
Submitted:
11 July 2024
Posted:
12 July 2024
You are already at the latest version
Abstract
Multidrug resistant bacteria pose a significant threat to global health, particularly in healthcare settings. This study aimed to explore the potential of aminoglycoside consumption and resistance data to correlate with multidrug resistance in Acinetobacter baumannii and Klebsiella pneumoniae. Data on aminoglycoside consumption and antibiotic resistance indices (ARI) were collected from 2010 to 2023. Descriptive statistics and Pearson correlation analyzes were performed to examine both immediate and delayed (one-year delay) correlations between aminoglycoside use (amikacin, tobramycin, gentamicin) and resistance patterns. The results indicated that the consumption of amikacin was consistently high and correlated with resistance in both bacterial species. Tobramycin and gentamicin showed variable resistance patterns, with negative correlations in some cases. Delayed effect analysis revealed that amikacin and tobramycin consumption had a slight delayed positive impact on multidrug resistance in A. baumannii, while gentamicin use was associated with a delayed reduction in resistance. In K. pneumoniae, gentamicin showed a strong delayed positive correlation with multidrug resistance, while amikacin and tobramycin had weaker associations. These findings highlight the complex and species-specific relationships between aminoglycoside consumption and resistance development, emphasizing the need for customized antibiotic management strategies that account for the immediate and delayed effects of antibiotic use.
Keywords:
aminoglycoside consumption
; multidrug resistance
; Acinetobacter baumannii
; Klebsiella pneumoniae
1. Introduction
Multidrug resistant bacteria constitute a significant risk to the overall well-being of the global population, constituting a substantial obstacle for healthcare systems [1]. Anticipating and predicting the emergence of multidrug resistance is crucial to designing efficient treatment plans and controlling the spread of these species. This study examines the potential of aminoglycoside resistance data to predict multidrug resistance in two medically important bacterial species, Acinetobacter baumannii and Klebsiella pneumoniae. These bacteria are notorious for causing serious and difficult-to-treat diseases.
A. baumannii, a Gram-negative nosocomial pathogen, has attracted considerable interest due to its impressive capacity to acquire resistance to many drugs, including carbapenems [2,3,4]. The tendency of this species for nosocomial infections, specifically in severely ill patients, and its ability to adapt to different surroundings have made it a significant menace to public health worldwide [5]. A. baumannii exhibits resistance mechanisms such as acquisition of β-lactamases, increased activity of multidrug efflux pumps, modification of aminoglycosides, decrease in permeability, and changes in antibiotic target structures [4]. Moreover, its effectiveness in hospital settings is due to its capacity to create long-lasting biofilms, which improve its ability to survive and spread [2]. Nevertheless, in a prior study, we noted that the susceptibility to aminoglycosides in this particular species varies significantly over time [6].
K. pneumoniae, also a Gram-negative bacterium, is a notable cause of nosocomial infections and the development of drug-resistant strains. Similar to A. baumannii, K. pneumoniae has also acquired resistance to a wide spectrum of antibiotics, including carbapenems, through several mechanisms such as the synthesis of carbapenemases, modification of the permeability of the outer membrane, and increased expression of efflux pumps [7,8]. Infections caused by these strains of K. pneumoniae that are resistant to several drugs have been linked to higher rates of illness and death, placing a significant load on healthcare systems [9].
The objective of this study is to examine the possible correlation between aminoglycoside resistance and the emergence of multidrug resistance in A. baumannii and K. pneumoniae isolates. Aminoglycoside resistance has been identified as a preliminary stage in the formation of more extensive resistance patterns in different types of bacteria, indicating that it could potentially function as an early sign of the advent of multidrug resistance [10]. Through the examination of aminoglycoside resistance patterns and their relationship with multidrug resistance in these two bacterial species, our aim is to gain valuable knowledge that can be used to improve the creation of more efficient surveillance and intervention methods to combat the proliferation of multidrug resistant strains.
2. Materials and Methods
2.1. Study Setting
Data were collected corresponding to the period from 1 January 2010–31 December 2023, at the Department of Medical Microbiology, University of Szeged, Hungary. Data collection was carried out electronically, in the laboratory information system records, corresponding to samples positive for A. baumannii and K. pneumoniae. Data were exported from the clinical microbiology laboratory information system (MedBakter, Asseco Central Europe Ltd., Hungary) and were reported into a customized database. Data included the types of specimens, isolate species, and antimicrobial susceptibility patterns. The results of antimicrobial susceptibility tests were determined and interpreted according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) [11].
2.2. Data Analysis
Data were exported from the laboratory information system into MS Excel 2016 (Microsoft Corp., Redmond, WA, USA) and GraphPad Prism version 8 (GraphPad Software, San Diego, CA, USA). MS Excel 2016 was used to store the data and to determine the different antibiotic resistance index (ARI) curves.
2.3. Calculating Antibiotic Resistance Index
To calculate the ARI, the model for measuring antibiotic resistance used by De Socio et al. was followed [12]. Briefly, for each antibiotic tested, a score of 0 was assigned for susceptibility, 0.5 for intermediate resistance, or 1 for resistance, and the ARI was calculated by dividing the sum of these scores by the number of antibiotics tested, giving a maximum score of 1.
2.4. Statistical Analysis
To analyze the relationship between aminoglycoside consumption and antibiotic resistance indices (ARI) for A. baumannii and K. pneumoniae, various statistical methods were used. Initial descriptive statistics, including means and ranges, were calculated for aminoglycoside consumption and ARI values over the study period from 2010 to 2023 to provide an overview of data distribution and variability. Pearson correlation coefficients were computed to assess the strength and direction of the linear relationship between aminoglycoside consumption and ARI values. This analysis was performed for the annual consumption of each aminoglycoside (amikacin, tobramycin, and gentamicin) and the corresponding ARI values within the same year for both A. baumannii and K. pneumoniae, as well as for the annual consumption of each aminoglycoside and the corresponding ARI values with a one-year delay to evaluate the delayed effects of antibiotic use on resistance. P-values were calculated to determine the statistical significance of Pearson correlation coefficients, with a p-value of less than 0.05 considered statistically significant. All statistical calculations and data visualization were performed using GraphPad Prism version 8 to create scatter plots and trend lines, facilitating the interpretation of correlation analyses and the identification of patterns and trends over time.
3. Results
3.1. Consumption and ARI Statistics for the Three Aminoglycosides Tested
In the first stage of our study, we analyzed data about the consumption and ARI of aminoglycosides tested for A. baumannii and K. pneumoniae. Amikacin continuously showed the greatest levels of consumption, ranging from around 1000 to 1500 grams per year, while the usage of tobramycin remained relatively low, with slight fluctuations around 100 grams per year (Figure 1A). The use of gentamicin was moderate, ranging from 300 to 600 grams per year (Figure 1A). These data revealed that there was significant heterogeneity in the total use of aminoglycosides, with amikacin being the most commonly used, followed by gentamicin and tobramycin.
An analysis was conducted on the ARI for the three aminoglycosides in the case of A. baumannii (Figure 1B). Amikacin has a consistently high ARI near 1.0, which indicates a high level of resistance. On the other hand, tobramycin and gentamicin have more variability, as indicated by ARI values that fall below 1.0 in many years, indicating alterations in resistance levels.
The same analysis was performed for K. pneumoniae (Figure 1C). The ARI for amikacin remains high, further highlighting its significant association with resistance. Tobramycin and gentamicin have more prominent variations, and some years demonstrating low resistance indices.
The analysis revealed an intricate connection between aminoglycoside intake and the development of resistance, specifically suggesting a substantial association between amikacin consumption and resistance for A. baumannii and K. pneumoniae.
3.2. Temporal Correlation Dynamics Between Aminoglycoside Consumption and Resistance Indices
In the next phase of our study, we examined the detailed correlation between aminoglycoside consumption and ARI data for A. baumannii. Consumption of amikacin and its ARI had a Pearson correlation value (r) of 0.29, showing a slight positive association (Figure 2A). On the other hand, tobramycin correlation between the consumption and its ARI showed a correlation coefficient of -0.16, indicating a weak negative correlation (Figure 2B). The use of gentamicin was more negatively correlated with ARI, as shown by a correlation value of -0.42 (Figure 2C). These findings demonstrate a mild correlation between amikacin consumption and the development of resistance in A. baumannii. Tobramycin and gentamicin exhibit different patterns in this regard.
Notable associations were also observed during the analysis of the use of aminoglycosides and ARI data for K. pneumoniae. The correlation between amikacin use and its ARI is represented by a Pearson correlation coefficient of 0.39, which indicates a moderate positive correlation (Figure 3A). On the other hand, the relationship between the amount of tobramycin consumed and its associated ARI shows a correlation coefficient of -0.42, suggesting a moderate negative association (Figure 3B). The intake of gentamicin is weakly negatively correlated with ARI, as shown by a Pearson correlation value of -0.25 (Figure 3C). The results indicate a clear link between the use of aminoglycosides and the development of resistance in K. pneumoniae. Amikacin shows a moderate positive correlation, while tobramycin and gentamicin have negative associations.
In the subsequent stage of the investigation, we analyzed the correlation between the consumption and ARI of aminoglycosides in A. baumannii with a one-year delay, to explore the delayed impact of antibiotic use on the development of resistance. Consumption of amikacin and its ARI exhibited a Pearson correlation value (r) of 0.27, demonstrating a slight positive association (Figure 4A). This indicates that there is a correlation between increased use of amikacin in the previous year and an increase in resistance in the upcoming one. However, the relationship between the amount of tobramycin consumed and its ARI showed a Pearson correlation value of -0.23, suggesting a mild negative connection (Figure 4B). The intake of gentamicin was somewhat negatively correlated with ARI, as shown by a correlation value of -0.42 (Figure 4C). The data presented indicate that there is a variable relationship between aminoglycoside consumption and the emergence of resistance in A. baumannii. Amikacin shows a slight positive association, while tobramycin and gentamicin show negative correlations, highlighting the delayed effect of these antibiotics.
Interesting associations were observed when we analyzed the consumption of aminoglycosides and ARI for K. pneumoniae with a one-year delay. The association between amikacin consumption and its ARI was represented by a Pearson correlation coefficient of 0.29, showing a modest positive correlation (Figure 5A). This indicates that a greater amount of amikacin used in the previous year is associated with a rise in resistance in K. pneumoniae. On the other hand, the relationship between the amount of tobramycin consumed and its ARI showed a Pearson correlation value of -0.42, which indicates a mild negative association (Figure 5B). The intake of gentamicin is somewhat negatively correlated with ARI, as shown by a correlation value of -0.25 (Figure 5C). These results demonstrate that there is a fluctuating relationship between aminoglycoside intake and the development of resistance in K. pneumoniae. Specifically, amikacin in this species also exhibits a mild positive connection, while tobramycin and gentamicin show negative correlations. This again highlights the delayed effects of antibiotic consumption on the development of resistance.
