cdc.gov/hiv/group/hiv-idu.html.
- Rosengard C, Anderson B, Stein M. Intravenous drug users’ HIV-risk behaviors with primary/other partners. Am J Drug Alcohol Abuse 2004; 30(2): 225-36.
- Amirkhanian Y. Review of HIV vulnerability and condom use in central and eastern Europe. Sex Health 2012; 9(1): 34-43.
- Basu D, Sharma AK, Gupta S, Nebhinani N, Kumar V. Hepatitis C virus (HCV) infection & risk factors for HCV positivity in injecting & non-injecting drug users attending a de-addiction centre in northern India. Indian J Med Res 2015; 142(3): 311-6.
- Bartholomew TS, Onugha J, Bullock C, Scaramutti C, Patel H, Forrest DW, et al. Baseline prevalence and correlates of HIV and HCV infection among people who inject drugs accessing a syringe services program. Harm Reduct J 2020; 17, 40.
- Mata-Marín JA, de Pablos-Leal AA, Mauss S, Arroyo-Anduiza CI, Rodríguez-Evaristo MS, Uribe-Noguéz LA, et al. Risk factors for HCV transmission in HIV-positive men who have sex with men in México. PLoS One 2022; 17(7): e0269977.
- European Study Group On Heterosexual Transmission Of HIV. Comparison Of Female To Male And Male To Female Transmission Of HIV In 563 Stable Couples. BMJ: British Medical Journal 1992; vol. 304, nr. 6830: 809–813.
- Ganley KY, Wilson-Barthes M, Zullo AR, Sosa-Rubí SG, Conde-Glez CJ, García-Cisneros S, et al. Incidence and time-varying predictors of HIV and sexually transmitted infections among male sex workers in Mexico City. Infect Dis Poverty 2021; 10(1): 7.
- Kloek M, Bulstra CA, Chabata ST, Fearon E, Taramusi I, de Vlas SJ, et al. No increased HIV risk in general population near sex work sites: A nationally representative cross-sectional study in Zimbabwe. Trop Med Int Health 2022; 27(8): 696-704. [CrossRef]
- European Centre for Disease Prevention and Control. HIV/AIDS surveillance in Europe 2023 (2022 data); https://www.ecdc.europa.eu/en/publications-data/hivaids-surveillance-europe-2023-2022-data.
- Ward H, Rönn M. Contribution of sexually transmitted infections to the sexual transmission of HIV. Curr Opin HIV AIDS 2010; 5(4): 305-10.
- Barker EK, Malekinejad M, Merai R, Lyles CM, Sipe TA, DeLuca JB, Ridpath D, et al. Risk of Human Immunodeficiency Virus Acquisition Among High-Risk Heterosexuals With Nonviral Sexually Transmitted Infections: A Systematic Review and Meta-Analysis. Sex Transm Dis 2022; 49(6): 383-397. [CrossRef]
- Council of Europe Annual Penal Statistics; https://wp.unil.ch/space/files/2021/04/210330_FinalReport_SPACE_I_2020.pdf.
- Barros I, Santana-da-Silva N, Nogami Y, Santos e Santos C, Pereira L; França E, et al. Immunogenetic Profile Associated with Patients Living with HIV-1 and Epstein–Barr Virus (EBV) in the Brazilian Amazon Region. Viruses 2024; 16, 1012.
Figure 1.
Variation in the probability of obtaining positive HIV and HCV screening tests or the presence of HIV-HCV coinfection based on the presence of the risk factor (intravenous drug users) among individuals in the general population and in the inmates’ population: (a) Graphical representation of how the probability of a positive HIV screening test varies based on the presence or absence of the risk factor among individuals of the same age in the general population; (b) HCV in the general population; (c) HIV-HCV co-infection in the general population; (d) Graphical representation of how the probability of a positive HIV screening test varies based on the presence or absence of the risk factor among individuals of the same age in the inmates’ population; (e) HCV in the inmates’ population; (f) HIV-HCV co-infection in the inmates’ population.
Figure 1.
Variation in the probability of obtaining positive HIV and HCV screening tests or the presence of HIV-HCV coinfection based on the presence of the risk factor (intravenous drug users) among individuals in the general population and in the inmates’ population: (a) Graphical representation of how the probability of a positive HIV screening test varies based on the presence or absence of the risk factor among individuals of the same age in the general population; (b) HCV in the general population; (c) HIV-HCV co-infection in the general population; (d) Graphical representation of how the probability of a positive HIV screening test varies based on the presence or absence of the risk factor among individuals of the same age in the inmates’ population; (e) HCV in the inmates’ population; (f) HIV-HCV co-infection in the inmates’ population.
