
Submitted:
29 September 2024
Posted:
01 October 2024
You are already at the latest version
Abstract
Antibiotic-loaded bone cement has been traditionally advocated as a key step for the success of one-stage hip revision surgery, while cementless techniques have been re-cently proposed with and without the use of local antibacterials as an equally suc-cessful alternative. Aim of this review is to investigate the effective role of local anti-microbial protection for one-stage cemented and cementless hip revision surgery. Twelve studies reporting the results of cemented single-stage procedure at a minimum two years follow-up were reviewed. When pooling together the data, no infection re-currence was observed on average in 83.3% of the patients (range 75.0% to 100%). Only two papers, both from the same French group, included patients treated without the use of antibiotic-loaded bone cement, with an average infection control of 95.9% in a total of 195 patients. This figure appears better that the 80.7% infection control ob-tained by pooling together all the remaining studies. Concerning cementless one-stage revision, a total of 17 studies, reporting on 521 patients, showed an average 90.0% (range 56.8% to 100%) no infection recurrence, at a minimum two years follow-up. Eight papers reported the outcomes of cementless implants without any local antibac-terial protection and nine more described four different techniques for local antimi-crobial implant protection. No comparative study investigated cementless revision with or without local antibacterial protection. Pooled data showed an average infection control of 86.7%, without the application of local antibacterials, compared to 90.1% to 100% with local antimicrobial protection, depending on the technology used. Howev-er, due to the relatively low number of patients treated with each local antimicrobial protection, no statistical difference could be found, either considering local antibacte-rial strategies alone or pooled together. No side effect had been reported by any local antibacterial technique. This review points out that local antibacterial protection for one-stage hip revision surgery, although safe and largely performed in the clinical set-ting, appears still to rely mainly on experts’ opinion and on observational series with no prospective or comparative trial, hence no definitive conclusion can be drawn con-cerning its effective role in one-stage hip revision surgery.
Keywords:
Hip
; Infection
; Prosthesis: PJI
; One‐stage
; Single‐stage
; Revision
; Review
; Local antibiotics
; Antibacterial coatings
1. Introduction
“Rates of peri-prosthetic joint infection (PJI) in primary total hip and total knee arthroplasty range between 0.3% and 1.9%, and up to 10% in revision cases. Significant morbidity is associated with this devastating complication, the economic burden on our healthcare system is considerable, and the personal cost to the affected patient is immeasurable” [1].
The occurrence of peri-prosthetic joint infection (PJI) generally requires the removal of the infected implant and its exchange in a single- or two-stage surgical procedure. The operative approach is determined by a combination of surgeon’s experience, clinical and radiological presentations, available bone-stock and infection factors, with the majority of surgeons opting for a two-stage procedure, which has been traditionally felt as more secure and succcessful [2,3]. On the other hand, a one-stage approach does offer self-evident advantages over a staged procedure, including reduced hospitalization, costs and time to recovery [4]. Moreover, several recent studies and systematic reviews, have pointed out the lack of a statistically significant difference in infection recurrence rate after one-stage or two-stage hip revision surgery [5,6]. These observations are progressively prompting more and more surgeons to propose one-stage strategies to their patients and novel one-stage techniques have been proposed in recent years.
In fact, the first and the most often reported one-stage technique requires the fixation of the new implant with antibiotic-loaded bone cement, which is considered a key step for the success of the procedure [7]. On the other hand, more recently, various authors reported that cementless revision hip prosthesis, with or without the application of local antibiotic delivery systems, can be equally effective [6].
Aim of the present review of the current literature is to investigate the effective role of local antibacterial protection technologies for one-stage cemented or cementless hip revision surgery, to test the hypothesis that local antibiotic implant protection may have a positive impact on reducing the infection recurrence rate after this surgery.
2. The role of local antibacterial protection in cemented one-stage hip revision surgery
In the early 1970s, Dr. Hans Wilhelm Buchholz conducted extensive research on antibiotics and polymethylmethacrylate (PMMA) in the context of hip and knee replacement surgery. He consistently reported lower infection rates with the addition of gentamycin antibiotics to the bone cement. Dr. Buchholz was among the first to demonstrate the successful use of antibiotic-loaded bone cement for preventing infections in endoprostheses, as well as using single exchange arthroplasty for treating infected prostheses [8]. One-stage exchange arthroplasty, using techniques and principles similar to those originally described by Buchholz’s team at the ENDO Klinik in Hamburg, Germany, has been since then adopted by various centers around the world [9,10,11,12].
The three key principles of the ENDO Klinik have been well described and recently reconfirmed [13,14]. First, the organism must be identified along with its sensitivities and minimum inhibitory concentrations. According to its original description, single-stage revision should not be performed without this information, as antibiotic treatment cannot be appropriately tailored to combat the infection. Joint aspiration is hence performed with the patient off antibiotics for at least 14 days, using an "as sterile as possible" technique, and with a culture incubation period of 14 days. The second principle is debridement. Aggressive debridement and complete removal of all infected tissues and implanted biomaterials is considered a pivotal step for the success of the technique. The third principle involves both local and systemic antibiotic delivery tailored to the identified pathogenic organism. Local antibiotic delivery is achieved through cement [15]. According to the authors that first described this method, PMMA ensures much higher tissue concentrations at the infection site than systemic administration. Bactericidal antibiotics, such as aminoglycosides, cephalosporins, fluoroquinolones, metronidazole, penicillin, and vancomycin can be advantageously mixed, while some authors consider also clindamycin an acceptable bacteriostatic option [5]. Up to 10% of the dry crystalline weight of antibiotics can be added to the cement without significant mechanical loss.
Concerning safety, while local antibiotics achieve high intra-articular concentrations with lower systemic risks, there are rare case reports of systemic complications like renal or hepatic failure, and allergic reactions [16]. However, pharmacokinetic studies investigating antibiotic concentrations released from PMMA showed serum and urine concentrations below toxic thresholds [17,18,19,20], while local cytotoxicity of eluted antibiotics demonstrated good cell survival/recovery capacities after high antibiotic concentration exposure for antibiotics as cephazolin, vancomycin and aminoglycosides [21,22], even if high local levels of gentamicin have been shown by some author to have a detrimental impact on osteogenesis [23]. Another big concern about prolonged local antibiotic delivery from bone cement is the development of microbial resistance. This has been disproven by several authors [24,25,26,27]. Overall, the potential toxic effects and risks of local release of antibiotics by bone cement are considered extremely low and rare and do not prevent the current widespread use of antibiotic-loaded bone cement in various clinical settings [28,29,30]. On the other hand, it should be emphasized that the presence of antibiotic in bone cement has been found able to reduce bacterial biofilm formation, but it may not completely inhibit its presence [31].
