
Submitted:
10 July 2024
Posted:
11 July 2024
You are already at the latest version
Abstract
Gastrointestinal bleeding (GIB) after heart transplantation (HT) remains a significant clinical issue. The study aimed to explore its incidence, trends, outcomes and clinical predictors of GIB in HT patients. Adult patients who underwent HT between 2015 and 2021 at Union Hospital were recruited and divided into two groups based on the presence or absence of postoperative GIB. Primary outcomes were evaluated by follow-up. Independent predictors of GIB after HT were identified by logistic regression analysis. A nomogram prediction model was constructed according to these independent variables, and the accuracy of the model was assessed using the receiver operating characteristic (ROC) curve and the calibration curve. Among 461 patients, 40 (8.7%) developed GIB post-HT. HT patients with postoperative GIB exhibited higher in-hospital, 30-day, 90-day and 1-year mortality (all P < 0.05). Multivariate analysis identified age, preoperative warfarin, postoperative continuous renal replacement therapy and postoperative nasogastric tube as independent risk factors for GIB following HT. The nomogram prediction model was performed using the 4 variables. The area under the curve (AUC) of this model was 0.852(95% CI: 0.787-0.917, P < 0.001) and the calibration curve was close to the ideal diagonal line. GIB following HT is associated with a poor clinical prognosis. The constructed nomogram, incorporating its independent risk factors, demonstrated a favorable predictive value for GIB.
Keywords:
heart transplantation
; gastrointestinal bleeding
; clinical outcomes
; risk factors
; nomogram
1. Introduction
Heart transplantation (HT) is one of the most remarkable achievements in modern medicine and has become a standard treatment option for patients with end-stage heart failure[1]. Over recent decades, advancements in organ donation and preservation, surgical techniques, immunosuppression and long-term graft surveillance have significantly improved the clinical outcomes of HT recipients. The median survival is now 10.7 years, with 1-year and 5-year survival rates being 82% and 69%, respectively, contributing to the greater success of HT[2,3]. However, the prolonged survival of HT recipients has also increased the risk of postoperative comorbidities such as renal dysfunction, embolism and diabetes, which seriously affect the quality of life of these patients[4,5].
Gastrointestinal bleeding (GIB) is a relatively rare complication after most cardiac surgeries (e.g., coronary artery bypass grafting, valve repair or replacement, etc.) but is associated with high mortality[6]. It is reported that postoperative GIB rates in patients who underwent cardiac surgery vary from 0.07% to 1.6%, with mortality rate reaching up to 47.6%[6,7]. However, the current research indicates that continuous flow left ventricular assist device (CF-LVAD) implantation, as a bridge to HT, is significantly associated with postoperative GIB, with a high incidence of 15-40%[8]. These GIB patients often require prolonged life support and extended stays in the intensive care unit (ICU), leading to an increase in procedure burden, economic costs and resource use[9]. Additionally, HT recipients are at high risk for venous thromboembolism and atrial fibrillation, necessitating anticoagulation therapy, which further increases the bleeding risk[10]. Despite this, the contemporary incidence of postoperative GIB in HT patients and its impact on clinical outcomes remain unclear. Therefore, this study aims to investigate the incidence, trends, and predictors of GIB after HT and analyze their association with clinical outcomes, providing new evidence for risk stratification and clinical practice in these patients.
2. Materials and Methods
2.1. Patients and Study Design
This is a retrospective study approved by the Ethics Committee of Tongji College, Huazhong University of Science and Technology (No: IORG0003571). From January 2015 to December 2021, adult patients aged 18 ≥ years who admitted to Union Hospital for HT were recruited. Patients were excluded if they met any of the following criteria: 1) experienced GIB within 30 days prior to HT; 2) underwent multi-organ transplantation; 3) died during the procedure; 4) had insufficient clinical data.
2.2. Data collection, Variables Definition and Grouping
All patients included in this study underwent a comprehensive assessment and data collection including demographics, medical history, preoperative laboratory and echocardiography results, preoperative treatment, operative details and postoperative treatment. Postoperative GIB was defined as the occurrence of GIB symptoms or signs following HT, including melena, hematochezia, hematemesis, or a positive occult blood test (OB) result in specimens of feces or gastric juice[11,12]. All patients were divided into 2 groups according to the postoperative GIB (the Non-GIB group and the GIB group), and were followed up for 1 year. The primary outcomes measured were in-hospital, 30-day, 90-day and 1-year mortality.
2.3. Statistical Analysis
The data were presented as mean ± standard deviation (SD) for normally distributed continuous variables, as median and interquartile range (IQR) for non-normally distributed continuous variables and as number (n) with percentages (%) for categorical variables. Between-group comparisons of normally distributed values were performed by t test and non-normally distributed values were conducted by Mann-Whitney U test, while categorical variables were compared by Chi-squared test. Trend analysis was conducted by Cochran-Armitage test. An unadjusted Cox proportional hazards model was conducted to estimate cumulative cause-specific hazard of all-cause mortality in association with postoperative GIB after HT and the time-to-event curves was presented as a cumulative incidence function. Univariate and multivariate logistic regression analysis was used to identify independent factors for GIB (variables with a P value < 0.1 and clinical significance were selected for multivariate regression analysis), which were further output for the construction of risk prediction model as nomogram. The discriminative ability of nomogram was assessed by receiver operating characteristic (ROC) curve and the calibration curve. All statistical analysis were carried out by R.4.3.2. A two-sided P < 0.05 was considered statistically significant.
3. Results
3.1. Patients’ Characteristics
A total of 507 adult patients who underwent HT were initially recruited for the study. Exclusions were made for 3 patients with GIB within 30 days before HT, 9 patients who underwent multi-organ transplantation, 7 patients who died during the procedure and 27 patients with insufficient clinical data. Consequently, 461 adult patients were enrolled in this study (Figure 1), of which 20.6% were male, and the median age was 50 years. The underlying diagnosis of heart failure in the overall population is presented in Figure 2, with dilated cardiomyopathy (DCM) accounting for more than half of HT cases. From 2015 to 2021, the incidence of GIB after HT increased from 3.1% to 20.0% and the Cochran-Armitage test showed this trend remained unchanged (Ptrend < 0.001, Figure 3).
The baseline characteristics are shown in Table 1. Compared to the Non-GIB group, the GIB group was older (P < 0.05), and had higher activated partial thromboplastin time (APTT), international normalized ratio (INR) levels, and lower red blood cell (RBC), hemoglobin (Hb) and albumin level (all P < 0.05), but none of these indicators had clinical significance. Besides, the preoperative use of warfarin and extracorporeal membrane oxygenation (ECMO) were higher in this group (all P < 0.05). In the intraoperative and postoperative data, the GIB group had longer cardiopulmonary bypass (CPB) time, operation time and intubation time (all P < 0.05) and received more continuous renal replacement therapy (CRRT), ECMO and nasogastric tube after surgery (all P < 0.05).
3.2. Postoperative GIB and Survival in HT Patients
As shown in Table 1, the ICU and postoperative hospital stay were longer and the rates of in-hospital, 30-day, 90-day and 1-year mortality was higher in the GIB group (all P < 0.05). In addition, the mortality rate was particularly evaluated during the first 90 days post-HT. However, postoperative GIB patients who survived the initial critical months did not exhibit a significantly worse long-term prognosis (Figure 4).
3.3. Risk Factors of Postoperative GIB in HT Patients
To further explore the independent factors associated with GIB after HT, the univariate and multivariate logistic regression analysis were performed. According to the results of univariate analysis, variables with a P value < 0.1 and clinical significance were selected for multivariate regression analysis. After adjusting for a series of variable (e.g., male, cross clamp time, operation time, etc.), the age (OR: 1.04, 95% CI: 1.00-1.07, P: 0.037), preoperative warfarin (OR: 3.01, 95% CI: 1.07-8.48, P: 0.037), postoperative CRRT (OR: 6.27, 95% CI: 2.50-15.72, P < 0.001) and postoperative nasogastric tube (OR: 5.73, 95% CI: 2.10-15.66, P: 0.001) were significantly associated with postoperative GIB in patients with HT, as illustrated in Figure 5 and Table 2.
Based on the results of the multivariate analysis, a nomogram model containing 4 independent variables was constructed to predict the occurrence of GIB after HT (Figure 6). The prediction model visually emphasized age as the most critical predictor. The probability of postoperative GIB was determined by the value at a vertical line from the corresponding total points, which was the sum of the relative scores for each parameter. In addition, the predictive accuracy of this model was evaluated by the ROC curve and the calibration curve. As shown in Figure 7, the area under the curve (AUC) was 0.852 (95% CI: 0.787-0.917, P < 0.001), with a sensitivity of 80.0% and specificity of 80.5% and the calibration curve was close to the ideal diagonal line.