In the following phase of our investigation, we analyzed the ARI of meropenem, as meropenem resistance is a reliable indicator of multidrug resistance for both bacterial species, in the context of aminoglycoside resistance. Examination of aminoglycoside ARIs revealed that the values for tobramycin, gentamicin, and amikacin were consistently high, with values near 1.0 (Figure 6). However, significant fluctuations were also observed for tobramycin and gentamicin. On the ARI other hand, the meropenem also exhibited notable oscillations, suggesting that there were changes in the levels of multidrug resistance over time. These results suggest an intricate interaction between aminoglycoside and meropenem resistance.
To gain a clearer understanding of this complex relationship, we also examined the correlation of ARI values of each aminoglycoside and meropenem in A. baumannii.
The relationship between amikacin ARI and meropenem ARI is characterized by a correlation coefficient of 0.18, suggesting a modest positive connection (Figure 7A). The link between the ARI of tobramycin and meropenem was characterized by a Pearson correlation value of 0.08, showing a very modest positive correlation (Figure 7B). The Pearson r value between the ARI of gentamicin and meropenem is -0.01, showing a very weak negative association (Figure 7C). These findings indicate that while amikacin shows a modest positive correlation with meropenem ARI, tobramycin and gentamicin exhibit minimal associations, suggesting a complex and varied relationship between aminoglycoside resistance and multidrug resistance in A. baumannii.
Examining ARI of different aminoglycosides and the multidrug resistance indicator meropenem reveals different trends in the case of K. pneumoniae (Figure 8). ARIs for tobramycin, gentamicin, and amikacin exhibited high variability, with values shifting considerably throughout the measured time frame. On the contrary, the meropenem ARI has lower overall values compared to the aminoglycosides and demonstrates less variability, indicating a somewhat constant but lower degree of multidrug resistance during the investigated time. Thus, meropenem ARI demonstrated multidrug resistance at a lower level in K. pneumoniae, serving as a strong contrast to the more prevalent multidrug-resistant A. baumannii.
Examination of the Pearson correlation between the antibiotic resistance indices of these aminoglycosides and meropenem demonstrated clear and separate associations. The association between amikacin ARI and meropenem ARI is characterized by a Pearson correlation coefficient of -0.08, suggesting a very weak negative correlation (Figure 9A). The link between tobramycin and meropenem was shown by a Pearson correlation coefficient of -0.01, suggesting a very weak negative correlation (Figure 9B). The correlation coefficient between gentamicin and the meropenem ARI is 0.03, showing a very weak positive link (Figure 9C). These findings indicate that the associations between aminoglycoside ARIs and meropenem ARI in K. pneumoniae are minimal, with tobramycin and amikacin showing very weak negative correlations and gentamicin showing a very weak positive correlation, highlighting the complexity of resistance mechanisms in this species.
To better understand this complex scenario, in the next part of our work, we compared the consumption data of each aminoglycoside separately for the two species with the meropenem ARI. According to the statistics, the use of amikacin differs significantly and remains higher than other aminoglycosides on average (Figure 10). Consumption experiences substantial fluctuations during the period under investigation. However, gentamicin and tobramycin show more stable and decreased patterns of use. In addition, the ARI of the meropenem for A. baumannii exhibits a fluctuating but increasing pattern of resistance over the years.
In order to ascertain if the use of certain aminoglycosides is associated with the occurrence of multidrug resistance, we conducted a separate analysis of the consumption data for each individual aminoglycoside in connection to the meropenem ARI data. The yearly intake of amikacin and meropenem ARI for A. baumannii exhibited a Pearson correlation coefficient of 0.2, showing a slight positive link (Figure 11A). This indicates that there is a correlation between increased yearly use of amikacin and increased resistance to multidrug. The annual intake of tobramycin has a very modest negative connection with ARI of the meropenem, as shown by a Pearson correlation coefficient of -0.04 (Figure 11B). These findings suggest that increased yearly tobramycin use is not correlate with multidrug resistance in A. baumannii. However, the relationship between the amount of gentamicin used each year and the appearance of meropenem antibiotic resistance reveals a Pearson correlation value of -0.32, showing a moderate negative connection (Figure 11C). These findings together imply that amikacin exhibits a weak positive connection, tobramycin exhibits a weak negative correlation, and gentamicin exhibits a substantial negative correlation with multidrug resistance indicator meropenem ARI.
In the next part of our work, we compared the consumption data of each aminoglycoside with the meropenem ARI for K. pneumoniae (Figure 12). The ARI of meropenem exhibited a fluctuating low pattern of resistance over the years, indicating variable decreased levels of multidrug resistance.
Examination of the Pearson connection between yearly aminoglycoside intake and meropenem ARI, which signifies multidrug resistance, for K. pneumoniae demonstrated interesting associations. The yearly consumption of amikacin and the meropenem ARI exhibited a Pearson correlation coefficient of -0.28, showing a slight negative link (Figure 13A). The yearly intake of tobramycin had a very modest positive link to ARI meropenem, as shown by a correlation coefficient of 0.09 (Figure 13B). On the other hand, the relationship between the amount of gentamicin used each year and the occurrence of resistance to antibiotics with meropenem was highly correlated, as shown by a Pearson correlation coefficient of 0.70, suggesting a significant positive association (Figure 13C). This is a considerable correlation between increasing yearly gentamicin intake and growth in multidrug resistance.
During the last stage of our project, we analyzed the ARI of meropenem with a one-year time delay compared to aminoglycoside consumption. This allowed us to evaluate the possible delayed impacts of aminoglycoside usage alterations on multidrug resistance. A weak positive association, indicated by the Pearson correlation coefficient of 0.33, was found between the annual consumption of amikacin and meropenem ARI for A. baumannii (Figure 14A). The relationship between the annual consumption of tobramycin and ARI of meropenem next year showed a very weak positive association, with a Pearson correlation value of 0.11 (Figure 14B). On the other hand, a weak negative association was detected with a correlation coefficient of -0.30 between the annual intake of gentamicin and ARI meropenem in the following year. The results indicate that the intake of amikacin and tobramycin has a slight delayed inducing effect on multidrug resistance in A. baumannii. On the other hand, the usage of gentamicin is linked to a weak delayed decrease in multidrug resistance.
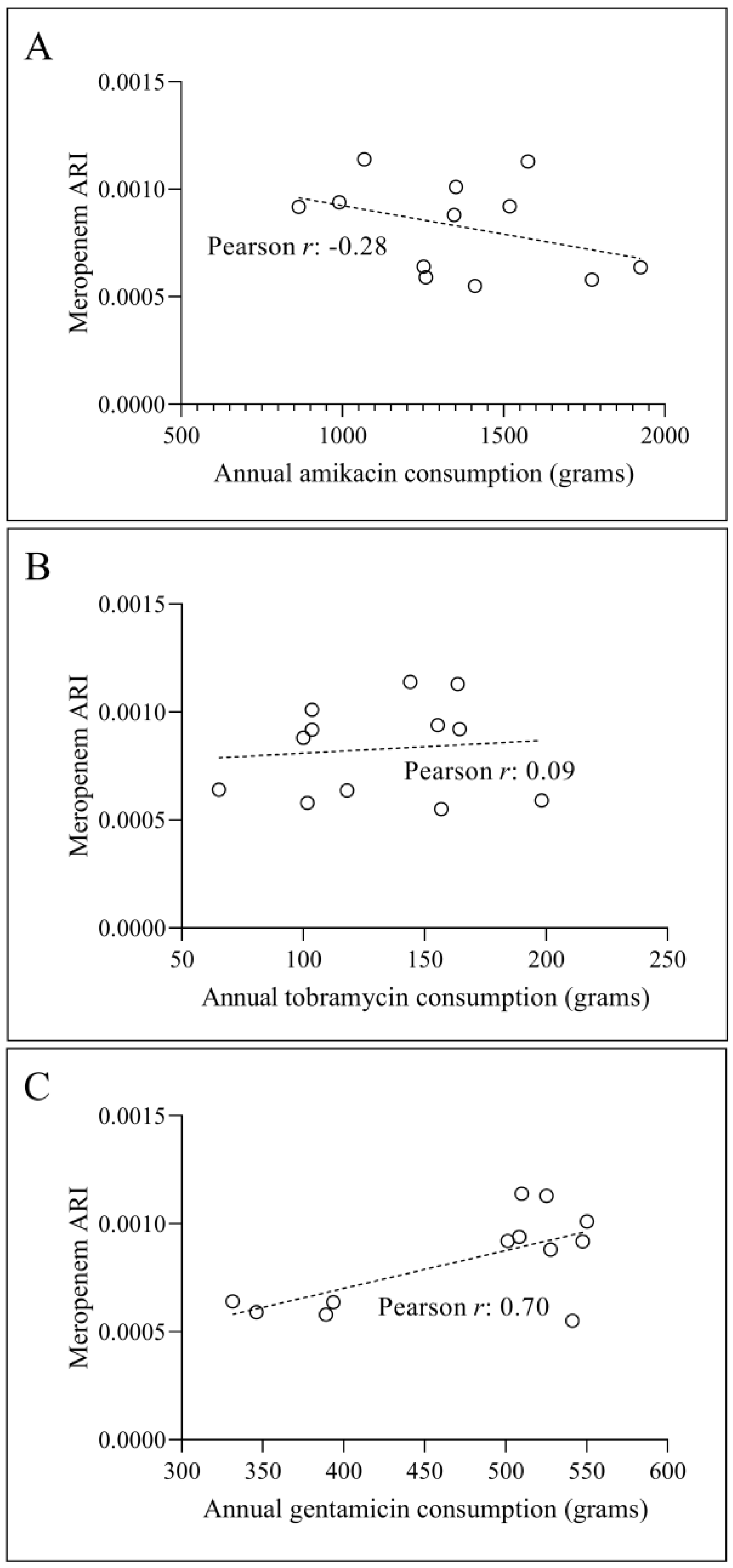
A weak negative association, as indicated by the Pearson correlation coefficient of -0.28, was found between the annual consumption of amikacin and the ARI of meropenem in the case of K. pneumoniae (Figure 15A). Annual consumption of tobramycin had a very modest positive link with meropenem ARI, as indicated by a correlation coefficient of 0.09 (Figure 15B). On the other hand, the relationship between the amount of gentamicin used each year and the occurrence of resistance to meropenem in the next year was highly correlated, with a Pearson correlation value of 0.70, showing a strong positive association (Figure 15C). This is a robust correlation between increasing annual gentamicin intake and an increase in multidrug resistance, as seen by meropenem ARI with a one-year delay.
4. Discussion
This study aims to examine the correlation between aminoglycoside consumption and the multidrug resistance phenomenon among Gram-negative nosocomial pathogens revealed a consistently elevated ARI observed for amikacin in both A. baumannii and K. pneumoniae (as shown in Figure 1B and 1C). This is in line with previous findings that have shown resistance to amikacin as a prevalent characteristic in multidrug-resistant strains of both pathogens [13,14]. The increased incidence of resistance emphasizes the need for vigilant surveillance and careful use of amikacin in clinical settings to reduce the development of resistance. Our further analysis revealed that gentamicin and tobramycin exhibited more variable resistance patterns compared to amikacin (Figure 1B, 1C). The oscillations in ARI can be ascribed to variations in consumption habits and the distinct effectiveness of these antibiotics against various strains and in different clinical situations. Furthermore, the varying resistance of gentamicin suggests that while it may retain effectiveness in certain situations, its use should be carefully supervised to avoid increasing resistance.