The scientific background of the clinical use of local antibiotics released from bone cement relies on in vitro [32,33] and in vivo studies [34,35]. Moreover, comparative clinical trials, investigating low- or high dose local antibiotics delivery and/or single versus dual antibiotics, do bring evidence that higher dose or combination of antibiotics improve post-surgical infection control compared to lower dose or single antibiotic. Jenny and co-workers, reported on a prospective, single center clinical trial, showing a statistically significant 50% reduction of infection recurrence rate after one-stage hip or knee revision surgery, using high dose gentamycin and clindamycin loaded bone cement, compared to low-dose [36]. Similarly, Smynski et al., recently reported the data from the German register, showing better infection prevention after hip prosthesis for femoral neck fracture management by using dual antibiotics in bone cement, compared to single antibiotic [37]. This study is in line and confirms a previous observation conducted in the United Kingdom [38]. However, to the best of our knowledge, there is a lack of prospective studies or systematic reviews and meta-analysis comparing local antibiotic delivery from PMMA to plain cement for one-stage treatment of peri-prosthetic hip infection.
We performed a thorough and comprehensive literature search of studies fully written or with an abstract in English on cemented and uncemented one-stage hip revision surgery for delayed periprosthetic hip infection, by searching the following internet databases,: EMBASE; PubMed/Medline; Medline Daily Update; Medline In-Process and other non-indexed citations; Google Scholar; SCOPUS; CINAHL; Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Reviews; NHS Health Technology Assessment; http://www.google.com, with the following keywords either alone or in a variety of combinations: hip; infection; arthroplasty; prosthesis; total hip replacement; THR; THA; prosthetic hip infection; periprosthetic hip infection; exchange arthroplasty; one-stage; single-stage; cemented; cementless; uncemented. The results of all studies of 5 or more cases and a minimum follow-up of 24 months are reported in Table 1 and Table 2.
Mean and standard deviations (SD) were calculated on pooled data and compared. Statistical analysis was performed using t-tests and Fisher’s Exact test where appropriate. A p-value of <0.05 was deemed to be statistically significant.
Pooling together the data of 12 studies available for our analysis, reporting on delayed (> 6 weeks from surgery) PJI, the average success rate of one-stage antibiotic-loaded cemented hip revision is 83.2% (range 75% to 100%) (cf. Table 1).

Table 1.
Data from studies reporting cemented one-stage hip revision surgery for delayed (> 6 weeks after surgery) peri-prosthetic hip infection, at a minimum follow-up of 24 months.
Table 1.
Data from studies reporting cemented one-stage hip revision surgery for delayed (> 6 weeks after surgery) peri-prosthetic hip infection, at a minimum follow-up of 24 months.
| Author | Year | Number of patients | Number of patients free from infection at follow-up | Percent of patients free from infection at follow-up | Follow-up (months) | Selection bias | Local antimicrobial protection | |||
| Min | Max | Mean | ||||||||
| Buchholz [39] | 1981 | 582 | 448 | 76.8 | 24 | 132 | No | Yes | ||
| Miley [40] | 1982 | 46 | 40 | 87 | 32 | 48.5 | Yes | Yes | ||
| Wroblewski [41] | 1986 | 102 | 93 | 91.2 | 38.8 | No | Yes | |||
| Sanzen [42] | 1988 | 102 | 77 | 75.5 | 24 | 108 | No | Yes | ||
| Raut [43] | 1995 | 57 | 49 | 86.0 | 24 | 151 | 88 | No | Yes | |
| Mulcahy [44] | 1996 | 15 | 15 | 100 | 24 | Yes | Yes | |||
| Ure [45] | 1998 | 20 | 20 | 100 | 42 | 205.2 | 118.8 | Yes | Yes | |
| Callaghan [46] | 1999 | 12 | 10 | 83.3 | 120 | Yes | Yes | |||
| Oussedik [47] | 2010 | 11 | 11 | 100 | 66 | 105.7 | 81.6 | Yes | Yes | |
| Klouche [48] | 2012 | 38 | 38 | 100 | 24 | 61 | 35 | No | No | |
| Zeller [49] | 2014 | 157 | 149 | 94.9 | 28.1 | 66.9 | 41.6 | Yes | No | |
| Jenny [50] | 2014 | 65 | 55 | 84.6 | 36 | 72 | Yes | Yes | ||
| Total | 1208 | 1005 | - | - | - | |||||
| Minimum | 11 | - | 75 | 24.0 | 61.0 | 35.0 | ||||
| Maximum | 583 | - | 100.0 | 120.0 | 205.2 | 118.8 | ||||
| Mean | 39.5 | - | 83.2 | 40.2 | 109.5 | 66.6 | ||||
| SD* | 38.8 | - | - | 27.9 | 46.9 | 30.4 | ||||
*SD: Standard deviation.
Local antibiotic(s) administration through bone cement appears as the preferred choice of the majority of authors reporting one-stage hip revision surgery. Seven our of the 12 studies included in our analysis disclosed a selection bias, as patients with draining fistula, unknown or multi-resistant pathogen(s) or immunocompromised hosts were excluded (cf. Table 1).
We found only 3 clinical trials, reporting cemented one-stage revision surgery without the use of local antibiotics. All those studies have been performed in France. Klouche and co-workers were the first to publish a striking 100% infection eradication rate at two years minimum follow-up, in a series of 38 patients [48]. In line with this, few years later, Zeller et al., in a large multi-center cohort study on 157 patients treated with one-stage exchange arthroplasty and twelve weeks of systemic antibiotics and no antibiotics in the cement, showed only two relapses and six new infections, with a cumulative infection control rate of nearly 95% at five years postoperatively [49]. In a more recent study, conducted in the same center [51], an overall infection eradication rate of 95.3% at a minimum two years follow-up was reported in a series of 66 patients treated either with cemented (N=21) or cementless revision prostheses (N=45), without the addition of local antibacterials. Moreover, all of these patients had a fistula at the time of surgery, actively draining in 76% of cases, a condition which is considered by many as a bad prognostic factor and even a contraindication to a one-stage procedure [52] (this study is not included in Table 1, as it does not distinguish between hip and knees).
When pooling together the data of the French studies from Klouche and Zeller (N=195) and comparing them with the results reported by all other authors (N=1013), the difference in average infection control, 95.9% versus 80.7%, is unexpectedly extremely statistically significant, in favor of no local antibiotic administration (p<0.0001). Similar results are obtained even excluding the oldest papers, published before year 1995. In this case, no infection recurrence is observed in 88.9% of 180 patients, a value which is still statistically inferior to the that of Klouche and Zeller (p=0.01).
While this comparison has obvious methodological limits, as it considers different patients’ populations across various centers, with possible bias and heterogeneous material, it adds to the fact that, on the basis of the available literature, there is no clinical evidence that delivering local antimicrobials through PMMA is necessary in single-stage hip revision surgery. Hence, more than four decades after its first description, the use of antibiotic-loaded bone cement appears to remain largely based on experts’ opinion and on data obtained in pre-clinical studies or comparative clinical trials in other settings [53].
3. The role of local antibacterial protection in cementless one-stage hip revision surgery
For various reasons, cementless fixation of hip implants is currently the predominant choice of surgeons, according to the UK National Joint Register [https://reports.njrcentre.org.uk/AR-Executive-Summary] and to the Swedish register [54], even if it has not been proven superior to cement in a recent systematic review [55].