4. Discussion
In the current study, we enrolled 461 patients who underwent HT and sought to ascertain the incidence, trends, outcomes, and clinical predictors of postoperative GIB in these patients. The primary observations gleaned from our study are as follows: 1) 8.7% (40/461 HT patients) of the patients developed GIB postoperatively, and its incidence increased between 2015 and 2021; 2) postoperative GIB patients after HT exhibited a higher risk of in-hospital, 30-day, 90-day, 1-year mortality; 3) age, preoperative warfarin, postoperative CRRT and postoperative nasogastric tube were independent risk factors for GIB after HT. Meanwhile, a nomogram prediction model was established according to these variables and could evaluate the possibility of this complication more effectively and accurately, providing a basis for decision making in clinical practice.
In the last 50 years, HT has undergone remarkable advancements in improving the survival of patients with advanced heart failure. Nonetheless, the persistence of postoperative complications poses a formidable challenge to clinical management, as they are frequently associated with adverse clinical outcomes[13]. It is reported that GIB following cardiac surgery is relatively rare entity but carries a pronounced mortality risk[6,7]. For instance, a cohort study involving 2956 patients who underwent cardiac surgery (e.g., aortocoronary bypass grafting, valve replacement, aortic aneurysm, etc.) revealed the postoperative incidence of GIB to be 0.9%, with an in-hospital mortality rate of 35%[14]. Another research based on 3 prospectively maintained databases of 9017 cardiac surgery patients (coronary artery bypass grafting and valve procedure), reported an overall incidence of postoperative GIB was 1.01%, with duodenal ulceration identified as the predominant bleeding source, constituting 78% of cases[15]. These GIB patients had prolonged postoperative hospital stay and heightened 30-day mortality rate (8.8%) in comparison to the control group[15]. However, despite high risk of bleeding complications among HT recipients[10], the current research lack comprehensive investigations into postoperative GIB in these patients’ cohort. In our study, we retrospectively analyzed a 461 HT patients’ cohort and found 8.7% of them experienced postoperative GIB, with an incidence increasing from 3.1% in 2015 to 20.0% in 2021.
To our best knowledge, it is the first study to focus on postoperative GIB among HT patients. The higher incidence of GIB observed in patients with HT compared to other forms of cardiac surgery may be attributed to several factors intrinsic to the transplantation procedure and the perioperative management of these patients, including the pre-existing comorbidities, immunosuppressive therapy[16], anticoagulant and antiplatelet therapy[17], altered hemodynamics[18] and reperfusion injury[19]. Additionally, we also observed that these postoperative GIB patients had a poorer clinical prognosis including a higher in-hospital (15.0%), 30-day (27.5%), 90-day (50.0%) and 1-year (52.5%) mortality and a longer postoperative hospital stay during the follow-up, which were consistent with previous reports of GIB following other cardiac surgery[6]. The patients who survived beyond this initial phase did not show a significantly worse long-term prognosis compared to those without GIB, suggesting that while GIB presents a substantial early risk, its impact may diminish over time if patients overcome the initial critical period. Overall, the above finding highlighting the importance of comprehensive risk assessment for developing GIB after HT and suggests the need for vigilant monitoring, and tailored management strategies to mitigate the risk of bleeding complications and optimize patient outcomes in the post-transplantation period.
Age emerged as a prominent independent risk factor in our study. The correlation between age and postoperative GIB has been investigated widely. Kim et al. conducted a nationwide population-based study of 1,319,807 patients with various surgery in Korea, and elucidated that a significant association between advancing age and the occurrence of postoperative GIB. Specifically, patients aged ≥ 70 years old had an around 20-fold increase in risk compared to their counterparts in their 20 years old[20]. Similarly, Hsu et al. developed a machine learning algorithm to prognosticate postoperative GIB among 159,959 individuals undergoing bariatric surgery, wherein age featured prominently as 1 of the 5 most influential predictors within the model[21]. Consistent with these findings, our study showed that age was higher in the GIB group (54.50 [47.50-58.00] vs 50.00 [39.00-57.00] years, P = 0.024) and independently associated with GIB after HT by multivariate analysis, which may be due to the high prevalence of various comorbidities in the elderly population[22].
Within a series of preoperative variables, we also observed a significant association between preoperative warfarin and postoperative GIB in HT recipients. Warfarin, as one of vitamin K antagonists (VKAs), has traditionally served as a primary oral anticoagulant for the prevention of ischemic stroke or systemic embolism[23], especially in patients with cardiac mechanical valve replacement[24]. However, its clinical utility is tempered by the propensity for hemorrhagic complications[23,25]. In our current study, we analyzed preoperative antithrombotic drugs in 2 groups of our study, and demonstrated that most of the drugs including heparin, low molecular weight heparin (LMWH), aspirin and clopidogrel were not related to GIB after HT, except for warfarin. These results suggest that for patients requiring heart transplantation after mechanical valve replacement, greater attention should be paid to their anticoagulant usage prior to the transplant procedure. For instance, patients with mechanical heart valves can be bridged with unfractionated heparin or LMWH until a therapeutic INR has been attained prior to the waiting period for the transplant procedure.
Furthermore, postoperative CRRT emerged as another important clinical predictor for postoperative GIB, which was consistent with previous studies[26,27,28]. For instance, Elizabeth Parsons et al. evaluated the outcomes of CRRT in pediatric liver transplantation recipients, revealing an elevated incidence of GIB in patients necessitating CRRT, but the results need further validation through larger-scale studies[27]. Similarly, both Granholm et al. and Asleh et al. confirmed the association between CRRT utilization and heightened GIB risk in patients with ICU or CF-LVAD implantation, respectively[26,28]. Since most patients undergoing CRRT are complicated with preexisting renal disease or acute renal failure, they often experience severe systemic congestion, which, in turn, increases venous pressure in the mesenteric circulation and leads to elevated shear stress and higher risk of GIB[29]. Moreover, the concomitant use of anticoagulants during CRRT further amplifies the risk of bleeding[30]. Thus, postoperative CRRT in HT patients should be comprehensively evaluated and individualized.
Interestingly, our analysis revealed that postoperative nasogastric tube significantly increased the risk of GIB following HT. Nasogastric tube is a common procedure for stomach decompression and administration of drugs and nutrients[31]. It is often used postoperatively to manage feeding intolerance, nausea, and vomiting after cardiac surgery, serving as a standard measure to minimize gastric symptoms and alleviate gastric distension[32,33,34].
Recently, recent debates have questioned the necessity and efficacy of postoperative gastrointestinal tubes and highlighted the potential complications they may cause. Some researchers reported that postoperative gastrointestinal tube use was associated with the incidence of respiratory complications, gastrointestinal complications, and postoperative pain and discomfort[35,36,37,38]. Herein, our study is the first to demonstrate that postoperative nasogastric tube increases the risk of GIB following HT, indicating that more mechanical injury, pressure and irritation may occurred in gastrointestinal tract by gastrointestinal tube insertion for patients after HT, leading to erosions, ulcerations, and ultimately bleeding. This finding also suggests the need for clinicians to exercise greater caution when using gastrointestinal tubes in HT patients and to monitor for signs of GIB closely in those with indwelling tubes.
Notably, several intraoperative indicators including cardiopulmonary bypass time (CPB) time, cross clamp time and operation time, have been reported as risk factors for gastrointestinal complications[12], yet evidence of their association with postoperative GIB in HT patients remains inconclusive. Previous studies suggested that prolonged CPB and aortic cross-clamp time may exert adverse effects on abdominal perfusion, and splanchnic perfusion during CPB procedure, leading to inadequate metabolic supply, thereby exacerbating gastrointestinal complications[12,39]. However, most of the evidence primarily focuses on intestinal ischemic injury rather than specifically on GIB. In our study, the univariate analyses revealed the CPB time, aortic cross-clamp time and operation time were significant, but after adjusting for other clinical variables, their significance were diminished, suggesting that these intraoperative variables may not independently predispose individuals to GIB.
Several limitations should be considered in the current study. First of all, due to the retrospective study design, selection bias and some residual confounders cannot be ruled out despite multivariate analysis being used for adjustment for relative variables. Second, there is a lack of assessment of the severity and cause of postoperative GIB in HT patients, which may also impact the research results. Third, data analysis is based on a single center, so that the external validity of our findings should be further evaluated. However, our findings have important implications for the management of HT patients. Recognizing high-risk patients with HT through our predictive model allows for targeted interventions and closer monitoring, potentially mitigating the incidence and severity of GIB. For instance, optimizing anticoagulation therapy and closely monitoring coagulation parameters preoperatively could reduce the risk of postoperative GIB after HT. Additionally, minimizing CRRT time and ensuring vigilant postoperative care could further improve outcomes for these patients.
5. Conclusions
In summary, our study demonstrated that GIB is a significant complication following HT, associated with increased mortality and morbidity, particularly in the early postoperative period. Our nomogram predictive model incorporating its independent risk factors including age, preoperative warfarin, postoperative CRRT and postoperative nasogastric tube, showed a favorable predictive value.
