
Submitted:
12 July 2024
Posted:
15 July 2024
You are already at the latest version
Abstract
Background and Aims: Obesity is a pervasive health issue in children. It affects multiple systems in the body including the gastrointestinal tract. Research on obesity-related gastrointestinal diseases has focused mostly on hepatobiliary disorders. However, non-hepatic gastrointestinal diseases such as gastroesophageal reflux, constipation, and functional abdominal pain, though common and debilitating, have not been highlighted in the context of obesity. These entities can downgrade the already compromised lifestyle of obese children. Some of these disorders are more difficult to treat in these children compared to their peers with normal body mass index. Method: We reviewed the available literature on the association between obesity and these three common gastrointestinal disorders.
Results: - There appears to be a strong correlation between childhood obesity and constipation and gastroesophageal reflux, and a probable correlation with functional abdominal pain.
Conclusion: We suggest that given the available literature, weight management should be an integral part of the management of gastroesophageal reflux, constipation, and functional abdominal pain in obese children. This gains relevance especially because of the recent availability of medications for the treatment of obesity in children.
Keywords:
children
; obesity
; constipation
; gastroesophageal reflux
; recurrent abdominal pain
1. Introduction:
Childhood obesity has reached endemic proportions. Worldwide, the number of overweight children has nearly tripled over the last 4 decades. Currently, over 340 million children and adolescents aged 5-19 years are classified as either obese or overweight [1]. In the United States alone, about 14.7 million children and adolescents aged 2-19 years are overweight with a prevalence rate of 19.7% [2]. Obesity causes major morbidity in children such as type-2 diabetes mellitus, cardiovascular diseases, asthma, stroke, obstructive sleep apnea, etc [3]. It also affects the quality of life and is associated with social and psychological problems such as depression, lowered self-esteem, etc. Studies have shown that childhood obesity is an important determinant of adult obesity and obesity-related co-morbidities and complications in later life [4].
Studies of obesity-related gastrointestinal morbidities have mostly focussed on Metabolic Disorders associated Steatotic liver disease (formerly known as NAFLD), Metabolic Disorder associated Steatohepatitis (formerly known as NASH), and cholelithiasis [5]. Emerging data indicate that pediatric obesity is also associated with other major gastrointestinal diseases such as constipation, gastroesophageal reflux and functional abdominal pain [6,7]. Such associations have not been emphasized enough in the pediatric literature. Recognition of this association and including weight management in the treatment protocol may help improve the overall outcome in these children.
The objective of this review is to discuss the known literature on the association of pediatric obesity with constipation, gastroesophageal reflux, and functional abdominal pain along with the pathophysiology. We hope to help the clinician recognize and use this association in their daily practice.
To highlight the recent developments and future direction of research, we have included a paragraph on microbiome in each section.
2. Method:
Ovid® and Pub Med® databases were queried with keywords such as ‘Reflux’ and phrases such as ‘Constipation AND Obesity’ with filters such as ‘Children’, ‘Adolescents’ etc as necessary. Bibliography of the key papers was also scanned for appropriate references. The relevant papers were reviewed and findings included in this article.
2.1. Obesity and Functional Constipation:
Functional constipation (FC) is one of the most prevalent gastrointestinal disorders reported in adults and children worldwide [8]. The reported prevalence of FC ranges between 0.5% to 32.2% among the pediatric population, with a pooled prevalence of 9.5% (95% CI, 7.5-12.1%) [9]. With abdominal pain(in as high as 47.5% [10]) and fecal incontinence. FC further degrades an already compromised lifestyle in obese children.
The available literature on obesity and FC is contradictory at first glance. FC has been reported to be the most common GI-related morbidity in obese children [11]. It was reported in 23% of obese children, compared to 8.9% in the general population [12]. When compared to the age and sex-matched healthy controls, there was a preponderance of constipation among the obese children (21% versus 1%) [13]. Such association was consistent with the findings (18.44% versus 7.82%) of another clinic-based Italian study [14]. A US-based study reported that obesity increased the risk of developing constipation in children by almost 2-folds (odds’ ratio1.83, p-value 0.01) [15]. In a retrospective observational study on children referred to the sub-speciality clinic for functional constipation, we observed a significantly higher number of overweight children among the constipation group than the control group (p-value <0.05) [16]. Another study on children referred to a pediatric gastroenterology clinic reported a higher prevalence of obesity in constipated children (22.7% versus 11.7%) than the controls (p-value <0.001) [17]. A prospective clinic-based case-control study also observed a higher obesity rate (8%) in constipated children [11]. Similar results were reported from outside Europe and North America as well. A study from India on 186 children reported obesity in 23.66% of cases with functional constipation. Encopresis with constipation was significantly higher among the obese children (88.64%, p<0.0001) [18].
On the other hand, two school-based studies from Columbia (N=2820) and Brazil (N=1077), did not document increased incidence of constipation in obese children (Obese/control; Columbia 14.9%/12.9%, p=0.73; Brazil 19.4%, 18%, p=0.76) [19,20]. Another study from the Netherlands (N=2420) found no significant increase in the incidence of obesity among children with constipation (OR 1.01; 95% CI: 0.69-1.46) compared to those with normal weight [21].
Figure 1.
Constipation and Obesity in Children.

On close analysis, it appears that while most of the clinic-based studies reported an association between obesity and constipation, community-based studies refuted such claims (Figure -1). We reviewed the charts of 955 children in the primary care clinic. [22] We concluded that there was no association between constipation and obesity in the community setting. But obese children with constipation were 3 times more likely to be referred to the subspecialty clinic, for apparent treatment failure. This may explain the preponderance of obesity among constipated children in clinic-based studies. A prospective study is warranted to test this hypothesis as weight management may be another non-pharmacological tool for treating constipation.
Several mechanisms have been proposed as the causes of both constipation and obesity. High carbohydrate, low-fiber diet and a sedentary lifestyle are associated with both obesity and constipation [21].A study on middle-aged post-menopausal women found significant improvement in constipation symptoms and quality of life after 12 weeks of increased physical activity and low-calorie diet intake [23]. The “ileal break” concept, where a high-fat diet slows down intestinal motility and causes constipation in obese adults, has been proposed [24]. However, a study involving morbidly obese children didn’t find any difference between the diet of children with or without constipation, including fiber and fat intake [13].
