
Submitted:
11 July 2024
Posted:
12 July 2024
You are already at the latest version
Abstract
Melanoma, one of the most aggressive forms of skin cancer, is also one of the most diagnosed cancer types. While surgical excision of the lesions is the primary treatment for melanoma, not all cases are candidates for surgical procedures. New treatments and complementary options are necessary, given the increasing diagnosis rate. In the present study, a norcantharidin-containing nanoemulsion was developed and evaluated in vivo using a syngeneic graft murine model. Our model contemplates an amputation surgery simulating the standard treatment and the role of the nanoemulsion as a potential adjuvant therapy. We observed a significant decrease in the growth rate of the melanoma lesion in the treated groups compared to the control group, both at the 20th and 30th days of treatment. Moreover, we evaluated the drug bioavailability in serum samples, and the results showed that norcantharidin was detectable in a range of 0.1 to 0.18 mg per mL in the treated groups. Furthermore, histopathological analysis was performed on the amputated tumors, where significant differences were found regarding size, mitosis rate, lymphocytic infiltration, and multispectral quantitative image analysis compared to the control group. The norcantharidin-containing nanoemulsion could be a potential alternative or adjuvant therapy if more clinical studies are conducted. Topical nanosystems can become or complement standard therapies, which is needed as melanoma affects not only in terms of mortality but also the patient's morbidity and life quality.
Keywords:
melanoma
; nanoemulsion
; nanosystems
; nanotechnology
; norcantharidin
; topical administration
1. Introduction
Melanoma is a malignant neoplasm caused by the uncontrolled growth of the skin's pigment-producing cells, melanocytes [1]. According to the International Agency for Research on Cancer's GLOBOCAN, in 2018, melanoma caused 60,712 deaths, and it is estimated that 466,914 new cases will be diagnosed in 2040 [2]. Melanoma-related mortality is relatively stable with a tendency to increase, but much slower than the incidence [3]. This discrepancy may be due to overdiagnosis, which correlates with an increase in early-stage diagnoses [4]. Furthermore, melanoma-related deaths commonly arise from rapidly progressing melanomas that are rarely detected during screening processes [5]. A favorable prognosis is attained only through early diagnosis, followed by the prompt excision of cutaneous lesions. The clinical ABCD rule is based on four clinical morphologies of melanoma: 1) Asymmetry, 2) Border irregularity, 3) Color variation, and 4) Diameter greater than 6 mm [6]; it has been established as a framework for distinguishing melanomas from benign pigmented skin lesions, forming the basis of current clinical diagnosis. However, melanomas with subtle indications are sometimes mistaken for benign lesions, and conversely, benign lesions are at times misdiagnosed as melanomas, leading to unnecessary biopsies [7]. Surgical excision offers a convenient therapeutic approach and, when viable, continues to represent the established standard of care. Subsequently, for the subset of patients for whom surgery is unsuitable, the spectrum of adjuvant treatment options can be progressively individualized, considering the disease's specific attributes and patient-related factors [8]. Furthermore, adjuvant treatments are frequently employed to diminish the risk of recurrence, encompassing options such as chemotherapy, radiation therapy, hormone therapy, targeted therapy, or biological therapy [9]. The primary treatment options typically are immune checkpoint inhibitors targeting cytotoxic T-lymphocyte antigen 4 (CTLA-4) or programmed cell death protein-1 (PD-1), along with small molecule BRAF (B-raf murine sarcoma viral oncogene homolog B1) inhibitors. However, the side effects of these therapies might be devastating; the effect is not durable, and hence, patients are more likely to relapse. Additionally, these therapies are not always readily available, possibly delaying their initiation for months [10]. The introduction of novel, though costly, treatments for melanoma brings hope to reduce mortality in the upcoming decades. Likewise, developing topical therapy options is promising as most melanoma lesions are detected on the skin [11]. Various topical formulations have been attempted to treat melanoma, including 5-fluorouracil (5-FU) [12], piplartine [13], curcumin [14], and dacarbazine [15]. While these drugs can potentially treat melanoma, they are in experimental stages, and there is limited information about their performance in both in vivo studies and clinical settings. However, given the complexity of determining antitumor efficacy through in vivo studies, topical skin treatments for melanoma are not widely accepted for treating patients [16]. The development of new strategies to treat melanoma can significantly contribute to the progression of the disease, increase the response to first-line treatments, and diminish treatment relapse. Norcantharidin (NCTD) is the demethylated analog of cantharidin, a terpenoid compound that has been proposed as a chemotherapeutic agent. In vitro evidence increasingly supports the effectiveness of NCTD as an oncological medication in several types of cell lines, such as colorectal, epithelial, ovarian [17], hepatocellular [18], esophageal, gastric, lung [19], and non-Hodgkin lymphoma [20]. Few attempts have been made to develop a clinical application of NCTD have been made [21]. However, the most relevant was described by Lixin teamwork where they developed NCTD containing microspheres for intradermal injection [22]. In 2020, a phase I clinical trial was submitted to evaluate NCTD-containing microspheres for injection in patients with solid tumors. However, the specific type of tumor was not disclosed, and the results have not been posted to this date [23]. Given the heterogeneous nature of melanoma, in vivo studies are necessary to determine early tumor onset progression, expansion, invasion, inflammatory and immune response, and metastasis propagation, complex features to evaluate in vitro [24]. In a previous study, our team developed and characterized a norcantharidin-loaded nanoemulsion with optimum droplet size, stability, and in vitro drug release profile. Furthermore, the antiproliferative effect against B16F1 melanoma cells was demonstrated in vitro [25]. In the present study, an in vivo murine model was used to evaluate the effectivity of our nanoemulsion in a B16F1 melanoma cells syngeneic graft model.
2. Results
2.1. Tumor Induction and Application of treatments
The formulated nanoemulsion was a non-Newtonian white fluid characterized by a droplet mean size of 117 nm, a polydispersity index of 0.26, and a pH of 6.5. Upon direct application, the consistency of the nanoemulsion allowed for the formation of a thin, uniform layer over the affected area, which was rapidly absorbed. When applied with microneedles, which serve as physical penetration enhancers by creating micro-channels in the outermost layer of the skin, there were instances where the skin was perforated too deeply. This excessive perforation occasionally led to bleeding and eventually resulted in the formation of callouses in the affected area. Despite these challenges, the nanoemulsion demonstrated potential for effective delivery, indicating that further optimization of the microneedle application technique could enhance therapeutic outcomes with minimum adverse effects.
In the initial photographic session capturing induced melanoma lesions twenty-one days into the treatment, substantial differences in tumor progression were observed among the groups. The control group showed a more pronounced advancement of the tumor lesion, with higher pigmentation. In the NCTDNem treatment group, there were varying degrees of tumor progression, ranging from advanced to those with imperceptible pigmentation. The NCTDNem + MD group displayed an overall reduction in tumor progression among individuals. Similarly, diminished progression was observed in the pentoxifylline-supplemented group (NCTDNem + MD + PTX) (Figure 1).
2.2. Tumor Progression
By the thirtieth day of treatment, the tumor progression observed at the 20-day mark continued. The control group exhibited increased tumor growth between the two photographic sessions, with notable peripheral redness and swelling. In the NCTDNem group, tumors varied widely, spanning from advanced progress to lesions with controlled tumor size. The NCTDNem + MD group showed minimal tumor growth; in some instances, significant macroscopical depigmentation of the tumor was observed. However, in the NCTDNem + MD + PTX group, there was a reversal of the previously observed trend (Figure 2).
The trend of tumor growth among the different treatment groups was reflected in the number of amputations conducted in each group. The control group required the most amputations (n=8), followed by the NCTDNem group (n=4), the NCTDNem + MD + PTX group (n=3), and the NCTDNem + MD group (n=2). These differences were statistically significant (p<0.01), indicating a clear impact of the treatments on tumor growth. While the mean weight values of the groups did not show any statistical significance, there was a noticeable weight gain in the NCTD Nem + MD and the NCTD Nem + MD + PTX group, in contrast to the NCTDNem and control groups, which showed weight loss during the assay. Additionally, there were no significant differences in tumor volume among the groups (Figure 3).
2.3. Drug Content in Serum Samples
The drug content in serum samples varied across the different groups. The NCTDNem group had the lowest NCTD concentration, measuring 0.10 mg/mL. The NCTDNem + MD group had the second-highest NCTD concentration at 0.13 mg/mL. The NCTDNem + MD + PTX group had the highest NCTD concentration, measuring 0.18 mg/mL. As expected, no traces of either NCTD or PTX were detected in the control group. The group that was administered PTX exclusively had a PTX concentration of 1.23 x 10-3 mg/mL in serum (Figure 4).