Author Contributions
Conceptualization, N.D. and J.S.; methodology, W.L.; software, C.Z.; validation, X.Z., Q.X. and K.W.; formal analysis, W.L. and C.Z.; writing—original draft preparation, W.L. and C.Z.; writing—review and editing, X.Z., Q.X., K.W. and R.L.; supervision, N.D. and J.S.; project administration, N.D. and J.S. All authors have read and agreed to the published version of the manuscript.
Funding
The study was funded by National Key Research and Development Program of China (No: 2023YFC2706205).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Tongji College, Huazhong University of Science and Technology (protocol number IORG0003571, dated 10 December 2014). The need for written informed consent was waived given the retrospective nature of the study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original data in the study are available on request to the corresponding author.
Acknowledgments
We would like to thank Mingjie Chen for statistical analysis.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Jou, S.; Mendez, S.R.; Feinman, J.; Mitrani, L.R.; Fuster, V.; Mangiola, M.; Moazami, N.; Gidea, C. Heart transplantation: advances in expanding the donor pool and xenotransplantation. Nat. Rev. Cardiol. 2024, 21, 25–36. [CrossRef]
- Asleh, R., Alnsasra, H., Villavicencio, M.A., Daly, R.C., Kushwaha, S.S. Cardiac Transplantation: Physiology and Natural History of the Transplanted Heart. Comprehensive Physiology. 2023;13(3):4719-65.
- Shoji, S., Kuno, T., Kohsaka, S., Amiya, E., Asleh, R., Alvarez, P., Kampaktsis, P., Staffa, S.J., Zurakowski, D., Doulamis, I., Briasoulis, A. Incidence and long-term outcome of heart transplantation patients who develop postoperative renal failure requiring dialysis. The Journal of heart and lung transplantation : the official publication of the International Society for Heart Transplantation. 2022;41(3):356-64.
- Kainuma, A.; Ning, Y.; Kurlansky, P.A.; Wang, A.S.; Latif, F.; Farr, M.A.; Sayer, G.T.; Uriel, N.; Takayama, H.; Naka, Y.; et al. Deep vein thrombosis and pulmonary embolism after heart transplantation. Clin. Transplant. 2022, 36, e14705. [CrossRef]
- Vest, A.R.M.; Cherikh, W.S.; Noreen, S.M.; Stehlik, J.; Khush, K.K.M. New-onset Diabetes Mellitus After Adult Heart Transplantation and the Risk of Renal Dysfunction or Mortality. Transplantation 2022, 106, 178–187. [CrossRef]
- Schwarzova, K.; Damle, S.; Sellke, F.W.; Robich, M.P. Gastrointestinal complications after cardiac surgery. Trauma Surg. Acute Care Open 2024, 9, e001324. [CrossRef]
- Fan, H.; Zheng, Z.; Feng, W.; Wang, W.; Song, Y.; Lin, Y.; Hu, S. Risk factors and prevention of upper gastrointestinal hemorrhage after a coronary artery bypass grafting operation. Surg. Today 2010, 40, 931–935. [CrossRef]
- Converse, M.P.; Sobhanian, M.; Taber, D.J.; Houston, B.A.; Meadows, H.B.; Uber, W.E. Effect of Angiotensin II Inhibitors on Gastrointestinal Bleeding in Patients With Left Ventricular Assist Devices. Circ. 2019, 73, 1769–1778. [CrossRef]
- Berg, D., Lebovics, E., Kai, M., Spielvogel, D. The Predicament of Gastrointestinal Bleeding in Patients With a Continuous-Flow Left Ventricular Assist Device: Pathophysiology, Evaluation, and Management. Cardiology in review. 2019;27(5):222-9.
- Henricksen, E.J., Tremblay-Gravel, M., Moayedi, Y., Yang, W., Lee, R., Ross, H.J., Hiesinger, W., Teuteberg, J.J., Khush, K.K. Use of direct oral anticoagulants after heart transplantation. The Journal of heart and lung transplantation : the official publication of the International Society for Heart Transplantation. 2020;39(4):399-401.
- Patel, S.R.; Oh, K.T.; Ogriki, T.; Sims, D.; Shin, J.J.; Madan, S.; Saeed, O.; Goldstein, D.J.; Jorde, U.P. Cessation of Continuous Flow Left Ventricular Assist Device–Related Gastrointestinal Bleeding After Heart Transplantation. Asaio J. 2018, 64, 191–195. [CrossRef]
- Li, Z.-Q.; Zhang, W.; Guo, Z.; Du, X.-W.; Wang, W. Risk factors of gastrointestinal bleeding after cardiopulmonary bypass in children: a retrospective study. Front. Cardiovasc. Med. 2023, 10, 1224872. [CrossRef]
- Bhagra, S.K.; Pettit, S.; Parameshwar, J. Cardiac transplantation: indications, eligibility and current outcomes. Heart 2019, 105, 252–260. [CrossRef]
- Halm, U., Halm, F., Thein, D., Mohr, F.W., Mössner, J. Helicobacter pylori infection: a risk factor for upper gastrointestinal bleeding after cardiac surgery? Critical care medicine. 2000;28(1):110-3.
- Krawiec, F.; Maitland, A.; Duan, Q.; Faris, P.; Belletrutti, P.J.; Kent, W.D. Duodenal ulcers are a major cause of gastrointestinal bleeding after cardiac surgery. J. Thorac. Cardiovasc. Surg. 2017, 154, 181–188. [CrossRef]
- Briasoulis, A.; Inampudi, C.; Pala, M.; Asleh, R.; Alvarez, P.; Bhama, J. Induction immunosuppressive therapy in cardiac transplantation: a systematic review and meta-analysis. Hear. Fail. Rev. 2018, 23, 641–649. [CrossRef]
- Rizk, J.; Mehra, M.R. WITHDRAWN: Anticoagulation management strategies in heart transplantation. Prog. Cardiovasc. Dis. 2020, 63. [CrossRef]
- Haberbusch, M.; De Luca, D.; Moscato, F. Changes in Resting and Exercise Hemodynamics Early After Heart Transplantation: A Simulation Perspective. Front. Physiol. 2020, 11. [CrossRef]
- Su, Y., Zhu, C., Wang, B., Zheng, H., McAlister, V., Lacefield, J.C., Quan, D., Mele, T., Greasley, A., Liu, K., Zheng, X. Circular RNA Foxo3 in cardiac ischemia-reperfusion injury in heart transplantation: A new regulator and target. American journal of transplantation : official journal of the American Society of Transplantation and the American Society of Transplant Surgeons. 2021;21(9):2992-3004.
- Kim, S.H.; Han, K.; Kang, G.; Lee, S.W.; Park, C.-M.; Cho, J.; Choi, J.W.; Park, S.J.; Kang, M.; Kim, T.J.; et al. Risk of Postoperative Gastrointestinal Bleeding and Its Associated Factors: A Nationwide Population-Based Study in Korea. J. Pers. Med. 2021, 11, 1222. [CrossRef]
- Hsu, J.L.; Chen, K.A.; Butler, L.R.; Bahraini, A.; Kapadia, M.R.; Gomez, S.M.; Farrell, T.M. Application of machine learning to predict postoperative gastrointestinal bleed in bariatric surgery. Surg. Endosc. 2023, 37, 7121–7127. [CrossRef]
- Lenti, M.V.; Pasina, L.; Cococcia, S.; Cortesi, L.; Miceli, E.; Dominioni, C.C.; Pisati, M.; Mengoli, C.; Perticone, F.; Nobili, A.; et al. Mortality rate and risk factors for gastrointestinal bleeding in elderly patients. Eur. J. Intern. Med. 2019, 61, 54–61. [CrossRef]
- Harel, Z.; Chertow, G.M.; Shah, P.S.; Harel, S.; Dorian, P.; Yan, A.T.; Saposnik, G.; Sood, M.M.; Molnar, A.O.; Perl, J.; et al. Warfarin and the Risk of Stroke and Bleeding in Patients With Atrial Fibrillation Receiving Dialysis: A Systematic Review and Meta-analysis. Can. J. Cardiol. 2017, 33, 737–746. [CrossRef]
- Kaneko, T.; Aranki, S.F. Anticoagulation for Prosthetic Valves. Thrombosis 2013, 2013, 1–4. [CrossRef]
- Eikelboom, J.W.; Connolly, S.J.; Brueckmann, M.; Granger, C.B.; Kappetein, A.P.; Mack, M.J.; Blatchford, J.; Devenny, K.; Friedman, J.; Guiver, K.; et al. Dabigatran versus Warfarin in Patients with Mechanical Heart Valves. New Engl. J. Med. 2013, 369, 1206–1214. [CrossRef]
- Asleh, R.; Schettle, S.; Briasoulis, A.; Killian, J.M.; Stulak, J.M.; Pereira, N.L.; Kushwaha, S.S.; Maltais, S.; Dunlay, S.M. Predictors and Outcomes of Renal Replacement Therapy After Left Ventricular Assist Device Implantation. Mayo Clin. Proc. 2019, 94, 1003–1014. [CrossRef]
- Elizabeth Parsons, C., Nelson, R., Book, L.S., Kyle Jensen, M. Renal replacement therapy in infants and children with hepatorenal syndrome awaiting liver transplantation: a case-control study. Liver transplantation : official publication of the American Association for the Study of Liver Diseases and the International Liver Transplantation Society. 2014;20(12):1468-74.