The temporal analysis indicated that amikacin consumption has a modest positive correlation with resistance in both A. baumannii and K. pneumoniae (Figure 2A, 3A), suggesting that increased usage may contribute to increased resistance over time. This finding is consistent with the existing literature that suggests that high levels of aminoglycoside usage can drive the selection of resistant strains [15]. In contrast, the negative correlations observed for tobramycin and gentamicin with resistance in both species (Figure 2B, 2C, 3B, 3C) suggest that these antibiotics may play a more complex role in resistance dynamics, possibly due to their varied mechanisms of action and the bacterial adaptive responses they induce.
The delayed effect analysis (Figure 4, 5) highlighted that the impact of aminoglycoside consumption on resistance could persist or manifest even after a year. This finding is crucial for understanding the long-term effects of antibiotic usage and for developing effective antibiotic stewardship programs that consider not only immediate but also delayed impacts on resistance patterns [16]. Examining meropenem ARI as an indicator of multidrug resistance revealed significant variability in resistance patterns over time (Figure 6). This variability emphasizes the need for continuous surveillance and the potential benefits of using meropenem ARI as a marker of wider resistance trends [17]. The differential correlations between ARIs of specific aminoglycosides and meropenem for both A. baumannii and K. pneumoniae (Figure 7, 8, 9) indicate that resistance mechanisms may differ significantly between these species. For A. baumannii, the modest positive correlation of amikacin with meropenem ARI suggests a link between these resistance pathways (Figure 7C), while the weak or negligible correlations for tobramycin and gentamicin suggest more complex interactions (Figure 7A, 7B) [18]. In contrast, for K. pneumoniae, the significant positive correlation of gentamicin with meropenem ARI (Figure 9C) highlights the potential role of gentamicin in driving multidrug resistance, which requires careful consideration in its clinical use [19,20]. Consideration of a one-year delay further emphasizes the need to take into account the consequences of resistance that occur later (Figure 14, 15). The delayed positive connection between amikacin, tobramycin, and meropenem ARI in A. baumannii (as shown in Figs. 14A and 14B), as well as the delayed negative correlation seen for gentamicin (as shown in Figs. 14C), suggest that prior antibiotic use could have long-term effects on resistance development [10]. Similarly, the variety of delayed correlations revealed for K. pneumoniae (Figure 15) indicates that antibiotic stewardship programs must include these long-term effects to efficiently control and reduce resistance.
5. Conclusions
In conclusion, our study highlights the intricate and species-specific relationships between aminoglycoside consumption and multidrug resistance. The findings underscore the need for customized antibiotic stewardship strategies that consider both immediate and long-term impacts of antibiotic usage on resistance development. Continuous monitoring and adaptive management practices will be essential in controlling the spread of multidrug-resistant pathogens and preserving the efficacy of existing antibiotics. More research is warranted to explore the underlying mechanisms that drive these resistance patterns and develop more effective interventions.
Author Contributions
Conceptualization, L.O. and K.B.; methodology, L.O. and A.S.; software, L.O. and B.S.; validation, K.M., B.K., and A.S.; formal analysis, L.O.; investigation, B.S. and A.S.; resources, K.B.; data curation, B.S. and A.S.; writing—original draft preparation, L.O.; writing—review and editing, K.B.; visualization, L.O.; supervision, K.B.; project administration, B.S. and K.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of the University of Szeged (protocol code 8/2021-SZTE RKEB; 25 January 2021).
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO Bacterial Priority Pathogens List, 2024: Bacterial Pathogens of Public Health Importance to Guide Research, Development and Strategies to Prevent and Control Antimicrobial Resistance. Available online: https://www.who.int/publications/i/item/9789240093461 (accessed on 6 July 2024).
- Mea, H.J.; Yong, P.V.C.; Wong, E.H. An Overview of Acinetobacter Baumannii Pathogenesis: Motility, Adherence and Biofilm Formation. Microbiological Research 2021, 247, 126722. [Google Scholar] [CrossRef] [PubMed]
- Ayoub Moubareck, C.; Hammoudi Halat, D. Insights into Acinetobacter Baumannii: A Review of Microbiological, Virulence, and Resistance Traits in a Threatening Nosocomial Pathogen. Antibiotics 2020, 9, 119. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-R.; Lee, J.H.; Park, M.; Park, K.S.; Bae, I.K.; Kim, Y.B.; Cha, C.-J.; Jeong, B.C.; Lee, S.H. Biology of Acinetobacter Baumannii: Pathogenesis, Antibiotic Resistance Mechanisms, and Prospective Treatment Options. Front. Cell. Infect. Microbiol. 2017, 7. [Google Scholar] [CrossRef] [PubMed]
- Gordon, N.C.; Wareham, D.W. Multidrug-Resistant Acinetobacter Baumannii: Mechanisms of Virulence and Resistance. International Journal of Antimicrobial Agents 2010, 35, 219–226. [Google Scholar] [CrossRef]
- Orosz, L.; Burián, K. The “COVID Effect” in Culture-Based Clinical Microbiology: Changes Induced by COVID-19 Pandemic in a Hungarian Tertiary Care Center. Journal of Infection and Public Health 2024, 17, 102453. [Google Scholar] [CrossRef] [PubMed]
- Nordmann, P.; Cuzon, G.; Naas, T. The Real Threat of Klebsiella Pneumoniae Carbapenemase-Producing Bacteria. The Lancet Infectious Diseases 2009, 9, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Podschun, R.; Ullmann, U. Klebsiella Spp. as Nosocomial Pathogens: Epidemiology, Taxonomy, Typing Methods, and Pathogenicity Factors. Clin Microbiol Rev 1998, 11, 589–603. [Google Scholar] [CrossRef] [PubMed]
- Paczosa, M.K.; Mecsas, J. Klebsiella Pneumoniae: Going on the Offense with a Strong Defense. Microbiol Mol Biol Rev 2016, 80, 629–661. [Google Scholar] [CrossRef] [PubMed]
- Mortazavi, S.M.; Farshadzadeh, Z.; Janabadi, S.; Musavi, M.; Shahi, F.; Moradi, M.; Khoshnood, S. Evaluating the Frequency of Carbapenem and Aminoglycoside Resistance Genes among Clinical Isolates of Acinetobacter Baumannii from Ahvaz, South-West Iran. New Microbes New Infect 2020, 38, 100779. [Google Scholar] [CrossRef] [PubMed]
- EUCAST: Disk Diffusion Methodology. Available online: https://www.eucast.org/ast_of_bacteria/disk_diffusion_methodology/ (accessed on 2 June 2022).
- De Socio, G.V.; Rubbioni, P.; Botta, D.; Cenci, E.; Belati, A.; Paggi, R.; Pasticci, M.B.; Mencacci, A. Measurement and Prediction of Antimicrobial Resistance in Bloodstream Infections by ESKAPE Pathogens and Escherichia Coli. Journal of Global Antimicrobial Resistance 2019, 19, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Mann, R.; Rafei, R.; Gunawan, C.; Harmer, C.J.; Hamidian, M. Variants of Tn6924, a Novel Tn7 Family Transposon Carrying the blaNDM Metallo-β-Lactamase and 14 Copies of the aphA6 Amikacin Resistance Genes Found in Acinetobacter Baumannii. Microbiol Spectr 2022, 10, e0174521. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Xu, L.; Chen, Y. Drug Resistance and Susceptibility of Amikacin in Children with Extended-Spectrum Beta-Lactamase-Producing Enterobacterales: A Systematic Review with Meta-Analysis. Diagnostic Microbiology and Infectious Disease 2023, 106, 115956. [Google Scholar] [CrossRef] [PubMed]
- Sedláková, M.H.; Urbánek, K.; Vojtová, V.; Suchánková, H.; Imwensi, P.; Kolář, M. Antibiotic Consumption and Its Influence on the Resistance in Enterobacteriaceae. BMC Res Notes 2014, 7, 454. [Google Scholar] [CrossRef] [PubMed]
- Alawi, M.M.; Tashkandi, W.A.; Basheikh, M.A.; Warshan, F.M.; Ghobara, H.A.; Ramos, R.B.; Guiriba, M.L.; Ayob, O.; Janah, S.S.; Sindi, A.A.; et al. Effectiveness of Antimicrobial Stewardship Program in Long-Term Care: A Five-Year Prospective Single-Center Study. Interdiscip Perspect Infect Dis 2022, 2022, 8140429. [Google Scholar] [CrossRef] [PubMed]
- Balázs, B.; Tóth, Z.; Nagy, F.; Kovács, R.; Tóth, H.; Nagy, J.B.; Tóth, Á.; Szarka, K.; Majoros, L.; Kardos, G. The Role of Uniform Meropenem Usage in Acinetobacter Baumannii Clone Replacement. Antibiotics (Basel) 2021, 10, 127. [Google Scholar] [CrossRef] [PubMed]
- Kyriakidis, I.; Vasileiou, E.; Pana, Z.D.; Tragiannidis, A. Acinetobacter Baumannii Antibiotic Resistance Mechanisms. Pathogens 2021, 10, 373. [Google Scholar] [CrossRef]
- Ahmed, O.B.; Asghar, A.H.; Bamaga, M.; Bahwerth, F.S.; Ibrahim, M.E. Characterization of Aminoglycoside Resistance Genes in Multidrug-Resistant Klebsiella Pneumoniae Collected from Tertiary Hospitals during the COVID-19 Pandemic. PLOS ONE 2023, 18, e0289359. [Google Scholar] [CrossRef] [PubMed]
- Almaghrabi, R.; Clancy, C.J.; Doi, Y.; Hao, B.; Chen, L.; Shields, R.K.; Press, E.G.; Iovine, N.M.; Townsend, B.M.; Wagener, M.M.; et al. Carbapenem-Resistant Klebsiella Pneumoniae Strains Exhibit Diversity in Aminoglycoside-Modifying Enzymes, Which Exert Differing Effects on Plazomicin and Other Agents. Antimicrob Agents Chemother 2014, 58, 4443–4451. [Google Scholar] [CrossRef]
Figure 1.
Consumption and ARI of aminoglycosides between 2010 and 2023. (A) Annual consumption of amikacin, tobramycin, and gentamicin in grams from 2010 to 2023 (B) ARI data for amikacin, tobramycin, and gentamicin in the case of A. baumannii during the same period. (C) ARIs for aminoglycosides in the case of K. pneumoniae from 2010 to 2023. The dashed line represents the mean ARI of all three aminoglycosides.
Figure 1.
Consumption and ARI of aminoglycosides between 2010 and 2023. (A) Annual consumption of amikacin, tobramycin, and gentamicin in grams from 2010 to 2023 (B) ARI data for amikacin, tobramycin, and gentamicin in the case of A. baumannii during the same period. (C) ARIs for aminoglycosides in the case of K. pneumoniae from 2010 to 2023. The dashed line represents the mean ARI of all three aminoglycosides.
