
Submitted:
08 July 2024
Posted:
10 July 2024
You are already at the latest version
Abstract
Extramammary Paget disease (EMPD) is an uncommon adenocarcinoma of apocrine gland-rich areas, presenting significant diagnostic challenges due to its nonspecific clinical appearance and frequent misidentification as benign, inflammatory skin conditions. Traditional diagnostic methods such as biopsy are invasive and uncomfortable, often required repeatedly due to high recurrence rates. Dermoscopy and non-invasive imaging techniques have been used but provide limited diagnostic accuracy due to their constraints in depth penetration and resolution. Recent advancements in imaging technologies, such as line-field confocal optical coherence tomography (LC-OCT), show promise in enhancing diagnostic precision while minimizing invasive procedures. LC-OCT merges high-resolution imaging with deep penetration capabilities, capturing detailed horizontal and vertical skin images akin to histopathology. This study evaluated the diagnostic performance of LC-OCT in detecting EMPD and its recurrence in 17 clinically suspicious anogenital regions, belonging to 6 patients. Data were collected prospectively at patient bedside by an LC-OCT expert with poor training for EMPD; and, then, reviewed retrospectively by an independent LC-OCT expert with adequate training for EMPD and no concerns about time. The prospective examination yielded 64.7%-accuracy, 71.4%-sensitivity, and 33.3%-specificity. The retrospective analysis achieved 94.1%-accuracy, 100%-sensitivity, and 66.7%-specificity, with the only false positive case being a difficult-to-diagnose concomitant presentation of a lichen sclerosus et atrophicus. Despite the need for specialized training, our results suggest that LC-OCT represents a valuable tool for accurately identifying EMPD and improve its management by reducing unnecessary biopsies. Further studies are needed to standardize its clinical application.
Keywords:
Extramammary Paget disease
; non-invasive imaging techniques
; line-field confocal optical coherence tomography
; LC-OCT
; recurrence
; diagnostic accuracy
1. Introduction
Extramammary Paget disease (EMPD) is a relatively uncommon form of adenocarcinoma localized on apocrine glands rich areas and first described by Henry Radcliffe Crocker in 1889 [1]. It typically occurs in individuals in their sixth decade of life and affects more frequently women than men worldwide, with an Asian exception where occurrence is equal across sex [2]. It appears clinically as slow-growing, demarcated, thickened, erythematous plaques, less commonly ulcerated, eroded or crusted due to recurrent trauma from pruritus or secondary infection, especially in long-standing disease [2,3]. EMPD often poses significant diagnostic challenges due firstly to its nonspecific clinical presentation [2,3], frequently resembling benign, inflammatory or infectious skin conditions and secondly to its frequent ill-defined [3] presentation affecting delicate areas such as genitalia [2,3,4,5]. This often leads to delayed diagnoses or suboptimal treatment [2,3]. Furthermore EMPD predominantly affects the perianal and genital regions and rarely can also be ectopic [2,4,5], making its accurate diagnosis and monitoring not only crucial for effective management but also sensitive. Current diagnostic methods, primarily histopathology requiring biopsy [2,4,5] are invasive and uncomfortable for patients especially in the context of a chronic pathology with a high rate of recurrence where multiple biopsies will be required throughout the course of the disease [2,3]. The morbidity and related cost associated with biopsies highlight the need for advancements in non-invasive, accurate diagnostic tools that can alleviate patient distress by minimizing invasive procedures and improving diagnostic timelines.
Among them, dermoscopy is the most widely used in dermatology since it has been confirmed to improve diagnostic accuracy in melanoma [6] and non-melanoma skin cancer [7]. Thanks to a 10-fold magnification and the use of polarized light, it allows the visualization of skin features not visible to the naked eye [8]. Mainly employed for pigmented lesion evaluation [8,9], it can also identify patterns of inflammatory skin diseases [8] which represent the most mimicking conditions of EMPD [10,11]. However, it provides limited microscopic information [12], which has resulted in a low number of reported dermoscopic findings for EMPD, highlighting the difficulty in differentiating the disease from other oncological conditions (e.g., Bowen’s disease) [13]. Additionally, certain dermoscopic criteria overlap between EMPD and its mimickers [10]. This means that, so far, dermoscopy of EMPD could only be employed as an adjunct tool to help in differential diagnosis and is not yet a diagnostic tool in itself [10,13].
Reflectance confocal microscopy (RCM) provides en face (horizontal) images of the skin, extending from the stratum corneum of the epidermis to the upper dermis. Despite its limited penetration depth of about 200 μm, RCM offers a high lateral resolution of 1 μm allowing the perfect visualization of the cells [14]. Its first use was oriented to dermato-oncology [14] including EMPD [11,15], but subsequent studies have established its usefulness also in inflammatory skin conditions [16]. However, contrary to what happens in histopathology, it enables the exploration of the skin only in the horizontal plane; despite this, previous studies showed a strong correlation between RCM and histological findings then confirming its ability to diagnose and differentiate EMPD from inflammatory or tumoral skin diseases [17,18]. A recent prospective study performed in 5 patients reported a 75%-sensitivity and a 100%-specificity, suggesting that this technique may potentially improve EMPD detection [19]. Nevertheless, the limited depth of examination and the need for specialized skills to interpret horizontal views restrict the deployment of these technologies to only a limited number of centers [14,20].
Conventional optical coherence tomography (c-OCT), offering both en face and cross-sectional imaging, provides a greater penetration depth (varying from 1 to 2 mm) and a lower axial and lateral resolution (around 15 μm) [21], which limits its utility in EMPD [11,22]. Conversely, full-field OCT (FF-OCT) achieves superior axial and lateral resolutions of 1.35 μm and 1 μm respectively, though at a reduced penetration depth of 400 μm [23]. This enhanced resolution makes FF-OCT particularly suitable for capturing detailed images of epidermal layers, essential in the accurate diagnosis of dermatological conditions like EMPD. This advancement, as demonstrated by Wang et al., enables the description of EMPD patterns well correlated to histopathology [23]. However, given the limited number of publications and the absence of large clinical trials, only a few selected centers appear to be using this technology at present.