- Granholm, A.; Krag, M.; Marker, S.; Alhazzani, W.; Perner, A.; Møller, M.H. Predictors of gastrointestinal bleeding in adult ICU patients in the SUP-ICU trial. Acta Anaesthesiol. Scand. 2021, 65, 792–800. [CrossRef]
- Sparrow, C.T.; Nassif, M.E.; Raymer, D.S.; Novak, E.; LaRue, S.J.; Schilling, J.D. Pre-Operative Right Ventricular Dysfunction Is Associated With Gastrointestinal Bleeding in Patients Supported With Continuous-Flow Left Ventricular Assist Devices. JACC: Hear. Fail. 2015, 3, 956–964. [CrossRef]
- Zhou, Z.; Liu, C.; Yang, Y.; Wang, F.; Zhang, L.; Fu, P. Anticoagulation options for continuous renal replacement therapy in critically ill patients: a systematic review and network meta-analysis of randomized controlled trials. Crit. Care 2023, 27, 1–17. [CrossRef]
- Sanaie, S.; Mirzalou, N.; Shadvar, K.; Golzari, S.E.J.; Soleimanpour, H.; Shamekh, A.; Bettampadi, D.; Safiri, S.; Mahmoodpoor, A. A comparison of nasogastric tube insertion by SORT maneuver (sniffing position, NGT orientation, contralateral rotation, and twisting movement) versus neck flexion lateral pressure in critically ill patients admitted to ICU: a prospective randomized clinical trial. Ann. Intensiv. Care 2020, 10, 1–8. [CrossRef]
- Nelson, R., Edwards, S., Tse, B. Prophylactic nasogastric decompression after abdominal surgery. The Cochrane database of systematic reviews. 2007;2007(3):Cd004929.
- Lin, Y.; Chen, M.; Peng, Y.; Chen, Q.; Li, S.; Chen, L. Feeding intolerance and risk of poor outcome in patients undergoing cardiopulmonary bypass surgery. Br. J. Nutr. 2021, 126, 1340–1346. [CrossRef]
- Lavi, R.; Katznelson, R.; Cheng, D.; Minkovich, L.; Klein, A.; Carroll, J.; Karski, J.; Djaiani, G. The Effect of Nasogastric Tube Application During Cardiac Surgery on Postoperative Nausea and Vomiting—A Randomized Trial. J. Cardiothorac. Vasc. Anesthesia 2011, 25, 105–109. [CrossRef]
- Kotfis, K.; Szylińska, A.; Listewnik, M.; Lechowicz, K.; Kosiorowska, M.; Drożdżal, S.; Brykczyński, M.; Rotter, I.; Żukowski, M. Balancing intubation time with postoperative risk in cardiac surgery patients – a retrospective cohort analysis. Ther. Clin. Risk Manag. 2018, 14, 2203–2212. [CrossRef]
- Marks, D.; Cox, A.; Prodromou, A.; Gadelrab, R.; Pakzad, F.; Harrison, R. Fatal consequences of nasogastric intubation: a clinical reminder. J. R. Soc. Med. 2009, 102, 157–159. [CrossRef]
- Mistry, R.C., Vijayabhaskar, R., Karimundackal, G., Jiwnani, S., Pramesh, C.S. Effect of short-term vs prolonged nasogastric decompression on major postesophagectomy complications: a parallel-group, randomized trial. Archives of surgery (Chicago, Ill : 1960). 2012;147(8):747-51.
- Gomes, C.A., Jr., Andriolo, R.B., Bennett, C., Lustosa, S.A., Matos, D., Waisberg, D.R., Waisberg, J. Percutaneous endoscopic gastrostomy versus nasogastric tube feeding for adults with swallowing disturbances. The Cochrane database of systematic reviews. 2015;2015(5):Cd008096.
- Adamik, B.; Kübler, A.; Gozdzik, A.; Gozdzik, W. Prolonged Cardiopulmonary Bypass is a Risk Factor for Intestinal Ischaemic Damage and Endotoxaemia. Hear. Lung Circ. 2017, 26, 717–723. [CrossRef]
Figure 1.
Study flow chart in the retrospective study. HT: heart transplantation; GIB: gastrointestinal bleeding.
Figure 1.
Study flow chart in the retrospective study. HT: heart transplantation; GIB: gastrointestinal bleeding.
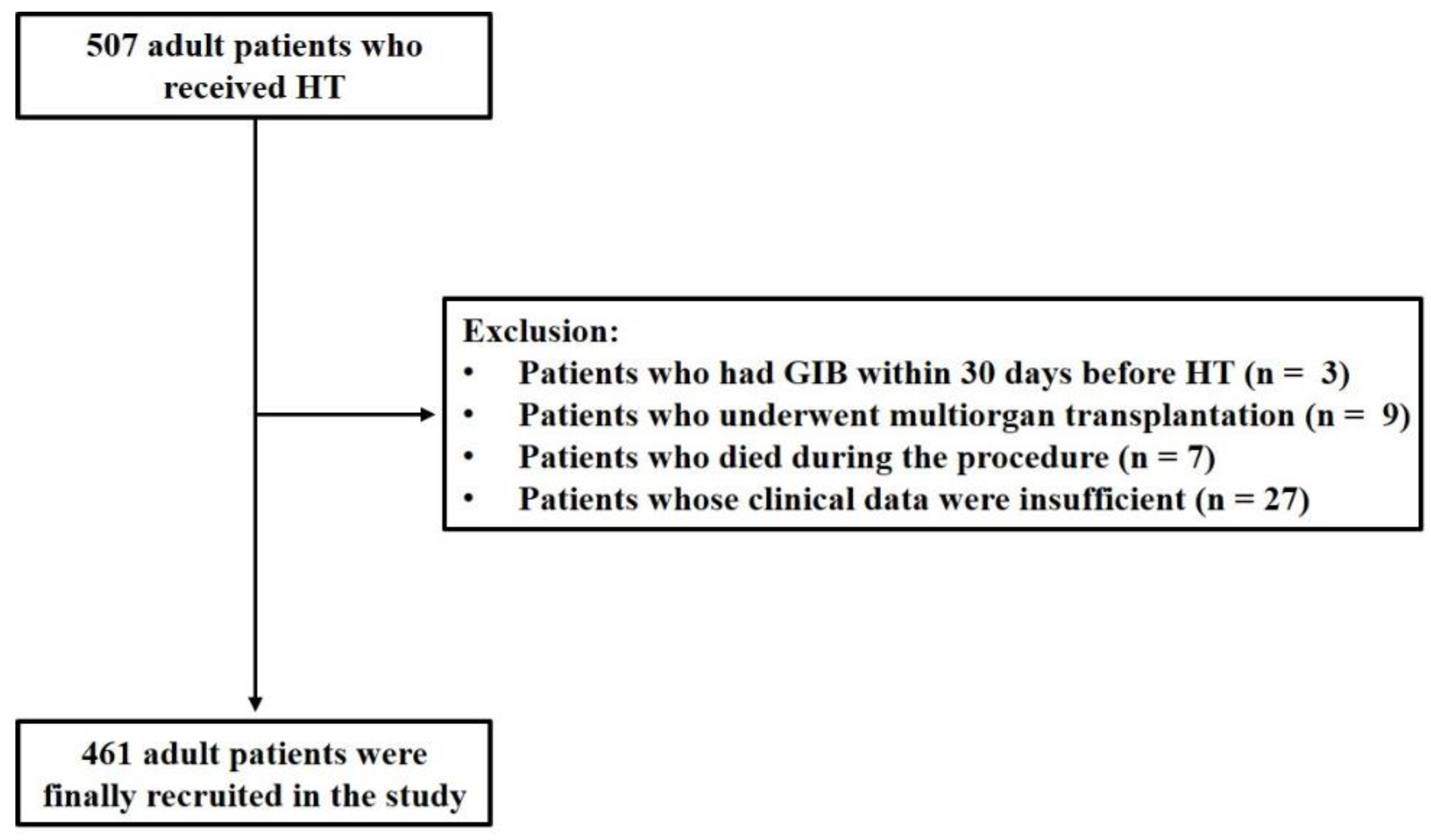
Figure 2.
Underlying diagnosis of heart failure resulting in HT among enrolled patients. DCM: dilated cardiomyopathy; RCM: restrictive cardiomyopathy; HCM: hypertrophic cardiomyopathy; ICM: ischemic cardiomyopathy; CHD: congenital heart disease; VHD: valvular heart disease; HT: heart transplantation.