2.4. Histopathological Analysis
Histopathological analysis revealed that all procured tumors exhibited typical characteristics of malignant epithelioid melanoma. Tumor size within the field of view was consistent across all groups. While the number of mitoses per high-power field did not show a statistically significant difference between the groups, the lowest mitotic count was observed in the NCTDNem + MD group. Additionally, this group displayed increased lymphocyte infiltration and signs of possible tumor regression. A complete summary of the optical field-of-view analysis is presented in Table 1.
Particle analysis highlighted areas with melanin deposits and cellular nuclei in micrographs. According to the results, both groups had practically similar particle counts, indicating comparable cellularity. Furthermore, although no statistical significance was found regarding particle average size, there is a tendency for larger particles in the control group, which could imply more extensive melanin deposits. Ultimately, this aligns with the finding of a higher total particle area in the control group, indicating increased melanin production and a more significant pigment presence (Figure 5).
3. Discussion
The current World Health Organization classification of skin melanoma is based on morphological aspects and archetypical patterns of clinical and histological nature. Following a biopsy of a suspected melanoma lesion, confirmation of the diagnosis is necessary, which includes assessing the lesion's size and the number of mitoses in 1.0 mm² field of view. This evaluation helps determine the prognosis based on the lesion's invasive capacity [26]. Additionally, advancements in fast-growing sequencing technologies are identifying recurrent mutations in specific oncogenes. Many of these mutations are significantly associated with specific clinical or histopathological subsets of lesions, strongly suggesting biologically distinct types of melanocytic neoplasms. Consequently, while intraepithelial features do not necessarily indicate that the cell of origin is within the epithelium, the mutational burden observed in non-glabrous skin melanoma suggests that many originate from epidermal melanocytes [2].
Topical pharmaceutical formulations aim to deliver a specific amount of drug to targeted skin locations while minimizing systemic uptake. This approach offers several advantages, including minimal invasiveness, easy application, consistent pharmacokinetics, and improved local bioavailability by eluding first-pass metabolism. While the viable epidermis can retain topically administered drugs, thereby limiting their dissemination beyond the epidermal layer, the stratum corneum is the bioavailability-controlling membrane for transporting xenobiotics across the skin. Therefore, local cutaneous bioavailability may not reflect systemic availability. Moreover, topical doses are often small, and the required concentration is often unknown [27].
A proper understanding of melanoma tumor growth requires the development of models that integrate as many factors as possible. These models should emulate the current landscape of diagnosis and treatment to help create new and effective treatment strategies [24]. Many melanoma-implanted murine models have been developed to study topical treatments with physical skin penetration strategies. Among these models are solid microneedle patches, liposomes, nanoemulsions, and transferosomes, to name a few [16]. Given the use of a nanoemulsion and the employability of the drug, a study that caught our attention assessed the in vivo effectiveness of a dacarbazine-loaded nanoemulsion that reduced melanoma growth [15]. Furthermore, an imiquimod-oleic acid prodrug cream induced toxicity and apoptosis in B16F1 synergenic C57BL murine model [28].
Norcantharidin (7-oxabicycloheptane-2,3-dicarboxylic acid; formula: C8H8O4; CAS-No.: 29745-04-8) is the demethylated analog of cantharidin. It is an experimental drug, and its use in humans has not been well established, as it has not been approved by any regulatory entity. In a preliminary toxicological study, we established a lethal dose 50 (LD50) of 8.8 mg/Kg and a therapeutic safe dose of 3 mg/Kg [29]. NCTD is primarily used in Eastern medicine, particularly in traditional Chinese practices. However, its administration in humans—whether orally, intravenously, or through local injection—results in significant irritation at the application site [30]. Currently, there is an ongoing clinical study investigating its use in treating solid tumors via intratumoral injection, but the results have not yet been disclosed [22].
Prior studies have demonstrated that NCTD inhibits tumor growth and induces apoptosis in various cell lines. In human osteosarcoma cells, NCTD showed dose-dependent inhibition of proliferation and induction of apoptosis through the c-Met/Akt/mTOR signaling pathway. This effect involved reducing the expression of the anti-apoptotic protein Bcl-2 and increasing the expression of the pro-apoptotic protein Bax [31]. Another study investigated NCTD's impact on melanoma, finding that it suppresses tumor growth and inhibits metastasis by downregulating MMP-2 expression, a protein linked to cancer cell invasion. Additionally, NCTD treatment led to a decrease in the activity of NF-κB, a transcription factor associated with MMP-2 regulation [33]. Furthermore, in a previous study, we demonstrated that NCTD inhibits cell proliferation in B16F1 melanoma cells and reduces the metabolic rate of these cells [25].
An important aspect to consider is that NCTD has limited solubility in water, with a maximum of 2.5 mg/mL at pH 6 and 9.5 mg/mL at pH 9.5 [32]. Additionally, norcantharidin’s capacity to partition between hydrophilic and lipophilic viable tissues may restrict its effectiveness in drug delivery [16]. The most promising approach to address this issue involves an injectable emulsion containing NCTD-lipid nanospheres. However, the concentration achieved in this formulation was only 8 mg/mL [23]. In the current study, we use a nanoemulsion as the delivery system. Nanoemulsions are biphasic liquid systems consisting of hydrophilic and hydrophobic phases, where one phase is dispersed as nanosized droplets into the second liquid, stabilized by surfactants [34]. Therefore, they can be an effective pharmaceutical form for enhancing drug delivery [35].
In a previous drug release study, we found that our NCTD-containing nanoemulsion (3% w/w for a final concentration of 30 mg/mL) released 15 mg of NCTD per gram of emulsion over a span of 3 hours [25]. In the present study, 0.1 grams of nanoemulsion was applied to the melanoma lesion, which is equivalent to approximately 1.5 mg of NCTD daily for 30 days. According to the results, this dosage effectively reduced tumor growth. Moreover, the amount of NCTD found in the serum samples of treated groups was 0.15 mg per mL on average, indicating that approximately one-tenth of the applied dose reached systemic bioavailability. Furthermore, applying the nanoemulsion with a microneedle pen would likely increase drug penetration and augment its effectiveness.
The histopathological analysis revealed that the selected syngeneic graft model is suitable for studying melanoma, as all tumors exhibited epithelial characteristics and were correctly located. Moreover, the homogeneity of tumor size across samples also indicates the model's fitness. However, given the syngeneic nature of the lesion, we cannot fully assess invasiveness, as this also depends on the intrinsic properties of the cell line used. In addition to size, other histopathological characteristics that can predict the response to current melanoma treatments include the mitotic rate and lymphocytic infiltration within the lesion. Although the mitotic rate may be also an inherent characteristic of the cell line, the lowest rate was observed in the NCTD Nem + MD group, which received the highest dose of NCTD.
Interestingly, the highest lymphocytic infiltration was found in the same group, suggesting that NCTD could act as an immunomodulator. These findings imply that immune system cells contribute to tumor reduction alongside the drug's effects, indicating potential use as an adjuvant treatment. Previous studies have reported that combined treatments of PTX and NCTD administered intragastrically (60 mg/kg + 0.75 mg/kg) in DBA/2 mice significantly recruit lymphocytes and iNKT cells to the tumor site [36]. However, in our study, the PTX-complemented group exhibited a reversed effect on tumor growth reduction. This could be attributed to a pharmacological interaction and/or increased blood filtration and clearance due to PTX's hemorheological effects.
Similarly, the reduced amount of pigment found in the treated groups may indicate either diminished melanin production or a reduction in tumoral mass. Additionally, probable regression was observed in the NCTD nanoemulsion group treated with a microneedle pen. Regression in cancer is very rare; however, melanoma, neuroblastoma, and lymphoma may show remission more frequently than carcinoma, with a reported frequency of 1/100,000 [37]. Furthermore, a study on invasive breast cancer suggested that 22% of patients could experience tumor regression [38]. While further studies are needed, processing micrographs to evaluate melanin content could reveal insights into internal processes within the model [11].