Daily exercise enhances colonic motility and accelerates gut peristalsis by stimulating the vagus nerve, increasing gut blood flow, and augmenting the release of GI hormones. Gut hormones like ghrelin and motilin take a pivotal role in the pathogenesis of constipation in overweight persons. Ghrelin, a “hunger hormone”, augments initiation of the migrating motor complex in the stomach, and stimulates gastrointestinal motility [25]. In obese children, lower serum concentrations of ghrelin may contribute to decreased gut motility, which, in turn, causes constipation. Fat intake potentiates increased release of Glucagon-like peptide-1, 2 (GLP-1, GLP-2), cholecystokinin (CCK), and inhibition of peptide YY (PYY), which leads to constipation by colonic smooth muscle relaxation. Obesity mediates tumor necrosis factor-alpha (TNF-a), IL-1, IL-6, and toll-like receptor (TLR) signalling, which are responsible for immunoinflammation [26]. It causes morphological changes in the interstitial cells of Cajal of the enteric nervous system and impairs the contractile function of intestinal smooth muscles.
Finally, psychosocial and behavioral abnormalities are postulated to play important roles in the co-occurrence of obesity and FC. Children with obesity have a 43% higher risk of anxiety and depression than the general population (p<0.0001). Moreover, obesity makes children and adolescents more vulnerable to having low self-esteem (risk estimate 1.53; 95% CI: 1.16-2.02; p=0.003) and body dissatisfaction (risk estimate 4.05; 95% CI: 2.34-7.023; p=0.0001) [27]. On the other hand, studies have identified childhood constipation as a potential risk factor for depression, attention difficulties, and poor school performance. Though there is little direct evidence identifying depression as a connecting bridge between constipation and obesity, we reported an increased incidence of psychological and behavioral problems in the group of overweight children with treatment-resistant chronic constipation [22]. A correlation between increased body weight and psychological stress [28]. Chronic stressful condition increases catecholamine production, especially epinephrine (E) and norepinephrine (NE). Both of these catecholamines affect GI blood flow, causes beta-receptor mediated GI smooth muscle relaxation, and ultimately, alter GI motility and increase GI transit time [24]. Additionally, stress releases cortisol by increasing corticotrophin releasing factor (CRF) and adrenocorticotropic hormone (ACTH). Cortisol increases plasma zinc concentration, which augments secretion of CCK, an inhibitor of colonic contraction. Weight reduction interventions might help in reduction of emotional stress, anxiety, poor self-esteem and thus augment the overall emotional and psychological well-being.
Gut microbiota is believed to hold the secrets of many human ailments. Disruption of gut microbiota, or dysbiosis, deranges the homeostasis between the ‘good’ and ‘bad’ bacteria of the colon and results in disease states. The role of the microbiome in obesity was dramatically revealed when a lean person became overweight after receiving fecal transplant from an obese donor [29]. At this point, research mostly focuses on changes in the composition of gut microbiota that can alter the energy metabolism and develop obesity [30]. In both mono and dizygotic twins studies, there were fewer Bacteroides (p=0.003), and abundant Actinobacteria(p=0.002) in the obese sibling [30]. It has been further suggested in mice studies, that alteration in gut microbiota affects the efficiency of energy harvest from diet, along with utilization and storage of the calories, causing differences in weight gain. Similarly, studies have suggested the involvement of gut microbiota in the development of constipation in obese children. A cross-sectional study examined the stool samples of children using rRNA gene pyrosequencing and found that the fecal microbiota of constipated obese children had decreased representation of Prevotella and abundance of genera of Firmicutes spp. compared with the non-constipated obese controls [31].Those with early insults to the gut microbiome due to necrotizing enterocolitis, sepsis, delayed enteral feeding, and other perinatal events were at greater risk of developing FC in later life [32]. These studies suggest that gut microbial population of constipated children contains less amount of Prevonella compared to healthy children. Increased levels Proteobacteria sp, Bacteroides sp., Parabacteroides sp., and Bifidobacterium longum, and decreased Alistipesfinegoldii and Ruminococcusspas were found in stool samples of children with intractable constipation.
Over the counter probiotic combinations have gained popularity for treatment of FC without any scientific proof of efficacy. From the scanty evidence available from the literature, probiotic supplements containing Prevotella and L.rhamnosus strains are more likely to be effective than the random mix of probiotics available over the counter.
3. In Summary:
It appears that obese children are more likely to have treatment-resistant constipation. Incorporating weight management strategies in the treatment protocol may help resolve constipation in these children. This strategy can improve the quality of life of these children as well. Large randomized studies are warranted to study the practical implications of weight management measures in treating childhood constipation.
3.1. Obesity and Gastro-Esophageal Reflux:
Gastroesophageal reflux (GER) is common. About 60% of the population have reflux symptoms at least once a year, 20-30% once a week [33]. Almost all premature babies and most newborns have 2-3 reflux episodes per hour. It is a clinical diagnosis, and symptoms, such as heartburn, upper abdominal pain, food regurgitation, and retching are common in pediatric primary care settings. Montreal Definition and Classification provides the clinical framework for diagnosing gastroesophageal reflux disease (GERD).
The association between obesity and GER is well-established in adults. A higher body mass index (BMI) is considered a risk factor for GER in adult population. A meta-analysis of 30 adult studies published over 60 years found a significant association between high BMI and GER symptoms. Risk of GER was significantly higher (odds ratio1.89, 95% CI: 1.70-2.09) among the obese adults compared to their non-obese peers [34]. Obesity is a well-known risk factor for complications of GERD, like reflux esophagitis and Barrett’s esophagus. An association between abdominal obesity and esophageal adenocarcinoma has been reported [35].
Pediatric studies, though sparser, support the association [Figure 2]. In a questionnaire-based study on children, obesity was significantly higher in boys with GERD (24.7% versus 16.7%, p=0.003) [36]. Another hospital-based study reported that obesity was more prevalent in children with GERD compared to controls (p<0.001) [11]. A higher prevalence of GER symptoms in obese children has been reported in questionnaire-based studies from the USA [37], Norway [38]and Italy [39]. One of these studies found abdominal obesity as a risk factor for developing GER symptoms (62% versus 24%, p<0.005) and higher reflux symptoms score (average scores 3.1 versus 0.84, p-value <0.005) [39]. The only population-based large-scale cross-sectional study showed moderate to extremely obese children between the age group 6-19 years were more likely to have GERD (odds ratio 1.16, 95% CI: 1.07-1.25), than children with normal BMI [40]. Overall 20.9-38% of children with obesity had at least one symptom of GI reflux across various studies [41]. Epigastric pain and regurgitation were the most frequent symptoms reported [37,39]. Some studies report that the risk and severity of reflux is directly proportional to BMI-Z score, irrespective of the child being obese [37,39].