Figure 2.
Underlying diagnosis of heart failure resulting in HT among enrolled patients. DCM: dilated cardiomyopathy; RCM: restrictive cardiomyopathy; HCM: hypertrophic cardiomyopathy; ICM: ischemic cardiomyopathy; CHD: congenital heart disease; VHD: valvular heart disease; HT: heart transplantation.
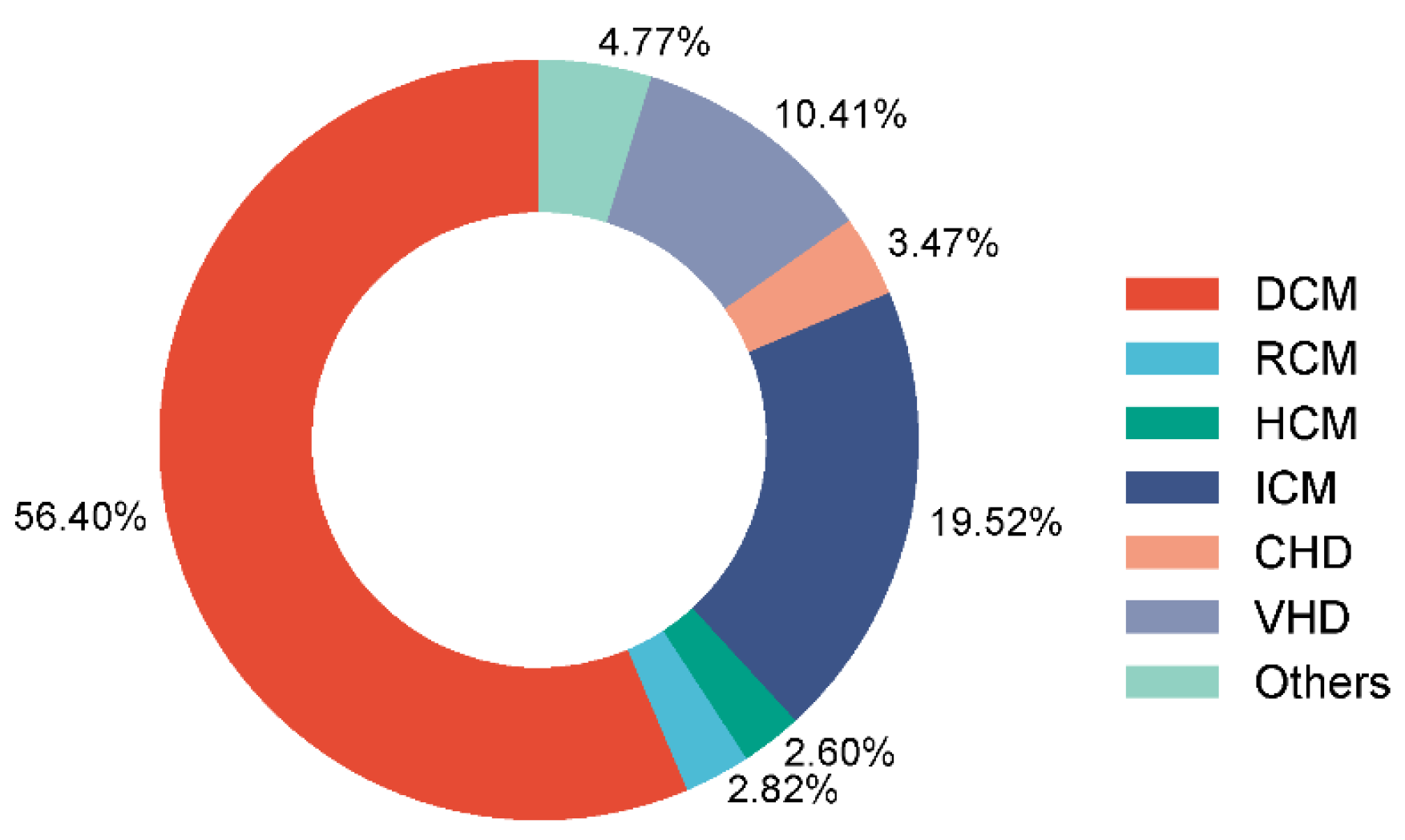
Figure 3.
Time trend of crude incidence of GIB after HT. GIB: gastrointestinal bleeding; HT: heart transplantation.
Figure 3.
Time trend of crude incidence of GIB after HT. GIB: gastrointestinal bleeding; HT: heart transplantation.
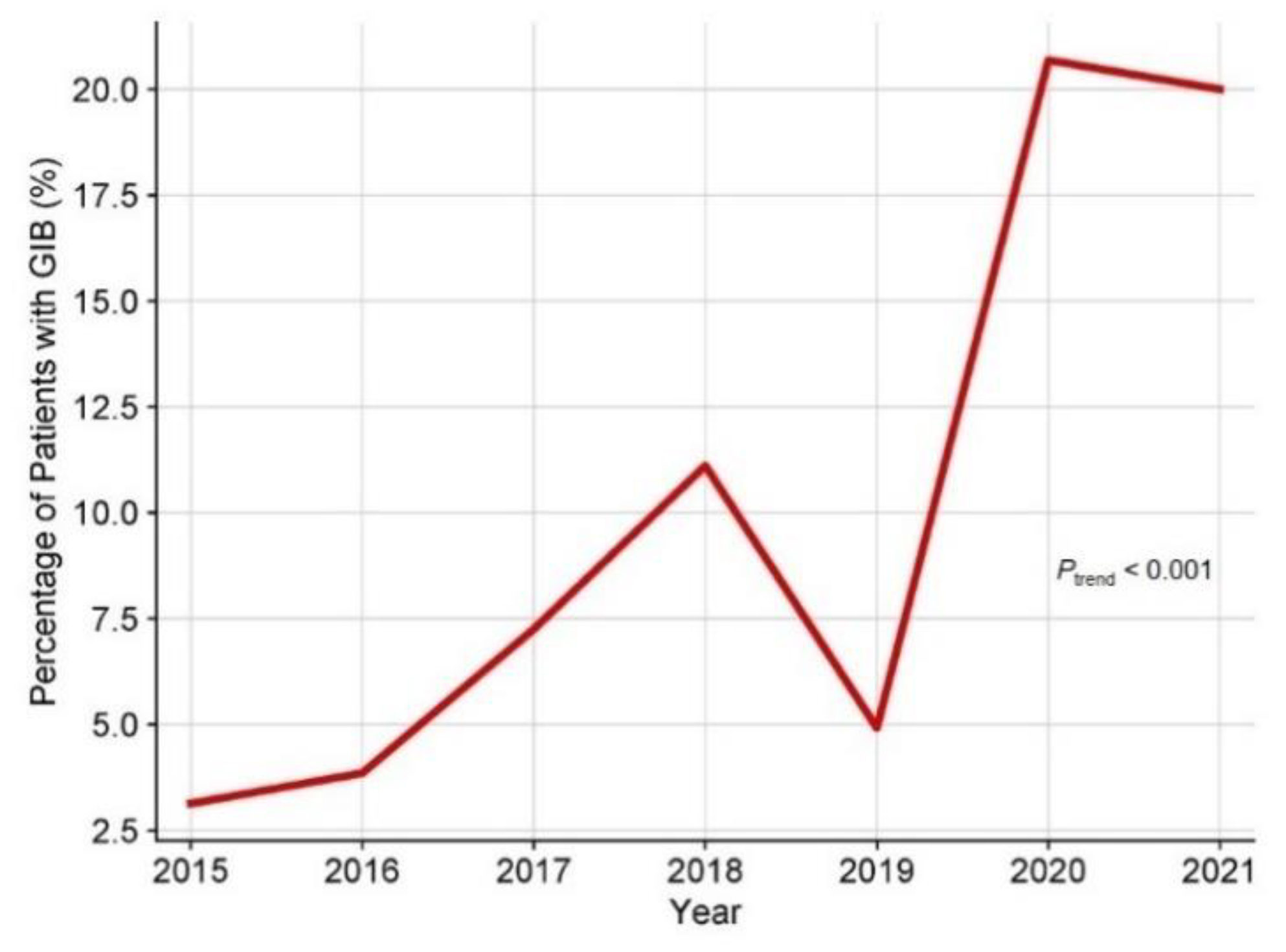
Figure 4.
The cumulative incidence of events comparing 1-year mortality between patients with and without postoperative GIB after HT. The shaded area around the curves represents the 95% CI. GIB: gastrointestinal bleeding; HT: heart transplantation; CI: confidence interval.
Figure 4.
The cumulative incidence of events comparing 1-year mortality between patients with and without postoperative GIB after HT. The shaded area around the curves represents the 95% CI. GIB: gastrointestinal bleeding; HT: heart transplantation; CI: confidence interval.