Ultrasound application in the field of dermatology has seen a significant increase due to their numerous advantages: readily accessible, quick, cost-effective and easy-to-use [11,24]. Conventional ultrasound devices typically face challenges in generating distinct images of superficial epidermal lesion such as those characteristic of EMPD, due to their low resolution and are generally effective for identifying large and deep skin abnormalities [24]. However ongoing advancements in ultrasound technology with the integration of higher frequency transducers (superior to 20 MHz) have markedly improved its utility in dermatology [24]. Consequently, the so-called high-frequency ultrasound (HF-US) has become increasingly effective through its enhanced resolution in evaluating morphological insights from more superficial dermatological conditions. HF-US now represents a critical tool in the preoperative assessment of skin cancers [24] including EMPD [25], enabling detailed examination of the lesion’s depth and margins [25,26], which are crucial for effective treatments. Despite these advancements, ultrasonographic characteristics of EMPD are not yet reliable for diagnostic purposes. Instead, HF-US may be used primarily to determine the extent of disease prior to surgery, or to identify invasive or infiltrative areas for scouting biopsy, and secondarily to assess the treatment success [25,26].
Line-field confocal OCT (LC-OCT) is one of the latest non-invasive imaging technology available on the market and offers a “virtual histology” of skin lesions [27]. This technology captures optical images in real time, both horizontally and vertically, with confocal-like resolution (axial resolution of 1.1 µm and lateral resolution of 1.3 µm) and conventional OCT-like depth of penetration (500 µm) [27]. Moreover, an integrated dermoscopic camera helps in navigating precisely into the lesion and in outlining margins. Merging the high-resolution benefits of RCM with the vertical imaging and deep penetration capabilities of OCT, LC-OCT has been the subject of numerous publications that explore a variety of dermatological disorders [28,29], emphasizing its value in the diagnosis of many skin conditions thus reducing the need for unnecessary biopsies. It has been reported that LC-OCT has a greater diagnostic accuracy for skin carcinomas than clinical/dermoscopic evaluation both in studies [30] and in real-life settings [31,32]. However, to date, there are only two publications on EMPD imaged by LC-OCT, which describe features that closely resemble histopathological observations [33,34]. Thanks to its resemblance to histopathological images, ease of use and ability to perform live, localized dermoscopic imaging, LC-OCT seems to be a valuable tool for improving clinical diagnostic accuracy of EMPD and assessment of EMPD-recurrence while reducing the number of avoidable biopsies.
The primary objective of this study was to evaluate the diagnostic performance of LC-OCT in detecting EMPD and, specifically, its recurrence following surgical or medical treatment. For this purpose, we employed data collected from a patient’s bedside prospective setting complemented by a subsequent, retrospective, expert image revision.
2. Materials and Methods
We retrospectively included a cohort of patients with histopathologically-proven EMPD referred to the Department of Dermatology of the Hôpital Erasme, Université Libre de Bruxelles (Brussels, Belgium) to rule out disease persistence or recurrence after diverse treatments approaches, including topical therapies (imiquimod) and surgical procedures. The patient evaluations spanned from February 2020 to January 2024. During this period, LC-OCT was used in each patient to evaluate clinically suspicious areas for the presence of EMPD prior to skin biopsy for confirmation or exclusion of EMPD diagnosis.
The study was structured into three distinct phases: (i) LC-OCT data were first prospectively collected at the patient’s bedside by a LC-OCT expert and methodically documented into the patient’s medical record; (ii) the imaged sites were subsequently biopsied for histopathological confirmation (deemed gold standard diagnostic test); and, finally, (iii) a subsequent retrospective evaluation of the previously collected LC-OCT images/videos, blinded to the histopathological data, was conducted by an independent LC-OCT expert. The expert’s review was based on a specific training regimen that incorporated LC-OCT insights from two recent publications [33,34] on EMPD, which were not available during the initial prospective evaluation. This phase aimed to assess the diagnostic reliability and accuracy of LC-OCT in a blinded and controlled setting.
In our assessment criteria, a site was considered to be affected by EMPD if Paget’s cells (PCs) were identified within the epidermis during LC-OCT evaluation, as previously shown [33,34]. PCs were characterized by their distinct appearance as dark to black cells, noticeably larger than the adjacent keratinocytes in the epidermis. PCs can be found either singly or clustered, forming dark glandular structures that are mainly located at the level of the dermal-epidermal junction. The identification of these specific characteristics was crucial for confirming or disagreeing with the presence of disease at the evaluated sites.
Categorical variables are presented with numbers with percentages, continuous variables with median and range. Key statistical measures were calculated to evaluate the diagnostic performance of the study: sensitivity was determined as the proportion of true positives (TP) out of the total actual positives (TP + false negatives [FN]); specificity as the proportion of true negatives (TN) out of the total actual negatives (TN + false positives [FP]); positive predictive value (PPV) as the ratio of TP to the total predicted positives (TP + FP); negative predictive value (NPV) as the ratio of TN to the total predicted negatives (TN + FN); and accuracy as the proportion of all true results (both TP and TN) out of the total cases. Statistical analyses were performed using Microsoft® Excel version 15.32 © 2017 (Microsoft Corporation, Redmond, Washington, United States).
3. Results
Overall, we included 17 clinically suspicious anogenital regions indicative of EMPD, belonging to 6 patients (3 females and 3 males) with a median age of 63 (38-72) years. Of these, 14 regions (82.4%) were histopathologically positive for either EMPD persistence or recurrence after the study biopsy, while 3 regions (17.6%) did not show histopathological signs of the disease.
During the initial prospective bedside evaluation, 10 out of 14 positive cases were correctly identified, and 1 out of 3 negative cases was accurately recognized, resulting in 4 false negatives and 2 false positives. This phase concluded with an overall accuracy of 64.7%, sensitivity at 71.4%, specificity at 33.3%, a positive predictive value (PPV) of 83.3%, and a negative predictive value (NPV) of 20% (Figure 1).
The subsequent retrospective evaluation correctly identified all (14/14) positive cases and 2/3 negative cases, (i.e., no false negative and 1 false positive case, also detected as such in the prospective evaluation setting). All 4 false negative cases that were detected by the first prospective evaluation were lesions that had undergone multiple surgical treatments but were then correctly identified as positive cases by the second retrospective evaluation (Figure 2). This yielded an improved diagnostic accuracy of 94.1%, with 100%-sensitivity, 66.7-specificity, 93.3%-PPV, and 100%-NPV.