However, when biopsy-proven reflux esophagitis was the diagnostic criteria for GERD, association with obesity disappeared. In a chart review of 738 children, obesity or overweight wasn’t found to be an independent risk factor (p= 0.098) [42]. Similarly, two other studies failed to establish a relationship between obesity and microscopic features of reflux esophagitis [43,44]. This may be due to selection bias as only severe or long-lasting cases are usually selected for endoscopy. Even then, only 20% of children with GERD symptoms had reflux esophagitis by endoscopic evaluation [36]. Histological changes of esophageal mucosa occur over a period of time; therefore, erosive esophagitis becomes more prevalent with advancing age. Only 12% of children suffering from symptomatic GER develop esophagitis by 21 years of age [45].
These findings lead to the next logical question of whether weight management can be a primary or ancillary non-pharmacological treatment of childhood reflux disease. Unfortunately, this issue has not been addressed in the pediatric literature. In adults, 65% of obese patients had complete resolution of GER symptoms after a structured weight loss program in an interventional trial [46]. Dietary and lifestyle modifications led to symptomatic relief in another group of patients with GERD [47]. A significant correlation between the degree of weight loss and reduction of GER symptom scores was also seen in other adult studies [46] [Figure 3]. Such studies are highly desirable in the pediatric population to evaluate weight management as another facet of the management of GERD in children.
GER is caused by the inappropriate transient relaxation of the lower esophageal sphincters (TLESRs). Factors contributing to obesity, such as increased dietary fat intake (p=0.017), smoking, and alcohol use (p=0.038) are found to be potential causes of both GERD symptoms and esophageal erosion in adults. Decreased gastric emptying time (GET) is another cause of GERD as it increases gastric acid secretion, increases gastric volume, and thus increases the gastroesophageal pressure gradient, increasing the odds of GER [48]. Among children, increased fatty acid consumption causes delayed emptying causing reflux symptoms [14]. A study showed direct relationship between waist circumferences, a surrogate for visceral adiposity, with GET. Symptomatic obese GER patients had a longer GET than their asymptomatic peers [49]. Feeding habits may also contribute to GER in obese children. Large amount of food intake in a short span of time may overwhelm the gastric accommodation capacity and increase intraluminal pressure leading to reflux symptoms [14,49]. Increased abdominal fat may increase intragastric pressure, interrupting the anti-reflux mechanisms of the lower esophagus [50]. Recent studies have also focussed on roles of pro-inflammatory cytokines such as TNF alpha, IL-1 beta, IL-6 produced by M1 macrophages and mature adipocytes. Interaction between adipokines like leptin and adiponectin is also being investigated as a causal factor for the disrupted esophageal mucosal barrier in adults.
Recently, studies based on genomic sequencing have focussed on the role of esophageal microbiome (EM) in GERD. Some investigators have put more emphasis on microbial dysbiosis than gastric acid secretion in the development of esophageal mucosal diseases in adults. Various factors like, age, diet, uses of antibiotics and other medications, oral hygiene, smoking etc. can disrupt the esophageal microbiome (EM). It results in persistent esophageal dysbiosis which generates a host of immunogenic response, which ultimately propagates the inflammatory cascade. Researchers have evidence that non-erosive reflux disease is associated with a shift of EM away from Fusobacteria, Actinobacter spp. towards Proteobacteria and bacteroidetes. This novel insight into EM opens further research options to study the aetiological role of esophageal microbiome in obesity and GERD.
4. In Summary
Unlike adults, the association between high BMI and GER symptoms has not been firmly established in children. However, sufficient evidence exist to suggest that such an association exists and that older obese children are more likely to have GER symptoms. More prospective pediatric studies are needed to establish the cause-and-effect relationship between the two. However, clinically, it may be wise to include weight management in the treatment regimen for GERD in obese children.
4.1. Obesity and Functional Abdominal Pain (FAP):
Functional abdominal pain syndrome (FAPS), may account for as much as 50% of all pediatric gastrointestinal clinic visits. Globally the prevalence of childhood functional abdominal pain is estimated to be around 15% [51]. It is defined by the latest Rome criteria, as a disorder of gut-brain interaction (DGBI) in children. FAP is more common in children older than 12 years (12.9% versus 13.8%). Its impact on the child and the family is highlighted by the fact that 80.5% of children with RAP reported missing school with a significant decline in quality of life [52].
There are few studies on FAP and obesity in children. In a cross-sectional school survey study with a validated questionnaire and Wong-Bakes FACES scale for FAP. FAP was significantly more frequent in obese children than in the control group (odds ratio 1.8, p-value 0.01) [53]. Every third of obese children reported abdominal pain. Similarly, obese children had more than a 2-fold increased risk of developing FAPS(odds’ ratio 2.1; p-value 0.007) [15].
A pediatric gastrointestinal clinic-based study showed that obesity was more prevalent (39.5% versus 30%, p-value 0.04) in adolescents with FAPS compared to healthy controls [41]. Obese children with FAP were older and were more likely to be hospitalized for FAP. Another pediatric study revealed a predominance of obesity among those diagnosed with FAP (16.2%, p-value 0.023 [11]). A small number of studies have refuted such findings. A study of 114 obese children showed no difference in the incidence of FAP, compared to the normal-weight children (2.60% versus 1.94%, p=1.00) [14,54]. Overall, the preponderance of evidence favors an association between FAP and obesity.
Various hypotheses have been postulated to explain how obesity can cause FAP. Dietary habit is considered the most likely connection between obesity and abdominal pain. Evidence suggest that a diet containing fermentable oligo-, di-, and monosaccharides and polyols (FODMAP) may precipitate gastrointestinal symptoms in patients with FAP [55]. These types of diet can cause weight gain as well. There are a few reports showing restriction of short chain carbohydrates and a low FODMAP diet offer significant symptom relief in adult patients, but no conclusive data is available in the pediatric population [56]. One pediatric study found an inverse relationship between fruit consumption and FAP prevalence [53]. Both obesity and low fruit consumption were found to be independent risk factors for FAP.
