
Submitted:
11 July 2024
Posted:
12 July 2024
You are already at the latest version
Abstract
Childhood obesity is a public health problem and most of the interventions are focused on healthy habits as reducing energy intake, avoiding a sedentary lifestyle and increasing physical activity. However, usually they are based in individual programs, with few structured interventions in health systems without satisfactory results. PinPo aims to carry out an integral intervention in children with obesity, as well as in their parents and caregivers, to get motivation to change towards healthy lifestyle habits. The program contains 9 educational grupal sessions directed by a multidisciplinary expert team. 10 boys and girls, and another group with 10 family members and/or caregivers participate in sessions during 90 min biweekly. Moreover, there is an individual adaptation depending on the severity and comorbidities. At the beginning and at the end of the program, an integral evaluation for health status is developed including anthropometric, nutritional, physical activity, and psychologist and analytical measurements. Finally, a satisfaction survey is carried out on the participants.In conclusion, the implementation of PinPo could offer to paediatric patients with obesity and their families, an integral intervention to treat obesity and its complications. So, there are expectations of achieving favorable results that also allow to optimize its effectiveness.
Keywords:
childhood
; grupal intervention
; habits
; obesity
; treatment
1. Introduction
Obesity is a complex chronic disease, with a multifactorial origin that negatively affects health [1]. The incidence of overweight and obesity in the child population has increased considerably in the last decades worldwide [2] being one of the public health challenges of the 21st century [3]. In Spain, more than a third of children are overweight or obese [4]. This condition a higher risk of comorbidities in early stages; and some of them, such as metabolic ones, can appear already in childhood with the consequent risk of developing cardiovascular disease (CVD) and type 2 diabetes [5,6]. Others described such as apnea or asthma, osteoarticular disorders, polycystic ovary syndrome [7], and psychological disorders such as anxiety and depression, attention deficit hyperactivity disorder (ADHD) and eating disorders (ED) [8,9] have also been related to early associated diseases and mortality [10,11] .
Childhood obesity represents one of the great challenges of current healthcare as there are no effective therapies to acquire healthy lifestyle habits that contribute to reduce excess weight and to be maintained over time [12] .Most interventions are aimed to reduce intake and increase physical activity (PA) although working on emotional regulation should be considered both in prevention and treatment [13]. Only in adolescents with morbid obesity and serious comorbidities, some drugs are considered, although the indications and options are still very scarce. Treatment of obesity, in many cases, is also limited by the lack of resources and the difficulty to get and adherence and compliance for it [14].
Therefore, it is necessary to implement strategies to reduce the incidence and prevalence, and to prevent comorbidities from early stages of life. Programs based on the modification of intake, behavior and PA in the school environment [15], community and mainly the family [16,17] seem to have a positive effect on the decrease in body mass index (BMI), especially in the age group of 6 to 12 years. Meta-analyses support the importance of combining behavioral and cognitive-behavioral approaches [18,19]. Interventions with specific approaches in emotional regulation [20], self-esteem [21]; or self-efficacy [22] seem to be promising [23]. In fact, good results have been obtained in some multicomponent programs (nutrition, PA, emotional regulation and family [24]). However, most of the interventions are short and it is necessary to improve their development extending the time and assessing their cost-effectiveness [25]. Moreover, the involvement of different disciplines and the cooperation of all professionals involved in a multidisciplinary program is essential: paediatricians, nurses, nutritionists, psychologists, surgeons, and experts in PA [16].
Traditional individualized treatment with general advice on diet and exercise is the most widespread and used in the clinical practice to address this pathology in childhood. In fact, despite the efforts of the health system, patients and families, it has not been possible to reduce the prevalence of childhood obesity. It seems necessary to implement programs that focus attention also on the physical and emotional health of the child, considering the family and social environment, instead of focus only in weight control, as frequently happens [26], placing above all emphasis in the acquisition of healthy lifestyle habits through health education aimed at children and their environment. So, the therapeutic approach should be designed by a multidisciplinary expert team that jointly contemplates all the aspects that occur in the develop and maintenance of obesity in children, and that can be evaluable not only by professionals, but also by patients, and families. Thus, the main objective of this work is to design a protocol to carry out a group-based therapeutic intervention program, with the participation of families of paediatric patients with obesity (PinPo Program: Program for intervention in Pediatric obesity).
2. Materials and Methods
This multidisciplinary intervention is based on a method of grouping family members/main caregivers, and pediatric patients with obesity. The selection of patients, clinical evaluation, as well as the design and development of the intervention will be carried out by professionals from the Spanish public health system with specific functions (Figure 1).
The PinPo intervention program is based on 9 educational sessions aimed at a group of 10 children with obesity and another group of family members and/or main caregivers.
Subjects
The sample of children with obesity will come from childhood obesity care units in a Spanish tertiary public hospital. The invitation to participate in the program will be made by the pediatricians and/or nurses who have specific knowledge about childhood obesity. The inclusion criteria are: children between 6 and 12 years old, with a BMI greater than p99 according to Cole criteria [27], and without any other underlying pathology except comorbidities associated with obesity, and/or therapeutic failure in primary care. The exclusion criteria are: children under 6 years of age or over 12 years of age, or those children with endogenous obesity or other chronic pathologies known or detected during the study, or children with intervention in other centers at once.
Ethical Aspects
The research protocol of this study has been approved by the Ethics Committee in Córdoba (Spain) (CEIC Córdoba: Acta 278/Ref. 3935) and it has been registered in Clinical Trials.gov (NCT06457412). This study follows the standards of the Declaration of Helsinki. Parents or legal representative, as well as children, will receive a detailed description of the study and families will be included in the study after sign the informed consent forms for participation.
Health Status Assessment
Health evaluation will be carried out before starting the group intervention. After finishing the intervention, two visits will be made at 3 and 6 months. Subsequently, children will continue monitorization in specialized visits as appropriate.
Clinical History and Physical Examination
A medical history and a physical examination, including the evaluation of sexual maturity according to Tanner’s five stages, will be assessed [28]. Anthropometric measurements and blood pressure will be taken by a single examiner. During the physical examination, participants will be dressed in light clothing and barefoot. Systolic (SBP) and diastolic (DBP) blood pressure will be measured twice in the participants’ right arm, using an electronic manometer (M6, HEM-7001-E, Omron®, Tokio, Japan), with a 5 min interval. If measures differed more than 20%, an additional measurement will be considered. The mean value is calculated as the average of the two closest measurements.
Adiposity, weight and height will be measured by trained registered dietitians. A precision scale (TANITA MS780SMA) will be used to measure body weight (kg) and body fat mass (kg). The height and waist circumference (cm) will be also evaluated [29], by a portable stadiometer (SECA 213) and a measuring tape (SECA 201), respectively. Weight status will be estimated according to BMI and categorized in underweight/normal weight or overweight/obesity according to the cut off points defined by Cole and Lobstein [27]. The fat mass index (FMI) is calculated as body fat mass (kg)/height (square meters) [30].
Nutritional Assessment
Nutritional data will be collected through a 3-day dietary record (3d-DR), including two weekdays and one nonconsecutive holiday to obtain information on the quantities of food consumed and assess macronutrients and fatty acids composition, both before and at the end of the program. When the 3d-DR is provided, trained dieticians will carefully inform the families on how to detail their children’s food consumption, explaining useful homemade measures to improve the reliability of data collection. A table with visual support (food pictures) to help identify food weights with the homemade measures [31] will be provided along with the 3d-DR. Nutritional information (energy intake, macro and micronutrients) of the meals will be obtained from the EvalFINUT computer application (EvalFINUT 2.0, Granada, Spain) from the Iberoamerican Foundation of Nutrition [32].