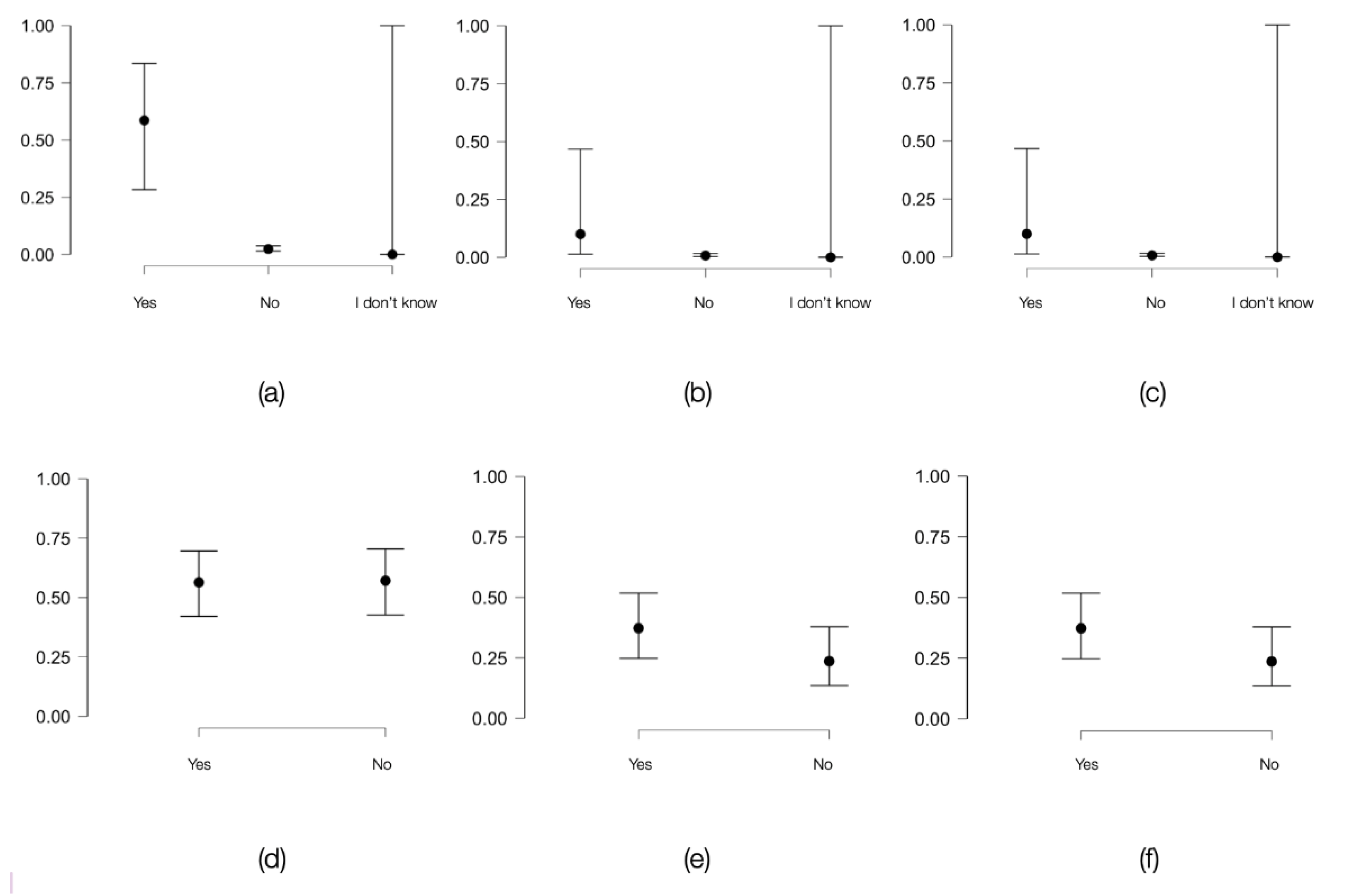
Figure 2.
Variation in the probability of obtaining positive HIV and HCV screening tests or the presence of HIV-HCV coinfection based on the presence of the risk factor (sharing injection materials such as syringes and needles within the last 12 months) among individuals in the general population and in the inmates’ population: (a) Graphical representation of how the probability of a positive HIV screening test varies based on the presence or absence of the risk factor among individuals of the same age in the general population; (b) HCV in the general population; (c) HIV-HCV co-infection in the general population; (d) Graphical representation of how the probability of a positive HIV screening test varies based on the presence or absence of the risk factor among individuals of the same age in the inmates’ population; (e) HCV in the inmates’ population; (f) HIV-HCV co-infection in the inmates’ population.
Figure 2.
Variation in the probability of obtaining positive HIV and HCV screening tests or the presence of HIV-HCV coinfection based on the presence of the risk factor (sharing injection materials such as syringes and needles within the last 12 months) among individuals in the general population and in the inmates’ population: (a) Graphical representation of how the probability of a positive HIV screening test varies based on the presence or absence of the risk factor among individuals of the same age in the general population; (b) HCV in the general population; (c) HIV-HCV co-infection in the general population; (d) Graphical representation of how the probability of a positive HIV screening test varies based on the presence or absence of the risk factor among individuals of the same age in the inmates’ population; (e) HCV in the inmates’ population; (f) HIV-HCV co-infection in the inmates’ population.
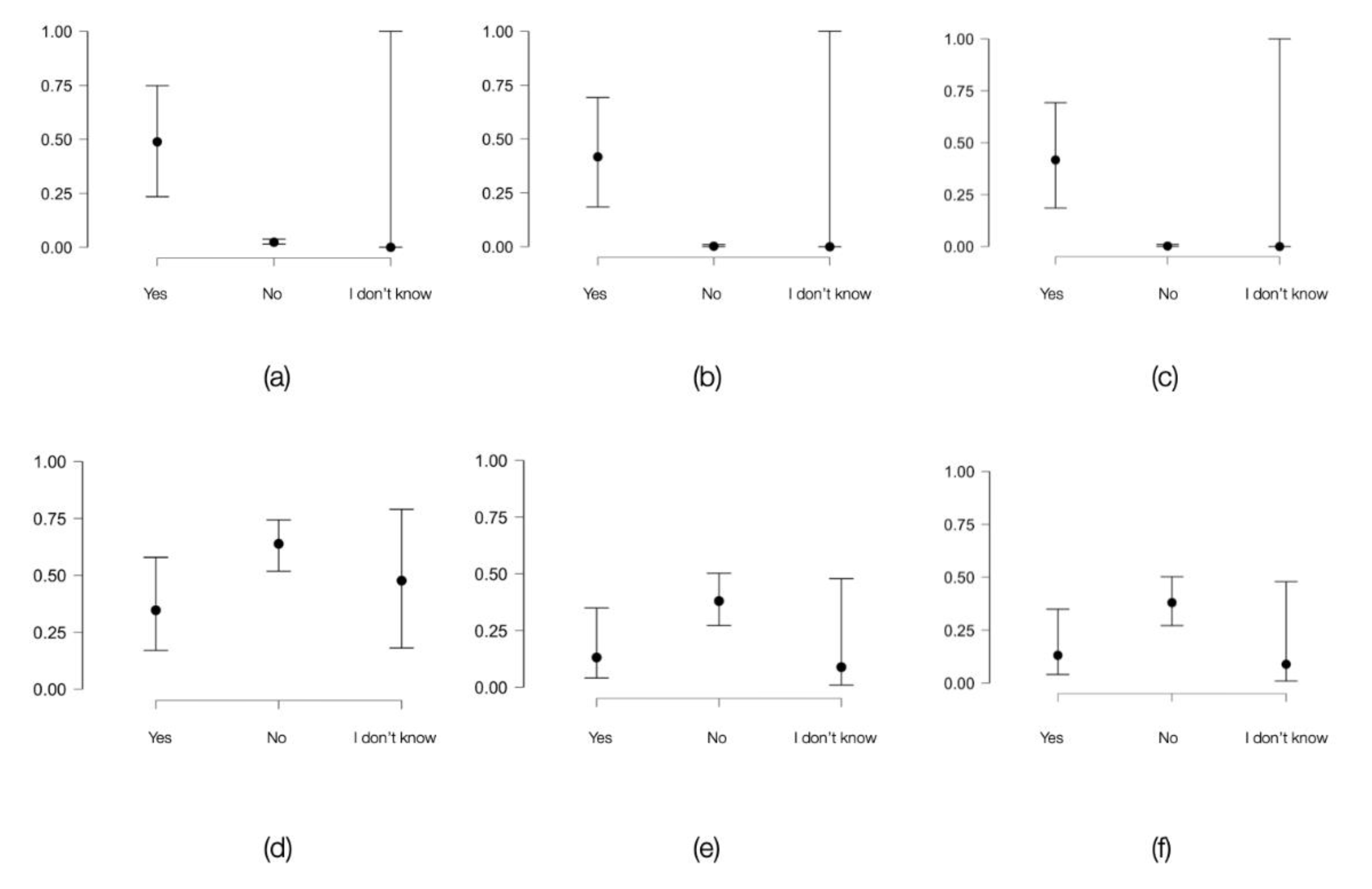
Figure 3.