The histopathological examination of the only remaining false positive case revealed the presence of lichen sclerosus et atrophicus (LSA) – a known comorbidity in this patient (a 72-year-old man with concomitant EMPD and LSA) – which was identified by the pathologist as the presence of a lymphocytic infiltrate and vacuolized keratinocytes within an edematous epidermis (spongiosis), which – albeit their smaller size – was mistaken for Paget’s cell infiltration in both LC-OCT assessment settings (Figure 3).
4. Discussion
The study at hand delves into the diagnostic challenges of EMPD, a condition known for its elusive presentation and the critical need for timely and accurate detection to avoid disease progression [35]. As EMPD often mimics other dermatological conditions in its initial stages, an early differential diagnosis is crucial to ensure appropriate treatment, to prevent disease progression, and to avoid greater morbidity due to extensive surgery [36].
To date, there is considerable variability in non-invasive diagnostic techniques applied to EMPD [11] as well as a lack of standardized interpretation criteria. The findings from our study with LC-OCT offer promising insights into how this non-invasive technique can improve accuracy and reduce the need for biopsies.
In this preliminary diagnostic study, we assessed the accuracy of LC-OCT for detecting persistence (i.e., continued existence of the disease after diagnosis) or recurrence (i.e., relapse after a period of absence or remission) of EMPD in a cohort of patients with histopathologically-proven EMPD. Two separate phases of data collection were conducted, initially by an LC-OCT expert with limited training in EMPD detection, who evaluated images and videos at the patient’s bedside (prospective setting); then by an independent LC-OCT expert with sufficient training in EMPD detection, who evaluated the same material and had the time to do so properly (retrospective setting).
The retrospective evaluation, performed by definition under ideal and optimal conditions, produced a remarkable diagnostic accuracy of 94.1%, with 100% sensitivity and 66.7% specificity. Of note, the suboptimal specificity might be explained by the limited amount of true negative cases (only 3 out of 17) and by the fact that the only false positive was detected in a site concomitantly affected by LSA, in which one of the histopathological hallmarks of the disease – the inflammatory infiltrate – was mistaken for Paget’s cells on LC-OCT. To date, only 2 cases of clinically diagnosed LSA with biopsy-proven EMPD have been reported in the literature [37,38] and no case of concomitant diseases proven by biopsy has been described yet, which highlights the exceptional and consequently unusual nature of our case, which undoubtedly lead us to misinterpretation.
Non-invasive imaging techniques have been previously employed to differentiate EMPD from LSA. Dermoscopy of EMPD (milky-red areas and polymorphous vessels) and LSA [inverse follicular plugs and reduced vessel density (so called “desertification”), not present in our case] were directly compared in one study [10]. Under RCM, LSA is characterized by the presence of dermal fibrosis corresponding to thick fiber-like structures together with typical honeycomb pattern, dilated and irregular dermal papillae and bright cells in the dermis [39]. Under c-OCT, LSA features sclerotic changes defined by disorganized extracellular matrix, increased blood flow and epidermal thinning [40]. Under HF-US, LSA is visualized as an hypoechoic band in the dermis [41]. None of the above-mentioned features were present in our case, neither at the dermoscopic or LC-OCT, thus confirming this particularly difficult presentation. Although there are many illustrations and descriptions of non-invasive imaging modalities for EMPD and LSA, there is still insufficient data from large studies demonstrating their ability to clearly differentiate EMPD from LSA, nor any data describing LSA in LC-OCT. To date, the only documented cases of LC-OCT related to LSA concern 5 cases of lichen planus (both belonging to interface dermatitis), which feature thickened stratum corneum and epidermis, hypergranulosis and inflammatory bright cells at the level of dermal-epidermal junction [42]. An explanation for the misdiagnosis of LSA as EMPD in LC-OCT could reside into 2 particular histopathological features of LSA [43]. These features involved in our case are a slight vacuolar alteration of keratinocytes and a focal lymphocytes exocytosis with spongiosis of the epidermis [43]: although smaller in diameter, these features resemble the dark epidermal structures corresponding to single PCs under LC-OCT examination, which prompted both the prospective and the retrospective observer to misdiagnose this very difficult case.
In a previous diagnostic study with RCM [19] carried out on a population with a more balanced distribution (22 sites, of which 12 true positives and 10 true negatives), the authors found a 100% specificity but none of their negative cases had concomitant inflammatory diseases and were, therefore, putatively less likely to be misinterpreted as false positive cases. Conversely, they only found a 75% sensitivity, as 3 false negative cases were identified on the lesion margins, deemed difficult locations as close to recent biopsies and due to hypothetical lower density of PCs. This comparison highlights the unique strengths and limitations of different imaging techniques, underscoring the importance of selecting the appropriate method based on the specific clinical scenario and patient needs. A possible explanation of the different sensitivity (i.e., ability to find the disease) between RCM in the study of Yélamos et al. and LC-OCT in our pilot study might reside in the ability of LC-OCT to ensure the comprehensive coverage of the examined area facilitated by its integrated dermoscopic camera and enabling to precisely select doubtful location for histopathological examination. This specific ability has already demonstrated remarkable efficacy in the field of oncology for basal cell carcinoma subtyping, as previously reported by Cappilli et al. [44].
Interestingly, our results confirm the need of good conditions for image interpretation as well as of a learning curve for the use of LC-OCT. Indeed, all diagnostic parameters improved from the preliminary prospective evaluation, performed by an operator considered poorly trained at that time and during the rush of a conventional consultation, to the more mature retrospective assessment, performed under ideal conditions. Of note, all 4 false negative cases of the first prospective evaluation (then correctly identified as positive cases by the second retrospective evaluation) had previously received multiple surgeries and were, therefore, more difficult to interpret during the consultation due to the conspicuous presence of scar tissue mirroring what was found challenging in Yélamos et al.’ study [19]. The challenges associated with interpreting post-surgical changes emphasize the need for highly skilled operators who can discern subtle differences between disease recurrence and post-treatment changes. Possibly, the better conditions of the retrospective evaluation (better training and more time) allowed the correct interpretation of these difficult cases but also represent the main limitation of this study, as all diagnoses were performed by a single skin imaging expert without any concern about the time employed to do so.