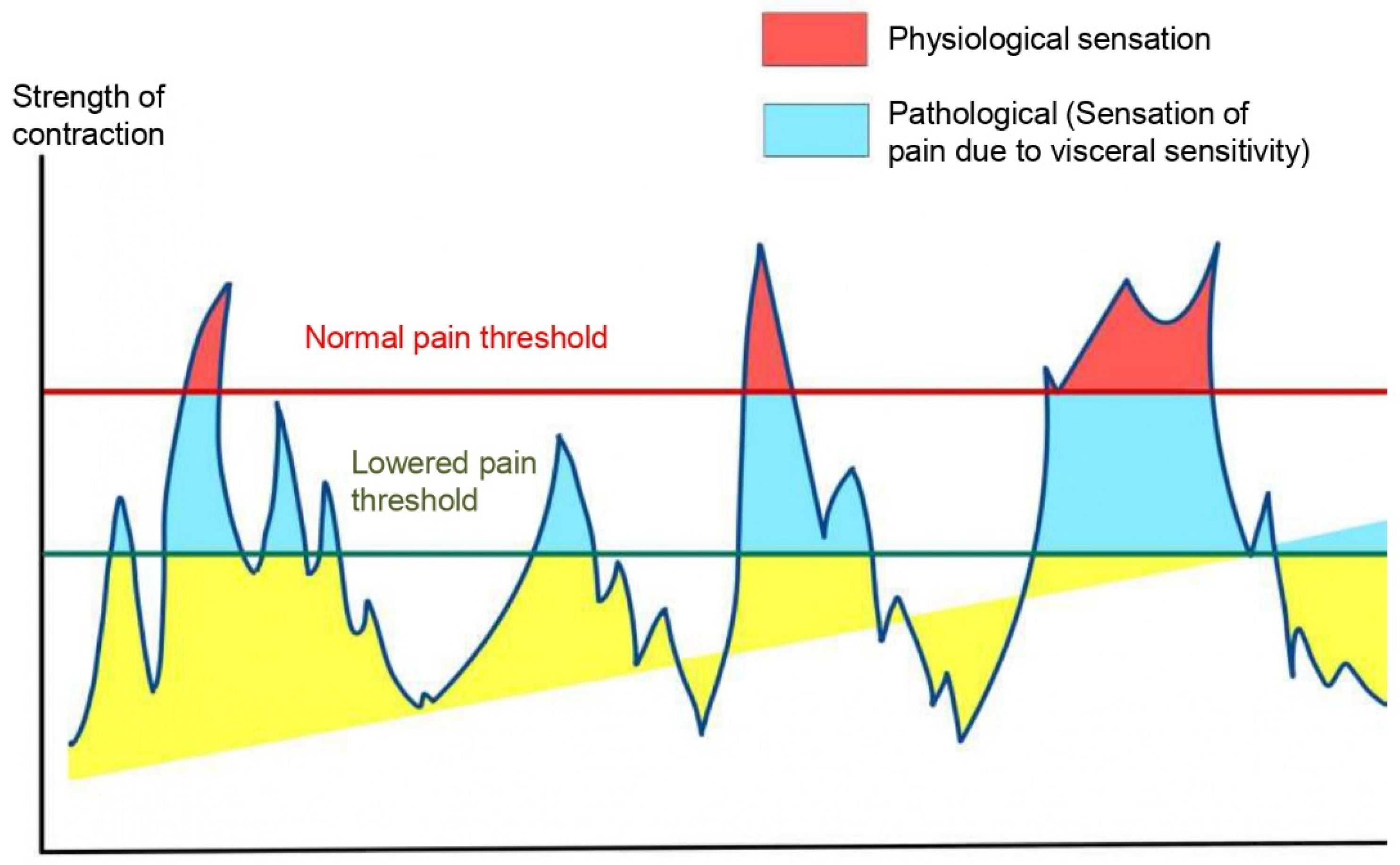
Visceral hypersensitivity, where the threshold of perception of pain is reduced, has been proposed to be the cause of co-existence of FAP and obesity [57] [Figure 4]. Hyperalgesia leads to the perception of pain even with physiological contractions of the gut. It is thought that obesity-induced inflammatory factors enhance pain perception of intestinal signals at CNS level. This hyperexcitability ultimately leads to abnormal bowel movement and chronic abdominal pain. Obesity, with associated low-grade chronic inflammation, causes dysregulation of gut-brain axis [58]. This non-infective, chronic persistent inflammation is caused by the low-grade synthesis of inflammatory mediators in the adipose tissues. These inflammatory mediators (adiponectin, TNF, IL-1, IL-6, leptin, resistin etc) induce neuroinflammation by activating free nerve endings and inducing pain-causing biological substances. Intestinal hyperpermeability and vitamin D deficiencies are other contributing factors that can enhance central pain perception via the gut-brain axis and increase the risk of chronic recurrent abdominal pain in the obese population [57].
The microbiome-gut-brain axis is the emerging concept explaining the shared biological mechanism between abdominal pain and obesity [59]. As discussed earlier, alteration of gut microbial diversity is evident in both children and adults with obesity compared to healthy ones [57]. Similarly, alteration of colonic bacterial flora, especially reduction in levels of beneficial bacteria like the actinobacteria, bifidobacteria in stool samples has been documented in patients with FAPS [60]. Both Lactobacillus and Bifidobacterium infantis are reported to downregulate T-helper cell response to provide an anti-inflammatory effect to the gut mucosa and cause symptomatic relief from abdominal pain. A randomized controlled trial with Bifidobacterium infantis, B. breve and B. Longum reported resolution of abdominal pain in a significantly higher proportion of children (p=0.006) [61]. Conversely, microbial metabolites of pathogenic bacteria, such as protease and serotonin, activate sub-mucosal nerve endings and induce pain in adults. Despite having significant roles in both obesity and FAP, till now no study or trial has been conducted to assert a direct causal association between obesity and FAP about gut microbial dysbiosis. Moreover, almost all the studies studying the probable shared pathophysiology were among adults and irritable bowel syndrome. There is a knowledge gap to connect obesity and FAP in children.