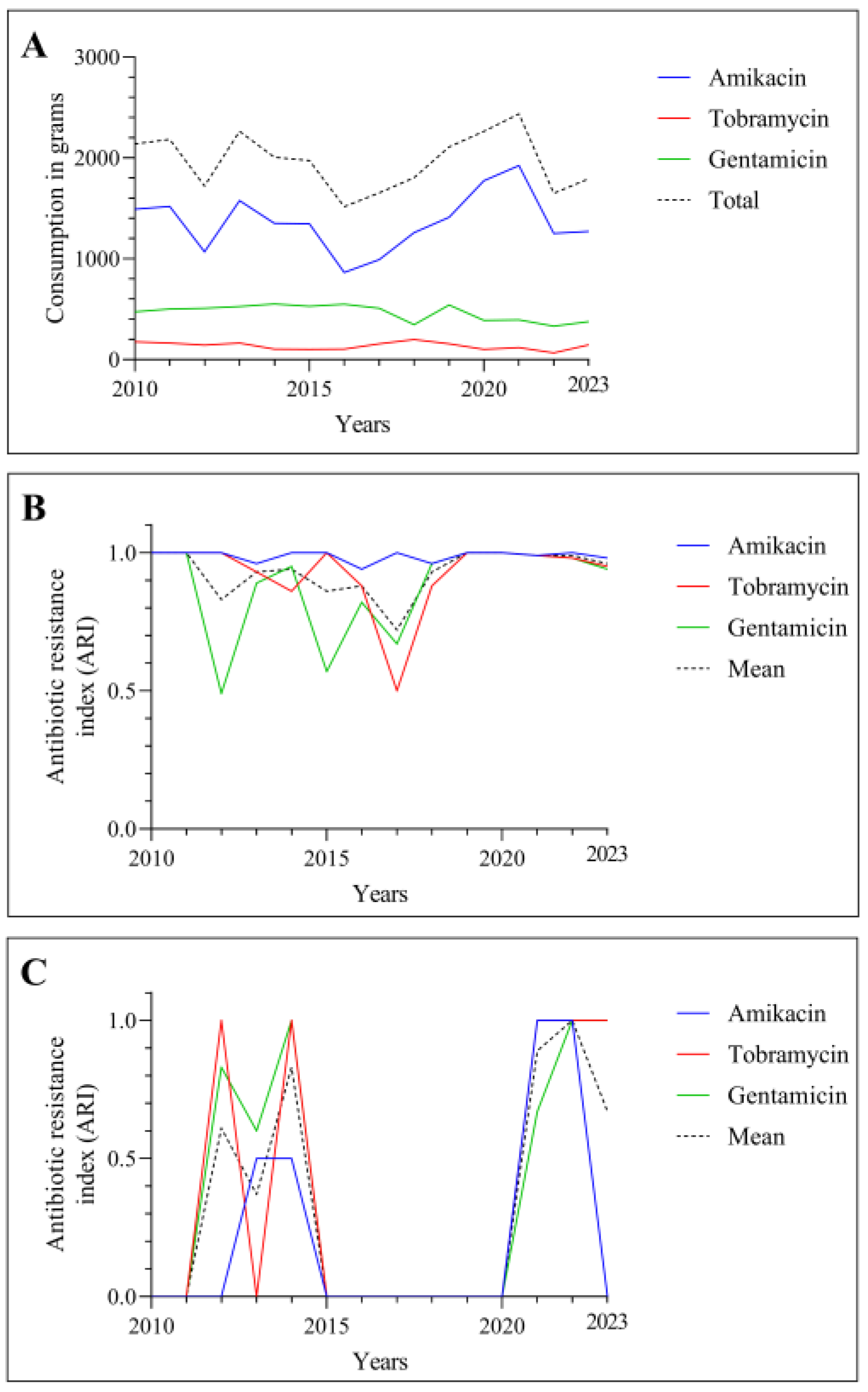
Figure 2.
The correlation between the amikacin (A), tobramycin (B) and gentamicin (C) consumption and ARI values for A. baumannii.
Figure 2.
The correlation between the amikacin (A), tobramycin (B) and gentamicin (C) consumption and ARI values for A. baumannii.
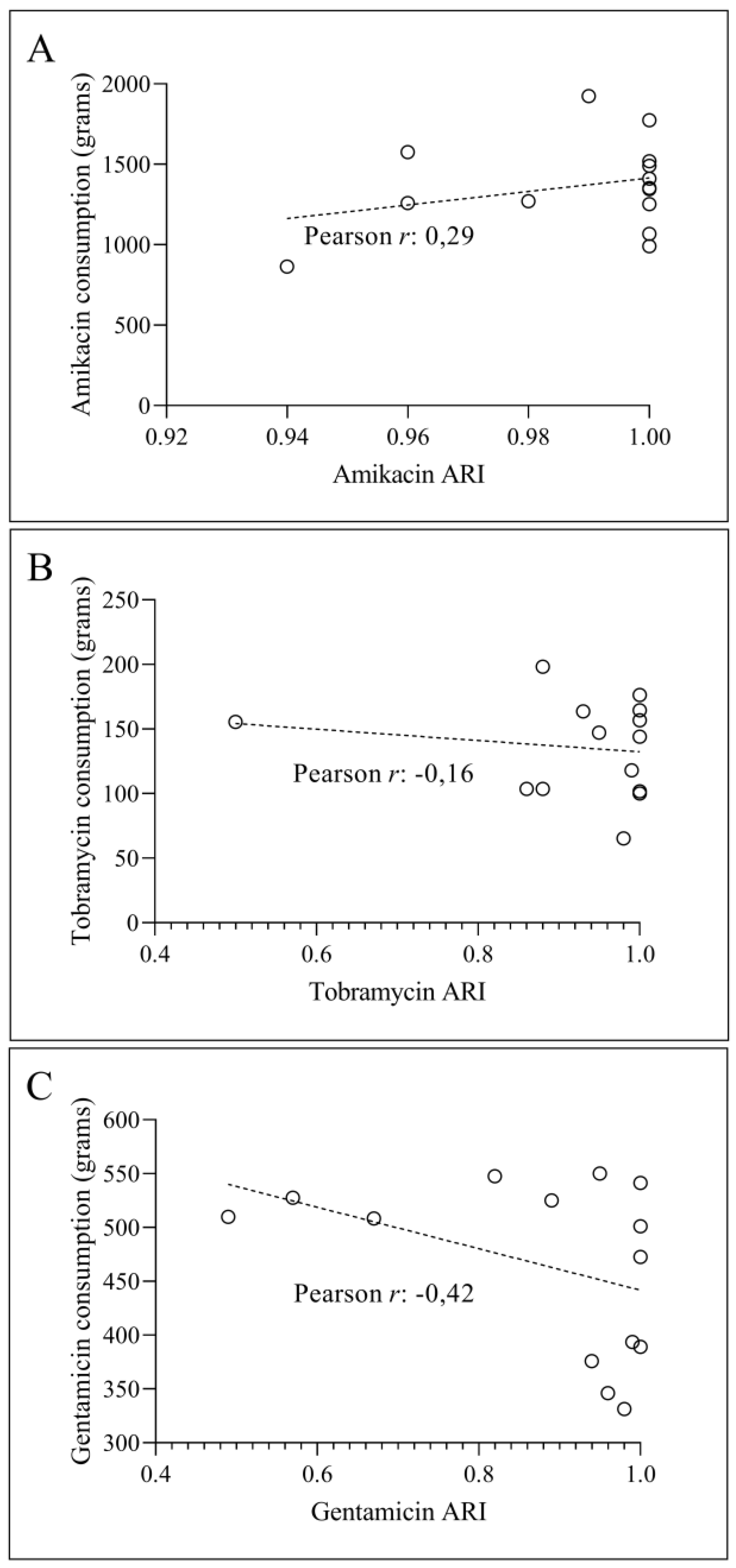
Figure 3.
The relationship between the consumption of amikacin (A), tobramycin (B), and gentamicin (C) in grams and the values of ARI for K. pneumoniae.
Figure 3.
The relationship between the consumption of amikacin (A), tobramycin (B), and gentamicin (C) in grams and the values of ARI for K. pneumoniae.
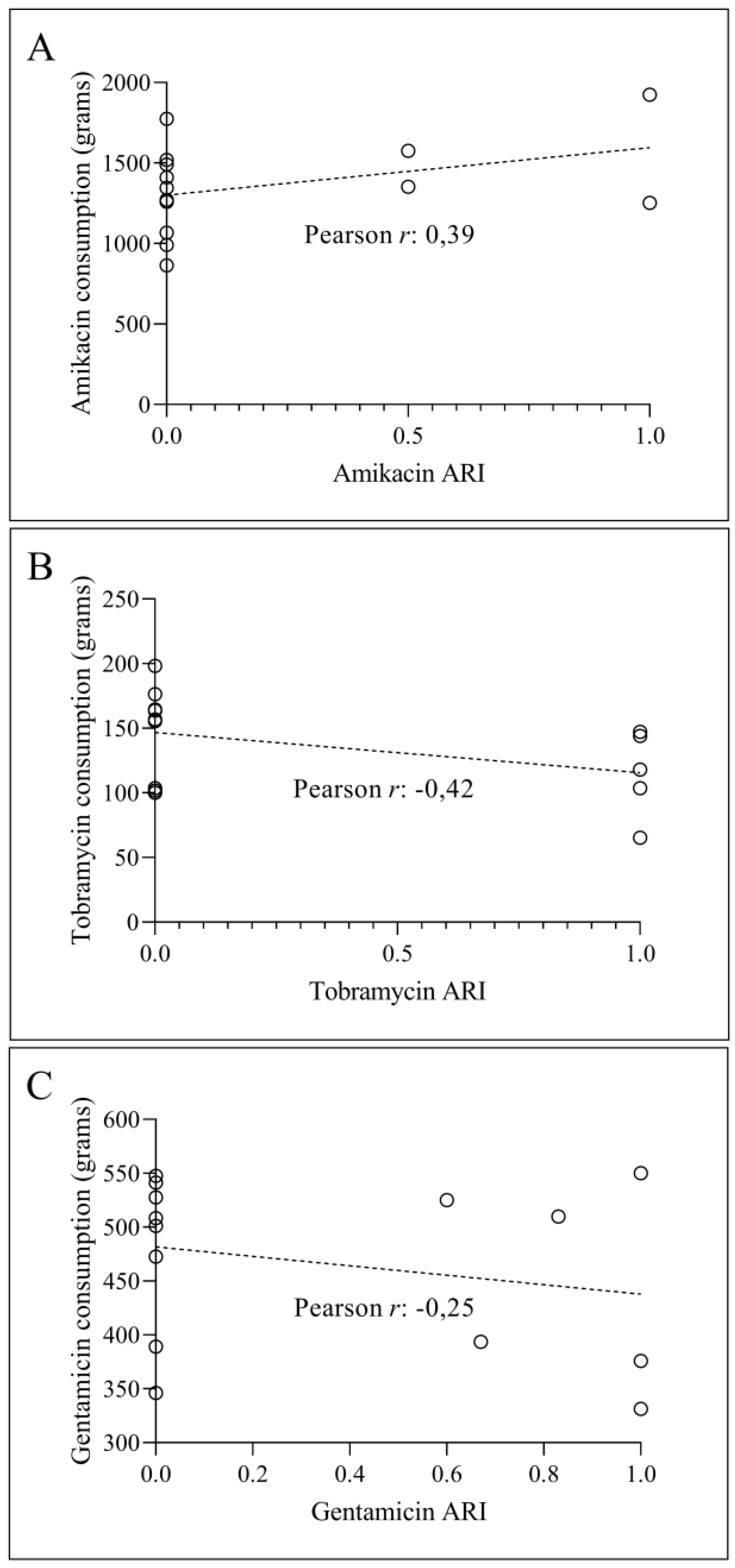
Figure 4.