The evident post-training improvement in diagnostic precision reinforces the role of LC-OCT as a powerful tool in the dermatological arsenal. The adoption of advanced imaging technologies such as LC-OCT in clinical settings not only enhances diagnostic accuracy but also appreciably improves the patient experience by reducing the need for invasive procedures. Indeed, the 100% sensitivity found in this study underscores the ability of LC-OCT to have at the same time good cellular resolution (thanks to the high numeric aperture of its microscope objective) and good lesion coverage (thanks to its coupling with an integrated dermoscopic camera), which potentially renders it a new, important candidate for the diagnosis and management of EMPD. Additionally, the integration of LC-OCT into clinical practice could potentially lead to earlier detection and treatment of EMPD, which is critical for improving patient outcomes. Also, our data suggest that thorough training is imperative for the effective use of LC-OCT for EMPD, and it may be beneficial for future studies to establish standardized practice and examination protocols to maximize diagnostic accuracy for EMPD during real-life consultation settings. In particular, the possibility of underlying additional diseases or sampling bias needs a cautious approach in interpreting LC-OCT findings. Proper training and standardized protocols are essential to ensure that LC-OCT is used effectively and consistently across different clinical settings. Future larger studies including more numerous and better distributed populations are needed to confirm these considerations.
Author Contributions
Conceptualization, G. D. and M.S.; methodology, G.D.; writing—original draft preparation, G.D. and M.S.; writing—review and editing, G. D., M.S.; supervision, M.S. and V.D.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of Erasme Hospital, Université Libre de Bruxelles (ULB) (protocol no. B2016/001, approved 24/11/2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study and written informed consent has been obtained from patients to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to privacy, legal and ethical reasons.
Acknowledgments
The Non-Invasive Skin Imaging Research Team of Hôpital Erasme, Université Libre de Bruxelles (Brussels, Belgium) would like to acknowledge the support of the Fonds Erasme (www.fondserasme.org)
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Crocker HR Paget’s Disease Affecting the Scrotum and the Penis. . Trans Pathol Soc 1888, 40, 187–191.
- Morris, C.R.; Hurst, E.A. Extramammary Paget Disease: A Review of the Literature—Part I: History, Epidemiology, Pathogenesis, Presentation, Histopathology, and Diagnostic Work-up. Dermatol. Surg. 2020, 46, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, J.; Flanagan, A.M. Mammary and extramammary Paget’s disease. J. Clin. Pathol. 2000, 53, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Kanitakis, J. Mammary and extramammary Paget’s disease. J. Eur. Acad. Dermatol. Venereol. 2007, 21, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Wagner, G.; Sachse, M.M. Extramammary Paget disease – clinical appearance, pathogenesis, management. JDDG: J. der Dtsch. Dermatol. Ges. 2011, 9, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Dinnes, J.; Deeks, J.J.; Chuchu, N.; di Ruffano, L.F.; Matin, R.N.; Thomson, D.R.; Wong, K.Y.; Aldridge, R.B.; Abbott, R.; Fawzy, M.; et al. Dermoscopy, with and without visual inspection, for diagnosing melanoma in adults. Cochrane Database Syst. Rev. 2018, 2018, CD011902. [Google Scholar] [CrossRef] [PubMed]
- Dinnes, J.; Deeks, J.J.; Chuchu, N.; Matin, R.N.; Wong, K.Y.; Aldridge, R.B.; Durack, A.; Gulati, A.; Chan, S.A.; Johnston, L.; et al. Visual inspection and dermoscopy, alone or in combination, for diagnosing keratinocyte skin cancers in adults. Cochrane Database Syst. Rev. 2018, 2018, CD011901. [Google Scholar] [CrossRef]
- Adya, K.A. Dermoscopy: An Overview of the Principles, Procedure and Practice. In Dermoscopy - Histopathology Correlation; Springer Singapore: Singapore, 2021; pp. 1–13. [Google Scholar]
- Rosendahl, C.; Tschandl, P.; Cameron, A.; Kittler, H. Diagnostic accuracy of dermatoscopy for melanocytic and nonmelanocytic pigmented lesions. J. Am. Acad. Dermatol. 2011, 64, 1068–1073. [Google Scholar] [CrossRef] [PubMed]
- Bazzacco, G.; Zalaudek, I.; Errichetti, E. Dermoscopy to differentiate clinically similar inflammatory and neoplastic skin lesions. Ital. J. Dermatol. Venereol. 2024, 159, 135–145. [Google Scholar] [CrossRef]
- Bayan, C.Y.; Khanna, T.; Rotemberg, V.; Samie, F.H.; Zeitouni, N.C. A review of non-invasive imaging in extramammary Paget’s disease. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1862–1873. [Google Scholar] [CrossRef]
- Hirokawa, D.; Lee, J.B. Dermatoscopy: An overview of subsurface morphology. Clin. Dermatol. 2011, 29, 557–565. [Google Scholar] [CrossRef]