5. In Summary:
The available studies don’t establish a definite causal relation between FAP and obesity in children. No study investigating the direct role of weight loss in relieving functional abdominal pain is available in the literature. Non-pharmacological measures like dietary modification and exercise had been shown to improve symptoms of FAP, which indirectly causes weight loss. Therefore, a common-sense approach of including weight-reducing interventions for treating childhood FAP with obesity may be indicated.
Funding/Support
No funding was secured for this study.
Data availability
Will not be available. But all references are provided.
Conflicts of Interest Disclosures (includes financial disclosures)
The authors have no conflicts of interest or financial interest to disclose.
Abbreviations:
| ACTH | Adrenocorticotrophic Hormone. |
| BMI | Body Mass Index. |
| CCK | Cholecystokinin. |
| CRF | Corticotrophin Releasing Factor. |
| EM | Esophageal microbiome |
| FAPS | Funcronal Abdominal Pain Syndrome. |
| FC | Functional Constipation. |
| FODMAP | Fermentable Oligo-, Di-, and Monosaccharides and Polyols |
| GER | Gastroesophageal Reflux |
| GERD | Gastroesophageal Reflux Disease |
| GET | Gastric Emptying Time. |
| GI | Gastrointestinal. |
| GLP | Glucagon Like Peptide |
| IL | Interleukin |
| OR | Odds Ratio |
| PYY | Peptide YY |
| TLESR | Transient Lower Esophageal Sphincter Relaxation |
| TNF | Tumor Necrosis Factor |
References
- World Health Organization. Obesity and overweight. 2021 Jun; Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
- Bryan S, Afful J, Carroll M, Te-Ching C, Orlando D, Fink S, et al. NHSR 158. National Health and Nutrition Examination Survey 2017–March 2020 Pre-pandemic Data Files [Internet]. National Center for Health Statistics (U.S.); 2021 Jun [cited 2023 Jul 22]. Available from: https://stacks.cdc.gov/view/cdc/106273.
- Smith JD, Fu E, Kobayashi MA. Prevention and Management of Childhood Obesity and Its Psychological and Health Comorbidities. Annu Rev Clin Psychol. 2020 May 7;16(1):351–78. [CrossRef] [PubMed]
- The GBD 2015 Obesity Collaborators. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N Engl J Med. 2017 Jul 6;377(1):13–27. [CrossRef]
- Huang JS, Barlow SE, Quiros-Tejeira RE, Scheimann A, Skelton J, Suskind D, et al. Childhood obesity for pediatric gastroenterologists. J Pediatr Gastroenterol Nutr. 2013 Jan;56(1):99–109. [CrossRef]
- Ho W, Spiegel BMR. The relationship between obesity and functional gastrointestinal disorders: causation, association, or neither? Gastroenterol Hepatol. 2008 Aug;4(8):572–8. [PubMed]
- Phatak UP, Pashankar DS. Obesity and Gastrointestinal Disorders in Children. J Pediatr Gastroenterol Nutr. 2015 Apr;60(4):441–5. [CrossRef]
- Silveira EA, Santos AS e A de C, Ribeiro JN, Noll M, dos Santos Rodrigues AP, de Oliveira C. Prevalence of constipation in adults with obesity class II and III and associated factors. BMC Gastroenterol. 2021 Dec;21(1):217. [CrossRef] [PubMed]
- Koppen IJN, Vriesman MH, Saps M, Rajindrajith S, Shi X, van Etten-Jamaludin FS, et al. Prevalence of Functional Defecation Disorders in Children: A Systematic Review and Meta-Analysis. J Pediatr. 2018 Jul;198:121-130.e6. [CrossRef] [PubMed]
- Kumar K, Gupta N, Malhotra S, Sibal A. Functional constipation: A common and often overlooked cause for abdominal pain in children. Indian J Gastroenterol. 2023 Apr;42(2):274–8. [CrossRef] [PubMed]
- Teitelbaum JE, Sinha P, Micale M, Yeung S, Jaeger J. Obesity is Related to Multiple Functional Abdominal Diseases. J Pediatr. 2009 Mar;154(3):444–6. [CrossRef] [PubMed]
- Fishman L, Lenders C, Fortunato C, Noonan C, Nurko S. Increased prevalence of constipation and fecal soiling in a population of obese children. J Pediatr. 2004 Aug;145(2):253–4. [CrossRef]
- Baan-Slootweg OH, Liem O, Bekkali N, van Aalderen WM, Rijcken THP, Di Lorenzo C, et al. Constipation and Colonic Transit Times in Children with Morbid Obesity. J Pediatr Gastroenterol Nutr. 2011 Apr;52(4):442–5. [CrossRef]
- Tambucci R, Quitadamo P, Ambrosi M, De Angelis P, Angelino G, Stagi S, et al. Association Between Obesity/Overweight and Functional Gastrointestinal Disorders in Children. J Pediatr Gastroenterol Nutr. 2019 Apr;68(4):517–20. [CrossRef]
- Phatak UP, Pashankar DS. Prevalence of functional gastrointestinal disorders in obese and overweight children. Int J Obes. 2014 Oct;38(10):1324–7. [CrossRef] [PubMed]
- Misra S, Lee A, Gensel K. Chronic Constipation in Overweight Children. J Parenter Enter Nutr. 2006 Mar;30(2):81–4. [CrossRef]