The relationship between the amount of amikacin (A), tobramycin (B), and gentamicin (C) used in the previous year and their ARI for A. baumannii in the next year.
Figure 4.
The relationship between the amount of amikacin (A), tobramycin (B), and gentamicin (C) used in the previous year and their ARI for A. baumannii in the next year.
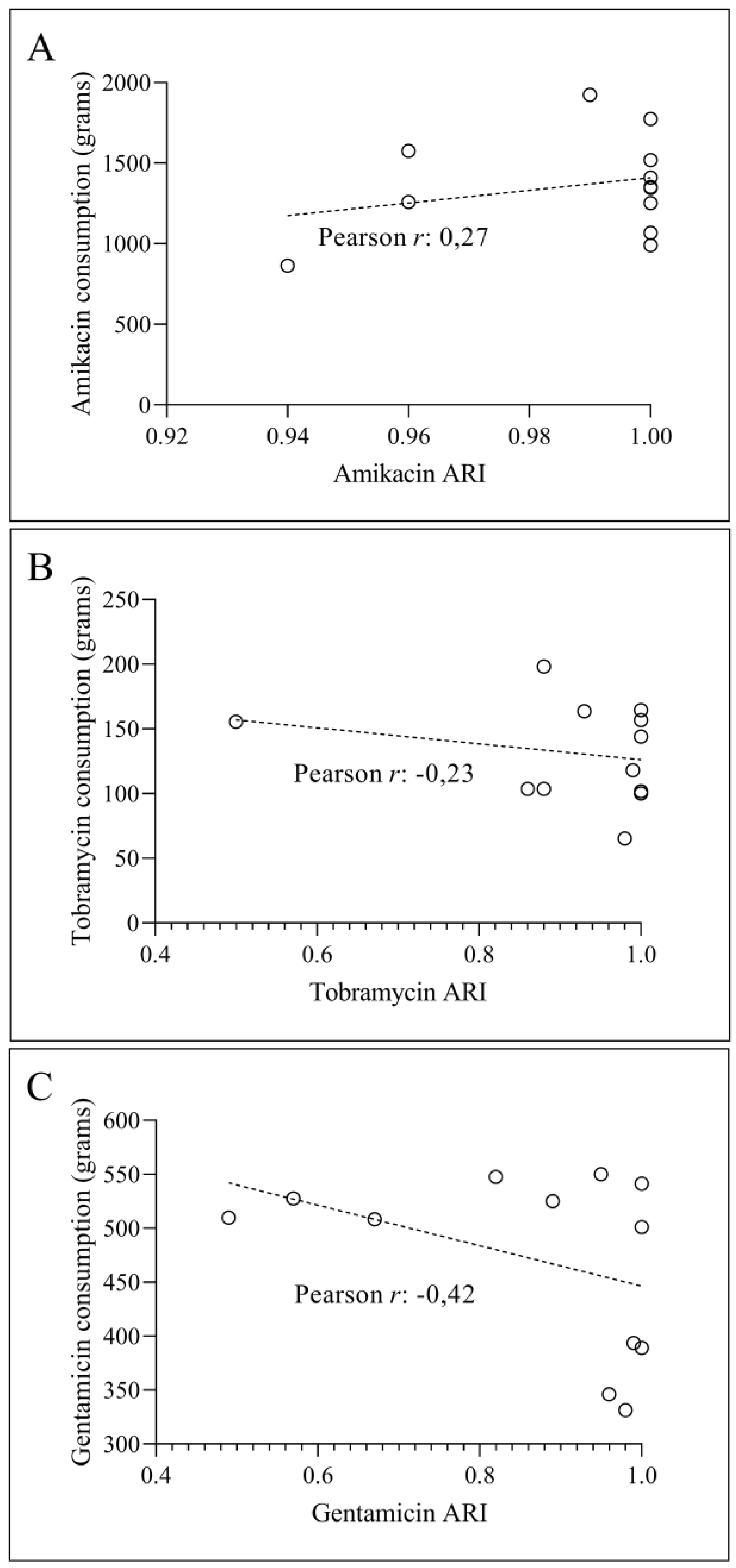
Figure 5.
The correlation between the quantity of amikacin (A), tobramycin (B), and genatmicin (C) administered in the preceding year and the ARI of these medications for K. pneumoniae in the next year.
Figure 5.
The correlation between the quantity of amikacin (A), tobramycin (B), and genatmicin (C) administered in the preceding year and the ARI of these medications for K. pneumoniae in the next year.
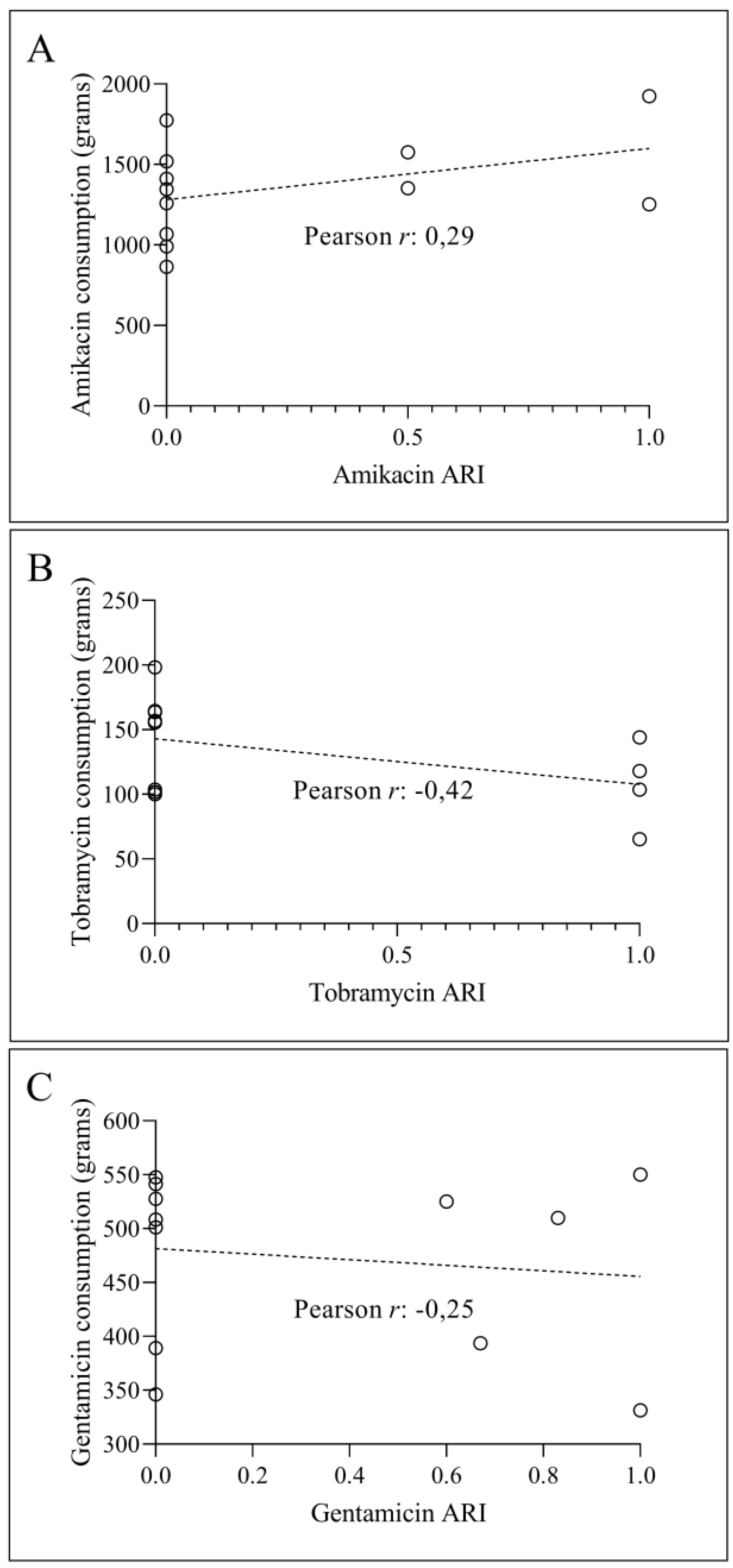
Figure 6.
ARI values for aminoglycosides and meropenem in the case of A. baumannii between 2010 and 2023.
Figure 6.
ARI values for aminoglycosides and meropenem in the case of A. baumannii between 2010 and 2023.
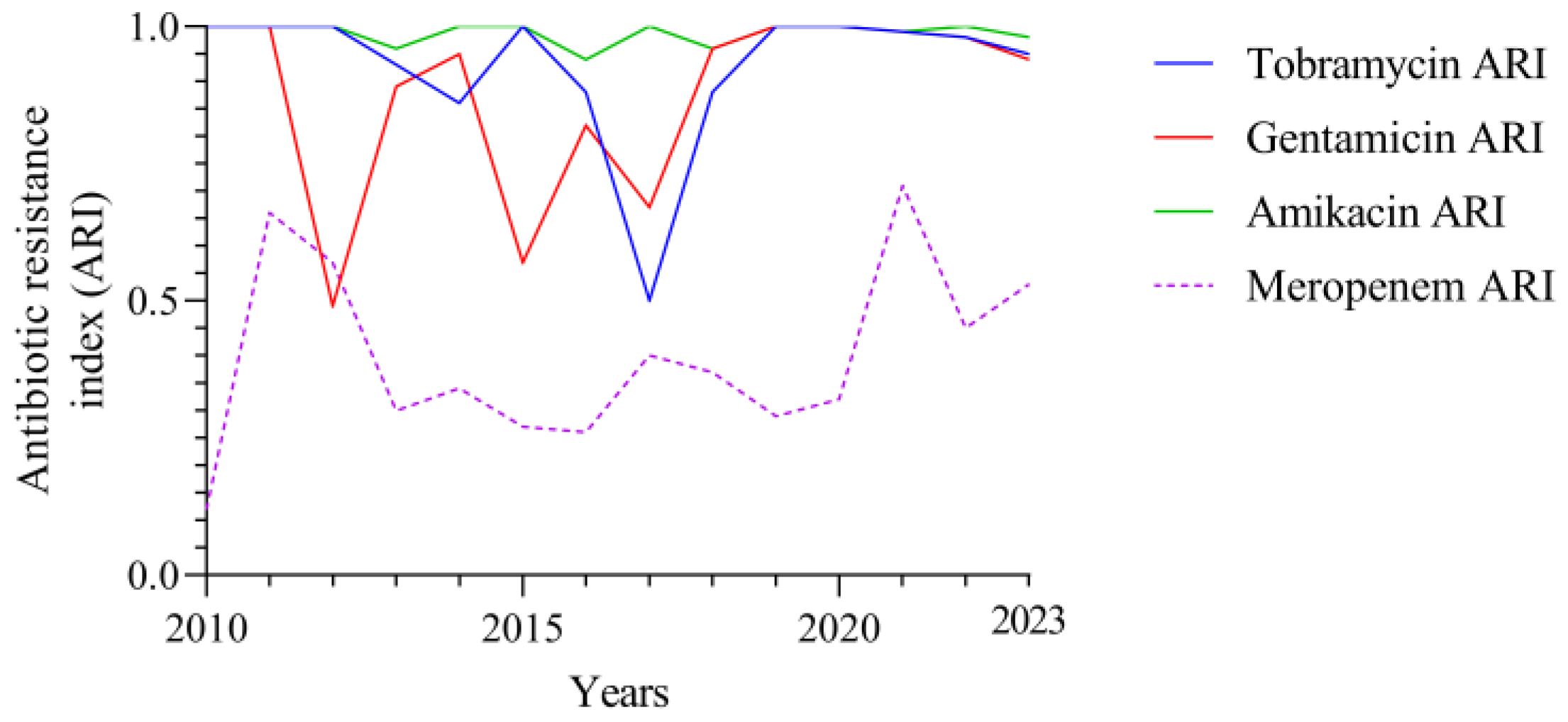
Figure 7.