The dietary intake assessment will be conducted using a recently validated semi-quantitative food frequency questionnaire (FFQ) tailored for children, which includes common foods consumed in Spain [33]. Parents or caregivers will be interviewed by a trained dietician, both before and at the end of the program. Consumption frequency of each food item in the last four weeks will be recorded as never or hardly ever (1–3 times per month; once, 2–4 or 5–6 times per week; and once, 2–3, 4–6 or >6 times per day). Food intake data will be converted into daily food volume/weight (in ml or g) to calculate the nutritional information (energy intake, macro and micronutrients) using the EvalFINUT computer application [32]. The 3d-DR and FFQ tests will be part of the trial period (run-in). If families are not available to complete these questionnaires, they will not proceed to the intervention phase.
Psychological Evaluation
This will be carried out on the program patients at the beginning (pre-intervention) and at the end of the intervention (post-intervention), and in a similar way or as required, a follow-up will be carried out after the end of the program.
To evaluate the emotional eating factor, the Three Factor Eating Questionnaire-R21 for children and adolescents [34] will be used. To measure the extent to which children felt able to regulate their negative emotions, the Regulatory Emotional Self-Efficacy Scale (RESE [35]) adapted to children will be also filled out. A short Spanish version of the Positive Affect and Negative Affect Scale (PANAS [36]), which is divided into two factors: positive affect (PA) and negative affect (NA) will be also considered. Satisfaction with life and self-esteem will be also measured using the Satisfaction With Life Scale questionnaire (SWLS [37]), and the Rosenberg scale adapted to children [38] respectively. Social support will be measured through the Multidimensional Scale of Perceived Social Support (MSPSS [39]) that assesses through 12 items the perception of support received from three social groups/factors: family, friends and significant others. Perceived ability related to the control of eating behaviors will be assessed through the Weight Efficacy Lifestyle scale (WEL [40]).
Some studies highlight the importance of parental support for healthy eating in children and find a strong influence of parents’ eating habits on their children’s eating behaviors [41,42]. For this reason, some variables will be also evaluated in parents through the Regulatory Scale of Emotional Self-Efficacy (RESE [35]) a short version in Spanish of the Positive Affect and Negative Affect Scale (PANAS [43]); parents’ expectations about positive and negative outcomes regarding their children with weight problems when trying to maintain a healthy diet [44] and Children’s Eating Behavior Questionnaire (CEBQ [45]; that evaluates the eating behavior styles of minors associated with obesity based on their parents. To know the parents’ self-efficacy for adherence to the Mediterranean diet, the Self-Efficacy Scale for Adherence to the Mediterranean Diet (SESAMeD [46]) will be used.
General Biochemical and Metabolic Parameters, and Intestinal Microbiota Anaylisis
Blood extractions will be performed at rest after 12 hours of overnight fasting, using a venous line in the arm. They will be carried out before starting the intervention, and after 6 months. All samples will be processed within 2 hours of extraction.
An hematimetry and general biochemical parameters will be determined: glucose (mg/dl), urea (mg/dl), creatinine (mg/dl), urate (mg/dl ), calcium (mg/dl) and protein-corrected calcium (mg/dl), protein (g/dl), sodium (mEq/l), potassium (mEq/l), chloride (mEq/l), iron (μg /dl), ferritin (ng/ml), aspartate aminotransferase (AST) (U/l) and alanine aminotransferase (ALT) (U/l), TAG (mg/dl), total cholesterol (mg/dl), HDL- c (mg/dl), LDL-c (mg/dl), apo A-I (mg/dl) and apo B (mg/dl) and insulin (mU/L), as well as ultrasensitive c-reactive protein (CRP). These will be determined by previously normalized colorimetric, enzymatic, kinetic, indirect potentiometry or immunoturbidimetry methods, using an automatic autoanalyzer (Architect c16000 and i2000SR autoanalyzers from Abbott Diagnostics®, and Advia 120 Hematology System from Bayer®). From the data obtained, the following relationships will be calculated: HDL-c/ LDL-c, HDL-c/ total cholesterol, and apo A-I/ apo-B. Insulin resistance will be calculated according to the equation HOMA-IR = glucose (mM) x insulin (μU/mL)/ 22.5. The leftover sample will be processed and stored at -80 °C for future determinations, such as inflammatory or hormonal biomarkers.
In addition, a stool sample will be requested before starting the study and after finishing it, with the aim of analyzing changes in the intestinal microbiota after the intervention. So, stool samples will be collected in sterile plastic bottles stored at -80ºC. DNA extraction will be carried out with the QIAamp DNA stool mini kit (QIAGEN, Barcelona, Spain). Subsequently, quantification will be carried out in a NanoDrop ND-1000 spectrophotometer (Nano-Drop Technologies). The DNA samples received will be amplified in the V3-V1 variable region of the 16S ribosomal RNA gene with a size of 600 base pairs (bp), using primers marked with barcodes. Massive polymerase chain reaction (PCR) amplification sequencing will be performed on the Roche/454 GS Titanium equipment (Branford, CT, USA). A taxonomic analysis will also be performed; The sequences will be selected to estimate the total bacterial diversity of the DNA samples in a comparable way. The selected sequences will undergo analysis with the RDP (Ribosomal data project) platform to define operational taxonomic units.
Design of the PinPo Group Intervention Program
The PinPo program will be developed in health facilities that allow group sessions for paediatric patients with professionals, and simultaneously but independently, sessions with family members/caregivers, also led by experts, with similar themes in both groups. It will contain 9 sessions; each session will last 90 minutes and will be held in the afternoon every 15 days to facilitate family attendance.
The elaboration of the content, the graphic format and the technological applications for each session have been designed by some of the professionals of the multidisciplinary team and are registered with intellectual property code 2007144741729 [47] (Figure 2).
Through the development of the different sessions, the aim is to educate in healthy lifestyle habits, with dynamic content adapted to each group. The topics include information on nutrition, PA, and social and psychological aspects. To adapt the content specifically to the group of children with obesity, graphic material has been designed with children’s characters and stories in relation to the theme that will be worked on in each session. In addition, there is parallel content to work with family members in group sessions. Moreover, in order to standardize the intervention, all professionals involved will receive a specific training based on a guide designed to the development for sessions.
Group Intervention
The content of the sessions is presented through notebooks with a central topic that will be addressed relating food, PA, and emotions, and maintaining a similar structure in each session for the group of children and adults (Figure 3A,B).
Each session will address a central topic and it will associating other concepts related with sedentarism or PA, o related to self-esteem, stigmatization, and motivation to change (Table 1).
On the other hand, after the assessment of the nutritional and health status, and at the beginning of the intervention program, an interview will be carried out with the entire family and the patient with the nurse to know and be able to adapt the objectives to the individual conditions of the child regarding to their preferences and beliefs, gradually introducing the pertinent changes in each case in relation to the topic worked on in the group. To do this, a weekly follow-up will be carried out by telephone call to each family. The objectives will be set consensually through an agreement between both parties, the professional and the child (and their family), in relation to what is perceived as an achievable and feasible goal. The achievements made in previous sessions should also be considered to increase motivation and adherence to change.
For this purpose, the program incorporates gamification through a video game to promote PA at home. Children can achieve personal PA challenges and receive recommendations and advice through animated characters. In addition, they have access to other PA sessions by videos, with exercises for every day.
The intervention for emotional regulation will be carried out in each of the sessions. However, in the final phase of the program, special emphasis will be placed on this treatment. For them, the Unified Protocol for the Transdiagnostic Treatment of Emotional Disorders in Children and Adolescents will be used [48]. It will be held in the last 3 face-to-face group sessions, in addition to two online sessions through an ERES mobile application adaptation. The ERES intervention is nourished by the principles of transdiagnostic therapy [48], various techniques in emotional regulation and work on emotional regulation through eHealth [49]. Self-efficacy, self-concept and self-esteem will be addressed transversally, in addition to emotions related to intake [50,51]. In the first session, motivation for change and the therapeutic relationship for adherence to the intervention will be specifically worked on.