Cementless one-stage revision to treat peri-prosthetic hip infection is also gaining more and more acceptance worldwide in recent years. In fact, the largest series on cemented one-stage hip revision surgery date back from four to one decade ago, while in the last 20 years a growing number of papers reporting on cementless one-stage reimplantation can be found (cf. Table 2).
Seventeen observational studies reporting on delayed peri-prosthetic hip infection, treated with cementless one-stage revision, for a total of 521 patients were retrieved by our search. No randomized, prospective controlled trial, comparing different cementless one-stage techniques could be found. The majority of papers described retrospective series, without a control group (Level of evidence: IV). The number of cases ranged from 5 to 111 (mean 30.6, ± 25.0). Overall, at an average follow-up of 65.5 ± 22.5 months (range 24 to 78 months), infection control was obtained in 90.0% of the cases (range 56.8% - 100%)(Table 2).
Table 2.
Data from studies reporting cementless one-stage hip revision surgery for delayed (> 6 weeks after surgery) peri-prosthetic hip infection, at a minimum follow-up of 24 months.
Table 2.
Data from studies reporting cementless one-stage hip revision surgery for delayed (> 6 weeks after surgery) peri-prosthetic hip infection, at a minimum follow-up of 24 months.
| Author | Year | Number of patients | Number of patients free from infection at follow-up | Percent of patients free from infection at follow-up | Follow-up (months) | Selection bias | Local antimicrobial protection | ||
| Min | Max | Mean | |||||||
| Garcia [56] | 2004 | 7 | 7 | 100 | 24 | No | No | ||
| Rudelli [57] | 2008 | 32 | 30 | 93.8 | 63 | 183 | 103 | Not reported | No |
| Winkler [58] | 2008 | 37 | 34 | 91.9 | 24 | 96 | 52.8 | Yes | Antibiotic-loaded allografts |
| Yoo [59] | 2009 | 12 | 10 | 83.3 | 39.6 | 135.6 | 86.4 | Yes | No |
| Wolf [60] | 2014 | 37 | 21 | 56.8 | 24 | No | No | ||
| Bori [61] | 2014 | 24 | 23 | 95.8 | 25 | 94 | 45 | Yes | No |
| Li [62] | 2015 | 6 | 6 | 100.0 | 78 | 187.2 | 103.2 | Yes | No |
| Born [63] | 2016 | 28 | 28 | 100.0 | 24 | 180 | 84 | Yes | No |
| Ebied [64] | 2016 | 33 | 32 | 97.0 | 48 | 96 | 60 | Yes | Antibiotic-loaded allografts |
| Whiteside [65] | 2017 | 21 | 20 | 95.2 | 25 | 157 | 63 | No | Intra-articular antibiotic infusion |
| Lange [66] | 2018 | 56 | 51 | 91.1 | 24 | 48 | No | Gentamicin collagen fleece | |
| Capuano [67] | 2018 | 5 | 5 | 100.0 | 24 | 36 | 29.3 | No | Antibiotic-loaded hydrogel coating |
| Ji [68] | 2019 | 111 | 99 | 89.2 | 24 | 107 | 58 | No | Vancomicin or Imipenem powder and intra-articular antibiotic infusion |
| Pellegrini [69] | 2021 | 10 | 10 | 100.0 | 24 | 60 | 37.2 | Yes | Antibiotic-loaded hydrogel coating |
| Ji [70] | 2022 | 29 | 26 | 89.7 | 24 | 133 | 85 | No | Intra-articular antibiotic infusion |
| Dersch [71] | 2022 | 38 | 35 | 92.1 | 24 | 187.2 | 67.2 | Yes | Antibiotic-loaded allografts |
| Mangin [72] | 2023 | 35 | 32 | 91.4 | 24 | 132 | 60 | Yes | No |
| Total | 521 | 469 | - | - | - | ||||
| Minimum | 5 | - | 56.8 | 24.0 | 36.0 | 29.3 | |||
| Maximum | 111 | - | 100.0 | 78 | 187.2 | 103.2 | |||
| Mean | 30.6 | - | 90.0 | 31.9 | 127.4 | 65.5 | |||
| SD* | 25.0 | - | - | 16.2 | 48.4 | 22.5 | |||
*SD: Standard deviation.
Eight studies reported one-stage cementless revision without the use of local antibiotics. Among these, 5 reported a selection bias, excluding patients with open fistulas and/or severe bone loss and/or unknown or multi-resistant pathogen(s) or immunocompromised hosts. Moreover, Bori et al. [61] and Born et al. [63] did report the use of antibiotic-loaded cemented cups in some cases, while Yoo et al. [59] performed only cup revision in 4 patients out of the 12 treated. Pooling the results of all studies reporting no local antibiotic administration together (N=181), an average infection control of 86.7% (range 56.8% - 100%), at a mean follow-up of 80.3 ± 23.4 months, can be calculated (cf. Table 3).
The remaining nine studies reported the results on four different local antibiotic delivery techniques, which, on the average, provided the following no infection recurrence rates: intra-articular post-operative antibiotic infusion or local antibiotic vancomicin powder application at the time of surgery: 90.1%; antibiotic-loaded collagen-fleece: 91.1%; antibiotic-impregnated allografts: 93.5%; antibiotic-loaded hydrogel coating: 100% (cf. Table 3).Three studies excluded patients with open fistulas, unknown or multi-resistant pathogen(s) or immunocompromised hosts (cf. Table 2). No side effects were reported with the use of any local antibacterial technology. Due to the relative low number of patients, no statistical difference could be demonstrated (p > 0.05) by single or pooled together local antimicrobial protection systems, compared to no local antibiotic application.
Table 3.
Local antibacterial protection and infection recurrence for one-stage cementless hip revision: pooled results.
Table 3.
Local antibacterial protection and infection recurrence for one-stage cementless hip revision: pooled results.
| Local antibacterial protection | Number of patients | Number of patients free from infection at follow-up | Percent of patients free from infection at follow-up (mean, min, max) | Follow-up (months) (mean and SD*) |
|---|---|---|---|---|
| None [56,57,59,60,61,62,63,72] | 181 | 157 | 86.7 (56.8-100) | 80.3 ± 23.4 |
| Intra-articular antibiotic infusion or local antibiotic vancomicin powder [65,68,70] | 161 | 145 | 90.1 (89.2-95.2) | 68.7 ± 14.4 |
| Gentamicin-loaded collagen fleece [66] | 56 | 51 | 91.1 | 48 |
| Antibiotic-loaded allografts [58,64,71] | 108 | 101 | 93.5 (91.9-92.1) | 60.0 ± 7.2 |
| Antibiotic-loaded hydrogel coating [67,69] | 15 | 15 | 100.0 | 30.1 ± 6.8 |
*SD: Standard deviation.