Pearson correlations between ARI of different aminoglycosides and meropenem in A. baumannii.
Figure 7.
Pearson correlations between ARI of different aminoglycosides and meropenem in A. baumannii.
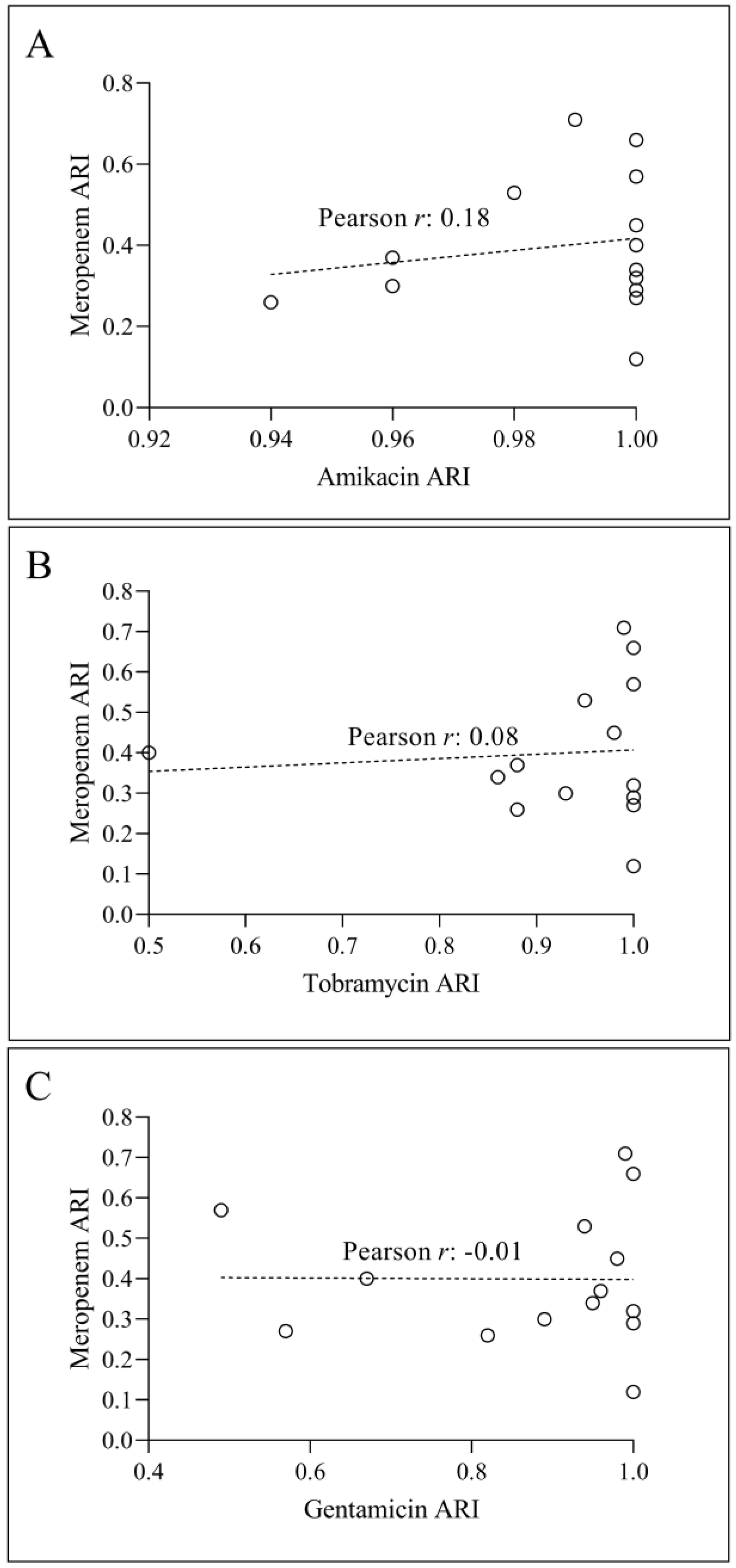
Figure 8.
ARI over time for aminoglycosides and meropenem in K. pneumoniae between 2010 and 2023. The y-axis on the left indicates the aminoglycoside ARI values, whereas the y-axis on the right shows the ARI meropenem.
Figure 8.
ARI over time for aminoglycosides and meropenem in K. pneumoniae between 2010 and 2023. The y-axis on the left indicates the aminoglycoside ARI values, whereas the y-axis on the right shows the ARI meropenem.
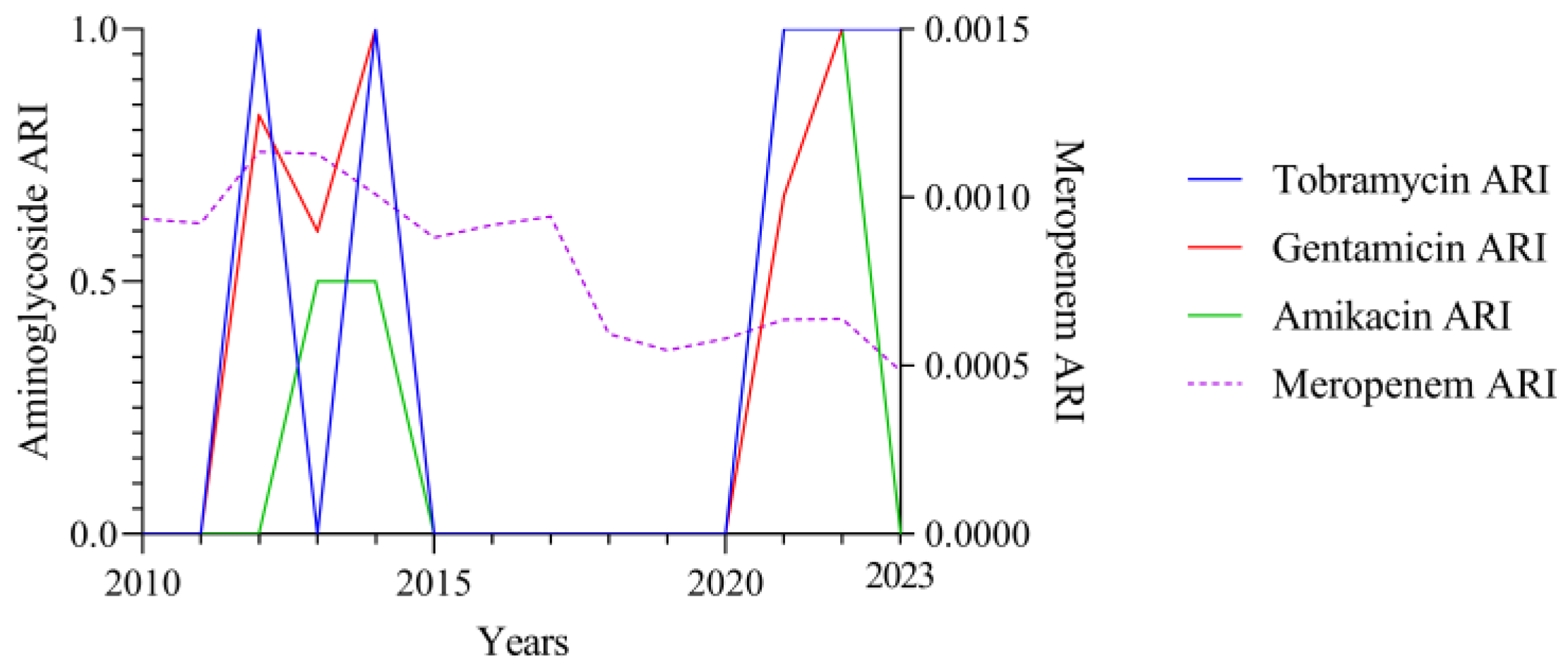
Figure 9.
Pearson correlations between ARI of various aminoglycosides and meropenem in K. pneumoniae.
Figure 9.
Pearson correlations between ARI of various aminoglycosides and meropenem in K. pneumoniae.