At the end of the intervention, an online satisfaction survey with 10 questions will be carried out to caregivers.
3. Discussion
The incidence and prevalence of childhood overweight and obesity remain high, and interventions effectiveness has shown low success. The prevention and treatment of childhood obesity requires effective strategies that allow changes to be maintained in the medium and long term.
Schools are main places of socialization and education during childhood. So, in the prevention for childhood obesity, a variety of school programs with different designs and outcomes have been developed [52,53] although they had diversity in study design, quality, or duration of interventions. The VIASANO community program aimed to reduce the prevalence of overweight in children aged 3 to 6 years. The intervention lasted 3 years and was based in the control of marketing and education in nutritional techniques. Preliminary follow-up results showed a decrease in the prevalence of overweight (-2.1%) and obesity (-2.4%) after carrying out the program [54]. Other promising results were found in the VIF Program which was performed on patient between 5 and 11 years old promoting PA, a healthy diet, sleep habits and well-being status. The prevalence of overweight and obesity in children from pre-schools (18.1% vs 13.0%) and primary schools (20.9% vs 16.9%) (P < 0.05) decreased through 7 years [52]. Authors suggest that age can be decisive in the success of programs. However, other related factors as the time of evolution of obesity and the roots of lifestyle habits related with age should be also considered.
It has been shown that social vulnerability can condition a higher risk for non-healthy dietary patterns (shorter breastfeeding time, higher consumption of ultra-processed foods [55] as well as incorrect sleep pattern [56] and increased screen time. Likewise, lower adherence to family obesity treatment programs has been documented in families with low socioeconomic resources [57] or the contrary in families with higher educational levels [58]. So, other factors as educational or socioeconomic family status, as well as other evaluation methods not only based in BMI changes, should be considered in the design for development and evaluation of intervention programs in children with obesity [59].
Group therapy has given promising results in different pathologies [60], and there are some examples of approaches against obesity [61]. An educational program within a controlled group therapy aims to offer the patient and their family, personalized medicine tools to intervene on their pathology from a comprehensive perspective: greater motivation to change, acquisition and greater adherence to healthy lifestyle habits, knowledge of calorie level of food, and a psychological approach focused especially on improving the self-esteem of pediatric patients with obesity. So, family-based therapy, in which parents and children participate actively is one of the emerging interventions in the treatment of childhood obesity. Families learn to make healthy decisions about nutrition and PA. The empowerment of patients and caregivers can also help to generate greater motivation for change and an improvement in the psychosocial state of the patient and their family [62].
These programs are not accessible to the entire population, so the digitalization offering electronic health programs has been proposed as a promising alternative. Family-based behavior change e-health programs in school-aged children have had a significant impact on weight loss and lifestyle habits. However, the effectiveness is limited because they focus on parents or children separately, and not considering the family unit. Moreover, measures program effectiveness is based only in weight changes [63]. According to a systematic review and meta-analysis carried out by Salam et al [19], the combination of dietary and exercise interventions could lead to a significant decrease in BMI. However, adding behavioral modifications such as family-based or cognitive behavioral therapies to dietary and PA interventions could have a greater impact adding other beneficial effects as improvement in psychological status, or in healthy habits, to ensure a better health for long time [64].
PinPo program has been designed to be carried out to address the treatment for paediatric patients with severe obesity. This condition could influence the expected results based in the reduction for BMI as in other studies considered. This greater severity probably maintained over time, can modulate the initial interest in participants; to improve their health or, on the contrary, with a low motivation to adhere to health guidelines and behaviors [17]. Likewise, as commented, the age and time of evolution in different pathologies can influence the results. It has been shown that the success of obesity interventions is greater when patients are referred at an early age [16]. Socio-educational level of the caregivers should be also considered because they can also affect motivation and adherence to the program [65]. In PinPo, this level will not determine the choice to enter in the program, although it may be considered in statistical associations.
In a recent non-randomized controlled trial [66] with a 52-week follow-up in children with obesity between 7 and 14 years of age in a multicomponent camp. For 10 weeks, an intervention was carried out focused on a diet balanced in macronutrients and a slight increase in protein consumption, with restriction of ultra-processed foods. In the intervention group, the goal was to replace carbohydrate-rich foods at breakfast and two intermediate meals with foods containing natural proteins (e.g., dairy products, nuts, eggs, meat products) to increase the amount of protein of ~ 10-15E% to ~25E% per day with minimal changes in total caloric intake. In the middle of the intervention, a family education session was held, participating in social and physical activities. From baseline to 10 weeks, there were no differences between groups in anthropometry or metabolic biomarkers. Following these results, the subgroups were grouped to investigate the overall effect of the camp on lifestyle. From week 10 to week 52 of follow-up, children showed lower BMI and body fat compared to baseline. Additionally, they had a reduction in cardiometabolic risk factors, liver markers, and uric acid after 10 weeks, suggesting favorable changes in metabolic health, that maintained at the 52-week follow-up. In line with this work, PinPo program focus not only on dietary habits but also in PA and psychological aspects. Moreover, through the methodology for evaluation anthropometric and body composition changes as well as other metabolic or cardiovascular risk factors, or in the microbiota as well as on variables of psychological health status, specific modifications can be done to adapt the program to improve the efficacy in different areas.
To develop an intervention to treat childhood obesity, there are other considerations to take in account. Some authors have observed that absence of a multidisciplinary team and the lack of time for adequate advice due to the high demand in primary care consultations condition unsatisfactory results in these interventions [67,68]. A study with 2-year of intervention in patients between 2-6 years of age in primary care based on motivational interviews, educational modules focused on healthy habits (reducing time in front of screens and the consumption of ultra-processed foods) and a subsequent year of follow-up with intervention visits and behavioral reinforcement, showed an adherence to the program only of 20% of the recruited patients. They did not show significant global changes in the reduction of BMI, although they obtained beneficial results changing some habits as in the reduction of screen time and improving in walking. Other intervention with a family behavior-based weight management program (FB-WMG) from primary care showed a better evolution in BMI in the 6-month follow-up period [69]. In PinPo, the coordinated and joint work of the experts can lead to good results, although the fact that it is carried out in an area close to the hospital could lead to lower adherence due to transportation difficulties, or lack of time, as well as a lower initial bond of professionals with the family, which is expected to be reinforced throughout the intervention.
In childhood obesity programs, multidisciplinary work and an approach that considers psychosocial variables is necessary. Emotional regulation and self-efficacy, understood as the confidence that an individual has in the ability to carry out various behaviors or attitudes in challenging situations must be specially considered in the evaluation and intervention [70,71] Ames et al [71] showed that the presence of self-efficacy in children helps them to lead a healthy life in relation to eating and PA. On the other hand, emotions can have a strong influence on eating self-efficacy, with results indicating more difficulties in resisting eating when people experience negative emotions, social pressure or difficulties for food accessibility. Difficulties in managing low mood and stress can lead to increased eating patterns or consumption of unhealthy foods, as well as other habits that contribute to obesity. This can result in perpetuation of overweight and obesity, or weight gain [72,73]. It is also important to consider the psychological variables of the parents [41]. It seems that parents’ ability to regulate their emotions might influence their perceived self-efficacy to care for their child’s health, but also their children’s consumption specially, for sweets and soft drinks [9,42].
PinPo would benefit from its multi-component approach [18,19,24], family bases approach [74,75] and its eHealth, or mobile health (mHealth), modules [76]. A chronic disease management requires sustained care over time, mHealth intervention appear as a suitable approach when devising psychological status as a novel and effective alternative to promote healthy behaviors [76]. This technology is also more cost-effective and therefore leads to a greater financial savings for healthcare systems. Furthermore, given the population’s internet connectivity, it is an accessible and attractive methodology for children and young people [77,78], highlighting the possible benefits obtained by combining it with face-to-face sessions [77].