Many studies have addressed melanoma syngeneic models and locoregional treatments [24,39]. However, there is a lack of consensus on high-quality data, and varying levels of evidence. Moreover, fewer studies adhere to the management protocols used in clinical practice, resulting in inconsistent response rates and heterogeneous outcome measures [40]. In the present study, the management protocol aims to adhere to clinical practice, incorporating dermatoscopic follow-up features, surgical incision (the primary treatment for melanoma stages I-III), and standard histopathological confirmation of the biopsy. Considering that various factors and patient characteristics may preclude surgery, it´s important to assess potential locoregional therapies, as they may significantly affect progression-free survival. Finally, these therapies should be evaluated not only for their effect on patient-rated outcomes but also for their feasibility and comparative health costs [8].
4. Conclusions
A novel NCTD-containing nanoemulsion that is systemically safe while allowing for higher doses to be applied directly to the tumor location and exerting the desired effect was successfully developed. This potential therapy led to improved therapeutic outcomes, such as tumor growth arrest observed during dermatoscopical follow-up, a reduction in surgical incision interventions, and positive histopathological features frequently used in clinical practice. This innovative scientific development, supported by robust evidence, could serve as an alternative in the current treatment of early-stage melanoma or as adjuvant therapy, improving disease progression outcomes and positively impacting the lives of melanoma patients.
5. Materials and Methods
5.1. Nanoemulsion Development
The nanoemulsion was made from an Oil/Water (O/W) pre-emulsion that contained almond oil, Carbopol® 940, cetyl alcohol, glycerin, glyceryl monostearate, methylparaben, propylparaben, stearic acid, triethanolamine, polysorbate 80, and urea, acquired from Merck (Burlington, MA, USA); Eumulgin® B1 (Ceteareth-12) provided by BASF (Ludwigshafen, Germany), and Norcantharidin obtained from Sigma-Aldrich (St. Louis, MO, USA). The oil phase was mixed with the water phase under constant stirring at 70 °C for one minute, and when the temperature dropped to 40°C, a solution of 0.3 g of norcantharidin dissolved in 1 mL of triethanolamine-water (20%) was added for a final drug concentration of 3.0% w/w NCTD (30 mg/mL). The pre-emulsion was sonicated for 5 min with an ultrasonic processor at 5.0 watts to obtain the final nanoemulsion (Vibracell, Sonics & Materials, Newton, MA, USA). The nanoemulsion was further characterized by droplet mean size and polydispersity index (PDI) with a Zetasizer Nano Series ZS apparatus (Malvern Panalytical, Malvern, UK). Additionally, the pH was measured using a pH meter (AB315, Fisher Scientific) (Figure 6).
5.2. Experimental Animals
ICR mice (n = 32) were acquired from the National School of Biological Sciences animal facility. All mice of both sexes were evaluated at 4 to 6 weeks of age, with a weight greater than 20 g. Mice were maintained at 23°C with a 12-hour cycle of darkness and light. Additionally, a humidity level of 40-60% was maintained. The mice had ad libitum access to water and food [41].
5.3. Cell Culture
The immortalized B16F1 melanoma cells were obtained from the American Type Culture Collection. Cells were cultured using a mixture of DMEM culture medium, supplemented with 5% fetal bovine serum, 2 nM glutamine, 1% antibiotics (erythromycin at 10,000 U/ml and ampicillin at 10,000 U/ml), and pyruvate (all bought from Life Technologies, Carlsbad, USA) in 75 cm2 flasks and placed under a humidified incubator at 37°C with a CO2 concentration of 5% and an air saturation of 95% in the atmosphere. Passages were performed using a trypsin-EDTA solution (0.25% w/v -0.02 %) in phosphate-buffered saline (PBS). In the ninth passage, cells were left to grow to over-confluence [42]. The culture medium was exchanged for a non-supplemented medium 24 hours before the assay. After time elapsed, culture debris and remanent medium were discarded. Cells were detached, and 1 mL of supplemented medium was added to neutralize trypsin. Cell suspensions were counted using a 0.4% w/v trypan blue dye solution. After counting, cell solutions were transferred into a 10 mL polypropylene for centrifugation (1200 x g for 5 min). Cell pellets were resuspended and adjusted to a concentration of 2 x 106 cells per 1.0 mL with injectable water and loaded in 1.0 ml ultrafine syringes U-100 30G 1ml/cc 5/16" (8mm).
5.4. Syngeneic Graft Model
Mice were held by the junction of the knee of the left hind leg and injected with 0.1 ml of the B16F1 cell solution to obtain a final inoculation of 200'000 cells. Three days after the initial inoculation, mice were randomly assigned to four treatment groups [43]. The first group received as treatment the application of 0.1 g of the norcantharidin nanoemulsion (NCTDNem; n=8) using a fine-tipped cotton swab where the tumor was inoculated. The second group was treated with the same amount of nanoemulsion, previously pressing the inoculation area with an adjustable Microneedling Pen with 36 nano pin cartridges (NCTDNem + MD; n=8). The third group was orally treated with pentoxifylline (PTX) using a 60 mm mouse feeding needle at a dose of 60 mg/kg of body weight, in addition to the application of nanoemulsion with the microneedling pen (NCTDNem + MD + PTX; n=8). All the groups were compared to the control group. The treatments were initiated three days after the initial syngeneic graft inoculation. On days 20 and 30 of the assay, melanoma lesions from all groups were photographed using a dermatoscope (DERMALITE) for amplification and captured with a high-resolution 48 MP smartphone camera.
5.5. Surgical Intervention
On the 30th day, lesions exceeding a diameter of 4 mm underwent amputation. For this purpose, mice were anesthetized in an induction chamber (RWD, vaporizer for isoflurane Mod. R5835, Sugar Land, TX, USA) saturated at 4.0% with isoflurane, complemented by 1.2 mg/kg of ketamine and 3 mg/kg of midazolam. A tourniquet was applied to the upper third of the leg below the femorotibial joint. Once circulation was reduced, the affected area was excised using stainless steel forceps and cauterized with a high-temperature electrocautery device (Bovie Clearwater, FL, USA). Post-operative care included cleaning the affected area and performing additional cauterization if bleeding was observed. Data is presented as the percentage of amputations performed, mean weight (g), and tumor volume (mm3) per group.
5.6. Blood Samples
After surgical procedures, each group resumed their assigned treatments. The NCTD nanoemulsion was applied to the limbs of mice that underwent surgery. Conversely, the nanoemulsion was applied directly to the left hind leg, where the tumor was initially inoculated for those who did not undergo amputation. PTX administration followed the procedure outlined in the previous section. This procedure aimed to replicate post-operative care in a realistic clinical context or an extended treatment period exceeding 30 days and to determine drug serum content. After a ten-day interval, all mice were anesthetized according to the previously described conditions and then euthanized. Blood samples were obtained through cardiac puncture and collected in tubes containing sodium citrate (109 mmol/L) as an anticoagulant. Subsequently, samples were centrifuged at 1200 x g for 5 minutes to separate the plasma.
5.7. Drug Content Determination
Both NCTD and PTX drugs were extracted from a 0.5 mL serum aliquot fortified with 25 µL of internal standard (Cyclophosphamide, 99.94% from MERK), 100 µL of 1 M hydrochloric acid, and 1.0 mL of acetone. The mixture was centrifuged at 10,000 rpm for 5 minutes, separating the supernatant from the precipitate. PTX was determined in the supernatant. Concurrently, the precipitate was utilized for NCTD determination after resuspension with 1.0 mL of acetone, followed by evaporation to dryness. The resulting residue was reconstituted with 150 µL of water. NCTD determination was determined by fluorescence spectroscopy with an excitation/emission wavelength of 300/450 nm, while PTX was determined by direct absorbance (280 nm) using a multi-mode microplate reader (Synergy MX, Biotek) in 96-well plates (Thermo Fisher Scientific, USA) [44].
5.8. Histological Analysis
Tumor samples underwent further processing using the paraffin inclusion technique and were stained with hematoxylin and eosin. Micrographs of 3-micron thick slices (Microtome RM2245, Leica Microsystems) were captured at 20x magnification using optical microscopy (Binocular optical microscope Leica Microsystems) [29]. Micrographs were divided into two groups: the controls (n=8) and the treated samples (n=9), regardless of treatment. Micrographs were analyzed per field-of-view, and subsequently, size (cm), mitosis by high power field (HPF), lymphocyte infiltration, and regression (a phenomenon in which cancer lesions shrink naturally or using drugs) were assessed [45].