- Pashankar DS, Loening-Baucke V. Increased Prevalence of Obesity in Children With Functional Constipation Evaluated in an Academic Medical Center. Pediatrics. 2005 Sep 1;116(3):e377–80. [CrossRef]
- Kumar SS, Kumar SS, Shirley SA. Prevalence of overweight and obesity in children with functional constipation aged 6 to 12 years attending outpatient department in a tertiary care hospital at Tamil Nadu, India. Int J Contemp Pediatr. 2020 Nov 24;7(12):2359. [CrossRef]
- Koppen IJN, Velasco-Benítez CA, Benninga MA, Di Lorenzo C, Saps M. Is There an Association between Functional Constipation and Excessive Bodyweight in Children? J Pediatr. 2016 Apr;171:178-182.e1. [CrossRef]
- Costa ML, Oliveira JN, Tahan S, Morais MB. Overweight and constipation in adolescents. BMC Gastroenterol. 2011 Dec;11(1):40. [CrossRef]
- Kiefte-de Jong JC, De Vries JH, Escher JC, Jaddoe VWV, Hofman A, Raat H, et al. Role of dietary patterns, sedentary behaviour and overweight on the longitudinal development of childhood constipation: the Generation R study: Dietary patterns and constipation. Matern Child Nutr. 2013 Oct;9(4):511–23. [CrossRef]
- Misra S, Liaw A. Controversies on the relationship between increased body mass index and treatment-resistant chronic constipation in children. J Parenter Enter Nutr. 2022 Jul;46(5):1031–5. [CrossRef] [PubMed]
- Tantawy S, Kamel D, Abdel-Basset W, Elgohary H. Effects of a proposed physical activity and diet control to manage constipation in middle-aged obese women. Diabetes Metab Syndr Obes Targets Ther. 2017 Dec;Volume 10:513–9. [CrossRef]
- Miron I. Gastrointestinal Motility Disorders in Obesity. Acta Endocrinol Buchar. 2019;15(4):497–504. [CrossRef] [PubMed]
- Chen CY, Tsai CY. Ghrelin and Motilin in the Gastrointestinal System. Curr Pharm Des. 2012 Sep 2;18(31):4755–65. [CrossRef] [PubMed]
- Ding S, Lund PK. Role of intestinal inflammation as an early event in obesity and insulin resistance: Curr Opin Clin Nutr Metab Care. 2011 Jul;14(4):328–33. [CrossRef]
- Moradi M, Mozaffari H, Askari M, Azadbakht L. Association between overweight/obesity with depression, anxiety, low self-esteem, and body dissatisfaction in children and adolescents: a systematic review and meta-analysis of observational studies. Crit Rev Food Sci Nutr. 2022 Jan 19;62(2):555–70. [CrossRef] [PubMed]
- Moore CJ, Cunningham SA. Social Position, Psychological Stress, and Obesity: A Systematic Review. J Acad Nutr Diet. 2012 Apr;112(4):518–26. [CrossRef] [PubMed]
- Alang N, Kelly CR. Weight Gain After Fecal Microbiota Transplantation. Open Forum Infect Dis. 2015 Jan 1;2(1):ofv004. [CrossRef] [PubMed]
- Turnbaugh PJ, Hamady M, Yatsunenko T, Cantarel BL, Duncan A, Ley RE, et al. A core gut microbiome in obese and lean twins. Nature. 2009 Jan;457(7228):480–4. [CrossRef] [PubMed]
- Zhu L, Liu W, Alkhouri R, Baker RD, Bard JE, Quigley EM, et al. Structural changes in the gut microbiome of constipated patients. Physiol Genomics. 2014 Sep 15;46(18):679–86. [CrossRef] [PubMed]
- Vandenplas Y, Carnielli VP, Ksiazyk J, Luna MS, Migacheva N, Mosselmans JM, et al. Factors affecting early-life intestinal microbiota development. Nutrition. 2020 Oct;78:110812. [CrossRef]
- Zhao Y, Encinosa W. Gastroesophageal Reflux Disease (GERD) Hospitalizations in 1998 and 2005. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006 [cited 2023 Jul 25]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK56308/.
- Eslick GD. Gastrointestinal symptoms and obesity: a meta-analysis: GI symptoms and obesity. Obes Rev. 2012 May;13(5):469–79. [CrossRef]
- Cho JH, Shin CM, Han KD, Yoon H, Park YS, Kim N, et al. Abdominal obesity increases risk for esophageal cancer: a nationwide population-based cohort study of South Korea. J Gastroenterol. 2020 Mar;55(3):307–16. [CrossRef]
- Malaty H. Obesity and gastroesophageal reflux disease and gastroesophageal reflux symptoms in children. Clin Exp Gastroenterol. 2009 Mar;31. [CrossRef]
- Pashankar DS, Corbin Z, Shah SK, Caprio S. Increased Prevalence of Gastroesophageal Reflux Symptoms in Obese Children Evaluated in an Academic Medical Center. J Clin Gastroenterol. 2009 May;43(5):410–3. [CrossRef]
- Størdal K, Johannesdottir GB, Bentsen BS, Carlsen KCL, Sandvik L. Asthma and overweight are associated with symptoms of gastro-oesophageal reflux. Acta Paediatr. 2006 Oct 1;95(10):1197–201. [CrossRef] [PubMed]
- Quitadamo P, Buonavolontà R, Miele E, Masi P, Coccorullo P, Staiano A. Total and Abdominal Obesity Are Risk Factors for Gastroesophageal Reflux Symptoms in Children. J Pediatr Gastroenterol Nutr. 2012 Jul;55(1):72–5. [CrossRef]