- Mun, J.-H.; Park, S.-M.; Kim, G.-W.; Song, M.; Kim, H.-S.; Ko, H.-C.; Kim, B.-S.; Kim, M.-B. Clinical and dermoscopic characteristics of extramammary Paget disease: a study of 35 cases. Br. J. Dermatol. 2015, 174, 1104–1107. [Google Scholar] [CrossRef]
- Que, S.K.T.; Fraga-Braghiroli, N.; Grant-Kels, J.M.; Rabinovitz, H.S.; Oliviero, M.; Scope, A. Through the looking glass: Basics and principles of reflectance confocal microscopy. J. Am. Acad. Dermatol. 2015, 73, 276–284. [Google Scholar] [CrossRef]
- Guitera, P.; Scolyer, R.; Gill, M.; Akita, H.; Arima, M.; Yokoyama, Y.; Matsunaga, K.; Longo, C.; Bassoli, S.; Bencini, P.; et al. Reflectance confocal microscopy for diagnosis of mammary and extramammary Paget’s disease. J. Eur. Acad. Dermatol. Venereol. 2012, 27, e24–e29. [Google Scholar] [CrossRef]
- Guida, S.; Longhitano, S.; Ardigò, M.; Pampena, R.; Ciardo, S.; Bigi, L.; Mandel, V.D.; Vaschieri, C.; Manfredini, M.; Pezzini, C.; et al. Dermoscopy, confocal microscopy and optical coherence tomography features of main inflammatory and autoimmune skin diseases: A systematic review. Australas. J. Dermatol. 2021, 63, 15–26. [Google Scholar] [CrossRef]
- Pan, Z.-Y.; Liang, J.; Zhang, Q.-A.; Lin, J.-R.; Zheng, Z.-Z. In vivo reflectance confocal microscopy of extramammary Paget disease: Diagnostic evaluation and surgical management. J. Am. Acad. Dermatol. 2012, 66, e47–e53. [Google Scholar] [CrossRef]
- Tan, L.; Huang, J.; Zhang, Y.; Zeng, L.; Tong, X.; Gao, L.; Zeng, J. Evaluation of in vivo reflectance confocal microscopy in the diagnosis of extramammary Paget’s disease. Microsc. Res. Tech. 2021, 85, 283–289. [Google Scholar] [CrossRef]
- Yélamos, O.; Hibler, B.P.; Cordova, M.; Hollmann, T.J.; Kose, K.; Marchetti, M.A.; Myskowski, P.L.; Pulitzer, M.P.; Rajadhyaksha, M.; Rossi, A.M.; et al. Handheld Reflectance Confocal Microscopy for the Detection of Recurrent Extramammary Paget Disease. JAMA Dermatol. 2017, 153, 689–693. [Google Scholar] [CrossRef]
- Shahriari, N.; Grant-Kels, J.M.; Rabinovitz, H.; Oliviero, M.; Scope, A. Reflectance confocal microscopy. J. Am. Acad. Dermatol. 2020, 84, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Welzel, J. Optical coherence tomography in dermatology: a review. Ski. Res. Technol. 2001, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Escobar, P.F.; Belinson, J.L.; White, A.; Shakhova, N.M.; Feldchtein, F.I.; Kareta, M.V.; Gladkova, N.D. Diagnostic efficacy of optical coherence tomography in the management of preinvasive and invasive cancer of uterine cervix and vulva. Int. J. Gynecol. Cancer 2004, 14, 470–474. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, Y.; Wu, Y. In vivo characterization of extramammary Paget’s disease by ultra-high cellular resolution optical coherence tomography. Ski. Res. Technol. 2020, 27, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Bard, R.L. High-Frequency Ultrasound Examination in the Diagnosis of Skin Cancer. Dermatol. Clin. 2017, 35, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Guo, L.; Yan, J.; Wang, Q.; Li, X.; Li, M.; Zhu, R.; Yang, W.; Xu, H. Ultrasound Biomicroscopy and High-Frequency Ultrasound for Evaluating Extramammary Paget Disease With Pathologic Correlation. J. Ultrasound Med. 2019, 38, 3229–3237. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Gong, X.; Wang, Q.; Wang, L.; Xu, H.; Guo, L. High-Frequency Ultrasound for Evaluation of the Pathological Invasion Level of Extramammary Paget Disease. J. Ultrasound Med. 2021, 41, 389–400. [Google Scholar] [CrossRef] [PubMed]
- Dubois, A.; Levecq, O.; Azimani, H.; Siret, D.; Barut, A.; Suppa, M.; del Marmol, V.; Malvehy, J.; Cinotti, E.; Rubegni, P.; et al. Line-field confocal optical coherence tomography for high-resolution noninvasive imaging of skin tumors. J. Biomed. Opt. 2018, 23, 106007–9. [Google Scholar] [CrossRef] [PubMed]
- Suppa, M.; Palmisano, G.; Tognetti, L.; Lenoir, C.; Cappilli, S.; Fontaine, M.; Cano, C.O.; Diet, G.; Perez-Anker, J.; Schuh, S.; et al. Line-field confocal optical coherence tomography in melanocytic and non-melanocytic skin tumors. Ital. J. Dermatol. Venereol. 2023, 158, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Latriglia, F.; Ogien, J.; Tavernier, C.; Fischman, S.; Suppa, M.; Perrot, J.-L.; Dubois, A. Line-Field Confocal Optical Coherence Tomography (LC-OCT) for Skin Imaging in Dermatology. Life 2023, 13, 2268. [Google Scholar] [CrossRef] [PubMed]
- Gust, C.; Schuh, S.; Welzel, J.; Daxenberger, F.; Hartmann, D.; French, L.E.; Ruini, C.; Sattler, E.C. Line-Field Confocal Optical Coherence Tomography Increases the Diagnostic Accuracy and Confidence for Basal Cell Carcinoma in Equivocal Lesions: A Prospective Study. Cancers 2022, 14, 1082. [Google Scholar] [CrossRef]
- Cinotti, E.; Brunetti, T.; Cartocci, A.; Tognetti, L.; Suppa, M.; Malvehy, J.; Perez-Anker, J.; Puig, S.; Perrot, J.L.; Rubegni, P. Diagnostic Accuracy of Line-Field Confocal Optical Coherence Tomography for the Diagnosis of Skin Carcinomas. Diagnostics 2023, 13, 361. [Google Scholar] [CrossRef]