5.9. Micrographs Image Analysis
Additionally, a quantitative analysis at object and spatial levels was conducted using Fiji software (NIH et al., USA, accessible at: https://imagej.nih.gov/ij/) [46]. The multispectral micrographs were split into color channels: red, blue, and green. Channel blue was used to capture the visible light from 450-495 nm, and the threshold was adjusted to 28% using the max entropy filter. Afterward, a selection was created, and a particle analysis was performed concerning particle count, average size, and the total area measured by pixels.
5.10. Data Analysis
Statistical analysis was performed on the assays to determine their fitness for symmetric distribution if applicable, using either normality testing or linearity in the case of regression analysis. A Fisher´s exact test was performed for the amputation count data in the treated groups. For the histopathological and particle analysis, data was compared using the Student t-test if the data showed normal behavior or the Mann-Whitney test if the data had non-normal behavior. Furthermore, the drug content in serum was estimated by regression analysis using calibration curves, which consisted of fixed amounts of NCTD from 0.002 mg to 0.008 mg dissolved in water (Eq.1: y=-78.43 x10^4+11.27 x10^3;R^2=0.993) and PTX from 2x10-5 to 8 x10-5 mg dissolved in water (Eq.2: y=7150+0.039;R^2=0.997). Statistical comparisons were calculated using PAST version 2.17c. [47]. Plots were created with Sigma Plot (Version 11.0 Buil 11.0.0.77, Systat Software, Inc., 2008) and figures using Publisher (Microsoft Corporation, USA).
Author Contributions
GMR conceived, conducted experiments, and wrote the manuscript; AA, ECV conducted experiments; PCP, MLDL, FC, ACPS data curation, formal analysis, validation, and visualization; AVL conceived, funding acquisition, project administration, writing - review & editing.
Funding
This study was supported by Secretaría de Investigación y Posgrado, Instituto Politécnico Nacional SIP code 20240926.
Institutional Review Board Statement
The study protocol was approved by the local Ethical Committee (license number: PE/001/2574-6/20). The guidelines of Article 38 and Chapter V of Directive 2010/63/EU of the European Parliament and Council, dated September 22, 2010, were followed.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data supporting reported results are available under request.
Acknowledgments
Author Martínez-Razo G. is a DSc. student who received scholarship from CONACyT and BEIFI-IPN. M.L. Dominguez-López, E. and A. Vega-López, are fellows of Estímulos al Desempeño en Investigación and Comisión y Fomento de Actividades Académicas (Instituto Politécnico Nacional) and Sistema Nacional de Investigadores (SNI, CONACyT, México).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| 5-FU | 5-Fluorouracil |
| BRAF | B-Raf Sarcoma Viral Oncogene B1 |
| CTLA-4 | Cytotoxic T-Lymphocyte Antigen 4 |
| LD50 | Lethal Dose 50 |
| NCTD | Norcantharidin |
| Nem | Nanoemulsion |
| MD | Microneedle |
| O/W | Oil/Water |
| PTX | Pentoxifylline |
| PBS | Phosphate-Buffered Saline |
| PDI | Polydispersity Index |
| PD-1 | Programmed Cell Death Protein-1 |
References
- Sladden, M.J.; Balch, C.; Barzilai, D.A.; Berg, D.; Freiman, A.; Handiside, T.; Hollis, S.; Lens, M.B.; Thompson, J.F. (2009). Surgical excision margins for primary cutaneous melanoma. The Cochrane Library. [CrossRef]
- Iarc.Fr. Retrieved June 28, 2024, from http://www.iarc.fr/en/publications/pdfs-online/pat-gen/bb6/.
- Eggermont, A.M.M.; Spatz, A.; Robert, C. Cutaneous melanoma. Lancet 2014, 383, 816–827. [Google Scholar] [CrossRef] [PubMed]
- Welch, H.G.; Woloshin, S.; Schwartz, L.M. Skin biopsy rates and incidence of melanoma: population based ecological study. BMJ 2005, 331, 481. [Google Scholar] [CrossRef]
- Tromme, I.; Legrand, C.; Devleesschauwer, B.; Leiter, U.; Suciu, S.; Eggermont, A.; Francart, J.; Calay, F.; Haagsma, J.A.; Baurain, J.-F.; Thomas, L.; Beutels, P.; Speybroeck, N. Melanoma burden by melanoma stage: Assessment through a disease transition model. Eur. J. Cancer 2016, 53, 33–41. [Google Scholar] [CrossRef]
- Friedman, R.J.; Rigel, D.S.; Kopf, A.W. Early detection of malignant melanoma: The role of physician examination and self-examination of the skin. CA: A Cancer Journal for Clinicians 1985, 35, 130–151. [Google Scholar] [CrossRef]
- Wang, S.Q.; Rabinovitz, H.; Kopf, A.W.; Oliviero, M. Current technologies for the in vivo diagnosis of cutaneous melanomas. Clinics in Dermatology 2004, 22, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Read, T.; Lonne, M.; Sparks, D.S.; David, M.; Wagels, M.; Schaider, H.; Soyer, H.P.; Smithers, B.M. A systematic review and meta-analysis of locoregional treatments for in-transit melanoma. Journal of Surgical Oncology 2019, 119, 887–896. [Google Scholar] [CrossRef]
- Nieweg, O.E.; Gallegos-Hernández, J.F. La cirugía en melanoma cutáneo maligno y las nuevas drogas. Cirugia y cirujanos 2015, 83, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Testori, A.A.E.; Ribero, S.; Indini, A.; Mandalà, M. Adjuvant treatment of melanoma: Recent developments and future perspectives. American Journal of Clinical Dermatology 2019, 20, 817–827. [Google Scholar] [CrossRef] [PubMed]
- Bastian, B.C. The molecular pathology of melanoma: An integrated taxonomy of melanocytic neoplasia. Annual Review of Pathology 2014, 9, 239–271. [Google Scholar] [CrossRef]
- Naguib, Y.W.; Kumar, A.; Cui, Z. The effect of microneedles on the skin permeability and antitumor activity of topical 5-fluorouracil. Acta Pharmaceutica Sinica. B 2014, 4, 94–99. [Google Scholar] [CrossRef]
- Giacone, D.V.; Dartora, V.F.M.C. , de Matos, J.K.R.; Passos, J.S.; Miranda, D.A.G., de Oliveira, E.A.; Silveira, E.R.; Costa-Lotufo, L.V.; Maria-Engler, S.S.; Lopes, L.B. Effect of nanoemulsion modification with chitosan and sodium alginate on the topical delivery and efficacy of the cytotoxic agent piplartine in 2D and 3D skin cancer models. International Journal of Biological Macromolecules 2020, 165, 1055–1065. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wu, Q.; Zhang, Z.; Yuan, L.; Liu, X.; Zhou, L. Preparation of curcumin-loaded liposomes and evaluation of their skin permeation and pharmacodynamics. Molecules 2012, 17, 5972–5987. [Google Scholar] [CrossRef] [PubMed]
- Tagne, J.-B.; Kakumanu, S.; Nicolosi, R.J. Nanoemulsion preparations of the anticancer drug dacarbazine significantly increase its efficacy in a xenograft mouse melanoma model. Molecular Pharmaceutics 2008, 5, 1055–1063. [Google Scholar] [CrossRef] [PubMed]
- Tambunlertchai, S.; Geary, S.M.; Salem, A.K. Skin penetration enhancement strategies used in the development of melanoma topical treatments. The AAPS Journal 2021, 23. [Google Scholar] [CrossRef]
- McCluskey, A.; Ackland, S.P.; Bowyer, M.C.; Baldwin, M.L.; Garner, J.; Walkom, C.C.; Sakoff, J.A. Cantharidin analogues: synthesis and evaluation of growth inhibition in a panel of selected tumour cell lines. Bioorganic Chemistry 2003, 31, 68–79. [Google Scholar] [CrossRef] [PubMed]
- Pachuta-Stec, A.; Szuster-Ciesielska, A. New norcantharidin analogs: Synthesis and anticancer activity. Archiv Der Pharmazie 2015, 348, 897–907. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Ren, Y.; Tan, L.; Song, X.; Wang, M.; Li, Y.; Cao, Z.; Guo, C. Norcantharidin: research advances in pharmaceutical activities and derivatives in recent years. Biomed. Pharmacother. Biomed. Pharmacother. 2020, 131, 110755. [Google Scholar] [CrossRef] [PubMed]
- Dorn, D.C.; Kou, C.A.; Png, K.J.; Moore, M.A.S. The effect of cantharidins on leukemic stem cells. International Journal of Cancer. Journal International Du Cancer 2009, 124, 2186–2199. [Google Scholar] [CrossRef] [PubMed]
- Xie, M.-H.; Ge, M.; Peng, J.-B.; Jiang, X.-R.; Wang, D.-S.; Ji, L.-Q.; Ying, Y.; Wang, Z. In-vivo anti-tumor activity of a novel poloxamer-based thermosensitive in situ gel for sustained delivery of norcantharidin. Pharmaceutical Development and Technology 2019, 24, 623–629. [Google Scholar] [CrossRef]
- Lixin, W.; Haibing, H.; Xing, T.; Ruiying, S.; Dawei, C. A less irritant norcantharidin lipid microspheres: Formulation and drug distribution. International Journal of Pharmaceutics 2006, 323, 161–167. [Google Scholar] [CrossRef]
- Clinicaltrials.gov. (n.d.). Clinicaltrials.gov. Retrieved July 4, 2024, from https://clinicaltrials.gov/ct2/show/NCT04673396.