One study [73] reported the results of single-stage cementless revision surgery without local antibiotic delivery for the treatment of early infections (< 6 weeks after implant); this report showed a remarkably low infection control (56% or 15/27 patients), at a mean follow-up of 50 months (range, 27-89 months). This observation compares to a similar one, conducted by Riemer and co-workers, that, with the use of gentamicin-loaded collagen fleece, reported successful implant retention at mean follow-up of 60 months in 18/18 patients [74].
3. Discussion
In this review we addressed the relative role of antibacterial local protection in one-stage cemented or cementless revision surgery for peri-prosthetic hip infection.
While this analysis does confirm previous observations concerning cementless one-stage hip revision success rates similar or even superior to that of cemented implants [6,75,76], the reviewed data do not support conclusively the need of local antibiotic delivery for periprosthetic infection control.
In particular, our findings challenge the superiority of antibiotic-loaded cemented one-stage hip revision surgery and contradicts the traditional prescription of antibiotic-loaded bone cement as a key factor to perform a successful one-stage hip revision surgery [8,77]. In the lack of comparative trials, this is mainly due to the French experience, reported by Klouche, Zeller and co-workers [10,48,49]. Further analysing those, data in light of the current knowledge regarding biofilms and bacterial adhesion capabilities, it appears evident the limit of bone cement as a local antibacterial implant protection system. In fact, antibiotic-loaded bone cement is only applied to the interface between the cup and/or the stem of the prosthesis, leaving all the extramedullary and the modular parts of the implant unprotected. This technical limit may not be overcome unless antibiotic-loaded bone cement is used in combination with other technologies able to protect also the uncemented parts of the prosthesis. Moreover, not all the antibiotic-loaded bone cements are the same and do provide the same antibiotic elution. Manual mixing of antibiotics to PMMA has been shown to provide significantly different release of various antibacterial, compared to pre-manufacture antibiotic-loaded bone cement [78]. Single or combinations of antibiotics, their relative concentration in bone cement and the porosity of PMMA are some of the many factors that come into play and determine the effective pharmacokinetic of the local antibiotic administration [79,80]. Finally, biofilms and small colony variants of bacteria have been retrieved in antibiotic-loaded bone cement [81,82], witnessing the ability of bacteria to overcome even local antibiotic protection, if favourable conditions to their persistence are met. The lack of a standard for local antibiotic administration though bone cement may well explain, among other factors, the wide range of results reported in the literature.
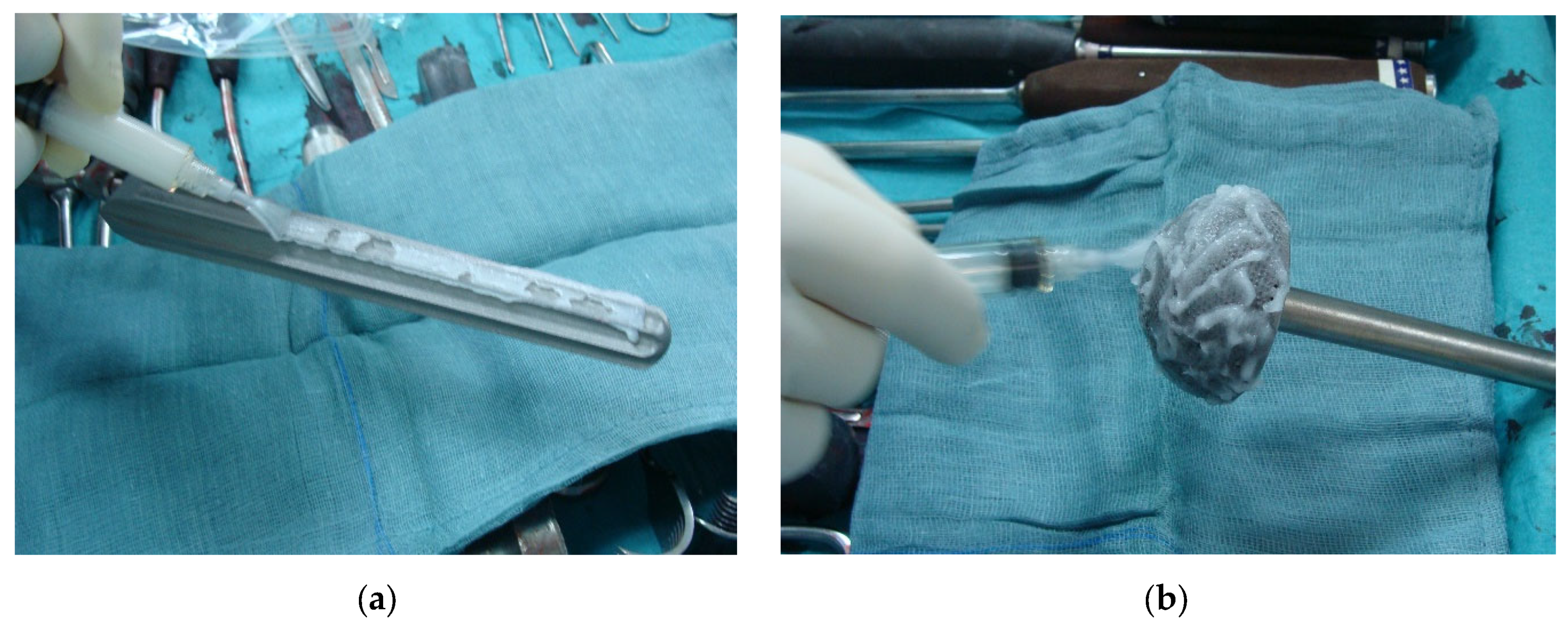
On the other side, our review reveals that also one-stage cementless hip revision surgery with local antibacterial protection has not been proven more effective that without in comparative clinical trials; moreover, when pooling together the results of single or combined local antibacterial protection strategies, no statistically significant difference in infection control can be demonstrated, compared to one-stage cementless hip revision without the use of local antibacterials. However, our results concerning the efficacy of local antibacterial protection in this setting should be interpreted with caution, due to many limitations of the material available for our analysis. First of all, the number of patients treated with each local antibacterial modality is quite low and heterogeneous, thus reducing the validity of the comparison of results. Additionally, pooling together the results of the patients treated with different local antimicrobial strategies can be questionable, as those chosen by the different authors were completely different one from the other, both as to concern the type of treatment and the site of application. As an example, while the antibiotic-loaded hydrogel coating may be applied to all the implant surfaces and components (cf. Figure 1), vancomycin powder, local antibiotic irrigation and other technologies may not. This may have a strong impact on the final outcome, as it is well known that the primary step of bacteria colonizing an implant is to attach to the inert surfaces of the biomaterials and immediately start forming the biofilms [83].
If the implant surface is effectively protected by an antibacterial coating, several in vivo and clinical studies have shown to be extremely effective in preventing implant-related infection development [84,85,86]. Moreover, while most of the proposed solutions to provide local antimicrobial protection did act at the very time of surgery, others, like local antibiotic irrigation, may only take effect after surgery, when the bacteria eventually present in the surgical field had the time to attach to the implant and hence become difficult to be reached by intra-wound irrigation.