- Donelli, C.; Suppa, M.; Tognetti, L.; Perrot, J.L.; Calabrese, L.; Pérez-Anker, J.; Malvehy, J.; Rubegni, P.; Cinotti, E. Line-Field Confocal Optical Coherence Tomography for the Diagnosis of Skin Carcinomas: Real-Life Data over Three Years. Curr. Oncol. 2023, 30, 8853–8864. [Google Scholar] [CrossRef] [PubMed]
- Di Stefani, A.; Fionda, B.; Cappilli, S.; Tagliaferri, L.; Peris, K. Extramammary Paget disease imaged by LC-OCT and treated with radiotherapy. Int. J. Dermatol. 2023, 62, E503–E505. [Google Scholar] [CrossRef] [PubMed]
- Delpuech, A.; Battistella, M.; Tavernier, C.; El Zeinaty, P.; Lebbé, C.; Baroudjian, B. Intérêt de la line-field confocal optical coherence tomography (LC-OCT) pour le diagnostic non invasif de la maladie de Paget. Ann. Dermatol. Vénéréologie–FMC 2023, 3, A182. [Google Scholar] [CrossRef]
- Fukuda, K.; Funakoshi, T. Metastatic Extramammary Paget’s Disease: Pathogenesis and Novel Therapeutic Approach. Front. Oncol. 2018, 8, 38. [Google Scholar] [CrossRef]
- Morris, C.R.; Hurst, E.A. Extramammary Paget’s Disease: A Review of the Literature Part II: Treatment and Prognosis. Dermatol. Surg. 2020, 46, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Bansal, D.; A Bowman, C. Extramammary Paget’s disease masquerading as lichen sclerosus. Int. J. STD AIDS 2004, 15, 141–142. [Google Scholar] [CrossRef] [PubMed]
- Papoutsis, D.; Antonakou, A.; Sahu, B. Vulvar Paget’s disease presenting on the background of clinically diagnosed lichen sclerosus. Hippokratia 2018, 22, 94–94. [Google Scholar] [PubMed]
- Kantere, D.; Neittaanmäki, N.; Maltese, K.; Larkö, A.-M.W.; Tunbäck, P. Exploring reflectance confocal microscopy as a non-invasive diagnostic tool for genital lichen sclerosus. Exp. Ther. Med. 2022, 23, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Huisman, B.W.; Pagan, L.; Naafs, R.G.B.; Voorde, W.M.T.; Rissmann, R.; Piek, J.M.; Damman, J.; Juachon, M.J.M.; Osse, M.B.; der Kolk, T.N.-V.; et al. Dermatoscopy and Optical Coherence Tomography in Vulvar High-Grade Squamous Intraepithelial Lesions and Lichen Sclerosus: A Prospective Observational Trial. J. Low. Genit. Tract Dis. 2023, 27, 255–261. [Google Scholar] [CrossRef]
- Wang, Y.; Hao, J.; Liu, J. High-frequency ultrasound assessment of vulvar lichen sclerosus treated with photodynamic therapy. Photodiagnosis Photodyn. Ther. 2023, 41, 103277. [Google Scholar] [CrossRef]
- Verzì, A.; Broggi, G.; Micali, G.; Sorci, F.; Caltabiano, R.; Lacarrubba, F. Line-field confocal optical coherence tomography of psoriasis, eczema and lichen planus: a case series with histopathological correlation. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1884–1889. [Google Scholar] [CrossRef] [PubMed]
- Regauer, S.; Liegl, B.; Reich, O. Early vulvar lichen sclerosus: a histopathological challenge. Histopathology 2005, 47, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Cappilli, S.; Dejonckheere, G.; Hajjar, N.; Cinotti, E.; Tognetti, L.; Perez-Anker, J.; Rubegni, P.; Puig, S.; Malvehy, J.; Perrot, J.L.; et al. Line-field confocal optical coherence tomography: a case on the importance of full-lesion examination for basal cell carcinoma. Int. J. Dermatol. 2022, 61, E248–E250. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Clinical images, line-field confocal optical coherence tomography (LC-OCT) and histopathology of extramammary Paget disease (EMPD) in a 38-year-old woman correctly identified both in the prospective and retrospective evaluations: (a) pinkish plaque of the peri-anal area previously treated with imiquimod; (b) circular markers indicate sites of scouting biopsies; (c, d, e) horizontal LC-OCT frames reveal solitary Paget’s cells (PCs) characterized by a dark cytoplasm and a slightly bright nucleus (red arrows) and larger than neighboring keratinocytes, as well as glandular structures representing clusters of PCs (yellow asterisks); (f) histopathology (periodic acid Schiff) shows PCs across the epidermis, structured as single (red arrows) or nested cells (yellow asterisks).
Figure 1.
Clinical images, line-field confocal optical coherence tomography (LC-OCT) and histopathology of extramammary Paget disease (EMPD) in a 38-year-old woman correctly identified both in the prospective and retrospective evaluations: (a) pinkish plaque of the peri-anal area previously treated with imiquimod; (b) circular markers indicate sites of scouting biopsies; (c, d, e) horizontal LC-OCT frames reveal solitary Paget’s cells (PCs) characterized by a dark cytoplasm and a slightly bright nucleus (red arrows) and larger than neighboring keratinocytes, as well as glandular structures representing clusters of PCs (yellow asterisks); (f) histopathology (periodic acid Schiff) shows PCs across the epidermis, structured as single (red arrows) or nested cells (yellow asterisks).
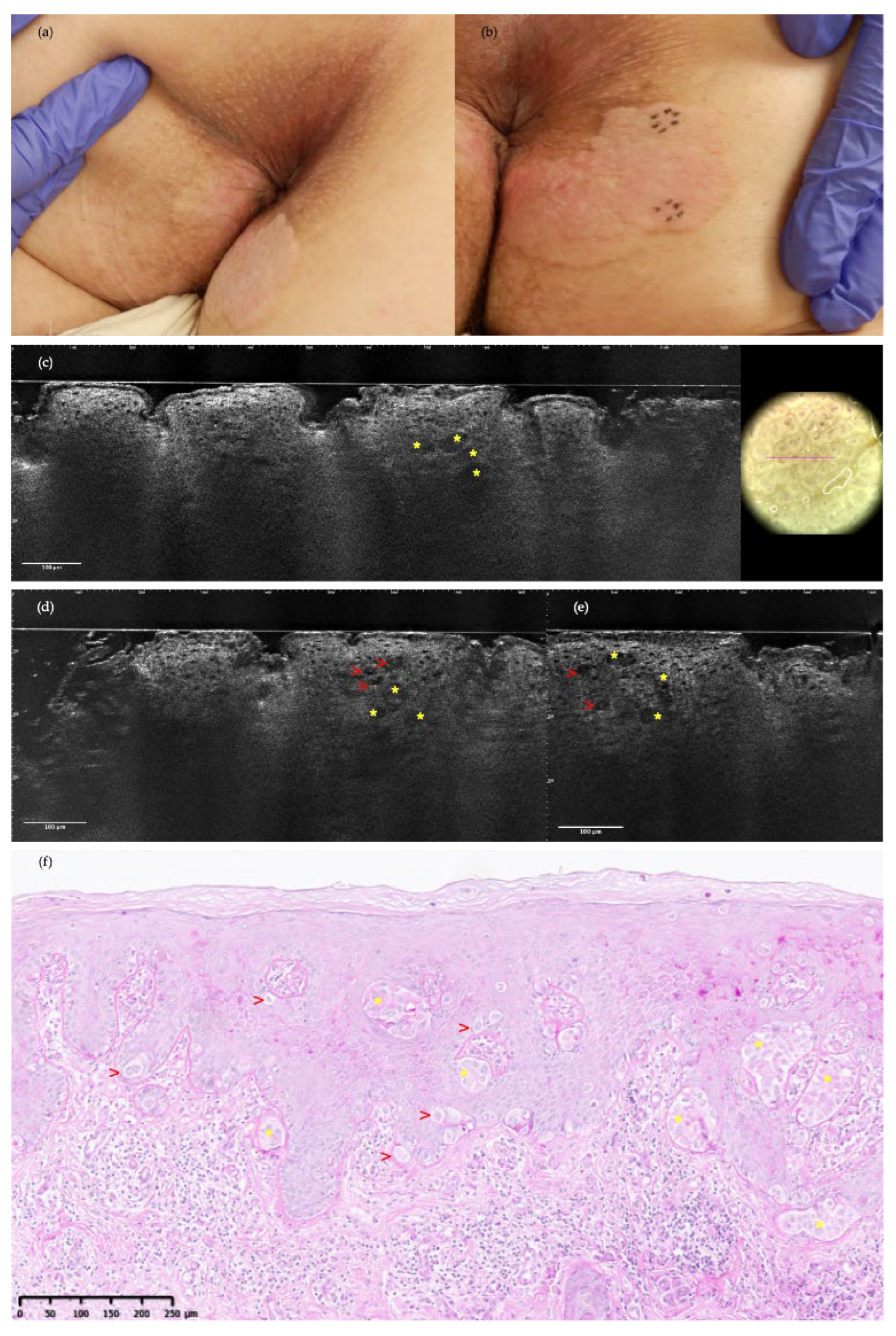
Figure 2.