- Potez, M.; Trappetti, V.; Bouchet, A.; Fernandez-Palomo, C.; Güç, E.; Kilarski, W.W.; Hlushchuk, R.; Laissue, J.; Djonov, V. Characterization of a B16-F10 melanoma model locally implanted into the ear pinnae of C57BL/6 mice. PloS One 2018, 13, e0206693. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Razo, G.; Pires, P.C.; Domínguez-López, M.L.; Veiga, F.; Vega-López, A.; Paiva-Santos, A.C. Norcantharidin nanoemulsion development, characterization, and in vitro antiproliferation effect on B16F1 melanoma cells. Pharmaceuticals 2023, 16, 501. [Google Scholar] [CrossRef] [PubMed]
- Gist.Pl. Retrieved June 28, 2024, from http://gist.pl/download/czerniak_esmo_rct_melanoma_guide_for_patients_2013.pdf.
- Herkenne, C.; Alberti, I.; Naik, A.; Kalia, Y.N.; Mathy, F.-X.; Préat, V.; Guy, R.H. In vivo methods for the assessment of topical drug bioavailability. Pharmaceutical Research 2008, 25. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Sharma, D.; Baldi, A.; Jyoti, K.; Chandra, R.; Madan, J. Imiquimod-oleic acid prodrug-loaded cream reduced drug crystallinity and induced indistinguishable cytotoxicity and apoptosis in mice melanoma tumour. Journal of Microencapsulation 2019, 36, 759–774. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Razo, G.; Domínguez-López, M.L. , de la Rosa, J.M.; Fabila-Bustos, D.A.; Reyes-Maldonado, E.; Conde-Vázquez, E.; Vega-López, A. Norcantharidin toxicity profile: an in vivo murine study. Naunyn-Schmiedeberg’s Archives of Pharmacology 2023, 396, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Pan, M.-S.; Cao, J.; Fan, Y.-Z. Insight into norcantharidin, a small-molecule synthetic compound with potential multi-target anticancer activities. Chinese Medicine 2020, 15. [Google Scholar] [CrossRef] [PubMed]
- Mei, L.; Sang, W.; Cui, K.; Zhang, Y.; Chen, F.; Li, X. Norcantharidin inhibits proliferation and promotes apoptosis via c-Met/Akt/mTOR pathway in human osteosarcoma cells. Cancer Science 2019, 110, 582–595. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.; Cao, M.; Mao, W.; Sun, X.; Tang, J.; Shen, Y.; Sui, M. Targeted acid-labile conjugates of norcantharidin for cancer chemotherapy. Journal of Materials Chemistry 2012, 22, 15804. [Google Scholar] [CrossRef]
- Wang, Z.; You, D.; Lu, M.; He, Y.; Yan, S. Inhibitory effect of norcantharidin on melanoma tumor growth and vasculogenic mimicry by suppressing MMP-2 expression. Oncology Letters 2017, 13, 1660–1664. [Google Scholar] [CrossRef]
- Santos, A.C.; Morais, F.; Simões, A.; Pereira, I.; Sequeira, J.A.D.; Pereira-Silva, M.; Veiga, F.; Ribeiro, A. Nanotechnology for the development of new cosmetic formulations. Expert Opinion on Drug Delivery 2019, 16, 313–330. [Google Scholar] [CrossRef]
- Nayak, A.K.; Hasnain, M.S.; Aminabhavi, T.M.; Torchilin, V.P. (2022). Systems of Nanovesicular Drug Delivery. Academic Press.
- Correa-Lara, M.V.M.; Lara-Vega, I.; Nájera-Martínez, M.; Domínguez-López, M.L.; Reyes-Maldonado, E.; Vega-López, A. (2023). Tumor-infiltrating iNKT cells activated through c-kit/Sca-1 are induced by pentoxifylline, norcantharidin, and their mixtures for killing Murine melanoma cells. Pharmaceuticals, 16, 1472. [CrossRef]
- Hobohm, U. Fever therapy revisited. British Journal of Cancer 2005, 92, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Zahl, P.-H.; Mæhlen, J.; Welch, H.G. The natural history of invasive breast cancers detected by screening mammography. Archives of Internal Medicine 2008, 168, 2311. [Google Scholar] [CrossRef] [PubMed]
- Güç, E.; Briquez, P.S.; Foretay, D.; Fankhauser, M.A.; Hubbell, J.A.; Kilarski, W.W.; Swartz, M.A. Local induction of lymphangiogenesis with engineered fibrin-binding VEGF-C promotes wound healing by increasing immune cell trafficking and matrix remodeling. Biomaterials 2017, 131, 160–175. [Google Scholar] [CrossRef] [PubMed]
- Bobek, V.; Kolostova, K.; Pinterova, D.; Kacprzak, G.; Adamiak, J.; Kolodziej, J.; Boubelik, M.; Kubecova, M.; Hoffman, R.M. A clinically relevant, syngeneic model of spontaneous, highly metastatic B16 mouse melanoma. Anticancer Research 2010, 30, 4799. [Google Scholar] [PubMed]
- Madera-Sandoval, R.L.; Tóvári, J.; Lövey, J.; Ranđelović, I.; Jiménez-Orozco, A.; Hernández-Chávez, V.G.; Reyes-Maldonado, E.; Vega-López, A. Combination of pentoxifylline and α-galactosylceramide with radiotherapy promotes necro-apoptosis and leukocyte infiltration and reduces the mitosis rate in murine melanoma. Acta Histochemica 2019, 121, 680–689. [Google Scholar] [CrossRef] [PubMed]
- Doornaert, B.; Leblond, V.; Galiacy, S.; Gras, G.; Planus, E.; Laurent, V.; Isabey, D.; Lafuma, C. Negative impact of DEP exposure on human airway epithelial cell adhesion, stiffness, and repair. American Journal of Physiology. Lung Cellular and Molecular Physiology 2003, 284, L119–L132. [Google Scholar] [CrossRef] [PubMed]
- Giavazzi, R.; Decio, A. (2014). Syngeneic Murine metastasis models: B16 melanoma. In Methods in Molecular Biology (pp. 131–140). Springer New York.
- Wei, C.-M.; Zhang, R.; Wang, B.-J.; Yuan, G.-Y.; Guo, R.-C. Determination and pharmacokinetic study of norcantharidin in human serum by HPLC-MS/MS method. Biomedical Chromatography: BMC 2008, 22, 44–49. [Google Scholar] [CrossRef]
- Lee, C.H.; Cho, J.; Lee, K. Tumour regression via integrative regulation of neurological, inflammatory, and hypoxic tumour microenvironment. Biomolecules & Therapeutics 2020, 28, 119–130. [Google Scholar] [CrossRef]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 years of image analysis. Nature Methods 2012, 9, 671–675. [Google Scholar] [CrossRef]
- Past: Paleontological statistics software package for education and data analysis. (n.d.). Palaeo-electronica.org. Retrieved June 28, 2024, from http://palaeo-electronica.org/2001_1/past/issue1_01.htm.
Figure 1.
Photographs of four individuals of each group (4 out of 8) on the 20th day of treatment. First row: Control group. Second row: Norcantharidin nanoemulsion NCTDNem. Third row: Norcantharidin nanoemulsion applied with microneedle (NCTDNem + MD). Fourth row: Norcantharidin nanoemulsion applied with microneedle and supplemented with pentoxifylline (NCTDNem + MD+PTX).