4. Conclusions
The design and implementation of PinPo after considering specific aspects of improvement described in the literature in other previous interventions, could offer to paediatric patients with obesity and their families, an integral intervention to treat obesity and its complications. So, there are expectations of achieving favorable results to improve the adherence to healthy habits and health status.
5. Patents
The elaboration of the content, the graphic format and the technological applications for each session have been designed by some of the professionals of the multidisciplinary team and are registered with intellectual property code 2007144741729 [47].
Author Contributions
“Conceptualization, MG-C and KF-R.; methodology, all the authors; writing—original draft preparation, all the authors; writing—review and editing MJC-M, BL and MG-C.; visualization, all the authors.; supervision, MG-C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. Edition of graphic material has been funded by COVAP.
Institutional Review Board Statement
This project has been approved by the Ethics Committee in Córdoba (Spain) (CEIC Córdoba: Acta 278/Ref. 3935) in Reina Sofia University Hospital (Córdoba, Spain).
Informed Consent Statement
The selected subjects were informed, and written consent was obtained. Participants under 18 years of age consented verbally, and written consent was signed by their parents or legal guardians.
Data Availability Statement
Data is contained within the article.
Acknowledgments
Authors would especially like to thank all the PinPo participants and their parents or caregivers.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships without potential conflicts of interest.
References
- Alberto Moreno Aznar L, Lorenzo Garrido H, Aznar M LA, Garrido Obesidad LH. Obesidad infantil. Available from: www.aeped.es/protocolos/.
- Obesity and overweight [Internet]. [cited 2024 Jul 8]. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
- Pulungan AB, Puteri HA, Ratnasari AF, Hoey H, Utari A, Darendeliler F, et al. Childhood Obesity as a Global Problem: a Cross-sectional Survey on Global Awareness and National Program Implementation. J Clin Res Pediatr Endocrinol [Internet]. 2024 Mar 11 [cited 2024 Jul 3];16(1):31–40. Available from: https://pubmed.ncbi.nlm.nih.gov/37622285/.
- Aesan - Agencia Española de Seguridad Alimentaria y Nutrición [Internet]. [cited 2024 Jul 8]. Available from: https://www.aesan.gob.es/AECOSAN/web/nutricion/detalle/aladino_2023.htm.
- Olza J, Gil-Campos M, Leis R, Bueno G, Aguilera CM, Valle M, et al. Presence of the metabolic syndrome in obese children at prepubertal age. Ann Nutr Metab [Internet]. 2011 Oct [cited 2024 Jul 3];58(4):343–50. Available from: https://pubmed.ncbi.nlm.nih.gov/21996789/.
- Pulgarón, ER. Childhood obesity: a review of increased risk for physical and psychological comorbidities. Clin Ther [Internet]. 2013 Jan [cited 2024 Jul 3];35(1). Available from: https://pubmed.ncbi.nlm.nih.gov/23328273/.
- Ciężki S, Odyjewska E, Bossowski A, Głowińska-Olszewska B. Not Only Metabolic Complications of Childhood Obesity. Vol. 16, Nutrients. Multidisciplinary Digital Publishing Institute (MDPI); 2024.
- Smith KE, Mason TB. Psychiatric comorbidity associated with weight status in 9 to 10 year old children. Pediatr Obes. 2022 May 1;17(5).
- Smith JD, Fu E, Kobayashi MA. Prevention and Management of Childhood Obesity and its Psychological and Health Comorbidities. Annu Rev Clin Psychol [Internet]. 2020 May 5 [cited 2024 Jul 3];16:351. Available from: /pmc/articles/PMC7259820/.
- Powell-Wiley TM, Baumer Y, Baah FO, Baez AS, Farmer N, Mahlobo CT, et al. Social Determinants of Cardiovascular Disease. Circ Res [Internet]. 2022 Mar 4 [cited 2024 Jul 2];130(5):782–99. Available from: https://pubmed.ncbi.nlm.nih.gov/35239404/.
- Chait A, den Hartigh LJ. Adipose Tissue Distribution, Inflammation and Its Metabolic Consequences, Including Diabetes and Cardiovascular Disease. Front Cardiovasc Med [Internet]. 2020 Feb 25 [cited 2024 Jul 3];7. Available from: https://pubmed.ncbi.nlm.nih.gov/32158768/.
- Mandelbaum J, Harrison SE. Perceived challenges to implementing childhood obesity prevention strategies in pediatric primary care. SSM - Qualitative Research in Health. 2022 Dec 1;2:100185.
- Aparicio E, Canals J, Arija V, De Henauw S, Michels N. The role of emotion regulation in childhood obesity: implications for prevention and treatment. Nutr Res Rev [Internet]. 2016 Jun 1 [cited 2024 Jul 3];29(1):17–29. Available from: https://pubmed.ncbi.nlm.nih.gov/27045966/.
- Brown T, Moore TH, Hooper L, Gao Y, Zayegh A, Ijaz S, et al. Interventions for preventing obesity in children. Cochrane Database Syst Rev [Internet]. 2019 Jul 23 [cited 2024 Jul 2];7(7). Available from: https://pubmed.ncbi.nlm.nih.gov/31332776/.
- Wyatt KM, Lloyd JJ, Abraham C, Creanor S, Dean S, Densham E, et al. The Healthy Lifestyles Programme (HeLP), a novel school-based intervention to prevent obesity in school children: Study protocol for a randomised controlled trial. Trials. 2013 Apr 4;14(1).
- Marten KA, Allen DB, Rehm J, Vanderwall C, Peterson AL, Carrel AL. A Multidisciplinary Approach to Pediatric Obesity Shows Improvement Postintervention. Acad Pediatr [Internet]. 2023 Jul 1 [cited 2024 Jul 2];23(5):947–51. Available from: https://pubmed.ncbi.nlm.nih.gov/36441091/.
- Rojo M, Lacruz T, Santos Solano |, Gutiérrez A, Sepúlveda AR, Sepulveda AR. Family-reported barriers and predictors of short-term attendance in a multidisciplinary intervention for managing childhood obesity: A psycho-family-system based randomised controlled trial (ENTREN-F) |. 2 | Montserrat Graell [Internet]. 2022 [cited 2024 Jul 2];3:4. Available from: https://onlinelibrary.wiley.com/doi/10.1002/erv.2913.
- Baygi F, Djalalinia S, Qorbani M, Larrabee Sonderlund A, Kousgaard Andersen MK, Thilsing T, et al. The effect of psychological interventions targeting overweight and obesity in school-aged children: a systematic review and meta-analysis. BMC Public Health [Internet]. 2023 Dec 1 [cited 2024 Jul 2];23(1). Available from: https://pubmed.ncbi.nlm.nih.gov/37537523/.
- Salam RA, Padhani ZA, Das JK, Shaikh AY, Hoodbhoy Z, Jeelani SM, et al. Effects of Lifestyle Modification Interventions to Prevent and Manage Child and Adolescent Obesity: A Systematic Review and Meta-Analysis. Nutrients [Internet]. 2020 Aug 1 [cited 2024 Jul 2];12(8):1–23. Available from: https://pubmed.ncbi.nlm.nih.gov/32722112/.
- Miri SF, Javadi M, Lin CY, Griffiths MD, Björk M, Pakpour AH. Effectiveness of cognitive-behavioral therapy on nutrition improvement and weight of overweight and obese adolescents: A randomized controlled trial. Diabetes Metab Syndr [Internet]. 2019 May 1 [cited 2024 Jul 3];13(3):2190–7. Available from: https://pubmed.ncbi.nlm.nih.gov/31235156/.