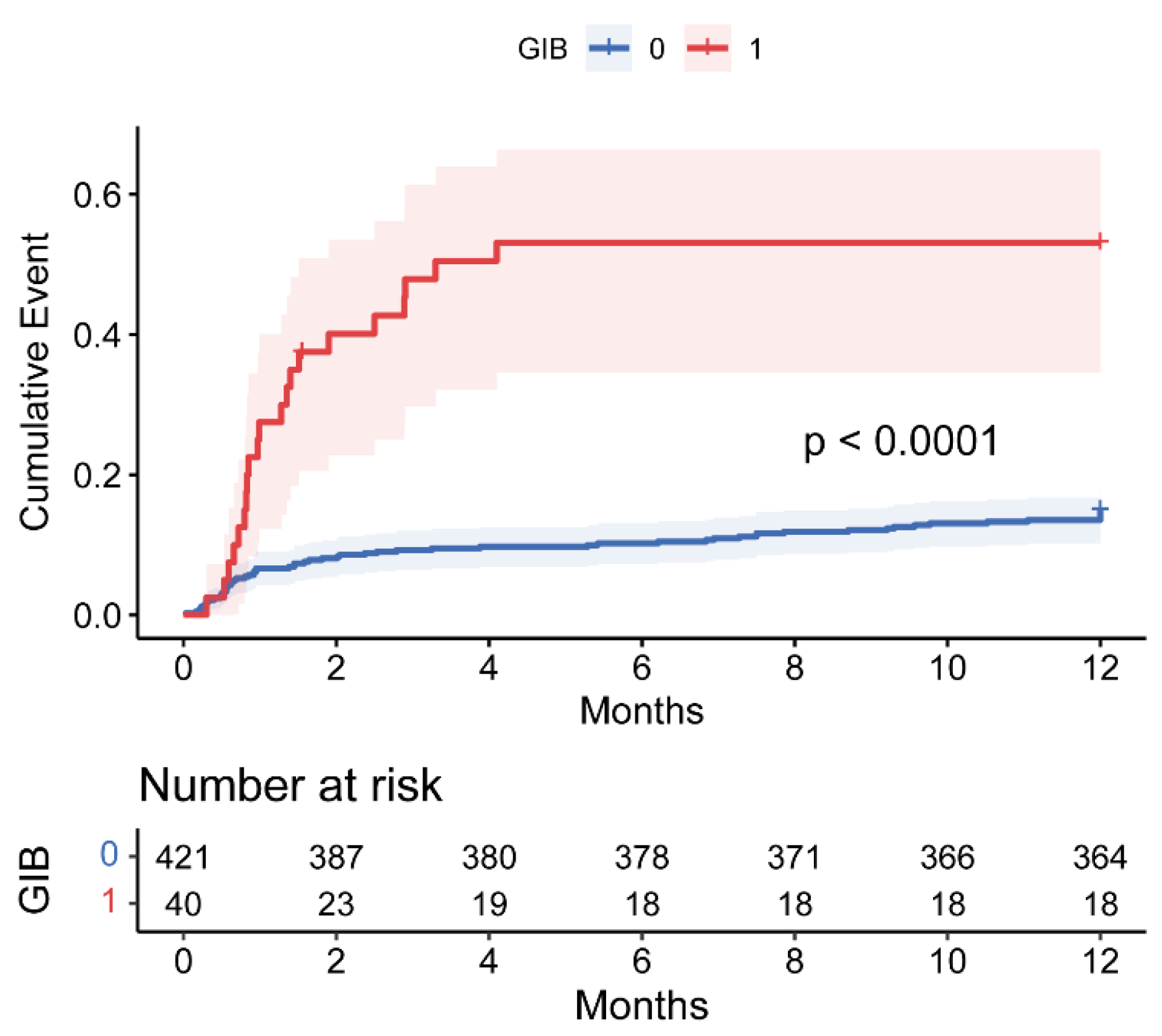
Figure 5.
Forest plot of independent risk factors for GIB after HT. OR: odds ratio; CI: confidence interval; CRRT: continuous renal replacement therapy; GIB: gastrointestinal bleeding; HT: heart transplantation.
Figure 5.
Forest plot of independent risk factors for GIB after HT. OR: odds ratio; CI: confidence interval; CRRT: continuous renal replacement therapy; GIB: gastrointestinal bleeding; HT: heart transplantation.
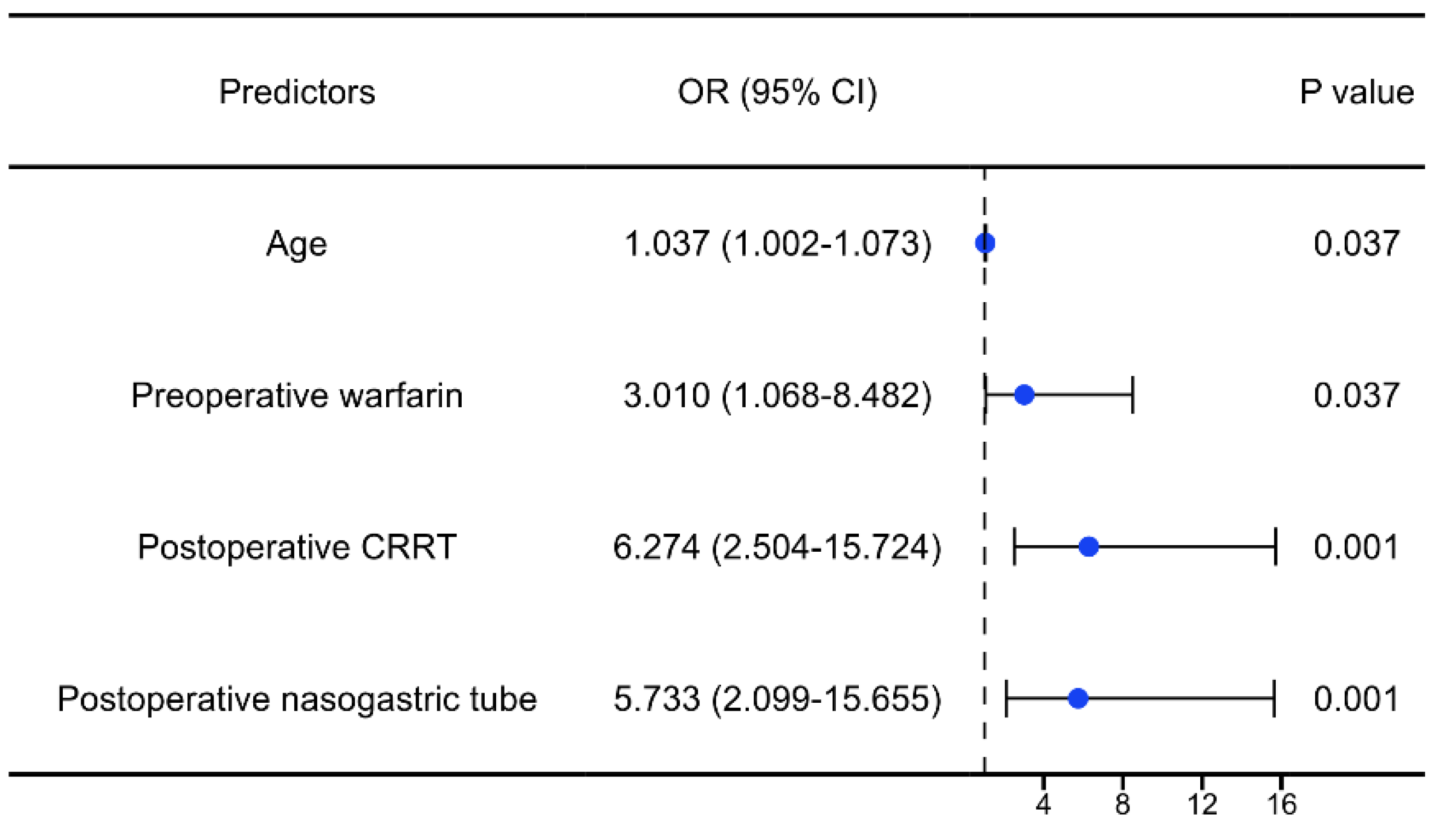
Figure 6.
Nomogram for the prediction of postoperative GIB risk in HT patients. CRRT: continuous renal replacement therapy; GIB: gastrointestinal bleeding; HT: heart transplantation.
Figure 6.
Nomogram for the prediction of postoperative GIB risk in HT patients. CRRT: continuous renal replacement therapy; GIB: gastrointestinal bleeding; HT: heart transplantation.