Variation in the probability of obtaining positive HIV and HCV screening tests or the presence of HIV-HCV coinfection based on the presence of the risk factor (unprotected sexual intercourse with intravenous drug users in the past 12 months) among individuals in the general population and in the inmates’ population: (a) Graphical representation of how the probability of a positive HIV screening test varies based on the presence or absence of the risk factor among individuals of the same age in the general population; (b) HCV in the general population; (c) HIV-HCV co-infection in the general population; (d) Graphical representation of how the probability of a positive HIV screening test varies based on the presence or absence of the risk factor among individuals of the same age in the inmates’ population; (e) HCV in the inmates’ population; (f) HIV-HCV co-infection in the inmates’ population.
Figure 3.
Variation in the probability of obtaining positive HIV and HCV screening tests or the presence of HIV-HCV coinfection based on the presence of the risk factor (unprotected sexual intercourse with intravenous drug users in the past 12 months) among individuals in the general population and in the inmates’ population: (a) Graphical representation of how the probability of a positive HIV screening test varies based on the presence or absence of the risk factor among individuals of the same age in the general population; (b) HCV in the general population; (c) HIV-HCV co-infection in the general population; (d) Graphical representation of how the probability of a positive HIV screening test varies based on the presence or absence of the risk factor among individuals of the same age in the inmates’ population; (e) HCV in the inmates’ population; (f) HIV-HCV co-infection in the inmates’ population.
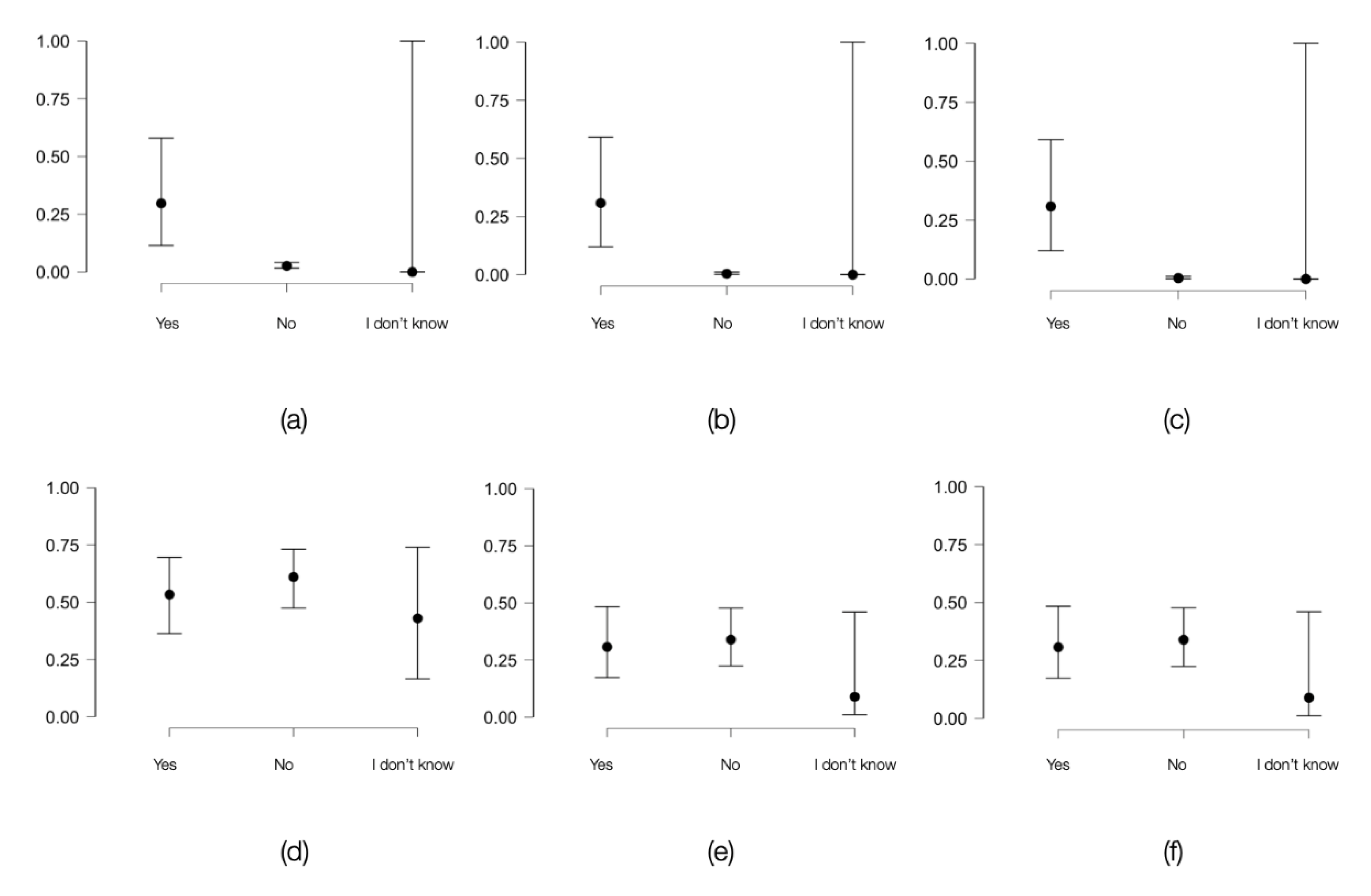
Figure 4.