Figure 1.
Photographs of four individuals of each group (4 out of 8) on the 20th day of treatment. First row: Control group. Second row: Norcantharidin nanoemulsion NCTDNem. Third row: Norcantharidin nanoemulsion applied with microneedle (NCTDNem + MD). Fourth row: Norcantharidin nanoemulsion applied with microneedle and supplemented with pentoxifylline (NCTDNem + MD+PTX).
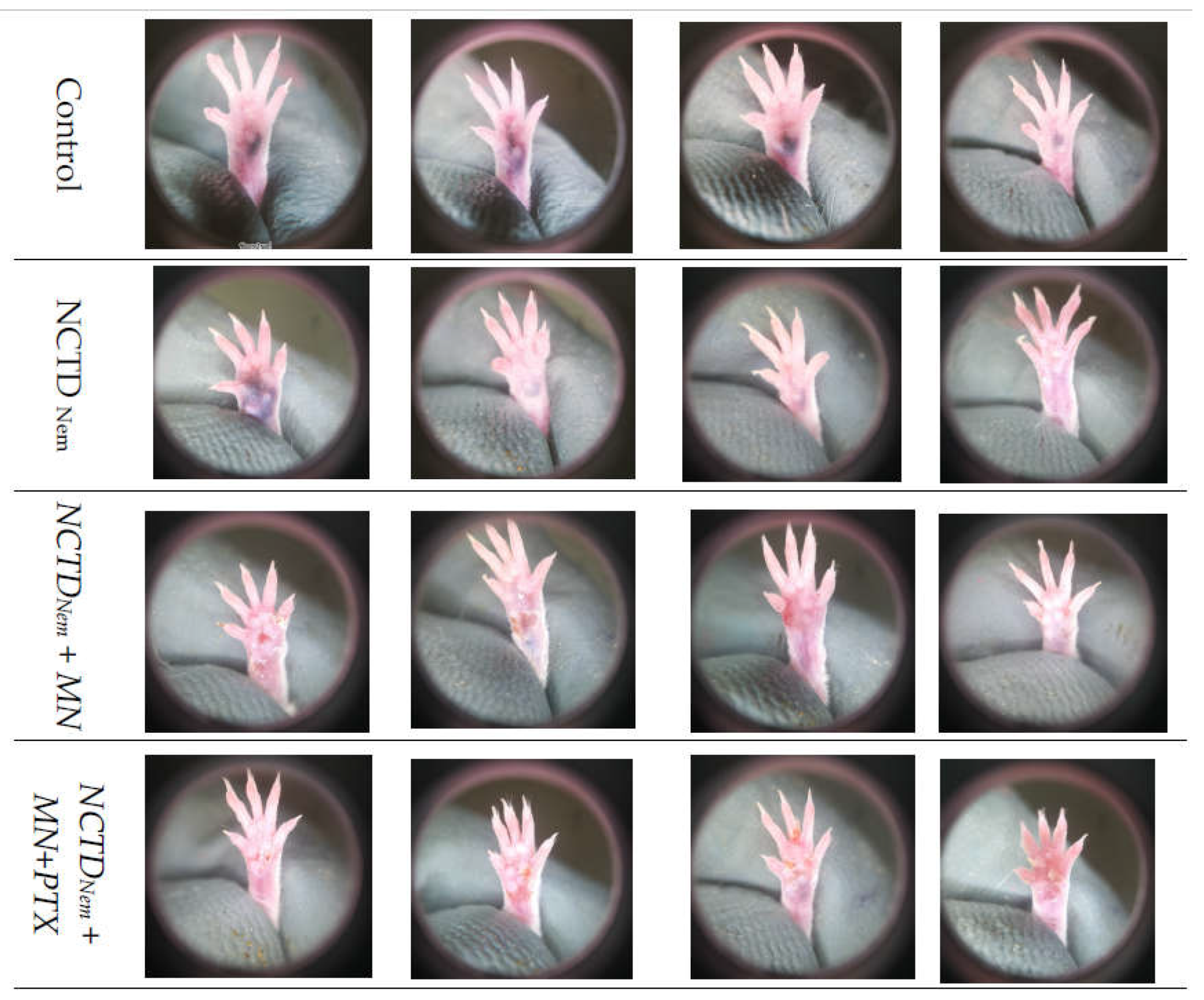
Figure 2.
Photographs of four individuals of each group (4 out of 8) on the 30th day of treatment. First row: Control group. Second row: Norcantharidin nanoemulsion NCTDNem. Third row: Norcantharidin nanoemulsion applied with microneedle (NCTDNem + MD). Fourth row: Norcantharidin nanoemulsion applied with microneedle and supplemented with pentoxifylline (NCTDNem + MD+PTX).
Figure 2.
Photographs of four individuals of each group (4 out of 8) on the 30th day of treatment. First row: Control group. Second row: Norcantharidin nanoemulsion NCTDNem. Third row: Norcantharidin nanoemulsion applied with microneedle (NCTDNem + MD). Fourth row: Norcantharidin nanoemulsion applied with microneedle and supplemented with pentoxifylline (NCTDNem + MD+PTX).
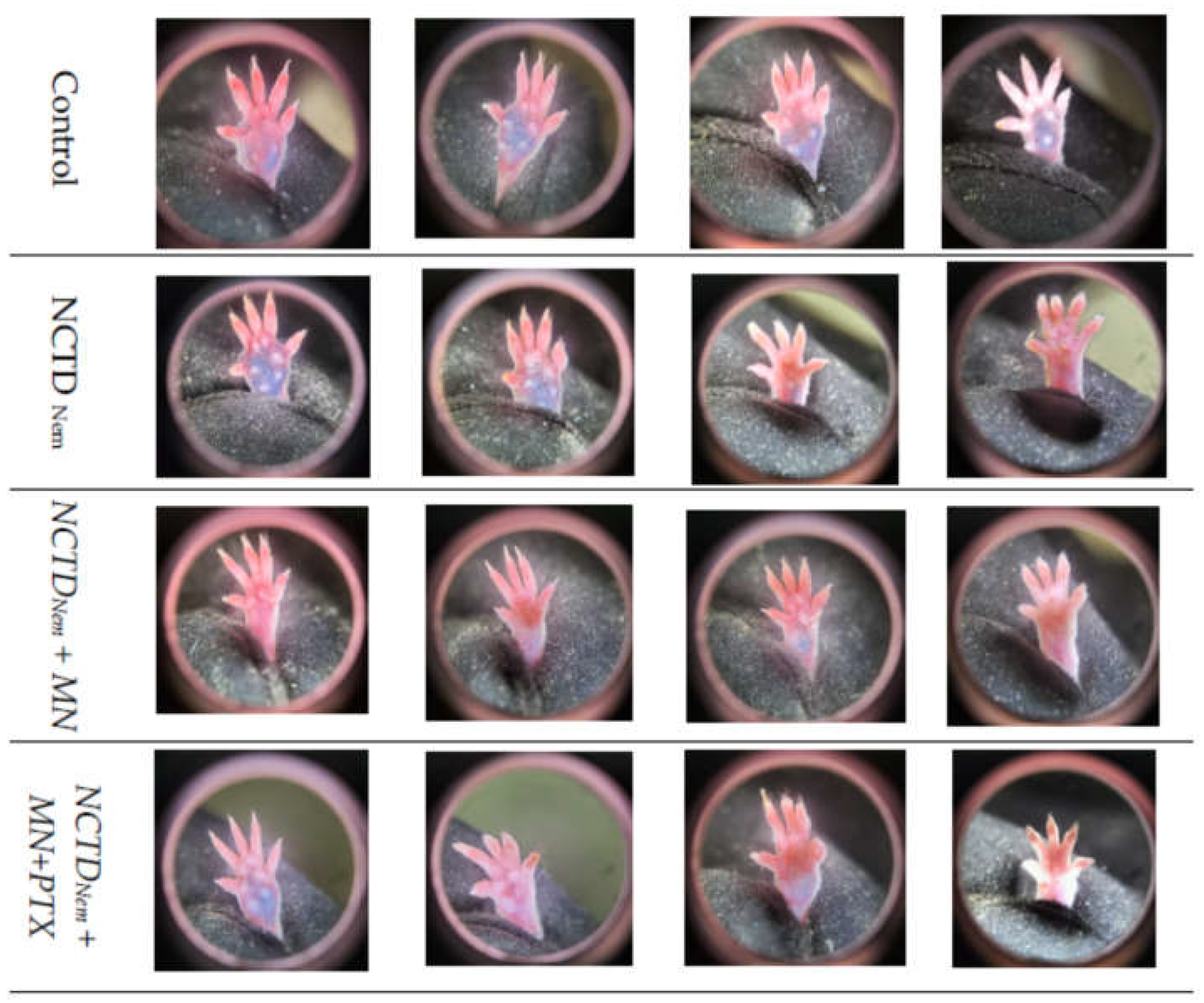
Figure 3.