Clinical images, LC-OCT and histopathology of pubic EMPD in a 71-year-old man: (a, b) recurrent erythematous patches in a surgical scar with unclear margins from recent surgery; (c) dermoscopy presenting red-pink structureless areas and polymorphous vessels; (d) prospective LC-OCT examination was interpreted as negative, although, after reevaluation (retrospective settings), few solitary PC were identified (red arrows) as prominent dark structures containing either bright centers or dark holes related to nucleus; (e, f) histopathology specimens (hematoxylin and eosin) match with LC-OCT frames, showing PCs exclusively organized as pale isolated cells predominantly present at the dermal-epidermal junction level (red arrows).
Figure 2.
Clinical images, LC-OCT and histopathology of pubic EMPD in a 71-year-old man: (a, b) recurrent erythematous patches in a surgical scar with unclear margins from recent surgery; (c) dermoscopy presenting red-pink structureless areas and polymorphous vessels; (d) prospective LC-OCT examination was interpreted as negative, although, after reevaluation (retrospective settings), few solitary PC were identified (red arrows) as prominent dark structures containing either bright centers or dark holes related to nucleus; (e, f) histopathology specimens (hematoxylin and eosin) match with LC-OCT frames, showing PCs exclusively organized as pale isolated cells predominantly present at the dermal-epidermal junction level (red arrows).
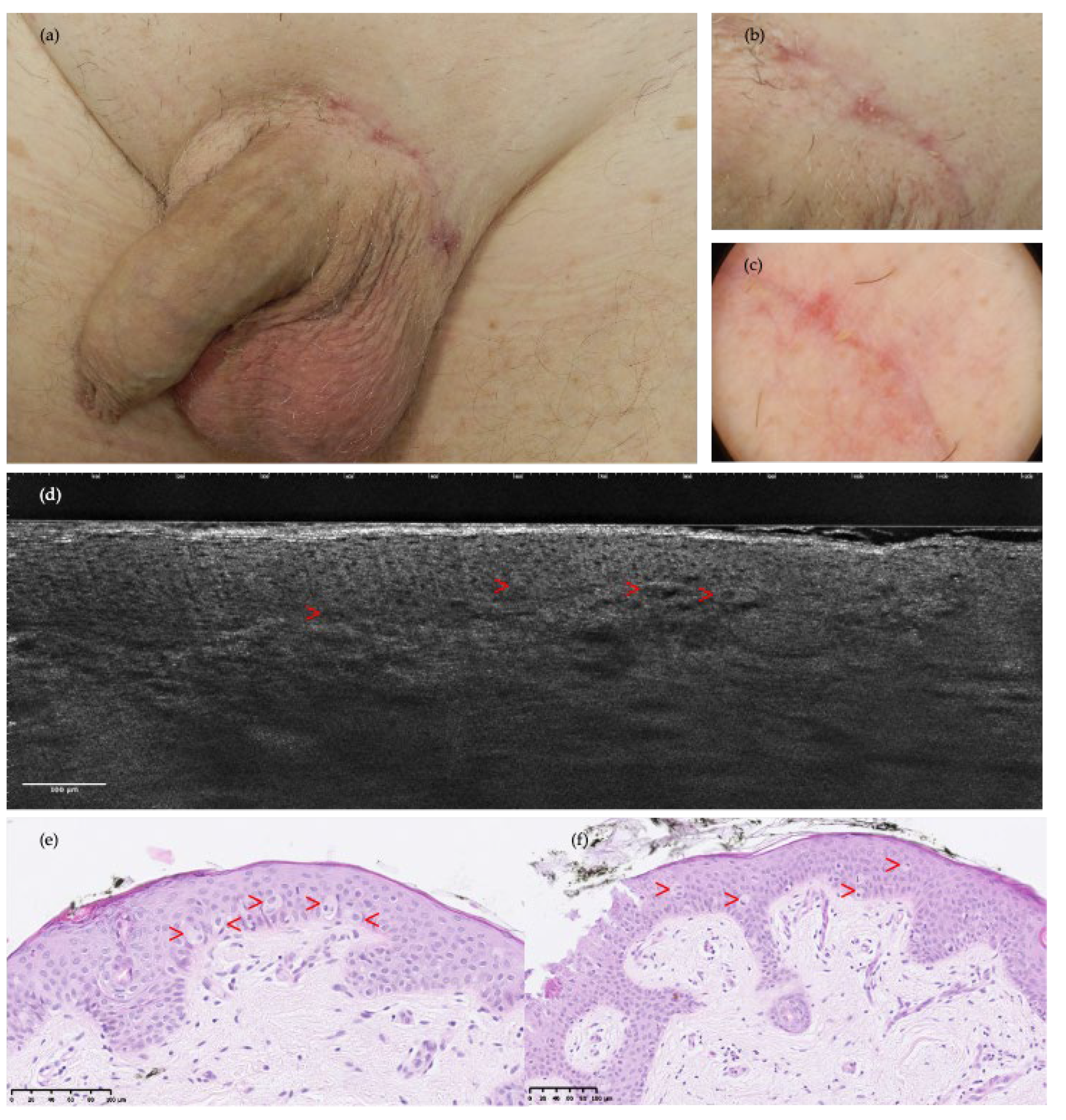
Figure 3.