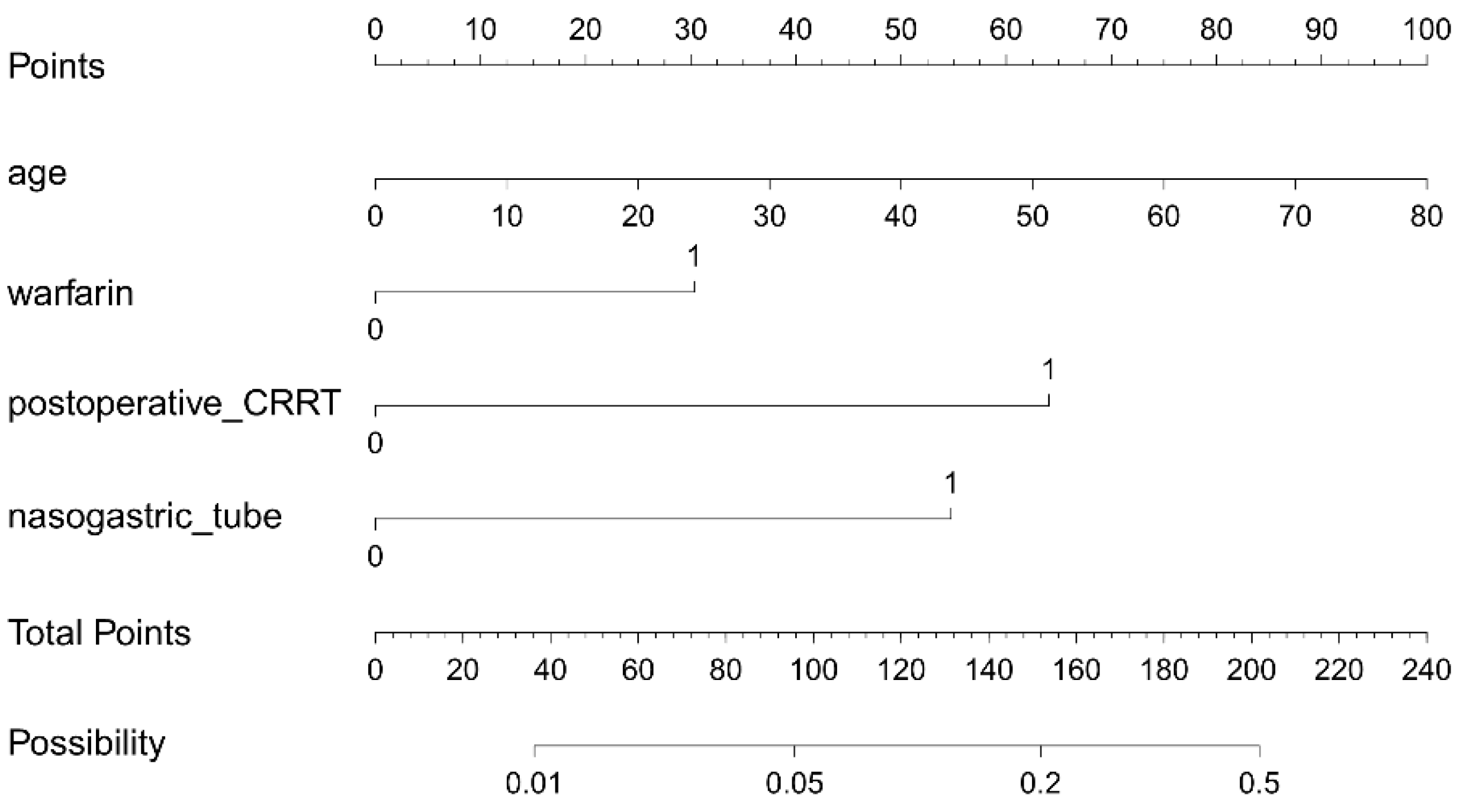
Figure 7.
(a) ROC curve and (b) Calibration curve for postoperative GIB prediction model. AUC: area under the curve; CI: confidence interval; ROC: receiver operating characteristic; GIB: gastrointestinal bleeding.
Figure 7.
(a) ROC curve and (b) Calibration curve for postoperative GIB prediction model. AUC: area under the curve; CI: confidence interval; ROC: receiver operating characteristic; GIB: gastrointestinal bleeding.
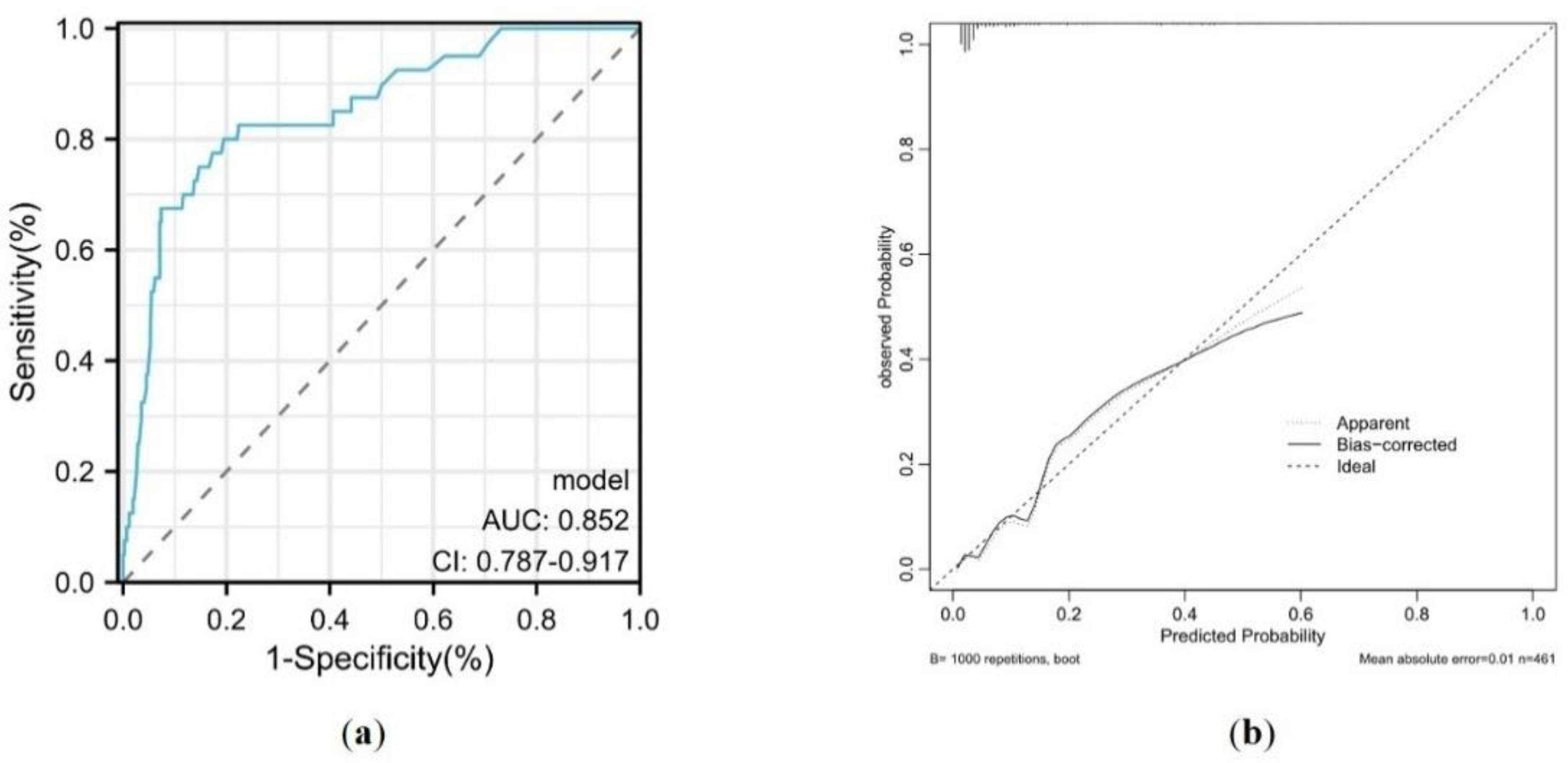

Table 1.