Results of treatments in percentage of amputations (vertical bars with standard error), group mean weight (left pie chart), and macroscopic tumor volume (right pie chart). Groups are Control, Norcantharidin nanoemulsion NCTDNem, Norcantharidin nanoemulsion applied with microneedle (NCTDNem + MD), Norcantharidin nanoemulsion applied with microneedle and supplemented with pentoxifylline (NCTDNem + MD+PTX).
Figure 3.
Results of treatments in percentage of amputations (vertical bars with standard error), group mean weight (left pie chart), and macroscopic tumor volume (right pie chart). Groups are Control, Norcantharidin nanoemulsion NCTDNem, Norcantharidin nanoemulsion applied with microneedle (NCTDNem + MD), Norcantharidin nanoemulsion applied with microneedle and supplemented with pentoxifylline (NCTDNem + MD+PTX).
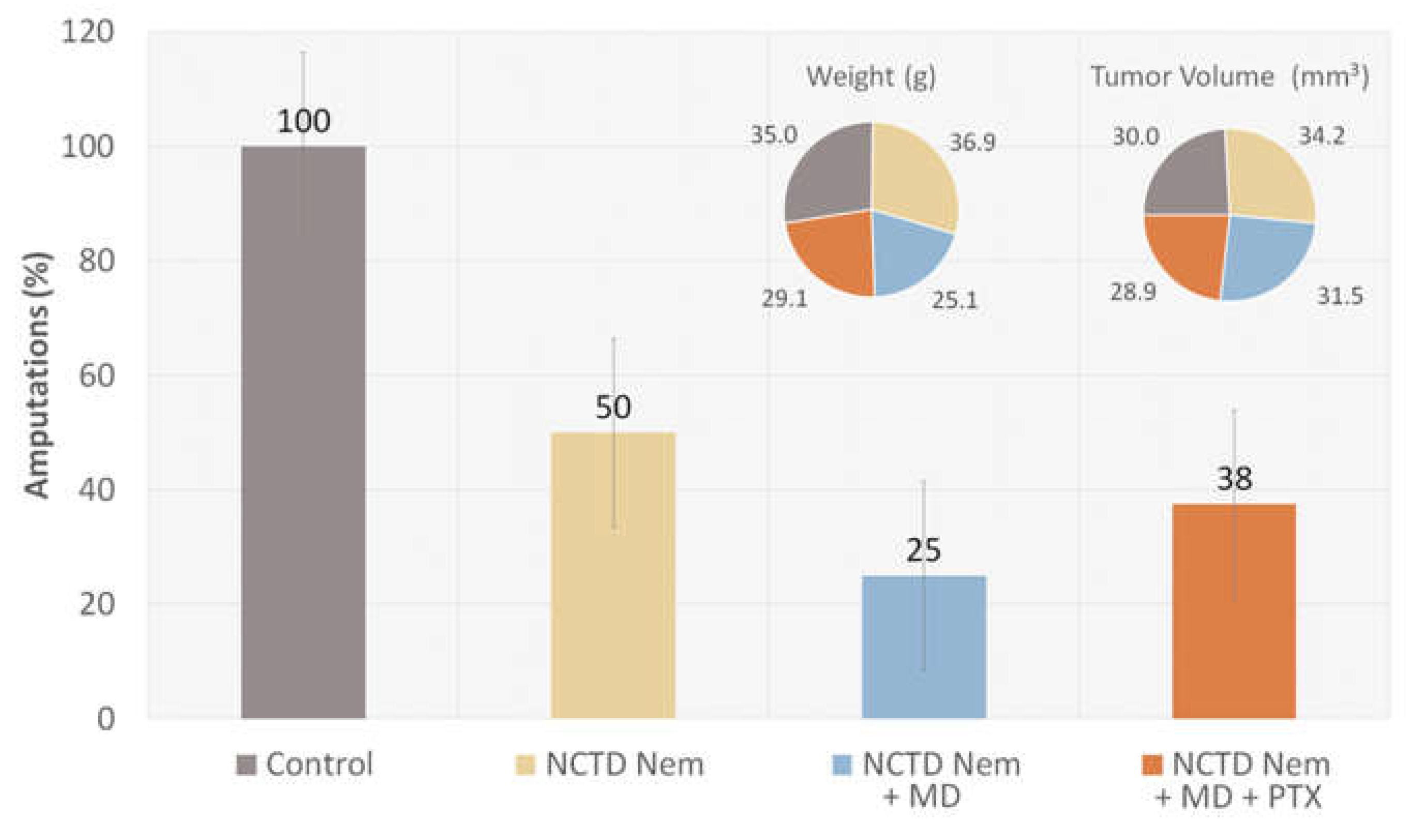
Figure 4.
Systemic bioavailability of NCTD and PTX in serum samples. Data is presented as mg per mL of serum in the different treated groups. Groups are Control, Norcantharidin nanoemulsion NCTDNem , Norcantharidin nanoemulsion applied with microneedle (NCTDNem + MD), Norcantharidin nanoemulsion applied with microneedle and supplemented with pentoxifylline (NCTDNem + MD+PTX). Significance: *: p<0.05; **:p<0.01.
Figure 4.
Systemic bioavailability of NCTD and PTX in serum samples. Data is presented as mg per mL of serum in the different treated groups. Groups are Control, Norcantharidin nanoemulsion NCTDNem , Norcantharidin nanoemulsion applied with microneedle (NCTDNem + MD), Norcantharidin nanoemulsion applied with microneedle and supplemented with pentoxifylline (NCTDNem + MD+PTX). Significance: *: p<0.05; **:p<0.01.

Figure 5.
Multispectral analysis of micrographs from tumor lesion fixed in and tainted histologically). First column hematoxylin and eosin (H&E) tainted samples. Second column: adjusted threshold using the image blue channel. Third column: Binary selection of the particle analysis. Bottom: Particle analysis presented as particle count, total area, and pixel average particle size. Groups are Control, Norcantharidin nanoemulsion NCTDNem , Norcantharidin nanoemulsion applied with microneedle (NCTDNem + MD), Norcantharidin nanoemulsion applied with microneedle and supplemented with pentoxifylline (NCTDNem + MD+PTX. Significance *: p<0.05 .
Figure 5.
Multispectral analysis of micrographs from tumor lesion fixed in and tainted histologically). First column hematoxylin and eosin (H&E) tainted samples. Second column: adjusted threshold using the image blue channel. Third column: Binary selection of the particle analysis. Bottom: Particle analysis presented as particle count, total area, and pixel average particle size. Groups are Control, Norcantharidin nanoemulsion NCTDNem , Norcantharidin nanoemulsion applied with microneedle (NCTDNem + MD), Norcantharidin nanoemulsion applied with microneedle and supplemented with pentoxifylline (NCTDNem + MD+PTX. Significance *: p<0.05 .