Moreover, it is worth noting that 5 out of 8 studies, reporting on one-stage treatment without local antibacterials, have been performed on selected patients with less severe infection, minor bone involvement and better hosts. In the only direct comparison between a single- and two-stage exchange, Wolf et al. [60] showed a mean infection control exceeding 96% after two-stage, compared to less than 57% after cementless single-stage without the use of local antibiotic protection. Further analysing the data, the authors provide evidence that the difference between the two treatments was due to the better results obtained with a two-stage approach in more compromised hosts, while one-stage and two-stage did perform equally well, when normal hosts and early infections were involved. Selection bias is also a well know limit when comparing the results of one-stage procedure with two-stage, as many authors prefer a staged approach to manage the most complicated cases and inevitably most of the retrospective series reported on one-stage include less severe patients’ populations [87].
Another limitation of the present review is that it did not explore how patient factors such as co-existing conditions, age, body mass index, gender, type of implant, prior surgeries, etc., might influence the outcomes. It also did not assess different surgical approaches including the type of hip revision prosthesis, the surgical technique, or the need for bone grafts. The role of the pathogen(s) and their antibiotic resistance profile was also not investigated, as that of systemic antibiotic administration and the use of single or dual local antibiotics. Furthermore, our analysis did not distinguish between cases of infection recurrence due to the same or to a different pathogen. Finally, comparison of historical studies with the most recent ones can be biased, as across the years the diagnostics and even the definition itself of peri-prosthetic joint infection has evolved and changed several times.
Its main limitations notwithstanding, this review shows that single-stage exchange arthroplasty is a viable option for the treatment of chronic periprosthetic hip infections. Local antibacterial treatment is safe, even if its superiority over no local antimicrobial protection is not proven. The fact that, with the current data available, is not possible to prove the clinical benefit of local antibacterial protection for one-stage hip revision surgery for the treatment of peri-prosthetic infection has a clear impact on research, clinical and medico-legal aspects. This also may ground the ethical basis for designing prospective comparative studies with and without local antibacterial protection. In fact, the limitations and biases in current literature underscore the need for large-scale, multicentre, prospective, randomized trials to definitively determine the real impact of local antibacterial implant protection, if any. Even if logistical challenges such as the low incidence of the disease, small patient populations, long-term follow-up requirements, and variations in microorganisms make conducting such studies exceptionally difficult, such studies are possible and have been performed successfully in other clinical settings [88,89].
Author Contributions
Conceptualization, C.R.; methodology, C.R., H.D.S., M.T.; formal analysis, L.B., G.B.; investigation, C.R., L.B., G.B.; writing—original draft preparation, C.R.; writing—review and editing, C.R., H.D.S., M.T.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
CR is co-inventor and receives royalties from Novagenit Srl, the company producing the DAC antibacterial hydrogel coating. The remaining authors declare that they have no competing interests.
References
- Dobson PF, Reed MR. Prevention of infection in primary THA and TKA. EFORT Open Rev. 2020 Oct 26;5(10):604-613. [CrossRef]
- Day CW, Costi K, Pannach S, Atkins GJ, Hofstaetter JG, Callary SA, Nelson R, Howie DW, Solomon LB. Long-Term Outcomes of Staged Revision Surgery for Chronic Periprosthetic Joint Infection of Total Hip Arthroplasty. J Clin Med. 2021 Dec 27;11(1):122. [CrossRef]
- Lenguerrand E, Whitehouse MR, Beswick AD, Kunutsor SK, Webb JCJ, Mehendale S, Porter M, Blom AW; National Joint Registry for England, Wales, Northern Ireland, the Isle of Man, and the States of Guernsey. Mortality and re-revision following single-stage and two-stage revision surgery for the management of infected primary hip arthroplasty in England and Wales. Bone Joint Res. 2023 May 9;12(5):321-330. [CrossRef]
- Blom AW, Lenguerrand E, Strange S, Noble SM, Beswick AD, Burston A, Garfield K, Gooberman-Hill R, Harris SRS, Kunutsor SK, Lane JA, MacGowan A, Mehendale S, Moore AJ, Rolfson O, Webb JCJ, Wilson M, Whitehouse MR; INFORM trial group. Clinical and cost effectiveness of single stage compared with two stage revision for hip prosthetic joint infection (INFORM): pragmatic, parallel group, open label, randomised controlled trial. BMJ. 2022 Oct 31;379:e071281. [CrossRef]
- Svensson K, Rolfson O, Kärrholm J, Mohaddes M. Similar Risk of Re-Revision in Patients after One- or Two-Stage Surgical Revision of Infected Total Hip Arthroplasty: An Analysis of Revisions in the Swedish Hip Arthroplasty Register 1979⁻2015. J Clin Med. 2019 Apr 10;8(4):485. [CrossRef]
- George DA, Logoluso N, Castellini G, Gianola S, Scarponi S, Haddad FS, Drago L, Romano CL. Does cemented or cementless single-stage exchange arthroplasty of chronic periprosthetic hip infections provide similar infection rates to a two-stage? A systematic review. BMC Infect Dis. 2016 Oct 10;16(1):553. [CrossRef]
- Zahar A, Gehrke TA. One-Stage Revision for Infected Total Hip Arthroplasty. Orthop Clin North Am. 2016 Jan;47(1):11-8. [CrossRef]
- Buchholz HW, Elson RA, Heinert K. Antibiotic-loaded acrylic cement: current concepts. Clin Orthop Relat Res. :1984: 96–108.
- Wroblewski BM. One-stage revision of infected cemented total hip arthroplasty. Clin Orthop Relat Res. :1986: 103–107.
- Zeller V, Lhotellier L, Marmor S, Leclerc P, Krain A, Graff W, Ducroquet F, Biau D, Leonard P, Desplaces N, Mamoudy P. One-stage exchange arthroplasty for chronic periprosthetic hip infection: results of a large prospective cohort study. J Bone Joint Surg Am. 2014;96:e1. [CrossRef]
- Callaghan JJ, Katz RP, Johnston RC. One-stage revision surgery of the infected hip. A minimum 10-year followup study. Clin Orthop Relat Res. :1999: 139–143. [CrossRef]
- Ure KJ, Amstutz HC, Nasser S, Schmalzried TP (1998) Direct exchange arthroplasty for the treatment of infection after total hip replacement. An average ten-year follow-up. J Bone Joint Surg Am 80:961–968.
- Gehrke T, Zahar A, Kendoff D. One-stage exchange: it all began here. Bone Joint J. 2013;95-B:77–83.