- M Bartelink NH, Mulkens S, Mujakovic S, J Jansen MW, J MW. Long-term effects of the RealFit intervention on self-esteem and food craving. Child Care in Practice [Internet]. 2018 [cited 2024 Jul 3];24(1):65–75. Available from: https://www.tandfonline.com/action/journalInformation?journalCode=cccp20.
- Danielsen YS, Nordhus IH, Júlíusson PB, Mæhle M, Pallesen S. Effect of a family-based cognitive behavioural intervention on body mass index, self-esteem and symptoms of depression in children with obesity (aged 7-13): a randomised waiting list controlled trial. Obes Res Clin Pract [Internet]. 2013 Mar [cited 2024 Jul 2];7(2). Available from: https://pubmed.ncbi.nlm.nih.gov/24331773/.
- Flores-Vázquez AS, Rodríguez-Rocha NP, Herrera-Echauri DD, Macedo-Ojeda G. A systematic review of educational nutrition interventions based on behavioral theories in school adolescents. Appetite [Internet]. 2024 Jan 1 [cited 2024 Jul 2];192. Available from: https://pubmed.ncbi.nlm.nih.gov/37865297/.
- Sepúlveda AR, Santos Solano |, Blanco M, Lacruz T, Veiga | Oscar, Solano S. Feasibility, acceptability, and effectiveness of a multidisciplinary intervention in childhood obesity from primary care: Nutrition, physical activity, emotional regulation, and family. Eur Eat Disorders Rev [Internet]. 2020 [cited 2024 Jul 2];28:184–98. Available from: https://onlinelibrary.wiley.com/doi/10.1002/erv.2702.
- Oude Luttikhuis H, Baur L, Jansen H, Shrewsbury VA, O’Malley C, Stolk RP, et al. WITHDRAWN: Interventions for treating obesity in children. Cochrane Database Syst Rev. 2019 Mar 7;3:CD001872.
- Rhee KE, Herrera L, Strong D, DeBenedetto AM, Shi Y, Boutelle KN. Design of the GOT Doc study: A randomized controlled trial comparing a Guided Self-Help obesity treatment program for childhood obesity in the primary care setting to traditional family-based behavioral weight loss. Contemp Clin Trials Commun [Internet]. 2021 Jun 1 [cited 2024 Jul 2];22. Available from: https://pubmed.ncbi.nlm.nih.gov/33997462/.
- Cole TJ, Lobstein T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes [Internet]. 2012 [cited 2024 Jul 2];7(4):284–94. Available from: https://pubmed.ncbi.nlm.nih.gov/22715120/.
- Bornstein, MH. The SAGE Encyclopedia of Lifespan Human Development. The SAGE Encyclopedia of Lifespan Human Development. 2018 Mar 27;
- Garcidueñas-Fimbres TE, Gómez-Martínez C, Pascual-Compte M, Jurado-Castro JM, Leis R, Moreno LA, et al. Adherence to a healthy lifestyle behavior composite score and cardiometabolic risk factors in Spanish children from the CORALS cohort. Eur J Pediatr. 2024 Apr 1;183(4):1819–30.
- VanItallie TB, Yang MU, Heymsfield SB, Funk RC, Boileau RA. Height-normalized indices of the body’s fat-free mass and fat mass: potentially useful indicators of nutritional status. Am J Clin Nutr [Internet]. 1990 [cited 2024 Jul 3];52(6):953–9. Available from: https://pubmed.ncbi.nlm.nih.gov/2239792/.
- Manual de Nutrición Coordinadores: Comité de Nutrición y Lactancia Materna de la AEP. [cited 2024 Jul 3]; Available from: www.luaediciones.com.
- ¿Qué es? - Fundación Iberoamericana de Nutrición [Internet]. [cited 2024 Jul 8]. Available from: https://www.finut.org/evalfinut/.
- Martin-moreno JM, Boyle P, Gorgojo L, Maisonneuve P, Fernandez-rodriguez JC, Salvini S, et al. Development and Validation of a Food Frequency Questionnaire in Spain. Int J Epidemiol [Internet]. 1993 Jun 1 [cited 2024 Jul 3];22(3):512–9. [CrossRef]
- Martín-García M, Vila-Maldonado S, Rodríguez-Gómez I, Faya FM, Plaza-Carmona M, Pastor-Vicedo JC, et al. The Spanish version of the Three Factor Eating Questionnaire-R21 for children and adolescents (TFEQ-R21C): Psychometric analysis and relationships with body composition and fitness variables. Physiol Behav [Internet]. 2016 Oct 15 [cited 2024 Jul 3];165:350–7. Available from: https://pubmed.ncbi.nlm.nih.gov/27538345/.
- Caprara GV, Di Giunta L, Eisenberg N, Gerbino M, Pastorelli C, Tramontano C. Assessing Regulatory Emotional Self-Efficacy in Three Countries. Psychol Assess [Internet]. 2008 Sep [cited 2024 Jul 3];20(3):227. Available from: /pmc/articles/PMC2713723/.
- Sanmartín R, Vicent M, Gonzálvez C, Inglés CJ, Díaz-Herrero Á, Granados L, et al. Positive and Negative Affect Schedule-Short Form: Factorial Invariance and Optimistic and Pessimistic Affective Profiles in Spanish Children. Front Psychol [Internet]. 2018 Mar 23 [cited 2024 Jul 3];9(MAR). Available from: https://pubmed.ncbi.nlm.nih.gov/29628906/.
- Atienza FL, Pons D, Balaguer I, García- Merita M. Propiedades Psicométricas de la Escala de Satisfacción con la Vida en Adolescentes | Psicothema. Psicthrma [Internet]. 2000 [cited 2024 Jul 3];314–9. Available from: https://reunido.uniovi.es/index.php/PST/article/view/7597.
- Wood C, Griffin M, Barton J, Sandercock G. Modification of the Rosenberg Scale to Assess Self-Esteem in Children. Front Public Health [Internet]. 2021 Jun 17 [cited 2024 Jul 3];9. Available from: https://pubmed.ncbi.nlm.nih.gov/34222169/.
- Mosqueda Díaz A, Mendoza Parra S, Jofré Aravena V, Barriga OA. Validez y confiabilidad de una escala de apoyo social percibido en población adolescente. Enfermería Global [Internet]. 2015 [cited 2024 Jul 3];14(39):125–36. Available from: https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1695-61412015000300006&lng=es&nrm=iso&tlng=es.
- Villaécija J, Luque B, Martínez S, Castillo-Mayén R, Cuadrado E, Domínguez-Escribano M, et al. Perceived social support and healthy eating self-efficacy on the well-being of children and adolescents. Revista Iberoamericana de Psicologia y Salud. 2022;13(1):56–72.
- Mahmood L, Flores-Barrantes P, Moreno LA, Manios Y, Gonzalez-Gil EM. The influence of parental dietary behaviors and practices on children’s eating habits. Nutrients [Internet]. 2021 Apr 1 [cited 2024 Jul 2];13(4):1138. Available from: https://www.mdpi.com/2072-6643/13/4/1138/htm.
- Sagui-Henson SJ, Armstrong LM, Mitchell AD, Basquin CA, Levens SM. The Effects of Parental Emotion Regulation Ability on Parenting Self-Efficacy and Child Diet. J Child Fam Stud. 2020 Aug 1;29(8):2290–302.
- López-Gómez I, Hervás G, Vázquez C. Adaptación de las “escalas de afecto positivo y negativo” (PANAS) en una muestra general española. Psicol Conductual [Internet]. 2015 [cited 2024 Jul 3];23:529–48. Available from: https://www.researchgate.net/publication/289993251_An_adaptation_of_the_Positive_and_Negative_Affect_Schedules_PANAS_in_a_Spanish_general_sample.