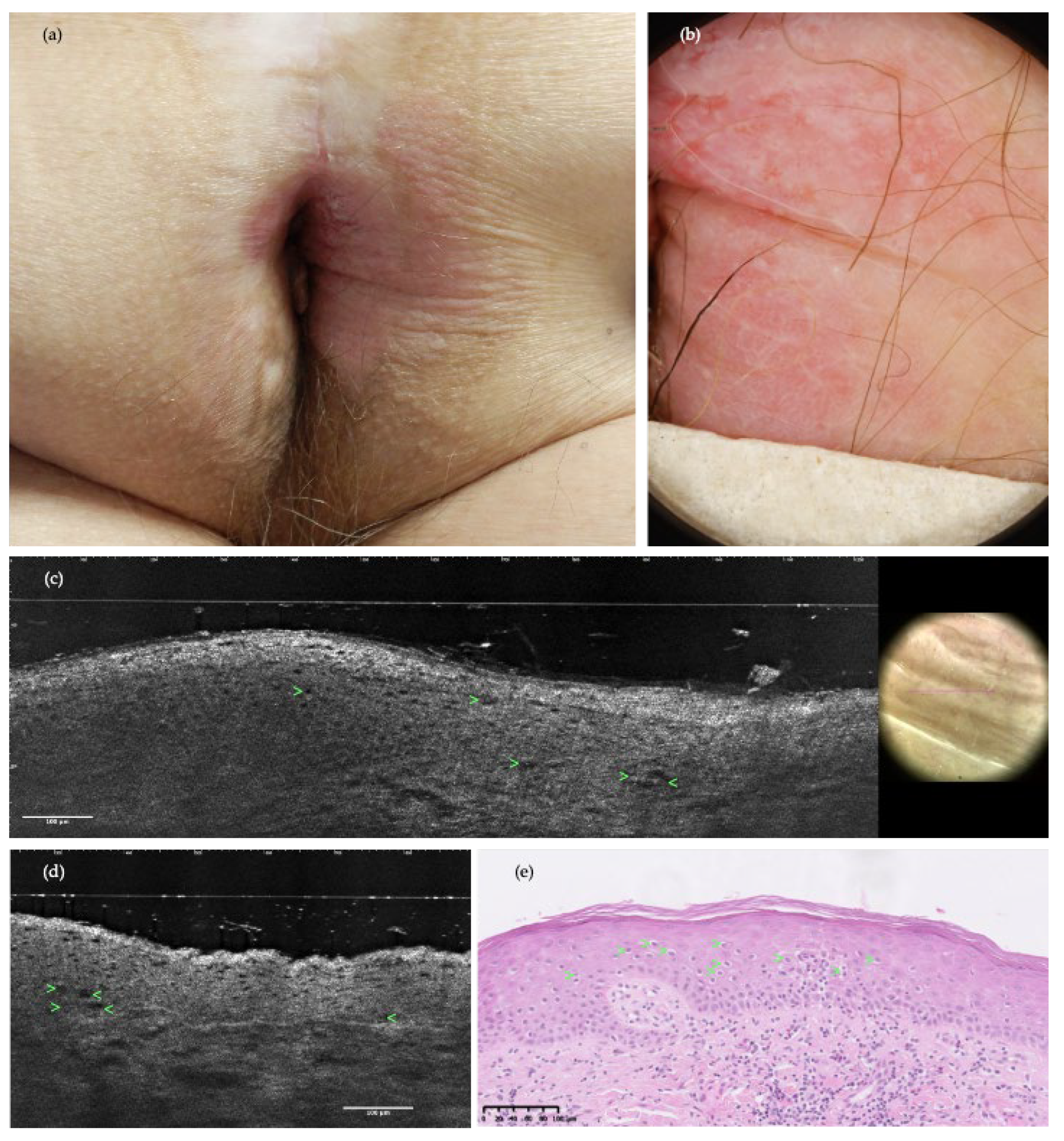
Clinical image, dermoscopy, LC-OCT and histopathology of the perianal area in a 72-year-old man with concomitant EMPD and lichen sclerosus atrophicus (LSA): (a) poorly delineated, atrophic, white and erythematous plaque; (b) dermoscopy exhibiting milky-red structureless areas, dotted and polymorphic vessels; (c, d) LC-OCT examination in both prospective and retrospective settings was misinterpreted as positive for EMPD recurrence, while histopathology pointed towards the diagnosis of LSA instead. Misinterpretation of EMPD was due to the visualization of vacuolized and enlarged keratinocytes (green arrows) looking similar to solitary PCs as they presented similar, but smaller central dark holes; (e) the H&E stained histopathological section shows vacuolized and enlarged keratinocytes (green arrows), which are indeed distinct from PCs as they are smaller in size.
Figure 3.
Clinical image, dermoscopy, LC-OCT and histopathology of the perianal area in a 72-year-old man with concomitant EMPD and lichen sclerosus atrophicus (LSA): (a) poorly delineated, atrophic, white and erythematous plaque; (b) dermoscopy exhibiting milky-red structureless areas, dotted and polymorphic vessels; (c, d) LC-OCT examination in both prospective and retrospective settings was misinterpreted as positive for EMPD recurrence, while histopathology pointed towards the diagnosis of LSA instead. Misinterpretation of EMPD was due to the visualization of vacuolized and enlarged keratinocytes (green arrows) looking similar to solitary PCs as they presented similar, but smaller central dark holes; (e) the H&E stained histopathological section shows vacuolized and enlarged keratinocytes (green arrows), which are indeed distinct from PCs as they are smaller in size.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