Established associations between risk factors and the results of the screening tests for HIV, HCV and coinfection in the general population and inmates’ population based on the phi coefficient and Cramer’s V coefficient.
Figure 4.
Established associations between risk factors and the results of the screening tests for HIV, HCV and coinfection in the general population and inmates’ population based on the phi coefficient and Cramer’s V coefficient.
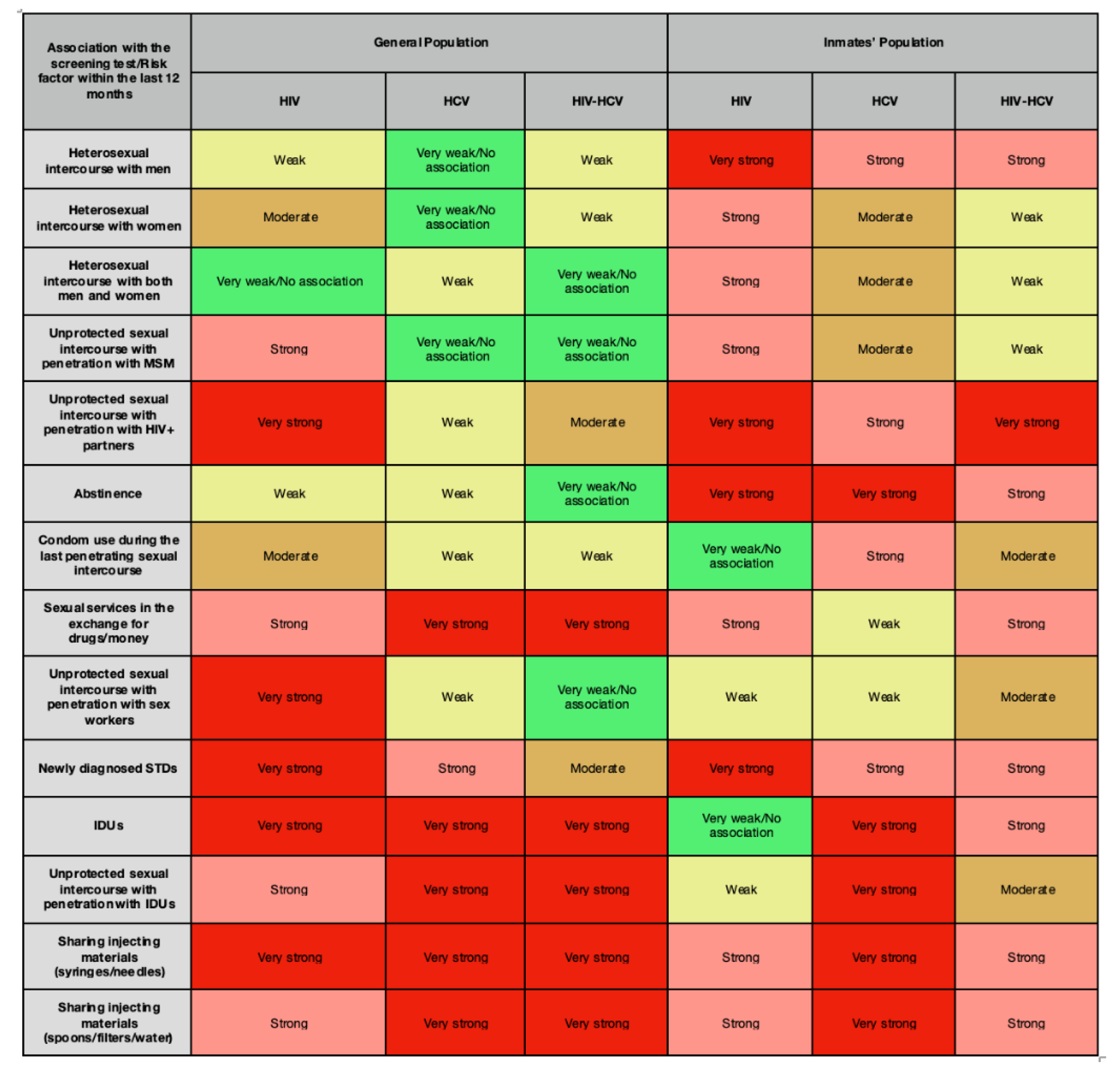

Table 1.
The correlation between risk factors and the outcomes of HIV, HCV and HIV-HCV coinfection screening tests in the general population (Chi-squared Test).
Table 1.
The correlation between risk factors and the outcomes of HIV, HCV and HIV-HCV coinfection screening tests in the general population (Chi-squared Test).