Baseline characteristic of study patients.
| Non-GIB (n=421) | GIB (n=40) | P values | |
|---|---|---|---|
| Age (years) | 50.00 (39.00-57.00) | 54.50 (47.50-58.00) | 0.024 |
| Gender, male (%) | 84 (20.0) | 11 (27.5) | 0.259 |
| BMI (kg/m2) | 23.02 ± 3.97 | 22.02 ± 2.89 | 0.120 |
| Blood type | 0.774 | ||
| A, n (%) | 146 (34.7) | 12 (30.0) | |
| B, n (%) | 116 (27.6) | 11 (27.5) | |
| AB, n (%) | 31 (7.4) | 2 (5.0) | |
| O, n (%) | 128 (30.4) | 15 (37.5) | |
| Current smoking, n (%) | 174 (41.3) | 12 (30.0) | 0.163 |
| Current drinking, n (%) | 116 (27.6) | 7 (17.5) | 0.170 |
| Medical history | |||
| Hypertension, n (%) | 70 (16.6) | 3 (7.5) | 0.131 |
| Hyperlipemia, n (%) | 28 (6.7) | 0 (0.0) | 0.157 |
| Diabetes, n (%) | 85 (20.2) | 8 (20.0) | 0.977 |
| Gastrointestinal disease, n (%) | 48 (11.4) | 5 (12.5) | 0.796 |
| NYHA classification | 0.932 | ||
| II, n (%) | 1 (0.2) | 0 (0.0) | |
| III, n (%) | 18 (4.3) | 2 (5.0) | |
| IV, n (%) | 402 (95.5) | 38 (95.0) | |
| Cardiac operation, n (%) | 121 (28.7) | 17 (42.5) | 0.069 |
| Dialysis, n (%) | 4 (1.0) | 0 (0.0) | 1.000 |
| Preoperative data | |||
| RBC (×1012/L) | 4.49 (4.08-4.89) | 4.16 (3.72-4.69) | 0.004 |
| Hb (g/L) | 138.00 (122.00-149.00) | 127.50 (105.75-141.25) | 0.004 |
| WBC (×109/L) | 6.36 (4.96-8.00) | 5.97 (4.46-6.93) | 0.089 |
| PLT (×109/L) | 172.50 (138.25-221.75) | 173.00 (119.25-235.25) | 0.782 |
| albumin (g/L) | 39.50 (36.60-42.30) | 37.90 (34.90-40.30) | 0.025 |
| AST (mmol/L) | 28.00 (21.00-41.00) | 26.00 (18.25-38.00) | 0.737 |
| ALT (mmol/L) | 28.00 (18.00-46.00) | 23.50 (13.25-44.75) | 0.226 |
| TBIL (mmol/L) | 22.00 (14.20-33.50) | 27.05 (13.68-40.85) | 0.737 |
| Cr (μmol/L) | 88.65 (72.43-108.33) | 87.35 (72.65-119.78) | 0.996 |
| BUN (mmol/L) | 7.31 (5.84-9.57) | 7.55 (6.30-11.09) | 0.291 |
| TG (mmol/L) | 1.06 (0.78-1.43) | 0.95 (0.74-1.29) | 0.381 |
| LDL-C (mmol/L) | 2.14 (1.69-2.63) | 2.09 (1.61-2.76) | 0.876 |
| APTT (s) | 39.00 (36.20-43.25) | 40.60 (38.18-46.50) | 0.027 |
| INR | 1.17 (1.07-1.37) | 1.31 (1.16-1.60) | 0.003 |
| NT-proBNP (pg/mL) | 3079.15 (1471.25-6723.78) | 3930 (1310-7974) | 0.597 |
| LVEF (%) | 24.20 (20.00-29.00) | 22.20 (16.00-29.50) | 0.264 |
| Preoperative treatment | |||
| Warfarin, n (%) | 45 (10.7) | 10 (25.0) | 0.017 |
| Heparin, n (%) | 97 (23.0) | 11 (27.5) | 0.525 |
| LMWH, n (%) | 108 (25.7) | 8 (20.0) | 0.431 |
| Aspirin, n (%) | 77 (18.3) | 10 (25.0) | 0.300 |
| Clopidogrel, n (%) | 21 (5.0) | 3 (7.5) | 0.453 |
| Intubation, n (%) | 6 (1.4) | 1 (2.5) | 0.473 |
| IABP, n (%) | 6 (1.4) | 2 (5.0) | 0.147 |
| ECMO, n (%) | 7 (1.7) | 3 (7.5) | 0.047 |
| Intraoperative data | |||
| Pulmonary artery systolic pressure (mmHg) | 48.00 (34.00-61.25) | 50.00 (40.00-59.00) | 0.557 |
| Cross clamp time (min) | 30.00 (26.00-36.00) | 33.00 (26.00-43.50) | 0.087 |
| CPB time (min) | 106.00 (91.00-130.00) | 133.00 (103.50-154.75) | < 0.001 |
| Operation time (min) | 240.00 (210.00-300.00) | 300.00 (242.50-360.00) | < 0.001 |
| Postoperative data | |||
| First 24 hours of drainage (mL) | 350.00 (250.00-520.00) | 375.00 (152.50-530.00) | 0.700 |
| Intubation time (min) | 2160.00 (1401.25-3254.25) | 6210.00 (2510.25-16530.00) | < 0.001 |
| CRRT, n (%) | 48 (11.4) | 26 (65.0) | < 0.001 |
| IABP, n (%) | 161 (38.2) | 21 (52.5) | 0.078 |
| ECMO, n (%) | 17 (4.0) | 9 (22.5) | < 0.001 |
| Nasogastric tube, n (%) | 97 (23.0) | 31 (77.5) | < 0.001 |
| ICU stay (hours) | 214.00 (158.50-279.50) | 424.00 (196.00-714.00) | < 0.001 |
| Postoperative hospital stay (days) | 34.00 (26.00-46.00) | 49.00 (29.25-72.75) | 0.001 |
| In-hospital deaths | 20 (4.8) | 6 (15.0) | 0.018 |
| 30-day deaths | 28 (6.7) | 11 (27.5) | < 0.001 |
| 90-day deaths | 39 (9.3) | 20 (50.0) | < 0.001 |
| 1-year deaths | 63 (15.0) | 21 (52.5) | < 0.001 |
Data are expressed as mean ± standard deviation, n (%), or medians (interquartile ranges). GIB: gastrointestinal bleeding; BMI: body mass index; NYHA: New York Heart Association; RBC: red blood cell; Hb: hemoglobin; WBC: white blood cell; PLT: platelet; AST: aspartate transaminase; ALT: alanine aminotransferase; TBIL: total bilirubin; Cr: creatinine; BUN: blood urea nitrogen; TG: triglyceride; LDL-C: low density lipoprotein cholesterol; APTT: activated partial thromboplastin time; INR: international normalized ratio; NT-proBNP: N-terminal pro-B-type natriuretic peptide; LVEF: left ventricular ejection fraction; LMWH: low molecular weight heparin; IABP: intra-aortic balloon pump; ECMO: extracorporeal membrane oxygenation; CPB: cardiopulmonary bypass; CRRT: continuous renal replacement therapy; ICU: intensive care unit.
Table 2.
Univariate and multivariate logistic regression analysis of postoperative GIB in patients with HT.
Table 2.
Univariate and multivariate logistic regression analysis of postoperative GIB in patients with HT.
| Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|
| OR (95% CI) | P values | OR (95% CI) | P values | |
| Age | 1.04 (1.00-1.07) | 0.027 | 1.04 (1.00-1.07) | 0.037 |
| Male | 1.52 (0.73-3.17) | 0.262 | 1.11 (0.45-2.77) | 0.820 |
| BMI | 0.93 (0.85-1.02) | 0.119 | ||
| Cardiac operation | 1.92 (0.93-3.98) | 0.078 | ||
| Gastrointestinal disease | 1.11 (0.42-2.97) | 0.835 | ||
| RBC | 0.62 (0.39-0.99) | 0.046 | ||
| Hb | 0.98 (0.96-0.99) | 0.003 | ||
| WBC | 0.89 (0.77-1.03) | 0.128 | ||
| albumin | 0.93 (0.87-1.00) | 0.050 | ||
| APTT | 1.01 (0.99-1.04) | 0.244 | ||
| INR | 1.24 (0.89-1.73) | 0.197 | ||
| Preoperative warfarin | 2.79 (1.28-6.07) | 0.010 | 3.01 (1.07-8.48) | 0.037 |
| Preoperative ECMO | 4.80 (1.19-19.32) | 0.027 | 1.741 (0.34-8.94) | 0.507 |
| Cross clamp time | 1.03 (1.00-1.06) | 0.056 | 1.00 (0.96-1.04) | 0.931 |
| CPB time | 1.00 (1.00-1.01) | 0.085 | 1.00 (0.99-1.01) | 0.937 |
| Operation time | 1.01 (1.00-1.01) | 0.001 | 1.00 (0.99-1.00) | 0.362 |
| Postoperative CRRT | 14.43 (7.05-29.53) | < 0.001 | 6.27 (2.50-15.72) | < 0.001 |
| Postoperative IABP | 1.79 (0.93-3.42) | 0.081 | 0.491 (0.21-1.18) | 0.112 |
| Postoperative ECMO | 6.90 (2.84-16.75) | < 0.001 | 2.36 (0.70-7.93) | 0.164 |
| Postoperative nasogastric tube | 11.51 (5.30-25.00) | < 0.001 | 5.73 (2.10-15.66) | 0.001 |
Multivariate analysis adjusted for male, preoperative ECMO, cross clamp time, CPB time, operation time, postoperative IABP, postoperative ECMO. GIB: gastrointestinal bleeding; HT: heart transplantation; OR: odds ratio; CI: confidence interval; BMI: body mass index; RBC: red blood cell; Hb: hemoglobin; WBC: white blood cell; APTT: activated partial thromboplastin time; INR: international normalized ratio; ECMO: extracorporeal membrane oxygenation; CPB: cardiopulmonary bypass; CRRT: continuous renal replacement therapy; IABP: intra-aortic balloon pump; ICU: intensive care unit.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