- Koebnick C, Getahun D, Smith N, Porter AH, Der-Sarkissian JK, Jacobsen SJ. Extreme childhood obesity is associated with increased risk for gastroesophageal reflux disease in a large population-based study. Int J Pediatr Obes. 2011 Jun;6(2–2):e257–63. [CrossRef]
- Galai T, Moran-Lev H, Cohen S, Ben-Tov A, Levy D, Weintraub Y, et al. Higher prevalence of obesity among children with functional abdominal pain disorders. BMC Pediatr. 2020 May 6;20(1):193. [CrossRef]
- Elitsur Y, Dementieva Y, Elitsur R, Rewalt M. Obesity Is Not a Risk Factor in Children With Reflux Esophagitis: A Retrospective Analysis of 738 Children. Metab Syndr Relat Disord. 2009 Jun;7(3):211–4. [CrossRef] [PubMed]
- Patel NR, Ward MJ, Beneck D, Cunningham-Rundles S, Moon A. The Association between Childhood Overweight and Reflux Esophagitis. J Obes. 2010;2010:1–5. [CrossRef]
- Rabinowitz SS, Goli S, Xu J, Zhang X, Nicastri A, Anderson V, et al. Lack of correlation between obesity and gastroesophageal reflux disease (GERD) in a pediatric cohort. Open J Pediatr. 2013;03(04):317–23. [CrossRef]
- Yamasaki T, Hemond C, Eisa M, Ganocy S, Fass R. The Changing Epidemiology of Gastroesophageal Reflux Disease: Are Patients Getting Younger? J Neurogastroenterol Motil. 2018 Oct 1;24(4):559–69. [CrossRef] [PubMed]
- Singh M, Lee J, Gupta N, Gaddam S, Smith BK, Wani SB, et al. Weight loss can lead to resolution of gastroesophageal reflux disease symptoms: A prospective intervention trial. Obesity. 2013 Feb;21(2):284–90. [CrossRef]
- De Groot NL, Burgerhart JS, Van De Meeberg PC, De Vries DR, Smout AJPM, Siersema PD. Systematic review: the effects of conservative and surgical treatment for obesity on gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2009 Dec;30(11–12):1091–102. [CrossRef]
- Buckles DC, Sarosiek I, McCallum RW, McMillin C. Delayed Gastric Emptying in Gastroesophageal Reflux Disease: Reassessment with New Methods and Symptomatic Correlations. Am J Med Sci. 2004 Jan;327(1):1–4. [CrossRef]
- Quitadamo P, Zenzeri L, Mozzillo E, Cuccurullo I, Rocco A, Franzese A, et al. Gastric Emptying Time, Esophageal pH-Impedance Parameters, Quality of Life, and Gastrointestinal Comorbidity in Obese Children and Adolescents. J Pediatr. 2018 Mar;194:94–9. [CrossRef]
- Barak N, Ehrenpreis ED, Harrison JR, Sitrin MD. Gastro-oesophageal reflux disease in obesity: pathophysiological and therapeutic considerations. Obes Rev. 2002 Feb;3(1):9–15. [CrossRef]
- Herzlinger M, Cerezo C. Functional Abdominal Pain and Related Syndromes. Child Adolesc Psychiatr Clin N Am. 2018 Jan;27(1):15–26. [CrossRef] [PubMed]
- Korterink JJ, Diederen K, Benninga MA, Tabbers MM. Epidemiology of Pediatric Functional Abdominal Pain Disorders: A Meta-Analysis. Zhang L, editor. PLOS ONE. 2015 May 20;10(5):e0126982. [CrossRef] [PubMed]
- Malaty HM, Abudayyeh S, Fraley K, Graham DY, Gilger MA, Hollier DR. Recurrent abdominal pain in school children: effect of obesity and diet. Acta Paediatr. 2007 Apr;96(4):572–6. [CrossRef]
- Fifi AC, Velasco-Benitez C, Saps M. Functional Abdominal Pain and Nutritional Status of Children. A School-Based Study. Nutrients. 2020 Aug 24;12(9):2559. [CrossRef]
- Shepherd SJ, Lomer MCE, Gibson PR. Short-Chain Carbohydrates and Functional Gastrointestinal Disorders. Am J Gastroenterol. 2013 May;108(5):707–17. [CrossRef] [PubMed]
- Thomassen RA, Luque V, Assa A, Borrelli O, Broekaert I, Dolinsek J, et al. An ESPGHAN Position Paper on the Use of Low-FODMAP Diet in Pediatric Gastroenterology. J Pediatr Gastroenterol Nutr. 2022 Sep;75(3):356–68. [CrossRef]
- Yanping W, Gao X, Cheng Y, Liu M, Liao S, Zhou J, et al. The interaction between obesity and visceral hypersensitivity. J Gastroenterol Hepatol. 2023 Mar;38(3):370–7. [CrossRef] [PubMed]
- Lee SH, Kim KN, Kim KM, Joo NS. Irritable Bowel Syndrome May Be Associated with Elevated Alanine Aminotransferase and Metabolic Syndrome. Yonsei Med J. 2016;57(1):146. [CrossRef] [PubMed]
- Mayer EA, Savidge T, Shulman RJ. Brain–Gut Microbiome Interactions and Functional Bowel Disorders. Gastroenterology. 2014 May;146(6):1500–12. [CrossRef] [PubMed]
- Mars RAT, Yang Y, Ward T, Houtti M, Priya S, Lekatz HR, et al. Longitudinal Multi-omics Reveals Subset-Specific Mechanisms Underlying Irritable Bowel Syndrome. Cell. 2020 Nov;183(4):1137–40. [CrossRef]
- Giannetti E, Maglione M, Alessandrella A, Strisciuglio C, De Giovanni D, Campanozzi A, et al. A Mixture of 3 Bifidobacteria Decreases Abdominal Pain and Improves the Quality of Life in Children With Irritable Bowel Syndrome: A Multicenter, Randomized, Double-Blind, Placebo-Controlled, Crossover Trial. J Clin Gastroenterol. 2017 Jan;51(1):e5–10. [CrossRef]
Figure 2.
Gastroesophageal Reflux and Obesity in Children.