- Lum ZC, Holland CT, Meehan JP. Systematic review of single stage revision for prosthetic joint infection. World J Orthop. 2020 Dec 18;11(12):559-572. [CrossRef]
- Gehrke T, Kendoff D. Peri-prosthetic hip infections: in favour of one-stage. Hip Int. 2012;22 Suppl 8:S40–S45. [CrossRef]
- Luu, A., Syed, F., Raman, G., Bhalla, A., Muldoon, E., Hadley, S., et al. (2013). Two-stage arthroplasty for prosthetic joint infection: a systematic review of acute kidney injury, systemic toxicity and infection control. J. Arthroplasty 149, e1. [CrossRef]
- Salvati, E. A., Callaghan, J. J., Brause, B. D., Klein, R. F., and Small, R. D. (1986). Reimplantation in infection. elution of gentamicin from cement and beads. Clin. Orthop. Relat. Res. 83–93.
- Walenkamp, G. H. (2007). “Antibiotic loaded cement: from research to clinical evidence,” in Infection and Local Treatment in Orthopedic Surgery, ed. E. Meani (Berlin: Springer), 170–175. [CrossRef]
- Sanz-Ruiz, P., Villanueva-Martinez, M., and Berberich, C. (2018b). “Benefit and risks of anti biotic-loaded bone cements,” in Management of Periprosthetic Joint Infection, ed. D. Kuhn (Heidelberg: Springer-Verlag), 217–218.
- Kendoff DO, Gehrke T, Stangenberg P, Frommelt L, Bösebeck H. Bioavailability of gentamicin and vancomycin released from an antibiotic containing bone cement in patients undergoing a septic one-stage total hip arthroplasty (THA) revision: a monocentric open clinical trial. Hip Int. 2016 Jan-Feb;26(1):90-6. [CrossRef]
- Miclau, T., Edin, M. L., Lester, G. E., Lindsey, R. W., and Dahners, L. E. (1995). Bone toxicity of locally applied aminoglycosides. J. Orthop. Trauma 9, 401–406. [CrossRef]
- Edin, M. L., Miclau, T., Lester, G. E., Lindsey, R. W., and Dahners, L. E. (1996). Effect of cefazolin and vancomycin on osteoblasts in vitro. Clin. Orthop. Relat. Res. 333, 245–251. [CrossRef]
- Isefuku, S., Joyner, C. J., and Simpson, A. H. (2003). Gentamicin may have an adverse effect on osteogenesis. J. Orthop. Trauma. 17, 212–216. [CrossRef]
- Hansen, E. N., Adeli, B., Kenyon, R., and Parvizi, J. (2014). Routine use of antibiotic laden bone cement for primary total knee arthroplasty: impact on infecting microbial patterns and resistance profiles. J. Arthroplasty. 29, 1123–1127. [CrossRef]
- Tootsi K, Heesen V, Lohrengel M, Enz AE, Illiger S, Mittelmeier W, Lohmann CH. The use of antibiotic-loaded bone cement does not increase antibiotic resistance after primary total joint arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2022 Sep;30(9):3208-3214. [CrossRef]
- Schmitt DR, Killen C, Murphy M, Perry M, Romano J, Brown N. The Impact of Antibiotic-Loaded Bone Cement on Antibiotic Resistance in Periprosthetic Knee Infections. Clin Orthop Surg. 2020 Sep;12(3):318-323. [CrossRef]
- Sabater-Martos M, Verdejo MA, Morata L, Muñoz-Mahamud E, Guerra-Farfan E, Martinez-Pastor JC, Soriano A. Antimicrobials in polymethylmethacrylate: from prevention to prosthetic joint infection treatment: basic principles and risk of resistance. Arthroplasty. 2023 Mar 2;5(1):12. [CrossRef]
- Xu T, Wu KL, Jie K. Comprehensive meta-analysis of antibiotic-impregnated bone cement versus plain bone cement in primary total knee arthroplasty for preventing periprosthetic joint infection. Chin J Traumatol. 2022 Nov;25(6):325-330. [CrossRef]
- Opalko M, Bösebeck H, Vogt S. Properties and clinical application safety of antibiotic-loaded bone cement in kyphoplasty. J Orthop Surg Res. 2019 Jul 27;14(1):238. [CrossRef]
- Blersch BP, Sax FH, Mederake M, Benda S, Schuster P, Fink B. Effect of Multiantibiotic-Loaded Bone Cement on the Treatment of Periprosthetic Joint Infections of Hip and Knee Arthroplasties-A Single-Center Retrospective Study. Antibiotics (Basel). 2024 Jun 3;13(6):524. [CrossRef]
- van Vugt TAG, Arts JJ, Geurts JAP. Antibiotic-Loaded Polymethylmethacrylate Beads and Spacers in Treatment of Orthopedic Infections and the Role of Biofilm Formation. Front Microbiol. 2019 Jul 25;10:1626. [CrossRef]
- Langlais F. Ciments orthopédiques aux antibiotiques: du laboratoire a la validation clinique [Antibiotic-loaded bone cements: from laboratory studies clinical evaluation]. Bull Acad Natl Med. 2004;188(6):1011-22.
- Cara A, Ferry T, Laurent F, Josse J. Prophylactic Antibiofilm Activity of Antibiotic-Loaded Bone Cements against Gram-Negative Bacteria. Antibiotics (Basel). 2022 Jan 21;11(2):137. [CrossRef]
- Nijhof MW, Stallmann HP, Vogely HC, Fleer A, Schouls LM, Dhert WJ, Verbout AJ. Prevention of infection with tobramycin-containing bone cement or systemic cefazolin in an animal model. J Biomed Mater Res. 2000 Dec 15;52(4):709-15.
- Nijhof MW, Fleer A, Hardus K, Vogely HC, Schouls LM, Verbout AJ, Dhert WJ. Tobramycin-containing bone cement and systemic cefazolin in a one-stage revision. Treatment of infection in a rabbit model. J Biomed Mater Res. 2001;58(6):747-53. [CrossRef]
- Jenny JY, Hamon M, Klein S, Reiter-Schatz A, Rondé-Oustau C, Boéri C, Wisniewski S, Gaudias J. Cement Loaded With High-Dose Gentamicin and Clindamycin Reduces the Risk of Subsequent Infection After One-Stage Hip or Knee Arthroplasty Exchange for Periprosthetic Infection: A Preliminary Study. J Arthroplasty. 2021 Dec;36(12):3973-3978. [CrossRef]
- Szymski D, Walter N, Krull P, Melsheimer O, Lang S, Grimberg A, Alt V, Steinbrück A, Rupp M. The Prophylactic Effect of Single vs. Dual Antibiotic-Loaded Bone Cement against Periprosthetic Joint Infection Following Hip Arthroplasty for Femoral Neck Fracture: An Analysis of the German Arthroplasty Registry. Antibiotics (Basel). 2023 Apr 8;12(4):732. [CrossRef]
- Sprowson A.P., Jensen C., Chambers S., Parsons N.R., Aradhyula N.M., Carluke I., Inman D., Reed M.R. The Use of High-Dose Dual-Impregnated Antibiotic-Laden Cement with Hemiarthroplasty for the Treatment of a Fracture of the Hip. Bone Jt. J. 2016;98-B:1534–1541. [CrossRef]
- Buchholz H, Elson R, Engelbrecht E, Lodenkamper H, Rottger J, Siegel A: Management of deep infection of total hip replacement. J Bone Joint Surg 1981, 63-B(3):342-353.