| Risk Factor | Chi-squared Test | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chi-squared Test | Adjusted Chi-squared Test | P Value of Chi-squared Test | P Value of Adjusted Chi-squared Test | Degrees of Freedom | Association Coefficient Phi | Cramer’s V Coefficient | |||||||
| Sexual intercourse with men | HIV | 4.71 | 3.87 | 0.03 | 0.04 | 1 | 0.07 | 0.07 | |||||
| HCV | 0.76 | 0.43 | 0.38 | 0.51 | 1 | 0.03 | 0.03 | ||||||
| HIV-HCV | 2.71 | 1.59 | 0.09 | 0.2 | 1 | 0.05 | 0.05 | ||||||
| Sexual intercourse with women | HIV | 10.24 | 8.89 | 1 | 3 | 1 | 0.11 | 0.11 | |||||
| HCV | 0.5 | 0.22 | 0.47 | 0.63 | 1 | 0.02 | 0.02 | ||||||
| HIV-HCV | 2.58 | 1.42 | 0.1 | 0.23 | 1 | 0.05 | 0.05 | ||||||
| Sexual intercourse with both men and women | HIV | 0.3 | 0.3 | 0.85 | 0.85 | 2 | - | 19 | |||||
| HCV | 2.93 | 2.93 | 0.23 | 0.23 | 2 | - | 0.06 | ||||||
| HIV-HCV | 0.08 | 0.08 | 0.96 | 0.96 | 2 | - | 0.01 | ||||||
| Unprotected sexual intercourse with men who have sex with men (MSM) | HIV | 18.58 | 18.58 | <0.001 | <0.001 | 2 | - | 0.15 | |||||
| HCV | 0.42 | 0.42 | 0.8 | 0.8 | 2 | - | 0.02 | ||||||
| HIV-HCV | 134 | 134 | 0.93 | 0.93 | 2 | - | 0.01 | ||||||
| Unprotected sexual intercourse with HIV+ partners | HIV | 104.65 | 104.65 | <0.001 | <0.001 | 2 | - | 0.36 | |||||
| HCV | 2.14 | 2.14 | 0.34 | 0.34 | 2 | - | 0.05 | ||||||
| HIV-HCV | 9.84 | 9.84 | 7 | 7 | 2 | - | 0.11 | ||||||
| Abstinence | HIV | 6.04 | 5.07 | 0.01 | 0.02 | 1 | 0.08 | 0.08 | |||||
| HCV | 3.93 | 3.09 | 0.04 | 0.07 | 1 | 0.07 | 0.07 | ||||||
| HIV-HCV | 0.05 | <1 | 0.81 | 1 | 1 | 8 | 8 | ||||||
| Condom use during the last penetrating sexual intercourse | HIV | 14.4 | 12.92 | <0.001 | <0.001 | 1 | 0.13 | 0.13 | |||||
| HCV | 4.17 | 3.32 | 0.04 | 0.06 | 1 | 0.07 | 0.07 | ||||||
| HIV-HCV | 5.55 | 3.09 | 0.01 | 0.04 | 1 | 0.08 | 0.08 | ||||||
| Sexual intercourse in exchange for drugs/money | HIV | 35.52 | 23.87 | <0.001 | <0.001 | 1 | 0.21 | 0.21 | |||||
| HCV | 125.52 | 100.77 | <0.001 | <0.001 | 1 | 0.39 | 0.39 | ||||||
| HIV-HCV | 144.6 | 99.58 | <0.001 | <0.001 | 1 | 0.42 | 0.42 | ||||||
| Unprotected sexual intercourse with sex workers | HIV | 56.65 | 56.65 | <0.001 | <0.001 | 2 | - | 0.26 | |||||
| HCV | 2.93 | 2.93 | 0.23 | 0.23 | 2 | - | 0.06 | ||||||
| HIV-HCV | 0.08 | 0.08 | 0.96 | 0.96 | 2 | - | 0.01 | ||||||
| Newly diagnosed sexually transmitted diseases (STDs) | HIV | 91.09 | 91.09 | <0.001 | <0.001 | 2 | - | 0.33 | |||||
| HCV | 29.64 | 29.64 | <0.001 | <0.001 | 2 | - | 0.19 | ||||||
| HIV-HCV | 7.98 | 7.98 | 0.01 | 0.01 | 2 | - | 0.1 | ||||||
| Intravenous drug users (IDUs) | HIV | 84.01 | 84.01 | <0.001 | <0.001 | 2 | - | 0.32 | |||||
| HCV | 284.38 | 284.38 | <0.001 | <0.001 | 2 | - | 0.59 | ||||||
| HIV-HCV | 263.95 | 263.95 | <0.001 | <0.001 | 2 | - | 0.57 | ||||||
| Unprotected sexual intercourse with IDUs | HIV | 32.2 | 32.2 | <0.001 | <0.001 | 2 | - | 0.2 | |||||
| HCV | 138.12 | 138.12 | <0.001 | <0.001 | 2 | - | 0.41 | ||||||
| HIV-HCV | 137.21 | 137.21 | <0.001 | <0.001 | 2 | - | 0.41 | ||||||
| Common use of injecting materials (syringes/needles) | HIV | 85.39 | 85.39 | <0.001 | <0.001 | 2 | - | 0.32 | |||||
| HCV | 141.86 | 141.86 | <0.001 | <0.001 | 2 | - | 0.42 | ||||||
| HIV-HCV | 235.5 | 235.5 | <0.001 | <0.001 | 2 | - | 0.54 | ||||||
| Common use of injecting materials (spoons/filters/water) | HIV | 30.53 | 30.53 | <0.001 | <0.001 | 2 | - | 0.19 | |||||
| HCV | 50.74 | 50.74 | <0.001 | <0.001 | 2 | - | 0.25 | ||||||
| HIV-HCV | 114.03 | 114.03 | <0.001 | <0.001 | 2 | - | 0.37 | ||||||
Legend: the results of the Chi-squared Test with the φ coefficient and Cramer’s V coefficient in the general population; p<0.05 was considered significant.
Table 2.
The correlation between risk factors and the outcomes of HIV, HCV and HIV-HCV coinfection screening tests in the inmates’ population (Chi-squared Test).
Table 2.
The correlation between risk factors and the outcomes of HIV, HCV and HIV-HCV coinfection screening tests in the inmates’ population (Chi-squared Test).