- Anderson E S, Winett R A, Wojcik J R. Social-cognitive determinants of nutrition behavior among supermarket food shoppers: a structural equation analysis - PubMed. Health Psychol [Internet]. 2000 [cited 2024 Jul 3];5:479–86. Available from: https://pubmed.ncbi.nlm.nih.gov/11007156/.
- Jimeno-Martínez A, Maneschy I, Moreno LA, Bueno-Lozano G, De Miguel-Etayo P, Flores-Rojas K, et al. Reliability and Validation of the Child Eating Behavior Questionnaire in 3- to 6-Year-Old Spanish Children. Front Psychol [Internet]. 2022 May 4 [cited 2024 Jul 3];13. Available from: https://pubmed.ncbi.nlm.nih.gov/35602745/.
- Cuadrado E, Gutiérrez-Domingo T, Castillo-Mayen R, Luque B, Arenas A, Taberneroa C. The Self-Efficacy Scale for Adherence to the Mediterranean Diet (SESAMeD): A scale construction and validation. Appetite [Internet]. 2018 Jan 1 [cited 2024 Jul 3];120:6–15. Available from: https://pubmed.ncbi.nlm.nih.gov/28823625/.
- Safe Creative: Obra #2007144741729 - PinPo [Internet]. [cited 2024 Jul 8]. Available from: https://www.safecreative.org/work/2007144741729-pinpo.%20PinPo.%20Programa%20de%20intervenci%C3%B3n%20grupal%20para%20el%20tratamiento%20de%20la%20obesidad%20infantil.%20Literary%20work%20registry.%20Jun%202020.%20Accessed%2001%20July%202024.?0.
- Ehrenreich-May J, Kennedy SM, Sherman JA, Bilek EL, Barlow DH. Protocolo unificado para el tratamiento transdiagnóstico de los trastornos emocionales en niños - Ediciones Pirámide [Internet]. Piramide; 2022 [cited 2024 Jul 3]. Available from: https://www.edicionespiramide.es/libro/manuales-practicos/protocolo-unificado-para-el-tratamiento-transdiagnostico-de-los-trastornos-emocionales-en-ninos-jill-ehrenreich-may-9788436844344/.
- Sandín B, García-Escalera J, Valiente RM, Espinosa V, Chorot P. Clinical Utility of an Internet-Delivered Version of the Unified Protocol for Transdiagnostic Treatment of Emotional Disorders in Adolescents (iUP-A): A Pilot Open Trial. Int J Environ Res Public Health [Internet]. 2020 Nov 2 [cited 2024 Jul 3];17(22):1–17. Available from: https://pubmed.ncbi.nlm.nih.gov/33182711/.
- MacHt M, Simons G. Emotional eating. Emotion Regulation and Well-Being. 2011;281–95.
- Michels N, Sioen I, Braet C, Eiben G, Hebestreit A, Huybrechts I, et al. Stress, emotional eating behaviour and dietary patterns in children. Appetite [Internet]. 2012 Dec [cited 2024 Jul 3];59(3):762–9. Available from: https://pubmed.ncbi.nlm.nih.gov/22918173/.
- Vanhelst J, Deken V, Boulic G, Raffin S, Duhamel A, Romon M. Trends in prevalence of childhood overweight and obesity in a community-based programme: The VIF Programme. Pediatr Obes. 2021 Jul 1;16(7).
- Sal S, Bektas M. Effectiveness of Obesity Prevention Program Developed for Secondary School Students. Am J Health Educ [Internet]. 2022 Jan 2 [cited 2024 Jul 2];53(1):45–55. Available from: https://www.tandfonline.com/doi/abs/10.1080/19325037.2021.2001774.
- Vinck J, Brohet C, Roillet M, Dramaix M, Borys JM, Beysens J, et al. Downward trends in the prevalence of childhood overweight in two pilot towns taking part in the VIASANO community-based programme in Belgium: Data from a national school health monitoring system. Pediatr Obes. 2016 Feb 1;11(1):61–7.
- de Melo JMM, Dourado BLLFS, de Menezes RCE, Longo-Silva G, da Silveira JAC. Early onset of overweight among children from low-income families: The role of exclusive breastfeeding and maternal intake of ultra-processed food. Pediatr Obes [Internet]. 2021 Dec 1 [cited 2024 Jul 2];16(12). Available from: https://pubmed.ncbi.nlm.nih.gov/34169658/.
- Gibson-Moore H, Chambers L. Sleep matters: Can a good night’s sleep help tackle the obesity crisis? Nutr Bull [Internet]. 2019 Jun 1 [cited 2024 Jul 2];44(2):123–9. Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/nbu.12386.
- Davison GM, Fowler LA, Ramel M, Stein RI, Conlon RPK, Saelens BE, et al. Racial and socioeconomic disparities in the efficacy of a family-based treatment programme for paediatric obesity. Pediatr Obes [Internet]. 2021 Oct 1 [cited 2024 Jul 2];16(10). Available from: https://pubmed.ncbi.nlm.nih.gov/33847074/.
- Conrey SC, Burrell AR, Brokamp C, Burke RM, Couch SC, Niu L, et al. Neighbourhood socio-economic environment predicts adiposity and obesity risk in children under two. Pediatr Obes [Internet]. 2022 Dec 1 [cited 2024 Jul 2];17(12). Available from: https://pubmed.ncbi.nlm.nih.gov/36350200/.
- Scaglioni S, De Cosmi V, Ciappolino V, Parazzini F, Brambilla P, Agostoni C. Factors Influencing Children’s Eating Behaviours. Nutrients [Internet]. 2018 Jun 1 [cited 2024 Jul 2];10(6). Available from: /pmc/articles/PMC6024598/.
- Lloyd J, McHugh C, Minton J, Eke H, Wyatt K. The impact of active stakeholder involvement on recruitment, retention and engagement of schools, children and their families in the cluster randomised controlled trial of the Healthy Lifestyles Programme (HeLP): A school-based intervention to prevent obesity. Trials. 2017 Aug 14;18(1).
- Verónica Marín B, Lorena Rodríguez O, Roxana Buscaglione A, María Luis Aguirre C, Raquel Burrows A, María Isabel Hodgson B, et al. MINSAL-FONASA Pilot Study in obese children and adolescents. Rev Chil Pediatr [Internet]. 2011 [cited 2024 Jul 2];82(1):21–8. Available from: http://www.scielo.cl/scielo.php?script=sci_arttext&pid=S0370-41062011000100003&lng=en&nrm=iso&tlng=es.
- Gago C, Aftosmes-Tobio A, Beckerman-Hsu JP, Oddleifson C, Garcia EA, Lansburg K, et al. Evaluation of a cluster-randomized controlled trial: Communities for Healthy Living, family-centered obesity prevention program for Head Start parents and children. International Journal of Behavioral Nutrition and Physical Activity. 2023 Dec 1;20(1).
- Chai LK, Farletti R, Fathi L, Littlewood R. A Rapid Review of the Impact of Family-Based Digital Interventions for Obesity Prevention and Treatment on Obesity-Related Outcomes in Primary School-Aged Children. Nutrients [Internet]. 2022 Nov 1 [cited 2024 Jul 3];14(22). Available from: https://pubmed.ncbi.nlm.nih.gov/36432522/.
- Viitasalo A, Eloranta AM, Lintu N, Väistö J, Venäläinen T, Kiiskinen S, et al. The effects of a 2-year individualized and family-based lifestyle intervention on physical activity, sedentary behavior and diet in children. Prev Med (Baltim). 2016 Jun 1;87:81–8.
- Jacobs J, Strugnell C, Allender S, Orellana L, Backholer K, Bolton KA, et al. The impact of a community-based intervention on weight, weight-related behaviours and health-related quality of life in primary school children in Victoria, Australia, according to socio-economic position. BMC Public Health [Internet]. 2021 Dec 1 [cited 2024 Jul 2];21(1). Available from: https://pubmed.ncbi.nlm.nih.gov/34837974/.