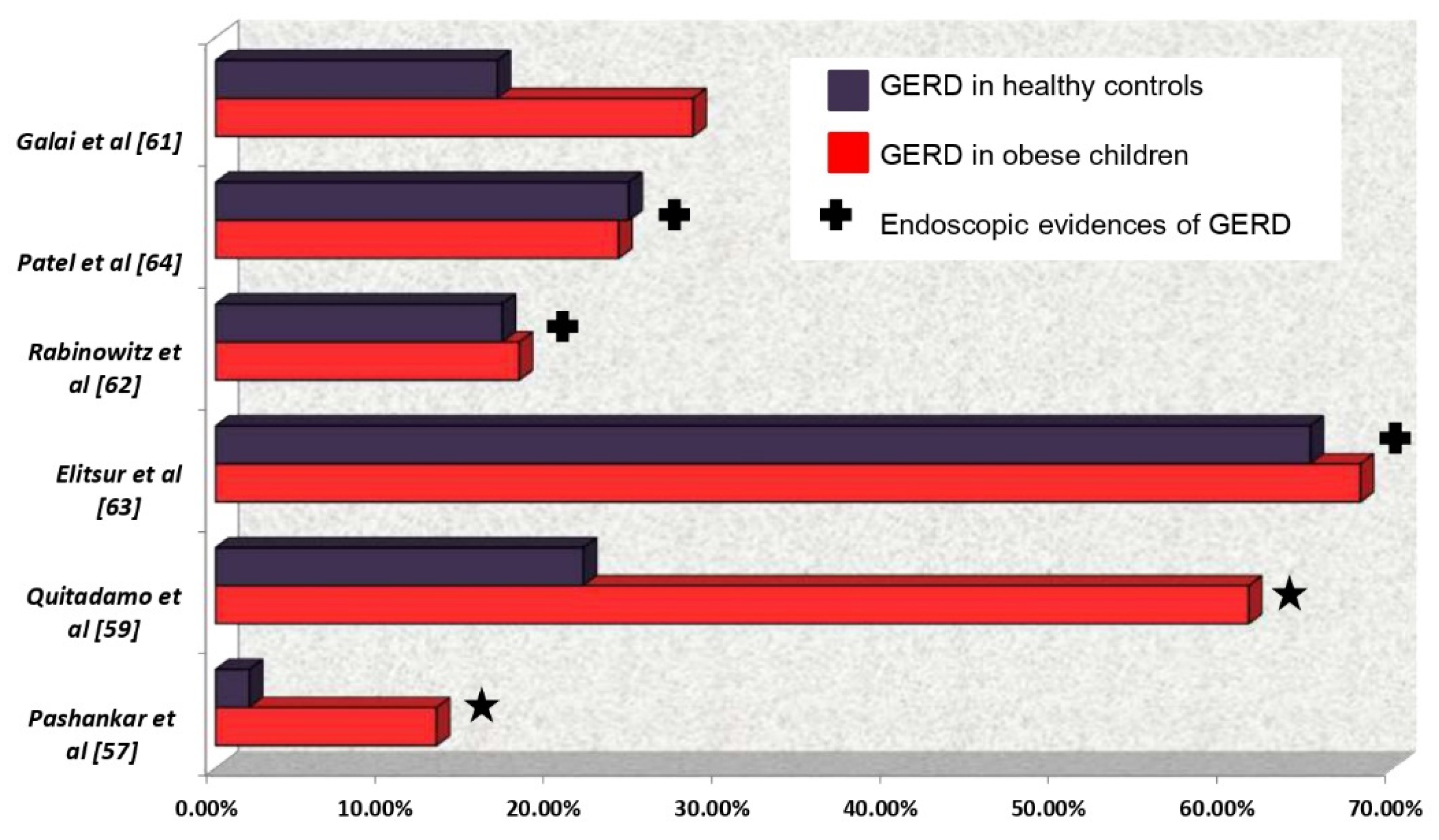
Figure 3.
Effect of weight management on GERD based on changes in GER symptom score and percentage (%) of adults with GERD.
Figure 3.
Effect of weight management on GERD based on changes in GER symptom score and percentage (%) of adults with GERD.
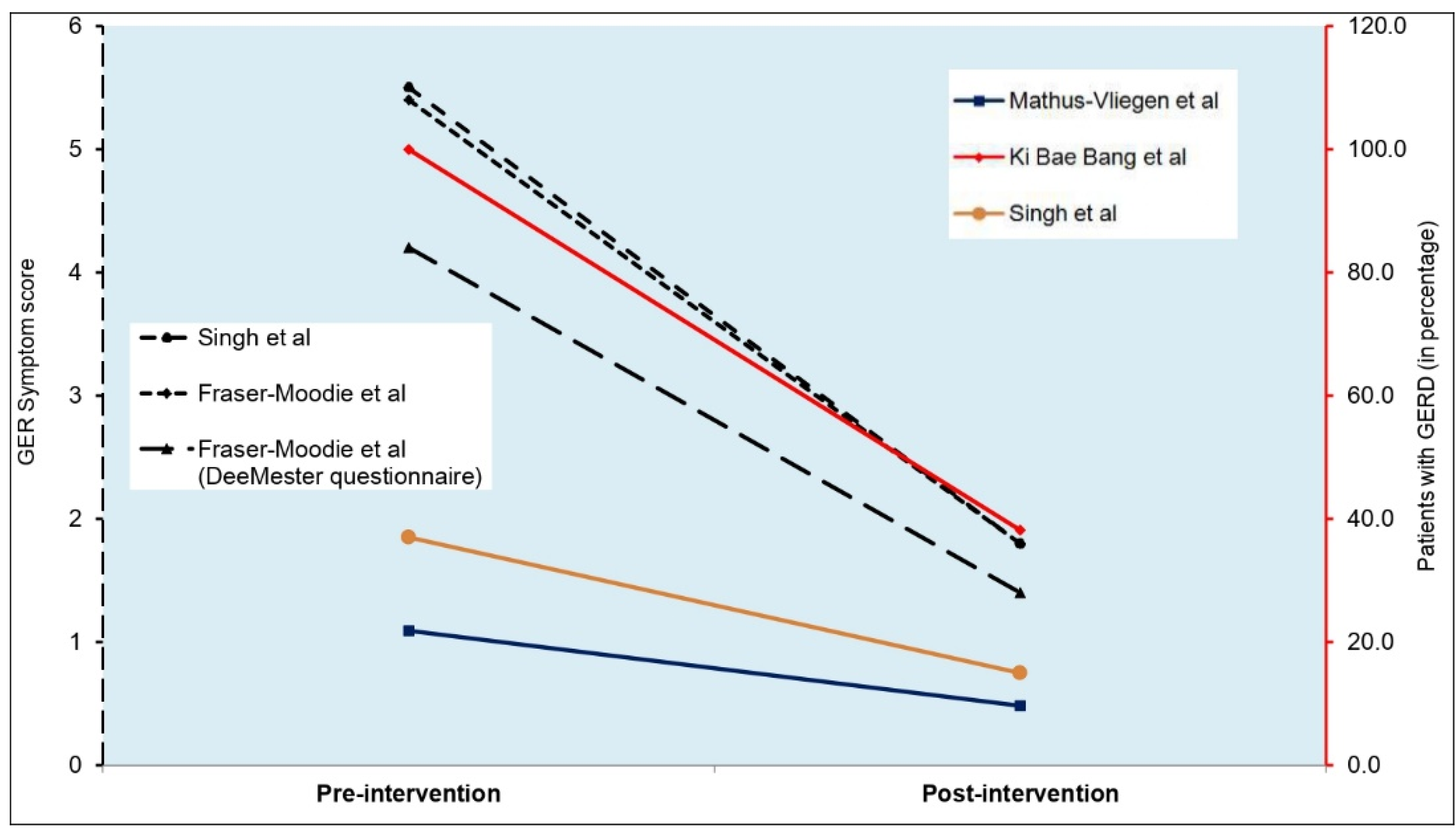
Figure 4.
Schematic Diagram of intestinal motility and visceral hyperalgesia.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