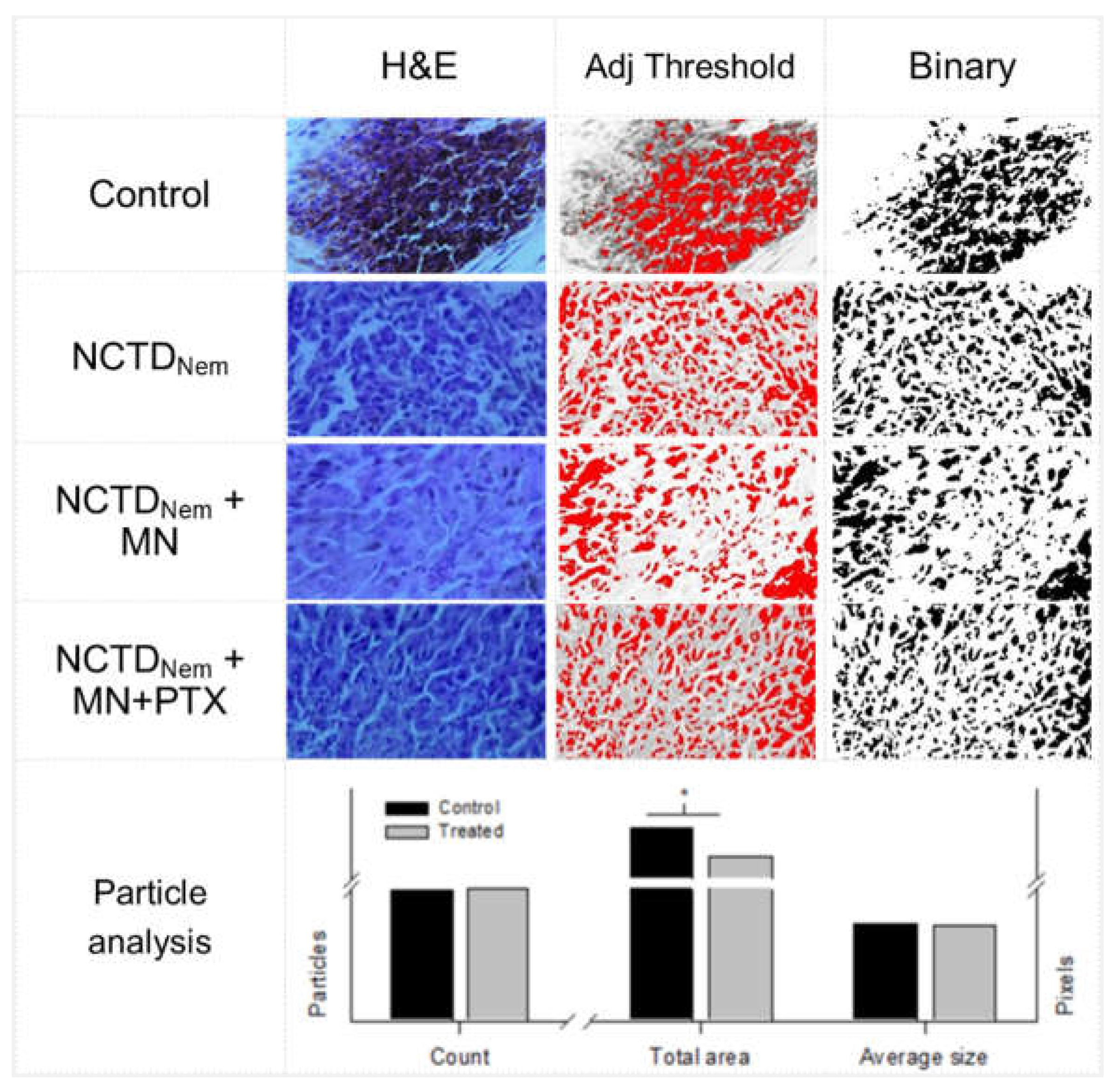
Figure 6.
Nanoemulsion preparation, characterization and application to the syngeneic graft inoculation area. 1) pre-emulsion preparation by mixing the oil phase into the water phase. 2) Nanoemulsion obtention through high-energy sonication. 3) Characterization of the nanoemulsion in droplet size and PDI. 4) Different forms of application forms, direct and using microneedle.
Figure 6.
Nanoemulsion preparation, characterization and application to the syngeneic graft inoculation area. 1) pre-emulsion preparation by mixing the oil phase into the water phase. 2) Nanoemulsion obtention through high-energy sonication. 3) Characterization of the nanoemulsion in droplet size and PDI. 4) Different forms of application forms, direct and using microneedle.
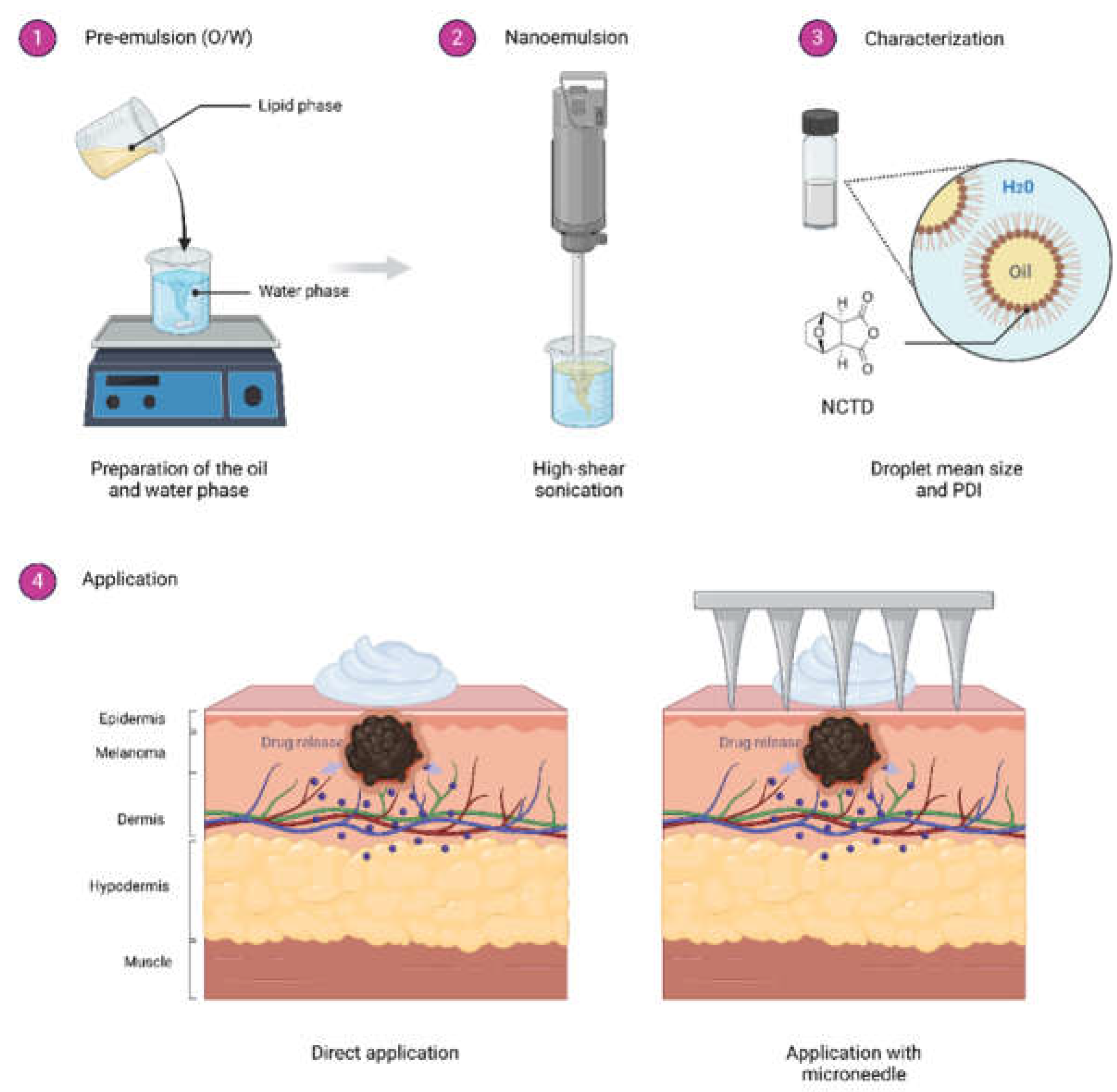

Table 1.
Micrographs field-of-view optical analysis of tumors amputated.
| Group | Size (cm) | +/-S.D | Mitosis | L.I. | Reg |
|---|---|---|---|---|---|
| Control | 0.6 | 0.09 | 1.6 | ** | - |
| NCTD Nem | 0.7 | 0.05 | 1.5 | ** | - |
| NCTD Nem + MD | 0.5 | 0.2 | 1 | *** | + |
| NCTD Nem | 0.6 | 0.2 | 2 | * | - |
* Size data is presented as the mean size of tumors in centimeters (cm) +/- standard deviation (S.D). Mitoses are counted per 1 mm of high-power field (HPF). Lymphocyte infiltration (L.I) was evaluated qualitative from less to more (*<**<***). Regression (Reg) is presented as presence (+) or absence. Groups are Control, Norcantharidin nanoemulsion NCTDNem , Norcantharidin nanoemulsion applied with microneedle (NCTDNem + MD), Norcantharidin nanoemulsion applied with microneedle and supplemented with pentoxifylline (NCTDNem + MD+PTX).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