| Risk Factor | Chi-squared Test | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chi-squared Test | Adjusted Chi-squared Test | P Value of Chi-squared Test | P Value of Adjusted Chi-squared Test | Degrees of Freedom | Association Coefficient Phi | Cramer’s V Coefficient | |||||||
| Sexual intercourse with men | HIV | 9.95 | 7.89 | <0.05 | <0.05 | 1 | 0.32 | 0.32 | |||||
| HCV | 3.87 | 2.67 | 0.04 | 0.1 | 1 | 0.2 | 0.2 | ||||||
| HIV-HCV | 4.99 | 3.05 | 0.02 | 0.06 | 1 | 0.22 | 0.22 | ||||||
| Sexual intercourse with women | HIV | 3.23 | 2.13 | 0.07 | 0.14 | 1 | 0.18 | 0.18 | |||||
| HCV | 1.69 | 0.93 | 0.19 | 0.33 | 1 | 0.13 | 0.13 | ||||||
| HIV-HCV | 0.62 | 0.18 | 0.42 | 0.66 | 1 | 0.08 | 0.08 | ||||||
| Sexual intercourse with both men and women | HIV | 2.67 | 0.83 | 0.1 | 0.36 | 1 | 0.16 | 0.16 | |||||
| HCV | 2 | 0.49 | 0.15 | 0.48 | 1 | 0.14 | 0.14 | ||||||
| HIV-HCV | 0.91 | 0.03 | 0.33 | 0.85 | 1 | 0.09 | 0.09 | ||||||
| Unprotected sexual intercourse with men who have sex with men (MSM) | HIV | 2.67 | 0.83 | 0.1 | 0.36 | 1 | 0.16 | 0.16 | |||||
| HCV | 2 | 0.49 | 0.15 | 0.48 | 1 | 0.14 | 0.14 | ||||||
| HIV-HCV | 0.91 | 0.03 | 0.33 | 0.85 | 1 | 0.09 | 0.09 | ||||||
| Unprotected sexual intercourse with HIV+ partners | HIV | 7.99 | 7.99 | 0.01 | 0.01 | 2 | - | 0.28 | |||||
| HCV | 8.74 | 8.74 | 0.01 | 0.01 | 2 | - | 0.3 | ||||||
| HIV-HCV | 5.12 | 5.12 | 0.07 | 0.07 | 2 | - | 0.23 | ||||||
| Abstinence | HIV | 0.21 | 0.21 | 0.89 | 0.89 | 2 | - | 0.04 | |||||
| HCV | 5.02 | 5.02 | 0.07 | 0.07 | 2 | - | 0.23 | ||||||
| HIV-HCV | 1.46 | 1.46 | 0.48 | 0.48 | 2 | - | 0.12 | ||||||
| Condom use during the last penetrating sexual intercourse | HIV | 4.17 | 2.61 | 0.04 | 0.1 | 1 | 0.2 | 0.2 | |||||
| HCV | 0.66 | 0.15 | 0.41 | 0.69 | 1 | 0.08 | 0.08 | ||||||
| HIV-HCV | 7.99 | 7.99 | 0.01 | 0.01 | 2 | - | 0.28 | ||||||
| Sexual intercourse in exchange for drugs/money | HIV | 4.17 | 2.61 | 0.04 | 0.1 | 1 | 0.2 | 0.2 | |||||
| HCV | 0.66 | 0.15 | 0.41 | 0.69 | 1 | 0.08 | 0.08 | ||||||
| HIV-HCV | 2.86 | 1.52 | 0.09 | 0.21 | 1 | 0.17 | 0.17 | ||||||
| Unprotected sexual intercourse with sex workers | HIV | 0.68 | 0.05 | 0.4 | 0.81 | 1 | 0.08 | 0.08 | |||||
| HCV | 0.32 | <1 | 0.57 | 1 | 1 | 0.05 | 0.05 | ||||||
| HIV-HCV | 1.38 | 0.29 | 0.23 | 0.58 | 1 | 0.12 | 0.12 | ||||||
| Newly diagnosed sexually transmitted diseases (STDs) | HIV | 9.28 | 8.05 | <0.05 | <0.05 | 1 | 0.3 | 0.3 | |||||
| HCV | 5.71 | 4.77 | 0.01 | 0.02 | 1 | 0.24 | 0.24 | ||||||
| HIV-HCV | 4.26 | 3.39 | 0.03 | 0.06 | 1 | 0.21 | 0.21 | ||||||
| Intravenous drug users (IDUs) | HIV | 8 | 0 | 0.92 | 1 | 1 | 9 | 9 | |||||
| HCV | 20.87 | 19.05 | <0.05 | <0.05 | 1 | 0.46 | 0.46 | ||||||
| HIV-HCV | 2.85 | 2.16 | 0.09 | 0.14 | 1 | 0.17 | 0.17 | ||||||
| Unprotected sexual intercourse with IDUs | HIV | 0.85 | 0.85 | 0.65 | 0.65 | 2 | - | 0.09 | |||||
| HCV | 13.72 | 13.72 | <0.05 | <0.05 | 2 | - | 0.37 | ||||||
| HIV-HCV | 1.82 | 1.82 | 0.4 | 0.4 | 2 | - | 0.13 | ||||||
| Common use of injecting materials (syringes/needles) | HIV | 4.27 | 4.27 | 0.11 | 0.11 | 2 | - | 0.21 | |||||
| HCV | 7.06 | 7.06 | 0.02 | 0.02 | 2 | - | 0.27 | ||||||
| HIV-HCV | 4.57 | 4.57 | 0.1 | 0.1 | 2 | - | 0.21 | ||||||
| Common use of injecting materials (spoons/filters/water) | HIV | 3.27 | 3.27 | 0.19 | 0.19 | 2 | - | 0.18 | |||||
| HCV | 8.06 | 8.06 | 0.01 | 0.01 | 2 | - | 0.28 | ||||||
| HIV-HCV | 4.06 | 4.06 | 0.13 | 0.13 | 2 | - | 0.2 | ||||||
Legend: the results of the Chi-squared Test with the φ coefficient and Cramer’s V coefficient in the inmates’ population; p<0.05 was considered significant.
Table 3.
The correlation between risk factors and the outcomes of HIV, HCV and HIV-HCV coinfection screening tests in the general population (Logistic Regression).
Table 3.