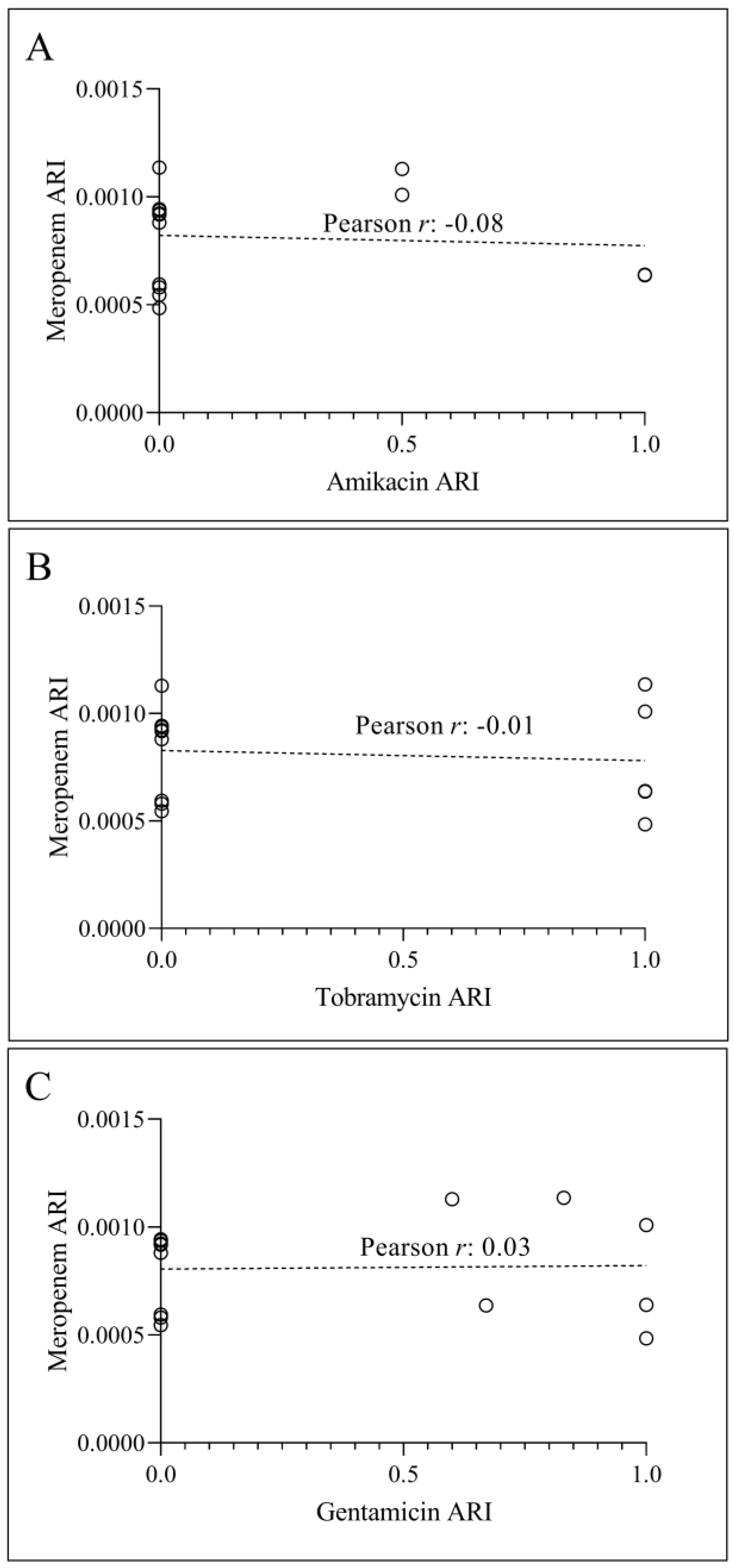
Figure 10.
Analysis of aminoglycoside intake and meropenem resistance in K. pneumoniae from 2010 to 2023. The left y-axis represents the yearly intake of aminoglycosides in grams, whereas the right y-axis represents the ARI meropenem.
Figure 10.
Analysis of aminoglycoside intake and meropenem resistance in K. pneumoniae from 2010 to 2023. The left y-axis represents the yearly intake of aminoglycosides in grams, whereas the right y-axis represents the ARI meropenem.
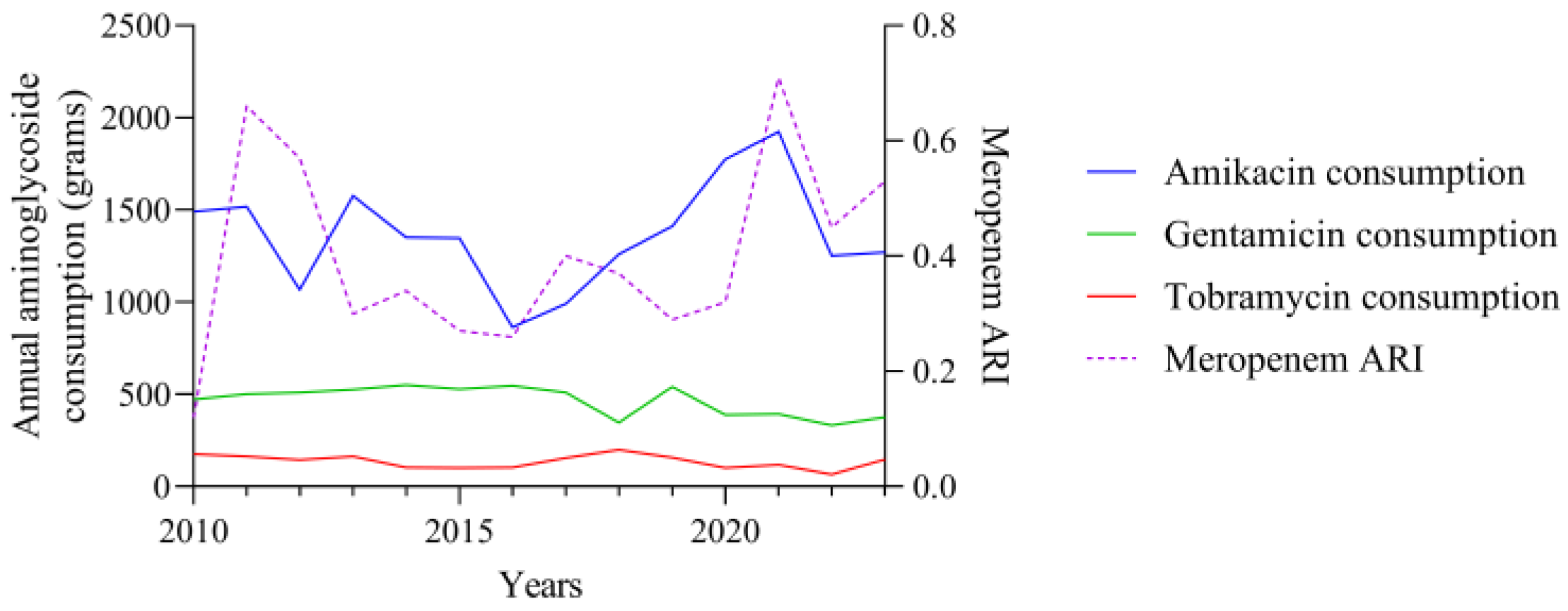
Figure 11.
Correlation between annual amikacin (A), tobramycin (B), and gentamicin (C) consumption and meropenem ARI in A. baumannii.
Figure 11.
Correlation between annual amikacin (A), tobramycin (B), and gentamicin (C) consumption and meropenem ARI in A. baumannii.
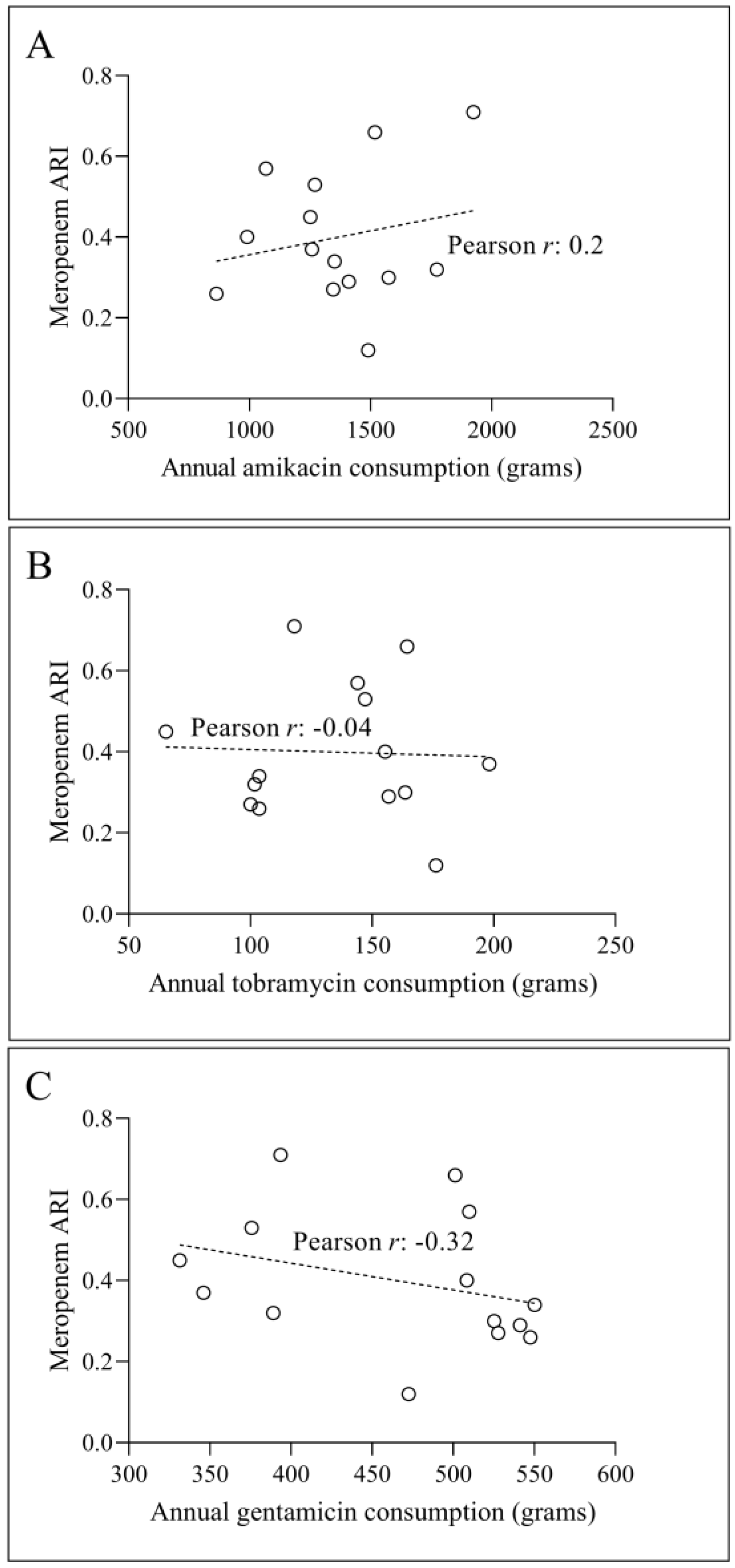
Figure 12.
Correlation between annual aminoglycoside consumption and ARI meropenem in K. pneumoniae. (A) Pearson correlation between annual amikacin consumption (in grams) and ARI meropenem. (B) Correlation between annual tobramycin intake and meropenem ARI. (C) Pearson correlation between annual gentamicin use and meropenem ARI.
Figure 12.
Correlation between annual aminoglycoside consumption and ARI meropenem in K. pneumoniae. (A) Pearson correlation between annual amikacin consumption (in grams) and ARI meropenem. (B) Correlation between annual tobramycin intake and meropenem ARI. (C) Pearson correlation between annual gentamicin use and meropenem ARI.