- Jakobsen DD, Brader L, Bruun JM. Effect of a higher protein diet and lifestyle camp intervention on childhood obesity (The COPE study): results from a nonrandomized controlled trail with 52-weeks follow-up. Eur J Nutr [Internet]. 2024 [cited 2024 Jul 2]; Available from: https://pubmed.ncbi.nlm.nih.gov/38724826/.
- Resnicow K, Delacroix E, Sonneville KR, Considine S, Grundmeier RW, Di Shu, et al. Outcome of BMI2+: Motivational Interviewing to Reduce BMI Through Primary Care AAP PROS Practices. Pediatrics [Internet]. 2024 Feb 1 [cited 2024 Jul 2];153(2). Available from: https://pubmed.ncbi.nlm.nih.gov/38282541/.
- Rifas-Shiman SL, Taveras EM, Gortmaker SL, Hohman KH, Horan CM, Kleinman KP, et al. Two-year follow-up of a primary care-based intervention to prevent and manage childhood obesity: the High Five for Kids study. Pediatr Obes [Internet]. 2017 Jun 1 [cited 2024 Jul 3];12(3):e24–7. Available from: https://pubmed.ncbi.nlm.nih.gov/27231236/.
- Else V, Chen Q, Cortez AB, Koebnick C. Effectiveness of a Family-Centered Pediatric Weight Management Program Integrated in Primary Care - PubMed. Perm J [Internet]. 2020 [cited 2024 Jul 3]; Available from: https://pubmed.ncbi.nlm.nih.gov/33635768/.
- Bandura, A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev [Internet]. 1977 [cited 2024 Jul 3];84(2):191–215. Available from: https://pubmed.ncbi.nlm.nih.gov/847061/.
- Ames GE, Heckman MG, Diehl NN, Grothe KB, Clark MM. Further statistical and clinical validity for the Weight Efficacy Lifestyle Questionnaire-Short Form. Eat Behav [Internet]. 2015 Aug 1 [cited 2024 Jul 3];18:115–9. Available from: https://pubmed.ncbi.nlm.nih.gov/26042918/.
- Ruiz LD, Zuelch ML, Dimitratos SM, Scherr RE. Adolescent Obesity: Diet Quality, Psychosocial Health, and Cardiometabolic Risk Factors. Nutrients [Internet]. 2019 Jan 1 [cited 2024 Jul 3];12(1). Available from: https://pubmed.ncbi.nlm.nih.gov/31877943/.
- Lee EY, Yoon KH. Epidemic obesity in children and adolescents: risk factors and prevention. Front Med [Internet]. 2018 Dec 1 [cited 2024 Jul 3];12(6):658–66. Available from: https://pubmed.ncbi.nlm.nih.gov/30280308/.
- Skelton JA, Vitolins M, Pratt KJ, DeWitt LH, Eagleton SG, Brown C. Rethinking family-based obesity treatment. Clin Obes [Internet]. 2023 Dec 1 [cited 2024 Jul 3];13(6). Available from: https://pubmed.ncbi.nlm.nih.gov/37532265/.
- Yackobovitch-Gavan M, Wolf Linhard D, Nagelberg N, Poraz I, Shalitin S, Phillip M, et al. Intervention for childhood obesity based on parents only or parents and child compared with follow-up alone. Pediatr Obes [Internet]. 2018 Nov 1 [cited 2024 Jul 3];13(11):647–55. Available from: https://pubmed.ncbi.nlm.nih.gov/29345113/.
- Azevedo LB, Stephenson J, Ells L, Adu-Ntiamoah S, DeSmet A, Giles EL, et al. The effectiveness of e-health interventions for the treatment of overweight or obesity in children and adolescents: A systematic review and meta-analysis. Obes Rev [Internet]. 2022 Feb 1 [cited 2024 Jul 3];23(2). Available from: https://pubmed.ncbi.nlm.nih.gov/34747118/.
- Tate EB, Spruijt-Metz D, O’Reilly G, Jordan-Marsh M, Gotsis M, Pentz MA, et al. mHealth approaches to child obesity prevention: successes, unique challenges, and next directions. Transl Behav Med [Internet]. 2013 Dec [cited 2024 Jul 3];3(4):406. Available from: /pmc/articles/PMC3830013/.
- Tozzi F, Nicolaidou I, Galani A, Antoniades A. eHealth Interventions for Anxiety Management Targeting Young Children and Adolescents: Exploratory Review. JMIR Pediatr Parent [Internet]. 2018 Jan 1 [cited 2024 Jul 3];1(1). Available from: /pmc/articles/PMC6716078/.
Figure 1.
Organization chart and distribution of tasks in PinPo program.
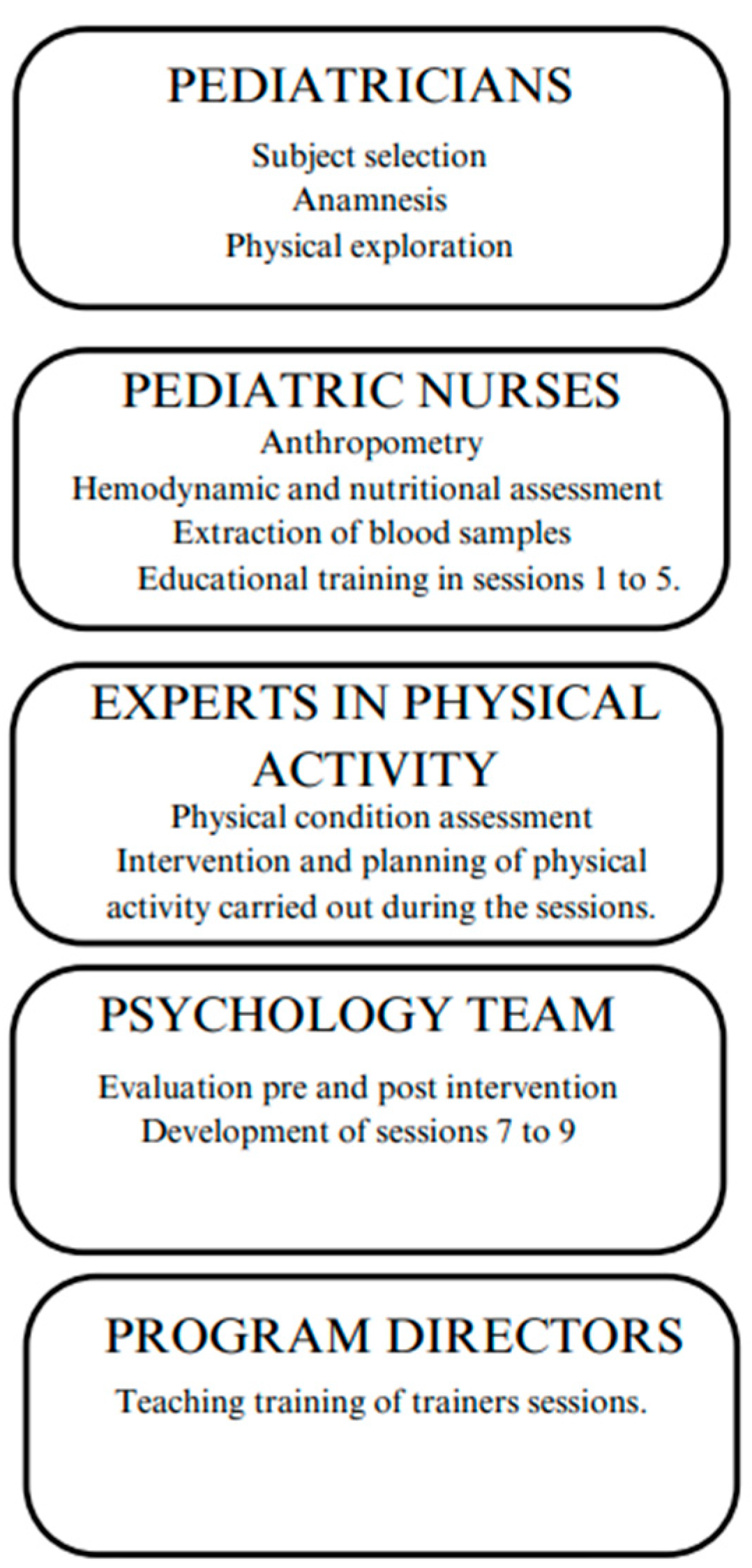
Figure 2.