- Miley GB, Scheller AD, Turner RH: Medical and surgical treatment of the septic hip with one-stage revision arthroplasty. Clin Orthop Relat Res 1982, 170(76-82).
- Wroblewski BM. One-stage revision of infected cemented total hip arthroplasty. Clin Orthop Relat Res. 1986 Oct;(211):103-7. [CrossRef]
- Sanzen L, Carlsson A, Josefsson G, Lindberg LT: Revision operations on infected total hip arthroplasties. Clin Orthop Relat Res 1988, 229:165-172.
- Raut VV, Siney PD, Wroblewski BM. One-stage revision of infected total hip replacements with discharging sinuses. J Bone Joint Surg Br. 1994 Sep;76(5):721-4.
- Mulcahy DM, O’Byrne JM, Fenelon GE. One stage surgical management of deep infection of total hip arthroplasty. Ir J Med Sci. 1996 Jan-Mar;165(1):17-9. [CrossRef]
- Ure KJ, Amstutz HC, Nasser S, Schmalzried TP. Direct-exchange arthroplasty for the treatment of infection after total hip replacement. An average ten-year follow-up. J Bone Joint Surg Am. 1998;80:961–968. [CrossRef]
- Callaghan JJ, Katz RP, Johnston RC. One-stage revision surgery of the infected hip. A minimum 10-year followup study. Clin Orthop Relat Res 1999 Dec;369: 139-43. [CrossRef]
- Oussedik SI, Dodd MB, Haddad FS: Outcomes of revision total hip replacement for infection after grading according to a standard protocol. J Bone Joint Surg 2010, 92-B(9):1222-1226.
- Klouche S1, Leonard P, Zeller V, Lhotellier L, Graff W, Leclerc P, Mamoudy P, Sariali E. Infected total hip arthroplasty revision: one- or two-stage procedure? Orthop Traumatol Surg Res. 2012 Apr;98(2):144-50. Epub 2012 Feb 24. [CrossRef]
- Zeller V, Lhotellier L, Marmor S, Leclerc P, Krain A, Graff W, Ducroquet F, Biau D, Leonard P, Desplaces N, Mamoudy P. One-stage exchange arthroplasty for chronic periprosthetic hip infection: results of a large prospective cohort study. J Bone Joint Surg Am. 2014 Jan 1;96(1):e1. [CrossRef]
- Jenny JY, Lengert R, Diesinger Y, Gaudias J, Boeri C, Kempf JF. Routine one-stage exchange for chronic infection after total hip replacement. Int Orthop. 2014 Dec;38(12):2477-81. [CrossRef]
- Marmor S, Kerroumi Y, Meyssonnier V, Lhotellier L, Mouton A, Graff W, Zeller V. One-Stage Exchange Arthroplasty for Fistulizing Periprosthetic Joint Infection of the Hip: An Effective Strategy. Front Med (Lausanne). 2020 Oct 16;7:540929. [CrossRef]
- Parvizi J, Gehrke T, Chen AF. Proceedings of the International Consensus on Periprosthetic Joint Infection. Bone Joint J. 2013 Nov;95-B(11):1450-2. [CrossRef]
- Manning L, Bori G, Klement MR. Does the Use of Cemented or Cementless Components at the Time of Reimplantation Affect the Success of Treating Chronic Periprosthetic Joint Infections (pjis)? If Yes, What Is the Optimal Antibiotic(s), Dosage and Cement to Maximize Antibiotic Delivery and Mechanical Properties of the Cement? International Consensus Meeting (icm) on Orthopaedic Infections. (2018). Available online at: https://icmphilly.com/questions/does-the-use-of-cemented-or-cementless-components-at-the-time-of-reimplantation-affect-the-success-of-treating-chronic-periprosthetic-joint-infections-pjis-if-yes-what-is-the-optimal-antibiotic/ (accessed 2024).
- Scanlon CM, Gemayel AC, Buehring W, Slover JD, Malchau H. Are current rates of uncemented fixation in total hip arthroplasty supported by the literature? An update on the uncemented paradox. Hip Int. 2024 May 3:11207000241249673. [CrossRef]
- Elbardesy H, Anazor F, Mirza M, Aly M, Maatough A. Cemented versus uncemented stems for revision total hip replacement: A systematic review and meta-analysis. World J Orthop. 2023 Aug 18;14(8):630-640. [CrossRef]
- García S, Soriano A, Esteban P, Almela M, Gallart X, Mensa J. Utilidad de la adición de antibiótico al cemento en el recambio en 1 tiempo en la infección crónica de una prótesis total de cadera [Usefulness of adding antibiotic to cement in one stage exchange of chronic infection in total hip arthroplasty]. Med Clin (Barc). 2005 Jun 25;125(4):138-9.
- Rudelli S, Uip D, Honda E, Lima AL. One-stage revision of infected total hip arthroplasty with bone graft. J Arthroplasty 2008;23(8):1165-77. [CrossRef]
- Winkler H, Stoiber A, Kaudela K, Winter F, Menschik F. One stage uncemented revision of infected total hip replacement using cancellous allograft bone impregnated with antibiotics. J Bone Joint Surg Br 2008;90(12):1580-4. [CrossRef]
- Yoo JJ, Kwon YS, Koo KH, Yoon KS, Kim YM, Kim HJ. One-stage cementless revision arthroplasty for infected hip replacements. Int Orthop. 2009;33(5):1195-1201. [CrossRef]
- Wolf M, Clar H, Friesenbichler J, et al. Prosthetic joint infection following total hip replacement: results of one-stage versus two-stage exchange. Int Orthop 2014;38(7):1363–1368. [CrossRef]
- Bori G, Muñoz-Mahamud E, Cuñé J, Gallart X, Fuster D, Soriano A. One-Stage Revision Arthroplasty Using Cementless Hip Arthroplasties. J Arthroplasty 2014;29:1076–1081.
- Li P, Hou M, Zhu ZQ, Shi ZJ. Cementless Revision for Infected Hip Arthroplasty: an 8.6 Years Follow-up. Orthopaedic surgery. 2015;7(1):37-42. [CrossRef]
- Born P, Ilchmann T, Zimmerli W, Zwicky L, Graber P, Ochsner PE, Clauss M. Eradication of infection, survival, and radiological results of uncemented revision stems in infected total hip arthroplasties. Acta Orthop. 2016 Dec;87(6):637-643. [CrossRef]
- Ebied AM, Elseedy AI, Gamal O. Single-stage revision for periprosthetic hip infection using antibiotic loaded impaction graft. Hip Int. 2016 Nov 10;26(6):573-579. [CrossRef]
- Whiteside LA, Roy ME. One-stage Revision With Catheter Infusion of Intraarticular Antibiotics Successfully Treats Infected THA. Clin Orthop Relat Res. 2017 Feb;475(2):419-429. [CrossRef]
- Lange J, Troelsen A, Solgaard S, Otte KS, Jensen NK, Søballe K; CORIHA Research Group. Cementless One-Stage Revision in Chronic Periprosthetic Hip Joint Infection. Ninety-One Percent Infection Free Survival in 56 Patients at Minimum 2-Year Follow-Up. J Arthroplasty. 2018 Apr;33(4):1160-1165.e1. [CrossRef]
- Capuano N, Logoluso N, Gallazzi E, Drago L, Romanò CL. One-stage exchange with antibacterial hydrogel coated implants provides similar results to two-stage revision, without the coating, for the treatment of peri-prosthetic infection. Knee Surg Sports Traumatol Arthrosc. 2018 Nov;26(11):3362-3367. [CrossRef]
- Ji B, Wahafu T, Li G, Zhang X, Wang Y, Momin M, Cao L. Single-stage treatment of chronically infected total hip arthroplasty with cementless reconstruction: results in 126 patients with broad inclusion criteria. Bone Joint J. 2019 Apr;101-B(4):396-402.