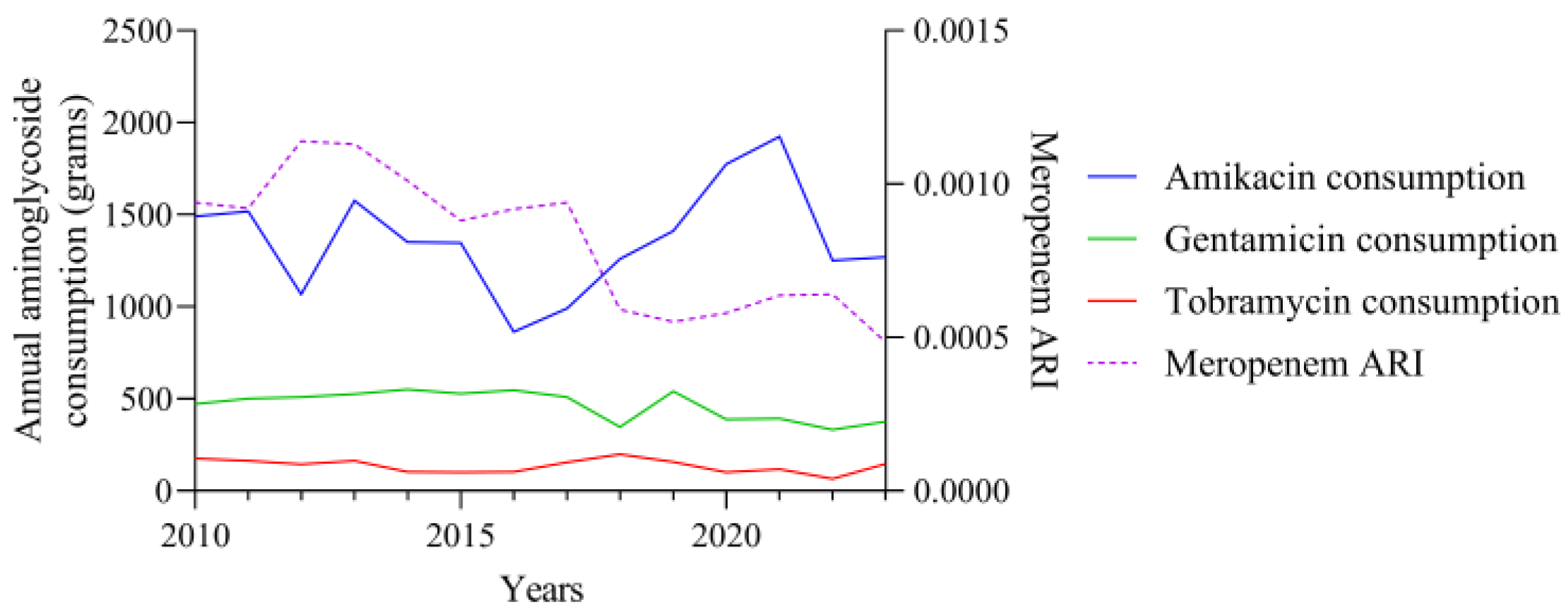
Figure 13.
Pearson correlation between annual consumption of amikacin (A), tobramycin (B), and gentamicin (C) and meropenem ARI in K. pneumoniae.
Figure 13.
Pearson correlation between annual consumption of amikacin (A), tobramycin (B), and gentamicin (C) and meropenem ARI in K. pneumoniae.
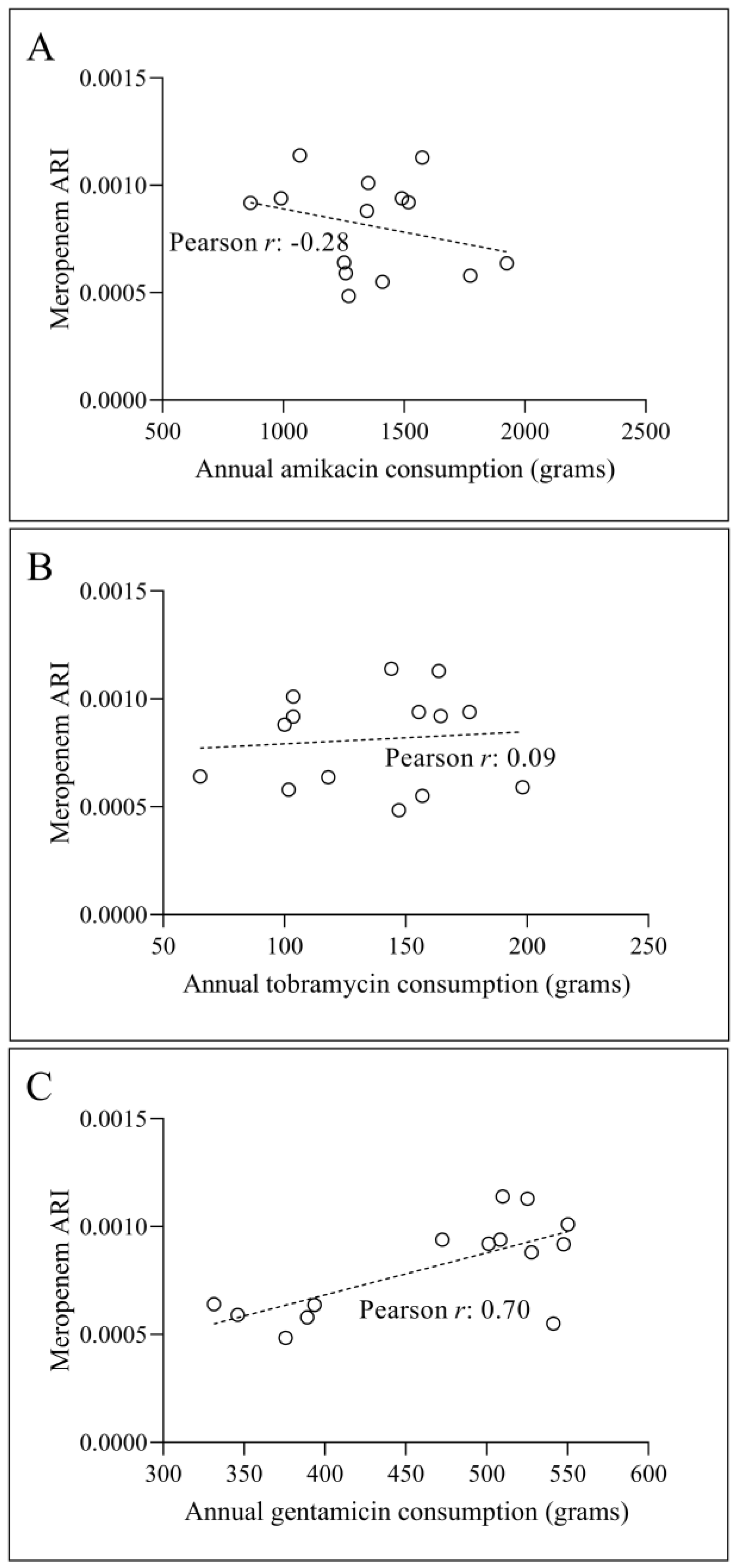
Figure 14.
Pearson correlation between annual consumption of amikacin (A), tobramycin (B) and gentamicin (C) consumption (grams) and ARI of meropenem with one-year-lag in A. baumannii.
Figure 14.
Pearson correlation between annual consumption of amikacin (A), tobramycin (B) and gentamicin (C) consumption (grams) and ARI of meropenem with one-year-lag in A. baumannii.
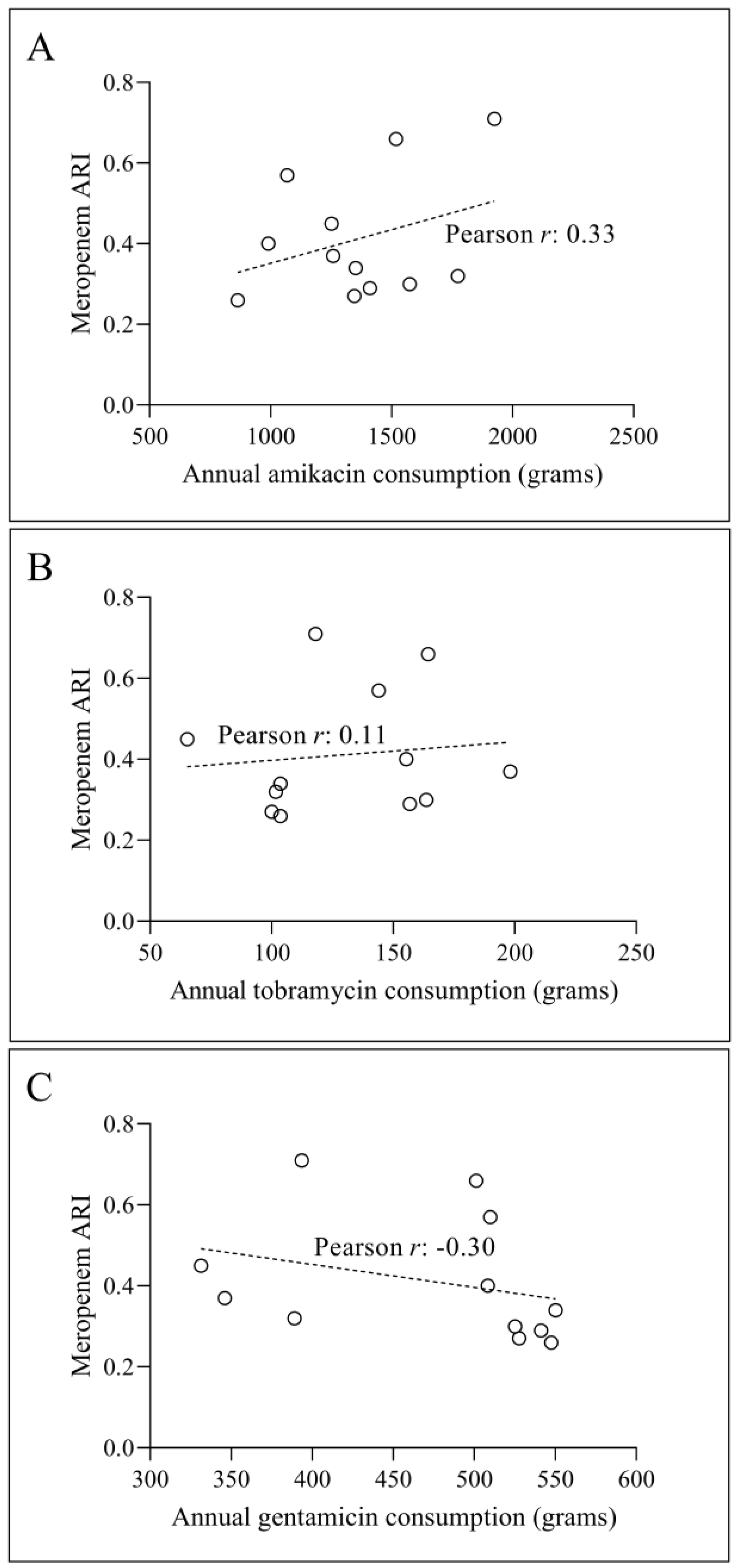
Figure 15.
Pearson correlation between annual consumption of amikacin (A), tobramycin (B), and gentamicin (C) (grams) and meropenem ARI with lag of one year in K. pneumoniae.
Figure 15.
Pearson correlation between annual consumption of amikacin (A), tobramycin (B), and gentamicin (C) (grams) and meropenem ARI with lag of one year in K. pneumoniae.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