Notebooks for patient sessions in PinPo program.

Figure 3.
Schedule of PinPo program sessions for caregivers and paediatric patients with obesity, respectively.
Figure 3.
Schedule of PinPo program sessions for caregivers and paediatric patients with obesity, respectively.
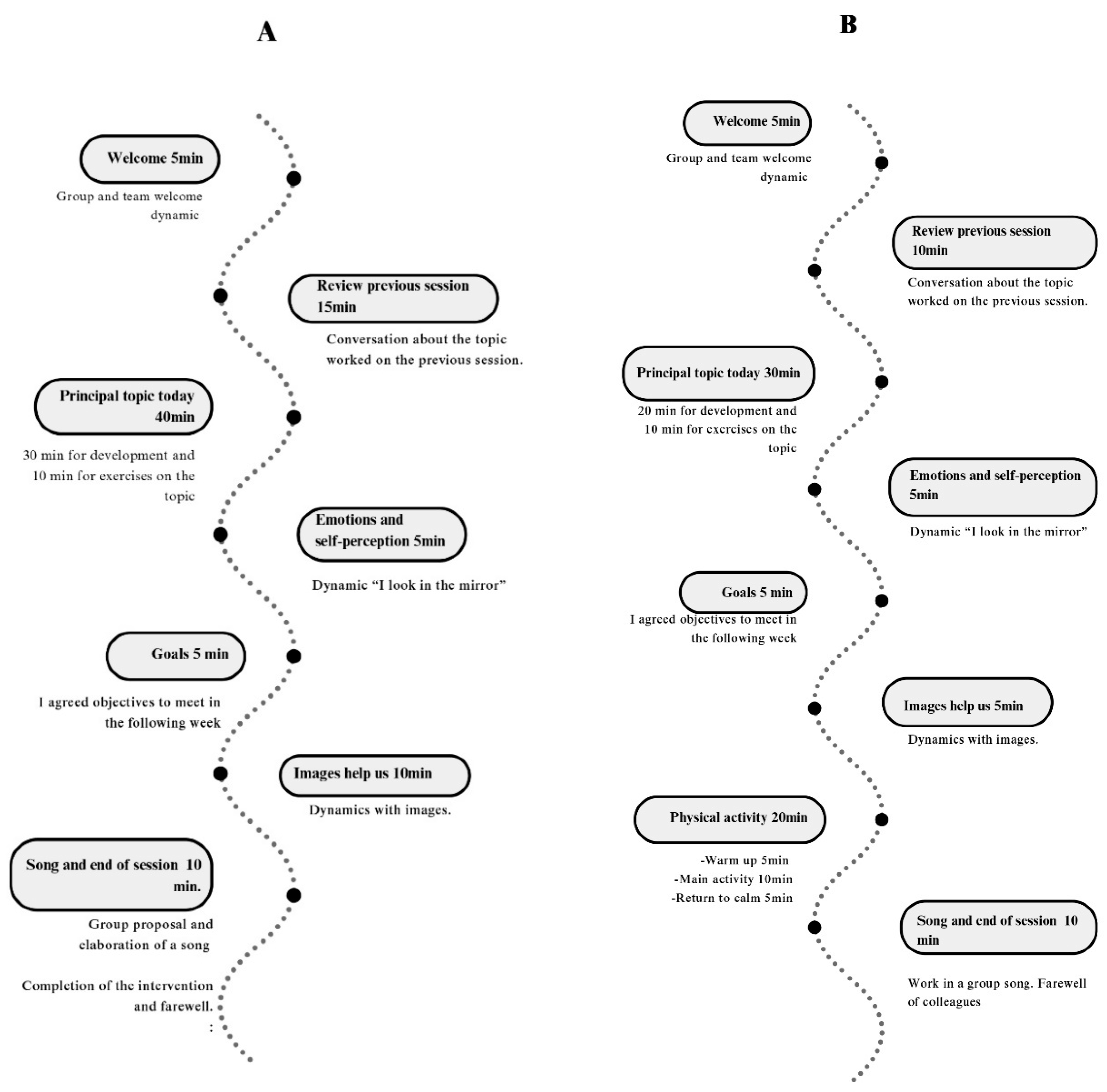

Table 1.
Specific content of 9 sessions of PinPo intervention for paediatric children with obesity.
| PinPo Sessions | Main topic | We look in the mirror | Images help us | Physical activity |
|---|---|---|---|---|
| SESSION 1 Knocking on the door. Will you open me? | -Healthy breakfast. -Food traffic light. -Hand method for food quantities |
-Quiz about breakfast. -Self-criticism and reflection about feelings. |
-Photograph of the pantry and refrigerator for the next session. | -Games with toy food. |
| SESSION 2 My five stars, my five meals. | -Traffic light and breakfast review. -The importance of the five meals. -Our body image. |
-Daily food record. -Write foods and quantities for a day. -Indicate the ultra-limited foods consumed. |
-Check photographs of the pantry and refrigerator. - Sort photos by food groups |
-Carrer. -Vertical jump. |
| SESSION 3 My friends, recess, the park and sports. | - Review of 5 meals and breakfast. -Types and frequency of exercise. -Mid-morning meals and snacks. |
-Record on PA of all family members. | -Search information about traditional games -Attend a friend or family member’s training or match. |
-Relay and cooperative games with balls |
| SESSION 4 My colorful friends, fruits and vegetables. | -Review of 5 meals, breakfast and physical activity. -Importance of fruit and vegetable consumption. -Food composition. |
- Write down the number of fruits and vegetables consumed in a day. | -Review the menus prior to starting the program. -Take photos of menus for the next session. |
-Games with balloons. |
| SESSION 5 Knowing nutrients, my new way of cooking. | -Nutritional labels. -Nutritional traffic light. -Content of main meal and dinners. -Ways of cooking. |
-Answer and debate the questions in this section. -Complete table on the nutrients of traditional meals. |
-Check photos of meals and write down the number of colors. -Bring food labels to analyze in the next session. |
-Games and exercises in pairs with tennis balls. |
| SESSION 6 My inner self: self-esteem. | -Self-esteem. Importance of expressing feelings -Types of communication |
-Self-criticism and debate on issues related to self-esteem and emotional regulation. | -Analyze the labels that we have brought from home. | -Individual challenges: exercises on the floor and with a chair. -Group challenges: races in pairs, balloon transfers. |
| SESSION 7 Obstacles, relapses… I am going to build. | -Recognize our feelings and express them. -Mediterranean diet -Food pyramid. |
-Test of adherence to the Mediterranean diet. | -Analyze food pyramid and healthy habits. |
-Animal Flow: Make movements of each animal. |
| SESSION 8 My new resolutions with my new friends. | -Relapses -School bullying -Motivation |
-Importance of meeting objectives. -Achievable goals. -Assess the small changes. |
-Stages of change test. | -Traditional games. |
| SESSION 9 My new resolutions with my new friends. | -Reflect on the achievements achieved at an individual level. -Importance of planning the menu. |
-Knowledge test of the PinPo program. |
-Write physical and psychological evolution throughout the development of the program. | -Presentation of the gamification program. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