- Pellegrini A, Legnani C. High rate of infection eradication following cementless one-stage revision hip arthroplasty with an antibacterial hydrogel coating. Int J Artif Organs. 2022 Jan;45(1):113-117. [CrossRef]
- Ji B, Li G, Zhang X, Xu B, Wang Y, Chen Y, Cao L. Effective single-stage revision using intra-articular antibiotic infusion after multiple failed surgery for periprosthetic joint infection : a mean seven years’ follow-up. Bone Joint J. 2022 Jul;104-B(7):867-874.
- Dersch G, Winkler H. Periprosthetic Joint Infection (PJI)-Results of One-Stage Revision with Antibiotic-Impregnated Cancellous Allograft Bone-A Retrospective Cohort Study. Antibiotics (Basel). 2022 Feb 25;11(3):310. [CrossRef]
- Mangin M, Aouzal Z, Leclerc G, Sergent AP, Bouiller K, Patry I, Garbuio P. One-stage revision hip arthroplasty for infection using primary cementless stems as first-line implants: About 35 cases. Orthop Traumatol Surg Res. 2023 Nov;109(7):103642. [CrossRef]
- Hansen E, Tetreault M, Zmistowski B, Della Valle CJ, Parvizi J, Haddad FS, Hozack WJ. Outcome of one-stage cementless exchange for acute postoperative periprosthetic hip infection. Clin Orthop Relat Res. 2013 Oct;471(10):3214-22. [CrossRef]
- Riemer K, Lange J. Early periprosthetic hip joint infection managed by cementless one-stage revision - a case series. J Bone Jt Infect. 2022 Feb 25;7(1):43-50. [CrossRef]
- Thakrar RR, Horriat S, Kayani B, Haddad FS. Indications for a single-stage exchange arthroplasty for chronic prosthetic joint infection: a systematic review. Bone Joint J. 2019 Jan;101-B(1_Supple_A):19-24.
- Lum ZC, Holland CT, Meehan JP. Systematic review of single stage revision for prosthetic joint infection. World J Orthop. 2020 Dec 18;11(12):559-572. [CrossRef]
- Carlsson AS, Josefsson G, Lindberg L. Revision with gentamicin-impregnated cement for deep infections in total hip arthroplasties. J Bone Joint Surg Am. 1978;60(8):1059–1064. [CrossRef]
- Wall V, Nguyen TH, Nguyen N, Tran PA. Controlling Antibiotic Release from Polymethylmethacrylate Bone Cement. Biomedicines. 2021 Jan 1;9(1):26. [CrossRef]
- Macaulay W, DiGiovanni CW, Restrepo A, Saleh KJ, Walsh H, Crossett LS, Peterson MG, Li S, Salvati EA. Differences in bone-cement porosity by vacuum mixing, centrifugation, and hand mixing. J Arthroplasty. 2002 Aug;17(5):569-75. [CrossRef]
- Gálvez-López R, Peña-Monje A, Antelo-Lorenzo R, Guardia-Olmedo J, Moliz J, Hernández-Quero J, Parra-Ruiz J. Elution kinetics, antimicrobial activity, and mechanical properties of 11 different antibiotic loaded acrylic bone cement. Diagn Microbiol Infect Dis. 2014 Jan;78(1):70-4. [CrossRef]
- Bertazzoni Minelli E, Della Bora T, Benini A. Different microbial biofilm formation on polymethylmethacrylate (PMMA) bone cement loaded with gentamicin and vancomycin. Anaerobe. 2011 Dec;17(6):380-3. [CrossRef]
- Ensing GT, van Horn JR, van der Mei HC, Busscher HJ, Neut D. Copal bone cement is more effective in preventing biofilm formation than Palacos R-G. Clin Orthop Relat Res. 2008 Jun;466(6):1492-8. [CrossRef]
- Ul Haq I, Khan TA, Krukiewicz K. Etiology, pathology, and host-impaired immunity in medical implant-associated infections. J Infect Public Health. 2024 Feb;17(2):189-203. [CrossRef]
- Lu Y, Cai WJ, Ren Z, Han P. The Role of Staphylococcal Biofilm on the Surface of Implants in Orthopedic Infection. Microorganisms. 2022 Sep 26;10(10):1909. [CrossRef]
- Akay S, Yaghmur A. Recent Advances in Antibacterial Coatings to Combat Orthopedic Implant-Associated Infections. Molecules. 2024 Mar 6;29(5):1172. [CrossRef]
- Onorato F, Masoni V, Gagliardi L, Comba LC, Rivera F. What to Know about Antimicrobial Coatings in Arthroplasty: A Narrative Review. Medicina (Kaunas). 2024 Mar 30;60(4):574. [CrossRef]
- Jamsen E, Stogiannidis J, Malmivaara A, Pajamaki J, Puolakka T, Konttinen YT. Outcome of prosthesis exchange for infected knee arthroplasty: the effect of treatment approach. A systematic review of the literature. Acta Orthopaedica 2009;80(1):67–77. [CrossRef]
- Romanò CL, Malizos K, Capuano N, Mezzoprete R, D’Arienzo M, Van Der Straeten C, Scarponi S, Drago L. Does an Antibiotic-Loaded Hydrogel Coating Reduce Early Post-Surgical Infection After Joint Arthroplasty? J Bone Jt Infect. 2016 Jul 19;1:34-41.
- Malizos K, Blauth M, Danita A, Capuano N, Mezzoprete R, Logoluso N, Drago L, Romanò CL. Fast-resorbable antibiotic-loaded hydrogel coating to reduce post-surgical infection after internal osteosynthesis: a multicenter randomized controlled trial. J Orthop Traumatol. 2017 Jun;18(2):159-169. [CrossRef]
Figure 1.
Application of the DAC antibiotic-loaded hydrogel coating to (a) a cementless hip stem revision prosthesis and (b) to an acetabular cup.
Figure 1.
Application of the DAC antibiotic-loaded hydrogel coating to (a) a cementless hip stem revision prosthesis and (b) to an acetabular cup.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