The correlation between risk factors and the outcomes of HIV, HCV and HIV-HCV coinfection screening tests in the general population (Logistic Regression).
| Risk Factor | Chi-squared Test | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| OR Reactive vs Non-reactive * | P Value | OR Age ** | P Value | OR Exposed vs Non-exposed *** | P Value | OR Exposed vs No response **** | P Value | ||
| Sexual intercourse with men | HIV | 0.04 | <0.001 | 0.98 | 0.2 | 2.56 | 0.02 | - | - |
| HCV | 4 | <0.001 | 0.99 | 0.92 | 1.54 | 0.12 | - | - | |
| HIV-HCV | 4 | <0.001 | 0.99 | 0.92 | 3.66 | 0.12 | - | - | |
| Sexual intercourse with women | HIV | 0.11 | <0.001 | 0.98 | 0.36 | 0.29 | 3 | - | - |
| HCV | 0.01 | <0.001 | 1 | 0.95 | 0.31 | 0.12 | - | - | |
| HIV-HCV | 0.01 | <0.001 | 1 | 0.95 | 0.31 | 0.12 | - | - | |
| Sexual intercourse with both men and women | HIV | <1 | 0.98 | 0.98 | 0.31 | >1 | 0.98 | 0.98 | 1 |
| HCV | <1 | 0.99 | 1 | 0.98 | >1 | 0.99 | 1 | 1 | |
| HIV-HCV | <1 | 0.99 | 1 | 0.98 | >1 | 0.99 | 1 | 1 | |
| Unprotected sexual intercourse with men who have sex with men (MSM) | HIV | 0.48 | 0.38 | 0.98 | 0.44 | 0.09 | <0.001 | <1 | 0.98 |
| HCV | <1 | 0.99 | 1 | 0.98 | >1 | 0.99 | 0.99 | 1 | |
| HIV-HCV | <1 | 0.99 | 1 | 0.98 | >1 | 0.99 | 0.99 | 1 | |
| Unprotected sexual intercourse with HIV+ partners | HIV | 2.06 | 0.28 | 0.98 | 0.36 | 0.01 | <0.001 | <1 | 0.98 |
| HCV | 0.11 | 0.04 | 1 | 0.99 | 0.06 | 0.01 | <1 | 0.99 | |
| HIV-HCV | 0.11 | 0.04 | 1 | 0.99 | 0.06 | 0.01 | <1 | 0.99 | |
| Abstinence | HIV | 0.08 | <0.001 | 0.98 | 0.31 | 0.27 | 0.02 | - | - |
| HCV | 8 | <0.001 | 1 | 0.99 | 1.02 | 0.81 | - | - | |
| HIV-HCV | 8 | <0.001 | 1 | 0.99 | 1.02 | 0.81 | - | - | |
| Condom use during the last penetrating sexual intercourse | HIV | 0.01 | <0.001 | 0.98 | 0.2 | 10.42 | 2 | - | - |
| HCV | <1 | 0.98 | 0.99 | 0.92 | >1 | 0.99 | - | - | |
| HIV-HCV | <1 | 0.98 | 0.99 | 0.92 | >1 | 0.99 | - | - | |
| Sexual intercourse in exchange for drugs/money | HIV | 1.21 | 0.83 | 0.98 | 0.38 | 0.04 | <0.001 | - | - |
| HCV | 0.73 | 0.69 | 1 | 0.91 | 7 | <0.001 | - | - | |
| HIV-HCV | 0.73 | 0.69 | 1 | 0.91 | 7 | <0.001 | - | - | |
| Unprotected sexual intercourse with sex workers | HIV | 1.45 | 0.66 | 0.98 | 0.47 | 0.03 | <0.001 | <1 | 0.98 |
| HCV | <1 | 0.99 | 1 | 0.98 | >1 | 0.99 | 1 | 1 | |
| HIV-HCV | <1 | 0.00 | 1 | 0.98 | >1 | 0.99 | 1 | 1 | |
| Newly diagnosed sexually transmitted diseases (STDs) | HIV | 0.29 | 0.19 | 0.98 | 0.27 | 0.16 | 0.02 | 7.05 | 0.03 |
| HCV | <1 | 0.99 | 1 | 0.98 | >1 | 0.99 | >1 | 0.99 | |
| HIV-HCV | <1 | 0.99 | 1 | 0.98 | >1 | 0.99 | >1 | 0.99 | |
| Intravenous drug users (IDUs) | HIV | 0.97 | 0.97 | 0.98 | 0.45 | 0.03 | <0.001 | <1 | 0.98 |
| HCV | 1 | 0.04 | 1.17 | 0.06 | <1 | 0.92 | <1 | 1 | |
| HIV-HCV | 1 | 0.04 | 1.17 | 0.06 | <1 | 0.92 | <1 | 1 | |
| Unprotected sexual intercourse with IDUs | HIV | 0.81 | 0.8 | 0.98 | 0.32 | 0.06 | <0.001 | <1 | 0.98 |
| HCV | 0.43 | 0.19 | 1 | 0.93 | 9 | <0.001 | <1 | 0.99 | |
| HIV-HCV | 0.43 | 0.19 | 1 | 0.93 | 9 | <0.001 | <1 | 0.99 | |
| Common use of injecting materials (syringes/needles) | HIV | 1.94 | 0.44 | 0.98 | 0.3 | 0.02 | <0.001 | <1 | 0.98 |
| HCV | 0.69 | 0.56 | 1 | 0.9 | 0.92 | <0.001 | >1 | 0.99 | |
| HIV-HCV | 0.69 | 0.56 | 1 | 0.9 | 4 | <0.001 | <1 | 0.99 | |
| Common use of injecting materials (spoons/filters/water) | HIV | 0.4 | 0.2 | 0.98 | 0.26 | 0.11 | <0.001 | <1 | 0.98 |
| HCV | 0.15 | 0.12 | 1 | 0.91 | <1 | 0.99 | <1 | 0.99 | |
| HIV-HCV | 0.15 | 0.12 | 1 | 0.91 | <1 | 0.99 | <1 | 0.99 | |
Legend: the results of the Logistic Regression in the general population. * The likelihood of a reactive test compared to a non-reactive one among individuals exposed to the risk factor. ** The likelihood of age influencing the screening test outcome in individuals from the same group (with or without a risk factor). *** The likelihood of a positive test among individuals exposed to the risk factor compared to those who were not exposed. **** The likelihood of a positive test among individuals exposed to the risk factor compared to those who did not recall exposure to the risk factor; p<0.05 was considered significant.
Table 4.
The correlation between risk factors and the outcomes of HIV, HCV and HIV-HCV coinfection screening tests in the inmates’ population (Logistic Regression).
Table 4.
The correlation between risk factors and the outcomes of HIV, HCV and HIV-HCV coinfection screening tests in the inmates’ population (Logistic Regression).
| Risk Factor | Chi-squared Test | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| OR Reactive vs Non-reactive * | P Value | OR Age ** | P Value | OR Exposed vs Non-exposed *** | P Value | OR Exposed vs No response **** | P Value | ||
| Sexual intercourse with men | HIV | 0.36 | 0.45 | 0.96 | 0.17 | 18.57 | <0.05 | - | - |
| HCV | <1 | 0.99 | 0.95 | 0.06 | >1 | 0.98 | - | - | |
| HIV-HCV | <1 | 0.99 | 0.95 | 0.06 | >1 | 0.98 | - | - | |
| Sexual intercourse with women | HIV | 3.65 | 0.19 | 0.97 | 0.35 | 0.26 | 0.06 | - | - |
| HCV | 2.25 | 0.44 | 0.96 | 0.13 | 0.45 | 0.34 | - | - | |
| HIV-HCV | 2.25 | 0.44 | 0.96 | 0.13 | 0.45 | 0.34 | - | - | |
| Sexual intercourse with both men and women | HIV | <1 | 0.98 | 0.98 | 0.44 | >1 | 0.98 | - | - |
| HCV | <1 | 0.99 | 0.96 | 0.15 | >1 | 0.99 | - | - | |
| HIV-HCV | <1 | 0.99 | 0.96 | 0.15 | >1 | 0.99 | - | - | |
| Unprotected sexual intercourse with men who have sex with men (MSM) | HIV | <1 | 0.98 | 0.98 | 0.44 | >1 | 0.98 | - | - |
| HCV | <1 | 0.99 | 0.96 | 0.15 | >1 | 0.99 | - | - | |
| HIV-HCV | <1 | 0.99 | 0.96 | 0.15 | >1 | 0.99 | - | - | |
| Unprotected sexual intercourse with HIV+ partners | HIV | <1 | 0.99 | 0.98 | 0.56 | >1 | 0.99 | >1 | 0.98 |
| HCV | <1 | 0.99 | 0.96 | 0.2 | >1 | 0.99 | >1 | 0.99 | |
| HIV-HCV | <1 | 0.99 | 0.96 | 0.2 | >1 | 0.99 | >1 | 0.99 | |
| Abstinence | HIV | 2.59 | 0.34 | 0.99 | 0.73 | 0.23 | 9 | 0.52 | 0.38 |
| HCV | 2.68 | 0.37 | 0.96 | 0.17 | 0.31 | 92 | 0.19 | 0.14 | |
| HIV-HCV | 2.68 | 0.37 | 0.96 | 0.17 | 0.31 | 0.09 | 0.19 | 0.14 | |
| Condom use during the last penetrating sexual intercourse | HIV | 2.36 | 0.41 | 0.98 | 0.48 | 1.12 | 0.82 | 0.76 | 0.75 |
| HCV | 2.37 | 0.46 | 0.95 | 0.11 | 1.17 | 0.77 | 0.26 | 0.26 | |
| HIV-HCV | 2.37 | 0.46 | 0.95 | 0.11 | 1.17 | 0.77 | 0.26 | 0.26 | |
| Sexual intercourse in exchange for drugs/money | HIV | 0.47 | 0.58 | 0.97 | 0.28 | 8.87 | 0.05 | - | - |
| HCV | <1 | 0.99 | 0.95 | 0.08 | >1 | 0.99 | - | - | |
| HIV-HCV | <1 | 0.99 | 0.95 | 0.08 | >1 | 0.99 | - | - | |
| Unprotected sexual intercourse with sex workers | HIV | 0.91 | 0.95 | 0.98 | 0.43 | 3.13 | 0.36 | - | - |
| HCV | <1 | 0.99 | 0.96 | 0.11 | >1 | 0.99 | - | - | |
| HIV-HCV | <1 | 0.99 | 0.96 | 0.11 | >1 | 0.99 | - | - | |
| Newly diagnosed sexually transmitted diseases (STDs) | HIV | 2.77 | 0.3 | 1.002 | 0.93 | 0.25 | 4 | - | - |
| HCV | 1.95 | 0.52 | 0.97 | 0.33 | 0.44 | 0.07 | - | - | |
| HIV-HCV | 1.95 | 0.52 | 0.97 | 0.33 | 0.44 | 0.07 | - | - | |
| Intravenous drug users (IDUs) | HIV | 2.04 | 0.36 | 0.98 | 0.51 | 1.03 | 0.94 | - | - |
| HCV | 1.86 | 0.55 | 0.97 | 0.28 | 0.52 | 0.15 | - | - | |
| HIV-HCV | 1.86 | 0.55 | 0.97 | 0.28 | 0.52 | 0.15 | - | - | |
| Unprotected sexual intercourse with IDUs | HIV | 2.63 | 0.32 | 0.98 | 0.38 | 1.36 | 0.49 | 0.65 | 0.58 |
| HCV | 2.65 | 0.37 | 0.95 | 0.1 | 1.15 | 0.76 | 0.22 | 0.19 | |
| HIV-HCV | 2.65 | 0.37 | 0.95 | 0.1 | 1.15 | 0.76 | 0.22 | 0.19 | |
| Common use of injecting materials (syringes/needles) | HIV | 1.62 | 0.63 | 0.97 | 0.25 | 3.32 | 0.03 | 1.71 | 0.53 |
| HCV | 1.38 | 0.78 | 0.94 | 51 | 4.05 | 0.04 | 0.64 | 0.73 | |
| HIV-HCV | 1.38 | 0.78 | 0.94 | 51 | 5.04 | 0.04 | 0.64 | 0.73 | |
| Common use of injecting materials (spoons/filters/water) | HIV | 1.62 | 0.63 | 0.97 | 0.29 | 2.86 | 0.05 | 1.56 | 0.6 |
| HCV | 1.37 | 0.79 | 0.95 | 0.06 | 3.06 | 0.06 | 0.6 | 0.69 | |
| HIV-HCV | 1.37 | 0.79 | 0.95 | 0.06 | 3.06 | 0.06 | 0.6 | 0.69 | |
Legend: the results of the Logistic Regression in the inmates’ population. * The likelihood of a reactive test compared to a non-reactive one among individuals exposed to the risk factor. ** The likelihood of age influencing the screening test outcome in individuals from the same group (with or without a risk factor). *** The likelihood of a positive test among individuals exposed to the risk factor compared to those who were not exposed. **** The likelihood of a positive test among individuals exposed to the risk factor compared to those who did not recall exposure to the risk factor; p<0.05 was considered significant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



